DISCLOSURES OBJECTIVES CARDIOLOGY GUIDELINE UPDATES: HEART FAILURE, CARDIAC ARREST & HYPERLIPIDEMIA
|
|
|
- Eleanor Chambers
- 6 years ago
- Views:
Transcription
1 CARDIOLOGY GUIDELINE UPDATES: HEART FAILURE, CARDIAC ARREST & HYPERLIPIDEMIA Michael Gillette, Pharm.D., BCPS-AQ Cardiology, AACC Clinical Pharmacy Specialist, Cardiology Michael DeBakey VA Medical Center April 28, DISCLOSURES FINANCIAL DISCLOSURE: There are no financial or other relationships to disclose related to this presentation. UNLABELED/UNAPPROVED USES DISCLOSURE: The unlabeled/unapproved use of medications will not be discussed. The views expressed in this presentation reflect those of the author, and not necessarily those of the Department of Veterans Affairs. 2 OBJECTIVES Discuss the most recent updates to the guidelines for the management of cardiac arrest and heart failure Briefly review the 2013 ACC/AHA guidelines for hyperlipidemia Introduce the most recent guidelines for the role of nonstatin therapies in the management of hyperlipidemia Highlight a recent landmark trial that may impact the treatment and management of hyperlipidemia Be able to apply the guideline updates to patient care 3 1







2 Classes of recommendations and level of evidence used in ACCF/AHA clinical practice guidelines. Raymond J. Gibbons et al. Circulation. 2003; 107: Copyright American Heart Association, Inc. All rights reserved. READY? 6 2

3 2015 AHA GUIDELINE UPDATES FOR CARDIOPULMONARY RESUSCITATION AHA KEY NON-DRUG UPDATES 2010 Guideline Recommendation 2015 Guideline Update Although conflicting evidence exists, expert consensus recommended systematic identification of patients at risk of cardiac arrest, an organized response to such patients, and an evaluation of of outcomes to foster continuous quality improvement. For adult patients, rapid response team (RRT) or medical emergency team (MET) systems can be effective in reducing the incidence of cardiac arrest, particularly in the general care wards (Class IIa, LOE C-LD) It is reasonable for lay rescuers and HCPs to perform chest compressions (CCs) at a rate of at least 100/min. In adult victims of cardiac arrest, it is reasonable for rescuers to perform chest compressions at a rate of /min. (Class IIa, LOE-C-LD) The adult sternum should be depressed at least 2 inches (5 cm). rescuers should perform CCs to a depth of at least 2 inches (5 cm) for an avg. adult, while avoiding excessive CC depths (greater than 2.4 inches [6 cm]). (Class I, LOE C-LD) Kleinman ME, Brennan EE, Goldberger ZD, et al. Circulation 2015; 132:s414-s
4 2015 NEW DRUG" GUIDELINES For patients with known or suspected opioid addiction who are unresponsive with no normal breathing but a pulse, it is reasonable for appropriately trained lay rescuers and BLS providers, in addition to providing standard BLS care, to administer intramuscular (IM) or intranasal (IN) naloxone (Class IIa, LOE-C-LD) There is inadequate evidence to support the routine use of lidocaine after cardiac arrest. However, the initiation or continuation of lidocaine may be considered immediately after ROSC from SCA due to VF/pVT. (Class IIb, LOE C-LD) There is inadequate evidence to support the routine use of a β-blocker after SCA. However, the initiation or continuation of an oral or IV β- blocker may be considered early after hospitalization from cardiac arrest due to VF/pVT. (Class IIb, LOE C-LD). For patients with OHCA, use of steroids during CPR is of uncertain benefit (Class IIb, LOE C-LD) Link MS, Berkow LC, Kudenchuk PJ, et al. Circulation. 2015; 132:s444-s DRUG GUIDELINE UPDATES Standard-dose epinephrine (1 mg every 3 to 5 minutes) may be reasonable for patients in cardiac arrest. (Class IIb, LOE B-R) Vasopressin offers no advantage as a substitute for epinephrine in cardiac arrest (Class IIb, LOE B-R) It may be reasonable to administer epinephrine as soon as feasible after the onset of cardiac arrest due to an initial non-shockable rhythm. (Class IIb, LOE C-LD) The routine use of magnesium for VF/pVT is NOT recommended in adult patients Class III, LOE B-R). Amiodarone may be considered for VT/pVT that is unresponsive to CPR, defibrillation, and a vasopressor therapy (Class IIb, LOE B-R). Link MS, Berkow LC, Kudenchuk PJ, et al. Circulation. 2015; 132:s444-s FOCUSED UPDATE ON NEW PHARMACOLOGICAL THERAPY FOR HEART FAILURE 12 4

5 13 RECOMMENDATIONS FOR RENIN-ANGIOTENSIN SYSTEM (RAS) INHIBITION WITH ACE-I or ARB or ARNI COR LOE Recommendations I ACE: A ARB: A ARNI: B-R The clinical strategy of inhibition of the RAS with ACE-Is OR ARBs OR ARNI in conjunction with beta-blockers, and aldosterone antagonists in selected patients is recommended for patients with chronic HFrEF to reduce morbidity and mortality. I I I ACE: A ARB: A ARNI: B-R The use of ACE-Is is beneficial for patients with prior or current symptoms of chronic HFrEF to reduce morbidity and mortality The use of ARBs to reduce morbidity and mortality is recommended in patients with prior or current symptoms of chronic HFrEF who are intolerant to ACE-Is because of cough or angioedema. In patients with chronic symptoms HFrEF NYHA Class II or III who tolerate an ACE-inhibitor or ARB, replacement by an ARNI is recommended to further reduce morbidity and mortality. Key: Angiotensin Converting Enzyme Inhibitor (ACE-I); Angiotensin Receptor Blocker (ARB); Angiotensin-Receptor-Neprilysin Inhibitor (ARNI); Heart Failure with reduced Ejection Fraction (HFrEF); New York Heart Association (NYHA) Yancy CW, Jessup M, Bozkurt B, et al. Circulation. 2016; 134(13);e RECOMMENDATIONS FOR ARNI (cont.) COR LOE Recommendations III: Harm B-R ARNI should not be administered concomitantly with ACE-Is or within 36 hours of the last dose of an ACE-I. III: Harm C-EO ARNI should not be administered to patients with a history of angioedema. Key: Angiotensin Converting Enzyme Inhibitor (ACE-I); Angiotensin Receptor Blocker (ARB); Angiotensin-Receptor-Neprilysin Inhibitor (ARNI) Yancy CW, Jessup M, Bozkurt B, et al. Circulation. 2016; 134(13);e
 who are receiving GDEM, including a beta-blocker at maximum tolerated dose, and who are in sinus rhythm with a heart rate of 70 bpm or greater at rest.")
6 RECOMMENDATIONS FOR IVABRADINE (CORLANOR ) COR LOE Recommendations IIa B-R Ivabradine can be beneficial to reduce HF hospitalizations for patients with symptomatic (NYHA Class II-III) stable chronic HFrEF (LVEF 35%) who are receiving GDEM, including a beta-blocker at maximum tolerated dose, and who are in sinus rhythm with a heart rate of 70 bpm or greater at rest. Key: Heart Failure with reduced Ejection Fraction (HFrEF); New York Heart Association (NYHA); Left Ventricular Ejection Fraction (LVEF); Guideline directed evidence and management (GDEM); beats per minute (bpm) Yancy CW, Jessup M, Bozkurt B, et al. Circulation. 2016; 134(13);e ACC EXPERT CONSENSUS ON THE ROLE OF NON-STATIN THERAPY FOR HYPERLIPIDEMIA


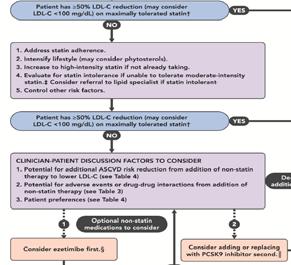
7 2013 ACC/AHA GUIDELINE REVIEW Used an evidence review based largely on RCT data. Central approach: To identify populations for whom benefit > risk for a given drug therapy. Clear net benefit with statin treatment for the 4 statin benefit groups. The amount of ASCVD risk reduction observed with statins was directly related to the amount of % LDL-C reduction from baseline. RCT data suggested: 50% LDL-C reduction with high-intensity statins; 30% to <50% reduction with moderate intensity statins No specific LDL-C targets to guide therapy; however majority of patients on high intensity statins had LDL-C level <100 mg/dl Consensus statement suggested these could be used as an indicator for adequate response and adherence to therapy. Stone NJ, Robinson JG, Lichtenstein AH, et al. J Am Coll Cardiol. 2014; 63: STATIN BENEFIT GROUPS Secondary Prevention Clinical ASCVD* Primary Prevention Adults with LDL 190 mg/dl Primary Prevention Diabetics, Age years & LDL mg/dl Primary Prevention Estimated 10- year ASCVD risk 7.5%, years old who have LDL *Atherosclerotic cardiovascular disease Requires risk discussion between clinician and patient before statin initiation Statin therapy may be considered if risk decision is uncertain after use of ASCVD risk calculator Stone NJ, Robinson JG, Lichtenstein AH, et al. J Am Coll Cardiol. 2014; 63: STATIN INTENSITY *Atherosclerotic cardiovascular disease Requires risk discussion between clinician and patient before statin initiation Statin therapy may be considered if risk decision is uncertain after use of ASCVD risk calculator *Individual responses to statin therapy varied in the RCTs and should be expected to vary in clinical practice. There might be a biologic basis for a less-than-average response. Evidence from 1 RCT only: down-titration if unable to tolerate atorvastatin 80 mg in IDEAL (Pedersen et al). Although simvastatin 80 mg was evaluated in RCTs, initiation of simvastatin 80 mg or titration to 80 mg is not recommended by the FDA due to the increased risk of myopathy, including rhabdomyolysis. 21 Stone NJ, Robinson JG, Lichtenstein AH, et al. J Am Coll Cardiol. 2014; 63:
8 USE OF NON-STATIN DRUGS IN 2013 ACC/AHA GUIDELINES At the time of the 2013 ACC/AHA Guideline publication: No data supporting the routine use of FDA-approved non-statin drugs combined with statin therapy for LDL-C reduction with the goal of further reducing ASCVD events. There were no published RCTs that assessed outcomes in statin-intolerant patients. (HPS2-THRIVE, IMPROVE-IT, PCSK9 inhibitor trials were ongoing) Therefore, the panel recommended: clinicians treating high-risk patients who have a less than-anticipated response to statins, who are unable to tolerate a less-than-recommended intensity of a statin, or who are completely statin intolerant, may consider the addition of a non-statin cholesterol lowering therapy. Stone NJ, Robinson JG, Lichtenstein AH, et al. J Am Coll Cardiol. 2014; 63: THE EXPERT CONSENSUS UPDATES Incorporate newer clinical trial data on niacin, ezetimibe, and the recently approved PCSK9 inhibitors to evidence base established by 2013 guideline. Provide practical guide for use of non-statin drugs for risk reduction in situations not covered by the 2013 ACC/AHA guideline. The process did not involve formal systematic reviews/evidence grading consensus statement. 23 COMPLETED TRIALS HPS2-THRIVE (NEJM 2014): in patients with clinical ASCVD: no benefit and significant harms from a long-acting niacin/laropiprant preparation in addition to simvastatin compared with simvastatin alone. IMPROVE-IT (NEJM 2015): in patients with recent ACS, addition of ezetimibe to simvastatin compared with statin monotherapy led to further reductions in LDL-C and statistically significant but clinically modest reduction in MACE over 7 years of follow up. FOURIER (NEJM 2017): in patients with established atherosclerotic cardiovascular disease, the addition of evolocumab on top of guideline directed statin therapy compared with statin monotherapy led to further reductions in LDL-C and statistically significant reductions in MACE over a period of 2.2 years. 24 8

9 KEY QUESTIONS ADDRESSED BY COMMITTEE 1) In what patient populations should non-statin therapies be considered? 2) In what situations should non-statin therapies be considered (i.e. when is the amount of LDL lowering less than anticipated, less than desired, or inadequate, and which treatment options should be considered in patients who are truly statin intolerant)? 3) If non-statin therapies are added, which agent or therapies should be considered and in what order? 25 APPROACHES TO STATIN INTOLERANCE Healthy lifestyle modification remains key to all patient groups (i.e., adhering to a heart healthy diet, regular exercise habits, avoidance of tobacco products, and maintenance of a healthy weight). Non-statin therapies are not considered to be an alternative evidence-based statin therapy. Statin intolerance should be systematically and rigorously evaluated and documented (i.e. obtain careful history; rule out other potential causes such as hypothyroidism, vitamin D deficiency, exercise; re-trial to verify recurrence of symptoms, etc). If unable to tolerate a statin then trial of lower doses/alternative statins and/or modified dosing intervals (i.e. every other day). 26 FACTORS TO CONSIDER WHEN USING NON-STATIN THERAPIES Pill Burden Available scientific evidence & clinical trials Adherence & lifestyle Preference in specific populations (i.e. pregnancy, elderly) Patient Preferences Efficacy & cost Drug-Drug interactions Safety & tolerability 27 9
10 I) In what patient populations should non-statin therapies be considered? QUESTIONS 1 AND 2 Numerous Algorithms Developed II) In what situations should non-statin therapies be considered? Adults 21 years old with clinical ASCVD, on Statin for Secondary Prevention Stable Clinical ASCVD without Comorbidities, on Statin for Secondary Prevention Clinical ASCVD with Comorbidities, on Statin for Secondary Prevention Clinical ASCVD and Baseline LDL 190 not due to Secondary Causes, on Statin for Secondary Prevention Adults 21 years old with LDL-C 190 not due to Secondary Causes, on Statin for Primary Prevention LDL-C 190 with Clinical ASCVD LDL-C 190 with or without Concomitant ASCVD Risk Factors Others (i.e. LDL-C 190 & Pregnancy; Familial Hyperlipidemia in Children/Adolescents, etc.) 28 QUESTION 3 3) If non-statin therapies are added, which agent or therapies should be considered and in what order? 29 NON-STATIN INTERVENTIONS **Referral to lipid specialist and dietitian Ezetimibe (Zetia ) PCSK9 Inhibitors (i.e. Alirocumab, Evolocumab) Phytosterols Soluble/Viscous Fiber Bile Acid Sequestrants (Colesevelam, Colestipol, etc) Mipomersen Lomitapide LDL apheresis 30 10

 for the treatment of patients with homozygous (HoFH) who require additional lowering of LDL-C.")

11 FDA APPROVED PCSK9 INHIBITORS Alirocumab is indicated as an adjunct to diet and maximally tolerated statin therapy for the treatment of adults with heterozygous familial (HeFH) or clinical atherosclerotic cardiovascular disease who require additional lowering of LDL-C. Evolocumab is indicated as an adjunct to diet and maximally tolerated statin therapy for the treatment of adults with heterozygous (HeFH) or clinical atherosclerotic cardiovascular disease who require additional lowering of LDL-C. Evolocumab is indicated as an adjunct to diet and other LDL-lowering therapies (e.g., statins, ezetimibe, LDL apheresis) for the treatment of patients with homozygous (HoFH) who require additional lowering of LDL-C. 31 LDL CLEARANCE ON HEPATIC SURFACE Plasma LDL Increased LDL-R surface concentration LDL LDL-R Clathrin vesicle Vesicle Lysosome LDL-R recycling Apo-B Hepatocyte Clathrin-coated vesicle Lysosomal degradation 1. Brown MS, et al. Proc Natl Acad Sci USA. 1979;76: Steinberg D, et al. Proc Natl Acad Sci USA. 2009;106: Brown MS, et al. Science. 1986;232: PCSK9 MECHANISM OF ACTION PCSK9 secretion LDL Decreased surface LDL-R PCSK9 Clathrin vesicle Lysosome Lysosomal degradation LDL-R/PCSK9 routed to lysosome Endosome 1. Horton JD, et al. J Lipid Res. 2009;50:S172-S Qian YW, et al. J Lipid Res. 2007;48: Zhang DW, et al. J Biol Chem. 2007; 282:


12

13

14 40 41 STABLE ASCVD ON STATIN (NO COMORBIDITIES) 42 14

15 CLINICAL ASCVD (LDL 190) ON STATIN 43 SUMMARY OF GUIDELINE UPDATES Ezetimibe is the first non-statin medication that should be considered in most patient scenarios, given its safety and tolerability, as well as demonstrated, though modest, efficacy when added to moderate-dose statin in one trial of patients with acute coronary syndrome. Bile acid sequestrants (BAS) may be considered as second-line therapy for patients in whom ezetimibe is not tolerated, but they should be avoided in patients with triglycerides >300 mg/dl. Alirocumab and Evolocumab : higher-risk patients with clinical ASCVD or familial hypercholesterolemia. Given the lack of long-term safety and efficacy data on these agents, they are not recommended for use in primary prevention patients in the absence of familial hypercholesterolemia. Don t recommend use of niacin given side effects/poor tolerability and data suggesting harm. For patients with HoFH or severe HeFH, referral to a lipid specialist is strongly recommended. Non-statin options include ezetimibe, BAS, PCSK-9 inhibitors with consideration for use of lomitapide, mipomerson, and LDL apheresis as necessary. 44 QUESTION 1 PT is a 59 year old man with a history of IV drug abuse who was found unconscious in the park. There was a bottle of oxycodone pills found immediately next to him. He is discovered to have a pulse but is not visibly breathing. BLS is instituted immediately until EMS arrives on the scene. Which of the following medications is included in the CPR guidelines as a reversal agent in those with known or suspected opioid overdose? A) Lidocaine B) Amiodarone C) Epinephrine D) Naloxone For patients with known or suspected opioid addiction who are unresponsive with no normal breathing but a pulse, it is reasonable for appropriately trained lay rescuers and BLS providers, in addition to providing standard BLS care, to administer intramuscular (IM) or intranasal (IN) naloxone (Class IIa, LOE-C-LD) 45 15
16 QUESTION 2 RS is a 67 year old man with a history of CAD s/p 4V CABG as well as NYHA Class III HFrEF (EF 25-30%) who presents to your clinic. His electrolytes and renal function are within normal limits. He is currently on lisinopril 40mg by mouth daily but is being switched by his cardiologist to Sacubitril/Valsartan. If he takes his lisinopril every morning. When should he take his first dose of Sacubitril/Valsartan? A) He may begin tonight after stopping Lisinopril B) He may begin tomorrow AM after stopping Lisinopril C) He should take it immediately and overlap with 1 dose of Lisinopril D) He should wait until at least tomorrow night after stopping Lisinopril COR LOE Recommendations III: Harm B-R ARNI should not be administered concomitantly with ACE-Is or within 36 hours of the last dose of an ACE-I. 46 QUESTION 3 Which of the following is a potential barrier to use of PCSK9 inhibitors? A) Must be injected everyday B) Lack of clinical outcomes C) Provides modest LDL lowering D) Potential to form drug neutralizing antibodies 47 ACKNOWLEDGEMENTS Salim Virani, M.D., Ph.D. Vijay Nambi, M.D., Ph.D. American College of Cardiology American Heart Association 48 16
17 QUESTIONS? 49 17
Deep Dive into Contemporary Cholesterol Management. Kim Allan Williams, Sr., MD, FACC Pamela B. Morris, MD, FACC 7 October 2016 Mexico City
 Deep Dive into Contemporary Cholesterol Management Kim Allan Williams, Sr., MD, FACC Pamela B. Morris, MD, FACC 7 October 2016 Mexico City Introduction: Pamela B. Morris, MD, FACC COMING TO CONSENSUS IN
Deep Dive into Contemporary Cholesterol Management Kim Allan Williams, Sr., MD, FACC Pamela B. Morris, MD, FACC 7 October 2016 Mexico City Introduction: Pamela B. Morris, MD, FACC COMING TO CONSENSUS IN
Case Studies The Role of Non-Statin Therapies for LDL-C Lowering in the Management of ASCVD Risk
 Case Studies The Role of Non-Statin Therapies for LDL-C Lowering in the Management of ASCVD Risk Kim K. Birtcher, PharmD, MS, AACC Clinical Professor University of Houston College of Pharmacy Houston,
Case Studies The Role of Non-Statin Therapies for LDL-C Lowering in the Management of ASCVD Risk Kim K. Birtcher, PharmD, MS, AACC Clinical Professor University of Houston College of Pharmacy Houston,
Dyslipidemia and Combination Therapy: A Framework for Clinical Decision Making
 Dyslipidemia and Combination Therapy: A Framework for Clinical Decision Making Shashank Sinha, MD Pamela B. Morris, MD, FACC 8 October 2016 Mexico City Introduction: Pamela B. Morris, MD, FACC COMING TO
Dyslipidemia and Combination Therapy: A Framework for Clinical Decision Making Shashank Sinha, MD Pamela B. Morris, MD, FACC 8 October 2016 Mexico City Introduction: Pamela B. Morris, MD, FACC COMING TO
The ACC Heart Failure Guidelines
 The ACC Heart Failure Guidelines Fakhr Alayoubi, Msc,R Ph President of SCCP Cardiology Clinical Pharmacist Assistant Professor At King Saud University King Khalid University Hospital Riyadh-KSA 2017 ACC/AHA/HFSA
The ACC Heart Failure Guidelines Fakhr Alayoubi, Msc,R Ph President of SCCP Cardiology Clinical Pharmacist Assistant Professor At King Saud University King Khalid University Hospital Riyadh-KSA 2017 ACC/AHA/HFSA
Managing Dyslipidemia and ASCVD Risk: Confusion, Controversy Consensus
 Managing Dyslipidemia and ASCVD Risk: Confusion, Controversy Consensus Pamela B. Morris, MD, FACC, FAHA, FASPC, FNLA Chair, ACC Prevention of Cardiovascular Disease Council and Section The Medical University
Managing Dyslipidemia and ASCVD Risk: Confusion, Controversy Consensus Pamela B. Morris, MD, FACC, FAHA, FASPC, FNLA Chair, ACC Prevention of Cardiovascular Disease Council and Section The Medical University
2017 Summer MAOFP Update
 2017 Summer MAOFP Update. Cardiology Update 2017 Landmark Trials Change Practice Guidelines David J. Strobl, DO, FNLA Heart Failure: Epidemiology More than 4 million patients affected 400,000 new cases
2017 Summer MAOFP Update. Cardiology Update 2017 Landmark Trials Change Practice Guidelines David J. Strobl, DO, FNLA Heart Failure: Epidemiology More than 4 million patients affected 400,000 new cases
Update in Cardiology What s Hot in 2017?
 Update in Cardiology What s Hot in 2017? Mark R. Milunski, MD, FACC, FACP Chief, Cardiology Section Orlando Veterans Affairs Medical Center Associate Professor of Medicine University of Central Florida
Update in Cardiology What s Hot in 2017? Mark R. Milunski, MD, FACC, FACP Chief, Cardiology Section Orlando Veterans Affairs Medical Center Associate Professor of Medicine University of Central Florida
4/24/15. AHA/ACC 2013 Guideline Key Points
 Review of the ACC/AHA 2013 Guidelines Anita Ralstin, MS, CNS, CNP Next Step Health Consultant, LLC 1! Discuss the rationale for the change in lipid guidelines and how that affects the decision to implement
Review of the ACC/AHA 2013 Guidelines Anita Ralstin, MS, CNS, CNP Next Step Health Consultant, LLC 1! Discuss the rationale for the change in lipid guidelines and how that affects the decision to implement
2017 ACC/AHA/HFSA Focused Update of the 2013 ACCF/AHA Guideline for the Management of Heart Failure
 2017 ACC/AHA/HFSA Focused Update of the 2013 ACCF/AHA Guideline for the Management of Heart Failure Developed in Collaboration With the American Academy of Family Physicians, American College of Chest
2017 ACC/AHA/HFSA Focused Update of the 2013 ACCF/AHA Guideline for the Management of Heart Failure Developed in Collaboration With the American Academy of Family Physicians, American College of Chest
ACLS/ACS Updates 2015
 ACLS/ACS Updates 2015 Advanced Cardiovascular Life Support by: Fareed Al Nozha, JBIM, ABIM, FKFSH&RC(Cardiology) Consultant Cardiologist Faculty, National CPR Committee, ACLS Program Head, SHA Dr Abdulhalim
ACLS/ACS Updates 2015 Advanced Cardiovascular Life Support by: Fareed Al Nozha, JBIM, ABIM, FKFSH&RC(Cardiology) Consultant Cardiologist Faculty, National CPR Committee, ACLS Program Head, SHA Dr Abdulhalim
REPATHA (PCSK9 INHIBITORS)
") REPATHA (PCSK9 INHIBITS) Indications: PCSK9 Inhibitors are indicated for treatment of adults with heterozygous familial hypercholesterolemia (HeFH) or clinical atherosclerotic cardiovascular disease as
REPATHA (PCSK9 INHIBITS) Indications: PCSK9 Inhibitors are indicated for treatment of adults with heterozygous familial hypercholesterolemia (HeFH) or clinical atherosclerotic cardiovascular disease as
PCSK9 Inhibitors: Promise or Pitfall?
 PCSK9 Inhibitors: Promise or Pitfall? Tracy Harlan, PharmD PGY2 Ambulatory Care Resident University of Iowa Hospitals and Clinics tracy harlan@uiowa.edu Tracy Harlan does not have any actual or potential
PCSK9 Inhibitors: Promise or Pitfall? Tracy Harlan, PharmD PGY2 Ambulatory Care Resident University of Iowa Hospitals and Clinics tracy harlan@uiowa.edu Tracy Harlan does not have any actual or potential
Long-Term Care Updates
 Long-Term Care Updates July 2015 By Amy Friedman Wilson, PharmD Heart failure (HF) is a clinical condition in which ventricular filling or ejection of blood is structurally or functionally impaired. 1
Long-Term Care Updates July 2015 By Amy Friedman Wilson, PharmD Heart failure (HF) is a clinical condition in which ventricular filling or ejection of blood is structurally or functionally impaired. 1
Drug Class Monograph
 Drug Class Monograph Class: Proprotein Convertase Subtilisin/Kexin Type 9 (PCSK9) Inhibitor Drugs: Praluent (alirocumab), Repatha (evolocumab) Line of Business: Medi-Cal Effective Date: February 17, 2016
Drug Class Monograph Class: Proprotein Convertase Subtilisin/Kexin Type 9 (PCSK9) Inhibitor Drugs: Praluent (alirocumab), Repatha (evolocumab) Line of Business: Medi-Cal Effective Date: February 17, 2016
What Role do the New PCSK9 Inhibitors Have in Lipid Lowering Treatment?
 What Role do the New PCSK9 Inhibitors Have in Lipid Lowering Treatment? Jennifer G. Robinson, MD, MPH Professor, Departments of Epidemiology & Medicine Director, Prevention Intervention Center University
What Role do the New PCSK9 Inhibitors Have in Lipid Lowering Treatment? Jennifer G. Robinson, MD, MPH Professor, Departments of Epidemiology & Medicine Director, Prevention Intervention Center University
UnitedHealthcare Pharmacy Clinical Pharmacy Programs
 UnitedHealthcare Pharmacy Clinical Pharmacy Programs Program Number 2017 P 2063-8 Program Prior Authorization/Medical Necessity Medication Repatha (evolocumab) P&T Approval Date 5/2015, 9/2015, 11/2015,
UnitedHealthcare Pharmacy Clinical Pharmacy Programs Program Number 2017 P 2063-8 Program Prior Authorization/Medical Necessity Medication Repatha (evolocumab) P&T Approval Date 5/2015, 9/2015, 11/2015,
It is the policy of health plans affiliated with PA Health & Wellness that Vytorin is medically necessary when the following criteria are met:
 Clinical Policy: Ezetimibe and Simvastatin (Vytorin) Reference Number: PA.CP.PMN.77 Effective Date: 02.01.17 Last Review Date: 07.18 Revision Log Description Ezetimibe/simvastatin (Vytorin ) contains ezetimibe,
Clinical Policy: Ezetimibe and Simvastatin (Vytorin) Reference Number: PA.CP.PMN.77 Effective Date: 02.01.17 Last Review Date: 07.18 Revision Log Description Ezetimibe/simvastatin (Vytorin ) contains ezetimibe,
Reducing Cardiovascular Risk Through Non-Statins. Kim K. Birtcher, PharmD Joseph Saseen, PharmD
 Reducing Cardiovascular Risk Through Non-Statins Kim K. Birtcher, PharmD Joseph Saseen, PharmD Target Audience: Pharmacists ACPE#: 0202-0000-18-049-L01-P Activity Type: Application-based This activity
Reducing Cardiovascular Risk Through Non-Statins Kim K. Birtcher, PharmD Joseph Saseen, PharmD Target Audience: Pharmacists ACPE#: 0202-0000-18-049-L01-P Activity Type: Application-based This activity
2015 Interim Training Materials
 2015 Interim Training Materials ACLS Manual and ACLS EP Manual Comparison Chart Assessment sequence Manual, Part 2: The Systematic Approach, and Part BLS Changes The HCP should check for response while
2015 Interim Training Materials ACLS Manual and ACLS EP Manual Comparison Chart Assessment sequence Manual, Part 2: The Systematic Approach, and Part BLS Changes The HCP should check for response while
Disclosures. Overview. Goal statement. Advances in Chronic Heart Failure Management 5/22/17
 Disclosures Advances in Chronic Heart Failure Management I have nothing to disclose Van N Selby, MD UCSF Advanced Heart Failure Program May 22, 2017 Goal statement To review recently-approved therapies
Disclosures Advances in Chronic Heart Failure Management I have nothing to disclose Van N Selby, MD UCSF Advanced Heart Failure Program May 22, 2017 Goal statement To review recently-approved therapies
What s new in the 2017 heart failure guidelines. Prof.Dr.Mehmet Birhan YILMAZ, FESC, FACC, FHFA
 What s new in the 2017 heart failure guidelines Prof.Dr.Mehmet Birhan YILMAZ, FESC, FACC, FHFA Key points to remember 2017 guidelines recommend using natriuretic peptides as biomarkers to screen for heart
What s new in the 2017 heart failure guidelines Prof.Dr.Mehmet Birhan YILMAZ, FESC, FACC, FHFA Key points to remember 2017 guidelines recommend using natriuretic peptides as biomarkers to screen for heart
B. Patient has not reached the percentage reduction goal with statin therapy
 Managing Cardiovascular Risk: The Importance of Lowering LDL Cholesterol and Reaching Treatment Goals for LDL Cholesterol The Role of the Pharmacist Learning Objectives 1. Review the role of lipid levels
Managing Cardiovascular Risk: The Importance of Lowering LDL Cholesterol and Reaching Treatment Goals for LDL Cholesterol The Role of the Pharmacist Learning Objectives 1. Review the role of lipid levels
HYPERLIPIDEMIA IN THE OLDER POPULATION NICOLE SLATER, PHARMD, BCACP AUBURN UNIVERSITY, HARRISON SCHOOL OF PHARMACY JULY 16, 2016
 HYPERLIPIDEMIA IN THE OLDER POPULATION NICOLE SLATER, PHARMD, BCACP AUBURN UNIVERSITY, HARRISON SCHOOL OF PHARMACY JULY 16, 2016 NOTHING TO DISCLOSE I, Nicole Slater, have no actual or potential conflict
HYPERLIPIDEMIA IN THE OLDER POPULATION NICOLE SLATER, PHARMD, BCACP AUBURN UNIVERSITY, HARRISON SCHOOL OF PHARMACY JULY 16, 2016 NOTHING TO DISCLOSE I, Nicole Slater, have no actual or potential conflict
Pamela B. Morris, MD, FACC, FAHA, FASPC, FNLA
 2017 Focused Update of the 2016 ACC Expert Consensus Decision Pathway on the Role of Non-statin Therapies for LDL-C Lowering in the Management of ASCVD Risk Pamela B. Morris, MD, FACC, FAHA, FASPC, FNLA
2017 Focused Update of the 2016 ACC Expert Consensus Decision Pathway on the Role of Non-statin Therapies for LDL-C Lowering in the Management of ASCVD Risk Pamela B. Morris, MD, FACC, FAHA, FASPC, FNLA
ADMINISTRATIVE POLICY AND PROCEDURE
 ADMINISTRATIVE POLICY PROCEDURE Policy #: Subject: PCSK9 INHIBITS (ex: Repatha) Section: Care Management Effective Date: January 1, 2015 Revision Date(s): NA Review Date(s): NA Responsible Parties: Patryce
ADMINISTRATIVE POLICY PROCEDURE Policy #: Subject: PCSK9 INHIBITS (ex: Repatha) Section: Care Management Effective Date: January 1, 2015 Revision Date(s): NA Review Date(s): NA Responsible Parties: Patryce
Request for Prior Authorization for PCSK9 inhibitor therapy Website Form Submit request via: Fax
 Request for Prior Authorization for PCSK9 inhibitor therapy Website Form www.highmarkhealthoptions.com Submit request via: Fax - 1-855-476-4158 PCSK9 is a protein that reduces the hepatic removal of low-density
Request for Prior Authorization for PCSK9 inhibitor therapy Website Form www.highmarkhealthoptions.com Submit request via: Fax - 1-855-476-4158 PCSK9 is a protein that reduces the hepatic removal of low-density
PCSK9 Agents Drug Class Prior Authorization Protocol
 PCSK9 Agents Drug Class Prior Authorization Protocol Line of Business: Medicaid P & T Approval Date: February 21, 2018 Effective Date: April 1, 2018 This policy has been developed through review of medical
PCSK9 Agents Drug Class Prior Authorization Protocol Line of Business: Medicaid P & T Approval Date: February 21, 2018 Effective Date: April 1, 2018 This policy has been developed through review of medical
HEART FAILURE: PHARMACOTHERAPY UPDATE
 HEART FAILURE: PHARMACOTHERAPY UPDATE 3 HEART FAILURE REVIEW 1 5.1 million x1.25 = 6.375 million 40 years old = MICHAEL F. AKERS, PHARM.D. CLINICAL PHARMACIST CENTRACARE HEALTH, ST. CLOUD HOSPITAL HF Diagnosis
HEART FAILURE: PHARMACOTHERAPY UPDATE 3 HEART FAILURE REVIEW 1 5.1 million x1.25 = 6.375 million 40 years old = MICHAEL F. AKERS, PHARM.D. CLINICAL PHARMACIST CENTRACARE HEALTH, ST. CLOUD HOSPITAL HF Diagnosis
Disclosures. Advances in Chronic Heart Failure Management 6/12/2017. Van N Selby, MD UCSF Advanced Heart Failure Program June 19, 2017
 Advances in Chronic Heart Failure Management Van N Selby, MD UCSF Advanced Heart Failure Program June 19, 2017 I have nothing to disclose Disclosures 1 Goal statement To review recently-approved therapies
Advances in Chronic Heart Failure Management Van N Selby, MD UCSF Advanced Heart Failure Program June 19, 2017 I have nothing to disclose Disclosures 1 Goal statement To review recently-approved therapies
1/4/18. Heart Failure Guideline Review and Update. Disclosure. Pharmacist Objectives. Pharmacy Technician Objectives. What is Heart Failure?
 Disclosure Heart Failure Guideline Review and Update I have had no financial relationship over the past 12 months with any commercial sponsor with a vested interest in this presentation. Natalie Beiter,
Disclosure Heart Failure Guideline Review and Update I have had no financial relationship over the past 12 months with any commercial sponsor with a vested interest in this presentation. Natalie Beiter,
2013 Cholesterol Guidelines. Anna Broz MSN, RN, CNP, AACC Adult Certified Nurse Practitioner North Ohio Heart, Inc.
 2013 Cholesterol Guidelines Anna Broz MSN, RN, CNP, AACC Adult Certified Nurse Practitioner North Ohio Heart, Inc. Disclosures Speaker Gilead Sciences NHLBI Charge to the Expert Panel Evaluate higher quality
2013 Cholesterol Guidelines Anna Broz MSN, RN, CNP, AACC Adult Certified Nurse Practitioner North Ohio Heart, Inc. Disclosures Speaker Gilead Sciences NHLBI Charge to the Expert Panel Evaluate higher quality
IOWA MEDICAID DRUG UTILIZATION REVIEW COMMISSION 100 Army Post Road (515)
") IOWA MEDICAID DRUG UTILIZATION REVIEW COMMISSION 100 Army Post Road (515) 974-3131 -866-626-0216 Brett Faine, Pharm.D. Larry Ambroson, R.Ph. Brian Couse, M.D. Professional Staff: Mark Graber, M.D., FACEP,
IOWA MEDICAID DRUG UTILIZATION REVIEW COMMISSION 100 Army Post Road (515) 974-3131 -866-626-0216 Brett Faine, Pharm.D. Larry Ambroson, R.Ph. Brian Couse, M.D. Professional Staff: Mark Graber, M.D., FACEP,
Clinical Policy: Lomitapide (Juxtapid) Reference Number: ERX.SPA.170 Effective Date:
 Reference Number: ERX.SPA.170 Effective Date:") Clinical Policy: (Juxtapid) Reference Number: ERX.SPA.170 Effective Date: 01.11.17 Last Review Date: 11.17 Revision Log See Important Reminder at the end of this policy for important regulatory and legal
Clinical Policy: (Juxtapid) Reference Number: ERX.SPA.170 Effective Date: 01.11.17 Last Review Date: 11.17 Revision Log See Important Reminder at the end of this policy for important regulatory and legal
Updates in Congestive Heart Failure
 Updates in Congestive Heart Failure GREGORY YOST, DO JOHNSTOWN CARDIOVASCULAR ASSOCIATES 1/28/2018 Disclosures Edwards speaker on Sapien3 valves (TAVR) Stages A-D and NYHA Classes I-IV Stage A: High risk
Updates in Congestive Heart Failure GREGORY YOST, DO JOHNSTOWN CARDIOVASCULAR ASSOCIATES 1/28/2018 Disclosures Edwards speaker on Sapien3 valves (TAVR) Stages A-D and NYHA Classes I-IV Stage A: High risk
Pharmacy Management Drug Policy
 SUBJECT: ; Praluent (alirocumab), Repatha (evolocumab) POLICY NUMBER: Pharmacy-61 EFFECTIVE DATE: 8/15 LAST REVIEW DATE: 9/22/2017 If the member s subscriber contract excludes coverage for a specific service
SUBJECT: ; Praluent (alirocumab), Repatha (evolocumab) POLICY NUMBER: Pharmacy-61 EFFECTIVE DATE: 8/15 LAST REVIEW DATE: 9/22/2017 If the member s subscriber contract excludes coverage for a specific service
What do the guidelines say about combination therapy?
 What do the guidelines say about combination therapy? Christie M. Ballantyne, MD Center for Cardiovascular Disease Prevention Methodist DeBakey Heart & Vascular Center Baylor College of Medicine Houston,
What do the guidelines say about combination therapy? Christie M. Ballantyne, MD Center for Cardiovascular Disease Prevention Methodist DeBakey Heart & Vascular Center Baylor College of Medicine Houston,
Drug Prior Authorization Guideline PCSK9 Inhibitors -
 Drug Prior Authorization Guideline PCSK9 Inhibitors - REPATHA (evolocumab) PRALUENT (alirocumab) PA9911 Covered Service: Yes when meets criteria below Prior Authorization Required: Yes-as shown below Additional
Drug Prior Authorization Guideline PCSK9 Inhibitors - REPATHA (evolocumab) PRALUENT (alirocumab) PA9911 Covered Service: Yes when meets criteria below Prior Authorization Required: Yes-as shown below Additional
Disclosures. This speaker has indicated there are no relevant financial relationships to be disclosed.
 Disclosures This speaker has indicated there are no relevant financial relationships to be disclosed. And the Beat Goes On: New Medications for Heart Failure Alison M. Walton, PharmD, BCPS The Case of
Disclosures This speaker has indicated there are no relevant financial relationships to be disclosed. And the Beat Goes On: New Medications for Heart Failure Alison M. Walton, PharmD, BCPS The Case of
A Report of the American College of Cardiology Task Force on Clinical Expert Consensus Documents
 JOURNAL OF THE AMERICAN COLLEGE OF CARDIOLOGY VOL. 68, NO. 1, 2016 ª 2016 BY THE AMERICAN COLLEGE OF CARDIOLOGY FOUNDATION ISSN 0735-1097/$36.00 PUBLISHED BY ELSEVIER http://dx.doi.org/10.1016/j.jacc.2016.03.519
JOURNAL OF THE AMERICAN COLLEGE OF CARDIOLOGY VOL. 68, NO. 1, 2016 ª 2016 BY THE AMERICAN COLLEGE OF CARDIOLOGY FOUNDATION ISSN 0735-1097/$36.00 PUBLISHED BY ELSEVIER http://dx.doi.org/10.1016/j.jacc.2016.03.519
2013 Cholesterol Guidelines. Anna Broz MSN, RN, CNP, AACC Cer=fied Adult Nurse Prac==oner North Ohio Heart, Inc.
 2013 Cholesterol Guidelines Anna Broz MSN, RN, CNP, AACC Cer=fied Adult Nurse Prac==oner North Ohio Heart, Inc. Disclosures Speaker Gilead Sciences NHLBI Charge to the Expert Panel Evaluate higher quality
2013 Cholesterol Guidelines Anna Broz MSN, RN, CNP, AACC Cer=fied Adult Nurse Prac==oner North Ohio Heart, Inc. Disclosures Speaker Gilead Sciences NHLBI Charge to the Expert Panel Evaluate higher quality
UnitedHealthcare Pharmacy Clinical Pharmacy Programs
 UnitedHealthcare Pharmacy Clinical Pharmacy Programs Program Number 2017 P 2062-8 Program Prior Authorization/Medical Necessity Medication Praluent (alirocumab) P&T Approval Date 5/2015, 8/2015, 9/2015,
UnitedHealthcare Pharmacy Clinical Pharmacy Programs Program Number 2017 P 2062-8 Program Prior Authorization/Medical Necessity Medication Praluent (alirocumab) P&T Approval Date 5/2015, 8/2015, 9/2015,
Saudi Heart Failure Guidelines. Waleed AlHabeeb, MD, MHA Consultant Heart Failure Cardiologist President of the Saudi Heart Failure Group
 Saudi Heart Failure Guidelines Waleed AlHabeeb, MD, MHA Consultant Heart Failure Cardiologist President of the Saudi Heart Failure Group Heart Failure Expert committee The Heart Failure Expert Committee,
Saudi Heart Failure Guidelines Waleed AlHabeeb, MD, MHA Consultant Heart Failure Cardiologist President of the Saudi Heart Failure Group Heart Failure Expert committee The Heart Failure Expert Committee,
Checklist for Treating Heart Failure. Alan M. Kaneshige MD, FACC, FASE Oklahoma Heart Institute
 Checklist for Treating Heart Failure Alan M. Kaneshige MD, FACC, FASE Oklahoma Heart Institute Novartis Disclosure Heart Failure (HF) a complex clinical syndrome that arises secondary to abnormalities
Checklist for Treating Heart Failure Alan M. Kaneshige MD, FACC, FASE Oklahoma Heart Institute Novartis Disclosure Heart Failure (HF) a complex clinical syndrome that arises secondary to abnormalities
Clinical Policy: Evolocumab (Repatha) Reference Number: ERX.SPMN.184 Effective Date: 01/2017
 Reference Number: ERX.SPMN.184 Effective Date: 01/2017") Clinical Policy: (Repatha) Reference Number: ERX.SPMN.184 Effective Date: 01/2017 Last Review Date: Revision Log See Important Reminder at the end of this policy for important regulatory and legal information.
Clinical Policy: (Repatha) Reference Number: ERX.SPMN.184 Effective Date: 01/2017 Last Review Date: Revision Log See Important Reminder at the end of this policy for important regulatory and legal information.
Medical Policy An independent licensee of the Blue Cross Blue Shield Association
 Neprilysin Inhibitor (Entresto ) Page 1 of 6 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: Neprilysin Inhibitor (Entresto ) Prime Therapeutics will review Prior
Neprilysin Inhibitor (Entresto ) Page 1 of 6 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: Neprilysin Inhibitor (Entresto ) Prime Therapeutics will review Prior
Clinical Policy: Mipomersen (Kynamro) Reference Number: ERX.SPMN.186 Effective Date: 01/2017
 Reference Number: ERX.SPMN.186 Effective Date: 01/2017") Clinical Policy: (Kynamro) Reference Number: ERX.SPMN.186 Effective Date: 01/2017 Last Review Date: Revision Log See Important Reminder at the end of this policy for important regulatory and legal information.
Clinical Policy: (Kynamro) Reference Number: ERX.SPMN.186 Effective Date: 01/2017 Last Review Date: Revision Log See Important Reminder at the end of this policy for important regulatory and legal information.
Heart Failure Therapies State of the Art 2017
 Heart Failure Therapies State of the Art 2017 Andrew J. Sauer, MD Assistant Professor Director, Center for Heart Failure Medical Director, Heart Transplantation UNOS Primary Transplant Physician asauer@kumc.edu
Heart Failure Therapies State of the Art 2017 Andrew J. Sauer, MD Assistant Professor Director, Center for Heart Failure Medical Director, Heart Transplantation UNOS Primary Transplant Physician asauer@kumc.edu
Confusion about guidelines: How should we treat lipids?
 Confusion about guidelines: How should we treat lipids? Anne Carol Goldberg, MD, FACP, FAHA, FNLA Professor of Medicine Washington University School of Medicine American College of Physicians Missouri
Confusion about guidelines: How should we treat lipids? Anne Carol Goldberg, MD, FACP, FAHA, FNLA Professor of Medicine Washington University School of Medicine American College of Physicians Missouri
EVOLOCUMAB Generic Brand HICL GCN Exception/Other EVOLOCUMAB REPATHA 42378
 Generic Brand HICL GCN Exception/Other EVOLOCUMAB REPATHA 42378 This drug requires a written request for prior authorization. All requests for Repatha (evolocumab) require review by a pharmacist prior
Generic Brand HICL GCN Exception/Other EVOLOCUMAB REPATHA 42378 This drug requires a written request for prior authorization. All requests for Repatha (evolocumab) require review by a pharmacist prior
Lipid Guidelines Who, What, and How Low. Anita Ralstin, MS, CNP Next Step Health Consultant, LLC New Mexico Heart Institute
 Lipid Guidelines Who, What, and How Low Anita Ralstin, MS, CNP Next Step Health Consultant, LLC New Mexico Heart Institute Disclosures! None Objectives! List factors used in screening for dyslipidemia
Lipid Guidelines Who, What, and How Low Anita Ralstin, MS, CNP Next Step Health Consultant, LLC New Mexico Heart Institute Disclosures! None Objectives! List factors used in screening for dyslipidemia
Pharmacy Policy Bulletin
 Pharmacy Policy Bulletin Title: Policy #: PCSK9 inhibitors Rx.01.170 Application of pharmacy policy is determined by benefits and contracts. Benefits may vary based on product line, group, or contract.
Pharmacy Policy Bulletin Title: Policy #: PCSK9 inhibitors Rx.01.170 Application of pharmacy policy is determined by benefits and contracts. Benefits may vary based on product line, group, or contract.
Lipid Therapy: Statins and Beyond. Ivan Anderson, MD RIHVH Cardiology
 Lipid Therapy: Statins and Beyond Ivan Anderson, MD RIHVH Cardiology Outline The cholesterol hypothesis and lipid metabolism The Guidelines 4 Groups that Benefit from Lipid therapy Initiation and monitoring
Lipid Therapy: Statins and Beyond Ivan Anderson, MD RIHVH Cardiology Outline The cholesterol hypothesis and lipid metabolism The Guidelines 4 Groups that Benefit from Lipid therapy Initiation and monitoring
Lipids & Hypertension Update
 Lipids & Hypertension Update No financial disclosures Michael W. Cullen, MD, FACC Senior Associate Consultant, Assistant Professor of Medicine Mayo Clinic Department of Cardiovascular Diseases 34 th Annual
Lipids & Hypertension Update No financial disclosures Michael W. Cullen, MD, FACC Senior Associate Consultant, Assistant Professor of Medicine Mayo Clinic Department of Cardiovascular Diseases 34 th Annual
The 2015 BLS & ACLS Guideline Updates What Does the Future Hold?
 The 2015 BLS & ACLS Guideline Updates What Does the Future Hold? Greater Kansas City Chapter Of AACN 2016 Visions Critical Care Conference Nicole Kupchik RN, MN, CCNS, CCRN, PCCN, CMC Independent CNS/Staff
The 2015 BLS & ACLS Guideline Updates What Does the Future Hold? Greater Kansas City Chapter Of AACN 2016 Visions Critical Care Conference Nicole Kupchik RN, MN, CCNS, CCRN, PCCN, CMC Independent CNS/Staff
Neprilysin Inhibitor (Entresto ) Prior Authorization and Quantity Limit Program Summary
 Prior Authorization and Quantity Limit Program Summary") Neprilysin Inhibitor (Entresto ) Prior Authorization and Quantity Limit Program Summary FDA APPROVED INDICATIONS DOSAGE 1 Indication Entresto Reduce the risk of cardiovascular (sacubitril/valsartan) death
Neprilysin Inhibitor (Entresto ) Prior Authorization and Quantity Limit Program Summary FDA APPROVED INDICATIONS DOSAGE 1 Indication Entresto Reduce the risk of cardiovascular (sacubitril/valsartan) death
Disclosures. Objectives 2/11/2017
 Role of Non-Statin Therapy in CV Risk Reduction James A. Underberg, MD, MS, FACPM, FACP, FASH, FNLA,FASPC Clinical Assistant Professor of Medicine NYU School of Medicine NYU Langone Center for Cardiovascular
Role of Non-Statin Therapy in CV Risk Reduction James A. Underberg, MD, MS, FACPM, FACP, FASH, FNLA,FASPC Clinical Assistant Professor of Medicine NYU School of Medicine NYU Langone Center for Cardiovascular
Get a Statin or Not? Learning objectives. Presentation overview 4/3/2018. Treatment Strategies in Dyslipidemia Management
 Get a Statin or Not? Treatment Strategies in Dyslipidemia Management Michelle Chu, PharmD, BCACP, CDE Assistant Professor of Clinical Pharmacy, USC School of Pharmacy Sahar Dagher, PharmD Virtual Care
Get a Statin or Not? Treatment Strategies in Dyslipidemia Management Michelle Chu, PharmD, BCACP, CDE Assistant Professor of Clinical Pharmacy, USC School of Pharmacy Sahar Dagher, PharmD Virtual Care
Learning Objectives. Patient Case
 Joseph Saseen, Pharm.D., FASHP, FCCP, BCPS Professor and Vice Chair, Department of Clinical Pharmacy University of Colorado Anschutz Medical Campus Learning Objectives Identify the 4 patient populations
Joseph Saseen, Pharm.D., FASHP, FCCP, BCPS Professor and Vice Chair, Department of Clinical Pharmacy University of Colorado Anschutz Medical Campus Learning Objectives Identify the 4 patient populations
Clinical Practice Guideline
 Clinical Practice Guideline Secondary Prevention for Patients with Coronary and Other Vascular Disease Since the 2001 update of the American Heart Association (AHA)/American College of Cardiology (ACC)
Clinical Practice Guideline Secondary Prevention for Patients with Coronary and Other Vascular Disease Since the 2001 update of the American Heart Association (AHA)/American College of Cardiology (ACC)
2014 Update in Medicine Update in Cholesterol Management. Donald L. Lappé MD, FACC, FAHA October 31, 2014
 2014 Update in Medicine Update in Cholesterol Management Donald L. Lappé MD, FACC, FAHA October 31, 2014 2013 ACC/AHA Guideline on the Treatment of Blood Cholesterol to Reduce Atherosclerotic Cardiovascular
2014 Update in Medicine Update in Cholesterol Management Donald L. Lappé MD, FACC, FAHA October 31, 2014 2013 ACC/AHA Guideline on the Treatment of Blood Cholesterol to Reduce Atherosclerotic Cardiovascular
Repatha. Repatha (evolocumab) Description
 Description") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.16.08 Subject: Repatha Page: 1 of 8 Last Review Date: September 18, 2015 Repatha Description Repatha
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.16.08 Subject: Repatha Page: 1 of 8 Last Review Date: September 18, 2015 Repatha Description Repatha
Lipid Management: The Next Level How Will the New ACC/AHA Guidelines Change My Practice
 Lipid Management: The Next Level How Will the New ACC/AHA Guidelines Change My Practice Vera Bittner, MD, MSPH Professor of Medicine Section Head, Preventive Cardiology Medical Director, Cardiac Rehabilitation
Lipid Management: The Next Level How Will the New ACC/AHA Guidelines Change My Practice Vera Bittner, MD, MSPH Professor of Medicine Section Head, Preventive Cardiology Medical Director, Cardiac Rehabilitation
Clinical Policy: Mipomersen (Kynamro) Reference Number: ERX.SPA.171 Effective Date:
 Reference Number: ERX.SPA.171 Effective Date:") Clinical Policy: (Kynamro) Reference Number: ERX.SPA.171 Effective Date: 01.11.17 Last Review Date: 08.18 Revision Log See Important Reminder at the end of this policy for important regulatory and legal
Clinical Policy: (Kynamro) Reference Number: ERX.SPA.171 Effective Date: 01.11.17 Last Review Date: 08.18 Revision Log See Important Reminder at the end of this policy for important regulatory and legal
Lipid Management C. Samuel Ledford, MD Interventional Cardiology Chattanooga Heart Institute
 Lipid Management 2018 C. Samuel Ledford, MD Interventional Cardiology Chattanooga Heart Institute Disclosures No Financial Disclosures Disclosures I am an Interventional Cardiologist I put STENTS in for
Lipid Management 2018 C. Samuel Ledford, MD Interventional Cardiology Chattanooga Heart Institute Disclosures No Financial Disclosures Disclosures I am an Interventional Cardiologist I put STENTS in for
Congestive Heart Failure: Outpatient Management
 The Chattanooga Heart Institute Cardiovascular Symposium Congestive Heart Failure: Outpatient Management E. Philip Lehman MD, MPP Disclosure No financial disclosures. Objectives Evidence-based therapy
The Chattanooga Heart Institute Cardiovascular Symposium Congestive Heart Failure: Outpatient Management E. Philip Lehman MD, MPP Disclosure No financial disclosures. Objectives Evidence-based therapy
PCSK9 Inhibitors Are They Worth The Money? Michael J. Blaha MD MPH
 PCSK9 Inhibitors Are They Worth The Money? Michael J. Blaha MD MPH Presented by: Michael J. Blaha November 16, 2017 1 Financial Disclosures Grants: Amgen Foundation, Aetna Foundation Advisory Boards: Amgen,
PCSK9 Inhibitors Are They Worth The Money? Michael J. Blaha MD MPH Presented by: Michael J. Blaha November 16, 2017 1 Financial Disclosures Grants: Amgen Foundation, Aetna Foundation Advisory Boards: Amgen,
Prevention Updates and Paradigm Shifts
 Prevention Updates and Paradigm Shifts Andrew Freeman, MD, FACC Director of Clinical Cardiology and Operations National Jewish Health Assistant Professor of Medicine National Jewish Health and University
Prevention Updates and Paradigm Shifts Andrew Freeman, MD, FACC Director of Clinical Cardiology and Operations National Jewish Health Assistant Professor of Medicine National Jewish Health and University
Heart.org/HFGuidelinesToolkit
 2017 /H/HFS Focused Update of the 2013 F/H 6.3.1 Biomarkers for Prevention: Recommendation OR LOE Recommendation a For patients at risk of developing HF, natriuretic peptide biomarker-based screening followed
2017 /H/HFS Focused Update of the 2013 F/H 6.3.1 Biomarkers for Prevention: Recommendation OR LOE Recommendation a For patients at risk of developing HF, natriuretic peptide biomarker-based screening followed
See Important Reminder at the end of this policy for important regulatory and legal information.
 Clinical Policy: (Vytorin) Reference Number: CP.PMN.77 Effective Date: 02.01.17 Last Review Date: 02.18 Line of Business: Commercial, Medicaid Revision Log See Important Reminder at the end of this policy
Clinical Policy: (Vytorin) Reference Number: CP.PMN.77 Effective Date: 02.01.17 Last Review Date: 02.18 Line of Business: Commercial, Medicaid Revision Log See Important Reminder at the end of this policy
See Important Reminder at the end of this policy for important regulatory and legal information.
 Clinical Policy: (Repatha) Reference Number: HIM.PA.SP46 Effective Date: 01.01.18 Last Review Date: Line of Business: Health Insurance Marketplace Revision Log See Important Reminder at the end of this
Clinical Policy: (Repatha) Reference Number: HIM.PA.SP46 Effective Date: 01.01.18 Last Review Date: Line of Business: Health Insurance Marketplace Revision Log See Important Reminder at the end of this
Ask the Experts: Clinical Case Studies Focusing on Non-statin Therapies for Treating Patients with Hypercholesterolemia
 Ask the Experts: Clinical Case Studies Focusing on Non-statin Therapies for Treating Patients with Hypercholesterolemia Presented as a Live Webinar Wednesday, March 1, 2017 1:00 p.m. 2:00 p.m. ET On-demand
Ask the Experts: Clinical Case Studies Focusing on Non-statin Therapies for Treating Patients with Hypercholesterolemia Presented as a Live Webinar Wednesday, March 1, 2017 1:00 p.m. 2:00 p.m. ET On-demand
Management Strategies for Advanced Heart Failure
 Management Strategies for Advanced Heart Failure Mary Norine Walsh, MD, FACC Medical Director, HF and Cardiac Transplantation St Vincent Heart Indianapolis, IN USA President American College of Cardiology
Management Strategies for Advanced Heart Failure Mary Norine Walsh, MD, FACC Medical Director, HF and Cardiac Transplantation St Vincent Heart Indianapolis, IN USA President American College of Cardiology
Conflicts of interest. What's the Skinny on the Lipid Guidelines? Key Differences. Are you applying the new ACC/AHA Lipid guidelines in your practice?
 Conflicts of interest What's the Skinny on the Lipid Guidelines? The presenter has no relevant conflicts of interest to disclose. Kathleen Vest, PharmD, CDE, BCACP At the end of this presentation, pharmacist
Conflicts of interest What's the Skinny on the Lipid Guidelines? The presenter has no relevant conflicts of interest to disclose. Kathleen Vest, PharmD, CDE, BCACP At the end of this presentation, pharmacist
Current Cholesterol Guidelines and Treatment of Residual Risk COPYRIGHT. J. Peter Oettgen, MD
 Current Cholesterol Guidelines and Treatment of Residual Risk J. Peter Oettgen, MD Associate Professor of Medicine Harvard Medical School Director, Preventive Cardiology Beth Israel Deaconess Medical Center
Current Cholesterol Guidelines and Treatment of Residual Risk J. Peter Oettgen, MD Associate Professor of Medicine Harvard Medical School Director, Preventive Cardiology Beth Israel Deaconess Medical Center
2016 Update to Heart Failure Clinical Practice Guidelines
 2016 Update to Heart Failure Clinical Practice Guidelines Mitchell T. Saltzberg, MD, FACC, FAHA, FHFSA Medical Director of Advanced Heart Failure Froedtert & Medical College of Wisconsin Stages, Phenotypes
2016 Update to Heart Failure Clinical Practice Guidelines Mitchell T. Saltzberg, MD, FACC, FAHA, FHFSA Medical Director of Advanced Heart Failure Froedtert & Medical College of Wisconsin Stages, Phenotypes
Clinical Policy: Evolocumab (Repatha) Reference Number: CP.CPA.269 Effective Date: Last Review Date: Line of Business: Commercial
 Reference Number: CP.CPA.269 Effective Date: Last Review Date: Line of Business: Commercial") Clinical Policy: (Repatha) Reference Number: CP.CPA.269 Effective Date: 11.16.16 Last Review Date: 11.17 Line of Business: Commercial Revision Log See Important Reminder at the end of this policy for important
Clinical Policy: (Repatha) Reference Number: CP.CPA.269 Effective Date: 11.16.16 Last Review Date: 11.17 Line of Business: Commercial Revision Log See Important Reminder at the end of this policy for important
PCSK9 Inhibitors Current Status
 PCSK9 Inhibitors Current Status Ryan T. Whitney, MD FACC Bryan Heart Fall Conference 2015 Disclosures, Conflicts, and Nefarious Connections I own no stock in the companies mentioned in this talk. I am
PCSK9 Inhibitors Current Status Ryan T. Whitney, MD FACC Bryan Heart Fall Conference 2015 Disclosures, Conflicts, and Nefarious Connections I own no stock in the companies mentioned in this talk. I am
Management of chronic heart failure: pharmacology. Giuseppe M.C. Rosano, MD, PhD, FHFA
 Management of chronic heart failure: pharmacology. Giuseppe M.C. Rosano, MD, PhD, FHFA Declaration of potential conflict of interests Type of job or financial support Salary Ordinary funds Position in
Management of chronic heart failure: pharmacology. Giuseppe M.C. Rosano, MD, PhD, FHFA Declaration of potential conflict of interests Type of job or financial support Salary Ordinary funds Position in
Statin Intolerance. Jason Evanchan DO, FACC April 20 th, 2018
 Statin Intolerance 2 nd Annual CV Course for Trainees and Early Career Physicians: Current Concepts in the Diagnosis and Management of Coronary Artery Disease Jason Evanchan DO, FACC April 20 th, 2018
Statin Intolerance 2 nd Annual CV Course for Trainees and Early Career Physicians: Current Concepts in the Diagnosis and Management of Coronary Artery Disease Jason Evanchan DO, FACC April 20 th, 2018
2/10/2016. Perspectives on the 2013 ACC/AHA Cholesterol Guidelines. Disclosures. ATP-III Update 2004
 Perspectives on the 2013 ACC/AHA Cholesterol Guidelines Donald M. Lloyd-Jones, MD ScM Senior Associate Dean Chair and Professor of Preventive Medicine Northwestern Feinberg School of Medicine Disclosures
Perspectives on the 2013 ACC/AHA Cholesterol Guidelines Donald M. Lloyd-Jones, MD ScM Senior Associate Dean Chair and Professor of Preventive Medicine Northwestern Feinberg School of Medicine Disclosures
4 th and Goal To Go How Low Should We Go? :
 4 th and Goal To Go How Low Should We Go? : Evaluating New Lipid Lowering Therapies Catherine Bourg Rebitch, PharmD, BCACP Clinical Associate Professor Disclosure The presenter has nothing to disclose
4 th and Goal To Go How Low Should We Go? : Evaluating New Lipid Lowering Therapies Catherine Bourg Rebitch, PharmD, BCACP Clinical Associate Professor Disclosure The presenter has nothing to disclose
High ( 50%) Restrictions mg 20-40mg PA; TS ⱡ 15 ⱡ
 Restrictions mg 20-40mg PA; TS ⱡ 15 ⱡ") MEDICATION COVERAGE POLICY PHARMACY AND THERAPEUTICS ADVISORY COMMITTEE POLICY: Cholesterol P&T DATE: 5/9/2017 THERAPEUTIC CLASS: Cardiovascular REVIEW HISTORY: 5/16, 5/15, 2/14, 5/12, LOB AFFECTED: Medi-Cal
MEDICATION COVERAGE POLICY PHARMACY AND THERAPEUTICS ADVISORY COMMITTEE POLICY: Cholesterol P&T DATE: 5/9/2017 THERAPEUTIC CLASS: Cardiovascular REVIEW HISTORY: 5/16, 5/15, 2/14, 5/12, LOB AFFECTED: Medi-Cal
PCSK9 INHIBITORS NEW DRUGS IN CARDIOLOGY 7/6/ ANNUAL MEETING OBJECTIVES PCSK9 AND HYPERCHOLESTEROLEMIA PRESENTATION OUTLINE
 NEW DRUGS IN CARDIOLOGY LORI FIALLO, PHARMD.,BCPS AQ-CARDIOLOGY PCSK9 INHIBITORS OBJECTIVES Identify recent FDA approvals in cardiology Describe the impact of recent FDA approvals on current practice Design
NEW DRUGS IN CARDIOLOGY LORI FIALLO, PHARMD.,BCPS AQ-CARDIOLOGY PCSK9 INHIBITORS OBJECTIVES Identify recent FDA approvals in cardiology Describe the impact of recent FDA approvals on current practice Design
Medical Policy An independent licensee of the Blue Cross Blue Shield Association
 Proprotein Convertase Subtilisin/kexin type 9 Page 1 of 24 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: Proprotein Convertase Subtilisin/kexin type 9 (PCSK9)
Proprotein Convertase Subtilisin/kexin type 9 Page 1 of 24 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: Proprotein Convertase Subtilisin/kexin type 9 (PCSK9)
New Cardiovascular Drugs 2015 CAM F. CAMPBELL MD FACC MERCY CARDIOLOGY 2/6/2015
 New Cardiovascular Drugs 2015 CAM F. CAMPBELL MD FACC MERCY CARDIOLOGY 2/6/2015 Disclosures Financial: None Personal: Married, 4 children, 2 grandchildren, 1 grandchild on the way Trivia: I have sailed
New Cardiovascular Drugs 2015 CAM F. CAMPBELL MD FACC MERCY CARDIOLOGY 2/6/2015 Disclosures Financial: None Personal: Married, 4 children, 2 grandchildren, 1 grandchild on the way Trivia: I have sailed
PCSK9 Inhibitors Current Status
 PCSK9 Inhibitors Current Status Ryan T. Whitney, MD FACC Bryan Heart Spring Conference 2016 Disclosures, Conflicts, and Nefarious Connections I own no stock in the companies mentioned in this talk. I am
PCSK9 Inhibitors Current Status Ryan T. Whitney, MD FACC Bryan Heart Spring Conference 2016 Disclosures, Conflicts, and Nefarious Connections I own no stock in the companies mentioned in this talk. I am
Repatha. Repatha (evolocumab) Description
 Description") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.40.08 Subject: Repatha Page: 1 of 8 Last Review Date: December 2, 2016 Repatha Description Repatha (evolocumab)
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.40.08 Subject: Repatha Page: 1 of 8 Last Review Date: December 2, 2016 Repatha Description Repatha (evolocumab)
THE 2013 ACC/AHA GUIDELINES ON THE TREATMENT OF BLOOD CHOLESTEROL
 THE 2013 ACC/AHA GUIDELINES ON THE TREATMENT OF BLOOD CHOLESTEROL Anne Carol Goldberg, MD, FACP, FAHA, FNLA Associate Professor of Medicine Washington University School of Medicine National Lipid Association
THE 2013 ACC/AHA GUIDELINES ON THE TREATMENT OF BLOOD CHOLESTEROL Anne Carol Goldberg, MD, FACP, FAHA, FNLA Associate Professor of Medicine Washington University School of Medicine National Lipid Association
Heart Failure: Guideline-Directed Management and Therapy
 Heart Failure: Guideline-Directed Management and Therapy Guideline-Directed Management and Therapy (GDMT) was developed by the American College of Cardiology and American Heart Association to define the
Heart Failure: Guideline-Directed Management and Therapy Guideline-Directed Management and Therapy (GDMT) was developed by the American College of Cardiology and American Heart Association to define the
High ( 50%) Restrictions mg 20-40mg Simvastatin (Zocor) 10mg 20-40mg $1.66 Pravastatin (Pravachol) mg $6.
 Restrictions mg 20-40mg Simvastatin (Zocor) 10mg 20-40mg $1.66 Pravastatin (Pravachol) mg $6.") MEDICATION COVERAGE POLICY PHARMACY AND THERAPEUTICS ADVISORY COMMITTEE POLICY: Cholesterol P&T DATE: 5/8/2018 THERAPEUTIC CLASS: Cardiovascular REVIEW HISTORY: 5/17, 5/16, 5/15, 2/14, LOB AFFECTED: Medi-Cal
MEDICATION COVERAGE POLICY PHARMACY AND THERAPEUTICS ADVISORY COMMITTEE POLICY: Cholesterol P&T DATE: 5/8/2018 THERAPEUTIC CLASS: Cardiovascular REVIEW HISTORY: 5/17, 5/16, 5/15, 2/14, LOB AFFECTED: Medi-Cal
SECONDARY PREVENTION OF CORONARY HEART DISEASE AND ISCHAEMIC STROKE/TIA
 PRIMARY PREVENTION OF CHD AND STROKE IN HIGH RISK PATIENTS Random non fasting test for total cholesterol, HDL cholesterol (TC:HDL ratio) and LFTs If cholesterol > 7.5 mmol/l or LDL C 5mmol/l exclude secondary
PRIMARY PREVENTION OF CHD AND STROKE IN HIGH RISK PATIENTS Random non fasting test for total cholesterol, HDL cholesterol (TC:HDL ratio) and LFTs If cholesterol > 7.5 mmol/l or LDL C 5mmol/l exclude secondary
Initiating New Medications in the Management of Heart Failure
 Initiating New Medications in the Management of Heart Failure Sandra Oliver-McNeil DNP, MSN, ACNP-BC, CHFN Associate Professor (Clinical) Wayne State University College of Nursing Objectives The participant
Initiating New Medications in the Management of Heart Failure Sandra Oliver-McNeil DNP, MSN, ACNP-BC, CHFN Associate Professor (Clinical) Wayne State University College of Nursing Objectives The participant
Cardiac Drugs - The Missing Links (Drugs we should have in New Zealand)
") Pharmac: Devices and Drugs Heart drugs the missing links John Elliott Chairs: Rob Doughty & Rajesh Nair Cardiac Drugs - The Missing Links (Drugs we should have in New Zealand) John Elliott University of
Pharmac: Devices and Drugs Heart drugs the missing links John Elliott Chairs: Rob Doughty & Rajesh Nair Cardiac Drugs - The Missing Links (Drugs we should have in New Zealand) John Elliott University of
When Statins Aren t Enough: Appropriate Therapies for High-Risk Patients with Diabetes
 When Statins Aren t Enough: Appropriate Therapies for High-Risk Patients with Diabetes Kim K. Birtcher, MS, PharmD, AACC, FNLA, CLS, BCPS (AQ-Cardiology), CDE Clinical Professor University of Houston College
When Statins Aren t Enough: Appropriate Therapies for High-Risk Patients with Diabetes Kim K. Birtcher, MS, PharmD, AACC, FNLA, CLS, BCPS (AQ-Cardiology), CDE Clinical Professor University of Houston College
Strategies for Managing Dyslipidemia Patients with Residual CVD Risk
 Strategies for Managing Dyslipidemia Patients with Residual CVD Risk Acknowledgements We acknowledge the work of Lynne T. Braun, PhD, CNP, FAHA, FPCNA, FAAN in the development of this presentation. Disclosures:
Strategies for Managing Dyslipidemia Patients with Residual CVD Risk Acknowledgements We acknowledge the work of Lynne T. Braun, PhD, CNP, FAHA, FPCNA, FAAN in the development of this presentation. Disclosures:
2013 ACC/AHA Cholesterol Guidelines JULIE HAMMOND, D.O. PGY-2 MATTHEW PAOLI, D.O. PGY-2
 2013 ACC/AHA Cholesterol Guidelines JULIE HAMMOND, D.O. PGY-2 MATTHEW PAOLI, D.O. PGY-2 GOALS ACC/AHA as publisher of guidelines Determining which patients are appropriate for statin therapy The treatment
2013 ACC/AHA Cholesterol Guidelines JULIE HAMMOND, D.O. PGY-2 MATTHEW PAOLI, D.O. PGY-2 GOALS ACC/AHA as publisher of guidelines Determining which patients are appropriate for statin therapy The treatment
Evolving Concepts on Lipid Management from Ezetimibe (IMPROVE IT) to PCSK9 Inhibitors
 to PCSK9 Inhibitors") Evolving Concepts on Lipid Management from Ezetimibe (IMPROVE IT) to PCSK9 Inhibitors Sidney C. Smith, Jr. MD, FACC, FAHA, FESC Professor of Medicine/Cardiology University of North Carolina at Chapel Hill
Evolving Concepts on Lipid Management from Ezetimibe (IMPROVE IT) to PCSK9 Inhibitors Sidney C. Smith, Jr. MD, FACC, FAHA, FESC Professor of Medicine/Cardiology University of North Carolina at Chapel Hill
Lipid Control Today: Management within the Context of other Cardiovascular Risk Factors
 Best Practices Lipid Control Today: Management within the Context of other Cardiovascular Risk Factors James A. Underberg, MD, MS, FACPM, FACP, FASH, FNLA, FASPC Lipidology & Cardiovascular Disease Prevention
Best Practices Lipid Control Today: Management within the Context of other Cardiovascular Risk Factors James A. Underberg, MD, MS, FACPM, FACP, FASH, FNLA, FASPC Lipidology & Cardiovascular Disease Prevention
Clinical Policy: Evolocumab (Repatha) Reference Number: ERX.SPA.169 Effective Date:
 Reference Number: ERX.SPA.169 Effective Date:") Clinical Policy: (Repatha) Reference Number: ERX.SPA.169 Effective Date: 01.11.17 Last Review Date: 11.17 Revision Log See Important Reminder at the end of this policy for important regulatory and legal
Clinical Policy: (Repatha) Reference Number: ERX.SPA.169 Effective Date: 01.11.17 Last Review Date: 11.17 Revision Log See Important Reminder at the end of this policy for important regulatory and legal