Blood Pressure Management in Acute Ischemic Stroke
|
|
|
- Terence Day
- 6 years ago
- Views:
Transcription
1 Blood Pressure Management in Acute Ischemic Stroke Kimberly Clark, PharmD, BCCCP Clinical Pharmacy Specialist Critical Care, Greenville Health System Adjunct Assistant Professor, South Carolina College of Pharmacy
2 Objectives Define acute hypertensive response and its impact on patient outcomes Review the guideline recommendations for blood pressure (BP) management in acute ischemic stroke (AIS) Examine newly published literature Compare available antihypertensive agents
3 Acute Hypertensive Response Profound BP elevations are common during the acute phase of stroke even among patients without a prior history of hypertension In the US National Hospital Ambulatory Medical Care Survey, 76.5% of patients with AIS had systolic blood pressure (SBP) 140 mm Hg on arrival Circulation 2015;133:e38-e360.
4 BP Effect on Outcomes Stroke 2002;33:
5 Why Not Treat? BP typically decreases spontaneously during AIS, starting within 90 minutes after onset of stroke symptoms Lowering BP in patients with hypertension might reduce blood flow from collateral vessels to the ischemic penumbra and lead to loss of neurons Stroke 2013;44:
6 Acute Ischemic Stroke (non-tpa) AHA/ASA 2013 Guideline Recommendation Do not lower blood pressure during the initial 24 hours of acute ischemic stroke unless the blood pressure is >220/120 mm Hg or there is a concomitant specific medical condition that would benefit from blood pressure lowering Stroke 2013;44:
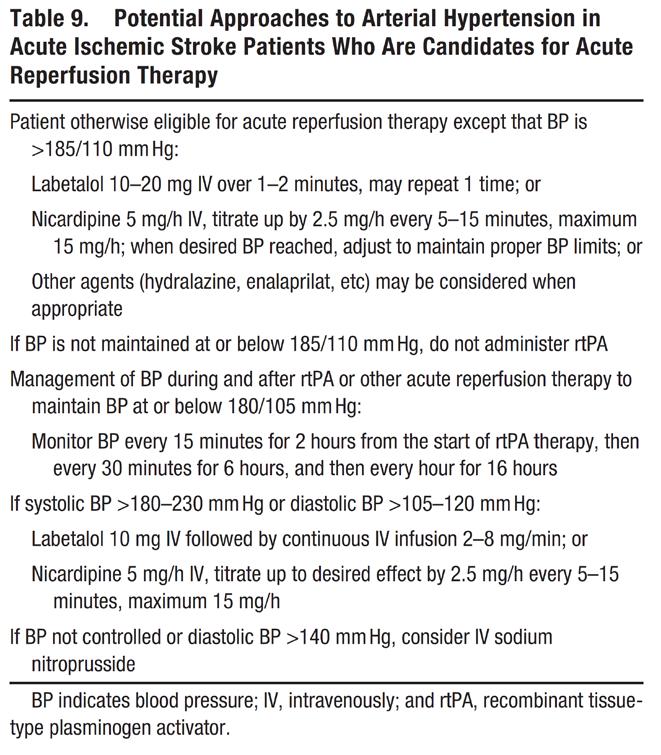
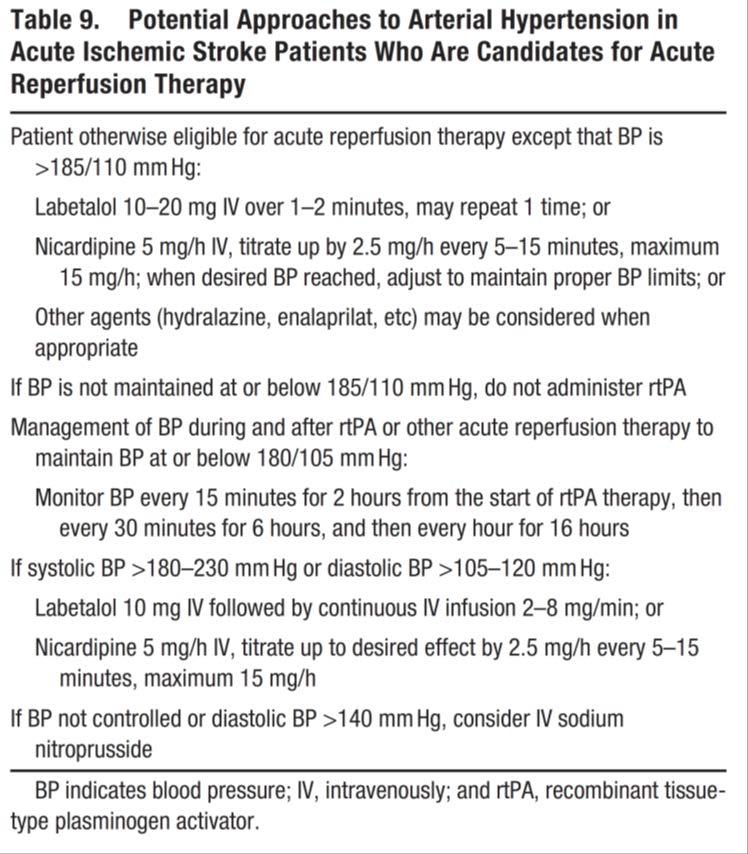
7 Acute Ischemic Stroke and tpa AHA/ASA 2013 Guideline Recommendation To limit the risk of ICH: Blood pressure should be lowered to <185/110 mmhg prior to fibrinolytic therapy with tpa Once tpa is given, the blood pressure must be maintained <180/105 mmhg for at least the first 24 hours Stroke 2013;44:
8 CATIS China Antihypertensive Trial in Acute Ischemic Stroke Randomized, controlled, single blind trial Multicenter 26 hospitals across China Inclusion 22 years old Ischemic stroke, confirmed by CT or MRI, within 48 hours of symptom onset Elevated SBP between 140 mmhg and 220 mmhg Exclusion Hemorrhagic stroke Severe heart failure, acute myocardial infarction or unstable angina, atrial fibrillation, aortic dissection, cerebrovascular stenosis SBP 220mmHg or DBP 120mmHg Resistant hypertension Treated with IV thrombolytic therapy (i.e. tpa) Deep coma Pregnant JAMA. 2014;311:
9 Intervention Antihypertensive treatment group Lower SBP by 10%-25% within the first 24 hrs BP < 140/90 mmhg within 7 days and for remainder of hospitalization Protocol did not require the use of specific antihypertensive medications For all patients On admission, home antihypertensive medications were held At discharge, patients were prescribed antihypertensive medications according to clinical guidelines JAMA. 2014;311:
10 Baseline Characteristics Treatment (n=2038) Control (n=2033) Age, years Male (%) Time from onset to randomization, hrs, mean (SD) 15 (13) 15 (13) History of HTN (%) Current use of BP meds (%) BP at entry, mmhg Systolic Diastolic NIHSS score, median 4 (2-7) 4 (3-8) Stroke subtype (%) Thrombotic Embolic Lacunar JAMA. 2014;311:

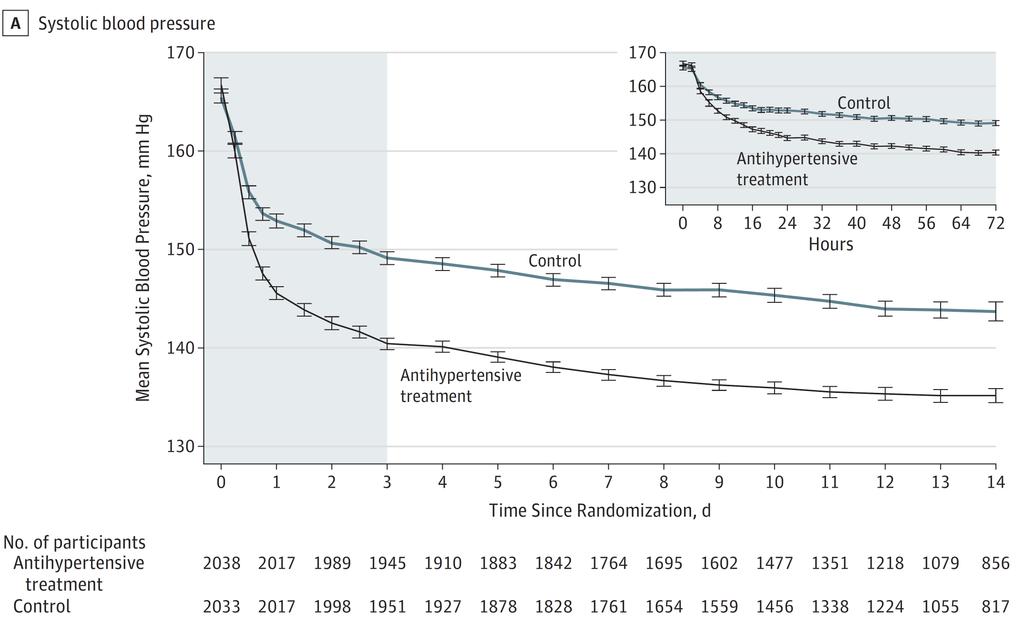
11 BP Reduction JAMA. 2014;311:
12 Outcomes Primary Outcome Death or major disability at 14 days or discharge Secondary Outcomes Death or major disability at 3 months Modified Rankin Scale at 14 days or discharge Modified Rankin Scale at 3 months Treatment (n=2038) Control (n=2033) p-value 34% 34% % 25% (1-3) 2 (1-3) (1-3) 1 (1-3) 0.52 Recurrent stroke 1.4% 2.2% 0.07 Vascular events 2.4% 3.0% 0.28 JAMA. 2014;311:
13 Subgroup Analysis JAMA. 2014;311:
14 Subgroup Analysis JAMA. 2014;311:
15 Author s Conclusion Unless a patient s SBP is 220 mmhg or DBP 120 mmhg, the decision to lower blood pressure with antihypertensive treatment in patients with AIS does not improve or worsen outcome and therefore should be based on individual clinical judgment JAMA. 2014;311:
16 Critique Strengths Meets statistical power Only ischemic stroke patients Discontinued home medications in both groups Not limited to a single medication or combination Well separated BP levels Limitations All Chinese patients Low median NIHSS score Did not repeat neurologic function tests or brain imaging within the first 24 hrs JAMA. 2014;311:
17 ENCHANTED ENhanced Control of Hypertension and Thrombolysis stroke study International (mostly China), multicenter, prospective, randomized, open-label trial with blinded outcome evaluation Intervention Conventional guideline-directed: SBP <180 mg (since all patients received tpa) Early and intensive: SBP mmhg within 1 hr (maintained for 72 hrs) Primary outcome Combined endpoint of death and disability (defined by the modified Rankin Scale) at 90 days Sample size 2,800 Study to be completed in 2018 World Stroke Organization 2015;10:
18 Acute Ischemic Stroke (non-tpa) AHA/ASA 2013 Guideline Recommendation Do not lower blood pressure during the initial 24 hours of acute ischemic stroke unless the blood pressure is >220/120 mm Hg or there is a concomitant specific medical condition that would benefit from blood pressure lowering Stroke 2013;44:
19 Additional Guideline Recommendations Reasonable to temporarily discontinue or reduce home antihypertensive medications at the onset of AIS Reasonable to initiate long-term antihypertensive therapy after the initial 24 hours from stroke onset but an optimal long-term antihypertensive therapy has not been definitively established Controlled blood pressure lowering can best be achieved with intravenous antihypertensive therapies but a single optimal medication has not been determined Stroke 2013;44:
20 IV Antihypertensive Therapies Stroke 2013;44:
21 Labetalol (Trandate) MOA: Non-selective beta-blocker with alpha blocker properties Alpha to beta ratios vary by route (1:7 IV, 1:3 PO) Dosing Continuous infusion: mg/min (300 mg max per 24hrs) IV bolus: mg IV every 15 min Caution: asthma, acute heart failure Adverse effects: bronchospasm, HF exacerbation, bradycardia/heart block, volume overload Lexicomp Online, Lexi-Drugs, Hudson, Ohio: Lexi-Comp, Inc.; September 9, 2016
22 Nicardipine (Cardene) MOA: Dihydropyridine calcium channel blocker; results in vasodilation (arteries > veins) Dosing Continuous infusion: 5-15 mg/hr Caution: angina/myocardial infarction, acute heart failure, aortic stenosis Adverse effects: Reflex tachycardia, headache, flushing, volume overload Lexicomp Online, Lexi-Drugs, Hudson, Ohio: Lexi-Comp, Inc.; September 9, 2016
23 Labetalol vs. Nicardipine Prospective, randomized, single-center study Inclusion > 18 years old Admitted for primary ICH, SAH, or AIS Exclusion Traumatic etiology History of intracranial neoplasm Received IV antihypertensive medication within 24 hrs Imminent brain death Acute myocardial infarction or bradycardia Neurocrit Care 2013;19:41-47.
24 Intervention Labetalol IV bolus starting at 20 mg Repeat dosing every 15 min up to a maximum cumulative dose of 300 mg/day Nicardipine IV infusion starting at 5 mg/hr Titrated every 15 min by 2.5 mg/hr until therapeutic response achieved or max rate of 15 mg/hr BP monitoring Every 15 min until goal achieved Hourly thereafter for 24 hr period Neurocrit Care 2013;19:41-47.
25 Outcomes Outcome Labetalol (n=28) Nicardipine (n=26) p-value Goal BP achieved (%) <0.001 Time to goal, min 90 (30-900) 30 (15-120) Time at goal (%) 36 (13-72) 89 (80-100) <0.001 Number adjustments to reach goal Number adjustments to maintain goal 2 (1-5) 0 (0-1) < (2-8) 3 (0-5) 0.05 Hypotension (%) Bradycardia (%) Reflex tachycardia (%) Neurocrit Care 2013;19:41-47.
26 Author s Conclusion Nicardipine provides better BP control than labetalol over the first 24 h in acutely hypertensive stroke patients Neurocrit Care 2013;19:41-47.
27 Critique Strengths 24 hr evaluation period Studied guideline recommended therapies Limitations Compared IV bolus to infusion Not designed to look at clinical outcomes Neurocrit Care 2013;19:41-47.
28 Additional Intravenous Options Drug Onset / Duration Dose Adverse Effects / Precautions Enalaprilat (Vasotec) Hydralazine (Apresoline) Sodium nitroprusside (Nipride) 30 min; hrs mg IV every 4 6 hrs Renal insufficiency/failure, hyperkalemia CI: Pregnancy, renal artery stenosis (Note: long half-life) 10 min; 1 4 hrs 5 20 mg IV every 4 6 hrs Reflex tachycardia, headache, flushing Caution: Angina/MI, aortic dissection Immediate / 2 3 min after stopped mcg/kg/min Cyanide/thiocyanate toxicity, methemoglobinemia CI: Renal, hepatic failure Lexicomp Online, Lexi-Drugs, Hudson, Ohio: Lexi-Comp, Inc.; September 9, 2016
29 Transitioning to Oral Therapy Drug Dose Adverse Effects / Precautions Amlodipine (Norvasc) Lisinopril (Zestril) Candesartan (Atacand) 5-10 mg PO daily Reflex tachycardia, nausea, vomiting, headache, flushing Caution: Angina/MI, acute HF, increased ICP mg PO daily Renal insufficiency/failure, hyperkalemia, cough, angioedema CI: Pregnancy, renal artery stenosis mg PO daily Renal insufficiency/failure, hyperkalemia, cough, angioedema CI: Pregnancy, renal artery stenosis Lexicomp Online, Lexi-Drugs, Hudson, Ohio: Lexi-Comp, Inc.; September 9, 2016
30 Transition Tips Study Objective Identify treatment options to reduce time on IV nicardipine while providing optimal blood pressure management Patient Population 50% were stroke patients Results Trend toward improved transitioning with amlodipine Shortest time from start of oral agent to nicardipine discontinuation Fewest number of agents required during transition Fewest nicardipine transition failures Multiple antihypertensives required for optimal transitioning 94% required 2 antihypertensive agents Oral antihypertensives added early in nicardipine therapy Possibly associated with decreased ICU length of stay and medication cost
31 Take Home Points The majority of patients with AIS have an elevated BP on arrival Based on recent literature and guideline recommendations, there is no clinical benefit of lowering BP during the initial 24 hours of AIS (non-tpa) unless the BP is >220/120 mm Hg Nicardipine may provide a more rapid and consistent BP lowering effect in stroke patients
32 Blood Pressure Management in Acute Ischemic Stroke Kimberly Clark, PharmD, BCCCP Clinical Pharmacy Specialist Critical Care, Greenville Health System Adjunct Assistant Professor, South Carolina College of Pharmacy
33 Hemorrhagic Stroke AHA/ASA 2015 Guideline Recommendation High SBP is associated with greater hematoma expansion, neurological deterioration, and death and dependency Acute lowering of SBP to 140 mm Hg is safe and can be effective for improving functional outcome May be reasonable to consider aggressive reduction of BP with a continuous intravenous infusion and frequent BP monitoring Stroke 2015;46:
34 Aneurysmal Subarachnoid Hemorrhage AHA/ASA 2012 Guideline Recommendation The magnitude of blood pressure control to reduce the risk of rebleeding has not been established, but a decrease in SBP <160 mmhg is reasonable Stroke. 2012;43:00-00.
35 Chronic Management AHA/ASA 2014 Guideline Recommendation Initiation of BP therapy is indicated for previously untreated patients with ischemic stroke or TIA who, after the first several days, have an established BP 140/90 mmhg Optimal drug regimen to achieve the recommended level of reductions is uncertain because direct comparisons between regimens are limited Available data indicate that diuretics or the combination of diuretics and an angiotensinconverting enzyme inhibitor (ACEI) is useful Stroke. 2014;45:00-00.
36 Oral Options Drug Dose Adverse Effects / Precautions Lisinopril (Zestril) Candesartan (Atacand) mg PO daily Renal insufficiency/failure, hyperkalemia, cough, angioedema CI: Pregnancy, renal artery stenosis mg PO daily Renal insufficiency/failure, hyperkalemia, cough, angioedema CI: Pregnancy, renal artery stenosis Hydrochlorothiazide mg PO daily Hypokalemia, hypercalcemia, photosensitivity Caution: Gout, sulfa allergy Amlodipine (Norvasc) 5-10 mg PO daily Reflex tachycardia, nausea, vomiting, headache, flushing Caution: Angina/MI, acute HF, increased ICP Lexicomp Online, Lexi-Drugs, Hudson, Ohio: Lexi-Comp, Inc.; September 9, 2016
37 Blood Pressure Variability (BPV) Meta-Analysis of 7 studies: Systolic BPV was significantly associated with poor functional outcome (death or disability): pooled odds ratio per 10 mm Hg increment, 1.2; confidence interval ( ) Retrospective observational study of 1161 AIS patients: Odds of early neurological deterioration increased 14 21% with each increase of one standard deviation in the BPV Prospective study of 608 AIS patients: No association between BPV and in-hospital outcomes Stroke. 2015;46: Journal of Hypertension. 2015;33: American Journal of Hypertension. 2016;29:
Blood Pressure Reduction Among Acute Stroke Patients A Randomized Controlled Clinical Trial
 Blood Pressure Reduction Among Acute Stroke Patients A Randomized Controlled Clinical Trial Jiang He, Yonghong Zhang, Tan Xu, Weijun Tong, Shaoyan Zhang, Chung-Shiuan Chen, Qi Zhao, Jing Chen for CATIS
Blood Pressure Reduction Among Acute Stroke Patients A Randomized Controlled Clinical Trial Jiang He, Yonghong Zhang, Tan Xu, Weijun Tong, Shaoyan Zhang, Chung-Shiuan Chen, Qi Zhao, Jing Chen for CATIS
Protocol for IV rtpa Treatment of Acute Ischemic Stroke
 Protocol for IV rtpa Treatment of Acute Ischemic Stroke Acute stroke management is progressing very rapidly. Our team offers several options for acute stroke therapy, including endovascular therapy and
Protocol for IV rtpa Treatment of Acute Ischemic Stroke Acute stroke management is progressing very rapidly. Our team offers several options for acute stroke therapy, including endovascular therapy and
NURSING DEPARTMENT CRITICAL CARE POLICY MANUAL CRITICAL CARE PROTOCOLS. ACUTE CEREBROVASCULAR ACCIDENT TPA (ACTIVASE /alteplase) FOR THROMBOLYSIS
 FOR THROMBOLYSIS") NURSING DEPARTMENT CRITICAL CARE POLICY MANUAL CRITICAL CARE PROTOCOLS ACUTE CEREBROVASCULAR ACCIDENT TPA (ACTIVASE /alteplase) FOR THROMBOLYSIS I. Purpose : A. To reduce morbidity and mortality associated
NURSING DEPARTMENT CRITICAL CARE POLICY MANUAL CRITICAL CARE PROTOCOLS ACUTE CEREBROVASCULAR ACCIDENT TPA (ACTIVASE /alteplase) FOR THROMBOLYSIS I. Purpose : A. To reduce morbidity and mortality associated
Blood Pressure Management in Acute Stroke. Bradley Molyneaux, M.D., Ph.D. Departments of Neurology & Critical Care Medicine University of Pittsburgh
 Blood Pressure Management in Acute Stroke Bradley Molyneaux, M.D., Ph.D. Departments of Neurology & Critical Care Medicine University of Pittsburgh 80 yo M w/ R MCA syndrome NIHSS 14 A balancing act Cerebral
Blood Pressure Management in Acute Stroke Bradley Molyneaux, M.D., Ph.D. Departments of Neurology & Critical Care Medicine University of Pittsburgh 80 yo M w/ R MCA syndrome NIHSS 14 A balancing act Cerebral
How Low Should You Go? Management of Blood Pressure in Intracranial Hemorrhage
 How Low Should You Go? Management of Blood Pressure in Intracranial Hemorrhage Rachael Scott, Pharm.D. PGY2 Critical Care Pharmacy Resident Pharmacy Grand Rounds August 21, 2018 2018 MFMER slide-1 Patient
How Low Should You Go? Management of Blood Pressure in Intracranial Hemorrhage Rachael Scott, Pharm.D. PGY2 Critical Care Pharmacy Resident Pharmacy Grand Rounds August 21, 2018 2018 MFMER slide-1 Patient
Hypertensive Urgency and Emergency. Definitions. Emergency or Urgency?
 Hypertensive Urgency and Emergency Joel Handler MD Kaiser Permanente Care Management Institute/ SCal Region Hypertension Lead Definitions Hypertensive Emergency: -Severe elevation in BP with evidence of
Hypertensive Urgency and Emergency Joel Handler MD Kaiser Permanente Care Management Institute/ SCal Region Hypertension Lead Definitions Hypertensive Emergency: -Severe elevation in BP with evidence of
Hypertension. Does it Matter What Medications We Use? Nishant K. Sekaran, M.D. M.Sc. Intermountain Heart Institute
 Hypertension Does it Matter What Medications We Use? Nishant K. Sekaran, M.D. M.Sc. Intermountain Heart Institute Hypertension 2017 Classification BP Category Systolic Diastolic Normal 120 and 80 Elevated
Hypertension Does it Matter What Medications We Use? Nishant K. Sekaran, M.D. M.Sc. Intermountain Heart Institute Hypertension 2017 Classification BP Category Systolic Diastolic Normal 120 and 80 Elevated
Hypertension (JNC-8)
") Hypertension (JNC-8) Southern California University of Health Sciences Physician Assistant Program Management and Treatment of Hypertension April 17, 2018, presented by Ezra Levy, Pharm.D.! The 8 th Joint
Hypertension (JNC-8) Southern California University of Health Sciences Physician Assistant Program Management and Treatment of Hypertension April 17, 2018, presented by Ezra Levy, Pharm.D.! The 8 th Joint
2018 Early Management of Acute Ischemic Stroke Guidelines Update
 2018 Early Management of Acute Ischemic Stroke Guidelines Update Brandi Bowman, PhC, Pharm.D. April 17, 2018 Pharmacist Objectives Describe the recommendations for emergency medical services and hospital
2018 Early Management of Acute Ischemic Stroke Guidelines Update Brandi Bowman, PhC, Pharm.D. April 17, 2018 Pharmacist Objectives Describe the recommendations for emergency medical services and hospital
Hypertensive Crises. Controlling high blood pressure prevents disease. Recognition and Management of Acute Hypertensive Emergencies
 Controlling high blood pressure prevents disease Recognition and Management of Acute Hypertensive Emergencies David idweiner, M.D. Co-holder, C. Craig and Audrae Tisher Chair in Nephrology Functional Genomics
Controlling high blood pressure prevents disease Recognition and Management of Acute Hypertensive Emergencies David idweiner, M.D. Co-holder, C. Craig and Audrae Tisher Chair in Nephrology Functional Genomics
Antihypertensive Agents Part-2. Assistant Prof. Dr. Najlaa Saadi PhD Pharmacology Faculty of Pharmacy University of Philadelphia
 Antihypertensive Agents Part-2 Assistant Prof. Dr. Najlaa Saadi PhD Pharmacology Faculty of Pharmacy University of Philadelphia Agents that block production or action of angiotensin Angiotensin-converting
Antihypertensive Agents Part-2 Assistant Prof. Dr. Najlaa Saadi PhD Pharmacology Faculty of Pharmacy University of Philadelphia Agents that block production or action of angiotensin Angiotensin-converting
Policy REVISED: 6/30/2016 3:30 PM. Applies To: ObGyn Responsible Department: ObGyn Revised: June 30, 2016
 Title: Antihypertensive Treatment for Severe Hypertension During Pregnancy Applies To: ObGyn Responsible Department: ObGyn Revised: June 30, 2016 Policy POLICY STATEMENT: Pregnant or postpartum patients
Title: Antihypertensive Treatment for Severe Hypertension During Pregnancy Applies To: ObGyn Responsible Department: ObGyn Revised: June 30, 2016 Policy POLICY STATEMENT: Pregnant or postpartum patients
Hypertensives Emergency and Urgency
 Hypertensives Emergency and Urgency Budi Yuli Setianto Cardiology Divisision Department of Internal Medicine Faculty of Medicine UGM Sardjito Hospital Yogyakarta Background USA: Hypertension is 30% of
Hypertensives Emergency and Urgency Budi Yuli Setianto Cardiology Divisision Department of Internal Medicine Faculty of Medicine UGM Sardjito Hospital Yogyakarta Background USA: Hypertension is 30% of
Cerebral Autoregulation What s the Big Deal? Kathy Morrison MSN, RN, CNRN Gayle Watson MSN, RN, CCNS, CCRN
 Cerebral Autoregulation What s the Big Deal? Kathy Morrison MSN, RN, CNRN Gayle Watson MSN, RN, CCNS, CCRN Background 30% of patients have history of hypertension prior to stroke 80% will present with
Cerebral Autoregulation What s the Big Deal? Kathy Morrison MSN, RN, CNRN Gayle Watson MSN, RN, CCNS, CCRN Background 30% of patients have history of hypertension prior to stroke 80% will present with
Tony L Smith DNP RN ACNP CCRN CFRN EMT-IV Vanderbilt LifeFlight
 Treatment of a Stroke patient: A look at how to care for the Stroke patient in the aeromedical setting Tony L Smith DNP RN ACNP CCRN CFRN EMT-IV Vanderbilt LifeFlight Objectives 1. Discuss the assessment
Treatment of a Stroke patient: A look at how to care for the Stroke patient in the aeromedical setting Tony L Smith DNP RN ACNP CCRN CFRN EMT-IV Vanderbilt LifeFlight Objectives 1. Discuss the assessment
Introductory Clinical Pharmacology Chapter 41 Antihypertensive Drugs
 Introductory Clinical Pharmacology Chapter 41 Antihypertensive Drugs Blood Pressure Normal = sys
Introductory Clinical Pharmacology Chapter 41 Antihypertensive Drugs Blood Pressure Normal = sys
HYPERTENSION IN EMERGENCY MEDICINE Michael Jay Bresler, M.D., FACEP
 HYPERTENSION IN EMERGENCY MEDICINE Michael Jay Bresler, M.D., FACEP What is normal blood pressure? Prehypertension 130-139/80-90 Compared with normal BP Double the risk for developing hypertension. Lifestyle
HYPERTENSION IN EMERGENCY MEDICINE Michael Jay Bresler, M.D., FACEP What is normal blood pressure? Prehypertension 130-139/80-90 Compared with normal BP Double the risk for developing hypertension. Lifestyle
Chapter (9) Calcium Antagonists
 Calcium Antagonists") Chapter (9) Calcium Antagonists (CALCIUM CHANNEL BLOCKERS) Classification Mechanism of Anti-ischemic Actions Indications Drug Interaction with Verapamil Contraindications Adverse Effects Treatment of Drug
Chapter (9) Calcium Antagonists (CALCIUM CHANNEL BLOCKERS) Classification Mechanism of Anti-ischemic Actions Indications Drug Interaction with Verapamil Contraindications Adverse Effects Treatment of Drug
Chapter 23. Media Directory. Cardiovascular Disease (CVD) Hypertension: Classified into Three Categories
 Hypertension: Classified into Three Categories") Chapter 23 Drugs for Hypertension Slide 37 Slide 41 Media Directory Nifedipine Animation Doxazosin Animation Upper Saddle River, New Jersey 07458 All rights reserved. Cardiovascular Disease (CVD) Includes
Chapter 23 Drugs for Hypertension Slide 37 Slide 41 Media Directory Nifedipine Animation Doxazosin Animation Upper Saddle River, New Jersey 07458 All rights reserved. Cardiovascular Disease (CVD) Includes
Management of Hypertension
 Clinical Practice Guidelines Management of Hypertension Definition and classification of blood pressure levels (mmhg) Category Systolic Diastolic Normal
Clinical Practice Guidelines Management of Hypertension Definition and classification of blood pressure levels (mmhg) Category Systolic Diastolic Normal
Starting or Resuming Anticoagulation or Antiplatelet Therapy after ICH: A Neurology Perspective
 Starting or Resuming Anticoagulation or Antiplatelet Therapy after ICH: A Neurology Perspective Cathy Sila MD George M Humphrey II Professor and Vice Chair of Neurology Director, Comprehensive Stroke Center
Starting or Resuming Anticoagulation or Antiplatelet Therapy after ICH: A Neurology Perspective Cathy Sila MD George M Humphrey II Professor and Vice Chair of Neurology Director, Comprehensive Stroke Center
Heart Failure Clinician Guide JANUARY 2018
 Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Heart Failure Clinician Guide JANUARY 2018 Introduction This evidence-based guideline summary is based on the 2018 National Heart Failure Guideline.
Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Heart Failure Clinician Guide JANUARY 2018 Introduction This evidence-based guideline summary is based on the 2018 National Heart Failure Guideline.
MANAGEMENT OF HYPERTENSION IN PREGNANCY, THE ALGORHITHM
 MANAGEMENT OF HYPERTENSION IN PREGNANCY, THE ALGORHITHM Are Particular Anti-hypertensives More Effective or Harmful Than Others in Hypertension in Pregnancy? Existing data is inadequate Methyldopa and
MANAGEMENT OF HYPERTENSION IN PREGNANCY, THE ALGORHITHM Are Particular Anti-hypertensives More Effective or Harmful Than Others in Hypertension in Pregnancy? Existing data is inadequate Methyldopa and
5/2/2016. Outpatient Stroke Management Sheila Smith MD May 5, 2016
 Outpatient Stroke Management Sheila Smith MD May 5, 2016 1 Management of Outpatient Stroke Objectives Review blood pressure management post stroke Review antithrombotic therapy Review statin therapy Discuss
Outpatient Stroke Management Sheila Smith MD May 5, 2016 1 Management of Outpatient Stroke Objectives Review blood pressure management post stroke Review antithrombotic therapy Review statin therapy Discuss
Stroke in Pregnancy. Stroke in Pregnancy 6/23/13
 G5#$#Preven*ng#Maternal#Morbidity#and#Mortality#Via# Expanded#Scope#of#Nursing#Prac*ce#As#First#Responder# in#hypertensive#crisis#of#preeclampsia# The$presenter$reports$no$relevant,$influencing$financial$rela5onships.$
G5#$#Preven*ng#Maternal#Morbidity#and#Mortality#Via# Expanded#Scope#of#Nursing#Prac*ce#As#First#Responder# in#hypertensive#crisis#of#preeclampsia# The$presenter$reports$no$relevant,$influencing$financial$rela5onships.$
Based on 2014 SOGC Guidelines
 Based on 2014 SOGC Guidelines 22nd Edition 2015 1 ICH + gestational hypertension by far the biggest cause of direct maternal deaths New stats coming in 2013 OCR 22nd Edition 2015 2 Diastolic 90 mmhg is
Based on 2014 SOGC Guidelines 22nd Edition 2015 1 ICH + gestational hypertension by far the biggest cause of direct maternal deaths New stats coming in 2013 OCR 22nd Edition 2015 2 Diastolic 90 mmhg is
Management of Hypertension. Ahmed El Hawary MD Suez Canal University
 Management of Hypertension Ahmed El Hawary MD Suez Canal University Minimal vs. Optimal Care Resources more than science affect type of care and level of management. what is possible (minimal care) and
Management of Hypertension Ahmed El Hawary MD Suez Canal University Minimal vs. Optimal Care Resources more than science affect type of care and level of management. what is possible (minimal care) and
Incidental Findings; Management of patients presenting with high BP. Phil Swales
 Incidental Findings; Management of patients presenting with high BP Phil Swales Consultant Physician Acute & General Medicine University Hospitals of Leicester NHS Trust Objectives The approach to an incidental
Incidental Findings; Management of patients presenting with high BP Phil Swales Consultant Physician Acute & General Medicine University Hospitals of Leicester NHS Trust Objectives The approach to an incidental
Recombinant Factor VIIa for Intracerebral Hemorrhage
 Recombinant Factor VIIa for Intracerebral Hemorrhage January 24, 2006 Justin Lee Pharmacy Resident University Health Network Outline 1. Introduction to patient case 2. Overview of intracerebral hemorrhage
Recombinant Factor VIIa for Intracerebral Hemorrhage January 24, 2006 Justin Lee Pharmacy Resident University Health Network Outline 1. Introduction to patient case 2. Overview of intracerebral hemorrhage
Heart Failure Clinician Guide JANUARY 2016
 Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Heart Failure Clinician Guide JANUARY 2016 Introduction This evidence-based guideline summary is based on the 2016 National Heart Failure Guideline.
Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Heart Failure Clinician Guide JANUARY 2016 Introduction This evidence-based guideline summary is based on the 2016 National Heart Failure Guideline.
JNC Evidence-Based Guidelines for the Management of High Blood Pressure in Adults
 JNC 8 2014 Evidence-Based Guidelines for the Management of High Blood Pressure in Adults Table of Contents Why Do We Treat Hypertension? Blood Pressure Treatment Goals Initial Therapy Strength of Recommendation
JNC 8 2014 Evidence-Based Guidelines for the Management of High Blood Pressure in Adults Table of Contents Why Do We Treat Hypertension? Blood Pressure Treatment Goals Initial Therapy Strength of Recommendation
Acute Medical Management. Bogachan Sahin, M.D., Ph.D. Department of Neurology
 Acute Medical Management Bogachan Sahin, M.D., Ph.D. Department of Neurology Outline Head-of-bed position Blood pressure management Antiplatelet therapy Anticoagulation Statin therapy Rehabilitation and
Acute Medical Management Bogachan Sahin, M.D., Ph.D. Department of Neurology Outline Head-of-bed position Blood pressure management Antiplatelet therapy Anticoagulation Statin therapy Rehabilitation and
Antihypertensive drugs: I. Thiazide and other diuretics:
 Clinical assessment of hypertensive patient: You have to take history regarding the presence of other risk factors for CAb like diabetes mellitus, smoking, etc. Take history whether the patient takes medications
Clinical assessment of hypertensive patient: You have to take history regarding the presence of other risk factors for CAb like diabetes mellitus, smoking, etc. Take history whether the patient takes medications
Managing Hypertension in the Perioperative Arena
 Managing Hypertension in the Perioperative Arena Optimizing Perioperative Management Strategies for Hypertension in the Cardiac Surgical Patient Objectives: Treatment of hypertensive emergencies. ALBERT
Managing Hypertension in the Perioperative Arena Optimizing Perioperative Management Strategies for Hypertension in the Cardiac Surgical Patient Objectives: Treatment of hypertensive emergencies. ALBERT
Review of the TICH-2 Trial
 Review of the TICH-2 Trial Mikaela Hofer, PharmD PGY-1 Pharmacy Resident Pharmacy Grand Rounds September 18, 2018 2018 MFMER slide-1 Objectives Review the pharmacologic options to limit hematoma expansion
Review of the TICH-2 Trial Mikaela Hofer, PharmD PGY-1 Pharmacy Resident Pharmacy Grand Rounds September 18, 2018 2018 MFMER slide-1 Objectives Review the pharmacologic options to limit hematoma expansion
New Frontiers in Intracerebral Hemorrhage
 New Frontiers in Intracerebral Hemorrhage Ryan Hakimi, DO, MS Director, Neuro ICU Director, Inpatient Neurology Services Greenville Health System Clinical Associate Professor Department of Medicine (Neurology)
New Frontiers in Intracerebral Hemorrhage Ryan Hakimi, DO, MS Director, Neuro ICU Director, Inpatient Neurology Services Greenville Health System Clinical Associate Professor Department of Medicine (Neurology)
BLOOD PRESSURE MANAGEMENT IN THE ACUTE PHASE
 BLOOD PRESSURE MANAGEMENT IN THE ACUTE PHASE Ελένη Κορομπόκη, MD, PhD, FESO Α Νευρολογική Κλινική, ΕΚΠΑ, Αιγινήτειο Νοσοκομείο Κλινική Ερευνήτρια, Department of Stroke Medicine, Imperial College London,
BLOOD PRESSURE MANAGEMENT IN THE ACUTE PHASE Ελένη Κορομπόκη, MD, PhD, FESO Α Νευρολογική Κλινική, ΕΚΠΑ, Αιγινήτειο Νοσοκομείο Κλινική Ερευνήτρια, Department of Stroke Medicine, Imperial College London,
ALLHAT. Major Outcomes in High Risk Hypertensive Patients Randomized to Angiotensin-Converting Enzyme Inhibitor or Calcium Channel Blocker vs Diuretic
 1 U.S. Department of Health and Human Services National Institutes of Health Major Outcomes in High Risk Hypertensive Patients Randomized to Angiotensin-Converting Enzyme Inhibitor or Calcium Channel Blocker
1 U.S. Department of Health and Human Services National Institutes of Health Major Outcomes in High Risk Hypertensive Patients Randomized to Angiotensin-Converting Enzyme Inhibitor or Calcium Channel Blocker
HEART AND SOUL STUDY OUTCOME EVENT - MORBIDITY REVIEW FORM
 REVIEW DATE REVIEWER'S ID HEART AND SOUL STUDY OUTCOME EVENT - MORBIDITY REVIEW FORM : DISCHARGE DATE: RECORDS FROM: Hospitalization ER Please check all that may apply: Myocardial Infarction Pages 2, 3,
REVIEW DATE REVIEWER'S ID HEART AND SOUL STUDY OUTCOME EVENT - MORBIDITY REVIEW FORM : DISCHARGE DATE: RECORDS FROM: Hospitalization ER Please check all that may apply: Myocardial Infarction Pages 2, 3,
The Failing Heart in Primary Care
 The Failing Heart in Primary Care Hamid Ikram How fares the Heart Failure Epidemic? 4357 patients, 57% women, mean age 74 years HFSA 2010 Practice Guideline (3.1) Heart Failure Prevention A careful and
The Failing Heart in Primary Care Hamid Ikram How fares the Heart Failure Epidemic? 4357 patients, 57% women, mean age 74 years HFSA 2010 Practice Guideline (3.1) Heart Failure Prevention A careful and
OHSU HEALTH CARE SYSTEM PRACTICE GUIDELINES
 OHSU HEALTH CARE SYSTEM NEUROSCIENCES (includes ischemic stroke, TIA, intracerebral hemorrhage and non-subarachnoid hemorrhage) Last Reviewed Date: September 2013 POLICY STATEMENT: OHSU hospitals and clinics
OHSU HEALTH CARE SYSTEM NEUROSCIENCES (includes ischemic stroke, TIA, intracerebral hemorrhage and non-subarachnoid hemorrhage) Last Reviewed Date: September 2013 POLICY STATEMENT: OHSU hospitals and clinics
SBP in range of 120 to 140 :no progression or regression of CAD. Sipahi et al., 2006
 Management of Hypertension in Patients with CAD M. Mohsen Ibrahim, MD Cardiology Department- Cairo University 1. What is the optimal BP in patients with hypertension and CAD? 2. What is the minimum safe
Management of Hypertension in Patients with CAD M. Mohsen Ibrahim, MD Cardiology Department- Cairo University 1. What is the optimal BP in patients with hypertension and CAD? 2. What is the minimum safe
Hypertensive Haemorrhagic Stroke. Dr Philip Lam Thuon Mine
 Hypertensive Haemorrhagic Stroke Dr Philip Lam Thuon Mine Intracerebral Haemorrhage Primary ICH Spontaneous rupture of small vessels damaged by HBP Basal ganglia, thalamus, pons and cerebellum Amyloid
Hypertensive Haemorrhagic Stroke Dr Philip Lam Thuon Mine Intracerebral Haemorrhage Primary ICH Spontaneous rupture of small vessels damaged by HBP Basal ganglia, thalamus, pons and cerebellum Amyloid
o Unenhanced Head CT
 Drip & Ship Protocol Acute Stroke Ready Hospital (ASRH) Duluth Area Primary Stroke Center (St. Luke s & St. Mary s Essentia) PATIENT LABEL Patient displays strokelike symptoms EMS/ED CSS > 0 Glucose >
Drip & Ship Protocol Acute Stroke Ready Hospital (ASRH) Duluth Area Primary Stroke Center (St. Luke s & St. Mary s Essentia) PATIENT LABEL Patient displays strokelike symptoms EMS/ED CSS > 0 Glucose >
Managing HTN in the Elderly: How Low to Go
 Managing HTN in the Elderly: How Low to Go Laxmi S. Mehta, MD, FACC The Ohio State University Medical Center Assistant Professor of Clinical Internal Medicine Clinical Director of the Women s Cardiovascular
Managing HTN in the Elderly: How Low to Go Laxmi S. Mehta, MD, FACC The Ohio State University Medical Center Assistant Professor of Clinical Internal Medicine Clinical Director of the Women s Cardiovascular
From PARADIGM-HF to Clinical Practice. Waleed AlHabeeb, MD, MHA Associate Professor of Medicine President of the Saudi Heart Failure Group
 From PARADIGM-HF to Clinical Practice Waleed AlHabeeb, MD, MHA Associate Professor of Medicine President of the Saudi Heart Failure Group PARADIGM-HF: Inclusion Criteria Chronic HF NYHA FC II IV with LVEF
From PARADIGM-HF to Clinical Practice Waleed AlHabeeb, MD, MHA Associate Professor of Medicine President of the Saudi Heart Failure Group PARADIGM-HF: Inclusion Criteria Chronic HF NYHA FC II IV with LVEF
Thrombolysis for acute ischaemic stroke Rapid Assessment Protocol NORTHERN IRELAND Regional Protocol (Version 002 July 08)
") Thrombolysis for acute ischaemic stroke Rapid Assessment Protocol NORTHERN IRELAND Regional Protocol (Version 002 July 08) Patient Details Time of onset? Capillary Blood glucose 2.8-22.2 mmol/l? Blood
Thrombolysis for acute ischaemic stroke Rapid Assessment Protocol NORTHERN IRELAND Regional Protocol (Version 002 July 08) Patient Details Time of onset? Capillary Blood glucose 2.8-22.2 mmol/l? Blood
Hypertension Update. Sarah J. Payne, MS, PharmD, BCPS Assistant Professor, Department of Pharmacotherapy UNT System College of Pharmacy
 Hypertension Update Sarah J. Payne, MS, PharmD, BCPS Assistant Professor, Department of Pharmacotherapy UNT System College of Pharmacy Introduction 1/3 of US adults have HTN More prevalent in non-hispanic
Hypertension Update Sarah J. Payne, MS, PharmD, BCPS Assistant Professor, Department of Pharmacotherapy UNT System College of Pharmacy Introduction 1/3 of US adults have HTN More prevalent in non-hispanic
HYPERTENSION. Background for understanding the Hypertension literature. Case presentation. Approach to Treatment. Jeffrey J. Kaufhold, MD Nephrology
 HYPERTENSION Background for understanding the Hypertension literature. Case presentation Approach to Treatment Jeffrey J. Kaufhold, MD Nephrology 2009 HYPERTENSION SUMMARY Background for understanding
HYPERTENSION Background for understanding the Hypertension literature. Case presentation Approach to Treatment Jeffrey J. Kaufhold, MD Nephrology 2009 HYPERTENSION SUMMARY Background for understanding
Hypertension Update 2009
 Hypertension Update 2009 New Drugs, New Goals, New Approaches, New Lessons from Clinical Trials Timothy C Fagan, MD, FACP Professor Emeritus University of Arizona New Drugs Direct Renin Inhibitors Endothelin
Hypertension Update 2009 New Drugs, New Goals, New Approaches, New Lessons from Clinical Trials Timothy C Fagan, MD, FACP Professor Emeritus University of Arizona New Drugs Direct Renin Inhibitors Endothelin
BY: Ramon Medina EMT-LP/RN
 BY: Ramon Medina EMT-LP/RN Discuss types of strokes Discuss the physical and neurological assessment of stroke patients Discuss pertinent historical findings Discuss pre-hospital and emergency management
BY: Ramon Medina EMT-LP/RN Discuss types of strokes Discuss the physical and neurological assessment of stroke patients Discuss pertinent historical findings Discuss pre-hospital and emergency management
Critical Care Management of Acute Ischemic Stroke
 Critical Care Management of Acute Ischemic Stroke Gene Sung, M.D., M.P.H. Past-President, Neurocritical Care Society Neurocritical Care and Stroke Division University of Southern California USC Stroke
Critical Care Management of Acute Ischemic Stroke Gene Sung, M.D., M.P.H. Past-President, Neurocritical Care Society Neurocritical Care and Stroke Division University of Southern California USC Stroke
OHSU Health Care System
 Acute Stroke Practice Standard for the Emergency Department (includes ischemic stroke, TIAs, intracerebral hemorrhage, and non-subarachnoid hemorrhage), PS 01.11 Last Reviewed Date: 2/2/10 STATEMENT OF
Acute Stroke Practice Standard for the Emergency Department (includes ischemic stroke, TIAs, intracerebral hemorrhage, and non-subarachnoid hemorrhage), PS 01.11 Last Reviewed Date: 2/2/10 STATEMENT OF
DRUG GUIDELINE. HYDRALAZINE (Intravenous severe hypertension in pregnancy)
") DRUG GUIDELINE HYDRALAZINE (Intravenous severe hypertension SCOPE (Area): FOR USE IN: Labour Ward, HDU, Theatre and ED EXCLUSIONS: Paediatrics (seek Paediatrician advice) and other general wards. SCOPE
DRUG GUIDELINE HYDRALAZINE (Intravenous severe hypertension SCOPE (Area): FOR USE IN: Labour Ward, HDU, Theatre and ED EXCLUSIONS: Paediatrics (seek Paediatrician advice) and other general wards. SCOPE
Thrombolysis administration
 Thrombolysis administration Liz Mackey Stroke Nurse Practitioner Western Health Sunshine & Footscray Hospital, Melbourne Thanks ASNEN committee members Skye Coote, Acute Stroke Nurse, Eastern Health (slide
Thrombolysis administration Liz Mackey Stroke Nurse Practitioner Western Health Sunshine & Footscray Hospital, Melbourne Thanks ASNEN committee members Skye Coote, Acute Stroke Nurse, Eastern Health (slide
Emergency Room Procedure The first few hours in hospital...
 Emergency Room Procedure The first few hours in hospital... ER 5 level Emergency Severity Index SOP s for Stroke Stroke = Level 2 Target Time = 1 Hour 10 min from door 2 Doctor 25 min from door 2 CT 60
Emergency Room Procedure The first few hours in hospital... ER 5 level Emergency Severity Index SOP s for Stroke Stroke = Level 2 Target Time = 1 Hour 10 min from door 2 Doctor 25 min from door 2 CT 60
ENCHANTED Era: Is it time to rethink treatment of acute ischemic stroke? Kristin J. Scherber, PharmD, BCPS Emergency Medicine Clinical Pharmacist
 ENCHANTED Era: Is it time to rethink treatment of acute ischemic stroke? Kristin J. Scherber, PharmD, BCPS Emergency Medicine Clinical Pharmacist Pharmacy Grand Rounds 26 July 2016 2015 MFMER slide-1 Learning
ENCHANTED Era: Is it time to rethink treatment of acute ischemic stroke? Kristin J. Scherber, PharmD, BCPS Emergency Medicine Clinical Pharmacist Pharmacy Grand Rounds 26 July 2016 2015 MFMER slide-1 Learning
Section 3, Lecture 2
 59-291 Section 3, Lecture 2 Diuretics: -increase in Na + excretion (naturesis) Thiazide and Related diuretics -decreased PVR due to decreases muscle contraction -an economical and effective treatment -protect
59-291 Section 3, Lecture 2 Diuretics: -increase in Na + excretion (naturesis) Thiazide and Related diuretics -decreased PVR due to decreases muscle contraction -an economical and effective treatment -protect
Emergency Treatment of Ischemic Stroke
 Emergency Treatment of Ischemic Stroke JEFFREY BOYLE, M.D., PHD CLINICAL DIRECTOR OF STROKE AT AVERA MCKENNAN AVERA MEDICAL GROUP NEUROLOGY SIOUX FALLS, SD Conflicts of Interest None I will discuss therapies
Emergency Treatment of Ischemic Stroke JEFFREY BOYLE, M.D., PHD CLINICAL DIRECTOR OF STROKE AT AVERA MCKENNAN AVERA MEDICAL GROUP NEUROLOGY SIOUX FALLS, SD Conflicts of Interest None I will discuss therapies
Stroke Transfer Checklist
 Stroke Transfer Checklist When preparing to transfer an acute stroke patient to the UF Health Shands Comprehensive Stroke Center, please make every attempt to include the following information: Results
Stroke Transfer Checklist When preparing to transfer an acute stroke patient to the UF Health Shands Comprehensive Stroke Center, please make every attempt to include the following information: Results
Stroke Update. Lacunar 19% Thromboembolic 6% SAH 13% ICH 13% Unknown 32% Hemorrhagic 26% Ischemic 71% Other 3% Cardioembolic 14%
 Stroke Update Michel Torbey, MD, MPH, FAHA, FNCS Medical Director, Neurovascular Stroke Center Professor Department of Neurology and Neurosurgery The Ohio State University Wexner Medical Center Objectives
Stroke Update Michel Torbey, MD, MPH, FAHA, FNCS Medical Director, Neurovascular Stroke Center Professor Department of Neurology and Neurosurgery The Ohio State University Wexner Medical Center Objectives
Antihypertensive drugs SUMMARY Made by: Lama Shatat
 Antihypertensive drugs SUMMARY Made by: Lama Shatat Diuretic Thiazide diuretics The loop diuretics Potassium-sparing Diuretics *Hydrochlorothiazide *Chlorthalidone *Furosemide *Torsemide *Bumetanide Aldosterone
Antihypertensive drugs SUMMARY Made by: Lama Shatat Diuretic Thiazide diuretics The loop diuretics Potassium-sparing Diuretics *Hydrochlorothiazide *Chlorthalidone *Furosemide *Torsemide *Bumetanide Aldosterone
Difficult to Treat Hypertension
 Difficult to Treat Hypertension According to Goldilocks JNC 8 Blood Pressure Goals (2014) BP Goal 60 years old and greater*- systolic < 150 and diastolic < 90. (Grade A)** BP Goal 18-59 years old* diastolic
Difficult to Treat Hypertension According to Goldilocks JNC 8 Blood Pressure Goals (2014) BP Goal 60 years old and greater*- systolic < 150 and diastolic < 90. (Grade A)** BP Goal 18-59 years old* diastolic
Hypertension CHAPTER-I CARDIOVASCULAR SYSTEM. Dr. K T NAIK Pharm.D Associate Professor Department of Pharm.D Krishna Teja Pharmacy College, Tirupati
 CHAPTER-I CARDIOVASCULAR SYSTEM Hypertension SUB: PHARMACOTHERAPEUTICS-I CODE:T0820006 Dr. K T NAIK Pharm.D Associate Professor Department of Pharm.D Krishna Teja Pharmacy College, Tirupati Hypertension
CHAPTER-I CARDIOVASCULAR SYSTEM Hypertension SUB: PHARMACOTHERAPEUTICS-I CODE:T0820006 Dr. K T NAIK Pharm.D Associate Professor Department of Pharm.D Krishna Teja Pharmacy College, Tirupati Hypertension
7/7/ CHD/MI LVH and LV dysfunction Dysrrhythmias Stroke PVD Renal insufficiency and failure Retinopathy. Normal <120 Prehypertension
 Prevalence of Hypertension Hypertension: Diagnosis and Management T. Villela, M.D. Program Director University of California, San Francisco-San Francisco General Hospital Family and Community Medicine
Prevalence of Hypertension Hypertension: Diagnosis and Management T. Villela, M.D. Program Director University of California, San Francisco-San Francisco General Hospital Family and Community Medicine
Children with Hypertension in ED
 Children with Hypertension in ED By Prof. Sanaa AK Helmy Professor of Anesthesia, Intensive Care and Pain Management, Faculty of Medicine, Cairo University Vice-chairman of the Egyptian Society of Emergency
Children with Hypertension in ED By Prof. Sanaa AK Helmy Professor of Anesthesia, Intensive Care and Pain Management, Faculty of Medicine, Cairo University Vice-chairman of the Egyptian Society of Emergency
TREATMENT OF HYPERTENSION
 TREATMENT OF HYPERTENSION Aim of treatment BP Goals Main items of treatment Lifestyle modification When to start drug Rx Pharmacological therapy 1. Relief of symptoms 2. Prevention of complications and
TREATMENT OF HYPERTENSION Aim of treatment BP Goals Main items of treatment Lifestyle modification When to start drug Rx Pharmacological therapy 1. Relief of symptoms 2. Prevention of complications and
Towards a Greater Understanding of Cardiac Medications Foundational Cardiac Concepts That Must Be Understood:
 Towards a Greater Understanding of Cardiac Medications Foundational Cardiac Concepts That Must Be Understood: Cardiac Output (CO) CO=SVxHR (stroke volume x heart rate) Cardiac output: The amount of blood
Towards a Greater Understanding of Cardiac Medications Foundational Cardiac Concepts That Must Be Understood: Cardiac Output (CO) CO=SVxHR (stroke volume x heart rate) Cardiac output: The amount of blood
CMQCC Preeclampsia Tool Kit: Hypertensive Disorders Across the Lifespan
 CMQCC Preeclampsia Tool Kit: Hypertensive Disorders Across the Lifespan Carol J Harvey, MS, BSN, RNC-OB, C-EFM, CS Northside Hospital Atlanta Cherokee - Forsyth New! Improving Health Care Response to Preeclampsia:
CMQCC Preeclampsia Tool Kit: Hypertensive Disorders Across the Lifespan Carol J Harvey, MS, BSN, RNC-OB, C-EFM, CS Northside Hospital Atlanta Cherokee - Forsyth New! Improving Health Care Response to Preeclampsia:
Managing Hypertension in Diabetes Sean Stewart, PharmD, BCPS, BCACP, CLS Internal Medicine Park Nicollet Clinic St Louis Park.
 Managing Hypertension in Diabetes 2015 Sean Stewart, PharmD, BCPS, BCACP, CLS Internal Medicine Park Nicollet Clinic St Louis Park Case Scenario Mike M is a 59 year old man with type 2 diabetes managed
Managing Hypertension in Diabetes 2015 Sean Stewart, PharmD, BCPS, BCACP, CLS Internal Medicine Park Nicollet Clinic St Louis Park Case Scenario Mike M is a 59 year old man with type 2 diabetes managed
MODERN MANAGEMENT OF HYPERTENSION Where Do We Draw the Line? Disclosure. No relevant financial relationships. Blood Pressure and Risk
 MODERN MANAGEMENT OF HYPERTENSION Where Do We Draw the Line? Disclosure No relevant financial relationships Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine baron@medicine.ucsf.edu
MODERN MANAGEMENT OF HYPERTENSION Where Do We Draw the Line? Disclosure No relevant financial relationships Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine baron@medicine.ucsf.edu
Antihypertensive Agents
 Antihypertensive Agents Southern California University of Health Sciences Physician Assistant Program Management and Treatment of Hypertension April 7, 08, presented by Ezra Levy, Pharm.D! Usual Dose,
Antihypertensive Agents Southern California University of Health Sciences Physician Assistant Program Management and Treatment of Hypertension April 7, 08, presented by Ezra Levy, Pharm.D! Usual Dose,
VA/DoD Clinical Practice Guideline for the Diagnosis and Management of Hypertension - Pocket Guide Update 2004 Revision July 2005
 VA/DoD Clinical Practice Guideline for the Diagnosis and Management of Hypertension - Pocket Guide Update 2004 Revision July 2005 1 Any adult in the health care system 2 Obtain blood pressure (BP) (Reliable,
VA/DoD Clinical Practice Guideline for the Diagnosis and Management of Hypertension - Pocket Guide Update 2004 Revision July 2005 1 Any adult in the health care system 2 Obtain blood pressure (BP) (Reliable,
A very short lecture.
 Medical Treatment of Type A Aortic Dissection: Tales of Turkeys, Tygon Tubing, and Evolving Paradigms The Houston Aortic Symposium April 4-6, 2008 John A. Elefteriades, MD William W.L. Glenn Professor
Medical Treatment of Type A Aortic Dissection: Tales of Turkeys, Tygon Tubing, and Evolving Paradigms The Houston Aortic Symposium April 4-6, 2008 John A. Elefteriades, MD William W.L. Glenn Professor
NIHSS. Category Scale Definition Date/Time Date/Time Date/Time. Score Initial. Drip & Ship Protocol. Initials: Signature: Initials: Signature:
 NIHSS 1a. Level of Consciousness (Alert, drowsy, etc.) Category Scale Definition Date/Time Date/Time Date/Time 1b. LOC Question (Month, age) 1c. LOC Commands (Open, close eyes, make fist, let go) 2. Best
NIHSS 1a. Level of Consciousness (Alert, drowsy, etc.) Category Scale Definition Date/Time Date/Time Date/Time 1b. LOC Question (Month, age) 1c. LOC Commands (Open, close eyes, make fist, let go) 2. Best
Heart Failure (HF) Treatment
 Treatment") Heart Failure (HF) Treatment Heart Failure (HF) Complex, progressive disorder. The heart is unable to pump sufficient blood to meet the needs of the body. Its cardinal symptoms are dyspnea, fatigue, and
Heart Failure (HF) Treatment Heart Failure (HF) Complex, progressive disorder. The heart is unable to pump sufficient blood to meet the needs of the body. Its cardinal symptoms are dyspnea, fatigue, and
Antihypertensive Trial Design ALLHAT
 1 U.S. Department of Health and Human Services Major Outcomes in High Risk Hypertensive Patients Randomized to Angiotensin-Converting Enzyme Inhibitor or Calcium Channel Blocker vs Diuretic National Institutes
1 U.S. Department of Health and Human Services Major Outcomes in High Risk Hypertensive Patients Randomized to Angiotensin-Converting Enzyme Inhibitor or Calcium Channel Blocker vs Diuretic National Institutes
Agenda. Management of Accelerated Hypertension (Updated in 2017) Salwa Roshdy Prof. of Cardiology Assiut University CardioEgypt 23/2/2017 2/27/2017
 Salwa Roshdy Prof. of Cardiology Assiut University CardioEgypt 23/2/2017 2/27/2017") Management of Accelerated Hypertension (Updated in 2017) By Salwa Roshdy Prof. of Cardiology Assiut University CardioEgypt 23/2/2017 Agenda Definition of Accelerated HTN Pathophysiology & Etiology Prognosis
Management of Accelerated Hypertension (Updated in 2017) By Salwa Roshdy Prof. of Cardiology Assiut University CardioEgypt 23/2/2017 Agenda Definition of Accelerated HTN Pathophysiology & Etiology Prognosis
Blood Pressure Targets: Where are We Now?
 Blood Pressure Targets: Where are We Now? Diana Cao, PharmD, BCPS-AQ Cardiology Assistant Professor Department of Clinical & Administrative Sciences California Northstate University College of Pharmacy
Blood Pressure Targets: Where are We Now? Diana Cao, PharmD, BCPS-AQ Cardiology Assistant Professor Department of Clinical & Administrative Sciences California Northstate University College of Pharmacy
Stroke Guidelines. November 19, 2011
 Stroke Guidelines November 19, 2011 Clinical Practice Guidelines American Stroke Association Guidelines are comprehensive statements that provide the highest level of scientific evidence for clinical practice.
Stroke Guidelines November 19, 2011 Clinical Practice Guidelines American Stroke Association Guidelines are comprehensive statements that provide the highest level of scientific evidence for clinical practice.
Hypertension diagnosis (see detail document) Diabetic. Target less than 130/80mmHg
 Diabetic. Target less than 130/80mmHg") Hypertension diagnosis (see detail document) Non-diabetic Diabetic Very elderly (older than 80 years) Target less than 140/90mmHg Target less than 130/80mmHg Consider SBP target less than 150mmHg Non-diabetic
Hypertension diagnosis (see detail document) Non-diabetic Diabetic Very elderly (older than 80 years) Target less than 140/90mmHg Target less than 130/80mmHg Consider SBP target less than 150mmHg Non-diabetic
Controversies in Hemorrhagic Stroke Management. Sarah L. Livesay, DNP, RN, ACNP-BC, ACNS-BC Associate Professor Rush University
 Controversies in Hemorrhagic Stroke Management Sarah L. Livesay, DNP, RN, ACNP-BC, ACNS-BC Associate Professor Rush University Disclosures AHA/ASA Outline Blood pressure VTE Coagulopathy Early mobilization
Controversies in Hemorrhagic Stroke Management Sarah L. Livesay, DNP, RN, ACNP-BC, ACNS-BC Associate Professor Rush University Disclosures AHA/ASA Outline Blood pressure VTE Coagulopathy Early mobilization
11/27/2017. Stroke Management in the Neurocritical Care Unit. Conflict of interest. Karel Fuentes MD Medical Director of Neurocritical Care
 Stroke Management in the Neurocritical Care Unit Karel Fuentes MD Medical Director of Neurocritical Care Conflict of interest None Introduction Reperfusion therapy remains the mainstay in the treatment
Stroke Management in the Neurocritical Care Unit Karel Fuentes MD Medical Director of Neurocritical Care Conflict of interest None Introduction Reperfusion therapy remains the mainstay in the treatment
Primary Stroke Center Acute Stroke Transfer Guidelines When to Consider a Transfer:
 When to Consider a Transfer: Hemorrhagic Stroke Large volume intracerebral hematoma greater than 5cm on CT Concern for expanding hematoma Rapidly declining mental status, especially requiring intubation
When to Consider a Transfer: Hemorrhagic Stroke Large volume intracerebral hematoma greater than 5cm on CT Concern for expanding hematoma Rapidly declining mental status, especially requiring intubation
Supplementary Online Content
 Supplementary Online Content Inohara T, Xian Y, Liang L, et al. Association of intracerebral hemorrhage among patients taking non vitamin K antagonist vs vitamin K antagonist oral anticoagulants with in-hospital
Supplementary Online Content Inohara T, Xian Y, Liang L, et al. Association of intracerebral hemorrhage among patients taking non vitamin K antagonist vs vitamin K antagonist oral anticoagulants with in-hospital
Evaluation and Management of Acute Decompensated Heart Failure (HF) with Reduced Ejection Fraction Systolic Heart Failure (HFrEF)(EF<40%
 with Reduced Ejection Fraction Systolic Heart Failure (HFrEF)(EF<40%") Evaluation and Management of Acute Decompensated Heart Failure (HF) with Reduced Ejection Fraction Systolic Heart Failure (HFrEF)(EF
Evaluation and Management of Acute Decompensated Heart Failure (HF) with Reduced Ejection Fraction Systolic Heart Failure (HFrEF)(EF
Get Healthy Stay Healthy
 Hypertension Management WHAT IS HYPERTENSION (HIGH BLOOD PRESSURE)? Blood pressure is a measure of how hard the blood pushes against the walls of your arteries as it moves through your body. It is normal
Hypertension Management WHAT IS HYPERTENSION (HIGH BLOOD PRESSURE)? Blood pressure is a measure of how hard the blood pushes against the walls of your arteries as it moves through your body. It is normal
Mortality as an Efficacy or Safety Endpoint : Lessons Learned from the Heart Failure Trials
 Mortality as an Efficacy or Safety Endpoint : Lessons Learned from the Heart Failure Trials Christopher M. O Connor, MD Professor of Medicine Director, Duke Heart Center Acting Chief, Division of Cardiology
Mortality as an Efficacy or Safety Endpoint : Lessons Learned from the Heart Failure Trials Christopher M. O Connor, MD Professor of Medicine Director, Duke Heart Center Acting Chief, Division of Cardiology
GUIDELINES FOR THE EARLY MANAGEMENT OF PATIENTS WITH ACUTE ISCHEMIC STROKE
 2018 UPDATE QUICK SHEET 2018 American Heart Association GUIDELINES FOR THE EARLY MANAGEMENT OF PATIENTS WITH ACUTE ISCHEMIC STROKE A Summary for Healthcare Professionals from the American Heart Association/American
2018 UPDATE QUICK SHEET 2018 American Heart Association GUIDELINES FOR THE EARLY MANAGEMENT OF PATIENTS WITH ACUTE ISCHEMIC STROKE A Summary for Healthcare Professionals from the American Heart Association/American
Antihypertensives. Antihypertensive Classes. RAAS Inhibitors. Renin-Angiotensin Cascade. Angiotensin Receptors. Approaches to Hypertension Treatment
 Approaches to Hypertension Treatment Antihypertensives Inhibit Sympathetic impulses Inhibit contractility Inhibit heart rate Inhibit vasoconstriction Inhibit smooth muscle function Inhibit RAAS Inhibit
Approaches to Hypertension Treatment Antihypertensives Inhibit Sympathetic impulses Inhibit contractility Inhibit heart rate Inhibit vasoconstriction Inhibit smooth muscle function Inhibit RAAS Inhibit
HYPERTENSION GUIDELINES WHERE ARE WE IN 2014
 HYPERTENSION GUIDELINES WHERE ARE WE IN 2014 Donald J. DiPette MD FACP Special Assistant to the Provost for Health Affairs Distinguished Health Sciences Professor University of South Carolina University
HYPERTENSION GUIDELINES WHERE ARE WE IN 2014 Donald J. DiPette MD FACP Special Assistant to the Provost for Health Affairs Distinguished Health Sciences Professor University of South Carolina University
What in the World is Functional Medicine?
 What in the World is Functional Medicine? An Introduction to a Systems Based Approach of Chronic Disease Meneah R Haworth, FNP-C Disclosure v I am a student of the Institute for Functional Medicine. They
What in the World is Functional Medicine? An Introduction to a Systems Based Approach of Chronic Disease Meneah R Haworth, FNP-C Disclosure v I am a student of the Institute for Functional Medicine. They
The Effect of Statin Therapy on Risk of Intracranial Hemorrhage
 The Effect of Statin Therapy on Risk of Intracranial Hemorrhage JENNIFER HANIFY, PHARM.D. PGY2 CRITICAL CARE RESIDENT UF HEALTH JACKSONVILLE JANUARY 23 RD 2016 Objectives Review benefits of statin therapy
The Effect of Statin Therapy on Risk of Intracranial Hemorrhage JENNIFER HANIFY, PHARM.D. PGY2 CRITICAL CARE RESIDENT UF HEALTH JACKSONVILLE JANUARY 23 RD 2016 Objectives Review benefits of statin therapy
Byvalson. (nebivolol, valsartan) New Product Slideshow
 New Product Slideshow") Byvalson (nebivolol, valsartan) New Product Slideshow Introduction Brand name: Byvalson Generic name: Nebivolol, valsartan Pharmacological class: Beta-blocker + angiotensin II receptor blocker (ARB) Strength
Byvalson (nebivolol, valsartan) New Product Slideshow Introduction Brand name: Byvalson Generic name: Nebivolol, valsartan Pharmacological class: Beta-blocker + angiotensin II receptor blocker (ARB) Strength
First line treatment of primary hypertension
 First line treatment of primary hypertension Dr. Vijaya Musini Assistant Professor, Dept. Anesthesiology, Pharmacology and Therapeutics Manager, Drug Assessment Working Group Therapeutics Initiative Editor,
First line treatment of primary hypertension Dr. Vijaya Musini Assistant Professor, Dept. Anesthesiology, Pharmacology and Therapeutics Manager, Drug Assessment Working Group Therapeutics Initiative Editor,
PUBLIC SUMMARY OF RISK MANAGEMENT PLAN (RMP) CANDESARTAN/HYDROCHLOROTHIAZIDE ORION 8 MG/12.5 MG, 16 MG/12.5 MG, 32 MG/12.5 MG, 32 MG/25 MG ORION
 CANDESARTAN/HYDROCHLOROTHIAZIDE ORION 8 MG/12.5 MG, 16 MG/12.5 MG, 32 MG/12.5 MG, 32 MG/25 MG ORION") PUBLIC SUMMARY OF RISK MANAGEMENT PLAN (RMP) CANDESARTAN/HYDROCHLOROTHIAZIDE ORION 8 MG/12.5 MG, 16 MG/12.5 MG, 32 MG/12.5 MG, 32 MG/25 MG ORION CORPORATION DATE: 17-04-2015, VERSION 2 VI.2 Elements for
PUBLIC SUMMARY OF RISK MANAGEMENT PLAN (RMP) CANDESARTAN/HYDROCHLOROTHIAZIDE ORION 8 MG/12.5 MG, 16 MG/12.5 MG, 32 MG/12.5 MG, 32 MG/25 MG ORION CORPORATION DATE: 17-04-2015, VERSION 2 VI.2 Elements for
Hypertension Guidelines: Are We Pressured to Change? Oregon Cardiovascular Symposium Portland, Oregon June 6, Financial Disclosures
 Hypertension Guidelines: Are We Pressured to Change? Oregon Cardiovascular Symposium Portland, Oregon June 6, 2015 William C. Cushman, MD Professor, Preventive Medicine, Medicine, and Physiology University
Hypertension Guidelines: Are We Pressured to Change? Oregon Cardiovascular Symposium Portland, Oregon June 6, 2015 William C. Cushman, MD Professor, Preventive Medicine, Medicine, and Physiology University
HYPERTENSION: Sustained elevation of arterial blood pressure above normal o Systolic 140 mm Hg and/or o Diastolic 90 mm Hg
 Lecture 39 Anti-Hypertensives B-Rod BLOOD PRESSURE: Systolic / Diastolic NORMAL: 120/80 Systolic = measure of pressure as heart is beating Diastolic = measure of pressure while heart is at rest between
Lecture 39 Anti-Hypertensives B-Rod BLOOD PRESSURE: Systolic / Diastolic NORMAL: 120/80 Systolic = measure of pressure as heart is beating Diastolic = measure of pressure while heart is at rest between
The P&T Committee Lisinopril (Qbrelis )
") Situation Background Assessment The P&T Committee Lisinopril (Qbrelis ) Qbrelis, 1 mg/ml lisinopril oral solution, has recently become an FDA- approved formulation. Current practice at UK Chandler Medical
Situation Background Assessment The P&T Committee Lisinopril (Qbrelis ) Qbrelis, 1 mg/ml lisinopril oral solution, has recently become an FDA- approved formulation. Current practice at UK Chandler Medical