ECMO: a breakthrough in care for respiratory failure. PD Dr. Thomas Müller Regensburg no conflict of interest
|
|
|
- Alvin Logan
- 5 years ago
- Views:
Transcription


1 ECMO: a breakthrough in care for respiratory failure? PD Dr. Thomas Müller Regensburg no conflict of interest 1



2 Overview Mortality of severe ARDS Indication for ECMO PaO 2 /FiO 2 Efficiency of ECMO: gas transfer, ventilation, outcome Problems of ECMO Conclusion 2

3 ARDS - Mortality Legionellosis Phua et al, Am J RespirCrit Care Med 2009;179:
4 ARDS - Mortality These results highlight the need for future effective therapeutic interventions in this highly lethal syndrome Phua et al, Am J RespirCrit Care Med 2009;179:
 with ARDS hospital mortality 40 %: 34.9 % - 40.3 % - 46.")
5 459 ICUs from 50 countries 3022 patients (10.4 %) with ARDS hospital mortality 40 %: 34.9 % % % mild moderate - severe JAMA 2016;315:
6 LUNG SAFE: Mortality and Driving/Plateau Pressure Driving Pressure Plateau Pressure JAMA 2016;315:

7 Case Presentation 49 yr, female, past history empty 30.01: dry cough, fatigue, flu-like symptoms, diarrhoea, temp 38.5 C : admission to external hospital, progressive dyspnoe PCT 20 µg/l, CRP 177 mg/l, lactate 113 mg/l, WBC 2.2/µl, Platelets 78/nl, INR 1.63, aptt 54 sec Ampicillin, Sulbactam, Clarithromycin CT-Scan: intubation referral broad spectrum antibiotic coverage expected mortality? 7


8 02.02: septic shock and MOF: + 11 liters volume PCT 177 ng/ml, CK 3475 U/l, troponin I 22.6 ng/ml, platelets 77/nl, INR 1.84, aptt 87 sec, AT-III 19 %, D-Dimers > 35 mg/l PaO 2 /FiO 2 98 mmhg, PaCO 2 40 mmhg PEEP/PIP 14/27 17/31 cm H 2 O noradrenaline 6 mg/h, epinephrine 0.5 mg/h lactate 90 mg/dl Case Presentation ECHO: septic cardiomyopathy 12:00 o clock decision for ECMO: veno-arterial cannulation, blood flow 3.8 l/min plasma exchange expected mortality? 8





9 18:00 o clock: Case Presentation noradrenaline 1.8 mg/h, epinephrine 0.3 mg/h lactate 110 mg/dl PaO 2 /FiO 2 50 mmhg, PaCO 2 45 mmhg PEEP/PIP 17/31 24/38 cm H 2 O decision for additional venous cannula: VAV ECMO: blood flow l/min chest X-ray: expected mortality? 9
10 Extracorporeal Gas Transfer 1. O 2 Transfer efficiency depends on blood flow and blood sat effects: avoid hxpoxemia protective ventilation: VILI, right heart strain gain of time po 2 Gas 760 mmhg p0 2 Blood ~ 500 mmhg p0 2 Blood ~ 35 mmhg 2. CO 2 Elimination efficiency depends on blood flow, gas flow and PvCO 2 (recirculation!) effects: protective ventilation over-inflation work of breathing facilitation of extubation? avoidance of intubation? pco 2 Gas 0 mmhg pc0 2 Blood ~ 25 mmhg pc0 2 Blood ~ 50 mmhg 10

11 Gas-transfer Capacity of MOs Lehle K et al, ICM 2014;40:
 ECLS should be considered when the risk of mortality is 50% or greater, and is indicated when the risk of mortality is 80% or")
12 Indication: ELSO 1. In hypoxic respiratory failure due to any cause (primary or secondary) ECLS should be considered when the risk of mortality is 50% or greater, and is indicated when the risk of mortality is 80% or greater. a. 50% mortality risk is associated with a PaO 2 /FiO 2 < 150 on FiO 2 > 90% and/or Murray score 2-3. b. 80% mortality risk is associated with a PaO 2 /FiO 2 < 100 on FiO 2 > 90% and/or Murray score 3-4 despite optimal care for 6 hours or more. 2. CO 2 retention on mechanical ventilation despite high Pplat (>30 cm H 2 O) 3. Severe air leak syndromes 4. Need for intubation in a patient on lung transplant list 5. Immediate cardiac or respiratory collapse (PE, blocked airway, unresponsive to optimal care) 12

 2.")

13 Indication for VV ECMO 1. rescue vital gas exchange can not be secured by conventional means, and rapidly progressive hemodynamic instability (P/F < 60 mm Hg, and ph < 7.2, and PIP > 35 cm H 2 O, and Nor > 1.5 mg/h) 2. semielektive lung protective ventilation not possible to secure vital gas exchange; no improvement after hours 3. given that: treatable cause all conventional therapeutic methods optimized no contraindication PaO 2 /FiO 2 < 80 mm Hg with PEEP > 15 cm H 2 O uncompensated respiratory acidosis: ph < 7,15 Brodie D, Bacchetta M, New Engl J Med 2011; 365:

14 Vv-ECMO: PaO 2 /FiO 2,PaCO 2 and TV NOR Müller et al, Dtsch Arztebl Int 2013;110:
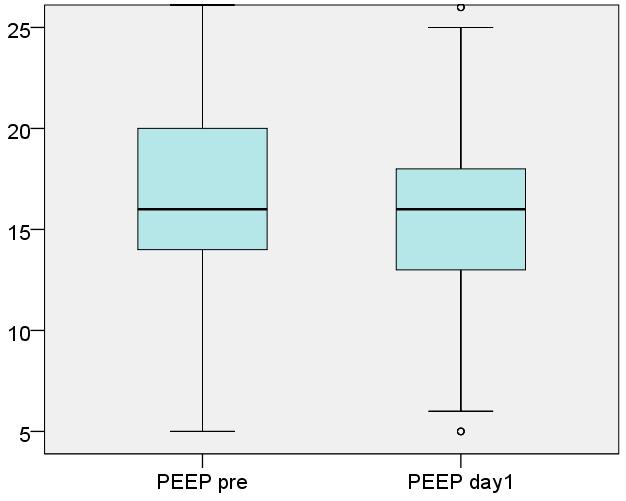
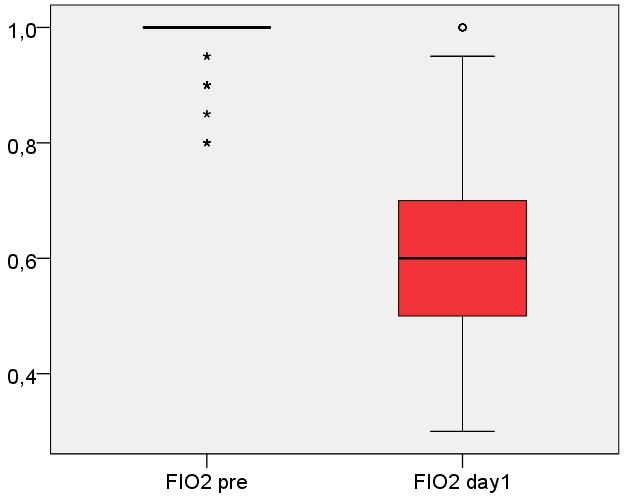
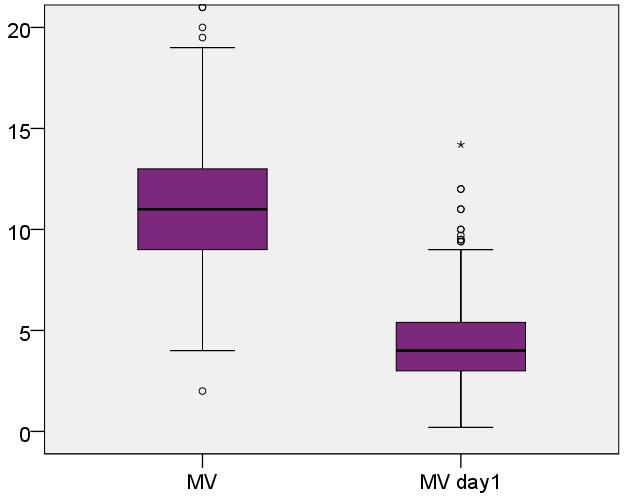
15 Ventilation on ECMO TV FiO 2 MV PEEP n = 375 PIP
16 Survival with modern ECMO Study Literature Number Age Survival ANZ ECMO Italian ECMOnet ELSO H1N1 registry (adults > 20 yrs) CESAR UK ECMO for H1N1 REVA Research Network JAMA 2009;302:online Oct 12 Intensive Care Med 2011;37: umich.edu/ April 13, 2011 Lancet 2009;374: JAMA 2011;306:online Oct 5 Am J Respir Crit Care Med 2013;187: % % 218? 70 % % % % 16
 in-hospital")

17 incidence VV-ECMO 2014: 2.4/ (n = 1944) in-hospital mortality 2014: 58 % case numbers mortality Intensive Care Med 2016, March 4 epub ahead of print 17
18 Survival RESP-Score Population N = 2355 Age (years) 41 (28-54) Schmidt M et al, AJRCCM in press 02.April

19 Model 2 (day 1): age day 1 FiO 2 immunocompromised state day 1 fibrinogen minute ventilation day 1 norepi. pre ECMO Hb day 1 CRP TB Enger...T Müller, Crit Care 2014;18:R67
 100% 80% 60% 14 40 56 59 80")


20 Outcome according to age (n = 551) 100% 80% 60% % 20% 0% < > 69 Tod an ECMO Tod nach ECMO Überleben 20

21 Crit Care Med Feb;45(2):
22 Crit Care Med Feb;45(2):








23 Risks of ECMO Ruptur of femoral vein tamponade broken cannula



![[mg/dl] 2500](/docs-images/80/81132761/images/24-4.jpg "2000 1500 1000")

24 Risk of Technical Failure LDH [U/l} free hemoglobin [mg/dl] pre 24hrs exchange +12 hrs +24 hrs + 36 hrs +48 hrs
 (n = 440)")

25 Avoid unnecessary interventions risk of bleeding: platelets day 4 (61%) (n = 440) no unnecessary blood transfusions Hb transfusion threshold 8.0 g/dl RBCs/day on ECMO: 0.31 (0.00;0.78)

 survival n = 27 (51%) ischemia n = 11 (4 %)")
26 VV-ECMO and Cerebral Complications: 04/ /2015 preliminary results 495 vv ECMO runs CCT n=290 no pathology n = 226 (78 %) survival n = 142 (63%) ICB n = 53 (18 %) survival n = 27 (51%) ischemia n = 11 (4 %) survival n = 8 (73%) 26
27 Requirements for an ECMO Center 1. experience in the treatment of severe ARDS: tertiary care ICU 2. transport possible with ECMO: mobile team 3. experience with ECMO: > 10 (20) cases per year 24/7 trained personel: intensivists, nurses, (perfusionists) 4. management of complications: blood bank, lab, CT 24/7 ECMO replacement equipment vascular surgery, (abdominal-, thoracic surgery) 5. quality managment: regular training data base M + M conference participation in national or international registry Am J Respir Crit Care Med Sep 1;190(5):
 3.")
28 Conclusion: ECMO: a breakthrough in care for respiratory failure? 1. ECMO safes lifes. 2. indications: relatively sure: severe refractory ARDS uncertain: CO 2 elimination (avoidance of intubation? facilitated weaning?) 3. balance benefits versus risks 4. costs! 5. experience necessary: ECMO Center 28

29 29
Outcomes From Severe ARDS Managed Without ECMO. Roy Brower, MD Johns Hopkins University Critical Care Canada Forum Toronto November 1, 2016
 Outcomes From Severe ARDS Managed Without ECMO Roy Brower, MD Johns Hopkins University Critical Care Canada Forum Toronto November 1, 2016 Severe ARDS Berlin Definition 2012 P:F ratio 100 mm Hg Prevalence:
Outcomes From Severe ARDS Managed Without ECMO Roy Brower, MD Johns Hopkins University Critical Care Canada Forum Toronto November 1, 2016 Severe ARDS Berlin Definition 2012 P:F ratio 100 mm Hg Prevalence:
Veno-Venous ECMO Support. Chris Cropsey, MD Sept. 21, 2015
 Veno-Venous ECMO Support Chris Cropsey, MD Sept. 21, 2015 Objectives List indications and contraindications for ECMO Describe hemodynamics and oxygenation on ECMO Discuss evidence for ECMO outcomes Identify
Veno-Venous ECMO Support Chris Cropsey, MD Sept. 21, 2015 Objectives List indications and contraindications for ECMO Describe hemodynamics and oxygenation on ECMO Discuss evidence for ECMO outcomes Identify
ARDS: an update 6 th March A. Hakeem Al Hashim, MD, FRCP SQUH
 ARDS: an update 6 th March 2017 A. Hakeem Al Hashim, MD, FRCP SQUH 30M, previously healthy Hx: 1 week dry cough Gradually worsening SOB No travel Hx Case BP 130/70, HR 100/min ph 7.29 pco2 35 po2 50 HCO3
ARDS: an update 6 th March 2017 A. Hakeem Al Hashim, MD, FRCP SQUH 30M, previously healthy Hx: 1 week dry cough Gradually worsening SOB No travel Hx Case BP 130/70, HR 100/min ph 7.29 pco2 35 po2 50 HCO3
Ventilator ECMO Interactions
 Ventilator ECMO Interactions Lorenzo Del Sorbo, MD CCCF Toronto, October 2 nd 2017 Disclosure Relevant relationships with commercial entities: none Potential for conflicts within this presentation: none
Ventilator ECMO Interactions Lorenzo Del Sorbo, MD CCCF Toronto, October 2 nd 2017 Disclosure Relevant relationships with commercial entities: none Potential for conflicts within this presentation: none
Extracorporeal support in acute respiratory failure. Dr Anthony Bastin Consultant in critical care Royal Brompton Hospital, London
 Extracorporeal support in acute respiratory failure Dr Anthony Bastin Consultant in critical care Royal Brompton Hospital, London Objectives By the end of this session, you will be able to: Describe different
Extracorporeal support in acute respiratory failure Dr Anthony Bastin Consultant in critical care Royal Brompton Hospital, London Objectives By the end of this session, you will be able to: Describe different
Adult Extracorporeal Life Support (ECLS)
") Adult Extracorporeal Life Support (ECLS) Steven Scott, M.D., F.A.C.S. Piedmont Heart Institute Cardiothoracic Surgery Disclosures None ECMO = ECLS A technique of life support that involves a continuous
Adult Extracorporeal Life Support (ECLS) Steven Scott, M.D., F.A.C.S. Piedmont Heart Institute Cardiothoracic Surgery Disclosures None ECMO = ECLS A technique of life support that involves a continuous
ECMO/ECCO 2 R in Acute Respiratory Failure
 ECMO/ECCO 2 R in Acute Respiratory Failure Alain Combes, MD, PhD, Hôpital Pitié-Salpêtrière, AP-HP Inserm UMRS 1166, ican, Institute of Cardiometabolism and Nutrition Sorbonne Pierre et Marie Curie University,
ECMO/ECCO 2 R in Acute Respiratory Failure Alain Combes, MD, PhD, Hôpital Pitié-Salpêtrière, AP-HP Inserm UMRS 1166, ican, Institute of Cardiometabolism and Nutrition Sorbonne Pierre et Marie Curie University,
Lesta Whalen, MD Medical Director, Sanford ECMO Pediatric Critical Care
 Lesta Whalen, MD Medical Director, Sanford ECMO Pediatric Critical Care Disclosures I have no financial disclosures. The use of certain devises for providing long-term cardiopulmonary support is investigational.
Lesta Whalen, MD Medical Director, Sanford ECMO Pediatric Critical Care Disclosures I have no financial disclosures. The use of certain devises for providing long-term cardiopulmonary support is investigational.
10/16/2017. Review the indications for ECMO in patients with. Respiratory failure Cardiac failure Cardiorespiratory failure
 Review the indications for ECMO in patients with Respiratory failure Cardiac failure Cardiorespiratory failure 1 Extracorporeal membrane lung and/or cardiac support. A support therapy, in no way definitive.
Review the indications for ECMO in patients with Respiratory failure Cardiac failure Cardiorespiratory failure 1 Extracorporeal membrane lung and/or cardiac support. A support therapy, in no way definitive.
BASIC CRITICAL CARE OF THE PATIENT. Hannelisa Callisen PA C February 2017
 BASIC CRITICAL CARE OF THE PATIENT Hannelisa Callisen PA C February 2017 Disclosures Industry: None ECMO is off label Objectives ECMO initiation selection, cannulation Physiology : Review of DO2 on ECMO
BASIC CRITICAL CARE OF THE PATIENT Hannelisa Callisen PA C February 2017 Disclosures Industry: None ECMO is off label Objectives ECMO initiation selection, cannulation Physiology : Review of DO2 on ECMO
Pro: Early use of VV ECMO for ARDS
 Pro: Early use of VV ECMO for ARDS Kyle J. Rehder, MD, FCCP Associate Professor Division of Pediatric Critical Care Medicine Department of Pediatrics Duke Children s Hospital The ventilator is slowly killing
Pro: Early use of VV ECMO for ARDS Kyle J. Rehder, MD, FCCP Associate Professor Division of Pediatric Critical Care Medicine Department of Pediatrics Duke Children s Hospital The ventilator is slowly killing
Option and Pitfalls in Cannulation for Extracorporeal Support
 Option and Pitfalls in Cannulation for Extracorporeal Support The Regensburg Experience Extracorporeal Life Support Group Dept. of Anaesthesiology Dept. of Internal Medicine Dept. of Cardiothoracic Surgery
Option and Pitfalls in Cannulation for Extracorporeal Support The Regensburg Experience Extracorporeal Life Support Group Dept. of Anaesthesiology Dept. of Internal Medicine Dept. of Cardiothoracic Surgery
ARDS Assisted ventilation and prone position. ICU Fellowship Training Radboudumc
 ARDS Assisted ventilation and prone position ICU Fellowship Training Radboudumc Fig. 1 Physiological mechanisms controlling respiratory drive and clinical consequences of inappropriate respiratory drive
ARDS Assisted ventilation and prone position ICU Fellowship Training Radboudumc Fig. 1 Physiological mechanisms controlling respiratory drive and clinical consequences of inappropriate respiratory drive
ECMO for Severe Hypoxemic Respiratory Failure: Pro-Con Debate. Carolyn Calfee, MD MAS Mark Eisner, MD MPH
 ECMO for Severe Hypoxemic Respiratory Failure: Pro-Con Debate Carolyn Calfee, MD MAS Mark Eisner, MD MPH June 3, 2010 Case Presentation Setting: Community hospital, November 2009 29 year old woman with
ECMO for Severe Hypoxemic Respiratory Failure: Pro-Con Debate Carolyn Calfee, MD MAS Mark Eisner, MD MPH June 3, 2010 Case Presentation Setting: Community hospital, November 2009 29 year old woman with
Extracorporeal Life Support Organization (ELSO) Guidelines for Pediatric Respiratory Failure
 Guidelines for Pediatric Respiratory Failure") Extracorporeal Life Support Organization (ELSO) Guidelines for Pediatric Respiratory Failure Introduction This pediatric respiratory failure guideline is a supplement to ELSO s General Guidelines for all
Extracorporeal Life Support Organization (ELSO) Guidelines for Pediatric Respiratory Failure Introduction This pediatric respiratory failure guideline is a supplement to ELSO s General Guidelines for all
ECMO BASICS CHLOE STEINSHOUER, MD PULMONARY AND SLEEP CONSULTANTS OF KANSAS
 ECMO BASICS CHLOE STEINSHOUER, MD PULMONARY AND SLEEP CONSULTANTS OF KANSAS DISCLOSURES No financial disclosures or conflicts of interest OBJECTIVES Define ECMO/ECLS and be able to identify the main types
ECMO BASICS CHLOE STEINSHOUER, MD PULMONARY AND SLEEP CONSULTANTS OF KANSAS DISCLOSURES No financial disclosures or conflicts of interest OBJECTIVES Define ECMO/ECLS and be able to identify the main types
ECLS Registry Form Extracorporeal Life Support Organization (ELSO)
") ECLS Registry Form Extracorporeal Life Support Organization (ELSO) Center ID: Center name: Run No (for this patient) Unique ID: Birth Date/Time Sex: (M, F) Race: (Asian, Black, Hispanic, White, Other)
ECLS Registry Form Extracorporeal Life Support Organization (ELSO) Center ID: Center name: Run No (for this patient) Unique ID: Birth Date/Time Sex: (M, F) Race: (Asian, Black, Hispanic, White, Other)
A simple case of.. Acute severe asthma. MasterclassIC Schiermonnikoog 2017
 A simple case of.. Acute severe asthma MasterclassIC Schiermonnikoog 2017 Case (1) Female, 27 - G1P0 (26 weeks) PMH - several admissions for severe acute asthma (no MV) Progressive dyspnea for 1 week Admitted
A simple case of.. Acute severe asthma MasterclassIC Schiermonnikoog 2017 Case (1) Female, 27 - G1P0 (26 weeks) PMH - several admissions for severe acute asthma (no MV) Progressive dyspnea for 1 week Admitted
Part 2 of park s Ventilator and ARDS slides for syllabus
 Part 2 of park s Ventilator and ARDS slides for syllabus Early Neuromuscular Blockade Question 4 The early use of cis-atracurium in severe ARDS is: A. Contraindicated in patients with diabetes B. Associated
Part 2 of park s Ventilator and ARDS slides for syllabus Early Neuromuscular Blockade Question 4 The early use of cis-atracurium in severe ARDS is: A. Contraindicated in patients with diabetes B. Associated
Surviving Sepsis Campaign. Guidelines for Management of Severe Sepsis/Septic Shock. An Overview
 Surviving Sepsis Campaign Guidelines for Management of Severe Sepsis/Septic Shock An Overview Mechanical Ventilation of Sepsis-Induced ALI/ARDS ARDSnet Mechanical Ventilation Protocol Results: Mortality
Surviving Sepsis Campaign Guidelines for Management of Severe Sepsis/Septic Shock An Overview Mechanical Ventilation of Sepsis-Induced ALI/ARDS ARDSnet Mechanical Ventilation Protocol Results: Mortality
Case discussion Acute severe asthma during pregnancy. J.G. van der Hoeven
 Case discussion Acute severe asthma during pregnancy J.G. van der Hoeven Case (1) 32-year-old female - gravida 3 - para 2 Previous medical history - asthma Pregnant (33 w) Acute onset fever with wheezing
Case discussion Acute severe asthma during pregnancy J.G. van der Hoeven Case (1) 32-year-old female - gravida 3 - para 2 Previous medical history - asthma Pregnant (33 w) Acute onset fever with wheezing
Case scenario V AV ECMO. Dr Pranay Oza
 Case scenario V AV ECMO Dr Pranay Oza Case Summary 53 y/m, k/c/o MVP with myxomatous mitral valve with severe Mitral regurgitation underwent Mitral valve replacement with mini thoracotomy Pump time nearly
Case scenario V AV ECMO Dr Pranay Oza Case Summary 53 y/m, k/c/o MVP with myxomatous mitral valve with severe Mitral regurgitation underwent Mitral valve replacement with mini thoracotomy Pump time nearly
My Special Cytosorb Case. Fabio Silvio TACCONE Dpt of Intensive Care Hôpital Erasme ULB Brussels (BE)
") My Special Cytosorb Case Fabio Silvio TACCONE Dpt of Intensive Care Hôpital Erasme ULB Brussels (BE) Conflicts of Interest Clinical Case - 1! 27 yo woman, 45 Kgs (Belgian Vietnam origin)! Blank medical
My Special Cytosorb Case Fabio Silvio TACCONE Dpt of Intensive Care Hôpital Erasme ULB Brussels (BE) Conflicts of Interest Clinical Case - 1! 27 yo woman, 45 Kgs (Belgian Vietnam origin)! Blank medical
ECMO for Refractory Septic Shock Prof. Alain Combes
 ECMO for Refractory Septic Shock Prof. Alain Combes Service de Réanimation ican, Institute of Cardiometabolism and Nutrition Hôpital Pitié-Salpêtrière, AP-HP, Paris Université Pierre et Marie Curie, Paris
ECMO for Refractory Septic Shock Prof. Alain Combes Service de Réanimation ican, Institute of Cardiometabolism and Nutrition Hôpital Pitié-Salpêtrière, AP-HP, Paris Université Pierre et Marie Curie, Paris
Management of refractory ARDS. Saurabh maji
 Management of refractory ARDS Saurabh maji Refractory hypoxemia as PaO2/FIO2 is less than 100 mm Hg, inability to keep plateau pressure below 30 cm H2O despite a VT of 4 ml/kg development of barotrauma
Management of refractory ARDS Saurabh maji Refractory hypoxemia as PaO2/FIO2 is less than 100 mm Hg, inability to keep plateau pressure below 30 cm H2O despite a VT of 4 ml/kg development of barotrauma
ICU management and referral guidelines for severe hypoxic respiratory failure
 Aim: ICU management and referral guidelines for severe hypoxic respiratory failure 1) To provide a concise management plan Non ventilatory Ventilatory 2) Timeline for referring patient with refractory
Aim: ICU management and referral guidelines for severe hypoxic respiratory failure 1) To provide a concise management plan Non ventilatory Ventilatory 2) Timeline for referring patient with refractory
Surgery Grand Rounds. Non-invasive Ventilation: A valuable tool. James Cromie, PGY 3 8/24/09
 Surgery Grand Rounds Non-invasive Ventilation: A valuable tool James Cromie, PGY 3 8/24/09 History of mechanical ventilation 1930 s: use of iron lung 1940 s: First NIV system (Bellevue Hospital) 1950 s:
Surgery Grand Rounds Non-invasive Ventilation: A valuable tool James Cromie, PGY 3 8/24/09 History of mechanical ventilation 1930 s: use of iron lung 1940 s: First NIV system (Bellevue Hospital) 1950 s:
PATIENT SELECTION FOR ACUTE APPLICATION OF ECMO, ECCOR, ETC.
 PATIENT SELECTION FOR ACUTE APPLICATION OF ECMO, ECCOR, ETC. J. CHRISTOPHER FARMER, MD PROFESSOR OF MEDICINE CHAIR OF CRITICAL CARE MEDICINE MAYO CLINIC PHOENIX, AZ Dr. Chris Farmer is a critical care
PATIENT SELECTION FOR ACUTE APPLICATION OF ECMO, ECCOR, ETC. J. CHRISTOPHER FARMER, MD PROFESSOR OF MEDICINE CHAIR OF CRITICAL CARE MEDICINE MAYO CLINIC PHOENIX, AZ Dr. Chris Farmer is a critical care
Effects of mechanical ventilation on organ function. Masterclass ICU nurses
 Effects of mechanical ventilation on organ function Masterclass ICU nurses Case Male, 60 - No PMH - L 1.74 m and W 85 kg Pneumococcal pneumonia Stable hemodynamics - No AKI MV in prone position (PEEP 16
Effects of mechanical ventilation on organ function Masterclass ICU nurses Case Male, 60 - No PMH - L 1.74 m and W 85 kg Pneumococcal pneumonia Stable hemodynamics - No AKI MV in prone position (PEEP 16
ECLS Bridge to Lung Transplantation Optimizing and Ambulating the Recipient
 ECLS Bridge to Lung Transplantation Optimizing and Ambulating the Recipient Shaf Keshavjee MD MSc FRCSC FACS Surgeon-in-Chief, University Health Network James Wallace McCutcheon Chair in Surgery Director,
ECLS Bridge to Lung Transplantation Optimizing and Ambulating the Recipient Shaf Keshavjee MD MSc FRCSC FACS Surgeon-in-Chief, University Health Network James Wallace McCutcheon Chair in Surgery Director,
Experience with Low Flow ECCO2R device on a CRRT platform : CO2 removal
 Experience with Low Flow ECCO2R device on a CRRT platform : CO2 removal Alain Combes, MD, PhD, Hôpital Pitié-Salpêtrière, AP-HP Inserm UMRS 1166, ican, Institute of Cardiometabolism and Nutrition Pierre
Experience with Low Flow ECCO2R device on a CRRT platform : CO2 removal Alain Combes, MD, PhD, Hôpital Pitié-Salpêtrière, AP-HP Inserm UMRS 1166, ican, Institute of Cardiometabolism and Nutrition Pierre
ECLS as Bridge to Transplant
 ECLS as Bridge to Transplant Marcelo Cypel MD, MSc Assistant Professor of Surgery Division of Thoracic Surgery Toronto General Hospital University of Toronto Application of ECLS Bridge to lung recovery
ECLS as Bridge to Transplant Marcelo Cypel MD, MSc Assistant Professor of Surgery Division of Thoracic Surgery Toronto General Hospital University of Toronto Application of ECLS Bridge to lung recovery
Prone ventilation revisited in H1N1 patients
 International Journal of Advanced Multidisciplinary Research ISSN: 2393-8870 www.ijarm.com DOI: 10.22192/ijamr Volume 5, Issue 10-2018 Case Report DOI: http://dx.doi.org/10.22192/ijamr.2018.05.10.005 Prone
International Journal of Advanced Multidisciplinary Research ISSN: 2393-8870 www.ijarm.com DOI: 10.22192/ijamr Volume 5, Issue 10-2018 Case Report DOI: http://dx.doi.org/10.22192/ijamr.2018.05.10.005 Prone
Noninvasive respiratory support:why is it working?
 Noninvasive respiratory support:why is it working? Paolo Pelosi Department of Surgical Sciences and Integrated Diagnostics (DISC) IRCCS San Martino IST University of Genoa, Genoa, Italy ppelosi@hotmail.com
Noninvasive respiratory support:why is it working? Paolo Pelosi Department of Surgical Sciences and Integrated Diagnostics (DISC) IRCCS San Martino IST University of Genoa, Genoa, Italy ppelosi@hotmail.com
EXTRACORPOREAL MEMBRANE OXYGENATION (ECMO) REFERRAL FORM
 REFERRAL FORM") Patient Label This form is accessible on www.royalpapworth.nhs.uk Intensive Care Unit EXTRACORPOREAL MEMBRANE OXYGENATION (ECMO) REFERRAL FORM Please always phone Papworth ECMO Coordinator on 01480 830541,
Patient Label This form is accessible on www.royalpapworth.nhs.uk Intensive Care Unit EXTRACORPOREAL MEMBRANE OXYGENATION (ECMO) REFERRAL FORM Please always phone Papworth ECMO Coordinator on 01480 830541,
ECMO CPR. Ravi R. Thiagarajan MBBS, MPH. Cardiac Intensive Care Unit
 ECMO CPR Ravi R. Thiagarajan MBBS, MPH Staff Intensivist Cardiac Intensive Care Unit Children s Hospital Boston PCICS 2008, Miami, FL No disclosures Disclosures Outline Outcomes for Pediatric in-hospital
ECMO CPR Ravi R. Thiagarajan MBBS, MPH Staff Intensivist Cardiac Intensive Care Unit Children s Hospital Boston PCICS 2008, Miami, FL No disclosures Disclosures Outline Outcomes for Pediatric in-hospital
ARDS: The Evidence. Topics. New definition Breaths: Little or Big? Wet or Dry? Moving or Still? Upside down or Right side up?
 ARDS: The Evidence Todd M Bull MD Professor of Medicine Division of Pulmonary Sciences and Critical Care Division of Cardiology Director Pulmonary Vascular Disease Center Director Center for Lungs and
ARDS: The Evidence Todd M Bull MD Professor of Medicine Division of Pulmonary Sciences and Critical Care Division of Cardiology Director Pulmonary Vascular Disease Center Director Center for Lungs and
Extracorporeal Membrane Oxygenation (ECMO)
") Extracorporeal Membrane Oxygenation (ECMO) Policy Number: Original Effective Date: MM.12.006 05/16/2006 Line(s) of Business: Current Effective Date: HMO; PPO; QUEST Integration 11/01/2014 Section: Other/Miscellaneous
Extracorporeal Membrane Oxygenation (ECMO) Policy Number: Original Effective Date: MM.12.006 05/16/2006 Line(s) of Business: Current Effective Date: HMO; PPO; QUEST Integration 11/01/2014 Section: Other/Miscellaneous
Extracorporeal Membrane Oxygenation (ECMO)
") Extracorporeal Membrane Oxygenation (ECMO) Policy Number: Original Effective Date: MM.12.006 05/16/2006 Line(s) of Business: Current Effective Date: HMO; PPO; QUEST Integration 01/01/2017 Section: Other/Miscellaneous
Extracorporeal Membrane Oxygenation (ECMO) Policy Number: Original Effective Date: MM.12.006 05/16/2006 Line(s) of Business: Current Effective Date: HMO; PPO; QUEST Integration 01/01/2017 Section: Other/Miscellaneous
Application of Lung Protective Ventilation MUST Begin Immediately After Intubation
 Conflict of Interest Disclosure Robert M Kacmarek Managing Severe Hypoxemia!" 9-28-17 FOCUS Bob Kacmarek PhD, RRT Massachusetts General Hospital, Harvard Medical School, Boston, Massachusetts I disclose
Conflict of Interest Disclosure Robert M Kacmarek Managing Severe Hypoxemia!" 9-28-17 FOCUS Bob Kacmarek PhD, RRT Massachusetts General Hospital, Harvard Medical School, Boston, Massachusetts I disclose
ECLS. The Basics. Jeannine Hermens Intensive Care Center UMC Utrecht
 ECLS The Basics Jeannine Hermens Intensive Care Center UMC Utrecht Conflict of interest None Terminology ECMO - ExtraCorporeal Membrane Oxygenation ECLS - ExtraCorporeal Life Support PLS - Veno-venous
ECLS The Basics Jeannine Hermens Intensive Care Center UMC Utrecht Conflict of interest None Terminology ECMO - ExtraCorporeal Membrane Oxygenation ECLS - ExtraCorporeal Life Support PLS - Veno-venous
Sepsis: Management ANUPOL PANITCHOTE, MD. Division of Critical Care Medicine Department of Medicine, Khon Kaen University, Thailand
 Sepsis: Management ANUPOL PANITCHOTE, MD. Division of Critical Care Medicine Department of Medicine, Khon Kaen University, Thailand Vital signs Symptoms LAB BT > 38.3 or < 36 ๐ C HR > 90 bpm RR > 20 /min
Sepsis: Management ANUPOL PANITCHOTE, MD. Division of Critical Care Medicine Department of Medicine, Khon Kaen University, Thailand Vital signs Symptoms LAB BT > 38.3 or < 36 ๐ C HR > 90 bpm RR > 20 /min
ECMO and refractory Hypoxemia
 ECMO and refractory Hypoxemia Dr. Vinay Dhingra MD FRCPC Clinical Associate Professor of Medicine Clinical Lead Critical Care BCPSQC Medical Director Quality VGH Disclosures ARDS Lancet 1967; 2:319-323
ECMO and refractory Hypoxemia Dr. Vinay Dhingra MD FRCPC Clinical Associate Professor of Medicine Clinical Lead Critical Care BCPSQC Medical Director Quality VGH Disclosures ARDS Lancet 1967; 2:319-323
Sepsis. From EMS to ER to ICU. What we need to be doing
 Sepsis From EMS to ER to ICU What we need to be doing NEHAL BHATT, MD ATHENS PULMONARY, CRITICAL CARE AND SLEEP Objectives 1. Define the changes to the definition of Sepsis 2. Describe the assessment,
Sepsis From EMS to ER to ICU What we need to be doing NEHAL BHATT, MD ATHENS PULMONARY, CRITICAL CARE AND SLEEP Objectives 1. Define the changes to the definition of Sepsis 2. Describe the assessment,
Prolonged Extracorporeal Membrane Oxygenation Support for Acute Respiratory Distress Syndrome
 CASE REPORT Prolonged Extracorporeal Membrane Oxygenation Support for Acute Respiratory Distress Syndrome Wen-Je Ko,* Hsao-Hsun Hsu, Pi-Ru Tsai When all conventional treatments for respiratory failure
CASE REPORT Prolonged Extracorporeal Membrane Oxygenation Support for Acute Respiratory Distress Syndrome Wen-Je Ko,* Hsao-Hsun Hsu, Pi-Ru Tsai When all conventional treatments for respiratory failure
R2R: Severe sepsis/septic shock. Surat Tongyoo Critical care medicine Siriraj Hospital
 R2R: Severe sepsis/septic shock Surat Tongyoo Critical care medicine Siriraj Hospital Diagnostic criteria ACCP/SCCM consensus conference 1991 SCCM/ESICM/ACCP/ATS/SIS International Sepsis Definitions Conference
R2R: Severe sepsis/septic shock Surat Tongyoo Critical care medicine Siriraj Hospital Diagnostic criteria ACCP/SCCM consensus conference 1991 SCCM/ESICM/ACCP/ATS/SIS International Sepsis Definitions Conference
ECMO FOR PEDIATRIC RESPIRATORY FAILURE. Novik Budiwardhana * PCICU Harapan Kita National Cardiovascular Center Jakarta
 ECMO FOR PEDIATRIC RESPIRATORY FAILURE Novik Budiwardhana * PCICU Harapan Kita National Cardiovascular Center Jakarta Introduction Case D 8 month old baby with severe ARDS with fungal sepsis. He was on
ECMO FOR PEDIATRIC RESPIRATORY FAILURE Novik Budiwardhana * PCICU Harapan Kita National Cardiovascular Center Jakarta Introduction Case D 8 month old baby with severe ARDS with fungal sepsis. He was on
EXTRA CORPOREAL MEMBRANE OXYGENATION
 EXTRA CORPOREAL MEMBRANE OXYGENATION Basic Overview and Case Study Bob Hayes, Chief Perfusionist Enloe Medical Center Jenny Humphries, RN, BSN, MBA, CFRN Chief Flight Nurse, Enloe FlightCare Normal Cardiopulmonary
EXTRA CORPOREAL MEMBRANE OXYGENATION Basic Overview and Case Study Bob Hayes, Chief Perfusionist Enloe Medical Center Jenny Humphries, RN, BSN, MBA, CFRN Chief Flight Nurse, Enloe FlightCare Normal Cardiopulmonary
Oxygenation Failure. Increase FiO2. Titrate end-expiratory pressure. Adjust duty cycle to increase MAP. Patient Positioning. Inhaled Vasodilators
 Oxygenation Failure Increase FiO2 Titrate end-expiratory pressure Adjust duty cycle to increase MAP Patient Positioning Inhaled Vasodilators Extracorporeal Circulation ARDS Radiology Increasing Intensity
Oxygenation Failure Increase FiO2 Titrate end-expiratory pressure Adjust duty cycle to increase MAP Patient Positioning Inhaled Vasodilators Extracorporeal Circulation ARDS Radiology Increasing Intensity
ERJ Express. Published on August 9, 2012 as doi: /
 ERJ Express. Published on August 9, 2012 as doi: 10.1183/09031936.00076912 Extracorporeal membrane oxygenation in a non intubated patient with acute respiratory distress syndrome (ARDS) Olaf Wiesner, *
ERJ Express. Published on August 9, 2012 as doi: 10.1183/09031936.00076912 Extracorporeal membrane oxygenation in a non intubated patient with acute respiratory distress syndrome (ARDS) Olaf Wiesner, *
Healing Breath. Disclosures. anuola. Extracorporeal Membrane Oxygenation Principles: Rest your lungs. Objectives ECMO: 8/28/17
 anuola Healing Breath ECMO Program of Hawaii Extracorporeal Membrane Oxygenation Principles: Rest your lungs Len Y. Tanaka, MD September 12, 2017 Disclosures No financial disclosures. However this presentation
anuola Healing Breath ECMO Program of Hawaii Extracorporeal Membrane Oxygenation Principles: Rest your lungs Len Y. Tanaka, MD September 12, 2017 Disclosures No financial disclosures. However this presentation
ACUTE RESPIRATORY DISTRESS SYNDROME
 ACUTE RESPIRATORY DISTRESS SYNDROME Angel Coz MD, FCCP, DCE Assistant Professor of Medicine UCSF Fresno November 4, 2017 No disclosures OBJECTIVES Identify current trends and risk factors of ARDS Describe
ACUTE RESPIRATORY DISTRESS SYNDROME Angel Coz MD, FCCP, DCE Assistant Professor of Medicine UCSF Fresno November 4, 2017 No disclosures OBJECTIVES Identify current trends and risk factors of ARDS Describe
Year in Review Intensive Care Training Program Radboud University Medical Centre Nijmegen
 Year in Review 2013 Intensive Care Training Program Radboud University Medical Centre Nijmegen Contents ARDS Ventilator associated pneumonia Tracheostomy and endotracheal intubation Enteral feeding Fluid
Year in Review 2013 Intensive Care Training Program Radboud University Medical Centre Nijmegen Contents ARDS Ventilator associated pneumonia Tracheostomy and endotracheal intubation Enteral feeding Fluid
11 th Annual Congress Turkish Thoracic Society. Mechanical Ventilation in Acute Hypoxemic Respiratory Failure
 11 th Annual Congress Turkish Thoracic Society Mechanical Ventilation in Acute Hypoxemic Respiratory Failure Lluis Blanch MD PhD Senior Critical Care Center Scientific Director Corporació Parc Taulí Universitat
11 th Annual Congress Turkish Thoracic Society Mechanical Ventilation in Acute Hypoxemic Respiratory Failure Lluis Blanch MD PhD Senior Critical Care Center Scientific Director Corporació Parc Taulí Universitat
Inhaled nitric oxide: clinical evidence for use in adults
 Inhaled nitric oxide: clinical evidence for use in adults Neill Adhikari Critical Care Medicine Sunnybrook Health Sciences Centre and University of Toronto 31 October 2014 Conflict of interest Ikaria provided
Inhaled nitric oxide: clinical evidence for use in adults Neill Adhikari Critical Care Medicine Sunnybrook Health Sciences Centre and University of Toronto 31 October 2014 Conflict of interest Ikaria provided
ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) Rv
 Rv") ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) Rv.8.18.18 ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) SUDDEN PROGRESSIVE FORM OF ACUTE RESPIRATORY FAILURE ALVEOLAR CAPILLARY MEMBRANE BECOMES DAMAGED AND MORE
ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) Rv.8.18.18 ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) SUDDEN PROGRESSIVE FORM OF ACUTE RESPIRATORY FAILURE ALVEOLAR CAPILLARY MEMBRANE BECOMES DAMAGED AND MORE
Kevin K. Nunnink Extracorporeal Membrane Oxygenation Program
 PATIE NT I N FO R M ATI O N Kevin K. Nunnink Extracorporeal Membrane Oxygenation Program A family s guide to understanding this specialized treatment for cardiac and pulmonary complications Saint Luke
PATIE NT I N FO R M ATI O N Kevin K. Nunnink Extracorporeal Membrane Oxygenation Program A family s guide to understanding this specialized treatment for cardiac and pulmonary complications Saint Luke
Extracorporeal Life Support (ECLS) as a Bridge to Decision in Lung Transplantation
 as a Bridge to Decision in Lung Transplantation") Extracorporeal Life Support (ECLS) as a Bridge to Decision in Lung Transplantation Gabriel Loor, MD Baylor St. Lukes Medical Center Surgical Director Lung Transplantation Co-chief Section of Adult Cardiac
Extracorporeal Life Support (ECLS) as a Bridge to Decision in Lung Transplantation Gabriel Loor, MD Baylor St. Lukes Medical Center Surgical Director Lung Transplantation Co-chief Section of Adult Cardiac
Sepsis overview. Dr. Tsang Hin Hung MBBS FHKCP FRCP
 Sepsis overview Dr. Tsang Hin Hung MBBS FHKCP FRCP Epidemiology Sepsis, severe sepsis, septic shock Pathophysiology of sepsis Recent researches and advances From bench to bedside Sepsis bundle Severe sepsis
Sepsis overview Dr. Tsang Hin Hung MBBS FHKCP FRCP Epidemiology Sepsis, severe sepsis, septic shock Pathophysiology of sepsis Recent researches and advances From bench to bedside Sepsis bundle Severe sepsis
In the setting of liver failure & transplantation?
 ECMO: In the setting of liver failure & transplantation? Dr. Robert Loveridge MA LL.M MRCP FRCA FFICM Consultant in adult & liver intensive care medicine King s College Hospital NHS Foundation Trust What
ECMO: In the setting of liver failure & transplantation? Dr. Robert Loveridge MA LL.M MRCP FRCA FFICM Consultant in adult & liver intensive care medicine King s College Hospital NHS Foundation Trust What
Keeping Patients Off the Vent: Bilevel, HFNC, Neither?
 Keeping Patients Off the Vent: Bilevel, HFNC, Neither? Robert Kempainen, MD Pulmonary and Critical Care Medicine Hennepin County Medical Center University of Minnesota School of Medicine Objectives Summarize
Keeping Patients Off the Vent: Bilevel, HFNC, Neither? Robert Kempainen, MD Pulmonary and Critical Care Medicine Hennepin County Medical Center University of Minnesota School of Medicine Objectives Summarize
The Association Between Oxygenation Thresholds and Mortality During Extracorporeal Life Support
 The Association Between Oxygenation Thresholds and Mortality During Extracorporeal Life Support Laveena Munshi, MD, MSc November 1, 2016 Critical Care Canada Forum Interdepartmental Division of Critical
The Association Between Oxygenation Thresholds and Mortality During Extracorporeal Life Support Laveena Munshi, MD, MSc November 1, 2016 Critical Care Canada Forum Interdepartmental Division of Critical
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE
 NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE INTERVENTIONAL PROCEDURES PROGRAMME Interventional procedure overview of extracorporeal carbon dioxide removal for acute respiratory failure Extracorporeal
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE INTERVENTIONAL PROCEDURES PROGRAMME Interventional procedure overview of extracorporeal carbon dioxide removal for acute respiratory failure Extracorporeal
Weaning and extubation in PICU An evidence-based approach
 Weaning and extubation in PICU An evidence-based approach Suchada Sritippayawan, MD. Div. Pulmonology & Crit Care Dept. Pediatrics Faculty of Medicine Chulalongkorn University Kanokporn Udomittipong, MD.
Weaning and extubation in PICU An evidence-based approach Suchada Sritippayawan, MD. Div. Pulmonology & Crit Care Dept. Pediatrics Faculty of Medicine Chulalongkorn University Kanokporn Udomittipong, MD.
AllinaHealthSystem 1
 : Definition End-organ hypoperfusion secondary to cardiac failure Venoarterial ECMO: Patient Selection Michael A. Samara, MD FACC Advanced Heart Failure, Cardiac Transplant & Mechanical Circulatory Support
: Definition End-organ hypoperfusion secondary to cardiac failure Venoarterial ECMO: Patient Selection Michael A. Samara, MD FACC Advanced Heart Failure, Cardiac Transplant & Mechanical Circulatory Support
Landmark articles on ventilation
 Landmark articles on ventilation Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity ARDS AECC DEFINITION-1994 ALI Acute onset Bilateral chest infiltrates PCWP
Landmark articles on ventilation Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity ARDS AECC DEFINITION-1994 ALI Acute onset Bilateral chest infiltrates PCWP
ECCO 2 Removal The Perfusionists Perspective
 ECCO 2 Removal The Perfusionists Perspective BelSECT Education evening 2016-06-15 D. Hella, Th. Amand, J-N Koch Definition ECCO 2 Removal: Process by which an extracorporeal circuit is used for removing
ECCO 2 Removal The Perfusionists Perspective BelSECT Education evening 2016-06-15 D. Hella, Th. Amand, J-N Koch Definition ECCO 2 Removal: Process by which an extracorporeal circuit is used for removing
(almost) 4/22/2016 Updated. AllinaHealthSystem. Things To Know About
 4/22/2016 Updated. AllinaHealthSystem. Things To Know About") (almost) Susan C Seatter MD Abbott Northwestern Hospital Intensivists Advanced Circulatory Support for the Critically Ill Adult April 22, 2016 1 Consider ECMO Early 2 Don t Use The Lungs 3a Know Your Circuit
(almost) Susan C Seatter MD Abbott Northwestern Hospital Intensivists Advanced Circulatory Support for the Critically Ill Adult April 22, 2016 1 Consider ECMO Early 2 Don t Use The Lungs 3a Know Your Circuit
Samphant Ponvilawan Bumrungrad International
 Samphant Ponvilawan Bumrungrad International Definitions Artificial circulation using VA ECMO as an alternative to ventilation and external cardiac massage Indications Out-of-Hospital Cardiac Arrest (OHCA)
Samphant Ponvilawan Bumrungrad International Definitions Artificial circulation using VA ECMO as an alternative to ventilation and external cardiac massage Indications Out-of-Hospital Cardiac Arrest (OHCA)
ECMO Experience from ECMO-ICU, Karolinska
 ECMO Experience from ECMO-ICU, Karolinska X Curso de Ventilacion Mecanica en Anestesia, Cuidados Criticos y Transplantes Madrid 2012 International numbers Totally since 1989; 46500 patients as of July
ECMO Experience from ECMO-ICU, Karolinska X Curso de Ventilacion Mecanica en Anestesia, Cuidados Criticos y Transplantes Madrid 2012 International numbers Totally since 1989; 46500 patients as of July
Weaning from Mechanical Ventilation. Dr Azmin Huda Abdul Rahim
 Weaning from Mechanical Ventilation Dr Azmin Huda Abdul Rahim Content Definition Classification Weaning criteria Weaning methods Criteria for extubation Introduction Weaning comprises 40% of the duration
Weaning from Mechanical Ventilation Dr Azmin Huda Abdul Rahim Content Definition Classification Weaning criteria Weaning methods Criteria for extubation Introduction Weaning comprises 40% of the duration
FOCUS CONFERENCE 2018
 FOCUS CONFERENCE 2018 Current Practice in Pediatric and Neonatal Extracorporeal Life Support Daniel W. Chipman, RRT Assistant Director of Respiratory Care Massachusetts General Hospital Boston, Massachusetts
FOCUS CONFERENCE 2018 Current Practice in Pediatric and Neonatal Extracorporeal Life Support Daniel W. Chipman, RRT Assistant Director of Respiratory Care Massachusetts General Hospital Boston, Massachusetts
CPR What Works, What Doesn t
 Resuscitation 2017 ECMO and ECLS April 1, 2017 Corey M. Slovis, M.D. Vanderbilt University Medical Center Metro Nashville Fire Department Nashville International Airport Nashville, TN Circulation 2013;128:417-35
Resuscitation 2017 ECMO and ECLS April 1, 2017 Corey M. Slovis, M.D. Vanderbilt University Medical Center Metro Nashville Fire Department Nashville International Airport Nashville, TN Circulation 2013;128:417-35
The Art and Science of Weaning from Mechanical Ventilation
 The Art and Science of Weaning from Mechanical Ventilation Shekhar T. Venkataraman M.D. Professor Departments of Critical Care Medicine and Pediatrics University of Pittsburgh School of Medicine Some definitions
The Art and Science of Weaning from Mechanical Ventilation Shekhar T. Venkataraman M.D. Professor Departments of Critical Care Medicine and Pediatrics University of Pittsburgh School of Medicine Some definitions
CASE PRESENTATION VV ECMO
 CASE PRESENTATION VV ECMO Joshua Huelster, MD Fellow in Critical Care Medicine Department of Pulmonary and Critical Care Medicine Hennepin County Medical Center Disclosure There are no conflicts of interest
CASE PRESENTATION VV ECMO Joshua Huelster, MD Fellow in Critical Care Medicine Department of Pulmonary and Critical Care Medicine Hennepin County Medical Center Disclosure There are no conflicts of interest
Management of Respiratory Failure: The Surgical Perspective. When Traditional Respiratory Support Techniques fail. ARDS: Evidence Based Practice
 Critical Care Medicine and Trauma Management of Respiratory Failure: The Surgical Perspective Jasleen Kukreja, M.D. Division of Cardiothoracic Surgery University of California San Francisco When Traditional
Critical Care Medicine and Trauma Management of Respiratory Failure: The Surgical Perspective Jasleen Kukreja, M.D. Division of Cardiothoracic Surgery University of California San Francisco When Traditional
Effective Date: Approved by: Laboratory Director, Jerry Barker (electronic signature)
") 1 of 5 Policy #: 702 (PHL-702-05) Effective Date: 9/30/2004 Reviewed Date: 8/1/2016 Subject: TRANSFUSION GUIDELINES Approved by: Laboratory Director, Jerry Barker (electronic signature) Approved by: Laboratory
1 of 5 Policy #: 702 (PHL-702-05) Effective Date: 9/30/2004 Reviewed Date: 8/1/2016 Subject: TRANSFUSION GUIDELINES Approved by: Laboratory Director, Jerry Barker (electronic signature) Approved by: Laboratory
Mechanical ventilation induced or exacerbated right ventricular failure
 Mechanical ventilation induced or exacerbated right ventricular failure Toronto 2016 Jesse Hall MD Professor of Medicine, Anesthesia & Critical Care University of Chicago Faculty Disclosures Dr. Hall
Mechanical ventilation induced or exacerbated right ventricular failure Toronto 2016 Jesse Hall MD Professor of Medicine, Anesthesia & Critical Care University of Chicago Faculty Disclosures Dr. Hall
Use of Blood Lactate Measurements in the Critical Care Setting
 Use of Blood Lactate Measurements in the Critical Care Setting John G Toffaletti, PhD Director of Blood Gas and Clinical Pediatric Labs Professor of Pathology Duke University Medical Center Chief, VAMC
Use of Blood Lactate Measurements in the Critical Care Setting John G Toffaletti, PhD Director of Blood Gas and Clinical Pediatric Labs Professor of Pathology Duke University Medical Center Chief, VAMC
ARDS and Lung Protection
 ARDS and Lung Protection Kristina Sullivan, MD Associate Professor University of California, San Francisco Department of Anesthesia and Perioperative Care Division of Critical Care Medicine Overview Low
ARDS and Lung Protection Kristina Sullivan, MD Associate Professor University of California, San Francisco Department of Anesthesia and Perioperative Care Division of Critical Care Medicine Overview Low
Staging Sepsis for the Emergency Department: Physician
 Staging Sepsis for the Emergency Department: Physician Sepsis Continuum 1 Sepsis Continuum SIRS = 2 or more clinical criteria, resulting in Systemic Inflammatory Response Syndrome Sepsis = SIRS + proven/suspected
Staging Sepsis for the Emergency Department: Physician Sepsis Continuum 1 Sepsis Continuum SIRS = 2 or more clinical criteria, resulting in Systemic Inflammatory Response Syndrome Sepsis = SIRS + proven/suspected
Cardiovascular Institute
 Allegheny Health Network Cardiovascular Institute Extracorporeal Membrane Oxygenation (ECMO) Program Our patient survival rate is higher than the national average. ECMO experts. Multidisciplinary team.
Allegheny Health Network Cardiovascular Institute Extracorporeal Membrane Oxygenation (ECMO) Program Our patient survival rate is higher than the national average. ECMO experts. Multidisciplinary team.
PHYSIOLOGY AND MANAGEMENT OF THE SEPTIC PATIENT
 PHYSIOLOGY AND MANAGEMENT OF THE SEPTIC PATIENT Melanie Sanchez, RN, MSNE, OCN, CCRN Clinical Nurse III City of Hope National Medical Center HOW THE EXPERTS TREAT HEMATOLOGIC MALIGNANCIES LAS VEGAS, NV
PHYSIOLOGY AND MANAGEMENT OF THE SEPTIC PATIENT Melanie Sanchez, RN, MSNE, OCN, CCRN Clinical Nurse III City of Hope National Medical Center HOW THE EXPERTS TREAT HEMATOLOGIC MALIGNANCIES LAS VEGAS, NV
Respiratory insufficiency in bariatric patients
 Respiratory insufficiency in bariatric patients Special considerations or just more of the same? Weaning and rehabilation conference 6th November 2015 Definition of obesity Underweight BMI< 18 Normal weight
Respiratory insufficiency in bariatric patients Special considerations or just more of the same? Weaning and rehabilation conference 6th November 2015 Definition of obesity Underweight BMI< 18 Normal weight
Back to the Future: Updated Guidelines for Evaluation and Management of Adrenal Insufficiency in the Critically Ill
 Back to the Future: Updated Guidelines for Evaluation and Management of Adrenal Insufficiency in the Critically Ill Joe Palumbo PGY-2 Critical Care Pharmacy Resident Buffalo General Medical Center Disclosures
Back to the Future: Updated Guidelines for Evaluation and Management of Adrenal Insufficiency in the Critically Ill Joe Palumbo PGY-2 Critical Care Pharmacy Resident Buffalo General Medical Center Disclosures
Innovative ECMO Configurations in Adults
 Innovative ECMO Configurations in Adults Practice at a Single Center with Platinum Level ELSO Award for Excellence in Life Support Monika Tukacs, BSN, RN, CCRN Columbia University Irving Medical Center,
Innovative ECMO Configurations in Adults Practice at a Single Center with Platinum Level ELSO Award for Excellence in Life Support Monika Tukacs, BSN, RN, CCRN Columbia University Irving Medical Center,
THE USE OF HYPERINFLATION IN THE MANAGEMENT OF INTUBATED AND VENTILATED ADULT PATIENTS RECOMMENDATIONS
 THE USE OF HYPERINFLATION IN THE MANAGEMENT OF INTUBATED AND VENTILATED ADULT PATIENTS RECOMMENDATIONS Recommendation 1 on website Hyperinflation (Ventilator or manual) might be included in the management
THE USE OF HYPERINFLATION IN THE MANAGEMENT OF INTUBATED AND VENTILATED ADULT PATIENTS RECOMMENDATIONS Recommendation 1 on website Hyperinflation (Ventilator or manual) might be included in the management
ECMO: the wave of the future??
 ECMO: the wave of the future?? 15th May 2018 P. Andrew Stephens, MD, FACEP LTC, MC, FS, DMO 19th Special Forces Group (Airborne) Surgeon Background Armored Cav Board EM Critical Care Neurocritical Care
ECMO: the wave of the future?? 15th May 2018 P. Andrew Stephens, MD, FACEP LTC, MC, FS, DMO 19th Special Forces Group (Airborne) Surgeon Background Armored Cav Board EM Critical Care Neurocritical Care
The new ARDS definitions: what does it mean?
 The new ARDS definitions: what does it mean? Richard Beale 7 th September 2012 METHODS ESICM convened an international panel of experts, with representation of ATS and SCCM The objectives were to update
The new ARDS definitions: what does it mean? Richard Beale 7 th September 2012 METHODS ESICM convened an international panel of experts, with representation of ATS and SCCM The objectives were to update
Sepsis is an important issue. Clinician s decision-making capability. Guideline recommendations
 Surviving Sepsis Campaign: International Guidelines for Management of Severe Sepsis and Septic Shock: 2012 Clinicians decision-making capability Guideline recommendations Sepsis is an important issue 8.7%
Surviving Sepsis Campaign: International Guidelines for Management of Severe Sepsis and Septic Shock: 2012 Clinicians decision-making capability Guideline recommendations Sepsis is an important issue 8.7%
How ARDS should be treated in 2017
 How ARDS should be treated in 2017 2017, Ostrava Luciano Gattinoni, MD, FRCP Georg-August-Universität Göttingen Germany ARDS 1. Keep the patient alive respiration circulation 2. Cure the disease leading
How ARDS should be treated in 2017 2017, Ostrava Luciano Gattinoni, MD, FRCP Georg-August-Universität Göttingen Germany ARDS 1. Keep the patient alive respiration circulation 2. Cure the disease leading
Extracorporeal Membrane Oxygenation (ECMO) Referrals
 Referrals") Children s Acute Transport Service Clinical Guideline Extracorporeal Membrane Oxygenation (ECMO) Referrals Document Control Information Author ECMO/CATS Author Position Service Coordinator Document Owner
Children s Acute Transport Service Clinical Guideline Extracorporeal Membrane Oxygenation (ECMO) Referrals Document Control Information Author ECMO/CATS Author Position Service Coordinator Document Owner
Introduction and Overview of Acute Respiratory Failure
 Introduction and Overview of Acute Respiratory Failure Definition: Acute Respiratory Failure Failure to oxygenate Inadequate PaO 2 to saturate hemoglobin PaO 2 of 60 mm Hg ~ SaO 2 of 90% PaO 2 of 50 mm
Introduction and Overview of Acute Respiratory Failure Definition: Acute Respiratory Failure Failure to oxygenate Inadequate PaO 2 to saturate hemoglobin PaO 2 of 60 mm Hg ~ SaO 2 of 90% PaO 2 of 50 mm
Bronchoalveolar lavage (BAL) with surfactant in pediatric ARDS
 with surfactant in pediatric ARDS") Bronchoalveolar lavage (BAL) with surfactant in pediatric ARDS M. Luchetti, E. M. Galassini, A. Galbiati, C. Pagani,, F. Silla and G. A. Marraro gmarraro@picu.it www.picu.it Anesthesia and Intensive Care
Bronchoalveolar lavage (BAL) with surfactant in pediatric ARDS M. Luchetti, E. M. Galassini, A. Galbiati, C. Pagani,, F. Silla and G. A. Marraro gmarraro@picu.it www.picu.it Anesthesia and Intensive Care
Difficult Ventilation in ARDS Patients
 Thank you for viewing this presentation. We would like to remind you that this material is the property of the author. It is provided to you by the ERS for your personal use only, as submitted by the author.
Thank you for viewing this presentation. We would like to remind you that this material is the property of the author. It is provided to you by the ERS for your personal use only, as submitted by the author.
ECMO in oncology and immunosupressed patients. Peter Schellongowski Department of Medicine I Intensive Care Unit 13.i2 Medical University of Vienna
 ECMO in oncology and immunosupressed patients Peter Schellongowski Department of Medicine I Intensive Care Unit 13.i2 Medical University of Vienna ECMO in immunocompromised patients? Is it feasible? Is
ECMO in oncology and immunosupressed patients Peter Schellongowski Department of Medicine I Intensive Care Unit 13.i2 Medical University of Vienna ECMO in immunocompromised patients? Is it feasible? Is
NIV in Acute Respiratory Failure: Where we fail? Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity
 NIV in Acute Respiratory Failure: Where we fail? Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity Use of NIV 1998-2010 50 45 40 35 30 25 20 15 10 5 0 1998
NIV in Acute Respiratory Failure: Where we fail? Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity Use of NIV 1998-2010 50 45 40 35 30 25 20 15 10 5 0 1998
Rounds in the ICU. Eran Segal, MD Director General ICU Sheba Medical Center
 Rounds in the ICU Eran Segal, MD Director General ICU Sheba Medical Center Real Clinical cases (including our mistakes) Emphasis on hemodynamic monitoring Usually no single correct answer We will conduct
Rounds in the ICU Eran Segal, MD Director General ICU Sheba Medical Center Real Clinical cases (including our mistakes) Emphasis on hemodynamic monitoring Usually no single correct answer We will conduct
WELCOME. Welcome to the Children s Hospital PICU (Pediatric Intensive Care Unit). We consider it a privilege to care for your child and your family.
. We consider it a privilege to care for your child and your family.") ECMO FAMILY GUIDE WELCOME Welcome to the Children s Hospital PICU (Pediatric Intensive Care Unit). We consider it a privilege to care for your child and your family. This book was created to give you the
ECMO FAMILY GUIDE WELCOME Welcome to the Children s Hospital PICU (Pediatric Intensive Care Unit). We consider it a privilege to care for your child and your family. This book was created to give you the
FAILURE OF NONINVASIVE VENTILATION FOR DE NOVO ACUTE HYPOXEMIC RESPIRATORY FAILURE: ROLE OF TIDAL VOLUME
 FAILURE OF NONINVASIVE VENTILATION FOR DE NOVO ACUTE HYPOXEMIC RESPIRATORY FAILURE: ROLE OF TIDAL VOLUME Guillaume CARTEAUX, Teresa MILLÁN-GUILARTE, Nicolas DE PROST, Keyvan RAZAZI, Shariq ABID, Arnaud
FAILURE OF NONINVASIVE VENTILATION FOR DE NOVO ACUTE HYPOXEMIC RESPIRATORY FAILURE: ROLE OF TIDAL VOLUME Guillaume CARTEAUX, Teresa MILLÁN-GUILARTE, Nicolas DE PROST, Keyvan RAZAZI, Shariq ABID, Arnaud