Protocols for the Management of Cardiac Conditions. By Pam Bayles, RN, BSN
|
|
|
- Marybeth Parrish
- 5 years ago
- Views:
Transcription
1 Protocols for the Management of Cardiac Conditions By Pam Bayles, RN, BSN
 Note: See Glossary for an explanation of Diseases of the Heart.")
2 Deaths in Thousands 1, Years Deaths from diseases of the heart (United States: ) Note: See Glossary for an explanation of Diseases of the Heart. Source: NCHS and NHLBI. 2
3 Guidelines/Standards In 2009, over ½ million people will have their first MI. Within 1 yr. of a recognized MI 25% of men and 38% of women will die 18% of men and 35% of women will have another MI within 6 years of their first event. Over 450,000 people suffer from recurrent coronary attacks each year 50% of all case of AMI are clinically silent or unremarkable 33% report symptoms other than CP, esp. women, older adults, diabetics and pts. With HF
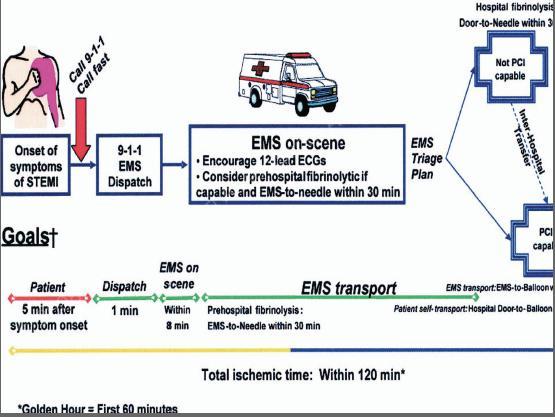
4 STEMI guidelines Reperfusion within 90 minutes with primary PCI Get artery open ASAP! Clopidogrel Loading dose of mg prior to PCI If pt. has received fibrinolytic therapy within hrs. of PCI, consider 300 mg loading dose Anticoagulants Fibrinolytics minimum of 48 hours UFH, enoxaparin (Lovenox), fondaparinux (Arixtra) Heparin or bivalirudin (Angiomax) Fibrinolytics ARB within 24 hrs. of symptom onset Statin therapy
5
6 Medical Management of STEMI 2007 Update: Class I Recommendations Initial Management O2 to keep Sat > 90% ASA mg ASAP NTG 0.4 mg SL q 5 min x 3, then decide on IV NTG ( if persistent ischemia, HF or HTN) Morphine 2-4 mg IV q 5-15 minutes for pain Discontinue NSAIDS except ASA Oral beta blocker within 24 hours
7 ACE Inhibitors in STEMI Should be started within 24 hrs. and continued indefinitely in all pts. With EF 40% With HTN, diabetes, or chronic kidney disease Who are not low risk pts. It is reasonable to give ACEI to all patients recovering from STEMI unless contraindications exist (class IIa) Should not be given if hypotensive: SBP < 100 mm Hg or 30 mm Hg below baseline
8
9
10 At least 10% of STEMI don t develop myocardial necrosis and subsequent Q waves on EKG after reperfusion therapy Successful restoration of flow is called aborting of MI If treated within the hour, about 25% of STEMI can be aborted Effectiveness of thrombolysis is highest within first 2 hours. After 12 hours, risk outweighs benefit Irreversible injury occurs within 2-4 hours of infarction Limited time for reperfusion
11 UA/NSTEMI guidelines
12 Anti-ischemic Therapy for NSTEMI O2 As needed to keep SaO2 > 90% NTG 0.4 mg SL every 5 minutes for 3 doses if ongoing ischemia IV NTG is indicated in first 48 hrs. for treatment of persistent ischemia, HF, or HTN Morphine IV if uncontrolled ischemic chest pain despite NTG (class IIa)
 Sign of HF Increased risk of cardiogenic shock Relative contraindications of beta-blockade")

13 Additional Anti-ischemic Therapy Beta Blockers Oral within 24 hrs. as with STEMI IV beta blocker for HTN if no contraindications (class IIa) Sign of HF Increased risk of cardiogenic shock Relative contraindications of beta-blockade PRI >.24 seconds 2 nd or 3 rd degree HB Active asthma or RAD Calcium Channel Blockers If continuing of frequently recurring ischemia and can t take beta blocker Verapamil or diltiazem preferred if no LV dysfunction or other contraindications Oral long acting verapamil or diltiazem for recurrent ischemia if beta blockers and nitrates have been full used (class IIa) Avoid short acting dihydropyridines (nifedipine, nicardipine)




14 Anti-ischemic Therapy continued ACEI Oral within 24 hours If pulmonary congestion or LVEF 40% Class IIa recommendations for all patients with UA/NSTEMI ARBs If patient intolerant of ACEI If clinical or X-ray signs of HF LVEF 40%

 if patient")

15 Anti-platelet Therapy for UA/NSTEMI Aspirin ASAP and indefinitely mg Plavix 300 mg (or higher) if patient unable to take ASA 75 mg daily for at least 1 month and ideally up to 1 year
16 If Invasive Therapy is Planned: Prior to Cath Lab Plavix 600 mg recommended Up to 900 mg has be used IIb/IIIa Inhibitor Eptifibatide (Integrilin) or Tirofiban (Aggrastat) preferred Abciximab (ReoPro) only if there is no delay to angiography and PCI is planned for sure
 or UFH Bivalirudin (Angiomax) or fondaparinux (Arixtra) are")

17 Anticoagulant Therapy Should be added to antiplatelet therapy ASAP Invasive Therapy Enoxaparin (lovenox) or UFH Bivalirudin (Angiomax) or fondaparinux (Arixtra) are acceptable alternatives Medical Therapy Enoxaparin or fondaparinux are preferable to UFH unless CABG planned within 24 hours Fondaparinux is preferred if patient at increased risk of bleeding

18 Long-term Therapy & Secondary Prevention




19 Additional long-term therapy & Prevention Prevention Calcium Channel Blockers For ischemic symptoms when beta blockers not effective or not tolerated Lipid Management New LDL-C goal is < 100 mg/dl (< 70 reasonable) Statin if baseline LDL-C is 100 mg/dl ( use highest dose immediately)
20 Discharge Medications Following ACS ACEI ASA Plavix Beta Blocker ARB if ACEI intolerant Statin
21 As part of other AHA guidelines, must also monitor/assess Smoking Cessation Weight Management Diabetes Management HbA1c < 7% Lipid Management LDL should be < 100 mg/dl and further reduction to < 70 mg/dl is reasonable Blood Pressure Control < 140/90 mmhg or < 130/80 if pt. has DM or chronic kidney disease Physical Activity Influenza Vaccination Projections have shown that implementation of secondary guidelines could result in saving more than 80,000 lives each year
22 Insulin drip control The presence of hyperglycemia in critically ill pts. Has been linked to adverse effects including multiple organ failure and death The Portland Diabetic Project was the first study to show the relationship between high blood glucose levels and increased risk of death, infection and length of hospital stay in cardiac surgery pts. Also showed that the use of an IV insulin infusion eradicated some of these complications Created the Portland Protocol that has been used since 1992 for tight glucose control Target
23 NICE - SUGAR Study was a multi-center, international controlled study with patients recruited from Intensive Care Units throughout Australia, New Zealand, Canada and the USA Treatment groups assigned either target blood glucose of or Found that intensive glucose control increased mortality among adults in the ICU: a blood glucose target of 180 mg or less resulted in lower mortality than did a target of 81 to 108 Severe hypoglycemia in intensive control group
24 DVT Prophylaxis Up to 2 million Americans suffer from DVT blood clots annually Approximately 300,000 patients die annually from pulmonary embolism; the majority of which result from DVT Complications from DVT will kill more Americans than AIDS and breast cancer combines Approximately 10% of all hospital deaths are directly attributed to PE DVT is the #1 cause of preventable hospital deaths
25 To meet National Patient Safety Goals, all patients are assessed upon admission for their risk of DVT The risk assessment tool looks at: Recent hip/joint surgery, fractures, trauma or spinal cord injury with resulting paralysis within the prior month History of DVT/PE of family history of clots/blood-clotting disorders Cancer, recent surgery lasting > 45 minutes, Limited mobility secondary to plaster cast, recently confined to bed > 72 hrs, central venous access Varicose veins, IBS/crohn s disease/ulcerative colitis, overweight/obese, MI, CHF, lung disease, serious infection Age Use of birth control or Hormone replacement therapy Pregnant or gave birth within last month
26 Lovenox Low molecular weight heparin Indicated for: Prophylaxis of DVT in abdominal surgery, hip replacement surgery, knee replacement surgery or medical patients with severely restricted mobility during acute illness Hip/Knee: 30 mg q12 hrs SC provided hemostasis established Hip: 40 mg SC 12 hrs. prior to OR the daily for 3 weeks Inpatient treatment of acute DVT with or without pulmonary embolism 1mg/kg q12 hrs. SC or 1.5mg/kg daily SC
27 Outpatient treatment of acute DVT without pulmonary embolism 1 mg/kg q12 hours SC Prophylaxis of ischemic complications of unstable angina and non-q wave MI 1 mg/kg SC q12 hours with ASA PO mg daily Treatment of acute STEMI managed medically or with subsequent percutaneous coronary intervention IV bolus of 30 mg plus a 1 mg/kg SC dose followed by a 1 mg/kg SC q 12hours
28 Heart Failure Complex clinical syndrome resulting from any structural or functional disorder impairing the ability of the ventricle to either fill or eject Affects 5 million in US Majority of pts. Have impaired left ventricular function Causes impaired functional capacity and quality of life Clinical syndrome resulting in Dyspnea and fatigue And/or fluid overload
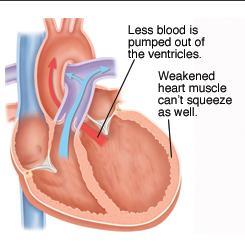
29 Systolic Dysfunction
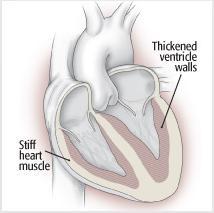
30 Diastolic Dysfunction
31
 Signs/symptoms result from elevated pulmonary pressures (SOB/paroxysmal nocturnal dyspnea) Right")

32 Left-sided Heart Failure Decrease in CO/stroke volume Pressure rises in the LV, LA, and pulmonary vasculature Hydrostatic forces can cause intracellular fluid to accumulate in the pulmonary capillary bed (pulmonary congestion) Signs/symptoms result from elevated pulmonary pressures (SOB/paroxysmal nocturnal dyspnea) Right sided Heart Failure Typically follows left-sided failure Isolated RV failure (COPD, pulmonary HTN) Pressure increases in the right side of heart Hydrostatic pressures force more blood into the systemic venous circulation Causing neck vein distention, peripheral edema, weight gain, engorgement of hepatic and gastric vessels
33 Heart Failure as Progress Disorder
34
35
36 Ace-Inhibitors Definitive evidence of mortality/morbidity reduction Interferes with ventricular remodeling Slows disease progression Used for mortality benefit not symptom relief May need to adjust diuretic dose and monitor K+ Suffix: pril Angiotensin Receptor Blockers (ARBs) Remain first choice for inhibition of RAAS Reasonable alternative to ACE inhibitor if intolerant due to cough or angioedema Combination of ACE-I and ARB not considered appropriate Suffix: sartan
37 Beta-blockers Decrease mortality/hospitalization Even better in combination with ACE-I Enhances overall well-being Slows disease progression Inhibits ventricular remodeling and apoptosis Decrease myocardial oxygen consumption Suffix: olol Diuretics Goal is to decrease congestive symptoms Loop diuretics preferred Keep K+ <4 and Mg >2
38 Digoxin For pts. With persistent symptoms already on ACE-I, Betablockers and diuretic Weak Positive inotropic effect Improved symptoms, exercise tolerance and quality of life Aldosterone Antagonists Pts. Already on ACE-I, Beta-Blocker, Diuretics, Digoxin Reduces death and rehospitalizations Spironolactone (RALES Trial) Survival benefit in NYHA Functional Class 3 or 4 HF High risk for hyperkalemia Don t initiate in pts. With elevated creatinine or elevated potassium
39 Warfarin recommended if has HF and A. Fib Antiarrhythmics ICD if had VF or unstable VT Amiodarone Medications for Diastolic Dysfunction are essentially the same Add Calcium Channel Blockers to control BP, decrease HR Suffix: pine Worsen systolic dysfunction
40
41 Left Ventricular Assist Device
42 New treatment of HF directed toward molecular cardiology The mapping of the human genome has opened up studies to look at the actual biochemical pathways of human health, disease and development As far as cardiovascular medicine, it has been realized into two pathways: Predictive diagnosis Pharmaceuticals Stem cell therapy to build new blood vessels and heart muscle
2010 ACLS Guidelines. Primary goals of therapy for patients
 2010 ACLS Guidelines Part 10: Acute Coronary Syndrome Present : 內科 R1 鍾伯欣 Supervisor: F1 吳亮廷 991110 Primary goals of therapy for patients of ACS Reduce the amount of myocardial necrosis that occurs in
2010 ACLS Guidelines Part 10: Acute Coronary Syndrome Present : 內科 R1 鍾伯欣 Supervisor: F1 吳亮廷 991110 Primary goals of therapy for patients of ACS Reduce the amount of myocardial necrosis that occurs in
Medical Management of Acute Coronary Syndrome: The roles of a noncardiologist. Norbert Lingling D. Uy, MD Professor of Medicine UERMMMCI
 Medical Management of Acute Coronary Syndrome: The roles of a noncardiologist physician Norbert Lingling D. Uy, MD Professor of Medicine UERMMMCI Outcome objectives of the discussion: At the end of the
Medical Management of Acute Coronary Syndrome: The roles of a noncardiologist physician Norbert Lingling D. Uy, MD Professor of Medicine UERMMMCI Outcome objectives of the discussion: At the end of the
Acute Coronary Syndromes
 Overview Acute Coronary Syndromes Rabeea Aboufakher, MD, FACC, FSCAI Section Chief of Cardiology Altru Health System Grand Forks, ND Epidemiology Pathophysiology Clinical features and diagnosis STEMI management
Overview Acute Coronary Syndromes Rabeea Aboufakher, MD, FACC, FSCAI Section Chief of Cardiology Altru Health System Grand Forks, ND Epidemiology Pathophysiology Clinical features and diagnosis STEMI management
Cardiovascular Health Practice Guideline Outpatient Management of Coronary Artery Disease 2003
 Authorized By: Medical Management Guideline Committee Approval Date: 12/13/01 Revision Date: 12/11/03 Beta-Blockers Nitrates Calcium Channel Blockers MEDICATIONS Indicated in post-mi, unstable angina,
Authorized By: Medical Management Guideline Committee Approval Date: 12/13/01 Revision Date: 12/11/03 Beta-Blockers Nitrates Calcium Channel Blockers MEDICATIONS Indicated in post-mi, unstable angina,
Heart Failure Clinician Guide JANUARY 2016
 Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Heart Failure Clinician Guide JANUARY 2016 Introduction This evidence-based guideline summary is based on the 2016 National Heart Failure Guideline.
Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Heart Failure Clinician Guide JANUARY 2016 Introduction This evidence-based guideline summary is based on the 2016 National Heart Failure Guideline.
Heart Failure Clinician Guide JANUARY 2018
 Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Heart Failure Clinician Guide JANUARY 2018 Introduction This evidence-based guideline summary is based on the 2018 National Heart Failure Guideline.
Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Heart Failure Clinician Guide JANUARY 2018 Introduction This evidence-based guideline summary is based on the 2018 National Heart Failure Guideline.
Clinical Case. Management of ACS Based on ACC/AHA & ESC Guidelines. Clinical Case 4/22/12. UA/NSTEMI: Definition
 Clinical Case Management of ACS Based on ACC/AHA & ESC Guidelines Dr Badri Paudel Mr M 75M Poorly controlled diabetic Smoker Presented on Sat 7pm Intense burning in the retrosternal area Clinical Case
Clinical Case Management of ACS Based on ACC/AHA & ESC Guidelines Dr Badri Paudel Mr M 75M Poorly controlled diabetic Smoker Presented on Sat 7pm Intense burning in the retrosternal area Clinical Case
Cardiac Drug Update. By Pamela P. Bayles, RN, BSN
 Cardiac Drug Update By Pamela P. Bayles, RN, BSN Advances in cardiovascular medicine over the last decade have dwarfed the major advances throughout all of history Advances over the last ten years have
Cardiac Drug Update By Pamela P. Bayles, RN, BSN Advances in cardiovascular medicine over the last decade have dwarfed the major advances throughout all of history Advances over the last ten years have
Appendix: ACC/AHA and ESC practice guidelines
 Appendix: ACC/AHA and ESC practice guidelines Definitions for guideline recommendations and level of evidence Recommendation Class I Class IIa Class IIb Class III Level of evidence Level A Level B Level
Appendix: ACC/AHA and ESC practice guidelines Definitions for guideline recommendations and level of evidence Recommendation Class I Class IIa Class IIb Class III Level of evidence Level A Level B Level
Management of Myocardial Infarction & Congestive Heart Failure. Dr. Dionne Dames-Rahming
 Management of Myocardial Infarction & Congestive Heart Failure Dr. Dionne Dames-Rahming Myocardial Infarction Objectives of Medical Management Decrease morbidity Reduce further myocardial damage or injury
Management of Myocardial Infarction & Congestive Heart Failure Dr. Dionne Dames-Rahming Myocardial Infarction Objectives of Medical Management Decrease morbidity Reduce further myocardial damage or injury
Treatment of Acute Coronary Syndromes
 Treatment of Acute Coronary Syndromes UC SF Jeffrey Tabas, M.D. sf g h Associate Professor UCSF School of Medicine Emergency Services, San Francisco General Hospital Objectives Review the updated AHA/ACC
Treatment of Acute Coronary Syndromes UC SF Jeffrey Tabas, M.D. sf g h Associate Professor UCSF School of Medicine Emergency Services, San Francisco General Hospital Objectives Review the updated AHA/ACC
Acute Coronary Syndromes. January 9, 2013 Chris Chiles M.D. FACC
 Acute Coronary Syndromes January 9, 2013 Chris Chiles M.D. FACC Disclosures None- not even a breakfast burrito from a drug company Hospitalizations in the U.S. Due to ACS Acute Coronary Syndromes* 1.57
Acute Coronary Syndromes January 9, 2013 Chris Chiles M.D. FACC Disclosures None- not even a breakfast burrito from a drug company Hospitalizations in the U.S. Due to ACS Acute Coronary Syndromes* 1.57
2018 Acute Coronary Syndrome. Robert Bender, DO, FACOI, FACC Central Maine Heart and Vascular Institute
 2018 Acute Coronary Syndrome Robert Bender, DO, FACOI, FACC Central Maine Heart and Vascular Institute Definitions: Acute Myocardial Ischemia Unstable Angina Non-ST-Elevation MI (NSTEMI) }2/3 ST-Elevation
2018 Acute Coronary Syndrome Robert Bender, DO, FACOI, FACC Central Maine Heart and Vascular Institute Definitions: Acute Myocardial Ischemia Unstable Angina Non-ST-Elevation MI (NSTEMI) }2/3 ST-Elevation
Acute Coronary Syndrome. Sonny Achtchi, DO
 Acute Coronary Syndrome Sonny Achtchi, DO Objectives Understand evidence based and practice based treatments for stabilization and initial management of ACS Become familiar with ACS risk stratification
Acute Coronary Syndrome Sonny Achtchi, DO Objectives Understand evidence based and practice based treatments for stabilization and initial management of ACS Become familiar with ACS risk stratification
Objectives. Treatment of ACS. Early Invasive Strategy. UA/NSTEMI General Concepts. UA/NSTEMI Initial Therapy/Antithrombotic
 Objectives Treatment of ACS Michael P. Gulseth, Pharm. D., BCPS Pharmacotherapy II Spring 2006 Define early invasive strategy and what patients typically receive this approach Compare/contrast the medications
Objectives Treatment of ACS Michael P. Gulseth, Pharm. D., BCPS Pharmacotherapy II Spring 2006 Define early invasive strategy and what patients typically receive this approach Compare/contrast the medications
Cindy Stephens, MSN, ANP Kelly Walker, MS, ACNP Peter Cohn, MD, FACC
 Cindy Stephens, MSN, ANP Kelly Walker, MS, ACNP Peter Cohn, MD, FACC Define Acute Coronary syndromes Explain the Cause Assessment, diagnosis and therapy Reperfusion for STEMI Complications to look for
Cindy Stephens, MSN, ANP Kelly Walker, MS, ACNP Peter Cohn, MD, FACC Define Acute Coronary syndromes Explain the Cause Assessment, diagnosis and therapy Reperfusion for STEMI Complications to look for
The Failing Heart in Primary Care
 The Failing Heart in Primary Care Hamid Ikram How fares the Heart Failure Epidemic? 4357 patients, 57% women, mean age 74 years HFSA 2010 Practice Guideline (3.1) Heart Failure Prevention A careful and
The Failing Heart in Primary Care Hamid Ikram How fares the Heart Failure Epidemic? 4357 patients, 57% women, mean age 74 years HFSA 2010 Practice Guideline (3.1) Heart Failure Prevention A careful and
Acute coronary syndromes
 Acute coronary syndromes 1 Acute coronary syndromes Acute coronary syndromes results primarily from diminished myocardial blood flow secondary to an occlusive or partially occlusive coronary artery thrombus.
Acute coronary syndromes 1 Acute coronary syndromes Acute coronary syndromes results primarily from diminished myocardial blood flow secondary to an occlusive or partially occlusive coronary artery thrombus.
ACS and Heart Failure
 ACS and Heart Failure Jonathon Firnhaber, MD, FAAFP Associate Professor The Brody School of Medicine at East Carolina University Greenville, North Carolina Learning Objectives Establish the diagnosis and
ACS and Heart Failure Jonathon Firnhaber, MD, FAAFP Associate Professor The Brody School of Medicine at East Carolina University Greenville, North Carolina Learning Objectives Establish the diagnosis and
Non ST Elevation-ACS. Michael W. Cammarata, MD
 Non ST Elevation-ACS Michael W. Cammarata, MD Case Presentation 65 year old man PMH: CAD s/p stent in 2008 HTN HLD Presents with chest pressure, substernally and radiating to the left arm and jaw, similar
Non ST Elevation-ACS Michael W. Cammarata, MD Case Presentation 65 year old man PMH: CAD s/p stent in 2008 HTN HLD Presents with chest pressure, substernally and radiating to the left arm and jaw, similar
Acute Coronary Syndrome (ACS) Initial Evaluation and Management
 Initial Evaluation and Management") Acute Coronary Syndrome (ACS) Initial Evaluation and Management Symptoms of Possible ACS Chest discomfort with or without radiation to the arm(s), jaw, or epigastrium Short of breath Weakness Diaphoresis
Acute Coronary Syndrome (ACS) Initial Evaluation and Management Symptoms of Possible ACS Chest discomfort with or without radiation to the arm(s), jaw, or epigastrium Short of breath Weakness Diaphoresis
LXIV: DRUGS: 4. RAS BLOCKADE
 LXIV: DRUGS: 4. RAS BLOCKADE ACE Inhibitors Components of RAS Actions of Angiotensin i II Indications for ACEIs Contraindications RAS blockade in hypertension RAS blockade in CAD RAS blockade in HF Limitations
LXIV: DRUGS: 4. RAS BLOCKADE ACE Inhibitors Components of RAS Actions of Angiotensin i II Indications for ACEIs Contraindications RAS blockade in hypertension RAS blockade in CAD RAS blockade in HF Limitations
Acute Coronary Syndrome
 Acute Coronary Syndrome Vik Gongidi, DO FACOI, FACC Indian River Medical Center Vero Beach, FL Slides adapted from Robert Bender, DO, FACOI, FACC Definition: Acute Myocardial Ischemia Unstable Angina Non-ST-Elevation
Acute Coronary Syndrome Vik Gongidi, DO FACOI, FACC Indian River Medical Center Vero Beach, FL Slides adapted from Robert Bender, DO, FACOI, FACC Definition: Acute Myocardial Ischemia Unstable Angina Non-ST-Elevation
Guideline for STEMI. Reperfusion at a PCI-Capable Hospital
 MANSOURA. 2015 Guideline for STEMI Reperfusion at a PCI-Capable Hospital Mahmoud Yossof MANSOURA 2015 Reperfusion Therapy for Patients with STEMI *Patients with cardiogenic shock or severe heart failure
MANSOURA. 2015 Guideline for STEMI Reperfusion at a PCI-Capable Hospital Mahmoud Yossof MANSOURA 2015 Reperfusion Therapy for Patients with STEMI *Patients with cardiogenic shock or severe heart failure
Antialdosterone treatment in heart failure
 Update on the Treatment of Chronic Heart Failure 2012 Antialdosterone treatment in heart failure 전남의대윤현주 Chronic Heart Failure Prognosis of Heart failure Cecil, Text book of Internal Medicine, 22 th edition
Update on the Treatment of Chronic Heart Failure 2012 Antialdosterone treatment in heart failure 전남의대윤현주 Chronic Heart Failure Prognosis of Heart failure Cecil, Text book of Internal Medicine, 22 th edition
Congestive Heart Failure: Outpatient Management
 The Chattanooga Heart Institute Cardiovascular Symposium Congestive Heart Failure: Outpatient Management E. Philip Lehman MD, MPP Disclosure No financial disclosures. Objectives Evidence-based therapy
The Chattanooga Heart Institute Cardiovascular Symposium Congestive Heart Failure: Outpatient Management E. Philip Lehman MD, MPP Disclosure No financial disclosures. Objectives Evidence-based therapy
6/1/18 LEARNING OBJECTIVES PATIENT POPULATION PRESENTATIONS
 PREVENTING HOSPITAL READMISSIONS IN CARDIOVASCULAR PATIENTS Christina Cortez Perry, MSN, FNP-C, CCCC Cardiology Coordinator- Corpus Christi Medical Center 1 2 LEARNING OBJECTIVES Identify the target patient
PREVENTING HOSPITAL READMISSIONS IN CARDIOVASCULAR PATIENTS Christina Cortez Perry, MSN, FNP-C, CCCC Cardiology Coordinator- Corpus Christi Medical Center 1 2 LEARNING OBJECTIVES Identify the target patient
Primary and Secondary Prevention of Cardiovascular Disease. Frank J. Green, M.D., F.A.C.C. St. Vincent Medical Group
 Primary and Secondary Prevention of Cardiovascular Disease Frank J. Green, M.D., F.A.C.C. St. Vincent Medical Group AHA Diet and Lifestyle Recommendations Balance calorie intake and physical activity to
Primary and Secondary Prevention of Cardiovascular Disease Frank J. Green, M.D., F.A.C.C. St. Vincent Medical Group AHA Diet and Lifestyle Recommendations Balance calorie intake and physical activity to
Cardiovascular Concerns in Intermediate Care
 Cardiovascular Concerns in Intermediate Care GINA ST. JEAN RN, MSN, CCRN-CSC CLINICAL NURSE EDUCATOR HEART AND & CRITICAL AND INTERMEDIATE CARE Objectives: Identify how to do a thorough assessment of the
Cardiovascular Concerns in Intermediate Care GINA ST. JEAN RN, MSN, CCRN-CSC CLINICAL NURSE EDUCATOR HEART AND & CRITICAL AND INTERMEDIATE CARE Objectives: Identify how to do a thorough assessment of the
M/39 CC D. => peak CKMB (12 hr later) ng/ml T.chol/TG/HDL/LDL 180/150/48/102 mg/dl #
 ng/ml T.chol/TG/HDL/LDL 180/150/48/102 mg/dl #") Acute Coronary Syndrome - Case Review - Young-Guk Ko, MD Yonsei Cardiovascular Center Yonsei University College of Medicine Case 1 M/39 #4306212 CC D : Severe squeezing chest pain : 4 hours, aggravated
Acute Coronary Syndrome - Case Review - Young-Guk Ko, MD Yonsei Cardiovascular Center Yonsei University College of Medicine Case 1 M/39 #4306212 CC D : Severe squeezing chest pain : 4 hours, aggravated
Acute Myocardial Infarction
 Acute Myocardial Infarction Hafeza Shaikh, DO, FACC, RPVI Lourdes Cardiology Services Asst.Program Director, Cardiology Fellowship Associate Professor, ROWAN-SOM Acute Myocardial Infarction Definition:
Acute Myocardial Infarction Hafeza Shaikh, DO, FACC, RPVI Lourdes Cardiology Services Asst.Program Director, Cardiology Fellowship Associate Professor, ROWAN-SOM Acute Myocardial Infarction Definition:
An update on the management of UA / NSTEMI. Michael H. Crawford, MD
 An update on the management of UA / NSTEMI Michael H. Crawford, MD New ACC/AHA Guidelines 2007 What s s new in the last 5 years CT imaging advances Ascendancy of troponin and BNP Clarification of ACEI/ARB
An update on the management of UA / NSTEMI Michael H. Crawford, MD New ACC/AHA Guidelines 2007 What s s new in the last 5 years CT imaging advances Ascendancy of troponin and BNP Clarification of ACEI/ARB
ST-elevation myocardial infarctions (STEMIs)
") Guidelines for Treating STEMI: Case-Based Questions As many as 25% of eligible patients presenting with STEMI do not receive any form of reperfusion therapy. The ACC/AHA guidelines highlight steps to improve
Guidelines for Treating STEMI: Case-Based Questions As many as 25% of eligible patients presenting with STEMI do not receive any form of reperfusion therapy. The ACC/AHA guidelines highlight steps to improve
Objectives. Identify early signs and symptoms of Acute Coronary Syndrome Initiate proper protocol for ACS patient 10/2013 2
 10/2013 1 Objectives Identify early signs and symptoms of Acute Coronary Syndrome Initiate proper protocol for ACS patient 10/2013 2 Purpose of this Education Module: Chest Pain Center Accreditation involves
10/2013 1 Objectives Identify early signs and symptoms of Acute Coronary Syndrome Initiate proper protocol for ACS patient 10/2013 2 Purpose of this Education Module: Chest Pain Center Accreditation involves
Acute Coronary Syndrome. ACC/AHA 2002 Guidelines
 Acute Coronary Syndrome ACC/AHA 2002 Guidelines ACS Unstable Angina Non ST elevation MI ST elevation MI ACS UA and Non STEMI described in these guidelines Management of STEMI described in separate guidelines
Acute Coronary Syndrome ACC/AHA 2002 Guidelines ACS Unstable Angina Non ST elevation MI ST elevation MI ACS UA and Non STEMI described in these guidelines Management of STEMI described in separate guidelines
ST Elevation Myocardial Infarction
 ST Elevation Myocardial Infarction Scott M. Lilly, MD, PhD Assistant Professor Clinical Department of Cardiovascular Medicine The Ohio State University Wexner Medical Center Case Presentation 46 year old
ST Elevation Myocardial Infarction Scott M. Lilly, MD, PhD Assistant Professor Clinical Department of Cardiovascular Medicine The Ohio State University Wexner Medical Center Case Presentation 46 year old
Heart Failure (HF) Treatment
 Treatment") Heart Failure (HF) Treatment Heart Failure (HF) Complex, progressive disorder. The heart is unable to pump sufficient blood to meet the needs of the body. Its cardinal symptoms are dyspnea, fatigue, and
Heart Failure (HF) Treatment Heart Failure (HF) Complex, progressive disorder. The heart is unable to pump sufficient blood to meet the needs of the body. Its cardinal symptoms are dyspnea, fatigue, and
ST Elevation Myocardial Infarction
 ST Elevation Myocardial Infarction Scott M. Lilly, MD, PhD Assistant Professor Clinical Department of Cardiovascular Medicine The Ohio State University Wexner Medical Center Outline Case Presentation STEMI
ST Elevation Myocardial Infarction Scott M. Lilly, MD, PhD Assistant Professor Clinical Department of Cardiovascular Medicine The Ohio State University Wexner Medical Center Outline Case Presentation STEMI
Prescribe appropriate immunizations for. Prescribe childhood immunization as per. Prescribe influenza vaccinations in high-risk
 Supplemental Digital Appendix 1 46 Health Care Problems and the Corresponding 59 Practice Indicators Expected of All Physicians Entering or in Practice Infectious and parasitic diseases Avoidable complications/death
Supplemental Digital Appendix 1 46 Health Care Problems and the Corresponding 59 Practice Indicators Expected of All Physicians Entering or in Practice Infectious and parasitic diseases Avoidable complications/death
CABG Surgery following STEMI
 CABG Surgery following STEMI Susana Harrington, MS,APRN-NP Cardio-Thoracic Surgery Nebraska Methodist Hospital February 15, 2018 2013 ACCF/AHA Guideline for the Management of ST-Elevation Myocardial Infarction:
CABG Surgery following STEMI Susana Harrington, MS,APRN-NP Cardio-Thoracic Surgery Nebraska Methodist Hospital February 15, 2018 2013 ACCF/AHA Guideline for the Management of ST-Elevation Myocardial Infarction:
Learning Objectives. Epidemiology of Acute Coronary Syndrome
 Cardiovascular Update: Antiplatelet therapy in acute coronary syndromes PHILLIP WEEKS, PHARM.D., BCPS-AQ CARDIOLOGY Learning Objectives Interpret guidelines as they relate to constructing an antiplatelet
Cardiovascular Update: Antiplatelet therapy in acute coronary syndromes PHILLIP WEEKS, PHARM.D., BCPS-AQ CARDIOLOGY Learning Objectives Interpret guidelines as they relate to constructing an antiplatelet
Heart Failure: Guideline-Directed Management and Therapy
 Heart Failure: Guideline-Directed Management and Therapy Guideline-Directed Management and Therapy (GDMT) was developed by the American College of Cardiology and American Heart Association to define the
Heart Failure: Guideline-Directed Management and Therapy Guideline-Directed Management and Therapy (GDMT) was developed by the American College of Cardiology and American Heart Association to define the
Controversies in Cardiac Pharmacology
 Controversies in Cardiac Pharmacology Thomas D. Conley, MD FACC FSCAI Disclosures I have no relevant relationships with commercial interests to disclose. 1 Doc, do I really need to take all these medicines?
Controversies in Cardiac Pharmacology Thomas D. Conley, MD FACC FSCAI Disclosures I have no relevant relationships with commercial interests to disclose. 1 Doc, do I really need to take all these medicines?
HEART FAILURE. Heart Failure in the US. Heart Failure (HF) 3/2/2014
 3/2/2014") HEART FAILURE Martina Frost, PA-C Desert Cardiology of Tucson Northwest Medical Center March 2014 Heart Failure in the US Prevalence - ~5 million 650,000 new cases annually 300,000 deaths annually Leading
HEART FAILURE Martina Frost, PA-C Desert Cardiology of Tucson Northwest Medical Center March 2014 Heart Failure in the US Prevalence - ~5 million 650,000 new cases annually 300,000 deaths annually Leading
Management of Stable Ischemic Heart Disease. Vinay Madan MD February 10, 2018
 Management of Stable Ischemic Heart Disease Vinay Madan MD February 10, 2018 1 Disclosure No financial disclosure. 2 Overview of SIHD Diagnosis Outline of talk Functional vs. Anatomic assessment Management
Management of Stable Ischemic Heart Disease Vinay Madan MD February 10, 2018 1 Disclosure No financial disclosure. 2 Overview of SIHD Diagnosis Outline of talk Functional vs. Anatomic assessment Management
Medicine Dr. Omed Lecture 2 Stable and Unstable Angina
 Medicine Dr. Omed Lecture 2 Stable and Unstable Angina Risk stratification in stable angina. High Risk; *post infarct angina, *poor effort tolerance, *ischemia at low workload, *left main or three vessel
Medicine Dr. Omed Lecture 2 Stable and Unstable Angina Risk stratification in stable angina. High Risk; *post infarct angina, *poor effort tolerance, *ischemia at low workload, *left main or three vessel
Management of Acute Myocardial Infarction
 Management of Acute Myocardial Infarction Prof. Hossam Kandil Professor of Cardiology Cairo University ST Elevation Acute Myocardial Infarction Aims Of Management Emergency care (Pre-hospital) Early care
Management of Acute Myocardial Infarction Prof. Hossam Kandil Professor of Cardiology Cairo University ST Elevation Acute Myocardial Infarction Aims Of Management Emergency care (Pre-hospital) Early care
2018 HPN Provider Summary Guide. Adult Cardiology Patients (18 Years and Older) Referral Guidelines
 Referral Guidelines") 12.2 CARDIOLOGY REFERRAL GUIDELINES Contracted Group: Southwest Medical Associates For Appointments: 888 S. Rancho Las Vegas, NV 89109 Phone: (702) 877-8654 Fax: (702) 242-7998 Adult Cardiology Patients
12.2 CARDIOLOGY REFERRAL GUIDELINES Contracted Group: Southwest Medical Associates For Appointments: 888 S. Rancho Las Vegas, NV 89109 Phone: (702) 877-8654 Fax: (702) 242-7998 Adult Cardiology Patients
CLINICAL PRACTICE GUIDELINE
 CLINICAL PRACTICE GUIDELINE Procedure: Congestive Heart Failure Guideline Review Cycle: Biennial Reviewed By: Amish Purohit, MD, MHA, CPE, FACHE Review Date: November 2014 Committee Approval Date: 11/12/2014
CLINICAL PRACTICE GUIDELINE Procedure: Congestive Heart Failure Guideline Review Cycle: Biennial Reviewed By: Amish Purohit, MD, MHA, CPE, FACHE Review Date: November 2014 Committee Approval Date: 11/12/2014
Jessica Bryan, Natalia Evans, Karlyn Henderson, & Whitney Parks
 Jessica Bryan, Natalia Evans, Karlyn Henderson, & Whitney Parks 1. What is the most common cause of death in hospitalized patients? 1. Hospital-acquired infection 2. Pulmonary embolism 3. Myocardial infarction
Jessica Bryan, Natalia Evans, Karlyn Henderson, & Whitney Parks 1. What is the most common cause of death in hospitalized patients? 1. Hospital-acquired infection 2. Pulmonary embolism 3. Myocardial infarction
Program Metrics. New Unique ID. Old Unique ID. Metric Set Metric Name Description. Old Metric Name
 Program Metrics The list below includes the metrics that will be calculated by the PINNACLE Registry for the outpatient office setting. These include metrics for, Atrial Fibrillation, Hypertension and.
Program Metrics The list below includes the metrics that will be calculated by the PINNACLE Registry for the outpatient office setting. These include metrics for, Atrial Fibrillation, Hypertension and.
Timing of Surgery After Percutaneous Coronary Intervention
 Timing of Surgery After Percutaneous Coronary Intervention Deepak Talreja, MD, FACC Bayview/EVMS/Sentara Outline/Highlights Timing of elective surgery What to do with medications Stopping anti-platelet
Timing of Surgery After Percutaneous Coronary Intervention Deepak Talreja, MD, FACC Bayview/EVMS/Sentara Outline/Highlights Timing of elective surgery What to do with medications Stopping anti-platelet
DISCUSSION QUESTION - 1
 CASE PRESENTATION 87 year old male No past history of diabetes, HTN, dyslipidemia or smoking Very active Medications: omeprazole for heart burn Admitted because of increasing retrosternal chest pressure
CASE PRESENTATION 87 year old male No past history of diabetes, HTN, dyslipidemia or smoking Very active Medications: omeprazole for heart burn Admitted because of increasing retrosternal chest pressure
APPENDIX F: CASE REPORT FORM
 APPENDIX F: CASE REPORT FORM Instruction: Complete this form to notify all ACS admissions at your centre to National Cardiovascular Disease Registry. Where check boxes are provided, check ( ) one or more
APPENDIX F: CASE REPORT FORM Instruction: Complete this form to notify all ACS admissions at your centre to National Cardiovascular Disease Registry. Where check boxes are provided, check ( ) one or more
Introductory Clinical Pharmacology Chapter 41 Antihypertensive Drugs
 Introductory Clinical Pharmacology Chapter 41 Antihypertensive Drugs Blood Pressure Normal = sys
Introductory Clinical Pharmacology Chapter 41 Antihypertensive Drugs Blood Pressure Normal = sys
Tailoring adjunctive antithrombotic therapy to reperfusion strategy in STEMI
 Tailoring adjunctive antithrombotic therapy to reperfusion strategy in STEMI Adel El-Etriby; MD Professor of Cardiology Ain Shams University President of the Egyptian Working Group of Interventional Cardiology
Tailoring adjunctive antithrombotic therapy to reperfusion strategy in STEMI Adel El-Etriby; MD Professor of Cardiology Ain Shams University President of the Egyptian Working Group of Interventional Cardiology
Beta-blockers in Patients with Mid-range Left Ventricular Ejection Fraction after AMI Improved Clinical Outcomes
 Beta-blockers in Patients with Mid-range Left Ventricular Ejection Fraction after AMI Improved Clinical Outcomes Seung-Jae Joo and other KAMIR-NIH investigators Department of Cardiology, Jeju National
Beta-blockers in Patients with Mid-range Left Ventricular Ejection Fraction after AMI Improved Clinical Outcomes Seung-Jae Joo and other KAMIR-NIH investigators Department of Cardiology, Jeju National
Acute Coronary Syndrome- The Role of the ACS Clinic in Providing Best Practice Care
 Acute Coronary Syndrome- The Role of the ACS Clinic in Providing Best Practice Care Deborah Pora MSN, ANP-C, RCIS Objectives Review the latest treatment guidelines for adults with acute coronary syndrome
Acute Coronary Syndrome- The Role of the ACS Clinic in Providing Best Practice Care Deborah Pora MSN, ANP-C, RCIS Objectives Review the latest treatment guidelines for adults with acute coronary syndrome
Quinn Capers, IV, MD
 Heart Attacks Mended Hearts Presentation, January, 2017 Quinn Capers, IV, MD Associate Professor of Medicine (Cardiovascular Medicine) Director, Transradial Coronary Interventions Division of Cardiovascular
Heart Attacks Mended Hearts Presentation, January, 2017 Quinn Capers, IV, MD Associate Professor of Medicine (Cardiovascular Medicine) Director, Transradial Coronary Interventions Division of Cardiovascular
Summary/Key Points Introduction
 Summary/Key Points Introduction Scope of Heart Failure (HF) o 6.5 million Americans 20 years of age have HF o 960,000 new cases of HF diagnosed annually o 5-year survival rate for HF is ~50% Classification
Summary/Key Points Introduction Scope of Heart Failure (HF) o 6.5 million Americans 20 years of age have HF o 960,000 new cases of HF diagnosed annually o 5-year survival rate for HF is ~50% Classification
2012 Core Measures. Acute Myocardial Infarction (AMI)
") 2012 Core Measures Acute Myocardial Infarction (AMI) Aspirin at Arrival Aspirin Prescribed at Discharge Angiotensin converting enzyme inhibitor (ACEI) or angiotensin receptor blocker (ARB) for left ventricular
2012 Core Measures Acute Myocardial Infarction (AMI) Aspirin at Arrival Aspirin Prescribed at Discharge Angiotensin converting enzyme inhibitor (ACEI) or angiotensin receptor blocker (ARB) for left ventricular
Clinical Policy: Dalteparin (Fragmin) Reference Number: ERX.SPA.207 Effective Date:
 Reference Number: ERX.SPA.207 Effective Date:") Clinical Policy: (Fragmin) Reference Number: ERX.SPA.207 Effective Date: 01.11.17 Last Review Date: 02.18 Revision Log See Important Reminder at the end of this policy for important regulatory and legal
Clinical Policy: (Fragmin) Reference Number: ERX.SPA.207 Effective Date: 01.11.17 Last Review Date: 02.18 Revision Log See Important Reminder at the end of this policy for important regulatory and legal
ST ELEVATION MYOCARDIAL INFARCTION (STEMI) Gordon Kritzer, MD, FACC Virginia Mason Medical Center, Seattle
 Gordon Kritzer, MD, FACC Virginia Mason Medical Center, Seattle") ST ELEVATION MYOCARDIAL INFARCTION (STEMI) Gordon Kritzer, MD, FACC Virginia Mason Medical Center, Seattle STEMI ACS and STEMI History and physical, differential diagnosis ECGs Initial Therapy and management
ST ELEVATION MYOCARDIAL INFARCTION (STEMI) Gordon Kritzer, MD, FACC Virginia Mason Medical Center, Seattle STEMI ACS and STEMI History and physical, differential diagnosis ECGs Initial Therapy and management
Acute Myocardial Infarction. Willis E. Godin D.O., FACC
 Acute Myocardial Infarction Willis E. Godin D.O., FACC Acute Myocardial Infarction Definition: Decreased delivery of oxygen and nutrients to the myocardium Myocardial tissue necrosis causing irreparable
Acute Myocardial Infarction Willis E. Godin D.O., FACC Acute Myocardial Infarction Definition: Decreased delivery of oxygen and nutrients to the myocardium Myocardial tissue necrosis causing irreparable
Cardiac evaluation for the noncardiac. Nathaen Weitzel MD University of Colorado Denver Dept of Anesthesiology
 Cardiac evaluation for the noncardiac patient Nathaen Weitzel MD University of Colorado Denver Dept of Anesthesiology Objectives! Review ACC / AHA guidelines as updated for 2009! Discuss new recommendations
Cardiac evaluation for the noncardiac patient Nathaen Weitzel MD University of Colorado Denver Dept of Anesthesiology Objectives! Review ACC / AHA guidelines as updated for 2009! Discuss new recommendations
ACUTE HEART FAILURE. Julie Gorchynski MD, MSc, FACEP, FAAEM. Department of Emergency Medicine Emergency Residency Program UTHSC, San Antonio TCEP 2014
 ACUTE HEART FAILURE Julie Gorchynski MD, MSc, FACEP, FAAEM Department of Emergency Medicine Emergency Residency Program UTHSC, San Antonio TCEP 2014 No disclosures Objectives Overview Cases Current Therapy
ACUTE HEART FAILURE Julie Gorchynski MD, MSc, FACEP, FAAEM Department of Emergency Medicine Emergency Residency Program UTHSC, San Antonio TCEP 2014 No disclosures Objectives Overview Cases Current Therapy
Current Treatment Of Ischemic Heart Disease In the United States: An Overview. By Dr Gary Mo
 Current Treatment Of Ischemic Heart Disease In the United States: An Overview By Dr Gary Mo 1 Ischemic Heart Disease in the US 1. Cardiovascular disease remains the most common cause of death and is responsible
Current Treatment Of Ischemic Heart Disease In the United States: An Overview By Dr Gary Mo 1 Ischemic Heart Disease in the US 1. Cardiovascular disease remains the most common cause of death and is responsible
Angina Luis Tulloch, MD 03/27/2012
 Angina Luis Tulloch, MD 03/27/2012 Acute coronary syndromes ACS STE > 1 mm, new LBBB* Increased cardiac enzymes STEMI Yes Yes NSTEMI No Yes UA No No *Recognize Wellen s sign/syndrome, posterior wall MI,
Angina Luis Tulloch, MD 03/27/2012 Acute coronary syndromes ACS STE > 1 mm, new LBBB* Increased cardiac enzymes STEMI Yes Yes NSTEMI No Yes UA No No *Recognize Wellen s sign/syndrome, posterior wall MI,
Acute Coronary Syndrome. Cindy Baker, MD FACC Director Peripheral Vascular Interventions Division of Cardiovascular Medicine
 Acute Coronary Syndrome Cindy Baker, MD FACC Director Peripheral Vascular Interventions Division of Cardiovascular Medicine Topics Timing is everything So many drugs to choose from What s a MINOCA? 2 Acute
Acute Coronary Syndrome Cindy Baker, MD FACC Director Peripheral Vascular Interventions Division of Cardiovascular Medicine Topics Timing is everything So many drugs to choose from What s a MINOCA? 2 Acute
Antihypertensive Agents Part-2. Assistant Prof. Dr. Najlaa Saadi PhD Pharmacology Faculty of Pharmacy University of Philadelphia
 Antihypertensive Agents Part-2 Assistant Prof. Dr. Najlaa Saadi PhD Pharmacology Faculty of Pharmacy University of Philadelphia Agents that block production or action of angiotensin Angiotensin-converting
Antihypertensive Agents Part-2 Assistant Prof. Dr. Najlaa Saadi PhD Pharmacology Faculty of Pharmacy University of Philadelphia Agents that block production or action of angiotensin Angiotensin-converting
Cardiovascular Pharmacotherapy
 Cardiovascular Pharmacotherapy Overview Mechanism of cardiovascular drugs Indications and clinical use in cardiology Renin-Angiotensin Inhibitors: Angiotensin-Converting Enzyme Inhibitors, Angiotensin
Cardiovascular Pharmacotherapy Overview Mechanism of cardiovascular drugs Indications and clinical use in cardiology Renin-Angiotensin Inhibitors: Angiotensin-Converting Enzyme Inhibitors, Angiotensin
Heart Failure. Jay Shavadia
 Heart Failure Jay Shavadia Definition Clinical syndrome characterized by: Symptoms: breathlessness at rest or on exercise, fatigue, tiredness or ankle swelling AND Signs: tachycardia, tachypnea, pulmonary
Heart Failure Jay Shavadia Definition Clinical syndrome characterized by: Symptoms: breathlessness at rest or on exercise, fatigue, tiredness or ankle swelling AND Signs: tachycardia, tachypnea, pulmonary
Chapter (9) Calcium Antagonists
 Calcium Antagonists") Chapter (9) Calcium Antagonists (CALCIUM CHANNEL BLOCKERS) Classification Mechanism of Anti-ischemic Actions Indications Drug Interaction with Verapamil Contraindications Adverse Effects Treatment of Drug
Chapter (9) Calcium Antagonists (CALCIUM CHANNEL BLOCKERS) Classification Mechanism of Anti-ischemic Actions Indications Drug Interaction with Verapamil Contraindications Adverse Effects Treatment of Drug
Medical Treatment for acute Decompensated Heart Failure. Vlasis Ninios Cardiologist St. Luke s s Hospital Thessaloniki 2011
 Medical Treatment for acute Decompensated Heart Failure Vlasis Ninios Cardiologist St. Luke s s Hospital Thessaloniki 2011 2010 HFSA guidelines for ADHF 2009 focused update of the 2005 American College
Medical Treatment for acute Decompensated Heart Failure Vlasis Ninios Cardiologist St. Luke s s Hospital Thessaloniki 2011 2010 HFSA guidelines for ADHF 2009 focused update of the 2005 American College
Acute Coronary Syndrome
 Acute Coronary Syndrome Clinical Manifestation of CAD Silent Ischemia/asymptomatic Stable Angina Acute Coronary Syndrome (Non- STEMI/UA and STEMI) Arrhythmias Heart Failure Sudden Death Pain patterns with
Acute Coronary Syndrome Clinical Manifestation of CAD Silent Ischemia/asymptomatic Stable Angina Acute Coronary Syndrome (Non- STEMI/UA and STEMI) Arrhythmias Heart Failure Sudden Death Pain patterns with
ADULT TRANSCATHETER AORTIC VALVE REPLACEMENT (TAVR) TELEMETRY BED TRANSFER ORDERS 1 of 4
 TELEMETRY BED TRANSFER ORDERS 1 of 4") TELEMETRY BED TRANSFER 1 of 4 9 Actual 9 Estimated Patient ID Area Weight kg 9 Actual 9 Estimated Height cm ALLERGIES: REFER TO ALLERGY PROFILE/ POWERCHART Transfer to: 10 South Attending Physician: Diagnosis:
TELEMETRY BED TRANSFER 1 of 4 9 Actual 9 Estimated Patient ID Area Weight kg 9 Actual 9 Estimated Height cm ALLERGIES: REFER TO ALLERGY PROFILE/ POWERCHART Transfer to: 10 South Attending Physician: Diagnosis:
2013 ACCF/AHA Guideline for the Management of ST-Elevation Myocardial Infarction
 2013 ACCF/AHA Guideline for the Management of ST-Elevation Myocardial Infarction Developed in Collaboration with American College of Emergency Physicians and Society for Cardiovascular Angiography and
2013 ACCF/AHA Guideline for the Management of ST-Elevation Myocardial Infarction Developed in Collaboration with American College of Emergency Physicians and Society for Cardiovascular Angiography and
A Report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines
 A Report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines 2013 ACCF/AHA Guideline for the Management of ST-Elevation Myocardial Infarction 1
A Report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines 2013 ACCF/AHA Guideline for the Management of ST-Elevation Myocardial Infarction 1
Role of Clopidogrel in Acute Coronary Syndromes. Hossam Kandil,, MD. Professor of Cardiology Cairo University
 Role of Clopidogrel in Acute Coronary Syndromes Hossam Kandil,, MD Professor of Cardiology Cairo University ACS Treatment Strategies Reperfusion/Revascularization Therapy Thrombolysis PCI (with/ without
Role of Clopidogrel in Acute Coronary Syndromes Hossam Kandil,, MD Professor of Cardiology Cairo University ACS Treatment Strategies Reperfusion/Revascularization Therapy Thrombolysis PCI (with/ without
Know the Quality of our Care at Every Step. Kansas City ACS Summit BI-State Cardiovascular Education Consortium
 Know the Quality of our Care at Every Step Kansas City ACS Summit BI-State Cardiovascular Education Consortium Welcome to the Kansas City ACS Summit Objectives: Follow the flow and care of an ACS patient
Know the Quality of our Care at Every Step Kansas City ACS Summit BI-State Cardiovascular Education Consortium Welcome to the Kansas City ACS Summit Objectives: Follow the flow and care of an ACS patient
Diagnosis and Management of Acute Myocardial Infarction
 Diagnosis and Management of Acute Myocardial Infarction Acute Myocardial Infarction (AMI) occurs as a result of prolonged myocardial ischemia Atherosclerosis leads to endothelial rupture or erosion that
Diagnosis and Management of Acute Myocardial Infarction Acute Myocardial Infarction (AMI) occurs as a result of prolonged myocardial ischemia Atherosclerosis leads to endothelial rupture or erosion that
Coronary Artery Disease (CAD) Clinician Guide SEPTEMBER 2017
 Clinician Guide SEPTEMBER 2017") Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Coronary Artery Disease (CAD) Clinician Guide SEPTEMBER 2017 Introduction This Clinician Guide is based on the 2017 KP National Coronary Artery Disease
Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Coronary Artery Disease (CAD) Clinician Guide SEPTEMBER 2017 Introduction This Clinician Guide is based on the 2017 KP National Coronary Artery Disease
Table 1. Proposed Measures for Use in Establishing Quality Performance Standards that ACOs Must Meet for Shared Savings
 CMS-1345-P 174 Table 1. Proposed Measures for Use in Establishing Quality Performance Standards that ACOs Must Meet for Shared Savings AIM: Better Care for Individuals 1. Patient/Care Giver Experience
CMS-1345-P 174 Table 1. Proposed Measures for Use in Establishing Quality Performance Standards that ACOs Must Meet for Shared Savings AIM: Better Care for Individuals 1. Patient/Care Giver Experience
SHOULD BETA BLOCKERS BE USED ROUTINELY IN POST MI PATIENTS WITH PRESERVED LV FUNCTION?
 SHOULD BETA BLOCKERS BE USED ROUTINELY IN POST MI PATIENTS WITH PRESERVED LV FUNCTION? Doron Zahger, MD Department of Cardiology, Soroka University Medical Center, Faculty of Health Sciences, Ben Gurion
SHOULD BETA BLOCKERS BE USED ROUTINELY IN POST MI PATIENTS WITH PRESERVED LV FUNCTION? Doron Zahger, MD Department of Cardiology, Soroka University Medical Center, Faculty of Health Sciences, Ben Gurion
Chest Pain Acute Coronary Syndrome Version 4 4/10/17 This order set is designed to be used with an admission set or for a patient already admitted
 Patient Name: Diagnosis: Allergies with reaction type: Chest Pain Acute Coronary Syndrome Version 4 4/10/17 This order set is designed to be used with an admission set or for a patient already admitted
Patient Name: Diagnosis: Allergies with reaction type: Chest Pain Acute Coronary Syndrome Version 4 4/10/17 This order set is designed to be used with an admission set or for a patient already admitted
2017 AHA/ACC Clinical Performance and Quality Measures for Adults With ST-Elevation and Non ST-Elevation Myocardial Infarction
 2017 AHA/ACC Clinical Performance and Quality Measures for Adults With ST-Elevation and Non ST-Elevation Myocardial Infarction Ramzi Khalil MD FACC Assistant Professor Allegheny Gen.Hospital AHN Speakers
2017 AHA/ACC Clinical Performance and Quality Measures for Adults With ST-Elevation and Non ST-Elevation Myocardial Infarction Ramzi Khalil MD FACC Assistant Professor Allegheny Gen.Hospital AHN Speakers
Therapies for ACS The Articles You ve Got to Know!!
 Therapies for ACS The Articles You ve Got to Know!! Amal Mattu, MD, FAAEM, FACEP Professor and Vice Chair Department of Emergency Medicine University of Maryland School of Medicine Baltimore, Maryland
Therapies for ACS The Articles You ve Got to Know!! Amal Mattu, MD, FAAEM, FACEP Professor and Vice Chair Department of Emergency Medicine University of Maryland School of Medicine Baltimore, Maryland
Cardiovascular Disorders Lecture 3 Coronar Artery Diseases
 Cardiovascular Disorders Lecture 3 Coronar Artery Diseases By Prof. El Sayed Abdel Fattah Eid Lecturer of Internal Medicine Delta University Coronary Heart Diseases It is the leading cause of death in
Cardiovascular Disorders Lecture 3 Coronar Artery Diseases By Prof. El Sayed Abdel Fattah Eid Lecturer of Internal Medicine Delta University Coronary Heart Diseases It is the leading cause of death in
AMI Talking Points. Provide appropriate treatment to Acute MI patients with these core measures:
 AMI Provide appropriate treatment to Acute MI patients with these core measures: Aspirin received within 24 hours of arrival or contraindication documented Primary PCI Received Within 90 Minutes of Hospital
AMI Provide appropriate treatment to Acute MI patients with these core measures: Aspirin received within 24 hours of arrival or contraindication documented Primary PCI Received Within 90 Minutes of Hospital
Incidence. 4.8 million in the United States. 400,000 new cases/year. 20 million patients with asymptomatic LV dysfunction
 Heart Failure Diagnosis According to the Working Group in Heart Failure, CHF is a syndrome where the diagnosis has the following essential components: A combination of: Symptoms, typically breathlessness
Heart Failure Diagnosis According to the Working Group in Heart Failure, CHF is a syndrome where the diagnosis has the following essential components: A combination of: Symptoms, typically breathlessness
Coronary Artery Disease Clinical Practice Guidelines
 Coronary Artery Disease Clinical Practice Guidelines Guidelines are systematically developed statements to assist patients and providers in choosing appropriate healthcare for specific clinical conditions.
Coronary Artery Disease Clinical Practice Guidelines Guidelines are systematically developed statements to assist patients and providers in choosing appropriate healthcare for specific clinical conditions.
2013, American Heart Association
 2013, American Heart Association Mission: Lifeline - Data, Reports and ACTION Registry - GWTG THE MISSION: BETTER HEART ATTACK CARE FOR YOUR COMMUNITY THE LIFELINE: THE AMERICAN HEART ASSOCIATION AND YOU
2013, American Heart Association Mission: Lifeline - Data, Reports and ACTION Registry - GWTG THE MISSION: BETTER HEART ATTACK CARE FOR YOUR COMMUNITY THE LIFELINE: THE AMERICAN HEART ASSOCIATION AND YOU
8/28/2018. Pre-op Evaluation for non cardiac surgery. A quick review from 2007!! Disclosures. John Steuter, MD. None
 Pre-op Evaluation for non cardiac surgery John Steuter, MD Disclosures None A quick review from 2007!! Fliesheret al, ACC/AHA 2007 Guidelines on Perioperative Cardiovascular Evaluation and are for Noncardiac
Pre-op Evaluation for non cardiac surgery John Steuter, MD Disclosures None A quick review from 2007!! Fliesheret al, ACC/AHA 2007 Guidelines on Perioperative Cardiovascular Evaluation and are for Noncardiac
STEMI update. Vijay Krishnamoorthy M.D. Interventional Cardiology
 STEMI update Vijay Krishnamoorthy M.D. Interventional Cardiology OVERVIEW Current Standard of Care in Management of STEMI Update in management of STEMI Pre-Cath Lab In the ED/Office/EMS. Cath Lab Post
STEMI update Vijay Krishnamoorthy M.D. Interventional Cardiology OVERVIEW Current Standard of Care in Management of STEMI Update in management of STEMI Pre-Cath Lab In the ED/Office/EMS. Cath Lab Post
Heart Failure. Dr. William Vosik. January, 2012
 Heart Failure Dr. William Vosik January, 2012 Questions for clinicians to ask Is this heart failure? What is the underlying cause? What are the associated disease processes? Which evidence-based treatment
Heart Failure Dr. William Vosik January, 2012 Questions for clinicians to ask Is this heart failure? What is the underlying cause? What are the associated disease processes? Which evidence-based treatment
Preoperative Cardiac Risk Assessment: Approach & Guidelines
 Preoperative Cardiac Risk Assessment: Approach & Guidelines By, Liam Morris, MD., FACC (02/03/18) CPG : Clinical Practice Guidelines GDMT : Guidelines Directed Medical Therapy GWC : Guideline Writing Committee
Preoperative Cardiac Risk Assessment: Approach & Guidelines By, Liam Morris, MD., FACC (02/03/18) CPG : Clinical Practice Guidelines GDMT : Guidelines Directed Medical Therapy GWC : Guideline Writing Committee
Disclosures. Inpatient Management of Non-ST Elevation Acute Coronary Syndromes. Edward McNulty MD, FACC. None
 Inpatient Management of Non-ST Elevation Acute Coronary Syndromes Edward McNulty MD, FACC Assistant Clinical Professor UCSF Director, SF VAMC Cardiac Catheterization Laboratory Disclosures None New Guidelines
Inpatient Management of Non-ST Elevation Acute Coronary Syndromes Edward McNulty MD, FACC Assistant Clinical Professor UCSF Director, SF VAMC Cardiac Catheterization Laboratory Disclosures None New Guidelines
HFpEF. April 26, 2018
 HFpEF April 26, 2018 (J Am Coll Cardiol 2017;70:2476 86) HFpEF 50% or more (40-71%) of patients with CHF have preserved LV systolic function. HFpEF is an increasingly frequent hospital discharge. Outcomes
HFpEF April 26, 2018 (J Am Coll Cardiol 2017;70:2476 86) HFpEF 50% or more (40-71%) of patients with CHF have preserved LV systolic function. HFpEF is an increasingly frequent hospital discharge. Outcomes
Impact of Nicorandil on Renal Function in Patients With Acute Heart Failure and Pre-Existing Renal Dysfunction
 Impact of Nicorandil on Renal Function in Patients With Acute Heart Failure and Pre-Existing Renal Dysfunction Masahito Shigekiyo, Kenji Harada, Ayumi Okada, Naho Terada, Hiroyoshi Yoshikawa, Akira Hirono,
Impact of Nicorandil on Renal Function in Patients With Acute Heart Failure and Pre-Existing Renal Dysfunction Masahito Shigekiyo, Kenji Harada, Ayumi Okada, Naho Terada, Hiroyoshi Yoshikawa, Akira Hirono,
Managing Quality of ACS Care in VHA The IDH Guideline Key Points and Metrics
 Managing Quality of ACS Care in VHA The IDH Guideline Key Points and Metrics Robert L. Jesse, MD, PhD National Program Director for Cardiology Veterans Health Administration Washington, DC Chief, Cardiology
Managing Quality of ACS Care in VHA The IDH Guideline Key Points and Metrics Robert L. Jesse, MD, PhD National Program Director for Cardiology Veterans Health Administration Washington, DC Chief, Cardiology