POLYPHARMACY AND POLYPRAGMASY IN CARDIOVASCULAR ELDERLY PATIENTS
|
|
|
- Doreen Stanley
- 6 years ago
- Views:
Transcription



1 POLYPHARMACY AND POLYPRAGMASY IN CARDIOVASCULAR ELDERLY PATIENTS Prof. Daniel Pella, MD, PhD. 1st Dept. of Medicine P. J. Safarik University and L. Pasteur University Hospital Košice Slovakia 2nd CPPEI, Vienna, July 07-09, 2017
2 POLYPHARMACY Concomitant use of at least two drugs (in some definitions at least 4-5 drugs) Evidence based polypharmacy very common in treatment of many CV diseases Trend towards use of FDC (fixed drug combinations) Concept of polypill
3 POLYPRAGMASY Too many drugs administered to the patient at the same time concurrent (or more) therapeutic approaches at the same time Prolonged use of drugs or in uncorrect dosages (usually higher) Both terms polypharmacy and polypragmasy are quite commonly wrongly interpreted by physicians In majority of cases polypragmasy represent not recommended and not-effective therapy
4 CLASSES OF RECOMMENDATION Class I Class II a Class II b Class III Evidences and common agreement about benefits and efficacy Not clear evidence, different opinions (benefits vs. efficacy), but in general positive opinion prevails Benefit and efficacy less confirmed by evidences or opinions Evidence or consensus treatment is not beneficial, not effective, or may be even harmful
5 LEVELS OF EVIDENCE Level of evidence A Level of evidence B Level of evidence C More randomized clinical trials or meta-analyses One randomized clinical trial or large non-randomized trials Experts opinions consensus or small trials, retrospective studies, registries
6 WHY IS POLYPHARMACY SO PREVALENT? Once drug is indicated and not prescribed who will protect doctor? (Medical chambers? Professional organizations? Lawyers? Patients? Media?) guidelines - clearly written, but... (use of personalized medicine is possibly better like EBM results from clinical studies where pts. are selected by inclusion and exclusion criteria real life patient is usually different comorbidities, other treatment, etc.)
7 WHY IS POLYPHARMACY SO PREVALENT? E-Health not yet available in all countries doctors are not properly informed about each other prescriptions (double prescriptions from the same class of drugs, physicians are not aware about possible interactions) Patient requests some drug I am aware I need this one (no prescription after examination of patient bad doctor - did not find something wrong, would like to save money for insurance company, etc.)
8 THE MOST COMMON CV DISEASE IN ELDERLY PATIENTS Arterial hypertension Atherosclerosis and its equivalents (all forms and locations, mainly coronary and cerebral circulation) Heart failure (both acute and chronic most frequent acute worsening of chronic heart failure) Dyslipidemia
9 ARTERIAL HYPERTENSION Prevalence is increasing with age, in elderly population more than 50 % Diastolic hypertension typical for younger individuals (or systolic-diastolic one), in the elderly mostly prevalent is isolated systolic hypertension Majority of HT subjects require for HT control at least two antihypertensives (in elderly preferred low doses more active substances fixed dose combinations, single pill)

10 Aged under 55 years A Aged over 55 years or black person of African or Caribbean family origin of any age C 2 Step 1 Summary of antihypertensive drug treatment A + C 2 A + C + D Resistant hypertension A + C + D + consider further diuretic 3, 4 or alpha- or beta-blocker 5 Consider seeking expert advice Step 2 Step 3 Step 4 Key A ACE inhibitor or low-cost angiotensin II receptor blocker (ARB) 1 C Calcium-channel blocker (CCB) D Thiazide-like diuretic NICE Guidelines Hypertension, 2011

11 OPTIMIZING THERAPY OF HYPERTENSIVE PATIENTS WITH HYPERTENSION AND/OR CAD USING FIXED COMBINATION OF PERINDOPRIL ARGININE/AMLODIPINE Hatala R, Pella D, Hatalová K, et al. Clin Drug Investig 2012
12 Demography BASELINE CHARACTERISTICS 9658 pts. Women (48%) Men (52%) Age 60,7 years 63,3 years 58,4 years Height 170,4 cm 164,1 cm 176,2 cm Weight 85,0 kg 79,1 kg 90,4 kg waist 97,3 cm 93,8 cm 100,5 cm BMI* 29,3 29,4 29,2 Arterial hypertension SBP (mmhg) DBP (mmhg) HR (rate/min) 158,0 158,6 157,4 94,6 94,1 95,0 74,8 75,1 74,6 *Overweight (BMI >25 kg /m 2 ) Hatala R, Pella D, Hatalová K, et al. Clin Drug Investig 2012
13 HYPERTENSION AND CAD THERAPY - BASELINE (25% PATIENTS WITH CAD) 9658 patients % ACE inhibítors 63 Calcium channel blockers 52 Betablockers 35 Diuretics 21 AT1 receptor blockers (sartans) 6 Central acting antihypertensives 15 Antithrombotic treatment 30 Lipid lowering drugs 34 Other coronary therapy* 11 Nitrates 7 Data on file * trimetazidine, ivabradine, molsidomíne Hatala R, Pella D, Hatalová K, et al. Clin Drug Investig 2012
14 COMBINED ANTIHYPERTENSIVE TREATMENT THE ONLY WAY HOW TO ACHIEVE TARGET BP LEVELS Study (final SBP) ASCOT-BPLA (136,9 mmhg) ALLHAT (138 mmhg) IDNT (138 mmhg) RENAAL (141 mmhg) UKPDS (144 mmhg) ABCD (132 mmhg) MDRD (132 mmhg) HOT (138 mmhg) AASK (128 mmhg) Bakris et al. Am J Med 2004;116(5A):30S 8 Dahlöf et al. Lancet 2005;366: The average number of antihypertensive agents needed
15 WHAT WE HAVE SHOWN IN SYMBIO TRIAL? - Hypertensive patients are usually treated according guidelines, majority of them with ACE-inhibitors and CCB, or even more antihypertensives were used - Despite this fact not achieving treatment goals (BP below 140/90 mm Hg) Hatala R, Pella D, Hatalová K, et al. Clin Drug Investig 2012

16 DECREASE OF BLOOD PRESSURE CHANGE FROM USUAL CARE TO PERINDOPRIL ARGININE + AMLODIPINE Hatala R, Pella D, Hatalova K, et al. Clin Drug Investig 2012; 32 (9):
17 SYMBIO TRIAL CONCLUSIONS I. - All previously prescribed ACE-inhibitors and CCB were changed to perindopril arginine and amlodipine administered in combination (not FDC) - This change led to additional significant decrease of BP Hatala R, Pella D, Hatalová K, et al. Clin Drug Investig 2012
18 SYMBIO TRIAL CONCLUSIONS II. - In the subsequent study we just changed free combination of perindopril arginine and amlodipine to fixed dose combination (FDC) - Surprisingly (? or not...) this change led to next additional significant decrease of BP Hatala R, Pella D, Hatalová K, et al. Clin Drug Investig 2012
19 THE SAME DOSAGE COHORT OF PTS. CHANGE FROM FREE COMBINATION TO FDC time (in months) Hatalova K, Pella D, Hatala R, et al. Clin Drug Investig 2012
20 SYMBIO TRIAL WHAT WE HAVE LEARNED? - One explanation better adherence (compliance) when administered in one tablet daily - Drugs could be effective only if patients are taking them... - There are moreover some other benefits of such FDC described (better availability, absorption, etc.) Hatala R, Pella D, Hatalová K, et al. Clin Drug Investig 2012
21 PARALLELS IN TREATMENT APPROACH ARTERIAL HYPERTENSION AND DYSLIPIDEMIA JNC I diuretics, subsequent dose titration JNC II-IV betablockers, CCB, ACE-inhibitors JNC V prefered high doses in monotherapy JNC VI possibly combined treatment like the first step in treatment ATP I target LDL-C levels 3,4 mmol/l resp. 4,1 mmol/l, the first choice - niacin and bile acid sequestrants, statins only exceptionally ATP II target LDL-C levels 2,6 mmol/l, resp. 3,4mmol/l - recommended statiny, niacin, bile acid sequestrants, fibrates ATP III complete dominance of statins, target level of LDL-C below 2,6mmol/l JNC VII combined treatment even in newly diagnosed arterial hypertension Addendum ATP III target level of LDL-C below 1,8 mmol/l??? combined treatment for majority of very high risk or high risk patients

22 MAJORITY OF VERY HIGH RISK AND HIGH RISK PTS.DID NOT REACH LDL-C TARGET <2,5 MMOL/L (<1,8 MMOL/L) 1 Pts. not at target LDL-C <2,5 mmol/l 49% 56% Pacienti dosahujúci cieľové hodnoty LDL-C, % a % 11% LDL-C < 2,5 mmol/l 47% 13% 50% 16% LDL-C <1,8 mmol/l 49% 15% 51% 16% (Jan Aug) N=178,027 N=220,084 N=227,517 N=166,497 N=168,790 Pts. not at target LDL-C <1,8 mmol/l 84% 89% a Study population defined as CHD or CHD-equivalent individuals (treated and untreated) identified by ICD-9 and CPT diagnosis and procedure codes. ICD-9 = International Classification of Diseases, ninth edition; CPT = Current Procedural Terminology. 1. Data available on request from Merck & Co., Inc., Professional Services-DAP, WP1-27, PO Box 4, West Point, PA
23 Relative change * after 12 weeks HYBRID TREATMENT SIGNIFICANTLY LOWER BOTH, CHOLESTEROL ABSORPTION AND PRODUCTION Placebo (n=62) 3 4 Statin mg (n=232) Ezetimib 10 mg + statin mg (n=229) total cholesterol cholesterol production cholesterol absorption *Ratio (sterol:tc)=mean(10 2 mmol/mol). Sterol=sitosterol (absorption) and lathosterol (production) Adapted from Assmann G et al. Poster presented at the American College of Cardiology, New Orleans, Louisiana, USA, March 7 10, 2004.
24 ATHEROGENIC LIPOPROTEINS PHENOTYPE AND ATHEROGENESIS - Increased triglycerides - Decreased HDL-C - Conglomerate of apolipoproteins B (mainly apo B100) - Increased apolipoprotein CIII (increased VLDL) - Increased small dense LDL-particles
25 MAY ADDING OF FENOFIBRATE TO STATIN THERAPY INCREASE ITS SAFETY? IN THE PAST WE LEARNED OPPOSITE...BUT Statins increase expression of PCSK9 This statin effect could be modified with fenofibrate by dual mechanisms (blocking of RNA expression of PCSK9 and increasing of expression of RNA furine, which inactivate protease PCSK9 PCSK9 activity correlates very well with increased BMI, increased TG and insulin rezistence - statins and risk of newly diagnosed DM type 2 may be decreased by adding of fenofibrate but......next tablet to be prescribed... Konrad JR, et al. Lipids Health Dis 2011
26 DYSLIPIDEMIA TREATMENT IN ELDERLY PATIENTS Elderly pts. mostly very high risk pts. (target of LDL<1,8 mmol/l at least hybrid therapy is needed 2 lipid lowering drugs ( statin +ezetimibe), possibly PCSK9 inhibitor Atherogenic lipoproteins phenotype - add fenofibrate (TG>2,3 mmol/l, HDL<0,9 mmol/l)??? The higher is the age the higher is risk of myopathy (arround 10-20% in elderly population) Risk may be dramatically increased with number of pills used (not only those of lipid lowering)
27 PHARMACOLOGICAL APPROACH CAD (STABLE ANGINA PECTORIS) Prognosis improvement Antithrombotic therapy Statins ACE inhibitors β-blockers Reduction or symptoms removal β-blockers, Long-acting nitrates Calcium channel blockers Metabolic treatment I f inhibitor - ivabradine
28 CHRONIC HEART FAILURE - EPIDEMIOLOGY Dramatically increasing at the age arround 75 years Prevalence years old: 10-20% Heart Failure Malignant Disease!!! (mortality 2-times higher like in breast cancer or urine bladder, identical with colonic cancer) Remember: 10% of all hospitalized pts. due to acute or acute worsening of CHF
29 NUMBER OF PILLS USSUALLY PRESCRIBED IN CHF ACE-inhibitors perindopril enalapril lisinopril ramipril trandolapril Sartans (AT 1 receptor blockers) candesartan valsartan -blocker bisoprolol carvedilol metoprolol succinate nebivolol (seniors) Aldosteron antagonists eplerenone spironolaktone
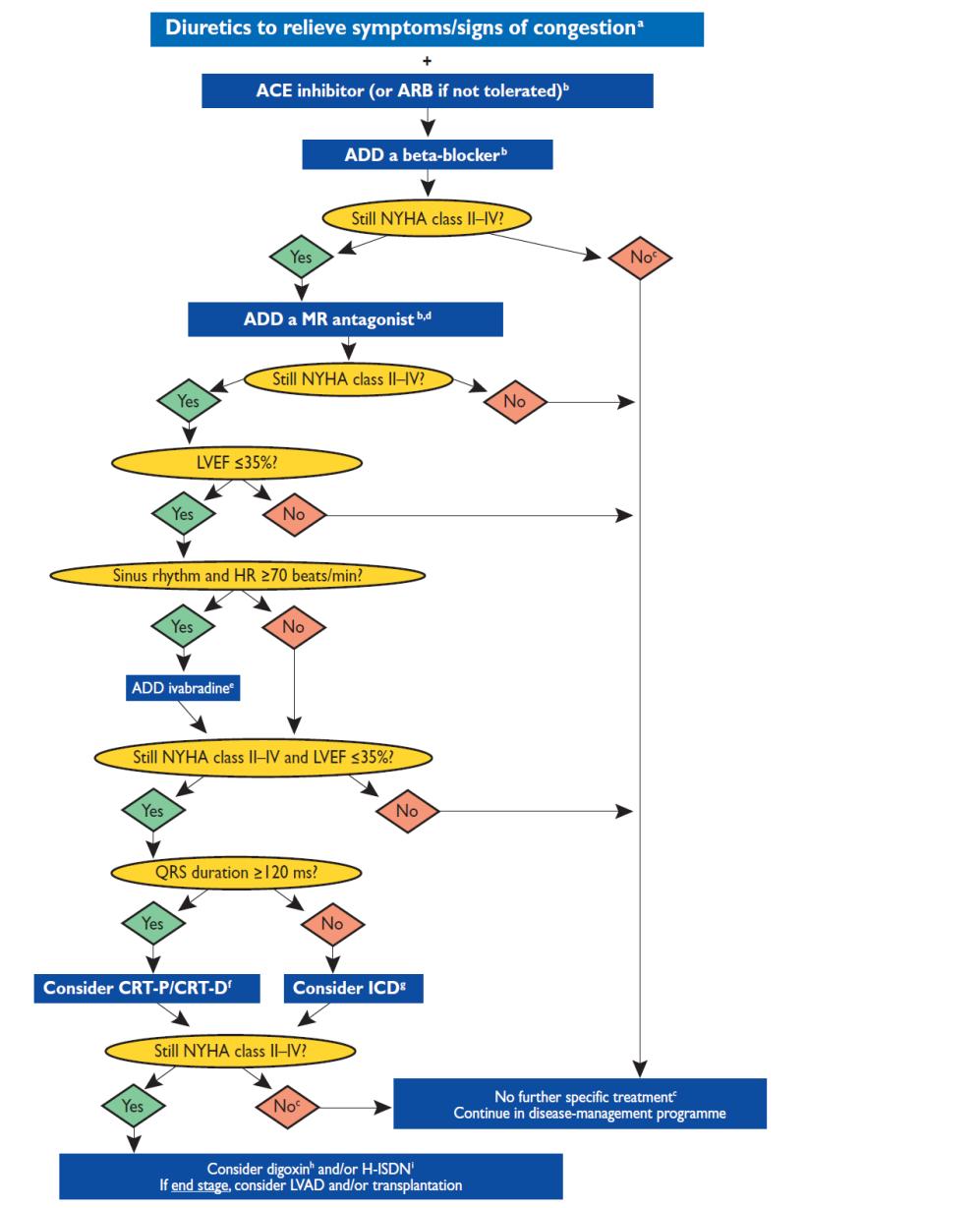
30 Guidelines for CHF
31 Patient XY, born after 1952 hypertensive, diabetes type 2, combined dyslipidemia, history of CAD with stable angina pectoris- suddenly hospitalized for acute myocardial infarction with LV dysfunction Treatment at discharge: (in red tablets before hospitalization) atorvastatin 80 mg tbl., bisoprolol 5 mg tbl., perindopril arginine 10 mg tbl., indapamid 1,5 mg tbl. ASA 100mg tbl., clopidogrel 75 mg tbl., fenofibrate 160 mg tbl., rilmenidine 1 mg tbl., ivabradine 2x5 mg tbl., amlodipine 2x5mg tbl., gliclazide 80 mg 13...not too many tablets? All prescribed when cardiologists follow guidelines...
32 Patient XY, born after 1952 hypertensive, diabetes type 2, combined dyslipidemia, history of CAD with stable angina pectoris- suddenly hospitalized for acute myocardial infarction with LV dysfunction - Moreover patient is suffering from back pain sporadically - Chronic obstructive pulmonary disease - after 3 months still not on the target with LDL- C (familial dyslipidemia or poor compliance?) - BP borderline values... - how to proceed? Add ezetimibe? PCSK9? Next antihypertensive agent?
33 Patient XY, born after 1952 hypertensive, diabetes type 2, combined dyslipidemia, history of CAD with stable angina pectoris- suddenly hospitalized for acute myocardial infarction with LV dysfunction Treatment at discharge: (in red tablets before hospitalization) atorvastatin 80 mg tbl., bisoprolol 5 mg tbl., perindopril arginine 10 mg tbl., indapamid 1,5 mg tbl. ASA 100mg tbl., clopidogrel 75 mg tbl., fenofibrate 160 mg tbl., rilmenidine 1 mg tbl., ivabradine 2x5 mg tbl., amlodipine 2x5mg tbl., gliklazid 80 mg New treatment: from 13 tablets to 7 tablets and even morfe effective Implicor 2x50/5 mg, Triplixam 10/2,5/10, Atozet 80/10mg,ASA 100mg, Clopidogrel 75 mg, gliclazide 80 mg
34 INNOVATIVE TREATMENT FOR CAD, CHF AND DYSLIPIDEMIA MORE DRUGS TO BE USED? sacubitril and valsartan (?) Canakinumab (?) PCSK 9 inhibitors Other monoclonal antibodies
35 EDUCATION AND HEALTHY LIFESTYLE BACKGROUND FOR RATIONAL POLYPHARMACY Etiology, diagnosis, prognosis, compliance to therapy Symptoms monitoring, more applied self-care The way how to increase drug adherence FDC (based on EBM) Regular physical activity may lead to reduction of number of tablets needed
36 EDUCATION AND HEALTHY LIFESTYLE BACKGROUND FOR RATIONAL POLYPHARMACY Quit smoking, limited consumption of alcohol Relax, entertainment, physical activity (sexual as well) prevent depression Always remember words from Hippocratic oath: primum nil nocere Usually is true - less is more (tablets...)
37 CONCLUSIONS OR HOW TO ELIMINATE POLYPHARMACY AND REDUCE POLYPHARMACY? Seems to be very easy question in ideal population Unfortunately, physicians have their knowledge limits, patients will still sometimes prefer something else like it is recommended
38 CONCLUSIONS OR HOW TO ELIMINATE POLYPHARMACY AND REDUCE POLYPHARMACY? Seems to be very easy question in ideal population Unfortunately, physicians have their knowledge limits, patients will still sometimes prefer something else like it is recommended What could be expected in the future?
39 NEAR FUTURE OR NEXT DECADES? More omics in medicine (genomics, metabolomics, proteomics, etc.) not only in diagnostics, but also in therapeutic process Dramatic increase of research in biomedicine and translational medicine More and more personalized medicine to be applied
40 NEAR FUTURE OR NEXT DECADES? Wide use of e-health systems Implementation of arteficial intelligence into common clinical practice Elimination of polypragmasy, limitation of polypharmacy could be expected

41 Ďakujem Thank you Danke Dziekuje bardzo
Update in Hypertension
 Update in Hypertension Eliseo J. PérezP rez-stable MD Professor of Medicine DGIM, Department of Medicine UCSF 20 May 2008 Declaration of full disclosure: No conflict of interest (I have never been funded
Update in Hypertension Eliseo J. PérezP rez-stable MD Professor of Medicine DGIM, Department of Medicine UCSF 20 May 2008 Declaration of full disclosure: No conflict of interest (I have never been funded
Management of Hypertension
 Clinical Practice Guidelines Management of Hypertension Definition and classification of blood pressure levels (mmhg) Category Systolic Diastolic Normal
Clinical Practice Guidelines Management of Hypertension Definition and classification of blood pressure levels (mmhg) Category Systolic Diastolic Normal
MANAGEMENT OF HYPERTENSION: TREATMENT THRESHOLDS AND MEDICATION SELECTION
 Management of Hypertension: Treatment Thresholds and Medication Selection Robert B. Baron, MD MS Professor and Associate Dean Declaration of full disclosure: No conflict of interest Presentation Goals
Management of Hypertension: Treatment Thresholds and Medication Selection Robert B. Baron, MD MS Professor and Associate Dean Declaration of full disclosure: No conflict of interest Presentation Goals
Causes of Poor BP control Rates
 Goals Of Hypertension Management in Clinical Practice World Hypertension League (WHL) Meeting Adel E. Berbari, MD, FAHA, FACP Professor of Medicine and Physiology Head, Division of Hypertension and Vascular
Goals Of Hypertension Management in Clinical Practice World Hypertension League (WHL) Meeting Adel E. Berbari, MD, FAHA, FACP Professor of Medicine and Physiology Head, Division of Hypertension and Vascular
New Lipid Guidelines. PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN: Implications of the New Guidelines for Hypertension and Lipids.
 PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN: Implications of the New Guidelines for Hypertension and Lipids Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Disclosure No relevant
PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN: Implications of the New Guidelines for Hypertension and Lipids Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Disclosure No relevant
Management of Lipid Disorders and Hypertension: Implications of the New Guidelines
 Management of Lipid Disorders and Hypertension Management of Lipid Disorders and Hypertension: Implications of the New Guidelines Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine
Management of Lipid Disorders and Hypertension Management of Lipid Disorders and Hypertension: Implications of the New Guidelines Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine
Treating Hypertension in Individuals with Diabetes
 Treating Hypertension in Individuals with Diabetes Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any
Treating Hypertension in Individuals with Diabetes Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any
The Latest Generation of Clinical
 The Latest Generation of Clinical Guidelines: HTN and HLD Dave Brackett Clinical Guideline Purpose Uniform approach Awareness of key details Diagnosis Treatment Monitoring Evidence based approach Inform
The Latest Generation of Clinical Guidelines: HTN and HLD Dave Brackett Clinical Guideline Purpose Uniform approach Awareness of key details Diagnosis Treatment Monitoring Evidence based approach Inform
Outcomes and Perspectives of Single-Pill Combination Therapy for the modern management of hypertension
 Outcomes and Perspectives of Single-Pill Combination Therapy for the modern management of hypertension Prof. Massimo Volpe, MD, FAHA, FESC, Chair of Cardiology, Department of Clinical and Molecular Medicine
Outcomes and Perspectives of Single-Pill Combination Therapy for the modern management of hypertension Prof. Massimo Volpe, MD, FAHA, FESC, Chair of Cardiology, Department of Clinical and Molecular Medicine
Long-Term Care Updates
 Long-Term Care Updates August 2015 By Darren Hein, PharmD Hypertension is a clinical condition in which the force of blood pushing on the arteries is higher than normal. This increases the risk for heart
Long-Term Care Updates August 2015 By Darren Hein, PharmD Hypertension is a clinical condition in which the force of blood pushing on the arteries is higher than normal. This increases the risk for heart
Highlights of the new blood pressure and cholesterol guidelines: A whole new philosophy. Jeremy L. Johnson, PharmD, BCACP, CDE, BC-ADM
 Highlights of the new blood pressure and cholesterol guidelines: A whole new philosophy Jeremy L. Johnson, PharmD, BCACP, CDE, BC-ADM OSHP 2014 Annual Meeting Oklahoma City, OK April 4, 2014 1 Objectives
Highlights of the new blood pressure and cholesterol guidelines: A whole new philosophy Jeremy L. Johnson, PharmD, BCACP, CDE, BC-ADM OSHP 2014 Annual Meeting Oklahoma City, OK April 4, 2014 1 Objectives
Clinical cases with Coversyl 10 mg
 Clinical cases Coversyl 10 mg For upgraded benefits in hypertension A Editorial This brochure, Clinical cases Coversyl 10 mg for upgraded benefits in hypertension, illustrates a variety of hypertensive
Clinical cases Coversyl 10 mg For upgraded benefits in hypertension A Editorial This brochure, Clinical cases Coversyl 10 mg for upgraded benefits in hypertension, illustrates a variety of hypertensive
Younger adults with a family history of premature artherosclerotic disease should have their cardiovascular risk factors measured.
 Appendix 2A - Guidance on Management of Hypertension Measurement of blood pressure All adults from 40 years should have blood pressure measured as part of opportunistic cardiovascular risk assessment.
Appendix 2A - Guidance on Management of Hypertension Measurement of blood pressure All adults from 40 years should have blood pressure measured as part of opportunistic cardiovascular risk assessment.
Hypertension (JNC-8)
") Hypertension (JNC-8) Southern California University of Health Sciences Physician Assistant Program Management and Treatment of Hypertension April 17, 2018, presented by Ezra Levy, Pharm.D.! The 8 th Joint
Hypertension (JNC-8) Southern California University of Health Sciences Physician Assistant Program Management and Treatment of Hypertension April 17, 2018, presented by Ezra Levy, Pharm.D.! The 8 th Joint
Clinical Recommendations: Patients with Periodontitis
 The American Journal of Cardiology and Journal of Periodontology Editors' Consensus: Periodontitis and Atherosclerotic Cardiovascular Disease. Friedewald VE, Kornman KS, Beck JD, et al. J Periodontol 2009;
The American Journal of Cardiology and Journal of Periodontology Editors' Consensus: Periodontitis and Atherosclerotic Cardiovascular Disease. Friedewald VE, Kornman KS, Beck JD, et al. J Periodontol 2009;
Combination Therapy for Hypertension
 Combination Therapy for Hypertension Se-Joong Rim, MD Cardiology Division, Yonsei University College of Medicine, Seoul, Korea Goals of Therapy Reduce CVD and renal morbidity and mortality. Treat to BP
Combination Therapy for Hypertension Se-Joong Rim, MD Cardiology Division, Yonsei University College of Medicine, Seoul, Korea Goals of Therapy Reduce CVD and renal morbidity and mortality. Treat to BP
Heart Failure Clinician Guide JANUARY 2018
 Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Heart Failure Clinician Guide JANUARY 2018 Introduction This evidence-based guideline summary is based on the 2018 National Heart Failure Guideline.
Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Heart Failure Clinician Guide JANUARY 2018 Introduction This evidence-based guideline summary is based on the 2018 National Heart Failure Guideline.
Rationale for the use of Single Pill Combination. Yong Jin Kim, MD Seoul National University Hospital
 Rationale for the use of Single Pill Combination Yong Jin Kim, MD Seoul National University Hospital Unmet Need of Hypertension Treatment Hypertension # 1 Risk Factor for Global Mortality 0 1 2 3 4 5 6
Rationale for the use of Single Pill Combination Yong Jin Kim, MD Seoul National University Hospital Unmet Need of Hypertension Treatment Hypertension # 1 Risk Factor for Global Mortality 0 1 2 3 4 5 6
Management of High Blood Pressure in Adults
 Management of High Blood Pressure in Adults Based on the Report from the Panel Members Appointed to the Eighth Joint National Committee (JNC8) James, P. A. (2014, February 05). 2014 Guideline for Management
Management of High Blood Pressure in Adults Based on the Report from the Panel Members Appointed to the Eighth Joint National Committee (JNC8) James, P. A. (2014, February 05). 2014 Guideline for Management
New Antihypertensive Strategies to Improve Blood Pressure Control
 New Antihypertensive Strategies to Improve Blood Pressure Control Antonio Coca, MD, PhD,, FRCP, FESC Hypertension and Vascular Risk Unit Department of Internal Medicine. Hospital Clínic (IDIBAPS) University
New Antihypertensive Strategies to Improve Blood Pressure Control Antonio Coca, MD, PhD,, FRCP, FESC Hypertension and Vascular Risk Unit Department of Internal Medicine. Hospital Clínic (IDIBAPS) University
Hypertension Guidelines: Are We Pressured to Change? Oregon Cardiovascular Symposium Portland, Oregon June 6, Financial Disclosures
 Hypertension Guidelines: Are We Pressured to Change? Oregon Cardiovascular Symposium Portland, Oregon June 6, 2015 William C. Cushman, MD Professor, Preventive Medicine, Medicine, and Physiology University
Hypertension Guidelines: Are We Pressured to Change? Oregon Cardiovascular Symposium Portland, Oregon June 6, 2015 William C. Cushman, MD Professor, Preventive Medicine, Medicine, and Physiology University
How would you manage Ms. Gold
 How would you manage Ms. Gold 32 yo Asian woman with dyslipidemia Current medications: Simvastatin 20mg QD Most recent lipid profile: TC = 246, TG = 100, LDL = 176, HDL = 50 What about Mr. Williams? 56
How would you manage Ms. Gold 32 yo Asian woman with dyslipidemia Current medications: Simvastatin 20mg QD Most recent lipid profile: TC = 246, TG = 100, LDL = 176, HDL = 50 What about Mr. Williams? 56
By Prof. Khaled El-Rabat
 What is The Optimum? By Prof. Khaled El-Rabat Professor of Cardiology - Benha Faculty of Medicine HT. Introduction Despite major worldwide efforts over recent decades directed at diagnosing and treating
What is The Optimum? By Prof. Khaled El-Rabat Professor of Cardiology - Benha Faculty of Medicine HT. Introduction Despite major worldwide efforts over recent decades directed at diagnosing and treating
HYPERTENSION GUIDELINES WHERE ARE WE IN 2014
 HYPERTENSION GUIDELINES WHERE ARE WE IN 2014 Donald J. DiPette MD FACP Special Assistant to the Provost for Health Affairs Distinguished Health Sciences Professor University of South Carolina University
HYPERTENSION GUIDELINES WHERE ARE WE IN 2014 Donald J. DiPette MD FACP Special Assistant to the Provost for Health Affairs Distinguished Health Sciences Professor University of South Carolina University
Hypertension Update 2009
 Hypertension Update 2009 New Drugs, New Goals, New Approaches, New Lessons from Clinical Trials Timothy C Fagan, MD, FACP Professor Emeritus University of Arizona New Drugs Direct Renin Inhibitors Endothelin
Hypertension Update 2009 New Drugs, New Goals, New Approaches, New Lessons from Clinical Trials Timothy C Fagan, MD, FACP Professor Emeritus University of Arizona New Drugs Direct Renin Inhibitors Endothelin
Cardiovascular Health Practice Guideline Outpatient Management of Coronary Artery Disease 2003
 Authorized By: Medical Management Guideline Committee Approval Date: 12/13/01 Revision Date: 12/11/03 Beta-Blockers Nitrates Calcium Channel Blockers MEDICATIONS Indicated in post-mi, unstable angina,
Authorized By: Medical Management Guideline Committee Approval Date: 12/13/01 Revision Date: 12/11/03 Beta-Blockers Nitrates Calcium Channel Blockers MEDICATIONS Indicated in post-mi, unstable angina,
Preventing and Treating High Blood Pressure
 Preventing and Treating High Blood Pressure: Finding the Right Balance of Integrative and Pharmacologic Approaches Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Blood Pressure
Preventing and Treating High Blood Pressure: Finding the Right Balance of Integrative and Pharmacologic Approaches Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Blood Pressure
Hypertension Update Warwick Jaffe Interventional Cardiologist Ascot Hospital
 Hypertension Update 2008 Warwick Jaffe Interventional Cardiologist Ascot Hospital Definition of Hypertension Continuous variable At some point the risk becomes high enough to justify treatment Treatment
Hypertension Update 2008 Warwick Jaffe Interventional Cardiologist Ascot Hospital Definition of Hypertension Continuous variable At some point the risk becomes high enough to justify treatment Treatment
How clinically important are the results of the large trials in hypertension?
 How clinically important are the results of the large trials in hypertension? Stéphane LAURENT, MD, PhD, FESC Pharmacology Department and PARCC / INSERM U970 Hôpital Européen Georges Pompidou, Université
How clinically important are the results of the large trials in hypertension? Stéphane LAURENT, MD, PhD, FESC Pharmacology Department and PARCC / INSERM U970 Hôpital Européen Georges Pompidou, Université
New Recommendations for the Treatment of Hypertension: From Population Salt Reduction to Personalized Treatment Targets
 New Recommendations for the Treatment of Hypertension: From Population Salt Reduction to Personalized Treatment Targets Sidney C. Smith, Jr. MD, FACC, FAHA Professor of Medicine/Cardiology University of
New Recommendations for the Treatment of Hypertension: From Population Salt Reduction to Personalized Treatment Targets Sidney C. Smith, Jr. MD, FACC, FAHA Professor of Medicine/Cardiology University of
Objectives. Describe results and implications of recent landmark hypertension trials
 Hypertension Update Daniel Schwartz, MD Assistant Professor of Medicine Associate Medical Director of Heart Transplantation Temple University School of Medicine Disclosures I currently have no relationships
Hypertension Update Daniel Schwartz, MD Assistant Professor of Medicine Associate Medical Director of Heart Transplantation Temple University School of Medicine Disclosures I currently have no relationships
Modern Management of Hypertension
 Modern Management of Hypertension Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Current Status of Hypertension Prevalence
Modern Management of Hypertension Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Current Status of Hypertension Prevalence
ADVANCES IN MANAGEMENT OF HYPERTENSION
 Advances in Management of Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Current Status of Prevalence 29%; Blacks 33.5%
Advances in Management of Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Current Status of Prevalence 29%; Blacks 33.5%
Approach to Dyslipidemia among diabetic patients
 Approach to Dyslipidemia among diabetic patients Farzad Hadaegh, MD, Professor of Internal Medicine & Endocrinology Prevention of Metabolic Disorders Research Center, Research Institute for Endocrine Sciences
Approach to Dyslipidemia among diabetic patients Farzad Hadaegh, MD, Professor of Internal Medicine & Endocrinology Prevention of Metabolic Disorders Research Center, Research Institute for Endocrine Sciences
Prevention of Heart Failure: What s New with Hypertension
 Prevention of Heart Failure: What s New with Hypertension Ali AlMasood Prince Sultan Cardiac Center Riyadh 3ed Saudi Heart Failure conference, Jeddah, 13 December 2014 Background 20-30% of Saudi adults
Prevention of Heart Failure: What s New with Hypertension Ali AlMasood Prince Sultan Cardiac Center Riyadh 3ed Saudi Heart Failure conference, Jeddah, 13 December 2014 Background 20-30% of Saudi adults
ADVANCES IN MANAGEMENT OF HYPERTENSION
 Prevalence 29%; Blacks 33.5% About 72.5% treated; 53.5% uncontrolled (>140/90) Risk for poor control: Latinos, Blacks, age 18-44 and 80,
Prevalence 29%; Blacks 33.5% About 72.5% treated; 53.5% uncontrolled (>140/90) Risk for poor control: Latinos, Blacks, age 18-44 and 80,
Heart Failure Clinician Guide JANUARY 2016
 Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Heart Failure Clinician Guide JANUARY 2016 Introduction This evidence-based guideline summary is based on the 2016 National Heart Failure Guideline.
Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Heart Failure Clinician Guide JANUARY 2016 Introduction This evidence-based guideline summary is based on the 2016 National Heart Failure Guideline.
Objectives. JNC 7 Is Nice But What s Up With JNC 8? Why Do We Care? Hypertension Background: Prevalence
 JNC 7 Is Nice But What s Up With JNC 8? 37 th Annual CAPA Conference October 4 th 2013 Ignacio de Artola, Jr. M.D. Assistant Professor of Clinical Family Medicine Medical Director, Primary Care Physician
JNC 7 Is Nice But What s Up With JNC 8? 37 th Annual CAPA Conference October 4 th 2013 Ignacio de Artola, Jr. M.D. Assistant Professor of Clinical Family Medicine Medical Director, Primary Care Physician
Marshall Tulloch-Reid, MD, MPhil, DSc, FACE Epidemiology Research Unit Tropical Medicine Research Institute The University of the West Indies, Mona,
 Marshall Tulloch-Reid, MD, MPhil, DSc, FACE Epidemiology Research Unit Tropical Medicine Research Institute The University of the West Indies, Mona, Jamaica At the end of this presentation the participant
Marshall Tulloch-Reid, MD, MPhil, DSc, FACE Epidemiology Research Unit Tropical Medicine Research Institute The University of the West Indies, Mona, Jamaica At the end of this presentation the participant
Updates in Cardiovascular Recommendations for Diabetic Patients
 Updates in Cardiovascular Recommendations for Diabetic Patients Chris Tawwater, Pharm.D., BCPS Clinical Pharmacist, Abilene Regional Medical Center Assistant Professor, Adult Medicine Division Pharmacotherapy
Updates in Cardiovascular Recommendations for Diabetic Patients Chris Tawwater, Pharm.D., BCPS Clinical Pharmacist, Abilene Regional Medical Center Assistant Professor, Adult Medicine Division Pharmacotherapy
Explore the Rationale for the Dual Mechanism CCB/ARB Approach in Hypertension Management
 Explore the Rationale for the Dual Mechanism CCB/ARB Approach in Hypertension Management Jeong Bae Park, MD,PhD Dept of Med/Cardiology, Cheil General Hospital, Kwandong University College of Medicine Apr
Explore the Rationale for the Dual Mechanism CCB/ARB Approach in Hypertension Management Jeong Bae Park, MD,PhD Dept of Med/Cardiology, Cheil General Hospital, Kwandong University College of Medicine Apr
Treatment to reduce cardiovascular risk: multifactorial management
 Treatment to reduce cardiovascular risk: multifactorial management Matteo Anselmino, MD PhD Assistant Professor San Giovanni Battista Hospital Division of Cardiology, Department of Internal Medicine University
Treatment to reduce cardiovascular risk: multifactorial management Matteo Anselmino, MD PhD Assistant Professor San Giovanni Battista Hospital Division of Cardiology, Department of Internal Medicine University
VA/DoD Clinical Practice Guideline for the Diagnosis and Management of Hypertension - Pocket Guide Update 2004 Revision July 2005
 VA/DoD Clinical Practice Guideline for the Diagnosis and Management of Hypertension - Pocket Guide Update 2004 Revision July 2005 1 Any adult in the health care system 2 Obtain blood pressure (BP) (Reliable,
VA/DoD Clinical Practice Guideline for the Diagnosis and Management of Hypertension - Pocket Guide Update 2004 Revision July 2005 1 Any adult in the health care system 2 Obtain blood pressure (BP) (Reliable,
Managing Hypertension in 2016
 Managing Hypertension in 2016: Where Do We Draw the Line? Disclosure No relevant financial relationships Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine baron@medicine.ucsf.edu
Managing Hypertension in 2016: Where Do We Draw the Line? Disclosure No relevant financial relationships Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine baron@medicine.ucsf.edu
PIEDMONT ACCESS TO HEALTH SERVICES, INC. Guidelines for Screening and Management of Dyslipidemia
 PIEDMONT ACCESS TO HEALTH SERVICES, INC. Policy Number: 01-09-021 SUBJECT: Guidelines for Screening and Management of Dyslipidemia EFFECTIVE DATE: 04/2008 REVIEWED/REVISED: 04/12/10, 03/17/2011, 4/10/2012,
PIEDMONT ACCESS TO HEALTH SERVICES, INC. Policy Number: 01-09-021 SUBJECT: Guidelines for Screening and Management of Dyslipidemia EFFECTIVE DATE: 04/2008 REVIEWED/REVISED: 04/12/10, 03/17/2011, 4/10/2012,
Disclosures. Diabetes and Cardiovascular Risk Management. Learning Objectives. Atherosclerotic Cardiovascular Disease
 Disclosures Diabetes and Cardiovascular Risk Management Tony Hampton, MD, MBA Medical Director Advocate Aurora Operating System Advocate Aurora Healthcare Downers Grove, IL No conflicts or disclosures
Disclosures Diabetes and Cardiovascular Risk Management Tony Hampton, MD, MBA Medical Director Advocate Aurora Operating System Advocate Aurora Healthcare Downers Grove, IL No conflicts or disclosures
Use of Beta-blocker Monotherapy in Hypertension: Situation in a Local General Outpatient Clinic
 Use of Beta-blocker Monotherapy in Hypertension: Situation in a Local General Outpatient Clinic Dr. Dao Man Chi Resident Department of Family Medicine and Primary Health Care, KWC HA Convention 2014 Introduction
Use of Beta-blocker Monotherapy in Hypertension: Situation in a Local General Outpatient Clinic Dr. Dao Man Chi Resident Department of Family Medicine and Primary Health Care, KWC HA Convention 2014 Introduction
Module 2. Global Cardiovascular Risk Assessment and Reduction in Women with Hypertension
 Module 2 Global Cardiovascular Risk Assessment and Reduction in Women with Hypertension 1 Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored,
Module 2 Global Cardiovascular Risk Assessment and Reduction in Women with Hypertension 1 Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored,
DISCLOSURE PHARMACIST OBJECTIVES 9/30/2014 JNC 8: A REVIEW OF THE LONG-AWAITED/MUCH-ANTICIPATED HYPERTENSION GUIDELINES. I have nothing to disclose.
 JNC 8: A REVIEW OF THE LONG-AWAITED/MUCH-ANTICIPATED HYPERTENSION GUIDELINES Tiffany Dickey, PharmD Assistant Professor, UAMS COP Clinical Pharmacy Specialist, Mercy Hospital Northwest AR DISCLOSURE I
JNC 8: A REVIEW OF THE LONG-AWAITED/MUCH-ANTICIPATED HYPERTENSION GUIDELINES Tiffany Dickey, PharmD Assistant Professor, UAMS COP Clinical Pharmacy Specialist, Mercy Hospital Northwest AR DISCLOSURE I
Long-Term Complications of Diabetes Mellitus Macrovascular Complication
 Long-Term Complications of Diabetes Mellitus Macrovascular Complication Sung Hee Choi MD, PhD Professor, Seoul National University College of Medicine, SNUBH, Bundang Hospital Diabetes = CVD equivalent
Long-Term Complications of Diabetes Mellitus Macrovascular Complication Sung Hee Choi MD, PhD Professor, Seoul National University College of Medicine, SNUBH, Bundang Hospital Diabetes = CVD equivalent
Hypertension, Hyperlipidemia and Obesity. Mi-CCSI
 Hypertension, Hyperlipidemia and Obesity Mi-CCSI Objectives Review the prevalence of hypertension, hyperlipidemia and obesity Correlation of the 3 conditions Discuss why it is important to treat these
Hypertension, Hyperlipidemia and Obesity Mi-CCSI Objectives Review the prevalence of hypertension, hyperlipidemia and obesity Correlation of the 3 conditions Discuss why it is important to treat these
Managing Hypertension in Diabetes Sean Stewart, PharmD, BCPS, BCACP, CLS Internal Medicine Park Nicollet Clinic St Louis Park.
 Managing Hypertension in Diabetes 2015 Sean Stewart, PharmD, BCPS, BCACP, CLS Internal Medicine Park Nicollet Clinic St Louis Park Case Scenario Mike M is a 59 year old man with type 2 diabetes managed
Managing Hypertension in Diabetes 2015 Sean Stewart, PharmD, BCPS, BCACP, CLS Internal Medicine Park Nicollet Clinic St Louis Park Case Scenario Mike M is a 59 year old man with type 2 diabetes managed
JNC Evidence-Based Guidelines for the Management of High Blood Pressure in Adults
 JNC 8 2014 Evidence-Based Guidelines for the Management of High Blood Pressure in Adults Table of Contents Why Do We Treat Hypertension? Blood Pressure Treatment Goals Initial Therapy Strength of Recommendation
JNC 8 2014 Evidence-Based Guidelines for the Management of High Blood Pressure in Adults Table of Contents Why Do We Treat Hypertension? Blood Pressure Treatment Goals Initial Therapy Strength of Recommendation
ANTI- HYPERTENSIVE AGENTS
 CLINICAL ANTI- HYPERTENSIVE AGENTS Jacqueline van Schoor, MPharm, BSc (Hons) Amayeza Info Centre Hypertension represents a major public health concern. It affects about a billion people worldwide and is
CLINICAL ANTI- HYPERTENSIVE AGENTS Jacqueline van Schoor, MPharm, BSc (Hons) Amayeza Info Centre Hypertension represents a major public health concern. It affects about a billion people worldwide and is
Disclosures. Learning Objectives. Hypertension: a sprint to the finish Ontario Pharmacists Association 1
 Disclosures I have no current or past relationships with commercial entities I have received a speaker s fee from the Ontario Pharmacists Association for this learning activity Laura Tsang PharmD Sunnybrook
Disclosures I have no current or past relationships with commercial entities I have received a speaker s fee from the Ontario Pharmacists Association for this learning activity Laura Tsang PharmD Sunnybrook
Diabetes and Hypertension
 Diabetes and Hypertension William C. Cushman, MD, FAHA, FACP, FASH Chief, Preventive Medicine, Veterans Affairs Medical Center Professor, Preventive Medicine, Medicine, and Physiology University of Tennessee
Diabetes and Hypertension William C. Cushman, MD, FAHA, FACP, FASH Chief, Preventive Medicine, Veterans Affairs Medical Center Professor, Preventive Medicine, Medicine, and Physiology University of Tennessee
Volume 6; Number 1 January 2012 NICE CLINICAL GUIDELINE 127: HYPERTENSION CLINICAL MANAGEMENT OF PRIMARY HYPERTENSION IN ADULTS (AUGUST 2011)
") Volume 6; Number 1 January 2012 NICE CLINICAL GUIDELINE 127: HYPERTENSION CLINICAL MANAGEMENT OF PRIMARY HYPERTENSION IN ADULTS (AUGUST 2011) What s new in hypertension? NICE has issued an updated Clinical
Volume 6; Number 1 January 2012 NICE CLINICAL GUIDELINE 127: HYPERTENSION CLINICAL MANAGEMENT OF PRIMARY HYPERTENSION IN ADULTS (AUGUST 2011) What s new in hypertension? NICE has issued an updated Clinical
Best Practices in Cardiac Care: Getting with the Guidelines
 Best Practices in Cardiac Care: Getting with the Guidelines December 9, 2014 Agenda Cardiovascular Disease: How do the guidelines fit into an implementation scheme? What the guidelines set out to accomplish
Best Practices in Cardiac Care: Getting with the Guidelines December 9, 2014 Agenda Cardiovascular Disease: How do the guidelines fit into an implementation scheme? What the guidelines set out to accomplish
Hypertension. Does it Matter What Medications We Use? Nishant K. Sekaran, M.D. M.Sc. Intermountain Heart Institute
 Hypertension Does it Matter What Medications We Use? Nishant K. Sekaran, M.D. M.Sc. Intermountain Heart Institute Hypertension 2017 Classification BP Category Systolic Diastolic Normal 120 and 80 Elevated
Hypertension Does it Matter What Medications We Use? Nishant K. Sekaran, M.D. M.Sc. Intermountain Heart Institute Hypertension 2017 Classification BP Category Systolic Diastolic Normal 120 and 80 Elevated
Difficult to Treat Hypertension
 Difficult to Treat Hypertension According to Goldilocks JNC 8 Blood Pressure Goals (2014) BP Goal 60 years old and greater*- systolic < 150 and diastolic < 90. (Grade A)** BP Goal 18-59 years old* diastolic
Difficult to Treat Hypertension According to Goldilocks JNC 8 Blood Pressure Goals (2014) BP Goal 60 years old and greater*- systolic < 150 and diastolic < 90. (Grade A)** BP Goal 18-59 years old* diastolic
Program Metrics. New Unique ID. Old Unique ID. Metric Set Metric Name Description. Old Metric Name
 Program Metrics The list below includes the metrics that will be calculated by the PINNACLE Registry for the outpatient office setting. These include metrics for, Atrial Fibrillation, Hypertension and.
Program Metrics The list below includes the metrics that will be calculated by the PINNACLE Registry for the outpatient office setting. These include metrics for, Atrial Fibrillation, Hypertension and.
2014 HYPERTENSION GUIDELINES
 2014 HYPERTENSION GUIDELINES Eileen M. Twomey, Pharm.D., BCPS 1 Learning Objectives Describe specific blood pressure thresholds at which antihypertensive therapy should be initiated and blood pressure
2014 HYPERTENSION GUIDELINES Eileen M. Twomey, Pharm.D., BCPS 1 Learning Objectives Describe specific blood pressure thresholds at which antihypertensive therapy should be initiated and blood pressure
Royal Wolverhampton Hospital Adult Lipid Lowering Therapy Guidelines Lipid Lowering Therapy for the Prevention of Cardiovascular Disease
 Royal Wolverhampton Hospital Adult Lipid Lowering Therapy Guidelines 1 This guideline is intended to assist rational and cost-effective prescribing of lipid regulating medications across both primary and
Royal Wolverhampton Hospital Adult Lipid Lowering Therapy Guidelines 1 This guideline is intended to assist rational and cost-effective prescribing of lipid regulating medications across both primary and
Is there a mechanism of interaction between hypertension and dyslipidaemia?
 Is there a mechanism of interaction between hypertension and dyslipidaemia? Neil R Poulter International Centre for Circulatory Health NHLI, Imperial College London Daegu, Korea April 2005 Observational
Is there a mechanism of interaction between hypertension and dyslipidaemia? Neil R Poulter International Centre for Circulatory Health NHLI, Imperial College London Daegu, Korea April 2005 Observational
STANDARD treatment algorithm mmHg
 STANDARD treatment algorithm 130-140mmHg (i) At BASELINE, If AVERAGE SBP 1 > 140mmHg If on no antihypertensive drugs: Start 1 drug: If >55 years old / Afro-Caribbean: Calcium channel blocker (CCB) 2 If
STANDARD treatment algorithm 130-140mmHg (i) At BASELINE, If AVERAGE SBP 1 > 140mmHg If on no antihypertensive drugs: Start 1 drug: If >55 years old / Afro-Caribbean: Calcium channel blocker (CCB) 2 If
Modern Management of Hypertension: Where Do We Draw the Line?
 Modern Management of Hypertension: Where Do We Draw the Line? Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Blood Pressure
Modern Management of Hypertension: Where Do We Draw the Line? Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Blood Pressure
MOLINA HEALTHCARE OF CALIFORNIA
 MOLINA HEALTHCARE OF CALIFORNIA HIGH BLOOD CHOLESTEROL IN ADULTS GUIDELINE Molina Healthcare of California has adopted the Third Report of the National Cholesterol Education Program (NCEP) Expert Panel
MOLINA HEALTHCARE OF CALIFORNIA HIGH BLOOD CHOLESTEROL IN ADULTS GUIDELINE Molina Healthcare of California has adopted the Third Report of the National Cholesterol Education Program (NCEP) Expert Panel
Hypertension Update Clinical Controversies Regarding Age and Race
 Hypertension Update Clinical Controversies Regarding Age and Race Allison Helmer, PharmD, BCACP Assistant Clinical Professor Auburn University Harrison School of Pharmacy July 22, 2017 DISCLOSURE/CONFLICT
Hypertension Update Clinical Controversies Regarding Age and Race Allison Helmer, PharmD, BCACP Assistant Clinical Professor Auburn University Harrison School of Pharmacy July 22, 2017 DISCLOSURE/CONFLICT
Management of Hypertension in special groups. DR-Mohammed Salah Assistant Lecturer of Cardiology Mansoura University
 Management of Hypertension in special groups BY DR-Mohammed Salah Assistant Lecturer of Cardiology Mansoura University AGENDA SPECIAL GROUPS SPECIFIC DRUDS FOR SPECIAL GROUPS TARGET BP FOR SPECIAL GROUPS:
Management of Hypertension in special groups BY DR-Mohammed Salah Assistant Lecturer of Cardiology Mansoura University AGENDA SPECIAL GROUPS SPECIFIC DRUDS FOR SPECIAL GROUPS TARGET BP FOR SPECIAL GROUPS:
Dyslipidemia in the light of Current Guidelines - Do we change our Practice?
 Dyslipidemia in the light of Current Guidelines - Do we change our Practice? Dato Dr. David Chew Soon Ping Senior Consultant Cardiologist Institut Jantung Negara Atherosclerotic Cardiovascular Disease
Dyslipidemia in the light of Current Guidelines - Do we change our Practice? Dato Dr. David Chew Soon Ping Senior Consultant Cardiologist Institut Jantung Negara Atherosclerotic Cardiovascular Disease
Hypertension in 2015: SPRINT-ing ahead of JNC-8. MAJ Charles Magee, MD MPH FACP Director, WRNMMC Hypertension Clinic
 Hypertension in 2015: SPRINT-ing ahead of JNC-8 MAJ Charles Magee, MD MPH FACP Director, WRNMMC Hypertension Clinic Conflits of interest? None Disclaimer The opinions contained herein are not to be considered
Hypertension in 2015: SPRINT-ing ahead of JNC-8 MAJ Charles Magee, MD MPH FACP Director, WRNMMC Hypertension Clinic Conflits of interest? None Disclaimer The opinions contained herein are not to be considered
Beyond LDL-Cholesterol
 Biomarkers for Risk Stratification Beyond LDL-Cholesterol Athanasios J.Manolis Director Cardioilogy Dep, Asklepeion Hospital, Athens, Greece Adj. Professor of Medicine, Emory University Atlanta, USA Adj.
Biomarkers for Risk Stratification Beyond LDL-Cholesterol Athanasios J.Manolis Director Cardioilogy Dep, Asklepeion Hospital, Athens, Greece Adj. Professor of Medicine, Emory University Atlanta, USA Adj.
How Low Do We Go? Update on Hypertension
 How Low Do We Go? Update on Beth L. Abramson, MD, FRCPC, FACC As presented at the University of Toronto s Saturday at the University Session (September 2003) Arecent World Health Organization report states
How Low Do We Go? Update on Beth L. Abramson, MD, FRCPC, FACC As presented at the University of Toronto s Saturday at the University Session (September 2003) Arecent World Health Organization report states
None. Disclosure: Relationships with Industry Conflicts of Interests. Learning Objectives: Participants will be able to:
 2014 Evidence-Based Guideline for the Management of High Blood Pressure in Adults: Report from the Panel Members Appointed to the Eighth Joint National Committee (JNC 8) James W. Shaw, MD Memorial Lecture
2014 Evidence-Based Guideline for the Management of High Blood Pressure in Adults: Report from the Panel Members Appointed to the Eighth Joint National Committee (JNC 8) James W. Shaw, MD Memorial Lecture
Int. J. Pharm. Sci. Rev. Res., 36(1), January February 2016; Article No. 06, Pages: JNC 8 versus JNC 7 Understanding the Evidences
, January February 2016; Article No. 06, Pages: JNC 8 versus JNC 7 Understanding the Evidences") Research Article JNC 8 versus JNC 7 Understanding the Evidences Anns Clara Joseph, Karthik MS, Sivasakthi R, Venkatanarayanan R, Sam Johnson Udaya Chander J* RVS College of Pharmaceutical Sciences, Coimbatore,
Research Article JNC 8 versus JNC 7 Understanding the Evidences Anns Clara Joseph, Karthik MS, Sivasakthi R, Venkatanarayanan R, Sam Johnson Udaya Chander J* RVS College of Pharmaceutical Sciences, Coimbatore,
Factors Involved in Poor Control of Risk Factors
 Factors Involved in Poor Control of Risk Factors Patient compliance Clinical inertia Health Care System structure 14781 M Limitations of Formal Studies Selection of patients Recruitment and follow-up alter
Factors Involved in Poor Control of Risk Factors Patient compliance Clinical inertia Health Care System structure 14781 M Limitations of Formal Studies Selection of patients Recruitment and follow-up alter
Should we prescribe aspirin and statins to all subjects over 65? (Or even all over 55?) Terje R.Pedersen Oslo University Hospital Oslo, Norway
 Terje R.Pedersen Oslo University Hospital Oslo, Norway") Should we prescribe aspirin and statins to all subjects over 65? (Or even all over 55?) Terje R.Pedersen Oslo University Hospital Oslo, Norway The Polypill A strategy to reduce cardiovascular disease by
Should we prescribe aspirin and statins to all subjects over 65? (Or even all over 55?) Terje R.Pedersen Oslo University Hospital Oslo, Norway The Polypill A strategy to reduce cardiovascular disease by
Hypertension Management in Diabetic Patients
 Hypertension Management in Diabetic Patients Park, Chang G, MD, PhD Cardiovascular Center, Guro Hospital, Korea University Medical School Contents (Treatment of 2 Cases) Type 2 Diabetes Mellitus Hypertension
Hypertension Management in Diabetic Patients Park, Chang G, MD, PhD Cardiovascular Center, Guro Hospital, Korea University Medical School Contents (Treatment of 2 Cases) Type 2 Diabetes Mellitus Hypertension
Ferrari R, Fox K, Bertrand M, Mourad J.J, Akkerhuis KM, Van Vark L, Boersma E.
 Effect of angiotensin-converting enzyme inhibitors and angiotensin II receptor blockers on cardiovascular mortality in hypertension: a meta-analysis of randomized controlled trials Ferrari R, Fox K, Bertrand
Effect of angiotensin-converting enzyme inhibitors and angiotensin II receptor blockers on cardiovascular mortality in hypertension: a meta-analysis of randomized controlled trials Ferrari R, Fox K, Bertrand
The Road to Renin System Optimization: Renin Inhibitor
 The Road to Renin System Optimization: Renin Inhibitor A New Perspective on the Renin-Angiotensin System (RAS) Yong-Jin Kim, MD Seoul National University Hospital Human and Economic Costs of Hypertension
The Road to Renin System Optimization: Renin Inhibitor A New Perspective on the Renin-Angiotensin System (RAS) Yong-Jin Kim, MD Seoul National University Hospital Human and Economic Costs of Hypertension
DISCLOSURES OUTLINE OUTLINE 9/29/2014 ANTI-HYPERTENSIVE MANAGEMENT OF CHRONIC KIDNEY DISEASE
 ANTI-HYPERTENSIVE MANAGEMENT OF CHRONIC KIDNEY DISEASE DISCLOSURES Editor-in-Chief- Nephrology- UpToDate- (Wolters Klewer) Richard J. Glassock, MD, MACP Geffen School of Medicine at UCLA 1 st Annual Internal
ANTI-HYPERTENSIVE MANAGEMENT OF CHRONIC KIDNEY DISEASE DISCLOSURES Editor-in-Chief- Nephrology- UpToDate- (Wolters Klewer) Richard J. Glassock, MD, MACP Geffen School of Medicine at UCLA 1 st Annual Internal
Management of Hypertension. M Misra MD MRCP (UK) Division of Nephrology University of Missouri School of Medicine
 Division of Nephrology University of Missouri School of Medicine") Management of Hypertension M Misra MD MRCP (UK) Division of Nephrology University of Missouri School of Medicine Disturbing Trends in Hypertension HTN awareness, treatment and control rates are decreasing
Management of Hypertension M Misra MD MRCP (UK) Division of Nephrology University of Missouri School of Medicine Disturbing Trends in Hypertension HTN awareness, treatment and control rates are decreasing
Using the New Hypertension Guidelines
 Using the New Hypertension Guidelines Kamal Henderson, MD Department of Cardiology, Preventive Medicine, University of North Carolina School of Medicine Kotchen TA. Historical trends and milestones in
Using the New Hypertension Guidelines Kamal Henderson, MD Department of Cardiology, Preventive Medicine, University of North Carolina School of Medicine Kotchen TA. Historical trends and milestones in
Management of Hypertension in Women
 Management of Hypertension in Women Eliseo J. Pérez-Stable MD Professor of Medicine DGIM, Department of Medicine July 1, 2013 Declaration of full disclosure: No conflict of interest (I have never been
Management of Hypertension in Women Eliseo J. Pérez-Stable MD Professor of Medicine DGIM, Department of Medicine July 1, 2013 Declaration of full disclosure: No conflict of interest (I have never been
JNC 8 -Controversies. Sagren Naidoo Nephrologist CMJAH
 JNC 8 -Controversies Sagren Naidoo Nephrologist CMJAH Joint National Committee (JNC) Panel appointed by the National Heart, Lung, and Blood Institute (NHLBI) First guidelines (JNC-1) published in 1977
JNC 8 -Controversies Sagren Naidoo Nephrologist CMJAH Joint National Committee (JNC) Panel appointed by the National Heart, Lung, and Blood Institute (NHLBI) First guidelines (JNC-1) published in 1977
The Indian Polycap Study 1 & 2 (TIPS 1 & 2) and The International Polycap Study 3 & 4 (TIPS 3 & 4)
 and The International Polycap Study 3 & 4 (TIPS 3 & 4)") The Indian Polycap Study 1 & 2 (TIPS 1 & 2) and The International Polycap Study 3 & 4 (TIPS 3 & 4) Denis Xavier MD, MSc Professor and Head, Pharmacology, St. John's Medical College Coordinator, Division
The Indian Polycap Study 1 & 2 (TIPS 1 & 2) and The International Polycap Study 3 & 4 (TIPS 3 & 4) Denis Xavier MD, MSc Professor and Head, Pharmacology, St. John's Medical College Coordinator, Division
Hypertension in the Elderly. John Puxty Division of Geriatrics Center for Studies in Aging and Health, Providence Care
 Hypertension in the Elderly John Puxty Division of Geriatrics Center for Studies in Aging and Health, Providence Care Learning Objectives Review evidence for treatment of hypertension in elderly Consider
Hypertension in the Elderly John Puxty Division of Geriatrics Center for Studies in Aging and Health, Providence Care Learning Objectives Review evidence for treatment of hypertension in elderly Consider
Managing HTN in the Elderly: How Low to Go
 Managing HTN in the Elderly: How Low to Go Laxmi S. Mehta, MD, FACC The Ohio State University Medical Center Assistant Professor of Clinical Internal Medicine Clinical Director of the Women s Cardiovascular
Managing HTN in the Elderly: How Low to Go Laxmi S. Mehta, MD, FACC The Ohio State University Medical Center Assistant Professor of Clinical Internal Medicine Clinical Director of the Women s Cardiovascular
Hypertension Management Focus on new RAAS blocker. Disclosure
 Hypertension Management Focus on new RAAS blocker Rameshkumar Raman M.D Endocrine Associates of The Quad Cities Disclosure Speaker bureau Abbott, Eli Lilly, Novo Nordisk, Novartis, Takeda, Merck, Solvay
Hypertension Management Focus on new RAAS blocker Rameshkumar Raman M.D Endocrine Associates of The Quad Cities Disclosure Speaker bureau Abbott, Eli Lilly, Novo Nordisk, Novartis, Takeda, Merck, Solvay
American Diabetes Association 2018 Guidelines Important Notable Points
 American Diabetes Association 2018 Guidelines Important Notable Points The Standards of Medical Care in Diabetes-2018 by ADA include the most current evidencebased recommendations for diagnosing and treating
American Diabetes Association 2018 Guidelines Important Notable Points The Standards of Medical Care in Diabetes-2018 by ADA include the most current evidencebased recommendations for diagnosing and treating
Individual management of arterial hypertension. Doumas Michael, Internist Lecturer, Aristotle University, Thessaloniki
 Individual management of arterial hypertension Doumas Michael, Internist Lecturer, Aristotle University, Thessaloniki From Population to Individual Management of Arterial Hypertension Epidemiologic impact
Individual management of arterial hypertension Doumas Michael, Internist Lecturer, Aristotle University, Thessaloniki From Population to Individual Management of Arterial Hypertension Epidemiologic impact
Metoprolol Succinate SelokenZOC
 Metoprolol Succinate SelokenZOC Blood Pressure Control and Far Beyond Mohamed Abdel Ghany World Health Organization - Noncommunicable Diseases (NCD) Country Profiles, 2014. 1 Death Rates From Ischemic
Metoprolol Succinate SelokenZOC Blood Pressure Control and Far Beyond Mohamed Abdel Ghany World Health Organization - Noncommunicable Diseases (NCD) Country Profiles, 2014. 1 Death Rates From Ischemic
Identification of patients with heart failure and PREserved systolic Function : an Epidemiologic Regional study
 Identification of patients with heart failure and PREserved systolic Function : an Epidemiologic Regional study Dr. Antonio Magaña M.D. (on behalf I-PREFER investigators group) Stockholm, Sweden, August
Identification of patients with heart failure and PREserved systolic Function : an Epidemiologic Regional study Dr. Antonio Magaña M.D. (on behalf I-PREFER investigators group) Stockholm, Sweden, August
How to Reduce CVD Complications in Diabetes?
 How to Reduce CVD Complications in Diabetes? Chaicharn Deerochanawong M.D. Diabetes and Endocrinology Unit Department of Medicine Rajavithi Hospital, Ministry of Public Health Framingham Heart Study 30-Year
How to Reduce CVD Complications in Diabetes? Chaicharn Deerochanawong M.D. Diabetes and Endocrinology Unit Department of Medicine Rajavithi Hospital, Ministry of Public Health Framingham Heart Study 30-Year
Chapter 2 - Cardiovascular System. Primary Care Prescribing Formulary - Preferred Drug Choices
 Chapter 2 - Cardiovascular System Primary Care Prescribing Formulary - Preferred Drug Choices Drug group Drug choice Comments/notes Cardiac glycosides Thiazide diuretics Loop diuretics Aldosterone antagonist
Chapter 2 - Cardiovascular System Primary Care Prescribing Formulary - Preferred Drug Choices Drug group Drug choice Comments/notes Cardiac glycosides Thiazide diuretics Loop diuretics Aldosterone antagonist
ATP IV: Predicting Guideline Updates
 Disclosures ATP IV: Predicting Guideline Updates Daniel M. Riche, Pharm.D., BCPS, CDE Speaker s Bureau Merck Janssen Boehringer-Ingelheim Learning Objectives Describe at least two evidence-based recommendations
Disclosures ATP IV: Predicting Guideline Updates Daniel M. Riche, Pharm.D., BCPS, CDE Speaker s Bureau Merck Janssen Boehringer-Ingelheim Learning Objectives Describe at least two evidence-based recommendations
APPENDIX D: PHARMACOTYHERAPY EVIDENCE
 Página 1 de 7 APPENDIX D: PHARMACOTYHERAPY EVIDENCE Table D1. Outcome Trials of Antihypertensive Agents Study Drug Regimen N Duration Primary Outcomes Remarks Antihypertensive Therapy vs Placebo SHEP 1991
Página 1 de 7 APPENDIX D: PHARMACOTYHERAPY EVIDENCE Table D1. Outcome Trials of Antihypertensive Agents Study Drug Regimen N Duration Primary Outcomes Remarks Antihypertensive Therapy vs Placebo SHEP 1991
Antihypertensive Trial Design ALLHAT
 1 U.S. Department of Health and Human Services Major Outcomes in High Risk Hypertensive Patients Randomized to Angiotensin-Converting Enzyme Inhibitor or Calcium Channel Blocker vs Diuretic National Institutes
1 U.S. Department of Health and Human Services Major Outcomes in High Risk Hypertensive Patients Randomized to Angiotensin-Converting Enzyme Inhibitor or Calcium Channel Blocker vs Diuretic National Institutes
State of the art treatment of hypertension: established and new drugs. Prof. M. Burnier Service of Nephrology and Hypertension Lausanne, Switzerland
 State of the art treatment of hypertension: established and new drugs Prof. M. Burnier Service of Nephrology and Hypertension Lausanne, Switzerland First line therapies in hypertension ACE inhibitors AT
State of the art treatment of hypertension: established and new drugs Prof. M. Burnier Service of Nephrology and Hypertension Lausanne, Switzerland First line therapies in hypertension ACE inhibitors AT
Hypertension Management Controversies in the Elderly Patient
 Hypertension Management Controversies in the Elderly Patient Juan Bowen, MD Geriatric Update for the Primary Care Provider November 17, 2016 2016 MFMER slide-1 Disclosure No financial relationships No
Hypertension Management Controversies in the Elderly Patient Juan Bowen, MD Geriatric Update for the Primary Care Provider November 17, 2016 2016 MFMER slide-1 Disclosure No financial relationships No