Hypertension Management. complications including stroke, dementia, coronary artery disease, left ventricular dysfunction, kidney
|
|
|
- Alexandrina Hodge
- 5 years ago
- Views:
Transcription
1 Hypertension Management Hypertension affects 19.7% of adult Canadians and is one of the most important modifiable risk factors for cardiovascular disease. 1 The prevalence continues to increase with more than 1000 people newly diagnosed with hypertension every day. 1 Uncontrolled hypertension can cause many different complications including stroke, dementia, coronary artery disease, left ventricular dysfunction, kidney disease, retinal disease and peripheral artery disease. 1 Assessment Blood pressure (BP) screening should be performed on all people over the age of 40 years to determine cardiovascular risk (ie. Framingham Risk Score) every 1-3 years. 1,2 Those with increased risk of cardiovascular disease should be screened more frequently. For the purposes of this study, the Framingham risk calculator will be used to determine cardiovascular risk for high risk patients and patients with chronic kidney disease. Other calculators that will be used in the study are for specific target populations. The UK Prospective Diabetes Study (UKPDS) 3 will be used for patients with diabetes and the International Model to Predict Recurrent Cardiovascular Disease 4 will be used for patients who have had a previous cardiovascular event (stroke, coronary artery disease or peripheral vascular disease). Diagnosis of hypertension can utilize ambulatory blood pressure measurements (ABPM), office blood pressure measurements (OBPM) or home blood pressure measurements (HBPM). Diagnosis is based on elevated systolic blood pressure (SBP), diastolic blood pressure (DBP) or both on several occasions. (See appendix 1 for a flow chart.) Current information suggests that HBPM has a stronger predictive association with cardiovascular prognosis than OBPM. 1 Home BP values greater than or equal to 135/85mmHg should be considered elevated and associated with an increased overall mortality risk analogous to office BP readings of greater than or equal to 140/90mmHg. Note that the diagnostic BP measurement for hypertension is not the same as the target BP for all groups.
2 Diagnosis of hypertension if BP greater than or equal to 1 OBPM ABPM HBPM Hypertensive urgency or emergency (SBP greater than 200mmHg or DBP greater than 130mmHg) Awake SBP 135 mmhg or DBP 85mmHg Greater than 180/100mmHg /90-109mmHg with organ damage or diabetes SBP 160mmHg or DBP 100mmHg over 3 visits SBP 140mmHg or DBP 90mmHg over 4-5 visit 24 hour average SBP 130mmHg or DBP 80mmHg Proper technique for BP measurement is critical to produce accurate results. Using a Average SBP 135 mmhg or DBP 85mmHg sphygmomanometer and stethoscope is the preferred method of determining blood pressure, but a calibrated automated blood pressure machine is acceptable. 1 Some automated machines can be programmed to take many measurements spaced 1-2 minutes apart. Wrist cuff blood pressure machines are not recommended for use in this study. See this link for additional information on blood pressure monitoring devices recommended by Hypertension Canada: BP measurement should be performed on both arms at least once to confirm similar readings. If the readings are different, always use the arm with the higher measurement for taking blood pressure. For the purposes of this study, use the same arm in the same position for all blood pressure monitoring. Steps for accurate blood pressure measurement: 1. Appropriate sized cuff 2. Rest 5 minutes, seated with back supported 3. No talking, do not cross legs 4. Bare arm resting and supported at heart level 5. Lower edge of cuff 3cm above elbow crease 6. Air bladder centered on brachial artery 7. 2 readings 1-2 minutes apart record average of the two readings 8. Record position (supine, sitting, standing) and arm (left or right) For more information see: pdf
 should target a systolic blood pressure less than 150mmHg since they are more susceptible to hypotension.")
3 The blood pressure target is less than 140/90mmHg in the majority of patients. 1 The exceptions are diabetics and very elderly. Diabetics should achieve a target blood pressure less than 130/80mmHg. 1 The very elderly (older than 80 years) should target a systolic blood pressure less than 150mmHg since they are more susceptible to hypotension. 1 Drug therapy should be titrated slowly to allow time for patients, especially elderly patients, to adjust. Hypotension places elderly patients at a high risk of falls that can have devastating consequences.
4 Treatment Once diagnosed with hypertension, antihypertensive therapy should be started when blood pressure is greater than 140/90mmHg. An important intervention is to address modifiable lifestyle risk factors that affect hypertension such as smoking cessation 1, physical exercise 1, weight reduction 1, alcohol consumption 1, healthy diet (DASH diet) 6, sodium intake 7 and stress management. 1 These health behaviours should be reinforced with every interaction with the patient in a non-threatening manner. Refer to the lifestyle management material for an in-depth discussion. The choice of initial antihypertensive should be individualized based on presence of comorbid conditions. In patients who have no heart disease, cerebrovascular disease, kidney disease or diabetes the choice of initial therapy is monotherapy with a thiazide diuretic, beta-blocker, angiotensin converting enzyme inhibitor (ACEi), angiotensin 2 receptor blocker (ARB) or long-acting calcium channel blocker (CCB). Thiazide diuretics are generally chosen first due to their cost efficiency. Patients taking a thiazide diuretic should be monitored for hypokalemia and prescribed potassium rich foods (such as bananas and oranges), a potassium supplement if required or potassium sparing diuretic. ACEi should not be used as first line in African Americans and beta-blockers should not be used as first line in patients older than 60 year. 1 Alpha blockers should not be used as first line monotherapy. 1 Combination therapy of both an ACEi and ARB is no longer recommended due to risk of adverse events except in patients with heart failure. 1 If a patient has SBP more than 20mmHg or DBP more than 10mmHg above their target, initial therapy with a combination may be considered; however, initiating more than one antihypertensive at the same time may cause significant hypotension and, therefore, in clinical practice usually one medication is initiated at a time. Useful combinations include a thiazide in combination with an ACEi, CCB, ARB or beta-blocker. 8 Consider starting on a low dose and titrating slowly as required until the patient reaches their target blood pressure. This information has been summarized in a table in Appendix 2.
5 Management of hypertension should follow a stepwise approach. If patients are intolerant, have side effects or have contraindications to initial therapy, another first line agent (thiazide, beta-blocker, ACEi, long-acting CCB or ARB) should be substituted. When patients continue to have SBP is 1-19mmHg or DBP is 1-9mmHg above goal with initial therapy, they should be assessed for any compliance or adherence issues, any other reasons for poor response and then prescribed a combination of first line agents such as a thiazide diuretic or CCB with an ACEi, ARB or beta-blocker. However, diltiazem or verapamil should be used very cautiously in combination with a beta-blocker. As mentioned before, the combination of an ACEi and ARB is not recommended for most patients. If patients have SBP more than 20mmHg or DBP more than 10mmHg above target with initial therapy, they should be assessed for any compliance or adherence issues, any other reasons for poor response and then prescribed additional antihypertensive drugs. Often these patients will require more than two antihypertensive drugs, but it is safer to start and titrate one at a time and assess response before adding a third medication. If the patient s blood pressure is below the target, the current regime should be continued. Individualization of therapy by comorbid conditions: The following information has been summarized in a table in Appendix 3. Patients with coronary artery disease should receive an ACEi or ARB; however, patients should not receive both an ACEi and an ARB. 1,8 If blood pressure is not controlled with a single agent the combination of an ACEi and dihydropyridine CCB (amlodipine, nifedipine, felodipine) is preferable over an ACEi and diuretic. 1 If the patient also has stable angina a beta-blocker is recommended. 1 All patients who have had a recent MI should be prescribed initial therapy of both an ACEi and betablocker. 1,8 If the patient is intolerant to or has side effects from the ACEi, an ARB may be combined with the beta-blocker. If a beta-blocker is not tolerated or contraindicated, the alternative is to prescribe a CCB; however, short acting CCB such as short acting nifedipine should not be used due to increase in hypotension and reflex sympathetic activation with tachycardia. 1,8,9
6 Patients who have left ventricle hypertrophy with normal ejection fraction and no symptoms of heart failure (edema, fatigue and dyspnea) have stage B heart failure. 9 Initial therapy for hypertension includes a thiazide diuretic, ACEi or beta-blocker; an ARB may be used in patients who have not tolerated an ACEi. 9,10 All these first line therapies are effective in preventing and delaying the onset of heart failure symptoms, although ACEi and ARB may be superior because they promote more regression of LVH than beta blockers or diuretics. 9,11 A proposed mechanism of how ACEi and ARB may slow or reversing cardiac remodelling is by reducing the effects of angiotensin II on the heart. Angiotensin II increases expression of proteins and myocyte hypertrophy and stimulates collagen synthesis that leads to fibrosis of the cardiac tissue. 12 A long-acting CCB may also be used, but they are not as effective as ACEi or beta-blockers in preventing or delaying the onset of heart failure symptoms. 9,11 These patients should not receive hydralazine or minoxidil because these direct arterial vasodilators do not alter the progression to heart failure and resulted in a poorer clinical course. 1 All patients with stage C heart failure (structural heart disease and symptoms of heart failure) should be prescribed an ACEi or ARB, a beta-blocker proven to reduce mortality (bisoprolol, carvedilol, and sustained release metoprolol succinate) and either spironolactone or eplerenone. 9 Caution should be exercised when starting a beta-blocker because heart failure patients are at risk of decompensation. 13 A thiazide or loop diuretic may be added for volume control. 1 If a patient can t tolerate an ACEi or ARB, the combination of hydralazine and isosorbide dinitrate may be prescribed. 9 Patients with heart failure symptoms should not receive verapamil or diltiazem because they can cause pulmonary congestion. 1 Initial therapy in diabetic patients depends on the presence of comorbid conditions. Diabetics with cardiovascular disease, kidney disease, albuminuria (albumin-creatinine ratio (ACR) greater than 2mg/mmol) or other cardiovascular risk factors should receive an ACEi or ARB. 14 Diabetics without any cardiovascular risk factors may receive initial therapy with ACEi, ARB, dihydropyridine CCB (amlodipine/nifedipine/felodipine), or thiazide diuretics. 1,14 If blood pressure is not controlled with monotherapy, the combination of ACEi or ARB with a dihydropyridine CCB
7 (amlodipine/nifedipine/felodipine) is preferred over the combination of an ACEi or ARB with a thiazide diuretic. 1,14 The treatment of hypertension during a stroke is divided into the acute period (onset-72hours) and 72 hours after stroke. 1 Treatment of hypertension within 24 hours of onset is not recommended unless the systolic BP is greater than 220mmHg or diastolic BP is greater than 120mmHg. After 24 hours, patients may receive an antihypertensive; however, caution must be exercised to gradually reduce blood pressure to prevent decreased cerebral blood flow and possibly worsen the effects of or induce further ischemia. 1,15 After the acute phase of the stroke, patients should be treated to target a blood pressure of 140/90mmHg. 1,15 The combination of a diuretic and ACEi is preferred over monotherapy with an ACEi or beta-blocker. 1,15 An ACEi and ARB should not be combined in patients with stroke. 1 For patients with chronic kidney disease (CKD) refer to the kidney disease education materials. For treatment of hypertension in CKD, the choice of initial therapy depends on the presence of albuminuria and diabetes. Patients with a urine albumin-creatinine ratio (ACR) greater 30 mg/mmol should receive an ACEi or ARB. 1,16 A thiazide diuretic may be added for additional antihypertensive effect since thiazides have very little diuretic effect when a patient has low kidney function. 1 A loop diuretic may be added to assist in volume control or to control peripheral edema. 1 Combination of a ACEi or ARB with a diuretic, NSAID or COX-2 inhibitor can increase the risk of clinically significant hyperkalemia and acute kidney injury. 16 It is common for serum creatinine to increase approximately 15-25% (GFR decreases by 15-25%) when starting an ACEi or ARB but sudden changes or increases in serum creatinine greater than 25% require stopping the ACEi or ARB and referral to a nephrologist. Many hypertensive CKD patients require using combinations of antihypertensives to reach targets. 1,17 Patients with diabetes and CKD should be treated similar to diabetics without CKD. Diabetic CKD patients should receive initial therapy with an ACEi or ARB if they have urine albumin-creatinine ratio greater than 2 mg/mmol, macrovascular complications (cardiac ischemia (silent or overt), peripheral
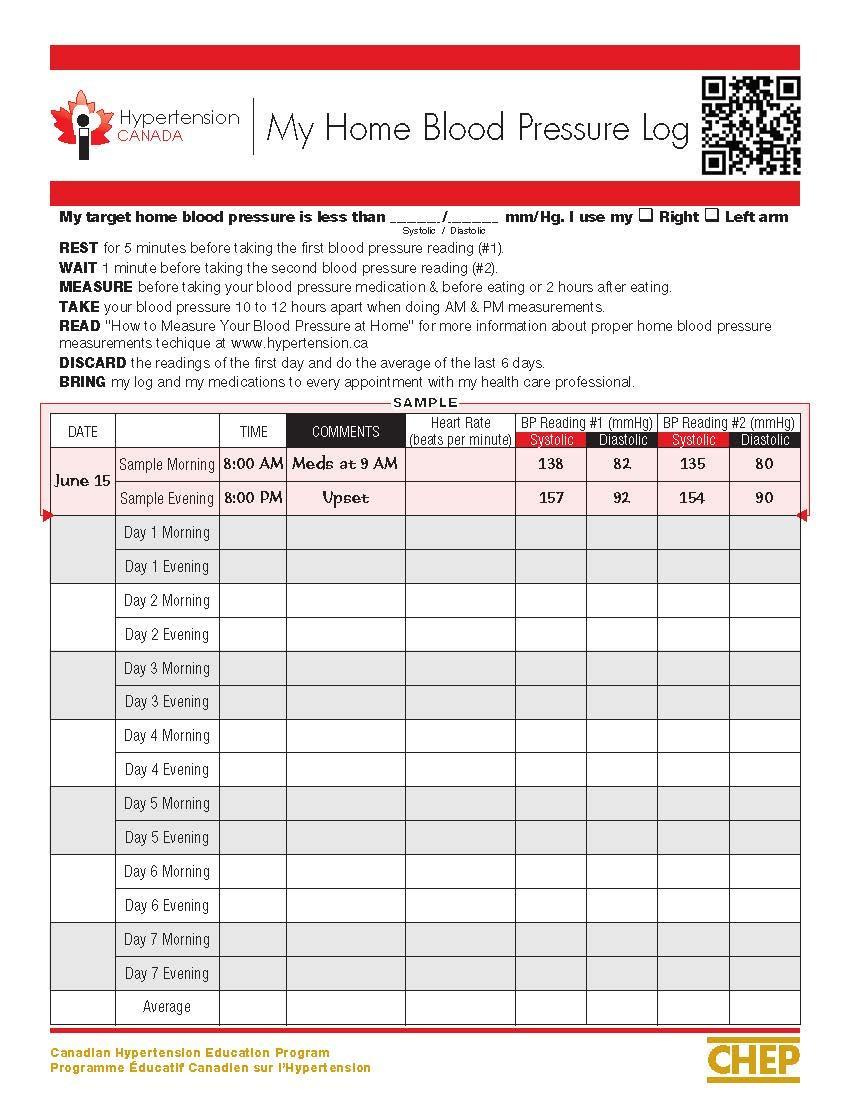
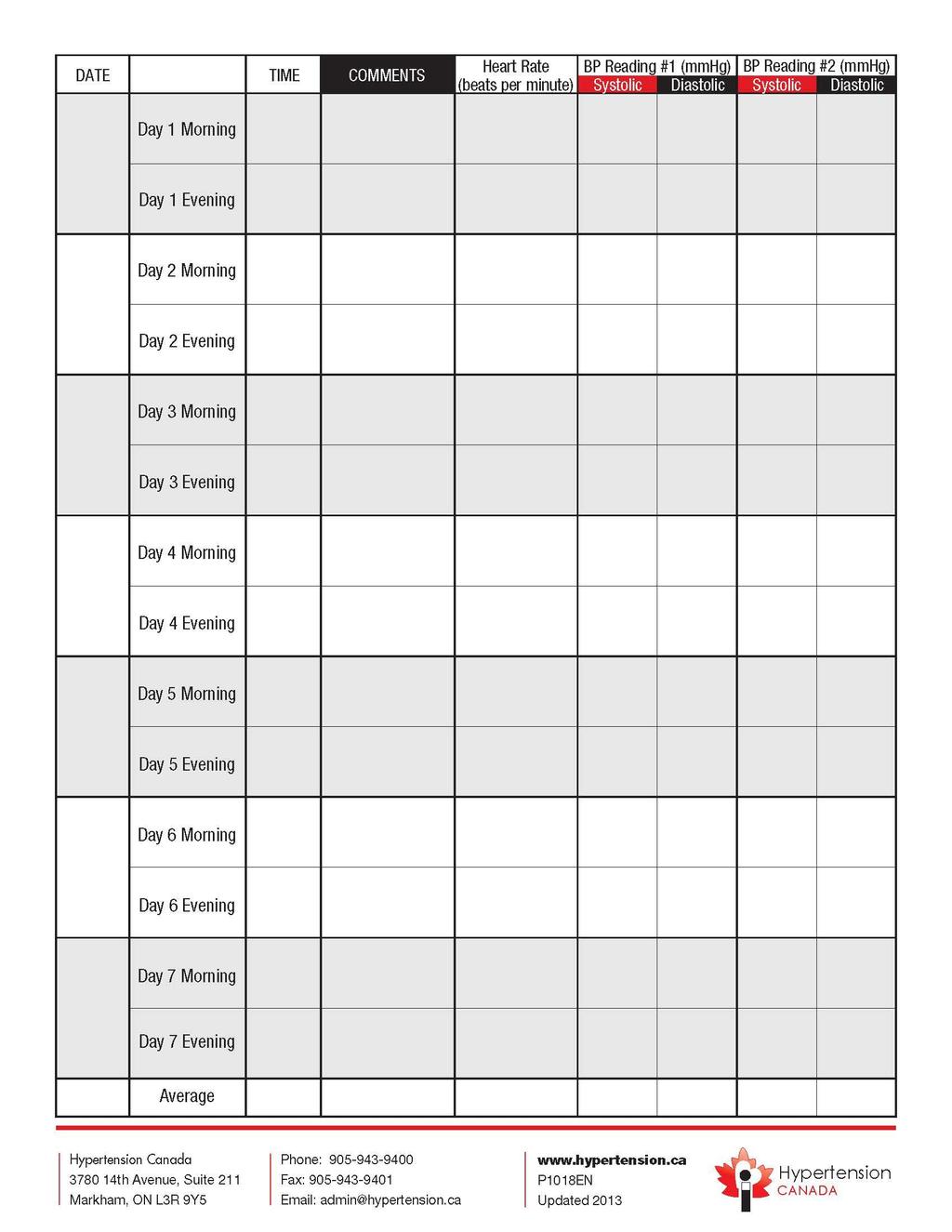
8 vascular disease or cerebrovascular or carotid disease), or microvascular complications (neuropathy, retinopathy). 14 If blood pressure is not controlled with monotherapy, the combination of ACEi or ARB with a dihydropyridine CCB (amlodipine/nifedipine/felodipine) is preferred over the combination of an ACEi or ARB with a thiazide diuretic. 1,14 Addition of a loop diuretic is recommended for patients who have extracellular volume overload demonstrated by peripheral edema. 1 Patients with renovascular disease should be treated in the same manner as patients without specific indications. 1 However, they should be monitored closely when prescribed an ACEi or ARB. Patients with renal artery stenosis with a solitary kidney or bilateral disease are at increased risk of acute kidney injury. 1 These patients are often identified by having very high blood pressure that is not easily controlled even when using up to four antihypertensives. 16 These patients require close monitoring for sudden changes or increases in serum creatinine greater than 15% and should be referred to their general practitioner with consideration for referral to a nephrologist. 16 Renal artery stenosis is managed by renal artery angioplasty or stenting. 1 Supplementation of potassium, calcium and magnesium is not recommended for the prevention or treatment of hypertension, but may be used if the patient has a documented deficiency. Other therapies such as omega 3 fatty acids are generally not recommended. Follow-up/monitoring Patients should perform regular home BP monitoring and keeping a log. A sample home blood pressure monitoring form has been included in Appendix 4. While no exact number of times per week is specified in the guidelines, most patients should monitor several times per week including both morning and evening measurements. More frequent monitoring may be required at times such as during acute illness and adjustment of medications. During every encounter, patients should be asked about symptoms of hypotension such as dizziness, light-headedness and patients should be evaluated for postural hypotension by performing supine and standing blood pressure measurements. 1,16 Patients
9 should be asked about progress with lifestyle modifications including smoking cessation at every encounter. 1 Initial assessment should include the following laboratory tests: urinalysis, blood chemistry (sodium, potassium, creatinine), fasting blood glucose (or HgB A1C in diabetics), fasting cholesterol, and standard 12-lead ECG. 1 The urinalysis detects the presence of protein or albumin or blood and may indicate the patient requires further assessment for kidney or other diseases. A 12-lead ECG is recommended because high blood pressure puts patients at risk of developing myocardial infarction, left ventricular hypertrophy and subsequent heart failure. During the maintenance phase of hypertension management, electrolytes and creatinine should be repeated with a frequency reflecting the clinical situation. 1 Patients starting an ACEi or ARB should have close monitoring of potassium and serum creatinine to monitor for hyperkalemia and changes in renal function. Likewise, patients taking a thiazide diuretic should be monitored for hypokalemia and given a supplement if required, and patients taking potassium sparing diuretics should be monitored for hyperkalemia especially when used in combination with an ACEi or ARB. Fasting blood glucose can detect the abnormalities in glucose that may cause development of diabetes. Hemoglobin A1C is used to monitor effectiveness of antidiabetic treatment. High cholesterol requires treatment with a statin medication to reduce the risk of cardiovascular events. If patients are unable to reach target blood pressures, they should be assessed for possible reasons for poor response. These can range from non-compliance with diet or medications to concomitant medications that cause hypertension to other reasons for secondary hypertension. Patients who are not controlled on three or more medications should be considered for referral to a nephrologist. Possible reasons for poor response 1 Non-compliance: diet or medications NSAIDS, oral contraceptive pills, sex hormones, corticosteroids, anabolic steroids, sympathomimetics and decongestants, cocaine, amphetamines, erythropoietin, cyclosporine, tacrolimus, licorice, midodrine, MAOI, SSRI and SNRI Dosage too low, inappropriate combinations
10 Obesity, smoking, alcohol consumption, sleep apnea, persistent pain, volume overload, excessive salt, renal sodium retention Secondary hypertension: renal insufficiency, renovascular disease, primary hyperaldosteronism, hyperthyroidism, obstructive sleep apnea, other rare endocrine disease Patient education The focus of patient education is adherence, lifestyle modification and monitoring parameters such as postural hypotension or dizziness. Patients should understand the role of each medication and why management of hypertension is important for their overall health. Key points for drug therapy 18 Medication Class Examples Possible adverse effects Thiazide diuretic hydrochlorothiazide, chlorthalidione, indapamide Hypokalemia, photosensitivity, GI upset. Cautions: Avoid in severe hepatic or renal disease. May precipitate gout in clients with history of gout Loop diuretic furosemide Electroltye depletion, muscle cramps. Caution: need potassium rich foods/supplements with long term use. Monitor potassium closely when also on digoxin or potassium depleting steroids. Potassium sparing diuretic ACEi ARB Beta blocker Cardioselective beta blocker spironolactone, amiloride triamterene captopril, cilazapril, enalapril, fosinopril, lisinopril, quinipril, ramipril, perindopril, trandolapril candesartan, eprosartan, irbesartan, losartan, valsartan, telmisartan nadolol, sotalol, timolol acebutolol, atenolol, bisoprolol, metoprolol, propranolol Gynecomastia (breast development in men), fatigue, impotence. Caution: elevated potassium with clients with renal disease, or on NSAIDS, ACEi or ARB Cough, angioedema, leukopenia (low white blood cell count, loss of taste or metallic taste. Caution for all ACEi: Don t use in pregnancy, use with caution in renal insufficiency and may cause hypotension when used with diuretic. May need to discontinue or reduce diuretic 2-3 days prior starting this medication. A rise in serum creatinine after initiating an ACE is common, but acute kidney injury is possible especially in patients with renovascular disease. Fatigue, dizziness, hyperkalemia. Caution: Don t use in pregnancy or in bilateral renal stenosis. A rise in serum creatinine after initiating an ARB is common, but acute kidney injury is possible especially in patients with renal stenosis. May cause hypotension when used with diuretic. May need to discontinue or reduce diuretic 2-3 days prior starting this medication. Advise patient to consult with MD. Bradycardia, masks hypoglycemia, fatigue, aggravate arterial insufficiency, bronchospasms, congestive heart failure. Cautions: Do not increase dose if heart rate is less than 45 beats per minute. Avoid or use with caution in asthmatics and type 1 diabetes; avoid in those with a heart block (Although beta blockers may rarely precipitate or worsen heart failure, research
11 Alpha-beta blocker Non-dihydropyridine CCB Dihydropyridine CCB Direct vasodilator carvedilol verapamil, diltiazem amlodipine, felodipine, nifedipine hydralazine, minoxidil shows beneficial outcomes with the use of carvedilol, bisoprolol and metoprolol SR in those with heart failure.) Headaches,flushing, ankle swelling, lightheadedness, gingival hyperplasia, constipation. Caution with severe aortic stenosis/severe liver disease; with BB or digoxin may result in conduction disorders; Avoid grapefruit or grapefruit juice which may enhance effect. Increased hair growth, headache, angina in CAD clients, tachycardia, edema. Cautions: Avoid in mitral valve rheumatic fever (may drug induced lupus syndrome) Alpha blocker doxazosin, terazosin Postural hypotension, dizziness, weakness, palpitations, headache. Since relaxes muscles in prostate and bladder may be used to treat pain of prostatis but should not be used in patients with prostate cancer or surgery, neurogenic bladder. Not recommended in severe renal or hepatic failure. Central alpha agonists clonidine (tablet, patch), methyldopa Nasal congestion, drowsiness, dizziness, pruritis with the patch, dry mouth. Cautions: don t use in liver disease current or past; or with MAOI therapy. Clonidine requires a slow withdrawal or rebound hypertension is possible. Methyldopa effectiveness is decreased with iron supplementation Direct renin inhibitor aliskiren Aliskiren is no longer indicated for use in combination with ACE inhibitors or ARBs in Type 2 Diabetes (due to increases in non-fatal strokes, renal issues, hypotension and hyperkalemia).
12 References 1. Hackam D, Quinn R, Ravani P, et al. The 2013 Canadian Hypertension Education Program Recommendations for Blood Pressure Measurement, Diagnosis, Assessment of Risk, Prevention, and Treatment of Hypertension. Canadian Journal of Cardiology 2013; 29(5): accessed at 2. Tobe S, Stone J, Brouwers M, et al. Harmonization of guidelines for the prevention and treatment of cardiovascular disease: the C-CHANGE initiative. Canadian Medical Association Journal 2011; 183(15):E1135-E Clarke PM, Gray AM, Briggs A, et al. A model to estimate the lifetime health outcomes of patients with type 2 diabetes: the United Kingdom Prospective Diabetes Study (UKPDS) Outcomes Model (UKPDS no. 68). Diabetologia 2004; 47(10): Wilson P, D'Agostino R, Bhatt DL, et al. An international model to predict recurrent cardiovascular disease. American Journal of Medicine 2012; 125(7): U.S. Department Of Health And Human Services. Your Guide to Lowering Your Blood Pressure With DASH. NIH Publication Bethesda, Maryland (2006). Accessed July 18, 2013 at 6. Appel L, Moore T, Obarzanek E, et al. A clinical trial of the effects of dietary patterns on blood pressure. New England Journal of Medicine 1997; 336(16): Sacks F, Svetkey L, Vollmer W, Et Al. Effects On Blood Pressure Of Reduced Dietary Sodium And The Dietary Approaches To Stop Hypertension (DASH) Diet. New England Journal of Medicine 2001; 344(1): O'Gara P, Kushner F, Ascheim D, et al ACCF/AHA Guideline for the Management of ST- Elevation Myocardial Infarction. Circulation. 2013; 127(4):e362-e Hunt S, Abraham W, Chin M, et al Focused Update Incorporated Into The ACC/AHA 2005 Guidelines for the Diagnosis and Management of Heart Failure in Adults Circulation 2009; 119(14):e391-e McKelvie R, Moe G, Ezekowitz J, et al. The 2012 Canadian Cardiovascular Society Heart Failure Management Guidelines Update: Focus on Acute and Chronic Heart Failure. Canadian Journal of Cardiology 2013; 29(2): Klingbeil A, Schneider M, Martus P, et al. A meta-analysis of the effects of treatment on left ventricular mass in essential hypertension American Journal of Medicine 2003; 115(1): Sadoshima J, Izumo S. Molecular characterization of angiotensin II--induced hypertrophy of cardiac myocytes and hyperplasia of cardiac fibroblasts. Critical role of the AT1 receptor subtype. Circulation Research 1993; 73(3): Krum H, Roecker EB, Mohacsi P, et al. Effects of initiating carvedilol in patients with severe chronic heart failure: results from the COPERNICUS Study. Journal of the American Medical Association 2003; 289(6): Gilbert R, Rabi D, LaRochelle P, et al. Clinical Practice Guidelines Treatment of Hypertension. Canadian Journal of Diabetes 2013; 37(1):S117-S Furie K, Kasner S, Adams R, et al. Guidelines for the Prevention of Stroke in Patients with Stroke or Transient Ischemic Attack. Stroke 2011; 42(1): Kidney Disease: Improving Global Outcomes (KDIGO) Blood Pressure Work Group. KDIGO Clinical Practice Guideline for the Management of Blood Pressure in Chronic Kidney Disease. Kidney International Supplements 2012; 2(5): Chronic Kidney Disease (CKD) Management in General Practice (2 nd edition). Kidney Health Australia, Melbourne Available at Hypertension Module Endocrinology and Metabolism Program Calgary Zone. fblackboard%2fexecute%2flauncher%3ftype%3dcourse%26id%3d_27719_1%26url%3d Updated May 2013, accessed July 23, 2013

13 Appendix 1 Assessment and Diagnosis of Patients with Hypertension Hackam D, Quinn R, Ravani P, et al. The 2013 Canadian Hypertension Education Program Recommendations for Blood Pressure Measurement, Diagnosis, Assessment of Risk, Prevention, and Treatment of Hypertension. Canadian Journal of Cardiology 2013; 29(5):
14 Appendix 2 Initial therapy Initial therapy but SBP more than 20mmHg or DBP more than 10mmHg above targets Adverse effects from initial therapy Uncontrolled with initial therapy, SBP 1-19mmHg or DBP 1-9mmHg above goal Thiazide, beta-blocker (if less than 60yrs), ACEi (except not in African American), long-acting CCB or ARB Start low, go slow Avoid hypokalemia with thiazide (supplemental potassium chloride if required) Combination therapy with thiazide + ACEi, CCB, ARB or beta-blocker 8 Substitute with another first line agent (thiazide, beta-blocker, ACEi, long-acting CCB or ARB) Address compliance/adherence Combinations include: thiazide or CCB with ACEi, ARB or beta-blocker Caution diltiazem/verapamil with beta-blocker Do not use ACEi + ARB Consider other reasons for poor response Uncontrolled with initial therapy, SBP more than Address compliance/adherence 20mmHg or DBP more than 10mmHg above goal Add two more antihypertensive drugs SBP and DBP below goal Continue current regime Margolis KL, Asche SE, Bergdall AR, et al. Effect of home blood pressure telemonitoring and pharmacist management on blood pressure control: a cluster randomized clinical trial. JAMA 2013; 310(1):46-56, online supplementary etable 1
15 Appendix 3 Individualization of therapy by comorbid conditions: Coronary artery disease ACEi/ARB, beta-blocker, ACEi + (amlodipine, nifedipine, felodipine) Recent MI ACEi + beta-blocker (or ARB + betablocker) Heart failure ACEi/ARB + beta-blocker + spironolactone and add thiazide or loop diuretic for volume control if can t tolerate ACEi or ARB, use hydralazine and isosorbide dinitrate Diabetes ACEi/ARB; amlodipine/nifedipine/felodipine, thiazide diuretic; combination ACEi/ARB + nondihydropyridine CCB Stroke 24 hours after stroke ACEi + diuretic Left ventricle ACEi/ARB, long-acting CCB, thiazide hypertrophy diuretic Non-diabetic chronic ACEi/ARB if proteinuria; kidney disease add thiazide for antihypertensive effect ; add loop diuretic for volume control Renal artery stenosis if beta-blocker not tolerated or contraindicated use CCB do not use verapamil or diltiazem ACEi/ARB especially if microvascular complications or macrovascular disease Suggest not using ACEi/ARB + thiazide do not use hydralazine or minoxidil Thiazides have very little diuretic effect caution with ACEi/ARB in solitary kidney or bilateral disease due to risk of acute kidney injury Adapted from: Hackam D, Quinn R, Ravani P, et al. The 2013 Canadian Hypertension Education Program Recommendations for Blood Pressure Measurement, Diagnosis, Assessment of Risk, Prevention, and Treatment of Hypertension. Canadian Journal of Cardiology 2013; 29(5):
16 Appendix 4 Home blood pressure monitoring form for patients
17
18
Hypertension Management - Summary
 Who should have blood pressure assessed? Hypertension Management - Summary All patients over the age of 40 years, every 1-3 years in order to determine their cardiovascular risk (ie. Framingham Risk Score)
Who should have blood pressure assessed? Hypertension Management - Summary All patients over the age of 40 years, every 1-3 years in order to determine their cardiovascular risk (ie. Framingham Risk Score)
Hypertension (JNC-8)
") Hypertension (JNC-8) Southern California University of Health Sciences Physician Assistant Program Management and Treatment of Hypertension April 17, 2018, presented by Ezra Levy, Pharm.D.! The 8 th Joint
Hypertension (JNC-8) Southern California University of Health Sciences Physician Assistant Program Management and Treatment of Hypertension April 17, 2018, presented by Ezra Levy, Pharm.D.! The 8 th Joint
Management of Hypertension
 Clinical Practice Guidelines Management of Hypertension Definition and classification of blood pressure levels (mmhg) Category Systolic Diastolic Normal
Clinical Practice Guidelines Management of Hypertension Definition and classification of blood pressure levels (mmhg) Category Systolic Diastolic Normal
Hypertension diagnosis (see detail document) Diabetic. Target less than 130/80mmHg
 Diabetic. Target less than 130/80mmHg") Hypertension diagnosis (see detail document) Non-diabetic Diabetic Very elderly (older than 80 years) Target less than 140/90mmHg Target less than 130/80mmHg Consider SBP target less than 150mmHg Non-diabetic
Hypertension diagnosis (see detail document) Non-diabetic Diabetic Very elderly (older than 80 years) Target less than 140/90mmHg Target less than 130/80mmHg Consider SBP target less than 150mmHg Non-diabetic
hypertension Head of prevention and control of CVD disease office Ministry of heath
 hypertension t. Samavat MD,Cadiologist,MPH Head of prevention and control of CVD disease office Ministry of heath RECOMMENDATIONS FOR HYPERTENSION DIAGNOSIS, ASSESSMENT, AND TREATMENT Definition of hypertension
hypertension t. Samavat MD,Cadiologist,MPH Head of prevention and control of CVD disease office Ministry of heath RECOMMENDATIONS FOR HYPERTENSION DIAGNOSIS, ASSESSMENT, AND TREATMENT Definition of hypertension
Younger adults with a family history of premature artherosclerotic disease should have their cardiovascular risk factors measured.
 Appendix 2A - Guidance on Management of Hypertension Measurement of blood pressure All adults from 40 years should have blood pressure measured as part of opportunistic cardiovascular risk assessment.
Appendix 2A - Guidance on Management of Hypertension Measurement of blood pressure All adults from 40 years should have blood pressure measured as part of opportunistic cardiovascular risk assessment.
Heart Failure Clinician Guide JANUARY 2018
 Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Heart Failure Clinician Guide JANUARY 2018 Introduction This evidence-based guideline summary is based on the 2018 National Heart Failure Guideline.
Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Heart Failure Clinician Guide JANUARY 2018 Introduction This evidence-based guideline summary is based on the 2018 National Heart Failure Guideline.
7/7/ CHD/MI LVH and LV dysfunction Dysrrhythmias Stroke PVD Renal insufficiency and failure Retinopathy. Normal <120 Prehypertension
 Prevalence of Hypertension Hypertension: Diagnosis and Management T. Villela, M.D. Program Director University of California, San Francisco-San Francisco General Hospital Family and Community Medicine
Prevalence of Hypertension Hypertension: Diagnosis and Management T. Villela, M.D. Program Director University of California, San Francisco-San Francisco General Hospital Family and Community Medicine
HypertensionTreatment Guidelines. Michaelene Urban APRN, MSN, ACNS-BC, ANP-BC
 HypertensionTreatment Guidelines Michaelene Urban APRN, MSN, ACNS-BC, ANP-BC Objectives: Review the definition of the different stages of HTN. Review the current guidelines for treatment of HTN. Provided
HypertensionTreatment Guidelines Michaelene Urban APRN, MSN, ACNS-BC, ANP-BC Objectives: Review the definition of the different stages of HTN. Review the current guidelines for treatment of HTN. Provided
Heart Failure Clinician Guide JANUARY 2016
 Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Heart Failure Clinician Guide JANUARY 2016 Introduction This evidence-based guideline summary is based on the 2016 National Heart Failure Guideline.
Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Heart Failure Clinician Guide JANUARY 2016 Introduction This evidence-based guideline summary is based on the 2016 National Heart Failure Guideline.
What in the World is Functional Medicine?
 What in the World is Functional Medicine? An Introduction to a Systems Based Approach of Chronic Disease Meneah R Haworth, FNP-C Disclosure v I am a student of the Institute for Functional Medicine. They
What in the World is Functional Medicine? An Introduction to a Systems Based Approach of Chronic Disease Meneah R Haworth, FNP-C Disclosure v I am a student of the Institute for Functional Medicine. They
Chapter 23. Media Directory. Cardiovascular Disease (CVD) Hypertension: Classified into Three Categories
 Hypertension: Classified into Three Categories") Chapter 23 Drugs for Hypertension Slide 37 Slide 41 Media Directory Nifedipine Animation Doxazosin Animation Upper Saddle River, New Jersey 07458 All rights reserved. Cardiovascular Disease (CVD) Includes
Chapter 23 Drugs for Hypertension Slide 37 Slide 41 Media Directory Nifedipine Animation Doxazosin Animation Upper Saddle River, New Jersey 07458 All rights reserved. Cardiovascular Disease (CVD) Includes
Introductory Clinical Pharmacology Chapter 41 Antihypertensive Drugs
 Introductory Clinical Pharmacology Chapter 41 Antihypertensive Drugs Blood Pressure Normal = sys
Introductory Clinical Pharmacology Chapter 41 Antihypertensive Drugs Blood Pressure Normal = sys
Dr Narender Goel MD (Internal Medicine and Nephrology) Financial Disclosure: None, Conflict of Interest: None
 Financial Disclosure: None, Conflict of Interest: None") Dr Narender Goel MD (Internal Medicine and Nephrology) drnarendergoel@gmail.com Financial Disclosure: None, Conflict of Interest: None 12 th December 2013, New York Visit us at: http://kidneyscience.info/
Dr Narender Goel MD (Internal Medicine and Nephrology) drnarendergoel@gmail.com Financial Disclosure: None, Conflict of Interest: None 12 th December 2013, New York Visit us at: http://kidneyscience.info/
Antihypertensive Agents Part-2. Assistant Prof. Dr. Najlaa Saadi PhD Pharmacology Faculty of Pharmacy University of Philadelphia
 Antihypertensive Agents Part-2 Assistant Prof. Dr. Najlaa Saadi PhD Pharmacology Faculty of Pharmacy University of Philadelphia Agents that block production or action of angiotensin Angiotensin-converting
Antihypertensive Agents Part-2 Assistant Prof. Dr. Najlaa Saadi PhD Pharmacology Faculty of Pharmacy University of Philadelphia Agents that block production or action of angiotensin Angiotensin-converting
Antihypertensive drugs SUMMARY Made by: Lama Shatat
 Antihypertensive drugs SUMMARY Made by: Lama Shatat Diuretic Thiazide diuretics The loop diuretics Potassium-sparing Diuretics *Hydrochlorothiazide *Chlorthalidone *Furosemide *Torsemide *Bumetanide Aldosterone
Antihypertensive drugs SUMMARY Made by: Lama Shatat Diuretic Thiazide diuretics The loop diuretics Potassium-sparing Diuretics *Hydrochlorothiazide *Chlorthalidone *Furosemide *Torsemide *Bumetanide Aldosterone
Hypertension Update. Objectives 4/28/2015. Beverly J. Mathis, D.O. OOA May 2015
 Hypertension Update Beverly J. Mathis, D.O. OOA May 2015 Objectives Learn new recommendations for BP treatment goals Approach to hypertension in the office Use of hypertensive drugs, and how to tailor
Hypertension Update Beverly J. Mathis, D.O. OOA May 2015 Objectives Learn new recommendations for BP treatment goals Approach to hypertension in the office Use of hypertensive drugs, and how to tailor
Antihypertensive Agents
 Antihypertensive Agents Southern California University of Health Sciences Physician Assistant Program Management and Treatment of Hypertension April 7, 08, presented by Ezra Levy, Pharm.D! Usual Dose,
Antihypertensive Agents Southern California University of Health Sciences Physician Assistant Program Management and Treatment of Hypertension April 7, 08, presented by Ezra Levy, Pharm.D! Usual Dose,
5.2 Key priorities for implementation
 5.2 Key priorities for implementation From the full set of recommendations, the GDG selected ten key priorities for implementation. The criteria used for selecting these recommendations are listed in detail
5.2 Key priorities for implementation From the full set of recommendations, the GDG selected ten key priorities for implementation. The criteria used for selecting these recommendations are listed in detail
Difficult to Treat Hypertension
 Difficult to Treat Hypertension According to Goldilocks JNC 8 Blood Pressure Goals (2014) BP Goal 60 years old and greater*- systolic < 150 and diastolic < 90. (Grade A)** BP Goal 18-59 years old* diastolic
Difficult to Treat Hypertension According to Goldilocks JNC 8 Blood Pressure Goals (2014) BP Goal 60 years old and greater*- systolic < 150 and diastolic < 90. (Grade A)** BP Goal 18-59 years old* diastolic
8/20/2018. Objectives. What is hypertension? cont. What is hypertension? Epidemiology cont. Epidemiology
 Objectives Hypertension (high blood pressure): Clinical Pearls for the Pharmacy Technician Tanya Schmidt PharmD, RPh Director of Central Operations at Thrifty White Pharmacy North Dakota Board of Pharmacy
Objectives Hypertension (high blood pressure): Clinical Pearls for the Pharmacy Technician Tanya Schmidt PharmD, RPh Director of Central Operations at Thrifty White Pharmacy North Dakota Board of Pharmacy
Section 3, Lecture 2
 59-291 Section 3, Lecture 2 Diuretics: -increase in Na + excretion (naturesis) Thiazide and Related diuretics -decreased PVR due to decreases muscle contraction -an economical and effective treatment -protect
59-291 Section 3, Lecture 2 Diuretics: -increase in Na + excretion (naturesis) Thiazide and Related diuretics -decreased PVR due to decreases muscle contraction -an economical and effective treatment -protect
Hypertension Update. Sarah J. Payne, MS, PharmD, BCPS Assistant Professor, Department of Pharmacotherapy UNT System College of Pharmacy
 Hypertension Update Sarah J. Payne, MS, PharmD, BCPS Assistant Professor, Department of Pharmacotherapy UNT System College of Pharmacy Introduction 1/3 of US adults have HTN More prevalent in non-hispanic
Hypertension Update Sarah J. Payne, MS, PharmD, BCPS Assistant Professor, Department of Pharmacotherapy UNT System College of Pharmacy Introduction 1/3 of US adults have HTN More prevalent in non-hispanic
Antihypertensives. Antihypertensive Classes. RAAS Inhibitors. Renin-Angiotensin Cascade. Angiotensin Receptors. Approaches to Hypertension Treatment
 Approaches to Hypertension Treatment Antihypertensives Inhibit Sympathetic impulses Inhibit contractility Inhibit heart rate Inhibit vasoconstriction Inhibit smooth muscle function Inhibit RAAS Inhibit
Approaches to Hypertension Treatment Antihypertensives Inhibit Sympathetic impulses Inhibit contractility Inhibit heart rate Inhibit vasoconstriction Inhibit smooth muscle function Inhibit RAAS Inhibit
VA/DoD Clinical Practice Guideline for the Diagnosis and Management of Hypertension - Pocket Guide Update 2004 Revision July 2005
 VA/DoD Clinical Practice Guideline for the Diagnosis and Management of Hypertension - Pocket Guide Update 2004 Revision July 2005 1 Any adult in the health care system 2 Obtain blood pressure (BP) (Reliable,
VA/DoD Clinical Practice Guideline for the Diagnosis and Management of Hypertension - Pocket Guide Update 2004 Revision July 2005 1 Any adult in the health care system 2 Obtain blood pressure (BP) (Reliable,
Heart Failure (HF) Treatment
 Treatment") Heart Failure (HF) Treatment Heart Failure (HF) Complex, progressive disorder. The heart is unable to pump sufficient blood to meet the needs of the body. Its cardinal symptoms are dyspnea, fatigue, and
Heart Failure (HF) Treatment Heart Failure (HF) Complex, progressive disorder. The heart is unable to pump sufficient blood to meet the needs of the body. Its cardinal symptoms are dyspnea, fatigue, and
Difficult-to-Control & Resistant Hypertension. Anthony Viera, MD, MPH, FAHA Professor and Chair
 Difficult-to-Control & Resistant Hypertension Anthony Viera, MD, MPH, FAHA Professor and Chair Objectives Define resistant hypertension Discuss evaluation strategy for patient with HTN that appears difficult
Difficult-to-Control & Resistant Hypertension Anthony Viera, MD, MPH, FAHA Professor and Chair Objectives Define resistant hypertension Discuss evaluation strategy for patient with HTN that appears difficult
HTN talk_l Davis_ /28/2018
 1 2 GUIDELINES PUBLISHED AHEAD OF PRINT NOV 13, 2017 = SAME DAY AS PUBLIC PRESENTATION LESLIE L DAVIS, PHD, RN, ANP-BC, FPCNA, FAANP, FAHA The New Guidelines Have Been Published! Whelton PK, Carey RM,
1 2 GUIDELINES PUBLISHED AHEAD OF PRINT NOV 13, 2017 = SAME DAY AS PUBLIC PRESENTATION LESLIE L DAVIS, PHD, RN, ANP-BC, FPCNA, FAANP, FAHA The New Guidelines Have Been Published! Whelton PK, Carey RM,
Hypertension CHAPTER-I CARDIOVASCULAR SYSTEM. Dr. K T NAIK Pharm.D Associate Professor Department of Pharm.D Krishna Teja Pharmacy College, Tirupati
 CHAPTER-I CARDIOVASCULAR SYSTEM Hypertension SUB: PHARMACOTHERAPEUTICS-I CODE:T0820006 Dr. K T NAIK Pharm.D Associate Professor Department of Pharm.D Krishna Teja Pharmacy College, Tirupati Hypertension
CHAPTER-I CARDIOVASCULAR SYSTEM Hypertension SUB: PHARMACOTHERAPEUTICS-I CODE:T0820006 Dr. K T NAIK Pharm.D Associate Professor Department of Pharm.D Krishna Teja Pharmacy College, Tirupati Hypertension
Categories of HTN. Overview of Hypertension. Types of Hypertension
 Categories of HTN Overview of Hypertension Normal SBP 100 Quick review of the Basics: What is
Categories of HTN Overview of Hypertension Normal SBP 100 Quick review of the Basics: What is
Antihypertensives. Diagnostic category
 Measurement of blood pressure At first assessment, take both arms then choose the one with the higher reading. Beware of orthostatic hypotension. Measure BP in sitting position, and repeat after patient
Measurement of blood pressure At first assessment, take both arms then choose the one with the higher reading. Beware of orthostatic hypotension. Measure BP in sitting position, and repeat after patient
Preventing and Treating High Blood Pressure
 Preventing and Treating High Blood Pressure: Finding the Right Balance of Integrative and Pharmacologic Approaches Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Blood Pressure
Preventing and Treating High Blood Pressure: Finding the Right Balance of Integrative and Pharmacologic Approaches Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Blood Pressure
Guideline-Directed Medical Therapy
 Guideline-Directed Medical Therapy Cardiovascular Outcomes Assessment of the MitraClip Percutaneous Therapy for Heart Failure Patients with Functional Mitral Regurgitation OPTIMAL THERAPY (As defined in
Guideline-Directed Medical Therapy Cardiovascular Outcomes Assessment of the MitraClip Percutaneous Therapy for Heart Failure Patients with Functional Mitral Regurgitation OPTIMAL THERAPY (As defined in
Antihypertensive drugs: I. Thiazide and other diuretics:
 Clinical assessment of hypertensive patient: You have to take history regarding the presence of other risk factors for CAb like diabetes mellitus, smoking, etc. Take history whether the patient takes medications
Clinical assessment of hypertensive patient: You have to take history regarding the presence of other risk factors for CAb like diabetes mellitus, smoking, etc. Take history whether the patient takes medications
Adult Blood Pressure Clinician Guide June 2018
 Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Adult Blood Pressure Clinician Guide June 2018 Adult Blood Pressure Clinician Guide June 2018 Introduction This Clinician Guide is based on the 2018
Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Adult Blood Pressure Clinician Guide June 2018 Adult Blood Pressure Clinician Guide June 2018 Introduction This Clinician Guide is based on the 2018
MODERN MANAGEMENT OF HYPERTENSION Where Do We Draw the Line? Disclosure. No relevant financial relationships. Blood Pressure and Risk
 MODERN MANAGEMENT OF HYPERTENSION Where Do We Draw the Line? Disclosure No relevant financial relationships Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine baron@medicine.ucsf.edu
MODERN MANAGEMENT OF HYPERTENSION Where Do We Draw the Line? Disclosure No relevant financial relationships Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine baron@medicine.ucsf.edu
COMPLEX HYPERTENSION. Anita Ralstin, FNP-BC Next Step Health Consultant, LLC
 COMPLEX HYPERTENSION Anita Ralstin, FNP-BC Next Step Health Consultant, LLC Incidence Of Hypertension About 70 million American adults have high blood pressure. About 33% of the population Only 52% have
COMPLEX HYPERTENSION Anita Ralstin, FNP-BC Next Step Health Consultant, LLC Incidence Of Hypertension About 70 million American adults have high blood pressure. About 33% of the population Only 52% have
Management of Hypertension. Ahmed El Hawary MD Suez Canal University
 Management of Hypertension Ahmed El Hawary MD Suez Canal University Minimal vs. Optimal Care Resources more than science affect type of care and level of management. what is possible (minimal care) and
Management of Hypertension Ahmed El Hawary MD Suez Canal University Minimal vs. Optimal Care Resources more than science affect type of care and level of management. what is possible (minimal care) and
RESISTENT HYPERTENSION. Dr. Helmy Bakr Professor and Head of Cardiology Dept. Mansoura University
 RESISTENT HYPERTENSION Dr. Helmy Bakr Professor and Head of Cardiology Dept. Mansoura University Resistant Hypertension Blood pressure remaining above goal in spite of concurrent use of 3 antihypertensive
RESISTENT HYPERTENSION Dr. Helmy Bakr Professor and Head of Cardiology Dept. Mansoura University Resistant Hypertension Blood pressure remaining above goal in spite of concurrent use of 3 antihypertensive
Combining Antihypertensives in People with Diabetes
 Combining ntihypertensives in People with Diabetes The majority of people with diabetes will develop hypertension and this subsequently increases the risk of microvascular and macrovascular complications.
Combining ntihypertensives in People with Diabetes The majority of people with diabetes will develop hypertension and this subsequently increases the risk of microvascular and macrovascular complications.
ANTI- HYPERTENSIVE AGENTS
 CLINICAL ANTI- HYPERTENSIVE AGENTS Jacqueline van Schoor, MPharm, BSc (Hons) Amayeza Info Centre Hypertension represents a major public health concern. It affects about a billion people worldwide and is
CLINICAL ANTI- HYPERTENSIVE AGENTS Jacqueline van Schoor, MPharm, BSc (Hons) Amayeza Info Centre Hypertension represents a major public health concern. It affects about a billion people worldwide and is
Byvalson. (nebivolol, valsartan) New Product Slideshow
 New Product Slideshow") Byvalson (nebivolol, valsartan) New Product Slideshow Introduction Brand name: Byvalson Generic name: Nebivolol, valsartan Pharmacological class: Beta-blocker + angiotensin II receptor blocker (ARB) Strength
Byvalson (nebivolol, valsartan) New Product Slideshow Introduction Brand name: Byvalson Generic name: Nebivolol, valsartan Pharmacological class: Beta-blocker + angiotensin II receptor blocker (ARB) Strength
1/4/18. Heart Failure Guideline Review and Update. Disclosure. Pharmacist Objectives. Pharmacy Technician Objectives. What is Heart Failure?
 Disclosure Heart Failure Guideline Review and Update I have had no financial relationship over the past 12 months with any commercial sponsor with a vested interest in this presentation. Natalie Beiter,
Disclosure Heart Failure Guideline Review and Update I have had no financial relationship over the past 12 months with any commercial sponsor with a vested interest in this presentation. Natalie Beiter,
Hypertension: JNC-7. Southern California University of Health Sciences Physician Assistant Program
 Hypertension: JNC-7 Southern California University of Health Sciences Physician Assistant Program Management and Treatment of Hypertension April 17, 2018, presented by Ezra Levy, Pharm.D.! Reference Card
Hypertension: JNC-7 Southern California University of Health Sciences Physician Assistant Program Management and Treatment of Hypertension April 17, 2018, presented by Ezra Levy, Pharm.D.! Reference Card
Hypertension and the 2017 Guidelines Meeting the Targets in Small Groups. Lisa Ivy APRN
 Hypertension and the 2017 Guidelines Meeting the Targets in Small Groups Lisa Ivy APRN The 2017 Guideline is an Update to JNC7 New information regarding BP related risk of CVD Ambulatory BP monitoring
Hypertension and the 2017 Guidelines Meeting the Targets in Small Groups Lisa Ivy APRN The 2017 Guideline is an Update to JNC7 New information regarding BP related risk of CVD Ambulatory BP monitoring
Hypertension Update Warwick Jaffe Interventional Cardiologist Ascot Hospital
 Hypertension Update 2008 Warwick Jaffe Interventional Cardiologist Ascot Hospital Definition of Hypertension Continuous variable At some point the risk becomes high enough to justify treatment Treatment
Hypertension Update 2008 Warwick Jaffe Interventional Cardiologist Ascot Hospital Definition of Hypertension Continuous variable At some point the risk becomes high enough to justify treatment Treatment
Managing Hypertension in 2016
 Managing Hypertension in 2016: Where Do We Draw the Line? Disclosure No relevant financial relationships Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine baron@medicine.ucsf.edu
Managing Hypertension in 2016: Where Do We Draw the Line? Disclosure No relevant financial relationships Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine baron@medicine.ucsf.edu
Hypertension. Risk of cardiovascular disease beginning at 115/75 mmhg doubles with every 20/10mm Hg increase. (Grade B)
") Practice Guidelines and Principles: Guidelines and principles are intended to be flexible. They serve as reference points or recommendations, not rigid criteria. Guidelines and principles should be followed
Practice Guidelines and Principles: Guidelines and principles are intended to be flexible. They serve as reference points or recommendations, not rigid criteria. Guidelines and principles should be followed
CONCORD INTERNAL MEDICINE HYPERTENSION PROTOCOL
 CONCORD INTERNAL MEDICINE HYPERTENSION PROTOCOL Douglas G. Kelling Jr., MD Carmella Gismondi-Eagan, MD, FACP George C. Monroe, III, MD Revised, April 8, 2012 The information contained in this protocol
CONCORD INTERNAL MEDICINE HYPERTENSION PROTOCOL Douglas G. Kelling Jr., MD Carmella Gismondi-Eagan, MD, FACP George C. Monroe, III, MD Revised, April 8, 2012 The information contained in this protocol
STANDARD treatment algorithm mmHg
 STANDARD treatment algorithm 130-140mmHg (i) At BASELINE, If AVERAGE SBP 1 > 140mmHg If on no antihypertensive drugs: Start 1 drug: If >55 years old / Afro-Caribbean: Calcium channel blocker (CCB) 2 If
STANDARD treatment algorithm 130-140mmHg (i) At BASELINE, If AVERAGE SBP 1 > 140mmHg If on no antihypertensive drugs: Start 1 drug: If >55 years old / Afro-Caribbean: Calcium channel blocker (CCB) 2 If
What s New? Hypertension Canada Guidelines for the Management of Hypertension
 What s New? 2017 Hypertension Canada Guidelines for the Management of Hypertension What s New? About This Booklet This booklet highlights key advancements and important, enduring aspects of the Hypertension
What s New? 2017 Hypertension Canada Guidelines for the Management of Hypertension What s New? About This Booklet This booklet highlights key advancements and important, enduring aspects of the Hypertension
Coronary Artery Disease (CAD) Clinician Guide SEPTEMBER 2017
 Clinician Guide SEPTEMBER 2017") Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Coronary Artery Disease (CAD) Clinician Guide SEPTEMBER 2017 Introduction This Clinician Guide is based on the 2017 KP National Coronary Artery Disease
Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Coronary Artery Disease (CAD) Clinician Guide SEPTEMBER 2017 Introduction This Clinician Guide is based on the 2017 KP National Coronary Artery Disease
Guide to the New Hypertension Guidelines
 Guide to the New Hypertension Guidelines LCDR J. Garrett Sims, PharmD, BCPS Advanced Practice Pharmacist Crow/Northern Cheyenne Hospital Hypertension St Disclosures None Objectives Describe the new hypertension
Guide to the New Hypertension Guidelines LCDR J. Garrett Sims, PharmD, BCPS Advanced Practice Pharmacist Crow/Northern Cheyenne Hospital Hypertension St Disclosures None Objectives Describe the new hypertension
2020 HYPERTENSION HIGHLIGHTS
 2020 HYPERTENSION HIGHLIGHTS A Practical Guide informed by the Hypertension Canada Guidelines for the Diagnosis, Risk Assessment, Prevention, and Treatment of Hypertension BLOOD PRESSURE MEASUREMENT TECHNIQUE
2020 HYPERTENSION HIGHLIGHTS A Practical Guide informed by the Hypertension Canada Guidelines for the Diagnosis, Risk Assessment, Prevention, and Treatment of Hypertension BLOOD PRESSURE MEASUREMENT TECHNIQUE
Volume 6; Number 1 January 2012 NICE CLINICAL GUIDELINE 127: HYPERTENSION CLINICAL MANAGEMENT OF PRIMARY HYPERTENSION IN ADULTS (AUGUST 2011)
") Volume 6; Number 1 January 2012 NICE CLINICAL GUIDELINE 127: HYPERTENSION CLINICAL MANAGEMENT OF PRIMARY HYPERTENSION IN ADULTS (AUGUST 2011) What s new in hypertension? NICE has issued an updated Clinical
Volume 6; Number 1 January 2012 NICE CLINICAL GUIDELINE 127: HYPERTENSION CLINICAL MANAGEMENT OF PRIMARY HYPERTENSION IN ADULTS (AUGUST 2011) What s new in hypertension? NICE has issued an updated Clinical
HYPERTENSION IN CKD. LEENA ONGAJYOOTH, M.D., Dr.med RENAL UNIT SIRIRAJ HOSPITAL
 HYPERTENSION IN CKD LEENA ONGAJYOOTH, M.D., Dr.med RENAL UNIT SIRIRAJ HOSPITAL Stages in Progression of Chronic Kidney Disease and Therapeutic Strategies Complications Normal Increased risk Damage GFR
HYPERTENSION IN CKD LEENA ONGAJYOOTH, M.D., Dr.med RENAL UNIT SIRIRAJ HOSPITAL Stages in Progression of Chronic Kidney Disease and Therapeutic Strategies Complications Normal Increased risk Damage GFR
Disclosures. Learning Objectives. Hypertension: a sprint to the finish Ontario Pharmacists Association 1
 Disclosures I have no current or past relationships with commercial entities I have received a speaker s fee from the Ontario Pharmacists Association for this learning activity Laura Tsang PharmD Sunnybrook
Disclosures I have no current or past relationships with commercial entities I have received a speaker s fee from the Ontario Pharmacists Association for this learning activity Laura Tsang PharmD Sunnybrook
ADVANCES IN MANAGEMENT OF HYPERTENSION
 Prevalence 29%; Blacks 33.5% About 72.5% treated; 53.5% uncontrolled (>140/90) Risk for poor control: Latinos, Blacks, age 18-44 and 80,
Prevalence 29%; Blacks 33.5% About 72.5% treated; 53.5% uncontrolled (>140/90) Risk for poor control: Latinos, Blacks, age 18-44 and 80,
 Hypertension Epidemiology 6% of deaths worldwide Defined as any of the following: systolic blood pressure 140 mmhg, diastolic blood pressure 90 mmhg, taking antihypertensive medications Pulse pressure=
Hypertension Epidemiology 6% of deaths worldwide Defined as any of the following: systolic blood pressure 140 mmhg, diastolic blood pressure 90 mmhg, taking antihypertensive medications Pulse pressure=
Network Hypertension Algorithm
 Network Hypertension Algorithm Content Review and Approval: This document is subject to review, revision, and (re)approval by the Clinical Integration and Oversight Committee (CIOC) annually and following
Network Hypertension Algorithm Content Review and Approval: This document is subject to review, revision, and (re)approval by the Clinical Integration and Oversight Committee (CIOC) annually and following
ADVANCES IN MANAGEMENT OF HYPERTENSION
 Advances in Management of Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Current Status of Prevalence 29%; Blacks 33.5%
Advances in Management of Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Current Status of Prevalence 29%; Blacks 33.5%
Modern Management of Hypertension
 Modern Management of Hypertension Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Current Status of Hypertension Prevalence
Modern Management of Hypertension Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Current Status of Hypertension Prevalence
Guide to the New Hypertension Guidelines. LCDR J. Garrett Sims, PharmD, BCPS Crow/Northern Cheyenne Hospital
 Guide to the New Hypertension Guidelines LCDR J. Garrett Sims, PharmD, BCPS Crow/Northern Cheyenne Hospital Disclosures None Objectives Describe the new hypertension staging and blood pressure goals and
Guide to the New Hypertension Guidelines LCDR J. Garrett Sims, PharmD, BCPS Crow/Northern Cheyenne Hospital Disclosures None Objectives Describe the new hypertension staging and blood pressure goals and
Management of Hypertension. M Misra MD MRCP (UK) Division of Nephrology University of Missouri School of Medicine
 Division of Nephrology University of Missouri School of Medicine") Management of Hypertension M Misra MD MRCP (UK) Division of Nephrology University of Missouri School of Medicine Disturbing Trends in Hypertension HTN awareness, treatment and control rates are decreasing
Management of Hypertension M Misra MD MRCP (UK) Division of Nephrology University of Missouri School of Medicine Disturbing Trends in Hypertension HTN awareness, treatment and control rates are decreasing
Cardiovascular Clinical Practice Guideline Pilot Implementation
 Cardiovascular Clinical Practice Guideline Pilot Implementation Pharmacologic Management of Chronic Heart Failure Sept 15, 2004 Angela Allerman, PharmD, BCPS DoD Pharmacoeconomic Center Promoting high
Cardiovascular Clinical Practice Guideline Pilot Implementation Pharmacologic Management of Chronic Heart Failure Sept 15, 2004 Angela Allerman, PharmD, BCPS DoD Pharmacoeconomic Center Promoting high
Modern Management of Hypertension: Where Do We Draw the Line?
 Modern Management of Hypertension: Where Do We Draw the Line? Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Blood Pressure
Modern Management of Hypertension: Where Do We Draw the Line? Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Blood Pressure
Egyptian Hypertension Guidelines
 Egyptian Hypertension Guidelines 2014 Egyptian Hypertension Guidelines Dalia R. ElRemissy, MD Lecturer of Cardiovascular Medicine Cairo University Why Egyptian Guidelines? Guidelines developed for rich
Egyptian Hypertension Guidelines 2014 Egyptian Hypertension Guidelines Dalia R. ElRemissy, MD Lecturer of Cardiovascular Medicine Cairo University Why Egyptian Guidelines? Guidelines developed for rich
The Failing Heart in Primary Care
 The Failing Heart in Primary Care Hamid Ikram How fares the Heart Failure Epidemic? 4357 patients, 57% women, mean age 74 years HFSA 2010 Practice Guideline (3.1) Heart Failure Prevention A careful and
The Failing Heart in Primary Care Hamid Ikram How fares the Heart Failure Epidemic? 4357 patients, 57% women, mean age 74 years HFSA 2010 Practice Guideline (3.1) Heart Failure Prevention A careful and
Combination Therapy for Hypertension
 Combination Therapy for Hypertension Se-Joong Rim, MD Cardiology Division, Yonsei University College of Medicine, Seoul, Korea Goals of Therapy Reduce CVD and renal morbidity and mortality. Treat to BP
Combination Therapy for Hypertension Se-Joong Rim, MD Cardiology Division, Yonsei University College of Medicine, Seoul, Korea Goals of Therapy Reduce CVD and renal morbidity and mortality. Treat to BP
ARNI (Angiotensin Receptor blocker / Neprilysin Inhibitors [Sacubutril/Valsartan]) Heart Failure Medication Initiation and Titration
![ARNI (Angiotensin Receptor blocker / Neprilysin Inhibitors [Sacubutril/Valsartan]) Heart Failure Medication Initiation and Titration](/thumbs/77/76069192.jpg "ARNI (Angiotensin Receptor blocker / Neprilysin Inhibitors [Sacubutril/Valsartan]) Heart Failure Medication Initiation and Titration") ARNI (Angiotensin Receptor blocker / Neprilysin Inhibitors [Sacubutril/Valsartan]) Heart Failure Medication and Symptomatic HF despite ACEI/ARB and B-blocker therapy Bilateral renal artery stenosis Moderate/Severe
ARNI (Angiotensin Receptor blocker / Neprilysin Inhibitors [Sacubutril/Valsartan]) Heart Failure Medication and Symptomatic HF despite ACEI/ARB and B-blocker therapy Bilateral renal artery stenosis Moderate/Severe
What s In the New Hypertension Guidelines?
 American College of Physicians Ohio/Air Force Chapters 2018 Scientific Meeting Columbus, OH October 5, 2018 What s In the New Hypertension Guidelines? Max C. Reif, MD, FACP Objectives: At the end of the
American College of Physicians Ohio/Air Force Chapters 2018 Scientific Meeting Columbus, OH October 5, 2018 What s In the New Hypertension Guidelines? Max C. Reif, MD, FACP Objectives: At the end of the
By Prof. Khaled El-Rabat
 What is The Optimum? By Prof. Khaled El-Rabat Professor of Cardiology - Benha Faculty of Medicine HT. Introduction Despite major worldwide efforts over recent decades directed at diagnosing and treating
What is The Optimum? By Prof. Khaled El-Rabat Professor of Cardiology - Benha Faculty of Medicine HT. Introduction Despite major worldwide efforts over recent decades directed at diagnosing and treating
Hypertension: Update
 Hypertension: Update Meenakshi A Bhalla MD,FACC Associate Professor of Medicine Director Preventive Cardiology Advanced Heart Failure and Transplant Cardiology University of Kentucky Faculty Disclosure
Hypertension: Update Meenakshi A Bhalla MD,FACC Associate Professor of Medicine Director Preventive Cardiology Advanced Heart Failure and Transplant Cardiology University of Kentucky Faculty Disclosure
HYPERTENSION: Sustained elevation of arterial blood pressure above normal o Systolic 140 mm Hg and/or o Diastolic 90 mm Hg
 Lecture 39 Anti-Hypertensives B-Rod BLOOD PRESSURE: Systolic / Diastolic NORMAL: 120/80 Systolic = measure of pressure as heart is beating Diastolic = measure of pressure while heart is at rest between
Lecture 39 Anti-Hypertensives B-Rod BLOOD PRESSURE: Systolic / Diastolic NORMAL: 120/80 Systolic = measure of pressure as heart is beating Diastolic = measure of pressure while heart is at rest between
Dr Diana R Holdright. MD, FRCP, FESC, FACC, MBBS, DA, BSc. Consultant Cardiologist HYPERTENSION.
 Dr Diana R Holdright MD, FRCP, FESC, FACC, MBBS, DA, BSc. Consultant Cardiologist HYPERTENSION www.drholdright.co.uk Blood pressure is the pressure exerted on the walls of the arteries when the heart pumps;
Dr Diana R Holdright MD, FRCP, FESC, FACC, MBBS, DA, BSc. Consultant Cardiologist HYPERTENSION www.drholdright.co.uk Blood pressure is the pressure exerted on the walls of the arteries when the heart pumps;
Management of High Blood Pressure in Adults
 Management of High Blood Pressure in Adults Based on the Report from the Panel Members Appointed to the Eighth Joint National Committee (JNC8) James, P. A. (2014, February 05). 2014 Guideline for Management
Management of High Blood Pressure in Adults Based on the Report from the Panel Members Appointed to the Eighth Joint National Committee (JNC8) James, P. A. (2014, February 05). 2014 Guideline for Management
Hypertension Update Clinical Controversies Regarding Age and Race
 Hypertension Update Clinical Controversies Regarding Age and Race Allison Helmer, PharmD, BCACP Assistant Clinical Professor Auburn University Harrison School of Pharmacy July 22, 2017 DISCLOSURE/CONFLICT
Hypertension Update Clinical Controversies Regarding Age and Race Allison Helmer, PharmD, BCACP Assistant Clinical Professor Auburn University Harrison School of Pharmacy July 22, 2017 DISCLOSURE/CONFLICT
Top 200 Section 4. Cardiovascular Drugs
 Top 200 Section 4 Cardiovascular Drugs Objectives After finishing this presentation the audience should be able to: Describe conditions/disease states that would make a person a candidate for drug therapy.
Top 200 Section 4 Cardiovascular Drugs Objectives After finishing this presentation the audience should be able to: Describe conditions/disease states that would make a person a candidate for drug therapy.
Summary/Key Points Introduction
 Summary/Key Points Introduction Scope of Heart Failure (HF) o 6.5 million Americans 20 years of age have HF o 960,000 new cases of HF diagnosed annually o 5-year survival rate for HF is ~50% Classification
Summary/Key Points Introduction Scope of Heart Failure (HF) o 6.5 million Americans 20 years of age have HF o 960,000 new cases of HF diagnosed annually o 5-year survival rate for HF is ~50% Classification
Beta 1 Beta blockers A - Propranolol,
 Pharma Lecture 3 Beta blockers that we are most interested in are the ones that target Beta 1 receptors. Beta blockers A - Propranolol, it s a non-selective competitive antagonist of beta 1 and beta 2
Pharma Lecture 3 Beta blockers that we are most interested in are the ones that target Beta 1 receptors. Beta blockers A - Propranolol, it s a non-selective competitive antagonist of beta 1 and beta 2
Treating Hypertension in Individuals with Diabetes
 Treating Hypertension in Individuals with Diabetes Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any
Treating Hypertension in Individuals with Diabetes Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any
ASEBP and ARTA TARP Drugs and Reference Price by Categories
 ASEBP Pantoprazole Sodium 40 mg (generic) $0.2016 ASEBP Dexlansoprazole 30 mg Dexlansoprazole 60 mg Esomeprazole 10 mg Esomeprazole 20 mg Esomeprazole 40 mg Lansoprazole 15 mg Lansoprazole 30 mg Omeprazole
ASEBP Pantoprazole Sodium 40 mg (generic) $0.2016 ASEBP Dexlansoprazole 30 mg Dexlansoprazole 60 mg Esomeprazole 10 mg Esomeprazole 20 mg Esomeprazole 40 mg Lansoprazole 15 mg Lansoprazole 30 mg Omeprazole
sympatholytics sympatholytics sympatholytics
 sympatholytics sympatholytics sympatholytics CNS-ACTING SYMPATHOPLEGICS Sympathetic brain signals Doesn t affect baroreceptor reflex (no orthostatic hypotension) Methyldopa α-methylne crosses BBB (+) α-adrenoreceptors
sympatholytics sympatholytics sympatholytics CNS-ACTING SYMPATHOPLEGICS Sympathetic brain signals Doesn t affect baroreceptor reflex (no orthostatic hypotension) Methyldopa α-methylne crosses BBB (+) α-adrenoreceptors
We are delighted to have Dr. Roetzheim with us today to discuss Managing Hypertension in Older Adult Patients.
 Richard Roetzheim, MD, MSPH is Professor and Chair, Department of Family Medicine at the University of South Florida Morsani College of Medicine. Dr. Roetzheim has considerable experience leading NIH funded
Richard Roetzheim, MD, MSPH is Professor and Chair, Department of Family Medicine at the University of South Florida Morsani College of Medicine. Dr. Roetzheim has considerable experience leading NIH funded
Factors Involved in Poor Control of Risk Factors
 Factors Involved in Poor Control of Risk Factors Patient compliance Clinical inertia Health Care System structure 14781 M Limitations of Formal Studies Selection of patients Recruitment and follow-up alter
Factors Involved in Poor Control of Risk Factors Patient compliance Clinical inertia Health Care System structure 14781 M Limitations of Formal Studies Selection of patients Recruitment and follow-up alter
Hypertension. Does it Matter What Medications We Use? Nishant K. Sekaran, M.D. M.Sc. Intermountain Heart Institute
 Hypertension Does it Matter What Medications We Use? Nishant K. Sekaran, M.D. M.Sc. Intermountain Heart Institute Hypertension 2017 Classification BP Category Systolic Diastolic Normal 120 and 80 Elevated
Hypertension Does it Matter What Medications We Use? Nishant K. Sekaran, M.D. M.Sc. Intermountain Heart Institute Hypertension 2017 Classification BP Category Systolic Diastolic Normal 120 and 80 Elevated
Hypertension. Most important public health problem in developed countries
 Hypertension Strategy for Continued Success in Treatment for the 21st Century November 15, 2005 Arnold B. Meshkov, M.D. Associate Professor of Medicine Temple University School of Medicine Philadelphia,
Hypertension Strategy for Continued Success in Treatment for the 21st Century November 15, 2005 Arnold B. Meshkov, M.D. Associate Professor of Medicine Temple University School of Medicine Philadelphia,
Cardiac Pathophysiology
 Cardiac Pathophysiology Evaluation Components Medical history Physical examination Routine laboratory tests Optional tests Medical History Duration and classification of hypertension. Patient history of
Cardiac Pathophysiology Evaluation Components Medical history Physical examination Routine laboratory tests Optional tests Medical History Duration and classification of hypertension. Patient history of
1. Despite the plethora of new ACE-inhibitors they offer little advantage over the earlier products captopril and enalapril.
 SUMMARY 1. Despite the plethora of new ACE-inhibitors they offer little advantage over the earlier products captopril and enalapril. 2. While diuretics and beta-blockers remain first-line antihypertensive
SUMMARY 1. Despite the plethora of new ACE-inhibitors they offer little advantage over the earlier products captopril and enalapril. 2. While diuretics and beta-blockers remain first-line antihypertensive
Diabetes and Hypertension
 Diabetes and Hypertension M.Nakhjvani,M.D Tehran University of Medical Sciences 20-8-96 Hypertension Common DM comorbidity Prevalence depends on diabetes type, age, BMI, ethnicity Major risk factor for
Diabetes and Hypertension M.Nakhjvani,M.D Tehran University of Medical Sciences 20-8-96 Hypertension Common DM comorbidity Prevalence depends on diabetes type, age, BMI, ethnicity Major risk factor for
SBP in range of 120 to 140 :no progression or regression of CAD. Sipahi et al., 2006
 Management of Hypertension in Patients with CAD M. Mohsen Ibrahim, MD Cardiology Department- Cairo University 1. What is the optimal BP in patients with hypertension and CAD? 2. What is the minimum safe
Management of Hypertension in Patients with CAD M. Mohsen Ibrahim, MD Cardiology Department- Cairo University 1. What is the optimal BP in patients with hypertension and CAD? 2. What is the minimum safe
VA/DoD Clinical Practice Guideline for the Management of Chronic Kidney Disease in Primary Care (2008) PROVIDER REFERENCE CARDS Chronic Kidney Disease
 PROVIDER REFERENCE CARDS Chronic Kidney Disease") VA/DoD Clinical Practice Guideline for the Management of Chronic Kidney Disease in Primary Care (2008) PROVIDER REFERECE CARDS Chronic Kidney Disease CKD VA/DoD Clinical Practice Guideline for the Management
VA/DoD Clinical Practice Guideline for the Management of Chronic Kidney Disease in Primary Care (2008) PROVIDER REFERECE CARDS Chronic Kidney Disease CKD VA/DoD Clinical Practice Guideline for the Management
JNC Evidence-Based Guidelines for the Management of High Blood Pressure in Adults
 JNC 8 2014 Evidence-Based Guidelines for the Management of High Blood Pressure in Adults Table of Contents Why Do We Treat Hypertension? Blood Pressure Treatment Goals Initial Therapy Strength of Recommendation
JNC 8 2014 Evidence-Based Guidelines for the Management of High Blood Pressure in Adults Table of Contents Why Do We Treat Hypertension? Blood Pressure Treatment Goals Initial Therapy Strength of Recommendation
New classification of HT Systolic Diastolic Normal <120 <80 Prehypertension Stage1HT Stage 2 HT >160 or >100
 Hypertension 1 Definition Hypertension can be defined as a condition where blood pressure is elevated to an extent that clinical benefit is obtained from blood pressure lowering. it is an important risk
Hypertension 1 Definition Hypertension can be defined as a condition where blood pressure is elevated to an extent that clinical benefit is obtained from blood pressure lowering. it is an important risk
Incidental Findings; Management of patients presenting with high BP. Phil Swales
 Incidental Findings; Management of patients presenting with high BP Phil Swales Consultant Physician Acute & General Medicine University Hospitals of Leicester NHS Trust Objectives The approach to an incidental
Incidental Findings; Management of patients presenting with high BP Phil Swales Consultant Physician Acute & General Medicine University Hospitals of Leicester NHS Trust Objectives The approach to an incidental
INDIAN HYPERTENSION GUIDELINES-II
 HYPERTENSION IN SPECIAL SITUATIONS Hypertension with diabetes mellitus Co-existence of hypertension and diabetes is being increasingly recognised. 30-35% of hypertensives are detected to have diabetes.
HYPERTENSION IN SPECIAL SITUATIONS Hypertension with diabetes mellitus Co-existence of hypertension and diabetes is being increasingly recognised. 30-35% of hypertensives are detected to have diabetes.
From the desk of the: THE VIRTUAL NEPHROLOGIST
 Hypertension, also referred to as high blood pressure or HTN, is a medical condition in which the blood pressure is chronically elevated. It is a very common illness. One out of three American adults has
Hypertension, also referred to as high blood pressure or HTN, is a medical condition in which the blood pressure is chronically elevated. It is a very common illness. One out of three American adults has
Managing Hypertension in Diabetes Sean Stewart, PharmD, BCPS, BCACP, CLS Internal Medicine Park Nicollet Clinic St Louis Park.
 Managing Hypertension in Diabetes 2015 Sean Stewart, PharmD, BCPS, BCACP, CLS Internal Medicine Park Nicollet Clinic St Louis Park Case Scenario Mike M is a 59 year old man with type 2 diabetes managed
Managing Hypertension in Diabetes 2015 Sean Stewart, PharmD, BCPS, BCACP, CLS Internal Medicine Park Nicollet Clinic St Louis Park Case Scenario Mike M is a 59 year old man with type 2 diabetes managed
Chapter 2 ~ Cardiovascular system
 Chapter 2 ~ Cardiovascular System: General Section 1 of 6 Chapter 2 ~ Cardiovascular system 2.1 Positive inotropic drugs 2.1.1 Cardiac glycosides DIGOXIN 2.2 Diuretics Elixir 50micrograms in 1ml Injection
Chapter 2 ~ Cardiovascular System: General Section 1 of 6 Chapter 2 ~ Cardiovascular system 2.1 Positive inotropic drugs 2.1.1 Cardiac glycosides DIGOXIN 2.2 Diuretics Elixir 50micrograms in 1ml Injection