hyperlipidemia in CKD DR MOJGAN MORTAZAVI ASSOCIATE PROFESSOR OF NEPHROLOGY ISFAHAN KIDNEY DISEASES RESEARCH CENTER
|
|
|
- Ralph McGee
- 5 years ago
- Views:
Transcription


1 Management of hyperlipidemia in CKD DR MOJGAN MORTAZAVI ASSOCIATE PROFESSOR OF NEPHROLOGY ISFAHAN KIDNEY DISEASES RESEARCH CENTER
2
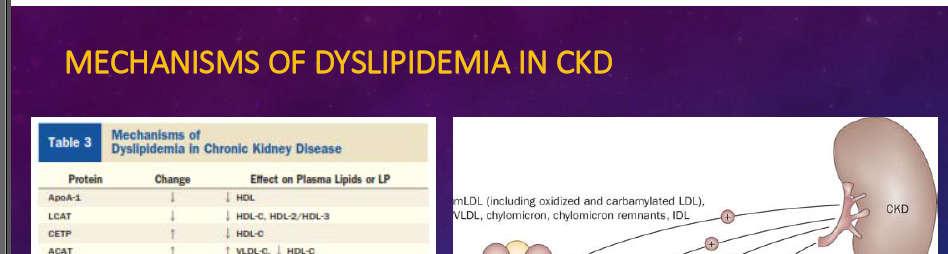
3 Background on Dyslipidemia in CKD In advanced chronic kidney disease (CKD), the lipid profile is characterized by the following: Markedly elevated triglycerides and triglyceriderich apob-containing lipoproteins Decreased HDL-cholesterol (HDL-C) Minimal to no change in LDL-cholesterol (LDL-C) This profile has been linked to high incidence of cardiovascular (CV) morbidity and mortality Adapted from Attman PO, et al: Curr Opin Lipidol 2009; 20(4):293-9.

4 Am J Kidney Dis I-IV, S1-91
5 The major determinants of dyslipidemia in CKD patients GFR, The presence of diabetes mellitus, Severity of proteinuria, Use of immunosuppressive agents, Method of renal replacement, Comorbidity Nutritional status
6 Management of hyperlipidemia in CKD

7
8 Recommendations for Monitoring Dyslipidemia in CKD Lipid profiles should be measured after an overnight fast (ideally 12 h duration) Total cholesterol, LDL-C, HDL-C and triglycerides should be measured Fasting lipid profiles should be measured no sooner than 6 weeks after initiation or change in pharmacologic therapy Thereafter, lipid profiles should be monitored every 6 12 months if the results could influence subsequent therapeutic decisions Adapted from Levin A, et al: CMAJ 2008; 179(11):
9 Recommendations for Monitoring for Adverse Effects of Medication Serial monitoring of creatinine kinase and alanine aminotransferase: Not required for asymptomatic patients with CKD taking a low to moderate dose of statin ( 20 mg/d of simvastatin or atorvastatin, or an equivalent dose of another statin) Should be measured every 3 months for patients with stage 4 CKD who are taking a moderate to high dose of statin ( 40 mg/d of simvastatin or atorvastatin, or an equivalent dose of another statin) A statin and fibrate should not be coadministered to patients with stage 4 CKD because of the risk of rhabdomyolysis Adapted from Levin A, et al: CMAJ 2008; 179(11):
10 Treatment
11
12 Evidence for Lipid-lowering Therapy in CKD: Subgroup Analyses of Major Trials Study n Results Comments Pravastatin pooling project 4491 patients with egfr ml/min Pravastatin reduced risk of composite endpoint (time to MI, coronary death or revascularization; HR 0.77) Suggested benefit in secondary prevention setting Heart Protection Study 375 patients with serum creatinine mg/dl (women), mg/dl (men) Simvastatin reduced risk of first major vascular event (HR 0.70) Supports benefit of treatment with statins in relatively mild CKD ASCOT-LLA 6517 hypertensive adults with undefined "renal dysfunction" Atorvastatin lowered the risk of nonfatal MI and fatal CHD (HR 0.61) Further supports a role for statins in relatively mild CKD Adapted from Nogueira J, et al: Clin J Am Soc Nephrol 2007; 2(4):
13 Updated Recommendations for Lipid-lowering Therapy in CKD It is advisable to aggressively treat individuals who have an egfr of 30 to 60 ml/min/1.73 m 2 and have known CHD. Adapted from Nogueira J, et al: Clin J Am Soc Nephrol 2007; 2(4):
14 Updated Recommendations for Lipid-lowering Therapy in CKD It may be advisable to treat those with high risk for atherosclerotic cardiac events regardless of initial LDL level to achieve a marked (at least 30 to 40%) reduction in LDL A lower goal LDL of 70 mg/dl may be a reasonable therapeutic option in patients with CKD The increase in mortality in hemodialysis patients at lower cholesterol levels demands caution within this population Adapted from Nogueira J, et al: Clin J Am Soc Nephrol 2007; 2(4):
15
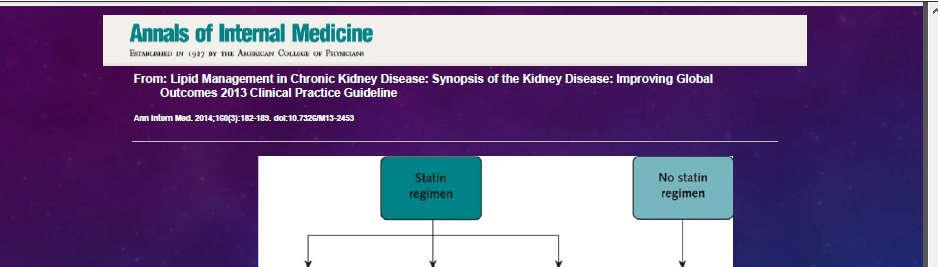
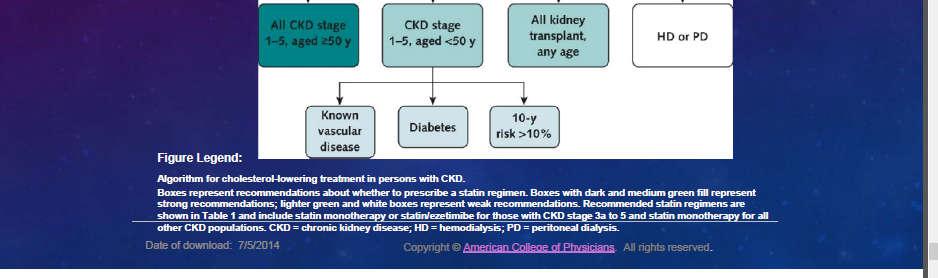
16 KDIGO Clinical Practice Guideline for Lipid Management in Chronic Kidney Disease In adults aged 50 years with egfr <60 ml/min/1.73 m² but not treated with chronic dialysis or kidney transplantation (GFR categories G3a-G5),is recommended treatment with a statin or statin/ezetimibe combination. (1A) Kidney International Supplements (2013) 3, 260-
17 Guideline for Lipid Management in Chronic Kidney Disease In adults aged years with CKD but not treated with chronic dialysis or kidney transplantation, is suggested statin treatment in people with one or more of the following (2A): Known coronary disease (myocardial infarction or coronary revascularization) Diabetes mellitus Prior ischemic stroke Estimated 10-year incidence of coronary death or non-fatal myocardial infarction >10%
18 KDIGO Clinical Practice Guideline for Lipid Management in Chronic Kidney Disease In adults with dialysis-dependent CKD, is suggested that statins or statin/ezetimibe combination not be initiated. (2A) In patients already receiving statins or statin/ezetimibe combination at the time of dialysis initiation, is suggested that these agents be continued. (2C) In adult kidney transplant recipients, is suggested treatment with a statin. (2B) Kidney International Supplements (2013) 3, 260-
19
20 Pharmacotherapy and Dosing of Statins in Adults With CKD adults 50 years In more advanced stages of CKD (Stage 3-5, egfr <60 ml/min/1.73 m 2 ) more than 50 years old, treatment with combination statin plus ezetimibe is recommended
21 Pharmacotherapy and Dosing of Statins in Adults With Stage 1 or 2 CKD (egfr >60 ml/min/1.73 m 2 Since drug toxicity is less of a concern with better renal excretion, those with Stage 1 or 2 CKD (egfr >60 ml/min/1.73 m 2 ) can be treated in the same way as the general population.
22 Baseline transaminase levels should be measured in all CKD patients prior to starting statin therapy, though routine transaminase for CK levels is not recommended in the absence of clinical evidence of hepatotoxicity or myopathy.
23
24 Why Aren't Statins Powerfully Effective in Stage 4 CKD? Statins are not very effective in reducing triglyceride-rich apob- and apoc-containing lipoproteins This is the major lipoprotein abnormality of advanced renal failure We should therefore not expect statins to significantly attenuate renal dyslipidemia in advanced CKD Adapted from Attman PO, et al: Curr Opin Lipidol 2009; 20(4):293-9.
25 Risk Reduction with Statins in Renal Dyslipidemia GFR 100 Cardiovascular risk reduction by statins? Renoprotection by statins? 50 Adapted from Attman PO, et al: Curr Opin Lipidol 2009; 20(4):293-9.
26 Study of Heart and Renal Protection (SHARP) BAIGENT C, ET AL: KIDNEY INT SUPPL 2003; (84):S
27 What Do We Know About the Impact of LDL-lowering in CKD? LDL may not play as large a role in mediating CV risk in CKD as it does in the general population Adapted from Baigent C, et al: Kidney Int Suppl 2003; (84):S
28 The Study of Heart and Renal Protection (SHARP) Objectives: To assess the effects of lowering cholesterol on major vascular events and on the rate of progression to ESRD among patients with CKD Subjects: ~9,000 patients with CKD (6,000 pre-dialysis, 3,000 on dialysis) Interventions: Simvastatin / ezetimibe combination vs. placebo Assessments: Effect of LDL lowering on time to first vascular event (primary) Effect of treatment on progression to ESRD Effect of treatment on various mortality and morbidity endpoint Adapted from Baigent C, et al: Kidney Int Suppl 2003; (84):S
29 Association Between Cholesterol and CV Mortality 100 General population 100 Hemodialysis patients CV mortality, % pe er annum 10 Non-diabetic Diabetic Total mortality, % pe er annum Total cholesterol, mmol/l Total cholesterol, mmol/l Adapted from Baigent C, et al: Kidney Int Suppl 2003; (84):S
 ~75%: Other causes")

30 Causes of CV Mortality in CKD ~25%: Directly attributable to MI (potentially avoidable with cholesterol reduction) ~75%: Other causes (cardiac arrest, arrhythmia, heart failure) Not as dependent on cholesterol reduction Adapted from Baigent C, et al: Kidney Int Suppl 2003; (84):S
31 2011
32 Conclusion Rosuvastatin administration reduced albuminuria, serum cystatin C levels, and inflammation, and improved lipid profiles, regardless of the presence or absence of DM, and the degree of the egfr.
33 Rosuvastatin Rosuvastatin is a high potency, efficacious and generally welltolerated statin indicated for the management of a variety of dyslipidemic states. It is the most effective statin currently available for reducing LDL-C and non-hdl-c and increasing HDLC. It has been shown to be safe and efficacious in women, and children with heterozygous familial hypercholesterolemia. Expert Opin. Drug Saf. (2011) 10(6)
34 Rosuvastatin The adverse event rate of rosuvastatin is comparable to other statins. Unlike statins that depend on CYP450 3A4 for metabolism, rosuvastatin has low risk for interacting with azole antifungal medications, macrolide antibiotics, calcium channel blockers (verapamil, diltiazem) and other drugs. Expert Opin. Drug Saf. (2011) 10(6)
35 Nephrotoxicity and proteinuria?? Rosuvastatin drew controversy because its use was associated with proteinuria in some patients. This was subsequently shown to be due to increased tubular secretion of low molecular weight proteins which was neither associated with nor promoted glomerulotoxicity or nephrotoxicity. The FDA subsequently agreed that rosuvastatin within its approved dosage range of 5-40 mg/ day did not induce renal toxicity. Expert Opin. Drug Saf. (2011) 10(6)


36 N.D. Vaziri, Division of Nephrology and Hypertension, University of California, Irvine Medical Center
37
38
39 Ezetimibe Treatment in Hypercholesterolemic Kidney Transplant Patients is Safe and Effective and Reduces the Decline of Renal Allograft Function: a Pilot Study TÜRK TR, ET AL: NEPHROL DIAL TRANSPLANT 2008; 23(1):
40 Ezetimibe in Hypercholesterolemic Kidney Transplant Patients Objective: To prospectively investigate the effect of ezetimibe on renal function in kidney transplant recipients Subjects: 56 patients with statin-resistant hypercholesterolemia (total cholesterol >200 mg/dl) after renal transplantation Methodology: Study patients received additional ezetimibe therapy (10 mg/day) for 12 months (n=56) A group receiving statin therapy (n=28) alone served as controls Investigators assessed changes in total cholesterol and LDL-C concentrations, as well as in creatinine clearance. Türk TR, et al: Nephrol Dial Transplant 2008; 23(1):
41 Changes in Total Cholesterol: Statin ± Ezetimibe in Kidney Transplant Patients mg/dl 0-10 Control Ezetimibe treated -20 p= Months Adapted from Türk TR, et al: Nephrol Dial Transplant 2008; 23(1):
42 Changes in LDL-C: Statin ± Ezetimibe in Kidney Transplant Patients 0 mg/dl Control Ezetimibe treated -30 p= Months Adapted from Türk TR, et al: Nephrol Dial Transplant 2008; 23(1):
43 Changes in Creatinine Clearance: Statin ± Ezetimibe in Kidney Transplant Patients mg/dl (Cockcroft-Gault formula) Control Ezetimibe treated Months p=0.025 mg/dl/1.73m (MDRD equation) Control Ezetimibe treated Months p=0.033 Adapted from Türk TR, et al: Nephrol Dial Transplant 2008; 23(1):
44 Other Observations with Ezetimibe in Kidney Transplant Patients The investigators reported that: Ezetimibe therapy was nearly without side effects in this population Ezetimibe s positive effects on endothelial function may be an explanation for the drug s positive effects on renal function Previous studies have indicated a direct positive effect of ezetimibe on endothelial function Adapted from Türk TR, et al: Nephrol Dial Transplant 2008; 23(1):
45 Other drugs Sevelamer L-carnitine
46 Elder et al., A meta-analysis of randomized controlled trials comparing Sevelamer vs CBBs Results All cause mortality (sevelamer vs CBBs) 13 studies, n=3799; significantly lower(46% reduction) in Sevelamer Group RR 0.54, 95% CI Cardiovascular mortality (sevelamer vs CBBs) 4 studies showed n=2712; RR 0.33, 95% CI Pleiotropic effects Total cholesterol Sevelamer significantly lower versus CBB recipients (MD mg/dl, 95% CI to mg/dl when pooled 14 studies (n=2039). Low-density lipoprotein cholesterol Sevelamer significantly lower versus CBBs, based on 12 studies(n=1171; MD mg/dl, 95% CI to mg/dl
47 Elder et al., A meta-analysis of randomized controlled trials comparing Sevelamer vs CBBs Conclusion Studies published from March of 2009 to March 31, 2015 were searched in PubMed and the Cochrane Central Register of Controlled Trials This meta-analysis, combining 25 studies and 4770 participants, shows a 46% reduction in all cause mortality risk for sevelamer. Sevelamer was also associated with lower serum Ca, higher ipth, lower total and LDL-C, a reduced risk of hypercalcemia versus CBBs, and a marginally increased risk of combined gastrointestinal adverse events.


48
49 Triglyceridelowering treatment in adults
50
51 In adults with CKD (including those treated with chronic dialysis or kidney transplantation) and hypertriglyceridemia, we suggest that therapeutic lifestyle changes(tlc) be advised
52 Non-pharmacological treatment of high triglycerides TLC( therapeutic lifestyle changes): Dietary modification, Weight reduction, Increased physical activity, Reducing alcohol intake, Treatment of hyperglycemia (if present).
53 Dietary changes that may reduce serum TGs: low-fat diet (o15% total calories), reduction of monosaccharide and disaccharide intake reducing the total amount of dietar carbohydrates reducing the total amount of dietar carbohydrates and use of fish oils to replace some long-chain TGs
54 Pharmacological treatment of high triglycerides: effects on risk of pancreatitis Fibric acid derivatives could be considered for the rare patients with CKD and markedly elevated fasting levels of serum TG (411.3 mmol/l [>1000 mg/dl]). If such therapy is prescribed, fibric acid derivatives must be dose-adjusted for kidney function.
55 Which fibric acid derivative is better? There is limited evidence to recommend one fibric acid derivative over another in the setting of CKD and therefore any of the alternatives may be used
56 Nicotinic acid has not been well studied in advanced CKD and therefore is not recommended for treatment of severe hypertriglyceridemia, given the risk of toxicity (especially flushing and hyperglycemia).
57
58 Fenofibrate and the kidney: an overview Clinicians should be cautious when fenofibrate is coadministered with antihypertensive drugs that affect renal hemodynamics. Fenofibrate may reduce vasodilatation of the afferent arteriole, thus decreasing glomerular capillary pressure and perfusion of the kidneys If this effect is combined with the vasodilatory actions of ACEi on the efferent arteriole, glomerula pressure might be further reduced resulting in prerenal azotemia.
59 Fenofibrate and the kidney: an overview Another important issue is that the nephrotoxic effect of fenofibrate might be dose dependent This may be associated with the accumulation of its active metabolite fenofibric acid Inappropriate use of fenofibrate in patients with impaired renal function (creatinine clearance < 50 ml/min) can result nephrotoxicity
60 Fenofibrate and the kidney: an overview increases in SCr levels are transient and reversible even without treatment discontinuation, fenofibrate can limit proteinuria, which is an independent risk factor for both CV events and CKD, fenofibrate was associated with long-term benefits on renal function. However, a close monitoring of SCr levels is relevant especially in high-risk patients. Increases in SCr levels 30% can impose treatment discontinuation.
61 Risk predictors of raising serum Cr level increased aged impaired renal function high dose treatment
62
63
64
65
66 summary
67 Alterations in Lipid Profiles in CKD Generally Increased Levels Generally Decreased Levels Triglycerids Lipoprotein(a) Apoprotein B VLDL-C IDL-C Total cholesterol LDL-C HDL-C Apoprotein A1 Adapted from Nogueira J, et al: Clin J Am Soc Nephrol 2007; 2(4):
68
69


70 Thanks for your attention
Management of Post-transplant hyperlipidemia
 Management of Post-transplant hyperlipidemia B. Gisella Carranza Leon, MD Assistant Professor of Medicine Lipid Clinic - Vanderbilt Heart and Vascular Institute Division of Diabetes, Endocrinology and
Management of Post-transplant hyperlipidemia B. Gisella Carranza Leon, MD Assistant Professor of Medicine Lipid Clinic - Vanderbilt Heart and Vascular Institute Division of Diabetes, Endocrinology and
Approach to Dyslipidemia among diabetic patients
 Approach to Dyslipidemia among diabetic patients Farzad Hadaegh, MD, Professor of Internal Medicine & Endocrinology Prevention of Metabolic Disorders Research Center, Research Institute for Endocrine Sciences
Approach to Dyslipidemia among diabetic patients Farzad Hadaegh, MD, Professor of Internal Medicine & Endocrinology Prevention of Metabolic Disorders Research Center, Research Institute for Endocrine Sciences
ATP IV: Predicting Guideline Updates
 Disclosures ATP IV: Predicting Guideline Updates Daniel M. Riche, Pharm.D., BCPS, CDE Speaker s Bureau Merck Janssen Boehringer-Ingelheim Learning Objectives Describe at least two evidence-based recommendations
Disclosures ATP IV: Predicting Guideline Updates Daniel M. Riche, Pharm.D., BCPS, CDE Speaker s Bureau Merck Janssen Boehringer-Ingelheim Learning Objectives Describe at least two evidence-based recommendations
Morbidity & Mortality from Chronic Kidney Disease
 Morbidity & Mortality from Chronic Kidney Disease Dr. Lam Man-Fai ( 林萬斐醫生 ) Honorary Clinical Assistant Professor MBBS, MRCP, FHKCP, FHKAM, PDipID (HK), FRCP (Edin, Glasg) Hong Kong Renal Registry Report
Morbidity & Mortality from Chronic Kidney Disease Dr. Lam Man-Fai ( 林萬斐醫生 ) Honorary Clinical Assistant Professor MBBS, MRCP, FHKCP, FHKAM, PDipID (HK), FRCP (Edin, Glasg) Hong Kong Renal Registry Report
Protecting the heart and kidney: implications from the SHARP trial
 Cardiology Update, Davos, 2013: Satellite Symposium Protecting the heart and kidney: implications from the SHARP trial Colin Baigent Professor of Epidemiology CTSU, University of Oxford S1 First CTT cycle:
Cardiology Update, Davos, 2013: Satellite Symposium Protecting the heart and kidney: implications from the SHARP trial Colin Baigent Professor of Epidemiology CTSU, University of Oxford S1 First CTT cycle:
Chapter 2: Pharmacological cholesterol-lowering treatment in adults Kidney International Supplements (2013) 3, ; doi: /kisup.2013.
 3, ; doi: /kisup.2013.") http://www.kidney-international.org chapter & 3 KDIGO Chapter : Pharmacological cholesterol-lowering treatment in adults Kidney International Supplements (3) 3, 7 79; doi:.38/kisup.3.34 INTRODUCTION Therapeutic
http://www.kidney-international.org chapter & 3 KDIGO Chapter : Pharmacological cholesterol-lowering treatment in adults Kidney International Supplements (3) 3, 7 79; doi:.38/kisup.3.34 INTRODUCTION Therapeutic
The CARI Guidelines Caring for Australians with Renal Impairment. Cardiovascular Risk Factors
 Cardiovascular Risk Factors ROB WALKER (Dunedin, New Zealand) Lipid-lowering therapy in patients with chronic kidney disease Date written: January 2005 Final submission: August 2005 Author: Rob Walker
Cardiovascular Risk Factors ROB WALKER (Dunedin, New Zealand) Lipid-lowering therapy in patients with chronic kidney disease Date written: January 2005 Final submission: August 2005 Author: Rob Walker
Cardiovascular Pharmacotherapy in Special Population: Cardio-Nephrology
 49 th Annual Scientific Meeting The Heart Association of Thailand under the Royal Patronage of H.M. the King Cardiology on the move 24-25 March 2017 @Sheraton, HuaHin Cardiovascular Pharmacotherapy in
49 th Annual Scientific Meeting The Heart Association of Thailand under the Royal Patronage of H.M. the King Cardiology on the move 24-25 March 2017 @Sheraton, HuaHin Cardiovascular Pharmacotherapy in
How would you manage Ms. Gold
 How would you manage Ms. Gold 32 yo Asian woman with dyslipidemia Current medications: Simvastatin 20mg QD Most recent lipid profile: TC = 246, TG = 100, LDL = 176, HDL = 50 What about Mr. Williams? 56
How would you manage Ms. Gold 32 yo Asian woman with dyslipidemia Current medications: Simvastatin 20mg QD Most recent lipid profile: TC = 246, TG = 100, LDL = 176, HDL = 50 What about Mr. Williams? 56
New Guidelines in Dyslipidemia Management
 The Fourth IAS-OSLA Course on Lipid Metabolism and Cardiovascular Risk Muscat, Oman, February 2018 New Guidelines in Dyslipidemia Management Dr. Khalid Al-Waili, MD, FRCPC, DABCL Senior Consultant Medical
The Fourth IAS-OSLA Course on Lipid Metabolism and Cardiovascular Risk Muscat, Oman, February 2018 New Guidelines in Dyslipidemia Management Dr. Khalid Al-Waili, MD, FRCPC, DABCL Senior Consultant Medical
PIEDMONT ACCESS TO HEALTH SERVICES, INC. Guidelines for Screening and Management of Dyslipidemia
 PIEDMONT ACCESS TO HEALTH SERVICES, INC. Policy Number: 01-09-021 SUBJECT: Guidelines for Screening and Management of Dyslipidemia EFFECTIVE DATE: 04/2008 REVIEWED/REVISED: 04/12/10, 03/17/2011, 4/10/2012,
PIEDMONT ACCESS TO HEALTH SERVICES, INC. Policy Number: 01-09-021 SUBJECT: Guidelines for Screening and Management of Dyslipidemia EFFECTIVE DATE: 04/2008 REVIEWED/REVISED: 04/12/10, 03/17/2011, 4/10/2012,
During the past several decades, the advent and refinement
 In-Depth Review The Unique Character of Cardiovascular Disease in Chronic Kidney Disease and Its Implications for Treatment with Lipid-Lowering Drugs Joseph Nogueira and Matthew Weir Department of Medicine,
In-Depth Review The Unique Character of Cardiovascular Disease in Chronic Kidney Disease and Its Implications for Treatment with Lipid-Lowering Drugs Joseph Nogueira and Matthew Weir Department of Medicine,
Dyslipidemia in the light of Current Guidelines - Do we change our Practice?
 Dyslipidemia in the light of Current Guidelines - Do we change our Practice? Dato Dr. David Chew Soon Ping Senior Consultant Cardiologist Institut Jantung Negara Atherosclerotic Cardiovascular Disease
Dyslipidemia in the light of Current Guidelines - Do we change our Practice? Dato Dr. David Chew Soon Ping Senior Consultant Cardiologist Institut Jantung Negara Atherosclerotic Cardiovascular Disease
New Guidelines in Dyslipidemia Management
 The Third IAS-OSLA Course on Lipid Metabolism and Cardiovascular Risk Muscat, Oman, February 2017 New Guidelines in Dyslipidemia Management Dr. Khalid Al-Waili, MD, FRCPC, DABCL Senior Consultant Medical
The Third IAS-OSLA Course on Lipid Metabolism and Cardiovascular Risk Muscat, Oman, February 2017 New Guidelines in Dyslipidemia Management Dr. Khalid Al-Waili, MD, FRCPC, DABCL Senior Consultant Medical
Conflict of Interest Disclosure. Learning Objectives. Learning Objectives. Guidelines. Update on Lifestyle Guidelines
 Conflict of Interest Disclosure Updates for the Ambulatory Care Pharmacist: Dyslipidemia and CV Risk Assessment No conflicts of interest to disclose 2014 Updates to the Updates in Ambulatory Care Pharmacy
Conflict of Interest Disclosure Updates for the Ambulatory Care Pharmacist: Dyslipidemia and CV Risk Assessment No conflicts of interest to disclose 2014 Updates to the Updates in Ambulatory Care Pharmacy
Review of guidelines for management of dyslipidemia in diabetic patients
 2012 international Conference on Diabetes and metabolism (ICDM) Review of guidelines for management of dyslipidemia in diabetic patients Nan Hee Kim, MD, PhD Department of Internal Medicine, Korea University
2012 international Conference on Diabetes and metabolism (ICDM) Review of guidelines for management of dyslipidemia in diabetic patients Nan Hee Kim, MD, PhD Department of Internal Medicine, Korea University
Royal Wolverhampton Hospital Adult Lipid Lowering Therapy Guidelines Lipid Lowering Therapy for the Prevention of Cardiovascular Disease
 Royal Wolverhampton Hospital Adult Lipid Lowering Therapy Guidelines 1 This guideline is intended to assist rational and cost-effective prescribing of lipid regulating medications across both primary and
Royal Wolverhampton Hospital Adult Lipid Lowering Therapy Guidelines 1 This guideline is intended to assist rational and cost-effective prescribing of lipid regulating medications across both primary and
Cardiovascular Complications of Diabetes
 VBWG Cardiovascular Complications of Diabetes Nicola Abate, M.D., F.N.L.A. Professor and Chief Division of Endocrinology and Metabolism The University of Texas Medical Branch Galveston, Texas Coronary
VBWG Cardiovascular Complications of Diabetes Nicola Abate, M.D., F.N.L.A. Professor and Chief Division of Endocrinology and Metabolism The University of Texas Medical Branch Galveston, Texas Coronary
Long-Term Complications of Diabetes Mellitus Macrovascular Complication
 Long-Term Complications of Diabetes Mellitus Macrovascular Complication Sung Hee Choi MD, PhD Professor, Seoul National University College of Medicine, SNUBH, Bundang Hospital Diabetes = CVD equivalent
Long-Term Complications of Diabetes Mellitus Macrovascular Complication Sung Hee Choi MD, PhD Professor, Seoul National University College of Medicine, SNUBH, Bundang Hospital Diabetes = CVD equivalent
ABCD and Renal Association Clinical Guidelines for Diabetic Nephropathy-CKD. Management of Dyslipidaemia and Hypertension in Adults Dr Peter Winocour
 ABCD and Renal Association Clinical Guidelines for Diabetic Nephropathy-CKD. Management of Dyslipidaemia and Hypertension in Adults Dr Peter Winocour Dr Indranil Dasgupta Rationale No national practical
ABCD and Renal Association Clinical Guidelines for Diabetic Nephropathy-CKD. Management of Dyslipidaemia and Hypertension in Adults Dr Peter Winocour Dr Indranil Dasgupta Rationale No national practical
MOLINA HEALTHCARE OF CALIFORNIA
 MOLINA HEALTHCARE OF CALIFORNIA HIGH BLOOD CHOLESTEROL IN ADULTS GUIDELINE Molina Healthcare of California has adopted the Third Report of the National Cholesterol Education Program (NCEP) Expert Panel
MOLINA HEALTHCARE OF CALIFORNIA HIGH BLOOD CHOLESTEROL IN ADULTS GUIDELINE Molina Healthcare of California has adopted the Third Report of the National Cholesterol Education Program (NCEP) Expert Panel
Managing Chronic Kidney Disease: Reducing Risk for CKD Progression
 Managing Chronic Kidney Disease: Reducing Risk for CKD Progression Arasu Gopinath, MD Clinical Nephrologist, Medical Director, Jordan Landing Dialysis Center Objectives: Identify the most important risks
Managing Chronic Kidney Disease: Reducing Risk for CKD Progression Arasu Gopinath, MD Clinical Nephrologist, Medical Director, Jordan Landing Dialysis Center Objectives: Identify the most important risks
Drug Class Review HMG-CoA Reductase Inhibitors (Statins) and Fixed-dose Combination Products Containing a Statin
 and Fixed-dose Combination Products Containing a Statin") Drug Class Review HMG-CoA Reductase Inhibitors (Statins) and Fixed-dose Combination Products Containing a Statin Final Report Update 5 November 2009 This report reviews information about the comparative
Drug Class Review HMG-CoA Reductase Inhibitors (Statins) and Fixed-dose Combination Products Containing a Statin Final Report Update 5 November 2009 This report reviews information about the comparative
DYSLIPIDEMIA PHARMACOLOGY. University of Hawai i Hilo Pre- Nursing Program NURS 203 General Pharmacology Danita Narciso Pharm D
 DYSLIPIDEMIA PHARMACOLOGY University of Hawai i Hilo Pre- Nursing Program NURS 203 General Pharmacology Danita Narciso Pharm D 1 LEARNING OBJECTIVES Know normal cholesterol levels Understand what the role
DYSLIPIDEMIA PHARMACOLOGY University of Hawai i Hilo Pre- Nursing Program NURS 203 General Pharmacology Danita Narciso Pharm D 1 LEARNING OBJECTIVES Know normal cholesterol levels Understand what the role
Introduction. Objective. Critical Questions Addressed
 Introduction Objective To provide a strong evidence-based foundation for the treatment of cholesterol for the primary and secondary prevention of ASCVD in women and men Critical Questions Addressed CQ1:
Introduction Objective To provide a strong evidence-based foundation for the treatment of cholesterol for the primary and secondary prevention of ASCVD in women and men Critical Questions Addressed CQ1:
Hyperlipidemia. Prepared by : Muhannad Mohammed Supervisor professor : Dr. Ahmed Yahya Dallalbashi
 Hyperlipidemia Prepared by : Muhannad Mohammed Supervisor professor : Dr. Ahmed Yahya Dallalbashi Outline The story of lipids Definition of hyperlipidemia Classification of hyperlipidemia Causes of hyperlipidemia
Hyperlipidemia Prepared by : Muhannad Mohammed Supervisor professor : Dr. Ahmed Yahya Dallalbashi Outline The story of lipids Definition of hyperlipidemia Classification of hyperlipidemia Causes of hyperlipidemia
Fibrate and cardiovascular disease: Evident from meta-analysis. Thongchai Pratipanawatr
 Fibrate and cardiovascular disease: Evident from meta-analysis Thongchai Pratipanawatr ??? ย คห นใหม ย คห นกลาง ย คห นเก า ?? Statin era? ย คห นใหม ย คห นกลาง ย คห นเก า CURRENT ROLE OF FIBRATE What are
Fibrate and cardiovascular disease: Evident from meta-analysis Thongchai Pratipanawatr ??? ย คห นใหม ย คห นกลาง ย คห นเก า ?? Statin era? ย คห นใหม ย คห นกลาง ย คห นเก า CURRENT ROLE OF FIBRATE What are
Disclosure. No relevant financial relationships. Placebo-Controlled Statin Trials
 MANAGEMENT OF HYPERLIPIDEMIA AND CARDIOVASCULAR RISK IN WOMEN: Balancing Benefits and Harms Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial
MANAGEMENT OF HYPERLIPIDEMIA AND CARDIOVASCULAR RISK IN WOMEN: Balancing Benefits and Harms Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial
Cholesterol Management Roy Gandolfi, MD
 Cholesterol Management 2017 Roy Gandolfi, MD Goals Interpreting cholesterol guidelines Cholesterol treatment in diabetics Statin use and side effects therapy Reporting- Comparison data among physicians
Cholesterol Management 2017 Roy Gandolfi, MD Goals Interpreting cholesterol guidelines Cholesterol treatment in diabetics Statin use and side effects therapy Reporting- Comparison data among physicians
CLINICAL OUTCOME Vs SURROGATE MARKER
 CLINICAL OUTCOME Vs SURROGATE MARKER Statin Real Experience Dr. Mostafa Sherif Senior Medical Manager Pfizer Egypt & Sudan Objective Difference between Clinical outcome and surrogate marker Proper Clinical
CLINICAL OUTCOME Vs SURROGATE MARKER Statin Real Experience Dr. Mostafa Sherif Senior Medical Manager Pfizer Egypt & Sudan Objective Difference between Clinical outcome and surrogate marker Proper Clinical
PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN
 PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest EXPLAINING THE DECREASE
PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest EXPLAINING THE DECREASE
Lipid Therapy: Statins and Beyond. Ivan Anderson, MD RIHVH Cardiology
 Lipid Therapy: Statins and Beyond Ivan Anderson, MD RIHVH Cardiology Outline The cholesterol hypothesis and lipid metabolism The Guidelines 4 Groups that Benefit from Lipid therapy Initiation and monitoring
Lipid Therapy: Statins and Beyond Ivan Anderson, MD RIHVH Cardiology Outline The cholesterol hypothesis and lipid metabolism The Guidelines 4 Groups that Benefit from Lipid therapy Initiation and monitoring
SIGN 149 Risk estimation and the prevention of cardiovascular disease. Quick Reference Guide July Evidence
 SIGN 149 Risk estimation and the prevention of cardiovascular disease Quick Reference Guide July 2017 Evidence ESTIMATING CARDIOVASCULAR RISK R Individuals with the following risk factors should be considered
SIGN 149 Risk estimation and the prevention of cardiovascular disease Quick Reference Guide July 2017 Evidence ESTIMATING CARDIOVASCULAR RISK R Individuals with the following risk factors should be considered
Lipids & Hypertension Update
 Lipids & Hypertension Update No financial disclosures Michael W. Cullen, MD, FACC Senior Associate Consultant, Assistant Professor of Medicine Mayo Clinic Department of Cardiovascular Diseases 34 th Annual
Lipids & Hypertension Update No financial disclosures Michael W. Cullen, MD, FACC Senior Associate Consultant, Assistant Professor of Medicine Mayo Clinic Department of Cardiovascular Diseases 34 th Annual
Non-Statin Lipid-Lowering Agents M Holler - Last updated: 10/2016
 Drug/Class Cholestyramine (Questran) Bile acid sequestrant Generic? Lipid Effects Y/N (monotherapy) Y LDL : 9% (4 g to 8 ; 21% (16 g to 20 ; 23% to 28% (>20 HDL : 4% to 8% (16 to 24 TG : 11% to 28% (4
Drug/Class Cholestyramine (Questran) Bile acid sequestrant Generic? Lipid Effects Y/N (monotherapy) Y LDL : 9% (4 g to 8 ; 21% (16 g to 20 ; 23% to 28% (>20 HDL : 4% to 8% (16 to 24 TG : 11% to 28% (4
2013 ACC AHA LIPID GUIDELINE JAY S. FONTE, MD
 2013 ACC AHA LIPID GUIDELINE JAY S. FONTE, MD How do you interpret my blood test results? What are our targets for these tests? Before the ACC/AHA Lipid Guidelines A1c:
2013 ACC AHA LIPID GUIDELINE JAY S. FONTE, MD How do you interpret my blood test results? What are our targets for these tests? Before the ACC/AHA Lipid Guidelines A1c:
LDL cholesterol and cardiovascular outcomes?
 LDL cholesterol and cardiovascular outcomes? Prof Kausik Ray, BSc (hons), MBChB, FRCP, MD, MPhil (Cantab), FACC, FESC Professor of Cardiovascular Disease Prevention St Georges University of London Honorary
LDL cholesterol and cardiovascular outcomes? Prof Kausik Ray, BSc (hons), MBChB, FRCP, MD, MPhil (Cantab), FACC, FESC Professor of Cardiovascular Disease Prevention St Georges University of London Honorary
Marshall Tulloch-Reid, MD, MPhil, DSc, FACE Epidemiology Research Unit Tropical Medicine Research Institute The University of the West Indies, Mona,
 Marshall Tulloch-Reid, MD, MPhil, DSc, FACE Epidemiology Research Unit Tropical Medicine Research Institute The University of the West Indies, Mona, Jamaica At the end of this presentation the participant
Marshall Tulloch-Reid, MD, MPhil, DSc, FACE Epidemiology Research Unit Tropical Medicine Research Institute The University of the West Indies, Mona, Jamaica At the end of this presentation the participant
REACH Risk Evaluation to Achieve Cardiovascular Health
 Dyslipidemia and transplantation History: An 8-year-old boy presented with generalized edema and hypertension. A renal biopsy confirmed a diagnosis of focal segmental glomerulosclerosis (FSGS). After his
Dyslipidemia and transplantation History: An 8-year-old boy presented with generalized edema and hypertension. A renal biopsy confirmed a diagnosis of focal segmental glomerulosclerosis (FSGS). After his
Financial Disclosures
 1 Lipids in Type 2 Diabetes July 20, 2013 Abhimanyu Garg, M.D. Professor of Internal Medicine Chief, Division of Nutrition and Metabolic Diseases Distinguished Chair in Human Nutrition Research UT Southwestern
1 Lipids in Type 2 Diabetes July 20, 2013 Abhimanyu Garg, M.D. Professor of Internal Medicine Chief, Division of Nutrition and Metabolic Diseases Distinguished Chair in Human Nutrition Research UT Southwestern
HYPERLIPIDEMIA IN THE OLDER POPULATION NICOLE SLATER, PHARMD, BCACP AUBURN UNIVERSITY, HARRISON SCHOOL OF PHARMACY JULY 16, 2016
 HYPERLIPIDEMIA IN THE OLDER POPULATION NICOLE SLATER, PHARMD, BCACP AUBURN UNIVERSITY, HARRISON SCHOOL OF PHARMACY JULY 16, 2016 NOTHING TO DISCLOSE I, Nicole Slater, have no actual or potential conflict
HYPERLIPIDEMIA IN THE OLDER POPULATION NICOLE SLATER, PHARMD, BCACP AUBURN UNIVERSITY, HARRISON SCHOOL OF PHARMACY JULY 16, 2016 NOTHING TO DISCLOSE I, Nicole Slater, have no actual or potential conflict
2013 Cholesterol Guidelines. Anna Broz MSN, RN, CNP, AACC Adult Certified Nurse Practitioner North Ohio Heart, Inc.
 2013 Cholesterol Guidelines Anna Broz MSN, RN, CNP, AACC Adult Certified Nurse Practitioner North Ohio Heart, Inc. Disclosures Speaker Gilead Sciences NHLBI Charge to the Expert Panel Evaluate higher quality
2013 Cholesterol Guidelines Anna Broz MSN, RN, CNP, AACC Adult Certified Nurse Practitioner North Ohio Heart, Inc. Disclosures Speaker Gilead Sciences NHLBI Charge to the Expert Panel Evaluate higher quality
4/7/ The stats on heart disease. + Deaths & Age-Adjusted Death Rates for
 + Update on Lipid Management Stacey Gardiner, MD Assistant Professor Division of Cardiovascular Medicine Medical College of Wisconsin + The stats on heart disease Over the past 10 years for which statistics
+ Update on Lipid Management Stacey Gardiner, MD Assistant Professor Division of Cardiovascular Medicine Medical College of Wisconsin + The stats on heart disease Over the past 10 years for which statistics
Achieving Lipid Goals: 2008 Update. Laura Hansen, Pharm.D. Associate Professor, University of Colorado School of Pharmacy
 Achieving Lipid Goals: 2008 Update Laura Hansen, Pharm.D. Associate Professor, University of Colorado School of Pharmacy Discuss relationship between lipid values and coronary events Evaluate clinical
Achieving Lipid Goals: 2008 Update Laura Hansen, Pharm.D. Associate Professor, University of Colorado School of Pharmacy Discuss relationship between lipid values and coronary events Evaluate clinical
ALLHAT RENAL DISEASE OUTCOMES IN HYPERTENSIVE PATIENTS STRATIFIED INTO 4 GROUPS BY BASELINE GLOMERULAR FILTRATION RATE (GFR)
") 1 RENAL DISEASE OUTCOMES IN HYPERTENSIVE PATIENTS STRATIFIED INTO 4 GROUPS BY BASELINE GLOMERULAR FILTRATION RATE (GFR) 6 / 5 / 1006-1 2 Introduction Hypertension is the second most common cause of end-stage
1 RENAL DISEASE OUTCOMES IN HYPERTENSIVE PATIENTS STRATIFIED INTO 4 GROUPS BY BASELINE GLOMERULAR FILTRATION RATE (GFR) 6 / 5 / 1006-1 2 Introduction Hypertension is the second most common cause of end-stage
A: Epidemiology update. Evidence that LDL-C and CRP identify different high-risk groups
 A: Epidemiology update Evidence that LDL-C and CRP identify different high-risk groups Women (n = 27,939; mean age 54.7 years) who were free of symptomatic cardiovascular (CV) disease at baseline were
A: Epidemiology update Evidence that LDL-C and CRP identify different high-risk groups Women (n = 27,939; mean age 54.7 years) who were free of symptomatic cardiovascular (CV) disease at baseline were
No relevant financial relationships
 MANAGEMENT OF LIPID DISORDERS: WHERE DO WE STAND WITH THE NEW PRACTICE GUIDELINES? Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Disclosure No relevant financial relationships
MANAGEMENT OF LIPID DISORDERS: WHERE DO WE STAND WITH THE NEW PRACTICE GUIDELINES? Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Disclosure No relevant financial relationships
FORTH VALLEY. LIPID LOWERING GUIDELINE v5 2016
 FORTH VALLEY LIPID LOWERING GUIDELINE v5 2016 This guideline applies to people over 16 years of age. This guideline is not intended to serve as a standard of medical care or be applicable in every situation.
FORTH VALLEY LIPID LOWERING GUIDELINE v5 2016 This guideline applies to people over 16 years of age. This guideline is not intended to serve as a standard of medical care or be applicable in every situation.
Metabolic Syndrome and Chronic Kidney Disease
 Metabolic Syndrome and Chronic Kidney Disease Definition of Metabolic Syndrome National Cholesterol Education Program (NCEP) Adult Treatment Panel (ATP) III Abdominal obesity, defined as a waist circumference
Metabolic Syndrome and Chronic Kidney Disease Definition of Metabolic Syndrome National Cholesterol Education Program (NCEP) Adult Treatment Panel (ATP) III Abdominal obesity, defined as a waist circumference
Disclosures. Diabetes and Cardiovascular Risk Management. Learning Objectives. Atherosclerotic Cardiovascular Disease
 Disclosures Diabetes and Cardiovascular Risk Management Tony Hampton, MD, MBA Medical Director Advocate Aurora Operating System Advocate Aurora Healthcare Downers Grove, IL No conflicts or disclosures
Disclosures Diabetes and Cardiovascular Risk Management Tony Hampton, MD, MBA Medical Director Advocate Aurora Operating System Advocate Aurora Healthcare Downers Grove, IL No conflicts or disclosures
Diabetic Dyslipidemia
 Diabetic Dyslipidemia Dr R V S N Sarma, M.D., (Internal Medicine), M.Sc., (Canada), Consultant Physician Cardiovascular disease (CVD) is a significant cause of illness, disability, and death among individuals
Diabetic Dyslipidemia Dr R V S N Sarma, M.D., (Internal Medicine), M.Sc., (Canada), Consultant Physician Cardiovascular disease (CVD) is a significant cause of illness, disability, and death among individuals
Elements for a Public Summary
 Rosuvastatin Stada 5 mg film-coated tablets Rosuvastatin Stada 10 mg film-coated tablets Rosuvastatin Stada 20 mg film-coated tablets Rosuvastatin Stada 40 mg film-coated tablets 25.8.2014, V1.1 PUBLIC
Rosuvastatin Stada 5 mg film-coated tablets Rosuvastatin Stada 10 mg film-coated tablets Rosuvastatin Stada 20 mg film-coated tablets Rosuvastatin Stada 40 mg film-coated tablets 25.8.2014, V1.1 PUBLIC
Andrew Cohen, MD and Neil S. Skolnik, MD INTRODUCTION
 2 Hyperlipidemia Andrew Cohen, MD and Neil S. Skolnik, MD CONTENTS INTRODUCTION RISK CATEGORIES AND TARGET LDL-CHOLESTEROL TREATMENT OF LDL-CHOLESTEROL SPECIAL CONSIDERATIONS OLDER AND YOUNGER ADULTS ADDITIONAL
2 Hyperlipidemia Andrew Cohen, MD and Neil S. Skolnik, MD CONTENTS INTRODUCTION RISK CATEGORIES AND TARGET LDL-CHOLESTEROL TREATMENT OF LDL-CHOLESTEROL SPECIAL CONSIDERATIONS OLDER AND YOUNGER ADULTS ADDITIONAL
Lipid Panel Management Refresher Course for the Family Physician
 Lipid Panel Management Refresher Course for the Family Physician Objectives Understand the evidence that was evaluated to develop the 2013 ACC/AHA guidelines Discuss the utility and accuracy of the new
Lipid Panel Management Refresher Course for the Family Physician Objectives Understand the evidence that was evaluated to develop the 2013 ACC/AHA guidelines Discuss the utility and accuracy of the new
Supplement Table 2. Categorization of Statin Intensity Based on Potential Low-Density Lipoprotein Cholesterol Reduction
 Supplement: Tables Supplement Table 1. Study Eligibility Criteria Supplement Table 2. Categorization of Statin Intensity Based on Potential Low-Density Lipoprotein Cholesterol Reduction Supplement Table
Supplement: Tables Supplement Table 1. Study Eligibility Criteria Supplement Table 2. Categorization of Statin Intensity Based on Potential Low-Density Lipoprotein Cholesterol Reduction Supplement Table
DYSLIPIDEMIA RECOMMENDATIONS
 DYSLIPIDEMIA RECOMMENDATIONS Α. DIAGNOSIS Recommendation 1 INITIAL LIPID PROFILING (Level of evidence II) It is recommended to GPs and other PHC Physicians to assess the lipid profile {total cholesterol
DYSLIPIDEMIA RECOMMENDATIONS Α. DIAGNOSIS Recommendation 1 INITIAL LIPID PROFILING (Level of evidence II) It is recommended to GPs and other PHC Physicians to assess the lipid profile {total cholesterol
The CARI Guidelines Caring for Australasians with Renal Impairment. Protein Restriction to prevent the progression of diabetic nephropathy GUIDELINES
 Protein Restriction to prevent the progression of diabetic nephropathy Date written: September 2004 Final submission: September 2005 Author: Kathy Nicholls GUIDELINES a. A small volume of evidence suggests
Protein Restriction to prevent the progression of diabetic nephropathy Date written: September 2004 Final submission: September 2005 Author: Kathy Nicholls GUIDELINES a. A small volume of evidence suggests
In the Know: Canadian Guidelines for Dyslipidemia, 2003
 In the Know: Canadian Guidelines for Dyslipidemia, 2003 In his reviews of Canadian dyslipidemia guidelines, Dr. Curnew explores the impact of major trials, the assessment and categories of risk, and both
In the Know: Canadian Guidelines for Dyslipidemia, 2003 In his reviews of Canadian dyslipidemia guidelines, Dr. Curnew explores the impact of major trials, the assessment and categories of risk, and both
Placebo-Controlled Statin Trials EXPLAINING THE DECREASE IN DEATHS FROM CHD! PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN EXPLAINING THE DECREASE IN
 PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest EXPLAINING THE DECREASE
PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest EXPLAINING THE DECREASE
The CARI Guidelines Caring for Australians with Renal Impairment. Control of Hypercholesterolaemia and Progression of Diabetic Nephropathy
 Control of Hypercholesterolaemia and Progression of Diabetic Nephropathy Date written: September 2004 Final submission: September 2005 Author: Kathy Nicholls GUIDELINES a. All hypercholesterolaemic diabetics
Control of Hypercholesterolaemia and Progression of Diabetic Nephropathy Date written: September 2004 Final submission: September 2005 Author: Kathy Nicholls GUIDELINES a. All hypercholesterolaemic diabetics
Diabetes Complications Guideline Based Screening, Management, and Referral
 Diabetes Complications Guideline Based Screening, Management, and Referral Eric L. Johnson, M.D. Associate Professor Department of Family and Community Medicine Assistant Medical Director Altru Diabetes
Diabetes Complications Guideline Based Screening, Management, and Referral Eric L. Johnson, M.D. Associate Professor Department of Family and Community Medicine Assistant Medical Director Altru Diabetes
Lecture 36 Dyslipidemia Therapeutics Barry LIPIDS:
 LIPIDS: PATHOPHYSIOLOGY: TC or LDL-C = CVD HDL-C = CVD Association between TG and CVD not established o HyperTG associated with pancreatitis o Reducing TG w/ drug therapy doesn t CVD TYPES OF DYSLIPIDEMIA:
LIPIDS: PATHOPHYSIOLOGY: TC or LDL-C = CVD HDL-C = CVD Association between TG and CVD not established o HyperTG associated with pancreatitis o Reducing TG w/ drug therapy doesn t CVD TYPES OF DYSLIPIDEMIA:
Clinical Recommendations: Patients with Periodontitis
 The American Journal of Cardiology and Journal of Periodontology Editors' Consensus: Periodontitis and Atherosclerotic Cardiovascular Disease. Friedewald VE, Kornman KS, Beck JD, et al. J Periodontol 2009;
The American Journal of Cardiology and Journal of Periodontology Editors' Consensus: Periodontitis and Atherosclerotic Cardiovascular Disease. Friedewald VE, Kornman KS, Beck JD, et al. J Periodontol 2009;
Update on Dyslipidemia and Recent Data on Treating the Statin Intolerant Patient
 Update on Dyslipidemia and Recent Data on Treating the Statin Intolerant Patient Steven E. Nissen MD Chairman, Department of Cardiovascular Medicine Cleveland Clinic Disclosure Consulting: Many pharmaceutical
Update on Dyslipidemia and Recent Data on Treating the Statin Intolerant Patient Steven E. Nissen MD Chairman, Department of Cardiovascular Medicine Cleveland Clinic Disclosure Consulting: Many pharmaceutical
Diabetes Mellitus: A Cardiovascular Disease
 Diabetes Mellitus: A Cardiovascular Disease Nestoras Mathioudakis, M.D. Assistant Professor of Medicine Division of Endocrinology, Diabetes, & Metabolism September 30, 2013 1 The ABCs of cardiovascular
Diabetes Mellitus: A Cardiovascular Disease Nestoras Mathioudakis, M.D. Assistant Professor of Medicine Division of Endocrinology, Diabetes, & Metabolism September 30, 2013 1 The ABCs of cardiovascular
APPENDIX 2F Management of Cholesterol
 Patients with established CVD: Coronary heart disease Cerebrovascular disease Peripheral vascular disease APPEDIX 2F Management of Cholesterol Patients at high risk of cardiovascular events: Chronic kidney
Patients with established CVD: Coronary heart disease Cerebrovascular disease Peripheral vascular disease APPEDIX 2F Management of Cholesterol Patients at high risk of cardiovascular events: Chronic kidney
Dyslipidemia: Lots of Good Evidence, Less Good Interpretation.
 Dyslipidemia: Lots of Good Evidence, Less Good Interpretation. G Michael Allan Evidence & CPD Program, ACFP Associate Professor, Dept of Family, U of A. CFPC CoI Templates: Slide 1 Faculty/Presenter Disclosure
Dyslipidemia: Lots of Good Evidence, Less Good Interpretation. G Michael Allan Evidence & CPD Program, ACFP Associate Professor, Dept of Family, U of A. CFPC CoI Templates: Slide 1 Faculty/Presenter Disclosure
Eugene Barrett M.D., Ph.D. University of Virginia 6/18/2007. Diagnosis and what is it Glucose Tolerance Categories FPG
 Diabetes Mellitus: Update 7 What is the unifying basis of this vascular disease? Eugene J. Barrett, MD, PhD Professor of Internal Medicine and Pediatrics Director, Diabetes Center and GCRC Health System
Diabetes Mellitus: Update 7 What is the unifying basis of this vascular disease? Eugene J. Barrett, MD, PhD Professor of Internal Medicine and Pediatrics Director, Diabetes Center and GCRC Health System
Janet B. Long, MSN, ACNP, CLS, FAHA, FNLA Rhode Island Cardiology Center
 Primary and Secondary Prevention of Coronary Artery Disease: What is the role of non statin drugs (fenofibrates, fish oil, niacin, folate and vitamins)? Janet B. Long, MSN, ACNP, CLS, FAHA, FNLA Rhode
Primary and Secondary Prevention of Coronary Artery Disease: What is the role of non statin drugs (fenofibrates, fish oil, niacin, folate and vitamins)? Janet B. Long, MSN, ACNP, CLS, FAHA, FNLA Rhode
Effects of Lowering LDL Cholesterol on Progression of Kidney Disease
 Effects of Lowering LDL Cholesterol on Progression of Kidney Disease Richard Haynes, David Lewis, Jonathan Emberson, Christina Reith, Lawrence Agodoa, Alan Cass, Jonathan C. Craig, Dick de Zeeuw, Bo Feldt-Rasmussen,
Effects of Lowering LDL Cholesterol on Progression of Kidney Disease Richard Haynes, David Lewis, Jonathan Emberson, Christina Reith, Lawrence Agodoa, Alan Cass, Jonathan C. Craig, Dick de Zeeuw, Bo Feldt-Rasmussen,
Major recommendations for statin therapy for ASCVD prevention
 2013 A/AHA Guidelines holesterol Rx to Reduce ASVD Risk in Adults Major recommendations for statin therapy for ASVD prevention *% in LDL can be used as indication of response & adherence to Rx but is not
2013 A/AHA Guidelines holesterol Rx to Reduce ASVD Risk in Adults Major recommendations for statin therapy for ASVD prevention *% in LDL can be used as indication of response & adherence to Rx but is not
Uric acid and CKD. Sunil Badve Conjoint Associate Professor, UNSW Staff Specialist, St George
 Uric acid and CKD Sunil Badve Conjoint Associate Professor, UNSW Staff Specialist, St George Hospital @Badves Case Mr J, 52 Male, referred in June 2015 DM type 2 (4 years), HTN, diabetic retinopathy, diabetic
Uric acid and CKD Sunil Badve Conjoint Associate Professor, UNSW Staff Specialist, St George Hospital @Badves Case Mr J, 52 Male, referred in June 2015 DM type 2 (4 years), HTN, diabetic retinopathy, diabetic
ESC Geoffrey Rose Lecture on Population Sciences Cholesterol and risk: past, present and future
 ESC Geoffrey Rose Lecture on Population Sciences Cholesterol and risk: past, present and future Rory Collins BHF Professor of Medicine & Epidemiology Clinical Trial Service Unit & Epidemiological Studies
ESC Geoffrey Rose Lecture on Population Sciences Cholesterol and risk: past, present and future Rory Collins BHF Professor of Medicine & Epidemiology Clinical Trial Service Unit & Epidemiological Studies
Title: Statins for haemodialysis patients with diabetes? Long-term follow-up endorses the original conclusions of the 4D study.
 Manuscript type: Invited Commentary: Title: Statins for haemodialysis patients with diabetes? Long-term follow-up endorses the original conclusions of the 4D study. Authors: David C Wheeler 1 and Bertram
Manuscript type: Invited Commentary: Title: Statins for haemodialysis patients with diabetes? Long-term follow-up endorses the original conclusions of the 4D study. Authors: David C Wheeler 1 and Bertram
Medical Policy An independent licensee of the Blue Cross Blue Shield Association
 Statin Therapy Page 1 of 10 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: Statin Therapy Prime Therapeutics will review Prior Authorization requests. Prior Authorization
Statin Therapy Page 1 of 10 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: Statin Therapy Prime Therapeutics will review Prior Authorization requests. Prior Authorization
2013 Cholesterol Guidelines. Anna Broz MSN, RN, CNP, AACC Cer=fied Adult Nurse Prac==oner North Ohio Heart, Inc.
 2013 Cholesterol Guidelines Anna Broz MSN, RN, CNP, AACC Cer=fied Adult Nurse Prac==oner North Ohio Heart, Inc. Disclosures Speaker Gilead Sciences NHLBI Charge to the Expert Panel Evaluate higher quality
2013 Cholesterol Guidelines Anna Broz MSN, RN, CNP, AACC Cer=fied Adult Nurse Prac==oner North Ohio Heart, Inc. Disclosures Speaker Gilead Sciences NHLBI Charge to the Expert Panel Evaluate higher quality
Diabetes: Use of Adjunctive Therapy ACEs, ARBs, ASA & STATINs --Oh My! Veronica J. Brady, PhD, FNP-BC, BC-ADM, CDE Project ECHO April 19, 2018
 Diabetes: Use of Adjunctive Therapy ACEs, ARBs, ASA & STATINs --Oh My! Veronica J. Brady, PhD, FNP-BC, BC-ADM, CDE Project ECHO April 19, 2018 Points to Ponder ASCVD is the leading cause of morbidity
Diabetes: Use of Adjunctive Therapy ACEs, ARBs, ASA & STATINs --Oh My! Veronica J. Brady, PhD, FNP-BC, BC-ADM, CDE Project ECHO April 19, 2018 Points to Ponder ASCVD is the leading cause of morbidity
Primary Prevention Patients aged 85yrs and over
 Rotherham Guideline for the management of Non-Familial Hypercholesterolaemia Type 1 Diabetes Offer lifestyle advice Over 40yrs of age? Diabetic for more than 10 years? Established nephropathy? Other CVD
Rotherham Guideline for the management of Non-Familial Hypercholesterolaemia Type 1 Diabetes Offer lifestyle advice Over 40yrs of age? Diabetic for more than 10 years? Established nephropathy? Other CVD
Antihyperlipidemic Drugs
 Antihyperlipidemic Drugs Hyperlipidemias. Hyperlipoproteinemias. Hyperlipemia. Hypercholestrolemia. Direct relationship with acute pancreatitis and atherosclerosis Structure Lipoprotein Particles Types
Antihyperlipidemic Drugs Hyperlipidemias. Hyperlipoproteinemias. Hyperlipemia. Hypercholestrolemia. Direct relationship with acute pancreatitis and atherosclerosis Structure Lipoprotein Particles Types
Common Repatha Documentation Requirements for Patients With Primary Hyperlipidemia and Established CVD 1,2
 Established CVD Common Repatha Documentation Requirements for Patients With Primary Hyperlipidemia and Established CVD 1,2 Primary and Secondary Diagnosis Codes Primary Diagnosis: Primary hyperlipidemia
Established CVD Common Repatha Documentation Requirements for Patients With Primary Hyperlipidemia and Established CVD 1,2 Primary and Secondary Diagnosis Codes Primary Diagnosis: Primary hyperlipidemia
Dyslipedemia New Guidelines
 Dyslipedemia New Guidelines New ACC/AHA Prevention Guidelines on Blood Cholesterol November 12, 2013 Mohammed M Abd El Ghany Professor of Cardiology Cairo Universlty 1 1 0 Cholesterol Management Pharmacotherapy
Dyslipedemia New Guidelines New ACC/AHA Prevention Guidelines on Blood Cholesterol November 12, 2013 Mohammed M Abd El Ghany Professor of Cardiology Cairo Universlty 1 1 0 Cholesterol Management Pharmacotherapy
Cardiovascular Risk and Dyslipidemia Management Clinician Guide SEPTEMBER 2017
 Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Cardiovascular Risk and Dyslipidemia Management Clinician Guide SEPTEMBER 2017 Introduction This Clinician Guide is based on the 2017 KP National
Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Cardiovascular Risk and Dyslipidemia Management Clinician Guide SEPTEMBER 2017 Introduction This Clinician Guide is based on the 2017 KP National
CVD Risk Assessment. Lipid Management in Women: Lessons Learned. Conflict of Interest Disclosure
 Lipid Management in Women: Lessons Learned Conflict of Interest Disclosure Emma A. Meagher, MD has no conflicts to disclose Emma A. Meagher, MD Associate Professor, Medicine and Pharmacology University
Lipid Management in Women: Lessons Learned Conflict of Interest Disclosure Emma A. Meagher, MD has no conflicts to disclose Emma A. Meagher, MD Associate Professor, Medicine and Pharmacology University
NCEP Report. Implications of Recent Clinical Trials for the National Cholesterol Education Program Adult Treatment Panel III Guidelines
 NCEP Report Implications of Recent Clinical Trials for the National Cholesterol Education Program Adult Treatment Panel III Guidelines Scott M. Grundy; James I. Cleeman; C. Noel Bairey Merz; H. Bryan Brewer,
NCEP Report Implications of Recent Clinical Trials for the National Cholesterol Education Program Adult Treatment Panel III Guidelines Scott M. Grundy; James I. Cleeman; C. Noel Bairey Merz; H. Bryan Brewer,
Pharmacy Drug Class Review
 Pharmacy Drug Class Review January 22, 2014 Authored By: Christina Manciocchi, Pharm.D. BCACP Disclaimer: Specific agents may have variations Edited By: Richard J. Kraft, Pharm.D.BCPS NEW CHOLESTEROL GUIDELINES
Pharmacy Drug Class Review January 22, 2014 Authored By: Christina Manciocchi, Pharm.D. BCACP Disclaimer: Specific agents may have variations Edited By: Richard J. Kraft, Pharm.D.BCPS NEW CHOLESTEROL GUIDELINES
No relevant financial relationships
 MANAGEMENT OF LIPID DISORDERS Balancing Benefits and harms Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial relationships baron@medicine.ucsf.edu
MANAGEMENT OF LIPID DISORDERS Balancing Benefits and harms Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial relationships baron@medicine.ucsf.edu
Cholesterol lowering intervention for cardiovascular prevention in high risk patients with or without LDL cholesterol elevation
 TrialResults-center.org www.trialresultscenter.org Cholesterol lowering intervention for cardiovascular prevention in high risk patients with or without LDL cholesterol elevation A systematic review and
TrialResults-center.org www.trialresultscenter.org Cholesterol lowering intervention for cardiovascular prevention in high risk patients with or without LDL cholesterol elevation A systematic review and
Effects of Kidney Disease on Cardiovascular Morbidity and Mortality
 Effects of Kidney Disease on Cardiovascular Morbidity and Mortality Joachim H. Ix, MD, MAS Assistant Professor in Residence Division of Nephrology University of California San Diego, and Veterans Affairs
Effects of Kidney Disease on Cardiovascular Morbidity and Mortality Joachim H. Ix, MD, MAS Assistant Professor in Residence Division of Nephrology University of California San Diego, and Veterans Affairs
SLOWING PROGRESSION OF KIDNEY DISEASE. Mark Rosenberg MD University of Minnesota
 SLOWING PROGRESSION OF KIDNEY DISEASE Mark Rosenberg MD University of Minnesota OUTLINE 1. Epidemiology of progression 2. Therapy to slow progression a. Blood Pressure control b. Renin-angiotensin-aldosterone
SLOWING PROGRESSION OF KIDNEY DISEASE Mark Rosenberg MD University of Minnesota OUTLINE 1. Epidemiology of progression 2. Therapy to slow progression a. Blood Pressure control b. Renin-angiotensin-aldosterone
Ο ρόλος των τριγλυκεριδίων στην παθογένεια των μικροαγγειοπαθητικών επιπλοκών του σακχαρώδη διαβήτη
 Ο ρόλος των τριγλυκεριδίων στην παθογένεια των μικροαγγειοπαθητικών επιπλοκών του σακχαρώδη διαβήτη Κωνσταντίνος Τζιόμαλος Επίκουρος Καθηγητής Παθολογίας Α Προπαιδευτική Παθολογική Κλινική, Νοσοκομείο
Ο ρόλος των τριγλυκεριδίων στην παθογένεια των μικροαγγειοπαθητικών επιπλοκών του σακχαρώδη διαβήτη Κωνσταντίνος Τζιόμαλος Επίκουρος Καθηγητής Παθολογίας Α Προπαιδευτική Παθολογική Κλινική, Νοσοκομείο
STATIN UTILIZATION MANAGEMENT CRITERIA
 STATIN UTILIZATION MANAGEMENT CRITERIA DRUG CLASS: HMG Co-A Reductase Inhibitors & Combinations Agents which require prior review: Advicor (niacin extended-release/lovastatin) Crestor (rosuvastatin)(5mg,10mg,
STATIN UTILIZATION MANAGEMENT CRITERIA DRUG CLASS: HMG Co-A Reductase Inhibitors & Combinations Agents which require prior review: Advicor (niacin extended-release/lovastatin) Crestor (rosuvastatin)(5mg,10mg,
New Lipid Guidelines. PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN: Implications of the New Guidelines for Hypertension and Lipids.
 PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN: Implications of the New Guidelines for Hypertension and Lipids Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Disclosure No relevant
PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN: Implications of the New Guidelines for Hypertension and Lipids Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Disclosure No relevant
Update On Diabetic Dyslipidemia: Who Should Be Treated With A Fibrate After ACCORD-LIPID?
 Update On Diabetic Dyslipidemia: Who Should Be Treated With A Fibrate After ACCORD-LIPID? Karen Aspry, MD, MS, ABCL, FACC Assistant Clinical Professor of Medicine Warren Alpert Medical School of Brown
Update On Diabetic Dyslipidemia: Who Should Be Treated With A Fibrate After ACCORD-LIPID? Karen Aspry, MD, MS, ABCL, FACC Assistant Clinical Professor of Medicine Warren Alpert Medical School of Brown
Is Lower Better for LDL or is there a Sweet Spot
 Is Lower Better for LDL or is there a Sweet Spot ALAN S BROWN MD, FACC FNLA FAHA FASPC DIRECTOR, DIVISION OF CARDIOLOGY ADVOCATE LUTHERAN GENERAL HOSPITAL, PARK RIDGE, ILLINOIS DIRECTOR OF CARDIOLOGY,
Is Lower Better for LDL or is there a Sweet Spot ALAN S BROWN MD, FACC FNLA FAHA FASPC DIRECTOR, DIVISION OF CARDIOLOGY ADVOCATE LUTHERAN GENERAL HOSPITAL, PARK RIDGE, ILLINOIS DIRECTOR OF CARDIOLOGY,
Learning Objectives. Patient Case
 Joseph Saseen, Pharm.D., FASHP, FCCP, BCPS Professor and Vice Chair, Department of Clinical Pharmacy University of Colorado Anschutz Medical Campus Learning Objectives Identify the 4 patient populations
Joseph Saseen, Pharm.D., FASHP, FCCP, BCPS Professor and Vice Chair, Department of Clinical Pharmacy University of Colorado Anschutz Medical Campus Learning Objectives Identify the 4 patient populations
Management of Lipid Disorders and Hypertension: Implications of the New Guidelines
 Management of Lipid Disorders and Hypertension Management of Lipid Disorders and Hypertension: Implications of the New Guidelines Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine
Management of Lipid Disorders and Hypertension Management of Lipid Disorders and Hypertension: Implications of the New Guidelines Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine
CKDinform: A PCP s Guide to CKD Detection and Delaying Progression
 CKDinform: A PCP s Guide to CKD Detection and Delaying Progression Learning Objectives Describe suitable screening tools, such as GFR and ACR, for proper utilization in clinical practice related to the
CKDinform: A PCP s Guide to CKD Detection and Delaying Progression Learning Objectives Describe suitable screening tools, such as GFR and ACR, for proper utilization in clinical practice related to the
Antihyperlipidemic drugs
 Antihyperlipidemic drugs The clinically important lipoproteins are LDL low density lipoprotein, VLDL very low density lipoprotein, HDL high density lipoprotein. Hyperlipidemia may caused 1. by individual
Antihyperlipidemic drugs The clinically important lipoproteins are LDL low density lipoprotein, VLDL very low density lipoprotein, HDL high density lipoprotein. Hyperlipidemia may caused 1. by individual
How to Reduce Residual Risk in Primary Prevention
 How to Reduce Residual Risk in Primary Prevention Helene Glassberg, MD Assistant Professor of Medicine Section of Cardiology Hospital of the University of Pennsylvania Philadelphia, PA USA Patients with
How to Reduce Residual Risk in Primary Prevention Helene Glassberg, MD Assistant Professor of Medicine Section of Cardiology Hospital of the University of Pennsylvania Philadelphia, PA USA Patients with
VA/DoD Clinical Practice Guideline for the Diagnosis and Management of Hypertension - Pocket Guide Update 2004 Revision July 2005
 VA/DoD Clinical Practice Guideline for the Diagnosis and Management of Hypertension - Pocket Guide Update 2004 Revision July 2005 1 Any adult in the health care system 2 Obtain blood pressure (BP) (Reliable,
VA/DoD Clinical Practice Guideline for the Diagnosis and Management of Hypertension - Pocket Guide Update 2004 Revision July 2005 1 Any adult in the health care system 2 Obtain blood pressure (BP) (Reliable,