Surviving Sepsis. Brian Woodcock MBChB MRCP FRCA FCCM
|
|
|
- Dorthy Lamb
- 5 years ago
- Views:
Transcription

1 1 Surviving Sepsis Brian Woodcock MBChB MRCP FRCA FCCM
2 2 Disclosures No conflicts of interest
3 3 Sepsis Principles of management of septic shock in the operating room "Surviving Sepsis" guidelines
4 4 Add-on Case for Your OR Please call the front desk Butt case Add-on from Hell
5 5 The Case from Hell 76 year old man for exploratory laparotomy. 100kg Acute peritonitis ARDS and septic shock On intermittent positive pressure ventilation On vasopressors? paracolic abscess on CT scan

6 The Patient is on Some Drips 6
7 What is Sepsis? 7
8 8 Sepsis Life-threatening organ dysfunction caused by a dysregulated host response to infection Increased Sequential [Sepsis-related] Organ Failure Assessment (SOFA) score of 2+ In-hospital mortality greater than 10%.
9 9
10 10 Septic Shock Subset of sepsis with profound circulatory, cellular, and metabolic abnormalities Associated with a greater risk of mortality than with sepsis alone Vasopressor to MAP > 65 mm Hg Lactate level > 2 mmol/l in the absence of hypovolemia Hospital mortality rates >40%
11 11 Rapid Identification Out-of-hospital, emergency department, or general hospital ward settings, adult patients with suspected infection quicksofa (qsofa) Respiratory rate >22/min Altered mentation Systolic <100 mm Hg Score >= 2 indicates poor outcomes
12 12 The Case from Hell 76 year old man for exploratory laparotomy. 100kg Acute peritonitis ARDS and septic shock On intermittent positive pressure ventilation On vasopressors? paracolic abscess on CT scan
13 13 Why Are We Doing This Case? He is too sick for the OR. Can t they stabilize him before we take him?
14 14 Why? Recommend anatomic diagnosis of infection requiring emergent source control be identified Or excluded as rapidly as possible in patients with sepsis or septic shock Source control as soon as medically and logistically practical (Best Practice Statement)
15 15 What to Do? How should we manage the hemodynamic compromise? What fluids should we give? What is the best way to oxygenate this patient? Is there anything else we should give? What is the evidence for these maneuvers?
16 16 Can t We Just Set Some Goals? Numbers to aim for to make management easier
17 17 Shoemaker s Goals of Therapy 1980s Supranormal Values Blood volume increased by 500ml Cardiac Index > 4.5 l/min/m 2 Oxygen delivery > 600 ml/min/m 2 Oxygen consumption > 170 ml/min/m 2
18 18 Goal Directed Therapy of Sepsis Elevation of systemic oxygen delivery in the treatment of critically ill patients. Hayes MA - N Engl J Med 1994 A trial of goal-oriented hemodynamic therapy in critically ill patients. SvO2 Collaborative Group. Gattinoni L - N Engl J Med 1995
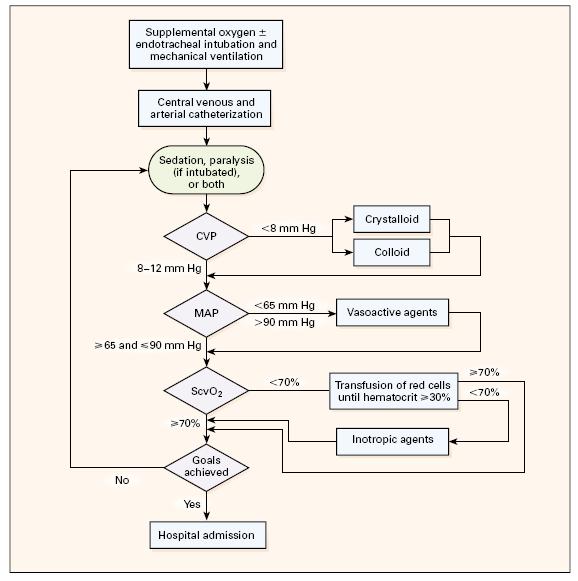
19 19 Early Goal-Directed Therapy Early goal-directed therapy in the treatment of severe sepsis and septic shock. Rivers E - N Engl J Med patients 130 randomized to early goal-directed therapy 133 randomized to standard therapy First 6 hours, prior to ICU admission
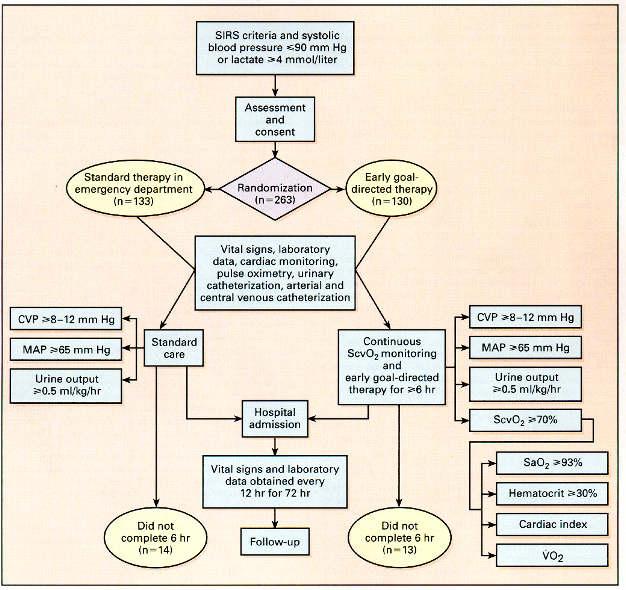
20 20
21 21
22 Results 22
23 23 Results During the 1 st 6 hours EGDT group received more intravenous fluid (5.0 vs. 3.5 L, p < 0.001) red cell transfusions (p < 0.001) inotropic therapy (p < 0.001) During the subsequent 66 hrs Control group More red cell transfusions (p < 0.001) More vasopressors (p = 0.03) More mechanical ventilation (p < 0.001) More pulmonary artery catheterization (p = 0.04)


24 A systematic review and meta-analysis of early goaldirected therapy for septic shock: the ARISE, ProCESS and ProMISe Investigators 24 Angus, D.C., Barnato, A.E., Bell, D. et al. Intensive Care Med (2015) 41: 1549
25 25 Surviving Sepsis Campaign Guidelines Critical Care Medicine International effort to increase awareness and improve outcome in severe sepsis 55 Critical Care and ID experts from 25 international organizations Consensus conference Graded review of the literature Graded recommendations
26 26
27 27 Initial Resuscitation At least 30 ml/kg of IV crystalloid fluid be given within the first 3 hours (strong recommendation, low quality of evidence) Additional fluids be guided by frequent reassessment of hemodynamic status (BPS) Assess cardiac function if the type of shock is not clear (BPS) Use dynamic over static variables to predict fluid responsiveness (weak recommendation, low quality of evidence)
28 28 Dynamic Variables to Predict Fluid Responsiveness Static variables CVP, left or right heart pressures or volumes Dynamic variables Passive leg raises Fluid challenges against: Stroke volume measurements Variations in systolic pressure, pulse pressure, or stroke volume to changes in intrathoracic pressure induced by mechanical ventilation
29 29
30 30 Initial Resuscitation Target MAP of 65 mm Hg if using vasopressors (strong recommendation, moderate quality of evidence). Guide resuscitation to normalize lactate, if elevated, as a marker of tissue hypoperfusion (weak recommendation, low quality of evidence)
 Balanced crystalloids or saline")
 No hetastarch")
31 31 Fluid Therapy - Colloid or Crystalloid 1 st Crystalloid? (strong recommendation, moderate quality of evidence) Balanced crystalloids or saline acceptable (weak recommendation, low quality of evidence) Albumin may be added if large amounts of crystalloid required (weak recommendation, low quality of evidence) No hetastarch (strong recommendation, high quality of evidence)
32 32 Safe Study Saline vs Albumin Fluid Evaluation ANZICS 16 academic tertiary hospitals 3497 patients resuscitated with albumin 3500 patients resuscitated with saline N Engl J Med 2004;350:

33 33 SAFE Results 726 deaths in the albumin group 729 deaths in the saline group
34 34 SAFE Results No significant differences Days spent in the ICU (6.5 albumin and 6.2 saline group) Days spent in the hospital (15.3 and 15.6) Days of mechanical ventilation (4.5 and 4.3) Days of renal-replacement therapy (0.5 and 0.4)
35 35 SAFE Results TBI mortality: Albumin 24.5% vs Saline 15.1%, p=0.009 Severe sepsis: Albumin 30.7% vs Saline 35.3%, p=0.09
 Sponsored by industry, had potential academic bias, or lack of blinding. Nicolai Haaseet al.")
36 Hetastarch Forest plot of all cause mortality in relation to risk of bias in trials 11% increased risk of mortality. And higher risk of RRT (RR, 1.36; 95% CI, ; (high-quality evidence) Sponsored by industry, had potential academic bias, or lack of blinding. Nicolai Haaseet al. BMJ 2013;346:bmj.f839
37 37 Back to our Patient Fully fluid resuscitated Still hypotensive What vasopressors should we choose?
38 38 Vasopressors Norepinephrine is the first-choice vasopressor (strong recommendation, moderate quality of evidence). Add either vasopressin (up to 0.03 U/min) (weak recommendation, moderate quality of evidence) to norepinephrine to raise MAP Or add epinephrine (weak recommendation, low quality of evidence) to norepinephrine to raise MAP Or add vasopressin (up to 0.03 U/min) (weak recommendation, moderate quality of evidence) to decrease norepinephrine dosage
39 39 VASST Vasopressin in Septic Shock Trial 1º hypothesis - Low dose vasopressin (0.03units/min) will decrease 28 day mortality from 60% to 50% in septic shock compared to norepinephrine alone 2º stratification Severe septic shock norepinephrine dose > 15 mcg/min Less severe septic shock = norepinephrne 5-14 mcg/min Resulted in 50% in each group Russell JA, et al; VASST Investigators: Vasopressin versus norepinephrine infusion in patients with septic shock. N Engl J Med 2008; 358:
40 40 VASST Inclusion Severe septic shock SIRS criteria 2/4 Infection 1 organ dysfunction Exclusion Septic shock > 24h Unstable heart Received any vasopressin Method Blinded infusion of vasopressin 0.01units/min or norepinephrine 5mcg/min Titrated to MAP mmhg If vasopressin reached 0.03units/min or norepi 15mcg/min then other pressors were added
41 41 VASST 28 day mortality Norepi Vasopressin p value Total 39.3% 35.4% 0.26 More severe sepsis 42.5% 44% 0.84 Less severe sepsis 35.7% 26.5% 0.04 Bottom line; mortality decreased with low dose vasopressin only in patients with less severe sepsis
42 42 Dopamine? Dopamine as an alternative agent to norepinephrine only in patients with low risk of tachyarrhythmias, who are bradycardic (weak recommendation, low quality of evidence) No low-dose dopamine for renal protection (strong recommendation, high quality of evidence).
43 43 Inotropes Dobutamine in patients with persistent hypoperfusion despite adequate fluid loading and the use of vasopressor agents (weak recommendation, low quality of evidence) Dobutamine titrated to an end point reflecting perfusion Reduced or discontinued if worsening hypotension or arrhythmias
44 44 Back to the OR Oxygen saturation is falling Volume control ventilation Vt 600ml (pt. weighs 100kg) Rate 14 Plateau pressure 35cm H2O FiO2 = 1 PEEP 5cm H2O ABG ph 7.32, po2 50, pco2 48, SO2 83%
45 45 Mechanical Ventilation of Sepsis-Induced Acute Lung Injury Lung protective ventilation (strong recommendation, high quality of evidence) Low tidal volume - 6 ml/kg End-inspiratory plateau pressures <30 cm H2 O Based on ARDSNet trial NEJM 2000 ; 342 :
46 46 ARDSNet Low Tidal Volumes 861 pts with acute lung injury Volume assist control mode Low tidal volume 6 ml/kg Predicted body weight Plateau pressure 30 cmh2o or less High tidal volume 12 ml/kg Plateau pressure 50 cmh2o or less
47 47 ARDSNet Mortality 31.0 % (Low Vt) vs 39.8 % (High Vt) P=0.007
48 48 ARDSNet Criticisms 12ml/kg is too much Nobody uses it U shaped dose response curve? Mortality Tidal volume ml/kg
49 49 Back to the OR Oxygen saturation is falling Volume control ventilation Vt 600ml (pt. weighs 100kg) Rate 14 Plateau pressure 35cm H2O FiO2 = 1 PEEP 5cm H2O Ht is 5 4 ; PBW is 60kg ABG ph 7.32, po2 50, pco2 48, SO2 83%
50 50 Mechanical Ventilation of Sepsis-Induced Acute Lung Injury Higher PEEP vs lower PEEP (weak recommendation, moderate quality of evidence) Recruitment maneuvers in severe ARDS (weak recommendation, moderate quality of evidence) Pronation in ARDS and a Pao2/Fio2 ratio < 150 (strong recommendation, moderate quality of evidence)
51 51 Methods to Ideal PEEP Titrate PEEP according to bedside measurements of thoraco-pulmonary compliance
52 52 Methods to Ideal PEEP Titrate PEEP upward on a tidal volume of 6 ml/kg PBW until the plateau airway pressure is cm H2O Use a PEEP/Fio2 titration table that titrates PEEP based on the combination of Fio2 and PEEP required to maintain adequate oxygenation
53 53 Pronation Gattinoni NEJM (2001) 345 : Significant improvement in oxygenation
54 54 Pronation Proseva Group, N Engl J Med 2013; 368: PaO 2 :FiO 2 ratio of <150 mm Hg Proned for 16 hours per day
55 55 ICU Strategies for Acute Lung Injury No high-frequency oscillatory ventilation in ARDS (strong recommendation, moderate quality of evidence) No recommendation for noninvasive ventilation in ARDS NMBs for 48 hours in ARDS and a Pao2/Fio2 ratio < 150 mm Hg (weak recommendation, moderate quality of evidence)
56 56 ICU Strategies Conservative fluid strategy for ARDS without tissue hypoperfusion (strong recommendation, moderate quality of evidence) No ß-2 agonists unless bronchospasm (strong recommendation, moderate quality of evidence) No pulmonary artery catheter for ARDS (strong recommendation, high quality of evidence) Lower tidal volumes over higher tidal volumes without ARDS (weak recommendation, low quality of evidence) Head of the bed elevated between 30 and 45 degrees to limit aspiration and ventilator-associated pneumonia (strong recommendation, low quality of evidence)
57 57 ICU Strategies Spontaneous breathing trials in ventilated patients ready for weaning (strong recommendation, high quality of evidence) Weaning protocol in ventilated patients when tolerated (strong recommendation, moderate quality of evidence)
58 58 Steroids High dose corticosteroids are ineffective or harmful - Grade A (2012) 1980s: Dexamethasone Shok-Pak:?1g Bone NEJM 317: , 1987 Mortality 59% vs 29%
59 59 Steroids Against using IV hydrocortisone to treat septic shock patients if adequate fluid resuscitation and vasopressor therapy are able to restore hemodynamic stability If this is not achievable, we suggest IV hydrocortisone at a dose of 200 mg per day (weak recommendation, low quality of evidence).
60 60 Low Dose Steroids All Patients Annane D Low Dose Steroids in Septic Shock JAMA 2002
61 61 CORTICUS 500 pateinets
62 62 CORTICUS Hydrocortisone does not decrease mortality in septic shock Does not increase reversal of shock but shock reverses quicker No polyneuropathy increase More superinfection ACTH is test not useful Hydrocortisone should not be routinely used in septic shock There may be a role in those still hypotensive after 1 hour
63 63 Glucose Control Protocolize treatment Start insulin when two blood glucose levels are > 180 mg/dl. Target an upper blood glucose level 180 mg/dl rather than 110 mg/dl (strong recommendation, high quality of evidence)
64 64 Tight Blood Glucose Control in ICU Prospective, randomized, controlled study 1548 patients Surgical intensive care unit 60% cardiac surgery On mechanical ventilation Conventional management Target BS 180 to 200 Insulin IVI started for BS > 215 Or Insulin IVI Target BS 80 to 110 Van Den Berghe G. NEJM 2001, 345;
65 65 Survival ICU Mortality 8% vs 4.6% p<0.04 In-hospital mortality reduced by 34 percent Van Den Berghe G. NEJM 2001, 345;
66 66 NICE-SUGAR Study 6104 patients randomized to tight (81-108) or loose (<180). ANZICS/Canada
67 67 Glucontrol ECCRN and ESICM sponsored, PRBCT, 21 ICUs across Europe At 1st interim analysis the study was stopped increased hypoglycemia increased mortality in tight Group increased protocol violations Other studies showed severe hypoglycemia (<40) in 6-29% with tight control
68 68 Blood Products Red cells Hb< 7 g/dl in the absence of myocardial ischemia, severe hypoxemia, or acute hemorrhage (strong recommendation, high quality of evidence) Erythropoietin: Not recommended (strong recommendation, moderate quality of evidence) FFP: Not recommended to correct PT/PTT, unless there is bleeding or a planned invasive procedures. (weak recommendation, very low quality of evidence). Platelets Prophylactic,in the absence of bleeding if < 10,000/mm3 Significant risk of bleeding if < 20,000/mm3 Active bleeding, surgery, or invasive procedures if < 50,000/mm3 (weak recommendation, very low quality of evidence)
69 69 Take Home Points Septic shock continues to have very high mortality Patients may presentto us in a very unstable state but still require surgery to treat the underlying cause of their sepsis Surviving Sepsis Campaign Guidelines Useful algorithm Based on the best available evidence
Sepsis Management: Past, Present, and Future
 Sepsis Management: Past, Present, and Future Benjamin Ferrell, MD Tennessee ACP Meeting October 28, 2017 Learning Objectives Identify the most updated definition and clinical criteria for sepsis Describe
Sepsis Management: Past, Present, and Future Benjamin Ferrell, MD Tennessee ACP Meeting October 28, 2017 Learning Objectives Identify the most updated definition and clinical criteria for sepsis Describe
Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock: 2016
 Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock: 2016 Mitchell M. Levy MD, MCCM Professor of Medicine Chief, Division of Pulmonary, Sleep, and Critical Care
Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock: 2016 Mitchell M. Levy MD, MCCM Professor of Medicine Chief, Division of Pulmonary, Sleep, and Critical Care
INTENSIVE CARE MEDICINE CPD EVENING. Dr Alastair Morgan Wednesday 13 th September 2017
 INTENSIVE CARE MEDICINE CPD EVENING Dr Alastair Morgan Wednesday 13 th September 2017 WHAT IS NEW IN ICU? (RELEVANT TO ANAESTHETISTS) Not much! SURVIVING SEPSIS How many deaths in England were thought
INTENSIVE CARE MEDICINE CPD EVENING Dr Alastair Morgan Wednesday 13 th September 2017 WHAT IS NEW IN ICU? (RELEVANT TO ANAESTHETISTS) Not much! SURVIVING SEPSIS How many deaths in England were thought
Sepsis overview. Dr. Tsang Hin Hung MBBS FHKCP FRCP
 Sepsis overview Dr. Tsang Hin Hung MBBS FHKCP FRCP Epidemiology Sepsis, severe sepsis, septic shock Pathophysiology of sepsis Recent researches and advances From bench to bedside Sepsis bundle Severe sepsis
Sepsis overview Dr. Tsang Hin Hung MBBS FHKCP FRCP Epidemiology Sepsis, severe sepsis, septic shock Pathophysiology of sepsis Recent researches and advances From bench to bedside Sepsis bundle Severe sepsis
Evidence-Based. Management of Severe Sepsis. What is the BP Target?
 Evidence-Based Management of Severe Sepsis Michael A. Gropper, MD, PhD Professor and Vice Chair of Anesthesia Director, Critical Care Medicine Chair, Quality Improvment University of California San Francisco
Evidence-Based Management of Severe Sepsis Michael A. Gropper, MD, PhD Professor and Vice Chair of Anesthesia Director, Critical Care Medicine Chair, Quality Improvment University of California San Francisco
Sepsis: Identification and Management in an Acute Care Setting
 Sepsis: Identification and Management in an Acute Care Setting Dr. Barbara M. Mills DNP Director Rapid Response Team/ Code Resuscitation Stony Brook University Medical Center SEPSIS LECTURE NPA 2018 OBJECTIVES
Sepsis: Identification and Management in an Acute Care Setting Dr. Barbara M. Mills DNP Director Rapid Response Team/ Code Resuscitation Stony Brook University Medical Center SEPSIS LECTURE NPA 2018 OBJECTIVES
Sepsis. From EMS to ER to ICU. What we need to be doing
 Sepsis From EMS to ER to ICU What we need to be doing NEHAL BHATT, MD ATHENS PULMONARY, CRITICAL CARE AND SLEEP Objectives 1. Define the changes to the definition of Sepsis 2. Describe the assessment,
Sepsis From EMS to ER to ICU What we need to be doing NEHAL BHATT, MD ATHENS PULMONARY, CRITICAL CARE AND SLEEP Objectives 1. Define the changes to the definition of Sepsis 2. Describe the assessment,
EFFECT OF EARLY VASOPRESSIN VS NOREPINEPHRINE ON KIDNEY FAILURE IN PATIENTS WITH SEPTIC SHOCK. Alexandria Rydz
 EFFECT OF EARLY VASOPRESSIN VS NOREPINEPHRINE ON KIDNEY FAILURE IN PATIENTS WITH SEPTIC SHOCK Alexandria Rydz BACKGROUND- SEPSIS Sepsis is defined as life-threatening organ dysfunction caused by a dysregulated
EFFECT OF EARLY VASOPRESSIN VS NOREPINEPHRINE ON KIDNEY FAILURE IN PATIENTS WITH SEPTIC SHOCK Alexandria Rydz BACKGROUND- SEPSIS Sepsis is defined as life-threatening organ dysfunction caused by a dysregulated
Early Goal-Directed Therapy
 Early Goal-Directed Therapy Where do we stand? Jean-Daniel Chiche, MD PhD MICU & Dept of Host-Pathogen Interaction Hôpital Cochin & Institut Cochin, Paris-F Resuscitation targets in septic shock 1 The
Early Goal-Directed Therapy Where do we stand? Jean-Daniel Chiche, MD PhD MICU & Dept of Host-Pathogen Interaction Hôpital Cochin & Institut Cochin, Paris-F Resuscitation targets in septic shock 1 The
The syndrome formerly known as. Severe Sepsis. James Rooks MD. Coordinator of critical care education OU College of Medicine, Tulsa
 The syndrome formerly known as Severe Sepsis James Rooks MD Coordinator of critical care education OU College of Medicine, Tulsa Disclosures I have no actual or practical conflicts of interest in relation
The syndrome formerly known as Severe Sepsis James Rooks MD Coordinator of critical care education OU College of Medicine, Tulsa Disclosures I have no actual or practical conflicts of interest in relation
Surviving Sepsis Campaign Guidelines 2012 & Update for David E. Tannehill, DO Critical Care Medicine Mercy Hospital St.
 Surviving Sepsis Campaign Guidelines 2012 & Update for 2015 David E. Tannehill, DO Critical Care Medicine Mercy Hospital St. Louis Be appropriately aggressive the longer one delays aggressive metabolic
Surviving Sepsis Campaign Guidelines 2012 & Update for 2015 David E. Tannehill, DO Critical Care Medicine Mercy Hospital St. Louis Be appropriately aggressive the longer one delays aggressive metabolic
OHSU. Update in Sepsis
 Update in Sepsis Jonathan Pak, MD June 1, 2017 Structure of Talk 1. Sepsis-3: The latest definition 2. Clinical Management - Is EGDT dead? - Surviving Sepsis Campaign Guidelines 3. A novel therapy: Vitamin
Update in Sepsis Jonathan Pak, MD June 1, 2017 Structure of Talk 1. Sepsis-3: The latest definition 2. Clinical Management - Is EGDT dead? - Surviving Sepsis Campaign Guidelines 3. A novel therapy: Vitamin
Sepsis and Hemodynamic Support in September 15, 2017 Carleen Risaliti
 Sepsis and Hemodynamic Support in 2017 September 15, 2017 Carleen Risaliti Objectives Review fluid resuscitation guidelines in septic shock Discuss volume assessment v. fluid responsiveness Evaluate pros
Sepsis and Hemodynamic Support in 2017 September 15, 2017 Carleen Risaliti Objectives Review fluid resuscitation guidelines in septic shock Discuss volume assessment v. fluid responsiveness Evaluate pros
Nothing to disclose 9/25/2017
 Jessie O Neal, PharmD, BCCCP Critical Care Clinical Pharmacist University of New Mexico Hospital New Mexico Society of Health-System Pharmacists 2017 Balloon Fiesta Symposium Nothing to disclose 1 Explain
Jessie O Neal, PharmD, BCCCP Critical Care Clinical Pharmacist University of New Mexico Hospital New Mexico Society of Health-System Pharmacists 2017 Balloon Fiesta Symposium Nothing to disclose 1 Explain
9/25/2017. Nothing to disclose
 Nothing to disclose Jessie O Neal, PharmD, BCCCP Critical Care Clinical Pharmacist University of New Mexico Hospital New Mexico Society of Health-System Pharmacists 2017 Balloon Fiesta Symposium Explain
Nothing to disclose Jessie O Neal, PharmD, BCCCP Critical Care Clinical Pharmacist University of New Mexico Hospital New Mexico Society of Health-System Pharmacists 2017 Balloon Fiesta Symposium Explain
Objectives. Management of Septic Shock. Definitions Progression of sepsis. Epidemiology of severe sepsis. Major goals of therapy
 Objectives Management of Septic Shock Review of the Evidence and Implementation of Pediatric Guidelines at Christus Santa Rosa Manish Desai, M.D. PL 5 2 nd year Pediatric Critical Care Fellow Review of
Objectives Management of Septic Shock Review of the Evidence and Implementation of Pediatric Guidelines at Christus Santa Rosa Manish Desai, M.D. PL 5 2 nd year Pediatric Critical Care Fellow Review of
Sepsis is an important issue. Clinician s decision-making capability. Guideline recommendations
 Surviving Sepsis Campaign: International Guidelines for Management of Severe Sepsis and Septic Shock: 2012 Clinicians decision-making capability Guideline recommendations Sepsis is an important issue 8.7%
Surviving Sepsis Campaign: International Guidelines for Management of Severe Sepsis and Septic Shock: 2012 Clinicians decision-making capability Guideline recommendations Sepsis is an important issue 8.7%
Controversies in Hospital Medicine: Critical Care. Vasopressors, Steroids, and Insulin Therapy
 Controversies in Hospital Medicine: Critical Care Vasopressors, Steroids, and Insulin Therapy Douglas Fish, Pharm.D. Professor of Pharmacy, University of Colorado Denver Clinical Specialist in Critical
Controversies in Hospital Medicine: Critical Care Vasopressors, Steroids, and Insulin Therapy Douglas Fish, Pharm.D. Professor of Pharmacy, University of Colorado Denver Clinical Specialist in Critical
Surviving Sepsis Campaign
 Surviving Sepsis Campaign Guidelines for Management of Severe Sepsis/Septic Shock An Overview By professor Ahmad Alaysh BMC-MICU 1 Surviving Sepsis A global program to Reduce mortality rates in severe
Surviving Sepsis Campaign Guidelines for Management of Severe Sepsis/Septic Shock An Overview By professor Ahmad Alaysh BMC-MICU 1 Surviving Sepsis A global program to Reduce mortality rates in severe
The Ever Changing World of Sepsis Management. Laura Evans MD MSc Medical Director of Critical Care Bellevue Hospital
 The Ever Changing World of Sepsis Management Laura Evans MD MSc Medical Director of Critical Care Bellevue Hospital COI Disclosures No financial interests to disclose Learning Objectives Review the evolution
The Ever Changing World of Sepsis Management Laura Evans MD MSc Medical Director of Critical Care Bellevue Hospital COI Disclosures No financial interests to disclose Learning Objectives Review the evolution
4/5/2018. Update on Sepsis NIKHIL JAGAN PULMONARY AND CRITICAL CARE CREIGHTON UNIVERSITY. I have no financial disclosures
 Update on Sepsis NIKHIL JAGAN PULMONARY AND CRITICAL CARE CREIGHTON UNIVERSITY I have no financial disclosures 1 Objectives Why do we care about sepsis Understanding the core measures by Centers for Medicare
Update on Sepsis NIKHIL JAGAN PULMONARY AND CRITICAL CARE CREIGHTON UNIVERSITY I have no financial disclosures 1 Objectives Why do we care about sepsis Understanding the core measures by Centers for Medicare
Initial Resuscitation of Sepsis & Septic Shock
 Initial Resuscitation of Sepsis & Septic Shock Dr. Fatema Ahmed MD (Critical Care Medicine) FCPS (Medicine) Associate professor Dept. of Critical Care Medicine BIRDEM General Hospital Is Sepsis a known
Initial Resuscitation of Sepsis & Septic Shock Dr. Fatema Ahmed MD (Critical Care Medicine) FCPS (Medicine) Associate professor Dept. of Critical Care Medicine BIRDEM General Hospital Is Sepsis a known
Update in Critical Care Medicine
 Update in Critical Care Medicine Michael A. Gropper, MD, PhD Professor and Executive Vice Chair Department of Anesthesia and Perioperative Care Director, Critical Care Medicine UCSF Disclosure None Update
Update in Critical Care Medicine Michael A. Gropper, MD, PhD Professor and Executive Vice Chair Department of Anesthesia and Perioperative Care Director, Critical Care Medicine UCSF Disclosure None Update
SEPSIS: IT ALL BEGINS WITH INFECTION. Theresa Posani, MS, RN, ACNS-BC, CCRN M/S CNS/Sepsis Coordinator Texas Health Harris Methodist Ft.
 SEPSIS: IT ALL BEGINS WITH INFECTION Theresa Posani, MS, RN, ACNS-BC, CCRN M/S CNS/Sepsis Coordinator Texas Health Harris Methodist Ft. Worth 1 2 3 OBJECTIVES Review the new Sepsis 3 definitions of sepsis
SEPSIS: IT ALL BEGINS WITH INFECTION Theresa Posani, MS, RN, ACNS-BC, CCRN M/S CNS/Sepsis Coordinator Texas Health Harris Methodist Ft. Worth 1 2 3 OBJECTIVES Review the new Sepsis 3 definitions of sepsis
Sepsis: Management ANUPOL PANITCHOTE, MD. Division of Critical Care Medicine Department of Medicine, Khon Kaen University, Thailand
 Sepsis: Management ANUPOL PANITCHOTE, MD. Division of Critical Care Medicine Department of Medicine, Khon Kaen University, Thailand Vital signs Symptoms LAB BT > 38.3 or < 36 ๐ C HR > 90 bpm RR > 20 /min
Sepsis: Management ANUPOL PANITCHOTE, MD. Division of Critical Care Medicine Department of Medicine, Khon Kaen University, Thailand Vital signs Symptoms LAB BT > 38.3 or < 36 ๐ C HR > 90 bpm RR > 20 /min
Surviving Sepsis Campaign. Guidelines for Management of Severe Sepsis/Septic Shock. An Overview
 Surviving Sepsis Campaign Guidelines for Management of Severe Sepsis/Septic Shock An Overview Mechanical Ventilation of Sepsis-Induced ALI/ARDS ARDSnet Mechanical Ventilation Protocol Results: Mortality
Surviving Sepsis Campaign Guidelines for Management of Severe Sepsis/Septic Shock An Overview Mechanical Ventilation of Sepsis-Induced ALI/ARDS ARDSnet Mechanical Ventilation Protocol Results: Mortality
SEPSIS 2015 DISCLOSURES FINANCIAL DISCLOSURES 9/1/2015. William M. Johnson, MD Nebraska Pulmonary Specialties. William Johnson
 SEPSIS 2015 William M. Johnson, MD Nebraska Pulmonary Specialties 1 DISCLOSURES William Johnson No financial interests related to this presentation 2 FINANCIAL DISCLOSURES I do however have 3 children
SEPSIS 2015 William M. Johnson, MD Nebraska Pulmonary Specialties 1 DISCLOSURES William Johnson No financial interests related to this presentation 2 FINANCIAL DISCLOSURES I do however have 3 children
Sepsis Update: Focus on Early Recognition and Intervention. Disclosures
 Sepsis Update: Focus on Early Recognition and Intervention Jessie Roske, MD October 2017 Disclosures I have no actual or potential conflict of interest in relation to this program/presentation. I will
Sepsis Update: Focus on Early Recognition and Intervention Jessie Roske, MD October 2017 Disclosures I have no actual or potential conflict of interest in relation to this program/presentation. I will
John Park, MD Assistant Professor of Medicine
 John Park, MD Assistant Professor of Medicine Faculty photo will be placed here park.john@mayo.edu 2015 MFMER 3543652-1 Sepsis Out with the Old, In with the New Mayo School of Continuous Professional Development
John Park, MD Assistant Professor of Medicine Faculty photo will be placed here park.john@mayo.edu 2015 MFMER 3543652-1 Sepsis Out with the Old, In with the New Mayo School of Continuous Professional Development
CORTICOSTEROID USE IN SEPTIC SHOCK THE ONGOING DEBATE DIEM HO, PHARMD PGY1 PHARMACY RESIDENT VALLEY BAPTIST MEDICAL CENTER BROWNSVILLE
 CORTICOSTEROID USE IN SEPTIC SHOCK THE ONGOING DEBATE DIEM HO, PHARMD PGY1 PHARMACY RESIDENT VALLEY BAPTIST MEDICAL CENTER BROWNSVILLE 1 ABBREVIATIONS ACCP = American College of Chest Physicians ARF =
CORTICOSTEROID USE IN SEPTIC SHOCK THE ONGOING DEBATE DIEM HO, PHARMD PGY1 PHARMACY RESIDENT VALLEY BAPTIST MEDICAL CENTER BROWNSVILLE 1 ABBREVIATIONS ACCP = American College of Chest Physicians ARF =
Fluid Resuscitation and Monitoring in Sepsis. Deepa Gotur, MD, FCCP Anne Rain T. Brown, PharmD, BCPS
 Fluid Resuscitation and Monitoring in Sepsis Deepa Gotur, MD, FCCP Anne Rain T. Brown, PharmD, BCPS Learning Objectives Compare and contrast fluid resuscitation strategies in septic shock Discuss available
Fluid Resuscitation and Monitoring in Sepsis Deepa Gotur, MD, FCCP Anne Rain T. Brown, PharmD, BCPS Learning Objectives Compare and contrast fluid resuscitation strategies in septic shock Discuss available
Sepsis Management Update 2014
 Sepsis Management Update 2014 Laura J. Moore, MD, FACS Associate Professor, Department of Surgery The University of Texas Health Science Center, Houston Medical Director, Shock Trauma ICU Texas Trauma
Sepsis Management Update 2014 Laura J. Moore, MD, FACS Associate Professor, Department of Surgery The University of Texas Health Science Center, Houston Medical Director, Shock Trauma ICU Texas Trauma
No conflicts of interest to disclose
 No conflicts of interest to disclose Introduction Epidemiology Surviving sepsis guidelines 2012 Updates Resuscitation protocols Map Goals Transfusion Sepsis-3 Bundle Management Questions Sepsis is a systemic,
No conflicts of interest to disclose Introduction Epidemiology Surviving sepsis guidelines 2012 Updates Resuscitation protocols Map Goals Transfusion Sepsis-3 Bundle Management Questions Sepsis is a systemic,
Staging Sepsis for the Emergency Department: Physician
 Staging Sepsis for the Emergency Department: Physician Sepsis Continuum 1 Sepsis Continuum SIRS = 2 or more clinical criteria, resulting in Systemic Inflammatory Response Syndrome Sepsis = SIRS + proven/suspected
Staging Sepsis for the Emergency Department: Physician Sepsis Continuum 1 Sepsis Continuum SIRS = 2 or more clinical criteria, resulting in Systemic Inflammatory Response Syndrome Sepsis = SIRS + proven/suspected
Fluids in Sepsis: How much and what type? John Fowler, MD, FACEP Kent Hospital, İzmir Eisenhower Medical Center, USA American Hospital Dubai, UAE
 Fluids in Sepsis: How much and what type? John Fowler, MD, FACEP Kent Hospital, İzmir Eisenhower Medical Center, USA American Hospital Dubai, UAE In critically ill patients: too little fluid Low preload,
Fluids in Sepsis: How much and what type? John Fowler, MD, FACEP Kent Hospital, İzmir Eisenhower Medical Center, USA American Hospital Dubai, UAE In critically ill patients: too little fluid Low preload,
What the ED clinician needs to know about SEPSIS - 3. Anna Morgan Consultant EM Barts Health
 What the ED clinician needs to know about SEPSIS - 3 Anna Morgan Consultant EM Barts Health Aims: (1) To review the Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3) (2)
What the ED clinician needs to know about SEPSIS - 3 Anna Morgan Consultant EM Barts Health Aims: (1) To review the Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3) (2)
UPDATES IN SEPSIS MANAGEMENT Shannon Fry, Pharm.D. Critical Care Pharmacy Specialist St. Joseph Medical Center
 UPDATES IN SEPSIS MANAGEMENT Shannon Fry, Pharm.D. Critical Care Pharmacy Specialist St. Joseph Medical Center ShannonFry@fhshealth.org DISCLOSURE I have no financial relationships to disclose OBJECTIVES
UPDATES IN SEPSIS MANAGEMENT Shannon Fry, Pharm.D. Critical Care Pharmacy Specialist St. Joseph Medical Center ShannonFry@fhshealth.org DISCLOSURE I have no financial relationships to disclose OBJECTIVES
DESIGNER RESUSCITATION: TITRATING TO TISSUE NEEDS
 DESIGNER RESUSCITATION: TITRATING TO TISSUE NEEDS R. Phillip Dellinger MD, MSc, MCCM Professor and Chair of Medicine Cooper Medical School of Rowan University Chief of Medicine Cooper University Hospital
DESIGNER RESUSCITATION: TITRATING TO TISSUE NEEDS R. Phillip Dellinger MD, MSc, MCCM Professor and Chair of Medicine Cooper Medical School of Rowan University Chief of Medicine Cooper University Hospital
Sepsis Learning Collaborative: Sepsis New Definitions
 Sepsis Learning Collaborative: Sepsis New Definitions Sepsis 3, a New Definition Todd L. Slesinger, MD, FACEP, FCCM, FCCP, FAAEM Program Director and Academic Chair Department of Emergency Medicine Disclosures
Sepsis Learning Collaborative: Sepsis New Definitions Sepsis 3, a New Definition Todd L. Slesinger, MD, FACEP, FCCM, FCCP, FAAEM Program Director and Academic Chair Department of Emergency Medicine Disclosures
6-horas 24 horas Coleta de lactato Hemoculturas. Corticosteróides. Controle glicêmico. Fluidos/vasopressores. Otimização de SvO 2
 Novas diretrizes da Surviving Sepsis Campaign 2012 o que foi atualizado? Os pacotes da sepse 6-horas 24 horas Coleta de lactato Hemoculturas Corticosteróides Antibióticos Proteína C ativdada Fluidos/vasopressores
Novas diretrizes da Surviving Sepsis Campaign 2012 o que foi atualizado? Os pacotes da sepse 6-horas 24 horas Coleta de lactato Hemoculturas Corticosteróides Antibióticos Proteína C ativdada Fluidos/vasopressores
6/5/2014. Sepsis Management and Hemodynamics. 2004: International group of experts,
 Sepsis Management and Hemodynamics Javier Perez-Fernandez, M.D., F.C.C.P. Medical Director Critical Care Services, Baptist t Hospital of Miamii Medical Director Pulmonary Services, West Kendall Baptist
Sepsis Management and Hemodynamics Javier Perez-Fernandez, M.D., F.C.C.P. Medical Director Critical Care Services, Baptist t Hospital of Miamii Medical Director Pulmonary Services, West Kendall Baptist
Tailored Volume Resuscitation in the Critically Ill is Achievable. Objectives. Clinical Case 2/16/2018
 Tailored Volume Resuscitation in the Critically Ill is Achievable Heath E Latham, MD Associate Professor Fellowship Program Director Pulmonary and Critical Care Objectives Describe the goal of resuscitation
Tailored Volume Resuscitation in the Critically Ill is Achievable Heath E Latham, MD Associate Professor Fellowship Program Director Pulmonary and Critical Care Objectives Describe the goal of resuscitation
Management of Severe Sepsis:
 Management of Severe Sepsis: Update from the Surviving Sepsis Campaign Barbara Birriel, MSN, ACNP-BC, FCCM The Pennsylvania State University NONE Disclosures Review evidence-based international sepsis
Management of Severe Sepsis: Update from the Surviving Sepsis Campaign Barbara Birriel, MSN, ACNP-BC, FCCM The Pennsylvania State University NONE Disclosures Review evidence-based international sepsis
ARDS: an update 6 th March A. Hakeem Al Hashim, MD, FRCP SQUH
 ARDS: an update 6 th March 2017 A. Hakeem Al Hashim, MD, FRCP SQUH 30M, previously healthy Hx: 1 week dry cough Gradually worsening SOB No travel Hx Case BP 130/70, HR 100/min ph 7.29 pco2 35 po2 50 HCO3
ARDS: an update 6 th March 2017 A. Hakeem Al Hashim, MD, FRCP SQUH 30M, previously healthy Hx: 1 week dry cough Gradually worsening SOB No travel Hx Case BP 130/70, HR 100/min ph 7.29 pco2 35 po2 50 HCO3
Septic Shock. Rontgene M. Solante, MD, FPCP,FPSMID
 Septic Shock Rontgene M. Solante, MD, FPCP,FPSMID Learning Objectives Identify situations wherein high or low BP are hemodynamically significant Recognize complications arising from BP emergencies Manage
Septic Shock Rontgene M. Solante, MD, FPCP,FPSMID Learning Objectives Identify situations wherein high or low BP are hemodynamically significant Recognize complications arising from BP emergencies Manage
Diagnosis and Management of Sepsis. Disclosures
 Diagnosis and Management of Sepsis David Shimabukuro, MDCM Medical Director, 13 ICU Physician Lead, UCSF Sepsis Bundle Compliance and Mortality Reduction I have no disclosures Disclosures 1 The following
Diagnosis and Management of Sepsis David Shimabukuro, MDCM Medical Director, 13 ICU Physician Lead, UCSF Sepsis Bundle Compliance and Mortality Reduction I have no disclosures Disclosures 1 The following
Jawad Nazir, MD, FACP Medical Director, Infection Prevention and Control Avera Health and Avera McKennan Hospital Clinical Associate Professor of
 Jawad Nazir, MD, FACP Medical Director, Infection Prevention and Control Avera Health and Avera McKennan Hospital Clinical Associate Professor of Medicine Sanford School of Medicine, Univ of South Dakota
Jawad Nazir, MD, FACP Medical Director, Infection Prevention and Control Avera Health and Avera McKennan Hospital Clinical Associate Professor of Medicine Sanford School of Medicine, Univ of South Dakota
Back to the Future: Updated Guidelines for Evaluation and Management of Adrenal Insufficiency in the Critically Ill
 Back to the Future: Updated Guidelines for Evaluation and Management of Adrenal Insufficiency in the Critically Ill Joe Palumbo PGY-2 Critical Care Pharmacy Resident Buffalo General Medical Center Disclosures
Back to the Future: Updated Guidelines for Evaluation and Management of Adrenal Insufficiency in the Critically Ill Joe Palumbo PGY-2 Critical Care Pharmacy Resident Buffalo General Medical Center Disclosures
Diagnosis and Management of Sepsis and Septic Shock. Martin D. Black MD Concord Pulmonary Medicine Concord, New Hampshire
 Diagnosis and Management of Sepsis and Septic Shock Martin D. Black MD Concord Pulmonary Medicine Concord, New Hampshire Financial: none Disclosures Objectives: Identify physiologic principles of septic
Diagnosis and Management of Sepsis and Septic Shock Martin D. Black MD Concord Pulmonary Medicine Concord, New Hampshire Financial: none Disclosures Objectives: Identify physiologic principles of septic
Update in Sepsis. Conflicts of Interest: None. Bill Janssen, M.D.
 Update in Sepsis Bill Janssen, M.D. Associate Professor of Medicine National Jewish Health University of Colorado Denver Conflicts of Interest: None A 62 year-old female presents to the ED with fever,
Update in Sepsis Bill Janssen, M.D. Associate Professor of Medicine National Jewish Health University of Colorado Denver Conflicts of Interest: None A 62 year-old female presents to the ED with fever,
Acute Liver Failure: Supporting Other Organs
 Acute Liver Failure: Supporting Other Organs Michael A. Gropper, MD, PhD Professor of Anesthesia and Physiology Director, Critical Care Medicine University of California San Francisco Acute Liver Failure
Acute Liver Failure: Supporting Other Organs Michael A. Gropper, MD, PhD Professor of Anesthesia and Physiology Director, Critical Care Medicine University of California San Francisco Acute Liver Failure
Objectives. Epidemiology of Sepsis. Review Guidelines for Resuscitation. Tx: EGDT, timing/choice of abx, activated
 Update on Surviving Sepsis 2008 Objectives Epidemiology of Sepsis Definition of Sepsis and Septic Shock Review Guidelines for Resuscitation Dx: Lactate, t cultures, SVO2 Tx: EGDT, timing/choice of abx,
Update on Surviving Sepsis 2008 Objectives Epidemiology of Sepsis Definition of Sepsis and Septic Shock Review Guidelines for Resuscitation Dx: Lactate, t cultures, SVO2 Tx: EGDT, timing/choice of abx,
3 papers from ED. counting sepsis sepsis 3 wet or dry?
 3 papers from ED counting sepsis sepsis 3 wet or dry? 5 million deaths/yr globally 24 billion USD annually in US system causes or contributes to half of US hospital deaths BP GCS RR From: The Third International
3 papers from ED counting sepsis sepsis 3 wet or dry? 5 million deaths/yr globally 24 billion USD annually in US system causes or contributes to half of US hospital deaths BP GCS RR From: The Third International
Sepsis Story At Intermountain Healthcare Intensive Medicine Clinical Program
 Sepsis Story At Intermountain Healthcare 2004-2012 Intensive Medicine Clinical Program The International Surviving Sepsis Campaign Was Organized In 2002 During The ESICM International Meeting In Barcelona,
Sepsis Story At Intermountain Healthcare 2004-2012 Intensive Medicine Clinical Program The International Surviving Sepsis Campaign Was Organized In 2002 During The ESICM International Meeting In Barcelona,
Actualités de la prise en charge hémodynamique initiale Daniel De Backer
 Actualités de la prise en charge hémodynamique initiale Daniel De Backer Head Dept Intensive Care, CHIREC hospitals, Belgium Professor of Intensive Care, Université Libre de Bruxelles Past- President European
Actualités de la prise en charge hémodynamique initiale Daniel De Backer Head Dept Intensive Care, CHIREC hospitals, Belgium Professor of Intensive Care, Université Libre de Bruxelles Past- President European
Sepsis or Severe Sepsis? Is there a right thing, and how do we do it?
 Sepsis or Severe Sepsis? Is there a right thing, and how do we do it? Steven Q Simpson, MD, FCCP, FACP Professor of Medicine Division of Pulmonary and Critical Care University of Kansas Disclosures No
Sepsis or Severe Sepsis? Is there a right thing, and how do we do it? Steven Q Simpson, MD, FCCP, FACP Professor of Medicine Division of Pulmonary and Critical Care University of Kansas Disclosures No
Ralph Palumbo, MD, FCCP
 Ralph Palumbo, MD, FCCP Septic shock is the leading cause of mortality in patients admitted to the ICU In the United States alone there are over 750,000 cases of severe sepsis and septic shock annually
Ralph Palumbo, MD, FCCP Septic shock is the leading cause of mortality in patients admitted to the ICU In the United States alone there are over 750,000 cases of severe sepsis and septic shock annually
The Management of Septic Shock
 The Management of Septic Shock Anthony J. Courey, MD Assistant Professor of Medicine Associate Director, CCMU Pulmonary & Critical Care Medicine No conflicts No disclosures Conflicts & Disclosures Overview
The Management of Septic Shock Anthony J. Courey, MD Assistant Professor of Medicine Associate Director, CCMU Pulmonary & Critical Care Medicine No conflicts No disclosures Conflicts & Disclosures Overview
Updates On Sepsis Updates based on 2016 updates on sepsis from The International Surviving Sepsis Campaign
 Updates On Sepsis Updates based on 2016 updates on sepsis from The International Surviving Sepsis Campaign Dr. Joseph K Erbe, DO Medical Director Hospitalist Division of Medicine Objectives 1. Review the
Updates On Sepsis Updates based on 2016 updates on sepsis from The International Surviving Sepsis Campaign Dr. Joseph K Erbe, DO Medical Director Hospitalist Division of Medicine Objectives 1. Review the
Rounds in the ICU. Eran Segal, MD Director General ICU Sheba Medical Center
 Rounds in the ICU Eran Segal, MD Director General ICU Sheba Medical Center Real Clinical cases (including our mistakes) Emphasis on hemodynamic monitoring Usually no single correct answer We will conduct
Rounds in the ICU Eran Segal, MD Director General ICU Sheba Medical Center Real Clinical cases (including our mistakes) Emphasis on hemodynamic monitoring Usually no single correct answer We will conduct
Early Goal Directed Therapy in 2015: What Did the Big Trials Teach us?
 Early Goal Directed Therapy in 2015: What Did the Big Trials Teach us? Mitchell M. Levy MD, FCCM Professor of Medicine Chief, Division of Pulmonary, Sleep, and Critical Care Warren Alpert Medical School
Early Goal Directed Therapy in 2015: What Did the Big Trials Teach us? Mitchell M. Levy MD, FCCM Professor of Medicine Chief, Division of Pulmonary, Sleep, and Critical Care Warren Alpert Medical School
Epidemiology of Severe Sepsis
 Dellinger et al Crit Care Med 2008 Surviving Sepsis Phase I: the Barcelona Declaration Phase II: development and publication of guidelines 2004, updated in 2008 Phase III: operationalize the guidelines,
Dellinger et al Crit Care Med 2008 Surviving Sepsis Phase I: the Barcelona Declaration Phase II: development and publication of guidelines 2004, updated in 2008 Phase III: operationalize the guidelines,
Sepsis 3 & Early Identification. Disclosures. Objectives 9/19/2016. David Carlbom, MD Medical Director, HMC Sepsis Program
 Sepsis 3 & Early Identification David Carlbom, MD Medical Director, HMC Sepsis Program Disclosures I have no relevant financial relationships with a commercial interest and will not discuss off-label use
Sepsis 3 & Early Identification David Carlbom, MD Medical Director, HMC Sepsis Program Disclosures I have no relevant financial relationships with a commercial interest and will not discuss off-label use
Early-goal-directed therapy and protocolised treatment in septic shock
 CAT reviews Early-goal-directed therapy and protocolised treatment in septic shock Journal of the Intensive Care Society 2015, Vol. 16(2) 164 168! The Intensive Care Society 2014 Reprints and permissions:
CAT reviews Early-goal-directed therapy and protocolised treatment in septic shock Journal of the Intensive Care Society 2015, Vol. 16(2) 164 168! The Intensive Care Society 2014 Reprints and permissions:
SHOCK. Emergency pediatric PICU division Pediatric Department Medical Faculty, University of Sumatera Utara H. Adam Malik Hospital
 SHOCK Emergency pediatric PICU division Pediatric Department Medical Faculty, University of Sumatera Utara H. Adam Malik Hospital 1 Definition Shock is an acute, complex state of circulatory dysfunction
SHOCK Emergency pediatric PICU division Pediatric Department Medical Faculty, University of Sumatera Utara H. Adam Malik Hospital 1 Definition Shock is an acute, complex state of circulatory dysfunction
Goal-directed resuscitation in sepsis; a case-based approach
 Goal-directed resuscitation in sepsis; a case-based approach Jorge A Guzman, MD, FCCM Head, Section Critical Care Medicine Respiratory Institute Cleveland Clinic Foundation The challenges to managing septic
Goal-directed resuscitation in sepsis; a case-based approach Jorge A Guzman, MD, FCCM Head, Section Critical Care Medicine Respiratory Institute Cleveland Clinic Foundation The challenges to managing septic
JAMA. 2016;315(8): doi: /jama
: doi: /jama") JAMA. 2016;315(8):801-810. doi:10.1001/jama.2016.0287 SEPSIS 3 life-threatening organ dysfunction caused by a dysregulated host response to infection organ dysfunction: an increase in the SOFA
JAMA. 2016;315(8):801-810. doi:10.1001/jama.2016.0287 SEPSIS 3 life-threatening organ dysfunction caused by a dysregulated host response to infection organ dysfunction: an increase in the SOFA
Wet Lungs Dry lungs Impact on Outcome in ARDS. Charlie Phillips MD Division of PCCM OHSU 2009
 Wet Lungs Dry lungs Impact on Outcome in ARDS Charlie Phillips MD Division of PCCM OHSU 2009 Today s talk Pathophysiology of ARDS The case for dry Targeting EVLW Disclosures Advisor for Pulsion Medical
Wet Lungs Dry lungs Impact on Outcome in ARDS Charlie Phillips MD Division of PCCM OHSU 2009 Today s talk Pathophysiology of ARDS The case for dry Targeting EVLW Disclosures Advisor for Pulsion Medical
Immunomodulation and Sepsis in Oncological Patients. Imad Haddad, M.D. Medical Director, PICU Banner Children s Hospital at BDMC
 Immunomodulation and Sepsis in Oncological Patients Imad Haddad, M.D. Medical Director, PICU Banner Children s Hospital at BDMC 1 Objectives Immune dys-regulation in oncological septic patients Implementation
Immunomodulation and Sepsis in Oncological Patients Imad Haddad, M.D. Medical Director, PICU Banner Children s Hospital at BDMC 1 Objectives Immune dys-regulation in oncological septic patients Implementation
EBM EGDT 每次都是RCT.有點煩 本來想簡單處理 那些年我們曾經打拼過的~~ By Maxy Lu 這次想要放鬆一下~~ EGDT (Early goal-directed therapy) Early go to ICU
 Early go to ICU") EBM 2014.03.24 By Maxy Lu 每次都是RCT.有點煩 這次想要放鬆一下~~ 本來想簡單處理 EGDT (Early goal-directed therapy) 那些年我們曾經打拼過的~~ EGDT Early go to ICU 想說這下開心了 Best practice Not Standard of care Screening and practice improvement
EBM 2014.03.24 By Maxy Lu 每次都是RCT.有點煩 這次想要放鬆一下~~ 本來想簡單處理 EGDT (Early goal-directed therapy) 那些年我們曾經打拼過的~~ EGDT Early go to ICU 想說這下開心了 Best practice Not Standard of care Screening and practice improvement
Titrating Critical Care Medications
 Titrating Critical Care Medications Chad Johnson, MSN (NED), RN, CNCC(C), CNS-cc Clinical Nurse Specialist: Critical Care and Neurosurgical Services E-mail: johnsoc@tbh.net Copyright 2017 1 Learning Objectives
Titrating Critical Care Medications Chad Johnson, MSN (NED), RN, CNCC(C), CNS-cc Clinical Nurse Specialist: Critical Care and Neurosurgical Services E-mail: johnsoc@tbh.net Copyright 2017 1 Learning Objectives
The Septic Patient. Dr Arunraj Navaratnarajah. Renal SpR Imperial College NHS Healthcare Trust
 The Septic Patient Dr Arunraj Navaratnarajah Renal SpR Imperial College NHS Healthcare Trust Objectives of this session Define SIRS / sepsis / severe sepsis / septic shock Early recognition of Sepsis The
The Septic Patient Dr Arunraj Navaratnarajah Renal SpR Imperial College NHS Healthcare Trust Objectives of this session Define SIRS / sepsis / severe sepsis / septic shock Early recognition of Sepsis The
Updates in Sepsis 2017
 Mortality Cases Total U.S. Population/1,000 Updates in 2017 Joshua Solomon, M.D. Associate Professor of Medicine National Jewish Health University of Colorado Denver Background New Definition of New Trials
Mortality Cases Total U.S. Population/1,000 Updates in 2017 Joshua Solomon, M.D. Associate Professor of Medicine National Jewish Health University of Colorado Denver Background New Definition of New Trials
UTILITY of ScvO 2 and LACTATE
 UTILITY of ScvO 2 and LACTATE Professor Jeffrey Lipman Department of Intensive Care Medicine Royal Brisbane Hospital University of Queensland THIS TRIP SPONSORED AND PAID FOR BY STRUCTURE Physiology -
UTILITY of ScvO 2 and LACTATE Professor Jeffrey Lipman Department of Intensive Care Medicine Royal Brisbane Hospital University of Queensland THIS TRIP SPONSORED AND PAID FOR BY STRUCTURE Physiology -
PHYSIOLOGY AND MANAGEMENT OF THE SEPTIC PATIENT
 PHYSIOLOGY AND MANAGEMENT OF THE SEPTIC PATIENT Melanie Sanchez, RN, MSNE, OCN, CCRN Clinical Nurse III City of Hope National Medical Center HOW THE EXPERTS TREAT HEMATOLOGIC MALIGNANCIES LAS VEGAS, NV
PHYSIOLOGY AND MANAGEMENT OF THE SEPTIC PATIENT Melanie Sanchez, RN, MSNE, OCN, CCRN Clinical Nurse III City of Hope National Medical Center HOW THE EXPERTS TREAT HEMATOLOGIC MALIGNANCIES LAS VEGAS, NV
R2R: Severe sepsis/septic shock. Surat Tongyoo Critical care medicine Siriraj Hospital
 R2R: Severe sepsis/septic shock Surat Tongyoo Critical care medicine Siriraj Hospital Diagnostic criteria ACCP/SCCM consensus conference 1991 SCCM/ESICM/ACCP/ATS/SIS International Sepsis Definitions Conference
R2R: Severe sepsis/septic shock Surat Tongyoo Critical care medicine Siriraj Hospital Diagnostic criteria ACCP/SCCM consensus conference 1991 SCCM/ESICM/ACCP/ATS/SIS International Sepsis Definitions Conference
PEEP recruitment maneuver
 Robert M. Rodriguez, MD FAAEM Clinical Professor of Medicine and Emergency Medicine, UCSF Case 1: 40 yo Male restrained driver high speed MVA P 140, RR 40 labored, BP 100/70, O 2 sat 70 Chest wheeze, crackles
Robert M. Rodriguez, MD FAAEM Clinical Professor of Medicine and Emergency Medicine, UCSF Case 1: 40 yo Male restrained driver high speed MVA P 140, RR 40 labored, BP 100/70, O 2 sat 70 Chest wheeze, crackles
BC Sepsis Network Emergency Department Sepsis Guidelines
 The provincial Sepsis Clinical Expert Group developed the BC, taking into account the most up-to-date literature (references below) and expert opinion. For more information about the guidelines, and to
The provincial Sepsis Clinical Expert Group developed the BC, taking into account the most up-to-date literature (references below) and expert opinion. For more information about the guidelines, and to
Sepsis and septic shock: can we win the battle against this hidden crisis?
 REVIEW ARTICLE Sepsis and septic shock: can we win the battle against this hidden crisis? V.G. Dassanayake Department of Surgery, Faculty of Medicine, University of Colombo, Sri Lanka Key words : Sepsis;
REVIEW ARTICLE Sepsis and septic shock: can we win the battle against this hidden crisis? V.G. Dassanayake Department of Surgery, Faculty of Medicine, University of Colombo, Sri Lanka Key words : Sepsis;
Sepsis: Update on Diagnosis, Evaluation and Management
 Sepsis: Epidemiology Sepsis: Update on Diagnosis, Evaluation and Management Michael J. Apostolakos, MD Professor of Medicine Director of Adult Critical Care University of Rochester ~ 750,000 cases per
Sepsis: Epidemiology Sepsis: Update on Diagnosis, Evaluation and Management Michael J. Apostolakos, MD Professor of Medicine Director of Adult Critical Care University of Rochester ~ 750,000 cases per
Case year old female nursing home resident with a hx CAD, PUD, recent hip fracture Transferred to ED with decreased mental status BP in ED 80/50
 Case 1 65 year old female nursing home resident with a hx CAD, PUD, recent hip fracture Transferred to ED with decreased mental status BP in ED 80/50 Case 1 65 year old female nursing home resident with
Case 1 65 year old female nursing home resident with a hx CAD, PUD, recent hip fracture Transferred to ED with decreased mental status BP in ED 80/50 Case 1 65 year old female nursing home resident with
Vasopressors for shock
 Vasopressors for shock Background Reviews and Observational Studies Holler 2015. Nontraumatic Hypotension and Shock in the Emergency Department and Prehospital Setting Prevalence, Etiology and Mortality:
Vasopressors for shock Background Reviews and Observational Studies Holler 2015. Nontraumatic Hypotension and Shock in the Emergency Department and Prehospital Setting Prevalence, Etiology and Mortality:
Vasopressors in Septic Shock. Keith R. Walley, MD St. Paul s Hospital University of British Columbia Vancouver, Canada
 Vasopressors in Septic Shock Keith R. Walley, MD St. Paul s Hospital University of British Columbia Vancouver, Canada Echocardiogram: EF=25% 57 y.o. female, pneumonia, shock Echocardiogram: EF=25% 57 y.o.
Vasopressors in Septic Shock Keith R. Walley, MD St. Paul s Hospital University of British Columbia Vancouver, Canada Echocardiogram: EF=25% 57 y.o. female, pneumonia, shock Echocardiogram: EF=25% 57 y.o.
Critical Care Treatment Guidelines
 Critical Care Treatment Guidelines West Virginia Office of Emergency Medical Services CCT Guidelines CCT Guidelines TABLE OF CONTENTS Preface Acknowledgments Using the Guidelines INITIAL TREATMENT / UNIVERSAL
Critical Care Treatment Guidelines West Virginia Office of Emergency Medical Services CCT Guidelines CCT Guidelines TABLE OF CONTENTS Preface Acknowledgments Using the Guidelines INITIAL TREATMENT / UNIVERSAL
FLUID RESUSCITATION AND MONITORING IN SEPSIS PROTOCOLIZED VS USUAL CARE DEEPA BANGALORE GOTUR MD, FCCP ASSISTANT PROFESSOR, WEILL CORNELL MEDICAL
 FLUID RESUSCITATION AND MONITORING IN SEPSIS PROTOCOLIZED VS USUAL CARE DEEPA BANGALORE GOTUR MD, FCCP ASSISTANT PROFESSOR, WEILL CORNELL MEDICAL COLLEGE NOVEMBER 10 TH 2017 TEXAS SCCM SYMPOSIUM Disclosures
FLUID RESUSCITATION AND MONITORING IN SEPSIS PROTOCOLIZED VS USUAL CARE DEEPA BANGALORE GOTUR MD, FCCP ASSISTANT PROFESSOR, WEILL CORNELL MEDICAL COLLEGE NOVEMBER 10 TH 2017 TEXAS SCCM SYMPOSIUM Disclosures
SEPSIS AND SEPTIC SHOCK INTERNATIONAL GUIDLINES 2016
 SEPSIS AND SEPTIC SHOCK INTERNATIONAL GUIDLINES 2016 Sepsis is defined as organ dysfunction due to excessive reaction to infection It is a consequence of sepsis Needs vasoactive drug administration for
SEPSIS AND SEPTIC SHOCK INTERNATIONAL GUIDLINES 2016 Sepsis is defined as organ dysfunction due to excessive reaction to infection It is a consequence of sepsis Needs vasoactive drug administration for
Should Roids Be the Rage in Septic Shock? Lauren Powell, MSN, RN, CCRN, AGACNP-BC CHI Baylor St. Luke s Medical Center, Houston, TX
 Should Roids Be the Rage in Septic Shock? Lauren Powell, MSN, RN, CCRN, AGACNP-BC CHI Baylor St. Luke s Medical Center, Houston, TX Learning Objectives 1. Review the mechanism of action for the use of
Should Roids Be the Rage in Septic Shock? Lauren Powell, MSN, RN, CCRN, AGACNP-BC CHI Baylor St. Luke s Medical Center, Houston, TX Learning Objectives 1. Review the mechanism of action for the use of
Introduction. Invasive Hemodynamic Monitoring. Determinants of Cardiovascular Function. Cardiovascular System. Hemodynamic Monitoring
 Introduction Invasive Hemodynamic Monitoring Audis Bethea, Pharm.D. Assistant Professor Therapeutics IV January 21, 2004 Hemodynamic monitoring is necessary to assess and manage shock Information obtained
Introduction Invasive Hemodynamic Monitoring Audis Bethea, Pharm.D. Assistant Professor Therapeutics IV January 21, 2004 Hemodynamic monitoring is necessary to assess and manage shock Information obtained
Fluid balance and clinically relevant outcomes
 Fluid balance and clinically relevant outcomes Rui Moreno, MD, PhD, Professor UCINC, Hospital de São José Centro Hospitalar de Lisboa Central, E.P.E. INSULT PRIMARY MODS SIRS SECONDARY MODS OUTCOME RECOVERY
Fluid balance and clinically relevant outcomes Rui Moreno, MD, PhD, Professor UCINC, Hospital de São José Centro Hospitalar de Lisboa Central, E.P.E. INSULT PRIMARY MODS SIRS SECONDARY MODS OUTCOME RECOVERY
Presented by: Indah Dwi Pratiwi
 Presented by: Indah Dwi Pratiwi Normal Fluid Requirements Resuscitation Fluids Goals of Resuscitation Maintain normal body temperature In most cases, elevate the feet and legs above the level of the heart
Presented by: Indah Dwi Pratiwi Normal Fluid Requirements Resuscitation Fluids Goals of Resuscitation Maintain normal body temperature In most cases, elevate the feet and legs above the level of the heart
Advancements in Sepsis
 Objectives Advancements in Sepsis Brian Gilbert, PharmD PGY-1 Pharmacy Resident Jackson Memorial Hospital 3/13/2016 www.fshp.org Pharmacist objectives Review recent updates in resuscitation strategies
Objectives Advancements in Sepsis Brian Gilbert, PharmD PGY-1 Pharmacy Resident Jackson Memorial Hospital 3/13/2016 www.fshp.org Pharmacist objectives Review recent updates in resuscitation strategies
Current State of Pediatric Sepsis. Jason Clayton, MD PhD Pediatric Critical Care 9/19/2018
 Current State of Pediatric Sepsis Jason Clayton, MD PhD Pediatric Critical Care 9/19/2018 Objectives Review the history of pediatric sepsis Review the current definition of pediatric sepsis Review triage
Current State of Pediatric Sepsis Jason Clayton, MD PhD Pediatric Critical Care 9/19/2018 Objectives Review the history of pediatric sepsis Review the current definition of pediatric sepsis Review triage
Nurse Driven Fluid Optimization Using Dynamic Assessments
 Nurse Driven Fluid Optimization Using Dynamic Assessments 2016 1 WHAT WE BELIEVE We believe that clinicians make vital fluid and drug decisions every day with limited and inconclusive information Cheetah
Nurse Driven Fluid Optimization Using Dynamic Assessments 2016 1 WHAT WE BELIEVE We believe that clinicians make vital fluid and drug decisions every day with limited and inconclusive information Cheetah
Patient Safety Safe Table Webcast: Sepsis (Part III and IV) December 17, 2014
 December 17, 2014") Patient Safety Safe Table Webcast: Sepsis (Part III and IV) December 17, 2014 Presenters Mark Blaney, RN Regional Nurse Educator CHI Franciscan Health Karen Lautermilch Director, Quality & Performance
Patient Safety Safe Table Webcast: Sepsis (Part III and IV) December 17, 2014 Presenters Mark Blaney, RN Regional Nurse Educator CHI Franciscan Health Karen Lautermilch Director, Quality & Performance
Ventilatory Management of ARDS. Alexei Ortiz Milan; MD, MSc
 Ventilatory Management of ARDS Alexei Ortiz Milan; MD, MSc 2017 Outline Ventilatory management of ARDS Protected Ventilatory Strategy Use of NMB Selection of PEEP Driving pressure Lung Recruitment Prone
Ventilatory Management of ARDS Alexei Ortiz Milan; MD, MSc 2017 Outline Ventilatory management of ARDS Protected Ventilatory Strategy Use of NMB Selection of PEEP Driving pressure Lung Recruitment Prone
Oxygenation Failure. Increase FiO2. Titrate end-expiratory pressure. Adjust duty cycle to increase MAP. Patient Positioning. Inhaled Vasodilators
 Oxygenation Failure Increase FiO2 Titrate end-expiratory pressure Adjust duty cycle to increase MAP Patient Positioning Inhaled Vasodilators Extracorporeal Circulation ARDS Radiology Increasing Intensity
Oxygenation Failure Increase FiO2 Titrate end-expiratory pressure Adjust duty cycle to increase MAP Patient Positioning Inhaled Vasodilators Extracorporeal Circulation ARDS Radiology Increasing Intensity
towards early goal directed therapy
 Paediatric Septic Shock- towards early goal directed therapy Elliot Long Paediatric Acute Care 2011 Conference Outline Emergency Department Rivers Protocol (EGDT) ACCM Sepsis Protocol Evidence Barriers
Paediatric Septic Shock- towards early goal directed therapy Elliot Long Paediatric Acute Care 2011 Conference Outline Emergency Department Rivers Protocol (EGDT) ACCM Sepsis Protocol Evidence Barriers
Vasopressors in septic shock
 Vasopressors in septic shock Prof. Jean-Louis TEBOUL Medical ICU Bicetre hospital University Paris-South France Questions 1- Why do we use vasopressors in septic shock? 2- Which first-line agent? 3- When
Vasopressors in septic shock Prof. Jean-Louis TEBOUL Medical ICU Bicetre hospital University Paris-South France Questions 1- Why do we use vasopressors in septic shock? 2- Which first-line agent? 3- When
Full Disclosure. The case for why it matters. Goal-directed Fluid Resuscitation
 Goal-directed Fluid Resuscitation Christopher G. Choukalas, MD, MS Department of Anesthesia and Perioperative Care University of California, San Francisco I own no stocks Full Disclosure The case for why
Goal-directed Fluid Resuscitation Christopher G. Choukalas, MD, MS Department of Anesthesia and Perioperative Care University of California, San Francisco I own no stocks Full Disclosure The case for why