Pattern and Timing of the Coronary Sinus Activation to Guide Rapid Diagnosis of Atrial Tachycardia after Atrial Fibrillation Ablation
|
|
|
- Randolph Lester
- 5 years ago
- Views:
Transcription
1 Pattern and Timing of the Coronary Sinus Activation to Guide Rapid Diagnosis of Atrial Tachycardia after Atrial Fibrillation Ablation Running title: Pascale et al.; Coronary sinus activation in atrial tachycardia Patrizio Pascale, MD; Ashok J. Shah, MD; Laurent Roten, MD; Daniel Scherr, MD; Yuki Komatsu, MD; Amir S. Jadidi, MD; Khaled Ramoul, MD; Matthew thew Daly, MD; Arnaud Denis, MD; Stephen B. Wilton, MD; Nicolas Derval, MD; Frédéric éric Sacher, MD; Mélèze Hocini, MD; Michel Haïssaguerre, e, MD; Pierre Jaïs, MD. Hôpital Cardiologique du Haut-Lévêque & Université Victor Segalen, Bordeaux II, LIRYC Institute, Bordeaux, France Correspondance: Patrizio Pascale, MD Hôpital Cardiologique du Haut-Lévêque Avenue de Magellan Bordeaux-Pessac, France Tel: Fax: Journal Subject Codes: 106 Electrophysiology; 22 Ablation/ICD/surgery Presented in part at the 33 rd Annual Scientific Sessions of the Heart Rhythm Society in Boston, MA, May
2 Abstract: Background - Atrial tachycardias (AT) during or after ablation of AF frequently pose a diagnostic challenge. We hypothesized that both the patterns and timing of coronary sinus (CS) activation could facilitate AT mapping. Methods and Results consecutive post-persistent AF ablation patients with sustained AT were investigated by conventional mapping. CS activation pattern was defined as chevron or reverse chevron when the activations recorded on both the proximal and distal CS dipoles were latest or earliest, respectively. The local activation of mid-cs was timed with reference to P peak - P peak (P-P) interval in lead V1. A ratio, mid-cs activation time to AT cycle length, was computed. Out of 223 diagnosed ATs, 124 were macroreentrant (56%) and 99 were centrifugal (44%). When CS activation was chevron / reverse chevron (n = 44, 4, 20%), macroreentries ri were mostly roof-dependent. of ende dent. With reference to P-P interval, mid-cs activation timing showed specific consistency for peritricuspid pid and perimitral AT. Proximal to distal CS activation atio ion pattern and mid-cs activation at 50-70% of the P-P interval (n = 30, 13%) diagnosed peritricuspid ricusp AT with 81% sensitivity and 89% specificity. Distal to proximal CS activation ation and mid-cs activation at 10-40% 0% of the P-P P interval (n = 44, 20%) diagnosed perimitral AT with 88% 8 sensitivity and 75% specificity. ic ity. Conclusions - The analysis of the patterns and timing of CS activation provides a rapid stratification of most likely macroreentrant ATs and points towards the likely origin of centrifugal ATs. It can be included in a stepwise diagnostic approach to rapidly select the most critical mapping maneuvers. Key words: coronary sinus; atrial tachycardia; mapping; atrial flutter; ablation; electrophysiology mapping; atrial fibrillation 2
3 Introduction Catheter ablation of persistent atrial fibrillation (AF) often requires adjunctive substrate modification strategies beyond pulmonary vein (PV) isolation to achieve a higher success rate 1, 2. The expansion of ablation approaches that include a greater amount of left atrial (LA) ablation is associated with a high incidence of atrial tachycardias (ATs) 3-6. Mapping of these postablation ATs is often challenging and time-consuming since multiple foci may coexist and extensive atrial substrate has been targeted. It is therefore critical for the operator to have a preconceived suspicion of possible mechanism and AT location to avoid more exhaustive, and sometimes m confusing, mapping and optimally rationalize the entrainment maneuvers. In this regard, and as a standard component nt of the electrophysiologic evaluation, ation, the analysis of the multipolar coronary sinus (CS) recordings rdings provides a unique opportunity to rapidly guide the operator r towards the most likely diagnosis by disclosing i the pattern of activation ion of the inferior i r LA. We therefore r aimed to better characterize rize the patterns of activation that t may be encountered ed during AT to get as much information as possible sibl from the CS recordings. rdin We also hypothesized ed that the timing of CS activation during the AT cycle may help in the differential AT diagnosis. The purpose of the study is to derive from the analysis of the CS recording a pragmatic strategy to select the most critical and limited number of activation and entrainment mapping maneuvers. Methods Study population. All consecutive patients who underwent mapping and ablation of sustained AT arising during or after ablation of symptomatic drug-refractory persistent AF at our institute from January 2009 to May 2011 were enrolled in the study. 3
4 Electrophysiological study. All patients provided written informed consent. All antiarrhythmic drugs except amiodarone were stopped 5 half-lives before ablation. Surface electrocardiograms and bipolar intracardiac electrograms (EGM) were monitored continuously and stored on a computer-based digital amplifier/recorder system (Labsystem Pro, Bard Electrophysiology, Lowell, MA, USA). Signals were sampled at 1 khz and filtered at Hz for surface electrocardiograms and Hz for intracardiac signals, displayed at an amplitude of 0.1 mv/cm. The following catheters were introduced through the right femoral vein: 1) a steerable erab decapolar catheter was positioned within the CS; 2) a 10-pole circumferential ia catheter ter (Lasso, Biosense Webster, er, Diamond Bar, CA, USA) was used for PV mapping 3) a 3.5-mm externally irrigated-tip ablation catheter (Biosense-Webster, Diamond Bar, CA, USA). The Lasso or the ablation catheter were stabilized with a long sheath (SLO, St. Jude Medical, St Paul, MN, USA) perfused continuously with heparinized iz ed DW solution. A single bolus of 50 IU/kg heparin was administered ed immediately after transseptal tal puncture. The activated ated clotting time was maintained thereafter within a range of 250 to 300 seconds. Ablation sequence for persistent AF. The index procedure for persistent AF was performed by using a stepwise ablation approach with a procedural end point of AF termination. If AF converted into AT, ablation was performed until the restoration of sinus rhythm. Details of this particular ablation approach have been published previously 1. In brief, as the first step, circumferential PV isolation was performed. The second step, EGM-guided LA ablation, targeted sites displaying complex fractionated EGMs and locally short AF cycle length (CL). When ablation of the inferior LA did not result in organization of the CS, additional ablation within the CS was performed. Linear LA ablation, the third step, targeted the LA roof followed 4
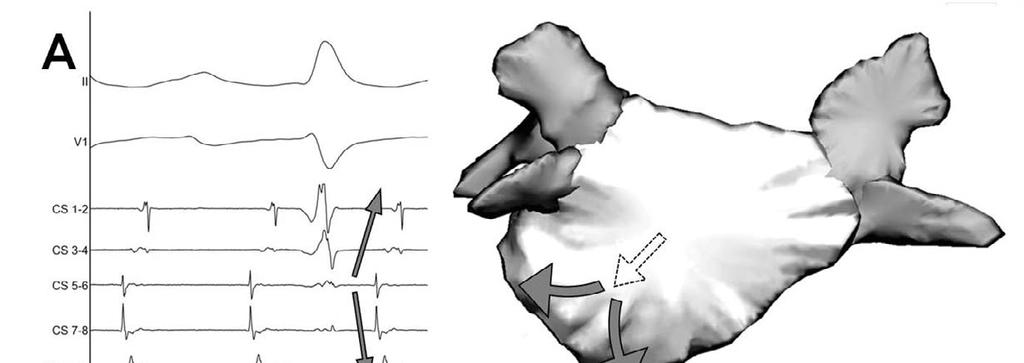
5 by the mitral isthmus (MI). In the presence of shorter AF CL in the right atrium, EGM-guided ablation was performed in that chamber. Cavotricuspid isthmus (CTI) ablation was performed in most patients. Characterization of the patterns and timing of CS activation. The CS activation patterns were determined from the recordings of a steerable decapolar catheter (Xtrem, Alcis, Besancon, France), mm electrode spacing. In order to reflect the left rather than right septal atrial activation, proximal bipoles were positioned 1-2 cm within the CS ostium, the location of which was estimated from the plane of the atrial septum in the left anterior oblique view. CS recordings were analyzed with high gain settings (0.1mV/cm). The CS activation ation pattern was categorized by two parallel criteria: ia: - The first criterion was based on the CS activation sequence. ence. Four patterns were defined. The activation pattern was defined as proximal to distal when proximal and lateral al CS bipoles were, respectively, the earliest and the latest. t With reversal of activation, atio the CS activation atio pattern was defined as distal to proximal. The recording of the earliest activation ation on the mid-cs bipoles and the latest on both the proximal and distal bipoles was defined as a chevron pattern ( C pattern, Figure 1 A). Inversely, the recording of the earliest CS activations on both the proximal and distal bipoles and the latest on the mid-cs was defined as a reverse chevron pattern ( D pattern, Figure 1 B). - The second criterion was based on the EGMs recorded along the CS. A uniform CS activation was defined as the recording of single potentials on each CS bipoles with sequential activation throughout the CS. A non-uniform CS activation was defined as the recording of double potentials on one or more contiguous CS bipoles. Two patterns were characterized: disparate LA-CS activation and stepped activation. 5
6 Disparate LA-CS activation: Since ablation often targets the endo- and epicardial aspects of the inferior LA/CS region, partial LA-CS disconnection may occur. As a consequence, split potentials may be observed with a disparate activation sequence of the two components along the CS because of a distinct activation of the local CS musculature and the contiguous LA. Details on the mechanisms and patterns of CS activation related to LA-CS disconnection during AT post AF ablation have been published previously 7. Stepped CS activation: double potentials recorded on CS bipoles may alternatively both represent the LA endocardial activation and result from sensing on both sides of a line of conduction block or delay. In such cases, the number of CS bipoles with split potentials is confined to the bipoles that straddle the line of block. The staggered activation of the two LA segments overlying the split CS bipoles results in a stepped ed CS activation pattern. In cases of non-uniform nifo CS recordings, the first criterion ion (ie the activation ation sequence) e was categorized according to the actual endocardial LA activation ation for disparate LA-CS activation t and, according to the activation ation of the proximal CS bipoles for steppeded activation. ation The timing of CS activation was referenced to the tachycardia P waves recorded on the surface electrocardiogram lead V1. Surface P waves were analyzed during higher (> 2:1) grades of atrioventricular block. Recordings of 2:1 block were used when the P waves that preceded the QRS complexes were free of T waves. For single component P waves, the peak of the positive (or negative) deflection was used as reference (P peak ). For biphasic or multicomponent P waves, P peak was defined as the middle of the P wave deflection. The timing of CS activation was defined as the delay from P peak to the earliest activation recorded on bipoles CS 5-6 (mid-cs activation). A ratio was calculated by computing the P peak to mid-cs activation-delay divided by the AT CL. 6
7 Classification of AT. ATs were classified as macro-reentry or centrifugal AT, the latter including focal AT and localized reentry 8. Macroreentry was defined as reentry around a large central obstacle. A postpacing interval (PPI) exceeding the AT CL by no more than 30 ms on two opposite segments of the central obstacle was required for diagnosis. Centrifugal AT was defined as atrial activity originating from a single focus and spreading out centrifugally. If localized reentry was considered; and if not, a focal AT was considered. Mapping of postablation AT. All ATs were conventionally mapped using a deductive strategy t detailed previously 8. Briefly, a combination of activation and entrainment mapping was then used to determine ermin e the mechanism and location of AT. As a first step, the possibility of a macroreentry r was investigated. Atrial activation was mapped by systematically comparing the mapping catheter er signals with a reference r channel nel from the decapolar ar CS catheter. In the presence of a consistent nt activation ation sequence ence of the CS, a perimitral i circuit cuit was suspected ed or ruled out based on the activation ation sequence ence of the anterior mitral annulus. In the absence of sequential e circumferential activation of the mitral annulus, a roof-dependent reentry was mapped by looking for a cranial or caudal activation of the anterior and posterior LA walls. In the presence of similar or opposite directions of activation on both walls, roof-dependent reentry was ruled out or ruled-in, respectively. Entrainment mapping was performed in two opposite segments as guided by the activation mapping. In the presence of a PPI exceeding the AT CL by more than 30 ms in any segment, LA macroreentry was ruled out. A centrifugal AT was then mapped, initially in the LA and then in the right atrium. Repeated pacing maneuvers with analysis of the PPI were also used to progressively approach the site of origin. Statistical analysis. Continuous variables are given as arithmetic means ± SD and categorical 7
8 variables as percentages. Analysis was performed using the software STATA, version 8 (Stat Corp, College Station, TX, USA). Results A total of 239 sustained ATs were analysed in 140 consecutive patients who underwent163 procedures. The mean age was 59 ± 10 years and 81% were male. Patients had their first episode of AF a median of 84 months before ablation (limits 5 to 276) and had persistent AF for a median of 10 months (limits 0.5 to 132 months). They had failed treatment with 2.1 ± 0.9 antiarrhythmic drugs including amiodarone in 46 %. The mean LA diameter was 46 ± 7 mm in the parasternal rnal window. 43 patients (31%) had an underlying structural heart disease. Mean left ventricular ejection fraction was 58 ± 10 %. AT occurred either during the index ablation at procedure (29%) or late after AF ablation (71%). The mechanism m of AT (93%) was elucidated, ed, with sites of centrifugal AT confirmed by successful ablation. AT mechanisms s could not be diagnosed in 16 cases: 8 AT (3%) were terminated during entrainment maneuvers and 8 (3%) could not be identified due to widespread alterations in EGMs. Mechanism of AT following persistent AF ablation. The mechanism of AT was macroreentry in 56% of cases and centrifugal in 44%. Of the 124 macroreentrant AT, 66 were perimitral reentry (53%) (3 of which were figureof-eight with a roof-dependent loop), 30 roof-dependent reentry (24%) and 26 CTI-dependent reentry (21%). Two additional atypical macroreentries were diagnosed: one right-sided reentry around the superior vena cava and one non roof-dependent reentry around the LA appendage. Of the 99 centrifugal AT, 79 were localized reentry (80%) and 20 were focal AT (20%). The origin of centrifugal AT was located in the LA and CS for the vast majority of cases (n = 96, 8
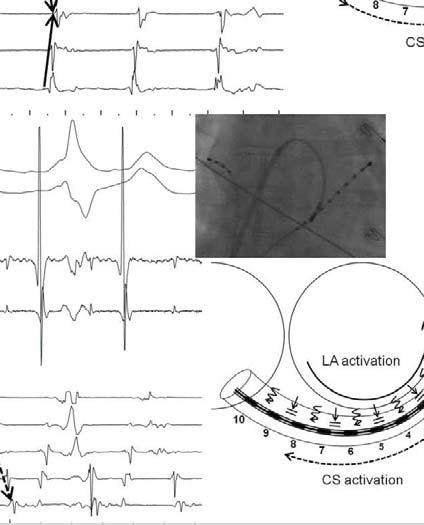
9 97%) with only three centrifugal ATs originating from the right atrium (two from the lateral wall and one from the superior vena cava). Prevalence of different CS activation patterns during AT. The CS activation sequence in the 239 ATs was proximal to distal in about half of the cases (49%). In the remaining half, the CS activation was distal to proximal in 31% of AT, chevron ( C pattern) in 13% and reverse chevron ( D pattern) in 6%. While in most patients the CS activation pattern was uniform, a non-uniform activation was recorded in 25% of ATs (n = 60). Non-uniform activation patterns were related to disparate LA-CS activations in 33 ATs (54%), stepped activation in 23 (39%), and both disparate ate LA-CS and stepped activation tion in 4 (7%). In disparate LA-CS activation, the activation sequence of the clinically relevant evant far-field inferior LA myocardium was from distal to proximal in 70% of cases (n = 26, Figure 2 A), chevron/reverse chevron in 16% (n = 6, Figure 2 B) and from proximal to distal in 14% (n = 5, Figure 2 C). In stepped p CS activation, despite the recording of split potentials on the laterall CS, the MI line was blocked only in about half of the cases (59%, n = 16). Three patterns of activation were observed (Figure 3): Pattern 1 (n = 11, 41%): a distinct pattern of the staggered activation recorded on the distal portion of the CS could be identified: the activation proceeded from distal to proximal, opposite to the activation recorded on the proximal portion of the CS (ie from proximal to distal). In doubtful cases, a more distal positioning of CS catheter could allow a better identification of the distal CS activation. These potentials resulted from the sensing of the adjacent LA activation wavefront on both sides of a blocked MI line (Figure 3 A). Pattern 2 (n = 5, 19%): as in Pattern 1, a distinct pattern of the staggered activation recorded on the distal CS could be identified which was instead in the same direction as the 9
10 activation recorded on the proximal CS portion (either proximal to distal or distal to proximal) (Figure 3 B). In these cases, the stepped activation resulted from the slow conduction through the MI line and, in most cases (n= 4), a perimitral AT was diagnosed with the split potentials outlining the gap on the MI line. Pattern 3 (n = 11, 41%): as against the Patterns 1 and 2, the stepped activation consisted of double potentials whose far-field components were recorded simultaneously on two or more bipoles with no discernable activation pattern. These potentials resulted from far-field LA appendage sensing rather than from the adjacent LA as in Patterns 1 and 2 (Figure 3 C). In this pattern, MI line conduction could not be anticipated: in about one third of cases (n = 4), the MI line was blocked whereas in the remaining cases, the stepped activation was related to conduction n delays through either the MI line or LA appendage. CS activation tion pattern in macroreentrant entr ant AT. The activation at io patterns observed in perimitral reentry were from distal to proximal (clockwise) in 62% (n = 41) and from proximal to distal (counterclockwise) ock e) in 38% (n = 25). In roof-dependent d reentry, the activation ation patterns were from proximal to distal in 43% of ATs (n = 13), chevron/reverse chevron in 30% (n = 9) and from distal to proximal in 27% (n = 8). The CS activation was from proximal to distal in all CTIdependent reentries (n = 20). Probability of AT mechanism and localization according to the CS activation pattern. The probability of AT diagnosis according to the patterns of CS activation is illustrated in Figure 4. In patients with proximal to distal CS activation, the whole range of possible AT mechanisms was observed (Figure 4 A). Right centrifugal ATs accounted for only 4% of cases. Consistent with the CS activation pattern, a clustering of the left centrifugal AT foci was observed on the septal side of the posterior LA (and CS). On the other hand, foci were widely 10
11 distributed over the anterior wall including lateral foci owing to the presence of MI block in 14% of the centrifugal ATs (Figure 4 A right). In distal to proximal CS activation (Figure 4 B), the majority (61%) of diagnosed ATs were clockwise perimitral ATs (n = 41, including 3 figure-of-eight with a roof-dependent loop). Consistent with the CS activation, centrifugal AT foci were exclusively localized on the lateral LA (Figure 4 B right). In chevron CS activation (Figure 4 C), the only macroreentrant AT observed was roof- dependent reentry which represented 17% of cases. Mapping consistently ntly revealed a descending activation of the posterior LA wall (Figure 4 C right). The remaining 83% were centrifugal ATs originating g exclusively ely from the posterior wall (including CS and roof). of). Similarly, in reverse chevron activation (Figure 4 D), macroreentrant ATs were roofdependent with one atypical reentry around the LA appendage (36%). Mapping pi of macroreentrant ATs consistently stently demonstrated ed a descending d activation tion of the anterior LA wall (Figure 4 D right). The remaining 64% were centrifugal ATs originating exclusively i el from the anterior wall (including the roof). Timing of CS activation and mechanism of AT. The delay from the surface P wave (P peak ) recorded in lead V1 to the local activation recorded on bipoles CS 5-6 could be analyzed in 97% of ATs. In centrifugal ATs, irrespective of the CS activation pattern, the timing of mid-cs activation was heterogeneous and spanned across the whole range of tachycardia cycle. Similarly, variable mid-cs activation timings were recorded in roof-dependent reentry. On the other hand, for other macroreentrant ATs, similar timings of CS activation were consistently observed among the study population: mid-cs activation occurred at 61 ± 13%, 0 ± 13% and 29 ± 11% of the P peak -P peak interval, for peritricuspid, counterclock- and clockwise perimitral AT, 11
12 respectively. The use of simple discriminant ranges of timings could help identify these macroreentrant ATs. Proximal to distal CS activation (Figure 5 A): A mid-cs activation at 50-70% of the P peak -P peak interval ( following the mid- P-P interval, n = 30, 14%) identified a peritricuspid AT with a positive and negative predictive value of 70% and 93%, respectively (sensitivity 81% and specificity 89%). A mid-cs activation at 80-99% or 0-20% of the P peak -P peak interval ( during the surface P wave, n = 54, 24%) identified counterclockwise perimitral AT with a sensitivity of 92%. A limited specificity was however observed (61%) due to the wide overlap with other AT mechanisms (positive and negative predictive value of 41% and 91%, respectively). el Distal to proximal CS activation (Figure 5 B): A mid-cs activation at 10-40% of the P peak -P peak interval ( immediately following P peak ak, n = 44, 20%) identified ed a clockwise ckwi perimitral AT with a positive and negative predictive value of 82% and 75%, respectively el (sensitivity ty 88% 8% and specificity 75%). Discussion Main findings. Our study demonstrates that a simple categorization of the patterns of CS activation could significantly narrow the differential diagnosis of macroreentrant ATs and aid localization of centrifugal ATs. Notably, in chevron and reverse chevron patterns, macroreentries were almost exclusively roof-dependent and mapping of centrifugal sources may be restricted to the posterior and anterior LA wall, respectively. Moreover, our study shows that despite extensive ablation, the timing of the mid-cs activation referenced to the surface P wave in V1 is remarkably constant for perimitral and peritricuspid AT. As a consequence, using a simple approach that integrates the analysis of both the pattern and timing of CS activation, a mapping 12
13 strategy can be deducted to select the most relevant activation and entrainment mapping maneuvers that should be undertaken first in more than one half of the cases. Background for a more deductive mapping strategy. Our study shows that more than half of the ATs occurring during or after persistent AF ablation are macroreentrant ATs (56%). The vast majority of them (98%) involved a circuit around at least one of these 3 fixed obstacles: ipsilateral PVs (left or right), the mitral and the tricuspid annulus. Centrifugal ATs mainly originating from the LA represented the remaining cases. The observation that only three types of macroreentrant circuits represent the majority of ATs after persistent AF ablation provide an opportunity to implement more pragmatic mapping strategies. The complexity of mapping often resides in the multiple areas with extensive voltage reduction and/or multiple component EGMs with altered sequence ence of activation. In these situations detailed mapping may prove either er difficult fi or confusing and will often impose the operator to take a step back to concentrate his initial itiai mapping on few selected ed points. A focused activation mappingpi of the anterior and posterior LA wall will allow to rapidly narrow the differential diagnosis and find the region of interest 8. For this purpose, the analysis of the CS recordings provides immediate segmental activation mapping of the inferior (annular) posterior LA wall. Depending on the inferior LA activation pattern, our study shows that major differences in the AT mechanisms and localizations exists. These differences can be taken as an opportunity to individualize the mapping strategy 9. Pitfalls in the analysis of the CS activation: the non-uniform patterns. A potential drawback of the CS activation pattern analysis lies in the interpretation of sometimes complex EGMs. A non-uniform CS activation pattern was identified in 25% of cases. About half of them were related to disparate LA-CS activation as a consequence of partial LA-CS disconnection due 13
14 to previous ablation 7. Failure to carefully inspect CS potentials at an adequate scale can easily mislead the operator considering that the more apparent CS muscle activation sequence is in fact opposite to the clinically more relevant LA activation. A stepped CS activation was observed in the remaining half, either alone or in combination with disparate LA-CS activation. The recording of a delayed activation of the two LA segments overlying the split CS potentials is often considered to result from sensing on both sides of a blocked MI line. In contrast, our study show that the MI line was not blocked in about 40% of such cases. Moreover, our study shows that stepped CS activation tion does not necessarily essasa add to the complexity of CS interpretation but could instead be used as a diagnostic ic opportunity. ortu In 60% of cases, s, a distinct pattern of activation of the far-field components nts of the double potentials could be identified (Patterns terns 1 and 2). In such cases, the presence of a MI block (opposite activation) tion or a MI gap with slow conduction (parallel activation) atio could be diagnosed. In the latter, perimitral reentries ries were almost exclusively ly diagnosed with termination i n of the AT during ablation ation on the gap outlined by the split potentials ti recorded on the CS catheter. t Timing of CS activation to guide the mapping strategy. Our study shows that the analysis of the CS activation timing with respect to the surface P wave in lead V1 provides a useful guide to the diagnosis of most peritricuspid and perimitral ATs, despite previous substrate ablation and the creation of lines of block. These findings probably relate to the fact that the P wave in reference lead V1 mainly results from the activation of the right atrium and its appendage especially after extensive LA ablation. The similar CS- right atrium timing sequence of activation therefore probably derives from the fact that both reentries are circuits around fixed anatomical obstacles located either in the right atrium or along the CS. However, most peritricuspid ATs observed after persistent AF ablation were counterclockwise reentries. As a 14
15 consequence, considering the expected differences in the CS-RA activation sequence, our findings may be less applicable to a selected population with clockwise peritricuspid AT. Categorization of the CS activation patterns and timing to rationalize the mapping strategy. - Proximal to distal CS activation: This pattern is the most non-specific pattern as the whole range of AT mechanism and location should be considered. However, whenever the mid- CS activation occurs at 50-70% of the P peak -P peak interval (ie following the mid- P-P interval), most peritricuspid ATs will be indentified with good specificity. The first mapping step will therefore be to rule-out this diagnosis by appropriate mapping and entrainment maneuvers. This single step will provide the diagnosis in about 20% of cases and, if negative, e, will allow low the operator to concentrate his mapping in the LA. This is all the more relevant e considering that in the setting of markedly abnormal atrial substrate following AF ablation, CTI-dependent endent AT rarely manifests with a typical saw-tooth oth appearance pearance on 12-lead ECG 10. Focused segmental LA activation mapping ping should be performed next to exclude the most frequent e LA macroreentries reentrr 8. For this purpose, the two-axis activation ation of both the anterior and posterior LA wall is first considered: the vertical axis activation (ascending or descending wavefront) and the septo-lateral axis activation of its annular segments (Figure 6 A). A lateral to septal anterior mitral annulus activation (ie opposite to the CS activation) will rule in perimitral AT, while an opposite anterior/posterior wall vertical activation will rule in roof-dependent AT. Appropriate entrainment maneuvers to confirm one or the other diagnosis will be performed. If both macroreentries are ruled out, the operator will concentrate his mapping on searching for the earliest activation of a LA focal source guided by the two-axis activation mapping. A right atrial origin will be considered in case of consistent LA mapping (ie septal to lateral anterior activation). Our study shows that most centrifugal sources are located on the septal half of the 15
16 LA (including the CS) (81%). However, a source from the lateral anterior wall should also be considered as a previous block (or slow conduction) across the MI line will also result in a proximal to distal CS activation despite the lateral origin 9. As discussed, a stepped CS activation will provide a clue in such situations. - Distal to proximal CS activation: This pattern is related to clockwise perimitral AT in the majority of cases (61%). The mapping strategy should therefore first aim at ruling in or out this possibility. Our study shows that the analysis of the timing of the mid-cs activation with respect to the surface P wave in lead V1 can aide identify most perimitral ATs with good od specificity. c Accordingly, whenever mid-cs activation occurs at 10-40% of the P peak -P peak interval (ie eak-p peak in immediately follows ows the P peak in V1), the first mapping step should be to rule-out perimitral AT by appropriate entrainment maneuver. This selectively applied plie pacing maneuvere will provide the diagnosis in more than half of distal to proximal ATs (54%). In the remaining ng cases, the two-axis segmental LA activation i mapping of both the anterior and posterior o LA will be performed. Only the vertical axis of activation ation (i.e. ascending or descending) d will be assesseded for those cases where perimitral AT has been ruled out. If roof-dependent AT is ruled out, mapping can concentrate on searching for the earliest activation of a focal source on the lateral part of the LA guided by the previously assessed vertical axis activation. - Chevron CS activation: This pattern results from either a posterior centrifugal, or descending, activation wavefront. As a consequence, perimitral and CTI-dependent AT are excluded and the only macrorentrant AT observed was roof-dependent. A pragmatic approach would therefore be to first exclude this diagnosis. Considering that only an ascending activation of the anterior wall will rule-in the diagnosis of roof-dependent AT (ie opposite to the posterior wall), only limited mapping of the anterior wall is required (Figure 6 B). In the event of opposite vertical activation 16
17 of both walls, selective entrainment will rule out or confirm the diagnosis. If roof-dependent AT is ruled out, further mapping can concentrate on searching for the earliest activation of a focal source on the posterior wall (including the roof and CS). - Reverse chevron CS activation: This pattern results from either an anterior centrifugal, or descending, activation wavefront. As a consequence perimitral AT is excluded and no peritricuspid AT was observed. Though unlikely, the diagnosis of CTI-dependent reentry can not formally be excluded since previous reports have shown the possible occurrence of reverse chevron pattern in clockwise peritricuspid AT 11, 12. In these cases, the LA is predominantly activated over the Bachmann s bundle as opposed to the CS ostium. Similar to the chevron pattern the first step will be to rule out a roof-dependent d nt AT. An ascending ng activation of the posterior wall will rule this diagnosis s in (ie opposite to the anterior wall) confirmed or not by entrainment maneuvers (Figure 6 C). If roof-dependent of d nt AT is ruled out, the operator r will be able to concentrate on searching for the earliest activation of a focal source on the anterior wall (including the roof). A summary of proposed initial mapping steps based on the CS activation patterns and timing is illustrated in Figure 7. The AT mechanism and localization may be provided in nearly half of the patients by using only focused mapping of one LA segment or the evaluation of the CS activation timing. Study limitations. The stepwise ablation approach performed in the study population included EGM-guided and LA linear lesions. Since the prevalence of both the type and localization of AT is closely related to the ablation strategy adopted, these findings may less apply in a patient population where a more conservative strategy is undertaken. On the other hand, the same 17
18 assumption strengthens the potential value of a pattern-based strategy to guide the initial mapping steps even in more complex underlying atrial substrate. A variety of atypical macroreentrant ATs other than those reported in our study may occur after persistent AF ablation. These ATs will require more extensive activation and entrainment mapping. However, their prevalence is low considering that only two of them were diagnosed (1%) while the mechanism of only 3% of AT could not be elucidated. Finally, relying on the CS activation pattern implies a proper positioning of the CS catheter which may occasionally prove difficult. Conclusion n The analysis of both the patterns terns and timing of CS activation at io can aid rapid diagnosis is of postablation o ATs. It provides a rapid stratification ic atio ion of the most likely ly macroreentrant reen entr an t ATs that should first be ruled out and points towards the likely origin in of centrifugal ATs. It can be included in a stepwise se diagnostic approach p to rapidly select the most critical cal activation ation and entrainment mapping maneuvers. Funding Sources: Patrizio Pascale acknowledges financial support from the Swiss National Science Foundation and the SICPA Foundation. Conflict of Interest Disclosures: None References: 1. Haissaguerre M, Sanders P, Hocini M, Takahashi Y, Rotter M, Sacher F, Rostock T, Hsu LF, Bordachar P, Reuter S, Roudaut R, Clementy J, Jais P. Catheter ablation of long-lasting persistent atrial fibrillation: Critical structures for termination. J Cardiovasc Electrophysiol. 2005;16: Nademanee K, McKenzie J, Kosar E, Schwab M, Sunsaneewitayakul B, Vasavakul T, Khunnawat C, Ngarmukos T. A new approach for catheter ablation of atrial fibrillation: Mapping 18
19 of the electrophysiologic substrate. J Am Coll Cardiol. 2004;43: Chugh A, Oral H, Lemola K, Hall B, Cheung P, Good E, Tamirisa K, Han J, Bogun F, Pelosi F, Jr., Morady F. Prevalence, mechanisms, and clinical significance of macroreentrant atrial tachycardia during and following left atrial ablation for atrial fibrillation. Heart Rhythm. 2005;2: Gerstenfeld EP, Marchlinski FE. Mapping and ablation of left atrial tachycardias occurring after atrial fibrillation ablation. Heart Rhythm. 2007;4:S Haissaguerre M, Hocini M, Sanders P, Sacher F, Rotter M, Takahashi Y, Rostock T, Hsu LF, Bordachar P, Reuter S, Roudaut R, Clementy J, Jais P. Catheter ablation of long-lasting persistent atrial fibrillation: Clinical outcome and mechanisms of subsequent arrhythmias. J Cardiovasc Electrophysiol. 2005;16: Rostock T, Drewitz I, Steven D, Hoffmann BA, Salukhe TV, Bock K, Servatius H, Aydin MA, Meinertz T, Willems S. Characterization, mapping, and catheter ablation of recurrent rent atrial tachycardias after stepwise ablation of long-lasting persistent atrial fibrillation. Circ Arrhythm Electrophysiol. ol. 2010;3: Pascale P, Shah AJ, Roten L, Whinnett Z, Wilton SB, Jadidi AS, Scherr D, Miyazaki S, Pedersen M, Derval N, Knecht S, Sacher F, Hocini M, Haissaguerre sa M, Jais P. Disparate activation of the coronary sinus and inferior left atrium during atrial tachycardia ardi a after persistent s atrial fibrillation lation ablation: Prevalence, en pitfalls, ls, and impact on mapping. J Cardiovasc Electrophysiol. 2012;23: Jais P, Matsuo S, Knecht S, Weerasooriya a R, Hocini M, Sacher F, Wright M, Nault I, Lellouche N, Klein G, Clementy J, Haissaguerre M. A deductive mapping strategy for atrial tachycardia following atrial fibrillation ablation: Importance of localized reentry. J Cardiovasc Electrophysiol. 2009;20: Steven D, Seiler J, Roberts-Thomson KC, Inada K, Stevenson WG. Mapping of atrial tachycardias after catheter ablation for atrial fibrillation: Use of bi-atrial activation patterns to facilitate recognition of origin. Heart Rhythm. 2010;7: Chugh A, Latchamsetty R, Oral H, Elmouchi D, Tschopp D, Reich S, Igic P, Lemerand T, Good E, Bogun F, Pelosi F, Jr., Morady F. Characteristics of cavotricuspid isthmus-dependent atrial flutter after left atrial ablation of atrial fibrillation. Circulation. 2006;113: Oshikawa N, Watanabe I, Masaki R, Okumura Y, Okubo K, Sugimura H, Kojima T, Saito S, Ozawa Y, Kanmatsuse K. Relationship between polarity of the flutter wave in the surface ecg and endocardial atrial activation sequence in patients with typical counterclockwise and clockwise atrial flutter. J Interv Card Electrophysiol. 2002;7: Marine JE, Korley VJ, Obioha-Ngwu O, Chen J, Zimetbaum P, Papageorgiou P, Milliez P, Josephson ME. Different patterns of interatrial conduction in clockwise and counterclockwise 19
20 atrial flutter. Circulation. 2001;104: Figure Legends: Figure 1. Chevron-like CS activation patterns. A. The chevron pattern results from the centrifugal activation of the CS from its mid portion (solid arrows) from a descending posteriorwall activation (dashed arrow). B. The reverse chevron results from the fusion of two activation wavefronts (solid arrows) from a descending anterior wall activation (dashed arrow). Figure 2. Disparate LA-CS activation patterns. A. Proximal to distal LA activation. Double potentials are recorded along the whole CS. The early component, on consisting ing of low-amplitude and broad potentials, represents esen ents the far-field field LA endocardial dial activity ty (solid arrow). The second component, consisting s ing of sharper potentials, represents the activation tion of the CS musculature and propagates in the opposite posi direction (dashed arrow). (right) The activation atio of the local CS musculature occurs when the endocardially propagating wavefront crosses over to the proximal CS epicardium (mid- and distal LA-CS disconnection) B. Reverse chevron LA activation. Double potentials are observed on the two distal CS bipoles; the broader potentials representing the far-field LA are activated earlier from distal to proximal (solid arrow on the distal CS) while CS musculature proceeds from proximal to distal (dashed arrow). (right) The distal LA-CS disconnection (up to CS bipoles CS 5-6) leads to the delayed distal local CS activation. C. Distal to proximal LA activation. The sequence of activation of the far-field LA is opposite to that shown in panel A (solid arrow). Endocardial mapping confirms that the local LA potential (RFd) facing CS 7-8 corresponds temporally to the first potential recorded on CS 7-8. (right) The local CS musculature is activated through intact distal LA-CS connections. 20
21 Figure 3. Patterns of stepped CS activation. A. Pattern 1: Double potentials are barely discernable with a staggered activation of the distal two CS bipoles (dashed arrows). The activation on the proximal CS proceeds from proximal to distal (solid arrows). (Lower panel) A more distal positioning of the CS catheter allows to identify a distinct opposite activation pattern on the distal CS portion (ie from distal to proximal). (right) This pattern results from two opposite inferior LA wavefronts activating both sides of a blocked MI line at different timings. B. Pattern 2: The two staggered activation pattern recorded on the proximal and distal portion of the CS are both parallel and proceeds from distal to proximal (solid arrows). rows). (right) The delay recorded on CS 5-6 results from the slowed conduction through the underlying ng MI line. C. Pattern 3: the stepped ed activation ation consists of double potentials whose far-field field components are recorded simultaneously with no discernable activation pattern. tern. (right) These potentials corresponds temporally ly to the LA appendage activation ation (RFd) recorded rd ed distally on the anterolateral CS. Figure 4. Diagnostic stratification based on the categorization of the CS activation. Proximal to distal (A), distal to proximal (B), chevron (C) and reverse chevron (D) CS activation. (left) Pie chart illustrating the prevalence of each AT mechanism. (right) Distribution of centrifugal AT sources and schematic activation of the LA macroreentries (solid arrows). In proximal to distal CS activation, centrifugal sources originating from the lateral side of the anterior LA wall were associated with MI block (labeled in red). including one atypical macroreentry around the LA appendage Figure 5. Scatterplot showing the individual values of the mid-cs activation timing for each AT mechanism and for proximal to distal (A) and distal to proximal (B) CS activation. A right 21
22 panels. (top) Mid-CS activation timing in a CTI-dependent AT: the activation of the mid-cs follows the mid-p-p interval with a calculated ratio of 62%. (bottom) Counterclockwise perimitral AT: the mid-cs activation immediately follows P peak with a calculated ratio of 11%. Figure 6. Mapping strategy based on the CS activation A. Proximal to distal CS activation. Step 1: the mid-cs activation occurs during the surface P wave in V1 (calculated ratio 89%) making a CTI-dependent AT unlikely. Step 2: The two-axis segmental LA activation mapping is performed: using CS 1-2 as a reference, and moving the RF catheter, the local activation time is obtained at the lateral, mid- and septal anterior mitral annulus. This allows lows to identify ify a lateral to septal activation of the anterior annular LA segment, i.e. opposite to the posterior annular LA activation. Counterclockwise ckwi perimitral itral AT is therefore ruled in later confirmed by entrainment maneuvers. B. Chevron CS activation ion pattern. Step 1: using CS 5-6 as a reference, er ence the local l activation time is obtained at the high and low anterior wall. l. This allows lows to identify a descending e anterior wall l activation t therefore ruling out a roof-dependent of-d e d nt AT. Step 2: The earliest est activation site of a centrifugal source is mapped on the posterior wall using the same technique. A descending posterior wall activation is observed with the earliest local activation time identified on the roof. Ablation at this site successfully restored sinus rhythm. C. Reverse chevron pattern. Step 1: using CS 1-2 as a reference, the local activation time is obtained at the low, mid- and high posterior wall. This allows to identify an ascending posterior wall activation which rules in a roof-dependent AT. Step 2: Entrainment maneuvers (shownon the mid-posterior wall) confirmed a roof-dependent AT. Figure 7. Stepwise algorithm of AT mapping based on the pattern and timing of CS activation. 22



23

24


25




26


27



28


29


30 Pattern and Timing of the Coronary Sinus Activation to Guide Rapid Diagnosis of Atrial Tachycardia after Atrial Fibrillation Ablation Patrizio Pascale, Ashok J. Shah, Laurent Roten, Daniel Scherr, Yuki Komatsu, Amir S. Jadidi, Khaled Ramoul, Matthew Daly, Arnaud Denis, Stephen B. Wilton, Nicolas Derval, Frédéric Sacher, Mélèze Hocini, Michel Haïssaguerre and Pierre Jaïs Circ Arrhythm Electrophysiol. published online April 29, 2013; Circulation: Arrhythmia and Electrophysiology is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX Copyright 2013 American Heart Association, Inc. All rights reserved. Print ISSN: Online ISSN: The online version of this article, along with updated information and services, is located on the World Wide Web at: Permissions: Requests for permissions to reproduce figures, tables, or portions of articles originally published in Circulation: Arrhythmia and Electrophysiology can be obtained via RightsLink, a service of the Copyright Clearance Center, not the Editorial Office. Once the online version of the published article for which permission is being requested is located, click Request Permissions in the middle column of the Web page under Services. Further information about this process is available in the Permissions and Rights Question and Answerdocument. Reprints: Information about reprints can be found online at: Subscriptions: Information about subscribing to Circulation: Arrhythmia and Electrophysiology is online at:
Peri-Mitral Atrial Flutter with Partial Conduction Block between Left Atrium and Coronary Sinus
 Accepted Manuscript Peri-Mitral Atrial Flutter with Partial Conduction Block between Left Atrium and Coronary Sinus Ryota Isogai, MD, Seiichiro Matsuo, MD, Ryohsuke Narui, MD, Shingo Seki, MD;, Michihiro
Accepted Manuscript Peri-Mitral Atrial Flutter with Partial Conduction Block between Left Atrium and Coronary Sinus Ryota Isogai, MD, Seiichiro Matsuo, MD, Ryohsuke Narui, MD, Shingo Seki, MD;, Michihiro
How to Distinguish Focal Atrial Tachycardia from Small Circuits and Reentry
 How to Distinguish Focal Atrial Tachycardia from Small Circuits and Reentry Pierre Jaïs; Bordeaux, France IHU LIRYC ANR-10-IAHU-04 Equipex MUSIC imaging platform ANR-11-EQPX-0030 Eutraf HEALTH-F2-2010-261057
How to Distinguish Focal Atrial Tachycardia from Small Circuits and Reentry Pierre Jaïs; Bordeaux, France IHU LIRYC ANR-10-IAHU-04 Equipex MUSIC imaging platform ANR-11-EQPX-0030 Eutraf HEALTH-F2-2010-261057
1995 Our First AF Ablation. Atrial Tachycardias During and After Atrial Fibrillation Ablation. Left Atrial Flutter. 13 Hours Later 9/25/2009
 1995 Our First AF Ablation Atrial Tachycardias During and After Atrial Fibrillation Ablation G. Neal Kay MD University of Alabama at Birmingham Right Anterior Oblique Left Anterior Oblique Left Atrial
1995 Our First AF Ablation Atrial Tachycardias During and After Atrial Fibrillation Ablation G. Neal Kay MD University of Alabama at Birmingham Right Anterior Oblique Left Anterior Oblique Left Atrial
How to ablate typical atrial flutter
 Europace (1999) 1, 151 155 HOW TO... SERIES How to ablate typical atrial flutter A. Takahashi, D. C. Shah, P. Jaïs and M. Haïssaguerre Electrophysiologie Cardiaque, Hopital Cardiologique du Haut-Lévêque,
Europace (1999) 1, 151 155 HOW TO... SERIES How to ablate typical atrial flutter A. Takahashi, D. C. Shah, P. Jaïs and M. Haïssaguerre Electrophysiologie Cardiaque, Hopital Cardiologique du Haut-Lévêque,
Electrical disconnection of pulmonary vein (PV) myocardium
 myocardium") Left Atrial Appendage Activity Masquerading as Pulmonary Vein Potentials Dipen Shah, MD; Michel Haissaguerre, MD; Pierre Jais, MD; Meleze Hocini, MD; Teiichi Yamane, MD; Laurent Macle, MD; Kee Joon Choi,
Left Atrial Appendage Activity Masquerading as Pulmonary Vein Potentials Dipen Shah, MD; Michel Haissaguerre, MD; Pierre Jais, MD; Meleze Hocini, MD; Teiichi Yamane, MD; Laurent Macle, MD; Kee Joon Choi,
Peri-mitral atrial flutter in patients with atrial fibrillation ablation
 Peri-mitral atrial flutter in patients with atrial fibrillation ablation Seiichiro Matsuo, MD,* Matthew Wright, MBBS, PhD,* Sébastien Knecht, MD,* Isabelle Nault, MD,* Nicolas Lellouche, MD,* Kang-Teng
Peri-mitral atrial flutter in patients with atrial fibrillation ablation Seiichiro Matsuo, MD,* Matthew Wright, MBBS, PhD,* Sébastien Knecht, MD,* Isabelle Nault, MD,* Nicolas Lellouche, MD,* Kang-Teng
Since pulmonary veins (PVs) have
 have") Case Report Hellenic J Cardiol 2011; 52: 371-376 Left Atrial-Pulmonary Vein Reentrant Tachycardia Following Pulmonary Vein Isolation Dionyssios Leftheriotis, Feifan Ouyang, Karl-Heinz Kuck II. Med. Abteilung,
Case Report Hellenic J Cardiol 2011; 52: 371-376 Left Atrial-Pulmonary Vein Reentrant Tachycardia Following Pulmonary Vein Isolation Dionyssios Leftheriotis, Feifan Ouyang, Karl-Heinz Kuck II. Med. Abteilung,
Ablation of long-standing AF. Is it wise to pursue it?
 Ablation of long-standing AF. Is it wise to pursue it? Carlo Pappone, MD and Vincenzo Santinelli, MD From: Department of Arrhythmology,GVM Care and Research, Cotignola, Ravenna, ITALY Address for correspondence:
Ablation of long-standing AF. Is it wise to pursue it? Carlo Pappone, MD and Vincenzo Santinelli, MD From: Department of Arrhythmology,GVM Care and Research, Cotignola, Ravenna, ITALY Address for correspondence:
Clinical Value of Noninducibility by High-Dose Isoproterenol Versus Rapid Atrial Pacing After Catheter Ablation of Paroxysmal Atrial Fibrillation
 13 Clinical Value of Noninducibility by High-Dose Isoproterenol Versus Rapid Atrial Pacing After Catheter Ablation of Paroxysmal Atrial Fibrillation THOMAS CRAWFORD, M.D., AMAN CHUGH, M.D., ERIC GOOD,
13 Clinical Value of Noninducibility by High-Dose Isoproterenol Versus Rapid Atrial Pacing After Catheter Ablation of Paroxysmal Atrial Fibrillation THOMAS CRAWFORD, M.D., AMAN CHUGH, M.D., ERIC GOOD,
Electrical isolation of the pulmonary veins (PVs) to treat
 to treat") Mechanisms of Organized Left Atrial Tachycardias Occurring After Pulmonary Vein Isolation Edward P. Gerstenfeld, MD; David J. Callans, MD; Sanjay Dixit, MD; Andrea M. Russo, MD; Hemal Nayak, MD; David
Mechanisms of Organized Left Atrial Tachycardias Occurring After Pulmonary Vein Isolation Edward P. Gerstenfeld, MD; David J. Callans, MD; Sanjay Dixit, MD; Andrea M. Russo, MD; Hemal Nayak, MD; David
We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists. International authors and editors
 We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists 3,800 116,000 120M Open access books available International authors and editors Downloads Our
We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists 3,800 116,000 120M Open access books available International authors and editors Downloads Our
A Narrow QRS Complex Tachycardia With An Apparently Concentric Retrograde Atrial Activation Sequence
 www.ipej.org 125 Case Report A Narrow QRS Complex Tachycardia With An Apparently Concentric Retrograde Atrial Activation Sequence Miguel A. Arias MD, PhD; Eduardo Castellanos MD, PhD; Alberto Puchol MD;
www.ipej.org 125 Case Report A Narrow QRS Complex Tachycardia With An Apparently Concentric Retrograde Atrial Activation Sequence Miguel A. Arias MD, PhD; Eduardo Castellanos MD, PhD; Alberto Puchol MD;
Arrhythmia/Electrophysiology. Characteristics of Cavotricuspid Isthmus Dependent Atrial Flutter After Left Atrial Ablation of Atrial Fibrillation
 Arrhythmia/Electrophysiology Characteristics of Cavotricuspid Isthmus Dependent Atrial Flutter After Left Atrial Ablation of Atrial Fibrillation Aman Chugh, MD; Rakesh Latchamsetty, MD; Hakan Oral, MD;
Arrhythmia/Electrophysiology Characteristics of Cavotricuspid Isthmus Dependent Atrial Flutter After Left Atrial Ablation of Atrial Fibrillation Aman Chugh, MD; Rakesh Latchamsetty, MD; Hakan Oral, MD;
480 April 2004 PACE, Vol. 27
 Incremental Value of Isolating the Right Inferior Pulmonary Vein During Pulmonary Vein Isolation Procedures in Patients With Paroxysmal Atrial Fibrillation HAKAN ORAL, AMAN CHUGH, CHRISTOPH SCHARF, BURR
Incremental Value of Isolating the Right Inferior Pulmonary Vein During Pulmonary Vein Isolation Procedures in Patients With Paroxysmal Atrial Fibrillation HAKAN ORAL, AMAN CHUGH, CHRISTOPH SCHARF, BURR
doi: /CIRCEP
 Prevalence and Types of Pitfall in the Assessment of Mitral Isthmus Linear Conduction Block Ashok J. Shah, Patrizio Pascale, Shinsuke Miyazaki, Xingpeng Liu, Laurent Roten, Nicolas Derval, Amir S. Jadidi,
Prevalence and Types of Pitfall in the Assessment of Mitral Isthmus Linear Conduction Block Ashok J. Shah, Patrizio Pascale, Shinsuke Miyazaki, Xingpeng Liu, Laurent Roten, Nicolas Derval, Amir S. Jadidi,
Reentry in a Pulmonary Vein as a Possible Mechanism of Focal Atrial Fibrillation
 824 Reentry in a Pulmonary Vein as a Possible Mechanism of Focal Atrial Fibrillation BERNARD BELHASSEN, M.D., AHARON GLICK, M.D., and SAMI VISKIN, M.D. From the Department of Cardiology, Tel-Aviv Sourasky
824 Reentry in a Pulmonary Vein as a Possible Mechanism of Focal Atrial Fibrillation BERNARD BELHASSEN, M.D., AHARON GLICK, M.D., and SAMI VISKIN, M.D. From the Department of Cardiology, Tel-Aviv Sourasky
Pulmonary vein isolation (PVI) is
 is") Case Report Hellenic J Cardiol 2012; 53: 163-167 The Use of the Multi-Electrode Duty-Cycled Radiofrequency Ablation Catheter PVAC for the Ablation of a Left Atrial Tachycardia Dionyssios Leftheriotis 1,
Case Report Hellenic J Cardiol 2012; 53: 163-167 The Use of the Multi-Electrode Duty-Cycled Radiofrequency Ablation Catheter PVAC for the Ablation of a Left Atrial Tachycardia Dionyssios Leftheriotis 1,
Effects of Stepwise Ablation of Chronic Atrial Fibrillation on Atrial Electrical and Mechanical Properties
 Journal of the American College of Cardiology Vol. 49, No. 12, 2007 2007 by the American College of Cardiology Foundation ISSN 0735-1097/07/$32.00 Published by Elsevier Inc. doi:10.1016/j.jacc.2006.11.033
Journal of the American College of Cardiology Vol. 49, No. 12, 2007 2007 by the American College of Cardiology Foundation ISSN 0735-1097/07/$32.00 Published by Elsevier Inc. doi:10.1016/j.jacc.2006.11.033
Journal of the American College of Cardiology Vol. 38, No. 5, by the American College of Cardiology ISSN /01/$20.
 Journal of the American College of Cardiology Vol. 38, No. 5, 2001 2001 by the American College of Cardiology ISSN 0735-1097/01/$20.00 Published by Elsevier Science Inc. PII S0735-1097(01)01578-9 Morphological
Journal of the American College of Cardiology Vol. 38, No. 5, 2001 2001 by the American College of Cardiology ISSN 0735-1097/01/$20.00 Published by Elsevier Science Inc. PII S0735-1097(01)01578-9 Morphological
Catheter ablation of AF Where do we stand, where do we go?
 Catheter ablation of AF Where do we stand, where do we go? Sébastien Knecht MD, PhD Hôpital cardiologique du Haut L Evêque, Bordeaux Declaration of conflict of interest ABLATION STRATEGIES Duration proc:
Catheter ablation of AF Where do we stand, where do we go? Sébastien Knecht MD, PhD Hôpital cardiologique du Haut L Evêque, Bordeaux Declaration of conflict of interest ABLATION STRATEGIES Duration proc:
Mechanism of Immediate Recurrences of Atrial Fibrillation After Restoration of Sinus Rhythm
 Mechanism of Immediate Recurrences of Atrial Fibrillation After Restoration of Sinus Rhythm AMAN CHUGH, MEHMET OZAYDIN, CHRISTOPH SCHARF, STEVE W.K. LAI, BURR HALL, PETER CHEUNG, FRANK PELOSI, JR, BRADLEY
Mechanism of Immediate Recurrences of Atrial Fibrillation After Restoration of Sinus Rhythm AMAN CHUGH, MEHMET OZAYDIN, CHRISTOPH SCHARF, STEVE W.K. LAI, BURR HALL, PETER CHEUNG, FRANK PELOSI, JR, BRADLEY
Case Report. Sumito Narita MD 1;3, Takeshi Tsuchiya MD, PhD 1, Hiroya Ushinohama MD, PhD 2, Shin-ichi Ando MD, PhD 3
 Case Report Identification and Radiofrequency Catheter Ablation of a Nonsustained Atrial Tachycardia at the Septal Mitral Annulus with the Use of a Noncontact Mapping System: A Case Report Sumito Narita
Case Report Identification and Radiofrequency Catheter Ablation of a Nonsustained Atrial Tachycardia at the Septal Mitral Annulus with the Use of a Noncontact Mapping System: A Case Report Sumito Narita
Disparate Evolution of Right and Left Atrial Rate During Ablation of Long-Lasting Persistent Atrial Fibrillation
 Journal of the American College of Cardiology Vol. 55, No. 10, 2010 2010 by the American College of Cardiology Foundation ISSN 0735-1097/10/$36.00 Published by Elsevier Inc. doi:10.1016/j.jacc.2009.09.060
Journal of the American College of Cardiology Vol. 55, No. 10, 2010 2010 by the American College of Cardiology Foundation ISSN 0735-1097/10/$36.00 Published by Elsevier Inc. doi:10.1016/j.jacc.2009.09.060
Characteristics of Rapid Rhythms Recorded Within Pulmonary Veins During Atrial Fibrillation
 Characteristics of Rapid Rhythms Recorded Within Pulmonary Veins During Atrial Fibrillation HIROSHI TADA, MEHMET ÖZAYDIN, HAKAN ORAL, BRADLEY P. KNIGHT, AMAN CHUGH, CHRISTOPH SCHARF, FRANK PELOSI, Jr.,
Characteristics of Rapid Rhythms Recorded Within Pulmonary Veins During Atrial Fibrillation HIROSHI TADA, MEHMET ÖZAYDIN, HAKAN ORAL, BRADLEY P. KNIGHT, AMAN CHUGH, CHRISTOPH SCHARF, FRANK PELOSI, Jr.,
The major thoracic veins, with their specific electrical
 Atrial Fibrillation Originating From Persistent Left Superior Vena Cava Li-Fern Hsu, MBBS; Pierre Jaïs, MD; David Keane, MD; J. Marcus Wharton, MD; Isabel Deisenhofer, MD; Mélèze Hocini, MD; Dipen C. Shah,
Atrial Fibrillation Originating From Persistent Left Superior Vena Cava Li-Fern Hsu, MBBS; Pierre Jaïs, MD; David Keane, MD; J. Marcus Wharton, MD; Isabel Deisenhofer, MD; Mélèze Hocini, MD; Dipen C. Shah,
From the Division of Cardiology, Department of Internal Medicine, University of Michigan Medical Center, Ann Arbor, Michigan
 118 Reprinted with permission from JOURNAL OF CARDIOVASCULAR ELECTROPHYSIOLOGY, Volume 13, No. 2, February 2002 Copyright 2002 by Futura Publishing Company, Inc., Armonk, NY 10504-0418 Differentiation
118 Reprinted with permission from JOURNAL OF CARDIOVASCULAR ELECTROPHYSIOLOGY, Volume 13, No. 2, February 2002 Copyright 2002 by Futura Publishing Company, Inc., Armonk, NY 10504-0418 Differentiation
Case Report Electroanatomical Mapping and Ablation of Upper Loop Reentry Atrial Flutter
 Hellenic J Cardiol 46: 74-78, 2005 Case Report Electroanatomical Mapping and blation of Upper Loop Reentry trial Flutter POSTOLOS KTSIVS, PNGIOTIS IONNIDIS, CHRLMOS VSSILOPOULOS, THIN GIOTOPOULOU, THNSIOS
Hellenic J Cardiol 46: 74-78, 2005 Case Report Electroanatomical Mapping and blation of Upper Loop Reentry trial Flutter POSTOLOS KTSIVS, PNGIOTIS IONNIDIS, CHRLMOS VSSILOPOULOS, THIN GIOTOPOULOU, THNSIOS
Because of renewed interest in the mechanism and treatment
 Different s of Interatrial Conduction in Clockwise and Counterclockwise Atrial Flutter Joseph E. Marine, MD; Victoria J. Korley, MD; Ogundu Obioha-Ngwu, MD; Jane Chen, MD; Peter Zimetbaum, MD; Panos Papageorgiou,
Different s of Interatrial Conduction in Clockwise and Counterclockwise Atrial Flutter Joseph E. Marine, MD; Victoria J. Korley, MD; Ogundu Obioha-Ngwu, MD; Jane Chen, MD; Peter Zimetbaum, MD; Panos Papageorgiou,
Prevalence and Types of Pitfall in the Assessment of Mitral Isthmus Linear. Conduction Block
 Prevalence and Types of Pitfall in the Assessment of Mitral Isthmus Linear Conduction Block Running title: Shah et al.; Pitfall in Assessment of Mitral Line Block Downloaded from http://circep.ahajournals.org/
Prevalence and Types of Pitfall in the Assessment of Mitral Isthmus Linear Conduction Block Running title: Shah et al.; Pitfall in Assessment of Mitral Line Block Downloaded from http://circep.ahajournals.org/
Catheter ablation of scar-related atypical atrial flutter
 Europace (2013) 15, 414 419 doi:10.1093/europace/eus312 CLINICAL RESEARCH Electrophysiology and ablation Catheter ablation of scar-related atypical atrial flutter James O. Coffey 1, Andre d Avila 1, Srinivas
Europace (2013) 15, 414 419 doi:10.1093/europace/eus312 CLINICAL RESEARCH Electrophysiology and ablation Catheter ablation of scar-related atypical atrial flutter James O. Coffey 1, Andre d Avila 1, Srinivas
Radiofrequency ablation for atrial fibrillation
 European Heart Journal Supplements (2003) 5 (Supplement H), H34 H39 Radiofrequency ablation for atrial fibrillation P. Jaïs 1, D.C. Shah 2, M. Hocini 1, L. Macle 1, K. J. Choi 1, M. Haïssaguerre 1 and
European Heart Journal Supplements (2003) 5 (Supplement H), H34 H39 Radiofrequency ablation for atrial fibrillation P. Jaïs 1, D.C. Shah 2, M. Hocini 1, L. Macle 1, K. J. Choi 1, M. Haïssaguerre 1 and
Catheter ablation of atrial macro re-entrant Tachycardia - How to use 3D entrainment mapping -
 Catheter ablation of atrial macro re-entrant Tachycardia - How to use 3D entrainment mapping - M. Esato, Y. Chun, G. Hindricks Kyoto Ijinkai Takeda Hosptial, Department of Arrhythmia, Japan Kyoto Koseikai
Catheter ablation of atrial macro re-entrant Tachycardia - How to use 3D entrainment mapping - M. Esato, Y. Chun, G. Hindricks Kyoto Ijinkai Takeda Hosptial, Department of Arrhythmia, Japan Kyoto Koseikai
How to Ablate Atrial Tachycardia Mechanisms and Approach. DrJo Jo Hai
 How to Ablate Atrial Tachycardia Mechanisms and Approach DrJo Jo Hai Contents Mechanisms of focal atrial tachycardia Various mapping techniques Detailed discussion on activation sequence mapping and entrainment
How to Ablate Atrial Tachycardia Mechanisms and Approach DrJo Jo Hai Contents Mechanisms of focal atrial tachycardia Various mapping techniques Detailed discussion on activation sequence mapping and entrainment
Atrial fibrillation (AF) is the most common arrhythmia in
 is the most common arrhythmia in") Distinctive Electrophysiological Properties of Pulmonary Veins in Patients With Atrial Fibrillation Pierre Jaïs, MD; Mélèze Hocini, MD; Laurent Macle, MD; Kee-Joon Choi, MD; Isabel Deisenhofer, MD; Rukshen
Distinctive Electrophysiological Properties of Pulmonary Veins in Patients With Atrial Fibrillation Pierre Jaïs, MD; Mélèze Hocini, MD; Laurent Macle, MD; Kee-Joon Choi, MD; Isabel Deisenhofer, MD; Rukshen
Electrophysiological Characteristics of Atrial Tachycardia After Pulmonary Vein Isolation of Atrial Fibrillation
 Circulation Journal Official Journal of the Japanese Circulation Society http://www.j-circ.or.jp Advance Publication by J-STAGE REVIEW Electrophysiological Characteristics of Atrial Tachycardia After Pulmonary
Circulation Journal Official Journal of the Japanese Circulation Society http://www.j-circ.or.jp Advance Publication by J-STAGE REVIEW Electrophysiological Characteristics of Atrial Tachycardia After Pulmonary
Case Report What Next After Failed Septal Ventricular Tachycardia Ablation?
 www.ipej.org 180 Case Report What Next After Failed Septal Ventricular Tachycardia Ablation? Laurent Roten, MD 1, Nicolas Derval, MD 1, Patrizio Pascale, MD 1, Pierre Jais, MD 1, Pierre Coste, MD 2, Frederic
www.ipej.org 180 Case Report What Next After Failed Septal Ventricular Tachycardia Ablation? Laurent Roten, MD 1, Nicolas Derval, MD 1, Patrizio Pascale, MD 1, Pierre Jais, MD 1, Pierre Coste, MD 2, Frederic
Conventional Mapping. Introduction
 Conventional Mapping Haitham Badran Ain Shams University it Introduction The mapping approach used to guide ablation depends on the type of arrhythmia being assessed. Simple fluoroscopic anatomy is essential
Conventional Mapping Haitham Badran Ain Shams University it Introduction The mapping approach used to guide ablation depends on the type of arrhythmia being assessed. Simple fluoroscopic anatomy is essential
Time to Cardioversion of Recurrent Atrial Arrhythmias After Catheter Ablation of Atrial Fibrillation and Long-Term Clinical Outcome
 Time to Cardioversion of Recurrent Atrial Arrhythmias After Catheter Ablation of Atrial Fibrillation and Long-Term Clinical Outcome TIMIR S. BAMAN, M.D., SANJAYA K. GUPTA, M.D., SREEDHAR R. BILLAKANTY,
Time to Cardioversion of Recurrent Atrial Arrhythmias After Catheter Ablation of Atrial Fibrillation and Long-Term Clinical Outcome TIMIR S. BAMAN, M.D., SANJAYA K. GUPTA, M.D., SREEDHAR R. BILLAKANTY,
EHRA Accreditation Exam - Sample MCQs Invasive cardiac electrophysiology
 EHRA Accreditation Exam - Sample MCQs Invasive cardiac electrophysiology Dear EHRA Member, Dear Colleague, As you know, the EHRA Accreditation Process is becoming increasingly recognised as an important
EHRA Accreditation Exam - Sample MCQs Invasive cardiac electrophysiology Dear EHRA Member, Dear Colleague, As you know, the EHRA Accreditation Process is becoming increasingly recognised as an important
A New Approach for Catheter Ablation of Atrial Fibrillation: Mapping of the Electrophysiologic Substrate
 Journal of the American College of Cardiology Vol. 43, No. 11, 2004 2004 by the American College of Cardiology Foundation ISSN 0735-1097/04/$30.00 Published by Elsevier Inc. doi:10.1016/j.jacc.2003.12.054
Journal of the American College of Cardiology Vol. 43, No. 11, 2004 2004 by the American College of Cardiology Foundation ISSN 0735-1097/04/$30.00 Published by Elsevier Inc. doi:10.1016/j.jacc.2003.12.054
Case Report Successful Multi-chamber Catheter Ablation of Persistent Atrial Fibrillation in Cor Triatriatum Sinister
 www.ipej.org 50 Case Report Successful Multi-chamber Catheter Ablation of Persistent Atrial Fibrillation in Cor Triatriatum Sinister Andrew Gavin, MBChB 1, Cameron B Singleton, MD 1, Andrew D McGavigan,
www.ipej.org 50 Case Report Successful Multi-chamber Catheter Ablation of Persistent Atrial Fibrillation in Cor Triatriatum Sinister Andrew Gavin, MBChB 1, Cameron B Singleton, MD 1, Andrew D McGavigan,
Journal of the American College of Cardiology Vol. 33, No. 7, by the American College of Cardiology ISSN /99/$20.
 Journal of the American College of Cardiology Vol. 33, No. 7, 1999 1999 by the American College of Cardiology ISSN 0735-1097/99/$20.00 Published by Elsevier Science Inc. PII S0735-1097(99)00117-5 Partial
Journal of the American College of Cardiology Vol. 33, No. 7, 1999 1999 by the American College of Cardiology ISSN 0735-1097/99/$20.00 Published by Elsevier Science Inc. PII S0735-1097(99)00117-5 Partial
Integration of CT and fluoroscopy images in the ablative treatment of atrial fibrillation
 Clinical applications Integration of CT and fluoroscopy images in the ablative treatment of atrial fibrillation C. Kriatselis M. Tang M. Roser J-H. erds-li E. leck Department of Internal Medicine/Cardiology,
Clinical applications Integration of CT and fluoroscopy images in the ablative treatment of atrial fibrillation C. Kriatselis M. Tang M. Roser J-H. erds-li E. leck Department of Internal Medicine/Cardiology,
Catheter Ablation of a Complex Atrial Tachycardia after Surgical Repair of Tetralogy of Fallot Guided by Combined Noncontact and Contact Mapping
 J Arrhythmia Vol 26 No 1 2010 Case Report Catheter Ablation of a Complex Atrial Tachycardia after Surgical Repair of Tetralogy of Fallot Guided by Combined Noncontact and Contact Mapping Eitaro Fujii MD,
J Arrhythmia Vol 26 No 1 2010 Case Report Catheter Ablation of a Complex Atrial Tachycardia after Surgical Repair of Tetralogy of Fallot Guided by Combined Noncontact and Contact Mapping Eitaro Fujii MD,
Linear Ablation Should Not Be a Standard Part of Ablation in Persistent AF. Disclosures. LA Ablation vs. Segmental Ostial Ablation With PVI for PAF
 Linear Ablation Should Not Be a Standard Part of Ablation in Persistent AF The CA Heart Rhythm Symposium September 7, 2012 Gregory K. Feld, MD Professor of Medicine Director, Cardiac EP Program University
Linear Ablation Should Not Be a Standard Part of Ablation in Persistent AF The CA Heart Rhythm Symposium September 7, 2012 Gregory K. Feld, MD Professor of Medicine Director, Cardiac EP Program University
Right and Left Atrial Flutter: How To Differentiate Them on the Basis of Surface Electrocardiogram?
 Right and Left Atrial Flutter: How To Differentiate Them on the Basis of Surface Electrocardiogram? G. INAMA, C. PEDRINAZZI,O.DURIN,P.GAZZANIGA,P.AGRICOLA Introduction Atrial flutter is a common arrhythmia
Right and Left Atrial Flutter: How To Differentiate Them on the Basis of Surface Electrocardiogram? G. INAMA, C. PEDRINAZZI,O.DURIN,P.GAZZANIGA,P.AGRICOLA Introduction Atrial flutter is a common arrhythmia
Author s Accepted Manuscript
 Author s Accepted Manuscript Cavo-tricuspid isthmus high density mapping Antonio De Simone, Vincenzo La Rocca, Francesco Solimene, Francesco Maddaluno, Maurizio Malacrida, Giuseppe Stabile www.elsevier.com/locate/buildenv
Author s Accepted Manuscript Cavo-tricuspid isthmus high density mapping Antonio De Simone, Vincenzo La Rocca, Francesco Solimene, Francesco Maddaluno, Maurizio Malacrida, Giuseppe Stabile www.elsevier.com/locate/buildenv
Evidence for Longitudinal and Transverse Fiber Conduction in Human Pulmonary Veins
 Evidence for Longitudinal and Transverse Fiber Conduction in Human Pulmonary Veins Relevance for Catheter Ablation Javier E. Sanchez, MD; Vance J. Plumb, MD; Andrew E. Epstein, MD; G. Neal Kay, MD Background
Evidence for Longitudinal and Transverse Fiber Conduction in Human Pulmonary Veins Relevance for Catheter Ablation Javier E. Sanchez, MD; Vance J. Plumb, MD; Andrew E. Epstein, MD; G. Neal Kay, MD Background
LONG RP TACHYCARDIA MAPPING AND RF ABLATION
 LONG RP TACHYCARDIA MAPPING AND RF ABLATION Dr. Hayam Eldamanhoury Ain shams univeristy Arrhythmia is a too broad topic SVT is broadly defined as narrow complex ( unless aberrant conduction ) Requires
LONG RP TACHYCARDIA MAPPING AND RF ABLATION Dr. Hayam Eldamanhoury Ain shams univeristy Arrhythmia is a too broad topic SVT is broadly defined as narrow complex ( unless aberrant conduction ) Requires
Characteristics of systolic and diastolic potentials recorded in the left interventricular septum in verapamil-sensitive left ventricular tachycardia
 CASE REPORT Cardiology Journal 2012, Vol. 19, No. 4, pp. 418 423 10.5603/CJ.2012.0075 Copyright 2012 Via Medica ISSN 1897 5593 Characteristics of systolic and diastolic potentials recorded in the left
CASE REPORT Cardiology Journal 2012, Vol. 19, No. 4, pp. 418 423 10.5603/CJ.2012.0075 Copyright 2012 Via Medica ISSN 1897 5593 Characteristics of systolic and diastolic potentials recorded in the left
Circulation: Arrhythmia and Electrophysiology CHALLENGE OF THE WEEK
 A 14-year-old girl with Wolff-Parkinson-White syndrome and recurrent paroxysmal palpitations due to atrioventricular reentry tachycardia had undergone two prior failed left lateral accessory pathway ablations
A 14-year-old girl with Wolff-Parkinson-White syndrome and recurrent paroxysmal palpitations due to atrioventricular reentry tachycardia had undergone two prior failed left lateral accessory pathway ablations
Lower loop reentry is defined as macroreentrant
 Lower Loop Reentry as a Mechanism of Clockwise Right Atrial Flutter Shulong Zhang, MD; George Younis, MD; Ramesh Hariharan, MD; John Ho, MD; Yanfei Yang, MD; John Ip, MD; Ranjun K. Thakur, MD; John Seger,
Lower Loop Reentry as a Mechanism of Clockwise Right Atrial Flutter Shulong Zhang, MD; George Younis, MD; Ramesh Hariharan, MD; John Ho, MD; Yanfei Yang, MD; John Ip, MD; Ranjun K. Thakur, MD; John Seger,
Two recent studies assessed the efficacy of radiofrequency. Original Articles
 Original Articles Randomized Evaluation of Right Atrial Ablation After Left Atrial Ablation of Complex Fractionated Atrial Electrograms for Long-Lasting Persistent Atrial Fibrillation Hakan Oral, MD; Aman
Original Articles Randomized Evaluation of Right Atrial Ablation After Left Atrial Ablation of Complex Fractionated Atrial Electrograms for Long-Lasting Persistent Atrial Fibrillation Hakan Oral, MD; Aman
Atrial Tachycardia During Ongoing Atrial Fibrillation Ablation
 Circulation Journal Official Journal of the Japanese Circulation Society http://www.j-circ.or.jp Advance Publication by J-STAGE Atrial Tachycardia During Ongoing Atrial Fibrillation Ablation EnSite Array
Circulation Journal Official Journal of the Japanese Circulation Society http://www.j-circ.or.jp Advance Publication by J-STAGE Atrial Tachycardia During Ongoing Atrial Fibrillation Ablation EnSite Array
Impact of Atrial Fibrillation Termination Site and Termination Mode in Catheter Ablation on Arrhythmia Recurrence
 78 MIYAZAKI S et al. Circulation Journal ORIGINAL ARTICLE Official Journal of the Japanese Circulation Society http://www.j-circ.or.jp Arrhythmia/Electrophysiology Impact of Atrial Fibrillation Termination
78 MIYAZAKI S et al. Circulation Journal ORIGINAL ARTICLE Official Journal of the Japanese Circulation Society http://www.j-circ.or.jp Arrhythmia/Electrophysiology Impact of Atrial Fibrillation Termination
Typical right atrial (RA) flutter in humans exemplifies the
 flutter in humans exemplifies the") Dual-Loop Intra-Atrial Reentry in Humans Dipen Shah, MD; Pierre Jaïs, MD; Atsushi Takahashi, MD; Meleze Hocini, MD; Jing Tian Peng, MD; Jacques Clementy, MD; Michel Haïssaguerre, MD Background Dual-loop
Dual-Loop Intra-Atrial Reentry in Humans Dipen Shah, MD; Pierre Jaïs, MD; Atsushi Takahashi, MD; Meleze Hocini, MD; Jing Tian Peng, MD; Jacques Clementy, MD; Michel Haïssaguerre, MD Background Dual-loop
Spontaneous clockwise (CW) and counterclockwise
 and counterclockwise") Atypical Right Atrial Flutter Patterns Yanfei Yang, MD; Jie Cheng, MD, PhD; Andy Bochoeyer, MD; Mohamed H. Hamdan, MD; Robert C. Kowal, MD, PhD; Richard Page, MD; Randall J. Lee, MD, PhD; Paul R. Steiner,
Atypical Right Atrial Flutter Patterns Yanfei Yang, MD; Jie Cheng, MD, PhD; Andy Bochoeyer, MD; Mohamed H. Hamdan, MD; Robert C. Kowal, MD, PhD; Richard Page, MD; Randall J. Lee, MD, PhD; Paul R. Steiner,
Ankara, Turkey 2 Department of Cardiology, Division of Arrhythmia and Electrophysiology, Yuksek Ihtisas
 258 Case Report Electroanatomic Mapping-Guided Radiofrequency Ablation of Adenosine Sensitive Incessant Focal Atrial Tachycardia Originating from the Non-Coronary Aortic Cusp in a Child Serhat Koca, MD
258 Case Report Electroanatomic Mapping-Guided Radiofrequency Ablation of Adenosine Sensitive Incessant Focal Atrial Tachycardia Originating from the Non-Coronary Aortic Cusp in a Child Serhat Koca, MD
Noninducibility of Atrial Fibrillation as an End Point of Left Atrial Circumferential Ablation for Paroxysmal Atrial Fibrillation A Randomized Study
 Noninducibility of Atrial Fibrillation as an End Point of Left Atrial Circumferential Ablation for Paroxysmal Atrial Fibrillation A Randomized Study Hakan Oral, MD; Aman Chugh, MD; Kristina Lemola, MD;
Noninducibility of Atrial Fibrillation as an End Point of Left Atrial Circumferential Ablation for Paroxysmal Atrial Fibrillation A Randomized Study Hakan Oral, MD; Aman Chugh, MD; Kristina Lemola, MD;
Surgical or catheter ablation of atrial fibrillation (AF) is an
 is an") Atrial Tachycardia After Ablation of Persistent Atrial Fibrillation Identification of the Critical Isthmus With a Combination of Multielectrode Activation Mapping and Targeted Entrainment Mapping Anshul
Atrial Tachycardia After Ablation of Persistent Atrial Fibrillation Identification of the Critical Isthmus With a Combination of Multielectrode Activation Mapping and Targeted Entrainment Mapping Anshul
Defin. Mapping & RF-ablation of Atrial Flutter 10/27/2013
 Mapping & RF-ablation of Atrial Flutter By Dr. Rania Samir Assistant Professor of Cardiology Ain Shams University Defin. Atrial flutter is a macro-reentrant AT characterized by a regular rate 200-350 bpm,
Mapping & RF-ablation of Atrial Flutter By Dr. Rania Samir Assistant Professor of Cardiology Ain Shams University Defin. Atrial flutter is a macro-reentrant AT characterized by a regular rate 200-350 bpm,
Mapping techniques in AFib. Helmut Pürerfellner, MD Public Hospital Elisabethinen Academic Teaching Hospital Linz, Austria
 Mapping techniques in AFib Helmut Pürerfellner, MD Public Hospital Elisabethinen Academic Teaching Hospital Linz, Austria critical zone Microreeentrant circuits LOM PV foci Sueda Ann Thorac Surg 1997 Haissaguerre
Mapping techniques in AFib Helmut Pürerfellner, MD Public Hospital Elisabethinen Academic Teaching Hospital Linz, Austria critical zone Microreeentrant circuits LOM PV foci Sueda Ann Thorac Surg 1997 Haissaguerre
KENTARO YOSHIDA, M.D., MAGNUS ULFARSSON, PH.D.,
 Complex Electrograms Within the Coronary Sinus: Time- and Frequency-Domain Characteristics, Effects of Antral Pulmonary Vein Isolation, and Relationship to Clinical Outcome in Patients with Paroxysmal
Complex Electrograms Within the Coronary Sinus: Time- and Frequency-Domain Characteristics, Effects of Antral Pulmonary Vein Isolation, and Relationship to Clinical Outcome in Patients with Paroxysmal
Although circumferential pulmonary vein ablation
 Circumferential Pulmonary Vein Ablation With Additional Linear Ablation Results in an Increased Incidence of Left Atrial Flutter Compared With Segmental Pulmonary Vein Isolation as an Initial Approach
Circumferential Pulmonary Vein Ablation With Additional Linear Ablation Results in an Increased Incidence of Left Atrial Flutter Compared With Segmental Pulmonary Vein Isolation as an Initial Approach
The pulmonary veins have been demonstrated to often
 Pulmonary Vein Isolation for Paroxysmal and Persistent Atrial Fibrillation Hakan Oral, MD; Bradley P. Knight, MD; Hiroshi Tada, MD; Mehmet Özaydın, MD; Aman Chugh, MD; Sohail Hassan, MD; Christoph Scharf,
Pulmonary Vein Isolation for Paroxysmal and Persistent Atrial Fibrillation Hakan Oral, MD; Bradley P. Knight, MD; Hiroshi Tada, MD; Mehmet Özaydın, MD; Aman Chugh, MD; Sohail Hassan, MD; Christoph Scharf,
Topographic Distribution of Focal Left Atrial Tachycardias Defined by Electrocardiographic and Electrophysiological Data
 Circ J 2005; 69: 205 210 Topographic Distribution of Focal Left Atrial Tachycardias Defined by Electrocardiographic and Electrophysiological Data Hitoshi Hachiya, MD; Sabine Ernst, MD; Feifan Ouyang, MD;
Circ J 2005; 69: 205 210 Topographic Distribution of Focal Left Atrial Tachycardias Defined by Electrocardiographic and Electrophysiological Data Hitoshi Hachiya, MD; Sabine Ernst, MD; Feifan Ouyang, MD;
Ablation of Ventricular Tachycardia in Non-Ischemic Cardiomyopathy
 Ablation of Ventricular Tachycardia in Non-Ischemic Cardiomyopathy Fermin C Garcia, MD University of Pennsylvania Cardiac Electrophysiology Philadelphia, PA Nothing to disclose No conflict of interest
Ablation of Ventricular Tachycardia in Non-Ischemic Cardiomyopathy Fermin C Garcia, MD University of Pennsylvania Cardiac Electrophysiology Philadelphia, PA Nothing to disclose No conflict of interest
Catheter Ablation of Supraventricular Arrhythmias: State of the Art
 124 NASPE 25TH ANNIVERSARY SERIES Catheter Ablation of Supraventricular Arrhythmias: State of the Art FRED MORADY, M.D. From the Division of Cardiology, Department of Medicine, University of Michigan,
124 NASPE 25TH ANNIVERSARY SERIES Catheter Ablation of Supraventricular Arrhythmias: State of the Art FRED MORADY, M.D. From the Division of Cardiology, Department of Medicine, University of Michigan,
Catheter ablation in AF patients with heart failure. What is possible?
 Catheter ablation in AF patients with heart failure What is possible? Sébastien Knecht, MD PhD Hôpital cardiologique du Haut L Evêque, Bordeaux HEART FAILURE AND AF Ehrlich. JCE 2002 (13): 399-405, Wang
Catheter ablation in AF patients with heart failure What is possible? Sébastien Knecht, MD PhD Hôpital cardiologique du Haut L Evêque, Bordeaux HEART FAILURE AND AF Ehrlich. JCE 2002 (13): 399-405, Wang
Catheter ablation of atrial fibrillation: Indications and tools for improvement of the success rate of the method. Konstantinos P.
 Ioannina 2015 Catheter ablation of atrial fibrillation: Indications and tools for improvement of the success rate of the method Konstantinos P. Letsas, MD, FESC SECOND DEPARTMENT OF CARDIOLOGY LABORATORY
Ioannina 2015 Catheter ablation of atrial fibrillation: Indications and tools for improvement of the success rate of the method Konstantinos P. Letsas, MD, FESC SECOND DEPARTMENT OF CARDIOLOGY LABORATORY
Accepted Manuscript. Inadvertent Atrial Dissociation Following Catheter Ablation: A Demonstration of Cardiac Anisotropy and Functional Block
 Accepted Manuscript Inadvertent Atrial Dissociation Following Catheter Ablation: A Demonstration of Cardiac Anisotropy and Functional Block Shashank Jain, MD, Sajid Mirza, MD, Gunjan Shukla, MD, FHRS PII:
Accepted Manuscript Inadvertent Atrial Dissociation Following Catheter Ablation: A Demonstration of Cardiac Anisotropy and Functional Block Shashank Jain, MD, Sajid Mirza, MD, Gunjan Shukla, MD, FHRS PII:
Surgical or catheter ablation of atrial fibrillation (AF) is an
 is an") Atrial Tachycardia After Ablation of Persistent Atrial Fibrillation Identification of the Critical Isthmus With a Combination of Multielectrode Activation Mapping and Targeted Entrainment Mapping Anshul
Atrial Tachycardia After Ablation of Persistent Atrial Fibrillation Identification of the Critical Isthmus With a Combination of Multielectrode Activation Mapping and Targeted Entrainment Mapping Anshul
Atrial fibrillation (AF) is the most common sustained
 is the most common sustained") Chronic Atrial Fibrillation in Patients With Rheumatic Heart Disease Mapping and Radiofrequency Ablation of Flutter Circuits Seen at Initiation After Cardioversion Mohan Nair, MD; Prasad Shah, MD; Ravinder
Chronic Atrial Fibrillation in Patients With Rheumatic Heart Disease Mapping and Radiofrequency Ablation of Flutter Circuits Seen at Initiation After Cardioversion Mohan Nair, MD; Prasad Shah, MD; Ravinder
High density substrate mapping In AF
 High density substrate mapping In AF A Pisapia J Seitz C Bars M Bremondy A Ferracci * J Khalifa ** * St Joseph Hospital Marseille ** Ann Arbor University Turin 2016 Hôpital Saint Joseph Marseille jseitz@hopital-saint-joseph.fr
High density substrate mapping In AF A Pisapia J Seitz C Bars M Bremondy A Ferracci * J Khalifa ** * St Joseph Hospital Marseille ** Ann Arbor University Turin 2016 Hôpital Saint Joseph Marseille jseitz@hopital-saint-joseph.fr
Overview of Atrial Flutter
 Overview of Atrial Flutter Samsung Medical Center Lee, Chang Hee Atrial Flutter A macro-reentrant reentrant atrial arrhythmia that is very regular with rates typically between 240 and 350 bpm. Demographics
Overview of Atrial Flutter Samsung Medical Center Lee, Chang Hee Atrial Flutter A macro-reentrant reentrant atrial arrhythmia that is very regular with rates typically between 240 and 350 bpm. Demographics
Ablation of atypical atrial flutters using ultra high density-activation sequence mapping
 J Interv Card Electrophysiol (2017) 48:177 184 DOI 10.1007/s10840-016-0207-5 MULTIMEDIA REPORT Ablation of atypical atrial flutters using ultra high density-activation sequence mapping Roger A. Winkle
J Interv Card Electrophysiol (2017) 48:177 184 DOI 10.1007/s10840-016-0207-5 MULTIMEDIA REPORT Ablation of atypical atrial flutters using ultra high density-activation sequence mapping Roger A. Winkle
Debate-STAR AF 2 study. PVI is not enough
 Debate-STAR AF 2 study PVI is not enough Debate about STAR AF 2 trial STAR AF trial Substrate and Trigger Ablation for Reduction of Atrial Fibrillation EHJ 2010 STAR-AF 2 trial One Size Fits All? PVI is
Debate-STAR AF 2 study PVI is not enough Debate about STAR AF 2 trial STAR AF trial Substrate and Trigger Ablation for Reduction of Atrial Fibrillation EHJ 2010 STAR-AF 2 trial One Size Fits All? PVI is
Catheter-Induced Linear Lesions in the Left Atrium in Patients With Atrial Fibrillation An Electroanatomic Study
 Journal of the American College of Cardiology Vol. 42, No. 7, 2003 2003 by the American College of Cardiology Foundation ISSN 0735-1097/03/$30.00 Published by Elsevier Inc. doi:10.1016/s0735-1097(03)00940-9
Journal of the American College of Cardiology Vol. 42, No. 7, 2003 2003 by the American College of Cardiology Foundation ISSN 0735-1097/03/$30.00 Published by Elsevier Inc. doi:10.1016/s0735-1097(03)00940-9
Catheter ablation of persistent AF: integrating advanced imaging and mapping solutions
 Investigations and research Catheter ablation of persistent AF: integrating advanced imaging and mapping solutions M. Wright R. Bullens M. Haïssaguerre P. Jaïs O. Leonard M. O Neill Hôpital Cardiologique
Investigations and research Catheter ablation of persistent AF: integrating advanced imaging and mapping solutions M. Wright R. Bullens M. Haïssaguerre P. Jaïs O. Leonard M. O Neill Hôpital Cardiologique
Basic Electrophysiology Protocols
 Indian Journal of Cardiology ISSN-0972-1622 2012 by the Indian Society of Cardiology Vol. 15, (3-4), 27-37 [ 27 Review Article Shomu Bohora Assistant Professor, Deptt. of Cardiology, U.N. Mehta Institute
Indian Journal of Cardiology ISSN-0972-1622 2012 by the Indian Society of Cardiology Vol. 15, (3-4), 27-37 [ 27 Review Article Shomu Bohora Assistant Professor, Deptt. of Cardiology, U.N. Mehta Institute
Raphael Rosso MD, Yuval Levi Med. Eng., Sami Viskin MD Tel Aviv Sourasky Medical Center
 Radiofrequency Ablation of Atrial Fibrillation: Comparison of Success Rate of Circular Ablation vs Point-by-Point Ablation with Contact Force Assessment in Paroxysmal and Persistent Atrial Fibrillation
Radiofrequency Ablation of Atrial Fibrillation: Comparison of Success Rate of Circular Ablation vs Point-by-Point Ablation with Contact Force Assessment in Paroxysmal and Persistent Atrial Fibrillation
Over the past few decades, continuous improvement of
 Catheter Ablation of Typical Atrial Flutter A Randomized Comparison of 2 Methods for Determining Complete Bidirectional Isthmus Block Frédéric Anselme, MD; Arnaud Savouré, MD; Alain Cribier, MD; Nadir
Catheter Ablation of Typical Atrial Flutter A Randomized Comparison of 2 Methods for Determining Complete Bidirectional Isthmus Block Frédéric Anselme, MD; Arnaud Savouré, MD; Alain Cribier, MD; Nadir
Atrial Fibrillation: Electrophysiological Mechanisms and the Results of Interventional Therapy
 Vol. 8, No. 3, September 2003 185 Atrial Fibrillation: Electrophysiological Mechanisms and the Results of Interventional Therapy A.SH. REVISHVILI Bakoulev Research Centre for Cardiovascular Surgery, Russian
Vol. 8, No. 3, September 2003 185 Atrial Fibrillation: Electrophysiological Mechanisms and the Results of Interventional Therapy A.SH. REVISHVILI Bakoulev Research Centre for Cardiovascular Surgery, Russian
The pulmonary veins (PVs) have been shown to trigger
 have been shown to trigger") Electrophysiological End Point for Catheter Ablation of Atrial Fibrillation Initiated From Multiple Pulmonary Venous Foci Michel Haïssaguerre, MD; Pierre Jaïs, MD; Dipen C. Shah, MD; Stéphane Garrigue,
Electrophysiological End Point for Catheter Ablation of Atrial Fibrillation Initiated From Multiple Pulmonary Venous Foci Michel Haïssaguerre, MD; Pierre Jaïs, MD; Dipen C. Shah, MD; Stéphane Garrigue,
Arrhythmia/Electrophysiology
 Arrhythmia/Electrophysiology Electrophysiological Findings During Ablation of Persistent Atrial Fibrillation With Electroanatomic Mapping and Double Lasso Catheter Technique Feifan Ouyang, MD; Sabine Ernst,
Arrhythmia/Electrophysiology Electrophysiological Findings During Ablation of Persistent Atrial Fibrillation With Electroanatomic Mapping and Double Lasso Catheter Technique Feifan Ouyang, MD; Sabine Ernst,
2017 HRS/EHRA/ECAS/APHRS/SOLAECE Expert Consensus Statement on Catheter and Surgical Ablation of Atrial Fibrillation
 Summary of Expert Consensus Statement for CLINICIANS 2017 HRS/EHRA/ECAS/APHRS/SOLAECE Expert Consensus Statement on Catheter and Surgical Ablation of Atrial Fibrillation This is a summary of the Heart
Summary of Expert Consensus Statement for CLINICIANS 2017 HRS/EHRA/ECAS/APHRS/SOLAECE Expert Consensus Statement on Catheter and Surgical Ablation of Atrial Fibrillation This is a summary of the Heart
Case 1 Left Atrial Tachycardia
 Case 1 Left Atrial Tachycardia A 16 years old woman was referred to our institution because of recurrent episodes of palpitations and dizziness despite previous ablation procedure( 13 years ago) of postero-septal
Case 1 Left Atrial Tachycardia A 16 years old woman was referred to our institution because of recurrent episodes of palpitations and dizziness despite previous ablation procedure( 13 years ago) of postero-septal
Tachy. Induction tachycardia lead ECG during Tachy /25/2009. Sinus Rhythm Single His
 12-lead ECG during Tachy 10.30.31 Sinus Rhythm Single His 11.20.02 Induction tachycardia 11.23.23 Tachy 11.25.23 1 I This finding excludes: (a) AVNRT (either typical or atypical) Tachy: Alternating cycle
12-lead ECG during Tachy 10.30.31 Sinus Rhythm Single His 11.20.02 Induction tachycardia 11.23.23 Tachy 11.25.23 1 I This finding excludes: (a) AVNRT (either typical or atypical) Tachy: Alternating cycle
Voltage-directed Cavo-tricuspid Isthmus Ablation using Novel Ablation Catheter Mapping Technology
 The Journal of Innovations in Cardiac Rhythm Management, 6 (2015), 1908 1912 INNOVATIVE TECHNIQUES RESEARCH ARTICLE Voltage-directed Cavo-tricuspid Isthmus Ablation using Novel Ablation Catheter Mapping
The Journal of Innovations in Cardiac Rhythm Management, 6 (2015), 1908 1912 INNOVATIVE TECHNIQUES RESEARCH ARTICLE Voltage-directed Cavo-tricuspid Isthmus Ablation using Novel Ablation Catheter Mapping
Case Report Figure-8 Tachycardia Confined to the Anterior Wall of the Left Atrium
 www.ipej.org 146 Case Report Figure-8 Tachycardia Confined to the Anterior Wall of the Left Atrium Ioan Liuba, M.D., Anders Jönsson, M.D., Håkan Walfridsson, M.D. Department of Cardiology, Heartcenter,
www.ipej.org 146 Case Report Figure-8 Tachycardia Confined to the Anterior Wall of the Left Atrium Ioan Liuba, M.D., Anders Jönsson, M.D., Håkan Walfridsson, M.D. Department of Cardiology, Heartcenter,
The characteristic anatomic distribution for focal atrial
 Electrophysiological and Electrocardiographic Characteristics of Focal Atrial Tachycardia Originating From the Pulmonary Veins Acute and Long-Term Outcomes of Radiofrequency Ablation Peter M. Kistler,
Electrophysiological and Electrocardiographic Characteristics of Focal Atrial Tachycardia Originating From the Pulmonary Veins Acute and Long-Term Outcomes of Radiofrequency Ablation Peter M. Kistler,
Trigger Activity More Than Three Years After Left Atrial Linear Ablation Without Pulmonary Vein Isolation in Patients With Atrial Fibrillation
 Journal of the American College of Cardiology Vol. 46, No. 2, 2005 2005 by the American College of Cardiology Foundation ISSN 0735-1097/05/$30.00 Published by Elsevier Inc. doi:10.1016/j.jacc.2005.03.063
Journal of the American College of Cardiology Vol. 46, No. 2, 2005 2005 by the American College of Cardiology Foundation ISSN 0735-1097/05/$30.00 Published by Elsevier Inc. doi:10.1016/j.jacc.2005.03.063
Journal of the American College of Cardiology Vol. 45, No. 9, by the American College of Cardiology Foundation ISSN /05/$30.
 Journal of the American College of Cardiology Vol. 45, No. 9, 2005 2005 by the American College of Cardiology Foundation ISSN 0735-1097/05/$30.00 Published by Elsevier Inc. doi:10.1016/j.jacc.2005.01.042
Journal of the American College of Cardiology Vol. 45, No. 9, 2005 2005 by the American College of Cardiology Foundation ISSN 0735-1097/05/$30.00 Published by Elsevier Inc. doi:10.1016/j.jacc.2005.01.042
Functional Nature of Electrogram Fractionation Demonstrated by Left Atrial High Density Mapping
 Functional Nature of Electrogram Fractionation Demonstrated by Left Atrial High Density Mapping Running title: Jadidi et al.; Functional Nature of CFAE Downloaded from http://circep.ahajournals.org/ by
Functional Nature of Electrogram Fractionation Demonstrated by Left Atrial High Density Mapping Running title: Jadidi et al.; Functional Nature of CFAE Downloaded from http://circep.ahajournals.org/ by
Electrical and Mechanical Insights of Human Atrial Fibrillation. Sághy László, MD. Summary of PhD Thesis
 Electrical and Mechanical Insights of Human Atrial Fibrillation Sághy László, MD Summary of PhD Thesis Second Department of Medicine and Cardiology Center, University of Szeged Szeged 2012 Introduction
Electrical and Mechanical Insights of Human Atrial Fibrillation Sághy László, MD Summary of PhD Thesis Second Department of Medicine and Cardiology Center, University of Szeged Szeged 2012 Introduction
Title. CitationJournal of Electrocardiology, 43(5): Issue Date Doc URL. Type. File Information.
: Issue Date Doc URL. Type. File Information.") Title Pleomorphic ventricular tachycardia originating from Author(s)Yokoshiki, Hisashi; Mitsuyama, Hirofumi; Watanabe, M CitationJournal of Electrocardiology, 43(5): 452-458 Issue Date 2010-09 Doc URL
Title Pleomorphic ventricular tachycardia originating from Author(s)Yokoshiki, Hisashi; Mitsuyama, Hirofumi; Watanabe, M CitationJournal of Electrocardiology, 43(5): 452-458 Issue Date 2010-09 Doc URL
Catheter Ablation of Atrial Fibrillation in Patients with Prosthetic Mitral Valve
 Catheter Ablation of Atrial Fibrillation in Patients with Prosthetic Mitral Valve Luigi Di Biase, MD, PhD, FHRS Senior Researcher Texas Cardiac Arrhythmia Institute at St. David s Medical Center, Austin,
Catheter Ablation of Atrial Fibrillation in Patients with Prosthetic Mitral Valve Luigi Di Biase, MD, PhD, FHRS Senior Researcher Texas Cardiac Arrhythmia Institute at St. David s Medical Center, Austin,
Circumferential Pulmonary-Vein Ablation for Chronic Atrial Fibrillation
 The new england journal of medicine original article Circumferential Pulmonary-Vein Ablation for Chronic Atrial Fibrillation Hakan Oral, M.D., Carlo Pappone, M.D., Aman Chugh, M.D., Eric Good, D.O., Frank
The new england journal of medicine original article Circumferential Pulmonary-Vein Ablation for Chronic Atrial Fibrillation Hakan Oral, M.D., Carlo Pappone, M.D., Aman Chugh, M.D., Eric Good, D.O., Frank
Mechanism of Ventricular Tachycardia Termination by Pacing at Left Ventricular Sites in Patients with Coronary Artery Disease
 Journal of Interventional Cardiac Electrophysiology 6, 35 41, 2002 C 2002 Kluwer Academic Publishers. Manufactured in The Netherlands. Mechanism of Ventricular Tachycardia Termination by Pacing at Left
Journal of Interventional Cardiac Electrophysiology 6, 35 41, 2002 C 2002 Kluwer Academic Publishers. Manufactured in The Netherlands. Mechanism of Ventricular Tachycardia Termination by Pacing at Left