BREAK 11:10-11:
|
|
|
- Reynard Richards
- 5 years ago
- Views:
Transcription
1 1. Sepsis Tom Heaps 09:30-10:20 2. Oncological Emergencies Clare Pollard 10:20-11: BREAK 11:10-11: Diabetic Ketoacidosis Tom Heaps 11:30-12:20 4. Close and Feedback 12:20-12:30
2

3

4 78-year-old male presenting to ED PMHx T2DM, CKD 1, IHD, BPH 48h history of dysuria, confusion and malaise T 38.3C, HR 112, BP 103/55mmHg, RR 24, SpO 2 93% o/a delirious ++ warm extremities, bounding pulse R basal crackles suprapubic tenderness Hb 11.1, WCC 18, platelets 103, urea 12, creatinine 144 (baseline ~120), LFTs normal, CRP 273, clotting normal
5 Systemic Inflammatory Response Syndrome (SIRS) defined by 2 of the following; temperature >38 C or <36 C HR >90min -1 RR >20min -1 or PaCO 2 <4.25kPa new onset confusion hyperglycaemia (CBG >7.7mmol/l) in absence of diabetes WBC >12 x10 9 or <4 x10 9 or high CRP (if available) infection, trauma, surgery, burns, pancreatitis SEPSIS = SIRS + infection +/- bacteraemia mortality increases with number of SIRS criteria
6 oxygen (if required to achieve target SpO 2 ) blood cultures IV antibiotics IV fluids VBG or ABG (plus FBC, U&E, LFT, CRP, coagulation) urinary catheter and commence fluid balance urine cultures CXR
7 lactate on VBG correlates well with arterial lactate except in cases of severe shock measure ABG if shocked or oxygenation/ventilation a concern lactate levels correlate highly with mortality 40% if lactate >4mmol/l 15% if lactate <2mmol/l serial measurements and lactate clearance in response to resuscitation more important than absolute values
8 hypovolaemia in sepsis is absolute (reduced fluid intake, fluid loss, insensible losses) and relative (vasodilatation) 500mL boluses up to 30mL/kg (~2L for 70kg person) over 30min repeated up to 60mL/kg (~4L for 70kg person) after senior review Which fluid? crystalloid vs colloid no evidence that albumin superior to saline (SAFE trial) colloids are more expensive and risks of AKI (HES), anaphylaxis and coagulopathy Which crystalloid? balanced solutions e.g. Hartmann s are more expensive less risk of hyperchloraemic acidosis than with 0.9% NaCl in vitro evidence only that hyperchloraemic acidosis is harmful
 separate guideline for suspected/proven febrile")
9 time to administration is critical factor 8% increase in mortality for every 1h delay after onset of hypotension aim to administer IV broad spectrum antibiotics within 1h of presentation with severe sepsis empirical choice governed by probable source of infection and local guidelines (available on intranet) separate guideline for suspected/proven febrile neutropenia
10 ABG on air ph 7.36, po 2 9.2, pco 2 2.8, lactate 4.8, BE -5.6 blood cultures taken CXR unremarkable catheterized urine dipstick leucocytes 3+, nitrite +ve, RBC 2+, protein + IV co-amoxiclav and gentamicin given for suspected UTI IV 0.9% NaCl 2L prescribed each over 8h 2h later BP 91/44mmHg and urine output 50ml total
11 SEVERE sepsis = sepsis plus evidence of organ dysfunction (or tissue hypoperfusion); alteration in mental state (confusion) hypoxemia (PaO 2 <9.6kPa at FiO in absence of pulmonary disease) elevated plasma lactate (>4mmol/l), increased CRT or skin mottling oliguria (urine output <30ml or <0.5 ml/kg for 1h) hypotension (sbp <90mmHg, MAP <65mmHg or reduction in sbp of 40mmHg from baseline) creatinine >177umol/l bilirubin >34umol/l platelets <100, INR >1.5 or disseminated intravascular coagulation (DIC)
12 SEVERE SEPSIS = sepsis plus evidence of sepsis-induced tissue hypoperfusion or organ dysfunction; alteration in mental state (confusion) hypoxemia (PaO 2 <9.6kPa at FiO in absence of pulmonary disease) elevated plasma lactate (>4mmol/l), increased CRT or skin mottling oliguria (urine output <30ml or <0.5 ml/kg for 1h) sepsis-induced hypotension (sbp <90mmHg, MAP <70mmHg or reduction in sbp of 40mmHg from baseline) creatinine >177umol/l bilirubin >34umol/l platelets <100, INR >1.5 or disseminated intravascular coagulation (DIC)
13 New concept introduced by latest guidelines from UK Sepsis Trust Early detection (MEWS-based) of patients at risk of deterioration who may benefit from more aggressive treatment as severe sepsis Many markers of severe sepsis may not be evident / available at time of first presentation 1. Tachycardia: HR >125/min 2. Hypotension: systolic BP <90mmHg 3. Tachypnoea: RR >20 4. Hypoxaemia: SpO 2 <90% (or only 90% with O 2 ) 5. Drowsiness: AVPU of V, P or U
14 given fluid challenge of 2L Hartmann s over 1h total fluid input now 3L repeat VBG shows lactate 6.2 no urine output in last 1h BP 80/52mmHg mottling of lower extremities increasing confusion
15 SEPTIC SHOCK = SEVERE SEPSIS + hypotension which is refractory to fluid replacement WHAT NEEDS TO HAPPEN NOW? senior review decisions re. CPR/escalation (if not already made!) transfer to ITU if appropriate Invasive monitoring, vasopressors, ventilation etc.
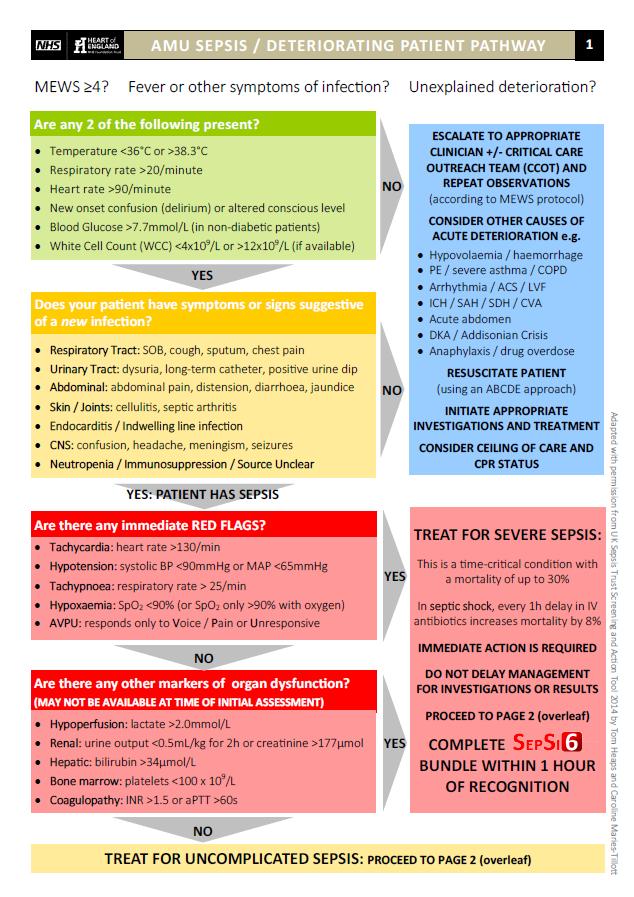
16 Recognize and screen for sepsis 1. Suspect Infection? MEWS 4 High temperature Symptoms suggestive of infection Risk of neutropenia/immunosuppression ELDERLY PATIENTS MAY PRESENT ATYPICALLY 2. Confirm diagnosis using SIRS criteria ( 2 positive) 3. Any features of red flag or severe sepsis? 4. Obtain medical review (immediate if severe sepsis)
17
 2. Blood cultures (and other cultures) 3.")

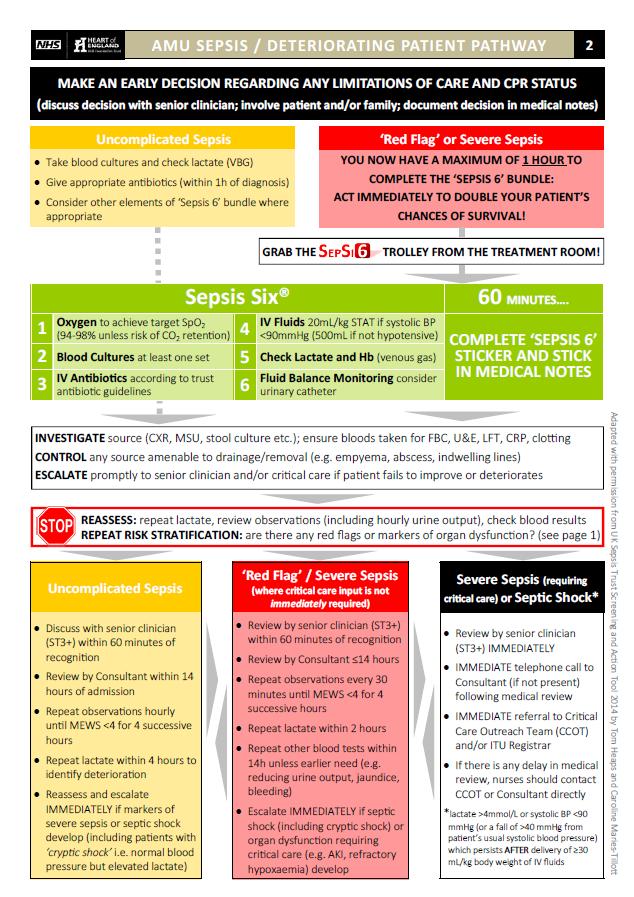
18 Get the SEPSI6 trolley and initiate the SEPSIS 6 BUNDLE 3x Investigations 1. VBG/ABG (and other bloods) 2. Blood cultures (and other cultures) 3. Urine output monitoring (insert catheter if severe sepsis) 3x Treatments 4. Oxygen 5. IV Fluids 6. IV antibiotics ALL WITHIN 1h OF RECOGNIZING RED FLAG OR SEVERE SEPSIS reduced mortality from 44% to 20% at GHH
19 Monitoring and Co-ordination of Care ensure antibiotics given promptly and fluids running to time hourly observations (for 1 st 4h even if MEWS <4) and urine output / fluid balance chart repeat VBG for lactate involve CCOT early prompt doctors to make escalation/cpr decisions alert senior medical staff if condition deteriorates or fails to improve as expected
20 SEPSIS = SIRS + infection SEVERE sepsis = sepsis plus 1 marker of organ dysfunction RED FLAG sepsis should be treated initially as SEVERE sepsis severe sepsis is a MEDICAL EMERGENCY which kills in 1/3 of cases early RECOGNITION and RESUSCITATION are key PROMPT antibiotics and ADEQUATE IV fluids will SAVE MORE LIVES than ITU GRAB THE SEPSI6 TROLLEY AND CARRY OUT THE SEPSIS SIX WITHIN 1h of recognition of SEVERE / RED FLAG sepsis escalate to senior and involve CCOT EARLY if patient fails to respond use the new AMU sepsis pathway and Sepsis 6 Stickers
The changing face of
 The changing face of sepsis. @SepsisUK Dr Ron Daniels B.E.M. CEO, UK Sepsis Trust CEO, Global Sepsis Alliance Special Adviser (maternal sepsis) to WHO Breast cancer Cognitive impairment Mild 3.8 7.1
The changing face of sepsis. @SepsisUK Dr Ron Daniels B.E.M. CEO, UK Sepsis Trust CEO, Global Sepsis Alliance Special Adviser (maternal sepsis) to WHO Breast cancer Cognitive impairment Mild 3.8 7.1
Staging Sepsis for the Emergency Department: Physician
 Staging Sepsis for the Emergency Department: Physician Sepsis Continuum 1 Sepsis Continuum SIRS = 2 or more clinical criteria, resulting in Systemic Inflammatory Response Syndrome Sepsis = SIRS + proven/suspected
Staging Sepsis for the Emergency Department: Physician Sepsis Continuum 1 Sepsis Continuum SIRS = 2 or more clinical criteria, resulting in Systemic Inflammatory Response Syndrome Sepsis = SIRS + proven/suspected
Sepsis Early Recognition and Management. Therese Hughes, PhD, MPA, RN
 Sepsis Early Recognition and Management Therese Hughes, PhD, MPA, RN 1 Sepsis a Deadly Progression Affects millions around the world each year, killing one in four Contributes to approximately 50% of all
Sepsis Early Recognition and Management Therese Hughes, PhD, MPA, RN 1 Sepsis a Deadly Progression Affects millions around the world each year, killing one in four Contributes to approximately 50% of all
MAKING SENSE OF IT ALL AUGUST 17
 MAKING SENSE OF IT ALL AUGUST 17 @SepsisUK Dr Ron Daniels B.E.M. CEO, UK Sepsis Trust CEO, Global Sepsis Alliance Special Adviser to WHO SCALE AND BURDEN @sepsisuk Dr Ron Daniels B.E.M. CEO, UK Sepsis
MAKING SENSE OF IT ALL AUGUST 17 @SepsisUK Dr Ron Daniels B.E.M. CEO, UK Sepsis Trust CEO, Global Sepsis Alliance Special Adviser to WHO SCALE AND BURDEN @sepsisuk Dr Ron Daniels B.E.M. CEO, UK Sepsis
Initial Resuscitation of Sepsis & Septic Shock
 Initial Resuscitation of Sepsis & Septic Shock Dr. Fatema Ahmed MD (Critical Care Medicine) FCPS (Medicine) Associate professor Dept. of Critical Care Medicine BIRDEM General Hospital Is Sepsis a known
Initial Resuscitation of Sepsis & Septic Shock Dr. Fatema Ahmed MD (Critical Care Medicine) FCPS (Medicine) Associate professor Dept. of Critical Care Medicine BIRDEM General Hospital Is Sepsis a known
Sepsis! Dr Eric Van Den Bergh Consultant in Emergency Medicine 2015
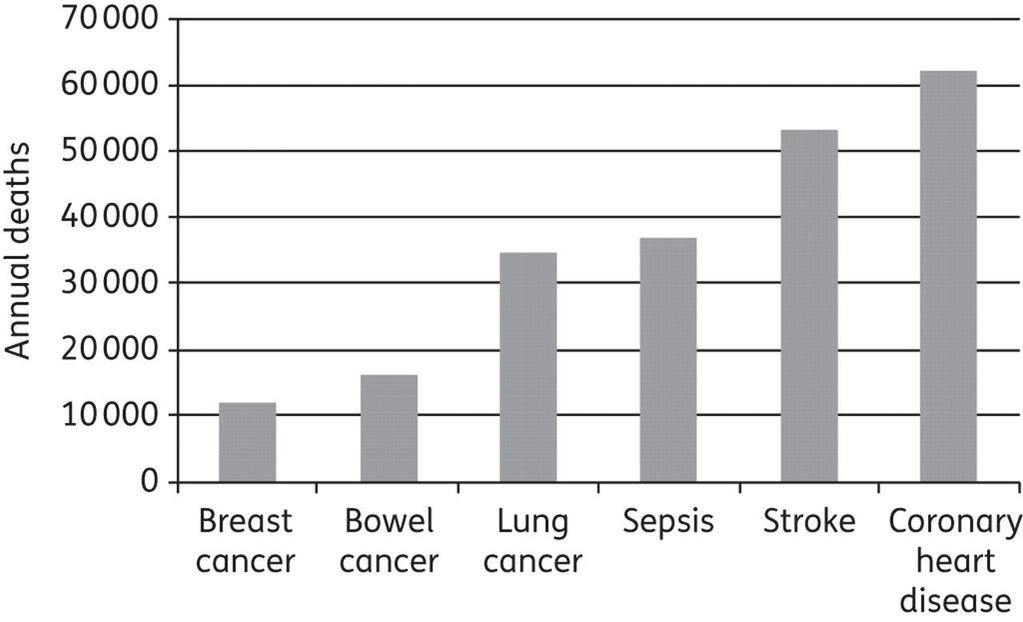
 Sepsis! Dr Eric Van Den Bergh Consultant in Emergency Medicine 2015 Annual UK Mortality Sepsis Stroke Heart attack COPD Lung cancer COPD Heart attack Stroke Sepsis Lung cancer 0 10000 20000 30000 40000
Sepsis! Dr Eric Van Den Bergh Consultant in Emergency Medicine 2015 Annual UK Mortality Sepsis Stroke Heart attack COPD Lung cancer COPD Heart attack Stroke Sepsis Lung cancer 0 10000 20000 30000 40000
The Septic Patient. Dr Arunraj Navaratnarajah. Renal SpR Imperial College NHS Healthcare Trust
 The Septic Patient Dr Arunraj Navaratnarajah Renal SpR Imperial College NHS Healthcare Trust Objectives of this session Define SIRS / sepsis / severe sepsis / septic shock Early recognition of Sepsis The
The Septic Patient Dr Arunraj Navaratnarajah Renal SpR Imperial College NHS Healthcare Trust Objectives of this session Define SIRS / sepsis / severe sepsis / septic shock Early recognition of Sepsis The
John Park, MD Assistant Professor of Medicine
 John Park, MD Assistant Professor of Medicine Faculty photo will be placed here park.john@mayo.edu 2015 MFMER 3543652-1 Sepsis Out with the Old, In with the New Mayo School of Continuous Professional Development
John Park, MD Assistant Professor of Medicine Faculty photo will be placed here park.john@mayo.edu 2015 MFMER 3543652-1 Sepsis Out with the Old, In with the New Mayo School of Continuous Professional Development
Printed copies of this document may not be up to date, obtain the most recent version from
 Children s Acute Transport Service Clinical Guidelines Septic Shock Document Control Information Author Claire Fraser P.Ramnarayan Author Position tanp CATS Consultant Document Owner E. Polke Document
Children s Acute Transport Service Clinical Guidelines Septic Shock Document Control Information Author Claire Fraser P.Ramnarayan Author Position tanp CATS Consultant Document Owner E. Polke Document
R2R: Severe sepsis/septic shock. Surat Tongyoo Critical care medicine Siriraj Hospital
 R2R: Severe sepsis/septic shock Surat Tongyoo Critical care medicine Siriraj Hospital Diagnostic criteria ACCP/SCCM consensus conference 1991 SCCM/ESICM/ACCP/ATS/SIS International Sepsis Definitions Conference
R2R: Severe sepsis/septic shock Surat Tongyoo Critical care medicine Siriraj Hospital Diagnostic criteria ACCP/SCCM consensus conference 1991 SCCM/ESICM/ACCP/ATS/SIS International Sepsis Definitions Conference
Sepsis: Management ANUPOL PANITCHOTE, MD. Division of Critical Care Medicine Department of Medicine, Khon Kaen University, Thailand
 Sepsis: Management ANUPOL PANITCHOTE, MD. Division of Critical Care Medicine Department of Medicine, Khon Kaen University, Thailand Vital signs Symptoms LAB BT > 38.3 or < 36 ๐ C HR > 90 bpm RR > 20 /min
Sepsis: Management ANUPOL PANITCHOTE, MD. Division of Critical Care Medicine Department of Medicine, Khon Kaen University, Thailand Vital signs Symptoms LAB BT > 38.3 or < 36 ๐ C HR > 90 bpm RR > 20 /min
Sepsis Awareness and Education
 Sepsis Awareness and Education Meets the updated New York State Department of Health (NYSDOH) requirements for Infection Control and Barrier Precautions coursework Element VII: Sepsis Awareness and Education
Sepsis Awareness and Education Meets the updated New York State Department of Health (NYSDOH) requirements for Infection Control and Barrier Precautions coursework Element VII: Sepsis Awareness and Education
Sepsis is an important issue. Clinician s decision-making capability. Guideline recommendations
 Surviving Sepsis Campaign: International Guidelines for Management of Severe Sepsis and Septic Shock: 2012 Clinicians decision-making capability Guideline recommendations Sepsis is an important issue 8.7%
Surviving Sepsis Campaign: International Guidelines for Management of Severe Sepsis and Septic Shock: 2012 Clinicians decision-making capability Guideline recommendations Sepsis is an important issue 8.7%
The Oxford AHSN Sepsis Pathway
 From confusion to consensus: The Oxford AHSN Sepsis Pathway Andrew Brent Sepsis Clinical Lead, Oxford AHSN & Oxford University Hospitals NHS Foundation Trust 2013 2014 2015 2016 2017 From: The Third International
From confusion to consensus: The Oxford AHSN Sepsis Pathway Andrew Brent Sepsis Clinical Lead, Oxford AHSN & Oxford University Hospitals NHS Foundation Trust 2013 2014 2015 2016 2017 From: The Third International
Septic Shock. Rontgene M. Solante, MD, FPCP,FPSMID
 Septic Shock Rontgene M. Solante, MD, FPCP,FPSMID Learning Objectives Identify situations wherein high or low BP are hemodynamically significant Recognize complications arising from BP emergencies Manage
Septic Shock Rontgene M. Solante, MD, FPCP,FPSMID Learning Objectives Identify situations wherein high or low BP are hemodynamically significant Recognize complications arising from BP emergencies Manage
Chapter 5: Sepsis Stephen Lo
 Chapter 5: Sepsis Stephen Lo Introduction Sepsis and its consequence are the bread and butter of intensive care medicine and management of it is time critical. This chapter will discuss the definitions,
Chapter 5: Sepsis Stephen Lo Introduction Sepsis and its consequence are the bread and butter of intensive care medicine and management of it is time critical. This chapter will discuss the definitions,
PHYSIOLOGY AND MANAGEMENT OF THE SEPTIC PATIENT
 PHYSIOLOGY AND MANAGEMENT OF THE SEPTIC PATIENT Melanie Sanchez, RN, MSNE, OCN, CCRN Clinical Nurse III City of Hope National Medical Center HOW THE EXPERTS TREAT HEMATOLOGIC MALIGNANCIES LAS VEGAS, NV
PHYSIOLOGY AND MANAGEMENT OF THE SEPTIC PATIENT Melanie Sanchez, RN, MSNE, OCN, CCRN Clinical Nurse III City of Hope National Medical Center HOW THE EXPERTS TREAT HEMATOLOGIC MALIGNANCIES LAS VEGAS, NV
INTRAVENOUS FLUID THERAPY. Tom Heaps Consultant Acute Physician
 INTRAVENOUS FLUID THERAPY Tom Heaps Consultant Acute Physician LEARNING OBJECTIVES 1. Crystalloids vs colloids 2. Balanced vs non-balanced solutions 3. Composition of various IV fluids 4. What is normal
INTRAVENOUS FLUID THERAPY Tom Heaps Consultant Acute Physician LEARNING OBJECTIVES 1. Crystalloids vs colloids 2. Balanced vs non-balanced solutions 3. Composition of various IV fluids 4. What is normal
Sepsis in primary care. what is good care?
 Sepsis in primary care @SepsisUK what is good care? Emmanuel Nsutebu Consultant Infectious Disease Physician & Clinical lead for sepsis Tropical and Infectious Disease Unit Royal Liverpool Hospital Do
Sepsis in primary care @SepsisUK what is good care? Emmanuel Nsutebu Consultant Infectious Disease Physician & Clinical lead for sepsis Tropical and Infectious Disease Unit Royal Liverpool Hospital Do
Updates in Sepsis 2017
 Mortality Cases Total U.S. Population/1,000 Updates in 2017 Joshua Solomon, M.D. Associate Professor of Medicine National Jewish Health University of Colorado Denver Background New Definition of New Trials
Mortality Cases Total U.S. Population/1,000 Updates in 2017 Joshua Solomon, M.D. Associate Professor of Medicine National Jewish Health University of Colorado Denver Background New Definition of New Trials
Sepsis. From EMS to ER to ICU. What we need to be doing
 Sepsis From EMS to ER to ICU What we need to be doing NEHAL BHATT, MD ATHENS PULMONARY, CRITICAL CARE AND SLEEP Objectives 1. Define the changes to the definition of Sepsis 2. Describe the assessment,
Sepsis From EMS to ER to ICU What we need to be doing NEHAL BHATT, MD ATHENS PULMONARY, CRITICAL CARE AND SLEEP Objectives 1. Define the changes to the definition of Sepsis 2. Describe the assessment,
Nephrology. 3 rd Year Revision Session 06/05/17 Cathal Hannan
 Nephrology 3 rd Year Revision Session 06/05/17 Cathal Hannan Aims Acute Kidney Injury-recognition and management Sample OSCE Station Clinically relevant renal physiology Aetiology of Chronic Kidney Disease
Nephrology 3 rd Year Revision Session 06/05/17 Cathal Hannan Aims Acute Kidney Injury-recognition and management Sample OSCE Station Clinically relevant renal physiology Aetiology of Chronic Kidney Disease
Core Measures SEPSIS UPDATES
 Patricia Walker, RN-BC, BSN Evidence Based Practice Manager Quality Management Services UCLA Health System, Ronald Reagan Medical Center Core Measures SEPSIS UPDATES Severe Sepsis and Septic Shock Based
Patricia Walker, RN-BC, BSN Evidence Based Practice Manager Quality Management Services UCLA Health System, Ronald Reagan Medical Center Core Measures SEPSIS UPDATES Severe Sepsis and Septic Shock Based
Patient Safety Safe Table Webcast: Sepsis (Part III and IV) December 17, 2014
 December 17, 2014") Patient Safety Safe Table Webcast: Sepsis (Part III and IV) December 17, 2014 Presenters Mark Blaney, RN Regional Nurse Educator CHI Franciscan Health Karen Lautermilch Director, Quality & Performance
Patient Safety Safe Table Webcast: Sepsis (Part III and IV) December 17, 2014 Presenters Mark Blaney, RN Regional Nurse Educator CHI Franciscan Health Karen Lautermilch Director, Quality & Performance
SEPSIS SYNDROME
 INTRODUCTION Sepsis has been defined as a life threatening condition that arises when the body s response to an infection injures its own tissues and organs. Sepsis may lead to shock, multiple organ failure
INTRODUCTION Sepsis has been defined as a life threatening condition that arises when the body s response to an infection injures its own tissues and organs. Sepsis may lead to shock, multiple organ failure
Fluids in Sepsis: How much and what type? John Fowler, MD, FACEP Kent Hospital, İzmir Eisenhower Medical Center, USA American Hospital Dubai, UAE
 Fluids in Sepsis: How much and what type? John Fowler, MD, FACEP Kent Hospital, İzmir Eisenhower Medical Center, USA American Hospital Dubai, UAE In critically ill patients: too little fluid Low preload,
Fluids in Sepsis: How much and what type? John Fowler, MD, FACEP Kent Hospital, İzmir Eisenhower Medical Center, USA American Hospital Dubai, UAE In critically ill patients: too little fluid Low preload,
Date written: April 2014 Review date: April 2016 Related documents: Paediatric Sepsis 6
 Scottish Paediatric Retrieval Service (Edinburgh) www.paedsretrieval.com Clinical Guideline SEPSIS Date written: April 2014 Review date: April 2016 Related documents: Paediatric Sepsis 6 Author: Steve
Scottish Paediatric Retrieval Service (Edinburgh) www.paedsretrieval.com Clinical Guideline SEPSIS Date written: April 2014 Review date: April 2016 Related documents: Paediatric Sepsis 6 Author: Steve
Acute Kidney Injury (AKI) Undergraduate nurse education
 Undergraduate nurse education") Acute Kidney Injury (AKI) Undergraduate nurse education Year Three Developed Summer 2017 Objectives Understand Acute Kidney Injury and its relevance to patient care. Brief revision of the Anatomy and physiology
Acute Kidney Injury (AKI) Undergraduate nurse education Year Three Developed Summer 2017 Objectives Understand Acute Kidney Injury and its relevance to patient care. Brief revision of the Anatomy and physiology
Effectively Managing Sepsis Denials
 Effectively Managing Sepsis Denials Krysten Brooks, RN, BSN, MBA Senior Inpatient Consultant 3M Health Information Systems This is the Full Title of a Session Atlanta, GA 1 Learning Objectives At the completion
Effectively Managing Sepsis Denials Krysten Brooks, RN, BSN, MBA Senior Inpatient Consultant 3M Health Information Systems This is the Full Title of a Session Atlanta, GA 1 Learning Objectives At the completion
Reducing the Door to Needle Time for Antibiotics in Suspected Neutropenic Sepsis using a Dedicated Clinical Pathway
 Reducing the Door to Needle Time for Antibiotics in Suspected Neutropenic Sepsis using a Dedicated Clinical Pathway Dr Alex Williams, Oncology Specialty Doctor. Cheltenham General Hospital Oncology Centre
Reducing the Door to Needle Time for Antibiotics in Suspected Neutropenic Sepsis using a Dedicated Clinical Pathway Dr Alex Williams, Oncology Specialty Doctor. Cheltenham General Hospital Oncology Centre
SHOCK Susanna Hilda Hutajulu, MD, PhD
 SHOCK Susanna Hilda Hutajulu, MD, PhD Div Hematology and Medical Oncology Department of Internal Medicine Universitas Gadjah Mada Yogyakarta Outline Definition Epidemiology Physiology Classes of Shock
SHOCK Susanna Hilda Hutajulu, MD, PhD Div Hematology and Medical Oncology Department of Internal Medicine Universitas Gadjah Mada Yogyakarta Outline Definition Epidemiology Physiology Classes of Shock
Shock Quiz! By Clare Di Bona
 Shock Quiz! By Clare Di Bona Test Question What is Mr Burns full legal name? Answer Charles Montgomery Plantagenet Schicklgruber Burns. (Season 22, episode 11) Question 1. What is the definition of shock?
Shock Quiz! By Clare Di Bona Test Question What is Mr Burns full legal name? Answer Charles Montgomery Plantagenet Schicklgruber Burns. (Season 22, episode 11) Question 1. What is the definition of shock?
SIRS, NICE, SOFAs and CQUINs: Challenges of changing definitions and guidelines. Dr Sian Coggle Consultant Acute Medicine and Infectious Diseases
 SIRS, NICE, SOFAs and CQUINs: Challenges of changing definitions and guidelines Dr Sian Coggle Consultant Acute Medicine and Infectious Diseases Objectives Context Case Changing definitions Systems for
SIRS, NICE, SOFAs and CQUINs: Challenges of changing definitions and guidelines Dr Sian Coggle Consultant Acute Medicine and Infectious Diseases Objectives Context Case Changing definitions Systems for
Sepsis. Reliability- can we achieve Dr Ron Daniels
 Sepsis. Reliability- can we achieve it? @SepsisUK Dr Ron Daniels Chief Executive, Global Sepsis Alliance Fellow: NHS Improvement Faculty Chief Executive: United Kingdom Sepsis Trust & Chair, UK SSC RRAILS
Sepsis. Reliability- can we achieve it? @SepsisUK Dr Ron Daniels Chief Executive, Global Sepsis Alliance Fellow: NHS Improvement Faculty Chief Executive: United Kingdom Sepsis Trust & Chair, UK SSC RRAILS
McHenry Western Lake County EMS System CE for Paramedics, EMT-B and PHRN s Sepsis Patients. November/December 2017
 McHenry Western Lake County EMS System CE for Paramedics, EMT-B and PHRN s Sepsis Patients November/December 2017 This month we are going to take a look at the patient with Sepsis. Webster s defines septic
McHenry Western Lake County EMS System CE for Paramedics, EMT-B and PHRN s Sepsis Patients November/December 2017 This month we are going to take a look at the patient with Sepsis. Webster s defines septic
Sepsis Story At Intermountain Healthcare Intensive Medicine Clinical Program
 Sepsis Story At Intermountain Healthcare 2004-2012 Intensive Medicine Clinical Program The International Surviving Sepsis Campaign Was Organized In 2002 During The ESICM International Meeting In Barcelona,
Sepsis Story At Intermountain Healthcare 2004-2012 Intensive Medicine Clinical Program The International Surviving Sepsis Campaign Was Organized In 2002 During The ESICM International Meeting In Barcelona,
Understand the scope of sepsis morbidity and mortality Identify risk factors that predispose a patient to development of sepsis Define and know the
 Understand the scope of sepsis morbidity and mortality Identify risk factors that predispose a patient to development of sepsis Define and know the differences between sepsis, severe sepsis and septic
Understand the scope of sepsis morbidity and mortality Identify risk factors that predispose a patient to development of sepsis Define and know the differences between sepsis, severe sepsis and septic
9/25/2017. Nothing to disclose
 Nothing to disclose Jessie O Neal, PharmD, BCCCP Critical Care Clinical Pharmacist University of New Mexico Hospital New Mexico Society of Health-System Pharmacists 2017 Balloon Fiesta Symposium Explain
Nothing to disclose Jessie O Neal, PharmD, BCCCP Critical Care Clinical Pharmacist University of New Mexico Hospital New Mexico Society of Health-System Pharmacists 2017 Balloon Fiesta Symposium Explain
Nothing to disclose 9/25/2017
 Jessie O Neal, PharmD, BCCCP Critical Care Clinical Pharmacist University of New Mexico Hospital New Mexico Society of Health-System Pharmacists 2017 Balloon Fiesta Symposium Nothing to disclose 1 Explain
Jessie O Neal, PharmD, BCCCP Critical Care Clinical Pharmacist University of New Mexico Hospital New Mexico Society of Health-System Pharmacists 2017 Balloon Fiesta Symposium Nothing to disclose 1 Explain
Transfusion Requirements and Management in Trauma RACHEL JACK
 Transfusion Requirements and Management in Trauma RACHEL JACK Overview Haemostatic resuscitation Massive Transfusion Protocol Overview of NBA research guidelines Haemostatic resuscitation Permissive hypotension
Transfusion Requirements and Management in Trauma RACHEL JACK Overview Haemostatic resuscitation Massive Transfusion Protocol Overview of NBA research guidelines Haemostatic resuscitation Permissive hypotension
Sepsis Management: Past, Present, and Future
 Sepsis Management: Past, Present, and Future Benjamin Ferrell, MD Tennessee ACP Meeting October 28, 2017 Learning Objectives Identify the most updated definition and clinical criteria for sepsis Describe
Sepsis Management: Past, Present, and Future Benjamin Ferrell, MD Tennessee ACP Meeting October 28, 2017 Learning Objectives Identify the most updated definition and clinical criteria for sepsis Describe
Use of surrogate inflammatory markers in the diagnosis & monitoring of patients with severe sepsis
 Thursday 11 th June 2015 Use of surrogate inflammatory markers in the diagnosis & monitoring of patients with severe sepsis Dr Duncan Wyncoll Guy s & St Thomas NHS Trust, London Conflicts of Interest In
Thursday 11 th June 2015 Use of surrogate inflammatory markers in the diagnosis & monitoring of patients with severe sepsis Dr Duncan Wyncoll Guy s & St Thomas NHS Trust, London Conflicts of Interest In
Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock: 2016
 Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock: 2016 Mitchell M. Levy MD, MCCM Professor of Medicine Chief, Division of Pulmonary, Sleep, and Critical Care
Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock: 2016 Mitchell M. Levy MD, MCCM Professor of Medicine Chief, Division of Pulmonary, Sleep, and Critical Care
Sepsis as Seen by the CMO. Randy C. Roth, MD Chief Medical Officer
 Sepsis as Seen by the CMO Randy C. Roth, MD Chief Medical Officer 1 Challenges of Sepsis Sepsis, like many disease processes, is much more than a clinical challenge. For Hospitalists, we are treating the
Sepsis as Seen by the CMO Randy C. Roth, MD Chief Medical Officer 1 Challenges of Sepsis Sepsis, like many disease processes, is much more than a clinical challenge. For Hospitalists, we are treating the
SEPSIS UPDATE WHY DO WE NEED A CORE MEASURE CHAD M. KOVALA DO, FACOEP, FACEP
 SEPSIS UPDATE WHY DO WE NEED A CORE MEASURE CHAD M. KOVALA DO, FACOEP, FACEP OBJECTIVES Arise, ProMISE, ProCESS Key points in sepsis management The CMS sepsis core measure COST OF SEPSIS CARE IN US Most
SEPSIS UPDATE WHY DO WE NEED A CORE MEASURE CHAD M. KOVALA DO, FACOEP, FACEP OBJECTIVES Arise, ProMISE, ProCESS Key points in sepsis management The CMS sepsis core measure COST OF SEPSIS CARE IN US Most
Managing Patients with Sepsis
 Managing Patients with Sepsis Diagnosis; Initial Resuscitation; ARRT Initiation Prof. Achim Jörres, M.D. Dept. of Nephrology and Medical Intensive Care Charité University Hospital Campus Virchow Klinikum
Managing Patients with Sepsis Diagnosis; Initial Resuscitation; ARRT Initiation Prof. Achim Jörres, M.D. Dept. of Nephrology and Medical Intensive Care Charité University Hospital Campus Virchow Klinikum
Bedside assessment of fluid status
 Bedside assessment of fluid status 2nd AKI Academy October 18 th 2014 David Treacher Guy s & St Thomas NHS Trust Assessing the circulation - the 3 key questions v Is my patient adequately filled? v What
Bedside assessment of fluid status 2nd AKI Academy October 18 th 2014 David Treacher Guy s & St Thomas NHS Trust Assessing the circulation - the 3 key questions v Is my patient adequately filled? v What
SHOCK. Emergency pediatric PICU division Pediatric Department Medical Faculty, University of Sumatera Utara H. Adam Malik Hospital
 SHOCK Emergency pediatric PICU division Pediatric Department Medical Faculty, University of Sumatera Utara H. Adam Malik Hospital 1 Definition Shock is an acute, complex state of circulatory dysfunction
SHOCK Emergency pediatric PICU division Pediatric Department Medical Faculty, University of Sumatera Utara H. Adam Malik Hospital 1 Definition Shock is an acute, complex state of circulatory dysfunction
AnnMarie Papa, DNP,RN,CEN,NE-BC,FAEN, FAAN Clinical Director, Emergency, Medical & Observation Nursing Hospital of the University of Pennsylvania
 AnnMarie Papa, DNP,RN,CEN,NE-BC,FAEN, FAAN Clinical Director, Emergency, Medical & Observation Nursing Hospital of the University of Pennsylvania Who Am I? Except on few occasions, the patient appears
AnnMarie Papa, DNP,RN,CEN,NE-BC,FAEN, FAAN Clinical Director, Emergency, Medical & Observation Nursing Hospital of the University of Pennsylvania Who Am I? Except on few occasions, the patient appears
2016 Sepsis Update: Pearls, Pitfalls, and Core Measure Quicksand
 2016 Sepsis Update: Pearls, Pitfalls, and Core Measure Quicksand Jack Perkins, MD FACEP, FAAEM, FACP Assistant Professor of Emergency and Internal Medicine Virginia Tech Carilion School of Medicine Why
2016 Sepsis Update: Pearls, Pitfalls, and Core Measure Quicksand Jack Perkins, MD FACEP, FAAEM, FACP Assistant Professor of Emergency and Internal Medicine Virginia Tech Carilion School of Medicine Why
Severe Sepsis & Septic Shock
 The College of Emergency Medicine Clinical Audits Severe Sepsis & Septic Shock EXCELLENCE IN EMERGENCY MEDICINE Contents Executive summary 3 Introduction 4 Audit history 4 Format of this report 4 Analysis
The College of Emergency Medicine Clinical Audits Severe Sepsis & Septic Shock EXCELLENCE IN EMERGENCY MEDICINE Contents Executive summary 3 Introduction 4 Audit history 4 Format of this report 4 Analysis
Admissions with severe sepsis in adult, general critical care units in England, Wales and Northern Ireland
 Admissions with severe sepsis in adult, general critical care units in England, Wales and Northern Ireland Question For all admissions to adult, general critical care units in the Case Mix Programme Database
Admissions with severe sepsis in adult, general critical care units in England, Wales and Northern Ireland Question For all admissions to adult, general critical care units in the Case Mix Programme Database
Sepsis overview. Dr. Tsang Hin Hung MBBS FHKCP FRCP
 Sepsis overview Dr. Tsang Hin Hung MBBS FHKCP FRCP Epidemiology Sepsis, severe sepsis, septic shock Pathophysiology of sepsis Recent researches and advances From bench to bedside Sepsis bundle Severe sepsis
Sepsis overview Dr. Tsang Hin Hung MBBS FHKCP FRCP Epidemiology Sepsis, severe sepsis, septic shock Pathophysiology of sepsis Recent researches and advances From bench to bedside Sepsis bundle Severe sepsis
Sepsis or Severe Sepsis? Is there a right thing, and how do we do it?
 Sepsis or Severe Sepsis? Is there a right thing, and how do we do it? Steven Q Simpson, MD, FCCP, FACP Professor of Medicine Division of Pulmonary and Critical Care University of Kansas Disclosures No
Sepsis or Severe Sepsis? Is there a right thing, and how do we do it? Steven Q Simpson, MD, FCCP, FACP Professor of Medicine Division of Pulmonary and Critical Care University of Kansas Disclosures No
SURVIVING SEPSIS: Early Management Saves Lives
 SURVIVING SEPSIS: Early Management Saves Lives Pat Posa RN, BSN, MSA System Performance Improvement Leader St. Joseph Mercy Health System Ann Arbor, MI Patricia.posa@stjoeshealth.org Objectives a. Understand
SURVIVING SEPSIS: Early Management Saves Lives Pat Posa RN, BSN, MSA System Performance Improvement Leader St. Joseph Mercy Health System Ann Arbor, MI Patricia.posa@stjoeshealth.org Objectives a. Understand
Printed copies of this document may not be up to date, obtain the most recent version from
 Children s Acute Transport Service Clinical Guidelines Septic Shock Document Control Information Author Shruti Dholakia L Chigaru Author Position Fellow CATS Consultant Document Owner E. Polke Document
Children s Acute Transport Service Clinical Guidelines Septic Shock Document Control Information Author Shruti Dholakia L Chigaru Author Position Fellow CATS Consultant Document Owner E. Polke Document
SEPSIS: IT ALL BEGINS WITH INFECTION. Theresa Posani, MS, RN, ACNS-BC, CCRN M/S CNS/Sepsis Coordinator Texas Health Harris Methodist Ft.
 SEPSIS: IT ALL BEGINS WITH INFECTION Theresa Posani, MS, RN, ACNS-BC, CCRN M/S CNS/Sepsis Coordinator Texas Health Harris Methodist Ft. Worth 1 2 3 OBJECTIVES Review the new Sepsis 3 definitions of sepsis
SEPSIS: IT ALL BEGINS WITH INFECTION Theresa Posani, MS, RN, ACNS-BC, CCRN M/S CNS/Sepsis Coordinator Texas Health Harris Methodist Ft. Worth 1 2 3 OBJECTIVES Review the new Sepsis 3 definitions of sepsis
What is sepsis? RECOGNITION. Sepsis I Know It When I See It 9/21/2017
 Sepsis I Know It When I See It September 15, 2017 Matthew Exline, MD MPH Medical Director, Medical ICU What is sepsis? I shall not today attempt further to define the kinds of material [b]ut I know it
Sepsis I Know It When I See It September 15, 2017 Matthew Exline, MD MPH Medical Director, Medical ICU What is sepsis? I shall not today attempt further to define the kinds of material [b]ut I know it
What the ED clinician needs to know about SEPSIS - 3. Anna Morgan Consultant EM Barts Health
 What the ED clinician needs to know about SEPSIS - 3 Anna Morgan Consultant EM Barts Health Aims: (1) To review the Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3) (2)
What the ED clinician needs to know about SEPSIS - 3 Anna Morgan Consultant EM Barts Health Aims: (1) To review the Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3) (2)
Sepsis 3 & Early Identification. Disclosures. Objectives 9/19/2016. David Carlbom, MD Medical Director, HMC Sepsis Program
 Sepsis 3 & Early Identification David Carlbom, MD Medical Director, HMC Sepsis Program Disclosures I have no relevant financial relationships with a commercial interest and will not discuss off-label use
Sepsis 3 & Early Identification David Carlbom, MD Medical Director, HMC Sepsis Program Disclosures I have no relevant financial relationships with a commercial interest and will not discuss off-label use
Current State of Pediatric Sepsis. Jason Clayton, MD PhD Pediatric Critical Care 9/19/2018
 Current State of Pediatric Sepsis Jason Clayton, MD PhD Pediatric Critical Care 9/19/2018 Objectives Review the history of pediatric sepsis Review the current definition of pediatric sepsis Review triage
Current State of Pediatric Sepsis Jason Clayton, MD PhD Pediatric Critical Care 9/19/2018 Objectives Review the history of pediatric sepsis Review the current definition of pediatric sepsis Review triage
Update in Sepsis. Conflicts of Interest: None. Bill Janssen, M.D.
 Update in Sepsis Bill Janssen, M.D. Associate Professor of Medicine National Jewish Health University of Colorado Denver Conflicts of Interest: None A 62 year-old female presents to the ED with fever,
Update in Sepsis Bill Janssen, M.D. Associate Professor of Medicine National Jewish Health University of Colorado Denver Conflicts of Interest: None A 62 year-old female presents to the ED with fever,
Sepsis: Identification and Management in an Acute Care Setting
 Sepsis: Identification and Management in an Acute Care Setting Dr. Barbara M. Mills DNP Director Rapid Response Team/ Code Resuscitation Stony Brook University Medical Center SEPSIS LECTURE NPA 2018 OBJECTIVES
Sepsis: Identification and Management in an Acute Care Setting Dr. Barbara M. Mills DNP Director Rapid Response Team/ Code Resuscitation Stony Brook University Medical Center SEPSIS LECTURE NPA 2018 OBJECTIVES
Case Scenario 3: Shock and Sepsis
 Name: Molly Boyle 1. Define the term shock (Lewis textbook): Shock is a syndrome characterized by decreased perfusion and impaired metabolism. Shock can have a number of causes that result in damage to
Name: Molly Boyle 1. Define the term shock (Lewis textbook): Shock is a syndrome characterized by decreased perfusion and impaired metabolism. Shock can have a number of causes that result in damage to
Early Goal-Directed Therapy
 Early Goal-Directed Therapy Where do we stand? Jean-Daniel Chiche, MD PhD MICU & Dept of Host-Pathogen Interaction Hôpital Cochin & Institut Cochin, Paris-F Resuscitation targets in septic shock 1 The
Early Goal-Directed Therapy Where do we stand? Jean-Daniel Chiche, MD PhD MICU & Dept of Host-Pathogen Interaction Hôpital Cochin & Institut Cochin, Paris-F Resuscitation targets in septic shock 1 The
TBSA Burn Estimation Chart Adult Major Burn Clinical Practice Guideline
 TBSA Burn Estimation Chart Adult Major Burn Clinical Practice Guideline Patient Label Anatomical Subunit Percent Total Percent One Side Anterior Posterior Injury Subtotal 3.5% 2nd and 3rd degree burns
TBSA Burn Estimation Chart Adult Major Burn Clinical Practice Guideline Patient Label Anatomical Subunit Percent Total Percent One Side Anterior Posterior Injury Subtotal 3.5% 2nd and 3rd degree burns
Guidelines are the Future of Sepsis Management Pro
 Guidelines are the Future of Sepsis Management Pro R. Phillip Dellinger MD, MCCM Professor and Chair of Medicine Director Adult Health Institute Senior Critical Care Attending Camden NJ USA Objectives
Guidelines are the Future of Sepsis Management Pro R. Phillip Dellinger MD, MCCM Professor and Chair of Medicine Director Adult Health Institute Senior Critical Care Attending Camden NJ USA Objectives
Non-invasive Ventilation protocol For COPD
 NHS LANARKSHIRE MONKLANDS HOSPITAL Non-invasive Ventilation protocol For COPD April 2017 S Baird Review Date: Oct 2019 Approved by Medical Directorate Indications for Non-Invasive Ventilation (NIV) NIV
NHS LANARKSHIRE MONKLANDS HOSPITAL Non-invasive Ventilation protocol For COPD April 2017 S Baird Review Date: Oct 2019 Approved by Medical Directorate Indications for Non-Invasive Ventilation (NIV) NIV
Objectives. Epidemiology of Sepsis. Review Guidelines for Resuscitation. Tx: EGDT, timing/choice of abx, activated
 Update on Surviving Sepsis 2008 Objectives Epidemiology of Sepsis Definition of Sepsis and Septic Shock Review Guidelines for Resuscitation Dx: Lactate, t cultures, SVO2 Tx: EGDT, timing/choice of abx,
Update on Surviving Sepsis 2008 Objectives Epidemiology of Sepsis Definition of Sepsis and Septic Shock Review Guidelines for Resuscitation Dx: Lactate, t cultures, SVO2 Tx: EGDT, timing/choice of abx,
Sepsis Bundle Project (SEP) Kathy Wonderly RN, MSEd, CPHQ Consultant Developed: April 2015 Most recent Revision: December 2018
 Kathy Wonderly RN, MSEd, CPHQ Consultant Developed: April 2015 Most recent Revision: December 2018") Sepsis Bundle Project (SEP) Kathy Wonderly RN, MSEd, CPHQ Consultant Developed: April 2015 Most recent Revision: December 2018 Objectives 1. To identify the symptom of severe sepsis and septic shock syndrome.
Sepsis Bundle Project (SEP) Kathy Wonderly RN, MSEd, CPHQ Consultant Developed: April 2015 Most recent Revision: December 2018 Objectives 1. To identify the symptom of severe sepsis and septic shock syndrome.
Acute Liver Failure: Supporting Other Organs
 Acute Liver Failure: Supporting Other Organs Michael A. Gropper, MD, PhD Professor of Anesthesia and Physiology Director, Critical Care Medicine University of California San Francisco Acute Liver Failure
Acute Liver Failure: Supporting Other Organs Michael A. Gropper, MD, PhD Professor of Anesthesia and Physiology Director, Critical Care Medicine University of California San Francisco Acute Liver Failure
INTENSIVE CARE MEDICINE CPD EVENING. Dr Alastair Morgan Wednesday 13 th September 2017
 INTENSIVE CARE MEDICINE CPD EVENING Dr Alastair Morgan Wednesday 13 th September 2017 WHAT IS NEW IN ICU? (RELEVANT TO ANAESTHETISTS) Not much! SURVIVING SEPSIS How many deaths in England were thought
INTENSIVE CARE MEDICINE CPD EVENING Dr Alastair Morgan Wednesday 13 th September 2017 WHAT IS NEW IN ICU? (RELEVANT TO ANAESTHETISTS) Not much! SURVIVING SEPSIS How many deaths in England were thought
PAEDIATRIC FEBRILE NEUTROPENIA CARE PATHWAY
 PAEDIATRIC FEBRILE NEUTROPENIA CARE PATHWAY Purpose: This document is intended as a guide to the investigation and management of children presenting in Salisbury District Hospital with suspected neutropenic
PAEDIATRIC FEBRILE NEUTROPENIA CARE PATHWAY Purpose: This document is intended as a guide to the investigation and management of children presenting in Salisbury District Hospital with suspected neutropenic
A Care Pathway exists for the management of neutropenic fever. Copies of the care pathway document are available in EAU, A&E, Deanesly and CHU.
 Subject: Neutropenic Fever Guideline for Junior Doctors Date of Implementation: January 2010 Date of Review: January 2012 Director Responsible for Implementation and Review: Policy location: Consultant
Subject: Neutropenic Fever Guideline for Junior Doctors Date of Implementation: January 2010 Date of Review: January 2012 Director Responsible for Implementation and Review: Policy location: Consultant
Jawad Nazir, MD, FACP Medical Director, Infection Prevention and Control Avera Health and Avera McKennan Hospital Clinical Associate Professor of
 Jawad Nazir, MD, FACP Medical Director, Infection Prevention and Control Avera Health and Avera McKennan Hospital Clinical Associate Professor of Medicine Sanford School of Medicine, Univ of South Dakota
Jawad Nazir, MD, FACP Medical Director, Infection Prevention and Control Avera Health and Avera McKennan Hospital Clinical Associate Professor of Medicine Sanford School of Medicine, Univ of South Dakota
-Cardiogenic: shock state resulting from impairment or failure of myocardium
 Shock chapter Shock -Condition in which tissue perfusion is inadequate to deliver oxygen, nutrients to support vital organs, cellular function -Affects all body systems -Classic signs of early shock: Tachycardia,tachypnea,restlessness,anxiety,
Shock chapter Shock -Condition in which tissue perfusion is inadequate to deliver oxygen, nutrients to support vital organs, cellular function -Affects all body systems -Classic signs of early shock: Tachycardia,tachypnea,restlessness,anxiety,
Oxygen: Is there a problem? Tom Heaps Acute Physician
 Oxygen: Is there a problem? Tom Heaps Acute Physician Case 1 79-year-old female, diabetic, morbidly obese Admitted with LVF Overnight Reduced GCS?cause 15l NRB in situ ABG showed ph 6.9, pco 2 15.9kPa
Oxygen: Is there a problem? Tom Heaps Acute Physician Case 1 79-year-old female, diabetic, morbidly obese Admitted with LVF Overnight Reduced GCS?cause 15l NRB in situ ABG showed ph 6.9, pco 2 15.9kPa
Sepsis - A Year in Transition
 Sepsis - A Year in Transition Todd L. Allen, MD, FACEP Chair, Emergency Department Development Team; Assistant Quality Officer, Institute for Healthcare Leadership Russell R. Miller, III, MD, MPH, FCCM
Sepsis - A Year in Transition Todd L. Allen, MD, FACEP Chair, Emergency Department Development Team; Assistant Quality Officer, Institute for Healthcare Leadership Russell R. Miller, III, MD, MPH, FCCM
Vasopressors in septic shock
 Vasopressors in septic shock Prof. Jean-Louis TEBOUL Medical ICU Bicetre hospital University Paris-South France Questions 1- Why do we use vasopressors in septic shock? 2- Which first-line agent? 3- When
Vasopressors in septic shock Prof. Jean-Louis TEBOUL Medical ICU Bicetre hospital University Paris-South France Questions 1- Why do we use vasopressors in septic shock? 2- Which first-line agent? 3- When
Sepsis new definitions of sepsis and septic shock and Novelities in sepsis treatment
 Sepsis new definitions of sepsis and septic shock and Novelities in sepsis treatment What is sepsis? Life-threatening organ dysfunction caused by a dysregulated host response to infection A 1991 consensus
Sepsis new definitions of sepsis and septic shock and Novelities in sepsis treatment What is sepsis? Life-threatening organ dysfunction caused by a dysregulated host response to infection A 1991 consensus
IDENTIFYING SEPSIS IN THE PREHOSPITAL SETTING
 IDENTIFYING SEPSIS IN THE PREHOSPITAL SETTING Christopher Hunter, MD, PhD, FACEP Director, Health Services Department Associate Medical Director, Orange County EMS System Medical Director, Orlando Health
IDENTIFYING SEPSIS IN THE PREHOSPITAL SETTING Christopher Hunter, MD, PhD, FACEP Director, Health Services Department Associate Medical Director, Orange County EMS System Medical Director, Orlando Health
Acute Kidney Injury shared guidance
 Acute Kidney Injury shared guidance Acute Kidney Injury (AKI) Fluid balance assessment (NICE CG 169) Assess the patient s likely fluid and electrolyte needs 1.History previous limited intake, thirst, abnormal
Acute Kidney Injury shared guidance Acute Kidney Injury (AKI) Fluid balance assessment (NICE CG 169) Assess the patient s likely fluid and electrolyte needs 1.History previous limited intake, thirst, abnormal
Paediatric Shock. Dr Andrew Pittaway Department of Anaesthesia Bristol Royal Hospital for Children Bristol, UK
 Paediatric Shock Dr Andrew Pittaway Department of Anaesthesia Bristol Royal Hospital for Children Bristol, UK Self-assessment: 1. What is the definition of shock? 2. List the different pathophysiological
Paediatric Shock Dr Andrew Pittaway Department of Anaesthesia Bristol Royal Hospital for Children Bristol, UK Self-assessment: 1. What is the definition of shock? 2. List the different pathophysiological
Management of Severe Sepsis:
 Management of Severe Sepsis: Update from the Surviving Sepsis Campaign Barbara Birriel, MSN, ACNP-BC, FCCM The Pennsylvania State University NONE Disclosures Review evidence-based international sepsis
Management of Severe Sepsis: Update from the Surviving Sepsis Campaign Barbara Birriel, MSN, ACNP-BC, FCCM The Pennsylvania State University NONE Disclosures Review evidence-based international sepsis
Organ Donor Management Recommended Guidelines ADULT CARDIAC DEATH (DCD)
") Date: Time: = Always applicable = Check if applicable ADMISSION INSTRUCTIONS Move to Comfort Care Note in chart. Contact initiated with BC Transplant Consent for Organ Donation obtained Code Status: Full
Date: Time: = Always applicable = Check if applicable ADMISSION INSTRUCTIONS Move to Comfort Care Note in chart. Contact initiated with BC Transplant Consent for Organ Donation obtained Code Status: Full
4/5/2018. Update on Sepsis NIKHIL JAGAN PULMONARY AND CRITICAL CARE CREIGHTON UNIVERSITY. I have no financial disclosures
 Update on Sepsis NIKHIL JAGAN PULMONARY AND CRITICAL CARE CREIGHTON UNIVERSITY I have no financial disclosures 1 Objectives Why do we care about sepsis Understanding the core measures by Centers for Medicare
Update on Sepsis NIKHIL JAGAN PULMONARY AND CRITICAL CARE CREIGHTON UNIVERSITY I have no financial disclosures 1 Objectives Why do we care about sepsis Understanding the core measures by Centers for Medicare
Brief summary of the NICE guidelines December 2013
 Brief summary of the NICE guidelines December 2013 Intravenous fluid therapy in adults in hospital the relevance to Emergency Department Care Applicable to patients 16 years and older receiving i.v. fluids
Brief summary of the NICE guidelines December 2013 Intravenous fluid therapy in adults in hospital the relevance to Emergency Department Care Applicable to patients 16 years and older receiving i.v. fluids
SCENARIO. Maternal Medicine -DKA LEARNING OBJECTIVES
 SCENARIO Maternal Medicine -DKA LEARNING OBJECTIVES Recognition of the of the seriously ill patient Diagnosis of DKA in pregnancy Recognition of precipitating factors for DKA Initiate emergency management
SCENARIO Maternal Medicine -DKA LEARNING OBJECTIVES Recognition of the of the seriously ill patient Diagnosis of DKA in pregnancy Recognition of precipitating factors for DKA Initiate emergency management
Organ Donor Management Recommended Guidelines ADULT Brain Death (NDD)
") Date: Time: = Always applicable = Check if applicable ADMISSION INSTRUCTIONS Neurological Determination of Death (NDD) has been performed by at least 2 licensed physicians Contact initiated with BC Transplant
Date: Time: = Always applicable = Check if applicable ADMISSION INSTRUCTIONS Neurological Determination of Death (NDD) has been performed by at least 2 licensed physicians Contact initiated with BC Transplant
Presented by: Indah Dwi Pratiwi
 Presented by: Indah Dwi Pratiwi Normal Fluid Requirements Resuscitation Fluids Goals of Resuscitation Maintain normal body temperature In most cases, elevate the feet and legs above the level of the heart
Presented by: Indah Dwi Pratiwi Normal Fluid Requirements Resuscitation Fluids Goals of Resuscitation Maintain normal body temperature In most cases, elevate the feet and legs above the level of the heart
Practical. Septic shock resuscitation ไชยร ตน เพ มพ ก ล พบ. ภาคว ชาอาย รศาสตร คณะแพทยศาสตร ศ ร ราชพยาบาล
 Practical Septic shock resuscitation ไ ไชยร ตน เพ มพ ก ล พบ. ภาคว ชาอาย รศาสตร คณะแพทยศาสตร ศ ร ราชพยาบาล ประช มว ชาการ 101 ป อาย รศาสตร ศ ร ราช 6 ก มภาพ นธ 2561 Early recognition Early resuscitation Early
Practical Septic shock resuscitation ไ ไชยร ตน เพ มพ ก ล พบ. ภาคว ชาอาย รศาสตร คณะแพทยศาสตร ศ ร ราชพยาบาล ประช มว ชาการ 101 ป อาย รศาสตร ศ ร ราช 6 ก มภาพ นธ 2561 Early recognition Early resuscitation Early
Sepsis care and the new core measures
 Sepsis care and the new core measures Daniel S. Hagg, MD January 15, 2016 Outline What is sepsis? A brief history of sepsis care How should we take care of septic patients now? Core measures What strategies
Sepsis care and the new core measures Daniel S. Hagg, MD January 15, 2016 Outline What is sepsis? A brief history of sepsis care How should we take care of septic patients now? Core measures What strategies
MANAGEMENT OF DENGUE INFECTION IN ADULTS (Revised 2 nd Edition) QUICK REFERENCE FOR HEALTHCARE PROVIDERS
 QUICK REFERENCE FOR HEALTHCARE PROVIDERS") 1 KEY MESSAGES Dengue is a dynamic disease and presented in three phases - febrile phase, critical phase and recovery phase. Clinical deterioration often occurs in the critical phase and is marked by plasma
1 KEY MESSAGES Dengue is a dynamic disease and presented in three phases - febrile phase, critical phase and recovery phase. Clinical deterioration often occurs in the critical phase and is marked by plasma
The Ever Changing World of Sepsis Management. Laura Evans MD MSc Medical Director of Critical Care Bellevue Hospital
 The Ever Changing World of Sepsis Management Laura Evans MD MSc Medical Director of Critical Care Bellevue Hospital COI Disclosures No financial interests to disclose Learning Objectives Review the evolution
The Ever Changing World of Sepsis Management Laura Evans MD MSc Medical Director of Critical Care Bellevue Hospital COI Disclosures No financial interests to disclose Learning Objectives Review the evolution
ACUTE KIDNEY INJURY FOCUS ON OBSTETRICS DONNA HIGGINS, CLINICAL NURSE EDUCATOR, NORTHERN LINCOLNSHIRE HOSPITALS NHS FOUNDATION TRUST
 ACUTE KIDNEY INJURY FOCUS ON OBSTETRICS DONNA HIGGINS, CLINICAL NURSE EDUCATOR, NORTHERN LINCOLNSHIRE HOSPITALS NHS FOUNDATION TRUST AIMS & OBJECTIVES Review the functions of the kidney Identify renal
ACUTE KIDNEY INJURY FOCUS ON OBSTETRICS DONNA HIGGINS, CLINICAL NURSE EDUCATOR, NORTHERN LINCOLNSHIRE HOSPITALS NHS FOUNDATION TRUST AIMS & OBJECTIVES Review the functions of the kidney Identify renal
6/5/2014. Sepsis Management and Hemodynamics. 2004: International group of experts,
 Sepsis Management and Hemodynamics Javier Perez-Fernandez, M.D., F.C.C.P. Medical Director Critical Care Services, Baptist t Hospital of Miamii Medical Director Pulmonary Services, West Kendall Baptist
Sepsis Management and Hemodynamics Javier Perez-Fernandez, M.D., F.C.C.P. Medical Director Critical Care Services, Baptist t Hospital of Miamii Medical Director Pulmonary Services, West Kendall Baptist
Rounds in the ICU. Eran Segal, MD Director General ICU Sheba Medical Center
 Rounds in the ICU Eran Segal, MD Director General ICU Sheba Medical Center Real Clinical cases (including our mistakes) Emphasis on hemodynamic monitoring Usually no single correct answer We will conduct
Rounds in the ICU Eran Segal, MD Director General ICU Sheba Medical Center Real Clinical cases (including our mistakes) Emphasis on hemodynamic monitoring Usually no single correct answer We will conduct
Communicable Diseases EMT REFRESHER NCCP 2018 JTEMPLE
 Communicable Diseases EMT REFRESHER NCCP 2018 JTEMPLE When are Standard Precautions used? The use of Standard Precautions during patient care is determined by the nature of the anticipated interaction
Communicable Diseases EMT REFRESHER NCCP 2018 JTEMPLE When are Standard Precautions used? The use of Standard Precautions during patient care is determined by the nature of the anticipated interaction
Please inform the Diabetes Nurse Specialist that this patient has been admitted within 24hrs of admission.
 Adult Diabetic Ketoacidosis Care Bundle (V1. Issued October 2014 Review October 2015) Improving patient care This pack includes: DKA Management Guideline Name: (Patient Addressograph) DOB: Hospital No:
Adult Diabetic Ketoacidosis Care Bundle (V1. Issued October 2014 Review October 2015) Improving patient care This pack includes: DKA Management Guideline Name: (Patient Addressograph) DOB: Hospital No: