Is bypass surgery needed for elderly patients with LMT disease? From the surgical point of view
|
|
|
- Derrick O’Brien’
- 5 years ago
- Views:
Transcription
1 CCT 2003 (Kobe) Is bypass surgery needed for elderly patients with LMT disease? From the surgical point of view Hitoshi Yaku, MD, PhD Department of Cardiovascular Surgery Kyoto Prefectural University of Medicine
2
3 Randomized Trials (PCI vs CABG) PCI CABG Mortality Cardiac Events Long-Term Survival
4 PCI for Unprotected LMT disease O Keefe JH et al. Am J Cardiol 1989;64: Technical feasibility 3-year mortality: 64% Ellis SG et al. Circulation 1997;96: Initial report from the ULTIMA registry (n=107) 6-months mortality: 10.6% Park S-J et al. J Am Coll Cardiol 1998;31: patients with normal LV In-hospital mortality: 0% Restenosis (unstable AP): 17% within 2 months Tan WA et al. Circulation 2001;104:1609 ULTIMA registry (n=279) Hospital mortality: 13.7%, 1-year mortality: 24.2% For low risk group (32%) In-hospital mortality: 0%, 1-year mortality: 3.4%
5 CABG for patients with LMT disease Ellis SG et al. Am Heart J 1998;135: In-hospital mortality: 2.3% 3-year mortality: 15.6% STS National Database 1997 In-hospital mortality: 2.8% Annual Report 2003 from JACAS In-hospital mortality (elective): 1.12% (LMT only) 0.91% (LMT + 1VD) 1.68% (LMT + 2VD) 1.68% (LMT + 3VD)
6 Recent Evolution of Techniques and Devices PCI Rotational Coronary Atherectomy Directional Coronary Atherectomy New Stents (Drug Eluting Stents) GP IIb/IIIa receptor blockers PCPS CABG Aggressive use of arterial conduits Off-Pump CABG techniques
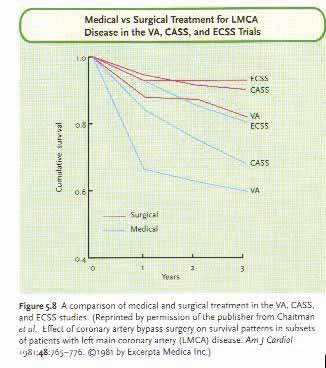
7 Coronary bypass surgery with internal-thoracic-artery grafts -Effects on survival over a 15-year-period Cameron A et al. N Engl J Med 1996;334:
8 Effect of arterial revascularization on survival: a systematic review of studies comparing bilateral and single internal mammary arteries Taggart DP. Lancet 2001;358:
9 Improved survival with multiple left-sided bilateral internal thoracic artery grafts Schmidt SE. Ann Thorac Surg 1997;64:9-15
10
11
12 Off-Pump CABG (Personal Experience, HY) Kyoto Prefectural University of Medicine (Kyoto) 310 cases Takahashi Hospital (Kobe) 129 cases Kyoto Miniren Chuo Hospital (Kyoto) 47 cases Saiseikai Suita Hospital (Osaka) 13 cases Makiminato Central Hospital (Okinawa) 10 cases Uemura Hospital (Kagoshima) 5 cases Marutamachi Hospital (Kyoto) 4 cases Kumamoto Red Cross Hospital (Kumamoto) 2 cases Total 520 cases
13 % of Off-Pump CABG in Isolated CABG (Kyoto Prefectural University of Medicine) (%)
14 Questions - Less Invasive? Operative Mortality & Morbidity - Quality of Grafting? Graft Patency Long-term Results
15 Subjects (Kyoto Prefectural University of Medicine) Off-Pump CABG ( ) Consecutive 311 cases (including MIDCAB) On-Pump CABG ( ) Consecutive 198 cases (isolated CABG) Aortic Cross Clamp 127 cases 71 cases
16 Patients Characteristics Off-Pump CABG On-Pump CABG (n = 311) (n = 198) p value Age (years) < Sex (M:F) 235 : : 56 NS Cerebrovasc Dis 177 (56%) 60 (30%) < > > moderate risk) Renal Dysfunction 33 (11%) 7 (4%) < 0.05 Cr > 1.5 mg/dl) DM 139 (44%) 78 (39%) NS Emergent/Urgent 136 (43%) 71 (36%) NS No. of Cor Dis NS LMT Lesion 112 (36%) 67 (34%) NS LVEF (%) < 0.05 Pre Op IABP 14 (5%) 14 (7%) NS
17 Early Results Off-Pump CABG On-Pump CABG (n = 311) (n = 198) p value LOS 17 (5%) 9 (5%) NS PMI 14 (4%) 11 (6%) NS CKMB max (IU/dl) < Circ Support 5 (2%) 8 (4%) NS Af 80 (25%) 23 (11%) NS Renal Dysfunction 53 (17%) 20 (10%) NS Cr max (mg/dl) NS Prolonged Ventilation 12 (4%) 16 (11%) < 0.01 Mediastinitis 0 (0%) 0 (0%) NS CRP max (mg/dl) NS Stroke Intraop 0 (0%) 4 (2%) < 0.05 Postop 3 (1%) 2 (1%) NS TIA 2 (0.6%) 3 (2%) NS Mortality 1 (0.3%) 1 (0.5%) NS
18 (rate) Survival On:89% Off:79% NS (Months) (Months)
19 (rate) Freedom from Cardiac Death On:94% Off:88% NS (Months)
20 (rate) Freedom from Cardiac Events On:81% Off:65% NS (Months)
21 (rate) Freedom from PCI On:90% Off:88% NS (Months)
22 Clinical Risk Factors Affecting In-Hospital Adverse Events Outcomes (PCI) Advanced age Female gender Diabetes Prior MI Multivessel disease Left main or equivalent coronary disease A large area of myocardium at risk Pre-existing impairment of LV or renal function Collateral vessels supplying significant areas of myocardium that originate distal to the segment to be dilated
23 Risk Factors Affecting Hospital Outcomes (CABG) Urgency of operation Advanced age 1 or more prior coronary bypass surgery Left ventricular EF < 40% Female sex Peripheral vascular disease Dialysis or creatinine > 2 mg/dl COPD Irrespective to Lesion site or Lesion Morphology
24 Patients Characteristics (Off-Pump CABG) LMT Lesion (+) LMT Lesion (-) (n = 113) (n = 186) p value Age (years) NS Sex (M:F) 90 : : 48 NS Cerebrovasc Dis 69 (62%) 101 (54%) NS > moderate risk) Renal Dysfunction 10 (9%) 21 (11%) NS Cr > 1.5 mg/dl) DM 48 (43%) 84 (45%) NS Emergent/Urgent 71 (64%) 61 (33%) < No. of Cor Dis < LVEF (%) NS Pre Op IABP 8 (7%) 6 (3%) NS
25 Early Results (Off-Pump CABG) LMT Lesion (+) LMT Lesion (-) (n = 113) (n = 186) p value LOS 9 (8%) 9 (5%) NS PMI 9 (8%) 5 (3%) < 0.05 CKMB max (IU/dl) < Af 32 (29%) 49 (26%) NS Renal Dysfunction 25 (22%) 28 (15%) NS Ventilation Time (hours) NS ICU Stay (days) NS Mediastinitis 0 (0%) 0 (0%) NS CRP max (mg/dl) NS Stroke Intraop 0 (0%) 0 (0%) NS Postop 2 (3%) 1 (0.5%) NS TIA 0 (0%) 3 (1.5%) NS Mortality 1 (0.9%) (pre op AMI) 0 (0%) NS
26 Survival (Off-Pump CABG) (rate) 1 LMT(-) :83% ns 0.5 LMT(+) :73% (Months)
27 (rate) Freedom from Cardiac Death (Off-Pump CABG) LMT(+) :91% LMT(-) :87% ns (Months)
28 (rate) 1 Freedom from Cardiac Events (Off-Pump CABG) LMT(+) :82% ns 0.5 LMT(-) :63% (Months)
29 (rate) 1 Freedom from PCI (Off-Pump CABG) LMT(+) :94% ns 0.5 LMT(-) :84% (Months)
30 Patients Characteristics (Off-Pump CABG, LMT Lesion (+)) Age > 70 years Age < 70 years (n = 61) (n = 52) p value Age (years) < Sex (M:F) 45 : : 6 < 0.05 Cerebrovasc Dis 42 (69%) 27 (52%) NS > moderate risk) Renal Dysfunction 5 (8%) 5 (10%) NS Cr > 1.5 mg/dl) DM 29 (48%) 19 (37%) NS Emergent/Urgent 49 (80%) 22 (42%) < No. of Cor Dis NS LVEF (%) NS Pre Op IABP 4 (7%) 4 (8%) NS
31 Early Results (Off-Pump CABG, LMT Lesion (+)) Age > 70 years Age <70 years (n = 61) (n = 52) p value LOS 4 (7%) 5 (10%) NS PMI 3 (5%) 6 (12%) NS CKMB max (IU/dl) NS Af 19 (31%) 13 (25%) NS Renal Dysfunction 18 (30%) 7 (13%) < 0.05 Ventilation Time (hours) NS ICU Stay (days) NS Mediastinitis 0 (0%) 0 (0%) NS CRP max (mg/dl) NS Stroke Intraop 0 (0%) 0 (0%) NS Postop 2 (3%) 0 (0%) NS TIA 0 (0%) 0 (0%) NS Mortality 1 (1.6%) (pre op AMI) 0 (0%) NS
32 Survival (Off-Pump CABG, LMT Lesion (+)) (rate) 1 Under 70 :91% ns 0.5 Over 70 :67% (Months)
33 Freedom from Cardiac Death (Off Pump CABG, LMT Lesion(+)) (rate) Under 70 :100% Over 70 :86% ns (Months)
34 Freedom from Cardiac Events (Off Pump CABG, LMT Lesion(+)) (rate) Under 70 :98% p < 0.05 Over 70 :74% (Months)
35 Freedom from PCI (Off-Pump CABG, LMT Lesion (+)) (rate) Under 70 :98% Over 70 :91% ns (Months)
36 Summary - The operative mortality, 1-year mortality, and 5-year mortality of Off-Pump CABG for patients with LMT disease were 0.9%, 3.5%, and 27%, respectively. - The operative mortality, 1-year mortality, and 5-year mortality of Off-Pump CABG for elderly patients with LMT disease were 1.8%, 4.9%, and 33%, respectively. - The operative mortality of Off-Pump CABG for patients with/without LMT disease without AMI was actually zero.
37 Conclusions - CABG can be performed even for elderly patients with LMT disease with reasonably low mortality and morbidity and good long-term results. - CABG is a choice of care even for elderly patients with LMT disease as long as the patients is in a stable hemodynamic condition.
Coronary Artery Bypass Grafting in Diabetics: All Arterial or Hybrid?
 Coronary Artery Bypass Grafting in Diabetics: All Arterial or Hybrid? Dr. Daniel Navia M.D. Chief Cardiac Surgery Department ICBA, Buenos Aires Argentina, 2018 No disclosures 2 Current evidence The FREEDOM
Coronary Artery Bypass Grafting in Diabetics: All Arterial or Hybrid? Dr. Daniel Navia M.D. Chief Cardiac Surgery Department ICBA, Buenos Aires Argentina, 2018 No disclosures 2 Current evidence The FREEDOM
Revascularization after Drug-Eluting Stent Implantation or Coronary Artery Bypass Surgery for Multivessel Coronary Disease
 Impact of Angiographic Complete Revascularization after Drug-Eluting Stent Implantation or Coronary Artery Bypass Surgery for Multivessel Coronary Disease Young-Hak Kim, Duk-Woo Park, Jong-Young Lee, Won-Jang
Impact of Angiographic Complete Revascularization after Drug-Eluting Stent Implantation or Coronary Artery Bypass Surgery for Multivessel Coronary Disease Young-Hak Kim, Duk-Woo Park, Jong-Young Lee, Won-Jang
Unprotected LM intervention
 Unprotected LM intervention Guideline for COMBAT Seung-Jung Park, MD, PhD Professor of Internal Medicine, Seoul, Korea Current Recommendation for unprotected LMCA Stenosis Class IIb C in ESC guideline
Unprotected LM intervention Guideline for COMBAT Seung-Jung Park, MD, PhD Professor of Internal Medicine, Seoul, Korea Current Recommendation for unprotected LMCA Stenosis Class IIb C in ESC guideline
Safety of Single- Versus Multi-vessel Angioplasty for Patients with AMI and Multi-vessel CAD
 Safety of Single- Versus Multi-vessel Angioplasty for Patients with AMI and Multi-vessel CAD Mun K. Hong, MD Associate Professor of Medicine Director, Cardiovascular Intervention and Research Weill Cornell
Safety of Single- Versus Multi-vessel Angioplasty for Patients with AMI and Multi-vessel CAD Mun K. Hong, MD Associate Professor of Medicine Director, Cardiovascular Intervention and Research Weill Cornell
LM stenting - Cypher
 LM stenting - Cypher Left main stenting with BMS Since 1995 Issues in BMS era AMC Restenosis and TLR (%) 3 27 TLR P=.282 Restenosis P=.71 28 2 1 15 12 Ostium 5 4 Shaft Bifurcation Left main stenting with
LM stenting - Cypher Left main stenting with BMS Since 1995 Issues in BMS era AMC Restenosis and TLR (%) 3 27 TLR P=.282 Restenosis P=.71 28 2 1 15 12 Ostium 5 4 Shaft Bifurcation Left main stenting with
On-Pump vs. Off-Pump CABG: The Controversy Continues. Miguel Sousa Uva Immediate Past President European Association for Cardiothoracic Surgery
 On-Pump vs. Off-Pump CABG: The Controversy Continues Miguel Sousa Uva Immediate Past President European Association for Cardiothoracic Surgery On-pump vs. Off-Pump CABG: The Controversy Continues Conflict
On-Pump vs. Off-Pump CABG: The Controversy Continues Miguel Sousa Uva Immediate Past President European Association for Cardiothoracic Surgery On-pump vs. Off-Pump CABG: The Controversy Continues Conflict
Declaration of conflict of interest NONE
 Declaration of conflict of interest NONE Claudio Muneretto MD, PhD Director of Division of Cardiac Surgery University of Brescia Medical School Italy Hybrid Chymera Different features and potential advantages
Declaration of conflict of interest NONE Claudio Muneretto MD, PhD Director of Division of Cardiac Surgery University of Brescia Medical School Italy Hybrid Chymera Different features and potential advantages
CORONARY ARTERY BYPASS GRAFT (CABG) MEASURES GROUP OVERVIEW
 MEASURES GROUP OVERVIEW") CONARY ARTERY BYPASS GRAFT (CABG) MEASURES GROUP OVERVIEW 2015 PQRS OPTIONS F MEASURES GROUPS: 2015 PQRS MEASURES IN CONARY ARTERY BYPASS GRAFT (CABG) MEASURES GROUP: #43 Coronary Artery Bypass Graft (CABG):
CONARY ARTERY BYPASS GRAFT (CABG) MEASURES GROUP OVERVIEW 2015 PQRS OPTIONS F MEASURES GROUPS: 2015 PQRS MEASURES IN CONARY ARTERY BYPASS GRAFT (CABG) MEASURES GROUP: #43 Coronary Artery Bypass Graft (CABG):
OPCAB IS NOT BETTER THAN CONVENTIONAL CABG
 OPCAB IS NOT BETTER THAN CONVENTIONAL CABG Harold L. Lazar, M.D. Harold L. Lazar, M.D. Professor of Cardiothoracic Surgery Boston Medical Center and the Boston University School of Medicine Boston, MA
OPCAB IS NOT BETTER THAN CONVENTIONAL CABG Harold L. Lazar, M.D. Harold L. Lazar, M.D. Professor of Cardiothoracic Surgery Boston Medical Center and the Boston University School of Medicine Boston, MA
Implications of the New ESC/EACTS Guidelines for Myocardial Revascularization in 2011
 Implications of the New ESC/EACTS Guidelines for Myocardial Revascularization in 2011 Prof. Dr. Volkmar Falk Klinik für Herz- und Gefäßchirurgie, Universitätsspital Zürich, Schweiz In 2004 headlines were
Implications of the New ESC/EACTS Guidelines for Myocardial Revascularization in 2011 Prof. Dr. Volkmar Falk Klinik für Herz- und Gefäßchirurgie, Universitätsspital Zürich, Schweiz In 2004 headlines were
PCI for Left Anterior Descending Artery Ostial Stenosis
 PCI for Left Anterior Descending Artery Ostial Stenosis Why do you hesitate PCI for LAD ostial stenosis? LAD Ostial Lesion Limitations of PCI High elastic recoil Involvement of the distal left main coronary
PCI for Left Anterior Descending Artery Ostial Stenosis Why do you hesitate PCI for LAD ostial stenosis? LAD Ostial Lesion Limitations of PCI High elastic recoil Involvement of the distal left main coronary
Ted Feldman, M.D., MSCAI FACC FESC
 Support Technologies and High Risk Intervention Patient Selection: When Not to Use Them Ted Feldman, M.D., MSCAI FACC FESC Evanston Hospital SCAI Fall Fellows Course Las Vegas December 7-10 th, 2014 Ted
Support Technologies and High Risk Intervention Patient Selection: When Not to Use Them Ted Feldman, M.D., MSCAI FACC FESC Evanston Hospital SCAI Fall Fellows Course Las Vegas December 7-10 th, 2014 Ted
Ischemic Heart Disease Interventional Treatment
 Ischemic Heart Disease Interventional Treatment Cardiac Catheterization Laboratory Procedures (N = 89) is a regional and national referral center for percutaneous coronary intervention (PCI). A total of
Ischemic Heart Disease Interventional Treatment Cardiac Catheterization Laboratory Procedures (N = 89) is a regional and national referral center for percutaneous coronary intervention (PCI). A total of
PCI in Patients with Transplant Coronary Artery Disease. Michael S. Lee, MD, FACC, FSCAI Assistant Professor UCLA School of Medicine
 PCI in Patients with Transplant Coronary Artery Disease Michael S. Lee, MD, FACC, FSCAI Assistant Professor UCLA School of Medicine Faculty Disclosure Honararia for Boston Scientific, BMS, Daiichi Sankyo,
PCI in Patients with Transplant Coronary Artery Disease Michael S. Lee, MD, FACC, FSCAI Assistant Professor UCLA School of Medicine Faculty Disclosure Honararia for Boston Scientific, BMS, Daiichi Sankyo,
Surgical vs. Percutaneous Revascularization in Patients with Diabetes and Acute Coronary Syndrome
 Surgical vs. Percutaneous Revascularization in Patients with Diabetes and Acute Coronary Syndrome Chris C. Cook, MD Associate Professor of Surgery Director, CT Residency Program, WVU ACOI 10/17/18 No Disclosures
Surgical vs. Percutaneous Revascularization in Patients with Diabetes and Acute Coronary Syndrome Chris C. Cook, MD Associate Professor of Surgery Director, CT Residency Program, WVU ACOI 10/17/18 No Disclosures
ISAR-LEFT MAIN: A Randomized Clinical Trial on Drug-Eluting Stents for Unprotected Left Main Lesions
 Julinda Mehilli, MD Deutsches Herzzentrum Technische Universität Munich Germany ISAR-LEFT MAIN: A Randomized Clinical Trial on Drug-Eluting Stents for Unprotected Left Main Lesions Background Left main
Julinda Mehilli, MD Deutsches Herzzentrum Technische Universität Munich Germany ISAR-LEFT MAIN: A Randomized Clinical Trial on Drug-Eluting Stents for Unprotected Left Main Lesions Background Left main
Measure #167 (NQF 0114): Coronary Artery Bypass Graft (CABG): Postoperative Renal Failure National Quality Strategy Domain: Effective Clinical Care
: Coronary Artery Bypass Graft (CABG): Postoperative Renal Failure National Quality Strategy Domain: Effective Clinical Care") Measure #167 (NQF 0114): Coronary Artery Bypass Graft (CABG): Postoperative Renal Failure National Quality Strategy Domain: Effective Clinical Care 2017 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY MEASURE
Measure #167 (NQF 0114): Coronary Artery Bypass Graft (CABG): Postoperative Renal Failure National Quality Strategy Domain: Effective Clinical Care 2017 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY MEASURE
Surgery Grand Rounds
 Surgery Grand Rounds Coronary Artery Bypass Grafting versus Coronary Artery Stenting Charles Ted Lord, R1 Coronary Artery Disease Stenosis of epicardial vessels Metabolic & hematologic Statistics 500,000
Surgery Grand Rounds Coronary Artery Bypass Grafting versus Coronary Artery Stenting Charles Ted Lord, R1 Coronary Artery Disease Stenosis of epicardial vessels Metabolic & hematologic Statistics 500,000
EACTS Adult Cardiac Database
 EACTS Adult Cardiac Database Quality Improvement Programme List of changes to Version 2.0, 13 th Dec 2018, compared to version 1.0, 1 st May 2014. INTRODUCTORY NOTES This document s purpose is to list
EACTS Adult Cardiac Database Quality Improvement Programme List of changes to Version 2.0, 13 th Dec 2018, compared to version 1.0, 1 st May 2014. INTRODUCTORY NOTES This document s purpose is to list
Multivessel Coronary Artery Disease : CABG. Zürich, F. Siclari MD
 Multivessel Coronary Artery Disease : CABG Zürich, 10.06.2015 F. Siclari MD Coronary Artery Ruptured Plaque Pathological process with definite subsequent vascular changes most of them irreversible CABG
Multivessel Coronary Artery Disease : CABG Zürich, 10.06.2015 F. Siclari MD Coronary Artery Ruptured Plaque Pathological process with definite subsequent vascular changes most of them irreversible CABG
Ischemic Heart Disease Interventional Treatment
 Ischemic Heart Disease Interventional Treatment Cardiac Catheterization Laboratory Procedures (N = 11,61) is a regional and national referral center for percutaneous coronary intervention (PCI). A total
Ischemic Heart Disease Interventional Treatment Cardiac Catheterization Laboratory Procedures (N = 11,61) is a regional and national referral center for percutaneous coronary intervention (PCI). A total
SURGICAL MYOCARDIAL REVASCULARIZATION: ARTERIAL VS VENOUS GRAFTS, SINGLE VS MULTIPLE GRAFTS?
 SURGICAL MYOCARDIAL REVASCULARIZATION: ARTERIAL VS VENOUS GRAFTS, SINGLE VS MULTIPLE GRAFTS? Luigi Martinelli Chief, Dept. of Surgery Istituto Clinico Ligure di Alta Specialità RAPALLO During 1987 2006,
SURGICAL MYOCARDIAL REVASCULARIZATION: ARTERIAL VS VENOUS GRAFTS, SINGLE VS MULTIPLE GRAFTS? Luigi Martinelli Chief, Dept. of Surgery Istituto Clinico Ligure di Alta Specialità RAPALLO During 1987 2006,
Lessons learned From The National PCI Registry
 Lessons learned From The National PCI Registry w a v e On Behalf of The Publication Committee of the National PCI Registry Objectives & Anticipated Achievements To determine the epidemiology of patients
Lessons learned From The National PCI Registry w a v e On Behalf of The Publication Committee of the National PCI Registry Objectives & Anticipated Achievements To determine the epidemiology of patients
PCI for Renal Artery stenosis
 PCI for Renal Artery stenosis Why should we treat Renal Artery Stenosis? Natural History of RAS RAS is progressive disease Study Follow-up (months) Pts Progression N (%) Total occlusion Wollenweber Meaney
PCI for Renal Artery stenosis Why should we treat Renal Artery Stenosis? Natural History of RAS RAS is progressive disease Study Follow-up (months) Pts Progression N (%) Total occlusion Wollenweber Meaney
VCU Pauley Heart Center: A 2009 US News Top 50 Heart and Heart Surgery Hospital
 VCU Pauley Heart Center: A 2009 US News Top 50 Heart and Heart Surgery Hospital Complex PCI: Multivessel Disease George W. Vetrovec, MD. Kimmerling Chair of Cardiology VCU Pauley Heart Center Virginia
VCU Pauley Heart Center: A 2009 US News Top 50 Heart and Heart Surgery Hospital Complex PCI: Multivessel Disease George W. Vetrovec, MD. Kimmerling Chair of Cardiology VCU Pauley Heart Center Virginia
Supplementary Online Content
 Supplementary Online Content Valle JA, Tamez H, Abbott JD, et al. Contemporary use and trends in unprotected left main coronary artery percutaneous coronary intervention in the United States: an analysis
Supplementary Online Content Valle JA, Tamez H, Abbott JD, et al. Contemporary use and trends in unprotected left main coronary artery percutaneous coronary intervention in the United States: an analysis
Most Patients with Elective Left Main Disease. Farrel Hellig
 Most Patients with Elective Left Main Disease Should be Treated with PCI! Farrel Hellig Sunnnghill and Sunward Park Hospitals Johannesburg South Africa Everything that can be invented has been invented
Most Patients with Elective Left Main Disease Should be Treated with PCI! Farrel Hellig Sunnnghill and Sunward Park Hospitals Johannesburg South Africa Everything that can be invented has been invented
CABG alone. It s enough? / Μόνο η αορτοστεφανιαία παράκαμψη είναι αρκετή;
 LV Aneurysm and VSD in Ischaemic Heart Failure / Στεφανιαία νόσος, ανεύρυσμα αριστεράς κοιλίας και VSD CABG alone. It s enough? / Μόνο η αορτοστεφανιαία παράκαμψη είναι αρκετή; THEODOROS KARAISKOS CONSULTANT
LV Aneurysm and VSD in Ischaemic Heart Failure / Στεφανιαία νόσος, ανεύρυσμα αριστεράς κοιλίας και VSD CABG alone. It s enough? / Μόνο η αορτοστεφανιαία παράκαμψη είναι αρκετή; THEODOROS KARAISKOS CONSULTANT
PCI for Left Main Coronary Artery Stenosis. Jean Fajadet Clinique Pasteur, Toulouse, France
 PCI for Left Main Coronary Artery Stenosis Jean Fajadet Clinique Pasteur, Toulouse, France Athens, October 19, 2018 Left Main Coronary Artery Disease Significant unprotected left main coronary artery disease
PCI for Left Main Coronary Artery Stenosis Jean Fajadet Clinique Pasteur, Toulouse, France Athens, October 19, 2018 Left Main Coronary Artery Disease Significant unprotected left main coronary artery disease
New Jersey Cardiac Catheterization Data Registry, Version 2.0 (Please report data only for patients 16 years or older.)
") A. ADMINISTRATIVE New Jersey Cardiac Catheterization Data Registry, Version 2.0 (Please report data only for patients 16 years or older.) 1. Facility Code: 2. Facility Name: 3. Procedure Type (Choose only
A. ADMINISTRATIVE New Jersey Cardiac Catheterization Data Registry, Version 2.0 (Please report data only for patients 16 years or older.) 1. Facility Code: 2. Facility Name: 3. Procedure Type (Choose only
Cardiac evaluation for the noncardiac. Nathaen Weitzel MD University of Colorado Denver Dept of Anesthesiology
 Cardiac evaluation for the noncardiac patient Nathaen Weitzel MD University of Colorado Denver Dept of Anesthesiology Objectives! Review ACC / AHA guidelines as updated for 2009! Discuss new recommendations
Cardiac evaluation for the noncardiac patient Nathaen Weitzel MD University of Colorado Denver Dept of Anesthesiology Objectives! Review ACC / AHA guidelines as updated for 2009! Discuss new recommendations
DESCRIPTION: Percentage of patients aged 18 years and older undergoing isolated CABG surgery who received an IMA graft
 Measure #43 (NQF 0134): Coronary Artery Bypass Graft (CABG): Use of Internal Mammary Artery (IMA) in Patients with Isolated CABG Surgery National Quality Strategy Domain: Effective Clinical Care 2017 OPTIONS
Measure #43 (NQF 0134): Coronary Artery Bypass Graft (CABG): Use of Internal Mammary Artery (IMA) in Patients with Isolated CABG Surgery National Quality Strategy Domain: Effective Clinical Care 2017 OPTIONS
Chronic Total Occlusions. Stephen Cook, MD Medical Director, Cardiac Catheterization Laboratory Oregon Heart & Vascular Institute
 Chronic Total Occlusions Stephen Cook, MD Medical Director, Cardiac Catheterization Laboratory Oregon Heart & Vascular Institute Financial Disclosures /see -tee-oh / abbr. Med. Chronic Total Occlusion,
Chronic Total Occlusions Stephen Cook, MD Medical Director, Cardiac Catheterization Laboratory Oregon Heart & Vascular Institute Financial Disclosures /see -tee-oh / abbr. Med. Chronic Total Occlusion,
Who is the high risk patient?
 Who is the high risk patient? High risk of periprocedural death or other major complications (hemodynamic compromise, MI, stroke, dialysis) Contributors of Risk Lesion/Procedure Governed by 1. Patient
Who is the high risk patient? High risk of periprocedural death or other major complications (hemodynamic compromise, MI, stroke, dialysis) Contributors of Risk Lesion/Procedure Governed by 1. Patient
Randomized comparison of single versus double mammary coronary artery bypass grafting: 5 year outcomes of the Arterial Revascularization Trial
 Randomized comparison of single versus double mammary coronary artery bypass grafting: 5 year outcomes of the Arterial Revascularization Trial Embargoed until 10:45 a.m. CT, Monday, Nov. 14, 2016 David
Randomized comparison of single versus double mammary coronary artery bypass grafting: 5 year outcomes of the Arterial Revascularization Trial Embargoed until 10:45 a.m. CT, Monday, Nov. 14, 2016 David
THE NATIONAL QUALITY FORUM
 THE NATIONAL QUALITY FORUM National Voluntary Consensus Standards for Patient Outcomes Table of Measures Submitted-Phase 1 As of March 5, 2010 Note: This information is for personal and noncommercial use
THE NATIONAL QUALITY FORUM National Voluntary Consensus Standards for Patient Outcomes Table of Measures Submitted-Phase 1 As of March 5, 2010 Note: This information is for personal and noncommercial use
Prevention of Coronary Stent Thrombosis and Restenosis
 Prevention of Coronary Stent Thrombosis and Restenosis Seong-Wook Park, MD, PhD, FACC Division of Cardiology, Asan Medical Center University of Ulsan College of Medicine, Seoul, Korea 9/12/03 Coronary
Prevention of Coronary Stent Thrombosis and Restenosis Seong-Wook Park, MD, PhD, FACC Division of Cardiology, Asan Medical Center University of Ulsan College of Medicine, Seoul, Korea 9/12/03 Coronary
How to Perform Hybrid Myocardial Revascularisation: Interventional Perspective
 How to Perform Hybrid Myocardial Revascularisation: Interventional Perspective Gerhard Schuler Herzzentrum Leipzig Nothing to disclose Hybrid An animal or a plant resulting from a cross between genetically
How to Perform Hybrid Myocardial Revascularisation: Interventional Perspective Gerhard Schuler Herzzentrum Leipzig Nothing to disclose Hybrid An animal or a plant resulting from a cross between genetically
High Risk PCI for Heart Failure
 High Risk PCI for Heart Failure Ray Matthews MD Professor of Clinical Medicine Chief, Division of Cardiovascular Medicine University of Southern California Los Angeles, California Disclosures Abiomed Research
High Risk PCI for Heart Failure Ray Matthews MD Professor of Clinical Medicine Chief, Division of Cardiovascular Medicine University of Southern California Los Angeles, California Disclosures Abiomed Research
Percutaneous Intervention of Unprotected Left Main Disease
 Percutaneous Intervention of Unprotected Left Main Disease Technical feasibility and Clinical outcomes Seung-Jung Park, MD, PhD, FACC Professor of Internal Medicine Asan Medical Center, Seoul, Korea Unprotected
Percutaneous Intervention of Unprotected Left Main Disease Technical feasibility and Clinical outcomes Seung-Jung Park, MD, PhD, FACC Professor of Internal Medicine Asan Medical Center, Seoul, Korea Unprotected
The MAIN-COMPARE Study
 Long-Term Outcomes of Coronary Stent Implantation versus Bypass Surgery for the Treatment of Unprotected Left Main Coronary Artery Disease Revascularization for Unprotected Left MAIN Coronary Artery Stenosis:
Long-Term Outcomes of Coronary Stent Implantation versus Bypass Surgery for the Treatment of Unprotected Left Main Coronary Artery Disease Revascularization for Unprotected Left MAIN Coronary Artery Stenosis:
Ziyad Ghazzal MD, FACC, FSCAI Professor of Medicine Deputy Vice President/Dean Associate Dean for Clinical Affairs American University of Beirut
 Ziyad Ghazzal MD, FACC, FSCAI Professor of Medicine Deputy Vice President/Dean Associate Dean for Clinical Affairs American University of Beirut Adjunct Professor Emory University School of Medicine Indication
Ziyad Ghazzal MD, FACC, FSCAI Professor of Medicine Deputy Vice President/Dean Associate Dean for Clinical Affairs American University of Beirut Adjunct Professor Emory University School of Medicine Indication
The Influence of Previous Percutaneous Coronary Intervention in Patients Undergoing Off-Pump Coronary Artery Bypass Grafting
 Original Article The Influence of Previous Percutaneous Coronary Intervention in Patients Undergoing Off-Pump Coronary Artery Bypass Grafting Toshihiro Fukui, MD, Susumu Manabe, MD, Tomoki Shimokawa, MD,
Original Article The Influence of Previous Percutaneous Coronary Intervention in Patients Undergoing Off-Pump Coronary Artery Bypass Grafting Toshihiro Fukui, MD, Susumu Manabe, MD, Tomoki Shimokawa, MD,
DECLARATION OF CONFLICT OF INTEREST
 DECLARATION OF CONFLICT OF INTEREST Multivessel disease and cardiogenic shock: CABG is the optimal revascularization therapy. Contra Prof. Christian JM Vrints Cardiogenic Shock Spiral Acute Myocardial
DECLARATION OF CONFLICT OF INTEREST Multivessel disease and cardiogenic shock: CABG is the optimal revascularization therapy. Contra Prof. Christian JM Vrints Cardiogenic Shock Spiral Acute Myocardial
DECISION - CTO. optimal Medical Treatment in patients with. Seung-Jung Park, MD, PhD, FACC for the DECISION-CTO Study investigators
 DECISION - CTO Drug-Eluting stent Implantation versus optimal Medical Treatment in patients with ChronIc Total OccluSION Seung-Jung Park, MD, PhD, FACC for the DECISION-CTO Study investigators Asan Medical
DECISION - CTO Drug-Eluting stent Implantation versus optimal Medical Treatment in patients with ChronIc Total OccluSION Seung-Jung Park, MD, PhD, FACC for the DECISION-CTO Study investigators Asan Medical
Paris, August 28 th Gian Paolo Ussia on behalf of the CoreValve Italian Registry Investigators
 Paris, August 28 th 2011 Is TAVI the definitive treatment in high risk patients? Impact Of Coronary Artery Disease In Elderly Patients Undergoing TAVI: Insight The Italian CoreValve Registry Gian Paolo
Paris, August 28 th 2011 Is TAVI the definitive treatment in high risk patients? Impact Of Coronary Artery Disease In Elderly Patients Undergoing TAVI: Insight The Italian CoreValve Registry Gian Paolo
The Second Best Arterial Graft:
 The Second Best Arterial Graft: A Propensity Analysis of the Radial Artery Versus the Right Internal Thoracic Artery to Bypass the Circumflex Coronary Artery American Association for Thoracic Surgery,
The Second Best Arterial Graft: A Propensity Analysis of the Radial Artery Versus the Right Internal Thoracic Artery to Bypass the Circumflex Coronary Artery American Association for Thoracic Surgery,
Management of Cardiogenic shock. Prof. Christian JM Vrints
 Management of Cardiogenic shock Prof. Christian JM Vrints none conflicts Management of Cardiogenic Shock Incidence and trends Importance of early revascularization Multivessel disease Left main disease
Management of Cardiogenic shock Prof. Christian JM Vrints none conflicts Management of Cardiogenic Shock Incidence and trends Importance of early revascularization Multivessel disease Left main disease
When should we indisputably perform CABG? Quand faut-il indiscutablement opérer? Dr Hakim BENAMER
 When should we indisputably perform CABG? Quand faut-il indiscutablement opérer? Dr Hakim BENAMER ICPS, Massy ICV-GVM La Roseraie, Aubervilliers Hôpital FOCH, Suresnes Disclosure Statement of Financial
When should we indisputably perform CABG? Quand faut-il indiscutablement opérer? Dr Hakim BENAMER ICPS, Massy ICV-GVM La Roseraie, Aubervilliers Hôpital FOCH, Suresnes Disclosure Statement of Financial
Division of Cardiovascular Medicine, Jichi Medical University Saitama Medical Center, Japan
 Association between continuously elevated C-reactive protein and restenosis after percutaneous coronary intervention using drug-eluting stent in angina patients Division of Cardiovascular Medicine, Jichi
Association between continuously elevated C-reactive protein and restenosis after percutaneous coronary intervention using drug-eluting stent in angina patients Division of Cardiovascular Medicine, Jichi
Adults With Diagnosed Diabetes
 Adults With Diagnosed Diabetes 1990 No data available Less than 4% 4%-6% Above 6% Mokdad AH, et al. Diabetes Care. 2000;23(9):1278-1283. Adults With Diagnosed Diabetes 2000 4%-6% Above 6% Mokdad AH, et
Adults With Diagnosed Diabetes 1990 No data available Less than 4% 4%-6% Above 6% Mokdad AH, et al. Diabetes Care. 2000;23(9):1278-1283. Adults With Diagnosed Diabetes 2000 4%-6% Above 6% Mokdad AH, et
Rationale for Prophylactic Support During Percutaneous Coronary Intervention
 Rationale for Prophylactic Support During Percutaneous Coronary Intervention Navin K. Kapur, MD, FACC, FSCAI Assistant Director, Interventional Cardiology Director, Interventional Research Laboratories
Rationale for Prophylactic Support During Percutaneous Coronary Intervention Navin K. Kapur, MD, FACC, FSCAI Assistant Director, Interventional Cardiology Director, Interventional Research Laboratories
MICS CABG. Putting the future of MICS in your hands today
 MICS CABG Putting the future of MICS in your hands today This presentation is based on a compilation of the surgical techniques and protocols of: Dr. Joseph McGinn - Staten Island, New York Dr. Marc Ruel
MICS CABG Putting the future of MICS in your hands today This presentation is based on a compilation of the surgical techniques and protocols of: Dr. Joseph McGinn - Staten Island, New York Dr. Marc Ruel
Controversies in Cardiac Surgery
 Controversies in Cardiac Surgery 3 years after SYNTAX : Percutaneous Coronary Intervention for Multivessel / Left main stem Coronary artery disease Pro ESC Congress 2010, 28 August 1 September Stockholm
Controversies in Cardiac Surgery 3 years after SYNTAX : Percutaneous Coronary Intervention for Multivessel / Left main stem Coronary artery disease Pro ESC Congress 2010, 28 August 1 September Stockholm
Can Angiographic Complete Revascularization Improve Outcomes for Patients with Decreased LV Function? NO!
 Can Angiographic Complete Revascularization Improve Outcomes for Patients with Decreased LV Function? NO! Young-Hak Kim, MD, PhD Heart Institute, University of Ulsan College of Medicine Asan Medical Center,
Can Angiographic Complete Revascularization Improve Outcomes for Patients with Decreased LV Function? NO! Young-Hak Kim, MD, PhD Heart Institute, University of Ulsan College of Medicine Asan Medical Center,
Assessing Cardiac Risk in Noncardiac Surgery. Murali Sivarajan, M.D. Professor University of Washington Seattle, Washington
 Assessing Cardiac Risk in Noncardiac Surgery Murali Sivarajan, M.D. Professor University of Washington Seattle, Washington Disclosure None. I have no conflicts of interest, financial or otherwise. CME
Assessing Cardiac Risk in Noncardiac Surgery Murali Sivarajan, M.D. Professor University of Washington Seattle, Washington Disclosure None. I have no conflicts of interest, financial or otherwise. CME
8/28/2018. Pre-op Evaluation for non cardiac surgery. A quick review from 2007!! Disclosures. John Steuter, MD. None
 Pre-op Evaluation for non cardiac surgery John Steuter, MD Disclosures None A quick review from 2007!! Fliesheret al, ACC/AHA 2007 Guidelines on Perioperative Cardiovascular Evaluation and are for Noncardiac
Pre-op Evaluation for non cardiac surgery John Steuter, MD Disclosures None A quick review from 2007!! Fliesheret al, ACC/AHA 2007 Guidelines on Perioperative Cardiovascular Evaluation and are for Noncardiac
SUPPLEMENTAL MATERIAL
 SUPPLEMENTAL MATERIAL Table S1: Number and percentage of patients by age category Distribution of age Age
SUPPLEMENTAL MATERIAL Table S1: Number and percentage of patients by age category Distribution of age Age
Intraaortic Balloon Counterpulsation- Supportive Data for a Role in Cardiogenic Shock ( Be Still My Friend )
") Intraaortic Balloon Counterpulsation- Supportive Data for a Role in Cardiogenic Shock ( Be Still My Friend ) Stephen G. Ellis, MD Section Head, Interventional Cardiology Professor of Medicine Cleveland
Intraaortic Balloon Counterpulsation- Supportive Data for a Role in Cardiogenic Shock ( Be Still My Friend ) Stephen G. Ellis, MD Section Head, Interventional Cardiology Professor of Medicine Cleveland
Southern Thoracic Surgical Association CABG in 2012: Implications of the New ESC/EACTS Guidelines
 Southern Thoracic Surgical Association 2011 CABG in 2012: Implications of the New ESC/EACTS Guidelines David P Taggart MD PhD FRCS Professor of Cardiovascular Surgery, University of Oxford Conflicts of
Southern Thoracic Surgical Association 2011 CABG in 2012: Implications of the New ESC/EACTS Guidelines David P Taggart MD PhD FRCS Professor of Cardiovascular Surgery, University of Oxford Conflicts of
Emergency surgery in acute coronary syndrome
 Emergency surgery in acute coronary syndrome Teerawoot Jantarawan Division of Cardiothoracic Surgery, Department of Surgery, Faculty of Medicine Siriraj Hospital, Mahidol University, Bangkok, Thailand
Emergency surgery in acute coronary syndrome Teerawoot Jantarawan Division of Cardiothoracic Surgery, Department of Surgery, Faculty of Medicine Siriraj Hospital, Mahidol University, Bangkok, Thailand
Rationale for Left Ventricular Support During Percutaneous Coronary Intervention
 Rationale for Left Ventricular Support During Percutaneous Coronary Intervention Navin K. Kapur, MD, FACC, FSCAI Associate Professor, Division of Cardiology Director, Acute Circulatory Support Program
Rationale for Left Ventricular Support During Percutaneous Coronary Intervention Navin K. Kapur, MD, FACC, FSCAI Associate Professor, Division of Cardiology Director, Acute Circulatory Support Program
8. Nov, 2018 Athens Clossroad 2018, Athens GREEK
 8. Nov, 2018 Athens Clossroad 2018, Athens GREEK Stent Less Bio prosthesis Aortic Valve replacement with Minimally Invasive Approach ~ Indication for the 1 st Surgical Aortic Valve Treatment Considering
8. Nov, 2018 Athens Clossroad 2018, Athens GREEK Stent Less Bio prosthesis Aortic Valve replacement with Minimally Invasive Approach ~ Indication for the 1 st Surgical Aortic Valve Treatment Considering
Master Class in Preventive Cardiology Focus on Diabetes and Cardiovascular Disease Geneva April
 Master Class in Preventive Cardiology Focus on Diabetes and Cardiovascular Disease Geneva April 14 2011 Coronary interventions in patients with diabetes Lars Rydén Karolinska Institutet Stockholm, Sweden
Master Class in Preventive Cardiology Focus on Diabetes and Cardiovascular Disease Geneva April 14 2011 Coronary interventions in patients with diabetes Lars Rydén Karolinska Institutet Stockholm, Sweden
Coronary Artery Bypass Graft: Monitoring Patients and Detecting Complications
 Coronary Artery Bypass Graft: Monitoring Patients and Detecting Complications Madhav Swaminathan, MD, FASE Professor of Anesthesiology Division of Cardiothoracic Anesthesia & Critical Care Duke University
Coronary Artery Bypass Graft: Monitoring Patients and Detecting Complications Madhav Swaminathan, MD, FASE Professor of Anesthesiology Division of Cardiothoracic Anesthesia & Critical Care Duke University
Setting The setting was a hospital. The economic study was carried out in Australia.
 Coronary artery bypass grafting (CABG) after initially successful percutaneous transluminal coronary angioplasty (PTCA): a review of 17 years experience Barakate M S, Hemli J M, Hughes C F, Bannon P G,
Coronary artery bypass grafting (CABG) after initially successful percutaneous transluminal coronary angioplasty (PTCA): a review of 17 years experience Barakate M S, Hemli J M, Hughes C F, Bannon P G,
Coronary Artery Bypass Grafting For Acute Myocardial Infarction in Stent ERA
 Original Article Coronary Artery Bypass Grafting For Acute Myocardial Infarction in Stent ERA Tamaki Takano, MD, Hirohisa Goto, MD, Kazuo Hoshino, MD, Hirohide Shimada, MD, Hiroyuki Ichinose, MD, and Norihiko
Original Article Coronary Artery Bypass Grafting For Acute Myocardial Infarction in Stent ERA Tamaki Takano, MD, Hirohisa Goto, MD, Kazuo Hoshino, MD, Hirohide Shimada, MD, Hiroyuki Ichinose, MD, and Norihiko
Comparison of 30-day outcomes of coronary artery bypass grafting surgery verus hybrid coronary revascularization stratified by SYNTAX and euroscore
 Comparison of 30-day outcomes of coronary artery bypass grafting surgery verus hybrid coronary revascularization stratified by SYNTAX and euroscore Marzia Leacche, MD, John G. Byrne, MD, Natalia S. Solenkova,
Comparison of 30-day outcomes of coronary artery bypass grafting surgery verus hybrid coronary revascularization stratified by SYNTAX and euroscore Marzia Leacche, MD, John G. Byrne, MD, Natalia S. Solenkova,
Left Main and Bifurcation Summit I. Lessons from European LM Studies
 Left Main and Bifurcation Summit I Apr 29 8.56-9.09 Lessons from European LM Studies Alaide Chieffo, MD S. Raffaele Hospital, Milan, Italy Nothing to disclose regarding this presentation Lesion Location
Left Main and Bifurcation Summit I Apr 29 8.56-9.09 Lessons from European LM Studies Alaide Chieffo, MD S. Raffaele Hospital, Milan, Italy Nothing to disclose regarding this presentation Lesion Location
Revascularization In HFrEF: Are We Close To The Truth. Ali Almasood
 Revascularization In HFrEF: Are We Close To The Truth Ali Almasood HF epidemic 1-2% of the population have HF At least one-half have heart failure with reduced ejection fraction (HF- REF) The most common
Revascularization In HFrEF: Are We Close To The Truth Ali Almasood HF epidemic 1-2% of the population have HF At least one-half have heart failure with reduced ejection fraction (HF- REF) The most common
About OMICS International Conferences
 About OMICS Group OMICS Group is an amalgamation of Open Access publications and worldwide international science conferences and events. Established in the year 2007 with the sole aim of making the information
About OMICS Group OMICS Group is an amalgamation of Open Access publications and worldwide international science conferences and events. Established in the year 2007 with the sole aim of making the information
2016 Physician Quality Reporting System Data Collection Form: Coronary Artery Bypass Graft (CABG) (for patients aged 18 years and older)
 (for patients aged 18 years and older)") 2016 Physician Quality Reporting System Data Collection Form: Coronary Artery Bypass Graft (CABG) (for patients aged 18 years and older) IMPORTANT: Any measure with a 0% performance rate (100% for inverse
2016 Physician Quality Reporting System Data Collection Form: Coronary Artery Bypass Graft (CABG) (for patients aged 18 years and older) IMPORTANT: Any measure with a 0% performance rate (100% for inverse
Clinical Seminar. Which Diabetic Patient is a Candidate for Percutaneous Coronary Intervention - European Perspective
 Clinical Seminar Which Diabetic Patient is a Candidate for Percutaneous Coronary Intervention - European Perspective Stephan Windecker Department of Cardiology Swiss Cardiovascular Center and Clinical
Clinical Seminar Which Diabetic Patient is a Candidate for Percutaneous Coronary Intervention - European Perspective Stephan Windecker Department of Cardiology Swiss Cardiovascular Center and Clinical
Better CABGs vs Better PCI Devices
 CABG vs PCI 2017 Multivessel Coronary Disease Better CABGs vs Better PCI Devices ACC New York, Dec 8, 2017 No Disclosures CABG vs PCI 2017 Stable Multivessel Coronary Disease 1. Are These The two Critical
CABG vs PCI 2017 Multivessel Coronary Disease Better CABGs vs Better PCI Devices ACC New York, Dec 8, 2017 No Disclosures CABG vs PCI 2017 Stable Multivessel Coronary Disease 1. Are These The two Critical
Left Main PCI vs. CABG: Real World
 Management of Patients with Stable CAD Left Main PCI vs. CABG: Real World Marco Roffi, MD, FESC University Hospital Geneva, Switzerland SYNTAX-LMT The SYNTAX trial included a pre-specified subgroup of
Management of Patients with Stable CAD Left Main PCI vs. CABG: Real World Marco Roffi, MD, FESC University Hospital Geneva, Switzerland SYNTAX-LMT The SYNTAX trial included a pre-specified subgroup of
Patient. Clinical data Indications: Operation date. Comorbidities: Patient code Birth date: / /
 Patient Patient code Birth date: / / Sex: Male Height (cm): Female Weight (kg): Risk Factors: Family history of coronary disease: Hypertension Dyslipidemia Peripheral disease Diabetes Comorbidities: No
Patient Patient code Birth date: / / Sex: Male Height (cm): Female Weight (kg): Risk Factors: Family history of coronary disease: Hypertension Dyslipidemia Peripheral disease Diabetes Comorbidities: No
Unprotected Left Main Stenting: Patient Selection and Recent Experience. Alaide Chieffo. S. Raffaele Hospital, Milan, Italy
 Unprotected Left Main Stenting: Patient Selection and Recent Experience Alaide Chieffo S. Raffaele Hospital, Milan, Italy Class IIa (Level B) AHA/ACC 2005 Guidelines Left Main CAD The use of PCI for pts
Unprotected Left Main Stenting: Patient Selection and Recent Experience Alaide Chieffo S. Raffaele Hospital, Milan, Italy Class IIa (Level B) AHA/ACC 2005 Guidelines Left Main CAD The use of PCI for pts
PCI vs. CABG From BARI to Syntax, Is The Game Over?
 PCI vs. CABG From BARI to Syntax, Is The Game Over? Seung-Jung Park, MD, PhD Professor of Medicine, University of Ulsan College of Medicine Asan Medical Center, Seoul, Korea PCI vs CABG Multi-Vessel Disease
PCI vs. CABG From BARI to Syntax, Is The Game Over? Seung-Jung Park, MD, PhD Professor of Medicine, University of Ulsan College of Medicine Asan Medical Center, Seoul, Korea PCI vs CABG Multi-Vessel Disease
PCI for Chronic Total Occlusions
 PCI for Chronic Total Occlusions Chronic Total Occlusions Why not Medical Treatment? Medical Treatment CTO in 891 pts over 24 years High 10% Mortality Low 2 % 1 year 10 years Puma JA, et al. JACC 1994;23:390A
PCI for Chronic Total Occlusions Chronic Total Occlusions Why not Medical Treatment? Medical Treatment CTO in 891 pts over 24 years High 10% Mortality Low 2 % 1 year 10 years Puma JA, et al. JACC 1994;23:390A
Prevention and Management of Cardiac Adverse Event
 Prevention and Management of Cardiac Adverse Event Carlo Cernetti Department of Interventional Cardiology Mirano (Italy) Cannes MEEC 14 June 2007 Are these risks factors of Haemodynamic Instability
Prevention and Management of Cardiac Adverse Event Carlo Cernetti Department of Interventional Cardiology Mirano (Italy) Cannes MEEC 14 June 2007 Are these risks factors of Haemodynamic Instability
Michael Mack, M.D. Baylor Healthcare System Heart Hospital Baylor Plano Dallas, TX
 Michael Mack, M.D. Baylor Healthcare System Heart Hospital Baylor Plano Dallas, TX Maquet, Inc.,- unpaid consultant Cordis, Inc.,- unpaid consultant Boston Scientific, Inc.,- travel expenses paid for Syntax
Michael Mack, M.D. Baylor Healthcare System Heart Hospital Baylor Plano Dallas, TX Maquet, Inc.,- unpaid consultant Cordis, Inc.,- unpaid consultant Boston Scientific, Inc.,- travel expenses paid for Syntax
Ray Matthews MD Professor of Clinical Medicine Chief of Cardiology University of Southern California
 High Risk PCI Making Possible the Impossible Ray Matthews MD Professor of Clinical Medicine Chief of Cardiology University of Southern California Disclosures Abiomed Research Support Consulting Agreement
High Risk PCI Making Possible the Impossible Ray Matthews MD Professor of Clinical Medicine Chief of Cardiology University of Southern California Disclosures Abiomed Research Support Consulting Agreement
In-Ho Chae. Seoul National University College of Medicine
 The Earlier, The Better: Quantum Progress in ACS In-Ho Chae Seoul National University College of Medicine Quantum Leap in Statin Landmark Trials in ACS patients Randomized Controlled Studies of Lipid-Lowering
The Earlier, The Better: Quantum Progress in ACS In-Ho Chae Seoul National University College of Medicine Quantum Leap in Statin Landmark Trials in ACS patients Randomized Controlled Studies of Lipid-Lowering
Cardiogenic Shock. Carlos Cafri,, MD
 Cardiogenic Shock Carlos Cafri,, MD SHOCK= Inadequate Tissue Mechanisms: Perfusion Inadequate oxygen delivery Release of inflammatory mediators Further microvascular changes, compromised blood flow and
Cardiogenic Shock Carlos Cafri,, MD SHOCK= Inadequate Tissue Mechanisms: Perfusion Inadequate oxygen delivery Release of inflammatory mediators Further microvascular changes, compromised blood flow and
Perioperative Cardiology Consultations for Noncardiac Surgery Ischemic Heart Disease
 2012 대한춘계심장학회 Perioperative Cardiology Consultations for Noncardiac Surgery Ischemic Heart Disease 울산의대울산대학병원심장내과이상곤 ECG CLASS IIb 1. Preoperative resting 12-lead ECG may be reasonable in patients with
2012 대한춘계심장학회 Perioperative Cardiology Consultations for Noncardiac Surgery Ischemic Heart Disease 울산의대울산대학병원심장내과이상곤 ECG CLASS IIb 1. Preoperative resting 12-lead ECG may be reasonable in patients with
CPORT E Trial. Atlantic C PORT
 CPORT E Trial Randomized trial comparing medical, economic and quality of life outcomes of non primary PCI at hospitals with and without on site cardiac surgery Mo#va#on for Trial Sustain primary PCI program
CPORT E Trial Randomized trial comparing medical, economic and quality of life outcomes of non primary PCI at hospitals with and without on site cardiac surgery Mo#va#on for Trial Sustain primary PCI program
TAVR y Enfermedad Coronaria. Mauricio G. Cohen, MD, FACC, FSCAI Director, Cardiac Catheterization Lab Associate Professor of Medicine
 TAVR y Enfermedad Coronaria Mauricio G. Cohen, MD, FACC, FSCAI Director, Cardiac Catheterization Lab Associate Professor of Medicine CAD and AS Similar Pathological Processes CAD in TAVR Patients (n=390)
TAVR y Enfermedad Coronaria Mauricio G. Cohen, MD, FACC, FSCAI Director, Cardiac Catheterization Lab Associate Professor of Medicine CAD and AS Similar Pathological Processes CAD in TAVR Patients (n=390)
Valve Disease in Patients With Heart Failure TAVI or Surgery? Miguel Sousa Uva Hospital Cruz Vermelha Lisbon, Portugal
 Valve Disease in Patients With Heart Failure TAVI or Surgery? Miguel Sousa Uva Hospital Cruz Vermelha Lisbon, Portugal I have nothing to disclose. Wide Spectrum Stable vs Decompensated NYHA II IV? Ejection
Valve Disease in Patients With Heart Failure TAVI or Surgery? Miguel Sousa Uva Hospital Cruz Vermelha Lisbon, Portugal I have nothing to disclose. Wide Spectrum Stable vs Decompensated NYHA II IV? Ejection
TREATMENT OF HIGHER RISK PATIENTS INTRODUCTION TO PROTECTED PCI WITH IMPELLA. IMP v4
 1 TREATMENT OF HIGHER RISK PATIENTS INTRODUCTION TO PROTECTED PCI WITH IMPELLA FDA APPROVES IMPELLA FOR HIGH-RISK PCI 2 Impella is the only hemodynamic support device proven safe and effective in elective
1 TREATMENT OF HIGHER RISK PATIENTS INTRODUCTION TO PROTECTED PCI WITH IMPELLA FDA APPROVES IMPELLA FOR HIGH-RISK PCI 2 Impella is the only hemodynamic support device proven safe and effective in elective
What do the guidelines say?
 Percutaneous coronary intervention in 3-vessel disease and main stem What do the guidelines say? Nothing to disclose Dariusz Dudek Institute of Cardiology, Jagiellonian University Krakow, Poland The European
Percutaneous coronary intervention in 3-vessel disease and main stem What do the guidelines say? Nothing to disclose Dariusz Dudek Institute of Cardiology, Jagiellonian University Krakow, Poland The European
Percutaneous Cardiopulmonary Support after Acute Myocardial Infarction at the Left Main Trunk
 Original Article Percutaneous Cardiopulmonary Support after Acute Myocardial Infarction at the Left Main Trunk Takashi Yamauchi, MD, PhD, 1 Takafumi Masai, MD, PhD, 1 Koji Takeda, MD, 1 Satoshi Kainuma,
Original Article Percutaneous Cardiopulmonary Support after Acute Myocardial Infarction at the Left Main Trunk Takashi Yamauchi, MD, PhD, 1 Takafumi Masai, MD, PhD, 1 Koji Takeda, MD, 1 Satoshi Kainuma,
Lack of Effect of Beta-blocker Therapy in Patients with ST-elevation Acute Myocardial Infarction in PCI Era
 Lack of Effect of Beta-blocker Therapy in Patients with ST-elevation Acute Myocardial Infarction in PCI Era B. Bao 1, N. Ozasa 1, T. Morimoto 2, Y. Furukawa 3, M. Shirotani 4, H. Ogawa 5, C. Tei 6, H.
Lack of Effect of Beta-blocker Therapy in Patients with ST-elevation Acute Myocardial Infarction in PCI Era B. Bao 1, N. Ozasa 1, T. Morimoto 2, Y. Furukawa 3, M. Shirotani 4, H. Ogawa 5, C. Tei 6, H.
Management of High-Risk Coronary Artery Disease
 Management of High-Risk Coronary Artery Disease Jeffrey J. Popma, MD Director, Interventional Cardiology Clinical Services Beth Israel Deaconess Medical Center Associate Professor of Medicine Harvard Medical
Management of High-Risk Coronary Artery Disease Jeffrey J. Popma, MD Director, Interventional Cardiology Clinical Services Beth Israel Deaconess Medical Center Associate Professor of Medicine Harvard Medical
CHRONIC HEART FAILURE : WHAT ELSE COULD WE OFFER TO OUR PATIENTS? Cardiac Rehabilitation Society of Thailand
 CHRONIC HEART FAILURE : WHAT ELSE COULD WE OFFER TO OUR PATIENTS? Cardiac Rehabilitation Society of Thailand ENHANCED EXTERNAL COUNTER PULSATION Piyanuj Ruckpanich, MD. Cardiac Rehabilitation Center Perfect
CHRONIC HEART FAILURE : WHAT ELSE COULD WE OFFER TO OUR PATIENTS? Cardiac Rehabilitation Society of Thailand ENHANCED EXTERNAL COUNTER PULSATION Piyanuj Ruckpanich, MD. Cardiac Rehabilitation Center Perfect
Masashi Kimura, MD Etsuo Tsuchikane, MD Osamu Katoh, MD Toyohashi Heart Center, Japan
 Masashi Kimura, MD Etsuo Tsuchikane, MD Osamu Katoh, MD, Japan Retrograde Approach for Coronary CTO Collateral channels A. bypass graft B. epicardial collateral C. septal perforator Retrograde wiring techniques
Masashi Kimura, MD Etsuo Tsuchikane, MD Osamu Katoh, MD, Japan Retrograde Approach for Coronary CTO Collateral channels A. bypass graft B. epicardial collateral C. septal perforator Retrograde wiring techniques
Current outcomes of off-pump coronary artery bypass grafting: evidence from real world practice
 Review Article Current outcomes of off-pump coronary artery bypass grafting: evidence from real world practice Piroze M. Davierwala Department of Cardiac Surgery, Heart Center, University of Leipzig, Leipzig,
Review Article Current outcomes of off-pump coronary artery bypass grafting: evidence from real world practice Piroze M. Davierwala Department of Cardiac Surgery, Heart Center, University of Leipzig, Leipzig,
CardioLucca2014. Fare luce sulla scelta ottimale del trattamento nella rivascolarizzazione delle stenosi carotidee. Fabrizio Tomai
 CardioLucca2014 Fare luce sulla scelta ottimale del trattamento nella rivascolarizzazione delle stenosi carotidee Fabrizio Tomai European Hospital e Aurelia Hospital Roma Treatment of Carotid Artery Disease
CardioLucca2014 Fare luce sulla scelta ottimale del trattamento nella rivascolarizzazione delle stenosi carotidee Fabrizio Tomai European Hospital e Aurelia Hospital Roma Treatment of Carotid Artery Disease
CONTEMPORARY USE OF ARTERIAL GRAFTS DURING CORONARY ARTERY BYPASS SURGERY: PARADIGM SHIFT? OR A LITTLE (MORE) TALK THAT NEEDS A LOT MORE ACTION
 TALK THAT NEEDS A LOT MORE ACTION") CONTEMPORARY USE OF ARTERIAL GRAFTS DURING CORONARY ARTERY BYPASS SURGERY: PARADIGM SHIFT? OR A LITTLE (MORE) TALK THAT NEEDS A LOT MORE ACTION JAMES L ZELLNER MD I have no financial disclosures. 1897
CONTEMPORARY USE OF ARTERIAL GRAFTS DURING CORONARY ARTERY BYPASS SURGERY: PARADIGM SHIFT? OR A LITTLE (MORE) TALK THAT NEEDS A LOT MORE ACTION JAMES L ZELLNER MD I have no financial disclosures. 1897
2018 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY. MEASURE TYPE: Process
 Quality ID #44 (NQF 0236): Coronary Artery Bypass Graft (CABG): Preoperative Beta-Blocker in Patients with Isolated CABG Surgery National Quality Strategy Domain: Effective Clinical Care 2018 OPTIONS FOR
Quality ID #44 (NQF 0236): Coronary Artery Bypass Graft (CABG): Preoperative Beta-Blocker in Patients with Isolated CABG Surgery National Quality Strategy Domain: Effective Clinical Care 2018 OPTIONS FOR
Contrast Induced Nephropathy
 Contrast Induced Nephropathy O CIAKI refers to an abrupt deterioration in renal function associated with the administration of iodinated contrast media O CIAKI is characterized by an acute (within 48 hours)
Contrast Induced Nephropathy O CIAKI refers to an abrupt deterioration in renal function associated with the administration of iodinated contrast media O CIAKI is characterized by an acute (within 48 hours)