Management of The Patients with Hypertension and High Risk Cardiovascular Disease
|
|
|
- Robert Fitzgerald
- 6 years ago
- Views:
Transcription

1 Management of The Patients with Hypertension and High Risk Cardiovascular Disease Songsak Kiatchoosakun, MD. Cardiology, Medicine Khon Kaen University
2 CVD and Hypertension: Worldwide Morbidity and Mortality Cardiovascular disease accounted for 16.6 million deaths in million ischemic heart disease deaths 5.4 million stroke deaths High blood pressure is associated with an estimated 7.1 million deaths Estimated 690 million persons have hypertension; most remain untreated or uncontrolled

3 Hypertension
4 Effect of Systolic BP and Diastolic BP on CHD Mortality CHD Death Rate per 10,000 Person-Years : MRFIT Study (N=316,099)* Diastolic BP (mm Hg) <70 *Men aged years followed for a mean of 12 years. Neaton et al. Arch Intern Med. 1992;152: < Systolic BP (mm Hg)
5 Classification of Hypertension Definitions and Classification of Blood Pressure (BP) Levels (mmhg) ( European Society of Cardiology 2007) Category Systolic Diastolic Optimal <120 and <80 Normal and/or High normal and/or Grade1 hypertension and/or Grade2 hypertension and/or Grade3 hypertension 180 and/or 110 Isolated systolic hypertension 140 and <90
6 Assessment of Patient with HT Establishing blood pressure levels Identifying secondary causes of hypertension Evaluating the overall cardiovascular risk Other risk factors Target organ damage Concomitant diseases

7 Blood Pressure Measurement Sir, your blood pressure is OK.
8 Secondary Cause of Hypertension Sings suggesting secondary hypertension Features of Cushing syndrome Skin stigmata of neurofibromatosis (pheochromocytoma) Palpation of enlarged kidneys (polycystic kidney) Auscultation of abdominal murmurs (renovascular hypertension) Diminished and delayed femoral pulses and reduced femoral BP (aortic coarctation, aortic disease)
9 Total Cardiovascular Risk Concepts Small number of patients have hypertension alone Blood pressure and metabolic risk factors potential each other and leading to greater cardiovascular risk Goals for treatment and treatment strategies are different between high risk and low risk patients
10 Patients With Hypertension Are Likely To Have Additional CV Risk Factors Men Women 3 RFs 22% 4+ RFs 8% 4+ RFs None None 12% 19% 17% 2 RFs 25% 1 RF 26% 3 RFs 20% 2 RFs 24% 1 RF 27% Kannel WB. Am J Hypertens. 2000;13:3S-10S.
 X1.")
, SBP 120 mm Hg, and no glucose intolerance, who is ECG-LVH negative and whose probability of developing CVD is 15/1000 (1.")
11 The Threat of Global CV Risk Dyslipidemia Hypertension TC 5.4 mmol/l X2.6 SBP 165 mm Hg (210 mg/dl) X1.9 X4.5 X1.3 X3.5 X2.3 Glucose intolerance X1.8 Hypertension SBP 195 mm Hg X3.0 X5.3 X8.7 X5.2 X2.9 Smoking X1.7 Dyslipidemia TC 6.1 mmol/l (235 mg/dl) X1.7 Risk shown above is compared with risk for a 40-year-old male nonsmoker with TC 4.7 mmol/l (185 mg/dl), SBP 120 mm Hg, and no glucose intolerance, who is ECG-LVH negative and whose probability of developing CVD is 15/1000 (1.5%) in 8 years Kannel W. In: Hypertension: Pathophysiology and Treatment. New York: McGraw-Hill, Inc.; 1977:
12 Factors Influencing Prognosis (1) Risk factors Systolic and diastolic BP levels and pulse pressure (in elderly) Age (M > 55 years; W > 65 years) Smoking Dyslipidemia - TC > 5.0 mmol/l (190 mg/dl) or: - LDL C >3.0 mmol/l (115 mg/dl) or: - HDL C: M < 1.0 mmol/l (40 mg/dl), W <1.2 mmol/l (46 mg/dl) or: - TG > 1.7 mmol/l (150 mg /dl) Fasting plasma glucose mmol/l ( mg /dl) Abdominal obesity (waist circumference > 102 cm (M), >88 cm (W) Family history of premature CV disease (M at age <55 years; W at age <65 years)
13 Factors Influencing Prognosis (2) Sub-clinical organ damage LVH by ECG or Echocardiography (LVMI M > 125 g/m 2, w > 110 g/m 2 ) Carotid wall thickening (IMT > 0.9 mm) or plaque Ankle/brachial BP index <0.9 Slight increase in plasma creatinine: M: umol/l ( mg/dl) W: umol/l ( mg/dl) Low estimated glomerular filtration rate + (60 ml/min/1.73 m 2 ) or creatinine clearance (< 60 ml/min) Microalbuminuria mg/ 24 h or albumin creatinine ratio: > 22 (M); or > 31 (W) mg/g creatinine Rike maximal for concentric LVH (left ventricular hypertrophy): increased LVMI (left ventricular mass index) with a wall thick ness/ radius ratio > 0.42.
14 Factors Influencing Prognosis (3) Established CV or Renal Disease Cerebrovascular disease Heart disease: CAD, CHF Renal disease: diabetic nephropathy; renal impairmant (creatinine;m > 133, W > 1 24 mmol/l); proteinuria (> 300 mg/24 h) Peripheral artery disease Advanced retinnopathy: haemorrhages or exudates, papilledema
15 Diagnostic Evaluation

16 Blood Test FBS Lipid panel Renal function Electrolyte

17 Waist Circumference
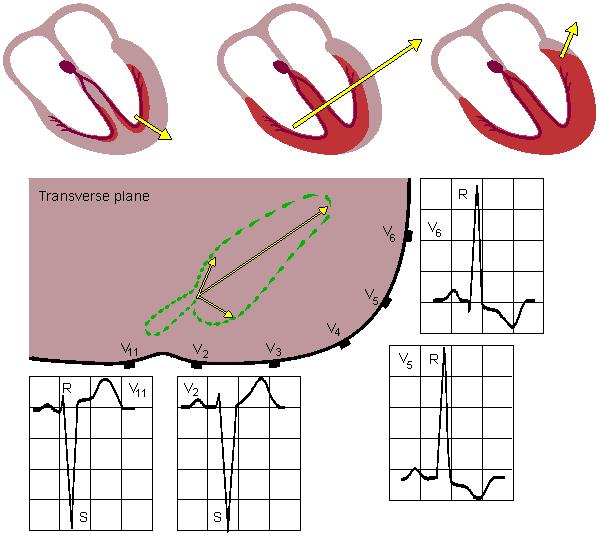
18 Electrocardiography
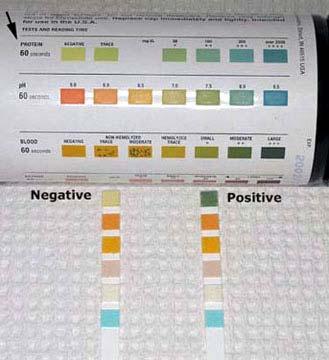
19 Proteinuria
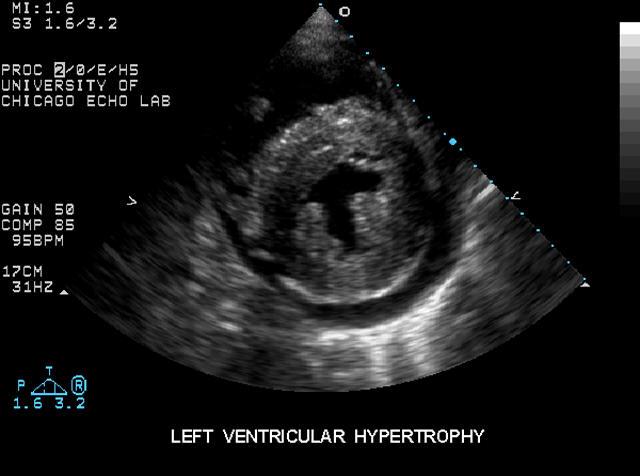
20 Echocardiography: LV Hypertrophy

21 Carotid Plaque
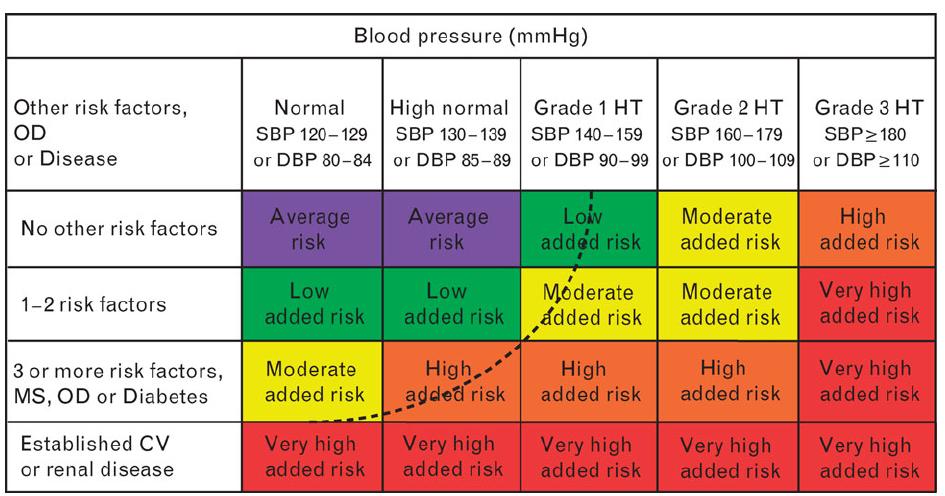
22 Total Cardiovascular Risk
23 High/Very High Risk Subjects BP > 180 mmhg systolic and/or > 110 mmhg diastolic Systolic BP > 160 mmhg with low diastolic BP ( < 70 mmhg) Diabetes mellitus Metabolic syndrome > 3 cardiovascular risk factors One or more of the following sub-clinical organ damages: - LV hypertrophy - Carotid plaque detected by ultrasound - Renal impairment/micro-albuminuria or proteinuria Established cardiovascular or renal disease
24 Goals of Treatment Primary goal is to achieve maximum reduction in the long term total risk of cardiovascular disease BP should be reduce to at least below 140/90 mmhg Target BP should be at least <130/80 mmhg in diabetics and in high or very high risk patients such as stroke, myocardial infarction, renal dysfunction, proteinuria In order to more easily achieve goal BP, antihypertensive treatment should be initiated before significant cardiovascular damage develops
25 Treatment Strategies Lifestyle changes Smoking cessation Moderation of alcohol consumption Sodium restriction Other dietary changes Weight reduction Physical exercise
26 Antihypertensive Therapy Five major classes Diuretics Beta-blocker ACE inhibition Angiotensin receptor antagonist Calcium antagonist
27 Effect of Antihypertensive Therapy 0 10 Cerebrovascular Disease Coronary Heart Disease 16% % Reduction % Systematic overviews showed that reductions in blood pressure of about mm Hg systolic and 5-6 mm Hg diastolic conferred relative reductionsinstrokeriskof38%andinriskof coronary heart disease of 16% within just a few years of beginning treatment. MacMahon SW et al. Prog Cardiovasc Dis. 1986;29(suppl 1):


28 Clinical Research Questions in Hypertension Is blood pressure lowering beneficial? Does it matter how elevated blood pressure is lowered?

29
30 Hypertension Treatment Significantly Reduced Mortality and Morbidity VA Cooperative Study Group Estimated Cumulative Incidence of All Morbid Events Over 5 Years Estimated Cumulative Incidence of All Morbid Events (%) Control - Placebo 380 male patients diastolic blood pressure (BP) averaging mmhg Years Active Treatment Groups - Diuretic-based regimen and hydralazine 37% risk reduction Veterans Administration Cooperative Study Group on antihypertensive agents JAMA 1970;213(7):
31 SHEP Trial: Endpoints Active Therapy (diuretic, beta-blocker vs Placebo) Relative Risk (95% CI) % -25% -37% -32% P=NS -54% Stroke CHD CHF CVD Death SHEP Cooperative Research Group. JAMA. 1991;265:3255; Kostis et al. JAMA. 1997;278:
32 Beta-blockers and Diuretic Lower Risk of Cardiovascular Mortality In hypertension, beta blockers and diuretics have proven risk reduction in cardiovascular morbidity and mortality vs. placebo (STOP, HEP, MRC) Hypertension guidelines recommend beta blockers or diuretics as one of the initial treatments for hypertension JNC-VII Guideline
33 Diuretic / Beta-blocker The benefits of diuretic therapy on coronary artery disease were less than than expected Metabolic side effects of diuretic/betablocker mitigated the beneficial effect of blood pressure reduction The beneficial effect of new treatment may beyond the blood pressure lowering effect

34 Renin-Angiotensin-Aldosterone (RAAS) and Hypertension Renin Angiotensin Converting Enzyme Angiotensinogen Angiotensin I Angiotensin II AT I receptor Vasoconstriction Sodium Retention Increase blood pressure
35 Manipulation of Ang II generation Angiotensinogen (Liver) Bradykinin ACEinhibitor Peptides Angiotensin I Angiotensin II AT 1 AT 2 de Gasparo et al. Pharmacol Rev. 2000; 52: 415
36 ACE Inhibition Blood pressure lowering Beyond blood pressure Anti-atherosclerotic effects Improvement in vascular endothelial function LV hypertrophy reduction Reduce new onset of diabetes Reduce cardiovascular complications of hypertension
37 The Heart Outcomes Prevention Evaluation Study: HOPE Study Aim: Effect of Ramipril (up to 10mg/d) vs placebo on CV death, MI or stroke (primary) Design:Randomized double blind, Wide entry criteria, large, simple trial Size: 9541 patients followed for 4 to 6 years Heart Outcomes Prevention Evaluation Study Investigators. N Engl J Med 2000;342:145.
38 HOPE Study Population: Typical Office Practice Patients Patients did not have clinical of heart failure 47% of had high blood pressure Patients were 55 years or older CV events 11% had previous stroke 52% had previous MI Vascular disease 80% had history of CAD 42% had history of PVD Diabetes 39% had diabetes + 1 or more CVD risk factors The HOPE Study Investigators. N Engl J Med. 2000;342:
39 HOPE: Primary Outcome Reductions in MI, Stroke, or Cardiovascular Death % of Patients Reaching Endpoints % Reduction in Events P=.0001* 15% Reduction in Events at 1 year Placebo Ramipril Days of Follow-up Note: Trial halted early due to the highly significant risk reductions seen with Ramipril
40 HOPE Study: Results (contd.) CV death MI Stroke Revasc Cardiac arrest Heart failure Total mortality Type 2 diabetes % -20% -32% -15% -37% -23% -16% -34% N Engl J Med 2000; 342: % risk reduction
41 HOPE: Dose-dependent Effects of Ramipril on LV Mass and Function Mean baseline LVEF 58% in all groups Placebo (n = 151) Ramipril 2.5 mg (n = 149) Ramipril 10 mg (n = 146) LV mass (g) LV 4 6 end 3 4 systolic 2 2 volume 1 (ml) P Trend = 0.03 P Trend = Lonn E et al. J Am Coll Cardiol. 2004;43:
42 HOPE:Conclusions In people with high risk for CVD, addition of ramipril to other effective therapies prevents: CV death, strokes and MI Total mortality Revascularization The benefit is beyond the effect on BP (3/2 mmhg)
43 HOPE-TOO: Primary Outcome (CV death, MI, Stroke) Primary outcome (% HOPE-TOO patients) Placebo Main HOPE study ends Ramipril HOPE-TOO begins RRR = 17% P = n Placebo Ramipril Years RRR = relative risk reduction HOPE/HOPE-TOO Study Investigators. Circulation. 2005;112:
44 HOPE-TOO: Additional Reduction in New-onset Diabetes Main HOPE study ends HOPE-TOO begins New-onset diabetes (% HOPE-TOO patients) Placebo Ramipril RRR 31% P = n Placebo Ramipril Years HOPE/HOPE-TOO Study Investigators. Circulation. 2005;112:
45 SECURE: Dose-dependent Effect of Ramipril on Carotid Atherosclerosis P = NS Slope of the mean maximum carotid-intima thickness (mm/y) % Reduction Placebo Ramipril 2.5 mg Ramipril 10 mg Lonn E et al. Circulation. 2001;103:



46 ACE Inhibitor Evidence: Post MI with HF SAVE Radionuclide EF < 40% AIRE Clinical and/or radiographic signs of HF TRACE Echocardiogram EF < 35% Probability of Event Placebo ACE-I Years OR: 0.74 ( ) 26 % reduction 4 ACE-I=Angiotensin converting enzyme inhibitors, LVSD=Left ventricular systolic dysfunction, MI=Myocardial infarction, OR=Odds ratio Flather MD, et al. Lancet. 2000;355:
47 Blood Pressure Lowering Treatment Trialists Collaboration. Lancet 2000;356:1955 Comparison of ACE Inhibitors and Calcium Antagonist Stroke Coronary heart disease Heart failure ACE inhibitors based therapy may reduce risk of CAD and heart failure Total mortality Relative risk Favor ACEI Favor calcium antagonist
48
49 Manipulation of Ang II generation Angiotensinogen (Liver) Angiotensin I ARB AT 1 receptor blocker Angiotensin II AT 1 AT 2 de Gasparo et al. Pharmacol Rev. 2000; 52: 415
50 The Losartan Intervention For Endpoint Reduction in Hypertension Study (LIFE Study) 9,193 hypertensive patients with LVH, aged years Mean 4.8-year follow-up 44,119 patient-years of follow-up 945 study sites in 7 countries Dahlöf B et al Lancet 2002;359:
51 LIFE: Primary Composite Endpoint Number at risk Proportion of patients with first event (%) Composite of CV death, stroke and MI Atenolol Losartan Adjusted Risk Reduction 13.0%, p=0.021 Unadjusted Risk Reduction 14.6%, p= Study Month Losartan (n) Atenolol (n) Dahlöf B et al Lancet 2002;359:
52 Stroke Proportion of patients with first event (%) Fatal and non-fatal stroke Atenolol Losartan Adjusted Risk Reduction 24.9%, p=0.001 Unadjusted Risk Reduction 25.8%, p= % Number at risk Losartan Atenolol Study Month Dahlöf B et al Lancet 2002;359:
53 Proportion of patients with first event (%) LIFE:Myocardial Infarction and Fatal and non-fatal MI Atenolol Losartan 0 Study Month Losartan Atenolol CV Mortality Adjusted RR -7.3%, p=0.491 Unadjusted RR -5.0%, p=0.628 Proportion of patients (%) Cardiovascular mortality Atenolol Losartan Adjusted RR 11.4%, p=0.206 Unadjusted RR 13.3%, p= Study Month Losartan Atenolol Dahlöf B et al Lancet 2002;359:
54 VBWG Results from ASCOT-BPLA: Anglo-Scandinavian Cardiac Outcomes Trial Blood lood Pressure Lowering Arm
55 ASCOT: Anglo-Scandinavian VBWG Cardiac Outcomes Trial Study 1: ASCOT-LLA Double-blind, randomized, placebo-controlled trial of a lipid-lowering agent in a sample of the total ASCOT patient population Study 2: ASCOT-BPLA Prospective, randomized, open, blinded endpoint (PROBE) design comparing two antihypertensive regimens in the total ASCOT patient population Sever PS et al. Lancet. 2003;361: Dahlöf B et al; ASCOT Investigators. Lancet. 2005;366:
56 VBWG ASCOT-BPLA: Study design Design: Population: Treatment: Double-blind, placebo controlled, randomized N = 19,257 with hypertension and 3 other CV risk factors Amlodipine 5 10 mg ± perindopril 4 8 mg prn (n = 9639) Atenolol mg ± bendroflumethiazide mg/potassium prn (n = 9618) Primary outcome: Secondary outcome: Nonfatal MI (including silent MI) and fatal CHD All-cause mortality, stroke, nonfatal MI (excluding silent MI), all coronary events, CV events/procedures, CV mortality, fatal/nonfatal HF
57 ASCOT-BPLA: Reduction in Primary Outcome (nonfatal MI and fatal CHD) 10 VBWG Proportion of events (%) HR = 0.90 (95% CI, ) RRR = 10% P = Time since randomization (years) Number at risk Amlodipine-based regimen (429 events) Atenolol-based regimen (474 events) *Atenolol mg ± bendroflumethiazide mg/potassium prn Amlodipine 5 10 mg ± perindopril 4 8 mg prn Atenolol-based regimen* Amlodipine-based regimen Dahlöf B et al; ASCOT Investigators. Lancet. 2005;366:
58 ASCOT-BPLA: Reduction in Fatal and Proportion of events (%) Nonfatal stroke HR = 0.77 (95% CI, ) RRR = 23% P = Time (years) Number at risk Amlodipine-based regimen (327 events) Atenolol-based regimen (422 events) *Atenolol mg ± bendroflumethiazide mg/potassium prn Amlodipine 5 10 mg ± perindopril 4 8 mg prn 5 Atenolol-based regimen* Amlodipine-based regimen 6 VBWG Dahlöf B et al; ASCOT Investigators. Lancet. 2005;366:
59 ASCOT-BPLA: Overall Results VBWG Study stopped prematurely after 5.5-year median follow-up because of higher death rate in assigned atenolol-based-regimen group Group receiving amlodipine-based regimen had nonsignificant 10% reduction in primary outcome (nonfatal MI plus fatal CHD) and significant reductions in nearly all secondary CV endpoints and new-onset diabetes Dahlöf B et al; ASCOT Investigators. Lancet. 2005;366:
60 ASCOT-BPLA: Summary VBWG Newer antihypertensive drug regimens should be considered in preference to older beta-blocker ± diuretic therapies Amlodipine ± perindopril showed reductions in: Major CV events 16% New-onset diabetes 30% Stroke 23% Mortality 11% ASCOT results support the use of newer drugs, in multi-drug combinations, to modify risk factors and/or metabolic disturbances, especially in patients with complicated hypertension Dahlöf B et al. Lancet. 2005;366: Poulter NR et al. Lancet. 2005;366:
61 New Onset Diabetes: Impact of Blood Pressure Lowering Drugs
62 Cardiovascular Events in Treated Hypertensive Subjects Rate of events (per 100 patient years) A B C A - without diabetes C - previously known diabetes B - new onset diabetes Total number of CV events - 63 Verdecchia, Hypertens 2004;43:
63 Risk of DM among 3804 Hypertensive Patients with Various Antihypertensive Medications Rx Hazard Ratio* None 1.0 ACEI 0.9 B-Blocker 1.25** CCB 1.17 Thiazides 0.95 * adjusted for age, race, BMI, CV risk factors, etc. ** significant difference Gress, et al. NEJM 2000;342:905-12
64 Pharmacological Therapy in Hypertension Choice of antihypertensive drugs The main benefits of antihypertensive therapy are due to lowering blood pressure Beta-blockers especially in combination with thiazide diuretic, should not be used in patients with metabolic syndrome or at high risk of diabetes ESC guideline 2007
65 British Hypertension Society Guideline 2006 Age < 55 Age > 55 or black ACEI or ARB CCB or Diuretic Add CCB Add ACEI or ARB ACEI or ARB + CCB+ Diuretic Add beta-blocker or alpha-blocker
66 Conditions Favoring use of Some Antihypertensive Drugs versus Others Thiazide diuretics Beta-blockers - Isolated systolic HT - Angina pectoris - Heart failure - Post-myocardial infarction - Heart failure - Tachyarrhymias ACE inhibitors Angiotensin receptor antagonists - Heart failure - Heart failure - LV dysfunction - Post-myocardial infarction - Post-myocardial infarction - Diabetic nephropathy - Diabetic nephropathy - Proteinuria - Non-diabetic nephropathy - LV hypertrophy - LV hypertrophy - Atrial fibrillation - Carotid atherosclerosis - Metabolic syndrome - Proteinuria/Microalbuminuria - ACEI-induced cough - Metabolic syndrome
67 Conditions Favoring use of Some Antihypertensive Drugs versus Others Calcium antagonists (dihydropyridines) Calcium antagonists (verapamil/diltiazem) - Isolated systolic hypertension - Angina pectoris (elderly) - Carotid atherosclerosis - Angina pectoris - Supraventricular tachycardia - LV hypertrophy - Carotid/Coronary Atherosclerosis - Pregnancy - Hypertension in blacks Diuretics (anti-aldosterone) Loop diuretics - Heart failure - End stage renal disease - Post-myocardial infarction - Heart failure

68 Thank You for Your Attention

69 VALUE Valsartan Antihypertensive Long-Term Use Evaluation
70 VALUE: Patient Population Treated or untreated hypertensive patients entry criteria for untreated hypertension: mmhg systolic, mmhg diastolic Age 50 years, male or female High-risk for cardiac events one or more defined risk factors or diseases Mann J, Julius S. Blood Press. 1998;7:
71 Proportion of Patients With First Event (%) VALUE: Primary Composite Cardiac Endpoint Valsartan-based regimen Amlodipine-based regimen HR = 1.03; 95% CI = ; P = 0.49 Number at risk Valsartan Time (months) Amlodipine Julius S et al. Lancet. June 2004;363.
72 HOPE (Heart Outcomes Prevention Evaluation) Study Patients > 55 years with a history of - CAD or stroke or peripheral artery disease - Diabetes plus at least one other CV risk factor (hypertension, elevated total cholesterol levels, low HDL levels, cigarette smoking or microalbuminuria) Patients did not have heart failure or LV dysfunction 9297 patients received ramipril or placebo Treatment duration: 4.5 years
73 Dyslipidemia Is More Common in Patients With Hypertension Patients with TC 6.5 mmol/l ( 250 mg/dl) (%) Normal BP High BP Antihypertensive Rx Men Women *Hypertension defined as BP 150/ 95 mm Hg MacMahon M, et al. Arteriosclerosis. 1985;5:
74 Monotherapy versus Combination Mild BP elevation Low/moderate CV risk Conventional BP target Therapy Strategies Choose between Marked BP elevation High/very high CV risk Lower BP target Single agent at low dose If goal BP not achieved Two-drug combination at low dose Previous agent Switch to different agent at full dose at low dose Previous combination Add a third drug at full dose at low dose If goal BP not achieved Two-to three-drug Combination at full dose Full dose Mono-therapy ESC guideline 2007 Two-three drug combination at full dose
75 Possible Combinations Between Some Classes of Antihypertensive Drugs
76 VALUE: Incidence of New-onset Diabetes % Risk Reduction With Valsartan P < New-Onset Diabetes (% of patients in treatment group) % 16.4% 2 0 Valsartan-based Regimen (n = 7649) Amlodipine-based Regimen (n = 7596) Julius S et al. Lancet. June 2004;363.
77 Rationale VBWG Cardiovascular (CV) disease continues to be the chief cause of mortality and morbidity worldwide Most of this is due to coronary heart disease (CHD) Multiple risk factors have synergistic effects in the pathogenesis of CV disease Combination treatment regimens using 2 agents are recommended to reach target BP goals Limited outcome data have led to an investigation comparing standard vs newer antihypertensive treatment options
78 ACE Inhibitor Evidence: CAD European Trial on Reduction of Cardiac Events with Perindopril in Stable Coronary Artery Disease (EUROPA) 13,655 patients with CAD and presumed normal left ventricular function randomized to perindopril (8 mg) or placebo for 4.2 years Cardiovascular death (0.86; ) Non-fatal MI (0.78; ) Cardiac arrest (0.54; ) Combined endpoint (0.80; ) Favors Perindopril Favors Placebo ACE-I=Angiotensin converting enzyme inhibitors, CAD=Coronary artery disease, CV=Cardiovascular, MI=Myocardial infarction EUROPA Investigators. Lancet 2003;362:
79 ACE Inhibitor Evidence: CAD Prevention of Events with Angiotensin Converting Enzyme Inhibition (PEACE) Trial 8,290 patients with stable coronary artery disease and normal left ventricular function randomized to trandolapril (4 mg) or placebo for 4.8 years Primary End Point (%)* Placebo Trandolapril Years After Randomization *Includes death from cardiovascular causes, myocardial infarction, or coronary revascularization PEACE Trial Investigators. NEJM 2004;351:
80 HOPE-TOO: Rationale HOPE-TOO was an extension of the HOPE trial, which examined the effects of ACE inhibition in reducing major CV events in highrisk patients with vascular disease or diabetes HOPE-TOO was designed to assess whether the CV and metabolic benefits of ramipril were sustained over time and occurred in subgroups based on varying risk and concomitant treatment HOPE/HOPE-TOO Study Investigators. Circulation. 2005;112:
81 HOPE-TOO: Study Design Heart Outcomes Prevention Evaluation The Ongoing Outcomes 4528 HOPE patients at 174 centers who agreed to further follow-up Blinded treatment ended and patients were advised to use ACEI 2.6-year post-trial extension ACEI use during extension HOPE ramipril arm (n = 2317): 72% HOPE placebo arm (n = 2211): 68% >90% of all HOPE-TOO patients used ramipril HOPE/HOPE-TOO Study Investigators. Circulation. 2005;112:
82 Major CV Events and New Diagnosis of Diabetes No. of patients (%) Ramipril (n = 3393) Placebo (n = 3393) RR (95% CI) P* MI, stroke, or CV death 699 (20.6) 820 (24.2) 0.83 ( ) MI 485 (14.3) 581 (17.1) 0.81 ( ) Stroke 174 (5.1) 215 (6.3) 0.79 ( ) CV death 327 (9.6) 374 (11.0) 0.86 ( ) Revascularization 767 (22.6) 880 (25.9) 0.84 ( ) New diagnosis of diabetes 152 (7.3) 216 (10.3) 0.69 ( ) *Calculated by log-rank test and data on all participants in the study extension, censored for period of observation HOPE/HOPE-TOO Study Investigators. Circulation. 2005;112:
83 HOPE-TOO: Effect of ACEI on Major CV Events and New-onset Diabetes No. of HOPE patients (%) Event* MI, stroke, or CV death MI Stroke Ramipril (n = 2317) 220 (7.9) 146 (5.1) 59 (2.0) Placebo (n = 2211) 225 (8.4) 169 (6.1) 56 (1.9) CV death 133 (4.4) 126 (4.2) Revascularization New diagnosis of diabetes 235 (9.1) 48 (2.7) 259 (10.5) 70 (4.0) *Event rates were calculated as proportions of events in those study participants who were event-free at the end of the in-trial period RR (95% CI) HOPE/HOPE-TOO Study Investigators. Circulation. 2005;112:
84 HOPE-TOO: Additional Reduction in MI Main HOPE study ends HOPE-TOO begins MI (% HOPE-TOO patients) Placebo 5 Ramipril RRR = 19% P = n Placebo Ramipril Years HOPE/HOPE-TOO Study Investigators. Circulation. 2005;112:
85 HOPE-TOO: Sustained Reduction 10 8 in Stroke Main HOPE study ends HOPE-TOO begins Stroke (% HOPE-TOO patients) 6 4 Placebo 2 Ramipril RRR = 21% P = n Placebo Ramipril Years HOPE/HOPE-TOO Study Investigators. Circulation. 2005;112:
86 HOPE-TOO: Sustained Reduction CV death (% HOPE-TOO patients) in CV Death Placebo Main HOPE study ends HOPE-TOO begins Ramipril RRR = 14% P = n Placebo Ramipril Years HOPE/HOPE-TOO Study Investigators. Circulation. 2005;112:
87 HOPE-TOO: Study Conclusions The benefits of ramipril were maintained during post-trial followup for CV death, stroke, and hospitalization for heart failure Additional reductions in MI, revascularization and new-onset diabetes were also observed despite similar rates of ACEI use in the randomized groups The reduction in CV outcomes demonstrated in the HOPE trial is most likely an underestimate of the full effects of long-term ramipril therapy Subgroup analyses demonstrate the benefits observed are additive to those of other life-saving therapies, and extend to all patients with vascular disease, independent of their baseline risk HOPE/HOPE-TOO Study Investigators. Circulation. 2005;112:
88 Major Clinical Outcome Trials of RAAS Manipulation ACE inhibition Angiotensin receptor blockade HOPE EUROPA ALLHAT ANBP2 INVEST LIFE GISSI-3 ISIS-4 AIRE SAVE SOLVD-Prevention TRACE CHARM-Preserved OPTIMAAL VALIANT CONSENSUS SOLVD-Treat CHARM-Added CHARM-Alternative ELITE II Val-HeFT
")
 Diabetic")

89 ACE Inhibition and Anti- atherosclerotic Effect (A) Control (B) Diabetic apoe-deficient mice (C) Diabetic apoe-deficient mice ACE inhibition treated Candido R et al. Circulation. 2002;106:
90 Algorithm for the Treatment of Hypertension Lifestyle Modifications Not at Goal Blood Pressure (<140/90 mmhg) (<130/80 mmhg for those with diabetes or chronic kidney disease) Initial Drug Choices Without Compelling Indications With Compelling Indications Stage 1 Hypertension (SBP or DBP mmhg) Thiazide-type diuretics for most. May consider ACEI, ARB, BB, CCB, or combination. Stage 2 Hypertension (SBP >160 or DBP >100 mmhg) 2-drug combination for most (usually thiazide-type diuretic and ACEI, or ARB, or BB, or CCB). Drug(s) for the compelling indications* Other antihypertensive drugs (diuretics, ACEI, ARB, BB, CCB) as needed. Not at Goal Blood Pressure Optimize dosages or add additional drugs until goal blood pressure is achieved. Consider consultation with hypertension specialist. *Compelling Indications Heart failure Post-MI High coronary artery disease risk Diabetes Chronic kidney disease Recurrent stroke prevention Chobanian AV et al. JAMA ;289: JNC 7
91 Major Outcomes in High-Risk Hypertensive Patients Randomized to Angiotensin- Converting Enzyme Inhibitor to Calcium Channel Blocker vs Diuretic The Antihypertensive and Lipid-Lowering Treatment to Prevent Heart Attack Trial (ALLHAT)
92 ALLHAT: Entry Criteria Age >55 years old Untreated systolic and/or diastolic hypertension (>140/90 mm Hg but <180/110 mm Hg ) At least 1 additional risk factor for CV morbidity, including: Old MI or stroke History of revascularization Other documented atherosclerosis Type 2 diabetes mellitus Cigarette smoking Low HDL cholesterol(<35mg/dl) LVH Davis et al. Am J Hypertens. 1996;9:
93 Cumulative Event Rates for the Primary Outcome (Fatal CHD or Nonfatal MI) by ALLHAT Treatment Group Cumulative CHD Event Rate A/C L/C RR (95% CI) 0.98 ( ) 0.99 ( ) Chlorthalidone Amlodipine Lisinopril p value Years to CHD Event Number at Risk: Chlorthalidone 15,255 14,477 13,820 13,102 11,362 6,340 2, Amlodipine 9,048 8,576 8,218 7,843 6,824 3,870 1, Lisinopril 9,054 8,535 8,123 7,711 6,662 3,832 1,
94 ACE Inhibitor Recommendations for Secondary Prevention I I IIa IIb III IIa IIb III Use in all patients with LVEF < 40%, and those with diabetes or chronic kidney disease indefinitely, unless contraindicated Consider for all other patients I IIa IIb III Among lower risk patients with normal LVEF where cardiovascular risk factors are well controlled and where revascularization has been performed, their use may be considered optional ACE=Angiotensin converting enzyme, LVEF= left ventricular ejection fraction
95 Hypertension and Dyslipidaemia Are Major Risk Factors for CHD Framingham Study 350 Age 140 Probability of CVD/ SBP (mm Hg) in men Kannel W. In: Hypertension: Pathophysiology and Treatment. New York: McGraw-Hill, Inc.; 1977: ; Castelli WP. Am J Med. 1984;76: Probability of CVD/ < TC (mg/dl) in men >295
96 Additive Effect of Cholesterol and SBP on Risk of CHD Death 34 N = 316,099 Deaths /10,000 patient-years Cholesterol quintile (mg/dl)* < < SBP quintile (mm Hg) Neaton JD, Wentworth D. Arch Intern Med. 1992;152: *To convert to mmol/l multiply by
97 Diuretic Based Regimens Substantially reduce the risk of stroke The benefits of diuretic therapy on coronary artery disease were less than than expected Metabolic side effects of diuretic mitigated the beneficial effect of blood pressure reduction


98 Major Clinical Outcome Trials of RAAS Manipulation ACE inhibition Angiotensin receptor blockade HOPE EUROPA PEACE ALLHAT ANBP2 INVEST LIFE GISSI-3 ISIS-4 AIRE SAVE SOLVD-Prevention TRACE CHARM-Preserved OPTIMAAL VALIANT SOLVD-Treat CHARM-Added CHARM-Alternative ELITE II Val-HeFT CONSENSUS
99 HOPE: Benefits in All Subgroups Younger than 65 years as well as 65 years and older With/without diabetes With/without evidence of cardiovascular disease With/without hypertension With/without microalbuminuria Whether or not taking aspirin or other antiplatelet agents, beta blockers, lipidlowering agents or antihypertensive agents NEJM 2000; 342:
VALUE OF ACEI IN THE MANAGEMENT OF HYPERTENSION
 VALUE OF ACEI IN THE MANAGEMENT OF HYPERTENSION Dr Catherine BESEME Paris 6 th December 2005 6 th International Congress of Bangladesh Society of Medicine Hypertension is a risk factor at the source, with
VALUE OF ACEI IN THE MANAGEMENT OF HYPERTENSION Dr Catherine BESEME Paris 6 th December 2005 6 th International Congress of Bangladesh Society of Medicine Hypertension is a risk factor at the source, with
Antihypertensive Trial Design ALLHAT
 1 U.S. Department of Health and Human Services Major Outcomes in High Risk Hypertensive Patients Randomized to Angiotensin-Converting Enzyme Inhibitor or Calcium Channel Blocker vs Diuretic National Institutes
1 U.S. Department of Health and Human Services Major Outcomes in High Risk Hypertensive Patients Randomized to Angiotensin-Converting Enzyme Inhibitor or Calcium Channel Blocker vs Diuretic National Institutes
Is there a mechanism of interaction between hypertension and dyslipidaemia?
 Is there a mechanism of interaction between hypertension and dyslipidaemia? Neil R Poulter International Centre for Circulatory Health NHLI, Imperial College London Daegu, Korea April 2005 Observational
Is there a mechanism of interaction between hypertension and dyslipidaemia? Neil R Poulter International Centre for Circulatory Health NHLI, Imperial College London Daegu, Korea April 2005 Observational
ΑΡΥΙΚΗ ΠΡΟΔΓΓΙΗ ΤΠΔΡΣΑΙΚΟΤ ΑΘΔΝΟΤ. Μ.Β.Παπαβαζιλείοσ Καρδιολόγος FESC - Γιεσθύνηρια ιζμανόγλειον ΓΝΑ Clinical Hypertension Specialist ESH
 ΑΡΥΙΚΗ ΠΡΟΔΓΓΙΗ ΤΠΔΡΣΑΙΚΟΤ ΑΘΔΝΟΤ Μ.Β.Παπαβαζιλείοσ Καρδιολόγος FESC - Γιεσθύνηρια ιζμανόγλειον ΓΝΑ Clinical Hypertension Specialist ESH Hypertension Co-Morbidities HTN Commonly Clusters with Other Risk
ΑΡΥΙΚΗ ΠΡΟΔΓΓΙΗ ΤΠΔΡΣΑΙΚΟΤ ΑΘΔΝΟΤ Μ.Β.Παπαβαζιλείοσ Καρδιολόγος FESC - Γιεσθύνηρια ιζμανόγλειον ΓΝΑ Clinical Hypertension Specialist ESH Hypertension Co-Morbidities HTN Commonly Clusters with Other Risk
ALLHAT. Major Outcomes in High Risk Hypertensive Patients Randomized to Angiotensin-Converting Enzyme Inhibitor or Calcium Channel Blocker vs Diuretic
 1 U.S. Department of Health and Human Services National Institutes of Health Major Outcomes in High Risk Hypertensive Patients Randomized to Angiotensin-Converting Enzyme Inhibitor or Calcium Channel Blocker
1 U.S. Department of Health and Human Services National Institutes of Health Major Outcomes in High Risk Hypertensive Patients Randomized to Angiotensin-Converting Enzyme Inhibitor or Calcium Channel Blocker
VA/DoD Clinical Practice Guideline for the Diagnosis and Management of Hypertension - Pocket Guide Update 2004 Revision July 2005
 VA/DoD Clinical Practice Guideline for the Diagnosis and Management of Hypertension - Pocket Guide Update 2004 Revision July 2005 1 Any adult in the health care system 2 Obtain blood pressure (BP) (Reliable,
VA/DoD Clinical Practice Guideline for the Diagnosis and Management of Hypertension - Pocket Guide Update 2004 Revision July 2005 1 Any adult in the health care system 2 Obtain blood pressure (BP) (Reliable,
Management of Hypertension
 Clinical Practice Guidelines Management of Hypertension Definition and classification of blood pressure levels (mmhg) Category Systolic Diastolic Normal
Clinical Practice Guidelines Management of Hypertension Definition and classification of blood pressure levels (mmhg) Category Systolic Diastolic Normal
Hypertension Update Clinical Controversies Regarding Age and Race
 Hypertension Update Clinical Controversies Regarding Age and Race Allison Helmer, PharmD, BCACP Assistant Clinical Professor Auburn University Harrison School of Pharmacy July 22, 2017 DISCLOSURE/CONFLICT
Hypertension Update Clinical Controversies Regarding Age and Race Allison Helmer, PharmD, BCACP Assistant Clinical Professor Auburn University Harrison School of Pharmacy July 22, 2017 DISCLOSURE/CONFLICT
In the Literature 1001 BP of 1.1 mm Hg). The trial was stopped early based on prespecified stopping rules because of a significant difference in cardi
. The trial was stopped early based on prespecified stopping rules because of a significant difference in cardi") Is Choice of Antihypertensive Agent Important in Improving Cardiovascular Outcomes in High-Risk Hypertensive Patients? Commentary on Jamerson K, Weber MA, Bakris GL, et al; ACCOMPLISH Trial Investigators.
Is Choice of Antihypertensive Agent Important in Improving Cardiovascular Outcomes in High-Risk Hypertensive Patients? Commentary on Jamerson K, Weber MA, Bakris GL, et al; ACCOMPLISH Trial Investigators.
HYPERTENSION GUIDELINES WHERE ARE WE IN 2014
 HYPERTENSION GUIDELINES WHERE ARE WE IN 2014 Donald J. DiPette MD FACP Special Assistant to the Provost for Health Affairs Distinguished Health Sciences Professor University of South Carolina University
HYPERTENSION GUIDELINES WHERE ARE WE IN 2014 Donald J. DiPette MD FACP Special Assistant to the Provost for Health Affairs Distinguished Health Sciences Professor University of South Carolina University
Hypertension Update 2009
 Hypertension Update 2009 New Drugs, New Goals, New Approaches, New Lessons from Clinical Trials Timothy C Fagan, MD, FACP Professor Emeritus University of Arizona New Drugs Direct Renin Inhibitors Endothelin
Hypertension Update 2009 New Drugs, New Goals, New Approaches, New Lessons from Clinical Trials Timothy C Fagan, MD, FACP Professor Emeritus University of Arizona New Drugs Direct Renin Inhibitors Endothelin
Hypertension Guidelines: Are We Pressured to Change? Oregon Cardiovascular Symposium Portland, Oregon June 6, Financial Disclosures
 Hypertension Guidelines: Are We Pressured to Change? Oregon Cardiovascular Symposium Portland, Oregon June 6, 2015 William C. Cushman, MD Professor, Preventive Medicine, Medicine, and Physiology University
Hypertension Guidelines: Are We Pressured to Change? Oregon Cardiovascular Symposium Portland, Oregon June 6, 2015 William C. Cushman, MD Professor, Preventive Medicine, Medicine, and Physiology University
JNC 8 -Controversies. Sagren Naidoo Nephrologist CMJAH
 JNC 8 -Controversies Sagren Naidoo Nephrologist CMJAH Joint National Committee (JNC) Panel appointed by the National Heart, Lung, and Blood Institute (NHLBI) First guidelines (JNC-1) published in 1977
JNC 8 -Controversies Sagren Naidoo Nephrologist CMJAH Joint National Committee (JNC) Panel appointed by the National Heart, Lung, and Blood Institute (NHLBI) First guidelines (JNC-1) published in 1977
Outcomes and Perspectives of Single-Pill Combination Therapy for the modern management of hypertension
 Outcomes and Perspectives of Single-Pill Combination Therapy for the modern management of hypertension Prof. Massimo Volpe, MD, FAHA, FESC, Chair of Cardiology, Department of Clinical and Molecular Medicine
Outcomes and Perspectives of Single-Pill Combination Therapy for the modern management of hypertension Prof. Massimo Volpe, MD, FAHA, FESC, Chair of Cardiology, Department of Clinical and Molecular Medicine
The Road to Renin System Optimization: Renin Inhibitor
 The Road to Renin System Optimization: Renin Inhibitor A New Perspective on the Renin-Angiotensin System (RAS) Yong-Jin Kim, MD Seoul National University Hospital Human and Economic Costs of Hypertension
The Road to Renin System Optimization: Renin Inhibitor A New Perspective on the Renin-Angiotensin System (RAS) Yong-Jin Kim, MD Seoul National University Hospital Human and Economic Costs of Hypertension
Hypertension. Does it Matter What Medications We Use? Nishant K. Sekaran, M.D. M.Sc. Intermountain Heart Institute
 Hypertension Does it Matter What Medications We Use? Nishant K. Sekaran, M.D. M.Sc. Intermountain Heart Institute Hypertension 2017 Classification BP Category Systolic Diastolic Normal 120 and 80 Elevated
Hypertension Does it Matter What Medications We Use? Nishant K. Sekaran, M.D. M.Sc. Intermountain Heart Institute Hypertension 2017 Classification BP Category Systolic Diastolic Normal 120 and 80 Elevated
ALLHAT Role of Diuretics in the Prevention of Heart Failure - The Antihypertensive and Lipid- Lowering Treatment to Prevent Heart Attack Trial
 1 ALLHAT Role of Diuretics in the Prevention of Heart Failure - The Antihypertensive and Lipid- Lowering Treatment to Prevent Heart Attack Trial Davis BR, Piller LB, Cutler JA, et al. Circulation 2006.113:2201-2210.
1 ALLHAT Role of Diuretics in the Prevention of Heart Failure - The Antihypertensive and Lipid- Lowering Treatment to Prevent Heart Attack Trial Davis BR, Piller LB, Cutler JA, et al. Circulation 2006.113:2201-2210.
T. Suithichaiyakul Cardiomed Chula
 T. Suithichaiyakul Cardiomed Chula The cardiovascular (CV) continuum: role of risk factors Endothelial Dysfunction Atherosclerosis and left ventricular hypertrophy Myocardial infarction & stroke Endothelial
T. Suithichaiyakul Cardiomed Chula The cardiovascular (CV) continuum: role of risk factors Endothelial Dysfunction Atherosclerosis and left ventricular hypertrophy Myocardial infarction & stroke Endothelial
Hypertension Management Focus on new RAAS blocker. Disclosure
 Hypertension Management Focus on new RAAS blocker Rameshkumar Raman M.D Endocrine Associates of The Quad Cities Disclosure Speaker bureau Abbott, Eli Lilly, Novo Nordisk, Novartis, Takeda, Merck, Solvay
Hypertension Management Focus on new RAAS blocker Rameshkumar Raman M.D Endocrine Associates of The Quad Cities Disclosure Speaker bureau Abbott, Eli Lilly, Novo Nordisk, Novartis, Takeda, Merck, Solvay
How would you manage Ms. Gold
 How would you manage Ms. Gold 32 yo Asian woman with dyslipidemia Current medications: Simvastatin 20mg QD Most recent lipid profile: TC = 246, TG = 100, LDL = 176, HDL = 50 What about Mr. Williams? 56
How would you manage Ms. Gold 32 yo Asian woman with dyslipidemia Current medications: Simvastatin 20mg QD Most recent lipid profile: TC = 246, TG = 100, LDL = 176, HDL = 50 What about Mr. Williams? 56
DISCLOSURE PHARMACIST OBJECTIVES 9/30/2014 JNC 8: A REVIEW OF THE LONG-AWAITED/MUCH-ANTICIPATED HYPERTENSION GUIDELINES. I have nothing to disclose.
 JNC 8: A REVIEW OF THE LONG-AWAITED/MUCH-ANTICIPATED HYPERTENSION GUIDELINES Tiffany Dickey, PharmD Assistant Professor, UAMS COP Clinical Pharmacy Specialist, Mercy Hospital Northwest AR DISCLOSURE I
JNC 8: A REVIEW OF THE LONG-AWAITED/MUCH-ANTICIPATED HYPERTENSION GUIDELINES Tiffany Dickey, PharmD Assistant Professor, UAMS COP Clinical Pharmacy Specialist, Mercy Hospital Northwest AR DISCLOSURE I
Treating Hypertension in Individuals with Diabetes
 Treating Hypertension in Individuals with Diabetes Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any
Treating Hypertension in Individuals with Diabetes Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any
Combination Therapy for Hypertension
 Combination Therapy for Hypertension Se-Joong Rim, MD Cardiology Division, Yonsei University College of Medicine, Seoul, Korea Goals of Therapy Reduce CVD and renal morbidity and mortality. Treat to BP
Combination Therapy for Hypertension Se-Joong Rim, MD Cardiology Division, Yonsei University College of Medicine, Seoul, Korea Goals of Therapy Reduce CVD and renal morbidity and mortality. Treat to BP
Understanding the importance of blood pressure control An overview of new guidelines: How do they impact daily current management?
 Understanding the importance of blood pressure control An overview of new guidelines: How do they impact daily current management? Slides presented during CDMC in Almaty, Kazakhstan on Saturday April 12,
Understanding the importance of blood pressure control An overview of new guidelines: How do they impact daily current management? Slides presented during CDMC in Almaty, Kazakhstan on Saturday April 12,
Jared Moore, MD, FACP
 Hypertension 101 Jared Moore, MD, FACP Assistant Program Director, Internal Medicine Residency Clinical Assistant Professor of Internal Medicine Division of General Medicine The Ohio State University Wexner
Hypertension 101 Jared Moore, MD, FACP Assistant Program Director, Internal Medicine Residency Clinical Assistant Professor of Internal Medicine Division of General Medicine The Ohio State University Wexner
Talking about blood pressure
 Talking about blood pressure Mrs Khan 56 BP 158/99 BMI 32 Total cholesterol 5.4 (HDL 0.8) HbA1c 43 She has been promising to do more exercise and eat more healthily for the last 2 years but her weight
Talking about blood pressure Mrs Khan 56 BP 158/99 BMI 32 Total cholesterol 5.4 (HDL 0.8) HbA1c 43 She has been promising to do more exercise and eat more healthily for the last 2 years but her weight
Clinical cases with Coversyl 10 mg
 Clinical cases Coversyl 10 mg For upgraded benefits in hypertension A Editorial This brochure, Clinical cases Coversyl 10 mg for upgraded benefits in hypertension, illustrates a variety of hypertensive
Clinical cases Coversyl 10 mg For upgraded benefits in hypertension A Editorial This brochure, Clinical cases Coversyl 10 mg for upgraded benefits in hypertension, illustrates a variety of hypertensive
ANTI- HYPERTENSIVE AGENTS
 CLINICAL ANTI- HYPERTENSIVE AGENTS Jacqueline van Schoor, MPharm, BSc (Hons) Amayeza Info Centre Hypertension represents a major public health concern. It affects about a billion people worldwide and is
CLINICAL ANTI- HYPERTENSIVE AGENTS Jacqueline van Schoor, MPharm, BSc (Hons) Amayeza Info Centre Hypertension represents a major public health concern. It affects about a billion people worldwide and is
Abbreviations Cardiology I
 Cardiology I and Clinical Controversies Joseph J. Saseen, Pharm.D., FCCP, BCPS (AQ Cardiology) Reviewed by Stuart T. Haines, Pharm.D., FCCP, BCPS; and Michelle M. Richardson, Pharm.D., FCCP, BCPS Learning
Cardiology I and Clinical Controversies Joseph J. Saseen, Pharm.D., FCCP, BCPS (AQ Cardiology) Reviewed by Stuart T. Haines, Pharm.D., FCCP, BCPS; and Michelle M. Richardson, Pharm.D., FCCP, BCPS Learning
Optimal blockade of the Renin- Angiotensin-Aldosterone. in chronic heart failure
 Optimal blockade of the Renin- Angiotensin-Aldosterone Aldosterone- (RAA)-System in chronic heart failure Jan Östergren Department of Medicine Karolinska University Hospital Stockholm, Sweden Key Issues
Optimal blockade of the Renin- Angiotensin-Aldosterone Aldosterone- (RAA)-System in chronic heart failure Jan Östergren Department of Medicine Karolinska University Hospital Stockholm, Sweden Key Issues
7/7/ CHD/MI LVH and LV dysfunction Dysrrhythmias Stroke PVD Renal insufficiency and failure Retinopathy. Normal <120 Prehypertension
 Prevalence of Hypertension Hypertension: Diagnosis and Management T. Villela, M.D. Program Director University of California, San Francisco-San Francisco General Hospital Family and Community Medicine
Prevalence of Hypertension Hypertension: Diagnosis and Management T. Villela, M.D. Program Director University of California, San Francisco-San Francisco General Hospital Family and Community Medicine
2003 World Health Organization (WHO) / International Society of Hypertension (ISH) Statement on Management of Hypertension.
 / International Society of Hypertension (ISH) Statement on Management of Hypertension.") 2003 World Health Organization (WHO) / International Society of Hypertension (ISH) Statement on Management of Hypertension Writing Group: Background Hypertension worldwide causes 7.1 million premature
2003 World Health Organization (WHO) / International Society of Hypertension (ISH) Statement on Management of Hypertension Writing Group: Background Hypertension worldwide causes 7.1 million premature
Should All Patients Be Treated with Ace-inh /ARB after STEMI with Preserved LV Function?
 Should All Patients Be Treated with Ace-inh /ARB after STEMI with Preserved LV Function? Avi Shimony, MD, FESC Cardiology Division Soroka University Medical Center Ben-Gurion University, Beer-Sheva Disclosure
Should All Patients Be Treated with Ace-inh /ARB after STEMI with Preserved LV Function? Avi Shimony, MD, FESC Cardiology Division Soroka University Medical Center Ben-Gurion University, Beer-Sheva Disclosure
LXIV: DRUGS: 4. RAS BLOCKADE
 LXIV: DRUGS: 4. RAS BLOCKADE ACE Inhibitors Components of RAS Actions of Angiotensin i II Indications for ACEIs Contraindications RAS blockade in hypertension RAS blockade in CAD RAS blockade in HF Limitations
LXIV: DRUGS: 4. RAS BLOCKADE ACE Inhibitors Components of RAS Actions of Angiotensin i II Indications for ACEIs Contraindications RAS blockade in hypertension RAS blockade in CAD RAS blockade in HF Limitations
hypertension Head of prevention and control of CVD disease office Ministry of heath
 hypertension t. Samavat MD,Cadiologist,MPH Head of prevention and control of CVD disease office Ministry of heath RECOMMENDATIONS FOR HYPERTENSION DIAGNOSIS, ASSESSMENT, AND TREATMENT Definition of hypertension
hypertension t. Samavat MD,Cadiologist,MPH Head of prevention and control of CVD disease office Ministry of heath RECOMMENDATIONS FOR HYPERTENSION DIAGNOSIS, ASSESSMENT, AND TREATMENT Definition of hypertension
New Recommendations for the Treatment of Hypertension: From Population Salt Reduction to Personalized Treatment Targets
 New Recommendations for the Treatment of Hypertension: From Population Salt Reduction to Personalized Treatment Targets Sidney C. Smith, Jr. MD, FACC, FAHA Professor of Medicine/Cardiology University of
New Recommendations for the Treatment of Hypertension: From Population Salt Reduction to Personalized Treatment Targets Sidney C. Smith, Jr. MD, FACC, FAHA Professor of Medicine/Cardiology University of
Update in Cardiology Pharmacologic Management of Cardiovascular Risk. Christopher C. Roe, MSN, ACNP
 Update in Cardiology Pharmacologic Management of Cardiovascular Risk Christopher C. Roe, MSN, ACNP Objectives 1. Verbalize understanding of new pharmacologic guidelines in the treatment of hypertension
Update in Cardiology Pharmacologic Management of Cardiovascular Risk Christopher C. Roe, MSN, ACNP Objectives 1. Verbalize understanding of new pharmacologic guidelines in the treatment of hypertension
Diabetes and Hypertension
 Diabetes and Hypertension William C. Cushman, MD, FAHA, FACP, FASH Chief, Preventive Medicine, Veterans Affairs Medical Center Professor, Preventive Medicine, Medicine, and Physiology University of Tennessee
Diabetes and Hypertension William C. Cushman, MD, FAHA, FACP, FASH Chief, Preventive Medicine, Veterans Affairs Medical Center Professor, Preventive Medicine, Medicine, and Physiology University of Tennessee
4/4/17 HYPERTENSION TARGETS: WHAT DO WE DO NOW? SET THE STAGE BP IN CLINICAL TRIALS?
 HYPERTENSION TARGETS: WHAT DO WE DO NOW? MICHAEL LEFEVRE, MD, MSPH PROFESSOR AND VICE CHAIR DEPARTMENT OF FAMILY AND COMMUNITY MEDICINE UNIVERSITY OF MISSOURI 4/4/17 DISCLOSURE: MEMBER OF THE JNC 8 PANEL
HYPERTENSION TARGETS: WHAT DO WE DO NOW? MICHAEL LEFEVRE, MD, MSPH PROFESSOR AND VICE CHAIR DEPARTMENT OF FAMILY AND COMMUNITY MEDICINE UNIVERSITY OF MISSOURI 4/4/17 DISCLOSURE: MEMBER OF THE JNC 8 PANEL
Cedars Sinai Diabetes. Michael A. Weber
 Cedars Sinai Diabetes Michael A. Weber Speaker Disclosures I disclose that I am a Consultant for: Ablative Solutions, Boston Scientific, Boehringer Ingelheim, Eli Lilly, Forest, Medtronics, Novartis, ReCor
Cedars Sinai Diabetes Michael A. Weber Speaker Disclosures I disclose that I am a Consultant for: Ablative Solutions, Boston Scientific, Boehringer Ingelheim, Eli Lilly, Forest, Medtronics, Novartis, ReCor
ADVANCES IN MANAGEMENT OF HYPERTENSION
 Advances in Management of Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Current Status of Prevalence 29%; Blacks 33.5%
Advances in Management of Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Current Status of Prevalence 29%; Blacks 33.5%
Hypertension (JNC-8)
") Hypertension (JNC-8) Southern California University of Health Sciences Physician Assistant Program Management and Treatment of Hypertension April 17, 2018, presented by Ezra Levy, Pharm.D.! The 8 th Joint
Hypertension (JNC-8) Southern California University of Health Sciences Physician Assistant Program Management and Treatment of Hypertension April 17, 2018, presented by Ezra Levy, Pharm.D.! The 8 th Joint
RAS Blockade Across the CV Continuum
 A Summary of Recent International Meetings RAS Blockade Across the CV Continuum Copyright New Evidence Presented at the 2009 Congress of the European Society of Cardiology (August 29-September 2, Barcelona)
A Summary of Recent International Meetings RAS Blockade Across the CV Continuum Copyright New Evidence Presented at the 2009 Congress of the European Society of Cardiology (August 29-September 2, Barcelona)
ALLHAT. ALLHAT Antihypertensive Trial Results by Baseline Diabetic & Fasting Glucose Status
 ALLHAT Antihypertensive Trial Results by Baseline Diabetic & Fasting Glucose Status 1 Introduction and Background Clinical trials have reported reduction in CV events with diuretics, CCBs, ACE inhibitors,
ALLHAT Antihypertensive Trial Results by Baseline Diabetic & Fasting Glucose Status 1 Introduction and Background Clinical trials have reported reduction in CV events with diuretics, CCBs, ACE inhibitors,
Hypertension Management Controversies in the Elderly Patient
 Hypertension Management Controversies in the Elderly Patient Juan Bowen, MD Geriatric Update for the Primary Care Provider November 17, 2016 2016 MFMER slide-1 Disclosure No financial relationships No
Hypertension Management Controversies in the Elderly Patient Juan Bowen, MD Geriatric Update for the Primary Care Provider November 17, 2016 2016 MFMER slide-1 Disclosure No financial relationships No
The Latest Generation of Clinical
 The Latest Generation of Clinical Guidelines: HTN and HLD Dave Brackett Clinical Guideline Purpose Uniform approach Awareness of key details Diagnosis Treatment Monitoring Evidence based approach Inform
The Latest Generation of Clinical Guidelines: HTN and HLD Dave Brackett Clinical Guideline Purpose Uniform approach Awareness of key details Diagnosis Treatment Monitoring Evidence based approach Inform
ACE inhibitors: still the gold standard?
 ACE inhibitors: still the gold standard? Session: Twenty-five years after CONSENSUS What have we learnt about the RAAS in heart failure? Lars Køber, MD, D.Sci Department of Cardiology Rigshospitalet University
ACE inhibitors: still the gold standard? Session: Twenty-five years after CONSENSUS What have we learnt about the RAAS in heart failure? Lars Køber, MD, D.Sci Department of Cardiology Rigshospitalet University
Hypertension. Most important public health problem in developed countries
 Hypertension Strategy for Continued Success in Treatment for the 21st Century November 15, 2005 Arnold B. Meshkov, M.D. Associate Professor of Medicine Temple University School of Medicine Philadelphia,
Hypertension Strategy for Continued Success in Treatment for the 21st Century November 15, 2005 Arnold B. Meshkov, M.D. Associate Professor of Medicine Temple University School of Medicine Philadelphia,
Hypertension Update Warwick Jaffe Interventional Cardiologist Ascot Hospital
 Hypertension Update 2008 Warwick Jaffe Interventional Cardiologist Ascot Hospital Definition of Hypertension Continuous variable At some point the risk becomes high enough to justify treatment Treatment
Hypertension Update 2008 Warwick Jaffe Interventional Cardiologist Ascot Hospital Definition of Hypertension Continuous variable At some point the risk becomes high enough to justify treatment Treatment
ADVANCES IN MANAGEMENT OF HYPERTENSION
 Prevalence 29%; Blacks 33.5% About 72.5% treated; 53.5% uncontrolled (>140/90) Risk for poor control: Latinos, Blacks, age 18-44 and 80,
Prevalence 29%; Blacks 33.5% About 72.5% treated; 53.5% uncontrolled (>140/90) Risk for poor control: Latinos, Blacks, age 18-44 and 80,
Clinical Updates in the Treatment of Hypertension JNC 7 vs. JNC 8. Lauren Thomas, PharmD PGY1 Pharmacy Practice Resident South Pointe Hospital
 Clinical Updates in the Treatment of Hypertension JNC 7 vs. JNC 8 Lauren Thomas, PharmD PGY1 Pharmacy Practice Resident South Pointe Hospital Objectives Review the Eighth Joint National Committee (JNC
Clinical Updates in the Treatment of Hypertension JNC 7 vs. JNC 8 Lauren Thomas, PharmD PGY1 Pharmacy Practice Resident South Pointe Hospital Objectives Review the Eighth Joint National Committee (JNC
APPENDIX D: PHARMACOTYHERAPY EVIDENCE
 Página 1 de 7 APPENDIX D: PHARMACOTYHERAPY EVIDENCE Table D1. Outcome Trials of Antihypertensive Agents Study Drug Regimen N Duration Primary Outcomes Remarks Antihypertensive Therapy vs Placebo SHEP 1991
Página 1 de 7 APPENDIX D: PHARMACOTYHERAPY EVIDENCE Table D1. Outcome Trials of Antihypertensive Agents Study Drug Regimen N Duration Primary Outcomes Remarks Antihypertensive Therapy vs Placebo SHEP 1991
Metabolic Consequences of Anti Hypertensives: Is It Clinically Important?
 Metabolic Consequences of Anti Hypertensives: Is It Clinically Important?,FACA,FICA,MASH,FVBWG,MISCP CONSULTANT OF CARDIOLOGY DIRECTOR OF PORT-FOUAD HOSPITAL CCU Consideration of antihypertensive agents
Metabolic Consequences of Anti Hypertensives: Is It Clinically Important?,FACA,FICA,MASH,FVBWG,MISCP CONSULTANT OF CARDIOLOGY DIRECTOR OF PORT-FOUAD HOSPITAL CCU Consideration of antihypertensive agents
Update on Current Trends in Hypertension Management
 Friday General Session Update on Current Trends in Hypertension Management Shawna Nesbitt, MD Associate Dean, Minority Student Affairs Associate Professor, Department of Internal Medicine Office of Student
Friday General Session Update on Current Trends in Hypertension Management Shawna Nesbitt, MD Associate Dean, Minority Student Affairs Associate Professor, Department of Internal Medicine Office of Student
1. Albuminuria an early sign of glomerular damage and renal disease. albuminuria
 1. Albuminuria an early sign of glomerular damage and renal disease albuminuria Cardio-renal continuum REGRESS Target organ damage Asymptomatic CKD New risk factors Atherosclerosis Target organ damage
1. Albuminuria an early sign of glomerular damage and renal disease albuminuria Cardio-renal continuum REGRESS Target organ damage Asymptomatic CKD New risk factors Atherosclerosis Target organ damage
Module 2. Global Cardiovascular Risk Assessment and Reduction in Women with Hypertension
 Module 2 Global Cardiovascular Risk Assessment and Reduction in Women with Hypertension 1 Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored,
Module 2 Global Cardiovascular Risk Assessment and Reduction in Women with Hypertension 1 Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored,
Individual management of arterial hypertension. Doumas Michael, Internist Lecturer, Aristotle University, Thessaloniki
 Individual management of arterial hypertension Doumas Michael, Internist Lecturer, Aristotle University, Thessaloniki From Population to Individual Management of Arterial Hypertension Epidemiologic impact
Individual management of arterial hypertension Doumas Michael, Internist Lecturer, Aristotle University, Thessaloniki From Population to Individual Management of Arterial Hypertension Epidemiologic impact
Cardiovascular Health Practice Guideline Outpatient Management of Coronary Artery Disease 2003
 Authorized By: Medical Management Guideline Committee Approval Date: 12/13/01 Revision Date: 12/11/03 Beta-Blockers Nitrates Calcium Channel Blockers MEDICATIONS Indicated in post-mi, unstable angina,
Authorized By: Medical Management Guideline Committee Approval Date: 12/13/01 Revision Date: 12/11/03 Beta-Blockers Nitrates Calcium Channel Blockers MEDICATIONS Indicated in post-mi, unstable angina,
ΥΠΕΡΤΑΣΗ ΚΑΙ ΣΤΕΦΑΝΙΑΙΑ ΝΟΣΟΣ Ι.Ε.ΚΑΝΟΝΙΔΗΣ
 ΥΠΕΡΤΑΣΗ ΚΑΙ ΣΤΕΦΑΝΙΑΙΑ ΝΟΣΟΣ Ι.Ε.ΚΑΝΟΝΙΔΗΣ CAD: Statistics CAD is the largest killer of American males and females 13 million Americans have CAD 1.1 million MI s per year Every 26 seconds an American
ΥΠΕΡΤΑΣΗ ΚΑΙ ΣΤΕΦΑΝΙΑΙΑ ΝΟΣΟΣ Ι.Ε.ΚΑΝΟΝΙΔΗΣ CAD: Statistics CAD is the largest killer of American males and females 13 million Americans have CAD 1.1 million MI s per year Every 26 seconds an American
How clinically important are the results of the large trials in hypertension?
 How clinically important are the results of the large trials in hypertension? Stéphane LAURENT, MD, PhD, FESC Pharmacology Department and PARCC / INSERM U970 Hôpital Européen Georges Pompidou, Université
How clinically important are the results of the large trials in hypertension? Stéphane LAURENT, MD, PhD, FESC Pharmacology Department and PARCC / INSERM U970 Hôpital Européen Georges Pompidou, Université
Prevention of Atrial Fibrillation and Heart Failure in the Hypertensive Patient
 Prevention of Atrial Fibrillation and Heart Failure in the Hypertensive Patient The Issue of Primary Prevention of A.Fib. (and Heart Failure) and not the Prevention of Recurrent A.Fib. after Electroconversion
Prevention of Atrial Fibrillation and Heart Failure in the Hypertensive Patient The Issue of Primary Prevention of A.Fib. (and Heart Failure) and not the Prevention of Recurrent A.Fib. after Electroconversion
MANAGEMENT OF HYPERTENSION: TREATMENT THRESHOLDS AND MEDICATION SELECTION
 Management of Hypertension: Treatment Thresholds and Medication Selection Robert B. Baron, MD MS Professor and Associate Dean Declaration of full disclosure: No conflict of interest Presentation Goals
Management of Hypertension: Treatment Thresholds and Medication Selection Robert B. Baron, MD MS Professor and Associate Dean Declaration of full disclosure: No conflict of interest Presentation Goals
Younger adults with a family history of premature artherosclerotic disease should have their cardiovascular risk factors measured.
 Appendix 2A - Guidance on Management of Hypertension Measurement of blood pressure All adults from 40 years should have blood pressure measured as part of opportunistic cardiovascular risk assessment.
Appendix 2A - Guidance on Management of Hypertension Measurement of blood pressure All adults from 40 years should have blood pressure measured as part of opportunistic cardiovascular risk assessment.
Pharmacologic Management of Hypertension
 Current Concepts In Management of Fernando Vega, MD Secondary - Definition Renovascular Disease (The kidney doesn t get impressed by blood pressure) Renovascular stenosis Renal artery stenosis Fibromuscular
Current Concepts In Management of Fernando Vega, MD Secondary - Definition Renovascular Disease (The kidney doesn t get impressed by blood pressure) Renovascular stenosis Renal artery stenosis Fibromuscular
JNC Evidence-Based Guidelines for the Management of High Blood Pressure in Adults
 JNC 8 2014 Evidence-Based Guidelines for the Management of High Blood Pressure in Adults Table of Contents Why Do We Treat Hypertension? Blood Pressure Treatment Goals Initial Therapy Strength of Recommendation
JNC 8 2014 Evidence-Based Guidelines for the Management of High Blood Pressure in Adults Table of Contents Why Do We Treat Hypertension? Blood Pressure Treatment Goals Initial Therapy Strength of Recommendation
Update in Hypertension
 Update in Hypertension Eliseo J. PérezP rez-stable MD Professor of Medicine DGIM, Department of Medicine UCSF 20 May 2008 Declaration of full disclosure: No conflict of interest (I have never been funded
Update in Hypertension Eliseo J. PérezP rez-stable MD Professor of Medicine DGIM, Department of Medicine UCSF 20 May 2008 Declaration of full disclosure: No conflict of interest (I have never been funded
New Lipid Guidelines. PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN: Implications of the New Guidelines for Hypertension and Lipids.
 PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN: Implications of the New Guidelines for Hypertension and Lipids Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Disclosure No relevant
PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN: Implications of the New Guidelines for Hypertension and Lipids Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Disclosure No relevant
Reframe the Paradigm of Hypertension treatment Focus on Diabetes
 Reframe the Paradigm of Hypertension treatment Focus on Diabetes Paola Atallah, MD Lecturer of Clinical Medicine SGUMC EDL monthly meeting October 25,2016 Overview Physiopathology of hypertension Classification
Reframe the Paradigm of Hypertension treatment Focus on Diabetes Paola Atallah, MD Lecturer of Clinical Medicine SGUMC EDL monthly meeting October 25,2016 Overview Physiopathology of hypertension Classification
Managing Hypertension in Diabetes Sean Stewart, PharmD, BCPS, BCACP, CLS Internal Medicine Park Nicollet Clinic St Louis Park.
 Managing Hypertension in Diabetes 2015 Sean Stewart, PharmD, BCPS, BCACP, CLS Internal Medicine Park Nicollet Clinic St Louis Park Case Scenario Mike M is a 59 year old man with type 2 diabetes managed
Managing Hypertension in Diabetes 2015 Sean Stewart, PharmD, BCPS, BCACP, CLS Internal Medicine Park Nicollet Clinic St Louis Park Case Scenario Mike M is a 59 year old man with type 2 diabetes managed
Traitements associés chez l hypertendu: Statines, Aspirine
 Traitements associés chez l hypertendu: Statines, Aspirine Pr Jean-Jacques Mourad CHU Avicenne, Université Paris 13, Bobigny DU HTA, Mars 2012 jean-jacques.mourad@avc.aphp.fr Global Mortality 2000: Impact
Traitements associés chez l hypertendu: Statines, Aspirine Pr Jean-Jacques Mourad CHU Avicenne, Université Paris 13, Bobigny DU HTA, Mars 2012 jean-jacques.mourad@avc.aphp.fr Global Mortality 2000: Impact
Heart Failure Clinician Guide JANUARY 2018
 Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Heart Failure Clinician Guide JANUARY 2018 Introduction This evidence-based guideline summary is based on the 2018 National Heart Failure Guideline.
Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Heart Failure Clinician Guide JANUARY 2018 Introduction This evidence-based guideline summary is based on the 2018 National Heart Failure Guideline.
Hypertension and Cardiovascular Disease
 Hypertension and Cardiovascular Disease Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any means graphic,
Hypertension and Cardiovascular Disease Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any means graphic,
2014 HYPERTENSION GUIDELINES
 2014 HYPERTENSION GUIDELINES Eileen M. Twomey, Pharm.D., BCPS 1 Learning Objectives Describe specific blood pressure thresholds at which antihypertensive therapy should be initiated and blood pressure
2014 HYPERTENSION GUIDELINES Eileen M. Twomey, Pharm.D., BCPS 1 Learning Objectives Describe specific blood pressure thresholds at which antihypertensive therapy should be initiated and blood pressure
By Prof. Khaled El-Rabat
 What is The Optimum? By Prof. Khaled El-Rabat Professor of Cardiology - Benha Faculty of Medicine HT. Introduction Despite major worldwide efforts over recent decades directed at diagnosing and treating
What is The Optimum? By Prof. Khaled El-Rabat Professor of Cardiology - Benha Faculty of Medicine HT. Introduction Despite major worldwide efforts over recent decades directed at diagnosing and treating
Metabolic Syndrome and Chronic Kidney Disease
 Metabolic Syndrome and Chronic Kidney Disease Definition of Metabolic Syndrome National Cholesterol Education Program (NCEP) Adult Treatment Panel (ATP) III Abdominal obesity, defined as a waist circumference
Metabolic Syndrome and Chronic Kidney Disease Definition of Metabolic Syndrome National Cholesterol Education Program (NCEP) Adult Treatment Panel (ATP) III Abdominal obesity, defined as a waist circumference
Modern Management of Hypertension
 Modern Management of Hypertension Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Current Status of Hypertension Prevalence
Modern Management of Hypertension Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Current Status of Hypertension Prevalence
Management of Lipid Disorders and Hypertension: Implications of the New Guidelines
 Management of Lipid Disorders and Hypertension Management of Lipid Disorders and Hypertension: Implications of the New Guidelines Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine
Management of Lipid Disorders and Hypertension Management of Lipid Disorders and Hypertension: Implications of the New Guidelines Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine
The Beneficial Role of Angiotensin- Converting Enzyme Inhibitor in Acute Myocardial Infarction
 The Beneficial Role of Angiotensin- Converting Enzyme Inhibitor in Acute Myocardial Infarction Cardiovascular Center, Korea University Guro Hospital 2007. 4. 20 Seung-Woon Rha, MD, PhD Introduction 1.
The Beneficial Role of Angiotensin- Converting Enzyme Inhibitor in Acute Myocardial Infarction Cardiovascular Center, Korea University Guro Hospital 2007. 4. 20 Seung-Woon Rha, MD, PhD Introduction 1.
Hypertension and CAD. Dr. Vinod Sharma. National Heart Institute New Delhi
 Hypertension and CAD Dr. Vinod Sharma National Heart Institute New Delhi Case History 1 AB 82 years female with - Hypertension 7 yrs treated with ACE inhibitors & Amlodipine, BP fluctuating between 160
Hypertension and CAD Dr. Vinod Sharma National Heart Institute New Delhi Case History 1 AB 82 years female with - Hypertension 7 yrs treated with ACE inhibitors & Amlodipine, BP fluctuating between 160
Metoprolol Succinate SelokenZOC
 Metoprolol Succinate SelokenZOC Blood Pressure Control and Far Beyond Mohamed Abdel Ghany World Health Organization - Noncommunicable Diseases (NCD) Country Profiles, 2014. 1 Death Rates From Ischemic
Metoprolol Succinate SelokenZOC Blood Pressure Control and Far Beyond Mohamed Abdel Ghany World Health Organization - Noncommunicable Diseases (NCD) Country Profiles, 2014. 1 Death Rates From Ischemic
Preventing and Treating High Blood Pressure
 Preventing and Treating High Blood Pressure: Finding the Right Balance of Integrative and Pharmacologic Approaches Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Blood Pressure
Preventing and Treating High Blood Pressure: Finding the Right Balance of Integrative and Pharmacologic Approaches Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Blood Pressure
heart failure John McMurray University of Glasgow.
 A to Z of RAAS blockade in heart failure John McMurray BHF Cardiovascular Research Centre University of Glasgow. RAAS inhibition in CHF ACE inhibition in patients with low LVEF CHF CONSENSUS Enalapril
A to Z of RAAS blockade in heart failure John McMurray BHF Cardiovascular Research Centre University of Glasgow. RAAS inhibition in CHF ACE inhibition in patients with low LVEF CHF CONSENSUS Enalapril
Egyptian Hypertension Guidelines
 Egyptian Hypertension Guidelines 2014 Egyptian Hypertension Guidelines Dalia R. ElRemissy, MD Lecturer of Cardiovascular Medicine Cairo University Why Egyptian Guidelines? Guidelines developed for rich
Egyptian Hypertension Guidelines 2014 Egyptian Hypertension Guidelines Dalia R. ElRemissy, MD Lecturer of Cardiovascular Medicine Cairo University Why Egyptian Guidelines? Guidelines developed for rich
Cardiovascular Complications of Diabetes
 VBWG Cardiovascular Complications of Diabetes Nicola Abate, M.D., F.N.L.A. Professor and Chief Division of Endocrinology and Metabolism The University of Texas Medical Branch Galveston, Texas Coronary
VBWG Cardiovascular Complications of Diabetes Nicola Abate, M.D., F.N.L.A. Professor and Chief Division of Endocrinology and Metabolism The University of Texas Medical Branch Galveston, Texas Coronary
Hypertension in 2015: SPRINT-ing ahead of JNC-8. MAJ Charles Magee, MD MPH FACP Director, WRNMMC Hypertension Clinic
 Hypertension in 2015: SPRINT-ing ahead of JNC-8 MAJ Charles Magee, MD MPH FACP Director, WRNMMC Hypertension Clinic Conflits of interest? None Disclaimer The opinions contained herein are not to be considered
Hypertension in 2015: SPRINT-ing ahead of JNC-8 MAJ Charles Magee, MD MPH FACP Director, WRNMMC Hypertension Clinic Conflits of interest? None Disclaimer The opinions contained herein are not to be considered
Blood Pressure Targets: Where are We Now?
 Blood Pressure Targets: Where are We Now? Diana Cao, PharmD, BCPS-AQ Cardiology Assistant Professor Department of Clinical & Administrative Sciences California Northstate University College of Pharmacy
Blood Pressure Targets: Where are We Now? Diana Cao, PharmD, BCPS-AQ Cardiology Assistant Professor Department of Clinical & Administrative Sciences California Northstate University College of Pharmacy
Treatment to reduce cardiovascular risk: multifactorial management
 Treatment to reduce cardiovascular risk: multifactorial management Matteo Anselmino, MD PhD Assistant Professor San Giovanni Battista Hospital Division of Cardiology, Department of Internal Medicine University
Treatment to reduce cardiovascular risk: multifactorial management Matteo Anselmino, MD PhD Assistant Professor San Giovanni Battista Hospital Division of Cardiology, Department of Internal Medicine University
Management of Hypertension. M Misra MD MRCP (UK) Division of Nephrology University of Missouri School of Medicine
 Division of Nephrology University of Missouri School of Medicine") Management of Hypertension M Misra MD MRCP (UK) Division of Nephrology University of Missouri School of Medicine Disturbing Trends in Hypertension HTN awareness, treatment and control rates are decreasing
Management of Hypertension M Misra MD MRCP (UK) Division of Nephrology University of Missouri School of Medicine Disturbing Trends in Hypertension HTN awareness, treatment and control rates are decreasing
Causes of death in Diabetes
 Rates of CV events in Diabetes patients Respiratory4.2 Cancer 7.6 Diabetes 1.3 CV disease 17.3 Causes of death in Diabetes 250 200 150 100 50 0 per 10,000 person-years 97 151 243 Framingham 5 X increase
Rates of CV events in Diabetes patients Respiratory4.2 Cancer 7.6 Diabetes 1.3 CV disease 17.3 Causes of death in Diabetes 250 200 150 100 50 0 per 10,000 person-years 97 151 243 Framingham 5 X increase
Difficult to Treat Hypertension
 Difficult to Treat Hypertension According to Goldilocks JNC 8 Blood Pressure Goals (2014) BP Goal 60 years old and greater*- systolic < 150 and diastolic < 90. (Grade A)** BP Goal 18-59 years old* diastolic
Difficult to Treat Hypertension According to Goldilocks JNC 8 Blood Pressure Goals (2014) BP Goal 60 years old and greater*- systolic < 150 and diastolic < 90. (Grade A)** BP Goal 18-59 years old* diastolic
Rationale for the use of Single Pill Combination (SPC) and Asian data of ARB/CCB SPC
 and Asian data of ARB/CCB SPC") Rationale for the use of Single Pill Combination (SPC) and Asian data of ARB/CCB SPC Seung Woo Park, MD Samsung Medical Center BP Control Rates in Asia BP controlled BP uncontrolled 24.3% 36.6% 19% Turkey
Rationale for the use of Single Pill Combination (SPC) and Asian data of ARB/CCB SPC Seung Woo Park, MD Samsung Medical Center BP Control Rates in Asia BP controlled BP uncontrolled 24.3% 36.6% 19% Turkey
Hypertension Pharmacotherapy: A Practical Approach
 Hypertension Pharmacotherapy: A Practical Approach Ronald Victor, MD Burns & Allen Chair in Cardiology Director, The Hypertension Center Associate Director, The Heart Institute Hypertension Center 1. 2.
Hypertension Pharmacotherapy: A Practical Approach Ronald Victor, MD Burns & Allen Chair in Cardiology Director, The Hypertension Center Associate Director, The Heart Institute Hypertension Center 1. 2.
SBP in range of 120 to 140 :no progression or regression of CAD. Sipahi et al., 2006
 Management of Hypertension in Patients with CAD M. Mohsen Ibrahim, MD Cardiology Department- Cairo University 1. What is the optimal BP in patients with hypertension and CAD? 2. What is the minimum safe
Management of Hypertension in Patients with CAD M. Mohsen Ibrahim, MD Cardiology Department- Cairo University 1. What is the optimal BP in patients with hypertension and CAD? 2. What is the minimum safe
DISCLOSURES OUTLINE OUTLINE 9/29/2014 ANTI-HYPERTENSIVE MANAGEMENT OF CHRONIC KIDNEY DISEASE
 ANTI-HYPERTENSIVE MANAGEMENT OF CHRONIC KIDNEY DISEASE DISCLOSURES Editor-in-Chief- Nephrology- UpToDate- (Wolters Klewer) Richard J. Glassock, MD, MACP Geffen School of Medicine at UCLA 1 st Annual Internal
ANTI-HYPERTENSIVE MANAGEMENT OF CHRONIC KIDNEY DISEASE DISCLOSURES Editor-in-Chief- Nephrology- UpToDate- (Wolters Klewer) Richard J. Glassock, MD, MACP Geffen School of Medicine at UCLA 1 st Annual Internal
Randomized Design of ALLHAT BP Trial
 Outcomes in Hypertensive Black and Nonblack Patients Treated with Chlorthalidone, Amlodipine, and Lisinopril* *Wright JT, Dunn JK, Cutler JA et al. JAMA 2005:293:1595-1608. 42,418 High-risk hypertensive
Outcomes in Hypertensive Black and Nonblack Patients Treated with Chlorthalidone, Amlodipine, and Lisinopril* *Wright JT, Dunn JK, Cutler JA et al. JAMA 2005:293:1595-1608. 42,418 High-risk hypertensive
The Failing Heart in Primary Care
 The Failing Heart in Primary Care Hamid Ikram How fares the Heart Failure Epidemic? 4357 patients, 57% women, mean age 74 years HFSA 2010 Practice Guideline (3.1) Heart Failure Prevention A careful and
The Failing Heart in Primary Care Hamid Ikram How fares the Heart Failure Epidemic? 4357 patients, 57% women, mean age 74 years HFSA 2010 Practice Guideline (3.1) Heart Failure Prevention A careful and
Hypertension Management: A Moving Target
 9:45 :30am Hypertension Management: A Moving Target SPEAKER Karol Watson, MD, PhD, FACC Presenter Disclosure Information The following relationships exist related to this presentation: Karol E. Watson,
9:45 :30am Hypertension Management: A Moving Target SPEAKER Karol Watson, MD, PhD, FACC Presenter Disclosure Information The following relationships exist related to this presentation: Karol E. Watson,
Hypertension Management in Diabetic Patients
 Hypertension Management in Diabetic Patients Park, Chang G, MD, PhD Cardiovascular Center, Guro Hospital, Korea University Medical School Contents (Treatment of 2 Cases) Type 2 Diabetes Mellitus Hypertension
Hypertension Management in Diabetic Patients Park, Chang G, MD, PhD Cardiovascular Center, Guro Hospital, Korea University Medical School Contents (Treatment of 2 Cases) Type 2 Diabetes Mellitus Hypertension
Hypertension: JNC-7. Southern California University of Health Sciences Physician Assistant Program
 Hypertension: JNC-7 Southern California University of Health Sciences Physician Assistant Program Management and Treatment of Hypertension April 17, 2018, presented by Ezra Levy, Pharm.D.! Reference Card
Hypertension: JNC-7 Southern California University of Health Sciences Physician Assistant Program Management and Treatment of Hypertension April 17, 2018, presented by Ezra Levy, Pharm.D.! Reference Card
Heart Failure Clinician Guide JANUARY 2016
 Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Heart Failure Clinician Guide JANUARY 2016 Introduction This evidence-based guideline summary is based on the 2016 National Heart Failure Guideline.
Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Heart Failure Clinician Guide JANUARY 2016 Introduction This evidence-based guideline summary is based on the 2016 National Heart Failure Guideline.