Highlights of the new blood pressure and cholesterol guidelines: A whole new philosophy. Jeremy L. Johnson, PharmD, BCACP, CDE, BC-ADM
|
|
|
- Kerry Miller
- 5 years ago
- Views:
Transcription
1 Highlights of the new blood pressure and cholesterol guidelines: A whole new philosophy Jeremy L. Johnson, PharmD, BCACP, CDE, BC-ADM OSHP 2014 Annual Meeting Oklahoma City, OK April 4, Objectives Recognize the differences between the NCEP ATP 3 guidelines and the ACC/AHA 2013 Blood Cholesterol Guidelines as well as between the JNC 7 and 2014 Guideline for Management of High Blood Pressure from the Panel Appointed to JNC 8. Implement principles of the ACC/AHA 2013 Blood Cholesterol Guidelines into a clinical pharmacy practice. Implement principles of the 2014 Guideline for Management of High Blood Pressure from the Panel Appointed to JNC 8 into a clinical pharmacy practice. 2
 NCEP ATP 3 2002 Updated 2004 Joint National Committee on Prevention, Detection, Evaluation, & Treatment")
2 Overview History and evolution of the guidelines Lipid Guidelines ATP ACC/AHA Blood pressure Guidelines JNC JNC 8 3 Clinical Practice Guidelines National Heart Lung and Blood Institute Detection, Evaluation, & Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel) NCEP ATP Updated 2004 Joint National Committee on Prevention, Detection, Evaluation, & Treatment of High Blood Pressure JNC


3 Clinical Practice Guidelines in Development To check status: 5 Clinical Practice Guidelines in Development Updated June
4 Lipid Guidelines Review of NCEP ATP 3 Highlights of the new 2013 ACC/AHA Blood Cholesterol Guidelines 7 NCEP ATP 3 Released: 2001 Updated:
5 Prevention of CHD Primary Prevention Prevention of 1 st cardiovascular event Goal: long term risk (>10 y) and short term (<10 y) Therapeutic Lifestyle Changes (TLC) are a focus saturated fat and cholesterol weight physical activity NCEP ATP III Expert panel. JAMA 2001; 285(19): Prevention of CHD Secondary Prevention Prevention of subsequent cardiovascular events after a first (MI, CABG, PCI, CVA) Goal: long term risk (>10 y) and short term (<10 y) TLC remains a focus Drug therapy typically required Higher risk = a stricter goal LDL NCEP ATP III Expert panel. JAMA 2001; 285(19):

6 Goal Values or Targets TC HDL TG < 200mg/dL > 40 mg/dl (>50mg/dL for women) < 150mg/dL LDL goal must be determined based on risk NCEP ATP III Expert panel. JAMA 2001; 285(19): NCEP ATP III Guidelines LDL is the major atherogenic lipoprotein and has long been identified by NCEP as the primary target of cholesterol-lowering therapy This focus on LDL has been strongly validated by recent clinical trials, which show the efficacy of LDL-lowering therapy for reducing risk for CHD NCEP ATP III Expert panel. JAMA 2001; 285(19):

 <100 <130 <160 NCEP ATP III Expert panel.")
7 NCEP ATP III Guidelines NCEP ATP III Expert panel. JAMA 2001; 285(19): Three Categories of Risk that Modify LDL-Cholesterol Goals Risk Category CHD and CHD risk equivalents Multiple (2+) risk factors Zero to one risk factor LDL Goal (mg/dl) <100 <130 <160 NCEP ATP III Expert panel. JAMA 2001; 285(19):
8 CHD Risk Equivalents Risk for major coronary events equal to that in established CHD 10-year risk for CHD event >20% NCEP ATP III Expert panel. JAMA 2001; 285(19): CHD Risk Equivalents Other clinical forms of atherosclerotic disease peripheral arterial disease abdominal aortic aneurysm symptomatic carotid artery disease Diabetes Multiple risk factors that confer a 10- year risk for CHD >20% NCEP ATP III Expert panel. JAMA 2001; 285(19):
9 Major Risk Factors (Exclusive of LDL Cholesterol) That Modify LDL Goals Cigarette smoking Hypertension (BP 140/90 mmhg or on antihypertensive medication) Low HDL cholesterol (<40 mg/dl) Family history of premature CHD CHD in male first degree relative <55 years CHD in female first degree relative <65 years Age (men 45 years; women 55 years) HDL cholesterol 60 mg/dl counts as a negative risk factor; its presence removes one risk factor from the total count. 17 NCEP ATP III Expert panel. JAMA 2001; 285(19): Risk Assessment Count major risk factors For patients with multiple (2+) risk factors Perform 10-year risk assessment (Framingham Risk Assessment) For patients with 0 1 risk factor 10 year risk assessment not required Most patients have 10-year risk <10% NCEP ATP III Expert panel. JAMA 2001; 285(19):
10 LDL Cholesterol Goals and Cutpoints for Therapeutic Lifestyle Changes (TLC) and Drug Therapy in Different Risk Categories Risk Category LDL Goal (mg/dl) LDL Level at Which to Initiate Therapeutic Lifestyle Changes (TLC) (mg/dl) LDL Level at Which to Consider Drug Therapy (mg/dl) CHD or CHD Risk Equivalents (10-year risk >20%) <100 (optional <70) (<100: consider drug options) 2+ Risk Factors (10-year risk 20%) < year risk 10 20%: 130 ( : consider drug options) 10-year risk <10%: Risk Factor < ( : LDLlowering drug optional) NCEP ATP III Expert panel. JAMA 2001; 285(19): Grundy SM. Circulation. 110:227-39; Optional LDL goal < 70 mg/dl Option for patients at very high risk Must have established CVD plus any of: Multiple major risk factors (especially diabetes) Severe and poorly controlled risk factors (especially cigarette smoking) Multiple risk factors of Metabolic Syndrome High TG > 200 mg/dl plus Non-HDL 130 mg/dl with low HDL < 40 mg/dl History of acute coronary syndromes (ACS) Grundy SM. Circulation. 110:227-39;
11 Algorithm for Lipid-Lowering Medication Therapy Initiate LDLlowering drug therapy If LDL goal not If LDL goal achieved, Monitor 6 wks not achieved, 6 wks intensify drug Q 6-12 mo response intensify therapy or and LDL-lowering refer to a lipid adherence therapy specialist to therapy Start statin or bile acid sequestrant First, maximize current statin or BAS dose Second, add ezetimibe, or fibrate, or niacin If LDL goal achieved and TG >200mg/dL, calculate non-hdl Treat other lipid risk factors and metabolic syndrome NCEP ATP III Expert panel. JAMA 2001; 285(19): Not good enough? Half of all myocardial infarctions and strokes occur despite apparently healthy men and women with LDL levels below currently recommended thresholds for treatment Even with adequate LDL lowering, many patients on statin therapy have significant CVD risk Ridker PM. Lancet. 2009; 373: Brunzell JD. Diabetes Care. 2008; 31:

12 2013 ACC/AHA Guideline on the Treatment of Blood Cholesterol to Reduce Atherosclerotic Cardiovascular Risk in Adults Released Mid-November 2013 Journal of the American College of Cardiology 23 Stone ACC/AHA Blood Cholesterol Guideline. Journal of the American College of Cardiology. 2013:doi: /j.jacc
13 2013 ACC/AHA Blood Cholesterol Guidelines Expert panel for ATP 4 Partnered with ACC/AHA Focus on ASCVD risk reduction, not comprehensive lipid management Only used RCT, systematic reviews, meta-analyses of RCT 25 3 Critical Questions 1. What is the evidence for LDL and non-hdl goals for the secondary prevention of ASCVD? 2. Same as #1, but primary prevention 3. For primary and secondary prevention, what is the impact on lipid levels, effectiveness, and safety of specific cholesterol-modifying drugs used for lipid management in general and in selected subgroups? Stone ACC/AHA Blood Cholesterol Guideline. Journal of the American College of Cardiology. 2013:doi: /j.jacc
14 Findings unable to find evidence to support titrating statins to a target LDL or non-hdl goal extensive evidence that appropriate statin intensity should be used to reduce ASCVD risk use of non-statins to additionally lower non- HDL once LDL goal achieved, DID NOT further reduce ASCVD outcomes Stone ACC/AHA Blood Cholesterol Guideline. Journal of the American College of Cardiology. 2013:doi: /j.jacc Findings Non-statin therapies in general have not demonstrated significant ASCVD event recuction. Lifestyle modifications remain a critical component of health promotion and ASCVD risk reduction Identification of 4 statin benefit groups to focus on ASCVD risk reduction Stone ACC/AHA Blood Cholesterol Guideline. Journal of the American College of Cardiology. 2013:doi: /j.jacc

15 4 Statin Benefit Groups Clinical ASCVD 75 yo (secondary prevention) Primary elevation of LDL 190 mg/dl yo with Diabetes and LDL mg/dl No clinical ASCVD or Diabetes, yo and LDL mg/dl and 10-year ASCVD risk of 7.5% or higher Stone ACC/AHA Blood Cholesterol Guideline. Journal of the American College of Cardiology. 2013:doi: /j.jacc Stone ACC/AHA Blood Cholesterol Guideline. Journal of the American College of Cardiology. 2013:doi: /j.jacc

16 Clinical ASCVD 75 years High-intensity statin therapy (1 st line) If not tolerated, use moderate-intensity If >70 years, consider benefits vs risks and may use moderate- or high-intensity statin Stone ACC/AHA Blood Cholesterol Guideline. Journal of the American College of Cardiology. 2013:doi: /j.jacc LDL 190 mg/dl High-intensity statin therapy If not tolerated, use maximum tolerated intensity Once maximum intensity achieved, may consider addition of non-statins to further lower LDL (weak data expert opinion) Stone ACC/AHA Blood Cholesterol Guideline. Journal of the American College of Cardiology. 2013:doi: /j.jacc

17 40-75 years with Diabetes and LDL mg/dl Moderate-intensity statin therapy If ASCVD 10-year risk 7.5%, use high-intensity If <40 or >75 years, consider benefits vs risks and patient preferences Stone ACC/AHA Blood Cholesterol Guideline. Journal of the American College of Cardiology. 2013:doi: /j.jacc No clinical ASCVD or Diabetes, yo and LDL mg/dl and 10-year ASCVD risk of 7.5% or higher Moderate- to High-intensity statin therapy Stone ACC/AHA Blood Cholesterol Guideline. Journal of the American College of Cardiology. 2013:doi: /j.jacc
18 Adults with LDL <190 mg/dl not fitting into a statin benefit group Additional factors may be considered to inform treatment decision making LDL 160 mg/dl Genetic hyperlipidemia Family history of premature ASCVD <55 years or <65 years High C-reactive Protein (CRP) >2 mg/l Coronary artery calcium score 300 Agatston units or 75 percentile for age, sex, ethnicity ABI <0.9 Lifetime risk of ASCVD Stone ACC/AHA Blood Cholesterol Guideline. Journal of the American College of Cardiology. 2013:doi: /j.jacc Intensity of Statin Therapy Expected LDL-lowering: High-intensity 50% Moderate-intensity 30 to <50% Low-intensity <30% High-intensity reduces ASCVD risk more However, moderate- or low-intensity still provides protection, just not as much as high-intensity Stone ACC/AHA Blood Cholesterol Guideline. Journal of the American College of Cardiology. 2013:doi: /j.jacc
19 Statin Intensity Categories and Drugs High-intensity Moderate-intensity Low-intensity Atorvastatin mg Atorvastatin mg Simvastatin 10 mg Rosuvastatin mg Rosuvastatin 5-10 mg Pravastatin mg Simvastatin mg Lovastatin 20 mg Pravastatin mg Fluvastatin mg Lovastatin 40 mg Pitavastatin 1 mg Fluvastatin XL 80 mg Fluvastatin 40 mg BID Pitavastatin 2-4 mg Stone ACC/AHA Blood Cholesterol Guideline. Journal of the American College of Cardiology. 2013:doi: /j.jacc Patient is a 58 year old male with diabetes and an LDL of 198 mg/dl. Per the 2013 ACC/AHA guidelines, how should he be treated? A. No statin B. Low-intensity statin C. Moderate-intensity statin D. High-intensity statin 38
20 Patient is a 58 year old male with diabetes and an LDL of 198 mg/dl. Per the 2013 ACC/AHA guidelines, how should he be treated? A. Pravastatin 80 mg B. Rosuvastatin 20 mg C. Atorvastatin 20 mg D. Fluvastatin 40 mg 39 Patient is a 62 year old female with diabetes, an LDL of 82 (on no statin), and an ASCVD 10- year risk of 7.8%. Per 2013 ACC/AHA guidelines, how should she be treated? A. Atorvastatin 80 mg B. Pitavastatin 1 mg C. Lovastatin 20 mg D. Pravastatin 80 mg 40

21 Calculation of ASCVD 10-year Risk (%) Pooled Cohorts Equations Calculates risk of CHD death, fatal or nonfatal MI or stroke Used for white and black men and women without clinical ASCVD Controversial calculation This places many more people in higher risk categories than the Framingham Risk tool Stone ACC/AHA Blood Cholesterol Guideline. Journal of the American College of Cardiology. 2013:doi: /j.jacc
22 Statin Safety Recommendations Moderate-intensity statin should be used instead of high-intensity if high risk of statin-associated adverse effects Impaired renal or hepatic function Previous stain intolerances or muscle disorder ALT >3 times upper limit of normal (CI) On drugs that affect statin metabolism >75 years of age Possibly history of hemorrhagic stroke Possibly Asian ancestry Stone ACC/AHA Blood Cholesterol Guideline. Journal of the American College of Cardiology. 2013:doi: /j.jacc Statin Safety Recommendations Monitor creatine kinase (CK or CPK) Baseline and if myopathy symptoms Monitor ALT (liver function) Baseline and if hepatotoxic symptoms Consider statin dose if 2 consecutive LDL <40 mg/dl Avoid simvastatin 80 mg Evaluate for new onset diabetes Stone ACC/AHA Blood Cholesterol Guideline. Journal of the American College of Cardiology. 2013:doi: /j.jacc
23 Management of Myopathy Establish baseline of muscle symptoms Unexplained symptoms: Stop statin Measure CK (10 x normal = rhabdomyolysis), Scr, and UA Stone ACC/AHA Blood Cholesterol Guideline. Journal of the American College of Cardiology. 2013:doi: /j.jacc Management of Myopathy Mild to moderate symptoms Stop statin evaluate for cause Sx resolve: give original or lower dose of same statin to establish causal relationship If recurrence, stop original statin When sx resolve, start new statin, low dose Once tolerated, increase dose If not resolved >2 months, likely not statin; resume original dose If intolerant of statins, may use non-statin Stone ACC/AHA Blood Cholesterol Guideline. Journal of the American College of Cardiology. 2013:doi: /j.jacc
24 Monitoring Statin Therapy Initial fasting lipid panel (then start drug) Check fasting lipid panel 4-12 weeks (often 6-8 weeks); to check adherence, NOT to achieve a target or goal Then check fasting lipid panel 3-12 months Stone ACC/AHA Blood Cholesterol Guideline. Journal of the American College of Cardiology. 2013:doi: /j.jacc Monitoring Statin Therapy Insufficient response to statin dose Reinforce adherence to med and lifestyle Exclude secondary causes If higher-risk ASCVD patients on max statin dose, may consider adding non-statin Clinical ASCVD <75 years Baseline LDL 190 mg/dl years old with diabetes Stone ACC/AHA Blood Cholesterol Guideline. Journal of the American College of Cardiology. 2013:doi: /j.jacc

25 49 Triglycerides >500 mg/dl Risk of pancreatitis Treat as a priority over LDL Treat with fibrates or niacin Once TG <500, focus on LDL reduction for ASCVD risk reduction (back to statins) 50
26 Summary of Lipid Guideline Differences ATP ACC/AHA Focus on LDL goals Use statins or any lipidlowering drugs to attain goal Focus on statin intensity Use statins almost exclusively 51 Blood Pressure Guidelines Review of JNC 7 Highlights of the new 2014 Blood Pressure Guidelines by the JNC 8 Panel 52

27 JNC 7 Released: 2003 AHA 2007: essentially an update to JNC 7 53 JNC-7 Classification of BP for Adults The JNC-7 Report. Hypertension. 2003; 42:
28 Specific BP Goals Uncomplicated hypertension (JNC-7) < 140 / < 90 mm Hg Diabetes (ADA ) < 140 / < 80 mm Hg (JNC-7 and NKF recommended <130/80) Renal disease (JNC-7, NKF) < 130 / < 80 mm Hg Diabetes with proteinuria (NKF) <(< 130 / < 80) mm Hg (JNC-VI reported this goal as <125/75) CAD or high CAD risk (AHA 2007) < 130 / < 80 mm Hg Heart failure (AHA 2007) < 120 / <80 mm Hg 55 CAD or high CAD risk (coronary artery disease) Stable angina Unstable angina Myocardial infarction (MI)(NSTEMI)(STEMI) Carotid artery disease Peripheral arterial disease (PAD)(PVD) Abdominal aortic aneurysm Diabetes Chronic kidney disease Framingham risk score 10% 56
29 JNC 7 Principles of Pharmacologic Therapy 57 Pharmacologic Therapy Overview JNC-7 and AHA 2007 There is much data proving that several drug classes reduce cardiovascular events associated with HTN Thiazide-type diuretics Angiotensin converting enzyme inhibitors (ACE-I) Angiotnesin receptor blockers (ARB) Beta-blockers (BB) Calcium channel blockers (CCB) The JNC-7 Report. Hypertension. 2003; 42:
30 AHA 2007 on BB Agree that there is protective data for thiazides, CCB, ACE-I, and ARBs in uncomplicated HTN Don t use a BB in uncomplicated HTN Continue to use BB initially in patients with compelling indications (angina, post MI, HF) American Heart Association: scientific statement Circulation. 115(21): , Preferred Initial Agent Thiazide-type Diuretics basis of antihypertensive therapy in most trials virtually unsurpassed in preventing cardiovascular complications of HTN generally well tolerated inexpensive The JNC-7 Report. Hypertension. 2003; 42:
31 ALLHAT JAMA. 2002;288: Showed thiazides BP as well as ACE-I, CCB, or alpha blocker Thiazide, ACE-I, and CCB similar in reduction of CHD death and non-fatal MI Thiazide superior to CCB preventing heart failure Thiazide superior to ACE-I preventing stroke, combined CVD events, and possibly heart failure 61 Principles of Drug Addition and Titration Begin low dose Use once-daily agents if possible to improve compliance Initial therapy with a thiazide diuretic alone or in combo with ACE-I, ARB, or CCB unless compelling indication for different initial therapy 62 The JNC-7 Report. Hypertension. 2003; 42:
:2761-88, 2007. 63 Compelling Indications The JNC-7 Report. Hypertension. 2003; 42:1206-1252.")
32 AHA 2007 on initial therapy of uncomplicated hypertension AHA reports that actual BP lowering is more important than the choice of drug class for primary prevention AHA recommends starting with thiazide, ACE-I, ARB, or CCB American Heart Association: scientific statement Circulation. 115(21): , Compelling Indications The JNC-7 Report. Hypertension. 2003; 42:
33 Compelling Indications Ischemic Heart Disease Heart Failure Diabetes Chronic Kidney Disease BB (ACE-I also protective) ACE-I and BB ACE-I or ARB ACE-I or ARB The JNC-7 Report. Hypertension. 2003; 42: Principles of Drug Addition and Titration If initial drug is not tolerated or is contraindicated, use one of the other classes proven to cardiovascular events Many patients will require 2 drugs to attain BP goal. Second drug should be added when first drug, at proper dose, fails to reach goal Allow about 4 weeks to assess effect before adjusting dose or adding another drug The JNC-7 Report. Hypertension. 2003; 42:
34 Principles of Drug Addition and Titration If BP > 20/10 mmhg above goal (or stage 2) Initiate therapy with 2 drugs (one a thiazide) If not at max doses this may reduce adverse effects Use caution in those at risk of orthostatic hypotension If a drug or dose is failing, consider possible reasons before adding new agent Noncompliance The JNC-7 Report. Hypertension. 2003; 42: Follow-up and Monitoring Once drug therapy begins, f/u monthly until at goal BP Once stable, potassium and creatinine should be checked 1-2 times/year Once BP at goal, f/u every 3-6 months The JNC-7 Report. Hypertension. 2003; 42:

35 HTN in African-Americans Lifestyle modifications to salt intake Less responsive to BB, ACE-I, or ARB More responsive to diuretics or CCB Drug of choice = thiazide diuretic The JNC-7 Report. Hypertension. 2003; 42: JNC 7;
 71 JNC-8")
36 2014 Evidence-Based Guideline for the Management of High Blood Pressure in Adults Report From the Panel Members Appointed to the Eight Joint National Committee (JNC-8) 71 JNC-8 72
37 JNC-8 Expert panel originally for NHLBI JNC-8 Independently published with JAMA Currently not endorsed by organizations Not meant to be a comprehensive guideline for BP management Only used RTC 73 3 Critical Questions 1. In adults with HTN, does initiating antihypertensive pharmacologic therapy at specific BP thresholds improve health outcomes? 2. In adults with HTN, does treatment with antihypertensive pharmacologic therapy to a specific BP goal lead to improvements in health outcomes? 3. In adults with HTN, do various antihypertensive drugs or drug classes differ in comparative benefits and harms on specific health outcomes? 74 James. JAMA. Doi: /jama Published on December 18, 2013.
38 Findings No change in definition of HTN ( 140/90) Still emphasize Lifestyle Modifications 9 recommendations 1-5 address critical questions address critical question 3 9 addresses strategies of add-on therapy James. JAMA. Doi: /jama Published on December 18, Recommendation 1 60 years, treat to <150/90 Okay if gets to SBP <140 Reduces stroke, CHF, CHD No benefit targeting SBP <140 James. JAMA. Doi: /jama Published on December 18,
39 Recommendations 2 & 3: General population <60 years old Recommendation 3 Treat to SBP <140 Recommendation 2 Treat to DBP <90 Only expert opinion Keep current recommendation If DBP <90, usually also see SBP <140 It is a typical recommendation in JNC-8 Reduces CVA, CHF, overall mortality No benefit treating to DBP <80 or <85 James. JAMA. Doi: /jama Published on December 18, Recommendation 4 Adults with CKD, treat to <140/90 Not enough evidence to determine if there is benefit treating to a lower BP goal such as <130/80 James. JAMA. Doi: /jama Published on December 18,
40 Recommendation 5 Adults with diabetes, treat to <140/90 Treating to SBP <150 improves cardiovascular and cerebrovascular outcomes and lowers mortality No RCT address if treating to SBP <140 is better. Panel chose <140/90 to be consistent with their other recommendations 79 James. JAMA. Doi: /jama Published on December 18, Recommendation 6 Non-black population, with or without diabetes Initiate therapy with either: Thiazide-type diuretic CCB ACE-I ARB These classes have strong protective data Panel feels achieving control is more important than which agent was used to achieve it 80 James. JAMA. Doi: /jama Published on December 18, 2013.

41 Recommendation 6 cont Important points Many will require multiple drugs Any of these 4 classes are used for add-on therapy Thiazide-type diuretics include Thiazide diuretics Chlorthalidone Indapamide Strive to target doses used in RCT See table 4 James. JAMA. Doi: /jama Published on December 18, James. JAMA. Doi: /jama Published on December 18,
42 Recommendation 7 Black population, with or without diabetes Initiate therapy with either: Thiazide-type diuretic CCB Controversy: The ADA still recommends starting an ACE-I or ARB in anyone with diabetes James. JAMA. Doi: /jama Published on December 18, Recommendation 8 Adults with CKD and HTN (all ages and races with/without DM) Initiate therapy with either: ACE-I ARB James. JAMA. Doi: /jama Published on December 18,

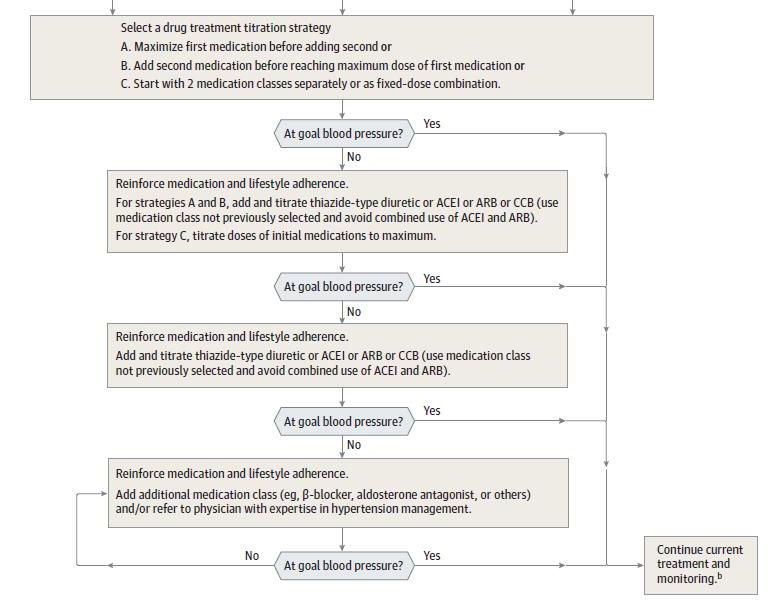
43 Conflict with 7 & 8 Controversy: Black patient with CKD Black patient with CKD with proteinuria ACE-I or ARB first line Black patient with CKD without proteinuria Start with either thiazide, CCB, ACE-I, or ARB Most patients with CKD and HTN will require multiple drugs; make sure an ACE-I or ARB is one of them James. JAMA. Doi: /jama Published on December 18, Recommendation 9 James. JAMA. Doi: /jama Published on December 18,
44 PJ is a 65 year old male with a history of HTN, arthritis and coronary artery disease. According to JNC 8, what is his goal BP? A. < 150/90 mmhg B. < 140/90 mmhg C. < 130/80 mmhg D. < 120/80 mmhg 87 JNC-8 BP Goals Age 60 years <150/90 Age <60 years <140/90 Diabetes <140/90 CKD <140/90 James. JAMA. Doi: /jama Published on December 18,
45 CC is a 55 year old African American male with HTN and diabetes. According to JNC 8, what drug should initially be used for HTN? A. Atenolol B. Amlodipine C. Lisinopril D. Valsartan 89 JNC-8 Initial Drug Recommendations Non-Black 60, <60, or with diabetes Black Thiazide-type diuretic, ACE-I, ARB, OR CCB 60, <60, or with diabetes CKD Thiazide-type diuretic OR CCB All ages, all races, with or without diabetes ACE-I OR ARB James. JAMA. Doi: /jama Published on December 18,

46 James. JAMA. Doi: /jama Published on December 18, James. JAMA. Doi: /jama Published on December 18,

47 Good Luck with That James. JAMA. Doi: /jama Published on December 18, Summary of Blood Pressure Guideline Differences JNC JNC 8 Blood pressure goals are low Goals based on comorbidities such as DM, CKD, CAD, or CHF Compelling indications for IHD, CHF, DM, CKD Blood pressure goals are not as low Goals based on age or comorbidities of DM or CKD (not CAD or CHF) Compelling indications for race and CKD 94
48 Highlights of the new blood pressure and cholesterol guidelines: A whole new philosophy Jeremy L. Johnson, PharmD, BCACP, CDE, BC-ADM OSHP 2014 Annual Meeting Oklahoma City, OK April 4, References Expert panel. Executive Summary of the Third Report of the National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III (ATP-III)). JAMA 2001; 285(19): Grundy SM, Cleeman JI, Bairey Merz CN, Brewer HB, Clark LT, Hunninghake DB, et al. Implications of Recent Clinical Trials for the National Cholesterol Education Program Adult Treatment Panel III Guidelines. Circulation. 2004;110: Ridker PM, Danielson E, Fonseca F, et al. Reduction in C-reactive protein and LDL cholesterol and cardiovascular event rates after initiation of rosuvastatin: a prospective study of the JUPITER trial. Lancet. 2009; 373: Brunzell JD, Davidson M, Furberg CD, et al. Diabetes Care 2008; 31: Stone NJ, Robinson J, Lichtenstein AH, Bairey Merz CN, et al ACC/AHA Guideline on the Treatment of Blood Cholesterol to Reduce Atherosclerotic Cardiovascular Risk in Adults. Journal of the American College of Cardiology. 2013:doi: /j.jacc The Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure. The Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure: The JNC-7 Report (Complete Version). Hypertension. 2003; 42: American Heart Association: scientific statement Circulation. 115(21): , James PA, Oparil S, Carter BL Evidence-Based Guideline for the Management of High Blood Pressure in Adults. Report From the Panel Members Appointed to the Eight Joint National Committee (JNC-8). JAMA. Doi: /jama Published on December 18,
4/7/ The stats on heart disease. + Deaths & Age-Adjusted Death Rates for
 + Update on Lipid Management Stacey Gardiner, MD Assistant Professor Division of Cardiovascular Medicine Medical College of Wisconsin + The stats on heart disease Over the past 10 years for which statistics
+ Update on Lipid Management Stacey Gardiner, MD Assistant Professor Division of Cardiovascular Medicine Medical College of Wisconsin + The stats on heart disease Over the past 10 years for which statistics
Dyslipidemia in the light of Current Guidelines - Do we change our Practice?
 Dyslipidemia in the light of Current Guidelines - Do we change our Practice? Dato Dr. David Chew Soon Ping Senior Consultant Cardiologist Institut Jantung Negara Atherosclerotic Cardiovascular Disease
Dyslipidemia in the light of Current Guidelines - Do we change our Practice? Dato Dr. David Chew Soon Ping Senior Consultant Cardiologist Institut Jantung Negara Atherosclerotic Cardiovascular Disease
How would you manage Ms. Gold
 How would you manage Ms. Gold 32 yo Asian woman with dyslipidemia Current medications: Simvastatin 20mg QD Most recent lipid profile: TC = 246, TG = 100, LDL = 176, HDL = 50 What about Mr. Williams? 56
How would you manage Ms. Gold 32 yo Asian woman with dyslipidemia Current medications: Simvastatin 20mg QD Most recent lipid profile: TC = 246, TG = 100, LDL = 176, HDL = 50 What about Mr. Williams? 56
Management of Lipid Disorders and Hypertension: Implications of the New Guidelines
 Management of Lipid Disorders and Hypertension Management of Lipid Disorders and Hypertension: Implications of the New Guidelines Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine
Management of Lipid Disorders and Hypertension Management of Lipid Disorders and Hypertension: Implications of the New Guidelines Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine
Speaker Disclosure. Pharmacist Objectives. Path to New Hypertension (HTN) Guidelines. Overview of New HTN Guidelines 8/21/2014
 Guidelines. Overview of New HTN Guidelines 8/21/2014") Speaker Disclosure Erica Pearce, Pharm.D. declares no conflicts of interest, real or apparent, and no financial interests in any company, product, or service mentioned in this program, including grants,
Speaker Disclosure Erica Pearce, Pharm.D. declares no conflicts of interest, real or apparent, and no financial interests in any company, product, or service mentioned in this program, including grants,
JNC Evidence-Based Guidelines for the Management of High Blood Pressure in Adults
 JNC 8 2014 Evidence-Based Guidelines for the Management of High Blood Pressure in Adults Table of Contents Why Do We Treat Hypertension? Blood Pressure Treatment Goals Initial Therapy Strength of Recommendation
JNC 8 2014 Evidence-Based Guidelines for the Management of High Blood Pressure in Adults Table of Contents Why Do We Treat Hypertension? Blood Pressure Treatment Goals Initial Therapy Strength of Recommendation
New Lipid Guidelines. PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN: Implications of the New Guidelines for Hypertension and Lipids.
 PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN: Implications of the New Guidelines for Hypertension and Lipids Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Disclosure No relevant
PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN: Implications of the New Guidelines for Hypertension and Lipids Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Disclosure No relevant
New Guidelines in Dyslipidemia Management
 The Fourth IAS-OSLA Course on Lipid Metabolism and Cardiovascular Risk Muscat, Oman, February 2018 New Guidelines in Dyslipidemia Management Dr. Khalid Al-Waili, MD, FRCPC, DABCL Senior Consultant Medical
The Fourth IAS-OSLA Course on Lipid Metabolism and Cardiovascular Risk Muscat, Oman, February 2018 New Guidelines in Dyslipidemia Management Dr. Khalid Al-Waili, MD, FRCPC, DABCL Senior Consultant Medical
Lipid Panel Management Refresher Course for the Family Physician
 Lipid Panel Management Refresher Course for the Family Physician Objectives Understand the evidence that was evaluated to develop the 2013 ACC/AHA guidelines Discuss the utility and accuracy of the new
Lipid Panel Management Refresher Course for the Family Physician Objectives Understand the evidence that was evaluated to develop the 2013 ACC/AHA guidelines Discuss the utility and accuracy of the new
2013 ACC/AHA Cholesterol Guidelines JULIE HAMMOND, D.O. PGY-2 MATTHEW PAOLI, D.O. PGY-2
 2013 ACC/AHA Cholesterol Guidelines JULIE HAMMOND, D.O. PGY-2 MATTHEW PAOLI, D.O. PGY-2 GOALS ACC/AHA as publisher of guidelines Determining which patients are appropriate for statin therapy The treatment
2013 ACC/AHA Cholesterol Guidelines JULIE HAMMOND, D.O. PGY-2 MATTHEW PAOLI, D.O. PGY-2 GOALS ACC/AHA as publisher of guidelines Determining which patients are appropriate for statin therapy The treatment
New Guidelines in Dyslipidemia Management
 The Third IAS-OSLA Course on Lipid Metabolism and Cardiovascular Risk Muscat, Oman, February 2017 New Guidelines in Dyslipidemia Management Dr. Khalid Al-Waili, MD, FRCPC, DABCL Senior Consultant Medical
The Third IAS-OSLA Course on Lipid Metabolism and Cardiovascular Risk Muscat, Oman, February 2017 New Guidelines in Dyslipidemia Management Dr. Khalid Al-Waili, MD, FRCPC, DABCL Senior Consultant Medical
Acute Coronary Syndromes (ACS)
") Sally A. Arif, Pharm.D., BCPS (AQ Cardiology) Assistant Professor of Pharmacy Practice Midwestern University, Chicago College of Pharmacy Cardiology Clinical Specialist, Rush University Medical Center
Sally A. Arif, Pharm.D., BCPS (AQ Cardiology) Assistant Professor of Pharmacy Practice Midwestern University, Chicago College of Pharmacy Cardiology Clinical Specialist, Rush University Medical Center
Learning Objectives. Patient Case
 Joseph Saseen, Pharm.D., FASHP, FCCP, BCPS Professor and Vice Chair, Department of Clinical Pharmacy University of Colorado Anschutz Medical Campus Learning Objectives Identify the 4 patient populations
Joseph Saseen, Pharm.D., FASHP, FCCP, BCPS Professor and Vice Chair, Department of Clinical Pharmacy University of Colorado Anschutz Medical Campus Learning Objectives Identify the 4 patient populations
Pharmacy Drug Class Review
 Pharmacy Drug Class Review January 22, 2014 Authored By: Christina Manciocchi, Pharm.D. BCACP Disclaimer: Specific agents may have variations Edited By: Richard J. Kraft, Pharm.D.BCPS NEW CHOLESTEROL GUIDELINES
Pharmacy Drug Class Review January 22, 2014 Authored By: Christina Manciocchi, Pharm.D. BCACP Disclaimer: Specific agents may have variations Edited By: Richard J. Kraft, Pharm.D.BCPS NEW CHOLESTEROL GUIDELINES
New Cholesterol Guidelines What the LDL are we supposed to do now?!
 New Cholesterol Guidelines What the LDL are we supposed to do now?! Michael D. Shapiro Assistant Professor of Medicine and Radiology Knight Cardiovascular Institute Oregon Health & Science University 2013
New Cholesterol Guidelines What the LDL are we supposed to do now?! Michael D. Shapiro Assistant Professor of Medicine and Radiology Knight Cardiovascular Institute Oregon Health & Science University 2013
Conflict of Interest Disclosure. Learning Objectives. Learning Objectives. Guidelines. Update on Lifestyle Guidelines
 Conflict of Interest Disclosure Updates for the Ambulatory Care Pharmacist: Dyslipidemia and CV Risk Assessment No conflicts of interest to disclose 2014 Updates to the Updates in Ambulatory Care Pharmacy
Conflict of Interest Disclosure Updates for the Ambulatory Care Pharmacist: Dyslipidemia and CV Risk Assessment No conflicts of interest to disclose 2014 Updates to the Updates in Ambulatory Care Pharmacy
2013 ACC AHA LIPID GUIDELINE JAY S. FONTE, MD
 2013 ACC AHA LIPID GUIDELINE JAY S. FONTE, MD How do you interpret my blood test results? What are our targets for these tests? Before the ACC/AHA Lipid Guidelines A1c:
2013 ACC AHA LIPID GUIDELINE JAY S. FONTE, MD How do you interpret my blood test results? What are our targets for these tests? Before the ACC/AHA Lipid Guidelines A1c:
HYPERLIPIDEMIA IN THE OLDER POPULATION NICOLE SLATER, PHARMD, BCACP AUBURN UNIVERSITY, HARRISON SCHOOL OF PHARMACY JULY 16, 2016
 HYPERLIPIDEMIA IN THE OLDER POPULATION NICOLE SLATER, PHARMD, BCACP AUBURN UNIVERSITY, HARRISON SCHOOL OF PHARMACY JULY 16, 2016 NOTHING TO DISCLOSE I, Nicole Slater, have no actual or potential conflict
HYPERLIPIDEMIA IN THE OLDER POPULATION NICOLE SLATER, PHARMD, BCACP AUBURN UNIVERSITY, HARRISON SCHOOL OF PHARMACY JULY 16, 2016 NOTHING TO DISCLOSE I, Nicole Slater, have no actual or potential conflict
Cholesterol Management Roy Gandolfi, MD
 Cholesterol Management 2017 Roy Gandolfi, MD Goals Interpreting cholesterol guidelines Cholesterol treatment in diabetics Statin use and side effects therapy Reporting- Comparison data among physicians
Cholesterol Management 2017 Roy Gandolfi, MD Goals Interpreting cholesterol guidelines Cholesterol treatment in diabetics Statin use and side effects therapy Reporting- Comparison data among physicians
2019 Update on Recent Guideline Releases for Diabetes, Hypertension, and Dyslipidemia: Can We, Please, All Just Get on the Same Page?!
 2019 Update on Recent Guideline Releases for Diabetes, Hypertension, and Dyslipidemia: Can We, Please, All Just Get on the Same Page?! Jeremy L. Johnson, PharmD, BCACP, CDE, BC-ADM Assistant Professor,
2019 Update on Recent Guideline Releases for Diabetes, Hypertension, and Dyslipidemia: Can We, Please, All Just Get on the Same Page?! Jeremy L. Johnson, PharmD, BCACP, CDE, BC-ADM Assistant Professor,
DISCLOSURE PHARMACIST OBJECTIVES 9/30/2014 JNC 8: A REVIEW OF THE LONG-AWAITED/MUCH-ANTICIPATED HYPERTENSION GUIDELINES. I have nothing to disclose.
 JNC 8: A REVIEW OF THE LONG-AWAITED/MUCH-ANTICIPATED HYPERTENSION GUIDELINES Tiffany Dickey, PharmD Assistant Professor, UAMS COP Clinical Pharmacy Specialist, Mercy Hospital Northwest AR DISCLOSURE I
JNC 8: A REVIEW OF THE LONG-AWAITED/MUCH-ANTICIPATED HYPERTENSION GUIDELINES Tiffany Dickey, PharmD Assistant Professor, UAMS COP Clinical Pharmacy Specialist, Mercy Hospital Northwest AR DISCLOSURE I
Long-Term Complications of Diabetes Mellitus Macrovascular Complication
 Long-Term Complications of Diabetes Mellitus Macrovascular Complication Sung Hee Choi MD, PhD Professor, Seoul National University College of Medicine, SNUBH, Bundang Hospital Diabetes = CVD equivalent
Long-Term Complications of Diabetes Mellitus Macrovascular Complication Sung Hee Choi MD, PhD Professor, Seoul National University College of Medicine, SNUBH, Bundang Hospital Diabetes = CVD equivalent
Andrew Cohen, MD and Neil S. Skolnik, MD INTRODUCTION
 2 Hyperlipidemia Andrew Cohen, MD and Neil S. Skolnik, MD CONTENTS INTRODUCTION RISK CATEGORIES AND TARGET LDL-CHOLESTEROL TREATMENT OF LDL-CHOLESTEROL SPECIAL CONSIDERATIONS OLDER AND YOUNGER ADULTS ADDITIONAL
2 Hyperlipidemia Andrew Cohen, MD and Neil S. Skolnik, MD CONTENTS INTRODUCTION RISK CATEGORIES AND TARGET LDL-CHOLESTEROL TREATMENT OF LDL-CHOLESTEROL SPECIAL CONSIDERATIONS OLDER AND YOUNGER ADULTS ADDITIONAL
The Latest Generation of Clinical
 The Latest Generation of Clinical Guidelines: HTN and HLD Dave Brackett Clinical Guideline Purpose Uniform approach Awareness of key details Diagnosis Treatment Monitoring Evidence based approach Inform
The Latest Generation of Clinical Guidelines: HTN and HLD Dave Brackett Clinical Guideline Purpose Uniform approach Awareness of key details Diagnosis Treatment Monitoring Evidence based approach Inform
Updates in Cardiovascular Recommendations for Diabetic Patients
 Updates in Cardiovascular Recommendations for Diabetic Patients Chris Tawwater, Pharm.D., BCPS Clinical Pharmacist, Abilene Regional Medical Center Assistant Professor, Adult Medicine Division Pharmacotherapy
Updates in Cardiovascular Recommendations for Diabetic Patients Chris Tawwater, Pharm.D., BCPS Clinical Pharmacist, Abilene Regional Medical Center Assistant Professor, Adult Medicine Division Pharmacotherapy
Hypertension Update Clinical Controversies Regarding Age and Race
 Hypertension Update Clinical Controversies Regarding Age and Race Allison Helmer, PharmD, BCACP Assistant Clinical Professor Auburn University Harrison School of Pharmacy July 22, 2017 DISCLOSURE/CONFLICT
Hypertension Update Clinical Controversies Regarding Age and Race Allison Helmer, PharmD, BCACP Assistant Clinical Professor Auburn University Harrison School of Pharmacy July 22, 2017 DISCLOSURE/CONFLICT
ATP IV: Predicting Guideline Updates
 Disclosures ATP IV: Predicting Guideline Updates Daniel M. Riche, Pharm.D., BCPS, CDE Speaker s Bureau Merck Janssen Boehringer-Ingelheim Learning Objectives Describe at least two evidence-based recommendations
Disclosures ATP IV: Predicting Guideline Updates Daniel M. Riche, Pharm.D., BCPS, CDE Speaker s Bureau Merck Janssen Boehringer-Ingelheim Learning Objectives Describe at least two evidence-based recommendations
Applying the Intricacies of the New Hypertension and Lipid Guidelines to Your Patients
 Applying the Intricacies of the New Hypertension and Lipid Guidelines to Your Patients Joe Anderson, PharmD, PhC, BCPS James Nawarskas, PharmD, PhC, BCPS Gretchen Ray, PharmD, PhC, BCACP University of
Applying the Intricacies of the New Hypertension and Lipid Guidelines to Your Patients Joe Anderson, PharmD, PhC, BCPS James Nawarskas, PharmD, PhC, BCPS Gretchen Ray, PharmD, PhC, BCACP University of
Conflicts of interest. What's the Skinny on the Lipid Guidelines? Key Differences. Are you applying the new ACC/AHA Lipid guidelines in your practice?
 Conflicts of interest What's the Skinny on the Lipid Guidelines? The presenter has no relevant conflicts of interest to disclose. Kathleen Vest, PharmD, CDE, BCACP At the end of this presentation, pharmacist
Conflicts of interest What's the Skinny on the Lipid Guidelines? The presenter has no relevant conflicts of interest to disclose. Kathleen Vest, PharmD, CDE, BCACP At the end of this presentation, pharmacist
2013 Cholesterol Guidelines. Anna Broz MSN, RN, CNP, AACC Adult Certified Nurse Practitioner North Ohio Heart, Inc.
 2013 Cholesterol Guidelines Anna Broz MSN, RN, CNP, AACC Adult Certified Nurse Practitioner North Ohio Heart, Inc. Disclosures Speaker Gilead Sciences NHLBI Charge to the Expert Panel Evaluate higher quality
2013 Cholesterol Guidelines Anna Broz MSN, RN, CNP, AACC Adult Certified Nurse Practitioner North Ohio Heart, Inc. Disclosures Speaker Gilead Sciences NHLBI Charge to the Expert Panel Evaluate higher quality
4/24/15. AHA/ACC 2013 Guideline Key Points
 Review of the ACC/AHA 2013 Guidelines Anita Ralstin, MS, CNS, CNP Next Step Health Consultant, LLC 1! Discuss the rationale for the change in lipid guidelines and how that affects the decision to implement
Review of the ACC/AHA 2013 Guidelines Anita Ralstin, MS, CNS, CNP Next Step Health Consultant, LLC 1! Discuss the rationale for the change in lipid guidelines and how that affects the decision to implement
Update in Cardiology Pharmacologic Management of Cardiovascular Risk. Christopher C. Roe, MSN, ACNP
 Update in Cardiology Pharmacologic Management of Cardiovascular Risk Christopher C. Roe, MSN, ACNP Objectives 1. Verbalize understanding of new pharmacologic guidelines in the treatment of hypertension
Update in Cardiology Pharmacologic Management of Cardiovascular Risk Christopher C. Roe, MSN, ACNP Objectives 1. Verbalize understanding of new pharmacologic guidelines in the treatment of hypertension
Introduction. Objective. Critical Questions Addressed
 Introduction Objective To provide a strong evidence-based foundation for the treatment of cholesterol for the primary and secondary prevention of ASCVD in women and men Critical Questions Addressed CQ1:
Introduction Objective To provide a strong evidence-based foundation for the treatment of cholesterol for the primary and secondary prevention of ASCVD in women and men Critical Questions Addressed CQ1:
PIEDMONT ACCESS TO HEALTH SERVICES, INC. Guidelines for Screening and Management of Dyslipidemia
 PIEDMONT ACCESS TO HEALTH SERVICES, INC. Policy Number: 01-09-021 SUBJECT: Guidelines for Screening and Management of Dyslipidemia EFFECTIVE DATE: 04/2008 REVIEWED/REVISED: 04/12/10, 03/17/2011, 4/10/2012,
PIEDMONT ACCESS TO HEALTH SERVICES, INC. Policy Number: 01-09-021 SUBJECT: Guidelines for Screening and Management of Dyslipidemia EFFECTIVE DATE: 04/2008 REVIEWED/REVISED: 04/12/10, 03/17/2011, 4/10/2012,
No relevant financial relationships
 MANAGEMENT OF LIPID DISORDERS Balancing Benefits and harms Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial relationships baron@medicine.ucsf.edu
MANAGEMENT OF LIPID DISORDERS Balancing Benefits and harms Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial relationships baron@medicine.ucsf.edu
Disclosure. No relevant financial relationships. Placebo-Controlled Statin Trials
 PREVENTING CARDIOVASCULAR DISEASE IN WOMEN: Current Guidelines for Hypertension, Lipids and Aspirin Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial
PREVENTING CARDIOVASCULAR DISEASE IN WOMEN: Current Guidelines for Hypertension, Lipids and Aspirin Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial
Int. J. Pharm. Sci. Rev. Res., 36(1), January February 2016; Article No. 06, Pages: JNC 8 versus JNC 7 Understanding the Evidences
, January February 2016; Article No. 06, Pages: JNC 8 versus JNC 7 Understanding the Evidences") Research Article JNC 8 versus JNC 7 Understanding the Evidences Anns Clara Joseph, Karthik MS, Sivasakthi R, Venkatanarayanan R, Sam Johnson Udaya Chander J* RVS College of Pharmaceutical Sciences, Coimbatore,
Research Article JNC 8 versus JNC 7 Understanding the Evidences Anns Clara Joseph, Karthik MS, Sivasakthi R, Venkatanarayanan R, Sam Johnson Udaya Chander J* RVS College of Pharmaceutical Sciences, Coimbatore,
MOLINA HEALTHCARE OF CALIFORNIA
 MOLINA HEALTHCARE OF CALIFORNIA HIGH BLOOD CHOLESTEROL IN ADULTS GUIDELINE Molina Healthcare of California has adopted the Third Report of the National Cholesterol Education Program (NCEP) Expert Panel
MOLINA HEALTHCARE OF CALIFORNIA HIGH BLOOD CHOLESTEROL IN ADULTS GUIDELINE Molina Healthcare of California has adopted the Third Report of the National Cholesterol Education Program (NCEP) Expert Panel
Dyslipedemia New Guidelines
 Dyslipedemia New Guidelines New ACC/AHA Prevention Guidelines on Blood Cholesterol November 12, 2013 Mohammed M Abd El Ghany Professor of Cardiology Cairo Universlty 1 1 0 Cholesterol Management Pharmacotherapy
Dyslipedemia New Guidelines New ACC/AHA Prevention Guidelines on Blood Cholesterol November 12, 2013 Mohammed M Abd El Ghany Professor of Cardiology Cairo Universlty 1 1 0 Cholesterol Management Pharmacotherapy
Disclosures No relationships (not even to an employer) No off-label uses. Cholesterol Lowering Guidelines: What now?
 No off-label uses. Cholesterol Lowering Guidelines: What now?") Disclosures No relationships (not even to an employer) No off-label uses Cholesterol Lowering Guidelines: What now?, FACP 1 2 65-year-old white woman Total cholesterol 175mg/dL HDL 54 mg/dl LDL 96 mg/dl
Disclosures No relationships (not even to an employer) No off-label uses Cholesterol Lowering Guidelines: What now?, FACP 1 2 65-year-old white woman Total cholesterol 175mg/dL HDL 54 mg/dl LDL 96 mg/dl
Egyptian Hypertension Guidelines
 Egyptian Hypertension Guidelines 2014 Egyptian Hypertension Guidelines Dalia R. ElRemissy, MD Lecturer of Cardiovascular Medicine Cairo University Why Egyptian Guidelines? Guidelines developed for rich
Egyptian Hypertension Guidelines 2014 Egyptian Hypertension Guidelines Dalia R. ElRemissy, MD Lecturer of Cardiovascular Medicine Cairo University Why Egyptian Guidelines? Guidelines developed for rich
Prevention of Heart Disease: The New Guidelines
 Prevention of Heart Disease: The New Guidelines Nisha I. Parikh MD MPH Assistant Professor of Medicine Division of Cardiology Department of Medicine University of California San Francisco May 18 th 2015
Prevention of Heart Disease: The New Guidelines Nisha I. Parikh MD MPH Assistant Professor of Medicine Division of Cardiology Department of Medicine University of California San Francisco May 18 th 2015
New Recommendations for the Treatment of Hypertension: From Population Salt Reduction to Personalized Treatment Targets
 New Recommendations for the Treatment of Hypertension: From Population Salt Reduction to Personalized Treatment Targets Sidney C. Smith, Jr. MD, FACC, FAHA Professor of Medicine/Cardiology University of
New Recommendations for the Treatment of Hypertension: From Population Salt Reduction to Personalized Treatment Targets Sidney C. Smith, Jr. MD, FACC, FAHA Professor of Medicine/Cardiology University of
ALLHAT. Major Outcomes in High Risk Hypertensive Patients Randomized to Angiotensin-Converting Enzyme Inhibitor or Calcium Channel Blocker vs Diuretic
 1 U.S. Department of Health and Human Services National Institutes of Health Major Outcomes in High Risk Hypertensive Patients Randomized to Angiotensin-Converting Enzyme Inhibitor or Calcium Channel Blocker
1 U.S. Department of Health and Human Services National Institutes of Health Major Outcomes in High Risk Hypertensive Patients Randomized to Angiotensin-Converting Enzyme Inhibitor or Calcium Channel Blocker
Hypertension. Does it Matter What Medications We Use? Nishant K. Sekaran, M.D. M.Sc. Intermountain Heart Institute
 Hypertension Does it Matter What Medications We Use? Nishant K. Sekaran, M.D. M.Sc. Intermountain Heart Institute Hypertension 2017 Classification BP Category Systolic Diastolic Normal 120 and 80 Elevated
Hypertension Does it Matter What Medications We Use? Nishant K. Sekaran, M.D. M.Sc. Intermountain Heart Institute Hypertension 2017 Classification BP Category Systolic Diastolic Normal 120 and 80 Elevated
Diabetes: Use of Adjunctive Therapy ACEs, ARBs, ASA & STATINs --Oh My! Veronica J. Brady, PhD, FNP-BC, BC-ADM, CDE Project ECHO April 19, 2018
 Diabetes: Use of Adjunctive Therapy ACEs, ARBs, ASA & STATINs --Oh My! Veronica J. Brady, PhD, FNP-BC, BC-ADM, CDE Project ECHO April 19, 2018 Points to Ponder ASCVD is the leading cause of morbidity
Diabetes: Use of Adjunctive Therapy ACEs, ARBs, ASA & STATINs --Oh My! Veronica J. Brady, PhD, FNP-BC, BC-ADM, CDE Project ECHO April 19, 2018 Points to Ponder ASCVD is the leading cause of morbidity
JNC 8 -Controversies. Sagren Naidoo Nephrologist CMJAH
 JNC 8 -Controversies Sagren Naidoo Nephrologist CMJAH Joint National Committee (JNC) Panel appointed by the National Heart, Lung, and Blood Institute (NHLBI) First guidelines (JNC-1) published in 1977
JNC 8 -Controversies Sagren Naidoo Nephrologist CMJAH Joint National Committee (JNC) Panel appointed by the National Heart, Lung, and Blood Institute (NHLBI) First guidelines (JNC-1) published in 1977
Blood Pressure LIMBO How Low To Go?
 Blood Pressure LIMBO How Low To Go? Joseph L. Kummer, MD, FACC Bryan Heart Spring Conference April 21 st, 2018 Hypertension Epidemiology Over a billion people have hypertension Major cause of morbidity
Blood Pressure LIMBO How Low To Go? Joseph L. Kummer, MD, FACC Bryan Heart Spring Conference April 21 st, 2018 Hypertension Epidemiology Over a billion people have hypertension Major cause of morbidity
ADVANCES IN MANAGEMENT OF HYPERTENSION
 Advances in Management of Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Current Status of Prevalence 29%; Blacks 33.5%
Advances in Management of Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Current Status of Prevalence 29%; Blacks 33.5%
Vincent J. Caracciolo, MD FACC FOMA May 2014
 Vincent J. Caracciolo, MD FACC FOMA May 2014 Goals of the Guidelines National Heart, lung and Blood Institute ( NHLBI) collaborated with ACC/AHA to develop guidelines a.) assess CV risk, b.) lifestyle
Vincent J. Caracciolo, MD FACC FOMA May 2014 Goals of the Guidelines National Heart, lung and Blood Institute ( NHLBI) collaborated with ACC/AHA to develop guidelines a.) assess CV risk, b.) lifestyle
Disclosures. Overview 9/30/ ACC/AHA Guidelines on the Treatment of Blood Cholesterol to Reduce Atherosclerotic Cardiovascular Risk in Adults
 2013 ACC/AHA Guidelines on the Treatment of Blood Cholesterol to Reduce Atherosclerotic Cardiovascular Risk in Adults 2014 AAHP Fall Seminar Sherry Myatt, PharmD, BCPS Assistant Director of Pharmacy for
2013 ACC/AHA Guidelines on the Treatment of Blood Cholesterol to Reduce Atherosclerotic Cardiovascular Risk in Adults 2014 AAHP Fall Seminar Sherry Myatt, PharmD, BCPS Assistant Director of Pharmacy for
Disclosure. No relevant financial relationships. Placebo-Controlled Statin Trials
 MANAGEMENT OF HYPERLIPIDEMIA AND CARDIOVASCULAR RISK IN WOMEN: Balancing Benefits and Harms Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial
MANAGEMENT OF HYPERLIPIDEMIA AND CARDIOVASCULAR RISK IN WOMEN: Balancing Benefits and Harms Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial
Lipids & Hypertension Update
 Lipids & Hypertension Update No financial disclosures Michael W. Cullen, MD, FACC Senior Associate Consultant, Assistant Professor of Medicine Mayo Clinic Department of Cardiovascular Diseases 34 th Annual
Lipids & Hypertension Update No financial disclosures Michael W. Cullen, MD, FACC Senior Associate Consultant, Assistant Professor of Medicine Mayo Clinic Department of Cardiovascular Diseases 34 th Annual
Lipid Management: The Next Level How Will the New ACC/AHA Guidelines Change My Practice
 Lipid Management: The Next Level How Will the New ACC/AHA Guidelines Change My Practice Vera Bittner, MD, MSPH Professor of Medicine Section Head, Preventive Cardiology Medical Director, Cardiac Rehabilitation
Lipid Management: The Next Level How Will the New ACC/AHA Guidelines Change My Practice Vera Bittner, MD, MSPH Professor of Medicine Section Head, Preventive Cardiology Medical Director, Cardiac Rehabilitation
Hypertension JNC 8 (2014)
") Hypertension JNC 8 (2014) Renewed: February 2018 Updated: February 2015 Comparison of Seventh Joint National Committee (JNC 7) vs. Eighth Joint National Committee (JNC 8) Hypertension Guidelines Methodology
Hypertension JNC 8 (2014) Renewed: February 2018 Updated: February 2015 Comparison of Seventh Joint National Committee (JNC 7) vs. Eighth Joint National Committee (JNC 8) Hypertension Guidelines Methodology
Antihypertensive Trial Design ALLHAT
 1 U.S. Department of Health and Human Services Major Outcomes in High Risk Hypertensive Patients Randomized to Angiotensin-Converting Enzyme Inhibitor or Calcium Channel Blocker vs Diuretic National Institutes
1 U.S. Department of Health and Human Services Major Outcomes in High Risk Hypertensive Patients Randomized to Angiotensin-Converting Enzyme Inhibitor or Calcium Channel Blocker vs Diuretic National Institutes
Pharmaceutical Help to Control Cholesterol
 Pharmaceutical Help to Control Cholesterol Catherine E. Cooke, PharmD, BCPS, PAHM President, PosiHealth, Inc. Clinical Associate Professor, Univ. of Maryland This program has been brought to you by PharmCon
Pharmaceutical Help to Control Cholesterol Catherine E. Cooke, PharmD, BCPS, PAHM President, PosiHealth, Inc. Clinical Associate Professor, Univ. of Maryland This program has been brought to you by PharmCon
Lipid Therapy: Statins and Beyond. Ivan Anderson, MD RIHVH Cardiology
 Lipid Therapy: Statins and Beyond Ivan Anderson, MD RIHVH Cardiology Outline The cholesterol hypothesis and lipid metabolism The Guidelines 4 Groups that Benefit from Lipid therapy Initiation and monitoring
Lipid Therapy: Statins and Beyond Ivan Anderson, MD RIHVH Cardiology Outline The cholesterol hypothesis and lipid metabolism The Guidelines 4 Groups that Benefit from Lipid therapy Initiation and monitoring
VA/DoD Clinical Practice Guideline for the Diagnosis and Management of Hypertension - Pocket Guide Update 2004 Revision July 2005
 VA/DoD Clinical Practice Guideline for the Diagnosis and Management of Hypertension - Pocket Guide Update 2004 Revision July 2005 1 Any adult in the health care system 2 Obtain blood pressure (BP) (Reliable,
VA/DoD Clinical Practice Guideline for the Diagnosis and Management of Hypertension - Pocket Guide Update 2004 Revision July 2005 1 Any adult in the health care system 2 Obtain blood pressure (BP) (Reliable,
Long-Term Care Updates
 Long-Term Care Updates August 2015 By Darren Hein, PharmD Hypertension is a clinical condition in which the force of blood pushing on the arteries is higher than normal. This increases the risk for heart
Long-Term Care Updates August 2015 By Darren Hein, PharmD Hypertension is a clinical condition in which the force of blood pushing on the arteries is higher than normal. This increases the risk for heart
An update on lipidology and cardiovascular risk management. Lipids, Metabolism & Vascular Risk Section - Royal Society of Medicine
 An update on lipidology and cardiovascular risk management Lipids, Metabolism & Vascular Risk Section - Royal Society of Medicine National and international lipid modification guidelines: A critical appraisal
An update on lipidology and cardiovascular risk management Lipids, Metabolism & Vascular Risk Section - Royal Society of Medicine National and international lipid modification guidelines: A critical appraisal
Disclosures. Prevention of Heart Disease: The New Guidelines. Summary of Talk. Four guidelines. No relevant disclosures.
 Disclosures Prevention of Heart Disease: The New Guidelines No relevant disclosures Nisha I. Parikh MD MPH Assistant Professor of Medicine Division of Cardiology Department of Medicine University of California
Disclosures Prevention of Heart Disease: The New Guidelines No relevant disclosures Nisha I. Parikh MD MPH Assistant Professor of Medicine Division of Cardiology Department of Medicine University of California
Hyperlipidemia: Lowering the Bar on the Lipid Limbo. Community Faculty Development Symposium March 13, 2004 Hugh Huizenga MD, MPH
 Mark slides Hyperlipidemia: Lowering the Bar on the Lipid Limbo Community Faculty Development Symposium March 13, 2004 Hugh Huizenga MD, MPH Hyperlipidemia is a common problem Nearly 50% of men in the
Mark slides Hyperlipidemia: Lowering the Bar on the Lipid Limbo Community Faculty Development Symposium March 13, 2004 Hugh Huizenga MD, MPH Hyperlipidemia is a common problem Nearly 50% of men in the
2013 Cholesterol Guidelines. Anna Broz MSN, RN, CNP, AACC Cer=fied Adult Nurse Prac==oner North Ohio Heart, Inc.
 2013 Cholesterol Guidelines Anna Broz MSN, RN, CNP, AACC Cer=fied Adult Nurse Prac==oner North Ohio Heart, Inc. Disclosures Speaker Gilead Sciences NHLBI Charge to the Expert Panel Evaluate higher quality
2013 Cholesterol Guidelines Anna Broz MSN, RN, CNP, AACC Cer=fied Adult Nurse Prac==oner North Ohio Heart, Inc. Disclosures Speaker Gilead Sciences NHLBI Charge to the Expert Panel Evaluate higher quality
Placebo-Controlled Statin Trials Prevention Of CVD in Women"
 MANAGEMENT OF HIGH BLOOD CHOLESTEROL: IMPLICATIONS OF THE NEW GUIDELINES Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest
MANAGEMENT OF HIGH BLOOD CHOLESTEROL: IMPLICATIONS OF THE NEW GUIDELINES Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest
A New Age of Dyslipidemia Treatment: Role of Non- Statin Therapies
 A New Age of Dyslipidemia Treatment: Role of Non- Statin Therapies BRODY MAACK, PHARMD, BCACP, CTTS Objectives 1. Review current guidelines regarding use of statin medications in the treatment and prevention
A New Age of Dyslipidemia Treatment: Role of Non- Statin Therapies BRODY MAACK, PHARMD, BCACP, CTTS Objectives 1. Review current guidelines regarding use of statin medications in the treatment and prevention
Disclosures. Diabetes and Cardiovascular Risk Management. Learning Objectives. Atherosclerotic Cardiovascular Disease
 Disclosures Diabetes and Cardiovascular Risk Management Tony Hampton, MD, MBA Medical Director Advocate Aurora Operating System Advocate Aurora Healthcare Downers Grove, IL No conflicts or disclosures
Disclosures Diabetes and Cardiovascular Risk Management Tony Hampton, MD, MBA Medical Director Advocate Aurora Operating System Advocate Aurora Healthcare Downers Grove, IL No conflicts or disclosures
Update on Lipid Management in Cardiovascular Disease: How to Understand and Implement the New ACC/AHA Guidelines
 Update on Lipid Management in Cardiovascular Disease: How to Understand and Implement the New ACC/AHA Guidelines Paul Mahoney, MD Sentara Cardiology Specialists Lipid Management in Cardiovascular Disease
Update on Lipid Management in Cardiovascular Disease: How to Understand and Implement the New ACC/AHA Guidelines Paul Mahoney, MD Sentara Cardiology Specialists Lipid Management in Cardiovascular Disease
ADVANCES IN MANAGEMENT OF HYPERTENSION
 Prevalence 29%; Blacks 33.5% About 72.5% treated; 53.5% uncontrolled (>140/90) Risk for poor control: Latinos, Blacks, age 18-44 and 80,
Prevalence 29%; Blacks 33.5% About 72.5% treated; 53.5% uncontrolled (>140/90) Risk for poor control: Latinos, Blacks, age 18-44 and 80,
Placebo-Controlled Statin Trials MANAGEMENT OF HIGH BLOOD CHOLESTEROL MANAGEMENT OF HIGH BLOOD CHOLESTEROL: IMPLICATIONS OF THE NEW GUIDELINES
 MANAGEMENT OF HIGH BLOOD CHOLESTEROL: IMPLICATIONS OF THE NEW GUIDELINES Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest
MANAGEMENT OF HIGH BLOOD CHOLESTEROL: IMPLICATIONS OF THE NEW GUIDELINES Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest
Lipid Management 2013 Statin Benefit Groups
 Clinical Integration Steering Committee Clinical Integration Chronic Disease Management Work Group Lipid Management 2013 Statin Benefit Groups Approved by Board Chair Signature Name (Please Print) Date
Clinical Integration Steering Committee Clinical Integration Chronic Disease Management Work Group Lipid Management 2013 Statin Benefit Groups Approved by Board Chair Signature Name (Please Print) Date
Using the New Hypertension Guidelines
 Using the New Hypertension Guidelines Kamal Henderson, MD Department of Cardiology, Preventive Medicine, University of North Carolina School of Medicine Kotchen TA. Historical trends and milestones in
Using the New Hypertension Guidelines Kamal Henderson, MD Department of Cardiology, Preventive Medicine, University of North Carolina School of Medicine Kotchen TA. Historical trends and milestones in
Objec ves To discuss the process of formulation of guidelines and how this may differ among professional societies 5/14/15
 Kellie McLain, NP- C, CLS Medical University of South Carolina Cardiology Division Seinsheimer Cardiovascular Prevention and Lipid Program May 29 th, 2015 Objecves To discuss the process of formulation
Kellie McLain, NP- C, CLS Medical University of South Carolina Cardiology Division Seinsheimer Cardiovascular Prevention and Lipid Program May 29 th, 2015 Objecves To discuss the process of formulation
No relevant financial relationships
 MANAGEMENT OF LIPID DISORDERS: WHERE DO WE STAND WITH THE NEW PRACTICE GUIDELINES? Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Disclosure No relevant financial relationships
MANAGEMENT OF LIPID DISORDERS: WHERE DO WE STAND WITH THE NEW PRACTICE GUIDELINES? Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Disclosure No relevant financial relationships
Managing Hypertension in 2016
 Managing Hypertension in 2016: Where Do We Draw the Line? Disclosure No relevant financial relationships Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine baron@medicine.ucsf.edu
Managing Hypertension in 2016: Where Do We Draw the Line? Disclosure No relevant financial relationships Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine baron@medicine.ucsf.edu
DYSLIPIDEMIA TREATMENT: HYBRIDIZING CLINICAL PRACTICE GUIDELINES
 DYSLIPIDEMIA TREATMENT: HYBRIDIZING CLINICAL PRACTICE GUIDELINES SATURDAY/4:30-5:30PM ACPE UAN: 0107-9999-17-249-L01-P 0.1 CEU/1.0 hr Activity Type: Knowledge-Based Learning Objectives for Pharmacists:
DYSLIPIDEMIA TREATMENT: HYBRIDIZING CLINICAL PRACTICE GUIDELINES SATURDAY/4:30-5:30PM ACPE UAN: 0107-9999-17-249-L01-P 0.1 CEU/1.0 hr Activity Type: Knowledge-Based Learning Objectives for Pharmacists:
Hypertension Guidelines: JNC- Late, JNC- 8, or JNC- Fake?
 Hypertension Guidelines: JNC- Late, JNC- 8, or JNC- Fake? Brian G. Choi, MD, MBA, FACC Associate Professor of Medicine Co-Director, Advanced Cardiac Imaging November 14, 2014 Washington, DC Disclosures
Hypertension Guidelines: JNC- Late, JNC- 8, or JNC- Fake? Brian G. Choi, MD, MBA, FACC Associate Professor of Medicine Co-Director, Advanced Cardiac Imaging November 14, 2014 Washington, DC Disclosures
What do the guidelines say about combination therapy?
 What do the guidelines say about combination therapy? Christie M. Ballantyne, MD Center for Cardiovascular Disease Prevention Methodist DeBakey Heart & Vascular Center Baylor College of Medicine Houston,
What do the guidelines say about combination therapy? Christie M. Ballantyne, MD Center for Cardiovascular Disease Prevention Methodist DeBakey Heart & Vascular Center Baylor College of Medicine Houston,
Hypertension in 2015: SPRINT-ing ahead of JNC-8. MAJ Charles Magee, MD MPH FACP Director, WRNMMC Hypertension Clinic
 Hypertension in 2015: SPRINT-ing ahead of JNC-8 MAJ Charles Magee, MD MPH FACP Director, WRNMMC Hypertension Clinic Conflits of interest? None Disclaimer The opinions contained herein are not to be considered
Hypertension in 2015: SPRINT-ing ahead of JNC-8 MAJ Charles Magee, MD MPH FACP Director, WRNMMC Hypertension Clinic Conflits of interest? None Disclaimer The opinions contained herein are not to be considered
Get a Statin or Not? Learning objectives. Presentation overview 4/3/2018. Treatment Strategies in Dyslipidemia Management
 Get a Statin or Not? Treatment Strategies in Dyslipidemia Management Michelle Chu, PharmD, BCACP, CDE Assistant Professor of Clinical Pharmacy, USC School of Pharmacy Sahar Dagher, PharmD Virtual Care
Get a Statin or Not? Treatment Strategies in Dyslipidemia Management Michelle Chu, PharmD, BCACP, CDE Assistant Professor of Clinical Pharmacy, USC School of Pharmacy Sahar Dagher, PharmD Virtual Care
Latest Guidelines for Lipid Management
 Latest Guidelines for Lipid Management Goals Recognize the differences between different guidelines Understand the effective strategies to tailor lipid lowering therapies based on evidence and guideline
Latest Guidelines for Lipid Management Goals Recognize the differences between different guidelines Understand the effective strategies to tailor lipid lowering therapies based on evidence and guideline
Combination Therapy for Hypertension
 Combination Therapy for Hypertension Se-Joong Rim, MD Cardiology Division, Yonsei University College of Medicine, Seoul, Korea Goals of Therapy Reduce CVD and renal morbidity and mortality. Treat to BP
Combination Therapy for Hypertension Se-Joong Rim, MD Cardiology Division, Yonsei University College of Medicine, Seoul, Korea Goals of Therapy Reduce CVD and renal morbidity and mortality. Treat to BP
HYPERTENSION GUIDELINES WHERE ARE WE IN 2014
 HYPERTENSION GUIDELINES WHERE ARE WE IN 2014 Donald J. DiPette MD FACP Special Assistant to the Provost for Health Affairs Distinguished Health Sciences Professor University of South Carolina University
HYPERTENSION GUIDELINES WHERE ARE WE IN 2014 Donald J. DiPette MD FACP Special Assistant to the Provost for Health Affairs Distinguished Health Sciences Professor University of South Carolina University
Preventing and Treating High Blood Pressure
 Preventing and Treating High Blood Pressure: Finding the Right Balance of Integrative and Pharmacologic Approaches Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Blood Pressure
Preventing and Treating High Blood Pressure: Finding the Right Balance of Integrative and Pharmacologic Approaches Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Blood Pressure
SBP in range of 120 to 140 :no progression or regression of CAD. Sipahi et al., 2006
 Management of Hypertension in Patients with CAD M. Mohsen Ibrahim, MD Cardiology Department- Cairo University 1. What is the optimal BP in patients with hypertension and CAD? 2. What is the minimum safe
Management of Hypertension in Patients with CAD M. Mohsen Ibrahim, MD Cardiology Department- Cairo University 1. What is the optimal BP in patients with hypertension and CAD? 2. What is the minimum safe
Sanger Heart & Vascular Institute Symposium 2015
 Sanger Heart & Vascular Institute Symposium 2015 Cardiovascular Update For Primary Care Physicians William E. Downey, MD FACC FSCAI Medical Director, Interventional Cardiology Sanger Heart & Vascular Institute
Sanger Heart & Vascular Institute Symposium 2015 Cardiovascular Update For Primary Care Physicians William E. Downey, MD FACC FSCAI Medical Director, Interventional Cardiology Sanger Heart & Vascular Institute
CPE Session 7. Update on Clinical Practice Guidelines and Best Evidence in the Management of Hyperlipidemia and Cardiovascular Risk Reduction
 CPE Session 7 Update on Clinical Practice Guidelines and Best Evidence in the Management of Hyperlipidemia and Cardiovascular Risk Reduction Saturday, April 25, 2015 ACPE UAN 0128-0000-15-027-L01-P 1.0
CPE Session 7 Update on Clinical Practice Guidelines and Best Evidence in the Management of Hyperlipidemia and Cardiovascular Risk Reduction Saturday, April 25, 2015 ACPE UAN 0128-0000-15-027-L01-P 1.0
4 th and Goal To Go How Low Should We Go? :
 4 th and Goal To Go How Low Should We Go? : Evaluating New Lipid Lowering Therapies Catherine Bourg Rebitch, PharmD, BCACP Clinical Associate Professor Disclosure The presenter has nothing to disclose
4 th and Goal To Go How Low Should We Go? : Evaluating New Lipid Lowering Therapies Catherine Bourg Rebitch, PharmD, BCACP Clinical Associate Professor Disclosure The presenter has nothing to disclose
Prevention Updates and Paradigm Shifts
 Prevention Updates and Paradigm Shifts Andrew Freeman, MD, FACC Director of Clinical Cardiology and Operations National Jewish Health Assistant Professor of Medicine National Jewish Health and University
Prevention Updates and Paradigm Shifts Andrew Freeman, MD, FACC Director of Clinical Cardiology and Operations National Jewish Health Assistant Professor of Medicine National Jewish Health and University
Hyperlipidemia. Intern Immersion Block 2015
 Hyperlipidemia Intern Immersion Block 2015 Christopher Wong, MD Division of General Internal Medicine University of Washington cjwong@u.washington.edu Welcome! Disclosures: royalties from book sales (not
Hyperlipidemia Intern Immersion Block 2015 Christopher Wong, MD Division of General Internal Medicine University of Washington cjwong@u.washington.edu Welcome! Disclosures: royalties from book sales (not
MODERN MANAGEMENT OF HYPERTENSION Where Do We Draw the Line? Disclosure. No relevant financial relationships. Blood Pressure and Risk
 MODERN MANAGEMENT OF HYPERTENSION Where Do We Draw the Line? Disclosure No relevant financial relationships Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine baron@medicine.ucsf.edu
MODERN MANAGEMENT OF HYPERTENSION Where Do We Draw the Line? Disclosure No relevant financial relationships Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine baron@medicine.ucsf.edu
2.3 CONTACT HOURS. Managing. By Kristine Anne Scordo, PhD, RN, ACNP-BC, FAANP
 2.3 CONTACT HOURS 2.3 CONTACT HOURS Managing hyperlipidemia The updated cholesterol treatment guidelines Abstract: The ACC/AHA 2013 cholesterol treatment guidelines focus on lowering the risk of heart
2.3 CONTACT HOURS 2.3 CONTACT HOURS Managing hyperlipidemia The updated cholesterol treatment guidelines Abstract: The ACC/AHA 2013 cholesterol treatment guidelines focus on lowering the risk of heart
None. Disclosure: Relationships with Industry Conflicts of Interests. Learning Objectives: Participants will be able to:
 2014 Evidence-Based Guideline for the Management of High Blood Pressure in Adults: Report from the Panel Members Appointed to the Eighth Joint National Committee (JNC 8) James W. Shaw, MD Memorial Lecture
2014 Evidence-Based Guideline for the Management of High Blood Pressure in Adults: Report from the Panel Members Appointed to the Eighth Joint National Committee (JNC 8) James W. Shaw, MD Memorial Lecture
Disclosures. Choosing a Statin/New Therapies. Case. How else would you do to treat him? LDL-C Reduction with Different Statin Strategies
 Disclosures I have no disclosures relevant to this talk Choosing a Statin/New Therapies Aryan Aiyer, MD Assistant Professor of Medicine University of Pittsburgh School of Medicine UPMC Heart and Vascular
Disclosures I have no disclosures relevant to this talk Choosing a Statin/New Therapies Aryan Aiyer, MD Assistant Professor of Medicine University of Pittsburgh School of Medicine UPMC Heart and Vascular
Management of Hypertension. Ahmed El Hawary MD Suez Canal University
 Management of Hypertension Ahmed El Hawary MD Suez Canal University Minimal vs. Optimal Care Resources more than science affect type of care and level of management. what is possible (minimal care) and
Management of Hypertension Ahmed El Hawary MD Suez Canal University Minimal vs. Optimal Care Resources more than science affect type of care and level of management. what is possible (minimal care) and
Placebo-Controlled Statin Trials EXPLAINING THE DECREASE IN DEATHS FROM CHD! PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN EXPLAINING THE DECREASE IN
 PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest EXPLAINING THE DECREASE
PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest EXPLAINING THE DECREASE
American Diabetes Association 2018 Guidelines Important Notable Points
 American Diabetes Association 2018 Guidelines Important Notable Points The Standards of Medical Care in Diabetes-2018 by ADA include the most current evidencebased recommendations for diagnosing and treating
American Diabetes Association 2018 Guidelines Important Notable Points The Standards of Medical Care in Diabetes-2018 by ADA include the most current evidencebased recommendations for diagnosing and treating
HYPERTENSION MANAGEMENT IN ELDERLY POPULATIONS
 HYPERTENSION MANAGEMENT IN ELDERLY POPULATIONS Michael J. Scalese, PharmD, BCPS, CACP Assistant Clinical Professor Auburn University Harrison School of Pharmacy July 14, 2018 DISCLOSURE/CONFLICT OF INTEREST
HYPERTENSION MANAGEMENT IN ELDERLY POPULATIONS Michael J. Scalese, PharmD, BCPS, CACP Assistant Clinical Professor Auburn University Harrison School of Pharmacy July 14, 2018 DISCLOSURE/CONFLICT OF INTEREST
How to Handle Statin Intolerance in the High Risk Patient
 How to Handle Statin Intolerance in the High Risk Patient Thomas D. Conley, MD FACC FSCAI Disclosures: None 1 Definition of High Risk Primary Prevention ASCVD Risk Calculator Adults >21 yrs, LDL 190 mg/dl
How to Handle Statin Intolerance in the High Risk Patient Thomas D. Conley, MD FACC FSCAI Disclosures: None 1 Definition of High Risk Primary Prevention ASCVD Risk Calculator Adults >21 yrs, LDL 190 mg/dl