New Advances in the Diagnosis and Management of Acute and Chronic Heart Failure
|
|
|
- Natalie Gilbert
- 5 years ago
- Views:
Transcription

1 New Advances in the Diagnosis and Management of Acute and Chronic Heart Failure Deborah Budge, MD Intermountain Healthcare Heart Failure Cardiologist Objectives: State the updates from the ACC 2013 HF Guidelines Describe guideline-directed medical therapy for HF with reduced EF Understand the mechanism of action of a new therapy for HF and the results of the initial study

2 Updates in Heart Failure ACC/AHA 2013 Guideline Update & PARADIGM Deborah Budge, MD
3 Heart Failure in the US Heart Failure Patients in US (Millions) ~ 6 million symptomatic patients, estimated 10 million in 2037 Incidence: About 550,000 new cases/year More deaths from heart failure than from all forms of cancer combined Prevalence is 1% between the ages of 50 and 59, progressively increasing to >10% over age 80 Over $35 billion/year (5% to 7% of total health care cost) American Heart Association Heart Disease and Stroke Statistical Update.
4 Classification I. Heart Failure with Reduced Ejection Fraction (HFrEF) II. Heart Failure with Preserved Ejection Fraction (HFpEF) a. HFpEF, Borderline Definition of Heart Failure Ejection Fraction 40% 50% 41% to 49% Description Also referred to as systolic HF. Randomized clinical trials have mainly enrolled patients with HFrEF and it is only in these patients that efficacious therapies have been demonstrated to date. Also referred to as diastolic HF. Several different criteria have been used to further define HFpEF. The diagnosis of HFpEF is challenging because it is largely one of excluding other potential noncardiac causes of symptoms suggestive of HF. To date, efficacious therapies have not been identified. These patients fall into a borderline or intermediate group. Their characteristics, treatment patterns, and outcomes appear similar to those of patient with HFpEF. b. HFpEF, Improved > 40% It has been recognized that a subset of patients with HFpEF previously had HFrEF. These patients with improvement or recovery in EF may be clinically distinct from those with persistently preserved or reduced EF. Further research is needed to better characterize these patients. Yancy CW et al. Circulation. 2013;128:e240-e327.
5 New Approach to the Classification of Heart Failure Stage A B C D High risk for developing heart failure (HF) Asymptomatic HF Symptomatic HF Refractory end-stage HF Patient Description Hypertension CAD Diabetes mellitus Family history of cardiomyopathy Previous MI LV systolic dysfunction Asymptomatic valvular disease Known structural heart disease Shortness of breath and fatigue Reduced exercise tolerance Marked symptoms at rest despite maximal medical therapy (eg, those who are recurrently hospitalized or cannot be discharged from the hospital without specialized interventions) Modified from Jessup M. et al. Circulation.2009
6 Classification of Heart Failure ACC/AHA Stage and NYHA Class ACC/AHA HF Stage 1 NYHA Functional Class 2 A At high risk for heart failure but without structural heart disease or symptoms of heart failure (eg, patients with HTN or coronary artery disease) None B Structural heart disease but without symptoms of heart failure C Structural heart disease with prior or current symptoms of heart failure I Asymptomatic II Symptomatic with moderate exertion III Symptomatic with minimal exertion D Refractory heart failure requiring specialized interventions IV Symptomatic at rest Jessup M. et al. Circulation.2009 New York Heart Association/Little Brown and Company, Adapted from: Farrell MH et al.jama.2002.
7 590,000 Stage A Diabetes Hypertension Obesity Atherosclerosis 480,000 Stage B MI Asymptomatic systolic/diastolic dysfunction Asymptomatic valvular disease Heart Failure Prevalence by Stage, Utah * 49,000 Stage C Symptomatic HF 4,900 Stage D Advanced HF *Estimates. Go AS, et al. Heart Disease and Stroke Statistics-2013 Update. Circulation 2013;127:e6-e245. Utah Department of Health. The Impact of Heart Disease and Stroke in Utah 2012.
8 Stages, Phenotypes and Treatment of HF At Risk for Heart Failure Heart Failure STAGE A At high risk for HF but without structural heart disease or symptoms of HF STAGE B Structural heart disease but without signs or symptoms of HF STAGE C Structural heart disease with prior or current symptoms of HF STAGE D Refractory HF e.g., Patients with: HTN Atherosclerotic disease DM Obesity Metabolic syndrome or Patients Using cardiotoxins With family history of cardiomyopathy Structural heart disease e.g., Patients with: Previous MI LV remodeling including LVH and low EF Asymptomatic valvular disease Development of symptoms of HF e.g., Patients with: Known structural heart disease and HF signs and symptoms Refractory symptoms of HF at rest, despite GDMT e.g., Patients with: Marked HF symptoms at rest Recurrent hospitalizations despite GDMT HFpEF HFrEF THERAPY Goals Heart healthy lifestyle Prevent vascular, coronary disease Prevent LV structural abnormalities Drugs ACEI or ARB in appropriate patients for vascular disease or DM Statins as appropriate THERAPY Goals Prevent HF symptoms Prevent further cardiac remodeling Drugs ACEI or ARB as appropriate Beta blockers as appropriate In selected patients ICD Revascularization or valvular surgery as appropriate THERAPY Goals Control symptoms Improve HRQOL Prevent hospitalization Prevent mortality Strategies Identification of comorbidities Treatment Diuresis to relieve symptoms of congestion Follow guideline driven indications for comorbidities, e.g., HTN, AF, CAD, DM Revascularization or valvular surgery as appropriate THERAPY Goals Control symptoms Patient education Prevent hospitalization Prevent mortality Drugs for routine use Diuretics for fluid retention ACEI or ARB Beta blockers Aldosterone antagonists Drugs for use in selected patients Hydralazine/isosorbide dinitrate ACEI and ARB Digoxin In selected patients CRT ICD Revascularization or valvular surgery as appropriate THERAPY Goals Control symptoms Improve HRQOL Reduce hospital readmissions Establish patient s endof-life goals Options Advanced care measures Heart transplant Chronic inotropes Temporary or permanent MCS Experimental surgery or drugs Palliative care and hospice ICD deactivation Yancy CW et al. Circulation. 2013;128:e240-e327.
9
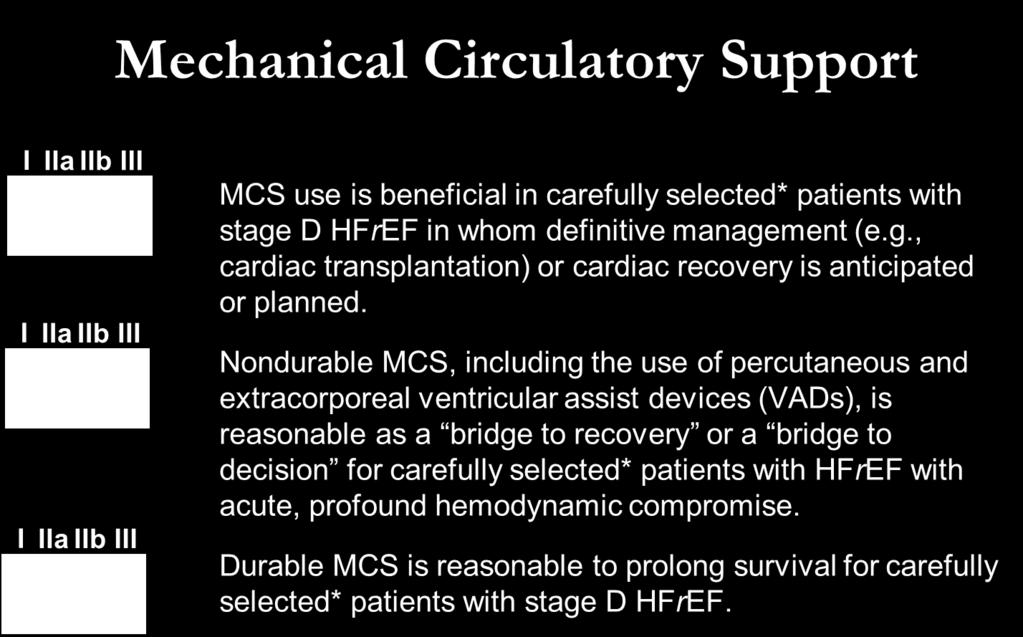
10 Area New Changes (2013) Format Practical system Guideline-directed medical therapy (GDMT) Harmonization with other guidelines, consensus documents Content Oral pharmacologic treatment Non-pharmacological interventions Device therapy Mechanical circulatory support ADHF Role of validated risk scores Role of biomarkers Broader indications for aldosterone antagonists (mild to moderate HF) Emphasis on education and transition of care Balanced approach to Na restriction Broader indications for CRT No change for ICDs Class IIa indication for BTT, BTR, DT Loop diuretics 1 st -line therapy Class IIb low-dose dopamine Class II vasodilators
11 Area New Changes (2013) Format Practical system Guideline-directed medical therapy (GDMT) Harmonization with other guidelines, consensus documents Content Oral pharmacologic treatment Non-pharmacological interventions Device therapy Mechanical circulatory support ADHF Role of validated risk scores Role of biomarkers Broader indications for aldosterone antagonists (mild to moderate HF) Emphasis on education and transition of care Balanced approach to Na restriction Broader indications for CRT No change for ICDs Class IIa indication for BTT, BTR, DT Loop diuretics 1 st -line therapy Class IIb low-dose dopamine Class II vasodilators
12 Practical System Recommendations COR LOE ICD therapy is recommended for primary prevention of SCD in selected patients with HFrEF at least 40 days post-mi with LVEF 35%, and NYHA class II or III symptoms on chronic GDMT, who are expected to live 1 year* I A CRT is indicated for patients who have LVEF 35%, sinus rhythm, LBBB with a QRS 150 ms ICD therapy is recommended for primary prevention of SCD in selected patients with HFrEF at least 40 days post-mi with LVEF 30%, and NYHA class I symptoms while receiving GDMT, who are expected to live 1 year* CRT can be useful for patients who have LVEF 35%, sinus rhythm, a non-lbbb pattern with a QRS 150 ms, and NYHA class III/ambulatory class IV symptoms on GDMT. CRT can be useful for patients who have LVEF 35%, sinus rhythm, LBBB with a QRS 120 to 149 ms, and NYHA class II, III or ambulatory IV symptoms on GDMT CRT can be useful in patients with AF and LVEF 35% on GDMT if a) the patient requires ventricular pacing or otherwise meets CRT criteria and b) AV nodal ablation or rate control allows near 100% ventricular pacing with CRT I I IIa IIa IIa A (NYHA class III/IV) B (NYHA class II) B A B B
13 Practical System Patient with cardiomyopathy on GDMT for >3 mo or on GDMT and >40 d after MI, or with implantation of pacing or defibrillation device for special indications LVEF <35% Evaluate general health status Acceptable noncardiac health Comorbidities and/or frailty limit survival with good functional capacity to <1 y Continue GDMT without implanted device Evaluate NYHA clinical status NYHA class I LVEF 30% QRS 150 ms LBBB pattern Ischemic cardiomyopathy QRS 150 ms Non-LBBB pattern NYHA class II LVEF 35% QRS 150 ms LBBB pattern Sinus rhythm LVEF 35% QRS ms LBBB pattern Sinus rhythm LVEF 35% QRS 150 ms Non-LBBB pattern Sinus rhythm QRS 150 ms Non-LBBB pattern NYHA class III & Ambulatory class IV LVEF 35% QRS 150 ms LBBB pattern Sinus rhythm LVEF 35% QRS ms LBBB pattern Sinus rhythm LVEF 35% QRS 150 ms Non-LBBB pattern Sinus rhythm LVEF 35% QRS ms Non-LBBB pattern Sinus rhythm Special CRT Indications Anticipated to require frequent ventricular pacing (>40%) Atrial fibrillation, if ventricular pacing is required and rate control will result in near 100% ventricular pacing with CRT Colors correspond to the class of recommendations in the ACCF/AHA Table 1. Benefit for NYHA class I and II patients has only been shown in CRT-D trials, and while patients may not experience immediate symptomatic benefit, late remodeling may be avoided along with long-term HF consequences. There are no trials that support CRT-pacing (without ICD) in NYHA class I and II patients. Thus, it is anticipated these patients would receive CRT-D unless clinical reasons or personal wishes make CRT-pacing more appropriate. In patients who are NYHA class III and ambulatory class IV, CRT-D may be chosen but clinical reasons and personal wishes may make CRT-pacing appropriate to improve symptoms and quality of life when an ICD is not expected to produce meaningful benefit in survival.
14 Area New Changes (2013) Format Represents optimal medical therapy as defined by the Content ACCF/AHA guidelinerecommended therapies (primarily Class I) Oral pharmacologic treatment Non-pharmacological interventions Practical system Guideline-directed medical therapy (GDMT) Harmonization with other guidelines, consensus documents Role of validated risk scores Role of biomarkers Broader indications for aldosterone antagonists (mild to moderate HF) Emphasis on education and transition of care Balanced approach to Na restriction Device therapy Mechanical circulatory support ADHF Broader indications for CRT No change for ICDs Class IIa indication for BTT, BTR, DT Loop diuretics 1 st -line therapy Class IIb low-dose dopamine Class II vasodilators
15 Area New Changes (2013) Format Practical system Guideline-directed medical therapy (GDMT) Harmonization with other guidelines, consensus documents Content Oral pharmacologic treatment Non-pharmacological interventions Device therapy Mechanical circulatory support ADHF Role of validated risk scores Role of biomarkers Broader indications for aldosterone antagonists (mild to moderate HF) Emphasis on education and transition of care Balanced approach to Na restriction Broader indications for CRT No change for ICDs Class IIa indication for BTT, BTR, DT Loop diuretics 1 st -line therapy Class IIb low-dose dopamine Class II vasodilators
16 Area New Changes (2013) Format Practical system Guideline-directed medical therapy (GDMT) Harmonization with other guidelines, consensus documents Content Oral pharmacologic treatment Non-pharmacological interventions Device therapy Mechanical circulatory support ADHF Role of validated risk scores Role of biomarkers Broader indications for aldosterone antagonists (mild to moderate HF) Emphasis on education and transition of care Balanced approach to Na restriction Broader indications for CRT No change for ICDs Class IIa indication for BTT, BTR, DT Loop diuretics 1 st -line therapy Class IIb low-dose dopamine Class II vasodilators
17 Risk Scoring Potential benefits of using risk scoring in HF: - Enables patients and families to have a realistic expectation of prognosis - Promotes open communication between clinicians, patients, and families to define goals of therapy - Enables selection of therapies most likely to positively affect the quality and quantity of life - Enables appropriate allocation of resources, including transplant, MCS, and ICD Goldberg LR, Jessup M. Circulation 2007;116(4):360.
18 Risk Scores to Predict Outcomes in HF Risk Score Chronic HF All patients with chronic HF Seattle Heart Failure Model Reference (from full-text guideline)/link (204) / Heart Failure Survival Score (200) / shtml CHARM Risk Score (207) CORONA Risk Score (208) Specific to chronic HFpEF I-PRESERVE Score (202) Acutely Decompensated HF ADHERE Classification and Regression Tree (CART) Model American Heart Association Get With the Guidelines Score EFFECT Risk Score (201) (206) / HFStroke/GetWithTheGuidelinesHeartFailureHomePage/Get-With-The-Guidelines- Heart-Failure-Home- %20Page_UCM_306087_SubHomePage.jsp (203) / ESCAPE Risk Model and Discharge Score (215) OPTIMIZE HF Risk-Prediction Nomogram (216) Yancy CW et al. Circulation. 2013;128:e240-e327.

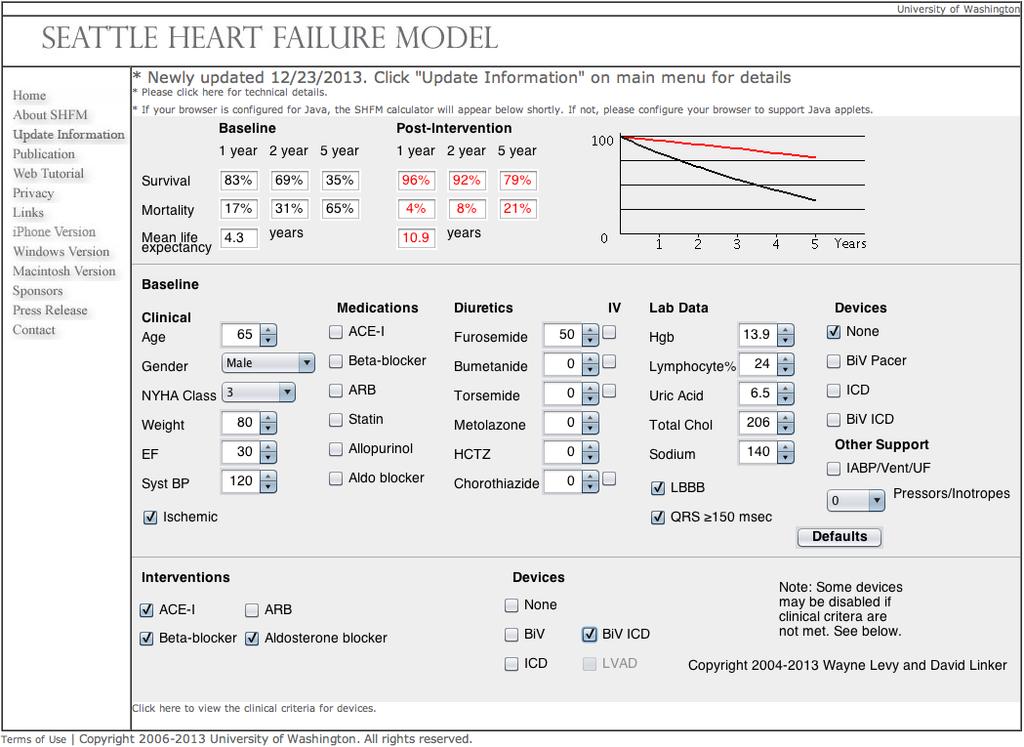
19 Seattle Heart Failure Model (SHFM)
20
21
22
23 Risk Scoring I IIa IIb III Validated multivariable risk scores can be useful to estimate subsequent risk of mortality in ambulatory or hospitalized patients with HF.
24 Area New Changes (2013) Format Practical system Guideline-directed medical therapy (GDMT) Harmonization with other guidelines, consensus documents Content Oral pharmacologic treatment Non-pharmacological interventions Device therapy Mechanical circulatory support ADHF Role of validated risk scores Role of biomarkers Broader indications for aldosterone antagonists (mild to moderate HF) Emphasis on education and transition of care Balanced approach to Na restriction Broader indications for CRT No change for ICDs Class IIa indication for BTT, BTR, DT Loop diuretics 1 st -line therapy Class IIb low-dose dopamine Class II vasodilators
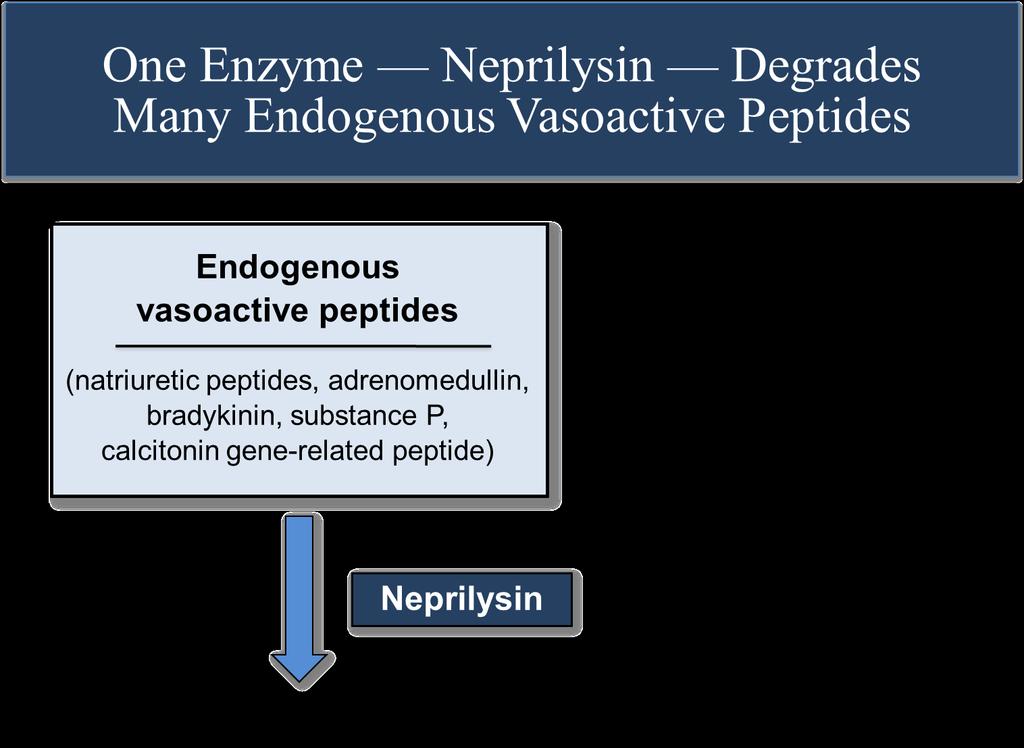
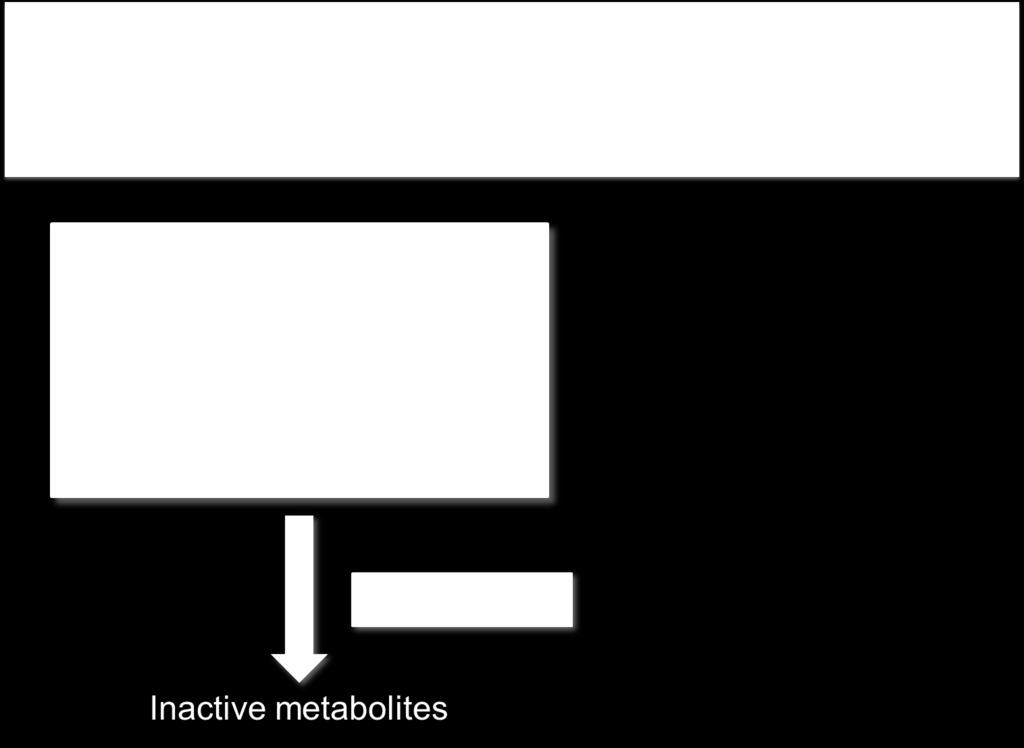
25 Natriuretic peptides: mechanisms UpToDate
26 Use of Natriuretic Peptides in Chronic Heart Failure Initial diagnosis Prognosis Chronic management in the outpatient setting

27 Natriuretic Peptides and Prognosis in Chronic Heart Failure 32% 9% theheart.org Masson S, et al. Clin Chem 2006;52:
28 Use of Natriuretic Peptides in Chronic Heart Failure I IIa IIb III Measurement of BNP or NT-proBNP is useful for establishing prognosis or disease severity in chronic HF.
29 Use of Natriuretic Peptides in Chronic Heart Failure Initial diagnosis Prognosis Chronic management in the outpatient setting
30 Patient Example 76-year-old man with ischemic cardiomyopathy, LVEF 25%, seen in clinic for routine evaluation Admitted for decompensated heart failure 4 months ago, uneventful hospitalization Reports NYHA Class II symptoms, denies congestive symptoms, says he feels great Medications: carvedilol 12.5 mg BID, lisinopril 10 mg QD, furosemide 40 mg QD PE: BP 110/62, HR 66, JVP 6 cm, lungs clear, grade 2 MR murmur, trace edema Labs: creatinine 1.4 mg/dl, BNP 329
31 Challenges with GDMT Therapeutic inertia Differentiation responders vs non-responders Knowing if a patient is truly maximized on meds Assessing volume status Monitoring those who are ostensibly stable for impending complications
32 Therapies which alter BNP levels Therapy BNP Level Diuresis ACE-I ARB Beta-Blockers Aldosterone Antagonists CRT Exercise Rate control of AF

33 Serial NP Measurements for Prognostication in Chronic HF theheart.org Masson S, et al. J Am Coll Cardiol 2008;52:

34 Understanding Heterogeneous Results in Guided Therapy Trials theheart.org Motiwala SR, et al. Clin Pharm Ther 2013;93:57-67.
 to usual care in high risk patients with")
35 Objective: To compare a strategy of medical therapy titration aimed at achieving and maintaining an NT-proBNP target of < 1000 pg/ml (biomarker-guided therapy) to usual care in high risk patients with HFrEF
36 Use of Natriuretic Peptides in Chronic Heart Failure I IIa IIb III I IIa IIb III BNP- or NT-proBNP guided HF therapy can be useful to achieve optimal dosing of GDMT in select clinically euvolemic patients followed in a wellstructured HF disease management program. The usefulness of serial measurement of BNP or NTproBNP to reduce hospitalization or mortality in patients with HF is not well established.
37 Area New Changes (2013) Format Practical system Guideline-directed medical therapy (GDMT) Harmonization with other guidelines, consensus documents Content Oral pharmacologic treatment Non-pharmacological interventions Device therapy Mechanical circulatory support ADHF Role of validated risk scores Role of biomarkers Broader indications for aldosterone antagonists (mild to moderate HF) Emphasis on education and transition of care Balanced approach to Na restriction Broader indications for CRT No change for ICDs Class IIa indication for BTT, BTR, DT Loop diuretics 1 st -line therapy Class IIb low-dose dopamine Class II vasodilators

38 Aldosterone Antagonist: Mechanism of Action

39 RALES Cardiosource.com NEJM 1999;341:

40 EPHESUS Cardiosource.com NEJM 2003;348:

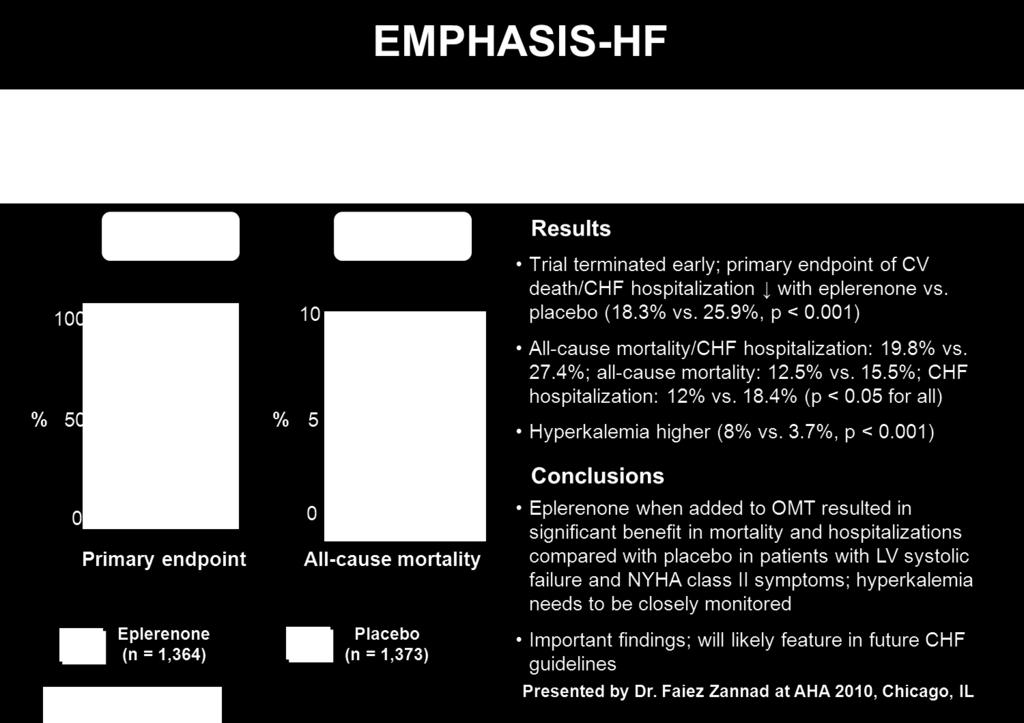
41 EMPHASIS-HF Cardiosource.com NEJM 2011;364:11-21.
42 Aldosterone Antagonists I IIa IIb III Aldosterone receptor antagonists are recommended in patients with NYHA class II-IV and who have LVEF of 35% or less, unless contraindicated, to reduce morbidity and mortality. Patients with NYHA class II should have a history of prior cardiovascular hospitalization or elevated plasma natriuretic peptide levels to be considered for aldosterone receptor antagonists. I IIa IIb III Aldosterone receptor antagonists are recommended to reduce morbidity and mortality following an acute MI in patients who have LVEF of 40% or less who develop symptoms of HF or who have a history of diabetes mellitus, unless contraindicated.
 and potassium should be less than 5.0 meq/l.")
43 Aldosterone Antagonists I IIa IIb III Creatinine should be 2.5 mg/dl or less in men or 2.0 mg/dl or less in women (or estimated glomerular filtration rate >30 ml/min/1.73m2) and potassium should be less than 5.0 meq/l. Careful monitoring of potassium, renal function, and diuretic dosing should be performed at initiation and closely followed thereafter to minimize risk of hyperkalemia and renal insufficiency. Check potassium and renal function: - 2 to 3 days after starting therapy - 1 week after starting therapy, AND - At least monthly for the first 3 months

44 IMPROVE-HF Fonarow G C et al. Circulation 2010;122:
45
46 Pharmacologic Treatment for Stage C HFrEF HFrEF Stage C NYHA Class I IV Treatment: Class I, LOE A ACEI or ARB AND Beta Blocker For all volume overload, NYHA class II-IV patients For persistently symptomatic African Americans, NYHA class III-IV For NYHA class II-IV patients. Provided estimated creatinine >30 ml/min and K+ <5.0 meq/dl Add Add Add Class I, LOE C Loop Diuretics Class I, LOE A Hydral-Nitrates Class I, LOE A Aldosterone Antagonist

47
48

49 Strategies for Achieving Optimal GDMT Yancy CW et al. Circulation. 2013;128:e240-e327.
50 Area New Changes (2013) Format Practical system Guideline-directed medical therapy (GDMT) Harmonization with other guidelines, consensus documents Content Oral pharmacologic treatment Non-pharmacological interventions Device therapy Mechanical circulatory support ADHF Role of validated risk scores Role of biomarkers Broader indications for aldosterone antagonists (mild to moderate HF) Emphasis on education and transition of care Balanced approach to Na restriction Broader indications for CRT No change for ICDs Class IIa indication for BTT, BTR, DT Loop diuretics 1 st -line therapy Class IIb low-dose dopamine Class II vasodilators
51 Need for Improved Care Coordination #1 reason for hospitalization for people >65 years of age National 30 day readmission rate 25% Mortality 50% at 5 years, 34% at 1 year following a hospitalization Many HF hospitalizations are driven by gaps in the process of care rather than worsening pathophysiology Collins SP, et al. J Am Coll Cardiol 2013;61:121-6.

52 Transitions of Care I IIa IIb III Throughout the hospitalization as appropriate, before hospital discharge, at the first postdischarge visit, and in subsequent follow-up visits, the following should be addressed: a. initiation of GDMT if not previously established and not contraindicated; b. precipitant causes of HF, barriers to optimal care transitions, and limitations in postdischarge support; Of the patients in Utah with HF, 87% c. assessment of volume status and supine/upright hypotension with have adjustment 3 or more of HF chronic therapy, conditions, as appropriate; and d. titration and optimization 54% of have chronic 5 or oral more HF therapy; chronic conditions. e. assessment of renal function and electrolytes, where appropriate; f. assessment and management of comorbid conditions; g. reinforcement of HF education, self-care, emergency plans, and need for adherence; and h. consideration for palliative care or hospice care in selected patients.
53 Transitions of Care I IIa IIb III I IIa IIb III I IIa IIb III Multidisciplinary HF disease-management programs are recommended for patients at high risk for hospital readmission, to facilitate the implementation of GDMT, to address different barriers to behavioral change, and to reduce the risk of subsequent rehospitalization for HF. Scheduling an early follow-up visit (within 7 to 14 days) and early telephone follow-up (within 3 days) of hospital discharge is reasonable. Use of clinical risk prediction tools and/or biomarkers to identify patients at higher risk for postdischarge clinical events is reasonable.
54 Sodium Restriction Mixed data evaluating sodium restriction in HF Observational data = association between sodium intake and risk for hospitalization RCTs = lower sodium intake is associated with worse outcomes in HFrEF No study has been done in optimally treated patients I IIa IIb III Sodium restriction is reasonable for patients with symptomatic HF to reduce congestive symptoms.
55 Area New Changes (2013) Format Practical system Guideline-directed medical therapy (GDMT) Harmonization with other guidelines, consensus documents Content Oral pharmacologic treatment Non-pharmacological interventions Device therapy Mechanical circulatory support ADHF Role of validated risk scores Role of biomarkers Broader indications for aldosterone antagonists (mild to moderate HF) Emphasis on education and transition of care Balanced approach to Na restriction Broader indications for CRT No change for ICDs Class IIa indication for BTT, BTR, DT Loop diuretics 1 st -line therapy Class IIb low-dose dopamine Class II vasodilators
56 Indications for CRT in HF Patient with cardiomyopathy on GDMT for >3 mo or on GDMT and >40 d after MI, or with implantation of pacing or defibrillation device for special indications LVEF <35% Evaluate general health status Acceptable noncardiac health Comorbidities and/or frailty limit survival with good functional capacity to <1 y Continue GDMT without implanted device Evaluate NYHA clinical status NYHA class I LVEF 30% QRS 150 ms LBBB pattern Ischemic cardiomyopathy QRS 150 ms Non-LBBB pattern NYHA class II LVEF 35% QRS 150 ms LBBB pattern Sinus rhythm LVEF 35% QRS ms LBBB pattern Sinus rhythm LVEF 35% QRS 150 ms Non-LBBB pattern Sinus rhythm QRS 150 ms Non-LBBB pattern NYHA class III & Ambulatory class IV LVEF 35% QRS 150 ms LBBB pattern Sinus rhythm LVEF 35% QRS ms LBBB pattern Sinus rhythm LVEF 35% QRS 150 ms Non-LBBB pattern Sinus rhythm LVEF 35% QRS ms Non-LBBB pattern Sinus rhythm Special CRT Indications Anticipated to require frequent ventricular pacing (>40%) Atrial fibrillation, if ventricular pacing is required and rate control will result in near 100% ventricular pacing with CRT Colors correspond to the class of recommendations in the ACCF/AHA Table 1. Benefit for NYHA class I and II patients has only been shown in CRT-D trials, and while patients may not experience immediate symptomatic benefit, late remodeling may be avoided along with long-term HF consequences. There are no trials that support CRT-pacing (without ICD) in NYHA class I and II patients. Thus, it is anticipated these patients would receive CRT-D unless clinical reasons or personal wishes make CRT-pacing more appropriate. In patients who are NYHA class III and ambulatory class IV, CRT-D may be chosen but clinical reasons and personal wishes may make CRT-pacing appropriate to improve symptoms and quality of life when an ICD is not expected to produce meaningful benefit in survival.
57 Area New Changes (2013) Format Practical system Guideline-directed medical therapy (GDMT) Harmonization with other guidelines, consensus documents Content Oral pharmacologic treatment Non-pharmacological interventions Device therapy Mechanical circulatory support ADHF Role of validated risk scores Role of biomarkers Broader indications for aldosterone antagonists (mild to moderate HF) Emphasis on education and transition of care Balanced approach to Na restriction Broader indications for CRT No change for ICDs Class IIa indication for BTT, BTR, DT Loop diuretics 1 st -line therapy Class IIb low-dose dopamine Class II vasodilators
58
59 Clinical Events and Findings Useful for Identifying Patients With Advanced HF Repeated ( 2) hospitalizations or ED visits for HF in the past year Progressive deterioration in renal function (e.g., rise in BUN and creatinine) Weight loss without other cause (e.g., cardiac cachexia) Intolerance to ACE inhibitors due to hypotension and/or worsening renal function Intolerance to beta blockers due to worsening HF or hypotension Frequent systolic blood pressure <90 mm Hg Persistent dyspnea with dressing or bathing requiring rest Inability to walk 1 block on the level ground due to dyspnea or fatigue Recent need to escalate diuretics to maintain volume status, often reaching daily furosemide equivalent dose >160 mg/d and/or use of supplemental metolazone therapy Progressive decline in serum sodium, usually to <133 meq/l Frequent ICD shocks
60 Mechanical Circulatory Support Patient selection and Evaluation 1. Does the patient have a reversible cause of heart failure? 2. Is the patient on the maximum/tolerated standard medical HF therapy? 3. Is the patient candidate for CRT-D? If yes, will it make a difference? 4. What is the patient s prognosis in the next year without MCS?(High risk for mortality 50%). 5. Does the patient have any irreversible co-morbidities that will affect quality of life and survival after MCS implantation? 6. Does the patient have adequate financial and psychosocial support, and safe living environment? 7. Does the patient have high risk behavior?
61 HeartMate II - BTT Outcomes J Am Coll Cardiol 2009;54:312 21
62 HeartWare (HVAD) - BTT Outcomes Circulation. 2012; 125:
63 HeartMate II - DT Outcomes Circ Heart Fail. 2012;5:241-48
64 Mechanical Circulatory Support
65 Area New Changes (2013) Format Practical system Guideline-directed medical therapy (GDMT) Harmonization with other guidelines, consensus documents Content Oral pharmacologic treatment Non-pharmacological interventions Device therapy Mechanical circulatory support ADHF Role of validated risk scores Role of biomarkers Broader indications for aldosterone antagonists (mild to moderate HF) Emphasis on education and transition of care Balanced approach to Na restriction Broader indications for CRT No change for ICDs Class IIa indication for BTT, BTR, DT Loop diuretics 1 st -line therapy Class IIb low-dose dopamine Class II vasodilators

66
67
68
69
70
71
72
73
74 PARADIGM-HF: Secondary Endpoints All-cause mortality Change from baseline in the clinical summary score of the Kansas City Cardiomyopathy Questionnaire at 8 months Time to new onset of atrial fibrillation Time to first occurrence of a protocol-defined decline in renal function
75
76 (all comparisons are versus enalapril 20 mg daily, not versus placebo)
 Kaplan-Meier Estimate of Cumulative Rates (%) 40 32")

 P = 0.")
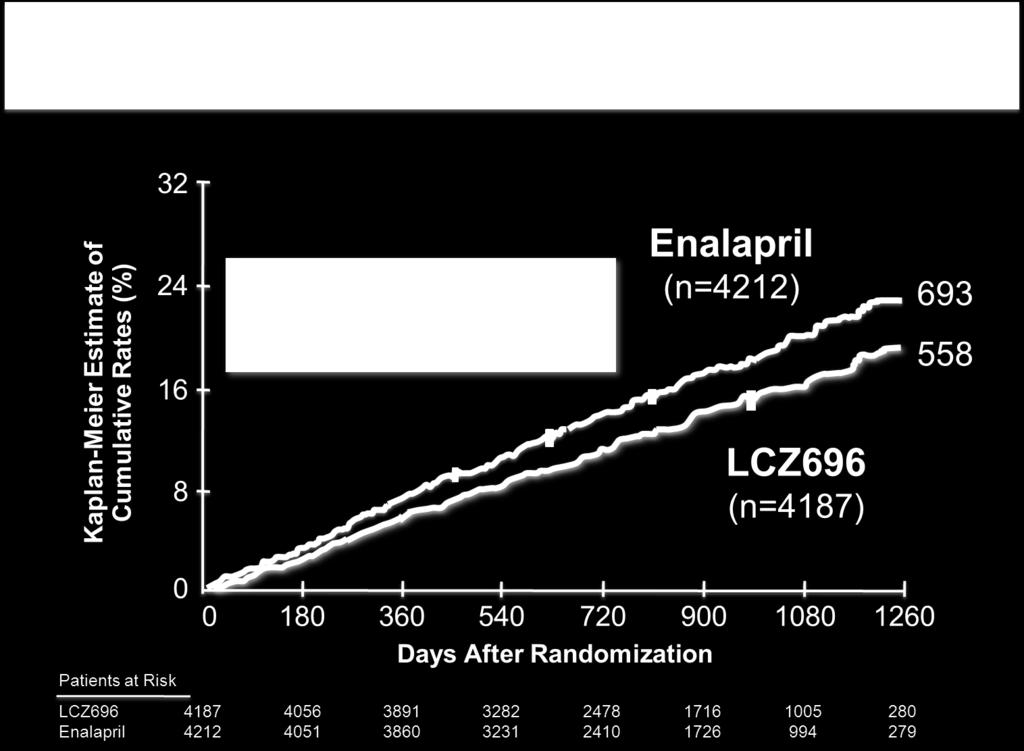
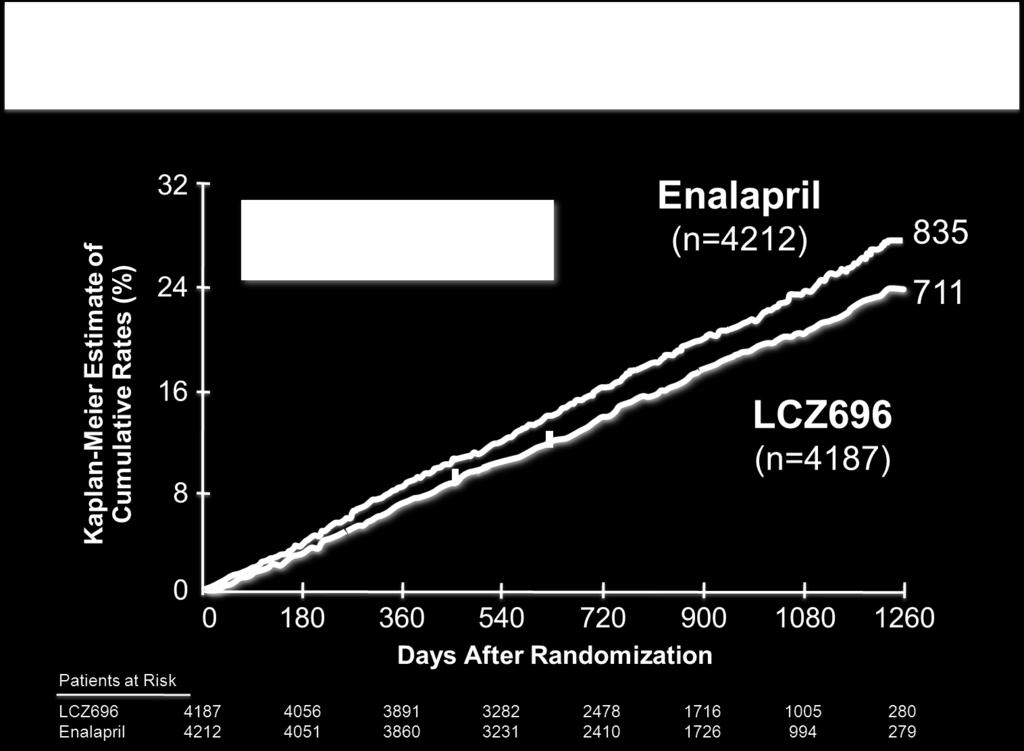
77 PARADIGM-HF: Cardiovascular Death or Heart Failure Hospitalization (Primary Endpoint) Kaplan-Meier Estimate of Cumulative Rates (%) Patients at Risk LCZ696 Enalapril 8 0 Enalapril (n=4212) Days After Randomization LCZ696 (n=4187) HR = 0.80 ( ) P = Number needed to treat =
78
79
80
81
82
83 Thank You!
2016 Update to Heart Failure Clinical Practice Guidelines
 2016 Update to Heart Failure Clinical Practice Guidelines Mitchell T. Saltzberg, MD, FACC, FAHA, FHFSA Medical Director of Advanced Heart Failure Froedtert & Medical College of Wisconsin Stages, Phenotypes
2016 Update to Heart Failure Clinical Practice Guidelines Mitchell T. Saltzberg, MD, FACC, FAHA, FHFSA Medical Director of Advanced Heart Failure Froedtert & Medical College of Wisconsin Stages, Phenotypes
Heart Failure Management. Waleed AlHabeeb, MD, MHA Assistant Professor of Medicine Consultant Heart Failure Cardiologist
 Heart Failure Management Waleed AlHabeeb, MD, MHA Assistant Professor of Medicine Consultant Heart Failure Cardiologist Heart failure prevalence is expected to continue to increase¹ 21 MILLION ADULTS WORLDWIDE
Heart Failure Management Waleed AlHabeeb, MD, MHA Assistant Professor of Medicine Consultant Heart Failure Cardiologist Heart failure prevalence is expected to continue to increase¹ 21 MILLION ADULTS WORLDWIDE
DISCLAIMER: ECHO Nevada emphasizes patient privacy and asks participants to not share ANY Protected Health Information during ECHO clinics.
 DISCLAIMER: Video will be taken at this clinic and potentially used in Project ECHO promotional materials. By attending this clinic, you consent to have your photo taken and allow Project ECHO to use this
DISCLAIMER: Video will be taken at this clinic and potentially used in Project ECHO promotional materials. By attending this clinic, you consent to have your photo taken and allow Project ECHO to use this
Citation. What is New in the 2013 ACC/AHA HF Guideline. Dimensions in Heart and Vascular Care Penn State Heart and Vascular Institute
 What is New in the 2013 ACC/AHA HF Guideline Dimensions in Heart and Vascular Care Penn State Heart and Vascular nstitute Friday October 18, 2013 Barry S. Clemson, MD Associate Professor of Medicine Penn
What is New in the 2013 ACC/AHA HF Guideline Dimensions in Heart and Vascular Care Penn State Heart and Vascular nstitute Friday October 18, 2013 Barry S. Clemson, MD Associate Professor of Medicine Penn
Heart Failure: Guideline-Directed Management and Therapy
 Heart Failure: Guideline-Directed Management and Therapy Guideline-Directed Management and Therapy (GDMT) was developed by the American College of Cardiology and American Heart Association to define the
Heart Failure: Guideline-Directed Management and Therapy Guideline-Directed Management and Therapy (GDMT) was developed by the American College of Cardiology and American Heart Association to define the
Congestive Heart Failure: Outpatient Management
 The Chattanooga Heart Institute Cardiovascular Symposium Congestive Heart Failure: Outpatient Management E. Philip Lehman MD, MPP Disclosure No financial disclosures. Objectives Evidence-based therapy
The Chattanooga Heart Institute Cardiovascular Symposium Congestive Heart Failure: Outpatient Management E. Philip Lehman MD, MPP Disclosure No financial disclosures. Objectives Evidence-based therapy
Summary/Key Points Introduction
 Summary/Key Points Introduction Scope of Heart Failure (HF) o 6.5 million Americans 20 years of age have HF o 960,000 new cases of HF diagnosed annually o 5-year survival rate for HF is ~50% Classification
Summary/Key Points Introduction Scope of Heart Failure (HF) o 6.5 million Americans 20 years of age have HF o 960,000 new cases of HF diagnosed annually o 5-year survival rate for HF is ~50% Classification
Systolic Dysfunction Clinical/Hemodynamic Guide for Management; New Medical and Interventional Therapeutic Challenges
 Systolic Dysfunction Clinical/Hemodynamic Guide for Management; New Medical and Interventional Therapeutic Challenges Clyde W. Yancy, MD, MSc, FACC, FAHA, MACP Magerstadt Professor of Medicine Professor,
Systolic Dysfunction Clinical/Hemodynamic Guide for Management; New Medical and Interventional Therapeutic Challenges Clyde W. Yancy, MD, MSc, FACC, FAHA, MACP Magerstadt Professor of Medicine Professor,
The ACC Heart Failure Guidelines
 The ACC Heart Failure Guidelines Fakhr Alayoubi, Msc,R Ph President of SCCP Cardiology Clinical Pharmacist Assistant Professor At King Saud University King Khalid University Hospital Riyadh-KSA 2017 ACC/AHA/HFSA
The ACC Heart Failure Guidelines Fakhr Alayoubi, Msc,R Ph President of SCCP Cardiology Clinical Pharmacist Assistant Professor At King Saud University King Khalid University Hospital Riyadh-KSA 2017 ACC/AHA/HFSA
From PARADIGM-HF to Clinical Practice. Waleed AlHabeeb, MD, MHA Associate Professor of Medicine President of the Saudi Heart Failure Group
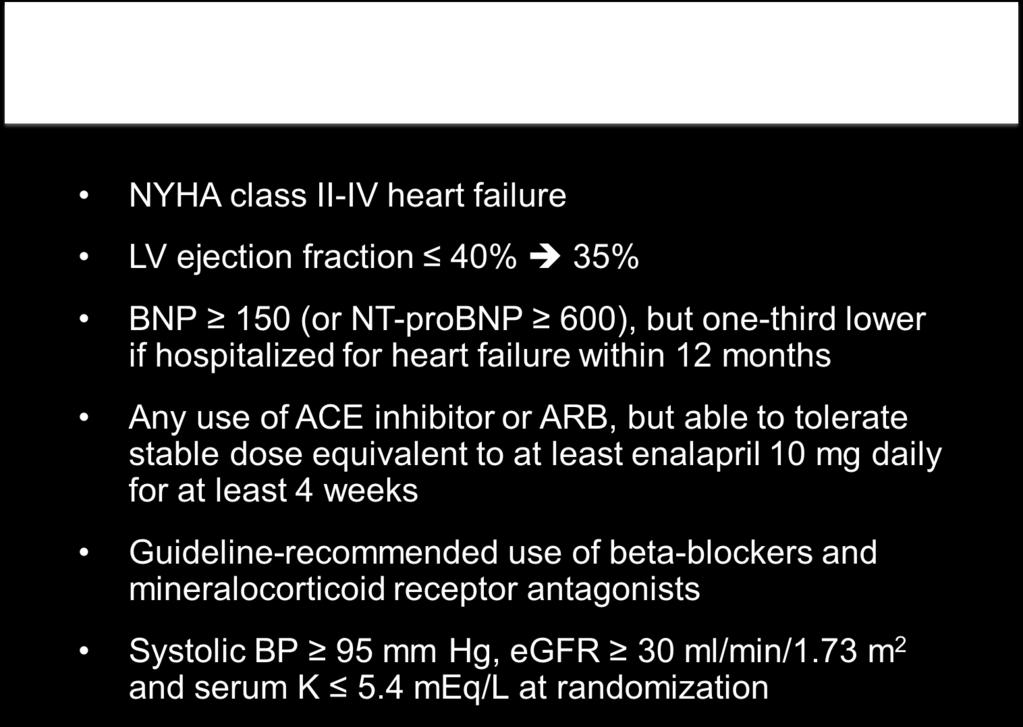
 From PARADIGM-HF to Clinical Practice Waleed AlHabeeb, MD, MHA Associate Professor of Medicine President of the Saudi Heart Failure Group PARADIGM-HF: Inclusion Criteria Chronic HF NYHA FC II IV with LVEF
From PARADIGM-HF to Clinical Practice Waleed AlHabeeb, MD, MHA Associate Professor of Medicine President of the Saudi Heart Failure Group PARADIGM-HF: Inclusion Criteria Chronic HF NYHA FC II IV with LVEF
Ventricular Assist Device: Are Early Interventions Superior? Hamang Patel, MD Section of Cardiomyopathy & Heart Transplantation
 Ventricular Assist Device: Are Early Interventions Superior? Hamang Patel, MD Section of Cardiomyopathy & Heart Transplantation Objectives Current rationale behind use of MCS Patient Selection Earlier?
Ventricular Assist Device: Are Early Interventions Superior? Hamang Patel, MD Section of Cardiomyopathy & Heart Transplantation Objectives Current rationale behind use of MCS Patient Selection Earlier?
Optimizing CHF Therapy: The Role of Digoxin, Diuretics, and Aldosterone Antagonists
 Optimizing CHF Therapy: The Role of Digoxin, Diuretics, and Aldosterone Antagonists Old Drugs for an Old Problem Jay Geoghagan, MD, FACC BHHI Primary Care Symposium February 28, 2014 None. Financial disclosures
Optimizing CHF Therapy: The Role of Digoxin, Diuretics, and Aldosterone Antagonists Old Drugs for an Old Problem Jay Geoghagan, MD, FACC BHHI Primary Care Symposium February 28, 2014 None. Financial disclosures
Chronic. Congestive^ Heart Failure: Update on Effective Monitoring and Treatment. Michael G. Shlipak, MD, MPH
 Chronic Congestive^ Heart Failure: Update on Effective Monitoring and Treatment Michael G. Shlipak, MD, MPH Professor of Medicine, UCSF Chief, Division of General Internal Medicine, SFVA Medical Center
Chronic Congestive^ Heart Failure: Update on Effective Monitoring and Treatment Michael G. Shlipak, MD, MPH Professor of Medicine, UCSF Chief, Division of General Internal Medicine, SFVA Medical Center
Heart Failure Management Policy and Procedure Phase 1
 1301 Punchbowl Street, Harkness Suite 225 Honolulu, Hawaii 96813 Phone (808) 691-7220 Fax: (808) 691-4099 www.queenscipn.org Policy and Procedure Phase 1 Policy Number: Effective Date: Revised: Approved
1301 Punchbowl Street, Harkness Suite 225 Honolulu, Hawaii 96813 Phone (808) 691-7220 Fax: (808) 691-4099 www.queenscipn.org Policy and Procedure Phase 1 Policy Number: Effective Date: Revised: Approved
Heart Failure Update. Bibiana Cujec MD May 2015
 Heart Failure Update Bibiana Cujec MD May 2015 Disclosures Participation in clinical trial GUIDE IT (BNP in management of HF) Plan Review of new trials/ccs guidelines Management of heart failure: cases
Heart Failure Update Bibiana Cujec MD May 2015 Disclosures Participation in clinical trial GUIDE IT (BNP in management of HF) Plan Review of new trials/ccs guidelines Management of heart failure: cases
2017 ACC/AHA/HFSA Focused Update of the 2013 ACCF/AHA Guideline for the Management of Heart Failure
 2017 ACC/AHA/HFSA Focused Update of the 2013 ACCF/AHA Guideline for the Management of Heart Failure Developed in Collaboration With the American Academy of Family Physicians, American College of Chest
2017 ACC/AHA/HFSA Focused Update of the 2013 ACCF/AHA Guideline for the Management of Heart Failure Developed in Collaboration With the American Academy of Family Physicians, American College of Chest
Heart Failure Guidelines For your Daily Practice
 Heart Failure Guidelines For your Daily Practice Juan M. Aranda, Jr., MD, FACC, FHFSA Professor of Medicine Director of Heart Failure and Cardiac Transplantation University of Florida College of Medicine
Heart Failure Guidelines For your Daily Practice Juan M. Aranda, Jr., MD, FACC, FHFSA Professor of Medicine Director of Heart Failure and Cardiac Transplantation University of Florida College of Medicine
DISCLAIMER: ECHO Nevada emphasizes patient privacy and asks participants to not share ANY Protected Health Information during ECHO clinics.
 DISCLAIMER: Video will be taken at this clinic and potentially used in Project ECHO promotional materials. By attending this clinic, you consent to have your photo taken and allow Project ECHO to use this
DISCLAIMER: Video will be taken at this clinic and potentially used in Project ECHO promotional materials. By attending this clinic, you consent to have your photo taken and allow Project ECHO to use this
What s new in the 2017 heart failure guidelines. Prof.Dr.Mehmet Birhan YILMAZ, FESC, FACC, FHFA
 What s new in the 2017 heart failure guidelines Prof.Dr.Mehmet Birhan YILMAZ, FESC, FACC, FHFA Key points to remember 2017 guidelines recommend using natriuretic peptides as biomarkers to screen for heart
What s new in the 2017 heart failure guidelines Prof.Dr.Mehmet Birhan YILMAZ, FESC, FACC, FHFA Key points to remember 2017 guidelines recommend using natriuretic peptides as biomarkers to screen for heart
What Is Best Care for Patients with End stage heart failure?
 What Is Best Care for Patients with End stage heart failure? Jin Joo Park, MD Cardiovascular Center, Department of Internal Medicine Bundang Hospital NYHA Class Class Patient Symptoms I No limitation of
What Is Best Care for Patients with End stage heart failure? Jin Joo Park, MD Cardiovascular Center, Department of Internal Medicine Bundang Hospital NYHA Class Class Patient Symptoms I No limitation of
Update in Congestive Hear Failure DRAGOS VESBIANU MD
 Update in Congestive Hear Failure DRAGOS VESBIANU MD Case 58 yo AAM c/o shortness of breath for 3 weeks. Used to walk one mile per day and now he has noticed that he gets short of breath after 2 blocks.
Update in Congestive Hear Failure DRAGOS VESBIANU MD Case 58 yo AAM c/o shortness of breath for 3 weeks. Used to walk one mile per day and now he has noticed that he gets short of breath after 2 blocks.
Updates in Congestive Heart Failure
 Updates in Congestive Heart Failure GREGORY YOST, DO JOHNSTOWN CARDIOVASCULAR ASSOCIATES 1/28/2018 Disclosures Edwards speaker on Sapien3 valves (TAVR) Stages A-D and NYHA Classes I-IV Stage A: High risk
Updates in Congestive Heart Failure GREGORY YOST, DO JOHNSTOWN CARDIOVASCULAR ASSOCIATES 1/28/2018 Disclosures Edwards speaker on Sapien3 valves (TAVR) Stages A-D and NYHA Classes I-IV Stage A: High risk
New Paradigms in Rx of Symptomati Heart Failure:Role of Ivabradine & Angiotensin Neprilysin Inhibition
 New Paradigms in Rx of Symptomati Heart Failure:Role of Ivabradine & Angiotensin Neprilysin Inhibition Prakash Deedwania, MD, FACC, FACP, FCCP, FAHA Professor of Medicine, UCSF School of Medicine, Director,
New Paradigms in Rx of Symptomati Heart Failure:Role of Ivabradine & Angiotensin Neprilysin Inhibition Prakash Deedwania, MD, FACC, FACP, FCCP, FAHA Professor of Medicine, UCSF School of Medicine, Director,
Checklist for Treating Heart Failure. Alan M. Kaneshige MD, FACC, FASE Oklahoma Heart Institute
 Checklist for Treating Heart Failure Alan M. Kaneshige MD, FACC, FASE Oklahoma Heart Institute Novartis Disclosure Heart Failure (HF) a complex clinical syndrome that arises secondary to abnormalities
Checklist for Treating Heart Failure Alan M. Kaneshige MD, FACC, FASE Oklahoma Heart Institute Novartis Disclosure Heart Failure (HF) a complex clinical syndrome that arises secondary to abnormalities
HFpEF, Mito or Realidad?
 HFpEF, Mito or Realidad? Ileana L. Piña, MD, MPH Professor of Medicine and Epidemiology/Population Health Associate Chief for Academic Affairs -- Cardiology Montefiore-Einstein Medical Center Bronx, NY
HFpEF, Mito or Realidad? Ileana L. Piña, MD, MPH Professor of Medicine and Epidemiology/Population Health Associate Chief for Academic Affairs -- Cardiology Montefiore-Einstein Medical Center Bronx, NY
The Failing Heart in Primary Care
 The Failing Heart in Primary Care Hamid Ikram How fares the Heart Failure Epidemic? 4357 patients, 57% women, mean age 74 years HFSA 2010 Practice Guideline (3.1) Heart Failure Prevention A careful and
The Failing Heart in Primary Care Hamid Ikram How fares the Heart Failure Epidemic? 4357 patients, 57% women, mean age 74 years HFSA 2010 Practice Guideline (3.1) Heart Failure Prevention A careful and
Treating HF Patients with ARNI s Why, When and How?
 Treating HF Patients with ARNI s Why, When and How? 19 th Annual San Diego Heart Failure Symposium for Primary Care Physicians January 11-12, 2019 La Jolla, CA Barry Greenberg M.D. Distinguished Professor
Treating HF Patients with ARNI s Why, When and How? 19 th Annual San Diego Heart Failure Symposium for Primary Care Physicians January 11-12, 2019 La Jolla, CA Barry Greenberg M.D. Distinguished Professor
9/10/ , American Heart Association 2
 Clyde W. Yancy, MD, MSc, MACC, FAHA, MACP Vice Dean, Diversity & Inclusion Magerstadt Professor of Medicine Professor of Medical Social Sciences Chief, Division of Cardiology Northwestern University, Feinberg
Clyde W. Yancy, MD, MSc, MACC, FAHA, MACP Vice Dean, Diversity & Inclusion Magerstadt Professor of Medicine Professor of Medical Social Sciences Chief, Division of Cardiology Northwestern University, Feinberg
Heart Failure Clinician Guide JANUARY 2016
 Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Heart Failure Clinician Guide JANUARY 2016 Introduction This evidence-based guideline summary is based on the 2016 National Heart Failure Guideline.
Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Heart Failure Clinician Guide JANUARY 2016 Introduction This evidence-based guideline summary is based on the 2016 National Heart Failure Guideline.
1/4/18. Heart Failure Guideline Review and Update. Disclosure. Pharmacist Objectives. Pharmacy Technician Objectives. What is Heart Failure?
 Disclosure Heart Failure Guideline Review and Update I have had no financial relationship over the past 12 months with any commercial sponsor with a vested interest in this presentation. Natalie Beiter,
Disclosure Heart Failure Guideline Review and Update I have had no financial relationship over the past 12 months with any commercial sponsor with a vested interest in this presentation. Natalie Beiter,
Management Strategies for Advanced Heart Failure
 Management Strategies for Advanced Heart Failure Mary Norine Walsh, MD, FACC Medical Director, HF and Cardiac Transplantation St Vincent Heart Indianapolis, IN USA President American College of Cardiology
Management Strategies for Advanced Heart Failure Mary Norine Walsh, MD, FACC Medical Director, HF and Cardiac Transplantation St Vincent Heart Indianapolis, IN USA President American College of Cardiology
HEART FAILURE: PHARMACOTHERAPY UPDATE
 HEART FAILURE: PHARMACOTHERAPY UPDATE 3 HEART FAILURE REVIEW 1 5.1 million x1.25 = 6.375 million 40 years old = MICHAEL F. AKERS, PHARM.D. CLINICAL PHARMACIST CENTRACARE HEALTH, ST. CLOUD HOSPITAL HF Diagnosis
HEART FAILURE: PHARMACOTHERAPY UPDATE 3 HEART FAILURE REVIEW 1 5.1 million x1.25 = 6.375 million 40 years old = MICHAEL F. AKERS, PHARM.D. CLINICAL PHARMACIST CENTRACARE HEALTH, ST. CLOUD HOSPITAL HF Diagnosis
ESC Guidelines for the Diagnosis and Treatment of Acute and Chronic Heart Failure
 Patients t with acute heart failure frequently develop chronic heart failure Patients with chronic heart failure frequently decompensate acutely ESC Guidelines for the Diagnosis and A clinical response
Patients t with acute heart failure frequently develop chronic heart failure Patients with chronic heart failure frequently decompensate acutely ESC Guidelines for the Diagnosis and A clinical response
UPDATES IN MANAGEMENT OF HF
 UPDATES IN MANAGEMENT OF HF Jennifer R Brown MD, MS Heart Failure Specialist Medstar Cardiology Associates DC ACP Meeting Fall 2017 Disclosures: speaker bureau for novartis speaker bureau for actelion
UPDATES IN MANAGEMENT OF HF Jennifer R Brown MD, MS Heart Failure Specialist Medstar Cardiology Associates DC ACP Meeting Fall 2017 Disclosures: speaker bureau for novartis speaker bureau for actelion
Akash Ghai MD, FACC February 27, No Disclosures
 Akash Ghai MD, FACC February 27, 2015 No Disclosures Epidemiology Lifetime risk is > 20% for American s older than 40 years old. > 650,000 new cases diagnosed each year. Incidence increases with age: 2%
Akash Ghai MD, FACC February 27, 2015 No Disclosures Epidemiology Lifetime risk is > 20% for American s older than 40 years old. > 650,000 new cases diagnosed each year. Incidence increases with age: 2%
Heart Failure. Jay Shavadia
 Heart Failure Jay Shavadia Definition Clinical syndrome characterized by: Symptoms: breathlessness at rest or on exercise, fatigue, tiredness or ankle swelling AND Signs: tachycardia, tachypnea, pulmonary
Heart Failure Jay Shavadia Definition Clinical syndrome characterized by: Symptoms: breathlessness at rest or on exercise, fatigue, tiredness or ankle swelling AND Signs: tachycardia, tachypnea, pulmonary
Heart Failure Clinician Guide JANUARY 2018
 Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Heart Failure Clinician Guide JANUARY 2018 Introduction This evidence-based guideline summary is based on the 2018 National Heart Failure Guideline.
Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Heart Failure Clinician Guide JANUARY 2018 Introduction This evidence-based guideline summary is based on the 2018 National Heart Failure Guideline.
Heart Failure Therapies State of the Art 2017
 Heart Failure Therapies State of the Art 2017 Andrew J. Sauer, MD Assistant Professor Director, Center for Heart Failure Medical Director, Heart Transplantation UNOS Primary Transplant Physician asauer@kumc.edu
Heart Failure Therapies State of the Art 2017 Andrew J. Sauer, MD Assistant Professor Director, Center for Heart Failure Medical Director, Heart Transplantation UNOS Primary Transplant Physician asauer@kumc.edu
HFpEF. April 26, 2018
 HFpEF April 26, 2018 (J Am Coll Cardiol 2017;70:2476 86) HFpEF 50% or more (40-71%) of patients with CHF have preserved LV systolic function. HFpEF is an increasingly frequent hospital discharge. Outcomes
HFpEF April 26, 2018 (J Am Coll Cardiol 2017;70:2476 86) HFpEF 50% or more (40-71%) of patients with CHF have preserved LV systolic function. HFpEF is an increasingly frequent hospital discharge. Outcomes
State-of-the-Art Management of Chronic Systolic Heart Failure
 State-of-the-Art Management of Chronic Systolic Heart Failure Michael McCulloch, MD 17 th Annual Cardiovascular Update Intermountain Medical Center December 16, 2017 Disclosures: I have no financial disclosures
State-of-the-Art Management of Chronic Systolic Heart Failure Michael McCulloch, MD 17 th Annual Cardiovascular Update Intermountain Medical Center December 16, 2017 Disclosures: I have no financial disclosures
Process Improvement in Heart Failure Patient Care: Transitions From Door to Discharge and Beyond
 Process Improvement in Heart Failure Patient Care: Transitions From Door to Discharge and Beyond Steven Sheris, M.D., FACC, FACP Chief of Cardiology Gagnon Cardiovascular Institute at Overlook Medical
Process Improvement in Heart Failure Patient Care: Transitions From Door to Discharge and Beyond Steven Sheris, M.D., FACC, FACP Chief of Cardiology Gagnon Cardiovascular Institute at Overlook Medical
CLINICAL PRACTICE GUIDELINE
 CLINICAL PRACTICE GUIDELINE Procedure: Congestive Heart Failure Guideline Review Cycle: Biennial Reviewed By: Amish Purohit, MD, MHA, CPE, FACHE Review Date: November 2014 Committee Approval Date: 11/12/2014
CLINICAL PRACTICE GUIDELINE Procedure: Congestive Heart Failure Guideline Review Cycle: Biennial Reviewed By: Amish Purohit, MD, MHA, CPE, FACHE Review Date: November 2014 Committee Approval Date: 11/12/2014
2017 Summer MAOFP Update
 2017 Summer MAOFP Update. Cardiology Update 2017 Landmark Trials Change Practice Guidelines David J. Strobl, DO, FNLA Heart Failure: Epidemiology More than 4 million patients affected 400,000 new cases
2017 Summer MAOFP Update. Cardiology Update 2017 Landmark Trials Change Practice Guidelines David J. Strobl, DO, FNLA Heart Failure: Epidemiology More than 4 million patients affected 400,000 new cases
Heart Failure 2014: It's No Longer about Failure
 Ohio-ACC Spring Summit 2014: 7th Annual CCA Cardiovascular Update & 51st Annual Carl J. Wiggers Memorial Lecture Heart Failure 2014: It's No Longer about Failure Clyde W. Yancy, MD, MSc, FACC, FAHA, MACP
Ohio-ACC Spring Summit 2014: 7th Annual CCA Cardiovascular Update & 51st Annual Carl J. Wiggers Memorial Lecture Heart Failure 2014: It's No Longer about Failure Clyde W. Yancy, MD, MSc, FACC, FAHA, MACP
OHSU HEALTH SYSTEM OFFICE OF CLINICAL INTEGRATION AND EVIDENCE-BASED PRACTICE
 OHSU HEALTH SYSTEM OFFICE OF CLINICAL INTEGRATION AND EVIDENCE-BASED PRACTICE GUIDELINE FOR THE MANAGEMENT OF HEART FAILURE Background: Heart failure (HF) is a complex clinical syndrome that results from
OHSU HEALTH SYSTEM OFFICE OF CLINICAL INTEGRATION AND EVIDENCE-BASED PRACTICE GUIDELINE FOR THE MANAGEMENT OF HEART FAILURE Background: Heart failure (HF) is a complex clinical syndrome that results from
2 I. Reduced EF (HFrEF)
") HF Classification EF Description 2 I. Reduced EF (HFrEF) 40% 1. Referred to as systolic HF. 2. Randomized trials mainly enrolled patients with HFrEF. 3. Efficacious therapies is shown only in these patients.
HF Classification EF Description 2 I. Reduced EF (HFrEF) 40% 1. Referred to as systolic HF. 2. Randomized trials mainly enrolled patients with HFrEF. 3. Efficacious therapies is shown only in these patients.
Antialdosterone treatment in heart failure
 Update on the Treatment of Chronic Heart Failure 2012 Antialdosterone treatment in heart failure 전남의대윤현주 Chronic Heart Failure Prognosis of Heart failure Cecil, Text book of Internal Medicine, 22 th edition
Update on the Treatment of Chronic Heart Failure 2012 Antialdosterone treatment in heart failure 전남의대윤현주 Chronic Heart Failure Prognosis of Heart failure Cecil, Text book of Internal Medicine, 22 th edition
Chronic. Outline. Congestive^ Heart Failure: Update on Effective Monitoring and Treatment. Heart Failure Epidemiology. Michael G.
 Chronic Congestive^ Heart Failure: Update on Effective Monitoring and Treatment Michael G. Shlipak, MD, MPH Professor of Medicine, UCSF Chief, Division of General Internal Medicine, SFVA Medical Center
Chronic Congestive^ Heart Failure: Update on Effective Monitoring and Treatment Michael G. Shlipak, MD, MPH Professor of Medicine, UCSF Chief, Division of General Internal Medicine, SFVA Medical Center
Heart Failure with Reduced EF. Dino Recchia, MD, FACC, FHFSA
 Heart Failure with Reduced EF Dino Recchia, MD, FACC, FHFSA Heart Failure HF is the end phenotype of almost all CV disorders Complex clinical syndrome resulting from any structural or functional impairment
Heart Failure with Reduced EF Dino Recchia, MD, FACC, FHFSA Heart Failure HF is the end phenotype of almost all CV disorders Complex clinical syndrome resulting from any structural or functional impairment
Tuesday October 18, :00pm 2:00pm Central Presenter: Clyde W. Yancy, MD, MSc
 Tuesday October 18, 2016 1:00pm 2:00pm Central Presenter: Clyde W. Yancy, MD, MSc Amgen Cardiovascular proudly sponsors Heart Science Amplified: An Online Speaker Series and Get With The Guidelines -Heart
Tuesday October 18, 2016 1:00pm 2:00pm Central Presenter: Clyde W. Yancy, MD, MSc Amgen Cardiovascular proudly sponsors Heart Science Amplified: An Online Speaker Series and Get With The Guidelines -Heart
A patient with decompensated HF
 A patient with decompensated HF Professor Michel KOMAJDA University Pierre & Marie Curie Pitie Salpetriere Hospital Department of Cardiology Paris (France) Declaration Of Interest 2010 Speaker : Servier,
A patient with decompensated HF Professor Michel KOMAJDA University Pierre & Marie Curie Pitie Salpetriere Hospital Department of Cardiology Paris (France) Declaration Of Interest 2010 Speaker : Servier,
All in the Past? Win K. Shen, MD Mayo Clinic Arizona Controversies and Advances in CV Diseases Cedars-Sinai Heart Institute, MFMER
 ICD for NICM All in the Past? Win K. Shen, MD Mayo Clinic Arizona Controversies and Advances in CV Diseases Cedars-Sinai Heart Institute, 2017 2017 MFMER 3686275-1 DISCLOSURE Relevant Financial Relationship(s)
ICD for NICM All in the Past? Win K. Shen, MD Mayo Clinic Arizona Controversies and Advances in CV Diseases Cedars-Sinai Heart Institute, 2017 2017 MFMER 3686275-1 DISCLOSURE Relevant Financial Relationship(s)
Keynote Address II Managing Acute Heart Failure: What Can We Do to Improve Outcomes?
 Keynote Address II Managing Acute Heart Failure: What Can We Do to Improve Outcomes? 24 th Annual San Diego Heart Failure Symposium June 1-2, 2018 La Jolla, CA Barry Greenberg, MD Distinguished Professor
Keynote Address II Managing Acute Heart Failure: What Can We Do to Improve Outcomes? 24 th Annual San Diego Heart Failure Symposium June 1-2, 2018 La Jolla, CA Barry Greenberg, MD Distinguished Professor
Disclosures. Overview. Goal statement. Advances in Chronic Heart Failure Management 5/22/17
 Disclosures Advances in Chronic Heart Failure Management I have nothing to disclose Van N Selby, MD UCSF Advanced Heart Failure Program May 22, 2017 Goal statement To review recently-approved therapies
Disclosures Advances in Chronic Heart Failure Management I have nothing to disclose Van N Selby, MD UCSF Advanced Heart Failure Program May 22, 2017 Goal statement To review recently-approved therapies
Guideline-Directed Medical Therapy
 Guideline-Directed Medical Therapy Cardiovascular Outcomes Assessment of the MitraClip Percutaneous Therapy for Heart Failure Patients with Functional Mitral Regurgitation OPTIMAL THERAPY (As defined in
Guideline-Directed Medical Therapy Cardiovascular Outcomes Assessment of the MitraClip Percutaneous Therapy for Heart Failure Patients with Functional Mitral Regurgitation OPTIMAL THERAPY (As defined in
Heart Failure. Disclosures. Objectives: 8/28/2017. This is not a virus. It doesn t go away. none
 Heart Failure This is not a virus. It doesn t go away Shelley Wojtaszczyk, FNP-C, CHFN Heart Failure Program Coordinator Mercy Hospital of Buffalo none Disclosures Objectives: Defining and identifying
Heart Failure This is not a virus. It doesn t go away Shelley Wojtaszczyk, FNP-C, CHFN Heart Failure Program Coordinator Mercy Hospital of Buffalo none Disclosures Objectives: Defining and identifying
Disclosures. Advances in Chronic Heart Failure Management 6/12/2017. Van N Selby, MD UCSF Advanced Heart Failure Program June 19, 2017
 Advances in Chronic Heart Failure Management Van N Selby, MD UCSF Advanced Heart Failure Program June 19, 2017 I have nothing to disclose Disclosures 1 Goal statement To review recently-approved therapies
Advances in Chronic Heart Failure Management Van N Selby, MD UCSF Advanced Heart Failure Program June 19, 2017 I have nothing to disclose Disclosures 1 Goal statement To review recently-approved therapies
WHAT S NEW IN HEART FAILURE
 WHAT S NEW IN HEART FAILURE Drugs, Devices and Diagnostics John M. Herre, MD, FACC, FACP Director, Advanced Heart Failure Program Sentara Helathcare Professor of Medicine Eastern Virginia Medical School
WHAT S NEW IN HEART FAILURE Drugs, Devices and Diagnostics John M. Herre, MD, FACC, FACP Director, Advanced Heart Failure Program Sentara Helathcare Professor of Medicine Eastern Virginia Medical School
Introduction to Heart Failure. Mauricio Velez, M.D. Transplant Cardiologist APACVS 2018 April 5-7 Miami, FL
 Introduction to Heart Failure Mauricio Velez, M.D. Transplant Cardiologist APACVS 2018 April 5-7 Miami, FL Disclosures No relevant financial relationships to disclose Objectives and Outline Define heart
Introduction to Heart Failure Mauricio Velez, M.D. Transplant Cardiologist APACVS 2018 April 5-7 Miami, FL Disclosures No relevant financial relationships to disclose Objectives and Outline Define heart
DISCLOSURES ACHIEVING SUCCESS THROUGH FAILURE: UPDATE ON HEART FAILURE WITH PRESERVED EJECTION FRACTION NONE
 ACHIEVING SUCCESS THROUGH FAILURE: UPDATE ON HEART FAILURE WITH PRESERVED EJECTION FRACTION Lori M. Tam, MD Providence Heart Institute DISCLOSURES NONE 1 OUTLINE Systolic vs. Diastolic Heart Failure New
ACHIEVING SUCCESS THROUGH FAILURE: UPDATE ON HEART FAILURE WITH PRESERVED EJECTION FRACTION Lori M. Tam, MD Providence Heart Institute DISCLOSURES NONE 1 OUTLINE Systolic vs. Diastolic Heart Failure New
Chronic. Outline. Congestive^ Heart Failure: Update on Effective Monitoring and Treatment. Heart Failure Epidemiology
 Chronic Congestive^ Heart Failure: Update on Effective Monitoring and Treatment Michael G. Shlipak, MD, MPH Professor of Medicine, UCSF Chief, Division of General Internal Medicine, SFVA Medical Center
Chronic Congestive^ Heart Failure: Update on Effective Monitoring and Treatment Michael G. Shlipak, MD, MPH Professor of Medicine, UCSF Chief, Division of General Internal Medicine, SFVA Medical Center
Long-Term Care Updates
 Long-Term Care Updates July 2015 By Amy Friedman Wilson, PharmD Heart failure (HF) is a clinical condition in which ventricular filling or ejection of blood is structurally or functionally impaired. 1
Long-Term Care Updates July 2015 By Amy Friedman Wilson, PharmD Heart failure (HF) is a clinical condition in which ventricular filling or ejection of blood is structurally or functionally impaired. 1
Heart Failure 101 The Basic Principles of Diagnosis & Management
 Heart Failure 101 The Basic Principles of Diagnosis & Management Bill Tran, MD Non Invasive Cardiologist February 24, 2018 What the eye does not see and the mind does not know, does not exist. DH Lawrence
Heart Failure 101 The Basic Principles of Diagnosis & Management Bill Tran, MD Non Invasive Cardiologist February 24, 2018 What the eye does not see and the mind does not know, does not exist. DH Lawrence
Heart Failure Medical and Surgical Treatment
 Heart Failure Medical and Surgical Treatment Daniel S. Yip, M.D. Medical Director, Heart Failure and Transplantation Mayo Clinic Second Annual Lakeland Regional Health Cardiovascular Symposium February
Heart Failure Medical and Surgical Treatment Daniel S. Yip, M.D. Medical Director, Heart Failure and Transplantation Mayo Clinic Second Annual Lakeland Regional Health Cardiovascular Symposium February
Outline. Chronic Heart Failure: Update on Effective Monitoring and Treatment. Heart Failure Epidemiology. Michael G.
 Chronic Heart Failure: Update on Effective Monitoring and Treatment Michael G. Shlipak, MD, MPH Professor of Medicine, UCSF Chief, Division of General Internal Medicine, SFVA Medical Center Scientific
Chronic Heart Failure: Update on Effective Monitoring and Treatment Michael G. Shlipak, MD, MPH Professor of Medicine, UCSF Chief, Division of General Internal Medicine, SFVA Medical Center Scientific
Chronic. Outline. Congestive^ Heart Failure: Update on Effective Monitoring and Treatment. Heart Failure Epidemiology. Michael G.
 Chronic Congestive^ Heart Failure: Update on Effective Monitoring and Treatment Michael G. Shlipak, MD, MPH Professor of Medicine, UCSF Chief, Division of General Internal Medicine, SFVA Medical Center
Chronic Congestive^ Heart Failure: Update on Effective Monitoring and Treatment Michael G. Shlipak, MD, MPH Professor of Medicine, UCSF Chief, Division of General Internal Medicine, SFVA Medical Center
Beta-blockers in Patients with Mid-range Left Ventricular Ejection Fraction after AMI Improved Clinical Outcomes
 Beta-blockers in Patients with Mid-range Left Ventricular Ejection Fraction after AMI Improved Clinical Outcomes Seung-Jae Joo and other KAMIR-NIH investigators Department of Cardiology, Jeju National
Beta-blockers in Patients with Mid-range Left Ventricular Ejection Fraction after AMI Improved Clinical Outcomes Seung-Jae Joo and other KAMIR-NIH investigators Department of Cardiology, Jeju National
Satish K Surabhi, MD.FACC,FSCAI,RPVI Medical Director, Cardiac Cath Labs AnMed Health Heart & Vascular Care
 Satish K Surabhi, MD.FACC,FSCAI,RPVI Medical Director, Cardiac Cath Labs AnMed Health Heart & Vascular Care None Fig. 1. Progression of Heart Failure.With each hospitalization for acute heart failure,
Satish K Surabhi, MD.FACC,FSCAI,RPVI Medical Director, Cardiac Cath Labs AnMed Health Heart & Vascular Care None Fig. 1. Progression of Heart Failure.With each hospitalization for acute heart failure,
Heart Failure: Combination Treatment Strategies
 Heart Failure: Combination Treatment Strategies M. McDonald MD, FRCP State of the Heart Symposium May 28, 2011 None Disclosures Case 69 F, prior MIs (LV ejection fraction 25%), HTN No demonstrable ischemia
Heart Failure: Combination Treatment Strategies M. McDonald MD, FRCP State of the Heart Symposium May 28, 2011 None Disclosures Case 69 F, prior MIs (LV ejection fraction 25%), HTN No demonstrable ischemia
Case (Coding Nightmare) Current Dilemmas in Heart Failure : Closing the Gap between Clinical Care and Coding. Current Dilemmas in Heart Failure :
 Current Dilemmas in Heart Failure : Closing the Gap between Clinical Care and Coding. Current Dilemmas in Heart Failure :") Current Dilemmas in Heart Failure : Closing the Gap between Clinical Care and Coding Interim Vice Chair for Clinical Affairs Department of Medicine, University of Florida 1 2 Case (Coding Nightmare) 69
Current Dilemmas in Heart Failure : Closing the Gap between Clinical Care and Coding Interim Vice Chair for Clinical Affairs Department of Medicine, University of Florida 1 2 Case (Coding Nightmare) 69
LITERATURE REVIEW: HEART FAILURE. Chief Residents
 LITERATURE REVIEW: HEART FAILURE Chief Residents Heart Failure EF 40% HFrEF Problem with contractility EF 40-50% HFmrEF EF > 50% HFpEF Problem with filling/relaxation RISK FACTORS Post MI HTN DM Obesity
LITERATURE REVIEW: HEART FAILURE Chief Residents Heart Failure EF 40% HFrEF Problem with contractility EF 40-50% HFmrEF EF > 50% HFpEF Problem with filling/relaxation RISK FACTORS Post MI HTN DM Obesity
2/3/2017. Objectives. Effective Heart Failure Management through Evidence Based Practice and Innovation
 Effective Heart Failure Management through Evidence Based Practice and Innovation Jennifer Bauerly RN, CHFN, APRN-BC CentraCare Heart and Vascular Center Objectives Describe the scope and impact of heart
Effective Heart Failure Management through Evidence Based Practice and Innovation Jennifer Bauerly RN, CHFN, APRN-BC CentraCare Heart and Vascular Center Objectives Describe the scope and impact of heart
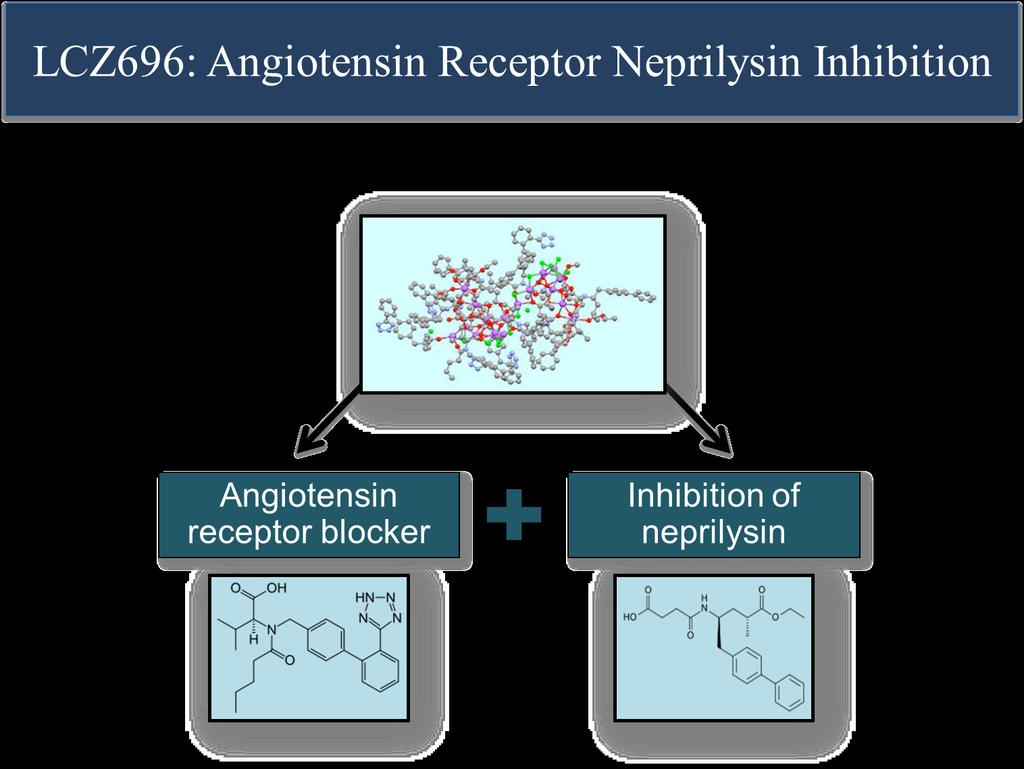
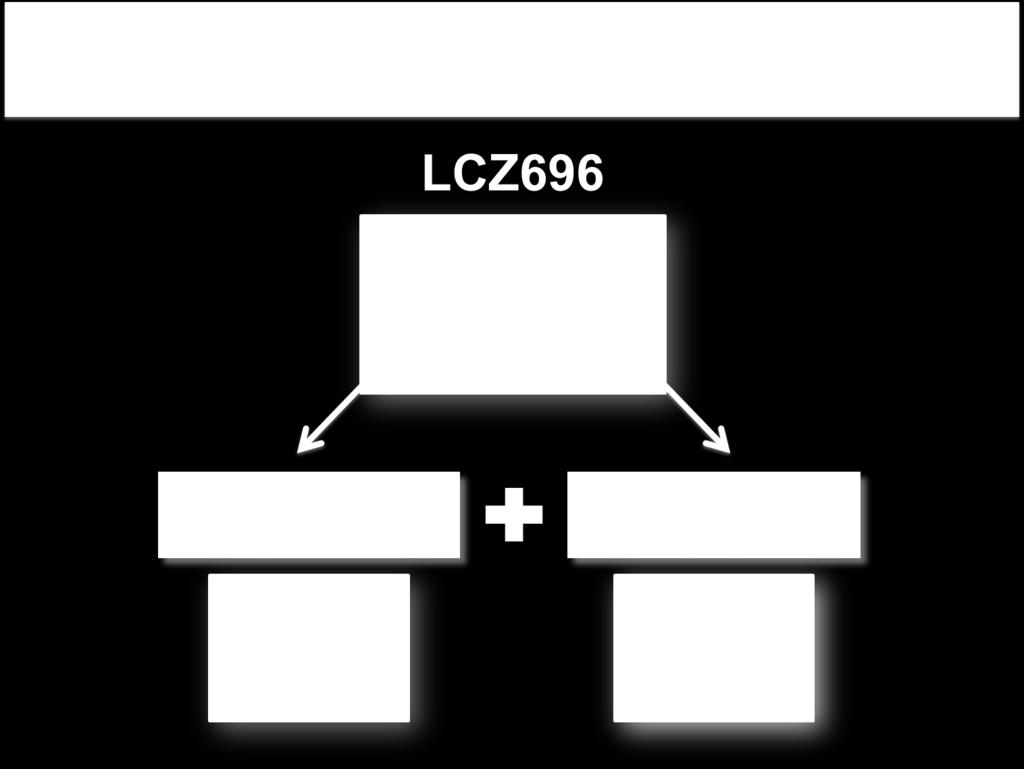
LCZ696 A First-in-Class Angiotensin Receptor Neprilysin Inhibitor
 The Angiotensin Receptor Neprilysin Inhibitor LCZ696 in Heart Failure with Preserved Ejection Fraction The Prospective comparison of ARNI with ARB on Management Of heart failure with preserved ejection
The Angiotensin Receptor Neprilysin Inhibitor LCZ696 in Heart Failure with Preserved Ejection Fraction The Prospective comparison of ARNI with ARB on Management Of heart failure with preserved ejection
CT Academy of Family Physicians Scientific Symposium October 2012 Amit Pursnani, MD
 CT Academy of Family Physicians Scientific Symposium October 2012 Amit Pursnani, MD Clinical syndrome resulting from a structural or functional cardiac disorder that impairs the ability of the heart to
CT Academy of Family Physicians Scientific Symposium October 2012 Amit Pursnani, MD Clinical syndrome resulting from a structural or functional cardiac disorder that impairs the ability of the heart to
ST2 in Heart Failure. ST2 as a Cardiovascular Biomarker. Competitive Model of ST2/IL-33 Signaling. ST2 and IL-33: Cardioprotective
 ST2 as a Cardiovascular Biomarker Lori B. Daniels, MD, MAS, FACC Professor of Medicine Director, Coronary Care Unit University of California, San Diego ST2 and IL-33: Cardioprotective ST2: member of the
ST2 as a Cardiovascular Biomarker Lori B. Daniels, MD, MAS, FACC Professor of Medicine Director, Coronary Care Unit University of California, San Diego ST2 and IL-33: Cardioprotective ST2: member of the
Heart Failure Background, recognition, diagnosis and management
 Heart Failure Background, recognition, diagnosis and management Speaker bureau: Novartis At the conclusion of this activity, participants will be able to: Recognize signs and symptoms of heart failure
Heart Failure Background, recognition, diagnosis and management Speaker bureau: Novartis At the conclusion of this activity, participants will be able to: Recognize signs and symptoms of heart failure
Heart Failure A Team Approach Background, recognition, diagnosis and management
 Heart Failure A Team Approach Background, recognition, diagnosis and management Speaker bureau: Novartis At the conclusion of this activity, participants will be able to: Recognize signs and symptoms of
Heart Failure A Team Approach Background, recognition, diagnosis and management Speaker bureau: Novartis At the conclusion of this activity, participants will be able to: Recognize signs and symptoms of
MEDICAL MANAGEMENT OF PATIENTS WITH HEART FAILURE AND REDUCED EJECTION FRACTION
 MEDICAL MANAGEMENT OF PATIENTS WITH HEART FAILURE AND REDUCED EJECTION FRACTION FRANCIS X. CELIS, D.O. OPSO FALL CONFERENCE PORTLAND, OR 16 SEPTEMBER 2017 OVERVIEW What are the ACC/AHA Stages of HF? What
MEDICAL MANAGEMENT OF PATIENTS WITH HEART FAILURE AND REDUCED EJECTION FRACTION FRANCIS X. CELIS, D.O. OPSO FALL CONFERENCE PORTLAND, OR 16 SEPTEMBER 2017 OVERVIEW What are the ACC/AHA Stages of HF? What
Diagnosing Heart Failure in Primary Care: Differentiating Zebras from Horses
 Diagnosing Heart Failure in Primary Care: Differentiating Zebras from Horses CANP March 2015 Maria Fe White, ACNP-BC Advanced Heart Disease Clinic Comprehensive Transplant Center Cedars-Sinai Medical Center
Diagnosing Heart Failure in Primary Care: Differentiating Zebras from Horses CANP March 2015 Maria Fe White, ACNP-BC Advanced Heart Disease Clinic Comprehensive Transplant Center Cedars-Sinai Medical Center
Advanced Care for Decompensated Heart Failure
 Advanced Care for Decompensated Heart Failure Sara Kalantari MD Assistant Professor of Medicine, University of Chicago Advanced Heart Failure, Mechanical Circulatory Support and Cardiac Transplantation
Advanced Care for Decompensated Heart Failure Sara Kalantari MD Assistant Professor of Medicine, University of Chicago Advanced Heart Failure, Mechanical Circulatory Support and Cardiac Transplantation
Guideline Management of Chronic Heart Failure
 Guideline Management of Chronic Heart Failure 2013 ACC/AHA Guideline Mgmt HF 2016 ACC/AHA/HFSA Focused Update 2017 ACCAHA/HFSA Focused Update October 17 th, 2017 Dawn Lombardo DO, MSc Professor of Medicine/Clinical
Guideline Management of Chronic Heart Failure 2013 ACC/AHA Guideline Mgmt HF 2016 ACC/AHA/HFSA Focused Update 2017 ACCAHA/HFSA Focused Update October 17 th, 2017 Dawn Lombardo DO, MSc Professor of Medicine/Clinical
WHAT IS ADVANCED HEART FAILURE? James C. Fang, MD, FACC Professor and Chief Cardiovascular Division University of Utah School of Medicine
 WHAT IS ADVANCED HEART FAILURE? James C. Fang, MD, FACC Professor and Chief Cardiovascular Division University of Utah School of Medicine Disclosures Data Safety Monitoring Board SOPRANO (J&J), EVALUATE-HF
WHAT IS ADVANCED HEART FAILURE? James C. Fang, MD, FACC Professor and Chief Cardiovascular Division University of Utah School of Medicine Disclosures Data Safety Monitoring Board SOPRANO (J&J), EVALUATE-HF
Beyond ACE-inhibitors for Heart Failure. Jacob Townsend, MD NCVH Birmingham 2015
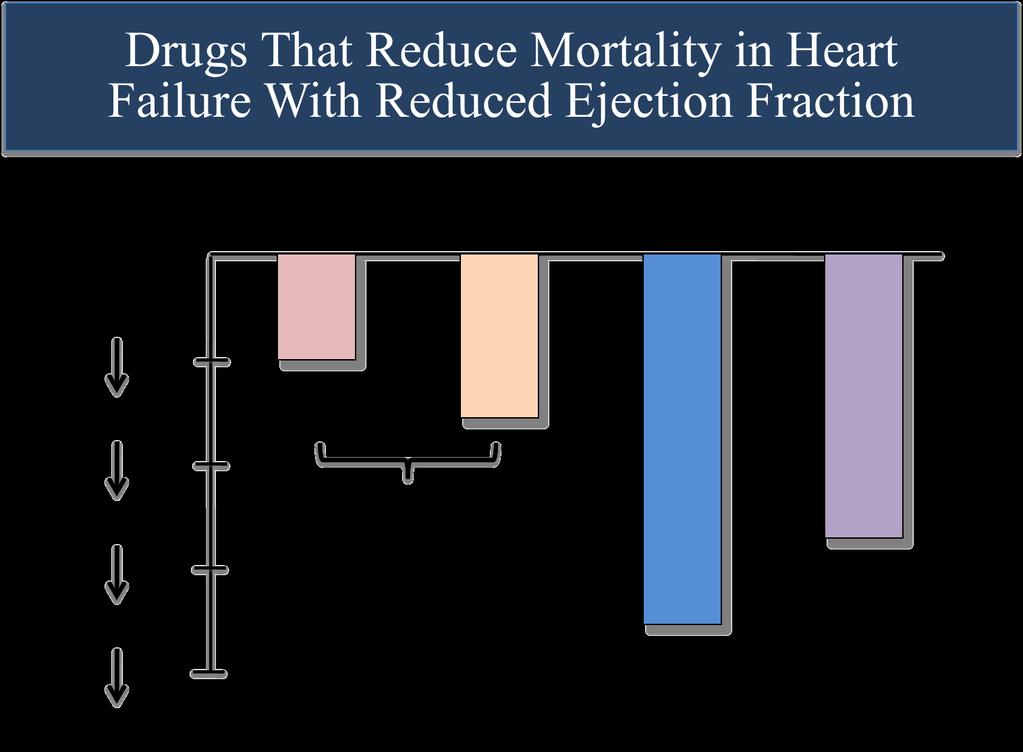
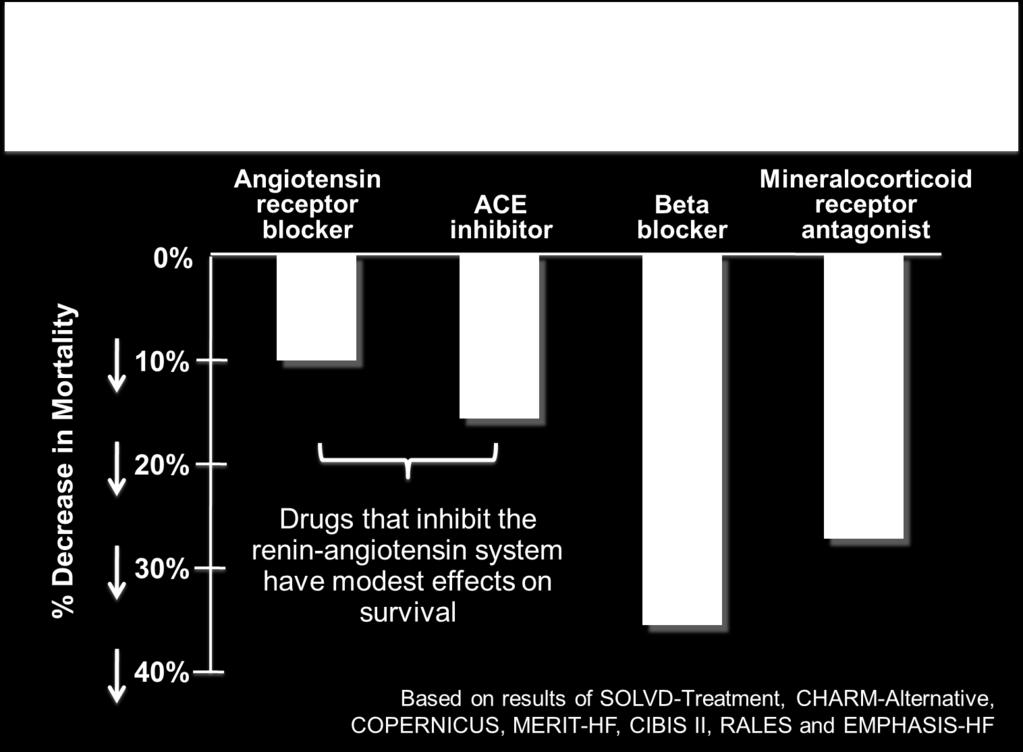
 Beyond ACE-inhibitors for Heart Failure Jacob Townsend, MD NCVH Birmingham 2015 % Decrease in Mortality Current Therapy HFrEF 0% Angiotensin receptor blocker ACE inhibitor Beta blocker Mineralocorticoid
Beyond ACE-inhibitors for Heart Failure Jacob Townsend, MD NCVH Birmingham 2015 % Decrease in Mortality Current Therapy HFrEF 0% Angiotensin receptor blocker ACE inhibitor Beta blocker Mineralocorticoid
Heart Failure. Dr. William Vosik. January, 2012
 Heart Failure Dr. William Vosik January, 2012 Questions for clinicians to ask Is this heart failure? What is the underlying cause? What are the associated disease processes? Which evidence-based treatment
Heart Failure Dr. William Vosik January, 2012 Questions for clinicians to ask Is this heart failure? What is the underlying cause? What are the associated disease processes? Which evidence-based treatment
Incidence. 4.8 million in the United States. 400,000 new cases/year. 20 million patients with asymptomatic LV dysfunction
 Heart Failure Diagnosis According to the Working Group in Heart Failure, CHF is a syndrome where the diagnosis has the following essential components: A combination of: Symptoms, typically breathlessness
Heart Failure Diagnosis According to the Working Group in Heart Failure, CHF is a syndrome where the diagnosis has the following essential components: A combination of: Symptoms, typically breathlessness
CRT Vs RV Pacing Benefits
 CRT-P & CRT-D Indications According to Guidelines are Guidelines Fully Adopted? Salama H. Omar M.D. Prof. Critical Care Medicine, Cairo University CRT Vs RV Pacing Benefits 1 Benefit of Upgrade CTR-P &
CRT-P & CRT-D Indications According to Guidelines are Guidelines Fully Adopted? Salama H. Omar M.D. Prof. Critical Care Medicine, Cairo University CRT Vs RV Pacing Benefits 1 Benefit of Upgrade CTR-P &
New CHF Patient in my Office: What Should I Do?
 New CHF Patient in my Office: What Should I Do? Joseph Mishkin MD FACC Advanced Heart Failure, Transplantation and Mechanical Circulatory Support No disclosures Disclosures Clinical Presentation 38 year
New CHF Patient in my Office: What Should I Do? Joseph Mishkin MD FACC Advanced Heart Failure, Transplantation and Mechanical Circulatory Support No disclosures Disclosures Clinical Presentation 38 year
Neprilysin Inhibitor (Entresto ) Prior Authorization and Quantity Limit Program Summary
 Prior Authorization and Quantity Limit Program Summary") Neprilysin Inhibitor (Entresto ) Prior Authorization and Quantity Limit Program Summary FDA APPROVED INDICATIONS DOSAGE 1 Indication Entresto Reduce the risk of cardiovascular (sacubitril/valsartan) death
Neprilysin Inhibitor (Entresto ) Prior Authorization and Quantity Limit Program Summary FDA APPROVED INDICATIONS DOSAGE 1 Indication Entresto Reduce the risk of cardiovascular (sacubitril/valsartan) death
Performance and Quality Measures 1. NQF Measure Number. Coronary Artery Disease Measure Set
 Unless indicated, the PINNACLE Registry measures are endorsed by the American College of Cardiology Foundation and the American Heart Association and may be used for purposes of health care insurance payer
Unless indicated, the PINNACLE Registry measures are endorsed by the American College of Cardiology Foundation and the American Heart Association and may be used for purposes of health care insurance payer
Disclosures for Presenter
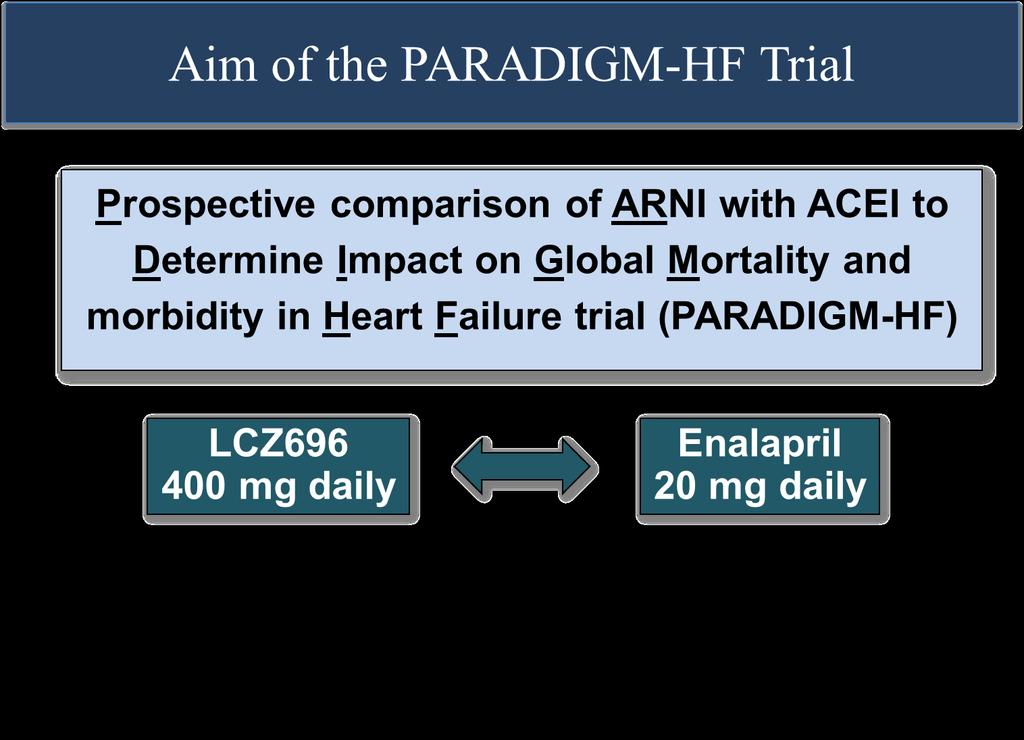
 A Comparison of Angiotensin Receptor- Neprilysin Inhibition (ARNI) With ACE Inhibition in the Long-Term Treatment of Chronic Heart Failure With a Reduced Ejection Fraction Milton Packer, John J.V. McMurray,
A Comparison of Angiotensin Receptor- Neprilysin Inhibition (ARNI) With ACE Inhibition in the Long-Term Treatment of Chronic Heart Failure With a Reduced Ejection Fraction Milton Packer, John J.V. McMurray,
Aldosterone Antagonism in Heart Failure: Now for all Patients?
 Aldosterone Antagonism in Heart Failure: Now for all Patients? Inder Anand, MD, FRCP, D Phil (Oxon.) Professor of Medicine, University of Minnesota, Director Heart Failure Program, VA Medical Center 111C
Aldosterone Antagonism in Heart Failure: Now for all Patients? Inder Anand, MD, FRCP, D Phil (Oxon.) Professor of Medicine, University of Minnesota, Director Heart Failure Program, VA Medical Center 111C
Online Appendix (JACC )
") Beta blockers in Heart Failure Collaborative Group Online Appendix (JACC013117-0413) Heart rate, heart rhythm and prognostic effect of beta-blockers in heart failure: individual-patient data meta-analysis
Beta blockers in Heart Failure Collaborative Group Online Appendix (JACC013117-0413) Heart rate, heart rhythm and prognostic effect of beta-blockers in heart failure: individual-patient data meta-analysis
I have no disclosures. Disclosures
 I have no disclosures Disclosures What is Heart Failure? Heart Failure (HF) A complex clinical syndrome where patients present with symptoms (i.e. dyspnea, fatigue, fluid retention) that result from any
I have no disclosures Disclosures What is Heart Failure? Heart Failure (HF) A complex clinical syndrome where patients present with symptoms (i.e. dyspnea, fatigue, fluid retention) that result from any
Outline. Pathophysiology: Heart Failure. Heart Failure. Heart Failure: Definitions. Etiologies. Etiologies
 Outline Pathophysiology: Mat Maurer, MD Irving Assistant Professor of Medicine Definitions and Classifications Epidemiology Muscle and Chamber Function Pathophysiology : Definitions An inability of the
Outline Pathophysiology: Mat Maurer, MD Irving Assistant Professor of Medicine Definitions and Classifications Epidemiology Muscle and Chamber Function Pathophysiology : Definitions An inability of the
2016 ESC Heart Failure Guidelines: what is new? Piotr Ponikowski Wroclaw, Poland
 2016 ESC Heart Failure Guidelines: what is new? Piotr Ponikowski Wroclaw, Poland Disclosures Consultancy fees and speaker s honoraria from: Amgen, Servier, Novartis, Johnson & Johnson, Merck, Berlin Chemie,
2016 ESC Heart Failure Guidelines: what is new? Piotr Ponikowski Wroclaw, Poland Disclosures Consultancy fees and speaker s honoraria from: Amgen, Servier, Novartis, Johnson & Johnson, Merck, Berlin Chemie,
What s new in heart failure management? Yonsei Cardiovascular Center Yonsei University College of Medicine
 What s new in heart failure management? Yonsei Cardiovascular Center Yonsei University College of Medicine Current Guideline of Treatment Asymptomatic Mild/Mod Severe Refractory Correct Cause: Arrhythmias
What s new in heart failure management? Yonsei Cardiovascular Center Yonsei University College of Medicine Current Guideline of Treatment Asymptomatic Mild/Mod Severe Refractory Correct Cause: Arrhythmias
The CCS Heart Failure Companion: Bridging Guidelines to your Practice
 The CCS Heart Failure Companion: Bridging Guidelines to your Practice Looking for practical answers concerning optimal heart failure care? The CCS Heart Failure Guidelines Companion can help. The Canadian
The CCS Heart Failure Companion: Bridging Guidelines to your Practice Looking for practical answers concerning optimal heart failure care? The CCS Heart Failure Guidelines Companion can help. The Canadian
Therapeutic Targets and Interventions
 Therapeutic Targets and Interventions Ali Valika, MD, FACC Advanced Heart Failure and Pulmonary Hypertension Advocate Medical Group Midwest Heart Foundation Disclosures: 1. Novartis: Speaker Honorarium
Therapeutic Targets and Interventions Ali Valika, MD, FACC Advanced Heart Failure and Pulmonary Hypertension Advocate Medical Group Midwest Heart Foundation Disclosures: 1. Novartis: Speaker Honorarium
8:30-10:30 WS #4: Cardiology :00-13:00 WS #11: Cardiology 101 (Repeated)
") Professor Ralph Stewart Cardiologist Auckland City Hospital Green Lane Cardiovascular Research Unit Auckland Heart Group Fiona Stewart Cardiologist Green Lane Hospital National Women's Hospital Professor
Professor Ralph Stewart Cardiologist Auckland City Hospital Green Lane Cardiovascular Research Unit Auckland Heart Group Fiona Stewart Cardiologist Green Lane Hospital National Women's Hospital Professor