Coronary Artery Calcium: Absence Makes the Heart Younger?
|
|
|
- Gary Boone
- 5 years ago
- Views:
Transcription

1 Coronary Artery Calcium: Absence Makes the Heart Younger? Parag H. Joshi, MD, MHS, FACC Assistant Professor of Medicine Division of Cardiology University of Texas Southwestern Medical Center Department of Internal Medicine Grand Rounds September 22, 2017 This is to acknowledge that Parag H. Joshi, M.D. has disclosed that he does not have any financial interests or other relationships with commercial concerns related directly or indirectly to this program. Dr. Joshi will not be discussing off-label uses in his presentation. 1
2 Parag H. Joshi, MD, MHS, FACC Assistant Professor of Medicine, Division of Cardiology, Department of Internal Medicine Director, Cardiology Grand Rounds University of Texas Southwestern Medical Center Biography: Dr. Joshi earned his medical degree at Texas Tech University School of Medicine. He completed an internal medicine residency at Emory University School of Medicine in He served as a Prevention Fellow at the Piedmont Heart Institute in Atlanta until 2011 before joining the Johns Hopkins School of Medicine where he completed a combined clinical and research fellowship in cardiovascular medicine. He was an inaugural Pollin Fellow in Cardiovascular Prevention which supported a Masters in Health Science in Clinical Investigation from the Johns Hopkins Bloomberg School of Public Health. Dr. Joshi joined the UT Southwestern faculty in He is a preventive cardiologist with special expertise atherosclerotic cardiovascular disease risk assessment and in noninvasive imaging. Dr. Joshi is certified by the American Board of Internal Medicine in both internal medicine and cardiovascular diseases and he also holds subspecialty certifications in cardiovascular computed tomography and adult echocardiography. Dr. Joshi is active in both research and patient care. His research focuses on cardiovascular disease, risk assessment, non-invasive coronary artery imaging, and lipids. He is a member of professional organizations that include the American Heart Association and the American College of Cardiology. Purpose and Overview: The purpose of this presentation is to discuss the utility of coronary artery calcium scoring in cardiovascular risk assessment and its potential role in shareddecision making between clinicians and patients in the primary prevention of atherosclerotic cardiovascular disease. Objectives: At the conclusion of this lecture, the listener should be able to a) Describe the association of coronary artery calcification with atherosclerotic cardiovascular disease; b) Recognize the importance of the absence of coronary artery calcium; c) Understand the potential role of coronary artery calcium in primary prevention and shared decision making under the current paradigm of the 2013 ACC/AHA guidelines; and d) Identify areas for future investigation of coronary artery calcium scoring as it relates to cardiovascular disease risk. 2

3 Current Paradigm of Primary Prevention In 2013, the American College of Cardiology/American Heart Association (ACC/AHA) released their paradigm shifting guidelines focusing on prioritizing statin treatment over other lipid lowering therapies for primary and secondary prevention. The guidelines for cardiovascular risk assessment introduced the pooled cohort equations (PCE) for estimating the 10-year risk of developing a first atherosclerotic cardiovascular disease (ASCVD) event. 1 Simultaneously, the ACC/AHA published guidelines addressing the treatment of blood cholesterol to reduce ASCVD. 2 The two guidelines shifted the field in several ways, and though there was some controversy, there were also several strengths. First, an emphasis was placed on weighing the absolute risk and benefits of statin therapy and other lipid lowering therapies were relegated to second line agents given a paucity of data supporting their use above statins at the time. The guidelines recommended 4 statin benefit groups, with the fourth group being the most controversial (Figure 1). Second, there was an expansion to a combined endpoint of ASCVD, comprised of fatal and non-fatal strokes, non-fatal myocardial infarctions (MI) and fatal coronary heart disease (CHD) events rather than only CHD events. Third, the risk assessment group developed a new ASCVD risk estimator from more contemporary cardiovascular cohort data, specifically including separate terms for Caucasian and African American populations, as well as for men and women. The prior approach relied on the Framingham risk estimate, mainly to predict CHD events, though this approach notably may have missed the majority of first heart attacks in younger adults. 3 Finally, and perhaps most importantly, the guidelines placed a heavy emphasis on shared decision making in the primary prevention group, highlighted by the clinician-patient discussion (Figure 1, yellow box). 3
 would be classified under the four statin benefit groups.")
4 While the new risk estimator represented an advance on several fronts, there were concerns about its implications. Pencina, et al applied the ACC/AHA cholesterol guidelines to the National Health and Nutrition Examination Surveys and found that 56 million U.S. adults (nearly 50%) would be classified under the four statin benefit groups. 4 This increased the statin eligible population by 12.8 million compared with prior guidelines, with the majority (10.4 million) belonging to the primary prevention group. Importantly, this was almost entirely driven by age as the dominant risk factor in the new risk estimator (Figure 2, red circle). The current guideline-based approach results in a higher sensitivity (statins recommended for adults who would develop ASCVD in the future) at the expense of lower specificity (statins recommended for adults who would not develop ASCVD in the future) compared to prior guidelines. 5 The increased eligibility for statin use per the ACC/AHA guidelines highlights an unmet need to refine cardiovascular risk assessment techniques, particularly to identify patients who are at lower risk for developing ASCVD events but are recommended statins. Non-traditional risk markers might be a solution to this problem as they can improve cardiovascular risk assessment and can guide preventive treatment decision making. Among non-traditional markers, coronary artery calcium (CAC) scoring has consistently improved risk-discrimination and correctly re-classified individuals to appropriate risk categories as reviewed below. Significance of Coronary Arterial Calcification Coronary artery calcification (CAC) is limited to the subintimal space of the arterial wall. It can begin as early as the second decade of life and is nearly pathognomonic for atherosclerosis. It is an active process with similarities to bone formation involving bone- 4

5 morphogenic proteins, osteoblasts, and calcium phosphate hydroxyapatite. Calcification occurs adjacent to inflammatory cells in the lipid core and is probably initiated by apoptosis of smooth muscles cells along a framework of extracellular matrix deposited by macrophages. 6 There is a direct relationship between coronary calcium burden and overall plaque burden such that calcified plaque represents approximately 20% of overall plaque burden. 7 On the causal pathway to ASCVD events, CAC is a marker of subclinical atherosclerosis which integrates exposure to both measured and unmeasured risk factors (Figure 3). Importantly, CAC is highly specific for some coronary atherosclerosis, and highly sensitive for clinically important coronary artery disease in that there is a high negative predictive value for obstructive CAD when CAC=0. A high CAC score is more likely to reflect obstructive disease, but overall, CAC is a poor marker for obstructive CAD (i.e. >70% coronary artery stenosis). 7 Association of CAC with ASCVD Risk Several studies have highlighted the ability of CAC to independently predict ASCVD events. The landmark cohort Multi-Ethnic Study of Atherosclerosis (MESA) demonstrated an independent association of CAC with incident CHD among four ethnic groups across 6 cities in the US. 8 The Dallas Heart Study provided important confirmation of this association in a younger multi-ethnic population recruited from Dallas County. 9 Most importantly, CAC consistently improves discrimination and reclassification above and beyond traditional risk factor assessment (Figure 4). 9 5

6 While prior studies focused on CHD risk, Yeboah et al evaluated the performance of CAC to predict ASCVD in MESA above and beyond both the Framingham risk score and the Pooled Cohort Equations calibrated to the MESA population. 10 CAC was compared to other non-traditional risk markers including high-sensitivity CRP, ankle-brachial index, as well as family history. CAC was the only marker to significantly improve discrimination above pooled cohort equation risk factors with a modest increase in the C-statistic from 0.74 to 0.76 (p 0.04). Similarly, in an analysis from the Heinz Nixdorf Recall study of CAC, carotid intima-media thickness, and ankle-brachial index added to traditional risk factors to discriminate ASCVD events, CAC led to the highest improvement in category-free net reclassification index (~55%). 11 The Role of CAC=0 CAC scoring is unique in that its absence is a strong indicator of low risk, especially over the short term. A series of studies showed that event rates over 4-5 years when CAC=0 are less than 1% (Table 1). 12 Recently, the longer-term implications of CAC=0 have become evident. Shaw, et al examined the national death index for all-cause mortality in an observational single-center study of over 9,500 patients who underwent clinically-indicated CAC scoring with nearly 15 years of followup. 13 Exactly half of the sample had CAC=0 with an all-cause mortality rate of 3% over 15 years compared with mortality rates of 14% or higher for those with CAC>100. These prior studies looked at short term events or long-term mortality when CAC=0. With the inclusion of stroke in the 2013 ACC/AHA guidelines, our group examined ASCVD events among MESA participants with CAC=0 using those with minimal CAC (1-10) as a 6

7 comparison over a median follow-up of 10 years, a benchmark in risk prediction. 14 We sought to examine event rates when CAC=0 across risk factor subgroups and across PCE risk categories. We also sought to understand the types of events that occur over 10 year follow-up and the risk factors that may predict these events when CAC=0. Among 6,814 MESA participants aged years old and without prior cardiovascular disease, there were 3,415 with CAC=0 and 508 with CAC 1-10 for comparisons. Over median follow-up of 10.3 years, among the group with CAC 0-10, there were 123 ASCVD events including 41 non-fatal MIs, 64 strokes, and 18 CHD deaths. The proportion of incident ASCVD events was similar between the CAC=0 and CAC 1-10 groups, highlighted by the finding that ~50% of these events were strokes. This is a significantly higher proportion of strokes among incident ASCVD than expected: strokes made up only 40% of the overall ASCVD events in the entire MESA study population. Upon further breakdown of the stroke data, a significant proportion (>40%) in which an etiology could be established were either hemorrhagic or cardio embolic, events that are not known to have a putative benefit from statins. The overall ASCVD event rates were 2.9/1,000 person years (~2.9% 10 year risk) among the CAC=0 group compared to 5.5/1,000 person years in the CAC 1-10 group, reflecting a nearly 2-fold increased hazard for ASCVD with even minimal CAC (Figure 5). 14 Across categories of risk factors and ASCVD risk categories, a CAC=0 heralded the lowest event rates (Figure 6), and none of the event rates exceeded the 7.5% 10-year risk established 7
8 by the 2013 ACC/AHA guidelines. Notably, even in those with PCE ASCVD risk up to 15%, the event rates were 4.4/1,000 person years (~4.4% 10 year risk). We also examined predictors of ASCVD among those with CAC=0 and minimal CAC. In multivariable models among CAC=0, only age (HR 1.5, 95%CI ), current smoking (HR 3.0; 95%CI ), and hypertension (HR 2.0; 95%CI ) significantly predict ASCVD. Similarly, among those with CAC 1-10, age and smoking remain significant predictors, but hypertension is a much stronger predictor (HR 9.9; 95%CI ) than for CAC=0 (p for interaction 0.02). We concluded that with ASCVD rates generally much lower than 7.5% when CAC=0, lifestyle modifications, smoking-cessation and hypertension-control should be top priorities. Among non-traditional markers, Blaha et al showed that CAC scoring is the strongest for de-risking an individual. 15 In this MESA analysis, multivariable adjusted diagnostic likelihood ratios (DLR) were used to assess the change from pretest risk to posttest risk in the presence of a negative risk marker (e.g. no family history of CHD, normal hscrp, CAC=0, etc ). Among all negative risk markers, CAC=0 was the strongest modifier of posttest risk with a mean DLR of 0.54 for CVD and 0.41 for CHD events (Figure 7). This suggests that on average, the posttest risk is 50% lower than the pretest risk when CAC=0; however, older participants and those with higher pre-test risk had lower average DLR. A zero CAC score resulted in the largest downward classification of risk with an NRI of approximately 14%. Finally, Nasir et al analyzed the ACC/AHA guidelines in a systematic fashion among the statin eligible MESA population in the context of CAC scoring. 16 Nearly half of the MESA study population would be recommended statins based on either LDL-C>190 mg/dl (4%), diabetes (19%) or a 10-year ASCVD risk 7.5%. Per the ACC/AHA guidelines, statins would be considered in another 12% of the study population because of a 10-year ASCVD risk between 5 and 7.5% and 38% of the population would not be recommended statins based on <5% 10 year ASCVD risk. The event rate among all MESA participants recommended for statins but with 8
.")
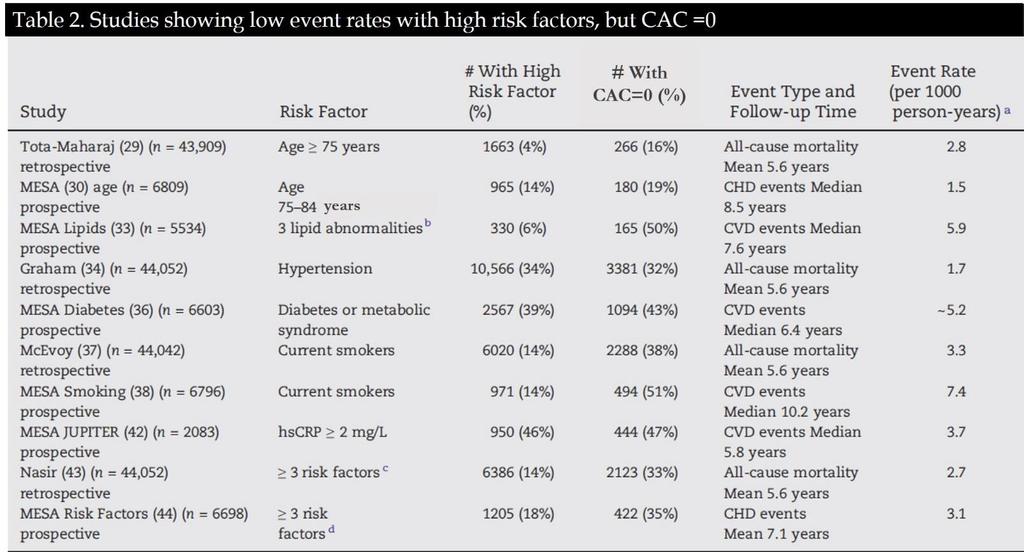
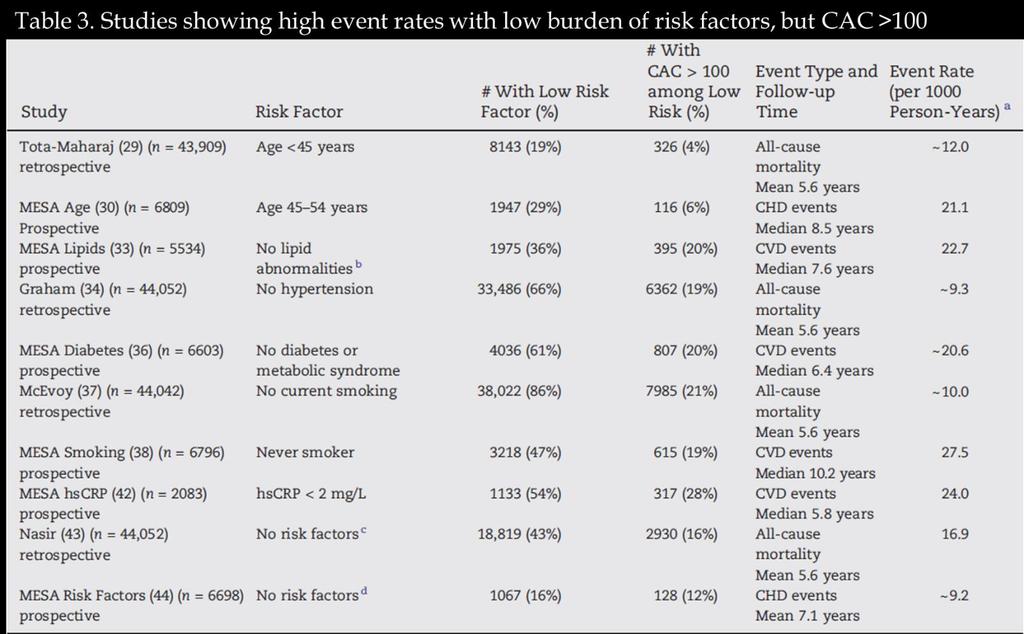
9 CAC=0 was 5.2/1,000 person years. 16 When examining this within estimated 10-year ACC/AHA pooled cohorts equation risk categories (Figure 8), those with 7.5 to 20% ASCVD risk and CAC=0 experienced only 4.6 ASCVD events per 1,000 person years (~4.6% 10 year risk). These studies show that there is significant heterogeneity between risk factors, risk estimates and burden of subclinical atherosclerosis. In a review of prospective and retrospective studies we examined the prevalence and event rates of both extremes: Presence of high risk factors with CAC=0 (Table 2) Presence of low risk factors with CAC>100 (Table 3). 17 We found that even in the presence of a high burden of traditional risk factors, the absence of CAC marked a low risk of events. On the other hand, among participants with normal values for traditional risk factors, a high CAC score (>100) marked a high risk of events. For example, Martin et al examined MESA participants by their burden of lipid abnormalities: high LDL-C, low HDL-C, or high triglycerides. 18 Approximately 20% of participants with no lipid abnormalities had CAC >100 and an ASCVD event rate of more than 20/1,000 person years over 7 years of follow-up. Conversely, approximately 50% of participants with 3 lipid abnormalities had CAC=0 and an ASCVD event rate of 5.9/1,000 person years. Similar findings are seen when examining extremes of age and burden of traditional risk factors (Tables 2 & 3). 17 9
10 10
, CKD (0.77, 0.60-0.98), COPD (0.61, 0.40-0.")
11 In a novel competing risks analysis from MESA, Handy et al examined the association of CAC with non-cvd outcomes over median 10.2 years followup. 19 In multi-variable adjusted analysis accounting for competing CVD events, those with CAC=0 had a decreased risk of incident cancer (0.76, ), CKD (0.77, ), COPD (0.61, ) and hip fracture (0.31, ) compared to those with CAC>0 (Figure 9). In summary, these studies suggest CAC=0 is a marker of health aging. Integrating CAC Scoring into Clinical Practice As stated previously, one of the major advances of the 2013 ACC/AHA guidelines was the codification of the clinician-patient discussion as an emphasis of shared decision making. There are several tools available from the MESA study to help integrate CAC scoring and results into the discussion with the patient ( One tool provides a reference percentile for the calcium score result in the context of the patient s age, gender, and ethnicity. Another provides an estimated arterial age calculator for the patient based on the calcium score result. The most useful tool provides a 10-year CHD risk estimate based off a combination of CAC score with traditional risk factors from MESA. 20 The score was validated in the Dallas Heart Study and the Heinz Nixdorf Recall Study and showed excellent discrimination in both validation populations (c-statistic 0.78 to 0.82). However, one key limitation is the inclusion of only CHD risk; a CVD risk estimator incorporating CAC scoring from MESA is currently in development. The 2013 ACC/AHA guidelines significantly increased the number of statin-eligible individuals; however, many patients may have an aversion to starting statins as a lifelong therapy in primary prevention. 4,21 With the large increase in statin-eligible patients, several studies have explored the role of CAC=0 to de-risk statin eligible patients. In general, these studies have assessed whether the ASCVD event rates in statin-indicated patients based on the guidelines are lower than the threshold for statin initiation when CAC=0. 11

12 In addition to the study by Nasir et al from MESA, Pursnani et al. also examined statin eligible participants from the Framingham offspring study who underwent CAC scoring and were followed for ASCVD events over 9.4 years. 22 They found the ACC/AHA guidelines were more accurate than the previous ATP III guidelines in discriminating those with incident ASCVD and those with prevalent subclinical atherosclerosis as measured by CAC (Figure 10). Across all CAC categories, the ACC/AHA guidelines increased statin eligibility. However, participants who were deemed eligible for statins by ACC/AHA criteria, but with CAC=0, had an ASCVD event rate of only 1.6%. Importantly, the event rate among statin ineligible participants did not increase significantly (1% to 1.1%) when reclassifying statin eligible participants with CAC=0 to statin ineligible. As opposed to a guideline based approach to statin eligibility, investigators applied trial eligibility criteria from 7 primary prevention statin trials to MESA participants. 23 The majority of MESA participants (73%) were eligible for statin therapy based on primary prevention statin RCT enrollment criteria. Approximately 45% of statin eligible MESA participants had CAC=0 and overall ASCVD event rates of 3.9/1,000 person years. Assuming a relative risk reduction of 30% from statin therapy, the number needed to treat to prevent one ASCVD event over 10 years among CAC=0 participants was 87. In contrast, among those with CAC>100, the number needed to treat was 19 (Figure 11). 12
 were eligible for statin therapy by ACC/AHA guidelines and 32% had CAC=0. The event rate among those with CAC=0 was 3.")
13 In using an atherosclerosis based approach to statin eligibility, Mortensen et al evaluated the utility of de-risking participants from the BioImage study with CAC=0. 24 Most of the study participants (86%) were eligible for statin therapy by ACC/AHA guidelines and 32% had CAC=0. The event rate among those with CAC=0 was 3.2/1,000 person years, well below the ACC/AHA 7.5% threshold. This imaging-based approach resulted in a binary NRI of 0.14 driven by down-classifying the 32% of the population with CAC=0 (Figure 12). 13
14 Lastly, investigators from the Heinz Nixdorf Recall study analyzed European guidelines and ACC/AHA guidelines in the context of CAC=0. 25 They found an event rate for ASCVD of 2.7/1,000 person years among participants who were eligible for statins but with CAC=0. This resulted in a NNT over 10 years to prevent an ASCVD event of 62 among those with CAC=0 and deemed eligible for statins by the ACC/AHA criteria, assuming a 30% relative risk reduction with statins. Similarly, the NNT was 59 among those deemed eligible for statins by European guidelines but with CAC=0. These studies strongly support the absence of CAC as a marker of low 10-year ASCVD risk despite statin eligibility by 2013 ACC/AHA pooled cohort risk estimation. They also show that CAC=0 is quite common among statin-eligible patients. In patients with CAC=0 and consequently low 10-year ASCVD event rate, statin therapy should be viewed as a means to reduce long term, or even lifelong risk, rather than 10 year benefit. The clinician-patient risk discussion over benefits and risks in such a scenario should encompass these considerations. Prevention encompasses more than just decisions over statin therapy. Recent work has evaluated the utility of CAC scoring to guide decisions for aspirin therapy and for systolic blood pressure targets. 26,27 In both cases, CAC=0 provides strong rationale to be less aggressive given the low absolute event rates for a fixed exposure to risk of therapy. Challenges to CAC Testing Coronary calcium scanning is available in most major cities and is typically not covered by insurance (with rare exception in Texas). The cost is approximately $100 in most major cities. Concerns over radiation exposure are valid given overall principles for limiting medical radiation exposure. With modern technology and approaches to CT imaging, the average radiation dose is approaching ~1 msv, or the equivalent of 2 mammograms. Finally, lung nodules or other incidental findings are present in up to 10% of studies which may stimulate further downstream testing and anxiety. Pre-scan counseling of patients about the possibility of incidental findings may be helpful in preventing anxiety and planning follow-up appropriately. There are justified criticisms of CAC scoring in that there has not been a screening trial to show that CAC scanning changes outcomes. This is partly due to ethical concerns over potentially randomizing patients with high CAC scores to placebo. Further, there are significant cost considerations as a randomized screening CAC trial has been estimated to require up to 30,000 patients and cost up to $100 million. 28 Creative solutions to approach this conundrum exist, and should be considered going forward (Figure 13)

15 McEvoy, et al. JACC CV Img. 2016;9(8): A CAC-based Approach to Primary Prevention Lifelong statin therapy in primary prevention can be intimidating for patients. In those patients who are reluctant to start a statin, but are otherwise eligible for statin therapy, CAC scoring can be particularly helpful. The absence of CAC can help reassure the patient and provider (for a few years at least) that the overall risk is low. While the absence of CAC does not indicate no-risk, it does reclassify many patients to ASCVD risk estimates below thresholds for statin initiation and suggests low 10-year risk. Based on the above evidence, one approach to 15
16 CAC scoring in the primary prevention of ASCVD is presented (Figure 14). CAC scanning should only be pursued if the result will impact decision making. If a patient is agreeable to starting a statin, then a CAC scan is not likely to help. It is mainly in the statin-reluctant patient that CAC scanning can be useful. Conclusion CAC is a well-validated marker of cardiovascular risk, but also a strong marker of low risk when absent. In the current approach to primary prevention of ASCVD there has been a large increase in the population deemed eligible for statins. Considering patient preferences and possible reluctance for starting lifelong therapies, CAC scoring is a highly valuable aid in shared decision making between the clinician and patient, particularly when CAC=0 in the statinreluctant patient. 16
17 References 1. Goff DC, Jr., Lloyd-Jones DM, Bennett G, et al ACC/AHA guideline on the assessment of cardiovascular risk: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. Circulation. 2014;129(25 Suppl 2):S Stone NJ, Robinson JG, Lichtenstein AH, et al ACC/AHA guideline on the treatment of blood cholesterol to reduce atherosclerotic cardiovascular risk in adults: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. Circulation. 2014;129(25 Suppl 2):S Akosah KO, Schaper A, Cogbill C, Schoenfeld P. Preventing myocardial infarction in the young adult in the first place: how do the National Cholesterol Education Panel III guidelines perform? J Am Coll Cardiol. 2003;41(9): Pencina MJ, Navar-Boggan AM, D'Agostino RB, Sr., et al. Application of new cholesterol guidelines to a population-based sample. N Engl J Med. 2014;370(15): Mehta A, Blaha M, Miller J, Joshi P. Coronary Artery Calcium Scoring: a Valuable Aid in Shared Decision Making Among Non-traditional Risk Markers. Curr Cardiovasc Imaging Rep. 2017;10(33). 6. Alexopoulos N, Raggi P. Calcification in atherosclerosis. Nat Rev Cardiol. 2009;6(11): O'Rourke RA, Brundage BH, Froelicher VF, et al. American College of Cardiology/American Heart Association Expert Consensus document on electron-beam computed tomography for the diagnosis and prognosis of coronary artery disease. Circulation. 2000;102(1): Detrano R, Guerci AD, Carr JJ, et al. Coronary calcium as a predictor of coronary events in four racial or ethnic groups. N Engl J Med. 2008;358(13): Paixao AR, Ayers CR, El Sabbagh A, et al. Coronary Artery Calcium Improves Risk Classification in Younger Populations. JACC Cardiovasc Imaging. 2015;8(11): Yeboah J, Young R, McClelland RL, et al. Utility of Nontraditional Risk Markers in Atherosclerotic Cardiovascular Disease Risk Assessment. J Am Coll Cardiol. 2016;67(2): Geisel MH, Bauer M, Hennig F, et al. Comparison of coronary artery calcification, carotid intimamedia thickness and ankle-brachial index for predicting 10-year incident cardiovascular events in the general population. Eur Heart J. 2017;38(23): Joshi PH, Blaha MJ, Blumenthal RS, Blankstein R, Nasir K. What is the role of calcium scoring in the age of coronary computed tomographic angiography? J Nucl Cardiol. 2012;19(6): Shaw LJ, Giambrone AE, Blaha MJ, et al. Long-Term Prognosis After Coronary Artery Calcification Testing in Asymptomatic Patients: A Cohort Study. Ann Intern Med. 2015;163(1): Joshi PH, Blaha MJ, Budoff MJ, et al. The 10-Year Prognostic Value of Zero and Minimal CAC. JACC Cardiovasc Imaging. 2017;10(8): Blaha MJ, Cainzos-Achirica M, Greenland P, et al. Role of Coronary Artery Calcium Score of Zero and Other Negative Risk Markers for Cardiovascular Disease: The Multi-Ethnic Study of Atherosclerosis (MESA). Circulation. 2016;133(9): Nasir K, Bittencourt MS, Blaha MJ, et al. Implications of Coronary Artery Calcium Testing Among Statin Candidates According to American College of Cardiology/American Heart Association Cholesterol Management Guidelines: MESA (Multi-Ethnic Study of Atherosclerosis). J Am Coll Cardiol. 2015;66(15): Joshi PH, Nasir K. Discordance between Risk Factors and Coronary Artery Calcium: Implications for Guiding Treatment Strategies in Primary Prevention Settings. Prog Cardiovasc Dis. 2015;58(1):
18 18. Martin SS, Blaha MJ, Blankstein R, et al. Dyslipidemia, coronary artery calcium, and incident atherosclerotic cardiovascular disease: implications for statin therapy from the multi-ethnic study of atherosclerosis. Circulation. 2014;129(1): Handy CE, Desai CS, Dardari ZA, et al. The Association of Coronary Artery Calcium With Noncardiovascular Disease: The Multi-Ethnic Study of Atherosclerosis. JACC Cardiovasc Imaging. 2016;9(5): McClelland RL, Jorgensen NW, Budoff M, et al. 10-Year Coronary Heart Disease Risk Prediction Using Coronary Artery Calcium and Traditional Risk Factors: Derivation in the MESA (Multi- Ethnic Study of Atherosclerosis) With Validation in the HNR (Heinz Nixdorf Recall) Study and the DHS (Dallas Heart Study). J Am Coll Cardiol. 2015;66(15): Fontana M, Asaria P, Moraldo M, et al. Patient-accessible tool for shared decision making in cardiovascular primary prevention: balancing longevity benefits against medication disutility. Circulation. 2014;129(24): Pursnani A, Massaro JM, D'Agostino RB, Sr., O'Donnell CJ, Hoffmann U. Guideline-Based Statin Eligibility, Coronary Artery Calcification, and Cardiovascular Events. JAMA. 2015;314(2): Mortensen MB, Falk E, Li D, et al. Statin Trials, Cardiovascular Events, and Coronary Artery Calcification: Implications for a Trial-Based Approach to Statin Therapy in MESA. JACC Cardiovasc Imaging Mortensen MB, Fuster V, Muntendam P, et al. A Simple Disease-Guided Approach to Personalize ACC/AHA-Recommended Statin Allocation in Elderly People: The BioImage Study. J Am Coll Cardiol. 2016;68(9): Mahabadi AA, Mohlenkamp S, Lehmann N, et al. CAC Score Improves Coronary and CV Risk Assessment Above Statin Indication by ESC and AHA/ACC Primary Prevention Guidelines. JACC Cardiovasc Imaging. 2017;10(2): Miedema MD, Duprez DA, Misialek JR, et al. Use of coronary artery calcium testing to guide aspirin utilization for primary prevention: estimates from the multi-ethnic study of atherosclerosis. Circ Cardiovasc Qual Outcomes. 2014;7(3): McEvoy JW, Martin SS, Dardari ZA, et al. Coronary Artery Calcium to Guide a Personalized Risk- Based Approach to Initiation and Intensification of Antihypertensive Therapy. Circulation. 2017;135(2): Ambrosius WT, Polonsky TS, Greenland P, et al. Design of the value of imaging in enhancing the wellness of your heart (VIEW) trial and the impact of uncertainty on power. Clin Trials. 2012;9(2): McEvoy JW, Martin SS, Blaha MJ, et al. The Case For and Against a Coronary Artery Calcium Trial: Means, Motive, and Opportunity. JACC Cardiovasc Imaging. 2016;9(8):
New Paradigms in Predicting CVD Risk
 New Paradigms in Predicting CVD Risk Imaging as an Integrator of Lifetime Risk Exposure Michael J. Blaha MD MPH Presented by: Michael J. Blaha September 24, 2014 1 Talk Outline Risk factors vs. Disease
New Paradigms in Predicting CVD Risk Imaging as an Integrator of Lifetime Risk Exposure Michael J. Blaha MD MPH Presented by: Michael J. Blaha September 24, 2014 1 Talk Outline Risk factors vs. Disease
Financial Disclosures. Coronary Artery Calcification. Objectives. Coronary Artery Calcium 6/6/2018. Heart Disease Statistics At-a-Glace 2017
 Coronary Artery Calcification Dharmendra A. Patel, MD MPH Director, Echocardiography Laboratory Associate Program Director Cardiovascular Disease Fellowship Program Erlanger Heart and Lung Institute UT
Coronary Artery Calcification Dharmendra A. Patel, MD MPH Director, Echocardiography Laboratory Associate Program Director Cardiovascular Disease Fellowship Program Erlanger Heart and Lung Institute UT
Khurram Nasir, MD MPH
 Non-invasive CAD Screening Khurram Nasir, MD MPH Disclosures I have no relevant commercial relationships to disclose, and my presentation will not include off label or unapproved usage. HOW & WHAT WOULD
Non-invasive CAD Screening Khurram Nasir, MD MPH Disclosures I have no relevant commercial relationships to disclose, and my presentation will not include off label or unapproved usage. HOW & WHAT WOULD
Subclinical atherosclerosis in CVD: Risk stratification & management Raul Santos, MD
 Subclinical atherosclerosis in CVD: Risk stratification & management Raul Santos, MD Sao Paulo Medical School Sao Paolo, Brazil Subclinical atherosclerosis in CVD risk: Stratification & management Prof.
Subclinical atherosclerosis in CVD: Risk stratification & management Raul Santos, MD Sao Paulo Medical School Sao Paolo, Brazil Subclinical atherosclerosis in CVD risk: Stratification & management Prof.
Atherosclerotic Disease Risk Score
 Atherosclerotic Disease Risk Score Kavita Sharma, MD, FACC Diplomate, American Board of Clinical Lipidology Director of Prevention, Cardiac Rehabilitation and the Lipid Management Clinics September 16,
Atherosclerotic Disease Risk Score Kavita Sharma, MD, FACC Diplomate, American Board of Clinical Lipidology Director of Prevention, Cardiac Rehabilitation and the Lipid Management Clinics September 16,
Coronary Artery Calcification
 Coronary Artery Calcification Julianna M. Czum, MD OBJECTIVES CORONARY ARTERY CALCIFICATION Julianna M. Czum, MD Dartmouth-Hitchcock Medical Center 1. To review the clinical significance of coronary heart
Coronary Artery Calcification Julianna M. Czum, MD OBJECTIVES CORONARY ARTERY CALCIFICATION Julianna M. Czum, MD Dartmouth-Hitchcock Medical Center 1. To review the clinical significance of coronary heart
Imaging-Guided Statin Allocation: Seeing Is Believing
 Imaging-Guided Statin Allocation: Seeing Is Believing The New Paradigm in Personalized Risk Assessment & Medication Prescribing Presented by: Michael J. Blaha May 15, 2014 1 General Principles of Talk
Imaging-Guided Statin Allocation: Seeing Is Believing The New Paradigm in Personalized Risk Assessment & Medication Prescribing Presented by: Michael J. Blaha May 15, 2014 1 General Principles of Talk
Learning Objectives. Predicting and Preventing Cardiovascular Disease. ACC/AHA Cholesterol Guidelines Key differences vs ATP III
 Presenter Disclosure Information 10:30 11:15am Predicting and Preventing Cardiovascular Disease: Can we put the Cardiologist out of business? The following relationships exist related to this presentation:
Presenter Disclosure Information 10:30 11:15am Predicting and Preventing Cardiovascular Disease: Can we put the Cardiologist out of business? The following relationships exist related to this presentation:
CVD risk assessment using risk scores in primary and secondary prevention
 CVD risk assessment using risk scores in primary and secondary prevention Raul D. Santos MD, PhD Heart Institute-InCor University of Sao Paulo Brazil Disclosure Honoraria for consulting and speaker activities
CVD risk assessment using risk scores in primary and secondary prevention Raul D. Santos MD, PhD Heart Institute-InCor University of Sao Paulo Brazil Disclosure Honoraria for consulting and speaker activities
Are We Ready for a Paradigm Shift From Risk Factors to Detection of Subclinical Coronary Atherosclerosis? Lessons From MESA. Khurram Nasir, MD MPH
 Are We Ready for a Paradigm Shift From Risk Factors to Detection of Subclinical Coronary Atherosclerosis? Lessons From MESA Khurram Nasir, MD MPH Disclosures No disclosures. Burden of Cardiovascular Disease
Are We Ready for a Paradigm Shift From Risk Factors to Detection of Subclinical Coronary Atherosclerosis? Lessons From MESA Khurram Nasir, MD MPH Disclosures No disclosures. Burden of Cardiovascular Disease
9/18/2017 DISCLOSURES. Consultant: RubiconMD. Research: Amgen, NHLBI OUTLINE OBJECTIVES. Review current CV risk assessment tools.
 UW MEDICINE UW MEDICINE UCSF ASIAN TITLE HEALTH OR EVENT SYMPOSIUM 2017 DISCLOSURES Consultant: RubiconMD ESTIMATING CV RISK IN ASIAN AMERICANS AND PREVENTION OF CVD Research: Amgen, NHLBI EUGENE YANG,
UW MEDICINE UW MEDICINE UCSF ASIAN TITLE HEALTH OR EVENT SYMPOSIUM 2017 DISCLOSURES Consultant: RubiconMD ESTIMATING CV RISK IN ASIAN AMERICANS AND PREVENTION OF CVD Research: Amgen, NHLBI EUGENE YANG,
The recently released American College of Cardiology
 Data Report Atherosclerotic Cardiovascular Disease Prevention A Comparison Between the Third Adult Treatment Panel and the New 2013 Treatment of Blood Cholesterol Guidelines Andre R.M. Paixao, MD; Colby
Data Report Atherosclerotic Cardiovascular Disease Prevention A Comparison Between the Third Adult Treatment Panel and the New 2013 Treatment of Blood Cholesterol Guidelines Andre R.M. Paixao, MD; Colby
2013 ACC/AHA Guidelines on the Assessment of Atherosclerotic Cardiovascular Risk: Overview and Commentary
 2013 ACC/AHA Guidelines on the Assessment of Atherosclerotic Cardiovascular Risk: Overview and Commentary The Johns Hopkins Ciccarone Center for the Prevention of Heart Disease Becky McKibben, MPH; Seth
2013 ACC/AHA Guidelines on the Assessment of Atherosclerotic Cardiovascular Risk: Overview and Commentary The Johns Hopkins Ciccarone Center for the Prevention of Heart Disease Becky McKibben, MPH; Seth
Current and Future Imaging Trends in Risk Stratification for CAD
 Current and Future Imaging Trends in Risk Stratification for CAD Brian P. Griffin, MD FACC Department of Cardiovascular Medicine, Heart and Vascular Institute, Cleveland Clinic Disclosures: None Introduction
Current and Future Imaging Trends in Risk Stratification for CAD Brian P. Griffin, MD FACC Department of Cardiovascular Medicine, Heart and Vascular Institute, Cleveland Clinic Disclosures: None Introduction
MEDICAL POLICY SUBJECT: CORONARY CALCIUM SCORING
 MEDICAL POLICY PAGE: 1 OF: 5 If the member's subscriber contract excludes coverage for a specific service it is not covered under that contract. In such cases, medical policy criteria are not applied.
MEDICAL POLICY PAGE: 1 OF: 5 If the member's subscriber contract excludes coverage for a specific service it is not covered under that contract. In such cases, medical policy criteria are not applied.
Dyslipidemia in the light of Current Guidelines - Do we change our Practice?
 Dyslipidemia in the light of Current Guidelines - Do we change our Practice? Dato Dr. David Chew Soon Ping Senior Consultant Cardiologist Institut Jantung Negara Atherosclerotic Cardiovascular Disease
Dyslipidemia in the light of Current Guidelines - Do we change our Practice? Dato Dr. David Chew Soon Ping Senior Consultant Cardiologist Institut Jantung Negara Atherosclerotic Cardiovascular Disease
Coronary Artery Calcium. Vimal Ramjee, MD FACC The Chattanooga Heart Institute
 Coronary Artery Calcium Vimal Ramjee, MD FACC The Chattanooga Heart Institute Disclosures I have no conflicts of interest to disclose. Objectives Recognize the utility of coronary artery calcium scoring
Coronary Artery Calcium Vimal Ramjee, MD FACC The Chattanooga Heart Institute Disclosures I have no conflicts of interest to disclose. Objectives Recognize the utility of coronary artery calcium scoring
Short and Long Term Prognosis after Coronary Artery Calcium Scoring
 Short and Long Term Prognosis after Coronary Artery Calcium Scoring In Pre-Elderly and Elderly Patients Michael J. Blaha MD MPH Presented by: Michael J. Blaha July 24, 2017 1 Talk Outline 1. Coronary artery
Short and Long Term Prognosis after Coronary Artery Calcium Scoring In Pre-Elderly and Elderly Patients Michael J. Blaha MD MPH Presented by: Michael J. Blaha July 24, 2017 1 Talk Outline 1. Coronary artery
ACC/AHA GUIDELINES ON LIPIDS AND PCSK9 INHIBITORS
 ACC/AHA GUIDELINES ON LIPIDS AND PCSK9 INHIBITORS Ziyad Ghazzal MD, FACC, FSCAI Professor of Medicine Deputy Vice President/Dean Associate Dean for Clinical Affairs American University of Beirut Adjunct
ACC/AHA GUIDELINES ON LIPIDS AND PCSK9 INHIBITORS Ziyad Ghazzal MD, FACC, FSCAI Professor of Medicine Deputy Vice President/Dean Associate Dean for Clinical Affairs American University of Beirut Adjunct
MEDICAL POLICY. 02/15/18 CATEGORY: Technology Assessment
 MEDICAL POLICY SUBJECT: CORONARY CALCIUM SCORING PAGE: 1 OF: 5 If a product excludes coverage for a service, it is not covered, and medical policy criteria do not apply. If a commercial product, including
MEDICAL POLICY SUBJECT: CORONARY CALCIUM SCORING PAGE: 1 OF: 5 If a product excludes coverage for a service, it is not covered, and medical policy criteria do not apply. If a commercial product, including
The Implication of Coronary Artery Calcium Testing for Cardiovascular Disease Prevention and Diabetes
 Baptist Health South Florida Scholarly Commons @ Baptist Health South Florida All Publications 217 The Implication of Coronary Artery Calcium Testing for Cardiovascular Disease Prevention and Diabetes
Baptist Health South Florida Scholarly Commons @ Baptist Health South Florida All Publications 217 The Implication of Coronary Artery Calcium Testing for Cardiovascular Disease Prevention and Diabetes
Using Coronary Artery Calcium Score in the Quest for Cardiac Health. Robert J. Hage, D.O.
 Using Coronary Artery Calcium Score in the Quest for Cardiac Health Robert J. Hage, D.O. Heart disease is the leading cause of death in the United States in both men and women. About 610,000 people die
Using Coronary Artery Calcium Score in the Quest for Cardiac Health Robert J. Hage, D.O. Heart disease is the leading cause of death in the United States in both men and women. About 610,000 people die
Disclosures CORONARY CALCIUM SCORING REVISITED. Learning Objectives. Scoring Methods. Consultant for M2S, Inc. Coronary Calcium Scoring: Software
 CORONARY CALCIUM SCORING REVISITED Disclosures Consultant for M2S, Inc. Julianna M. Czum, MD Director, Division of Cardiothoracic Imaging Department of Radiology Dartmouth Hitchcock Medical Center Assistant
CORONARY CALCIUM SCORING REVISITED Disclosures Consultant for M2S, Inc. Julianna M. Czum, MD Director, Division of Cardiothoracic Imaging Department of Radiology Dartmouth Hitchcock Medical Center Assistant
Coronary Artery Calcium Scoring Mirvat Alasnag FACP, FRCP, FSCCT, FSCAI, FASE King Fahd Armed Forces Hospital, Jeddah. March 2017
 Coronary Artery Calcium Scoring Mirvat Alasnag FACP, FRCP, FSCCT, FSCAI, FASE King Fahd Armed Forces Hospital, Jeddah March 2017 Newspapers Referrals 62 year old female CT chest and abdomen following
Coronary Artery Calcium Scoring Mirvat Alasnag FACP, FRCP, FSCCT, FSCAI, FASE King Fahd Armed Forces Hospital, Jeddah March 2017 Newspapers Referrals 62 year old female CT chest and abdomen following
JUPITER NEJM Poll. Panel Discussion: Literature that Should Have an Impact on our Practice: The JUPITER Study
 Panel Discussion: Literature that Should Have an Impact on our Practice: The Study Kaiser COAST 11 th Annual Conference Maui, August 2009 Robert Blumberg, MD, FACC Ralph Brindis, MD, MPH, FACC Primary
Panel Discussion: Literature that Should Have an Impact on our Practice: The Study Kaiser COAST 11 th Annual Conference Maui, August 2009 Robert Blumberg, MD, FACC Ralph Brindis, MD, MPH, FACC Primary
Cardiac CT for Risk Assessment: Do we need to look beyond Coronary Artery Calcification
 Cardiac CT for Risk Assessment: Do we need to look beyond Coronary Artery Calcification Matthew Budoff, MD, FACC, FAHA Professor of Medicine Director, Cardiac CT Harbor-UCLA Medical Center, Torrance, CA
Cardiac CT for Risk Assessment: Do we need to look beyond Coronary Artery Calcification Matthew Budoff, MD, FACC, FAHA Professor of Medicine Director, Cardiac CT Harbor-UCLA Medical Center, Torrance, CA
LDL cholesterol (p = 0.40). However, higher levels of HDL cholesterol (> or =1.5 mmol/l [60 mg/dl]) were associated with less progression of CAC
![LDL cholesterol (p = 0.40). However, higher levels of HDL cholesterol (> or =1.5 mmol/l [60 mg/dl]) were associated with less progression of CAC](/thumbs/88/116891773.jpg "LDL cholesterol (p = 0.40). However, higher levels of HDL cholesterol (> or =1.5 mmol/l [60 mg/dl]) were associated with less progression of CAC") Am J Cardiol (2004);94:729-32 Relation of degree of physical activity to coronary artery calcium score in asymptomatic individuals with multiple metabolic risk factors M. Y. Desai, et al. Ciccarone Preventive
Am J Cardiol (2004);94:729-32 Relation of degree of physical activity to coronary artery calcium score in asymptomatic individuals with multiple metabolic risk factors M. Y. Desai, et al. Ciccarone Preventive
Supplementary Online Content
 Supplementary Online Content Kavousi M, Leening MJG, Nanchen D, et al. Comparison of application of the ACC/AHA guidelines, Adult Treatment Panel III guidelines, and European Society of Cardiology guidelines
Supplementary Online Content Kavousi M, Leening MJG, Nanchen D, et al. Comparison of application of the ACC/AHA guidelines, Adult Treatment Panel III guidelines, and European Society of Cardiology guidelines
2/20/2013. Why use imaging in CV prevention? Update on coronary CTA in 2013 Coronary CTA for 1 0 prevention: pros and cons Are we there yet?
 Evolving Role of Coronary CTA in Primary Cardiovascular Disease Prevention: Are We There Yet? Ron Blankstein, M.D., F.A.C.C. Co-Director, Cardiovascular Imaging Training Program Associate Physician, Preventive
Evolving Role of Coronary CTA in Primary Cardiovascular Disease Prevention: Are We There Yet? Ron Blankstein, M.D., F.A.C.C. Co-Director, Cardiovascular Imaging Training Program Associate Physician, Preventive
Diagnostic and Prognostic Value of Coronary Ca Score
 Diagnostic and Prognostic Value of Coronary Ca Score Dr. Ghormallah Alzahrani Cardiac imaging division, Adult Cardiology department Prince Sultan Cardiac Center ( PSCC) Madina, June 2 Coronary Calcium
Diagnostic and Prognostic Value of Coronary Ca Score Dr. Ghormallah Alzahrani Cardiac imaging division, Adult Cardiology department Prince Sultan Cardiac Center ( PSCC) Madina, June 2 Coronary Calcium
Observations on US CVD Prevention Guidelines. Donald M. Lloyd-Jones, MD ScM FACC FAHA
 Observations on US CVD Prevention Guidelines Donald M. Lloyd-Jones, MD ScM FACC FAHA What are Guidelines? Evidence Base for Guidelines Tricoci, JAMA 2009 Evidence Base for Guidelines Tricoci, JAMA 2009
Observations on US CVD Prevention Guidelines Donald M. Lloyd-Jones, MD ScM FACC FAHA What are Guidelines? Evidence Base for Guidelines Tricoci, JAMA 2009 Evidence Base for Guidelines Tricoci, JAMA 2009
2/9/2017. Financial Disclosures/Unapproved Use. Achieving Harmony in Blood Pressure Guidelines Around the Globe. Roger S. Blumenthal, MD.
 Achieving Harmony in Blood Pressure Guidelines Around the Globe Roger S. Blumenthal, MD The Kenneth Jay Pollin Professor of Cardiology Director, The Johns Hopkins Ciccarone Center for the Prevention Of
Achieving Harmony in Blood Pressure Guidelines Around the Globe Roger S. Blumenthal, MD The Kenneth Jay Pollin Professor of Cardiology Director, The Johns Hopkins Ciccarone Center for the Prevention Of
Lipid Management 2013 Statin Benefit Groups
 Clinical Integration Steering Committee Clinical Integration Chronic Disease Management Work Group Lipid Management 2013 Statin Benefit Groups Approved by Board Chair Signature Name (Please Print) Date
Clinical Integration Steering Committee Clinical Integration Chronic Disease Management Work Group Lipid Management 2013 Statin Benefit Groups Approved by Board Chair Signature Name (Please Print) Date
Update on Lipid Management in Cardiovascular Disease: How to Understand and Implement the New ACC/AHA Guidelines
 Update on Lipid Management in Cardiovascular Disease: How to Understand and Implement the New ACC/AHA Guidelines Paul Mahoney, MD Sentara Cardiology Specialists Lipid Management in Cardiovascular Disease
Update on Lipid Management in Cardiovascular Disease: How to Understand and Implement the New ACC/AHA Guidelines Paul Mahoney, MD Sentara Cardiology Specialists Lipid Management in Cardiovascular Disease
Use of Risk Assessment Tools to Guide Decision-Making in the Primary Prevention of Atherosclerotic Cardiovascular Disease
 Accepted Manuscript Use of Risk Assessment Tools to Guide Decision-Making in the Primary Prevention of Atherosclerotic Cardiovascular Disease Donald M. Lloyd-Jones, MD, ScM, FACC, FAHA, Lynne T. Braun,
Accepted Manuscript Use of Risk Assessment Tools to Guide Decision-Making in the Primary Prevention of Atherosclerotic Cardiovascular Disease Donald M. Lloyd-Jones, MD, ScM, FACC, FAHA, Lynne T. Braun,
Guideline for Assessment of Cardiovascular Risk in Asymptomatic Adults. Learn and Live SM. ACCF/AHA Pocket Guideline
 Learn and Live SM ACCF/AHA Pocket Guideline Based on the 2010 ACCF/AHA Guideline Guideline for Assessment of Cardiovascular Risk in Asymptomatic Adults November 2010 Guideline for Assessment of Cardiovascular
Learn and Live SM ACCF/AHA Pocket Guideline Based on the 2010 ACCF/AHA Guideline Guideline for Assessment of Cardiovascular Risk in Asymptomatic Adults November 2010 Guideline for Assessment of Cardiovascular
Sanger Heart & Vascular Institute Symposium 2015
 Sanger Heart & Vascular Institute Symposium 2015 Cardiovascular Update For Primary Care Physicians William E. Downey, MD FACC FSCAI Medical Director, Interventional Cardiology Sanger Heart & Vascular Institute
Sanger Heart & Vascular Institute Symposium 2015 Cardiovascular Update For Primary Care Physicians William E. Downey, MD FACC FSCAI Medical Director, Interventional Cardiology Sanger Heart & Vascular Institute
The role of coronary artery calcium score on the detection of subclinical atherosclerosis in metabolic diseases
 The role of coronary artery calcium score on the detection of subclinical atherosclerosis in metabolic diseases Eun-Jung Rhee Department of Endocrinology and Metabolism Kangbuk Samsung Hospital Sungkyunkwan
The role of coronary artery calcium score on the detection of subclinical atherosclerosis in metabolic diseases Eun-Jung Rhee Department of Endocrinology and Metabolism Kangbuk Samsung Hospital Sungkyunkwan
Corporate Medical Policy
 Corporate Medical Policy Computed Tomography to Detect Coronary Artery Calcification File Name: computed_tomography_to_detect_coronary_artery_calcification Origination: 3/1994 Last CAP Review 10/2017 Next
Corporate Medical Policy Computed Tomography to Detect Coronary Artery Calcification File Name: computed_tomography_to_detect_coronary_artery_calcification Origination: 3/1994 Last CAP Review 10/2017 Next
Treatment of Cardiovascular Risk Factors. Kevin M Hayes D.O. F.A.C.C. First Coast Heart and Vascular Center
 Treatment of Cardiovascular Risk Factors Kevin M Hayes D.O. F.A.C.C. First Coast Heart and Vascular Center Disclosures: None Objectives What do risk factors tell us What to check and when Does treatment
Treatment of Cardiovascular Risk Factors Kevin M Hayes D.O. F.A.C.C. First Coast Heart and Vascular Center Disclosures: None Objectives What do risk factors tell us What to check and when Does treatment
The role of coronary artery calcium score on the detection of subclinical atherosclerosis in metabolic diseases
 The role of coronary artery calcium score on the detection of subclinical atherosclerosis in metabolic diseases Eun-Jung Rhee Department of Endocrinology and Metabolis Kangbuk Samsung Hospital Sungkyunkwan
The role of coronary artery calcium score on the detection of subclinical atherosclerosis in metabolic diseases Eun-Jung Rhee Department of Endocrinology and Metabolis Kangbuk Samsung Hospital Sungkyunkwan
John J.P. Kastelein MD PhD Professor of Medicine Dept. of Vascular Medicine Academic Medial Center / University of Amsterdam
 Latest Insights from the JUPITER Study John J.P. Kastelein MD PhD Professor of Medicine Dept. of Vascular Medicine Academic Medial Center / University of Amsterdam Inflammation, hscrp, and Vascular Prevention
Latest Insights from the JUPITER Study John J.P. Kastelein MD PhD Professor of Medicine Dept. of Vascular Medicine Academic Medial Center / University of Amsterdam Inflammation, hscrp, and Vascular Prevention
Which CVS risk reduction strategy fits better to carotid US findings?
 Which CVS risk reduction strategy fits better to carotid US findings? Dougalis A, Soulaidopoulos S, Cholongitas E, Chalevas P, Vettas Ch, Doumtsis P, Vaitsi K, Diavasti M, Mandala E, Garyfallos A 4th Department
Which CVS risk reduction strategy fits better to carotid US findings? Dougalis A, Soulaidopoulos S, Cholongitas E, Chalevas P, Vettas Ch, Doumtsis P, Vaitsi K, Diavasti M, Mandala E, Garyfallos A 4th Department
4/7/ The stats on heart disease. + Deaths & Age-Adjusted Death Rates for
 + Update on Lipid Management Stacey Gardiner, MD Assistant Professor Division of Cardiovascular Medicine Medical College of Wisconsin + The stats on heart disease Over the past 10 years for which statistics
+ Update on Lipid Management Stacey Gardiner, MD Assistant Professor Division of Cardiovascular Medicine Medical College of Wisconsin + The stats on heart disease Over the past 10 years for which statistics
Potential recommendations for CT coronary angiography in athletes
 Potential recommendations for CT coronary angiography in athletes B.K. Velthuis Dept. of Radiology UMC Utrecht, the Netherlands EuroPRevent 15 April 2011 Declaration of interest Philips Medical Systems
Potential recommendations for CT coronary angiography in athletes B.K. Velthuis Dept. of Radiology UMC Utrecht, the Netherlands EuroPRevent 15 April 2011 Declaration of interest Philips Medical Systems
Acute Coronary Syndromes (ACS)
") Sally A. Arif, Pharm.D., BCPS (AQ Cardiology) Assistant Professor of Pharmacy Practice Midwestern University, Chicago College of Pharmacy Cardiology Clinical Specialist, Rush University Medical Center
Sally A. Arif, Pharm.D., BCPS (AQ Cardiology) Assistant Professor of Pharmacy Practice Midwestern University, Chicago College of Pharmacy Cardiology Clinical Specialist, Rush University Medical Center
Combining Coronary Artery Calcium Scanning with SPECT/PET Myocardial Perfusion Imaging
 Combining Coronary Artery Calcium Scanning with SPECT/PET Myocardial Perfusion Imaging Daniel S. Berman, MD Director, Cardiac Imaging Cedars-Sinai Heart Institute Professor of Medicine and Imaging Cedars-Sinai
Combining Coronary Artery Calcium Scanning with SPECT/PET Myocardial Perfusion Imaging Daniel S. Berman, MD Director, Cardiac Imaging Cedars-Sinai Heart Institute Professor of Medicine and Imaging Cedars-Sinai
CORONARY ARTERY CALCIUM AND INCIDENT STROKE IN THE MULTI-ETHNIC STUDY OF ATHEROSCLEROSIS (MESA) COHORT ASHLEIGH A. OWEN, MD
 COHORT ASHLEIGH A. OWEN, MD") CORONARY ARTERY CALCIUM AND INCIDENT STROKE IN THE MULTI-ETHNIC STUDY OF ATHEROSCLEROSIS (MESA) COHORT BY ASHLEIGH A. OWEN, MD A Thesis Submitted to the Graduate Faculty of WAKE FOREST UNIVERSITY GRADUATE
CORONARY ARTERY CALCIUM AND INCIDENT STROKE IN THE MULTI-ETHNIC STUDY OF ATHEROSCLEROSIS (MESA) COHORT BY ASHLEIGH A. OWEN, MD A Thesis Submitted to the Graduate Faculty of WAKE FOREST UNIVERSITY GRADUATE
2/10/2016. Perspectives on the 2013 ACC/AHA Cholesterol Guidelines. Disclosures. ATP-III Update 2004
 Perspectives on the 2013 ACC/AHA Cholesterol Guidelines Donald M. Lloyd-Jones, MD ScM Senior Associate Dean Chair and Professor of Preventive Medicine Northwestern Feinberg School of Medicine Disclosures
Perspectives on the 2013 ACC/AHA Cholesterol Guidelines Donald M. Lloyd-Jones, MD ScM Senior Associate Dean Chair and Professor of Preventive Medicine Northwestern Feinberg School of Medicine Disclosures
New Guidelines in Dyslipidemia Management
 The Fourth IAS-OSLA Course on Lipid Metabolism and Cardiovascular Risk Muscat, Oman, February 2018 New Guidelines in Dyslipidemia Management Dr. Khalid Al-Waili, MD, FRCPC, DABCL Senior Consultant Medical
The Fourth IAS-OSLA Course on Lipid Metabolism and Cardiovascular Risk Muscat, Oman, February 2018 New Guidelines in Dyslipidemia Management Dr. Khalid Al-Waili, MD, FRCPC, DABCL Senior Consultant Medical
Description. Section: Radiology Effective Date: October 15, 2015 Subsection: Radiology Original Policy Date: December 7, 2011 Subject:
 Last Review Status/Date: September 2015 Page: 1 of 15 Description Background Coronary artery calcium (CAC) has been recognized to be associated with CAD on the basis of anatomic studies for decades. The
Last Review Status/Date: September 2015 Page: 1 of 15 Description Background Coronary artery calcium (CAC) has been recognized to be associated with CAD on the basis of anatomic studies for decades. The
The Art of Cardiovascular Risk Assessment
 The Art of Cardiovascular Risk Assessment Laurence S. Sperling, M.D., FACC, FACP,FAHA, FASPC Professor of Medicine (Cardiology) Professor of Global Health Director- Center for Heart Disease Prevention
The Art of Cardiovascular Risk Assessment Laurence S. Sperling, M.D., FACC, FACP,FAHA, FASPC Professor of Medicine (Cardiology) Professor of Global Health Director- Center for Heart Disease Prevention
Preclinical Detection of CAD: Is it worth the effort? Michael H. Crawford, MD
 Preclinical Detection of CAD: Is it worth the effort? Michael H. Crawford, MD 1 Preclinical? No symptoms No physical findings No diagnostic ECG findings No chest X-ray X findings No diagnostic events 2
Preclinical Detection of CAD: Is it worth the effort? Michael H. Crawford, MD 1 Preclinical? No symptoms No physical findings No diagnostic ECG findings No chest X-ray X findings No diagnostic events 2
Aortic Root Calcification: A Possible Imaging Biomarker of Coronary Atherosclerosis
 Published online: January 8, 216 216 S. Karger AG, Basel 2235 8676/16/34 167$39.5/ Mini-Review Aortic Root Calcification: A Possible Imaging Biomarker of Coronary Hussein Nafakhi a Hasan A. Al-Nafakh b
Published online: January 8, 216 216 S. Karger AG, Basel 2235 8676/16/34 167$39.5/ Mini-Review Aortic Root Calcification: A Possible Imaging Biomarker of Coronary Hussein Nafakhi a Hasan A. Al-Nafakh b
Chapter 15 Coronary Calcium Scoring for Individualized, Disease-Guided Management: Evidence Is Accumulating
 Chapter 15 Coronary Calcium Scoring for Individualized, Disease-Guided Management: Evidence Is Accumulating GEEVAR ZACHARIAH JAMES K.J. INTRODUCTION Coronary artery calcium (CAC) is virtually pathognomonic
Chapter 15 Coronary Calcium Scoring for Individualized, Disease-Guided Management: Evidence Is Accumulating GEEVAR ZACHARIAH JAMES K.J. INTRODUCTION Coronary artery calcium (CAC) is virtually pathognomonic
BENEFIT APPLICATION BLUECARD/NATIONAL ACCOUNT ISSUES
 Medical Policy Medical Policy MP 6.01.03 BCBSA Ref. Policy: 6.01.03 Last Review: 09/19/2018 Effective Date: 09/19/2018 Section: Medicine Related Policies 9.01.502 Experimental / Investigational Services
Medical Policy Medical Policy MP 6.01.03 BCBSA Ref. Policy: 6.01.03 Last Review: 09/19/2018 Effective Date: 09/19/2018 Section: Medicine Related Policies 9.01.502 Experimental / Investigational Services
CVD Risk Assessment. Michal Vrablík Charles University, Prague Czech Republic
 CVD Risk Assessment Michal Vrablík Charles University, Prague Czech Republic What is Risk? A cumulative probability of an event, usually expressed as percentage e.g.: 5 CV events in 00 pts = 5% risk This
CVD Risk Assessment Michal Vrablík Charles University, Prague Czech Republic What is Risk? A cumulative probability of an event, usually expressed as percentage e.g.: 5 CV events in 00 pts = 5% risk This
Achieving Cholesterol Management Goals: Identifying Clinician-Centered Challenges to Optimal Patient Care
 Achieving Cholesterol Management Goals: Identifying Clinician-Centered Challenges to Optimal Patient Care Purpose Explore the adherence rates to cholesterol treatment targets among patients who seek care
Achieving Cholesterol Management Goals: Identifying Clinician-Centered Challenges to Optimal Patient Care Purpose Explore the adherence rates to cholesterol treatment targets among patients who seek care
NEW GUIDELINES FOR CHOLESTEROL
 NEW GUIDELINES FOR CHOLESTEROL NEW CHOLESTEROL GUIDELINES 2013 Recently updated guidelines for the treatment of high blood cholesterol levels is a major update since 2002. The news media have trumpeted
NEW GUIDELINES FOR CHOLESTEROL NEW CHOLESTEROL GUIDELINES 2013 Recently updated guidelines for the treatment of high blood cholesterol levels is a major update since 2002. The news media have trumpeted
What have We Learned in Dyslipidemia Management Since the Publication of the 2013 ACC/AHA Guideline?
 What have We Learned in Dyslipidemia Management Since the Publication of the 2013 ACC/AHA Guideline? Salim S. Virani, MD, PhD, FACC, FAHA Associate Professor, Section of Cardiovascular Research Baylor
What have We Learned in Dyslipidemia Management Since the Publication of the 2013 ACC/AHA Guideline? Salim S. Virani, MD, PhD, FACC, FAHA Associate Professor, Section of Cardiovascular Research Baylor
Northwestern University Feinberg School of Medicine Calculating the CVD Risk Score: Which Tool for Which Patient?
 Northwestern University Feinberg School of Medicine Calculating the CVD Risk Score: Which Tool for Which Patient? Donald M. Lloyd-Jones, MD, ScM, FACC, FAHA Senior Associate Dean Chair, Department of Preventive
Northwestern University Feinberg School of Medicine Calculating the CVD Risk Score: Which Tool for Which Patient? Donald M. Lloyd-Jones, MD, ScM, FACC, FAHA Senior Associate Dean Chair, Department of Preventive
Vascular calcification in patients with Diabetes Mellitus. Dr Jamie Bellinge University of Western Australia Royal Perth Hospital
 Vascular calcification in patients with Diabetes Mellitus Dr Jamie Bellinge University of Western Australia Royal Perth Hospital Risk of cardiovascular disease Cardiovascular disease; - Stroke - Coronary
Vascular calcification in patients with Diabetes Mellitus Dr Jamie Bellinge University of Western Australia Royal Perth Hospital Risk of cardiovascular disease Cardiovascular disease; - Stroke - Coronary
Coronary Artery Calcium to Predict All-Cause Mortality in Elderly Men and Women
 Journal of the American College of Cardiology Vol. 52, No. 1, 28 28 by the American College of Cardiology Foundation ISSN 735-197/8/$34. Published by Elsevier Inc. doi:1.116/j.jacc.28.4.4 CLINICAL RESEARCH
Journal of the American College of Cardiology Vol. 52, No. 1, 28 28 by the American College of Cardiology Foundation ISSN 735-197/8/$34. Published by Elsevier Inc. doi:1.116/j.jacc.28.4.4 CLINICAL RESEARCH
Medical Policy. Medical Policy. MP Computed Tomography to Detect Coronary Artery Calcification
 Medical Policy Medical Policy MP 6.01.03 BCBSA Ref. Policy: 6.01.03 Last Review: 09/28/2017 Effective Date: 09/28/2017 Section: Medicine Related Policies 6.01.43 Contrast-Enhanced Computed Tomography Angiography
Medical Policy Medical Policy MP 6.01.03 BCBSA Ref. Policy: 6.01.03 Last Review: 09/28/2017 Effective Date: 09/28/2017 Section: Medicine Related Policies 6.01.43 Contrast-Enhanced Computed Tomography Angiography
CT Calcium Score and Statins in Primary CV Prevention. Dr Selwyn Wong
 CT Calcium Score and Statins in Primary CV Prevention. Dr Selwyn Wong Promises, Pitfalls and Hard Truths of Coronary Calcium Scanning Selwyn Wong Ascot and Middlemore Hospitals Coronary Calcium Scoring
CT Calcium Score and Statins in Primary CV Prevention. Dr Selwyn Wong Promises, Pitfalls and Hard Truths of Coronary Calcium Scanning Selwyn Wong Ascot and Middlemore Hospitals Coronary Calcium Scoring
Clinical Investigations
 Clinical Investigations Implications of the New US Cholesterol Guidelines in the Brazilian Longitudinal Study of Adult Health (ELSA-Brasil) Address for correspondence: Marcio Sommer Bittencourt, MD University
Clinical Investigations Implications of the New US Cholesterol Guidelines in the Brazilian Longitudinal Study of Adult Health (ELSA-Brasil) Address for correspondence: Marcio Sommer Bittencourt, MD University
1. Which one of the following patients does not need to be screened for hyperlipidemia:
 Questions: 1. Which one of the following patients does not need to be screened for hyperlipidemia: a) Diabetes mellitus b) Hypertension c) Family history of premature coronary disease (first degree relatives:
Questions: 1. Which one of the following patients does not need to be screened for hyperlipidemia: a) Diabetes mellitus b) Hypertension c) Family history of premature coronary disease (first degree relatives:
Section: Radiology Last Reviewed Date: December Policy No: 6 Effective Date: February 1, 2014
 Medical Policy Manual Topic: Computed Tomography to Detect Coronary Artery Calcification Date of Origin: January 1996 Section: Radiology Last Reviewed Date: December 2013 Policy No: 6 Effective Date: February
Medical Policy Manual Topic: Computed Tomography to Detect Coronary Artery Calcification Date of Origin: January 1996 Section: Radiology Last Reviewed Date: December 2013 Policy No: 6 Effective Date: February
No relevant financial relationships
 MANAGEMENT OF LIPID DISORDERS Balancing Benefits and harms Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial relationships baron@medicine.ucsf.edu
MANAGEMENT OF LIPID DISORDERS Balancing Benefits and harms Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial relationships baron@medicine.ucsf.edu
Carotid Ultrasound Scans for Assessing Cardiovascular Risk
 Transcript Details This is a transcript of an educational program accessible on the ReachMD network. Details about the program and additional media formats for the program are accessible by visiting: https://reachmd.com/programs/lipid-luminations/carotid-ultrasound-scans-for-assessing-cardiovascularrisk/4004/
Transcript Details This is a transcript of an educational program accessible on the ReachMD network. Details about the program and additional media formats for the program are accessible by visiting: https://reachmd.com/programs/lipid-luminations/carotid-ultrasound-scans-for-assessing-cardiovascularrisk/4004/
Disclosure. No relevant financial relationships. Placebo-Controlled Statin Trials
 PREVENTING CARDIOVASCULAR DISEASE IN WOMEN: Current Guidelines for Hypertension, Lipids and Aspirin Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial
PREVENTING CARDIOVASCULAR DISEASE IN WOMEN: Current Guidelines for Hypertension, Lipids and Aspirin Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial
10/8/2015. MN Nursing Conference October 7th, 2015 Michael Miedema, MD MPH. None
 MN Nursing Conference October 7th, 2015 Michael Miedema, MD MPH None 1 Objectives Why the need for change in the guidelines? What is the potential impact of these guidelines? Where do we go from here?
MN Nursing Conference October 7th, 2015 Michael Miedema, MD MPH None 1 Objectives Why the need for change in the guidelines? What is the potential impact of these guidelines? Where do we go from here?
New Guidelines in Dyslipidemia Management
 The Third IAS-OSLA Course on Lipid Metabolism and Cardiovascular Risk Muscat, Oman, February 2017 New Guidelines in Dyslipidemia Management Dr. Khalid Al-Waili, MD, FRCPC, DABCL Senior Consultant Medical
The Third IAS-OSLA Course on Lipid Metabolism and Cardiovascular Risk Muscat, Oman, February 2017 New Guidelines in Dyslipidemia Management Dr. Khalid Al-Waili, MD, FRCPC, DABCL Senior Consultant Medical
The use of statins for primary prevention and evidencebased
 Impact of Statin Guidelines on Statin Utilization and Costs in an Employer-Based Primary Care Clinic Holly E. Gurgle, PharmD, BCACP, CDE; Marisa B. Schauerhamer, PharmD; Simón A. Rodriguez, PharmD; and
Impact of Statin Guidelines on Statin Utilization and Costs in an Employer-Based Primary Care Clinic Holly E. Gurgle, PharmD, BCACP, CDE; Marisa B. Schauerhamer, PharmD; Simón A. Rodriguez, PharmD; and
An update on lipidology and cardiovascular risk management. Lipids, Metabolism & Vascular Risk Section - Royal Society of Medicine
 An update on lipidology and cardiovascular risk management Lipids, Metabolism & Vascular Risk Section - Royal Society of Medicine National and international lipid modification guidelines: A critical appraisal
An update on lipidology and cardiovascular risk management Lipids, Metabolism & Vascular Risk Section - Royal Society of Medicine National and international lipid modification guidelines: A critical appraisal
Dr Chris Ellis. Consultant Cardiologist Auckland
 Dr Chris Ellis Consultant Cardiologist Auckland CVD Risk Prevention in NZ 2013 & Beyond: The Clinicians View Dr Chris Ellis Cardiologist Green Lane CVS Service, Cardiology Department, Auckland City Hospital
Dr Chris Ellis Consultant Cardiologist Auckland CVD Risk Prevention in NZ 2013 & Beyond: The Clinicians View Dr Chris Ellis Cardiologist Green Lane CVS Service, Cardiology Department, Auckland City Hospital
Application of New Cholesterol Guidelines to a Population-Based Sample
 The new england journal of medicine original article Application of New Cholesterol to a Population-Based Sample Michael J. Pencina, Ph.D., Ann Marie Navar-Boggan, M.D., Ph.D., Ralph B. D Agostino, Sr.,
The new england journal of medicine original article Application of New Cholesterol to a Population-Based Sample Michael J. Pencina, Ph.D., Ann Marie Navar-Boggan, M.D., Ph.D., Ralph B. D Agostino, Sr.,
Dyslipidemia in women: Who should be treated and how?
 Dyslipidemia in women: Who should be treated and how? Lale Tokgozoglu, MD, FACC, FESC Professor of Cardiology Hacettepe University Faculty of Medicine Ankara, Turkey. Cause of Death in Women: European
Dyslipidemia in women: Who should be treated and how? Lale Tokgozoglu, MD, FACC, FESC Professor of Cardiology Hacettepe University Faculty of Medicine Ankara, Turkey. Cause of Death in Women: European
Application of New Cholesterol Guidelines to a Population-Based Sample
 The new england journal of medicine original article Application of New Cholesterol to a Population-Based Sample Michael J. Pencina, Ph.D., Ann Marie Navar-Boggan, M.D., Ph.D., Ralph B. D Agostino, Sr.,
The new england journal of medicine original article Application of New Cholesterol to a Population-Based Sample Michael J. Pencina, Ph.D., Ann Marie Navar-Boggan, M.D., Ph.D., Ralph B. D Agostino, Sr.,
Assessing atherosclerotic risk for long term preventive treatment
 Assessing atherosclerotic risk for long term preventive treatment Donald A. Smith, MD, MPH Endocrinologist, Clinical Lipidologist Associate Professor of Medicine and Preventive Medicine Icahn School of
Assessing atherosclerotic risk for long term preventive treatment Donald A. Smith, MD, MPH Endocrinologist, Clinical Lipidologist Associate Professor of Medicine and Preventive Medicine Icahn School of
Assessing Cardiovascular Risk to Optimally Stratify Low- and Moderate- Risk Patients. Copyright. Not for Sale or Commercial Distribution
 CLINICAL Viewpoint Assessing Cardiovascular Risk to Optimally Stratify Low- and Moderate- Risk Patients Copyright Not for Sale or Commercial Distribution By Ruth McPherson, MD, PhD, FRCPC Unauthorised
CLINICAL Viewpoint Assessing Cardiovascular Risk to Optimally Stratify Low- and Moderate- Risk Patients Copyright Not for Sale or Commercial Distribution By Ruth McPherson, MD, PhD, FRCPC Unauthorised
Primary prevention of Cardiovascular Diseases: Differences between European and United States Guidelines
 18 MEDICINSKI GLASNIK / str. 18-23 Vojislav Giga 1,2, Marija Petrović 1 Primary prevention of Cardiovascular Diseases: Differences between European and United States Guidelines Abstract: European Society
18 MEDICINSKI GLASNIK / str. 18-23 Vojislav Giga 1,2, Marija Petrović 1 Primary prevention of Cardiovascular Diseases: Differences between European and United States Guidelines Abstract: European Society
ORIGINAL INVESTIGATION. Application of the Screening for Heart Attack Prevention and Education Task Force Recommendations to an Urban Population
 ORIGINAL INVESTIGATION Application of the Screening for Heart Attack Prevention and Education Task Force Recommendations to an Urban Population Observations From the Dallas Heart Study Raphael See, MD;
ORIGINAL INVESTIGATION Application of the Screening for Heart Attack Prevention and Education Task Force Recommendations to an Urban Population Observations From the Dallas Heart Study Raphael See, MD;
Carotid Ddisease, Carotid IMT and Risk of Stroke
 Carotid Ddisease, Carotid IMT and Risk of Stroke TATJANA RUNDEK, MD PhD Professor of Neurology, Epidemiology and Public Health Director, Clinical translational Division Department of Neurology, Miller
Carotid Ddisease, Carotid IMT and Risk of Stroke TATJANA RUNDEK, MD PhD Professor of Neurology, Epidemiology and Public Health Director, Clinical translational Division Department of Neurology, Miller
Who Cares About the Past?
 Risk Factors, the New Calcium Score, Rheology and Atherosclerosis Progression Arthur Agatston 2/21/15 The Vulnerable Plaque vs. Plaque Burden CT Angiogram Is There a Role for Coronary Artery Calcium Scoring
Risk Factors, the New Calcium Score, Rheology and Atherosclerosis Progression Arthur Agatston 2/21/15 The Vulnerable Plaque vs. Plaque Burden CT Angiogram Is There a Role for Coronary Artery Calcium Scoring
Current Cholesterol Guidelines and Treatment of Residual Risk COPYRIGHT. J. Peter Oettgen, MD
 Current Cholesterol Guidelines and Treatment of Residual Risk J. Peter Oettgen, MD Associate Professor of Medicine Harvard Medical School Director, Preventive Cardiology Beth Israel Deaconess Medical Center
Current Cholesterol Guidelines and Treatment of Residual Risk J. Peter Oettgen, MD Associate Professor of Medicine Harvard Medical School Director, Preventive Cardiology Beth Israel Deaconess Medical Center
Prevention of Heart Disease: The New Guidelines
 Prevention of Heart Disease: The New Guidelines Nisha I. Parikh MD MPH Assistant Professor of Medicine Division of Cardiology Department of Medicine University of California San Francisco May 18 th 2015
Prevention of Heart Disease: The New Guidelines Nisha I. Parikh MD MPH Assistant Professor of Medicine Division of Cardiology Department of Medicine University of California San Francisco May 18 th 2015
Effective for dates of service on or after April 1, 2013, refer to:
 Effective for dates of service on or after April 1, 2013, refer to: https://www.bcbsal.org/providers/policies/carecore.cfm Name of Policy: Computed Tomography to Detect Coronary Artery Calcification Policy
Effective for dates of service on or after April 1, 2013, refer to: https://www.bcbsal.org/providers/policies/carecore.cfm Name of Policy: Computed Tomography to Detect Coronary Artery Calcification Policy
CONTRIBUTING FACTORS FOR STROKE:
 CONTRIBUTING FACTORS FOR STROKE: HYPERTENSION AND HYPERCHOLESTEROLEMIA Melissa R. Stephens, MD, FAAFP Associate Professor of Clinical Sciences William Carey University College of Osteopathic Medicine LEARNING
CONTRIBUTING FACTORS FOR STROKE: HYPERTENSION AND HYPERCHOLESTEROLEMIA Melissa R. Stephens, MD, FAAFP Associate Professor of Clinical Sciences William Carey University College of Osteopathic Medicine LEARNING
New Cholesterol Guidelines What the LDL are we supposed to do now?!
 New Cholesterol Guidelines What the LDL are we supposed to do now?! Michael D. Shapiro Assistant Professor of Medicine and Radiology Knight Cardiovascular Institute Oregon Health & Science University 2013
New Cholesterol Guidelines What the LDL are we supposed to do now?! Michael D. Shapiro Assistant Professor of Medicine and Radiology Knight Cardiovascular Institute Oregon Health & Science University 2013
CLINICAL OUTCOME Vs SURROGATE MARKER
 CLINICAL OUTCOME Vs SURROGATE MARKER Statin Real Experience Dr. Mostafa Sherif Senior Medical Manager Pfizer Egypt & Sudan Objective Difference between Clinical outcome and surrogate marker Proper Clinical
CLINICAL OUTCOME Vs SURROGATE MARKER Statin Real Experience Dr. Mostafa Sherif Senior Medical Manager Pfizer Egypt & Sudan Objective Difference between Clinical outcome and surrogate marker Proper Clinical
Landmesser U et al. Eur Heart J 2017; https://doi.org/ /eurheartj/ehx549
 2017 Update of ESC/EAS Task Force on Practical Clinical Guidance for PCSK9 inhibition in Patients with Atherosclerotic Cardiovascular Disease or in Familial Hypercholesterolaemia Cardiovascular Outcomes
2017 Update of ESC/EAS Task Force on Practical Clinical Guidance for PCSK9 inhibition in Patients with Atherosclerotic Cardiovascular Disease or in Familial Hypercholesterolaemia Cardiovascular Outcomes
Contemporary management of Dyslipidemia
 Contemporary management of Dyslipidemia Todd Anderson Feb 2018 Disclosure Statement Within the past two years: I have not had an affiliation (financial or otherwise) with a commercial organization that
Contemporary management of Dyslipidemia Todd Anderson Feb 2018 Disclosure Statement Within the past two years: I have not had an affiliation (financial or otherwise) with a commercial organization that
Disclosure. No relevant financial relationships. Placebo-Controlled Statin Trials
 MANAGEMENT OF HYPERLIPIDEMIA AND CARDIOVASCULAR RISK IN WOMEN: Balancing Benefits and Harms Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial
MANAGEMENT OF HYPERLIPIDEMIA AND CARDIOVASCULAR RISK IN WOMEN: Balancing Benefits and Harms Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial
Review current guideline recommendations for lipid-lowering therapy
 Breakout Session #3 New Paradigms in the Management of Dyslipidemia Review current guideline recommendations for lipid-lowering therapy Dr Meral KAYIKCIOGLU Ege University Medical School, Cardiology Dept,
Breakout Session #3 New Paradigms in the Management of Dyslipidemia Review current guideline recommendations for lipid-lowering therapy Dr Meral KAYIKCIOGLU Ege University Medical School, Cardiology Dept,
When Statins Aren t Enough: Appropriate Therapies for High-Risk Patients with Diabetes
 When Statins Aren t Enough: Appropriate Therapies for High-Risk Patients with Diabetes Kim K. Birtcher, MS, PharmD, AACC, FNLA, CLS, BCPS (AQ-Cardiology), CDE Clinical Professor University of Houston College
When Statins Aren t Enough: Appropriate Therapies for High-Risk Patients with Diabetes Kim K. Birtcher, MS, PharmD, AACC, FNLA, CLS, BCPS (AQ-Cardiology), CDE Clinical Professor University of Houston College
Coronary Artery Calcium Score
 Coronary Artery Calcium Score August 19, 2014 by Axel F. Sigurdsson MD 174 Comments essential for living organisms. Calcium is a chemical element that is Most of the calcium within the human body is found
Coronary Artery Calcium Score August 19, 2014 by Axel F. Sigurdsson MD 174 Comments essential for living organisms. Calcium is a chemical element that is Most of the calcium within the human body is found
Using Cardiovascular Risk to Guide Antihypertensive Treatment Implications For The Pre-elderly and Elderly
 Using Cardiovascular Risk to Guide Antihypertensive Treatment Implications For The Pre-elderly and Elderly Paul Muntner, PhD MHS Professor and Vice Chair Department of Epidemiology University of Alabama
Using Cardiovascular Risk to Guide Antihypertensive Treatment Implications For The Pre-elderly and Elderly Paul Muntner, PhD MHS Professor and Vice Chair Department of Epidemiology University of Alabama
Prevention Updates and Paradigm Shifts
 Prevention Updates and Paradigm Shifts Andrew Freeman, MD, FACC Director of Clinical Cardiology and Operations National Jewish Health Assistant Professor of Medicine National Jewish Health and University
Prevention Updates and Paradigm Shifts Andrew Freeman, MD, FACC Director of Clinical Cardiology and Operations National Jewish Health Assistant Professor of Medicine National Jewish Health and University
CLINICAL STUDY. Yasser Khalil, MD; Bertrand Mukete, MD; Michael J. Durkin, MD; June Coccia, MS, RVT; Martin E. Matsumura, MD
 117 CLINICAL STUDY A Comparison of Assessment of Coronary Calcium vs Carotid Intima Media Thickness for Determination of Vascular Age and Adjustment of the Framingham Risk Score Yasser Khalil, MD; Bertrand
117 CLINICAL STUDY A Comparison of Assessment of Coronary Calcium vs Carotid Intima Media Thickness for Determination of Vascular Age and Adjustment of the Framingham Risk Score Yasser Khalil, MD; Bertrand