INTRAVENOUS FLUID THERAPY. Tom Heaps Consultant Acute Physician
|
|
|
- Roderick Farmer
- 5 years ago
- Views:
Transcription
1 INTRAVENOUS FLUID THERAPY Tom Heaps Consultant Acute Physician
2 LEARNING OBJECTIVES 1. Crystalloids vs colloids 2. Balanced vs non-balanced solutions 3. Composition of various IV fluids 4. What is normal about Normal Saline? 5. Goals of fluid therapy 6. Recognizing and managing hypovolaemia 7. Daily electrolyte and fluid requirements 8. Maintenance, Replacement and Redistribution 9. Summary: The 5 Rs and NICE CG174


3 WHAT IS THE PROBLEM WITH FLUID THERAPY? Cautious IV Fluids....Because the patient has angina?!


4 THE POPCORN MODEL OF FLUID THERAPY Daily fluid requirement = +
 of fluid? 5. What rate (how fast)? > POLL ENGAGE BRAIN!")
5 QUESTIONS TO ASK BEFORE PRESCRIBING FLUID 1. Does my patient need IV fluid? 2. For what purpose? 3. What type of fluid? 4. What amount (volume) of fluid? 5. What rate (how fast)? > POLL ENGAGE BRAIN!
6 DAILY ELECTROLYTE REQUIREMENTS 1. Sodium 1-2mmol/kg/d (70-140mmol/d) Serum concentration 140mmol/L 2. Potassium 0.5-1mmol/kg/d (35-70mmol/d) Serum concentration 4mmol/L 1mmol/kg/d of each 3. Chloride 1mmol/kg/d (70mmol/d) Serum concentration 100mmol/L
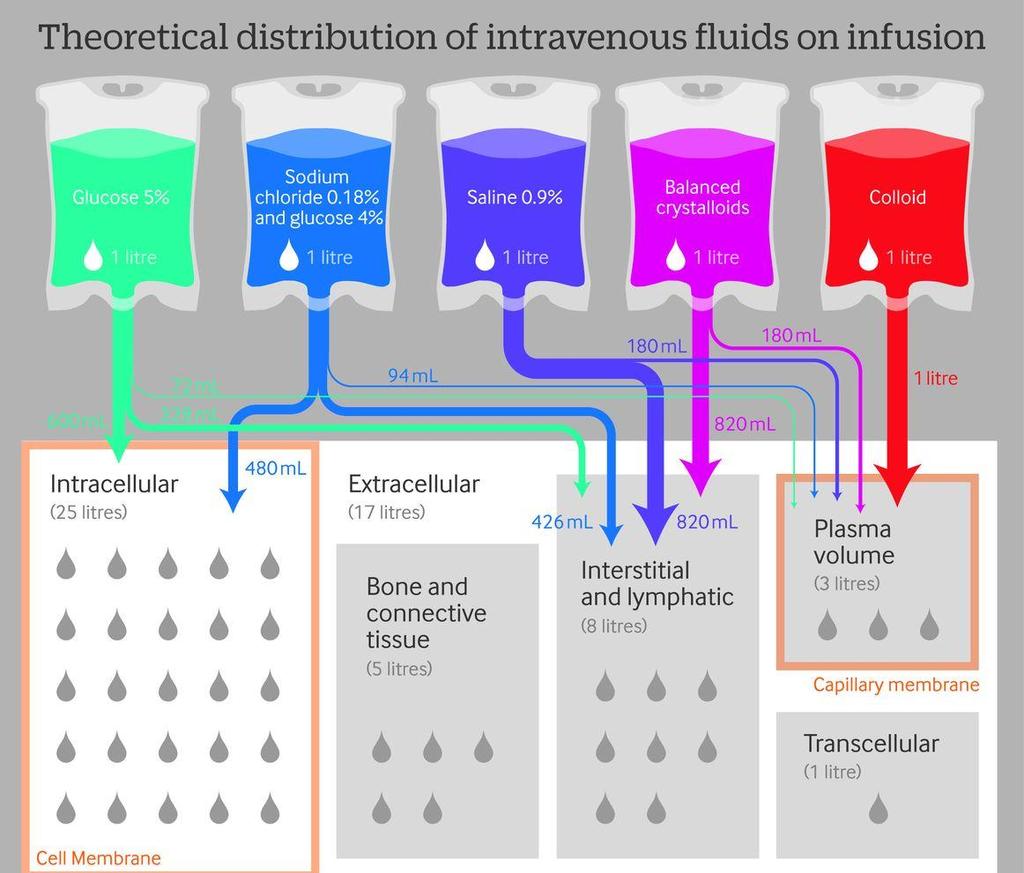
7 WHAT S IN YOUR CUPBOARD? 1. Crystalloids (hopefully) Isotonic ( normal ) 0.9% saline +/ mmol KCl Hartmann s solution 5% and 10% glucose 4% glucose/0.18% saline ( dex-saline ) +/ mmol KCl Plasmalyte 148 (if you are lucky) 2. Colloids (possibly) Albumins Gelatins e.g. Gelofusine, Volplex Starches > POLL
8 WHAT S NORMAL ABOUT NORMAL SALINE? Tonicity ( isotonic.almost) osmolality 308mOsmol/L (plasma mOsmol/L)..and not a lot else! Sodium 154mmol/L (140mmol/L) Chloride 154mmol/L (100mmol/L) ph 5.5 (7.4) Potassium 0mmol/L (4mmol/L) > POLL
9 COMPOSITION OF DIFFERENT CRYSTALLOIDS Content (mmol/l) Plasma 0.9% Saline Hartmann s Plasmalyte 148 5% Glucose 0.18% Saline-4% Glcuose Sodium Potassium Chloride Lactate etc. < (gluconate 23, acetate 27) 0 Calcium (Mg 1.5) 0 0 Glucose (50g) 222 (40g) ph Osmolality
10 WHAT HAPPENS IF YOU GIVE NORMAL SALINE? ph depends on difference between strong +ve ions (e.g. Na + ) and strong ve ions (e.g. (Cl - ) = strong ion difference (Stewart s Theory) Physiological strong ion difference 40mmol/L ( ) 0.9% Saline contains 154mmol/L Na + and 154mmol/L Cl - Chloride rises disproportionately to sodium reducing the strong ion gap and resulting in (hyperchloraemic) acidosis Renal vasoconstriction and impaired secretion of sodium Clinicians often respond to acidosis by giving more fluids Don t forget, 0.9% saline is also present in colloids e.g. HAS, Gelofusine, Volplex, Voluven Balanced colloids now available e.g. Gelaspan, Isoplex, Volulyte
11 MYTHS ABOUT BALANCED CRYSTALLOIDS but it s got potassium in it Hyperchloraemia causes acidosis which exacerbates hyperkalaemia Normal saline may raise [K + ] more than balanced solutions in AKI but it s got lactate in it O Malley et al, Anesthesia and Analgesia, 2005 Lactate per se is not bad for you: it is a marker of disease severity Lactate in Hartmann s lactic acid; it is a conjugate base (potential HCO 3- ) and will NEVER increase acidosis The patient will be making a lot more lactate (1500mmol/d in health) than you will be giving therefore effect on total body lactate negligible
12 THE GREAT FLUID DEBATE CONTINUES Balanced vs non-balanced crystalloids 0.9% Saline slightly cheaper than Hartmann s ( 0.78/L vs 1.00/L) but is associated with hyperchloraemic acidosis: Potential for renal vasoconstriction (AKI and hyperkalaemia), impaired GI perfusion and coagulopathy Relevance in terms of clinical outcomes uncertain (large trials on-going) Crystalloids vs colloids Equivalent patient outcomes in most studies Colloids associated with greater expense, risk of anaphylaxis, coagulopathy and increased risk of AKI (especially starches - withdrawn) Albumin probably reasonable choice in sepsis?
13 FLUID THERAPY: BACK TO BASICS Restore circulating volume Diagnosis and treatment of hypovolaemia Correct dehydration Reduced total body water with preservation of circulating volume Maintain circulating volume and electrolytes Understand and anticipate physiological requirements
14 RECOGNIZING & TREATING HYPOVOLAEMIA 1. Vital signs and MEWS 2. Diagnostic tests 3. CVP and oliguria 4. The fluid challenge Treating Hypotension Hypovolaemia Record patient Tachycardia observations Central Urine Venous output (Oliguria) Pressure Choose Tachypnoea your weapon! Does Cannot not describe Delayed diagnose euvolaemia capillary hypovolaemia Give 500mL QUICKLY ( 15mins) refill Is Oliguria no longer should recommended Passive leg Cool raise peripheries trigger a volume as a Stay assessment, resuscitation by the patient NOT a test target and repeat fluid challenge observations Autotransfusion Other Oliguria (less of invasive) may 500mL indicate means of blood dehydration of from guiding Repeat legs boluses and fluid abdomen resuscitation until patient no longer hypovolaemic Urine output is not a good target in the Effect Helpful maximal acutely at extremes at unwell 30-90s of patient filling only If no haemodynamic response after 2L 10% increase of fluid (i.e. in sbp ve and/or test) contact reduction Critical in Care HR predictive of fluid responsiveness > POLL
15
16 GETTING IT WRONG Dry Over-transfusion: fluid in the wrong place Wet Pulmonary oedema, gut oedema, peripheral oedema, anasarca Capillary injury and shedding of EGL Dry Wet Under-transfusion: hypoperfusion and persisting shock AKI Ischaemic hepatitis / colitis Arrhythmias / ACS Cerebrovascular events Multi-organ failure
17 WET, DRY OR SOMEWHERE IN-BETWEEN? Dry (Restricted) Wet (Liberal)
18 GETTING IT RIGHT FOR MEDICAL PATIENTS Dry (Restricted) Dry Wet (Liberal) Wet Frequent Reassessment is Key!
19 MAINTENANCE FLUIDS Wet 25-30mL/kg/day 1mmol/kg/day of Na +, Cl - and K + 25mL/kg/day of: Dry Hartmann s 4% 0.9% Glucose-0.18% NaCl Saline + 40KCl > 3.3mmol/kg/day 0.45mmol/kg/day > 4mmol/kg/day Na Na Na + + > 2.8mmol/kg/day 0.45mmol/kg/day > 4mmol/kg/day Cl Cl Cl > 0.125mmol/kg/day 1mmol/kg/day K+ K+ > 70g glucose

20 REPLACEMENT One of the few indications for normal saline

21 SUMMARY: 5 Rs
22

23 DISCUSSION QUESTIONS COMMENTS
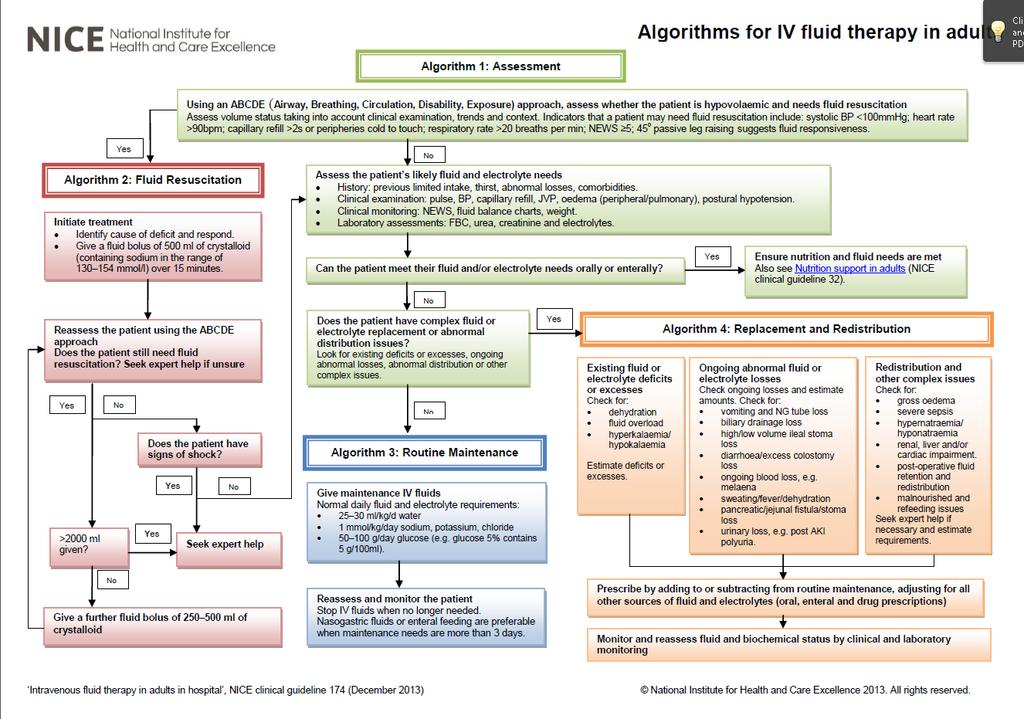
Brief summary of the NICE guidelines December 2013
 Brief summary of the NICE guidelines December 2013 Intravenous fluid therapy in adults in hospital the relevance to Emergency Department Care Applicable to patients 16 years and older receiving i.v. fluids
Brief summary of the NICE guidelines December 2013 Intravenous fluid therapy in adults in hospital the relevance to Emergency Department Care Applicable to patients 16 years and older receiving i.v. fluids
How and why I give IV fluid Disclosures SCA Fluids and public health 4/1/15. Andrew Shaw MB FRCA FCCM FFICM
 How and why I give IV fluid Andrew Shaw MB FRCA FCCM FFICM Professor and Chief Cardiothoracic Anesthesiology Vanderbilt University Medical Center 2015 Disclosures Consultant for Grifols manufacturer of
How and why I give IV fluid Andrew Shaw MB FRCA FCCM FFICM Professor and Chief Cardiothoracic Anesthesiology Vanderbilt University Medical Center 2015 Disclosures Consultant for Grifols manufacturer of
Intravenous Fluid Therapy in Critical Illness
 Intravenous Fluid Therapy in Critical Illness GINA HURST, MD DIVISION OF EMERGENCY CRITICAL CARE HENRY FORD HOSPITAL DETROIT, MI Objectives Establish goals of IV fluid therapy Review fluid types and availability
Intravenous Fluid Therapy in Critical Illness GINA HURST, MD DIVISION OF EMERGENCY CRITICAL CARE HENRY FORD HOSPITAL DETROIT, MI Objectives Establish goals of IV fluid therapy Review fluid types and availability
IV Fluids Do you know what you are doing?
 IV Fluids Do you know what you are doing? Probably not Dr Mike Stroud Gastroenterologist and Senior Lecturer in Medicine & Nutrition Southampton University Hospitals Foundation Trust CG 174 December 2013
IV Fluids Do you know what you are doing? Probably not Dr Mike Stroud Gastroenterologist and Senior Lecturer in Medicine & Nutrition Southampton University Hospitals Foundation Trust CG 174 December 2013
Using Balanced Fluids in Paediatrics: Implementing NICE Guidance without breaking the bank
 Using Balanced Fluids in Paediatrics: Implementing NICE Guidance without breaking the bank Adam Sutherland Senior Clinical Pharmacist, RMCH Clinical Lecturer, University of Manchester NIHR MClinRes Trainee,
Using Balanced Fluids in Paediatrics: Implementing NICE Guidance without breaking the bank Adam Sutherland Senior Clinical Pharmacist, RMCH Clinical Lecturer, University of Manchester NIHR MClinRes Trainee,
SIMPLY. Fluids. Dr Will Dooley
 SIMPLY. Fluids Dr Will Dooley Plan Maintenance vs Resuscitation Prescribing Common Errors Calculations Drip rates Case 54 yo presents with severe diarrhoea and vomiting. How would you proceed? Assessment
SIMPLY. Fluids Dr Will Dooley Plan Maintenance vs Resuscitation Prescribing Common Errors Calculations Drip rates Case 54 yo presents with severe diarrhoea and vomiting. How would you proceed? Assessment
BREAK 11:10-11:
 1. Sepsis Tom Heaps 09:30-10:20 2. Oncological Emergencies Clare Pollard 10:20-11:10 ------------------------ BREAK 11:10-11:30 ------------------------ 3. Diabetic Ketoacidosis Tom Heaps 11:30-12:20 4.
1. Sepsis Tom Heaps 09:30-10:20 2. Oncological Emergencies Clare Pollard 10:20-11:10 ------------------------ BREAK 11:10-11:30 ------------------------ 3. Diabetic Ketoacidosis Tom Heaps 11:30-12:20 4.
HYPOVOLEMIA AND HEMORRHAGE UPDATE ON VOLUME RESUSCITATION HEMORRHAGE AND HYPOVOLEMIA DISTRIBUTION OF BODY FLUIDS 11/7/2015
 UPDATE ON VOLUME RESUSCITATION HYPOVOLEMIA AND HEMORRHAGE HUMAN CIRCULATORY SYSTEM OPERATES WITH A SMALL VOLUME AND A VERY EFFICIENT VOLUME RESPONSIVE PUMP. HOWEVER THIS PUMP FAILS QUICKLY WITH VOLUME
UPDATE ON VOLUME RESUSCITATION HYPOVOLEMIA AND HEMORRHAGE HUMAN CIRCULATORY SYSTEM OPERATES WITH A SMALL VOLUME AND A VERY EFFICIENT VOLUME RESPONSIVE PUMP. HOWEVER THIS PUMP FAILS QUICKLY WITH VOLUME
Getting smart with fluids in the critically ill. NOR AZIM MOHD YUNOS Jeffrey Cheah School of Medicine & Health Sciences Monash University Malaysia
 Getting smart with fluids in the critically ill NOR AZIM MOHD YUNOS Jeffrey Cheah School of Medicine & Health Sciences Monash University Malaysia Isotonic Solutions and Major Adverse Renal Events Trial
Getting smart with fluids in the critically ill NOR AZIM MOHD YUNOS Jeffrey Cheah School of Medicine & Health Sciences Monash University Malaysia Isotonic Solutions and Major Adverse Renal Events Trial
The History & Practice of IV Fluid Therapy have we advanced in 185 years?
 The History & Practice of IV Fluid Therapy have we advanced in 185 years? Liam Plant Clinical Professor of Renal Medicine University College Cork Consultant Renal Physician Cork University Hospital National
The History & Practice of IV Fluid Therapy have we advanced in 185 years? Liam Plant Clinical Professor of Renal Medicine University College Cork Consultant Renal Physician Cork University Hospital National
SIMPLY. Fluids. Dr William Dooley
 SIMPLY. Fluids Dr William Dooley Plan Fluid management Resuscitation Routine Maintenance Replacement Redistribution Reassessment Common Errors Calculations Assessment?ORAL vs. IVF History Limited intake
SIMPLY. Fluids Dr William Dooley Plan Fluid management Resuscitation Routine Maintenance Replacement Redistribution Reassessment Common Errors Calculations Assessment?ORAL vs. IVF History Limited intake
THe Story of salty Sam
 THe Story of salty Sam Understanding fluids, urea and electrolyte balance; a quantitative approach. A self-directed learning activity. Part One. meet salty sam Salty Sam is a pretty average 70 kg bloke,
THe Story of salty Sam Understanding fluids, urea and electrolyte balance; a quantitative approach. A self-directed learning activity. Part One. meet salty sam Salty Sam is a pretty average 70 kg bloke,
CLINICAL GUIDELINE FOR INTRAVENOUS FLUID THERAPY FOR ADULTS IN HOSPITAL 1. Aim/Purpose of this Guideline
 CLINICAL GUIDELINE FOR INTRAVENOUS FLUID THERAPY FOR ADULTS IN HOSPITAL 1. Aim/Purpose of this Guideline 1.1. This guideline contains recommendations about general principles for managing intravenous (IV)
CLINICAL GUIDELINE FOR INTRAVENOUS FLUID THERAPY FOR ADULTS IN HOSPITAL 1. Aim/Purpose of this Guideline 1.1. This guideline contains recommendations about general principles for managing intravenous (IV)
Salty Solutions or Salty Problems? Outline. Outline 29/04/2013
 Salty Solutions or Salty Problems? 18 th October 2012 Richard Seigne Anaesthetist 1 - Non fluid 40% T o t a l b o d y f l u i d 60% NaCl NaCl Intra-cellular fluid 2/3 KCl Interstitial fluid 3/4 of ECF
Salty Solutions or Salty Problems? 18 th October 2012 Richard Seigne Anaesthetist 1 - Non fluid 40% T o t a l b o d y f l u i d 60% NaCl NaCl Intra-cellular fluid 2/3 KCl Interstitial fluid 3/4 of ECF
Fluids in Sepsis: How much and what type? John Fowler, MD, FACEP Kent Hospital, İzmir Eisenhower Medical Center, USA American Hospital Dubai, UAE
 Fluids in Sepsis: How much and what type? John Fowler, MD, FACEP Kent Hospital, İzmir Eisenhower Medical Center, USA American Hospital Dubai, UAE In critically ill patients: too little fluid Low preload,
Fluids in Sepsis: How much and what type? John Fowler, MD, FACEP Kent Hospital, İzmir Eisenhower Medical Center, USA American Hospital Dubai, UAE In critically ill patients: too little fluid Low preload,
Fluids and electrolytes: the basics
 Fluids and electrolytes: the basics This document is based on the handout from the Surgery for Finals course. The notes provided here summarise key aspects, focusing on areas that are popular in clinical
Fluids and electrolytes: the basics This document is based on the handout from the Surgery for Finals course. The notes provided here summarise key aspects, focusing on areas that are popular in clinical
INTRAVENOUS FLUIDS PRINCIPLES
 INTRAVENOUS FLUIDS PRINCIPLES Postnatal physiological weight loss is approximately 5-10% Postnatal diuresis is delayed in Respiratory Distress Syndrome (RDS) Preterm babies have limited capacity to excrete
INTRAVENOUS FLUIDS PRINCIPLES Postnatal physiological weight loss is approximately 5-10% Postnatal diuresis is delayed in Respiratory Distress Syndrome (RDS) Preterm babies have limited capacity to excrete
Fluid Therapy in Critical Illness
 Fluid Therapy in Critical Illness Ruth Roadley-Battin Advanced Clinical Pharmacist- Critical Care, UHB With thanks to Dr Zahid Khan, Emma Boxall and Fraser Hanks. Fluids in Critical Care Most common intervention
Fluid Therapy in Critical Illness Ruth Roadley-Battin Advanced Clinical Pharmacist- Critical Care, UHB With thanks to Dr Zahid Khan, Emma Boxall and Fraser Hanks. Fluids in Critical Care Most common intervention
INTENSIVE CARE MEDICINE CPD EVENING. Dr Alastair Morgan Wednesday 13 th September 2017
 INTENSIVE CARE MEDICINE CPD EVENING Dr Alastair Morgan Wednesday 13 th September 2017 WHAT IS NEW IN ICU? (RELEVANT TO ANAESTHETISTS) Not much! SURVIVING SEPSIS How many deaths in England were thought
INTENSIVE CARE MEDICINE CPD EVENING Dr Alastair Morgan Wednesday 13 th September 2017 WHAT IS NEW IN ICU? (RELEVANT TO ANAESTHETISTS) Not much! SURVIVING SEPSIS How many deaths in England were thought
Update in Critical Care Medicine
 Update in Critical Care Medicine Michael A. Gropper, MD, PhD Professor and Executive Vice Chair Department of Anesthesia and Perioperative Care Director, Critical Care Medicine UCSF Disclosure None Update
Update in Critical Care Medicine Michael A. Gropper, MD, PhD Professor and Executive Vice Chair Department of Anesthesia and Perioperative Care Director, Critical Care Medicine UCSF Disclosure None Update
Fluid assessment, monitoring and therapy for the acute nurse
 Fluid assessment, monitoring and therapy for the acute nurse Kelly Wright Lead Nurse for AKI King s College Hospital Aims and objectives Aims and objectives Why do we worry about volume assessment? Completing
Fluid assessment, monitoring and therapy for the acute nurse Kelly Wright Lead Nurse for AKI King s College Hospital Aims and objectives Aims and objectives Why do we worry about volume assessment? Completing
Modern fluid therapy. Anders Perner. Dept of Intensive Care, Rigshospitalet, University of Copenhagen
 Modern fluid therapy Anders Perner Dept of Intensive Care, Rigshospitalet, University of Copenhagen Scandinavian Critical Care Trials Group www.ssai.info/research/scctg Intensive Care Medicine www.icmjournal.esicm.org
Modern fluid therapy Anders Perner Dept of Intensive Care, Rigshospitalet, University of Copenhagen Scandinavian Critical Care Trials Group www.ssai.info/research/scctg Intensive Care Medicine www.icmjournal.esicm.org
Standard Operating Procedure (SOP) Management of intervention group patients SOP 001
 Management of intervention group patients SOP 001") ` Standard Operating Procedure (SOP) Management of intervention group patients SOP 001 Authors: Mark Edwards & Rupert Pearse Authorisation: Rupert Pearse (Chief Investigator) Scope To provide guidance
` Standard Operating Procedure (SOP) Management of intervention group patients SOP 001 Authors: Mark Edwards & Rupert Pearse Authorisation: Rupert Pearse (Chief Investigator) Scope To provide guidance
IV Fluids. I.V. Fluid Osmolarity Composition 0.9% NaCL (Normal Saline Solution, NSS) Uses/Clinical Considerations
 Uses/Clinical Considerations") IV Fluids When administering IV fluids, the type and amount of fluid may influence patient outcomes. Make sure to understand the differences between fluid products and their effects. Crystalloids Crystalloid
IV Fluids When administering IV fluids, the type and amount of fluid may influence patient outcomes. Make sure to understand the differences between fluid products and their effects. Crystalloids Crystalloid
Dr. Nai Shun Tsoi Department of Paediatric and Adolescent Medicine Queen Mary Hospital Hong Kong SAR
 Dr. Nai Shun Tsoi Department of Paediatric and Adolescent Medicine Queen Mary Hospital Hong Kong SAR A very important aspect in paediatric intensive care and deserve more attention Basic principle is to
Dr. Nai Shun Tsoi Department of Paediatric and Adolescent Medicine Queen Mary Hospital Hong Kong SAR A very important aspect in paediatric intensive care and deserve more attention Basic principle is to
Fluids and Lactate. A/Prof Peter Morley
 Fluids and Lactate A/Prof Peter Morley RCTs Other evidence 5 6 Plan Background information Crystalloids Which crystalloid? Colloids Crystalloids v colloids Once that s settled, how much fluid Plan Background
Fluids and Lactate A/Prof Peter Morley RCTs Other evidence 5 6 Plan Background information Crystalloids Which crystalloid? Colloids Crystalloids v colloids Once that s settled, how much fluid Plan Background
Paediatric Shock. Dr Andrew Pittaway Department of Anaesthesia Bristol Royal Hospital for Children Bristol, UK
 Paediatric Shock Dr Andrew Pittaway Department of Anaesthesia Bristol Royal Hospital for Children Bristol, UK Self-assessment: 1. What is the definition of shock? 2. List the different pathophysiological
Paediatric Shock Dr Andrew Pittaway Department of Anaesthesia Bristol Royal Hospital for Children Bristol, UK Self-assessment: 1. What is the definition of shock? 2. List the different pathophysiological
Staging Sepsis for the Emergency Department: Physician
 Staging Sepsis for the Emergency Department: Physician Sepsis Continuum 1 Sepsis Continuum SIRS = 2 or more clinical criteria, resulting in Systemic Inflammatory Response Syndrome Sepsis = SIRS + proven/suspected
Staging Sepsis for the Emergency Department: Physician Sepsis Continuum 1 Sepsis Continuum SIRS = 2 or more clinical criteria, resulting in Systemic Inflammatory Response Syndrome Sepsis = SIRS + proven/suspected
Acute Kidney Injury (AKI) Undergraduate nurse education
 Undergraduate nurse education") Acute Kidney Injury (AKI) Undergraduate nurse education Year Three Developed Summer 2017 Objectives Understand Acute Kidney Injury and its relevance to patient care. Brief revision of the Anatomy and physiology
Acute Kidney Injury (AKI) Undergraduate nurse education Year Three Developed Summer 2017 Objectives Understand Acute Kidney Injury and its relevance to patient care. Brief revision of the Anatomy and physiology
INTRAVENOUS FLUID THERAPY
 INTRAVENOUS FLUID THERAPY PRINCIPLES Postnatal physiological weight loss is approximately 5 10% in first week of life Preterm neonates have more total body water and may lose 10 15% of their weight in
INTRAVENOUS FLUID THERAPY PRINCIPLES Postnatal physiological weight loss is approximately 5 10% in first week of life Preterm neonates have more total body water and may lose 10 15% of their weight in
SLCOA National Guidelines
 SLCOA National Guidelines Peri - operative Fluid & Electrolyte Management SLCOA National Guidelines Contents List of Contributors 92 Paediatric fasting guidelines for elective procedures 93 Guidelines
SLCOA National Guidelines Peri - operative Fluid & Electrolyte Management SLCOA National Guidelines Contents List of Contributors 92 Paediatric fasting guidelines for elective procedures 93 Guidelines
Acute Renal Failure. Dr Kawa Ahmad
 62 Acute Renal Failure Dr Kawa Ahmad Acute Renal Failure It is characterised by an abrupt reduction (usually within a 48- h period) in kidney function. This results in an accumulation of nitrogenous waste
62 Acute Renal Failure Dr Kawa Ahmad Acute Renal Failure It is characterised by an abrupt reduction (usually within a 48- h period) in kidney function. This results in an accumulation of nitrogenous waste
Salt of the earth or a drop in the ocean An overview of the properties of iv fluids
 Bapen Conference 2009 13 th October 2009 Cardiff International Arena Salt of the earth or a drop in the ocean An overview of the properties of iv fluids Peter Gosling BSc MSc PhD FRCPath Consultant Clinical
Bapen Conference 2009 13 th October 2009 Cardiff International Arena Salt of the earth or a drop in the ocean An overview of the properties of iv fluids Peter Gosling BSc MSc PhD FRCPath Consultant Clinical
SHOCK Susanna Hilda Hutajulu, MD, PhD
 SHOCK Susanna Hilda Hutajulu, MD, PhD Div Hematology and Medical Oncology Department of Internal Medicine Universitas Gadjah Mada Yogyakarta Outline Definition Epidemiology Physiology Classes of Shock
SHOCK Susanna Hilda Hutajulu, MD, PhD Div Hematology and Medical Oncology Department of Internal Medicine Universitas Gadjah Mada Yogyakarta Outline Definition Epidemiology Physiology Classes of Shock
INTRAVENOUS FLUIDS. Ahmad AL-zu bi
 INTRAVENOUS FLUIDS Ahmad AL-zu bi Types of IV fluids Crystalloids colloids Crystalloids Crystalloids are aqueous solutions of low molecular weight ions,with or without glucose. Isotonic, Hypotonic, & Hypertonic
INTRAVENOUS FLUIDS Ahmad AL-zu bi Types of IV fluids Crystalloids colloids Crystalloids Crystalloids are aqueous solutions of low molecular weight ions,with or without glucose. Isotonic, Hypotonic, & Hypertonic
The Septic Patient. Dr Arunraj Navaratnarajah. Renal SpR Imperial College NHS Healthcare Trust
 The Septic Patient Dr Arunraj Navaratnarajah Renal SpR Imperial College NHS Healthcare Trust Objectives of this session Define SIRS / sepsis / severe sepsis / septic shock Early recognition of Sepsis The
The Septic Patient Dr Arunraj Navaratnarajah Renal SpR Imperial College NHS Healthcare Trust Objectives of this session Define SIRS / sepsis / severe sepsis / septic shock Early recognition of Sepsis The
Fluid therapy in children
 Fluid therapy in children TJ Neuhaus and G Reusz Lucerne and Budapest ESPN 2012 Kraków Parenteral maintenance in children Daily requirements - Holliday and Segar, 1957 Fluid Patient weight: 25 kg 1-10
Fluid therapy in children TJ Neuhaus and G Reusz Lucerne and Budapest ESPN 2012 Kraków Parenteral maintenance in children Daily requirements - Holliday and Segar, 1957 Fluid Patient weight: 25 kg 1-10
Fluids in ICU. JMO teaching 5th July 2016
 Fluids in ICU JMO teaching 5th July 2016 Objectives Physiology of fluid infusion History of fluid resuscitation Physiology of fluid resuscitation Types of resuscitation fluid The ideal resuscitation fluid
Fluids in ICU JMO teaching 5th July 2016 Objectives Physiology of fluid infusion History of fluid resuscitation Physiology of fluid resuscitation Types of resuscitation fluid The ideal resuscitation fluid
Vasoactive Medications. Matthew J. Korobey Pharm.D., BCCCP Critical Care Clinical Specialist Mercy St. Louis
 Vasoactive Medications Matthew J. Korobey Pharm.D., BCCCP Critical Care Clinical Specialist Mercy St. Louis Objectives List components of physiology involved in blood pressure Review terminology related
Vasoactive Medications Matthew J. Korobey Pharm.D., BCCCP Critical Care Clinical Specialist Mercy St. Louis Objectives List components of physiology involved in blood pressure Review terminology related
Respiratory problems with severe malaria: an opportunity to talk about fluid trials!!! Kathryn Maitland
 Respiratory problems with severe malaria: an opportunity to talk about fluid trials!!! Kathryn Maitland Severe malaria-the numbers Up to 1 million deaths in African children
Respiratory problems with severe malaria: an opportunity to talk about fluid trials!!! Kathryn Maitland Severe malaria-the numbers Up to 1 million deaths in African children
Fine-tuning Management in Dengue Fever
 Fine-tuning Management in Dengue Fever Annual Scientific Meeting On Intensive Care 16 August 2014 Eg Kah Peng University of Malaya Medical Centre Rise In Dengue Infection New Straits Times 8 July 2014
Fine-tuning Management in Dengue Fever Annual Scientific Meeting On Intensive Care 16 August 2014 Eg Kah Peng University of Malaya Medical Centre Rise In Dengue Infection New Straits Times 8 July 2014
Albumina nel paziente critico. Savona 18 aprile 2007
 Albumina nel paziente critico Savona 18 aprile 2007 What Is Unique About Critical Care RCTs patients eligibility is primarily defined by location of care in the ICU rather than by the presence of a specific
Albumina nel paziente critico Savona 18 aprile 2007 What Is Unique About Critical Care RCTs patients eligibility is primarily defined by location of care in the ICU rather than by the presence of a specific
FLUID THERAPY: IT S MORE THAN JUST LACTATED RINGERS
 FLUID THERAPY: IT S MORE THAN JUST LACTATED RINGERS Elisa M. Mazzaferro, MS, DVM, PhD, DACVECC Cornell University Veterinary Specialists, Stamford, CT, USA Total body water constitutes approximately 60%
FLUID THERAPY: IT S MORE THAN JUST LACTATED RINGERS Elisa M. Mazzaferro, MS, DVM, PhD, DACVECC Cornell University Veterinary Specialists, Stamford, CT, USA Total body water constitutes approximately 60%
Presented by: Indah Dwi Pratiwi
 Presented by: Indah Dwi Pratiwi Normal Fluid Requirements Resuscitation Fluids Goals of Resuscitation Maintain normal body temperature In most cases, elevate the feet and legs above the level of the heart
Presented by: Indah Dwi Pratiwi Normal Fluid Requirements Resuscitation Fluids Goals of Resuscitation Maintain normal body temperature In most cases, elevate the feet and legs above the level of the heart
Sepsis Awareness and Education
 Sepsis Awareness and Education Meets the updated New York State Department of Health (NYSDOH) requirements for Infection Control and Barrier Precautions coursework Element VII: Sepsis Awareness and Education
Sepsis Awareness and Education Meets the updated New York State Department of Health (NYSDOH) requirements for Infection Control and Barrier Precautions coursework Element VII: Sepsis Awareness and Education
SHOCK. Pathophysiology
 SHOCK Dr. Ahmed Saleem FICMS TUCOM / 3rd Year / 2015 Shock is the most common and therefore the most important cause of death of surgical patients. Death may occur rapidly due to a profound state of shock,
SHOCK Dr. Ahmed Saleem FICMS TUCOM / 3rd Year / 2015 Shock is the most common and therefore the most important cause of death of surgical patients. Death may occur rapidly due to a profound state of shock,
Comment on infusion solutions containing HES
 Comment on infusion solutions containing HES The European Medicines Agency (EMA) published on 14 June 2013 Pharmacovigilance Risk Assessment Committee (PRAC) recommends suspending marketing authorisations
Comment on infusion solutions containing HES The European Medicines Agency (EMA) published on 14 June 2013 Pharmacovigilance Risk Assessment Committee (PRAC) recommends suspending marketing authorisations
KASHVET VETERINARIAN RESOURCES FLUID THERAPY AND SELECTION OF FLUIDS
 KASHVET VETERINARIAN RESOURCES FLUID THERAPY AND SELECTION OF FLUIDS INTRODUCTION Formulating a fluid therapy plan for the critical small animal patient requires careful determination of the current volume
KASHVET VETERINARIAN RESOURCES FLUID THERAPY AND SELECTION OF FLUIDS INTRODUCTION Formulating a fluid therapy plan for the critical small animal patient requires careful determination of the current volume
Fundamentals of Pharmacology for Veterinary Technicians Chapter 19
 Figure 19-1 Figure 19-2A Figure 19-2B Figure 19-3 Figure 19-4A1 Figure 19-4A2 Figure 19-4B Figure 19-4C Figure 19-4D Figure 19-5 Figure 19-6A Figure 19-6B A Figure 19-7A B Figure 19-7B C Figure 19-7C D
Figure 19-1 Figure 19-2A Figure 19-2B Figure 19-3 Figure 19-4A1 Figure 19-4A2 Figure 19-4B Figure 19-4C Figure 19-4D Figure 19-5 Figure 19-6A Figure 19-6B A Figure 19-7A B Figure 19-7B C Figure 19-7C D
PAEDIATRIC FLUIDS RCH DEHYDRATION
 PAEDIATRIC FLUIDS RCH DEHYDRATION AIMS Understand normal fluids electrolyte requirements/ maintenance Understand how to assess DEHYDRATION in children Understand the difference between DEHYDRATION and
PAEDIATRIC FLUIDS RCH DEHYDRATION AIMS Understand normal fluids electrolyte requirements/ maintenance Understand how to assess DEHYDRATION in children Understand the difference between DEHYDRATION and
Fluid and electrolyte management
 281 Chapter Appendix 5B Fluid and electrolyte management Learning outcomes After reading this appendix, you will be able to: Describe the approach to the management of fluid and electrolytes in the seriously
281 Chapter Appendix 5B Fluid and electrolyte management Learning outcomes After reading this appendix, you will be able to: Describe the approach to the management of fluid and electrolytes in the seriously
Initial Resuscitation of Sepsis & Septic Shock
 Initial Resuscitation of Sepsis & Septic Shock Dr. Fatema Ahmed MD (Critical Care Medicine) FCPS (Medicine) Associate professor Dept. of Critical Care Medicine BIRDEM General Hospital Is Sepsis a known
Initial Resuscitation of Sepsis & Septic Shock Dr. Fatema Ahmed MD (Critical Care Medicine) FCPS (Medicine) Associate professor Dept. of Critical Care Medicine BIRDEM General Hospital Is Sepsis a known
Fluid Resuscitation in Sepsis. A Literature Review
 Fluid Resuscitation in Sepsis A Literature Review "On the floor lay a girl of slender make and juvenile height, but with the face of a superannuated hag... The colour of her countenance was that of lead
Fluid Resuscitation in Sepsis A Literature Review "On the floor lay a girl of slender make and juvenile height, but with the face of a superannuated hag... The colour of her countenance was that of lead
Nephrology. 3 rd Year Revision Session 06/05/17 Cathal Hannan
 Nephrology 3 rd Year Revision Session 06/05/17 Cathal Hannan Aims Acute Kidney Injury-recognition and management Sample OSCE Station Clinically relevant renal physiology Aetiology of Chronic Kidney Disease
Nephrology 3 rd Year Revision Session 06/05/17 Cathal Hannan Aims Acute Kidney Injury-recognition and management Sample OSCE Station Clinically relevant renal physiology Aetiology of Chronic Kidney Disease
WHICH FLUIDS SHOULD BE USED IN THE CLINICAL SETTING? My personal strategy : crystalloids + colloids. Why?
 WHICH FLUIDS SHOULD BE USED IN THE CLINICAL SETTING? Big debate: crystalloids colloids crystalloids + colloids My personal strategy : crystalloids + colloids Why? Crystalloids + colloids end of the story?
WHICH FLUIDS SHOULD BE USED IN THE CLINICAL SETTING? Big debate: crystalloids colloids crystalloids + colloids My personal strategy : crystalloids + colloids Why? Crystalloids + colloids end of the story?
MODULE 8B: Management of Group B Dengue with Warning Signs or Dengue with Co-existing Conditions
 MODULE 8B: Management of Group B Dengue with Warning Signs or Dengue with Co-existing Conditions Dengue Clinical Management Acknowledgements This curriculum was developed with technical assistance from
MODULE 8B: Management of Group B Dengue with Warning Signs or Dengue with Co-existing Conditions Dengue Clinical Management Acknowledgements This curriculum was developed with technical assistance from
Printed copies of this document may not be up to date, obtain the most recent version from
 Children s Acute Transport Service Clinical Guidelines Septic Shock Document Control Information Author Claire Fraser P.Ramnarayan Author Position tanp CATS Consultant Document Owner E. Polke Document
Children s Acute Transport Service Clinical Guidelines Septic Shock Document Control Information Author Claire Fraser P.Ramnarayan Author Position tanp CATS Consultant Document Owner E. Polke Document
Care of the Critically Unwell Patient. fluids
 Care of the Critically Unwell Patient fluids Are we made of water? YES! Humans are like cucumbers Water content at least half of body weight in healty adults (60%) blood volume 7% bw males 6% bw females
Care of the Critically Unwell Patient fluids Are we made of water? YES! Humans are like cucumbers Water content at least half of body weight in healty adults (60%) blood volume 7% bw males 6% bw females
SEPSIS UPDATE WHY DO WE NEED A CORE MEASURE CHAD M. KOVALA DO, FACOEP, FACEP
 SEPSIS UPDATE WHY DO WE NEED A CORE MEASURE CHAD M. KOVALA DO, FACOEP, FACEP OBJECTIVES Arise, ProMISE, ProCESS Key points in sepsis management The CMS sepsis core measure COST OF SEPSIS CARE IN US Most
SEPSIS UPDATE WHY DO WE NEED A CORE MEASURE CHAD M. KOVALA DO, FACOEP, FACEP OBJECTIVES Arise, ProMISE, ProCESS Key points in sepsis management The CMS sepsis core measure COST OF SEPSIS CARE IN US Most
I Suggest Abnormal Saline
 I Suggest Abnormal Saline Sean M Bagshaw, MD, MSc Division of Critical Care Medicine University of Alberta CCCF Oct 27, 2015 2015 Disclosures Salary support: Canada/Alberta government Grant support: Canada/Alberta
I Suggest Abnormal Saline Sean M Bagshaw, MD, MSc Division of Critical Care Medicine University of Alberta CCCF Oct 27, 2015 2015 Disclosures Salary support: Canada/Alberta government Grant support: Canada/Alberta
SHOCK and the Trauma Victim. JP Pretorius Department of Surgery & SICU Steve Biko Academic Hospital.
 SHOCK and the Trauma Victim JP Pretorius Department of Surgery & SICU Steve Biko Academic Hospital. Classification of Shock Cardiogenic - Myopathic Arrythmic Mechanical Hypovolaemic - Haemorrhagic Non-haemorrhagic
SHOCK and the Trauma Victim JP Pretorius Department of Surgery & SICU Steve Biko Academic Hospital. Classification of Shock Cardiogenic - Myopathic Arrythmic Mechanical Hypovolaemic - Haemorrhagic Non-haemorrhagic
Written 01/09/17 Rewritten 3/29/17 for Interior Regional EMS Symposium
 Written 01/09/17 Rewritten 3/29/17 for Interior Regional EMS Symposium MARIA E. MANDICH MD Fairbanks Memorial Hospital Emergency Department Attending Physician Interior Region EMS Council Medical Director
Written 01/09/17 Rewritten 3/29/17 for Interior Regional EMS Symposium MARIA E. MANDICH MD Fairbanks Memorial Hospital Emergency Department Attending Physician Interior Region EMS Council Medical Director
Approach to Severe Sepsis. Jan Hau Lee, MBBS, MRCPCH. MCI Children s Intensive Care Unit KK Women s and Children's Hospital, Singapore
 Approach to Severe Sepsis Jan Hau Lee, MBBS, MRCPCH. MCI Children s Intensive Care Unit KK Women s and Children's Hospital, Singapore 1 2 No conflict of interest Overview Epidemiology of Pediatric Severe
Approach to Severe Sepsis Jan Hau Lee, MBBS, MRCPCH. MCI Children s Intensive Care Unit KK Women s and Children's Hospital, Singapore 1 2 No conflict of interest Overview Epidemiology of Pediatric Severe
John Park, MD Assistant Professor of Medicine
 John Park, MD Assistant Professor of Medicine Faculty photo will be placed here park.john@mayo.edu 2015 MFMER 3543652-1 Sepsis Out with the Old, In with the New Mayo School of Continuous Professional Development
John Park, MD Assistant Professor of Medicine Faculty photo will be placed here park.john@mayo.edu 2015 MFMER 3543652-1 Sepsis Out with the Old, In with the New Mayo School of Continuous Professional Development
DIABETIC KETOACIDOSIS MANAGEMENT PLAN:
 DIABETIC KETOACIDOSIS MANAGEMENT PLAN: 1. Assessment (weight, blood glucose level (BGL), blood pressure (BP), heart rate (HR), respiratory rate (RR), temperature, history & examination) 2. Resuscitation
DIABETIC KETOACIDOSIS MANAGEMENT PLAN: 1. Assessment (weight, blood glucose level (BGL), blood pressure (BP), heart rate (HR), respiratory rate (RR), temperature, history & examination) 2. Resuscitation
Shock Quiz! By Clare Di Bona
 Shock Quiz! By Clare Di Bona Test Question What is Mr Burns full legal name? Answer Charles Montgomery Plantagenet Schicklgruber Burns. (Season 22, episode 11) Question 1. What is the definition of shock?
Shock Quiz! By Clare Di Bona Test Question What is Mr Burns full legal name? Answer Charles Montgomery Plantagenet Schicklgruber Burns. (Season 22, episode 11) Question 1. What is the definition of shock?
Sepsis: Identification and Management in an Acute Care Setting
 Sepsis: Identification and Management in an Acute Care Setting Dr. Barbara M. Mills DNP Director Rapid Response Team/ Code Resuscitation Stony Brook University Medical Center SEPSIS LECTURE NPA 2018 OBJECTIVES
Sepsis: Identification and Management in an Acute Care Setting Dr. Barbara M. Mills DNP Director Rapid Response Team/ Code Resuscitation Stony Brook University Medical Center SEPSIS LECTURE NPA 2018 OBJECTIVES
Amjad Bani Hani Ass.Prof. of Cardiac Surgery & Intensive Care FLUIDS AND ELECTROLYTES
 Amjad Bani Hani Ass.Prof. of Cardiac Surgery & Intensive Care FLUIDS AND ELECTROLYTES Body Water Content Water Balance: Normal 2500 2000 1500 1000 500 Metab Food Fluids Stool Breath Sweat Urine
Amjad Bani Hani Ass.Prof. of Cardiac Surgery & Intensive Care FLUIDS AND ELECTROLYTES Body Water Content Water Balance: Normal 2500 2000 1500 1000 500 Metab Food Fluids Stool Breath Sweat Urine
FLUID MANAGEMENT AND BLOOD COMPONENT THERAPY
 Manual: Section: Protocol #: Approval Date: Effective Date: Revision Due Date: 10/2019 LifeLine Patient Care Protocols Adult/Pediatrics AP1-011 10/2018 10/2018 FLUID MANAGEMENT AND BLOOD COMPONENT THERAPY
Manual: Section: Protocol #: Approval Date: Effective Date: Revision Due Date: 10/2019 LifeLine Patient Care Protocols Adult/Pediatrics AP1-011 10/2018 10/2018 FLUID MANAGEMENT AND BLOOD COMPONENT THERAPY
-Cardiogenic: shock state resulting from impairment or failure of myocardium
 Shock chapter Shock -Condition in which tissue perfusion is inadequate to deliver oxygen, nutrients to support vital organs, cellular function -Affects all body systems -Classic signs of early shock: Tachycardia,tachypnea,restlessness,anxiety,
Shock chapter Shock -Condition in which tissue perfusion is inadequate to deliver oxygen, nutrients to support vital organs, cellular function -Affects all body systems -Classic signs of early shock: Tachycardia,tachypnea,restlessness,anxiety,
Is there a role for Sodium Bicarbonate in NICU? Stephen Wardle Consultant Neonatologist Nottingham University Hospitals
 Is there a role for Sodium Bicarbonate in NICU? Stephen Wardle Consultant Neonatologist Nottingham University Hospitals Aim / Objectives To persuade you:- there is no evidence in favour of using bicarbonate
Is there a role for Sodium Bicarbonate in NICU? Stephen Wardle Consultant Neonatologist Nottingham University Hospitals Aim / Objectives To persuade you:- there is no evidence in favour of using bicarbonate
Principles of Infusion Therapy: Fluids
 Principles of Infusion Therapy: Fluids Christie Heinzman, MSN, APRN-CNP Acute Care Pediatric Nurse Practitioner Cincinnati Children s Hospital Medical Center May 22, 2018 Conflict of Interest Disclosure
Principles of Infusion Therapy: Fluids Christie Heinzman, MSN, APRN-CNP Acute Care Pediatric Nurse Practitioner Cincinnati Children s Hospital Medical Center May 22, 2018 Conflict of Interest Disclosure
Ricky Bell Renal/ICM Registrar
 Ricky Bell Renal/ICM Registrar Objectives When to call renal How to manage the patient with AKI How the manage the patient with CKD (HD/PD) Special AKI situations What do the guidelines say? My referral
Ricky Bell Renal/ICM Registrar Objectives When to call renal How to manage the patient with AKI How the manage the patient with CKD (HD/PD) Special AKI situations What do the guidelines say? My referral
ANAESTHESIA FOR BLEEDING TONSIL
 ANAESTHESIA FOR BLEEDING TONSIL BY Dr.S.C.Ganeshprabu, MD., D.A., Professor of Anaesthesiology, Madurai Medical College & Govt. Rajaji Hospital, Madurai -652 020. A 5-year-old child who had tonsillectomy
ANAESTHESIA FOR BLEEDING TONSIL BY Dr.S.C.Ganeshprabu, MD., D.A., Professor of Anaesthesiology, Madurai Medical College & Govt. Rajaji Hospital, Madurai -652 020. A 5-year-old child who had tonsillectomy
Managing Acid Base and Electrolyte Disturbances with RRT
 Managing Acid Base and Electrolyte Disturbances with RRT John R Prowle MA MSc MD MRCP FFICM Consultant in Intensive Care & Renal Medicine RRT for Regulation of Acid-base and Electrolyte Acid base load
Managing Acid Base and Electrolyte Disturbances with RRT John R Prowle MA MSc MD MRCP FFICM Consultant in Intensive Care & Renal Medicine RRT for Regulation of Acid-base and Electrolyte Acid base load
Fluid & Electrolyte Therapy. Prof. Soliman Ali Hassan Prof. of Surgery Taibah university
 Fluid & Electrolyte Therapy By Prof. Soliman Ali Hassan Prof. of Surgery Taibah university Fluid and electrolyte therapy Learning objectives At the end of this lecture, 1-The student should have an idea
Fluid & Electrolyte Therapy By Prof. Soliman Ali Hassan Prof. of Surgery Taibah university Fluid and electrolyte therapy Learning objectives At the end of this lecture, 1-The student should have an idea
Troubleshooting Audio
 Welcome! Audio for this event is available via ReadyTalk Internet Streaming. No telephone line is required. Computer speakers or headphones are necessary to listen to streaming audio. Limited dial-in lines
Welcome! Audio for this event is available via ReadyTalk Internet Streaming. No telephone line is required. Computer speakers or headphones are necessary to listen to streaming audio. Limited dial-in lines
ACUTE KIDNEY INJURY FOCUS ON OBSTETRICS DONNA HIGGINS, CLINICAL NURSE EDUCATOR, NORTHERN LINCOLNSHIRE HOSPITALS NHS FOUNDATION TRUST
 ACUTE KIDNEY INJURY FOCUS ON OBSTETRICS DONNA HIGGINS, CLINICAL NURSE EDUCATOR, NORTHERN LINCOLNSHIRE HOSPITALS NHS FOUNDATION TRUST AIMS & OBJECTIVES Review the functions of the kidney Identify renal
ACUTE KIDNEY INJURY FOCUS ON OBSTETRICS DONNA HIGGINS, CLINICAL NURSE EDUCATOR, NORTHERN LINCOLNSHIRE HOSPITALS NHS FOUNDATION TRUST AIMS & OBJECTIVES Review the functions of the kidney Identify renal
HHS. Hyperglycaemic Hyperosmolar State Care Pathway 1 Presenta8on to 6 hours. Page 1 of 2 AFFIX PATIENT LABEL ! INFORM DIABETES TEAM OF ADMISSION!
 Hyperglycaemic Hyperosmolar State Care Pathway 1 Presenta8on to 6 hours Page 1 of 2 Time of Arrival Loca8on Date / / Diagnosis the characteris8c features of a person with HHS are a) Hypovolaemia b) Marked
Hyperglycaemic Hyperosmolar State Care Pathway 1 Presenta8on to 6 hours Page 1 of 2 Time of Arrival Loca8on Date / / Diagnosis the characteris8c features of a person with HHS are a) Hypovolaemia b) Marked
METHODS RESULTS. Int. J. Med. Sci. 2012, 9. Methods of measurement. Outcome measures. Primary data analysis. Study design and setting
 59 Research Paper Ivyspring International Publisher International Journal of Medical Sciences 2012; 9(1):59-64 A Randomized Clinical Trial Comparing the Effect of Rapidly Infused Crystalloids on Acid-Base
59 Research Paper Ivyspring International Publisher International Journal of Medical Sciences 2012; 9(1):59-64 A Randomized Clinical Trial Comparing the Effect of Rapidly Infused Crystalloids on Acid-Base
Taking the shock factor out of shock
 Taking the shock factor out of shock Julie Antonellis, BS, LVT, VTS (ECC) Northern Virginia Regional Director for the VALVT Technician Supervisor VCA Animal Emergency Critical Care Business owner Antonellis
Taking the shock factor out of shock Julie Antonellis, BS, LVT, VTS (ECC) Northern Virginia Regional Director for the VALVT Technician Supervisor VCA Animal Emergency Critical Care Business owner Antonellis
Surgical Resuscitation Management in Poly-Trauma Patients
 Surgical Resuscitation Management in Poly-Trauma Patients Andrew Bernard, MD FACS Paul Kearney MD Chair of Trauma Surgery Associate Professor Medical Director of Trauma and Acute Care Surgery UK Healthcare
Surgical Resuscitation Management in Poly-Trauma Patients Andrew Bernard, MD FACS Paul Kearney MD Chair of Trauma Surgery Associate Professor Medical Director of Trauma and Acute Care Surgery UK Healthcare
IV fluid administration in sepsis. Dr David Inwald Consultant in PICU St Mary s Hospital, London CATS, London
 IV fluid administration in sepsis Dr David Inwald Consultant in PICU St Mary s Hospital, London CATS, London The talk What is septic shock? What are the recommendations? What is the evidence? Do we follow
IV fluid administration in sepsis Dr David Inwald Consultant in PICU St Mary s Hospital, London CATS, London The talk What is septic shock? What are the recommendations? What is the evidence? Do we follow
ISOVALERIC ACIDAEMIA -ACUTE DECOMPENSATION (standard version)
") Contact Details Name: Hospital Telephone: This protocol has 5 pages ISOVALERIC ACIDAEMIA -ACUTE DECOMPENSATION (standard version) Please read carefully. Meticulous treatment is very important as there
Contact Details Name: Hospital Telephone: This protocol has 5 pages ISOVALERIC ACIDAEMIA -ACUTE DECOMPENSATION (standard version) Please read carefully. Meticulous treatment is very important as there
PRODUCT INFORMATION. NAME OF THE MEDICINE Compound Sodium Lactate (Hartmann's) Solution for Injection
 Solution for Injection") PRODUCT INFORMATION NAME OF THE MEDICINE Compound Sodium Lactate (Hartmann's) Solution for Injection DESCRIPTION Molecular formulae. Potassium chloride: KCl; sodium chloride: NaCl; calcium chloride dihydrate:
PRODUCT INFORMATION NAME OF THE MEDICINE Compound Sodium Lactate (Hartmann's) Solution for Injection DESCRIPTION Molecular formulae. Potassium chloride: KCl; sodium chloride: NaCl; calcium chloride dihydrate:
PARENTERAL NUTRITION
 PARENTERAL NUTRITION DEFINITION Parenteral nutrition [(PN) or total parenteral nutrition (TPN)] is the intravenous infusion of some or all nutrients for tissue maintenance, metabolic requirements and growth
PARENTERAL NUTRITION DEFINITION Parenteral nutrition [(PN) or total parenteral nutrition (TPN)] is the intravenous infusion of some or all nutrients for tissue maintenance, metabolic requirements and growth
Core Measures SEPSIS UPDATES
 Patricia Walker, RN-BC, BSN Evidence Based Practice Manager Quality Management Services UCLA Health System, Ronald Reagan Medical Center Core Measures SEPSIS UPDATES Severe Sepsis and Septic Shock Based
Patricia Walker, RN-BC, BSN Evidence Based Practice Manager Quality Management Services UCLA Health System, Ronald Reagan Medical Center Core Measures SEPSIS UPDATES Severe Sepsis and Septic Shock Based
Solution for cardiac perfusion in viaflex plastic container
 CARDIOPLEGIA SOLUTION A Solution for cardiac perfusion in viaflex plastic container DESCRIPTION Cardioplegia Solution A is a sterile, non-pyrogenic solution in a Viaflex bag. It is used to induce cardiac
CARDIOPLEGIA SOLUTION A Solution for cardiac perfusion in viaflex plastic container DESCRIPTION Cardioplegia Solution A is a sterile, non-pyrogenic solution in a Viaflex bag. It is used to induce cardiac
Acute Kidney Injury in The Acute Oncology Patient
 Acute Kidney Injury in The Acute Oncology Patient Dr Andrew Lewington BSc MEd MD FRCP Consultant Renal Physician/Honorary Senior Lecturer Leeds Teaching Hospitals Definition Definitions and terminology
Acute Kidney Injury in The Acute Oncology Patient Dr Andrew Lewington BSc MEd MD FRCP Consultant Renal Physician/Honorary Senior Lecturer Leeds Teaching Hospitals Definition Definitions and terminology
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE
 NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE Centre for Clinical Practice SCOPE Clinical guideline title: Intravenous fluid therapy in adults in hospital Quality standard title: Intravenous fluid
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE Centre for Clinical Practice SCOPE Clinical guideline title: Intravenous fluid therapy in adults in hospital Quality standard title: Intravenous fluid
Colic: medical treatment and management in horses
 Vet Times The website for the veterinary profession https://www.vettimes.co.uk Colic: medical treatment and management in horses Author : Nicola Menzies-Gow Categories : Equine, Vets Date : July 4, 2016
Vet Times The website for the veterinary profession https://www.vettimes.co.uk Colic: medical treatment and management in horses Author : Nicola Menzies-Gow Categories : Equine, Vets Date : July 4, 2016
Abbreviated Prescribing Information
 Abbreviated Prescribing Information balance 1.5% glucose, 1.75 mmol/l calcium, solution for peritoneal dialysis balance 2.3% glucose, 1.75 mmol/l calcium, solution for peritoneal dialysis balance 4.25%
Abbreviated Prescribing Information balance 1.5% glucose, 1.75 mmol/l calcium, solution for peritoneal dialysis balance 2.3% glucose, 1.75 mmol/l calcium, solution for peritoneal dialysis balance 4.25%
Diabetic Ketoacidosis
 Diabetic Ketoacidosis Definition: Diabetic Ketoacidosis is one of the most serious acute complications of diabetes. It s more common in young patients with type 1 diabetes mellitus. It s usually characterized
Diabetic Ketoacidosis Definition: Diabetic Ketoacidosis is one of the most serious acute complications of diabetes. It s more common in young patients with type 1 diabetes mellitus. It s usually characterized
Fluid Therapy and Outcome: Balance Is Best
 The Journal of ExtraCorporeal Technology Fluid Therapy and Outcome: Balance Is Best Sara J. Allen, FANZCA, FCICM Department of Anaesthesia and the Cardiothoracic and Vascular Intensive Care Unit, Auckland
The Journal of ExtraCorporeal Technology Fluid Therapy and Outcome: Balance Is Best Sara J. Allen, FANZCA, FCICM Department of Anaesthesia and the Cardiothoracic and Vascular Intensive Care Unit, Auckland
DISTRIBUTED SIMULATION PROJECT Management of IV Fluids and Electrolytes. Joy Hills 2013 RN, BSN, MSN (Cancer), SpecCertCR (Onc)
, SpecCertCR (Onc)") DISTRIBUTED SIMULATION PROJECT Management of IV Fluids and Electrolytes Joy Hills 2013 RN, BSN, MSN (Cancer), SpecCertCR (Onc) Professional responsibilities Obtaining and adhering to organisational guidelines.
DISTRIBUTED SIMULATION PROJECT Management of IV Fluids and Electrolytes Joy Hills 2013 RN, BSN, MSN (Cancer), SpecCertCR (Onc) Professional responsibilities Obtaining and adhering to organisational guidelines.
The changing face of
 The changing face of sepsis. @SepsisUK Dr Ron Daniels B.E.M. CEO, UK Sepsis Trust CEO, Global Sepsis Alliance Special Adviser (maternal sepsis) to WHO Breast cancer Cognitive impairment Mild 3.8 7.1
The changing face of sepsis. @SepsisUK Dr Ron Daniels B.E.M. CEO, UK Sepsis Trust CEO, Global Sepsis Alliance Special Adviser (maternal sepsis) to WHO Breast cancer Cognitive impairment Mild 3.8 7.1
Sepsis Management: Past, Present, and Future
 Sepsis Management: Past, Present, and Future Benjamin Ferrell, MD Tennessee ACP Meeting October 28, 2017 Learning Objectives Identify the most updated definition and clinical criteria for sepsis Describe
Sepsis Management: Past, Present, and Future Benjamin Ferrell, MD Tennessee ACP Meeting October 28, 2017 Learning Objectives Identify the most updated definition and clinical criteria for sepsis Describe
What is the Role of Albumin in Sepsis? An Evidenced Based Affair. Justin Belsky MD PGY3 2/6/14
 What is the Role of Albumin in Sepsis? An Evidenced Based Affair Justin Belsky MD PGY3 2/6/14 Microcirculation https://www.youtube.com/watch?v=xao1gsyur7q Capillary Leak in Sepsis Asking the RIGHT Question
What is the Role of Albumin in Sepsis? An Evidenced Based Affair Justin Belsky MD PGY3 2/6/14 Microcirculation https://www.youtube.com/watch?v=xao1gsyur7q Capillary Leak in Sepsis Asking the RIGHT Question
JOURNAL CLUB: THE FLUIDS DEBATE. Veronica Ueckermann
 JOURNAL CLUB: THE FLUIDS DEBATE Veronica Ueckermann INTRODUCTION The selection and use of resuscitation fluids should be based on physiological principles. However, historically, clinical practice has
JOURNAL CLUB: THE FLUIDS DEBATE Veronica Ueckermann INTRODUCTION The selection and use of resuscitation fluids should be based on physiological principles. However, historically, clinical practice has
National Institute for Health and Care Excellence. Intravenous Fluid Therapy - Adults Guideline Consultation Comments Table
 National Institute for Health and Care Excellence Intravenous Fluid Therapy - Adults Guideline Consultation Comments Table Typ e Stakeholder Order No of Anaesthetis ts of Anaesthetis ts Docum ent Section
National Institute for Health and Care Excellence Intravenous Fluid Therapy - Adults Guideline Consultation Comments Table Typ e Stakeholder Order No of Anaesthetis ts of Anaesthetis ts Docum ent Section