Michigan Society of Echocardiography 30 th Year Jubilee
|
|
|
- Delphia West
- 6 years ago
- Views:
Transcription

1 Michigan Society of Echocardiography 30 th Year Jubilee Stress Echocardiography in Valvular Heart Disease Moving Beyond CAD Karthik Ananthasubramaniam, MD FRCP (Glas) FACC FASE FASNC Associate Professor of Medicine Wayne State University Director, Echocardiography and Nuclear Cardiology Program Director, Advanced Cardiac Imaging Fellowship Edith and Benson Ford Heart and Vascular Institute Dept of Medicine, Henry Ford Hospital
2 Disclosures Research Grants : Astellas Pharma Global Development, Inc GE Healthcare Trovis Pharmaceuticals Glaxo-Smith-Kline Speakers Bureau/Honoraria : Astellas Pharma US Inc Lantheus Medical Imaging Consultant/Advisory Board : Lantheus Medical Imaging Astellas Pharma Global Development, Inc No conflicts of interest for this talk
3 Stress Echo in Valve Disease Who needs testing? What test to do? What parameters to measure and focus on? How to use the information in patient management?


4 Exertional dyspnea Pulmonary hypertension Coronary artery disease Stress Doppler Echo Mitral valve disease Aortic valve disease Cardiomyopathy Prosthetic valves

5 Superiority of Stress Echocardiography over ANY OTHER MODALITY Diagnostic Evaluation and Planning strategies for Management in 1Co-existing Valvular Heart Disease 2. Dynamic obstructive disease, 3. Unexplained dyspnea, correlating 4. Exercise hemodynamics to function, pressures and diastology

6 Exercise Vs Bicycle Echo
7 Management strategy for patients with severe aortic stenosis Bonow, R. O. et al. J Am Coll Cardiol 2006;48:e1-e148 Copyright 2006 American College of Cardiology Foundation. Restrictions may apply.
8 Exercise Test in AS : Clinical and EKG Amato et al Heart 2001 ST depression and outcomes Das et al, Eur Heart J 2005 Symptoms and outcomes
9 Exercise Echo and Outcomes in AS Role of Gradient and EF Reserve Lancelloti et al Circulation 2005 Marechaux et al Echocardiography 2007
10

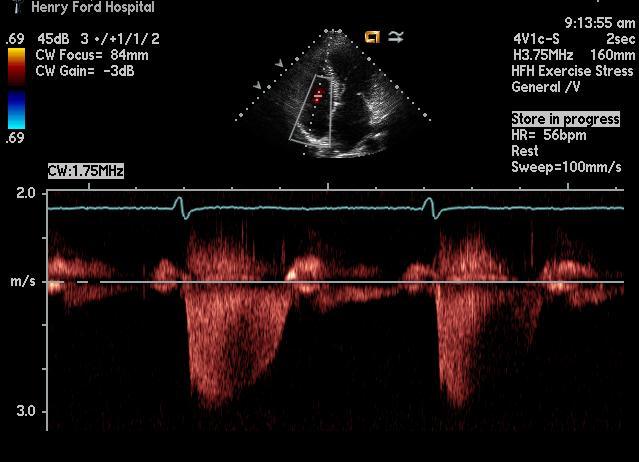
11 Exercise Echo in AS
12 Stress Data AORTIC STENOSIS Clinical Parameters Symptoms BP response Impact on Outcome Impact on AVR ESC versus ACC guidelines Onset of symptoms indaily life, cardiac death, AVR ESC 1 ESC 2A ACC 2b ACC 2b EKG Vent Arrhythmias ST depression Onset of symptoms in daily life, cardiac death, AVR ESC 2B Echo Increase in mean gradient > 18 ; > 20 mm hg Spontaneous symptoms, cardiac death, AVR Decrease or minimal increase in EF Spontaneous symptoms, cardiac death, AVR
13 Caveats Increase in transvalvular gradient may not always correlate with presence or onset of symptoms during stress echo in AS Transvalvular gradient depends on 1.severity of AS at rest 2.aortic valve compliance 3.concomitant CAD 4.LV contractile reserve 5.duration of exercise 6.maximal heart rate 7.workload achieved

14 Newer Stress Parameters in AS Tissue Doppler and Stress Echocardiography Van Pelt et al Heart 2007 Lack of substantial increase in S between rest and exercise as a sign of LV contractile abnormality in AS Correlates with BNP, exercise duration and increase in systolic pressure
15
16 Some Formulas EOA ( proj) = EOA res + Valve compliance x ( 250- Q rest ) Valve compliance =slope of the regression equation of the EOA to flow rate( mil/sec) or absolute increase in AVA with dobutamine infusion / increase in flow rate Valve resistance = 1333 x mean gradient / flow rate = SV/ejection time) Stroke work loss = 100 x ( mean gradient /mean gradient +systolic pressure )
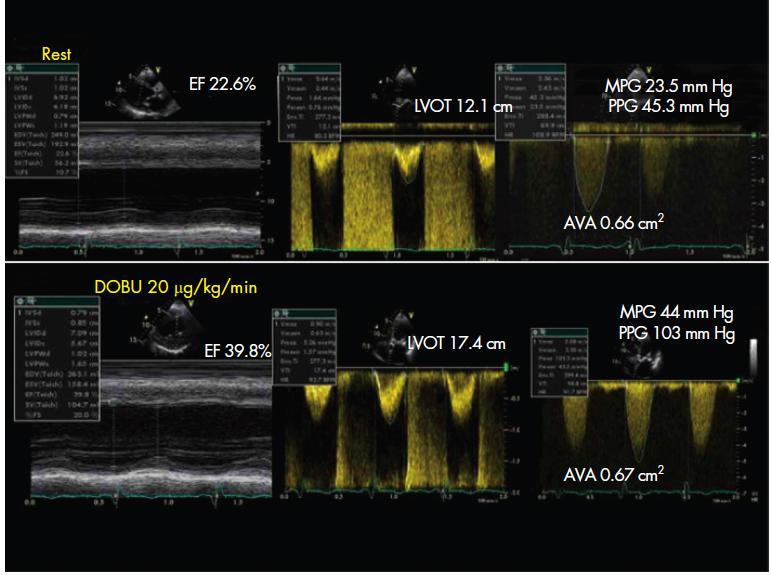
17 Low Flow/Low-Gradient AS Class IIa 1 Dobutamine stress echocardiography is reasonable to evaluate patients with lowflow/low-gradient AS and LV dysfunction. (Level of Evidence: B) 2 Cardiac catheterization for hemodynamic measurements with infusion of dobutamine can be useful for evaluation of patients with lowflow/low-gradient AS and LV dysfunction. (Level of Evidence: C)



18 Low Flow Low Gradient AS Role of Phamacologic Stress Echo AVA < 1 sq cm MG : <30-<40 mm hg EF < 40%
19
20 DSE in Low Flow Low Gradient AS and Normal Ejection Fraction 1. Increasingly recognized and challenging entity 2. EF >/= 50%, low mean gradients < 30 mm hg, AVA < 1 sq cm 3. Low indexed stroke volume, < 35ml/sqm, small concentric remodelled ventricles 4. Important to rule out technical errors prior to making the diagnosis. Consider EOA projected, Zva, Energy Loss index 5.? Role of Dobutamine challenge to increase CO to differentiate
21 Indications MITRAL STENOSIS Stress Data Parameters Impact on Outcome Impact of decision making ESC and ACC Guidlelines Asymptomatic MS ( MVA < 1.5 sq cm ) Clinical Echo Symptoms or PASP > 60 mm hg exercise testing` ESC 2A ACC1 ACC 1 Symptomatic MS ( MVA < 1.5 sq cm) Echo PASP > 60 or mean mitral gradient> 15 mm hg with exercise Mean mitral gradient > 20 mm hg with DSE Clinical deterioration and need for surgery ACC 2b ACC 2b
22
23 At rest there is significant overlap of gradients in patients with varying severity of MS Exercise echo helps to further stratify patients based on their severity Cheriex et al In Jnl of Cardiol 1994

24 Stress Echo in MS


25 Stress Echo in MS CAVEATS 1. Atrial fibrillation : importance of averaging 2. Avoidance of use of pressure half time which can be shortened with tachycardia 3. Presence of cocomitant mitral regurgitation which may increase gradient and PA pressure

26 Exercise Echo in MS

27 Semi supine Bike

28 Stress Echo and Mitral Regurgitation Known Severe MR 1. Look for Exercise capacity 2. Pulmonary HTN new / worse 3. LV response Mild or No MR and Unexplained Dyspnea, Pulmonary HTN 1. Exercise capacity 2. New or worsening MR 3. Worsening Pul HTN 4. LV response
29

30
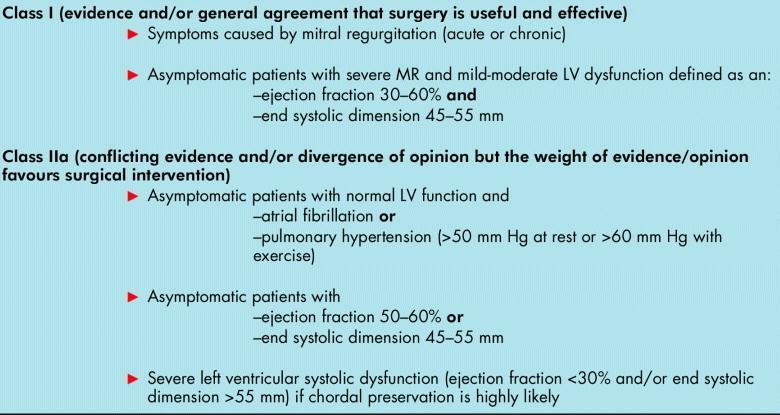
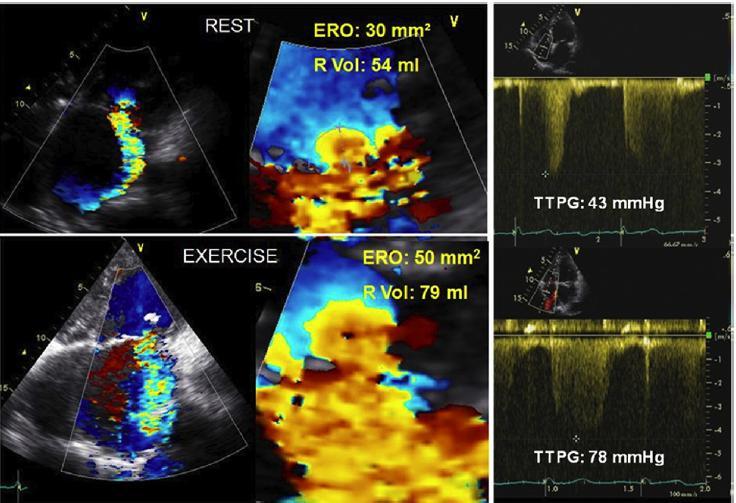
31 Indications MITRAL REGURGITATION Asymptomatic MR Stress Data Parameters Impact on Outcome Clinical -Exercise capacity -Symptoms Development of symptoms Impact of decision making ESC and ACC Guidelines Echo PASP > 60 mm hg with exercise testing` Increase in ERO >/=10 sq mm reduced symptom free survival post-op LV dysfunction ACC 2A Increase in EF < 4 % Increase in LVESV index > 25ml/sq m increase in GLS < 1.9% cardiac morbidity deterioration of LV function Symptomatic MR Echo PASP > 60mm hg ACC 2b Severe MR during exercise
32

33 Stress Echo in Ischemic MR LV Parameters Mitral Valve Deformation Parameters MR Parameters LVEDV LVESV LV EF Regional wall thickening Color TDI for dyssynchrony Mitral annulus tenting area Coapation distance ERO Regurgitant volume MR ERO changes with exercise correlate with exercise transtricuspid pressure gradient and increased ERO with exercise correlates with MACE in patients with LV dysfunction and mild MR at rest Exercise echo can unmask severe MR and marked increase in PASP in patients with dyspnea and mild MR. ERO at rest does not correlate with dynamic changes in ERO with exercise Lebrun F et al JACC 2001
34 Determinants of MV Dynamics Characteristics of Exercise Induced Functional MR (FMR) 1. Greatly varies among patients 2. Des not correlated with FMR at rest 3. Does not correlate with LV dysfunction 4. Mainly correlates with changes in mitral valve deformation 5. Affected by local rather than global LV function and remodelling 6. Favorably affected by recruitable contractile reserve

35 Functional Mitral Regurgitation : Interplay of Dynamics
36

37 Exercise echo in Functional MR

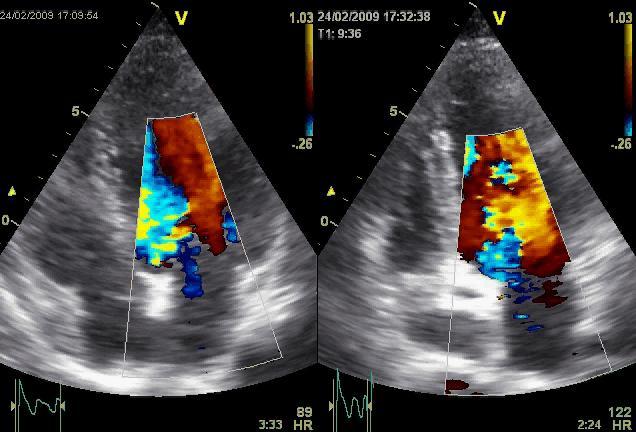
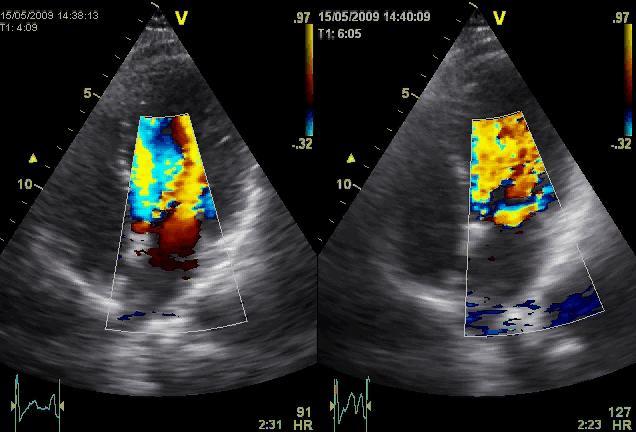
38 Rest Stress Rest Stress Rest Stress


39 Stress Echo PE=pulmonary edema FMR=functional MR Bigi et al Cardiovascular Ultrasound 2009
40

41

42 Stress Echo in AI
43 Stress Echo And Prosthetic Valves Normal prosthetic valves inherently stenotic due to small EOA Type of prosthesis : mechanical versus bioprosthetic /stentless location and annulus size ( aortic) determine gradients Resting gradients tend to overlap for normal and abnormal functioning prosthesis many times In general gradients across prosthetic valves will increase depending on transvalvular flow rate The exaggerated /absolute percentage of increase maybe the most important factor provided by stress echo
44 Evaluation of St Jude and Medtronic Hall Prosthesis By Stress Echo Small size of aortic prosthesis technical factors contributing to increased gradients across aortic prosthesis Note that normal functioning aortic prosthesis can have substantial increases in gradient with exercise Circulation 1989; 80;116-23
45 Exercise Gradients in MS and Post MVR with Normal Prosthetic function JACC 1991;17; Normal increase of TMG is mild with no or mild increase in EOA by P1/2 time. A 100% or greater increase is likely pathological van de Brink et al Am J Cardiol 1992
46


47 Stress Echo in HOCM REST STRESS



48 REST STRESS Kay Role of Stress Echo in HCM: provocation, hemodynamics, arrhythmias, worsening MR

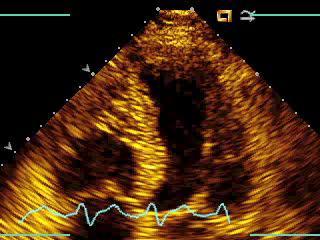
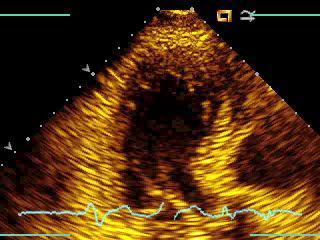
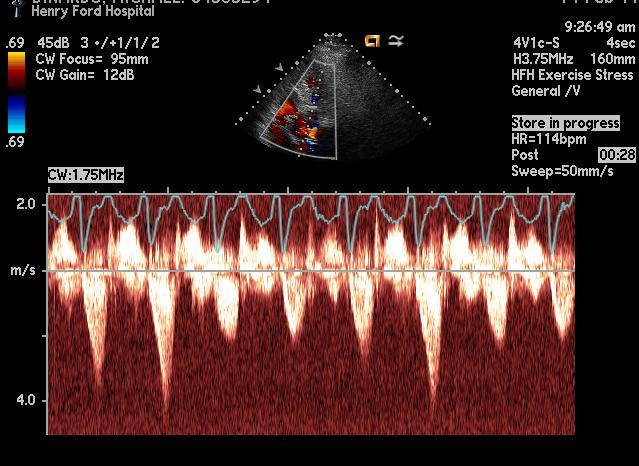
49 Exercise Echo and Dyspnea Evaluation In Chronic Lung Disease normal patients chronic lung disease and normal resting PA pressures chronic lung disease and abnormal resting PA pressures Imp : regardless of PASP pts with chronic lung disease have exercise induced increase in PASP reflecting abnormal PVR

50 Exercise Echo in Dyspnea Evaluation
51


52 Dynamic Diastology with Exercise E E E/E Normal DFP DFP diastolic filling pressure
53 THANK YOU
Michigan Society of Echocardiography ECHO IN SLOPES How We Do It? Accelerated Dobutamine Echocardiography Henry Ford Initial Experience
 Michigan Society of Echocardiography ECHO IN SLOPES 2012 How We Do It? Accelerated Dobutamine Echocardiography Henry Ford Initial Experience Karthik Ananthasubramaniam, MD FRCP FACC FASE FASNC Associate
Michigan Society of Echocardiography ECHO IN SLOPES 2012 How We Do It? Accelerated Dobutamine Echocardiography Henry Ford Initial Experience Karthik Ananthasubramaniam, MD FRCP FACC FASE FASNC Associate
Low Gradient Severe AS: Who Qualifies for TAVR? Andrzej Boguszewski MD, FACC, FSCAI Vice Chairman, Cardiology Mid-Michigan Health Associate Professor
 Low Gradient Severe AS: Who Qualifies for TAVR? Andrzej Boguszewski MD, FACC, FSCAI Vice Chairman, Cardiology Mid-Michigan Health Associate Professor Michigan State University, Central Michigan University
Low Gradient Severe AS: Who Qualifies for TAVR? Andrzej Boguszewski MD, FACC, FSCAI Vice Chairman, Cardiology Mid-Michigan Health Associate Professor Michigan State University, Central Michigan University
Low Gradient Severe? AS
 Low Gradient Severe? AS Philippe Pibarot, DVM, PhD, FACC, FAHA, FESC, FASE Canada Research Chair in Valvular Heart Diseases Institut Universitaire de Cardiologie et de Pneumologie de Québec / Québec Heart
Low Gradient Severe? AS Philippe Pibarot, DVM, PhD, FACC, FAHA, FESC, FASE Canada Research Chair in Valvular Heart Diseases Institut Universitaire de Cardiologie et de Pneumologie de Québec / Québec Heart
Comprehensive Echo Assessment of Aortic Stenosis
 Comprehensive Echo Assessment of Aortic Stenosis Smonporn Boonyaratavej, MD, MSc King Chulalongkorn Memorial Hospital Bangkok, Thailand Management of Valvular AS Medical and interventional approaches to
Comprehensive Echo Assessment of Aortic Stenosis Smonporn Boonyaratavej, MD, MSc King Chulalongkorn Memorial Hospital Bangkok, Thailand Management of Valvular AS Medical and interventional approaches to
Stress Testing in Valvular Disease
 2017 ASE Florida Orlando, FL October 10, 2017 2:40 2:50 PM 10 min Grand Harbor Ballroom South Stress Testing in Valvular Disease Muhamed Sarić MD, PhD, MPA Director of Noninvasive Cardiology Echo Lab Associate
2017 ASE Florida Orlando, FL October 10, 2017 2:40 2:50 PM 10 min Grand Harbor Ballroom South Stress Testing in Valvular Disease Muhamed Sarić MD, PhD, MPA Director of Noninvasive Cardiology Echo Lab Associate
ECHO HAWAII. Role of Stress Echo in Valvular Heart Disease. Not only ischemia! Cardiomyopathy. Prosthetic Valve. Diastolic Dysfunction
 Role of Stress Echo in Valvular Heart Disease ECHO HAWAII January 15 19, 2018 Kenya Kusunose, MD, PhD, FASE Tokushima University Hospital Japan Not only ischemia! Cardiomyopathy Prosthetic Valve Diastolic
Role of Stress Echo in Valvular Heart Disease ECHO HAWAII January 15 19, 2018 Kenya Kusunose, MD, PhD, FASE Tokushima University Hospital Japan Not only ischemia! Cardiomyopathy Prosthetic Valve Diastolic
Valvular Guidelines: The Past, the Present, the Future
 Valvular Guidelines: The Past, the Present, the Future Robert O. Bonow, MD, MS Northwestern University Feinberg School of Medicine Bluhm Cardiovascular Institute Northwestern Memorial Hospital Editor-in-Chief,
Valvular Guidelines: The Past, the Present, the Future Robert O. Bonow, MD, MS Northwestern University Feinberg School of Medicine Bluhm Cardiovascular Institute Northwestern Memorial Hospital Editor-in-Chief,
Exercise Testing/Echocardiography in Asymptomatic AS
 Exercise Testing/Echocardiography in Asymptomatic AS Raluca Dulgheru, MD Heart Valve Clinic, University of Liège, CHU Sart Tilman, BELGIUM Disclosure related to this presentation: None VALVULAR HEART DISEASE
Exercise Testing/Echocardiography in Asymptomatic AS Raluca Dulgheru, MD Heart Valve Clinic, University of Liège, CHU Sart Tilman, BELGIUM Disclosure related to this presentation: None VALVULAR HEART DISEASE
MAKING SENSE OF MODERATE GRADIENTS IN PATIENTS WITH SYMPTOMATIC AORTIC STENOSIS
 MAKING SENSE OF MODERATE GRADIENTS IN PATIENTS WITH SYMPTOMATIC AORTIC STENOSIS David A. Orsinelli, MD, FACC, FASE Professor, Internal Medicine Director, Structural Heart Imaging The Ohio State University
MAKING SENSE OF MODERATE GRADIENTS IN PATIENTS WITH SYMPTOMATIC AORTIC STENOSIS David A. Orsinelli, MD, FACC, FASE Professor, Internal Medicine Director, Structural Heart Imaging The Ohio State University
Μαρία Μπόνου Διευθύντρια ΕΣΥ, ΓΝΑ Λαϊκό
 Μαρία Μπόνου Διευθύντρια ΕΣΥ, ΓΝΑ Λαϊκό Diastolic HF DD: Diastolic Dysfunction DHF: Diastolic HF HFpEF: HF with preserved EF DD Pathophysiologic condition: impaired relaxation, LV compliance, LV filling
Μαρία Μπόνου Διευθύντρια ΕΣΥ, ΓΝΑ Λαϊκό Diastolic HF DD: Diastolic Dysfunction DHF: Diastolic HF HFpEF: HF with preserved EF DD Pathophysiologic condition: impaired relaxation, LV compliance, LV filling
«Paradoxical» low-flow, low-gradient AS with preserved LV function: A Silent Killer
 «Paradoxical» low-flow, low-gradient AS with preserved LV function: A Silent Killer Philippe Pibarot, DVM, PhD, FACC, FAHA, FESC, FASE Canada Research Chair in Valvular Heart Diseases Université LAVAL
«Paradoxical» low-flow, low-gradient AS with preserved LV function: A Silent Killer Philippe Pibarot, DVM, PhD, FACC, FAHA, FESC, FASE Canada Research Chair in Valvular Heart Diseases Université LAVAL
Natural History and Echo Evaluation of Aortic Stenosis
 Natural History and Echo Evaluation of Aortic Stenosis Prof. Patrizio LANCELLOTTI, MD, PhD Heart Valve Clinic, University of Liège, CHU Sart Tilman, Liège, BELGIUM AORTIC STENOSIS First valvular disease
Natural History and Echo Evaluation of Aortic Stenosis Prof. Patrizio LANCELLOTTI, MD, PhD Heart Valve Clinic, University of Liège, CHU Sart Tilman, Liège, BELGIUM AORTIC STENOSIS First valvular disease
LV geometric and functional changes in VHD: How to assess? Mi-Seung Shin M.D., Ph.D. Gachon University Gil Hospital
 LV geometric and functional changes in VHD: How to assess? Mi-Seung Shin M.D., Ph.D. Gachon University Gil Hospital LV inflow across MV LV LV outflow across AV LV LV geometric changes Pressure overload
LV geometric and functional changes in VHD: How to assess? Mi-Seung Shin M.D., Ph.D. Gachon University Gil Hospital LV inflow across MV LV LV outflow across AV LV LV geometric changes Pressure overload
AS with reduced LV ejection fraction: Contractile reserve should be systematically assessed: PRO
 AS with reduced LV ejection fraction: Contractile reserve should be systematically assessed: PRO Jean-Luc MONIN, MD, PhD Henri Mondor University Hospital Créteil, FRANCE Potential conflicts of interest
AS with reduced LV ejection fraction: Contractile reserve should be systematically assessed: PRO Jean-Luc MONIN, MD, PhD Henri Mondor University Hospital Créteil, FRANCE Potential conflicts of interest
Asymptomatic Valvular Disease:
 Asymptomatic Valvular Disease: Can Echocardiography Help You Decide When to Intervene? Neil J. Weissman, MD MedStar Health Research Inst at MedStar Washington Hospital Center & Professor of Medicine Georgetown
Asymptomatic Valvular Disease: Can Echocardiography Help You Decide When to Intervene? Neil J. Weissman, MD MedStar Health Research Inst at MedStar Washington Hospital Center & Professor of Medicine Georgetown
Δυναμική υπερηχοκαρδιογραφία στις μυοκαρδιοπάθειες : έχει θέση και ποια ;
 Ελληνική Καρδιολογική Εταιρεία Σεμινάρια ομάδων εργασίας Θεσσαλονίκη, 8-10 Φεβρουαρίου 2018 Ομάδα εργασίας Ηχωκαρδιολογίας Δυναμική υπερηχοκαρδιογραφία στις μυοκαρδιοπάθειες : έχει θέση και ποια ; ΑΓΑΘΗ-ΡΟΖΑ
Ελληνική Καρδιολογική Εταιρεία Σεμινάρια ομάδων εργασίας Θεσσαλονίκη, 8-10 Φεβρουαρίου 2018 Ομάδα εργασίας Ηχωκαρδιολογίας Δυναμική υπερηχοκαρδιογραφία στις μυοκαρδιοπάθειες : έχει θέση και ποια ; ΑΓΑΘΗ-ΡΟΖΑ
History of Stress Testing. Disclosure. Overview. Stress Echocardiography New Applications. and Comparison with Other Stress.
 Stress Echocardiography New Applications and Comparison with Other Stress Modalities Robert T. Palac, MD April 28, 2016 Overview Stress Testing Basics Stress Echocardiography and Stress Nuclear Perfusion
Stress Echocardiography New Applications and Comparison with Other Stress Modalities Robert T. Palac, MD April 28, 2016 Overview Stress Testing Basics Stress Echocardiography and Stress Nuclear Perfusion
The difficult patient with mitral regurgitation
 Clinical pathways The difficult patient with mitral regurgitation Stress echo can be the best tool Challenging cases Maria João Andrade, Lisbon PT Management of Severe Chronic Organic MR Echo Exercise
Clinical pathways The difficult patient with mitral regurgitation Stress echo can be the best tool Challenging cases Maria João Andrade, Lisbon PT Management of Severe Chronic Organic MR Echo Exercise
HOW IMPORTANT ARE THESE ECHO MEASUREMENTS ANYWAY?
 HOW IMPORTANT ARE THESE ECHO MEASUREMENTS ANYWAY? John D. Carroll, MD Professor, Director of Interventional Cardiology and Co-Medical Director of the Cardiac and Vascular Center, University of Colorado
HOW IMPORTANT ARE THESE ECHO MEASUREMENTS ANYWAY? John D. Carroll, MD Professor, Director of Interventional Cardiology and Co-Medical Director of the Cardiac and Vascular Center, University of Colorado
Role of Stress Echo in Valvular Heart Disease. Satoshi Nakatani Osaka University Graduate School of Medicine Osaka, Japan
 Role of Stress Echo in Valvular Heart Disease Satoshi Nakatani Osaka University Graduate School of Medicine Osaka, Japan Exercise echocardiography Dobutamine echocardiography Usefulness of exercise echo
Role of Stress Echo in Valvular Heart Disease Satoshi Nakatani Osaka University Graduate School of Medicine Osaka, Japan Exercise echocardiography Dobutamine echocardiography Usefulness of exercise echo
Primary Mitral Valve Disease: Natural History & Triggers for Intervention ACC Latin American Conference 2017
 Disclosures: GE stock, Primary Mitral Valve Disease: Natural History & Triggers for Intervention ACC Latin American Conference 2017 Athena Poppas, MD FACC Past ACC Scientific Sessions Chair, ACC Board
Disclosures: GE stock, Primary Mitral Valve Disease: Natural History & Triggers for Intervention ACC Latin American Conference 2017 Athena Poppas, MD FACC Past ACC Scientific Sessions Chair, ACC Board
Prof. Patrizio LANCELLOTTI, MD, PhD Heart Valve Clinic, University of Liège, CHU Sart Tilman, Liège, BELGIUM
 The Patient with Aortic Stenosis and Mitral Regurgitation Prof. Patrizio LANCELLOTTI, MD, PhD Heart Valve Clinic, University of Liège, CHU Sart Tilman, Liège, BELGIUM Aortic Stenosis + Mitral Regurgitation?
The Patient with Aortic Stenosis and Mitral Regurgitation Prof. Patrizio LANCELLOTTI, MD, PhD Heart Valve Clinic, University of Liège, CHU Sart Tilman, Liège, BELGIUM Aortic Stenosis + Mitral Regurgitation?
Aortic Stenosis: UPDATE Anjan Sinha, MD Krannert Institute of Cardiology
 Aortic Stenosis: UPDATE 2010 Anjan Sinha, MD Krannert Institute of Cardiology None Disclosures 67-Year-Old Male Dyspnea and angina Class III heart failure No PND or orthopnea 3/6 late peak SEM Diminished
Aortic Stenosis: UPDATE 2010 Anjan Sinha, MD Krannert Institute of Cardiology None Disclosures 67-Year-Old Male Dyspnea and angina Class III heart failure No PND or orthopnea 3/6 late peak SEM Diminished
Usually we DON T need to go beyond the gradient
 Aortic Stenosis Going Beyond the Gradient James D. Thomas, MD, FACC, FASE Director, Center for Heart Valve Disease Bluhm Cardiovascular Institute Professor of Medicine, Feinberg School of Medicine, Northwestern
Aortic Stenosis Going Beyond the Gradient James D. Thomas, MD, FACC, FASE Director, Center for Heart Valve Disease Bluhm Cardiovascular Institute Professor of Medicine, Feinberg School of Medicine, Northwestern
Steven J. Lester MD, FRCP(C), FACC, FASE Relevant Financial Relationship(s) None Off Label Usage None
, FACC, FASE Relevant Financial Relationship(s) None Off Label Usage None") Steven J. Lester MD, FRCP(C), FACC, FASE Relevant Financial Relationship(s) None Off Label Usage None 1 2,000 Noninvasive Procedures 1,600 Units of Service/ 1,000 Beneficiaries 1,200 800 Evaluation and
Steven J. Lester MD, FRCP(C), FACC, FASE Relevant Financial Relationship(s) None Off Label Usage None 1 2,000 Noninvasive Procedures 1,600 Units of Service/ 1,000 Beneficiaries 1,200 800 Evaluation and
DOPPLER HEMODYNAMICS (1) QUANTIFICATION OF PRESSURE GRADIENTS and INTRACARDIAC PRESSURES
 QUANTIFICATION OF PRESSURE GRADIENTS and INTRACARDIAC PRESSURES") THORAXCENTRE DOPPLER HEMODYNAMICS (1) QUANTIFICATION OF PRESSURE GRADIENTS and INTRACARDIAC PRESSURES J. Roelandt DOPPLER HEMODYNAMICS Intracardiac pressures and pressure gradients Volumetric measurement
THORAXCENTRE DOPPLER HEMODYNAMICS (1) QUANTIFICATION OF PRESSURE GRADIENTS and INTRACARDIAC PRESSURES J. Roelandt DOPPLER HEMODYNAMICS Intracardiac pressures and pressure gradients Volumetric measurement
TAVR: Echo Measurements Pre, Post And Intra Procedure
 2017 ASE Florida, Orlando, FL October 10, 2017 8:00 8:25 AM 25 min TAVR: Echo Measurements Pre, Post And Intra Procedure Muhamed Sarić MD, PhD, MPA Director of Noninvasive Cardiology Echo Lab Associate
2017 ASE Florida, Orlando, FL October 10, 2017 8:00 8:25 AM 25 min TAVR: Echo Measurements Pre, Post And Intra Procedure Muhamed Sarić MD, PhD, MPA Director of Noninvasive Cardiology Echo Lab Associate
Sténose aortique à Bas Débit et Bas Gradient
 3.6 m/s Sténose aortique à Bas Débit et Bas Gradient Philippe Pibarot, DVM, PhD, FACC, FAHA, FESC, FASE Canada Research Chair in Valvular Heart Diseases Doctorate Honoris Causa, Université de Liège Institut
3.6 m/s Sténose aortique à Bas Débit et Bas Gradient Philippe Pibarot, DVM, PhD, FACC, FAHA, FESC, FASE Canada Research Chair in Valvular Heart Diseases Doctorate Honoris Causa, Université de Liège Institut
How to Avoid Prosthesis-Patient Mismatch
 How to Avoid Prosthesis-Patient Mismatch Philippe Pibarot, DVM, PhD, FACC, FAHA, FASE, FESC Canada Research Chair in Valvular Heart Diseases INSTITUT UNIVERSITAIRE DE CARDIOLOGIE ET DE PNEUMOLOGIE DE QUÉBEC
How to Avoid Prosthesis-Patient Mismatch Philippe Pibarot, DVM, PhD, FACC, FAHA, FASE, FESC Canada Research Chair in Valvular Heart Diseases INSTITUT UNIVERSITAIRE DE CARDIOLOGIE ET DE PNEUMOLOGIE DE QUÉBEC
Load and Function - Valvular Heart Disease. Tom Marwick, Cardiovascular Imaging Cleveland Clinic
 Load and Function - Valvular Heart Disease Tom Marwick, Cardiovascular Imaging Cleveland Clinic Indications for surgery in common valve lesions Risks Operative mortality Failed repair - to MVR Operative
Load and Function - Valvular Heart Disease Tom Marwick, Cardiovascular Imaging Cleveland Clinic Indications for surgery in common valve lesions Risks Operative mortality Failed repair - to MVR Operative
25 different brand names >44 different models Sizes mm
 Types of Prosthetic Valves BIOLOGIC STENTED Porcine xenograft Pericardial xenograft STENTLESS Porcine xenograft Pericardial xenograft Homograft (allograft) Autograft PERCUTANEOUS MECHANICAL Bileaflet Single
Types of Prosthetic Valves BIOLOGIC STENTED Porcine xenograft Pericardial xenograft STENTLESS Porcine xenograft Pericardial xenograft Homograft (allograft) Autograft PERCUTANEOUS MECHANICAL Bileaflet Single
Prosthesis-Patient Mismatch or Prosthetic Valve Stenosis?
 EuroValves 2015, Nice Prosthesis-Patient Mismatch or Prosthetic Valve Stenosis? Philippe Pibarot, DVM, PhD, FACC, FAHA, FASE FESC Canada Research Chair in Valvular Heart Diseases Université LAVAL Disclosure
EuroValves 2015, Nice Prosthesis-Patient Mismatch or Prosthetic Valve Stenosis? Philippe Pibarot, DVM, PhD, FACC, FAHA, FASE FESC Canada Research Chair in Valvular Heart Diseases Université LAVAL Disclosure
Indicator Mild Moderate Severe
 Indicator Mild Moderate Severe Jet velocity (m/s) 2.0-2.9 3.0-3.9 4.0 Mean gradient (mmhg) < 20 20-39 40 Valve area (cm 2 ) 1.0 Valve area index (cm 2 /m 2 ) 0.6 1 Abnormal AV with Reduced Systolic Opening
Indicator Mild Moderate Severe Jet velocity (m/s) 2.0-2.9 3.0-3.9 4.0 Mean gradient (mmhg) < 20 20-39 40 Valve area (cm 2 ) 1.0 Valve area index (cm 2 /m 2 ) 0.6 1 Abnormal AV with Reduced Systolic Opening
Nothing to Disclose. Questions. Disclosure Asymptomatic Severe Aortic Stenosis: (When) Should One Intervene? Paul Wood at the Nathanson Lecture, 1958
 Should One Intervene? Paul Wood at the Nathanson Lecture, 1958") Disclosure Asymptomatic Severe Aortic Stenosis: (When) Should One Intervene? Nothing to Disclose Gabriel Gregoratos, MD, FACC, FAHA Questions Can one improve globally on the asymptomatic state? and if
Disclosure Asymptomatic Severe Aortic Stenosis: (When) Should One Intervene? Nothing to Disclose Gabriel Gregoratos, MD, FACC, FAHA Questions Can one improve globally on the asymptomatic state? and if
Ejection across stenotic aortic valve requires a systolic pressure gradient between the LV and aorta. This places a pressure load on the LV.
 Valvular Heart Disease Etiology General Principles Cellular and molecular mechanism of valve damage Structural pathology Functional pathology - stenosis/regurgitation Loading conditions - pressure/volume
Valvular Heart Disease Etiology General Principles Cellular and molecular mechanism of valve damage Structural pathology Functional pathology - stenosis/regurgitation Loading conditions - pressure/volume
Managing the Low Output Low Gradient Aortic Stenosis Patient
 Managing the Low Output Low Gradient Aortic Stenosis Patient R A Nishimura MD Judd and Mary Leighton Professor of CV Mayo Clinic No disclosures Valvular Stenosis Severity of Aortic Stenosis Mean gradient
Managing the Low Output Low Gradient Aortic Stenosis Patient R A Nishimura MD Judd and Mary Leighton Professor of CV Mayo Clinic No disclosures Valvular Stenosis Severity of Aortic Stenosis Mean gradient
Prosthetic valve dysfunction: stenosis or regurgitation
 Prosthetic valve dysfunction: stenosis or regurgitation Jean G. Dumesnil MD, FRCP(C), FACC, FASE(Hon) Quebec Heart and Lung Institute, Québec, Québec No disclosures Possible Causes of High Gradients in
Prosthetic valve dysfunction: stenosis or regurgitation Jean G. Dumesnil MD, FRCP(C), FACC, FASE(Hon) Quebec Heart and Lung Institute, Québec, Québec No disclosures Possible Causes of High Gradients in
Ejection across stenotic aortic valve requires a systolic pressure gradient between the LV and aorta. This places a pressure load on the LV.
 Valvular Heart Disease General Principles Etiology Cellular and molecular mechanism of valve damage Structural pathology Functional pathology - stenosis/regurgitation Loading conditions - pressure/volume
Valvular Heart Disease General Principles Etiology Cellular and molecular mechanism of valve damage Structural pathology Functional pathology - stenosis/regurgitation Loading conditions - pressure/volume
How does Pulmonary Hypertension Affect the Decision to Intervene in Mitral Valve Disease? NO DISCLOSURE
 How does Pulmonary Hypertension Affect the Decision to Intervene in Mitral Valve Disease? Prof. Patrizio LANCELLOTTI, MD, PhD GIGA Cardiovascular Sciences, Heart Valve Clinic, University of Liège, CHU
How does Pulmonary Hypertension Affect the Decision to Intervene in Mitral Valve Disease? Prof. Patrizio LANCELLOTTI, MD, PhD GIGA Cardiovascular Sciences, Heart Valve Clinic, University of Liège, CHU
 Stress Echocardiography: Illustrative Cases Sunil Mankad, MD, FACC, FCCP, FASE Associate Professor of Medicine Mayo Clinic College of Medicine Director, Transesophageal Echocardiography Associate Director,
Stress Echocardiography: Illustrative Cases Sunil Mankad, MD, FACC, FCCP, FASE Associate Professor of Medicine Mayo Clinic College of Medicine Director, Transesophageal Echocardiography Associate Director,
HIGHLIGHT SESSION. Imaging. J. L. Zamorano Gomez (Madrid, ES) Disclosures: Speaker Philips
 Disclosures: Speaker Philips") Imaging. J. L. Zamorano Gomez (Madrid, ES) Disclosures: Speaker Philips Agenda ECHO Diagnosis & Prognosis : Functional MR Severity Aortic Stenosis CT How to select pts for TAVI Adding prognostic info to
Imaging. J. L. Zamorano Gomez (Madrid, ES) Disclosures: Speaker Philips Agenda ECHO Diagnosis & Prognosis : Functional MR Severity Aortic Stenosis CT How to select pts for TAVI Adding prognostic info to
Aortic Valve Replacement Improves Outcome in Patients with Preserved Ejection Fraction: PRO!
 ESC 2011, Paris Controversies in Low-Flow, Low-Gradient Aortic Stenosis Aortic Valve Replacement Improves Outcome in Patients with Preserved Ejection Fraction: PRO! Philippe Pibarot, DVM, PhD, FACC, FAHA,
ESC 2011, Paris Controversies in Low-Flow, Low-Gradient Aortic Stenosis Aortic Valve Replacement Improves Outcome in Patients with Preserved Ejection Fraction: PRO! Philippe Pibarot, DVM, PhD, FACC, FAHA,
Aortic Valve Stenosis: When stress TTE and/or TEE is required to make the diagnosis and guide treatment
 Aortic Valve Stenosis: When stress TTE and/or TEE is required to make the diagnosis and guide treatment Stefanos Karagiannis MD PhD Cardiologist Director Echocardiology Dpt Athens Medical Center ESC 2017
Aortic Valve Stenosis: When stress TTE and/or TEE is required to make the diagnosis and guide treatment Stefanos Karagiannis MD PhD Cardiologist Director Echocardiology Dpt Athens Medical Center ESC 2017
Valvular Heart Disease
 Valvular Heart Disease B K Singh, MD, FACC Disclosures: None 1 CARDIAC CYCLE S2 S2=A2P2 S1=M1T1 S4 S1 S3 2 JVP Carotid S1 Slitting of S2 S3 S4 Ejection click Opening snap Dynamic Auscultation What is the
Valvular Heart Disease B K Singh, MD, FACC Disclosures: None 1 CARDIAC CYCLE S2 S2=A2P2 S1=M1T1 S4 S1 S3 2 JVP Carotid S1 Slitting of S2 S3 S4 Ejection click Opening snap Dynamic Auscultation What is the
Spotlight on Valvular Heart Disease Guidelines
 Spotlight on Valvular Heart Disease Guidelines Aortic Valve Disease Raphael Rosenhek Department of Cardiology Medical University of Vienna Palermo, April 26 th 2018 1998 2002 2006 2007 2008 2012 2014 2017
Spotlight on Valvular Heart Disease Guidelines Aortic Valve Disease Raphael Rosenhek Department of Cardiology Medical University of Vienna Palermo, April 26 th 2018 1998 2002 2006 2007 2008 2012 2014 2017
Low Gradient AS: Multi-Imaging Modalities
 Low Gradient AS: Multi-Imaging Modalities Philippe Pibarot, DVM, PhD, FACC, FAHA, FESC, FASE Canada Research Chair in Valvular Heart Diseases Institut Universitaire de Cardiologie et de Pneumologie de
Low Gradient AS: Multi-Imaging Modalities Philippe Pibarot, DVM, PhD, FACC, FAHA, FESC, FASE Canada Research Chair in Valvular Heart Diseases Institut Universitaire de Cardiologie et de Pneumologie de
Imaging Assessment of Aortic Stenosis/Aortic Regurgitation
 Imaging Assessment of Aortic Stenosis/Aortic Regurgitation Craig E Fleishman, MD FACC FASE The Heart Center at Arnold Palmer Hospital for Children, Orlando SCAI Fall Fellows Course 2014 Las Vegas Disclosure
Imaging Assessment of Aortic Stenosis/Aortic Regurgitation Craig E Fleishman, MD FACC FASE The Heart Center at Arnold Palmer Hospital for Children, Orlando SCAI Fall Fellows Course 2014 Las Vegas Disclosure
Aortic Stenosis and Perioperative Risk With Non-cardiac Surgery
 Aortic Stenosis and Perioperative Risk With Non-cardiac Surgery Aortic stenosis (AS) is characterized as a high-risk index for cardiac complications during non-cardiac surgery. A critical analysis of old
Aortic Stenosis and Perioperative Risk With Non-cardiac Surgery Aortic stenosis (AS) is characterized as a high-risk index for cardiac complications during non-cardiac surgery. A critical analysis of old
Coronary Artery Bypass Graft: Monitoring Patients and Detecting Complications
 Coronary Artery Bypass Graft: Monitoring Patients and Detecting Complications Madhav Swaminathan, MD, FASE Professor of Anesthesiology Division of Cardiothoracic Anesthesia & Critical Care Duke University
Coronary Artery Bypass Graft: Monitoring Patients and Detecting Complications Madhav Swaminathan, MD, FASE Professor of Anesthesiology Division of Cardiothoracic Anesthesia & Critical Care Duke University
Stage of Valvular AS. Outline 10/14/16. Low-flow and Other Challenges to the Assessment of Aortic Stenosis. Severe AS
 Low-flow and Other Challenges to the Assessment of Aortic Stenosis Nithima Ratanasit, MD, FACC, FASE Siriraj Hospital, Mahidol University Bangkok, Thailand Outline Types of low-flow aortic stenosis Assessment
Low-flow and Other Challenges to the Assessment of Aortic Stenosis Nithima Ratanasit, MD, FACC, FASE Siriraj Hospital, Mahidol University Bangkok, Thailand Outline Types of low-flow aortic stenosis Assessment
Dobutamine Stress testing In Low Flow, Low EF, Low Gradient Aortic Stenosis Case Studies
 Dobutamine Stress testing In Low Flow, Low EF, Low Gradient Aortic Stenosis Case Studies Mitral Regurgitation The New ASE Guidelines: Role of 2D/3D and CMR William A. Zoghbi MD, FASE, MACC Professor and
Dobutamine Stress testing In Low Flow, Low EF, Low Gradient Aortic Stenosis Case Studies Mitral Regurgitation The New ASE Guidelines: Role of 2D/3D and CMR William A. Zoghbi MD, FASE, MACC Professor and
TSDA Boot Camp September 13-16, Introduction to Aortic Valve Surgery. George L. Hicks, Jr., MD
 TSDA Boot Camp September 13-16, 2018 Introduction to Aortic Valve Surgery George L. Hicks, Jr., MD Aortic Valve Pathology and Treatment Valvular Aortic Stenosis in Adults Average Course (Post mortem data)
TSDA Boot Camp September 13-16, 2018 Introduction to Aortic Valve Surgery George L. Hicks, Jr., MD Aortic Valve Pathology and Treatment Valvular Aortic Stenosis in Adults Average Course (Post mortem data)
Diastolic Heart Function: Applying the New Guidelines Case Studies
 Diastolic Heart Function: Applying the New Guidelines Case Studies Mitral Regurgitation The New ASE William Guidelines: A. Zoghbi Role MD, of FASE, 2D/3D MACCand CMR Professor and Chairman, Department
Diastolic Heart Function: Applying the New Guidelines Case Studies Mitral Regurgitation The New ASE William Guidelines: A. Zoghbi Role MD, of FASE, 2D/3D MACCand CMR Professor and Chairman, Department
Aortic stenosis aetiology: morphology of calcific AS,
 How to improve patient selection in aortic stenosis? Fausto J. Pinto, FESC Aortic stenosis aetiology: morphology of calcific AS, bicuspid valve, and rheumatic AS (Adapted from C. Otto, Principles of
How to improve patient selection in aortic stenosis? Fausto J. Pinto, FESC Aortic stenosis aetiology: morphology of calcific AS, bicuspid valve, and rheumatic AS (Adapted from C. Otto, Principles of
Choose the grading of diastolic function in 82 yo woman
 Question #1 Choose the grading of diastolic function in 82 yo woman E= 80 cm/s A= 70 cm/s LAVI < 34 ml/m 2 1= Grade 1 2= Grade 2 3= Grade 3 4= Normal 5= Indeterminate 2018 MFMER 3712003-1 Choose the grading
Question #1 Choose the grading of diastolic function in 82 yo woman E= 80 cm/s A= 70 cm/s LAVI < 34 ml/m 2 1= Grade 1 2= Grade 2 3= Grade 3 4= Normal 5= Indeterminate 2018 MFMER 3712003-1 Choose the grading
Bogdan A. Popescu. University of Medicine and Pharmacy Bucharest, Romania. EAE Course, Bucharest, April 2010
 Bogdan A. Popescu University of Medicine and Pharmacy Bucharest, Romania EAE Course, Bucharest, April 2010 This is how it started Mitral stenosis at a glance 2D echo narrow diastolic opening of MV leaflets
Bogdan A. Popescu University of Medicine and Pharmacy Bucharest, Romania EAE Course, Bucharest, April 2010 This is how it started Mitral stenosis at a glance 2D echo narrow diastolic opening of MV leaflets
Valve Disease in Patients With Heart Failure TAVI or Surgery? Miguel Sousa Uva Hospital Cruz Vermelha Lisbon, Portugal
 Valve Disease in Patients With Heart Failure TAVI or Surgery? Miguel Sousa Uva Hospital Cruz Vermelha Lisbon, Portugal I have nothing to disclose. Wide Spectrum Stable vs Decompensated NYHA II IV? Ejection
Valve Disease in Patients With Heart Failure TAVI or Surgery? Miguel Sousa Uva Hospital Cruz Vermelha Lisbon, Portugal I have nothing to disclose. Wide Spectrum Stable vs Decompensated NYHA II IV? Ejection
Pregnancy and Heart Disease Sharon L. Roble, MD Echo Hawaii 2016
 1 Pregnancy and Heart Disease Sharon L. Roble, MD Echo Hawaii 2016 DISCLOSURES I have no disclosures relevant to today s talk 2 Cardiovascular Effects of Pregnancy Anatomic Ventricular muscle mass increases
1 Pregnancy and Heart Disease Sharon L. Roble, MD Echo Hawaii 2016 DISCLOSURES I have no disclosures relevant to today s talk 2 Cardiovascular Effects of Pregnancy Anatomic Ventricular muscle mass increases
SONOGRAPHER & NURSE LED VALVE CLINICS
 SONOGRAPHER & NURSE LED VALVE CLINICS Frequency of visits and alerts AORTIC STENOSIS V max > 4.0 m/s or EOA < 1.0 cm 2 V max 3.5 4.0 m/s + Ca+ V max 3.0 4.0 m/s or EOA 1.0-1.5 cm 2 V max 2.5 3.0 m/s every
SONOGRAPHER & NURSE LED VALVE CLINICS Frequency of visits and alerts AORTIC STENOSIS V max > 4.0 m/s or EOA < 1.0 cm 2 V max 3.5 4.0 m/s + Ca+ V max 3.0 4.0 m/s or EOA 1.0-1.5 cm 2 V max 2.5 3.0 m/s every
Percutaneous Mitral Valve Repair: What Can We Treat and What Should We Treat
 Percutaneous Mitral Valve Repair: What Can We Treat and What Should We Treat Innovative Procedures, Devices & State of the Art Care for Arrhythmias, Heart Failure & Structural Heart Disease October 8-10,
Percutaneous Mitral Valve Repair: What Can We Treat and What Should We Treat Innovative Procedures, Devices & State of the Art Care for Arrhythmias, Heart Failure & Structural Heart Disease October 8-10,
Outline. Pathophysiology: Heart Failure. Heart Failure. Heart Failure: Definitions. Etiologies. Etiologies
 Outline Pathophysiology: Mat Maurer, MD Irving Assistant Professor of Medicine Definitions and Classifications Epidemiology Muscle and Chamber Function Pathophysiology : Definitions An inability of the
Outline Pathophysiology: Mat Maurer, MD Irving Assistant Professor of Medicine Definitions and Classifications Epidemiology Muscle and Chamber Function Pathophysiology : Definitions An inability of the
Heart Failure. Cardiac Anatomy. Functions of the Heart. Cardiac Cycle/Hemodynamics. Determinants of Cardiac Output. Cardiac Output
 Cardiac Anatomy Heart Failure Professor Qing ZHANG Department of Cardiology, West China Hospital www.blaufuss.org Cardiac Cycle/Hemodynamics Functions of the Heart Essential functions of the heart to cover
Cardiac Anatomy Heart Failure Professor Qing ZHANG Department of Cardiology, West China Hospital www.blaufuss.org Cardiac Cycle/Hemodynamics Functions of the Heart Essential functions of the heart to cover
Objectives. Diastology: What the Radiologist Needs to Know. LV Diastolic Function: Introduction. LV Diastolic Function: Introduction
 Objectives Diastology: What the Radiologist Needs to Know. Jacobo Kirsch, MD Cardiopulmonary Imaging, Section Head Division of Radiology Cleveland Clinic Florida Weston, FL To review the physiology and
Objectives Diastology: What the Radiologist Needs to Know. Jacobo Kirsch, MD Cardiopulmonary Imaging, Section Head Division of Radiology Cleveland Clinic Florida Weston, FL To review the physiology and
Degenerative Mitral Regurgitation: Etiology and Natural History of Disease and Triggers for Intervention
 Degenerative Mitral Regurgitation: Etiology and Natural History of Disease and Triggers for Intervention John N. Hamaty D.O. FACC, FACOI November 17 th 2017 I have no financial disclosures Primary Mitral
Degenerative Mitral Regurgitation: Etiology and Natural History of Disease and Triggers for Intervention John N. Hamaty D.O. FACC, FACOI November 17 th 2017 I have no financial disclosures Primary Mitral
A patient with aortic stenosis and LV dysfunction EuroECHO & Other Imaging Modalities 2012 Athens, Greece
 A patient with aortic stenosis and LV dysfunction EuroECHO & Other Imaging Modalities 2012 Athens, Greece Jean-Luc MONIN, MD, PhD. University Hospital, Créteil, FRANCE My disclosures: Lecture and/ or consulting
A patient with aortic stenosis and LV dysfunction EuroECHO & Other Imaging Modalities 2012 Athens, Greece Jean-Luc MONIN, MD, PhD. University Hospital, Créteil, FRANCE My disclosures: Lecture and/ or consulting
TAVR-Update Andrzej Boguszewski MD, FACC, FSCAI Vice Chairman, Cardiology Mid-Michigan Health Associate Professor Michigan State University, Central
 TAVR-Update Andrzej Boguszewski MD, FACC, FSCAI Vice Chairman, Cardiology Mid-Michigan Health Associate Professor Michigan State University, Central Michigan University 1 Disclosure Chiesi Pharma- Consultant
TAVR-Update Andrzej Boguszewski MD, FACC, FSCAI Vice Chairman, Cardiology Mid-Michigan Health Associate Professor Michigan State University, Central Michigan University 1 Disclosure Chiesi Pharma- Consultant
PROSTHETIC VALVE BOARD REVIEW
 PROSTHETIC VALVE BOARD REVIEW The correct answer D This two chamber view shows a porcine mitral prosthesis with the typical appearance of the struts although the leaflets are not well seen. The valve
PROSTHETIC VALVE BOARD REVIEW The correct answer D This two chamber view shows a porcine mitral prosthesis with the typical appearance of the struts although the leaflets are not well seen. The valve
New Imaging for Aortic Valve Disease. Anthony DeMaria Judy and Jack White Chair Director, Sulpizio CV Center University of California, San Diego
 New Imaging for Aortic Valve Disease Anthony DeMaria Judy and Jack White Chair Director, Sulpizio CV Center University of California, San Diego Imaging in Aortic Stenosis Valve morphology calcification
New Imaging for Aortic Valve Disease Anthony DeMaria Judy and Jack White Chair Director, Sulpizio CV Center University of California, San Diego Imaging in Aortic Stenosis Valve morphology calcification
Pathophysiology: Heart Failure
 Pathophysiology: Heart Failure Mat Maurer, MD Irving Assistant Professor of Medicine Outline Definitions and Classifications Epidemiology Muscle and Chamber Function Pathophysiology Heart Failure: Definitions
Pathophysiology: Heart Failure Mat Maurer, MD Irving Assistant Professor of Medicine Outline Definitions and Classifications Epidemiology Muscle and Chamber Function Pathophysiology Heart Failure: Definitions
Diastolic Function Overview
 Diastolic Function Overview Richard Palma BS, RDCS, RCS, APS, FASE Director and Clinical Coordinator The Hoffman Heart and Vascular Institute School of Cardiac Ultrasound None Disclosures Learning Objectives
Diastolic Function Overview Richard Palma BS, RDCS, RCS, APS, FASE Director and Clinical Coordinator The Hoffman Heart and Vascular Institute School of Cardiac Ultrasound None Disclosures Learning Objectives
2019 Qualified Clinical Data Registry (QCDR) Performance Measures
 Performance Measures") 2019 Qualified Clinical Data Registry (QCDR) Performance Measures Description: This document contains the 18 performance measures approved by CMS for inclusion in the 2019 Qualified Clinical Data Registry
2019 Qualified Clinical Data Registry (QCDR) Performance Measures Description: This document contains the 18 performance measures approved by CMS for inclusion in the 2019 Qualified Clinical Data Registry
An Integrated Approach to Study LV Diastolic Function
 An Integrated Approach to Study LV Diastolic Function Assoc. Prof. Adriana Ilieşiu, FESC University of Medicine Carol Davila Bucharest, Romania LV Diastolic Dysfunction impaired relaxation (early diastole)
An Integrated Approach to Study LV Diastolic Function Assoc. Prof. Adriana Ilieşiu, FESC University of Medicine Carol Davila Bucharest, Romania LV Diastolic Dysfunction impaired relaxation (early diastole)
Management of Difficult Aortic Root, Old and New solutions
 Management of Difficult Aortic Root, Old and New solutions Hani K. Najm MD, Msc, FRCSC,, FACC, FESC Chairman, Pediatric and Congenital Heart Surgery Cleveland Clinic Conflict of Interest None Difficult
Management of Difficult Aortic Root, Old and New solutions Hani K. Najm MD, Msc, FRCSC,, FACC, FESC Chairman, Pediatric and Congenital Heart Surgery Cleveland Clinic Conflict of Interest None Difficult
How to assess ischaemic MR?
 ESC 2012 How to assess ischaemic MR? Luc A. Pierard, MD, PhD, FESC, FACC Professor of Medicine Head, Department of Cardiology University Hospital Sart Tilman, Liège ESC 2012 No conflict of interest Luc
ESC 2012 How to assess ischaemic MR? Luc A. Pierard, MD, PhD, FESC, FACC Professor of Medicine Head, Department of Cardiology University Hospital Sart Tilman, Liège ESC 2012 No conflict of interest Luc
Hemodynamics of Exercise
 Hemodynamics of Exercise Joe M. Moody, Jr, MD UTHSCSA and ALMMVAH, STVAHCS Exercise Physiology - Acute Effects Cardiac Output (Stroke volume, Heart Rate ) Oxygen Extraction (Arteriovenous O 2 difference,
Hemodynamics of Exercise Joe M. Moody, Jr, MD UTHSCSA and ALMMVAH, STVAHCS Exercise Physiology - Acute Effects Cardiac Output (Stroke volume, Heart Rate ) Oxygen Extraction (Arteriovenous O 2 difference,
Journal of the American College of Cardiology Vol. 44, No. 9, by the American College of Cardiology Foundation ISSN /04/$30.
 Journal of the American College of Cardiology Vol. 44, 9, 2004 2004 by the American College of Cardiology Foundation ISSN 0735-1097/04/$30.00 Published by Elsevier Inc. doi:10.1016/j.jacc.2004.04.062 Relation
Journal of the American College of Cardiology Vol. 44, 9, 2004 2004 by the American College of Cardiology Foundation ISSN 0735-1097/04/$30.00 Published by Elsevier Inc. doi:10.1016/j.jacc.2004.04.062 Relation
The Doppler Examination. Katie Twomley, MD Wake Forest Baptist Health - Lexington
 The Doppler Examination Katie Twomley, MD Wake Forest Baptist Health - Lexington OUTLINE Principles/Physics Use in valvular assessment Aortic stenosis (continuity equation) Aortic regurgitation (pressure
The Doppler Examination Katie Twomley, MD Wake Forest Baptist Health - Lexington OUTLINE Principles/Physics Use in valvular assessment Aortic stenosis (continuity equation) Aortic regurgitation (pressure
Vinod H. Thourani, MD
 Triggers for Aortic Stenosis and Regurgitation Vinod H. Thourani, MD Professor of Surgery Chair, Department of Cardiac Surgery MedStar Heart and Vascular Institute Georgetown University Washington, DC,
Triggers for Aortic Stenosis and Regurgitation Vinod H. Thourani, MD Professor of Surgery Chair, Department of Cardiac Surgery MedStar Heart and Vascular Institute Georgetown University Washington, DC,
Diagnosis is it really Heart Failure?
 ESC Congress Munich - 25-29 August 2012 Heart Failure with Preserved Ejection Fraction From Bench to Bedside Diagnosis is it really Heart Failure? Prof. Burkert Pieske Department of Cardiology Med.University
ESC Congress Munich - 25-29 August 2012 Heart Failure with Preserved Ejection Fraction From Bench to Bedside Diagnosis is it really Heart Failure? Prof. Burkert Pieske Department of Cardiology Med.University
Aortic Valve Practice Guidelines: What Has Changed and What You Need to Know
 Aortic Valve Practice Guidelines: What Has Changed and What You Need to Know James F. Burke, MD Program Director Cardiovascular Disease Fellowship Lankenau Medical Center Disclosure Dr. Burke has no conflicts
Aortic Valve Practice Guidelines: What Has Changed and What You Need to Know James F. Burke, MD Program Director Cardiovascular Disease Fellowship Lankenau Medical Center Disclosure Dr. Burke has no conflicts
Aortic Stenosis: Spectrum of Disease, Low Flow/Low Gradient and Variants
 Aortic Stenosis: Spectrum of Disease, Low Flow/Low Gradient and Variants Martin G. Keane, MD, FASE Professor of Medicine Lewis Katz School of Medicine at Temple University Basic root structure Parasternal
Aortic Stenosis: Spectrum of Disease, Low Flow/Low Gradient and Variants Martin G. Keane, MD, FASE Professor of Medicine Lewis Katz School of Medicine at Temple University Basic root structure Parasternal
Disclosures. Stress Echocardiography 2010 Appropriate Use & Further Applications. Stress Echo Clinical Utility 9/8/10
 2010 & Further Applications Disclosures None Geoffrey A. Rose, MD FACC FASE Director, Cardiac Ultrasound Laboratory Sanger Heart & Vascular Institute Clinical Utility and Event-free Survival Cortigiani,
2010 & Further Applications Disclosures None Geoffrey A. Rose, MD FACC FASE Director, Cardiac Ultrasound Laboratory Sanger Heart & Vascular Institute Clinical Utility and Event-free Survival Cortigiani,
Adult Echocardiography Examination Content Outline
 Adult Echocardiography Examination Content Outline (Outline Summary) # Domain Subdomain Percentage 1 2 3 4 5 Anatomy and Physiology Pathology Clinical Care and Safety Measurement Techniques, Maneuvers,
Adult Echocardiography Examination Content Outline (Outline Summary) # Domain Subdomain Percentage 1 2 3 4 5 Anatomy and Physiology Pathology Clinical Care and Safety Measurement Techniques, Maneuvers,
A Health Care Professional s Guide Aortic Stenosis in Seniors
 A Health Care Professional s Guide Aortic Stenosis in Seniors With highlights from the 2014 ACC/AHA practice guidelines for valve disease Aortic stenosis (AS) is primarily caused by calcification of the
A Health Care Professional s Guide Aortic Stenosis in Seniors With highlights from the 2014 ACC/AHA practice guidelines for valve disease Aortic stenosis (AS) is primarily caused by calcification of the
Echocardiographic Evaluation of Mitral Valve Prostheses
 Echocardiographic Evaluation of Mitral Valve Prostheses Dennis A. Tighe, M.D., FACC, FACP, FASE Cardiovascular Medicine University of Massachusetts Medical School Worcester, MA www.asecho.org 1 Nishimura
Echocardiographic Evaluation of Mitral Valve Prostheses Dennis A. Tighe, M.D., FACC, FACP, FASE Cardiovascular Medicine University of Massachusetts Medical School Worcester, MA www.asecho.org 1 Nishimura
Echocardiography as a diagnostic and management tool in medical emergencies
 Echocardiography as a diagnostic and management tool in medical emergencies Frank van der Heusen MD Department of Anesthesia and perioperative Care UCSF Medical Center Objective of this presentation Indications
Echocardiography as a diagnostic and management tool in medical emergencies Frank van der Heusen MD Department of Anesthesia and perioperative Care UCSF Medical Center Objective of this presentation Indications
Valvular Regurgitation: Can We Do Better Than Colour Doppler?
 Valvular Regurgitation: Can We Do Better Than Colour Doppler? A/Prof David Prior St Vincent s Hospital Melbourne Sports Cardiology Valvular Regurgitation Valve regurgitation volume loads the ventricles
Valvular Regurgitation: Can We Do Better Than Colour Doppler? A/Prof David Prior St Vincent s Hospital Melbourne Sports Cardiology Valvular Regurgitation Valve regurgitation volume loads the ventricles
Disclosures. ESC Munich 2012 Bernard Iung, MD Consultancy: Abbott Boehringer Ingelheim Bayer Servier Valtech
 Disclosures ESC Munich 2012 Bernard Iung, MD Consultancy: Abbott Boehringer Ingelheim Bayer Servier Valtech Speaker s fee Edwards Lifesciences Sanofi-Aventis Decision Making in Patients with Multivalvular
Disclosures ESC Munich 2012 Bernard Iung, MD Consultancy: Abbott Boehringer Ingelheim Bayer Servier Valtech Speaker s fee Edwards Lifesciences Sanofi-Aventis Decision Making in Patients with Multivalvular
HFpEF. April 26, 2018
 HFpEF April 26, 2018 (J Am Coll Cardiol 2017;70:2476 86) HFpEF 50% or more (40-71%) of patients with CHF have preserved LV systolic function. HFpEF is an increasingly frequent hospital discharge. Outcomes
HFpEF April 26, 2018 (J Am Coll Cardiol 2017;70:2476 86) HFpEF 50% or more (40-71%) of patients with CHF have preserved LV systolic function. HFpEF is an increasingly frequent hospital discharge. Outcomes
Exercise PHT in valvular heart disease. Julien Magne CHU Limoges, France
 Exercise PHT in valvular heart disease Julien Magne CHU Limoges, France Faculty disclosure Julien Magne I disclose the following financial relationships: I have no financial relationships to disclose.
Exercise PHT in valvular heart disease Julien Magne CHU Limoges, France Faculty disclosure Julien Magne I disclose the following financial relationships: I have no financial relationships to disclose.
Hypertension in Aortic Valve Disease
 Hypertension in Aortic Valve Disease Hanna M. Nosseir MRCP, FRCP Head of Cardiology department Galaa Military Medical Complex Aortic stenosis: Introduction Arterial hypertension and aortic stenosis are
Hypertension in Aortic Valve Disease Hanna M. Nosseir MRCP, FRCP Head of Cardiology department Galaa Military Medical Complex Aortic stenosis: Introduction Arterial hypertension and aortic stenosis are
Outline. EuroScore II. Society of Thoracic Surgeons Score. EuroScore II
 SURGICAL RISK IN VALVULAR HEART DISEASE: WHAT 2D AND 3D ECHO CAN TELL YOU AND WHAT THEY CAN'T Ernesto E Salcedo, MD Professor of Medicine University of Colorado School of Medicine Director of Echocardiography
SURGICAL RISK IN VALVULAR HEART DISEASE: WHAT 2D AND 3D ECHO CAN TELL YOU AND WHAT THEY CAN'T Ernesto E Salcedo, MD Professor of Medicine University of Colorado School of Medicine Director of Echocardiography
Echo Doppler Assessment of Right and Left Ventricular Hemodynamics.
 Echo Doppler Assessment of Right and Left Ventricular Hemodynamics. Itzhak Kronzon, MD, FASE, FACC, FESC, FAHA, FACP, FCCP Northwell, Lenox Hill Hospital, New York Professor of Cardiology Hofstra University
Echo Doppler Assessment of Right and Left Ventricular Hemodynamics. Itzhak Kronzon, MD, FASE, FACC, FESC, FAHA, FACP, FCCP Northwell, Lenox Hill Hospital, New York Professor of Cardiology Hofstra University
Low gradient severe aortic stenosis with preserved left ventricular ejection fraction
 Review Article Low gradient severe aortic stenosis with preserved left ventricular ejection fraction Alper Ozkan Heart and Vascular Institute, Cleveland Clinic, Cleveland, Ohio, USA Corresponding to: Alper
Review Article Low gradient severe aortic stenosis with preserved left ventricular ejection fraction Alper Ozkan Heart and Vascular Institute, Cleveland Clinic, Cleveland, Ohio, USA Corresponding to: Alper
The FORMA Early Feasibility Study: 30-Day Outcomes of Transcatheter Tricuspid Valve Therapy in Patients with Severe Secondary Tricuspid Regurgitation
 The FORMA Early Feasibility Study: 30-Day Outcomes of Transcatheter Tricuspid Valve Therapy in Patients with Severe Secondary Tricuspid Regurgitation Susheel Kodali, MD Director, Structural Heart & Valve
The FORMA Early Feasibility Study: 30-Day Outcomes of Transcatheter Tricuspid Valve Therapy in Patients with Severe Secondary Tricuspid Regurgitation Susheel Kodali, MD Director, Structural Heart & Valve
Welcome 17 Michigan TAVR Participating Hospitals!
 Welcome 17 Michigan TAVR Participating Hospitals! 1 MICHIGAN TAVR BRIEF OVERVIEW HOW AND WHY PRE-TAVR IMAGING EVALUATION AND THE TVT Michael Grossman, MD Co-Director, BMC2 Coordinating Center Why Michigan
Welcome 17 Michigan TAVR Participating Hospitals! 1 MICHIGAN TAVR BRIEF OVERVIEW HOW AND WHY PRE-TAVR IMAGING EVALUATION AND THE TVT Michael Grossman, MD Co-Director, BMC2 Coordinating Center Why Michigan
Interventions in Adult Congenital Heart Disease: Role of CV Imaging. Associate Professor. ACHD mortality. Pillutla. Am Heart J 2009;158:874-9
 Interventions in Adult Congenital Heart Disease: Role of CV Imaging Sangeeta Shah MD, FACC, FASE Associate Professor ACHD mortality Pillutla. Am Heart J 2009;158:874-9 Adult Congenital Heart Disease Heterogenity
Interventions in Adult Congenital Heart Disease: Role of CV Imaging Sangeeta Shah MD, FACC, FASE Associate Professor ACHD mortality Pillutla. Am Heart J 2009;158:874-9 Adult Congenital Heart Disease Heterogenity
The Athlete s Heart. Role of Echo. Neil J. Weissman, MD MedStar Health Research Institute & Professor of Medicine Georgetown University
 The Athlete s Heart Role of Echo Neil J. Weissman, MD MedStar Health Research Institute & Professor of Medicine Georgetown University Washington, D.C. Disclosures Grant support (to institution) for Core
The Athlete s Heart Role of Echo Neil J. Weissman, MD MedStar Health Research Institute & Professor of Medicine Georgetown University Washington, D.C. Disclosures Grant support (to institution) for Core
Imaging in Heart Failure: A Multimodality Approach. Thomas Ryan, MD
 Imaging in Heart Failure: A Multimodality Approach Thomas Ryan, MD Heart Failure HFrEF HFpEF EF50% Lifetime risk 20% Prevalence 6M Americans Societal costs - $30B 50% 5-year survival 1 Systolic
Imaging in Heart Failure: A Multimodality Approach Thomas Ryan, MD Heart Failure HFrEF HFpEF EF50% Lifetime risk 20% Prevalence 6M Americans Societal costs - $30B 50% 5-year survival 1 Systolic
Relevant Financial Relationship(s) Off Label Usage. None. None
 Off Label Usage. None. None") Different Variants Amr E Abbas, MD, FACC, FSCAI, FASE, FSVM Director, Interventional Cardiology Research Beaumont Health Associate Professor of Medicine, OU/WB School of Medicine ASCeXAM/ReASCeXAM 2018
Different Variants Amr E Abbas, MD, FACC, FSCAI, FASE, FSVM Director, Interventional Cardiology Research Beaumont Health Associate Professor of Medicine, OU/WB School of Medicine ASCeXAM/ReASCeXAM 2018