Septic shock. Babak Tamizi Far M.D Isfahan university of medical sciences
|
|
|
- Kelley Amberlynn McCoy
- 5 years ago
- Views:
Transcription


1 Septic shock Babak Tamizi Far M.D Isfahan university of medical sciences


2 Definitions Used to Describe the Condition of Septic Patients
3 Approximately 750,000 cases of severe sepsis or septic shock occur every year in the United States. Sepsis causes as many deaths as acute myocardial infarction, and septic shock and its complications are the most common causes of death in noncoronary intensive care units.
4 Septic shock may be caused by grampositive or gram-negative bacteria, fungi, and, very rarely, protozoa or rickettsiae. Increasingly common causes of septic shock are gram-positive bacteria, especially methicillin-resistant Staphylococcus aureus, vancomycinresistant enterococci, penicillin-resistant Streptococcus pneumoniae, and resistant gram-negative bacilli.
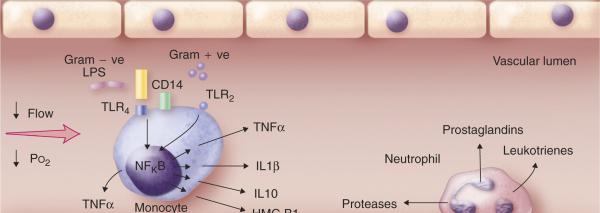
5 Pathobiology Initially, septic shock activates inflammation, thereby leading to enhanced coagulation, activated platelets, increased neutrophils and mononuclear cells, and diminished fibrinolysis
6
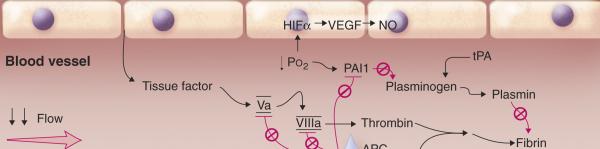
7 Procoagulant response in sepsis
8 Clinical Manifestations Cardiovascular dysfunction decreased preload (because of decreased intake, fluid losses, third spacing resulting from increased permeability, and venodilation), decreased afterload, and often decreased ventricular contractility.
9 Diagnosis Even as the diagnostic evaluation is beginning, the initial assessment of a critically ill patient must focus immediately on the airway (need for intubation), breathing (respiratory rate, respiratory distress, pulse oximetry), circulation (heart rate, blood pressure, jugular venous pressure, skin perfusion), and rapid initiation of resuscitation
10 Vital signs and the leukocyte count Arterial blood gases and lactate levels are useful immediate complementary tests


11 Algorithm for clinical and laboratory evaluation and management approach to septic shock


12
13 The major differential diagnoses of classic septic shock are other nonseptic causes of SIRS, such as acute pancreatitis,acute respiratory distress syndrome, aspiration pneumonitis, multiple trauma, and recent major surgery without infection
14 The differential diagnosis of septic shock must include the other causes of shock: hypovolemic, cardiogenic, and obstructive shock
15 shock (from internal or external fluid losses, hemorrhage) present with a suggestive history and signs of hypovolemia (low jugular venous pressure) and skin hypoperfusion (cool, clammy, cyanotic extremities).
16 Cardiogenic shock (resulting from myocardial infarction or acute on chronic congestive heart failure or occurring after cardiovascular surgery) is suggested by the history, signs of increased filling pressure (increased jugular venous pressure, crackles, S3, pulmonary edema, cardiomegaly) and skin hypoperfusion
17 Obstructive shock (from pulmonary thromboembolism, cardiac tamponade, pneumothorax) manifests similarly to cardiogenic shock.
18 Initial Antimicrobial Therapy for Severe Sepsis with No Obvious Source in Adults with Normal Renal Function


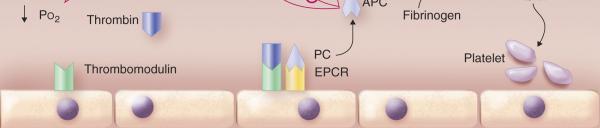
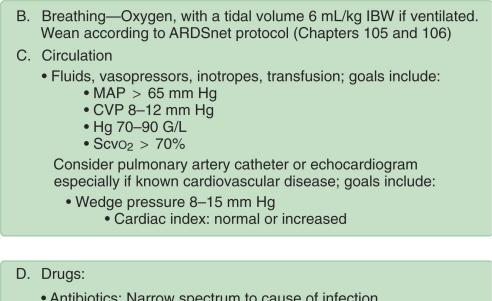
19 FIGURE Ongoing critical care support and management in septic shock
20 Respiratory Therapy require oxygen initially, and many will require mechanical ventilation. Mechanical ventilation is required in most patients who have septic shock because acute lung injury is the most common complication. Lung protective ventilation (mechanical ventilation that minimizes lung injury by using relatively low tidal volume, i.e., <6 ml/kg of predicted body weight) decreases mortality of acute lung injury and acute respiratory distress syndrome
21 Patients who require ventilation need adequate but not excessive sedation, which can worsen hemodynamic instability, prolong ventilation, and increase the risks of nosocomial pneumonia. Sedation should be titrated using objective assessment. Daily interruption of sedation decreases the duration of mechanical ventilation and intensive care. Neuromuscular blocking agents should be avoided because of the risks of prolonged neuromuscular dysfunction.
22 Circulatory Therapy Ventilator therapy is indicated for progressive hypoxemia, hypercapnia, neurologic deterioration, or respiratory muscle failure. Sustained tachypnea (respiratory rate, >30 breaths/min) is frequently a harbinger of impending respiratory collapse; mechanical ventilation is often initiated to ensure adequate oxygenation, to divert blood from the muscles of respiration, to prevent aspiration of oropharyngeal contents, and to reduce the cardiac afterload.
23 The results of recent studies favor the use of low tidal volumes (6 ml/kg of ideal body weight, or as low as 4 ml/kg if the plateau pressure exceeds 30 cmh2o). Patients undergoing mechanical ventilation require careful sedation, with daily interruptions; elevation of the head of the bed helps to prevent nosocomial pneumonia. Stress-ulcer prophylaxis with a histamine H2receptor antagonist may decrease the risk of gastrointestinal hemorrhage in ventilated patients.
24 Fluids should be used to maintain a central venous pressure 8 to 12 mm Hg; at present, no convincing data indicate that albumin is better than normal saline solution.
25 Vasopressors (e.g., norepinephrine, 1 to 50 μg/minute; epinephrine, 1 to 30 μg/minute) should be added if the mean arterial pressure is less than 65 mm Hg. Dobutamine (2.5 to 20 μg/kg/minute) is required if central venous pressure, mean arterial pressure, and hematocrit are optimized yet the central venous oxygen saturation remains less than 70%.
26 If hypotension persists despite adequate fluid resuscitation, then vasopressors such as norepinephrine (1 to 50 μg/minute) are added.
27 The overall goal is to achieve an adequate mean arterial pressure (>65 mm Hg), central venous pressure, and mixed venous oxygen saturation while other indices of adequate perfusion are monitored such as hourly urine output (>0.5 ml/kg/hour), arterial lactate levels (<2 mmol/l), mental status, and skin perfusion.
28 A reasonable approach is to use a hematocrit level of 30% as a threshold to erythrocyte transfusion for the first 6 hours and then to lower the threshold to a hemoglobin of 7 to 9 g/dl for the rest of the hospital course, except in patients with underlying cardiac disease.
29 After appropriate cultures are obtained, intravenous broad-spectrum antibiotics should be administered on an emergency basis
30 Antibiotics If a causative organism is identified (>20% of septic patients have negative cultures), then the antibiotic regimen should be narrowed to decrease the emergence of resistant organisms.
31 The duration of antibiotics should be guided by the cause of septic shock, but patients generally require 10 to 14 days of therapy.
32 Corticosteroids hydrocortisone may decrease the duration of required vasopressor support in septic shock these drugs may increase survival in septic patients who have an increase in their serum cortisol levels to 9 μg/dl or less after a 250-μg corticotropin stimulation
33 The recommended treatment is hydrocortisone (50 mg intravenously every 6 hours) plus fludrocortisone (50 μg tablet per nasogastric tube or orally daily) for 7 days
34 Activated protein C infusion (24 μg/kg/hour for 96 hours) decreases mortality, improves organ dysfunction, and decreases biomarkers of inflammation and coagulation in severe sepsis and septic shock.] Activated protein C is approved for patients who have severe sepsis and a high risk of death,
35 Activated protein C should not be used in surgical patients who have severe sepsis. By comparison, activated protein C is not beneficial in low-risk patients
36 RELEVANT RANDOMIZED CONTROLLED TRIALS IN SEVERE SEPSIS, SEPTIC SHOCK, AND ACUTE LUNG INJURY Intervention Mortality (%)[*] Control Mortality (%)[*] NN T[ ] Patient Group Intervention Control ALI/ARDS[ ][2] Low tidal volume (6 ml/kg) High tidal volume (12 ml/kg) Sepsis and septic shock[1] Early goalusual directed therapy therapy Severe sepsis and septic shock[3] Activated protein C Placebo Severe sepsis and septic shock at increased risk of death[ ][3] Activated protein C Placebo Septic shock[8] Hydrocortisone and fludrocortisone Placebo ] ] 10
37 Controversial Therapies in Septic Shock Vasopressin Deficiency and Use of Vasopressin Hyperglycemia and Intensive Insulin Therapy Renal Dysfunction and Dialysis Low-dose dopamine (2 to 4 μg/kg/minute)


38
39 Vasopressin selectively dilates renal afferent but not efferent glomerular arterioles, as well as pulmonary, cerebral, and coronary arterioles. Low-dose vasopressin infusion (0.03 to 0.04 U/minute) increases blood pressure, urine output, and creatinine clearance while dramatically decreasing the doses of norepinephrine required to maintain blood pressure in patients with septic shock.
40 Low-dose dopamine (2 to 4 μg/kg/minute) does not decrease the need for renal support, does not improve outcomes, and is not recommended
41 Deep venous thrombosis prophylaxis using low-dose heparin, which may be administered in combination with activated protein C, is recommended for patients who do not have active bleeding, coagulopathy, or a contraindication to heparin
42 Stress ulcer prophylaxis using H2-receptor antagonists decreases the risk of gastrointestinal hemorrhage. Proton pump inhibitors may also be effective, but they have not been as fully evaluated in septic shock.
43 Enteral nutrition is generally safer and more effective than total parenteral nutrition, but total parenteral nutrition is sometimes required in patients who have had abdominal sepsis, surgery, or trauma. The use of sedation, neuromuscular blocking agents, and corticosteroids should be minimized because they can exacerbate septic encephalopathy and the polyneuropathy/myopathy of sepsis. Neutropenic patients may benefit from granulocyte colony-stimulating factor
44 The risk of nosocomial infection is decreased by narrow spectrum antibiotics, early weaning from ventilation, and periodic removal and replacement of catheters
45 ANTIBIOTICS FOR PATIENTS WHO HAVE SEPTIC SHOCK Source of Sepsis Communityacquired pneumonia Initial Antibiotic Regimen Alternative Antibiotic Regimen Third-generation cephalosporin: cefotaxime 2 g IV q6h; Piperacillin-tazobactam (3.375 ceftriaxone 2 g IV q12h; ceftizoxime 2 g IV q8h) g IV q6h) PLUS PLUS Fluoroquinolone (e.g., ciprofloxacin 400 mg IV q12h; levofloxacin 750 mg IV q24h; moxifloxacin 400 mg IV q24h) OR Fluoroquinolone OR Macrolide Macrolide (e.g., azithromycin 500 mg IV q24h) Hospitalacquired pneumonia Imipenem (0.5 g IV q6h) OR Meropenem (1 g IV q8h) Fluoroquinolone (ciprofloxacin 400 mg IV q12h) PLUS Vancomycin (1.5 g IV q12h) OR Piperacillin/tazobactam (3.375 g IV q6h) PLUS Tobramycin (1.5 mg/kg q8h) PLUS Vancomycin
46 Abdominal (mixed aerobic/anae robic) Piperacillin/tazobactam (3.375 g IV q6h) OR Ampicillin (2 g IV q4h) PLUS Imipenem (0.5 g IV q6h) (or meropenem 1 g IV q8h) Metronidazole (500 mg IV q8h) PLUS Fluoroquinolone (ciprofloxacin 400 mg IV q12h) Urinary tract Fluoroquinolone (ciprofloxacin 400 mg IV q12h) Ampicillin (2 g IV q4h) PLUS Gentamicin (1.5 mg/kg IV q8h) OR Third-generation cephalosporin (cefotaxime 2 g IV q6h; OR ceftriaxone 2 g IV q12h; OR ceftizoxime 2 g IV q8h) Necrotizing fasciitis Imipenem (0.5 g IV q6h) Penicillin G (if confirmed group A streptococci)
47 Primary bacteremia (normal host) Piperacillin/tazobactam (3.375 g IV q6h) PLUS Imipenem (0.5 g IV q6h) PLUS Vancomycin (1.5 g IV q12h) Vancomycin (1.5 g IV q12h) Primary bacteremia (intravenous drug user) Cellulitis Vancomycin (1.5 g IV q12h) PLUS Piperacillin/tazobactam (3.375 g IV q6h) PLUS Fluoroquinolone (e.g., ciprofloxacin 400 mg IV q12h) Vancomycin (1.5 g IV q12h) Ciprofloxacin (400 mg IV q12h) PLUS Imipenem (0.5 g IV q6h) Clindamycin (900 mg IV q8h)
48 Febrile neutropenia Cefepime (2 g IV q8h) PLUS Piperacillin/tazobactam (3.375 g IV q6h) PLUS Vancomycin (1.5 g IV q12h) Gentamicin (1.5 mg/kg q8h) OR Imipenem (0.5 g IV q6h) PLUS Gentamicin (1.5 mg/kg q8h) Bacterial meningitis Ceftriaxone (2 g IV q12h) PLUS Gram-positive cocci: Vancomycin PLUS Ampicillin (3 g IV q6h) PLUS Ceftriaxone (2 g IV q12h) Vancomycin (1.5 g IV q12h) PLUS Gram-negative diplococci: Cefotaxime (2 g IV q4 6h) Dexamethasone (0.15 mg/kg IV q6h for 2 4 days) Gram-positive bacilli: Ampicillin (3 g IV q6h) PLUS Gentamicin Gram-negative bacilli: Ceftazidime (2 g IV q8h) PLUS Gentamicin (1.5 mg/kg IV q8h) All above PLUS Dexamethasone
49
50 Prognosis The 28-day mortality rate of septic shock is 40 to 70%. Early deaths (in the first 72 hours) are usually the result of refractory, progressive shock despite escalating life support.
51 The number of dysfunctional organs and the progression or lack of improvement of organ dysfunction are indicators of increased risk of death


52 Good luck
New Strategies in the Management of Patients with Severe Sepsis
 New Strategies in the Management of Patients with Severe Sepsis Michael Zgoda, MD, MBA President, Medical Staff Medical Director, ICU CMC-University, Charlotte, NC Factors of increases in the dx. of severe
New Strategies in the Management of Patients with Severe Sepsis Michael Zgoda, MD, MBA President, Medical Staff Medical Director, ICU CMC-University, Charlotte, NC Factors of increases in the dx. of severe
Sepsis new definitions of sepsis and septic shock and Novelities in sepsis treatment
 Sepsis new definitions of sepsis and septic shock and Novelities in sepsis treatment What is sepsis? Life-threatening organ dysfunction caused by a dysregulated host response to infection A 1991 consensus
Sepsis new definitions of sepsis and septic shock and Novelities in sepsis treatment What is sepsis? Life-threatening organ dysfunction caused by a dysregulated host response to infection A 1991 consensus
Severe β-lactam allergy. Alternative (use for mild-moderate β-lactam allergy) therapy
 therapy") Recommended Empirical Antibiotic Regimens for MICU Patients Notes: The antibiotic regimens shown are general guidelines and should not replace clinical judgment. Always assess for antibiotic allergies.
Recommended Empirical Antibiotic Regimens for MICU Patients Notes: The antibiotic regimens shown are general guidelines and should not replace clinical judgment. Always assess for antibiotic allergies.
SHOCK. Emergency pediatric PICU division Pediatric Department Medical Faculty, University of Sumatera Utara H. Adam Malik Hospital
 SHOCK Emergency pediatric PICU division Pediatric Department Medical Faculty, University of Sumatera Utara H. Adam Malik Hospital 1 Definition Shock is an acute, complex state of circulatory dysfunction
SHOCK Emergency pediatric PICU division Pediatric Department Medical Faculty, University of Sumatera Utara H. Adam Malik Hospital 1 Definition Shock is an acute, complex state of circulatory dysfunction
-Cardiogenic: shock state resulting from impairment or failure of myocardium
 Shock chapter Shock -Condition in which tissue perfusion is inadequate to deliver oxygen, nutrients to support vital organs, cellular function -Affects all body systems -Classic signs of early shock: Tachycardia,tachypnea,restlessness,anxiety,
Shock chapter Shock -Condition in which tissue perfusion is inadequate to deliver oxygen, nutrients to support vital organs, cellular function -Affects all body systems -Classic signs of early shock: Tachycardia,tachypnea,restlessness,anxiety,
Staging Sepsis for the Emergency Department: Physician
 Staging Sepsis for the Emergency Department: Physician Sepsis Continuum 1 Sepsis Continuum SIRS = 2 or more clinical criteria, resulting in Systemic Inflammatory Response Syndrome Sepsis = SIRS + proven/suspected
Staging Sepsis for the Emergency Department: Physician Sepsis Continuum 1 Sepsis Continuum SIRS = 2 or more clinical criteria, resulting in Systemic Inflammatory Response Syndrome Sepsis = SIRS + proven/suspected
SHOCK AETIOLOGY OF SHOCK (1) Inadequate circulating blood volume ) Loss of Autonomic control of the vasculature (3) Impaired cardiac function
 Inadequate circulating blood volume ) Loss of Autonomic control of the vasculature (3) Impaired cardiac function") SHOCK Shock is a condition in which the metabolic needs of the body are not met because of an inadequate cardiac output. If tissue perfusion can be restored in an expeditious fashion, cellular injury may
SHOCK Shock is a condition in which the metabolic needs of the body are not met because of an inadequate cardiac output. If tissue perfusion can be restored in an expeditious fashion, cellular injury may
Surviving Sepsis Campaign
 Surviving Sepsis Campaign Guidelines for Management of Severe Sepsis/Septic Shock An Overview By professor Ahmad Alaysh BMC-MICU 1 Surviving Sepsis A global program to Reduce mortality rates in severe
Surviving Sepsis Campaign Guidelines for Management of Severe Sepsis/Septic Shock An Overview By professor Ahmad Alaysh BMC-MICU 1 Surviving Sepsis A global program to Reduce mortality rates in severe
Surviving Sepsis Campaign. Guidelines for Management of Severe Sepsis/Septic Shock. An Overview
 Surviving Sepsis Campaign Guidelines for Management of Severe Sepsis/Septic Shock An Overview Mechanical Ventilation of Sepsis-Induced ALI/ARDS ARDSnet Mechanical Ventilation Protocol Results: Mortality
Surviving Sepsis Campaign Guidelines for Management of Severe Sepsis/Septic Shock An Overview Mechanical Ventilation of Sepsis-Induced ALI/ARDS ARDSnet Mechanical Ventilation Protocol Results: Mortality
Index. Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type. A Abdomen, and aorta, as causes of shock, point-of-care ultrasonography in assessment of, 915 917 Abdominal compartment syndrome, trauma patient
Note: Page numbers of article titles are in boldface type. A Abdomen, and aorta, as causes of shock, point-of-care ultrasonography in assessment of, 915 917 Abdominal compartment syndrome, trauma patient
Dilemmas in Septic Shock
 Dilemmas in Septic Shock William Janssen, M.D. Assistant Professor of Medicine National Jewish Health University of Colorado Denver Health Sciences Center A 62 year-old female presents to the ED with fever,
Dilemmas in Septic Shock William Janssen, M.D. Assistant Professor of Medicine National Jewish Health University of Colorado Denver Health Sciences Center A 62 year-old female presents to the ED with fever,
Printed copies of this document may not be up to date, obtain the most recent version from
 Children s Acute Transport Service Clinical Guidelines Septic Shock Document Control Information Author Claire Fraser P.Ramnarayan Author Position tanp CATS Consultant Document Owner E. Polke Document
Children s Acute Transport Service Clinical Guidelines Septic Shock Document Control Information Author Claire Fraser P.Ramnarayan Author Position tanp CATS Consultant Document Owner E. Polke Document
Septic Shock. Rontgene M. Solante, MD, FPCP,FPSMID
 Septic Shock Rontgene M. Solante, MD, FPCP,FPSMID Learning Objectives Identify situations wherein high or low BP are hemodynamically significant Recognize complications arising from BP emergencies Manage
Septic Shock Rontgene M. Solante, MD, FPCP,FPSMID Learning Objectives Identify situations wherein high or low BP are hemodynamically significant Recognize complications arising from BP emergencies Manage
Sepsis: Identification and Management in an Acute Care Setting
 Sepsis: Identification and Management in an Acute Care Setting Dr. Barbara M. Mills DNP Director Rapid Response Team/ Code Resuscitation Stony Brook University Medical Center SEPSIS LECTURE NPA 2018 OBJECTIVES
Sepsis: Identification and Management in an Acute Care Setting Dr. Barbara M. Mills DNP Director Rapid Response Team/ Code Resuscitation Stony Brook University Medical Center SEPSIS LECTURE NPA 2018 OBJECTIVES
December 3, 2015 Severe Sepsis and Septic Shock Antibiotic Guide
 Severe Sepsis and Septic Shock Antibiotic Guide Surviving Sepsis: The choice of empirical antimicrobial therapy depends on complex issues related to the patient s history, including drug intolerances,
Severe Sepsis and Septic Shock Antibiotic Guide Surviving Sepsis: The choice of empirical antimicrobial therapy depends on complex issues related to the patient s history, including drug intolerances,
4/4/2014. Of patients diagnosed with sepsis 50% will develop severe sepsis 25% will develop shock. SIRS Sepsis Severe Septic Sepsis Shock.
 A summary of pathophysiology, therapeutics, and how the pharmacy TECHNICIAN can help improve OUTCOMES Anthony Nelson 2014 Pharm.D. Candidate Tricia Aggers, Pharm.D. Affiliate Faculty, ISU College of Pharmacy
A summary of pathophysiology, therapeutics, and how the pharmacy TECHNICIAN can help improve OUTCOMES Anthony Nelson 2014 Pharm.D. Candidate Tricia Aggers, Pharm.D. Affiliate Faculty, ISU College of Pharmacy
9/25/2017. Nothing to disclose
 Nothing to disclose Jessie O Neal, PharmD, BCCCP Critical Care Clinical Pharmacist University of New Mexico Hospital New Mexico Society of Health-System Pharmacists 2017 Balloon Fiesta Symposium Explain
Nothing to disclose Jessie O Neal, PharmD, BCCCP Critical Care Clinical Pharmacist University of New Mexico Hospital New Mexico Society of Health-System Pharmacists 2017 Balloon Fiesta Symposium Explain
Nothing to disclose 9/25/2017
 Jessie O Neal, PharmD, BCCCP Critical Care Clinical Pharmacist University of New Mexico Hospital New Mexico Society of Health-System Pharmacists 2017 Balloon Fiesta Symposium Nothing to disclose 1 Explain
Jessie O Neal, PharmD, BCCCP Critical Care Clinical Pharmacist University of New Mexico Hospital New Mexico Society of Health-System Pharmacists 2017 Balloon Fiesta Symposium Nothing to disclose 1 Explain
Sepsis is an important issue. Clinician s decision-making capability. Guideline recommendations
 Surviving Sepsis Campaign: International Guidelines for Management of Severe Sepsis and Septic Shock: 2012 Clinicians decision-making capability Guideline recommendations Sepsis is an important issue 8.7%
Surviving Sepsis Campaign: International Guidelines for Management of Severe Sepsis and Septic Shock: 2012 Clinicians decision-making capability Guideline recommendations Sepsis is an important issue 8.7%
Case Scenario 3: Shock and Sepsis
 Name: Molly Boyle 1. Define the term shock (Lewis textbook): Shock is a syndrome characterized by decreased perfusion and impaired metabolism. Shock can have a number of causes that result in damage to
Name: Molly Boyle 1. Define the term shock (Lewis textbook): Shock is a syndrome characterized by decreased perfusion and impaired metabolism. Shock can have a number of causes that result in damage to
Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock: 2016
 Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock: 2016 Mitchell M. Levy MD, MCCM Professor of Medicine Chief, Division of Pulmonary, Sleep, and Critical Care
Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock: 2016 Mitchell M. Levy MD, MCCM Professor of Medicine Chief, Division of Pulmonary, Sleep, and Critical Care
Fluids in Sepsis: How much and what type? John Fowler, MD, FACEP Kent Hospital, İzmir Eisenhower Medical Center, USA American Hospital Dubai, UAE
 Fluids in Sepsis: How much and what type? John Fowler, MD, FACEP Kent Hospital, İzmir Eisenhower Medical Center, USA American Hospital Dubai, UAE In critically ill patients: too little fluid Low preload,
Fluids in Sepsis: How much and what type? John Fowler, MD, FACEP Kent Hospital, İzmir Eisenhower Medical Center, USA American Hospital Dubai, UAE In critically ill patients: too little fluid Low preload,
Initial Resuscitation of Sepsis & Septic Shock
 Initial Resuscitation of Sepsis & Septic Shock Dr. Fatema Ahmed MD (Critical Care Medicine) FCPS (Medicine) Associate professor Dept. of Critical Care Medicine BIRDEM General Hospital Is Sepsis a known
Initial Resuscitation of Sepsis & Septic Shock Dr. Fatema Ahmed MD (Critical Care Medicine) FCPS (Medicine) Associate professor Dept. of Critical Care Medicine BIRDEM General Hospital Is Sepsis a known
Online Supplement for:
 Online Supplement for: INFLUENCE OF COMBINED INTRAVENOUS AND TOPICAL ANTIBIOTIC PROPHYLAXIS ON THE INCIDENCE OF INFECTIONS, ORGAN DYSFUNCTIONS, AND MORTALITY IN CRITICALLY ILL SURGICAL PATIENTS A PROSPECTIVE,
Online Supplement for: INFLUENCE OF COMBINED INTRAVENOUS AND TOPICAL ANTIBIOTIC PROPHYLAXIS ON THE INCIDENCE OF INFECTIONS, ORGAN DYSFUNCTIONS, AND MORTALITY IN CRITICALLY ILL SURGICAL PATIENTS A PROSPECTIVE,
Sepsis overview. Dr. Tsang Hin Hung MBBS FHKCP FRCP
 Sepsis overview Dr. Tsang Hin Hung MBBS FHKCP FRCP Epidemiology Sepsis, severe sepsis, septic shock Pathophysiology of sepsis Recent researches and advances From bench to bedside Sepsis bundle Severe sepsis
Sepsis overview Dr. Tsang Hin Hung MBBS FHKCP FRCP Epidemiology Sepsis, severe sepsis, septic shock Pathophysiology of sepsis Recent researches and advances From bench to bedside Sepsis bundle Severe sepsis
Printed copies of this document may not be up to date, obtain the most recent version from
 Children s Acute Transport Service Clinical Guidelines Septic Shock Document Control Information Author Shruti Dholakia L Chigaru Author Position Fellow CATS Consultant Document Owner E. Polke Document
Children s Acute Transport Service Clinical Guidelines Septic Shock Document Control Information Author Shruti Dholakia L Chigaru Author Position Fellow CATS Consultant Document Owner E. Polke Document
6-horas 24 horas Coleta de lactato Hemoculturas. Corticosteróides. Controle glicêmico. Fluidos/vasopressores. Otimização de SvO 2
 Novas diretrizes da Surviving Sepsis Campaign 2012 o que foi atualizado? Os pacotes da sepse 6-horas 24 horas Coleta de lactato Hemoculturas Corticosteróides Antibióticos Proteína C ativdada Fluidos/vasopressores
Novas diretrizes da Surviving Sepsis Campaign 2012 o que foi atualizado? Os pacotes da sepse 6-horas 24 horas Coleta de lactato Hemoculturas Corticosteróides Antibióticos Proteína C ativdada Fluidos/vasopressores
Supplementary Appendix
 Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: Sprung CL, Annane D, Keh D, et al. Hydrocortisone therapy for
Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: Sprung CL, Annane D, Keh D, et al. Hydrocortisone therapy for
Critical Care Treatment Guidelines
 Critical Care Treatment Guidelines West Virginia Office of Emergency Medical Services CCT Guidelines CCT Guidelines TABLE OF CONTENTS Preface Acknowledgments Using the Guidelines INITIAL TREATMENT / UNIVERSAL
Critical Care Treatment Guidelines West Virginia Office of Emergency Medical Services CCT Guidelines CCT Guidelines TABLE OF CONTENTS Preface Acknowledgments Using the Guidelines INITIAL TREATMENT / UNIVERSAL
The Pharmacology of Hypotension: Vasopressor Choices for HIE patients. Keliana O Mara, PharmD August 4, 2018
 The Pharmacology of Hypotension: Vasopressor Choices for HIE patients Keliana O Mara, PharmD August 4, 2018 Objectives Review the pathophysiology of hypotension in neonates Discuss the role of vasopressors
The Pharmacology of Hypotension: Vasopressor Choices for HIE patients Keliana O Mara, PharmD August 4, 2018 Objectives Review the pathophysiology of hypotension in neonates Discuss the role of vasopressors
Objectives. Management of Septic Shock. Definitions Progression of sepsis. Epidemiology of severe sepsis. Major goals of therapy
 Objectives Management of Septic Shock Review of the Evidence and Implementation of Pediatric Guidelines at Christus Santa Rosa Manish Desai, M.D. PL 5 2 nd year Pediatric Critical Care Fellow Review of
Objectives Management of Septic Shock Review of the Evidence and Implementation of Pediatric Guidelines at Christus Santa Rosa Manish Desai, M.D. PL 5 2 nd year Pediatric Critical Care Fellow Review of
Useful diagnostic measures: chest x ray to check pulmonary edema, ECG and ECHO to detect cardiac abnormalities (1).
.") Cardiogenic shock Etiology The most common cause of cardiogenic shock is LV dysfunction and necrosis as a result of acute myocardial infarction (AMI) (1). Acute valvular insufficiency or stenosis prevents
Cardiogenic shock Etiology The most common cause of cardiogenic shock is LV dysfunction and necrosis as a result of acute myocardial infarction (AMI) (1). Acute valvular insufficiency or stenosis prevents
SEPSIS: IT ALL BEGINS WITH INFECTION. Theresa Posani, MS, RN, ACNS-BC, CCRN M/S CNS/Sepsis Coordinator Texas Health Harris Methodist Ft.
 SEPSIS: IT ALL BEGINS WITH INFECTION Theresa Posani, MS, RN, ACNS-BC, CCRN M/S CNS/Sepsis Coordinator Texas Health Harris Methodist Ft. Worth 1 2 3 OBJECTIVES Review the new Sepsis 3 definitions of sepsis
SEPSIS: IT ALL BEGINS WITH INFECTION Theresa Posani, MS, RN, ACNS-BC, CCRN M/S CNS/Sepsis Coordinator Texas Health Harris Methodist Ft. Worth 1 2 3 OBJECTIVES Review the new Sepsis 3 definitions of sepsis
Guidebook for ED and Inpatient Sepsis Order Set Initiatives 2018
 Background The leadership of the Surviving Sepsis Campaign (SSC) believes, since its inception, that both the SSC Guidelines and the SSC performance improvement indicators (1) will evolve as new evidence
Background The leadership of the Surviving Sepsis Campaign (SSC) believes, since its inception, that both the SSC Guidelines and the SSC performance improvement indicators (1) will evolve as new evidence
DESIGNER RESUSCITATION: TITRATING TO TISSUE NEEDS
 DESIGNER RESUSCITATION: TITRATING TO TISSUE NEEDS R. Phillip Dellinger MD, MSc, MCCM Professor and Chair of Medicine Cooper Medical School of Rowan University Chief of Medicine Cooper University Hospital
DESIGNER RESUSCITATION: TITRATING TO TISSUE NEEDS R. Phillip Dellinger MD, MSc, MCCM Professor and Chair of Medicine Cooper Medical School of Rowan University Chief of Medicine Cooper University Hospital
Sepsis Management: Past, Present, and Future
 Sepsis Management: Past, Present, and Future Benjamin Ferrell, MD Tennessee ACP Meeting October 28, 2017 Learning Objectives Identify the most updated definition and clinical criteria for sepsis Describe
Sepsis Management: Past, Present, and Future Benjamin Ferrell, MD Tennessee ACP Meeting October 28, 2017 Learning Objectives Identify the most updated definition and clinical criteria for sepsis Describe
Evidence-Based. Management of Severe Sepsis. What is the BP Target?
 Evidence-Based Management of Severe Sepsis Michael A. Gropper, MD, PhD Professor and Vice Chair of Anesthesia Director, Critical Care Medicine Chair, Quality Improvment University of California San Francisco
Evidence-Based Management of Severe Sepsis Michael A. Gropper, MD, PhD Professor and Vice Chair of Anesthesia Director, Critical Care Medicine Chair, Quality Improvment University of California San Francisco
Sepsis and Shock States
 Sepsis and Shock States Presented By: Cynthia Webner BSN, RN, CCRN, CMC www.cardionursing.com CNEA 2009 1 INFECTION Inflammatory response to microorganisms, or Invasion of normally sterile tissues SYSTEMIC
Sepsis and Shock States Presented By: Cynthia Webner BSN, RN, CCRN, CMC www.cardionursing.com CNEA 2009 1 INFECTION Inflammatory response to microorganisms, or Invasion of normally sterile tissues SYSTEMIC
Tissue oxygenation is dependent upon, cardiac output, hemoglobin saturation and peripheral micro circulation.
 Editorial Shock occurs when there is circulatory failure that results in inadequate cellular oxygen, that is arterial blood flow is inadequate to meet tissue metabolic needs. Tissue oxygenation is dependent
Editorial Shock occurs when there is circulatory failure that results in inadequate cellular oxygen, that is arterial blood flow is inadequate to meet tissue metabolic needs. Tissue oxygenation is dependent
Ralph Palumbo, MD, FCCP
 Ralph Palumbo, MD, FCCP Septic shock is the leading cause of mortality in patients admitted to the ICU In the United States alone there are over 750,000 cases of severe sepsis and septic shock annually
Ralph Palumbo, MD, FCCP Septic shock is the leading cause of mortality in patients admitted to the ICU In the United States alone there are over 750,000 cases of severe sepsis and septic shock annually
ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) Rv
 Rv") ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) Rv.8.18.18 ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) SUDDEN PROGRESSIVE FORM OF ACUTE RESPIRATORY FAILURE ALVEOLAR CAPILLARY MEMBRANE BECOMES DAMAGED AND MORE
ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) Rv.8.18.18 ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) SUDDEN PROGRESSIVE FORM OF ACUTE RESPIRATORY FAILURE ALVEOLAR CAPILLARY MEMBRANE BECOMES DAMAGED AND MORE
SHOCK Susanna Hilda Hutajulu, MD, PhD
 SHOCK Susanna Hilda Hutajulu, MD, PhD Div Hematology and Medical Oncology Department of Internal Medicine Universitas Gadjah Mada Yogyakarta Outline Definition Epidemiology Physiology Classes of Shock
SHOCK Susanna Hilda Hutajulu, MD, PhD Div Hematology and Medical Oncology Department of Internal Medicine Universitas Gadjah Mada Yogyakarta Outline Definition Epidemiology Physiology Classes of Shock
Effectively Managing Sepsis Denials
 Effectively Managing Sepsis Denials Krysten Brooks, RN, BSN, MBA Senior Inpatient Consultant 3M Health Information Systems This is the Full Title of a Session Atlanta, GA 1 Learning Objectives At the completion
Effectively Managing Sepsis Denials Krysten Brooks, RN, BSN, MBA Senior Inpatient Consultant 3M Health Information Systems This is the Full Title of a Session Atlanta, GA 1 Learning Objectives At the completion
Cardiovascular Management of Septic Shock
 Cardiovascular Management of Septic Shock R. Phillip Dellinger, MD Professor of Medicine Robert Wood Johnson Medical School/UMDNJ Director, Critical Care Medicine and Med/Surg ICU Cooper University Hospital
Cardiovascular Management of Septic Shock R. Phillip Dellinger, MD Professor of Medicine Robert Wood Johnson Medical School/UMDNJ Director, Critical Care Medicine and Med/Surg ICU Cooper University Hospital
Sepsis Combine experience and Evidence. Eran Segal, MD Director General ICU, Sheba Medical Center, Israel
 Sepsis Combine experience and Evidence Eran Segal, MD Director General ICU, Sheba Medical Center, Israel The Science of Sepsis A complex and diverse clinical entity Outcome is affected by: Infecting organism
Sepsis Combine experience and Evidence Eran Segal, MD Director General ICU, Sheba Medical Center, Israel The Science of Sepsis A complex and diverse clinical entity Outcome is affected by: Infecting organism
CORTICOSTEROID USE IN SEPTIC SHOCK THE ONGOING DEBATE DIEM HO, PHARMD PGY1 PHARMACY RESIDENT VALLEY BAPTIST MEDICAL CENTER BROWNSVILLE
 CORTICOSTEROID USE IN SEPTIC SHOCK THE ONGOING DEBATE DIEM HO, PHARMD PGY1 PHARMACY RESIDENT VALLEY BAPTIST MEDICAL CENTER BROWNSVILLE 1 ABBREVIATIONS ACCP = American College of Chest Physicians ARF =
CORTICOSTEROID USE IN SEPTIC SHOCK THE ONGOING DEBATE DIEM HO, PHARMD PGY1 PHARMACY RESIDENT VALLEY BAPTIST MEDICAL CENTER BROWNSVILLE 1 ABBREVIATIONS ACCP = American College of Chest Physicians ARF =
Unrestricted. Dr ppooransari fellowship of perenatalogy
 Unrestricted Dr ppooransari fellowship of perenatalogy Assessment of severity of hemorrhage Significant drops in blood pressure are generally not manifested until substantial bleeding has occurred, and
Unrestricted Dr ppooransari fellowship of perenatalogy Assessment of severity of hemorrhage Significant drops in blood pressure are generally not manifested until substantial bleeding has occurred, and
Surviving Sepsis Campaign Guidelines 2012 & Update for David E. Tannehill, DO Critical Care Medicine Mercy Hospital St.
 Surviving Sepsis Campaign Guidelines 2012 & Update for 2015 David E. Tannehill, DO Critical Care Medicine Mercy Hospital St. Louis Be appropriately aggressive the longer one delays aggressive metabolic
Surviving Sepsis Campaign Guidelines 2012 & Update for 2015 David E. Tannehill, DO Critical Care Medicine Mercy Hospital St. Louis Be appropriately aggressive the longer one delays aggressive metabolic
INTENSIVE CARE MEDICINE CPD EVENING. Dr Alastair Morgan Wednesday 13 th September 2017
 INTENSIVE CARE MEDICINE CPD EVENING Dr Alastair Morgan Wednesday 13 th September 2017 WHAT IS NEW IN ICU? (RELEVANT TO ANAESTHETISTS) Not much! SURVIVING SEPSIS How many deaths in England were thought
INTENSIVE CARE MEDICINE CPD EVENING Dr Alastair Morgan Wednesday 13 th September 2017 WHAT IS NEW IN ICU? (RELEVANT TO ANAESTHETISTS) Not much! SURVIVING SEPSIS How many deaths in England were thought
TERMINOLOGY SIRS 10/30/2014 SURVIVING SEPSIS: FROM THE OFFICE TO THE ICU
 Lisa Johnson DrNP, CRNP, ACNP BC Director, AG ACNP Program, DeSales University ACNP with Eastern Pennsylvania Infectious Disease Associates SURVIVING SEPSIS: FROM THE OFFICE TO THE ICU TERMINOLOGY Infection
Lisa Johnson DrNP, CRNP, ACNP BC Director, AG ACNP Program, DeSales University ACNP with Eastern Pennsylvania Infectious Disease Associates SURVIVING SEPSIS: FROM THE OFFICE TO THE ICU TERMINOLOGY Infection
EFFECT OF EARLY VASOPRESSIN VS NOREPINEPHRINE ON KIDNEY FAILURE IN PATIENTS WITH SEPTIC SHOCK. Alexandria Rydz
 EFFECT OF EARLY VASOPRESSIN VS NOREPINEPHRINE ON KIDNEY FAILURE IN PATIENTS WITH SEPTIC SHOCK Alexandria Rydz BACKGROUND- SEPSIS Sepsis is defined as life-threatening organ dysfunction caused by a dysregulated
EFFECT OF EARLY VASOPRESSIN VS NOREPINEPHRINE ON KIDNEY FAILURE IN PATIENTS WITH SEPTIC SHOCK Alexandria Rydz BACKGROUND- SEPSIS Sepsis is defined as life-threatening organ dysfunction caused by a dysregulated
12/1/2009. Chapter 19: Hemorrhage. Hemorrhage and Shock Occurs when there is a disruption or leak in the vascular system Internal hemorrhage
 Chapter 19: Hemorrhage Hemorrhage and Shock Occurs when there is a disruption or leak in the vascular system External hemorrhage Internal hemorrhage Associated with higher morbidity and mortality than
Chapter 19: Hemorrhage Hemorrhage and Shock Occurs when there is a disruption or leak in the vascular system External hemorrhage Internal hemorrhage Associated with higher morbidity and mortality than
Physiological Response to Hypovolemic Shock Dr Khwaja Mohammed Amir MD Assistant Professor(Physiology) Objectives At the end of the session the
 Objectives At the end of the session the") Physiological Response to Hypovolemic Shock Dr Khwaja Mohammed Amir MD Assistant Professor(Physiology) Objectives At the end of the session the students should be able to: List causes of shock including
Physiological Response to Hypovolemic Shock Dr Khwaja Mohammed Amir MD Assistant Professor(Physiology) Objectives At the end of the session the students should be able to: List causes of shock including
Pediatric emergencies (SHOCK & COMA) Dr Mubarak Abdelrahman Assistant Professor Jazan University
 Dr Mubarak Abdelrahman Assistant Professor Jazan University") Pediatric emergencies (SHOCK & COMA) Dr Mubarak Abdelrahman Assistant Professor Jazan University SHOCK Definition: Shock is a syndrome = inability to provide sufficient oxygenated blood to tissues. Oxygen
Pediatric emergencies (SHOCK & COMA) Dr Mubarak Abdelrahman Assistant Professor Jazan University SHOCK Definition: Shock is a syndrome = inability to provide sufficient oxygenated blood to tissues. Oxygen
Acute Liver Failure: Supporting Other Organs
 Acute Liver Failure: Supporting Other Organs Michael A. Gropper, MD, PhD Professor of Anesthesia and Physiology Director, Critical Care Medicine University of California San Francisco Acute Liver Failure
Acute Liver Failure: Supporting Other Organs Michael A. Gropper, MD, PhD Professor of Anesthesia and Physiology Director, Critical Care Medicine University of California San Francisco Acute Liver Failure
PHYSIOLOGY AND MANAGEMENT OF THE SEPTIC PATIENT
 PHYSIOLOGY AND MANAGEMENT OF THE SEPTIC PATIENT Melanie Sanchez, RN, MSNE, OCN, CCRN Clinical Nurse III City of Hope National Medical Center HOW THE EXPERTS TREAT HEMATOLOGIC MALIGNANCIES LAS VEGAS, NV
PHYSIOLOGY AND MANAGEMENT OF THE SEPTIC PATIENT Melanie Sanchez, RN, MSNE, OCN, CCRN Clinical Nurse III City of Hope National Medical Center HOW THE EXPERTS TREAT HEMATOLOGIC MALIGNANCIES LAS VEGAS, NV
Patient Safety Safe Table Webcast: Sepsis (Part III and IV) December 17, 2014
 December 17, 2014") Patient Safety Safe Table Webcast: Sepsis (Part III and IV) December 17, 2014 Presenters Mark Blaney, RN Regional Nurse Educator CHI Franciscan Health Karen Lautermilch Director, Quality & Performance
Patient Safety Safe Table Webcast: Sepsis (Part III and IV) December 17, 2014 Presenters Mark Blaney, RN Regional Nurse Educator CHI Franciscan Health Karen Lautermilch Director, Quality & Performance
Frank Sebat, MD - June 29, 2006
 Types of Shock Hypovolemic Shock Low blood volume decreasing cardiac output. AN INTEGRATED SYSTEM OF CARE FOR PATIENTS AT RISK SHOCK TEAM and RAPID RESPONSE TEAM Septic or Distributive Shock Decrease in
Types of Shock Hypovolemic Shock Low blood volume decreasing cardiac output. AN INTEGRATED SYSTEM OF CARE FOR PATIENTS AT RISK SHOCK TEAM and RAPID RESPONSE TEAM Septic or Distributive Shock Decrease in
Surviving Sepsis. Brian Woodcock MBChB MRCP FRCA FCCM
 1 Surviving Sepsis Brian Woodcock MBChB MRCP FRCA FCCM 2 Disclosures No conflicts of interest 3 Sepsis Principles of management of septic shock in the operating room "Surviving Sepsis" guidelines 4 Add-on
1 Surviving Sepsis Brian Woodcock MBChB MRCP FRCA FCCM 2 Disclosures No conflicts of interest 3 Sepsis Principles of management of septic shock in the operating room "Surviving Sepsis" guidelines 4 Add-on
PREVENTION AND TREATMENT OF BACTERIAL INFECTIONS IN CIRRHOSIS
 PREVENTION AND TREATMENT OF BACTERIAL INFECTIONS IN CIRRHOSIS Dr. J. Fernández. Head of the Liver Unit Hospital Clinic Barcelona, Spain AEEH Postgraduate Course, Madrid, February 15 2017 Prevalence of
PREVENTION AND TREATMENT OF BACTERIAL INFECTIONS IN CIRRHOSIS Dr. J. Fernández. Head of the Liver Unit Hospital Clinic Barcelona, Spain AEEH Postgraduate Course, Madrid, February 15 2017 Prevalence of
Sepsis Bundle Project (SEP) Kathy Wonderly RN, MSEd, CPHQ Consultant Developed: April 2015 Most recent Revision: December 2018
 Kathy Wonderly RN, MSEd, CPHQ Consultant Developed: April 2015 Most recent Revision: December 2018") Sepsis Bundle Project (SEP) Kathy Wonderly RN, MSEd, CPHQ Consultant Developed: April 2015 Most recent Revision: December 2018 Objectives 1. To identify the symptom of severe sepsis and septic shock syndrome.
Sepsis Bundle Project (SEP) Kathy Wonderly RN, MSEd, CPHQ Consultant Developed: April 2015 Most recent Revision: December 2018 Objectives 1. To identify the symptom of severe sepsis and septic shock syndrome.
Case year old female nursing home resident with a hx CAD, PUD, recent hip fracture Transferred to ED with decreased mental status BP in ED 80/50
 Case 1 65 year old female nursing home resident with a hx CAD, PUD, recent hip fracture Transferred to ED with decreased mental status BP in ED 80/50 Case 1 65 year old female nursing home resident with
Case 1 65 year old female nursing home resident with a hx CAD, PUD, recent hip fracture Transferred to ED with decreased mental status BP in ED 80/50 Case 1 65 year old female nursing home resident with
Septic Shock. Col. Danabhand Phiboonbanakit, M.D., Ph.D, Division of Infectious Diseases, Department of Medicine
 Septic Shock Col. Danabhand Phiboonbanakit, M.D., Ph.D, Division of Infectious Diseases, Department of Medicine Phramongkutklao Hospital Sepsis = Infection + SIRS Bone RC et al. chest 1992; 101: 1644-55
Septic Shock Col. Danabhand Phiboonbanakit, M.D., Ph.D, Division of Infectious Diseases, Department of Medicine Phramongkutklao Hospital Sepsis = Infection + SIRS Bone RC et al. chest 1992; 101: 1644-55
SHOCK. Pathophysiology
 SHOCK Dr. Ahmed Saleem FICMS TUCOM / 3rd Year / 2015 Shock is the most common and therefore the most important cause of death of surgical patients. Death may occur rapidly due to a profound state of shock,
SHOCK Dr. Ahmed Saleem FICMS TUCOM / 3rd Year / 2015 Shock is the most common and therefore the most important cause of death of surgical patients. Death may occur rapidly due to a profound state of shock,
The Septic Patient. Dr Arunraj Navaratnarajah. Renal SpR Imperial College NHS Healthcare Trust
 The Septic Patient Dr Arunraj Navaratnarajah Renal SpR Imperial College NHS Healthcare Trust Objectives of this session Define SIRS / sepsis / severe sepsis / septic shock Early recognition of Sepsis The
The Septic Patient Dr Arunraj Navaratnarajah Renal SpR Imperial College NHS Healthcare Trust Objectives of this session Define SIRS / sepsis / severe sepsis / septic shock Early recognition of Sepsis The
Case I: Shock. A) What additional history would you like from the nursing home staff, patient s chart, and ambulance team?
 What additional history would you like from the nursing home staff, patient s chart, and ambulance team?") Case I: Shock It is your first night of call during your subinternship month, and you are asked by your resident to evaluate a patient in the emergency room. The patient is a 85yo female with a history
Case I: Shock It is your first night of call during your subinternship month, and you are asked by your resident to evaluate a patient in the emergency room. The patient is a 85yo female with a history
The syndrome formerly known as. Severe Sepsis. James Rooks MD. Coordinator of critical care education OU College of Medicine, Tulsa
 The syndrome formerly known as Severe Sepsis James Rooks MD Coordinator of critical care education OU College of Medicine, Tulsa Disclosures I have no actual or practical conflicts of interest in relation
The syndrome formerly known as Severe Sepsis James Rooks MD Coordinator of critical care education OU College of Medicine, Tulsa Disclosures I have no actual or practical conflicts of interest in relation
Titrating Critical Care Medications
 Titrating Critical Care Medications Chad Johnson, MSN (NED), RN, CNCC(C), CNS-cc Clinical Nurse Specialist: Critical Care and Neurosurgical Services E-mail: johnsoc@tbh.net Copyright 2017 1 Learning Objectives
Titrating Critical Care Medications Chad Johnson, MSN (NED), RN, CNCC(C), CNS-cc Clinical Nurse Specialist: Critical Care and Neurosurgical Services E-mail: johnsoc@tbh.net Copyright 2017 1 Learning Objectives
Sepsis. From EMS to ER to ICU. What we need to be doing
 Sepsis From EMS to ER to ICU What we need to be doing NEHAL BHATT, MD ATHENS PULMONARY, CRITICAL CARE AND SLEEP Objectives 1. Define the changes to the definition of Sepsis 2. Describe the assessment,
Sepsis From EMS to ER to ICU What we need to be doing NEHAL BHATT, MD ATHENS PULMONARY, CRITICAL CARE AND SLEEP Objectives 1. Define the changes to the definition of Sepsis 2. Describe the assessment,
DEFINITION. Imbalance in supply/demand for O2 and nutrients
 NURS 452 SHOCK Outcome Relate the pathophysiology to the clinical manifestations of the different types of shock: cardiogenic, hypovolemic, distributive, and obstructive Compare the collaborative care,
NURS 452 SHOCK Outcome Relate the pathophysiology to the clinical manifestations of the different types of shock: cardiogenic, hypovolemic, distributive, and obstructive Compare the collaborative care,
The Ever Changing World of Sepsis Management. Laura Evans MD MSc Medical Director of Critical Care Bellevue Hospital
 The Ever Changing World of Sepsis Management Laura Evans MD MSc Medical Director of Critical Care Bellevue Hospital COI Disclosures No financial interests to disclose Learning Objectives Review the evolution
The Ever Changing World of Sepsis Management Laura Evans MD MSc Medical Director of Critical Care Bellevue Hospital COI Disclosures No financial interests to disclose Learning Objectives Review the evolution
CEDR 2018 QCDR Measures for CMS 2018 MIPS Performance Year Reporting
 ACEP19 Emergency Department Utilization of CT for Minor Blunt Head Trauma for Aged 18 Years and Older Percentage of visits for aged 18 years and older who presented with a minor blunt head trauma who had
ACEP19 Emergency Department Utilization of CT for Minor Blunt Head Trauma for Aged 18 Years and Older Percentage of visits for aged 18 years and older who presented with a minor blunt head trauma who had
Organ Donor Management Recommended Guidelines ADULT CARDIAC DEATH (DCD)
") Date: Time: = Always applicable = Check if applicable ADMISSION INSTRUCTIONS Move to Comfort Care Note in chart. Contact initiated with BC Transplant Consent for Organ Donation obtained Code Status: Full
Date: Time: = Always applicable = Check if applicable ADMISSION INSTRUCTIONS Move to Comfort Care Note in chart. Contact initiated with BC Transplant Consent for Organ Donation obtained Code Status: Full
Organ Donor Management Recommended Guidelines ADULT Brain Death (NDD)
") Date: Time: = Always applicable = Check if applicable ADMISSION INSTRUCTIONS Neurological Determination of Death (NDD) has been performed by at least 2 licensed physicians Contact initiated with BC Transplant
Date: Time: = Always applicable = Check if applicable ADMISSION INSTRUCTIONS Neurological Determination of Death (NDD) has been performed by at least 2 licensed physicians Contact initiated with BC Transplant
Sepsis Awareness and Education
 Sepsis Awareness and Education Meets the updated New York State Department of Health (NYSDOH) requirements for Infection Control and Barrier Precautions coursework Element VII: Sepsis Awareness and Education
Sepsis Awareness and Education Meets the updated New York State Department of Health (NYSDOH) requirements for Infection Control and Barrier Precautions coursework Element VII: Sepsis Awareness and Education
Management of Severe Sepsis:
 Management of Severe Sepsis: Update from the Surviving Sepsis Campaign Barbara Birriel, MSN, ACNP-BC, FCCM The Pennsylvania State University NONE Disclosures Review evidence-based international sepsis
Management of Severe Sepsis: Update from the Surviving Sepsis Campaign Barbara Birriel, MSN, ACNP-BC, FCCM The Pennsylvania State University NONE Disclosures Review evidence-based international sepsis
PALS Pulseless Arrest Algorithm.
 PALS Pulseless Arrest Algorithm. Kleinman M E et al. Circulation 2010;122:S876-S908 PALS Bradycardia Algorithm. Kleinman M E et al. Circulation 2010;122:S876-S908 PALS Tachycardia Algorithm. Kleinman M
PALS Pulseless Arrest Algorithm. Kleinman M E et al. Circulation 2010;122:S876-S908 PALS Bradycardia Algorithm. Kleinman M E et al. Circulation 2010;122:S876-S908 PALS Tachycardia Algorithm. Kleinman M
4/5/2018. Update on Sepsis NIKHIL JAGAN PULMONARY AND CRITICAL CARE CREIGHTON UNIVERSITY. I have no financial disclosures
 Update on Sepsis NIKHIL JAGAN PULMONARY AND CRITICAL CARE CREIGHTON UNIVERSITY I have no financial disclosures 1 Objectives Why do we care about sepsis Understanding the core measures by Centers for Medicare
Update on Sepsis NIKHIL JAGAN PULMONARY AND CRITICAL CARE CREIGHTON UNIVERSITY I have no financial disclosures 1 Objectives Why do we care about sepsis Understanding the core measures by Centers for Medicare
Supplementary appendix
 Supplementary appendix This appendix formed part of the original submission and has been peer reviewed. We post it as supplied by the authors. Supplement to: Blum CA, Nigro N, Briel M, et al. Adjunct prednisone
Supplementary appendix This appendix formed part of the original submission and has been peer reviewed. We post it as supplied by the authors. Supplement to: Blum CA, Nigro N, Briel M, et al. Adjunct prednisone
Morbid Obesity: Multi system Considerations for Acute Care
 Morbid Obesity: Multi system Considerations for Acute Care BRENDA ENGLER, MSN, ACNP BC, CCRN GEISINGER MEDICAL CENTER Disclosures None 1 Obesity Statistics 30 % of the adult population of Pennsylvania
Morbid Obesity: Multi system Considerations for Acute Care BRENDA ENGLER, MSN, ACNP BC, CCRN GEISINGER MEDICAL CENTER Disclosures None 1 Obesity Statistics 30 % of the adult population of Pennsylvania
5/1/2015 SEPSIS SURVIVING SEPSIS CAMPAIGN HOW TO APPROACH THE POSSIBLE SEPTIC CHILD 2015 INFECTION CAN BE CONFIRMED BY:
 SURVIVING SEPSIS CAMPAIGN HOW TO APPROACH THE POSSIBLE SEPTIC CHILD 2015 Omer Nasiroglu MD Baptist Children s Hospital Pediatric Emergency Department SEPSIS IS A SYSTEMIC INFLAMMATORY RESPONSE SYNDROME
SURVIVING SEPSIS CAMPAIGN HOW TO APPROACH THE POSSIBLE SEPTIC CHILD 2015 Omer Nasiroglu MD Baptist Children s Hospital Pediatric Emergency Department SEPSIS IS A SYSTEMIC INFLAMMATORY RESPONSE SYNDROME
How Normal Body Processes Are Altered By Disease and Injury
 1 Chapter 4, General Principles of Pathophysiology Part 1 How Normal Body Processes Are Altered By Disease and Injury 2 How Cells Respond to Change and Injury 3 Pathology & Pathophysiology : the study
1 Chapter 4, General Principles of Pathophysiology Part 1 How Normal Body Processes Are Altered By Disease and Injury 2 How Cells Respond to Change and Injury 3 Pathology & Pathophysiology : the study
Surviving Sepsis: A CRASH Course. Justin Jones, PharmD Sanford Medical Center, Fargo Staff Education 2015
 Surviving Sepsis: A CRASH Course Justin Jones, PharmD Sanford Medical Center, Fargo Staff Education 2015 Disclosures No financial conflicts of interest Abbreviations ULN Upper limit of normal SVCO2 Central
Surviving Sepsis: A CRASH Course Justin Jones, PharmD Sanford Medical Center, Fargo Staff Education 2015 Disclosures No financial conflicts of interest Abbreviations ULN Upper limit of normal SVCO2 Central
Acute Respiratory Distress Syndrome (ARDS) An Update
 An Update") Acute Respiratory Distress Syndrome (ARDS) An Update Prof. A.S.M. Areef Ahsan FCPS(Medicine) MD(Critical Care Medicine) MD ( Chest) Head, Dept. of Critical Care Medicine BIRDEM General Hospital INTRODUCTION
Acute Respiratory Distress Syndrome (ARDS) An Update Prof. A.S.M. Areef Ahsan FCPS(Medicine) MD(Critical Care Medicine) MD ( Chest) Head, Dept. of Critical Care Medicine BIRDEM General Hospital INTRODUCTION
Shock, Hemorrhage and Thrombosis
 Shock, Hemorrhage and Thrombosis 1 Shock Systemic hypoperfusion due to: Reduction in cardiac output Reduction in effective circulating blood volume Hypotension Impaired tissue perfusion Cellular hypoxia
Shock, Hemorrhage and Thrombosis 1 Shock Systemic hypoperfusion due to: Reduction in cardiac output Reduction in effective circulating blood volume Hypotension Impaired tissue perfusion Cellular hypoxia
Bachelor of Chinese Medicine Shock
 BCM Year 2 Dr. Irene Ng Jan 28, 2003 9:30 am 1:00 pm Rm 004 UPB Bachelor of Chinese Medicine 2002 2003 Shock Learning objectives Be able to: know the definition of shock know the classification and causes
BCM Year 2 Dr. Irene Ng Jan 28, 2003 9:30 am 1:00 pm Rm 004 UPB Bachelor of Chinese Medicine 2002 2003 Shock Learning objectives Be able to: know the definition of shock know the classification and causes
Medical Treatment for acute Decompensated Heart Failure. Vlasis Ninios Cardiologist St. Luke s s Hospital Thessaloniki 2011
 Medical Treatment for acute Decompensated Heart Failure Vlasis Ninios Cardiologist St. Luke s s Hospital Thessaloniki 2011 2010 HFSA guidelines for ADHF 2009 focused update of the 2005 American College
Medical Treatment for acute Decompensated Heart Failure Vlasis Ninios Cardiologist St. Luke s s Hospital Thessaloniki 2011 2010 HFSA guidelines for ADHF 2009 focused update of the 2005 American College
Irreversible shock can defined as last phase of shock where despite correcting the initial insult leading to shock and restoring circulation there is
 R. Siebert Irreversible shock can defined as last phase of shock where despite correcting the initial insult leading to shock and restoring circulation there is a progressive decline in blood pressure
R. Siebert Irreversible shock can defined as last phase of shock where despite correcting the initial insult leading to shock and restoring circulation there is a progressive decline in blood pressure
Infections In Cirrhotic patients. Dr Abid Suddle Institute of Liver Studies King s College Hospital
 Infections In Cirrhotic patients Dr Abid Suddle Institute of Liver Studies King s College Hospital Infection in cirrhotic patients Leading cause morbidity/mortality Common: 30-40% of hospitalised cirrhotic
Infections In Cirrhotic patients Dr Abid Suddle Institute of Liver Studies King s College Hospital Infection in cirrhotic patients Leading cause morbidity/mortality Common: 30-40% of hospitalised cirrhotic
Update in Critical Care Medicine
 Update in Critical Care Medicine Michael A. Gropper, MD, PhD Professor and Executive Vice Chair Department of Anesthesia and Perioperative Care Director, Critical Care Medicine UCSF Disclosure None Update
Update in Critical Care Medicine Michael A. Gropper, MD, PhD Professor and Executive Vice Chair Department of Anesthesia and Perioperative Care Director, Critical Care Medicine UCSF Disclosure None Update
BREAK 11:10-11:
 1. Sepsis Tom Heaps 09:30-10:20 2. Oncological Emergencies Clare Pollard 10:20-11:10 ------------------------ BREAK 11:10-11:30 ------------------------ 3. Diabetic Ketoacidosis Tom Heaps 11:30-12:20 4.
1. Sepsis Tom Heaps 09:30-10:20 2. Oncological Emergencies Clare Pollard 10:20-11:10 ------------------------ BREAK 11:10-11:30 ------------------------ 3. Diabetic Ketoacidosis Tom Heaps 11:30-12:20 4.
Pediatric Code Blue. Goals of Resuscitation. Focus Conference November Ensure organ perfusion
 Pediatric Code Blue Focus Conference November 2015 Duane C. Williams, MD Pediatric Critical Care Department of Pediatrics Children s Hospital of Richmond at VCU Goals of Resuscitation Ensure organ perfusion
Pediatric Code Blue Focus Conference November 2015 Duane C. Williams, MD Pediatric Critical Care Department of Pediatrics Children s Hospital of Richmond at VCU Goals of Resuscitation Ensure organ perfusion
Key Points. Angus DC: Crit Care Med 29:1303, 2001
 Sepsis Key Points Sepsis is the combination of a known or suspected infection and an accompanying systemic inflammatory response (SIRS) Severe sepsis is sepsis with acute dysfunction of one or more organ
Sepsis Key Points Sepsis is the combination of a known or suspected infection and an accompanying systemic inflammatory response (SIRS) Severe sepsis is sepsis with acute dysfunction of one or more organ
How Normal Body Processes Are Altered By Disease and Injury
 1 Chapter 4, GENERAL PRINCIPLES OF PATHOPHYSIOLOGY. Part 1 How Normal Body Processes Are Altered By Disease and Injury 2 How Cells Respond to Change and Injury 3 Pathology & Pathophysiology : the study
1 Chapter 4, GENERAL PRINCIPLES OF PATHOPHYSIOLOGY. Part 1 How Normal Body Processes Are Altered By Disease and Injury 2 How Cells Respond to Change and Injury 3 Pathology & Pathophysiology : the study
Choc septique. Frédéric Pène
 Choc septique Frédéric Pène Réanimation Médicale, Hôpital Cochin, AP-HP Université Paris Descartes Institut Cochin, Inserm U1016, CNRS UMR-8104, Département 3i No conflict of interest A 54 y.o. male patient
Choc septique Frédéric Pène Réanimation Médicale, Hôpital Cochin, AP-HP Université Paris Descartes Institut Cochin, Inserm U1016, CNRS UMR-8104, Département 3i No conflict of interest A 54 y.o. male patient
PAEDIATRIC FEBRILE NEUTROPENIA CARE PATHWAY
 PAEDIATRIC FEBRILE NEUTROPENIA CARE PATHWAY Purpose: This document is intended as a guide to the investigation and management of children presenting in Salisbury District Hospital with suspected neutropenic
PAEDIATRIC FEBRILE NEUTROPENIA CARE PATHWAY Purpose: This document is intended as a guide to the investigation and management of children presenting in Salisbury District Hospital with suspected neutropenic
How to maintain optimal perfusion during Cardiopulmonary By-pass. Herdono Poernomo, MD
 How to maintain optimal perfusion during Cardiopulmonary By-pass Herdono Poernomo, MD Cardiopulmonary By-pass Target Physiologic condition as a healthy person Everything is in Normal Limit How to maintain
How to maintain optimal perfusion during Cardiopulmonary By-pass Herdono Poernomo, MD Cardiopulmonary By-pass Target Physiologic condition as a healthy person Everything is in Normal Limit How to maintain
SEPSIS MANAGEMENT. Abdulhadi Tashkandi, MD, FRCP(c) Assistant Prof. Of Medicine Head of E.D. PMBAH-National Guard hospital Al-Madinah Al-Munawarah
 Assistant Prof. Of Medicine Head of E.D. PMBAH-National Guard hospital Al-Madinah Al-Munawarah") SEPSIS MANAGEMENT Abdulhadi Tashkandi, MD, FRCP(c) Assistant Prof. Of Medicine Head of E.D. PMBAH-National Guard hospital Al-Madinah Al-Munawarah goals Treatment of pts. with septic shock consists of
SEPSIS MANAGEMENT Abdulhadi Tashkandi, MD, FRCP(c) Assistant Prof. Of Medicine Head of E.D. PMBAH-National Guard hospital Al-Madinah Al-Munawarah goals Treatment of pts. with septic shock consists of
Sepsis as Seen by the CMO. Randy C. Roth, MD Chief Medical Officer
 Sepsis as Seen by the CMO Randy C. Roth, MD Chief Medical Officer 1 Challenges of Sepsis Sepsis, like many disease processes, is much more than a clinical challenge. For Hospitalists, we are treating the
Sepsis as Seen by the CMO Randy C. Roth, MD Chief Medical Officer 1 Challenges of Sepsis Sepsis, like many disease processes, is much more than a clinical challenge. For Hospitalists, we are treating the
Taking the shock factor out of shock
 Taking the shock factor out of shock Julie Antonellis, BS, LVT, VTS (ECC) Northern Virginia Regional Director for the VALVT Technician Supervisor VCA Animal Emergency Critical Care Business owner Antonellis
Taking the shock factor out of shock Julie Antonellis, BS, LVT, VTS (ECC) Northern Virginia Regional Director for the VALVT Technician Supervisor VCA Animal Emergency Critical Care Business owner Antonellis