Contemporary Management of Acute Type B Aortic Dissection
|
|
|
- Scott McKenzie
- 6 years ago
- Views:
Transcription


1 Contemporary Management of Acute Type B Aortic Dissection Bradley G. Leshnower MD Assistant Professor of Surgery Division of Cardiothoracic Surgery Emory University School of Medicine Georgia Vascular Society 5 th Annual Scientific Sessions September 9, 2017
2 Disclosures Medtronic: Speaker Cardiac Surgeon with Endovascular Skills
3 Acute Type B Aortic Dissection (atbad) Definitions Complicated Rupture Contained or Impending Periaortic hematoma Irregular aortic contour Malperfusion Clinical Absent pulse Claudication Acute renal failure with normal sized kidneys Radiographic Renal, Massive TL compression Morphologic evolution Rapid expansion in diameter Change in false lumen status Uncomplicated High risk features


4 Impending Rupture

5 Contained Rupture
6 atbad Definitions Complicated Rupture Contained or Impending Periaortic hematoma Irregular aortic contour Malperfusion Clinical Absent pulse Claudication Acute renal failure with normal sized kidneys Radiographic Renal Massive TL compression Morphologic evolution Rapid expansion in diameter Change in false lumen status Uncomplicated High risk uncomplicated


7 Radiographic Malperfusion Renal Massive TL compression
8 atbad Definitions Complicated Rupture Contained or Impending Periaortic hematoma Irregular aortic contour Malperfusion Clinical Absent pulse Claudication Acute renal failure with normal sized kidneys Radiographic Renal, Massive TL compression Morphologic evolution Rapid expansion in diameter Change in false lumen status Uncomplicated High risk uncomplicated
9 IRAD: Acute Type B Aortic Dissection (atbad) IRAD-All patients with the diagnosis of atbad Mortality at 3 years : 24.9% IRAD-Open Surgical Results for complicated atbad Overall In-Hospital Mortality: 29.3% Malperfusion: 27.8% Rupture: 62.5% Surgery < 48 hours: 39.2% Surgery > 48 hours: 18.1% LOS for survivors: 26 days Tsai TT, et al. N Engl J Med 2007:357: Trimarchi S, et al. Circulation 2006:114:I-357-I-364.

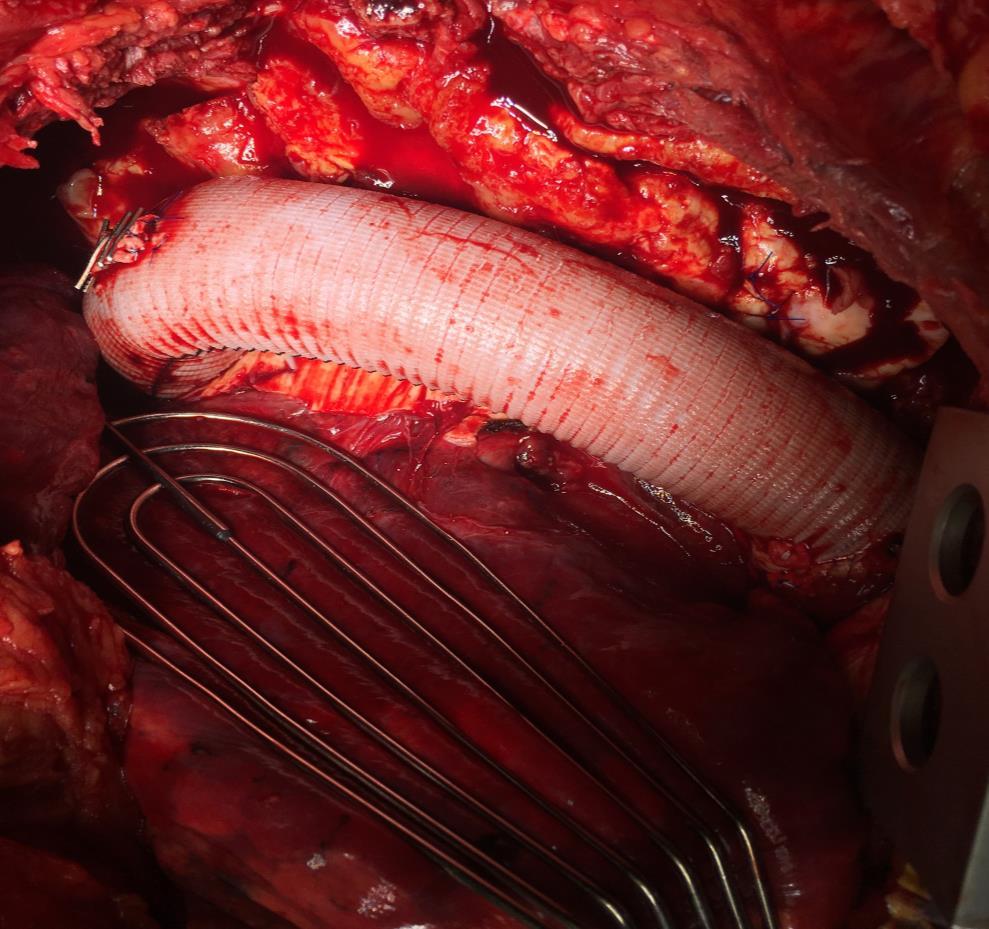
10 Open DTA repair in atbad

11 Principles of TEVAR in atbad Cover primary intimal tear Eliminate antegrade flow into the false lumen Expand true lumen to restore adequate inflow to the distal aorta Stent entire thoracic aorta if necessary
12 Aortic Remodeling in Type B Aortic Dissection Relocate the dissection flap back to its native position against the false lumen wall True Lumen Expansion False Lumen Thrombosis Obliteration

13 IVUS for TEVAR in atbad MANDATORY! Confirms True and False Lumen Identify Primary Intimal Tear Identify Large Secondary Thoracic Intimal Tears Aorta/branch vessel sizing Decreases contrast use

14 atbad and Malperfusion: 1. Cover primary tear site Algorithm 2. Evaluation and treatment of persistent malperfusion Measure femoral pressures IVUS/Aortograms Extend TEVAR to celiac Adjunctive stenting Celiac/SMA Renals Infrarenal stents Ileofemoral stents Open surgical revascularization

15 atbad and Rupture Must cover primary tear site Must cover site of rupture Be prepared to cover entire thoracic aorta from LCCA to celiac
16 TEVAR for Complicated atbad: Results
17 TEVAR for Complicated atbad PENN n=35 patients Indications: Rupture: 51.4% Malperfusion: 48.6% Distal Stenting Infrarenal Aorta: 11.4% Rena/Celiac: 11.4% Ileofemoral: 20% Ann Thorac Surg 2008;86:87-94
 Paraplegia Transient: n=2 (5.7%) Permanent: n=1 (2.8%) Renal Failure: n=1 (2.")
18 TEVAR for complicated atbad Mortality 30 day: n=1 (2.8%) 1 year: n=2 (5.7%) Morbidity CVA: n=1 (2.8%) Paraplegia Transient: n=2 (5.7%) Permanent: n=1 (2.8%) Renal Failure: n=1 (2.8%) TEVAR: Optimal therapy for complicated atbad Ann Thorac Surg 2008;86:87-94
19 Ann Thorac Surg 2017;103: EMORY TEVAR for Complicated atbad patients Mortality 30 day: 3.9% 1 year: 5.8% Morbidity CVA: 3.9% Transient Paraperesis: 5.9% Permanent Paraplegia: 0% Renal failure: 0% 11 reinterventions Open: n=6 Endovascular: n =5
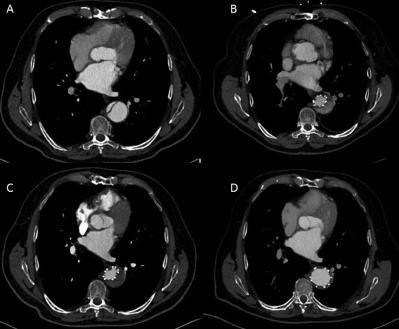
20 Aortic Remodeling with Extended TEVAR


21 Aortic Remodeling: TEVAR Induces Thoracic FL Thrombosis
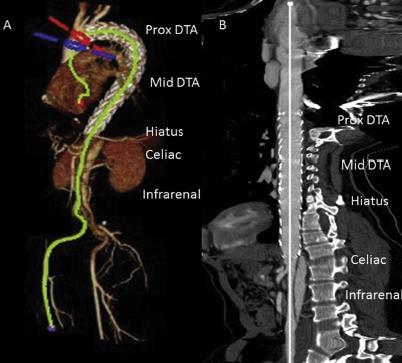
22 Aortic Remodeling: Impact of TEVAR on Aortic Diameter

23 TEVAR for complicated atbad Low Morbidity and Mortality Aortic Remodeling Stented Thoracic aorta TL Expansion FL obliteration Stabilization of Aortic diameter Abdominal aortic Patent FL Aortic Growth CAREFUL SURVEILLANCE IS WARRANTED Ann Thorac Surg 2017;103:
24 Emory Complicated atbad Case
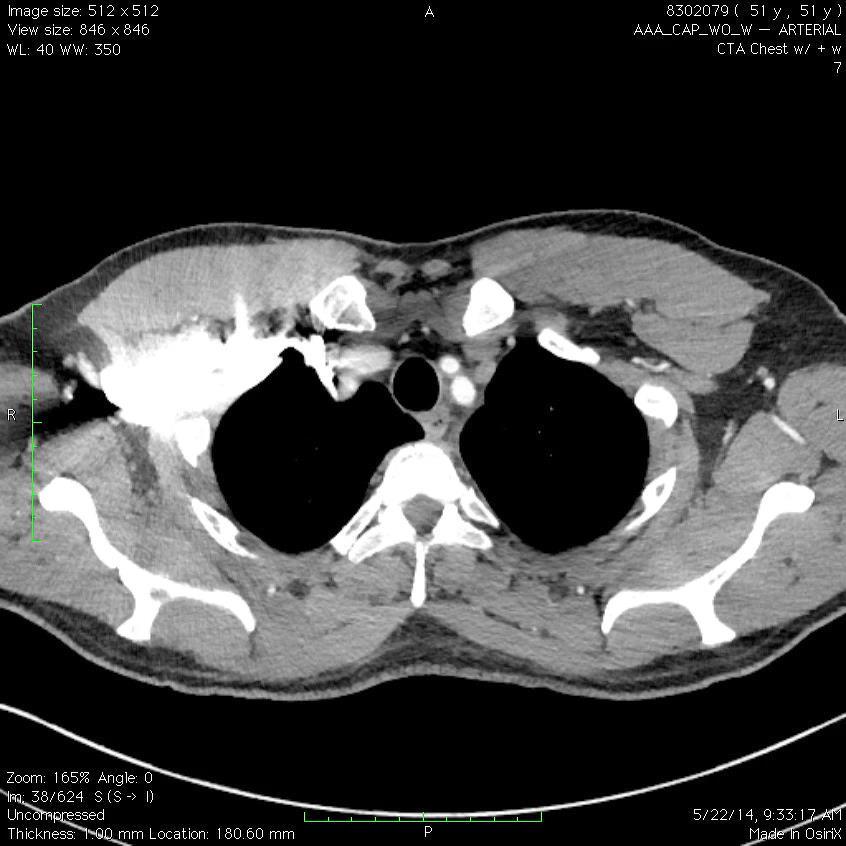
25 Case 1 51 yo presented to an OSH with an acute onset of sharp back and abdominal pain. CT scan: Acute Type B Aortic Dissection PE : Neuro: Somnolent ABD: Soft, NT,ND Pulses: Femoral pulses non Palpable Anuric Labs: Cr. 2.5 Platelets 67K Lactate 4.0

26

27 Hybrid OR Open exposure of R CFA: Pulseless 5 Fr L CFA Sheath BP s : R Radial: 121/58 R CFA: 41/37 L CFA 58/43 R Radial R CFA
28 Conduct of operation IVUS Lunderquist and Pigtail in TL Sizing: Zone 2 Aorta 30mm TEVAR: Valiant 32 x 32 x 200 Magnified Arch aortogram Decrease SBP <90mm Hg Deployment bare metal over LSA BP R Radial: 119/55 R CFA: 84/51

29 Conduct of operation TEVAR: 34 x 30 x 150 IVUS to mark Celiac No AORTOGRAM R Radial 116/52 R CFA: 101/52 L CFA: 99/51 AORTOGRAM Normal renal perfusion R Radial R CFA MALPERFUSION RESOLVED
30 Postoperative Course Immediately increased SBP>150 Immediate urine output in foley Extubated in OR Not moving legs! STAT lumbar drain in OR Moved legs 1 hour later in ICU CSF drainage for 3 days, MAP>100 DC on POD#11 Normal neurologic exam, Cr. 1.8 Palpable DP pulses 1 month Postop CTA
31
32 Management of atbad in 2017 Complicated TEVAR: GOLD STANDARD Uncomplicated Medical Management vs TEVAR CONTROVERSIAL!

33 What is the data on Uncomplicated TBAD (utbad)? What is the data on OMT for uncomplicated TBAD? What is the data on TEVAR for uncomplicated TBAD? Natural History Data ADSORB (acute) INSTEAD (chronic)
 Long Term Survival 1 year: 83-100% 5 years: 70-89% JACC")
34 Uncomplicated atbad Medical Management In hospital mortality: 6.4% (n=1480) Long Term Survival 1 year: % 5 years: 70-89% JACC 2013;61:

35 Natural History of OMT for autbad MGH pts autbad OMT Mean F/U: 4.3±3.5 yrs OMT failure: 58.4% Death: 38% (119 pts) Aortic related interventions: 29% (87 pts) J Vasc Surg 2015;61:1192-9
36 Intervention-free Survival Natural History of OMT for autbad Less than half (41%) enjoyed intervention-free survival at 6 years 41.0%
37 Natural History of OMT for autbad 76.4% 59.3% Intervention OMT P<0.05 Those who ultimately required intervention had significant survival advantage

38 EMORY TEVAR for TBAD patients De Novo Acute TBAD Ann Thorac Surg In Press
39 EMORY AORTIC CENTER Acute de novo TBADs presenting between (N = 398) Complicated Uncomplicated TEVAR within 14 days of presentation (atevar: N = 80) Optimal medical management (N = 318) Open surgery (OPEN: N = 59) TEVAR (ctevar: N = 87) Optimal medical management (OMT: N = 172)
40 In-hospital mortality at index hospitalization atevar (N = 80) Uncomplicated (N = 318) P-value In-hospital mortality 5.0% (4/80) 5.0% (16/318) Data presented as % (count/total).
41 Kaplan-Meier Survival Curve Complicated vs Uncomplicated atbad
42 Kaplan-Meier Survival Curve All atbad pts based upon definitive treatment received
43 Kaplan-Meier Survival Curve All intervention groups from time of intervention
44 Kaplan-Meier Intervention-free Survival Curve Uncomplicated atbad patients from time of presentation
45 Conclusions Complicated atbads undergoing TEVAR have excellent early (95%) and long-term outcomes (>80% survival at 10 years). The natural history of uncomplicated atbads treated with OMT: Short term mortality: 5% 46% required intervention in the chronic phase Intervention-free survival: ~50% at 5 years and ~30% at 10 years.
46 Conclusions TEVAR at the index hospitalization may confer a survival advantage and serve as optimal therapy for both complicated and uncomplicated acute TBADs A more aggressive endovascular approach to uncomplicated TBADs is warranted to improve long-term survival.
47 EMORY ATBAD ALGORITHM 2017 Complicated Malperfusion Rupture Uncomplicated Emergent TEVAR High Risk Intractable Pain Intractable HTN Total Aortic Diameter 40 mm FL > 22 mm Low Risk Pain free BP controlled No change in size or morphology on serial imaging TEVAR (24-72 hrs) OMT
48 Contemporary Management of Acute Type B Aortic Dissection Bradley G. Leshnower MD Assistant Professor of Surgery Division of Cardiothoracic Surgery Emory University School of Medicine Georgia Vascular Society 5 th Annual Scientific Sessions September 9, 2017
49 Contemporary Management of Chronic Type B Dissection
50 TEVAR for Chronic TBAD Issues in 2017 Efficacy dependent upon aortic remodeling Rigid dissection flap Retrograde FL perfusion Lack of a dissection-specific device Patient selection Age and comorbidities Anatomy Management of the distal LZ Limited Data
 Malper/rupture: n=5 (7%) Age: 61± 5 years Mean f/u: 24 ± 26")
51 Cleveland Clinic patients Aneurysm: n=47 (62%) Pain: n=15 (20%) Rapid growth: n=9 (12%) Malper/rupture: n=5 (7%) Age: 61± 5 years Mean f/u: 24 ± 26 months
52 TEVAR Details DeBakey 3a n=30 DeBakey 3b n=46 Age of Dissection: 25 months LSA Coverage: 39% Preop LSA revasc: 10% Device oversized 10-15% Short segment coverage Primary tear coverage only Gore TAG n=32 MDT Talent n=3 Cook TX2 n=27
53 Morbidity and Mortality Respiratory failure n=7 Limb ischemia n=1 Stroke n=1 Paraplegia n=0 Periop mortality n=4 Malperfusion n =1 Stroke n=1 Retrograde type A n=1 Unknown n=1 Late mortality n=12 Ruptured type A n=1 Unknown n=3 Non-aortic related n=8
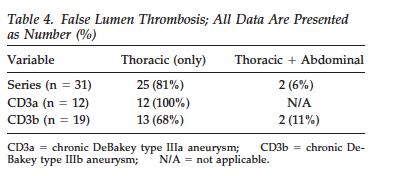
54 Aortic remodeling Decrease of 3.9mm (p<0.001) in Thoracic aortic diameter in the stent grafted aorta in both 3a and 3b patients Total FL thrombosis 3a n =78% 3b n=13% Increase in ABD aorta in 3b patients of 6.2 mm (p<0.05)
55 CCF: TEVAR in Chronic TBAD Safe procedure Low perioperative morbidity and mortality Excellent treatment for 3a patient Aortic remodeling Effective in FL thrombosis in the thoracic aorta ABD FL remains patent Decrease in Thoracic aortic size Increase in ABD aortic size 22% aortic reintervention rate >50% TEVAR extensions

56 PENN Chronic DeBakey III Aneurysms Open n=58 TEVAR n=31 Periop morbidity and mortality Aortic remodeling Mean f/u: 21 ± 20 months
57
58 TEVAR details DeBakey 3a n=12 DeBakey 3b n=19 Age of Dissection: 47 months Length of coverage: 22±4 cm LSA Coverage: 55% Preop LSA revasc: 42% Aortic reinterventions: n=4 Gore TAG n=24 MDT Talent n=2 Cook TX2 n=5
59

60
61 PENN TEVAR in Chronic TBAD Safe procedure Low morbidity and mortality Equivalent aortic related mortality to Open at 5 years Aortic remodeling TL Expansion FL Reduction Stabilizes total aortic diameter 3a patients Total FL thrombosis 100% 3b patients Highly effective in Thoracic FL thrombosis ABD FL remains patent


62 Duke Chronic DeBakey 3B Aneurysms n=32 Age: 58 ± 12 years Median f/u: 54 months No TAAA Aortic diameter at celiac axis : 3.5 ± 0.5 cm

63 TEVAR details DeBakey 3a n=0 DeBakey 3b n=32 Age of Dissection: 32 mos Length of coverage: 22±6cm LSA Coverage: 81% Preop LSA revasc: 19% Gore TAG n=24 MDT Talent n=2 Cook TX2 n=6
64 Morbidity & Mortality Mortality: n=0 Stroke: n=0 Paraplegia: n=0 Retrograde type A: n=2 (6.3%) No mortalities Aortic reintervention: n=5 (15%) Median LOS: 3 days
65 Aortic remodeling 89% 1 cm decrease in Thoracic aortic size 15% Total FL thrombosis 44% Total Thoracic FL thrombosis 15% FL thrombosis along stent graft 25% Retrograde FL perfusion along stent graft
66 DUKE TEVAR for Chronic TBAD Safe Low morbidity, no mortality Highly effective remodeling procedure for patients DeBakey 3B patients with DTAA (not TAAA) Recommendations/Observation Cover all Thoracic FL fenestrations Total FL thrombosis observed when all viscerals originate from the TL and < 3 distal fenestrations
67 TEVAR for CTBAD in 2017 What do we know? Technically feasible Low perioperative morbidity & mortality Excellent therapy for DeBakey IIIa Efficacy is variable for DeBakey IIIb Length of aortic coverage: Cover all Thoracic FL fenestrations Cover to the celiac artery

68 TEVAR for CTBAD in 2017 Ideal Anatomy What we do not know? DTAA not TAAA? Number of FL viscerals and distal fenestrations Management of distal LZ Management of retrograde FL perfusion Hughes GC, et al. Op Tech Thorac Cardiovasc Surg 2013;18:
69 Management of Distal LZ: Controversies Graft size at distal LZ TL size Total aortic diameter Balloon rupture of dissection flap Goal Expand endograft to oppose the flap to outer FL wall Achieve a distal seal Eliminate retrograde FL perfusion
70 Knickerbocker Technique Kolbel T, et al. J Endovasc Ther 2014;21:117-
71 EMORY TEVAR for Residual DeBakey I with 7.6cm DTAA using Knickerbocker Technique
72 Case Presentation 52 yo male morbidly obese truck driver s/p Asc/Hemiarch for and Acute DeBakey 1 aortic dissection in 2009 Lost to follow up Presents with chest pain radiating to his back to an OSH PMH: HTN, Morbid obesity, DM, CHF, Stage II CKD 5 7, 343 lbs
73 Case presentation 7.6 cm TAAA Tapers down to 4.2cm at Celiac Non dissected Proximal LZ Atrophic L Kidney Poor Open candidate due to body habitus, risk of pulmonary and renal failure

74
75 Procedure L Carotid-Subclavian Bypass Proximal LSA emoblization with 16mm Amplatz plug TEVAR Prox LZ: Zone 2 Aorta 34 mm Distal LZ: Celiac: Aorta 42 mm\ Valiant 40 x 40 x 200, 46 x 46 x 200 Balloon rupture 4cm cephalad to celiac

76 Balloon Rupture of Dissection Flap
77 Postop CT scans Arterial Delayed venous
78 Management of Retrograde FL perfusion Mechanical occlusion of retrograde FL perfusion Candy-Plug Technique Covered stent grafts in the FL
79 EMORY False Lumen Embolization in Chronic Complicated TBAD
80 History of Present Illness 64 yo female presented to an OSH with acute onset of chest and back pain associated with a syncopal episode PMH HTN COPD CT Scan
81 Preoperative CT
82 Diagnosis and Treatment Plan Ruptured Acute Type B Aortic Dissection with L Hemothorax Transferred to Emory On arrival to Emory Pain Free Hemodynamically stable on IV esmolol Physical exam unremarkable 2+ palpable pulses in all four extremities
83 Conduct of operation Hybrid OR Awake, totally percutaneous TEVAR Avoids risk of rupture with induction of general anesthesia Allows real time neuromonitoring for spinal cord ischemia Bilateral femoral arterial access IVUS Confirm TL wire placement L Fem: TL R Fem: Unable to access TL Right radial artery access 4 Fr Pigtail
84 Conduct of operation Proximal landing zone Zone 2 Non-dissected aorta Aortic diameter: 32mm Must cover LSA in rupture Distal landing zone 1cm cephalad to celiac artery Aortic diameter: 34 mm Valiant 34 x 34 x 200, 36 x 36 x 200
85 Post-operative course Neurologically intact SBP>150 L Chest tube placed on POD#2 1.5L of dark blood Hemodynamically stable CT scan on POD#4 Retained small left hemothorax VATS on POD#7 DC home on POD#11
86 CT Scan POD#4
87 Post-op visit at 1 month Chief complaint: 5/10 interscapular back pain PE Normal 2+ palpable pulses in all four extremities CT Scan

88 CT scan -1 month postop Arterial phase Delayed venous phase

89 CT Scan-1 month postop 6.1cm
90 CT Scan-1 month postop 6.1cm
91 Diagnosis Rapidly expanding 6.1 cm DTA Aneurysm 1cm growth in 1 month No antegrade FL filling Retrograde FL filling Options Open DTA Repair with TEVAR explant using HCA Endovascular FL Embolization Placement of a covered stent graft into the FL to eliminate retrograde FL perfusion of the DTA

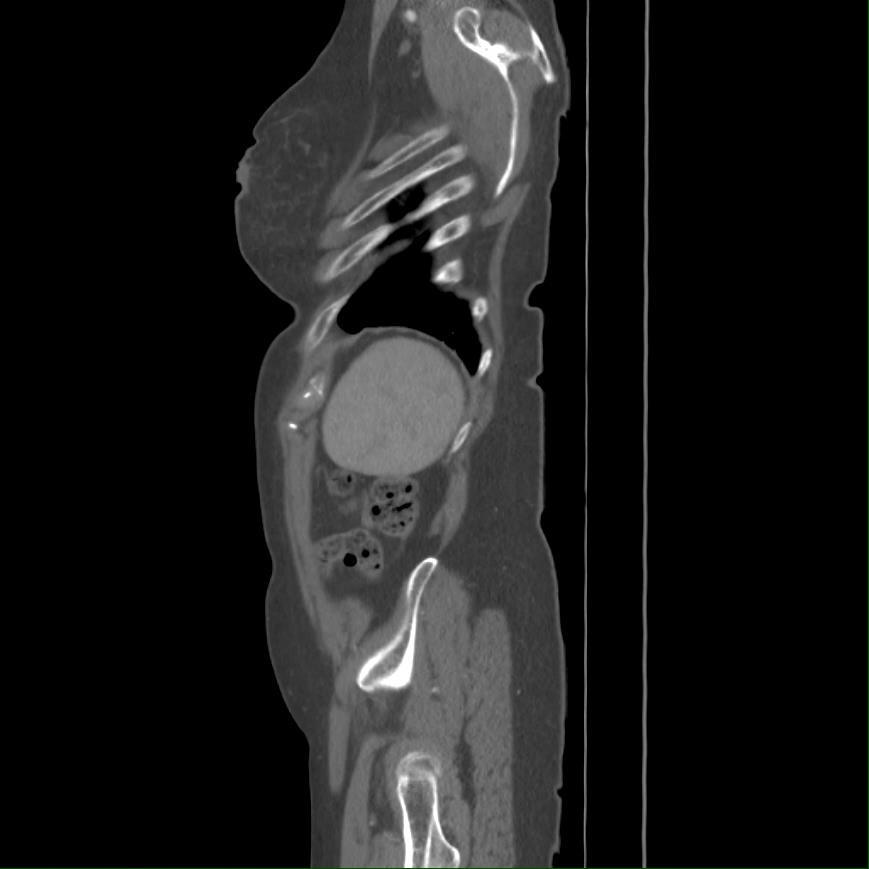
92 FL Embolization procedure Gain TL and FL access Perform Proximal aortogram Rule out antegrade FL filling Perform Distal aortogram in FL to confirm retrograde filling Place a covered stent graft with an iliac plug into the FL Cook Flex AAA converter 36 x x 30 ZIP Iliac plug
93 FL Embolization
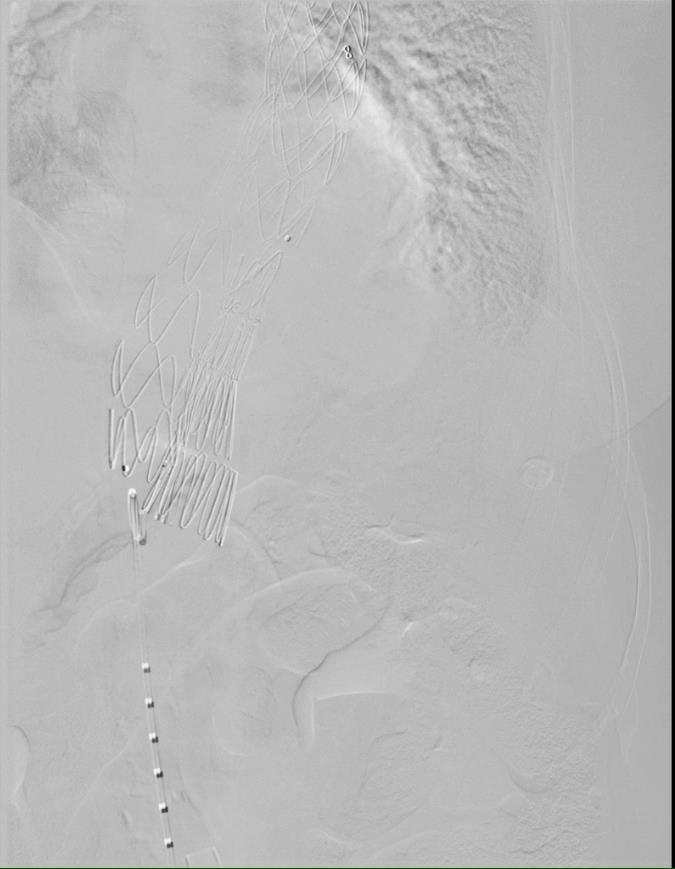

94 FL Embolization
95 Post FL Embolization CT Scan
96
97
98 Retrograde FL perfusion Post FL Embolization
99 TEVAR for Chronic TBAD 2017 DeBakey 3a: Non-inferior to Open surgery DeBakey 3b with DTAA: Excellent results DeBakey 3b with TAAA: Unclear efficacy Evolving adjunct procedures to manage the distal LZ and retrograde FL perfusion are improving results
100 Contemporary Management of Acute Type B Aortic Dissection Bradley G. Leshnower MD Assistant Professor of Surgery Division of Cardiothoracic Surgery Emory University School of Medicine Georgia Vascular Society 5 th Annual Scientific Sessions September 9, 2017
101 Is there a role for prophylactic TEVAR in uncomplicated atbad?

102 ADSORB Prospective randomized trial of BMT vs BMT+TEVAR (Gore TAG) for uncomplicated atbad 17 European centers Treatment within 14 days of onset of symptoms
103 ADSORB: Methods Enrollment : 61 patients BMT n=31 BMT + TEVAR n=30 3 patients crossed over from BMT to TEVAR group 2 patients withdrawn from TEVAR group Consent issue: n=1 Proximal LZ inadequate: n=1 TEVAR group Proximal LZ: 2cm Treatment length: 15 cm (Physician discretion)
104 ADSORB: Methods Composite Primary Endpoint at 1 year Incomplete or no FL thrombosis along the length of the stent graft, excluding distal 2cm Increase in total aortic diameter of 5mm Aortic rupture CT scans per protocol at DC/1, 3 and 12 months, then q 6months x 3 years Intention to treat analysis

105 ADSORB: Results Baseline demographics equivalent 14 patients overall failed the primary endpoint due to inadequate/no imaging
106 ADSORB: Results Per Protocol Analysis 1 yr follow up imaging: 23 pts in each group Composite Primary Endpoint at 1 year Incomplete/no FL thrombosis along the length of the stent BMT: 21/23 (91.3%) NO THROMBOSIS TEVAR: 4/23(17.4%) NO THROMBOSIS Aortic rupture Zero in either group Zero 30 day deaths in either group 1 yr mortality: TEVAR n=1 (Cardiac arrest, no autopsy) BMT n=0 Increase in total aortic diameter of 5mm
107 TEVAR 22.5mm TEVAR 32.2mm BMT 23.6 mm p=0.83 BMT 25.5 mm p<0.01
108 BMT 22.1 mm BMT 25.1 mm TEVAR 23.9 mm p=0.79 TEVAR 18.5 mm p<0.01
109 BMT 42.1 mm TEVAR 38.8 mm p=0.62
110 ADSORB: Conclusions The addition of TEVAR to BMT significantly increased the freedom from the composite primary endpoint TEVAR is more effective than BMT in promoting positive aortic remodeling TL expansion FL thrombosis and shrinkage Larger RCT with longer follow-up necessary to determine whether TEVAR provides a survival benefit over BMT in patients with uncomplicated atbad
111 Is there a role for prophylactic TEVAR in uncomplicated atbad? Risk Periprocedural morbidity & mortality Potential adverse downstream false lumen remodeling Cost (TEVAR) Benefit Improve long-term survival in patients with atbad Prevent aneurysmal degeneration of the TAAA Induce aortic remodeling
112 Uncomplicated atbad: Questions Do all Uncomplicated atbad s have similar long term outcomes? Approximately 20-40% will require surgery within 5 years Elefteriades JA, et al. Ann Thorac Surg Schor JS, et al. Ann Thorac Surg Onitsuka S, et al. Ann Thorac Surg Gysi J, et al. Eur J Cardiothorac Surg Juvonen T, et al. J Thorac Cardiovasc Surg Are there clinical or morphologic features of atbad s which predict unfavorable outcomes? Is there a role for prophylactic TEVAR in uncomplicated atbad?


113 IRAD: Impact of Refractory Pain and Hypertension in atbad Uncomplicated n=296 Uncomplicated with refractory back pain and/or hypertension: n=69 Endovascular: 39% Open: 36% Medical: 25%


114 IRAD Significance of Refractory HTN and Pain Uncomplicated Refractory HTN/Pain Uncomplicated Refractory HTN/Pain Medical + Open+Endovascular Therapy Medical Therapy
115 IRAD Significance of Refractory HTN and Pain: Conclusions In-hospital mortality significantly higher with medical management 2/3 rd deaths due to aortic rupture Refractory pain/htn independent predictor of in-hospital mortality: OR 3.31 ( , p=0.04) Open or endovascular surgery improved outcomes over medical management for refractory pain/htn
116 Radiographic predictors of Aneurysmal Degeneration/Mortality Initial aortic diameter of 40mm and/or a patent false lumen is predictive of aortic enlargement 60mm Marui A, et al. Circulation 1999;100:II-275-II-280. Patent false lumen is an independent risk factor for increasing aortic diameter Sueyoshi E, et al. Circulation 2004;110:II-256-II-261. Partially thrombosed false lumen is an independent predictor of mortality Tsai TTet al. N Eng J Med 2007;357: False lumen diameter 22mm in the proximal DTA correlates with aneurysmal change and mortality Song JM et al. J Am Coll Cardiol 2007;50:
117 High Risk Uncomplicated atbad Refractory HTN and Pain False lumen 22 mm Total aortic diameter of DTA 40 mm False lumen status: unclear
118 Acute Uncomplicated TBAD Controversial Medical Therapy Excellent short term outcomes Poor long term outcomes High rate of aneurysm formation Low rate intervention-free survival TEVAR High risk features? All acute type B s RCT needed
119 Management of Acute Type B Aortic Dissection Bradley G. Leshnower MD Assistant Professor of Surgery Division of Cardiothoracic Surgery Emory University School of Medicine
120 Aortic Dissection: Incidence Worldwide: 5-30 cases/1,000,000 people/year U.S: 2-8 cases/1,000,000 people/year 2/3 type A, 1/3 type B Acute Type B 30% complicated, uncomplicated 70%

121 emergency stent grafting with life-threatening complications of acute type B aortic dissection may save many lives and that this could well become the most clinically valuable application of thoracic aortic stent-grafting in the future. In patients with uncomplicated acute type B aortic dissection, (medical management) constitutes a benchmark that will be difficult to surpass or even match by endovascular stent-graft treatment D. Craig Miller MD Ann Thorac Surg 2008;85:S1-41
122 Adverse events among all patients undergoing intervention atevar (N = 80) OPEN (N = 59) ctevar (N = 87) P-value In-hospital mortality 5.0% (4/80) 16.9% (10/59) 2.3% (2/87) Paraplegia 0.0% (0/80) 3.4% (2/59) 2.3% (2/87) Paraparesis 2.5% (2/80) 1.7% (1/59) 1.1% (1/87) Stroke 7.5% (6/80) 1.7% (1/59) 0.0% (0/87) Renal failure 1.3% (1/80) 10.2% (6/59) 4.6% (4/87) Data presented as % (count/total).

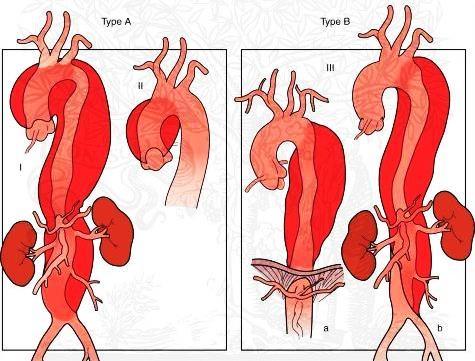
123 DeBakey Classification IIIa IIIb IIIa IIIb A B Stanford Frank Criado, MD
124 Definitions Acute: < 2 weeks Subacute: 2 weeks 2 months Chronic: > 2 months Mery CM, Reece TB, Kron IL. Aortic Dissection. In Cohn LH, ed. Cardiac Surgery in the Adult. New York, NY: McGraw Hill: , 2012.

125 New IRAD Definitions Hyperacute: 0-24 hrs Acute: 2-7 days Subacute: 8-30 days Chronic: > 30 days Booher AM et al. Am J Med 2013:126:730:e19-24.
126 Type B Aortic Dissection Acute Complicated Uncomplicated Chronic Complicated Uncomplicated FDA Approval for Endovascular Therapy for all subgroups
UC SF An Algorithm to Choose Which Uncomplicated (Asymptomatic) Acute Type B Dissection Patients Should Undergo TEVAR. Disclosures.
 Acute Type B Dissection Patients Should Undergo TEVAR. Disclosures.") An Algorithm to Choose Which Uncomplicated (Asymptomatic) Acute Type B Dissection Patients Should Undergo TEVAR Disclosures Royalties and research grant support from Cook Medical, Inc. Jade S. Hiramoto,
An Algorithm to Choose Which Uncomplicated (Asymptomatic) Acute Type B Dissection Patients Should Undergo TEVAR Disclosures Royalties and research grant support from Cook Medical, Inc. Jade S. Hiramoto,
I-Hui Wu, M.D. Ph.D. Clinical Assistant Professor Cardiovascular Surgical Department National Taiwan University Hospital
 Comparisons of Aortic Remodeling and Outcomes after Endovascular Repair of Acute and Chronic Complicated Type B Aortic Dissections I-Hui Wu, M.D. Ph.D. Clinical Assistant Professor Cardiovascular Surgical
Comparisons of Aortic Remodeling and Outcomes after Endovascular Repair of Acute and Chronic Complicated Type B Aortic Dissections I-Hui Wu, M.D. Ph.D. Clinical Assistant Professor Cardiovascular Surgical
The Petticoat Technique Managing Type B Dissection with both Early and Long Term Considerations
 The Petticoat Technique Managing Type B Dissection with both Early and Long Term Considerations Joseph V. Lombardi, MD Professor & Chief, Division of Vascular & Endovascular Surgery Department of Surgery,
The Petticoat Technique Managing Type B Dissection with both Early and Long Term Considerations Joseph V. Lombardi, MD Professor & Chief, Division of Vascular & Endovascular Surgery Department of Surgery,
Endovascular therapy for Ischemic versus Nonischemic complicated acute type B aortic dissection (catbad).
.") Endovascular therapy for Ischemic versus Nonischemic complicated acute type B aortic dissection (catbad). AS. Eleshra, MD 1, T. Kölbel, MD, PhD 1, F. Rohlffs, MD 1, N. Tsilimparis, MD, PhD 1,2 Ahmed Eleshra
Endovascular therapy for Ischemic versus Nonischemic complicated acute type B aortic dissection (catbad). AS. Eleshra, MD 1, T. Kölbel, MD, PhD 1, F. Rohlffs, MD 1, N. Tsilimparis, MD, PhD 1,2 Ahmed Eleshra
Challenges. 1. Sizing. 2. Proximal landing zone 3. Distal landing zone 4. Access vessels 5. Spinal cord ischemia 6. Endoleak
 Disclosure I have the following potential conflicts of interest to report: Consulting: Medtronic, Gore Employment in industry Stockholder of a healthcare company Owner of a healthcare company Other(s)
Disclosure I have the following potential conflicts of interest to report: Consulting: Medtronic, Gore Employment in industry Stockholder of a healthcare company Owner of a healthcare company Other(s)
Animesh Rathore, MD 4/22/17. The Great Debate 45yo Man With Uncomplicated Acute TBAD: The Case For Medical Management
 Animesh Rathore, MD 4/22/17 The Great Debate 45yo Man With Uncomplicated Acute TBAD: The Case For Medical Management Disclosures Just a young vascular surgeon who would like to keep his job My opponent
Animesh Rathore, MD 4/22/17 The Great Debate 45yo Man With Uncomplicated Acute TBAD: The Case For Medical Management Disclosures Just a young vascular surgeon who would like to keep his job My opponent
Acute dissections of the descending thoracic aorta (Debakey
 Endovascular Treatment of Acute Descending Thoracic Aortic Dissections Nimesh D. Desai, MD, PhD, and Joseph E. Bavaria, MD Acute dissections of the descending thoracic aorta (Debakey type III or Stanford
Endovascular Treatment of Acute Descending Thoracic Aortic Dissections Nimesh D. Desai, MD, PhD, and Joseph E. Bavaria, MD Acute dissections of the descending thoracic aorta (Debakey type III or Stanford
Do the Data Support Endovascular Therapy for Descending Thoracic AD? Woong Chol Kang, M.D.
 Do the Data Support Endovascular Therapy for Descending Thoracic AD? Woong Chol Kang, M.D. Gil Hospital, Gachon University Incheon, Korea Classification of AD Acute vs. Chronic (2weeks) (IIIa, b) type
Do the Data Support Endovascular Therapy for Descending Thoracic AD? Woong Chol Kang, M.D. Gil Hospital, Gachon University Incheon, Korea Classification of AD Acute vs. Chronic (2weeks) (IIIa, b) type
Global Evidence for the Treatment of Type B Aortic Dissection
 Global Evidence for the Treatment of Type B Aortic Dissection Ross Milner, MD Professor of Surgery Director, Center for Aortic Diseases September 17, 2016 Disclosures Consultant Cook, Endospan, Medtronic,
Global Evidence for the Treatment of Type B Aortic Dissection Ross Milner, MD Professor of Surgery Director, Center for Aortic Diseases September 17, 2016 Disclosures Consultant Cook, Endospan, Medtronic,
Combined Endovascular and Surgical Repair of Thoracoabdominal Aortic Pathology: Hybrid TEVAR
 Combined Endovascular and Surgical Repair of Thoracoabdominal Aortic Pathology: Hybrid TEVAR William J. Quinones-Baldrich MD Professor of Surgery Director UCLA Aortic Center UCLA Medical Center Los Angeles,
Combined Endovascular and Surgical Repair of Thoracoabdominal Aortic Pathology: Hybrid TEVAR William J. Quinones-Baldrich MD Professor of Surgery Director UCLA Aortic Center UCLA Medical Center Los Angeles,
Hybrid Repair of a Complex Thoracoabdominal Aortic Aneurysm
 Hybrid Repair of a Complex Thoracoabdominal Aortic Aneurysm Virendra I. Patel MD MPH Assistant Professor of Surgery Massachusetts General Hospital Division of Vascular and Endovascular Surgery Disclosure
Hybrid Repair of a Complex Thoracoabdominal Aortic Aneurysm Virendra I. Patel MD MPH Assistant Professor of Surgery Massachusetts General Hospital Division of Vascular and Endovascular Surgery Disclosure
UC SF. Disclosures. Thoracic Endovascular Aortic Repair 4/24/2009. Management of Acute Dissections: Is There Still a Role for Open Surgery?
 UC SF Management of Acute Dissections: Is There Still a Role for Open Surgery? Darren B. Schneider, M.D. Assistant Professor of Surgery and Radiology Division of Vascular Surgery University of California
UC SF Management of Acute Dissections: Is There Still a Role for Open Surgery? Darren B. Schneider, M.D. Assistant Professor of Surgery and Radiology Division of Vascular Surgery University of California
Performance of the conformable GORE TAG device in Type B aortic dissection from the GORE GREAT real world registry
 University of Milan Thoracic Aortic Research Center Performance of the conformable GORE TAG device in Type B aortic dissection from the GORE GREAT real world registry Santi Trimarchi, MD, PhD Associate
University of Milan Thoracic Aortic Research Center Performance of the conformable GORE TAG device in Type B aortic dissection from the GORE GREAT real world registry Santi Trimarchi, MD, PhD Associate
UC SF Early Intervention in Type B Dissection: Results From the INSTEAD XL Trial. Acute Type B Dissection. Outline. Disclosures.
 Early Intervention in Type B Dissection: Results From the INSTEAD XL Trial None Disclosures Jade S. Hiramoto, MD, MAS April 4, 2014 Outline Background Current treatment Results from INSTEAD trial Results
Early Intervention in Type B Dissection: Results From the INSTEAD XL Trial None Disclosures Jade S. Hiramoto, MD, MAS April 4, 2014 Outline Background Current treatment Results from INSTEAD trial Results
Are stent-grafts for acute type B dissection durable? Est-ce que les stents graft pour la dissection aigue de type B sont efficaces à moyen terme?
 Are stent-grafts for acute type B dissection durable? Est-ce que les stents graft pour la dissection aigue de type B sont efficaces à moyen terme? Martin Björck, Johnny Steuer, Anders Wanhainen Uppsala
Are stent-grafts for acute type B dissection durable? Est-ce que les stents graft pour la dissection aigue de type B sont efficaces à moyen terme? Martin Björck, Johnny Steuer, Anders Wanhainen Uppsala
Abdominal and thoracic aneurysm repair
 Abdominal and thoracic aneurysm repair William A. Gray MD Director, Endovascular Intervention Cardiovascular Research Foundation Columbia University Medical Center Abdominal Aortic Aneurysm Endografts
Abdominal and thoracic aneurysm repair William A. Gray MD Director, Endovascular Intervention Cardiovascular Research Foundation Columbia University Medical Center Abdominal Aortic Aneurysm Endografts
Is there a way to predict the risk in uncomplicated Type B aortic dissections? FRANS MOLL University Medical Centre Utrecht - Netherlands
 Is there a way to predict the risk in uncomplicated Type B aortic dissections? FRANS MOLL University Medical Centre Utrecht - Netherlands Disclosures: - Consultant Philips Health Care - Best Doctors Overview
Is there a way to predict the risk in uncomplicated Type B aortic dissections? FRANS MOLL University Medical Centre Utrecht - Netherlands Disclosures: - Consultant Philips Health Care - Best Doctors Overview
What is the best treatment for False Lumen growth after type B Dissection
 What is the best treatment for False Lumen growth after type B Dissection Nikolaos Tsilimparis, Fiona Rohlffs, Yuk Law, Sebastian Debus, Tilo Kölbel N. Tsilimparis, MD, PhD, FEBVS Deputy Head of German
What is the best treatment for False Lumen growth after type B Dissection Nikolaos Tsilimparis, Fiona Rohlffs, Yuk Law, Sebastian Debus, Tilo Kölbel N. Tsilimparis, MD, PhD, FEBVS Deputy Head of German
Malperfusion Syndromes Type B Aortic Dissection with Malperfusion
 Malperfusion Syndromes Type B Aortic Dissection with Malperfusion Jade S. Hiramoto, MD, MAS April 27, 2012 Associated with early mortality Occurs when there is end organ ischemia secondary to aortic branch
Malperfusion Syndromes Type B Aortic Dissection with Malperfusion Jade S. Hiramoto, MD, MAS April 27, 2012 Associated with early mortality Occurs when there is end organ ischemia secondary to aortic branch
Technique and Outcome of Laser Fenestration For Arch Vessels
 Technique and Outcome of Laser Fenestration For Arch Vessels Jean M. Panneton MD, FRCSC, FACS Professor of Surgery Chief & Program Director Division of Vascular Surgery Eastern Virginia Medical School
Technique and Outcome of Laser Fenestration For Arch Vessels Jean M. Panneton MD, FRCSC, FACS Professor of Surgery Chief & Program Director Division of Vascular Surgery Eastern Virginia Medical School
Endovascular Management of Thoracic Aortic Pathology Stéphan Haulon, J Sobocinski, B Maurel, T Martin-Gonzalez, R Spear, A Hertault, R Azzaoui
 Endovascular Management of Thoracic Aortic Pathology Stéphan Haulon, J Sobocinski, B Maurel, T Martin-Gonzalez, R Spear, A Hertault, R Azzaoui Aortic Center, Lille University Hospital, France Disclosures
Endovascular Management of Thoracic Aortic Pathology Stéphan Haulon, J Sobocinski, B Maurel, T Martin-Gonzalez, R Spear, A Hertault, R Azzaoui Aortic Center, Lille University Hospital, France Disclosures
Clinical Trials of Acute and Chronic Dissections. Gregory Landry MD
 Clinical Trials of Acute and Chronic Dissections Gregory Landry MD No disclosures Acute vs chronic dissection: Definitions 1950s: Acute < 2 weeks, Chronic > 2 weeks 2013: European Interdisciplinary Consensus
Clinical Trials of Acute and Chronic Dissections Gregory Landry MD No disclosures Acute vs chronic dissection: Definitions 1950s: Acute < 2 weeks, Chronic > 2 weeks 2013: European Interdisciplinary Consensus
Percutaneous Approaches to Aortic Disease in 2018
 Percutaneous Approaches to Aortic Disease in 2018 Wendy Tsang, MD, SM Assistant Professor, University of Toronto Toronto General Hospital, University Health Network Case 78 year old F Lower CP and upper
Percutaneous Approaches to Aortic Disease in 2018 Wendy Tsang, MD, SM Assistant Professor, University of Toronto Toronto General Hospital, University Health Network Case 78 year old F Lower CP and upper
Total Endovascular Repair Type A Dissection. Eric Herget Interventional Radiology
 Total Endovascular Repair Type A Dissection Eric Herget Interventional Radiology 65 year old male Acute Type A Dissection Severe Aortic Regurgitation No co-morbidities Management? Part II Evolving Global
Total Endovascular Repair Type A Dissection Eric Herget Interventional Radiology 65 year old male Acute Type A Dissection Severe Aortic Regurgitation No co-morbidities Management? Part II Evolving Global
TEVAR for Chronic dissections: indications for TEVAR, long term results
 TEVAR for Chronic dissections: indications for TEVAR, long term results J Sobocinski, R Azzaoui, B Maurel, R Spear, T Martin-Gonzalez, A Hertault, S Haulon Centre de l Aorte, Chirurgie vasculaire, Hôpital
TEVAR for Chronic dissections: indications for TEVAR, long term results J Sobocinski, R Azzaoui, B Maurel, R Spear, T Martin-Gonzalez, A Hertault, S Haulon Centre de l Aorte, Chirurgie vasculaire, Hôpital
Management of Acute Aortic Syndromes. M. Grabenwoger, MD Dept. of Cardiovascular Surgery Hospital Hietzing, Vienna, Austria
 Management of Acute Aortic Syndromes M. Grabenwoger, MD Dept. of Cardiovascular Surgery Hospital Hietzing, Vienna, Austria I have nothing to disclose. Acute Aortic Syndromes Acute Aortic Dissection Type
Management of Acute Aortic Syndromes M. Grabenwoger, MD Dept. of Cardiovascular Surgery Hospital Hietzing, Vienna, Austria I have nothing to disclose. Acute Aortic Syndromes Acute Aortic Dissection Type
Antegrade Thoracic Stent Grafting during Repair of Acute Debakey I Dissection: Promotes Distal Aortic Remodeling and Reduces Late Open Re-operation
 Antegrade Thoracic Stent Grafting during Repair of Acute Debakey I Dissection: Promotes Distal Aortic Remodeling and Reduces Late Open Re-operation Vallabhajosyula, P: Szeto, W; Desai, N; Pulsipher, A;
Antegrade Thoracic Stent Grafting during Repair of Acute Debakey I Dissection: Promotes Distal Aortic Remodeling and Reduces Late Open Re-operation Vallabhajosyula, P: Szeto, W; Desai, N; Pulsipher, A;
Neurological Complications of TEVAR. Frank J Criado, MD. Union Memorial-MedStar Health Baltimore, MD USA
 ISES Online Neurological Complications of Frank J Criado, MD TEVAR Union Memorial-MedStar Health Baltimore, MD USA frank.criado@medstar.net Paraplegia Incidence is 0-4% after surgical Rx of TAAs confined
ISES Online Neurological Complications of Frank J Criado, MD TEVAR Union Memorial-MedStar Health Baltimore, MD USA frank.criado@medstar.net Paraplegia Incidence is 0-4% after surgical Rx of TAAs confined
Residual Dissection and False Lumen Aneurysm After TEVAR
 WHAT WOULD YOU DO? Residual Dissection and False Lumen Aneurysm After MODERATOR: MARK FARBER, MD PANEL: YAZAN DUWAYRI, MD; MATTHEW J. EAGLETON, MD; WILLIAM D. JORDAN Jr, MD; TILO KÖLBEL, MD, PhD; AND ERIC
WHAT WOULD YOU DO? Residual Dissection and False Lumen Aneurysm After MODERATOR: MARK FARBER, MD PANEL: YAZAN DUWAYRI, MD; MATTHEW J. EAGLETON, MD; WILLIAM D. JORDAN Jr, MD; TILO KÖLBEL, MD, PhD; AND ERIC
Endovascular Repair of Aortic Arch/Thoracic Aneurysms: Bolton RelayBranch Device
 Endovascular Repair of Aortic Arch/Thoracic Aneurysms: Bolton RelayBranch Device Luis A. Sanchez MD Gregorio A. Sicard Distinguished Professor of Surgery & Radiology Chief, Section of Vascular Surgery
Endovascular Repair of Aortic Arch/Thoracic Aneurysms: Bolton RelayBranch Device Luis A. Sanchez MD Gregorio A. Sicard Distinguished Professor of Surgery & Radiology Chief, Section of Vascular Surgery
AORTIC DISSECTIONS Current Management. TOMAS D. MARTIN, MD, LAT Professor, TCV Surgery Director UF Health Aortic Disease Center University of Florida
 AORTIC DISSECTIONS Current Management TOMAS D. MARTIN, MD, LAT Professor, TCV Surgery Director UF Health Aortic Disease Center University of Florida DISCLOSURES Terumo Medtronic Cook Edwards Cryolife AORTIC
AORTIC DISSECTIONS Current Management TOMAS D. MARTIN, MD, LAT Professor, TCV Surgery Director UF Health Aortic Disease Center University of Florida DISCLOSURES Terumo Medtronic Cook Edwards Cryolife AORTIC
No Disclosure. Aortic Dissection in Japan. This. The Challenge of Acute and Chronic Type B Aortic Dissections with Endovascular Aortic Repair
 No Disclosure The Challenge of Acute and Chronic Type B Aortic Dissections with Endovascular Aortic Repair Toru Kuratani Department of Cardiovascular Surgery Osaka University Graduate School of Medicine,
No Disclosure The Challenge of Acute and Chronic Type B Aortic Dissections with Endovascular Aortic Repair Toru Kuratani Department of Cardiovascular Surgery Osaka University Graduate School of Medicine,
WHICH PLACE FOR EMERGENT INTERVENTION IN COMPLICATED ACUTE TYPE B DISSECTION (ctbaod)
") WHICH PLACE FOR EMERGENT INTERVENTION IN COMPLICATED ACUTE TYPE B DISSECTION (ctbaod) Epidemiology of type B Aortic Dissection TYPE B dissection: 0,5-2,1/100.000/year (40% of all dissection) Hospital mortality
WHICH PLACE FOR EMERGENT INTERVENTION IN COMPLICATED ACUTE TYPE B DISSECTION (ctbaod) Epidemiology of type B Aortic Dissection TYPE B dissection: 0,5-2,1/100.000/year (40% of all dissection) Hospital mortality
Pioneering EVAR techniques in aortic dissection
 Pioneering EVAR techniques in aortic dissection Jianing Yue, Weiguo Fu Department of Vascular Surgery Zhongshan Hospital Fudan University Shanghai, China LINC Asia-Pacific 2016 March 8-10, 2016 Hong Kong
Pioneering EVAR techniques in aortic dissection Jianing Yue, Weiguo Fu Department of Vascular Surgery Zhongshan Hospital Fudan University Shanghai, China LINC Asia-Pacific 2016 March 8-10, 2016 Hong Kong
TEVAR. (Thoracic Endovascular Aortic Repair) for Aneurysm and Dissection. Bruce Tjaden MD Vascular Surgery Fellow
 for Aneurysm and Dissection. Bruce Tjaden MD Vascular Surgery Fellow") Department of Cardiothoracic & Vascular Surgery McGovern Medical School / The University of Texas Health Science Center at Houston TEVAR (Thoracic Endovascular Aortic Repair) for Aneurysm and Dissection
Department of Cardiothoracic & Vascular Surgery McGovern Medical School / The University of Texas Health Science Center at Houston TEVAR (Thoracic Endovascular Aortic Repair) for Aneurysm and Dissection
Acute Type B dissection. Closure of the infra diaphragmatic tear: how and when?
 Acute Type B dissection. Closure of the infra diaphragmatic tear: how and when? Prof. Olgierd Rowiński II Department of Clinical Radiology Medical University of Warsaw Disclosure Speaker name: Olgierd
Acute Type B dissection. Closure of the infra diaphragmatic tear: how and when? Prof. Olgierd Rowiński II Department of Clinical Radiology Medical University of Warsaw Disclosure Speaker name: Olgierd
Aggressive Resection/Reconstruction of the Aortic Arch in Type A Dissection
 Aggressive Resection/Reconstruction of the Aortic Arch in Type A Dissection M. Grabenwoger Dept. of Cardiovascular Surgery Hospital Hietzing Vienna, Austria Disclosure Statement Consultant of Jotec, Hechingen,
Aggressive Resection/Reconstruction of the Aortic Arch in Type A Dissection M. Grabenwoger Dept. of Cardiovascular Surgery Hospital Hietzing Vienna, Austria Disclosure Statement Consultant of Jotec, Hechingen,
Optimal Treatment of Chronic Dissection
 Optimal Treatment of Chronic Dissection Chun-Che Shih 施俊哲 MD, Ph.D. Chief, Professor Institute of Clinical Medicine National Yang Ming University Division of Cardiovascular Surgery Taipei Veterans General
Optimal Treatment of Chronic Dissection Chun-Che Shih 施俊哲 MD, Ph.D. Chief, Professor Institute of Clinical Medicine National Yang Ming University Division of Cardiovascular Surgery Taipei Veterans General
Jean M Panneton, MD Professor of Surgery Program Director Vascular Surgery Chief EVMS. Arch Pathology: The Endovascular Era is here
 Jean M Panneton, MD Professor of Surgery Program Director Vascular Surgery Chief EVMS Arch Pathology: The Endovascular Era is here Disclosures Consultant: Cook Medical, Bolton Medical, Medtronic Inc, Volcano,
Jean M Panneton, MD Professor of Surgery Program Director Vascular Surgery Chief EVMS Arch Pathology: The Endovascular Era is here Disclosures Consultant: Cook Medical, Bolton Medical, Medtronic Inc, Volcano,
EVAR and TEVAR: Extending Their Use for Rupture and Traumatic Injury. Conflict of Interest. Hypotensive shock 5/5/2014. none
 EVAR and TEVAR: Extending Their Use for Rupture and Traumatic Injury Bruce H. Gray, DO MSVM FSCAI Professor of Surgery/Vascular Medicine USC SOM-Greenville Greenville, South Carolina none Conflict of Interest
EVAR and TEVAR: Extending Their Use for Rupture and Traumatic Injury Bruce H. Gray, DO MSVM FSCAI Professor of Surgery/Vascular Medicine USC SOM-Greenville Greenville, South Carolina none Conflict of Interest
False Lumen Occlusion Techniques in CAD:
 University Heart Center Hamburg GERMAN AORTIC CENTER False Lumen Occlusion Techniques in CAD: What is ist role? How is it done? Tilo Kölbel Fiona Rohlffs, Nikos Tsilimparis, Sebastian Debus German Aortic
University Heart Center Hamburg GERMAN AORTIC CENTER False Lumen Occlusion Techniques in CAD: What is ist role? How is it done? Tilo Kölbel Fiona Rohlffs, Nikos Tsilimparis, Sebastian Debus German Aortic
Treatment of acute type B aortic dissection: Current status
 MEET Cannes, 18. - 21.06.2009 Treatment of acute type B aortic dissection: Current status Christoph A. Nienaber, MD, FACC University of Rostock Department of Internal Medicine, Cardiology christoph.nienaber@med.uni-rostock.de
MEET Cannes, 18. - 21.06.2009 Treatment of acute type B aortic dissection: Current status Christoph A. Nienaber, MD, FACC University of Rostock Department of Internal Medicine, Cardiology christoph.nienaber@med.uni-rostock.de
Dissection de type B: l étude Instead et corollaire stratégique
 Dissection de type B: l étude Instead et corollaire stratégique Christoph A. Nienaber, MD, FACC University Rostock Heartcenter Med. Clinic I Cardiology christoph.nienaber@med.uni-rostock.de Type B aortic
Dissection de type B: l étude Instead et corollaire stratégique Christoph A. Nienaber, MD, FACC University Rostock Heartcenter Med. Clinic I Cardiology christoph.nienaber@med.uni-rostock.de Type B aortic
Is a Paradigm Shift towards Early Endovascular Treatment of Type B Dissection justified?
 Is a Paradigm Shift towards Early Endovascular Treatment of Type B Dissection justified? Dittmar Böckler Department of Vascular and Endovascular Surgery University of Heidelberg, Germany Disclosure Speaker
Is a Paradigm Shift towards Early Endovascular Treatment of Type B Dissection justified? Dittmar Böckler Department of Vascular and Endovascular Surgery University of Heidelberg, Germany Disclosure Speaker
Chungbuk Regional Cardiovascular Center, Division of Cardiology, Departments of Internal Medicine, Chungbuk National University Hospital Sangmin Kim
 Endovascular Procedures for Isolated Common Iliac and Internal Iliac Aneurysm Chungbuk Regional Cardiovascular Center, Division of Cardiology, Departments of Internal Medicine, Chungbuk National University
Endovascular Procedures for Isolated Common Iliac and Internal Iliac Aneurysm Chungbuk Regional Cardiovascular Center, Division of Cardiology, Departments of Internal Medicine, Chungbuk National University
Understanding the Predictors of Aneurysmal Degeneration in Type B Dissection
 Understanding the Predictors of Aneurysmal Degeneration in Type B Dissection A case example illustrating when early endovascular intervention may provide the best outcome. BY DITTMAR BÖCKLER, MD, PhD;
Understanding the Predictors of Aneurysmal Degeneration in Type B Dissection A case example illustrating when early endovascular intervention may provide the best outcome. BY DITTMAR BÖCKLER, MD, PhD;
Introducing the GORE TAG Conformable Thoracic Stent Graft with ACTIVE CONTROL System
 Introducing the GORE TAG Conformable Thoracic Stent Graft with ACTIVE CONTROL System K. Oikonomou Department of Vascular Surgery Regensburg University Disclosures W.L. Gore & Associates Sponsored Presentation
Introducing the GORE TAG Conformable Thoracic Stent Graft with ACTIVE CONTROL System K. Oikonomou Department of Vascular Surgery Regensburg University Disclosures W.L. Gore & Associates Sponsored Presentation
Development of Stent Graft. Kato et al. Development of an expandable intra-aortic prothesis for experimental aortic dissection.
 Development of Stent Graft Kato et al. Development of an expandable intra-aortic prothesis for experimental aortic dissection. ASAIO J 1993 The New England Journal of Medicine Downloaded from nejm.org
Development of Stent Graft Kato et al. Development of an expandable intra-aortic prothesis for experimental aortic dissection. ASAIO J 1993 The New England Journal of Medicine Downloaded from nejm.org
Thoracic Endovascular Aortic Repair (TEVAR) Indications and Basic Procedure
 Indications and Basic Procedure") Thoracic Endovascular Aortic Repair (TEVAR) Indications and Basic Procedure Tilo Kölbel, MD, PhD University Heart Center Hamburg University Hospital Eppendorf Disclosure Speaker name: Tilo Kölbel, MD I
Thoracic Endovascular Aortic Repair (TEVAR) Indications and Basic Procedure Tilo Kölbel, MD, PhD University Heart Center Hamburg University Hospital Eppendorf Disclosure Speaker name: Tilo Kölbel, MD I
Challenges with Complex Anatomies Advancing Care in Endovascular Aortic Treatment
 Challenges with Complex Anatomies Advancing Care in Endovascular Aortic Treatment Robert Y. Rhee, MD Chief, Vascular and Endovascular Surgery Director, Aortic Center Maimonides Medical Center Brooklyn,
Challenges with Complex Anatomies Advancing Care in Endovascular Aortic Treatment Robert Y. Rhee, MD Chief, Vascular and Endovascular Surgery Director, Aortic Center Maimonides Medical Center Brooklyn,
High Risk Uncomplicated Type B Dissection
 High Risk Uncomplicated Type B Dissection Ali Azizzadeh, MD, FACS Director, Vascular Surgery Vice Chair, Department of Surgery Associate Director, Heart Institute Cedars-Sinai Medical Center Los Angeles,
High Risk Uncomplicated Type B Dissection Ali Azizzadeh, MD, FACS Director, Vascular Surgery Vice Chair, Department of Surgery Associate Director, Heart Institute Cedars-Sinai Medical Center Los Angeles,
Follow-up of Aortic Dissection: How, How Often, Which Consequences Euro Echo 2011
 Follow-up of Aortic Dissection: How, How Often, Which Consequences Euro Echo 2011 Susan E. Wiegers, MD, FASE Director of Clinical Echocardiography Hospital of the University of Pennsylvania Disclosure
Follow-up of Aortic Dissection: How, How Often, Which Consequences Euro Echo 2011 Susan E. Wiegers, MD, FASE Director of Clinical Echocardiography Hospital of the University of Pennsylvania Disclosure
Emerging Roles for Distal Aortic Interventions in Type A Dissection Surgery
 Emerging Roles for Distal Aortic Interventions in Type A Dissection Surgery Type A Dissection Workshop 2014 CCC Vancouver Oct 26 th, 2014 Jehangir Appoo Libin Cardiovascular Institute University of Calgary
Emerging Roles for Distal Aortic Interventions in Type A Dissection Surgery Type A Dissection Workshop 2014 CCC Vancouver Oct 26 th, 2014 Jehangir Appoo Libin Cardiovascular Institute University of Calgary
Early outcomes of acute retrograde dissection in the aortic arch and the ascending aorta data from IRAD
 Early outcomes of acute retrograde dissection in the aortic arch and the ascending aorta data from IRAD Foeke JH Nauta, MD, PhD Resident Cardiothoracic Surgery, Academic Medical Center, Amsterdam Disclosure
Early outcomes of acute retrograde dissection in the aortic arch and the ascending aorta data from IRAD Foeke JH Nauta, MD, PhD Resident Cardiothoracic Surgery, Academic Medical Center, Amsterdam Disclosure
Early Clinical Results with the Valiant Mona LSA Branch Stent-Graft
 Early Clinical Results with the Valiant Mona LSA Branch Stent-Graft Frank R. Arko III, MD Professor of Cardiovascular Surgery Director, Endovascular Surgery Co-Director, Aortic Institute Carolinas Medical
Early Clinical Results with the Valiant Mona LSA Branch Stent-Graft Frank R. Arko III, MD Professor of Cardiovascular Surgery Director, Endovascular Surgery Co-Director, Aortic Institute Carolinas Medical
ADSORB trial results: Is it enough to switch the paradigm?
 ADSORB trial results: Is it enough to switch the paradigm? Jan Brunkwall, MD, PhD Professor and Chairman Complications to acute type B dissection Mortality Rupture Organ Ischemia Dilatation/Aneurysm Refractory
ADSORB trial results: Is it enough to switch the paradigm? Jan Brunkwall, MD, PhD Professor and Chairman Complications to acute type B dissection Mortality Rupture Organ Ischemia Dilatation/Aneurysm Refractory
My personal experience with INCRAFT in standard and challenging cases
 My personal experience with INCRAFT in standard and challenging cases G Pratesi, MD Vascular Surgery University of Rome Tor Vergata giovanni.pratesi@uniroma2.it Disclosure Speaker name: Giovanni Pratesi,
My personal experience with INCRAFT in standard and challenging cases G Pratesi, MD Vascular Surgery University of Rome Tor Vergata giovanni.pratesi@uniroma2.it Disclosure Speaker name: Giovanni Pratesi,
Indications for stent grafts in type B aortic dissection
 expert opinion I Akin C A Nienaber Indications for stent grafts in type B aortic dissection ibrahim akin christoph a nienaber Department of Medicine, Divisions of Cardiology, Pulmology and Intensive Care
expert opinion I Akin C A Nienaber Indications for stent grafts in type B aortic dissection ibrahim akin christoph a nienaber Department of Medicine, Divisions of Cardiology, Pulmology and Intensive Care
Open fenestration for complicated acute aortic B dissection
 Art of Operative Techniques Open fenestration for complicated acute aortic B dissection Santi Trimarchi 1, Sara Segreti 1, Viviana Grassi 1, Chiara Lomazzi 1, Marta Cova 1, Gabriele Piffaretti 2, Vincenzo
Art of Operative Techniques Open fenestration for complicated acute aortic B dissection Santi Trimarchi 1, Sara Segreti 1, Viviana Grassi 1, Chiara Lomazzi 1, Marta Cova 1, Gabriele Piffaretti 2, Vincenzo
Title. Different arch branched devices are available, is morphology the. main criteria of choice? Ciro Ferrer, MD
 Different arch branched devices are available, is morphology the Title main criteria of choice? Ciro Ferrer, MD Vascular Surgery Unit Sapienza University of Rome Disclosure Speaker name: Ciro Ferrer Proctoring/speaking
Different arch branched devices are available, is morphology the Title main criteria of choice? Ciro Ferrer, MD Vascular Surgery Unit Sapienza University of Rome Disclosure Speaker name: Ciro Ferrer Proctoring/speaking
Indications for use. Contraindications within the United States
 Indications for use Indications within the United States The GORE TAG Thoracic Endoprosthesis is intended for endovascular repair of all lesions of the descending thoracic aorta, including: Isolated lesions
Indications for use Indications within the United States The GORE TAG Thoracic Endoprosthesis is intended for endovascular repair of all lesions of the descending thoracic aorta, including: Isolated lesions
Free Esophageal Perforation Following Hybrid Visceral Debranching and Distal Endograft Extension to Repair a Ruptured Thoracoabdominal Aortic
 Free Esophageal Perforation Following Hybrid Visceral Debranching and Distal Endograft Extension to Repair a Ruptured Thoracoabdominal Aortic Aneurysm History A 56-year-old gentleman, who had been referred
Free Esophageal Perforation Following Hybrid Visceral Debranching and Distal Endograft Extension to Repair a Ruptured Thoracoabdominal Aortic Aneurysm History A 56-year-old gentleman, who had been referred
Optimal repair of acute aortic dissection
 Optimal repair of acute aortic dissection Dept. of Vascular Surgery, The 2nd Xiang-Yale Hospital, Central-South University, China Hunan Major Vessels Diseases Clinical Center Chang Shu Email:changshu01@yahoo.com
Optimal repair of acute aortic dissection Dept. of Vascular Surgery, The 2nd Xiang-Yale Hospital, Central-South University, China Hunan Major Vessels Diseases Clinical Center Chang Shu Email:changshu01@yahoo.com
Asymptomatic Radiology / Clinical data Report / Cohort bias Referral bias. UCSF Vascular Symposium April 7-9, Acute Aortic Dissection
 Aortic Dissection: Natural History What is the Natural History of Aortic Dissection? UCSF Vascular Symposium April 7-9, 2011 Asymptomatic Radiology / Clinical data Report / Cohort bias Referral bias Stephen
Aortic Dissection: Natural History What is the Natural History of Aortic Dissection? UCSF Vascular Symposium April 7-9, 2011 Asymptomatic Radiology / Clinical data Report / Cohort bias Referral bias Stephen
The Role of Stent-Grafts in Marfan Syndrome
 The Role of Stent-Grafts in Marfan Syndrome James H. Black, III, MD, FACS The David Goldfarb, MD, Associate Professor of Surgery Chief, Division of Vascular Surgery and Endovascular Therapy The Johns Hopkins
The Role of Stent-Grafts in Marfan Syndrome James H. Black, III, MD, FACS The David Goldfarb, MD, Associate Professor of Surgery Chief, Division of Vascular Surgery and Endovascular Therapy The Johns Hopkins
FEVAR FIFTEEN YEARS OF EFFICIENCY E.DUCASSE MD PHD FEBVS CHU DE BORDEAUX
 FEVAR FIFTEEN YEARS OF EFFICIENCY E.DUCASSE MD PHD FEBVS CHU DE BORDEAUX 2018 A BIT OF HISTORY First use of F-EVAR : 1990s Park et al. J Vasc Interv Radiol. 1996;7:819-823. Faruqi et al. J Endovasc Surg.
FEVAR FIFTEEN YEARS OF EFFICIENCY E.DUCASSE MD PHD FEBVS CHU DE BORDEAUX 2018 A BIT OF HISTORY First use of F-EVAR : 1990s Park et al. J Vasc Interv Radiol. 1996;7:819-823. Faruqi et al. J Endovasc Surg.
account for 10% to 15% of all traffic fatalities majority fatal at the scene 50% who survive the initial injury die in the first 24 hours 90% die
 account for 10% to 15% of all traffic fatalities majority fatal at the scene 50% who survive the initial injury die in the first 24 hours 90% die within the first month if aorta not repaired 30-90% overall
account for 10% to 15% of all traffic fatalities majority fatal at the scene 50% who survive the initial injury die in the first 24 hours 90% die within the first month if aorta not repaired 30-90% overall
Modified candy-plug technique for chronic type B aortic dissection with aneurysmal dilatation: a case report
 Kotani et al. Journal of Cardiothoracic Surgery (2017) 12:77 DOI 10.1186/s13019-017-0647-8 CASE REPORT Modified candy-plug technique for chronic type B aortic dissection with aneurysmal dilatation: a case
Kotani et al. Journal of Cardiothoracic Surgery (2017) 12:77 DOI 10.1186/s13019-017-0647-8 CASE REPORT Modified candy-plug technique for chronic type B aortic dissection with aneurysmal dilatation: a case
IMH/Penetrating Aortic Ulcers/ Saccular Aneurysms: How to manage and when to intervene
 IMH/Penetrating Aortic Ulcers/ Saccular Aneurysms: How to manage and when to intervene UCSF Vascular Surgery Symposium 2018 Sukgu M Han, MD, MS Assistant Professor of Clinical Surgery Co-director, Comprehensive
IMH/Penetrating Aortic Ulcers/ Saccular Aneurysms: How to manage and when to intervene UCSF Vascular Surgery Symposium 2018 Sukgu M Han, MD, MS Assistant Professor of Clinical Surgery Co-director, Comprehensive
Acute Aortic Dissection: Decision and Outcome
 Acute Aortic Dissection: Decision and Outcome Marc R. Moon, M.D. John M. Shoenberg Chair in CV Disease Chief, Cardiac Surgery Director, Center for Diseases of the Thoracic Aorta Washington University School
Acute Aortic Dissection: Decision and Outcome Marc R. Moon, M.D. John M. Shoenberg Chair in CV Disease Chief, Cardiac Surgery Director, Center for Diseases of the Thoracic Aorta Washington University School
I have the following financial relationships to disclose:
 Novel Approaches to Endovascular Management of Aortic Aneurysms Rodney A White, MD Medical Director, Vascular Services MemorialCare Heart & Vascular Institute Long Beach Memorial Hospital Long Beach, California
Novel Approaches to Endovascular Management of Aortic Aneurysms Rodney A White, MD Medical Director, Vascular Services MemorialCare Heart & Vascular Institute Long Beach Memorial Hospital Long Beach, California
Paraplegia in endovascular repair of TAA and in TEVAR: Incidence, prevention and therapy. Johannes Lammer Medical University Vienna, Austria
 Paraplegia in endovascular repair of TAA and in TEVAR: Incidence, prevention and therapy Johannes Lammer Medical University Vienna, Austria Conflict of interests: none 68y, male, PAU in coral reef aorta,
Paraplegia in endovascular repair of TAA and in TEVAR: Incidence, prevention and therapy Johannes Lammer Medical University Vienna, Austria Conflict of interests: none 68y, male, PAU in coral reef aorta,
Endovascular Treatment of Malperfusion Syndrome
 Endovascular Treatment of Malperfusion Syndrome in Type B Aortic Dissection Department of Cardiology, Pusan National luniveristy i Hospital, Han Cheol Lee Endovascular Treatment Indication of Type B Aortic
Endovascular Treatment of Malperfusion Syndrome in Type B Aortic Dissection Department of Cardiology, Pusan National luniveristy i Hospital, Han Cheol Lee Endovascular Treatment Indication of Type B Aortic
Development of a Branched LSA Endograft & Ascending Aorta Endograft
 Development of a Branched LSA Endograft & Ascending Aorta Endograft Frank R. Arko III, MD Sanger Heart & Vascular Institute Carolinas Medical Center Charlotte, North Carolina, USA Disclosures Proximal
Development of a Branched LSA Endograft & Ascending Aorta Endograft Frank R. Arko III, MD Sanger Heart & Vascular Institute Carolinas Medical Center Charlotte, North Carolina, USA Disclosures Proximal
Redo treatment and open conversion after TEVAR
 Redo treatment and open conversion after TEVAR Roberto Chiesa Vascular Surgery, Vita-Salute University Scientific Institute San Raffaele Milan, Italy Number of procedures Off-Label indications for TEVAR
Redo treatment and open conversion after TEVAR Roberto Chiesa Vascular Surgery, Vita-Salute University Scientific Institute San Raffaele Milan, Italy Number of procedures Off-Label indications for TEVAR
False Lumen Backflow In Chronic Aortic Dissections: What Is Its Role and How Can It Be Treated?
 University Heart Center Hamburg GERMAN AORTIC CENTER False Lumen Backflow In Chronic Aortic Dissections: What Is Its Role and How Can It Be Treated? Tilo Kölbel, Nikos Tsilimparis, Sabine Wipper, Sebastian
University Heart Center Hamburg GERMAN AORTIC CENTER False Lumen Backflow In Chronic Aortic Dissections: What Is Its Role and How Can It Be Treated? Tilo Kölbel, Nikos Tsilimparis, Sabine Wipper, Sebastian
RETROGRADE BRANCH. Gustavo S. Oderich MD Professor of Surgery Director of Endovascular Therapy Division of Vascular and Endovascular Surgery
 RETROGRADE BRANCH Gustavo S. Oderich MD Professor of Surgery Director of Endovascular Therapy Division of Vascular and Endovascular Surgery FACULTY DISCLOSURE Consulting* Cook Medical Inc., WL Gore Research
RETROGRADE BRANCH Gustavo S. Oderich MD Professor of Surgery Director of Endovascular Therapy Division of Vascular and Endovascular Surgery FACULTY DISCLOSURE Consulting* Cook Medical Inc., WL Gore Research
Stanford Division of Vascular Surgery
 Stanford Division of Vascular Surgery Interesting Cases 10/11/10 Vascular Surgery HPI: 62yoM with h/o CAD, HTN, ETOH abuse. S/P EVAR in 5/08 for 6cm AAA and right CIA aneurysm. Cook 30x96mm Main Body 24
Stanford Division of Vascular Surgery Interesting Cases 10/11/10 Vascular Surgery HPI: 62yoM with h/o CAD, HTN, ETOH abuse. S/P EVAR in 5/08 for 6cm AAA and right CIA aneurysm. Cook 30x96mm Main Body 24
CT angiography in type I acute aortic dissection complicated with malperfusion - a visual review of obstruciton patterns
 CT angiography in type I acute aortic dissection complicated with malperfusion - a visual review of obstruciton patterns Eneva M. St. Ekaterna University Hospital Report objectives 1. Review malperfusion
CT angiography in type I acute aortic dissection complicated with malperfusion - a visual review of obstruciton patterns Eneva M. St. Ekaterna University Hospital Report objectives 1. Review malperfusion
Toward Total Endovascular Therapy of the Aorta. Adam W. Beck, MD. Associate Professor of Surgery Division of Vascular Surgery and Endovascular Therapy
 Toward Total Endovascular Therapy of the Aorta Adam W. Beck, MD Associate Professor of Surgery Division of Vascular Surgery and Endovascular Therapy University of Alabama at Birmingham Disclosures Grant
Toward Total Endovascular Therapy of the Aorta Adam W. Beck, MD Associate Professor of Surgery Division of Vascular Surgery and Endovascular Therapy University of Alabama at Birmingham Disclosures Grant
Accepted Manuscript. Is A More Extensive Operation Justified for Acute Type A Dissection Repair? Dr. Leonard N. Girardi
 Accepted Manuscript Is A More Extensive Operation Justified for Acute Type A Dissection Repair? Dr. Leonard N. Girardi PII: S0022-5223(18)32552-2 DOI: 10.1016/j.jtcvs.2018.09.048 Reference: YMTC 13502
Accepted Manuscript Is A More Extensive Operation Justified for Acute Type A Dissection Repair? Dr. Leonard N. Girardi PII: S0022-5223(18)32552-2 DOI: 10.1016/j.jtcvs.2018.09.048 Reference: YMTC 13502
Talent Abdominal Stent Graft
 Talent Abdominal with THE Xcelerant Hydro Delivery System Expanding the Indications for EVAR Treat More Patients Short Necks The Talent Abdominal is the only FDA-approved device for proximal aortic neck
Talent Abdominal with THE Xcelerant Hydro Delivery System Expanding the Indications for EVAR Treat More Patients Short Necks The Talent Abdominal is the only FDA-approved device for proximal aortic neck
Type B Dissection Sub-Categories
 Disclosure Nothing to disclose Type B Dissection On Whom to Operate on and When to do it Charles Eichler Professor, Department of Surgery Division of Vascular and Endovascular Surgery University of California
Disclosure Nothing to disclose Type B Dissection On Whom to Operate on and When to do it Charles Eichler Professor, Department of Surgery Division of Vascular and Endovascular Surgery University of California
The role of false lumen intervention to promote remodelling via induced thrombosis the FLIRT concept
 The role of false lumen intervention to promote remodelling via induced thrombosis the FLIRT concept Professor Christoph A. Nienaber The Royal Brompton and Harefield NHS Trust Cardiology and Aortic Centre
The role of false lumen intervention to promote remodelling via induced thrombosis the FLIRT concept Professor Christoph A. Nienaber The Royal Brompton and Harefield NHS Trust Cardiology and Aortic Centre
Nellix Endovascular System: Clinical Outcomes and Device Overview
 Nellix Endovascular System: Clinical Outcomes and Device Overview Jeffrey P. Carpenter, MD Professor and Chief, Department of Surgery CAUTION: Investigational device. This product is under clinical investigation
Nellix Endovascular System: Clinical Outcomes and Device Overview Jeffrey P. Carpenter, MD Professor and Chief, Department of Surgery CAUTION: Investigational device. This product is under clinical investigation
Current State of Thoracic Branch Devices and Ongoing Clinical Trials
 Current State of Thoracic Branch Devices and Ongoing Clinical Trials Hiroo Takayama, MD, PhD Associate Professor of Surgery Director of Cardiovascular Institute Co-Director of Aortic Center NY Presbyterian/Columbia
Current State of Thoracic Branch Devices and Ongoing Clinical Trials Hiroo Takayama, MD, PhD Associate Professor of Surgery Director of Cardiovascular Institute Co-Director of Aortic Center NY Presbyterian/Columbia
Current treatment of Aortic Aneurysms and Dissections. Adam Keefer, MD, FACS Sean Hislop, MD, FACS
 Current treatment of Aortic Aneurysms and Dissections Adam Keefer, MD, FACS Sean Hislop, MD, FACS Patient 1 69 year old well-educated man with reoccurring pain in his upper abdomen and a pulsatile mass.
Current treatment of Aortic Aneurysms and Dissections Adam Keefer, MD, FACS Sean Hislop, MD, FACS Patient 1 69 year old well-educated man with reoccurring pain in his upper abdomen and a pulsatile mass.
Thoracoabdominal Aorta: Advances and Novel Therapies
 Thoracoabdominal Aorta: Advances and Novel Therapies Robert Meisner, MD FACS Sidney Kimmel Medical Center Assistant Professor of Surgery Vascular / Endovascular Surgeon at Lankenau Medical Center November
Thoracoabdominal Aorta: Advances and Novel Therapies Robert Meisner, MD FACS Sidney Kimmel Medical Center Assistant Professor of Surgery Vascular / Endovascular Surgeon at Lankenau Medical Center November
Subclavian Artery Plug Embolization (SAPE study): a real experience about endovascular subclavian occlusion prior to thoracic vascular repair
: a real experience about endovascular subclavian occlusion prior to thoracic vascular repair") Subclavian Artery Plug Embolization (SAPE study): a real experience about endovascular subclavian occlusion prior to thoracic vascular repair Simone Salvati, Luca Bertoglio, Alessandra Fittipaldi, Andrea
Subclavian Artery Plug Embolization (SAPE study): a real experience about endovascular subclavian occlusion prior to thoracic vascular repair Simone Salvati, Luca Bertoglio, Alessandra Fittipaldi, Andrea
Re-interventions after TEVAR:
 Re-interventions after TEVAR: How often does it occur and what are procedures most commonly utilized to treat these issues? Pacific Northwest Endovascular Conference Seattle, WA June 15, 2018 PENN Surgery
Re-interventions after TEVAR: How often does it occur and what are procedures most commonly utilized to treat these issues? Pacific Northwest Endovascular Conference Seattle, WA June 15, 2018 PENN Surgery
La sindrome aortica acuta oggi
 University of Milan Thoracic Aortic Research Center La sindrome aortica acuta oggi Santi Trimarchi, MD, PhD Professore Associato di Chirurgia Vascolare, Università degli Studi di Milano Direttore, Divisione
University of Milan Thoracic Aortic Research Center La sindrome aortica acuta oggi Santi Trimarchi, MD, PhD Professore Associato di Chirurgia Vascolare, Università degli Studi di Milano Direttore, Divisione
THORACOABDOMINAL AORTIC ANEURYSMS HYBRID REPAIR
 Update on Open and Endovascular Therapeutic Option for Aortic Repair CENTRE CARDIO-TORACIQUE DE MONACO Friday November 7 th, 2014 THORACOABDOMINAL AORTIC ANEURYSMS HYBRID REPAIR Roberto Chiesa Vascular
Update on Open and Endovascular Therapeutic Option for Aortic Repair CENTRE CARDIO-TORACIQUE DE MONACO Friday November 7 th, 2014 THORACOABDOMINAL AORTIC ANEURYSMS HYBRID REPAIR Roberto Chiesa Vascular
Improving Endograft Durability with EndoAnchors
 Improving Endograft Durability with EndoAnchors William D. Jordan, Jr., M.D. John E. Skandalakis Chair in Surgery Professor and Chief Division of Vascular Surgery and Endovascular Therapy Emory University
Improving Endograft Durability with EndoAnchors William D. Jordan, Jr., M.D. John E. Skandalakis Chair in Surgery Professor and Chief Division of Vascular Surgery and Endovascular Therapy Emory University
ENCORE, a Study to Investigate the Durability of Polymer EVAR with Ovation A Contemporary Review of 1296 Patients
 ENCORE, a Study to Investigate the Durability of Polymer EVAR with Ovation A Contemporary Review of 1296 Patients The Ovation System is approved to treat infrarenal abdominal aortic aneurysms and is not
ENCORE, a Study to Investigate the Durability of Polymer EVAR with Ovation A Contemporary Review of 1296 Patients The Ovation System is approved to treat infrarenal abdominal aortic aneurysms and is not
Aortic Neck Issues Associated Clinical Sequelae/Implications for Graft Choice
 Aortic Neck Issues Associated Clinical Sequelae/Implications for Graft Choice Eric Verhoeven, MD, PhD, A. Katsargyris, MD Department of Vascular and Endovascular Surgery, Paracelsus Medical University,
Aortic Neck Issues Associated Clinical Sequelae/Implications for Graft Choice Eric Verhoeven, MD, PhD, A. Katsargyris, MD Department of Vascular and Endovascular Surgery, Paracelsus Medical University,
COMPLICATIONS OF TEVAR
 COMPLICATIONS OF TEVAR P. Bergeron, A.Petrosyan, F.Markatis, T.Abdulamit, J.-C. Trastour IMAD CONGRESS 2010 Liège Belgium BACKGROUND Stentgrafting is a recognized treatment for TAA & TAD and has been proposed
COMPLICATIONS OF TEVAR P. Bergeron, A.Petrosyan, F.Markatis, T.Abdulamit, J.-C. Trastour IMAD CONGRESS 2010 Liège Belgium BACKGROUND Stentgrafting is a recognized treatment for TAA & TAD and has been proposed
Risks for Retrograde Type-A Dissection After TEVAR
 Risks for Retrograde Type-A Dissection After TEVAR Frank R. Arko, III, MD Chief, Vascular and Endovascular Surgery Professor, Cardiovascular Surgery Co-Director, Aortic Institute Sanger Heart and Vascular
Risks for Retrograde Type-A Dissection After TEVAR Frank R. Arko, III, MD Chief, Vascular and Endovascular Surgery Professor, Cardiovascular Surgery Co-Director, Aortic Institute Sanger Heart and Vascular
STS/EACTS LatAm CV Conference 2017
 STS/EACTS LatAm CV Conference 2017 Joseph E. Bavaria, MD Director, Thoracic Aortic Surgery Program Roberts-Measey Professor and Vice Chair of CV Surgery University of Pennsylvania Immediate-Past President
STS/EACTS LatAm CV Conference 2017 Joseph E. Bavaria, MD Director, Thoracic Aortic Surgery Program Roberts-Measey Professor and Vice Chair of CV Surgery University of Pennsylvania Immediate-Past President
Intravascular Ultrasound in the Treatment of Complex Aortic Pathologies. Naixin Kang, M.D. Vascular Surgery Fellow April 26 th, 2018
 Intravascular Ultrasound in the Treatment of Complex Aortic Pathologies Naixin Kang, M.D. Vascular Surgery Fellow April 26 th, 2018 DISCLOSURES Nothing To Disclose 2 ENDOVASCULAR AORTIC INTERVENTION Improved
Intravascular Ultrasound in the Treatment of Complex Aortic Pathologies Naixin Kang, M.D. Vascular Surgery Fellow April 26 th, 2018 DISCLOSURES Nothing To Disclose 2 ENDOVASCULAR AORTIC INTERVENTION Improved
Retrograde Embolization of a Symptomatic Hypogastric Artery Aneurysm
 Retrograde Embolization of a Symptomatic Hypogastric Artery Aneurysm Andrew Unzeitig MD Piedmont Atlanta Hospital Georgia Vascular Society 2017 Annual Meeting Lake Oconee, Georgia Disclosures None Case
Retrograde Embolization of a Symptomatic Hypogastric Artery Aneurysm Andrew Unzeitig MD Piedmont Atlanta Hospital Georgia Vascular Society 2017 Annual Meeting Lake Oconee, Georgia Disclosures None Case