Blood Pressure Treatment Goals
|
|
|
- Jordan Ramsey
- 5 years ago
- Views:
Transcription
1 Blood Pressure Treatment Goals Kenneth Izuora, MD, MBA, FACE Associate Professor UNLV School of Medicine November 18, 2017
2 Learning Objectives Discuss the recent studies on treating hypertension Review the AACE hypertension guidelines. Does the evidence support the guidelines? What should the blood pressure goal be for people with type 2 DM?
3 Definition Sustained elevation of blood pressure above a given goal. BP = Cardiac Output x Peripheral Resistance
4 Hypertension Hypergylcemia Hyperlipidemia ASCVD ACS/MI Angina CAD Stroke/TIA PVD
5 Screening and Diagnosis Measure BP during every routine clinic visit. Repeat BP on separate day (within 1 month) if elevated to confirm diagnosis. Monitor BP at home to identify white coat HTN Orthostatic BP at initial visit and if symptomatic.
6 Why bother?
7 Too High?
8 Too Low? 43% risk of hip fracture in first 45 days of treatment Population: 301,591 patients, 66 years, first anti-htn prescription Arch Intern Med. 2012;172(22): doi: /2013.jamainternmed.469
9 CV mortality rate Per 10,000 person-years Association of SBP and CV Mortality in Men with T2DM No diabetes Diabetes < SBP (mmhg) 200 CV = cardiovascular; SBP = systolic blood pressure; T2DM = type 2 diabetes mellitus. Stamler J, et al. Diabetes Care. 16: , 1993.
 Tight control")
 UKPDS Study Group.")

10 Patients with events (%) Hypertension in Diabetes, UKPDS Less tight control (mean BP 154/87 mmhg) Tight control (mean BP 144/82 mmhg) Tight BP control: 24% reduction of events (95% CI 8-38) UKPDS Study Group. BMJ 317:703-13, Years from randomization BP = blood pressure; UKPDS = United Kingdom Prospective Diabetes Study Group.
11 Ann Intern Med. 2001;134(5): doi: / Copyright American College of Physicians. All rights reserved.
12 What is an optimal BP target?
13 The Hypertension J curve CVD (Hazard Ratio) ? Blood Pressure
14 Key Studies
15 ACCORD BP 4733 T2DM patients y/o with prior CVD or multiple CVD risk factors Blood pressure target: <120 vs Blood pressure achieved: 119/64 vs. 133/70 Outcomes: Primary: Major CVD event [composite of nonfatal MI, nonfatal stroke or CVD death]
16 The ACCORD Study Group. N Engl J Med 2010;362:
17 The ACCORD Study Group. N Engl J Med 2010;362:
18 ACCORD Conclusions No benefit in primary end point [Nonfatal MI, nonfatal stroke and CVD death]. Intensive treatment reduced the rate of total stroke and nonfatal stroke. Elevated creatinine and electrolyte abnormalities more common in intensive group.
19 SPRINT Participants: 9,361 persons with increased CVD risk (without DM or stroke). Planned for 5 years but stopped at 3.26 years. Blood Pressure Standard Intensive Target <140 <120 Achieved
20 The SPRINT Research Group. N Engl J Med 2015;373:
21 25% MI ACS Stroke HF CVD death 27% Death from any cause The SPRINT Research Group. N Engl J Med 2015;373:
22 The SPRINT Research Group. N Engl J Med 2015;373:
23 SPRINT Conclusion Intensive SBP treatment lowered risk for [MI,ACS, Stroke, HF, and CVD death] by 25% Intensive target reduced risk of all cause mortality by 27% Rates of hypotension, syncope, electrolyte abnormalities and AKI higher in intensive treatment group.
24 HOPE 3 12,705 intermediate risk patients without CVD randomized to candesartan + HCTZ or placebo. Baseline blood pressure: 138.1/81.9 mm Hg Post treatment blood pressure: 132/79 Co-primary outcomes: [CVD death, non-fatal MI, non-fatal stroke] Resuscitated cardiac arrest, HF and revascularization
25 Lonn EM et al. N Engl J Med 2016;374:
26 Lonn EM et al. N Engl J Med 2016;374:
27 Lonn EM et al. N Engl J Med 2016;374:
28 HOPE 3 Conclusion Therapy with candesartan + HCTZ was not associated with a lower rate of major cardiovascular events than placebo in intermediate risk patients without CVD.
29 Hypertension Optimal Treatment (HOT) Study Aim: Assess relationship between [MI, stroke, CVD death] and diastolic BP N=18790, 1501 with DM, baseline BP 169/105 Blood pressure target: 80, 85 or 90 Blood pressure achieved: 140/81, 141/83 and 144/85 Lancet 1998; 351:
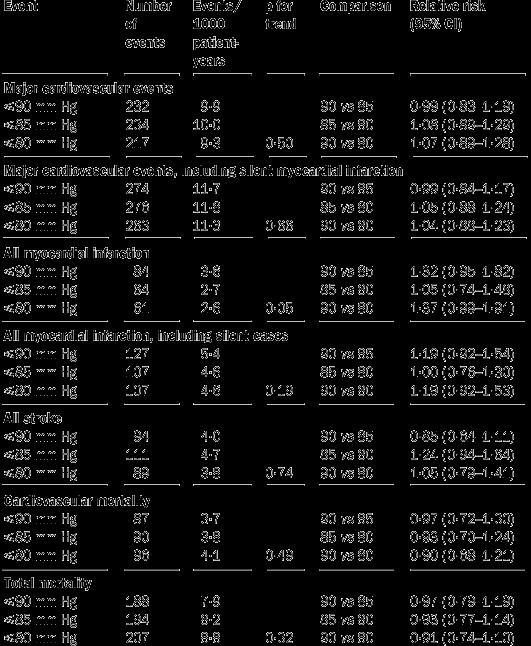
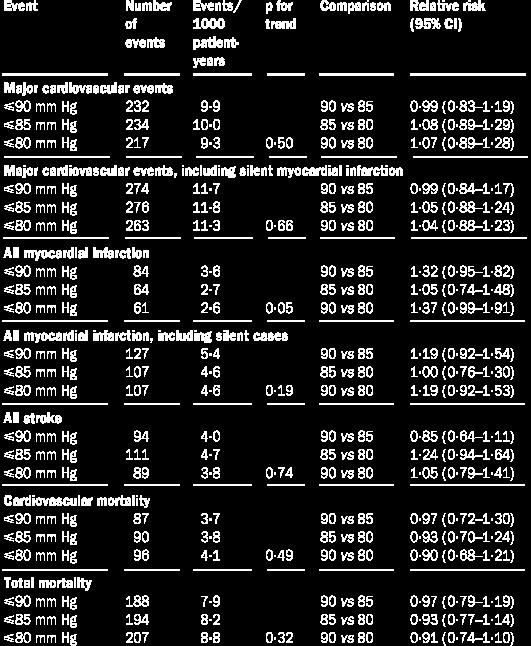
30 Overall

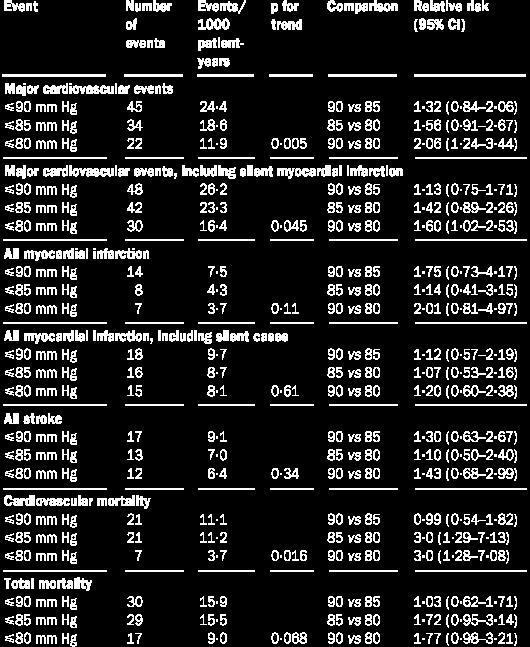
31 DM Patients
32 HOT Lowest Points of Risk Diastolic BP Systolic BP Major CV event Myocardial Infarction Stroke < CV Mortality
33 HOT Results No cardiovascular benefit of lower BP target in overall trial. In DM patients, there was a 51% reduction in major CVD events with intensive control.
34
35 Metanalysis included 13 studies (37,736 patients) Selection criteria; Randomized control trials Enrolled at least 100 patients with T2DM or IFG At least 1 year of follow up Achieved SBP 135 in intensive group and 140 in standard group Minimum difference in SBP of 3 mm Hg Outcomes Macrovascular events; [All cause mortality], [CV mortality], [MI], [stroke], [HF], [angina] and [revascularization] Microvascular events; [microalbuminuria], [nephropathy], [ESRD/Dialysis], [neuropathy] and [retinopathy]

36 Intensive versus standard blood pressure control and (A) all-cause mortality and (B) cardiovascular mortality. 10% reduction in all cause mortality in intensive group. Sripal Bangalore et al. Circulation. 2011;123: Copyright American Heart Association, Inc. All rights reserved.

37 Intensive versus standard blood pressure control and (A) myocardial infarction and (B) heart failure. Sripal Bangalore et al. Circulation. 2011;123: Copyright American Heart Association, Inc. All rights reserved.

38 Intensive versus standard blood pressure control and stroke. 17% reduction in stroke with intensive treatment 47% reduction in stroke with more intensive treatment Sripal Bangalore et al. Circulation. 2011;123: Copyright American Heart Association, Inc. All rights reserved.
39 Study Conclusions No single optimal SBP can be identified in all patients with T2DM. Intensive BP control ( 135) was associated with significant reduction in all cause mortality and stroke. More intensive BP lowering was only associated with lower risk for stroke and not other CV outcomes. There was 20% increase in risk of serious adverse effects with intensive control (40% with more intensive control).

40 Cochrane Database of Systematic Reviews 2017, Issue 10. Art. No.: CD DOI: / CD pub2.
41 Meta analysis of 5 studies; AASK (2002) ACCORD BP (2010) HOT (1998) Past BP (2016) SPRINT (2015) SPS3 (2013) All studies were RCT with >50 participants per group, and 6 months follow up. Objective: Determine if lower BP was associated with reduction in mortality and morbidity Population: Hypertension patients with CVD (MI, angina, stroke, PVD) BP targets: 135/85 versus /90 100) Outcome measures; Total mortality Cardiovascular events Cardiovascular mortality
42 Total Mortality Cochrane Database of Systematic Reviews 11 OCT 2017 DOI: / CD pub2
43 Cardiovascular Mortality There was a lower rate of cardiovascular events but no impact on CV mortality. Cochrane Database of Systematic Reviews 11 OCT 2017 DOI: / CD pub2
44 Conclusion No evidence of difference in mortality with lower BP target despite small reduction in cardiovascular events. Insufficient evidence to justify lower BP targets in this population. MORE TRIALS ARE NEEDED!!!!!
45 Current Recommendations
46 JNC 8 Population Age SBP DBP General 60 years <150 <90 <60 years <140 <90 CKD 18 years <140 <90 DM 18 years <140 <90
47 ADA BP recommendations Goal <140 systolic and 90 diastolic for most patients. Lower goal <130/80 or <120/80 for select patients with high ASCVD risk if lower BP can be achieved safely.
48 Kidney Disease Improving Global Outcomes (KDIGO) Non-DM patients with CKD (not on dialysis) 140 systolic and 90 diastolic if albumin excretion < systolic and 80 diastolic if albumin excretion >30 DM patients with CKD (not on dialysis) 140 systolic and 90 diastolic if albumin excretion < systolic and 80 diastolic if albumin excretion >30 Post transplant patients: 130 systolic and 80 diastolic KDIGO Blood Pressure Work Group. KDIGO Clinical Practice Guideline for the Management of Blood Pressure in Chronic Kidney Disease. Kidney inter., Suppl. 2012; 2:

49 Garber AJ et al. Endocr Pract. 2017,doi: /EP CS
50 AACE Hypertension Guidelines Hypertension Type Blood Pressure Goal Uncomplicated <140/90 Complicated Diabetes mellitus <130/80 # Kidney disease <130/80* Other high risk (stroke, MI) <130/80 #Less stringent if frail, comorbidities or adverse medication effects *Lower if proteinuria is >1 g/day ( 120/75). Alan J. Garber et al. AACE T2DM Algorithm, Executive Summary, Endocr Pract. 2017; 23(No. 2) Joseph J. Torre. AACE Hypertension Guidelines, Endocr Pract. 2006;12(No. 2)
51 Blood Pressure goal for T2DM? There is evidence of CVD benefit in lowering BP below 140 mm Hg in T2DM. In T2DM, BP target between 130/80 140/90 mm Hg is reasonable for most patients. Further BP lowering below 130/80 mm Hg is associated with reduced risk for stroke. Attempts to achieve lower BP goals result in increased risk for serious adverse effects. It is therefore important to balance risk of lower BP with risk for adverse effects of medication.
52 Summary Blood pressure is normally distributed with no specific cut off to definitely define hypertension. Variation in recommendations exists depending on the population studied. Studies on BP goals apply uniform targets to a population and do not reflect real life clinical scenarios. It is important to use clinical judgement and to individualize treatment targets.
53 Thank you.
The earlier BP control the better cardiovascular outcome. Jin Oh Na Cardiovascular center Korea University Medical College
 The earlier BP control the better cardiovascular outcome Jin Oh Na Cardiovascular center Korea University Medical College Index Introduction HOPE-3 Trial Sprint Study Summary Each 2 mmhg decrease in SBP
The earlier BP control the better cardiovascular outcome Jin Oh Na Cardiovascular center Korea University Medical College Index Introduction HOPE-3 Trial Sprint Study Summary Each 2 mmhg decrease in SBP
Blood Pressure Targets: Where are We Now?
 Blood Pressure Targets: Where are We Now? Diana Cao, PharmD, BCPS-AQ Cardiology Assistant Professor Department of Clinical & Administrative Sciences California Northstate University College of Pharmacy
Blood Pressure Targets: Where are We Now? Diana Cao, PharmD, BCPS-AQ Cardiology Assistant Professor Department of Clinical & Administrative Sciences California Northstate University College of Pharmacy
Hypertension targets: sorting out the confusion. Brian Rayner, Division of Nephrology and Hypertension, University of Cape Town
 Hypertension targets: sorting out the confusion Brian Rayner, Division of Nephrology and Hypertension, University of Cape Town Historical Perspective The most famous casualty of this approach was the
Hypertension targets: sorting out the confusion Brian Rayner, Division of Nephrology and Hypertension, University of Cape Town Historical Perspective The most famous casualty of this approach was the
ADVANCE post trial ObservatioNal Study
 Hot Topics in Diabetes 50 th EASD, Vienna 2014 ADVANCE post trial ObservatioNal Study Sophia Zoungas The George Institute The University of Sydney Rationale and Study Design Sophia Zoungas The George Institute
Hot Topics in Diabetes 50 th EASD, Vienna 2014 ADVANCE post trial ObservatioNal Study Sophia Zoungas The George Institute The University of Sydney Rationale and Study Design Sophia Zoungas The George Institute
Systolic Blood Pressure Intervention Trial (SPRINT)
") 09:30-09:50 2016.4.15 Systolic Blood Pressure Intervention Trial (SPRINT) IN A NEPHROLOGIST S VIEW Sejoong Kim Seoul National University Bundang Hospital Current guidelines for BP control Lowering BP
09:30-09:50 2016.4.15 Systolic Blood Pressure Intervention Trial (SPRINT) IN A NEPHROLOGIST S VIEW Sejoong Kim Seoul National University Bundang Hospital Current guidelines for BP control Lowering BP
Objectives. Describe results and implications of recent landmark hypertension trials
 Hypertension Update Daniel Schwartz, MD Assistant Professor of Medicine Associate Medical Director of Heart Transplantation Temple University School of Medicine Disclosures I currently have no relationships
Hypertension Update Daniel Schwartz, MD Assistant Professor of Medicine Associate Medical Director of Heart Transplantation Temple University School of Medicine Disclosures I currently have no relationships
4/4/17 HYPERTENSION TARGETS: WHAT DO WE DO NOW? SET THE STAGE BP IN CLINICAL TRIALS?
 HYPERTENSION TARGETS: WHAT DO WE DO NOW? MICHAEL LEFEVRE, MD, MSPH PROFESSOR AND VICE CHAIR DEPARTMENT OF FAMILY AND COMMUNITY MEDICINE UNIVERSITY OF MISSOURI 4/4/17 DISCLOSURE: MEMBER OF THE JNC 8 PANEL
HYPERTENSION TARGETS: WHAT DO WE DO NOW? MICHAEL LEFEVRE, MD, MSPH PROFESSOR AND VICE CHAIR DEPARTMENT OF FAMILY AND COMMUNITY MEDICINE UNIVERSITY OF MISSOURI 4/4/17 DISCLOSURE: MEMBER OF THE JNC 8 PANEL
The Diabetes Link to Heart Disease
 The Diabetes Link to Heart Disease Anthony Abe DeSantis, MD September 18, 2015 University of WA Division of Metabolism, Endocrinology and Nutrition Oswald Toosweet Case #1 68 yo M with T2DM Diagnosed DM
The Diabetes Link to Heart Disease Anthony Abe DeSantis, MD September 18, 2015 University of WA Division of Metabolism, Endocrinology and Nutrition Oswald Toosweet Case #1 68 yo M with T2DM Diagnosed DM
Hypertension and the SPRINT Trial: Is Lower Better
 Hypertension and the SPRINT Trial: Is Lower Better 8th Annual Orange County Symposium on Cardiovascular Disease Prevention Saturday, October 8, 2016 Keith C. Norris, MD, PhD, FASN Professor of Medicine,
Hypertension and the SPRINT Trial: Is Lower Better 8th Annual Orange County Symposium on Cardiovascular Disease Prevention Saturday, October 8, 2016 Keith C. Norris, MD, PhD, FASN Professor of Medicine,
Hypertension Management Controversies in the Elderly Patient
 Hypertension Management Controversies in the Elderly Patient Juan Bowen, MD Geriatric Update for the Primary Care Provider November 17, 2016 2016 MFMER slide-1 Disclosure No financial relationships No
Hypertension Management Controversies in the Elderly Patient Juan Bowen, MD Geriatric Update for the Primary Care Provider November 17, 2016 2016 MFMER slide-1 Disclosure No financial relationships No
The Latest Generation of Clinical
 The Latest Generation of Clinical Guidelines: HTN and HLD Dave Brackett Clinical Guideline Purpose Uniform approach Awareness of key details Diagnosis Treatment Monitoring Evidence based approach Inform
The Latest Generation of Clinical Guidelines: HTN and HLD Dave Brackett Clinical Guideline Purpose Uniform approach Awareness of key details Diagnosis Treatment Monitoring Evidence based approach Inform
Treating Hypertension in 2018: What Makes the Most Sense Today?
 Treating Hypertension in 2018: What Makes the Most Sense Today? Daniel Blanchard, MD Professor of Medicine UC San Diego Cardiovascular Center La Jolla, California 1 2 Speaker Disclosures Consultant and/or
Treating Hypertension in 2018: What Makes the Most Sense Today? Daniel Blanchard, MD Professor of Medicine UC San Diego Cardiovascular Center La Jolla, California 1 2 Speaker Disclosures Consultant and/or
HYPERTENSION: UPDATE 2018
 HYPERTENSION: UPDATE 2018 From the Cardiologist point of view Richard C Padgett, MD I have no disclosures HYPERTENSION ALWAYS THE ELEPHANT IN THE EXAM ROOM BUT SOMETIMES IT CHARGES HTN IN US ~78 million
HYPERTENSION: UPDATE 2018 From the Cardiologist point of view Richard C Padgett, MD I have no disclosures HYPERTENSION ALWAYS THE ELEPHANT IN THE EXAM ROOM BUT SOMETIMES IT CHARGES HTN IN US ~78 million
New Clinical Trends in Geriatric Medicine. April 8, 2016 Amanda Lathia, MD, MPhil Staff, Center for Geriatric Medicine
 New Clinical Trends in Geriatric Medicine April 8, 2016 Amanda Lathia, MD, MPhil Staff, Center for Geriatric Medicine Objectives Review current guidelines for blood pressure (BP) control in older adults
New Clinical Trends in Geriatric Medicine April 8, 2016 Amanda Lathia, MD, MPhil Staff, Center for Geriatric Medicine Objectives Review current guidelines for blood pressure (BP) control in older adults
DISCLOSURE PHARMACIST OBJECTIVES 9/30/2014 JNC 8: A REVIEW OF THE LONG-AWAITED/MUCH-ANTICIPATED HYPERTENSION GUIDELINES. I have nothing to disclose.
 JNC 8: A REVIEW OF THE LONG-AWAITED/MUCH-ANTICIPATED HYPERTENSION GUIDELINES Tiffany Dickey, PharmD Assistant Professor, UAMS COP Clinical Pharmacy Specialist, Mercy Hospital Northwest AR DISCLOSURE I
JNC 8: A REVIEW OF THE LONG-AWAITED/MUCH-ANTICIPATED HYPERTENSION GUIDELINES Tiffany Dickey, PharmD Assistant Professor, UAMS COP Clinical Pharmacy Specialist, Mercy Hospital Northwest AR DISCLOSURE I
Hypertension and Cardiovascular Disease
 Hypertension and Cardiovascular Disease Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any means graphic,
Hypertension and Cardiovascular Disease Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any means graphic,
Blood pressure treatment target in diabetes. Should it be <130 mmhg?
 Blood pressure treatment target in diabetes Should it be
Blood pressure treatment target in diabetes Should it be
Hypertension in 2015: SPRINT-ing ahead of JNC-8. MAJ Charles Magee, MD MPH FACP Director, WRNMMC Hypertension Clinic
 Hypertension in 2015: SPRINT-ing ahead of JNC-8 MAJ Charles Magee, MD MPH FACP Director, WRNMMC Hypertension Clinic Conflits of interest? None Disclaimer The opinions contained herein are not to be considered
Hypertension in 2015: SPRINT-ing ahead of JNC-8 MAJ Charles Magee, MD MPH FACP Director, WRNMMC Hypertension Clinic Conflits of interest? None Disclaimer The opinions contained herein are not to be considered
Hypertension Update Clinical Controversies Regarding Age and Race
 Hypertension Update Clinical Controversies Regarding Age and Race Allison Helmer, PharmD, BCACP Assistant Clinical Professor Auburn University Harrison School of Pharmacy July 22, 2017 DISCLOSURE/CONFLICT
Hypertension Update Clinical Controversies Regarding Age and Race Allison Helmer, PharmD, BCACP Assistant Clinical Professor Auburn University Harrison School of Pharmacy July 22, 2017 DISCLOSURE/CONFLICT
Hypertension Update. Mayo Clinic 90 th Annual Clinical Reviews November 2 nd and 16 th, 2016
 Mayo Clinic 90 th Annual Clinical Reviews November 2 nd and 16 th, 2016 Hypertension Update Vincent J. Canzanello, M.D. Consultant, Division of Nephrology and Hypertension Professor or Medicine College
Mayo Clinic 90 th Annual Clinical Reviews November 2 nd and 16 th, 2016 Hypertension Update Vincent J. Canzanello, M.D. Consultant, Division of Nephrology and Hypertension Professor or Medicine College
T. Suithichaiyakul Cardiomed Chula
 T. Suithichaiyakul Cardiomed Chula The cardiovascular (CV) continuum: role of risk factors Endothelial Dysfunction Atherosclerosis and left ventricular hypertrophy Myocardial infarction & stroke Endothelial
T. Suithichaiyakul Cardiomed Chula The cardiovascular (CV) continuum: role of risk factors Endothelial Dysfunction Atherosclerosis and left ventricular hypertrophy Myocardial infarction & stroke Endothelial
Hypertension and Diabetes Should we be SPRINTING or Reaching an ACCORD?
 Hypertension and Diabetes Should we be SPRINTING or Reaching an ACCORD? Suzanne Oparil, MD Distinguished Professor of Medicine, Professor of Cell, Developmental and Integrative Biology Director, Vascular
Hypertension and Diabetes Should we be SPRINTING or Reaching an ACCORD? Suzanne Oparil, MD Distinguished Professor of Medicine, Professor of Cell, Developmental and Integrative Biology Director, Vascular
What s the Goal? Individualizing Glycemic Targets. Matthew Freeby M.D. December 3 rd, 2016
 What s the Goal? Individualizing Glycemic Targets Matthew Freeby M.D. December 3 rd, 2016 Diabetes Mellitus: Complications and Co-Morbid Conditions Retinopathy Between 2005-2008, 28.5% of patients with
What s the Goal? Individualizing Glycemic Targets Matthew Freeby M.D. December 3 rd, 2016 Diabetes Mellitus: Complications and Co-Morbid Conditions Retinopathy Between 2005-2008, 28.5% of patients with
Diabetes Mellitus: A Cardiovascular Disease
 Diabetes Mellitus: A Cardiovascular Disease Nestoras Mathioudakis, M.D. Assistant Professor of Medicine Division of Endocrinology, Diabetes, & Metabolism September 30, 2013 1 The ABCs of cardiovascular
Diabetes Mellitus: A Cardiovascular Disease Nestoras Mathioudakis, M.D. Assistant Professor of Medicine Division of Endocrinology, Diabetes, & Metabolism September 30, 2013 1 The ABCs of cardiovascular
JNC 8 -Controversies. Sagren Naidoo Nephrologist CMJAH
 JNC 8 -Controversies Sagren Naidoo Nephrologist CMJAH Joint National Committee (JNC) Panel appointed by the National Heart, Lung, and Blood Institute (NHLBI) First guidelines (JNC-1) published in 1977
JNC 8 -Controversies Sagren Naidoo Nephrologist CMJAH Joint National Committee (JNC) Panel appointed by the National Heart, Lung, and Blood Institute (NHLBI) First guidelines (JNC-1) published in 1977
Why is Earlier and More Aggressive Treatment of T2 Diabetes Better?
 Blood glucose (mmol/l) Why is Earlier and More Aggressive Treatment of T2 Diabetes Better? Disclosures Dr Kennedy has provided CME, been on advisory boards or received travel or conference support from:
Blood glucose (mmol/l) Why is Earlier and More Aggressive Treatment of T2 Diabetes Better? Disclosures Dr Kennedy has provided CME, been on advisory boards or received travel or conference support from:
Hypertension Management in Diabetic Patients
 Hypertension Management in Diabetic Patients Park, Chang G, MD, PhD Cardiovascular Center, Guro Hospital, Korea University Medical School Contents (Treatment of 2 Cases) Type 2 Diabetes Mellitus Hypertension
Hypertension Management in Diabetic Patients Park, Chang G, MD, PhD Cardiovascular Center, Guro Hospital, Korea University Medical School Contents (Treatment of 2 Cases) Type 2 Diabetes Mellitus Hypertension
Blood Pressure LIMBO How Low To Go?
 Blood Pressure LIMBO How Low To Go? Joseph L. Kummer, MD, FACC Bryan Heart Spring Conference April 21 st, 2018 Hypertension Epidemiology Over a billion people have hypertension Major cause of morbidity
Blood Pressure LIMBO How Low To Go? Joseph L. Kummer, MD, FACC Bryan Heart Spring Conference April 21 st, 2018 Hypertension Epidemiology Over a billion people have hypertension Major cause of morbidity
Blood Pressure Targets in Diabetes
 Stockholm, 29 th August 2010 ESC Meeting Blood Pressure Targets in Diabetes Peter M Nilsson, MD, PhD Department of Clinical Sciences University Hospital, Malmö Sweden Studies on BP in DM2 ADVANCE RCT (Lancet
Stockholm, 29 th August 2010 ESC Meeting Blood Pressure Targets in Diabetes Peter M Nilsson, MD, PhD Department of Clinical Sciences University Hospital, Malmö Sweden Studies on BP in DM2 ADVANCE RCT (Lancet
Managing HTN in the Elderly: How Low to Go
 Managing HTN in the Elderly: How Low to Go Laxmi S. Mehta, MD, FACC The Ohio State University Medical Center Assistant Professor of Clinical Internal Medicine Clinical Director of the Women s Cardiovascular
Managing HTN in the Elderly: How Low to Go Laxmi S. Mehta, MD, FACC The Ohio State University Medical Center Assistant Professor of Clinical Internal Medicine Clinical Director of the Women s Cardiovascular
HYPERTENSION GUIDELINES WHERE ARE WE IN 2014
 HYPERTENSION GUIDELINES WHERE ARE WE IN 2014 Donald J. DiPette MD FACP Special Assistant to the Provost for Health Affairs Distinguished Health Sciences Professor University of South Carolina University
HYPERTENSION GUIDELINES WHERE ARE WE IN 2014 Donald J. DiPette MD FACP Special Assistant to the Provost for Health Affairs Distinguished Health Sciences Professor University of South Carolina University
Συμπεράσματα από τις νέες μελέτες για την αρτηριακή υπέρταση (SPRINT,PATHAY 2,HOPE 3)
") Συμπεράσματα από τις νέες μελέτες για την αρτηριακή υπέρταση (SPRINT,PATHAY 2,HOPE 3) Χάρης Γράσσος MD,FESC,PhD,EHS Διευθυντής Καρδιολόγος Γ.Ν.Α ΚΑΤ Visiting Professor University of Bolton U.K New England
Συμπεράσματα από τις νέες μελέτες για την αρτηριακή υπέρταση (SPRINT,PATHAY 2,HOPE 3) Χάρης Γράσσος MD,FESC,PhD,EHS Διευθυντής Καρδιολόγος Γ.Ν.Α ΚΑΤ Visiting Professor University of Bolton U.K New England
The New Hypertension Guidelines
 The New Hypertension Guidelines Joseph Saseen, PharmD Professor and Vice Chair, Department of Clinical Pharmacy University of Colorado Anschutz Medical Campus Disclosure Joseph Saseen reports no conflicts
The New Hypertension Guidelines Joseph Saseen, PharmD Professor and Vice Chair, Department of Clinical Pharmacy University of Colorado Anschutz Medical Campus Disclosure Joseph Saseen reports no conflicts
Managing Hypertension in Diabetes Sean Stewart, PharmD, BCPS, BCACP, CLS Internal Medicine Park Nicollet Clinic St Louis Park.
 Managing Hypertension in Diabetes 2015 Sean Stewart, PharmD, BCPS, BCACP, CLS Internal Medicine Park Nicollet Clinic St Louis Park Case Scenario Mike M is a 59 year old man with type 2 diabetes managed
Managing Hypertension in Diabetes 2015 Sean Stewart, PharmD, BCPS, BCACP, CLS Internal Medicine Park Nicollet Clinic St Louis Park Case Scenario Mike M is a 59 year old man with type 2 diabetes managed
Masked Hypertension. Why Should We Care? Dr. Peter J. Lin Director Primary Care Initiatives - Canadian Heart Research Centre
 Masked Hypertension Why Should We Care? Dr. Peter J. Lin Director Primary Care Initiatives - Canadian Heart Research Centre PRESENTER DISCLOSURE Faculty: Dr. Peter Lin Relationships with commercial interests:
Masked Hypertension Why Should We Care? Dr. Peter J. Lin Director Primary Care Initiatives - Canadian Heart Research Centre PRESENTER DISCLOSURE Faculty: Dr. Peter Lin Relationships with commercial interests:
ABCD and Renal Association Clinical Guidelines for Diabetic Nephropathy-CKD. Management of Dyslipidaemia and Hypertension in Adults Dr Peter Winocour
 ABCD and Renal Association Clinical Guidelines for Diabetic Nephropathy-CKD. Management of Dyslipidaemia and Hypertension in Adults Dr Peter Winocour Dr Indranil Dasgupta Rationale No national practical
ABCD and Renal Association Clinical Guidelines for Diabetic Nephropathy-CKD. Management of Dyslipidaemia and Hypertension in Adults Dr Peter Winocour Dr Indranil Dasgupta Rationale No national practical
Individualized Treatment Goals for Optimal Long-Term Health Outcomes among Patients with Type 2 Diabetes Mellitus
 1 Dissertation Title Page: Individualized Treatment Goals for Optimal Long-Term Health Outcomes among Patients with Type 2 Diabetes Mellitus Qian Shi, MPH, PhD candidate Department of Global Health Management
1 Dissertation Title Page: Individualized Treatment Goals for Optimal Long-Term Health Outcomes among Patients with Type 2 Diabetes Mellitus Qian Shi, MPH, PhD candidate Department of Global Health Management
ESC GUIDELINES ON DIABETES AND CARDIOVASCULAR DISEASES
 ESC GUIDELINES ON DIABETES AND CARDIOVASCULAR DISEASES Pr. Michel KOMAJDA Institute of Cardiology - IHU ICAN Pitie Salpetriere Hospital - University Pierre and Marie Curie, Paris (France) DEFINITION A
ESC GUIDELINES ON DIABETES AND CARDIOVASCULAR DISEASES Pr. Michel KOMAJDA Institute of Cardiology - IHU ICAN Pitie Salpetriere Hospital - University Pierre and Marie Curie, Paris (France) DEFINITION A
Prevention And Treatment of Diabetic Nephropathy. MOH Clinical Practice Guidelines 3/2006 Dr Stephen Chew Tec Huan
 Prevention And Treatment of Diabetic Nephropathy MOH Clinical Practice Guidelines 3/2006 Dr Stephen Chew Tec Huan Prevention Tight glucose control reduces the development of diabetic nephropathy Progression
Prevention And Treatment of Diabetic Nephropathy MOH Clinical Practice Guidelines 3/2006 Dr Stephen Chew Tec Huan Prevention Tight glucose control reduces the development of diabetic nephropathy Progression
Disclosures. Diabetes and Cardiovascular Risk Management. Learning Objectives. Atherosclerotic Cardiovascular Disease
 Disclosures Diabetes and Cardiovascular Risk Management Tony Hampton, MD, MBA Medical Director Advocate Aurora Operating System Advocate Aurora Healthcare Downers Grove, IL No conflicts or disclosures
Disclosures Diabetes and Cardiovascular Risk Management Tony Hampton, MD, MBA Medical Director Advocate Aurora Operating System Advocate Aurora Healthcare Downers Grove, IL No conflicts or disclosures
Firenze 22 settembre 2007
 Istituto di di medicina dello sport di di Firenze AMES Prevenzione cardiovascolare e cambiamenti negli stili di vita Firenze 22 settembre 2007 Orientamenti attuali per un intervento farmacologico e non
Istituto di di medicina dello sport di di Firenze AMES Prevenzione cardiovascolare e cambiamenti negli stili di vita Firenze 22 settembre 2007 Orientamenti attuali per un intervento farmacologico e non
ADVANCES IN MANAGEMENT OF HYPERTENSION
 Advances in Management of Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Current Status of Prevalence 29%; Blacks 33.5%
Advances in Management of Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Current Status of Prevalence 29%; Blacks 33.5%
Hypertension Update 2016 AREEF ISHANI, MD MS CHIEF OF MEDICINE MINNEAPOLIS VA MEDICAL CENTER PROFESSOR OF MEDICINE UNIVERSITY OF MINNESOTA
 Hypertension Update 2016 AREEF ISHANI, MD MS CHIEF OF MEDICINE MINNEAPOLIS VA MEDICAL CENTER PROFESSOR OF MEDICINE UNIVERSITY OF MINNESOTA Case 1 What should be your BP goal for an elderly (> 75 yrs of
Hypertension Update 2016 AREEF ISHANI, MD MS CHIEF OF MEDICINE MINNEAPOLIS VA MEDICAL CENTER PROFESSOR OF MEDICINE UNIVERSITY OF MINNESOTA Case 1 What should be your BP goal for an elderly (> 75 yrs of
Update on CVD and Microvascular Complications in T2D
 Update on CVD and Microvascular Complications in T2D Jay S. Skyler, MD, MACP Division of Endocrinology, Diabetes, and Metabolism and Diabetes Research Institute University of Miami Miller School of Medicine
Update on CVD and Microvascular Complications in T2D Jay S. Skyler, MD, MACP Division of Endocrinology, Diabetes, and Metabolism and Diabetes Research Institute University of Miami Miller School of Medicine
Update sulla terapia antiipertensiva e antiaggregante nel paziente cardiometabolico
 Update sulla terapia antiipertensiva e antiaggregante nel paziente cardiometabolico G. Mazzanti UO Cardiologia Ospedale SS. Annunziata, Cento (FE) AUSL di Ferrara Antiplatelet therapy Aspirin Aspirin:
Update sulla terapia antiipertensiva e antiaggregante nel paziente cardiometabolico G. Mazzanti UO Cardiologia Ospedale SS. Annunziata, Cento (FE) AUSL di Ferrara Antiplatelet therapy Aspirin Aspirin:
1. Albuminuria an early sign of glomerular damage and renal disease. albuminuria
 1. Albuminuria an early sign of glomerular damage and renal disease albuminuria Cardio-renal continuum REGRESS Target organ damage Asymptomatic CKD New risk factors Atherosclerosis Target organ damage
1. Albuminuria an early sign of glomerular damage and renal disease albuminuria Cardio-renal continuum REGRESS Target organ damage Asymptomatic CKD New risk factors Atherosclerosis Target organ damage
How to Reduce CVD Complications in Diabetes?
 How to Reduce CVD Complications in Diabetes? Chaicharn Deerochanawong M.D. Diabetes and Endocrinology Unit Department of Medicine Rajavithi Hospital, Ministry of Public Health Framingham Heart Study 30-Year
How to Reduce CVD Complications in Diabetes? Chaicharn Deerochanawong M.D. Diabetes and Endocrinology Unit Department of Medicine Rajavithi Hospital, Ministry of Public Health Framingham Heart Study 30-Year
Diabetes and Hypertension
 Diabetes and Hypertension William C. Cushman, MD, FAHA, FACP, FASH Chief, Preventive Medicine, Veterans Affairs Medical Center Professor, Preventive Medicine, Medicine, and Physiology University of Tennessee
Diabetes and Hypertension William C. Cushman, MD, FAHA, FACP, FASH Chief, Preventive Medicine, Veterans Affairs Medical Center Professor, Preventive Medicine, Medicine, and Physiology University of Tennessee
New Antihypertensive Strategies to Improve Blood Pressure Control
 New Antihypertensive Strategies to Improve Blood Pressure Control Antonio Coca, MD, PhD,, FRCP, FESC Hypertension and Vascular Risk Unit Department of Internal Medicine. Hospital Clínic (IDIBAPS) University
New Antihypertensive Strategies to Improve Blood Pressure Control Antonio Coca, MD, PhD,, FRCP, FESC Hypertension and Vascular Risk Unit Department of Internal Medicine. Hospital Clínic (IDIBAPS) University
Reframe the Paradigm of Hypertension treatment Focus on Diabetes
 Reframe the Paradigm of Hypertension treatment Focus on Diabetes Paola Atallah, MD Lecturer of Clinical Medicine SGUMC EDL monthly meeting October 25,2016 Overview Physiopathology of hypertension Classification
Reframe the Paradigm of Hypertension treatment Focus on Diabetes Paola Atallah, MD Lecturer of Clinical Medicine SGUMC EDL monthly meeting October 25,2016 Overview Physiopathology of hypertension Classification
Evaluation and Management of Hypertension in Women. Vesna D. Garovic, M.D. Moscow, Russia, December 2016
 Evaluation and Management of Hypertension in Women Vesna D. Garovic, M.D. Moscow, Russia, December 2016 2016 MFMER 3508058-1 Women are not small men There is nothing as powerful as an idea whose time has
Evaluation and Management of Hypertension in Women Vesna D. Garovic, M.D. Moscow, Russia, December 2016 2016 MFMER 3508058-1 Women are not small men There is nothing as powerful as an idea whose time has
Hypertension Controversies: SPRINTing to New Goals
 Hypertension Controversies: SPRINTing to New Goals Diana Isaacs, PharmD, BCPS, BC-ADM, CDE Clinical Pharmacy Specialist Cleveland Clinic Lauren Wolfe, PharmD Primary Care Clinical Specialist Cleveland
Hypertension Controversies: SPRINTing to New Goals Diana Isaacs, PharmD, BCPS, BC-ADM, CDE Clinical Pharmacy Specialist Cleveland Clinic Lauren Wolfe, PharmD Primary Care Clinical Specialist Cleveland
Felix Vallotton Ball (1899) LDL-C management in Asian diabetes: moderate vs. high intensity statin --- a lesson from EMPATHY study
 LDL-C management in Asian diabetes: moderate vs. high intensity statin --- a lesson from EMPATHY study") Felix Vallotton Ball (1899) LDL-C management in Asian diabetes: moderate vs. high intensity statin --- a lesson from EMPATHY study Conflict of interest disclosure None Committee of Scientific Affairs Committee
Felix Vallotton Ball (1899) LDL-C management in Asian diabetes: moderate vs. high intensity statin --- a lesson from EMPATHY study Conflict of interest disclosure None Committee of Scientific Affairs Committee
Hypertension. Does it Matter What Medications We Use? Nishant K. Sekaran, M.D. M.Sc. Intermountain Heart Institute
 Hypertension Does it Matter What Medications We Use? Nishant K. Sekaran, M.D. M.Sc. Intermountain Heart Institute Hypertension 2017 Classification BP Category Systolic Diastolic Normal 120 and 80 Elevated
Hypertension Does it Matter What Medications We Use? Nishant K. Sekaran, M.D. M.Sc. Intermountain Heart Institute Hypertension 2017 Classification BP Category Systolic Diastolic Normal 120 and 80 Elevated
A Fork in the Road: Navigating Through New Terrain
 A Fork in the Road: Navigating Through New Terrain Carol Hatch Wysham, MD Clinical Associate Professor of Medicine University of Washington School of Medicine Section Head, Rockwood Center for Diabetes
A Fork in the Road: Navigating Through New Terrain Carol Hatch Wysham, MD Clinical Associate Professor of Medicine University of Washington School of Medicine Section Head, Rockwood Center for Diabetes
ADVANCES IN MANAGEMENT OF HYPERTENSION
 Prevalence 29%; Blacks 33.5% About 72.5% treated; 53.5% uncontrolled (>140/90) Risk for poor control: Latinos, Blacks, age 18-44 and 80,
Prevalence 29%; Blacks 33.5% About 72.5% treated; 53.5% uncontrolled (>140/90) Risk for poor control: Latinos, Blacks, age 18-44 and 80,
What s In the New Hypertension Guidelines?
 American College of Physicians Ohio/Air Force Chapters 2018 Scientific Meeting Columbus, OH October 5, 2018 What s In the New Hypertension Guidelines? Max C. Reif, MD, FACP Objectives: At the end of the
American College of Physicians Ohio/Air Force Chapters 2018 Scientific Meeting Columbus, OH October 5, 2018 What s In the New Hypertension Guidelines? Max C. Reif, MD, FACP Objectives: At the end of the
Treating Hypertension in Individuals with Diabetes
 Treating Hypertension in Individuals with Diabetes Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any
Treating Hypertension in Individuals with Diabetes Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any
Tread Carefully Because you Tread on my Nephrons. Prescribing Hints in Renal Disease
 Tread Carefully Because you Tread on my Nephrons Prescribing Hints in Renal Disease David WP Lappin,, MB PhD FRCPI Clinical Lecturer in Medicine and Consultant Nephrologist and General Physician, Merlin
Tread Carefully Because you Tread on my Nephrons Prescribing Hints in Renal Disease David WP Lappin,, MB PhD FRCPI Clinical Lecturer in Medicine and Consultant Nephrologist and General Physician, Merlin
Managing Hypertension in 2018
 MANAGING HYPERTENSION IN 2018 How Do We Work With Conflicting Data and Conflicting Guidelines? Disclosure No relevant financial relationships Robert B. Baron, MD MS Professor and Associate Dean UCSF School
MANAGING HYPERTENSION IN 2018 How Do We Work With Conflicting Data and Conflicting Guidelines? Disclosure No relevant financial relationships Robert B. Baron, MD MS Professor and Associate Dean UCSF School
Disclosure. No relevant financial relationships. Placebo-Controlled Statin Trials
 PREVENTING CARDIOVASCULAR DISEASE IN WOMEN: Current Guidelines for Hypertension, Lipids and Aspirin Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial
PREVENTING CARDIOVASCULAR DISEASE IN WOMEN: Current Guidelines for Hypertension, Lipids and Aspirin Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial
J-curve Revisited. An Analysis of Blood Pressure and Cardiovascular Events in the Treating to New Targets (TNT) Trial
 Trial") J-curve Revisited An Analysis of Blood Pressure and Cardiovascular Events in the Treating to New Targets (TNT) Trial Sripal Bangalore, MD, MHA, Franz H Messerli, MD, Chuan-Chuan Wun, PhD, Andrea L. Zuckerman,
J-curve Revisited An Analysis of Blood Pressure and Cardiovascular Events in the Treating to New Targets (TNT) Trial Sripal Bangalore, MD, MHA, Franz H Messerli, MD, Chuan-Chuan Wun, PhD, Andrea L. Zuckerman,
Diabetes and Hypertension
 Diabetes and Hypertension M.Nakhjvani,M.D Tehran University of Medical Sciences 20-8-96 Hypertension Common DM comorbidity Prevalence depends on diabetes type, age, BMI, ethnicity Major risk factor for
Diabetes and Hypertension M.Nakhjvani,M.D Tehran University of Medical Sciences 20-8-96 Hypertension Common DM comorbidity Prevalence depends on diabetes type, age, BMI, ethnicity Major risk factor for
None. Disclosure: Relationships with Industry Conflicts of Interests. Learning Objectives: Participants will be able to:
 2014 Evidence-Based Guideline for the Management of High Blood Pressure in Adults: Report from the Panel Members Appointed to the Eighth Joint National Committee (JNC 8) James W. Shaw, MD Memorial Lecture
2014 Evidence-Based Guideline for the Management of High Blood Pressure in Adults: Report from the Panel Members Appointed to the Eighth Joint National Committee (JNC 8) James W. Shaw, MD Memorial Lecture
Cardiovascular Risk Reduction and Other Co-Morbidities in Type 2 Diabetes
 Cardiovascular Risk Reduction and Other Co-Morbidities in Type 2 Diabetes Following this presentation, you will be able to: Describe the relationship between major CV risk factors and CVD outcomes Select
Cardiovascular Risk Reduction and Other Co-Morbidities in Type 2 Diabetes Following this presentation, you will be able to: Describe the relationship between major CV risk factors and CVD outcomes Select
A factorial randomized trial of blood pressure lowering and intensive glucose control in 11,140 patients with type 2 diabetes
 A factorial randomized trial of blood pressure lowering and intensive glucose control in 11,140 patients with type 2 diabetes Hypotheses: Among individuals with type 2 diabetes, the risks of major microvascular
A factorial randomized trial of blood pressure lowering and intensive glucose control in 11,140 patients with type 2 diabetes Hypotheses: Among individuals with type 2 diabetes, the risks of major microvascular
Diabetes Mellitus: Implications of New Clinical Trials and New Medications
 Diabetes Mellitus: Implications of New Clinical Trials and New Medications Estimates of Diagnosed Diabetes in Adults, 2005 Alka M. Kanaya, MD Asst. Professor of Medicine UCSF, Primary Care CME October
Diabetes Mellitus: Implications of New Clinical Trials and New Medications Estimates of Diagnosed Diabetes in Adults, 2005 Alka M. Kanaya, MD Asst. Professor of Medicine UCSF, Primary Care CME October
Management of Lipid Disorders and Hypertension: Implications of the New Guidelines
 Management of Lipid Disorders and Hypertension Management of Lipid Disorders and Hypertension: Implications of the New Guidelines Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine
Management of Lipid Disorders and Hypertension Management of Lipid Disorders and Hypertension: Implications of the New Guidelines Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine
Complications of Diabetes: Screening and Prevention
 Complications of Diabetes: Screening and Prevention Dr Steve Cleland Consultant Physician GGH and QEUH Diabetes Staff Education Course June 17 Diabetic Complications Microvascular: Retinopathy Nephropathy
Complications of Diabetes: Screening and Prevention Dr Steve Cleland Consultant Physician GGH and QEUH Diabetes Staff Education Course June 17 Diabetic Complications Microvascular: Retinopathy Nephropathy
Management of Cardiovascular Disease in Diabetes
 Management of Cardiovascular Disease in Diabetes Radha J. Sarma, MBBS, FACP. FACC. FAHA. FASE Professor of Internal Medicine Western University of Health Sciences. Director, Heart and Vascular Center Western
Management of Cardiovascular Disease in Diabetes Radha J. Sarma, MBBS, FACP. FACC. FAHA. FASE Professor of Internal Medicine Western University of Health Sciences. Director, Heart and Vascular Center Western
Diabetes and kidney disease.
 Diabetes and kidney disease. What are the implications? Can it be prevented? Nice 18 june 2010 Lars G Weiss. M.D. Ph.D. Department of Neprology Central Hospital Karlstad Sweden Diabetic nephropathy vs
Diabetes and kidney disease. What are the implications? Can it be prevented? Nice 18 june 2010 Lars G Weiss. M.D. Ph.D. Department of Neprology Central Hospital Karlstad Sweden Diabetic nephropathy vs
Difficult to Treat Hypertension
 Difficult to Treat Hypertension According to Goldilocks JNC 8 Blood Pressure Goals (2014) BP Goal 60 years old and greater*- systolic < 150 and diastolic < 90. (Grade A)** BP Goal 18-59 years old* diastolic
Difficult to Treat Hypertension According to Goldilocks JNC 8 Blood Pressure Goals (2014) BP Goal 60 years old and greater*- systolic < 150 and diastolic < 90. (Grade A)** BP Goal 18-59 years old* diastolic
American Diabetes Association Standards of Medical Care in Diabetes 2017: Focus on Complications
 American Diabetes Association Standards of Medical Care in Diabetes 2017: Focus on Complications Juan Pablo Frias, M.D., FACE President and CEO, National Research Institute, Los Angeles, CA Clinical Faculty,
American Diabetes Association Standards of Medical Care in Diabetes 2017: Focus on Complications Juan Pablo Frias, M.D., FACE President and CEO, National Research Institute, Los Angeles, CA Clinical Faculty,
Guest Speaker Evaluations Viewer Call-In Thanks to our Sponsors: Phone: Fax: Public Health Live T 2 B 2
 Public Health Live T 2 B 2 Chronic Kidney Disease in Diabetes: Early Identification and Intervention Guest Speaker Joseph Vassalotti, MD, FASN Chief Medical Officer National Kidney Foundation Thanks to
Public Health Live T 2 B 2 Chronic Kidney Disease in Diabetes: Early Identification and Intervention Guest Speaker Joseph Vassalotti, MD, FASN Chief Medical Officer National Kidney Foundation Thanks to
Disclosures. Hypertension: Nationwide Dilemma. Learning Objectives. What s Currently Recommended? Specific Concerns 3/9/2012
 How Should We ACCOMPLISH Good Blood Pressure Control In Our VETS? Disclosures No conflicts of interest to disclose Updates in the Management of HypertensionIn the Elderly Antoine T. Jenkins, Pharm.D.,
How Should We ACCOMPLISH Good Blood Pressure Control In Our VETS? Disclosures No conflicts of interest to disclose Updates in the Management of HypertensionIn the Elderly Antoine T. Jenkins, Pharm.D.,
New Lipid Guidelines. PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN: Implications of the New Guidelines for Hypertension and Lipids.
 PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN: Implications of the New Guidelines for Hypertension and Lipids Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Disclosure No relevant
PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN: Implications of the New Guidelines for Hypertension and Lipids Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Disclosure No relevant
Hypertension Guidelines: Are We Pressured to Change? Oregon Cardiovascular Symposium Portland, Oregon June 6, Financial Disclosures
 Hypertension Guidelines: Are We Pressured to Change? Oregon Cardiovascular Symposium Portland, Oregon June 6, 2015 William C. Cushman, MD Professor, Preventive Medicine, Medicine, and Physiology University
Hypertension Guidelines: Are We Pressured to Change? Oregon Cardiovascular Symposium Portland, Oregon June 6, 2015 William C. Cushman, MD Professor, Preventive Medicine, Medicine, and Physiology University
Combination Therapy for Hypertension
 Combination Therapy for Hypertension Se-Joong Rim, MD Cardiology Division, Yonsei University College of Medicine, Seoul, Korea Goals of Therapy Reduce CVD and renal morbidity and mortality. Treat to BP
Combination Therapy for Hypertension Se-Joong Rim, MD Cardiology Division, Yonsei University College of Medicine, Seoul, Korea Goals of Therapy Reduce CVD and renal morbidity and mortality. Treat to BP
American Academy of Insurance Medicine
 American Academy of Insurance Medicine October 2012 Dr. Alison Moy Liberty Mutual Dr. John Kirkpatrick Thrivent Financial for Lutherans 1 59 year old male, diagnosed with T2DM six months ago Nonsmoker
American Academy of Insurance Medicine October 2012 Dr. Alison Moy Liberty Mutual Dr. John Kirkpatrick Thrivent Financial for Lutherans 1 59 year old male, diagnosed with T2DM six months ago Nonsmoker
Oral Hypoglycemics and Risk of Adverse Cardiac Events: A Summary of the Controversy
 Oral Hypoglycemics and Risk of Adverse Cardiac Events: A Summary of the Controversy Jeffrey Boord, MD, MPH Advances in Cardiovascular Medicine Kingston, Jamaica December 7, 2012 VanderbiltHeart.com Outline
Oral Hypoglycemics and Risk of Adverse Cardiac Events: A Summary of the Controversy Jeffrey Boord, MD, MPH Advances in Cardiovascular Medicine Kingston, Jamaica December 7, 2012 VanderbiltHeart.com Outline
Objective & Outline. How the JNC Process Has Evolved. Expertise Represented on JNC 8 Panel
 Implementation: Joint National Committee on High Blood Pressure JNC 8 Joel Handler, MD Kaiser Permanente Care Management Institute Hypertension Lead Southern California Permanente Group Objective & Outline
Implementation: Joint National Committee on High Blood Pressure JNC 8 Joel Handler, MD Kaiser Permanente Care Management Institute Hypertension Lead Southern California Permanente Group Objective & Outline
Management of Hypertension. M Misra MD MRCP (UK) Division of Nephrology University of Missouri School of Medicine
 Division of Nephrology University of Missouri School of Medicine") Management of Hypertension M Misra MD MRCP (UK) Division of Nephrology University of Missouri School of Medicine Disturbing Trends in Hypertension HTN awareness, treatment and control rates are decreasing
Management of Hypertension M Misra MD MRCP (UK) Division of Nephrology University of Missouri School of Medicine Disturbing Trends in Hypertension HTN awareness, treatment and control rates are decreasing
The Clinical Unmet need in the patient with Diabetes and ACS
 The Clinical Unmet need in the patient with Diabetes and ACS Professor Kausik Ray (UK) BSc(hons), MBChB, MD, MPhil, FRCP (lon), FRCP (ed), FACC, FESC, FAHA Diabetes is a global public health challenge
The Clinical Unmet need in the patient with Diabetes and ACS Professor Kausik Ray (UK) BSc(hons), MBChB, MD, MPhil, FRCP (lon), FRCP (ed), FACC, FESC, FAHA Diabetes is a global public health challenge
Management of Type 2 Diabetes Cardiovascular Outcomes Trials Tom Blevins MD Texas Diabetes and Endocrinology Austin, Texas
 Management of Type 2 Diabetes Cardiovascular Outcomes Trials 2018 Tom Blevins MD Texas Diabetes and Endocrinology Austin, Texas Speaker Disclosure Dr. Blevins has disclosed that he has received grant support
Management of Type 2 Diabetes Cardiovascular Outcomes Trials 2018 Tom Blevins MD Texas Diabetes and Endocrinology Austin, Texas Speaker Disclosure Dr. Blevins has disclosed that he has received grant support
Modern Management of Hypertension
 Modern Management of Hypertension Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Current Status of Hypertension Prevalence
Modern Management of Hypertension Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Current Status of Hypertension Prevalence
Predicting and changing the future for people with CKD
 Predicting and changing the future for people with CKD I. David Weiner, M.D. Co-holder, C. Craig and Audrae Tisher Chair in Nephrology Professor of Medicine and Physiology and Functional Genomics University
Predicting and changing the future for people with CKD I. David Weiner, M.D. Co-holder, C. Craig and Audrae Tisher Chair in Nephrology Professor of Medicine and Physiology and Functional Genomics University
Implications of Drug-related Increases in Blood Pressure
 Implications of Drug-related Increases in Blood Pressure Preston M. Dunnmon, MD, FACP, FACC Division of Cardiovascular and Renal Products US Food and Drug Administration July 18, 2012 Disclaimer The findings
Implications of Drug-related Increases in Blood Pressure Preston M. Dunnmon, MD, FACP, FACC Division of Cardiovascular and Renal Products US Food and Drug Administration July 18, 2012 Disclaimer The findings
Cedars Sinai Diabetes. Michael A. Weber
 Cedars Sinai Diabetes Michael A. Weber Speaker Disclosures I disclose that I am a Consultant for: Ablative Solutions, Boston Scientific, Boehringer Ingelheim, Eli Lilly, Forest, Medtronics, Novartis, ReCor
Cedars Sinai Diabetes Michael A. Weber Speaker Disclosures I disclose that I am a Consultant for: Ablative Solutions, Boston Scientific, Boehringer Ingelheim, Eli Lilly, Forest, Medtronics, Novartis, ReCor
Outline. Outline 10/14/2014 CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW. Question 1: Which of these patients has CKD?
 CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW MICHAEL G. SHLIPAK, MD, MPH CHIEF-GENERAL INTERNAL MEDICINE, SAN FRANCISCO VA MEDICAL CENTER PROFESSOR OF MEDICINE, EPIDEMIOLOGY AND BIOSTATISTICS,
CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW MICHAEL G. SHLIPAK, MD, MPH CHIEF-GENERAL INTERNAL MEDICINE, SAN FRANCISCO VA MEDICAL CENTER PROFESSOR OF MEDICINE, EPIDEMIOLOGY AND BIOSTATISTICS,
PROTECTING YOUR SWEET HEART
 PROTECTING YOUR SWEET HEART Cardiovascular risk reducdon in diabetes too many choices and so much confusion! Dr. Arden Barry, BSc, BSc(Pharm), PharmD, ACPR Clinical Pharmacy and Research Specialist, Chilliwack
PROTECTING YOUR SWEET HEART Cardiovascular risk reducdon in diabetes too many choices and so much confusion! Dr. Arden Barry, BSc, BSc(Pharm), PharmD, ACPR Clinical Pharmacy and Research Specialist, Chilliwack
Angiotensin Converting Enzyme inhibitor (ACEi) / Angiotensin Receptor Blocker (ARB) To STOP OR Not in Advanced Renal Disease
 / Angiotensin Receptor Blocker (ARB) To STOP OR Not in Advanced Renal Disease") Angiotensin Converting Enzyme inhibitor (ACEi) / Angiotensin Receptor Blocker (ARB) To STOP OR Not in Advanced Renal Disease Investigator Meeting 12 th September 2017 - Sheffield Prof Sunil Bhandari Consultant
Angiotensin Converting Enzyme inhibitor (ACEi) / Angiotensin Receptor Blocker (ARB) To STOP OR Not in Advanced Renal Disease Investigator Meeting 12 th September 2017 - Sheffield Prof Sunil Bhandari Consultant
Hypertension Update 2009
 Hypertension Update 2009 New Drugs, New Goals, New Approaches, New Lessons from Clinical Trials Timothy C Fagan, MD, FACP Professor Emeritus University of Arizona New Drugs Direct Renin Inhibitors Endothelin
Hypertension Update 2009 New Drugs, New Goals, New Approaches, New Lessons from Clinical Trials Timothy C Fagan, MD, FACP Professor Emeritus University of Arizona New Drugs Direct Renin Inhibitors Endothelin
Hypertension Putting the Guidelines into Practice
 Hypertension 2017 Putting the Guidelines into Practice Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or
Hypertension 2017 Putting the Guidelines into Practice Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or
Standards of Medical Care in Diabetes 2016
 Standards of Medical Care in Diabetes 2016 Care Delivery Systems 33-49% of patients still do not meet targets for A1C, blood pressure, or lipids. 14% meet targets for all A1C, BP, lipids, and nonsmoking
Standards of Medical Care in Diabetes 2016 Care Delivery Systems 33-49% of patients still do not meet targets for A1C, blood pressure, or lipids. 14% meet targets for all A1C, BP, lipids, and nonsmoking
The target blood pressure in patients with diabetes is <130 mm Hg
 Controversies in hypertension, About Diabetes diabetes and and metabolic Cardiovascular syndrome Risk ESC annual congress August 29, 2011 The target blood pressure in patients with diabetes is
Controversies in hypertension, About Diabetes diabetes and and metabolic Cardiovascular syndrome Risk ESC annual congress August 29, 2011 The target blood pressure in patients with diabetes is
Eugene Barrett M.D., Ph.D. University of Virginia 6/18/2007. Diagnosis and what is it Glucose Tolerance Categories FPG
 Diabetes Mellitus: Update 7 What is the unifying basis of this vascular disease? Eugene J. Barrett, MD, PhD Professor of Internal Medicine and Pediatrics Director, Diabetes Center and GCRC Health System
Diabetes Mellitus: Update 7 What is the unifying basis of this vascular disease? Eugene J. Barrett, MD, PhD Professor of Internal Medicine and Pediatrics Director, Diabetes Center and GCRC Health System
Updates in Diabetes and Cardiovascular Disease Management: Are You Making the Link?
 Updates in Diabetes and Cardiovascular Disease Management: Are You Making the Link? Denise Kolanczyk, PharmD, BCPS AQ Cardiology 1 Erika Hellenbart, PharmD, BCPS 2 Jennifer D Souza, PharmD, CDE, BC ADM
Updates in Diabetes and Cardiovascular Disease Management: Are You Making the Link? Denise Kolanczyk, PharmD, BCPS AQ Cardiology 1 Erika Hellenbart, PharmD, BCPS 2 Jennifer D Souza, PharmD, CDE, BC ADM
RATIONALE. chapter 4 & 2012 KDIGO
 http://www.kidney-international.org chapter 4 & 2012 KDIGO Chapter 4: Blood pressure management in CKD ND patients with diabetes mellitus Kidney International Supplements (2012) 2, 363 369; doi:10.1038/kisup.2012.54
http://www.kidney-international.org chapter 4 & 2012 KDIGO Chapter 4: Blood pressure management in CKD ND patients with diabetes mellitus Kidney International Supplements (2012) 2, 363 369; doi:10.1038/kisup.2012.54
Metformin should be considered in all patients with type 2 diabetes unless contra-indicated
 November 2001 N P S National Prescribing Service Limited PPR fifteen Prescribing Practice Review PPR Managing type 2 diabetes For General Practice Key messages Metformin should be considered in all patients
November 2001 N P S National Prescribing Service Limited PPR fifteen Prescribing Practice Review PPR Managing type 2 diabetes For General Practice Key messages Metformin should be considered in all patients
Preventing and Treating High Blood Pressure
 Preventing and Treating High Blood Pressure: Finding the Right Balance of Integrative and Pharmacologic Approaches Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Blood Pressure
Preventing and Treating High Blood Pressure: Finding the Right Balance of Integrative and Pharmacologic Approaches Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Blood Pressure