Massive and Submassive Pulmonary Embolism: 2017 Update and Future Directions
|
|
|
- Janis Bates
- 5 years ago
- Views:
Transcription

1 Massive and Submassive Pulmonary Embolism: 2017 Update and Future Directions Kush R Desai, MD Assistant Professor of Radiology Northwestern University Feinberg School of Medicine Chicago, IL
2 Disclosures Speakers bureau/consulting, Cook Medical, Boston Scientific, AngioDynamics Consulting, Spectranetics




3 Estimated Prevalence (%) Shock Highintermediate risk PE Low-intermediate risk PE Symptomatic PE affects 600,000 people annually - US 25 Low risk PE 40 Asymptomatic Becattini C, Agnelli G. Thromb Haemost. 2008; 100(5): Abrahams van-doorn P. and Hartmann IJC. Imaging Insights. 2011; 2: Dalen JE. Chest. 2002; 122:




4 Life after acute PE Persistent thrombi 15-33% All PE patients CTEPH 0.1-4% Reduced functional status 50% Measurable limitation 10-30% Klok Blood Reviews 2014 Matthews Pulm Circulation 2016
5 Definitions
6 Pulmonary Embolism Definitions AHA Guidelines 2011 Massive: Acute PE with sustained hypotension SBP <90mmHg for at least 15 min or requiring inotropic support, not due to a cause other than PE (arrythmias, hypovolemia, sepsis, LV dysfunction, pulselessness, profound bradycardia with shock) Submassive: Acute PE without systemic hypotension (SBP >90mmHG) AND either.. RV dysfunction (RV/LV ratio >0.9, RV dysfunction on echo, RV dilation on CT scan, Elevated BNP (90) or NtproBNP (500), EKG evidence RV strain) Myocardial necrosis (elevated TNI >0.4ng/mL, TNT >0.1ng/mL) Non-massive Acute PE without clinical markers of adverse prognosis ESC Guidelines 2014 High Risk: Acute PE with shock or hypotension SBP <90mmHg, or SBP drop by > 40mmHg, for at least 15 min, not due to a cause other than PE Intermediate High Risk: Acute PE without hypotension and elevated PESI score with RV dysfunction AND serology Pos Intermediate Low Risk: Acute PE without hypotension and elevated PESI score with or without RV dysfunction OR serology Pos Low Risk: Acute PE with low PESI score * Jaff et al; Circulation. 2011; 123: ** Konstantinides et al; EurHeartJ. 2014; t Kearon et al; CHEST. 2016; 149(2): ACCP/CHEST Guidelines 2016 PE with Hypotension: Acute PE with sustained hypotension SBP <90mmHg for at least 15 min, not due to a cause other than PE High vs Low Bleeding Risk PE without Hypotension: Acute PE without systemic hypotension (SBP >90mmHG) and Using clinical judgement and testing (imaging, serology etc..) to determine level of monitoring and support needed
7 Risk Stratification in PE Mortality Related to Hemodynamic Stability Hypotensive (SBP < 90mmHG) Normotensive t International Cooperative Pulmonary Embolism Registry (ICOPER) * 52.4% [43.3, 62.1] 14.7% [13.3, 16.2] Management Strategy and Prognosis of Pulmonary Embolism Registry (MAPPET) ** 25% (65% if required CPR) 8.1% * Goldhaber et al; Lancet 1999 **Kasper et al; JACC 1997 t Wood et al; Chest, 2002
8 Treatment of Massive Pulmonary Embolism Supportive Anticoagulation Ventilatory/Pressor support ECMO Systemic/Interventional/Surgical IV tpa CDT Open embolectomy
 Circulation.")
9 Systemic thrombolysis 11 trials, 748 patients Reduction in death and recurrent PE in trials that included unstable PE patients (9.4 19%, OR 0.45, 95% CI NNT=10) Circulation Aug 10;110(6):744-9

10 Chest 2016
11 Systemic thrombolysis protocol Evaluate for contraindications Active bleeding Intracranial mass or metastasis (relative) Several other relative contraindications 100 mg tpa IV over 2 hours Benefit greatest if administered within first 48 hours

12 Role of catheter directed therapies Time is the enemy IV tpa is faster May have a role in patients who have not improved with IV tpa or have worsening shock before systemic lytic can take effect
13 Surgical embolectomy Depends on local expertise Current experience has shown lower morbidity and mortality relative to historic data Benefit larger volume of thrombus removal relative to CDT
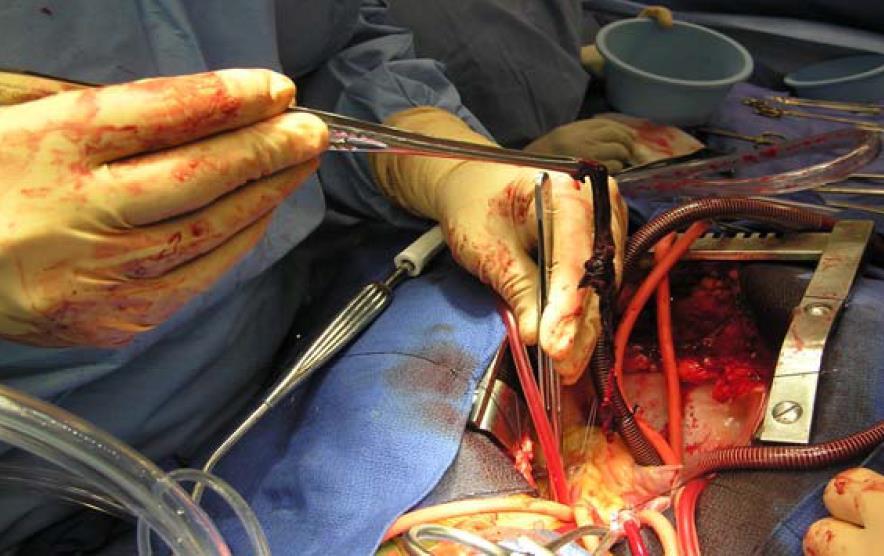
14 Surgical embolectomy

15 Surgical embolectomy
16 Patient support in massive PE RV fatigue Impending shock Cardiac arrest VA ECMO
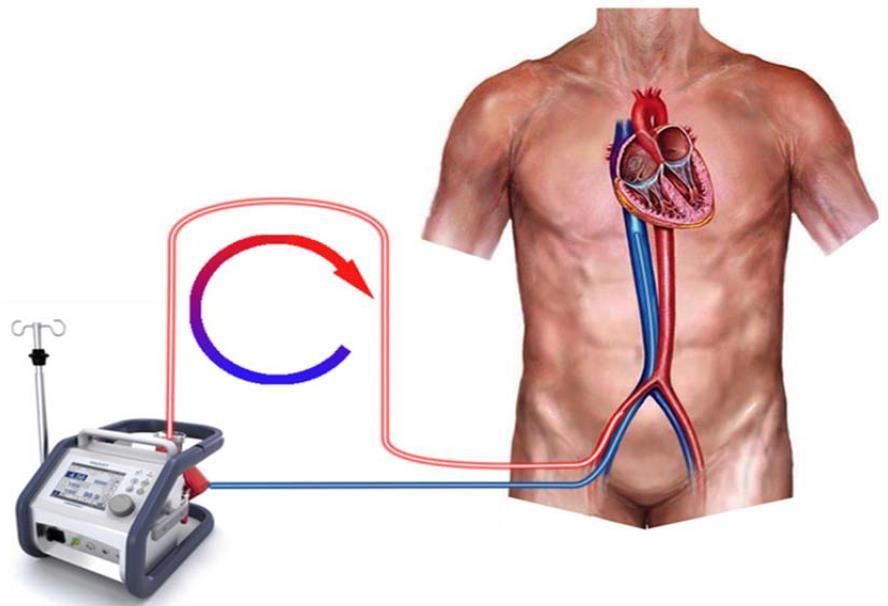
17 VA ECMO
18 Pulmonary Embolism Definitions AHA Guidelines 2011 Massive: Acute PE with sustained hypotension SBP <90mmHg for at least 15 min or requiring inotropic support, not due to a cause other than PE (arrythmias, hypovolemia, sepsis, LV dysfunction, pulselessness, profound bradycardia with shock) Submassive: Acute PE without systemic hypotension (SBP >90mmHG) AND either.. RV dysfunction (RV/LV ratio >0.9, RV dysfunction on echo, RV dilation on CT scan, Elevated BNP (90) or NtproBNP (500), EKG evidence RV strain) Myocardial necrosis (elevated TNI >0.4ng/mL, TNT >0.1ng/mL) Non-massive Acute PE without clinical markers of adverse prognosis ESC Guidelines 2014 High Risk: Acute PE with shock or hypotension SBP <90mmHg, or SBP drop by > 40mmHg, for at least 15 min, not due to a cause other than PE Intermediate High Risk: Acute PE without hypotension and elevated PESI score with RV dysfunction AND serology Pos Intermediate Low Risk: Acute PE without hypotension and elevated PESI score with or without RV dysfunction OR serology Pos Low Risk: Acute PE with low PESI score * Jaff et al; Circulation. 2011; 123: ** Konstantinides et al; EurHeartJ. 2014; t Kearon et al; CHEST. 2016; 149(2): ACCP/CHEST Guidelines 2016 PE with Hypotension: Acute PE with sustained hypotension SBP <90mmHg for at least 15 min, not due to a cause other than PE High vs Low Bleeding Risk PE without Hypotension: Acute PE without systemic hypotension (SBP >90mmHG) and Using clinical judgement and testing (imaging, serology etc..) to determine level of monitoring and support needed
19 ICOPER alerted us to RV dysfunction
20 Risk Stratification in PE Predictors of Early Mortality in Acute PE Test or Biomarker Echo CT scan Cut off RV dysfunction OR or HR 2.4 * [1.3, 4.3] RV/LV>1 1.5 * [0.7, 3.4] RV/LV > ** [0.9, 8.2] BNP pg 6.5 t [2.0, 21] NT-proBNP 600pg/ml 6.3 [ ] TNI Var 4.0 tt [2.2, 7.2] *Coutance et al Crit Care 2011; , t Klok et al, AJRCCM; 2008 ** Becattini Eur Heart J 2011; , tt becattini circ; 2007 Becattini et al Chest 2013; 144 (5): patients normotensive PE with echo and troponin. More evidence of RV strain larger the risk of death or clinical decompensation
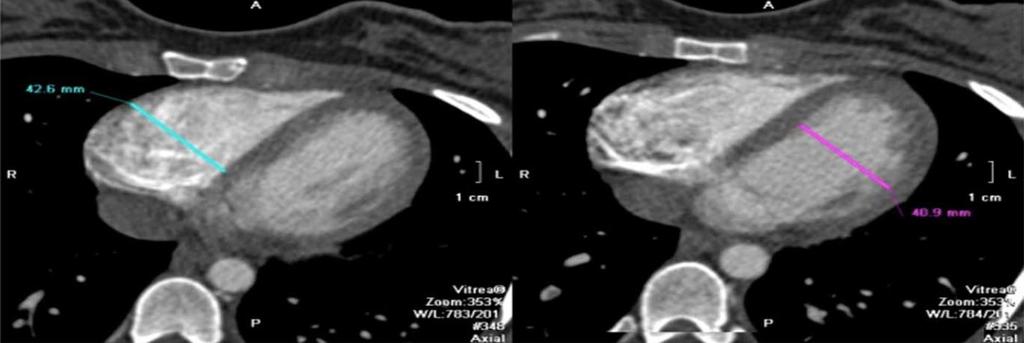
21 Evaluating the RV Biomarkers BNP, Troponin Imaging Echocardiography CT RV/LV ratio
22
23 PESI score Aujesky et al, Am J Resp Crit Care Med 2005
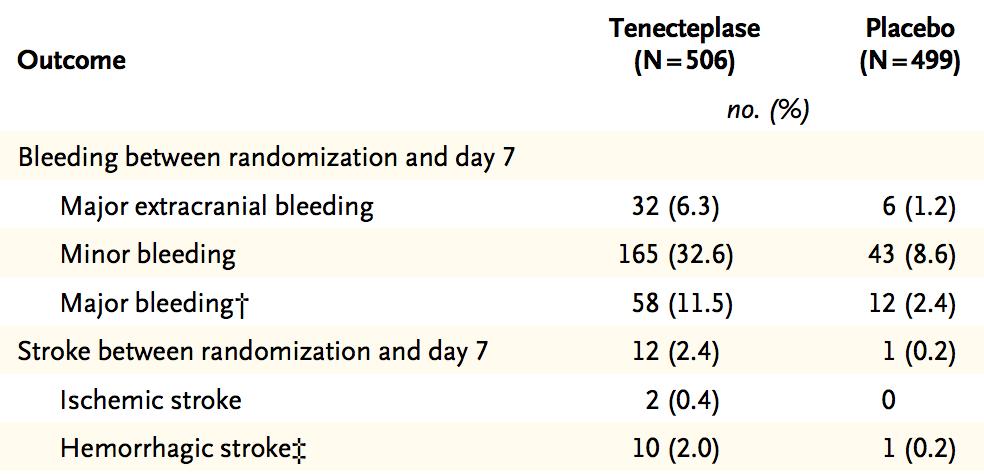
24 Role of systemic thrombolytics in PE PEITHO trial 2014 Placebo controlled, multicenter RCT Heparin + fibrinolytic vs heparin alone Patients had elevated troponin and RV dysfunction Treatment arm weight based tenecteplase dosing (30-50 mg)
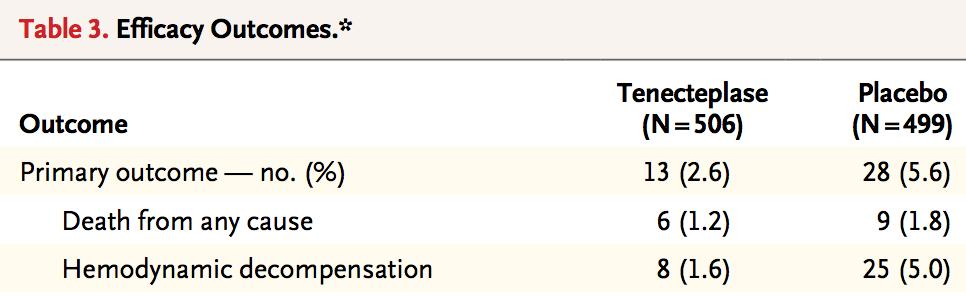
25

26 Stroke risk 2.4% vs 0.2% N Engl J Med Apr 10;370(15):

27 The rationale for catheter directed therapy
28
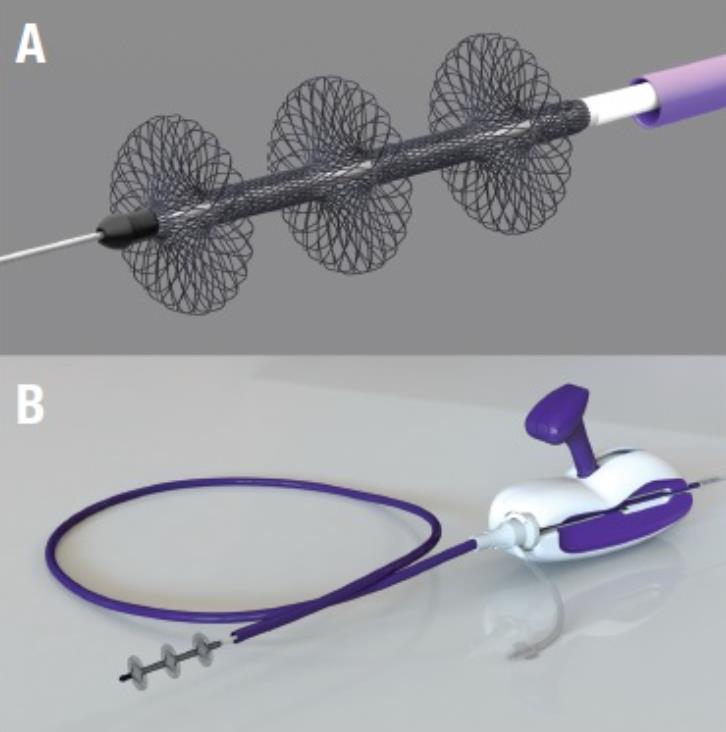
29 Catheter-Directed techniques Infusion of thrombolytics via drug dispersion catheters Mechanical thrombectomy Ultrasound-assisted thrombolytic infusion

30
31


32
33

34 Ultrasound-assisted thrombolysis FDA approved for treatment of acute PE

35 59 patients, intermediate risk (RV:LV ratio >1) US-assisted CDT (USAT) vs. heparin alone Reduction in RV/LV ratio at 24 hours Ratio reduction: USAT 0.3+/-0.2 vs heparin /-0.16 (p<0.001) No major bleeding, 4 minor bleeding episodes Circulation Jan 28;129(4):479-86
 1 groin hematoma, no intracranial bleeding JACC Cardiovasc Interv.")
36 150 patients, massive and submassive PE, single-arm Reduction of RV/LV ratio at 24 hours Low dose, total 1 mg tpa/h (split-dose for bilateral) Mean ratio reduction of 0.42, mean PA pressure reduction 14.5 mmhg (p<0.0001) 1 groin hematoma, no intracranial bleeding JACC Cardiovasc Interv Aug 24;8(10):
37 101 patients, massive and submassive PE Operator discretion on method of CDT Clinical success defined as HD stabilization, pulm HTN and/or improvement in RV strain, survival at discharge Success in 85.7% massive PE pts, 97.3 submassive PE pts, 89.1% showed improvement in RV strain on echo (p<0.0001) No major complications Chest Sep;148(3):667-73
38 What about endpoints? Studies thus far have examined endpoints such as reduction of RV/LV ratio, PA systolic pressure Clinically meaningful? Physiologic parameters?

39 Prospective cohort study, 100 patients, Measurement of cardiopulmonary exercise testing at 1 and 12 months, QOL, 6 minute walk distance, residual clot burden, cardiac function, PFTs 46.5% (40/86) patients had VO 2 peak < 80% at 1 year Associated with decreased QOL, dyspnea, 6MWD Kahn et al, Chest 2017
40 Future directions: PE-TRACT Multicenter, blinded, randomized trial comparing CDT + anticoagulation vs anticoagulation alone Primary outcome to assess patient endurance post therapy at 1 yr 6 minute walk distance Secondary outcomes to include QOL measures, NYHA class, safety events, and recurrent VTE rates amongst others Planned submission to NIH/NHLBI
41 Tips for PE intervention How I do it Select the appropriate patient (AHA guidelines) Right IJ access x 2 (my preference) Long, 7Fr 45 cm curved sheaths, sheath in the PA Access PA with C2 and J-wire 90 cm (10-20 cm infusion length) catheters 0.45 mg/hr per catheter Q6 fibrinogen, hr infusion Measure peak systolic pressure before and after through sheath

42 Thank You
RISK STRATIFICATION OF PATIENTS WITH ACUTE SYMPTOMATIC PULMONARY EMBOLISM. David Jiménez, MD, PhD, FCCP Ramón y Cajal Hospital, IRYCIS Madrid, Spain
 RISK STRATIFICATION OF PATIENTS WITH ACUTE SYMPTOMATIC PULMONARY EMBOLISM David Jiménez, MD, PhD, FCCP Ramón y Cajal Hospital, IRYCIS Madrid, Spain Potential Conflicts of Interest Financial conflicts of
RISK STRATIFICATION OF PATIENTS WITH ACUTE SYMPTOMATIC PULMONARY EMBOLISM David Jiménez, MD, PhD, FCCP Ramón y Cajal Hospital, IRYCIS Madrid, Spain Potential Conflicts of Interest Financial conflicts of
Mark H. Meissner, MD Peter Gloviczki Professor of Venous & Lymphatic Disorders University of Washington School of Medicine
 Pulmonary Embolism Response Teams Not So Fast Early Interventions is a House of Cards Mark H. Meissner, MD Peter Gloviczki Professor of Venous & Lymphatic Disorders University of Washington School of Medicine
Pulmonary Embolism Response Teams Not So Fast Early Interventions is a House of Cards Mark H. Meissner, MD Peter Gloviczki Professor of Venous & Lymphatic Disorders University of Washington School of Medicine
Epidemiology. Update on Pulmonary Embolism. Keys to PE Management 5/5/2014. Diagnosis. Risk stratification. Treatment
 Update on Pulmonary Embolism Steven M. Dean, DO, FACP, RPVI Program Director- Vascular Medicine Associate Professor of Internal Medicine Division of Cardiovascular Medicine The Ohio State University Keys
Update on Pulmonary Embolism Steven M. Dean, DO, FACP, RPVI Program Director- Vascular Medicine Associate Professor of Internal Medicine Division of Cardiovascular Medicine The Ohio State University Keys
Management of Acute Pulmonary Embolism. Judith Hurdman Consultant Respiratory Physician
 Management of Acute Pulmonary Embolism Judith Hurdman Consultant Respiratory Physician Judith.hurdman@sth.nhs.uk Overview Risk Stratification Who can be managed as an outpatient? To thrombolyse or not
Management of Acute Pulmonary Embolism Judith Hurdman Consultant Respiratory Physician Judith.hurdman@sth.nhs.uk Overview Risk Stratification Who can be managed as an outpatient? To thrombolyse or not
Venous Thrombosis. Magnitude of the Problem. DVT 2 Million PE 600,000. Death 60,000. Estimated Cost of VTE Care $1.5 Billion/year.
 Venous Thrombosis Magnitude of the Problem DVT 2 Million Postthrombotic Syndrome 800,000 PE 600,000 Death 60,000 Silent PE 1 Million Pulmonary Hypertension 30,000 Estimated Cost of VTE Care $1.5 Billion/year
Venous Thrombosis Magnitude of the Problem DVT 2 Million Postthrombotic Syndrome 800,000 PE 600,000 Death 60,000 Silent PE 1 Million Pulmonary Hypertension 30,000 Estimated Cost of VTE Care $1.5 Billion/year
Single-Center, Retrospective, Observational Analysis of Patients with Submassive Pulmonary Embolism (PE) Receiving Catheter- Directed Thrombolysis
 Receiving Catheter- Directed Thrombolysis") Single-Center, Retrospective, Observational Analysis of Patients with Submassive Pulmonary Embolism (PE) Receiving Catheter- Directed Thrombolysis John A. Phillips, M.D. OhioHealth Heart and Vascular Physicians
Single-Center, Retrospective, Observational Analysis of Patients with Submassive Pulmonary Embolism (PE) Receiving Catheter- Directed Thrombolysis John A. Phillips, M.D. OhioHealth Heart and Vascular Physicians
Acute and long-term treatment of VTE. Cecilia Becattini University of Perugia
 Acute and long-term treatment of VTE Cecilia Becattini University of Perugia Acute and long-term treatment of VTE The goals The acute PE phase After the acute phase Treatment for VTE Goals of acute treatment
Acute and long-term treatment of VTE Cecilia Becattini University of Perugia Acute and long-term treatment of VTE The goals The acute PE phase After the acute phase Treatment for VTE Goals of acute treatment
Disclosures. Objectives
 BRIGHAM AND WOMEN S HOSPITAL Treatment of Massive and Submassive Pulmonary Embolism Gregory Piazza, MD, MS Assistant Professor of Medicine Harvard Medical School Staff Physician, Cardiovascular Division
BRIGHAM AND WOMEN S HOSPITAL Treatment of Massive and Submassive Pulmonary Embolism Gregory Piazza, MD, MS Assistant Professor of Medicine Harvard Medical School Staff Physician, Cardiovascular Division
Catheter Directed Interventions for Pulmonary Embolism
 Catheter Directed Interventions for Pulmonary Embolism Rabih A. Chaer, MD, MSc Professor of Surgery, UPMC Residency Program Director Site chief, Presbyterian campus Division of Vascular Surgery Pittsburgh,
Catheter Directed Interventions for Pulmonary Embolism Rabih A. Chaer, MD, MSc Professor of Surgery, UPMC Residency Program Director Site chief, Presbyterian campus Division of Vascular Surgery Pittsburgh,
Management of Massive and Sub-Massive Pulmonary Embolism
 Management of Massive and Sub-Massive Pulmonary Embolism M. Montero-Baker, MD L Leon Jr., MD, RVT, FACS Tucson Medical Center Vascular and Endovascular Surgery Section CASE PRESENTATION 54 YEAR- OLD CAUCASIAN
Management of Massive and Sub-Massive Pulmonary Embolism M. Montero-Baker, MD L Leon Jr., MD, RVT, FACS Tucson Medical Center Vascular and Endovascular Surgery Section CASE PRESENTATION 54 YEAR- OLD CAUCASIAN
Single Center 4 year series of 114 consecutive patients treated for massive and submassive PE. Mark Goodwin, MD
 Single Center 4 year series of 114 consecutive patients treated for massive and submassive PE Mark Goodwin, MD Disclosure Speaker name:... I have the following potential conflicts of interest to report:
Single Center 4 year series of 114 consecutive patients treated for massive and submassive PE Mark Goodwin, MD Disclosure Speaker name:... I have the following potential conflicts of interest to report:
The OPTALYSE PE Trial Reducing thrombolytic dose and treatment times with EKOS in the treatment of pulmonary embolism patients
 The OPTALYSE PE Trial Reducing thrombolytic dose and treatment times with EKOS in the treatment of pulmonary embolism patients Keith M. Sterling, M.D. Director, Cardiovascular & Interventional Radiology
The OPTALYSE PE Trial Reducing thrombolytic dose and treatment times with EKOS in the treatment of pulmonary embolism patients Keith M. Sterling, M.D. Director, Cardiovascular & Interventional Radiology
Innovative Endovascular Approach to Pulmonary Embolism by Ultrasound Enhanced Thrombolysis. Prof. Ralf R.Kolvenbach MD,PhD,FEBVS
 Innovative Endovascular Approach to Pulmonary Embolism by Ultrasound Enhanced Thrombolysis Prof. Ralf R.Kolvenbach MD,PhD,FEBVS Catheter-based thrombolysis Local administration of lytic agent Higher local
Innovative Endovascular Approach to Pulmonary Embolism by Ultrasound Enhanced Thrombolysis Prof. Ralf R.Kolvenbach MD,PhD,FEBVS Catheter-based thrombolysis Local administration of lytic agent Higher local
DECLARATION OF CONFLICT OF INTEREST
 DECLARATION OF CONFLICT OF INTEREST IDENTIFYING LOW-RISK PULMONARY EMBOLISM CLINICAL SCORES David Jiménez, MD, PhD Respiratory Department Ramón y Cajal Hospital Madrid, Spain Potential Conflicts of Interest
DECLARATION OF CONFLICT OF INTEREST IDENTIFYING LOW-RISK PULMONARY EMBOLISM CLINICAL SCORES David Jiménez, MD, PhD Respiratory Department Ramón y Cajal Hospital Madrid, Spain Potential Conflicts of Interest
What is New in Acute Pulmonary Embolism? Interventional Treatment. Prof. Nils Kucher University Hospital Bern Switzerland
 What is New in Acute Pulmonary Embolism? Interventional Treatment Prof. Nils Kucher University Hospital Bern Switzerland nils.kucher@insel.ch Disclosure of Interest Dr. Kucher received research grants
What is New in Acute Pulmonary Embolism? Interventional Treatment Prof. Nils Kucher University Hospital Bern Switzerland nils.kucher@insel.ch Disclosure of Interest Dr. Kucher received research grants
Case. Case. Management of Pulmonary Embolism in the ICU
 Management of Pulmonary Embolism in the ICU Todd M Bull, M.D. Associate Professor of Medicine Division of Pulmonary Sciences and Critical Care Medicine Pulmonary Hypertension Center University of Colorado
Management of Pulmonary Embolism in the ICU Todd M Bull, M.D. Associate Professor of Medicine Division of Pulmonary Sciences and Critical Care Medicine Pulmonary Hypertension Center University of Colorado
Acute and long-term treatment of PE. Cecilia Becattini University of Perugia
 Acute and long-term treatment of PE Cecilia Becattini University of Perugia Acute and long-term treatment of VTE What is the optimal acute phase treatment for the patient? Intravenous thrombolysis One
Acute and long-term treatment of PE Cecilia Becattini University of Perugia Acute and long-term treatment of VTE What is the optimal acute phase treatment for the patient? Intravenous thrombolysis One
Epidemiology: Incidence VTE: Mortality Morbidity Risk Factors: Acute Chronic : Genetic
 Submassive PE Pulmonary Embolism Epidemiology: Incidence VTE: 100-200/100,000 = 3rd most frequent cardiovascular disease Symptomatic DVT complicated by PE = 40-50% Sudden fatal PE = 34% Intermediate-risk
Submassive PE Pulmonary Embolism Epidemiology: Incidence VTE: 100-200/100,000 = 3rd most frequent cardiovascular disease Symptomatic DVT complicated by PE = 40-50% Sudden fatal PE = 34% Intermediate-risk
Epidemiology of Pulmonary Embolism (PE)
") Why Treat Submassive PE Abstract: Massive Pulmonary Embolism (PE) requires immediate lifesaving intervention for the patient. For the submassive PE patient, characterized by presence of right ventricular
Why Treat Submassive PE Abstract: Massive Pulmonary Embolism (PE) requires immediate lifesaving intervention for the patient. For the submassive PE patient, characterized by presence of right ventricular
Management of Intermediate-Risk Pulmonary Embolism
 Management of Intermediate-Risk Pulmonary Embolism Stavros V. Konstantinides, MD, PhD, FESC Professor, Clinical Trials in Antithrombotic Therapy Center for Thrombosis und Hemostasis, University of Mainz,
Management of Intermediate-Risk Pulmonary Embolism Stavros V. Konstantinides, MD, PhD, FESC Professor, Clinical Trials in Antithrombotic Therapy Center for Thrombosis und Hemostasis, University of Mainz,
PREVENTION AND TREATMENT OF VENOUS THROMBOEMBOLISM
 PREVENTION AND TREATMENT OF VENOUS THROMBOEMBOLISM International Consensus Statement 2013 Guidelines According to Scientific Evidence Developed under the auspices of the: Cardiovascular Disease Educational
PREVENTION AND TREATMENT OF VENOUS THROMBOEMBOLISM International Consensus Statement 2013 Guidelines According to Scientific Evidence Developed under the auspices of the: Cardiovascular Disease Educational
How and Why to Form a PERT, Pulmonary Embolism Response Team
 Disclosures How and Why to Form a PERT, Pulmonary Embolism Response Team Rachel P. Rosovsky, MD, MPH No disclosures Rachel P. Rosovsky, MD, MPH April 21, 2017 AC Forum 2017 2 Agenda Pulmonary Embolism
Disclosures How and Why to Form a PERT, Pulmonary Embolism Response Team Rachel P. Rosovsky, MD, MPH No disclosures Rachel P. Rosovsky, MD, MPH April 21, 2017 AC Forum 2017 2 Agenda Pulmonary Embolism
Severe pulmonary embolism: Catheter-based thrombolysis and medical treatment
 Severe pulmonary embolism: Catheter-based thrombolysis and medical treatment Rolf P. Engelberger, MD Division of Angiology Cantonal Hospital Fribourg & University Hospital Bern, Switzerland Overview Reperfusion
Severe pulmonary embolism: Catheter-based thrombolysis and medical treatment Rolf P. Engelberger, MD Division of Angiology Cantonal Hospital Fribourg & University Hospital Bern, Switzerland Overview Reperfusion
Ryan Walsh, MD Department of Emergency Medicine Madigan Army Medical Center
 Ryan Walsh, MD Department of Emergency Medicine Madigan Army Medical Center The opinions expressed herein are solely those of the author and do not represent the official views of the Department of Defense
Ryan Walsh, MD Department of Emergency Medicine Madigan Army Medical Center The opinions expressed herein are solely those of the author and do not represent the official views of the Department of Defense
Innovative Endovascular Approach to Pulmonary Embolism by Ultrasound Enhanced Thrombolysis. Prof. Ralf R.Kolvenbach MD,PhD,FEBVS
 Innovative Endovascular Approach to Pulmonary Embolism by Ultrasound Enhanced Thrombolysis Prof. Ralf R.Kolvenbach MD,PhD,FEBVS Conflict of Interest BTG Standard PE therapy ANTICOAGULATION (AC) HEPARIN
Innovative Endovascular Approach to Pulmonary Embolism by Ultrasound Enhanced Thrombolysis Prof. Ralf R.Kolvenbach MD,PhD,FEBVS Conflict of Interest BTG Standard PE therapy ANTICOAGULATION (AC) HEPARIN
Use of EKOS Catheter in the management of Venous Mr. Manoj Niverthi, Mr. Sarang Pujari, and Ms. Nupur Dandavate, The GTF Group
 Use of EKOS Catheter in the management of Venous Thromboembolism @ Mr. Manoj Niverthi, Mr. Sarang Pujari, and Ms. Nupur Dandavate, The GTF Group Introduction Georgia Thrombosis Forum (GTF, www.gtfonline.net)
Use of EKOS Catheter in the management of Venous Thromboembolism @ Mr. Manoj Niverthi, Mr. Sarang Pujari, and Ms. Nupur Dandavate, The GTF Group Introduction Georgia Thrombosis Forum (GTF, www.gtfonline.net)
Updates in venous thromboembolism. Cecilia Becattini University of Perugia
 Updates in venous thromboembolism Cecilia Becattini University of Perugia News for VTE Diagnosis Treatment the acute phase the agents Pulmonary embolism: diagnosis Vein ultrasonography Meta-analysis 15
Updates in venous thromboembolism Cecilia Becattini University of Perugia News for VTE Diagnosis Treatment the acute phase the agents Pulmonary embolism: diagnosis Vein ultrasonography Meta-analysis 15
The spectrum of clinical outcome of PE
 Practical treatment approach for patients with PE Cecilia Becattini University of Perugia The spectrum of clinical presentation of PE PE-related shock Mild clinical symptoms The spectrum of clinical outcome
Practical treatment approach for patients with PE Cecilia Becattini University of Perugia The spectrum of clinical presentation of PE PE-related shock Mild clinical symptoms The spectrum of clinical outcome
L embolia polmonare ad alto rischio, dalla diagnosi alla terapia riperfusiva.
 L embolia polmonare ad alto rischio, dalla diagnosi alla terapia riperfusiva. Centro di riferimento regione toscana per la diagnosi e la terapia della tromboembolia polmonare Dip Emergenza Urgenza- Careggi
L embolia polmonare ad alto rischio, dalla diagnosi alla terapia riperfusiva. Centro di riferimento regione toscana per la diagnosi e la terapia della tromboembolia polmonare Dip Emergenza Urgenza- Careggi
PULMONARY EMBOLISM AND PERT. Jonathon Kirkland, DO OSU Department Chair, Radiology Head of Interventional Radiology
 PULMONARY EMBOLISM AND PERT Jonathon Kirkland, DO OSU Department Chair, Radiology Head of Interventional Radiology No financial disclosures 1. What are the clinical signs/symptoms of submassive PE? 2.
PULMONARY EMBOLISM AND PERT Jonathon Kirkland, DO OSU Department Chair, Radiology Head of Interventional Radiology No financial disclosures 1. What are the clinical signs/symptoms of submassive PE? 2.
Thrombus Removal in Acute Pulmonary Embolism: When and How?
 Thrombus Removal in Acute Pulmonary Embolism: When and How? Kenneth Rosenfield, MD, MHCDS, MSCAI Cardiology Division Section of Vascular Medicine and Intvn MGH Kenneth Rosenfield, MD, MHCDS Conflicts of
Thrombus Removal in Acute Pulmonary Embolism: When and How? Kenneth Rosenfield, MD, MHCDS, MSCAI Cardiology Division Section of Vascular Medicine and Intvn MGH Kenneth Rosenfield, MD, MHCDS Conflicts of
Management of Pulmonary Embolism. Michael Hooper, M.D., MSc Associate Professor, Pulmonary and Critical Care Medicine Eastern Virginia Medical School
 Management of Pulmonary Embolism Michael Hooper, M.D., MSc Associate Professor, Pulmonary and Critical Care Medicine Eastern Virginia Medical School I have no conflicts of interest to report. VTE Overview
Management of Pulmonary Embolism Michael Hooper, M.D., MSc Associate Professor, Pulmonary and Critical Care Medicine Eastern Virginia Medical School I have no conflicts of interest to report. VTE Overview
Catheter-directed Thrombolysis for Pulmonary Embolism
 Catheter-directed Thrombolysis for Pulmonary Embolism Is It Good Advice to Lyse? Texas Society of Health-System Pharmacists April 7, 2018 Rebecca L. Attridge, PharmD, MSc, BCPS Associate Professor, University
Catheter-directed Thrombolysis for Pulmonary Embolism Is It Good Advice to Lyse? Texas Society of Health-System Pharmacists April 7, 2018 Rebecca L. Attridge, PharmD, MSc, BCPS Associate Professor, University
Is Thrombolysis Only for a Crisis?
 Is Thrombolysis Only for a Crisis? December 19, 2017 Is Thrombolysis Only for a Crisis? Indications for Thrombolytic Therapy in Patients with Acute Pulmonary Embolism Case Scenario A 28 year old woman
Is Thrombolysis Only for a Crisis? December 19, 2017 Is Thrombolysis Only for a Crisis? Indications for Thrombolytic Therapy in Patients with Acute Pulmonary Embolism Case Scenario A 28 year old woman
Management of sub-massive and massive pulmonary embolism:
 Management of sub-massive and massive pulmonary embolism: Evidence and Controversy Boonsong Patjanasoontorn, MD, FCCP, FCCM Immediate Past President, Thai Society of Critical Care Medicine(TSCCM) Chief,
Management of sub-massive and massive pulmonary embolism: Evidence and Controversy Boonsong Patjanasoontorn, MD, FCCP, FCCM Immediate Past President, Thai Society of Critical Care Medicine(TSCCM) Chief,
RECOMMENDATIONS FOR THE MANAGEMENT OF MASSIVE AND SUBMASSIVE PULMONARY EMBOLISM IN ADULT PATIENTS.
 RECOMMENDATIONS FOR THE MANAGEMENT OF MASSIVE AND SUBMASSIVE PULMONARY EMBOLISM IN ADULT PATIENTS. Target Audience: Physicians managing adult patients with massive and submassive pulmonary emboli in the
RECOMMENDATIONS FOR THE MANAGEMENT OF MASSIVE AND SUBMASSIVE PULMONARY EMBOLISM IN ADULT PATIENTS. Target Audience: Physicians managing adult patients with massive and submassive pulmonary emboli in the
National Institute for Health and Care Excellence
 National Institute for Health and Care Excellence IP1243 Ultrasound enhanced catheter-directed thrombolysis for pulmonary embolism Consultation Comments table IPAC date: Thursday 12 March 2015 1 1 Manufacturer
National Institute for Health and Care Excellence IP1243 Ultrasound enhanced catheter-directed thrombolysis for pulmonary embolism Consultation Comments table IPAC date: Thursday 12 March 2015 1 1 Manufacturer
Optimal Management of Intermediate-Risk Pulmonary Embolism
 Optimal Management of Intermediate-Risk Pulmonary Embolism Stavros V. Konstantinides, MD, PhD, FESC Professor, Clinical Trials in Antithrombotic Therapy Center for Thrombosis und Hemostasis, University
Optimal Management of Intermediate-Risk Pulmonary Embolism Stavros V. Konstantinides, MD, PhD, FESC Professor, Clinical Trials in Antithrombotic Therapy Center for Thrombosis und Hemostasis, University
Catheter Interventions for pulmonary embolism:
 Catheter Interventions for pulmonary embolism: From Directed tpa Drips to Suction Thrombectomy Efthymios Avgerinos, MD Associate Professor of Surgery Division of Vascular Surgery University of Pittsburgh
Catheter Interventions for pulmonary embolism: From Directed tpa Drips to Suction Thrombectomy Efthymios Avgerinos, MD Associate Professor of Surgery Division of Vascular Surgery University of Pittsburgh
VTE & Medical Patients: Case Scenario
 The Saudi Association for Venous Thromboembolism SAVTE The 2 nd SAVTE Symposium 1-3 May, 2012 Casablanca, Morocco VTE & Medical Patients: Case Scenario Majdy Idrees Riyadh, Saudi Arabia Majdy M Idrees,
The Saudi Association for Venous Thromboembolism SAVTE The 2 nd SAVTE Symposium 1-3 May, 2012 Casablanca, Morocco VTE & Medical Patients: Case Scenario Majdy Idrees Riyadh, Saudi Arabia Majdy M Idrees,
PULMONARY EMBOLISM (PE): DIAGNOSIS AND TREATMENT
: DIAGNOSIS AND TREATMENT") PULMONARY EMBOLISM (PE): DIAGNOSIS AND TREATMENT OBJECTIVE: To provide a diagnostic algorithm and treatment options for patients with acute pulmonary embolism (PE). BACKGROUND: Venous thromboembolism (VTE)
PULMONARY EMBOLISM (PE): DIAGNOSIS AND TREATMENT OBJECTIVE: To provide a diagnostic algorithm and treatment options for patients with acute pulmonary embolism (PE). BACKGROUND: Venous thromboembolism (VTE)
Thrombolysis in PE. Outline. Disclosure. Overview on Pulmonary Embolism. Hot Topics in Emergency Medicine 2012 Midyear Clinical Meeting
 Disclosure Thrombolysis in PE Daniel P. Hays, PharmD, BCPS, FASHP reports no relevant financial relationships. Daniel P. Hays, PharmD, BCPS, FASHP Outline 55 YOF presents to ED with SOB PMH of DVT + noncompliance
Disclosure Thrombolysis in PE Daniel P. Hays, PharmD, BCPS, FASHP reports no relevant financial relationships. Daniel P. Hays, PharmD, BCPS, FASHP Outline 55 YOF presents to ED with SOB PMH of DVT + noncompliance
Pulmonary embolism: Acute management. Cecilia Becattini University of Perugia, Italy
 Pulmonary embolism: Acute management Cecilia Becattini University of Perugia, Italy Acute pulmonary embolism: Acute management Diagnosis Risk stratification Treatment Non-high risk PE: diagnosis 3-mo VTE
Pulmonary embolism: Acute management Cecilia Becattini University of Perugia, Italy Acute pulmonary embolism: Acute management Diagnosis Risk stratification Treatment Non-high risk PE: diagnosis 3-mo VTE
RECOMMENDATIONS FOR THE MANAGEMENT OF MASSIVE AND SUBMASSIVE PULMONARY EMBOLISM IN ADULT PATIENTS.
 DRAFT-2018 UPDATES RECOMMENDATIONS FOR THE MANAGEMENT OF MASSIVE AND SUBMASSIVE PULMONARY EMBOLISM IN ADULT PATIENTS. Target Audience: MultiCare physicians managing adult patients with massive and submassive
DRAFT-2018 UPDATES RECOMMENDATIONS FOR THE MANAGEMENT OF MASSIVE AND SUBMASSIVE PULMONARY EMBOLISM IN ADULT PATIENTS. Target Audience: MultiCare physicians managing adult patients with massive and submassive
Understanding Best Practices in Anticoagulation Therapy in Patients with Venous Thromboembolism. Rajat Deo, MD, MTR
 Understanding Best Practices in Anticoagulation Therapy in Patients with Venous Thromboembolism Rajat Deo, MD, MTR Director of Translational Research in Cardiac Arrhythmias Division of Cardiovascular Medicine
Understanding Best Practices in Anticoagulation Therapy in Patients with Venous Thromboembolism Rajat Deo, MD, MTR Director of Translational Research in Cardiac Arrhythmias Division of Cardiovascular Medicine
Chapter 1. Introduction
 Chapter 1 Introduction Introduction 9 Even though the first reports on venous thromboembolism date back to the 13 th century and the mechanism of acute pulmonary embolism (PE) was unraveled almost 150
Chapter 1 Introduction Introduction 9 Even though the first reports on venous thromboembolism date back to the 13 th century and the mechanism of acute pulmonary embolism (PE) was unraveled almost 150
Rationale for catheter directed therapy in pulmonary embolism
 Mini-Review Rationale for catheter directed therapy in pulmonary embolism Sailen G. Naidu, Martha-Gracia Knuttinen, J. Scott Kriegshauser, William G. Eversman, Rahmi Oklu Department of Radiology, Division
Mini-Review Rationale for catheter directed therapy in pulmonary embolism Sailen G. Naidu, Martha-Gracia Knuttinen, J. Scott Kriegshauser, William G. Eversman, Rahmi Oklu Department of Radiology, Division
Acute Pulmonary Embolism and Deep Vein Thrombosis. Barbara LeVarge MD Beth Israel Deaconess Medical Center Pulmonary Hypertension Center COPYRIGHT
 Acute Pulmonary Embolism and Deep Vein Thrombosis Barbara LeVarge MD Beth Israel Deaconess Medical Center Pulmonary Hypertension Center Acute PE and DVT No disclosures. Acute PE and DVT Learning objectives
Acute Pulmonary Embolism and Deep Vein Thrombosis Barbara LeVarge MD Beth Israel Deaconess Medical Center Pulmonary Hypertension Center Acute PE and DVT No disclosures. Acute PE and DVT Learning objectives
Interventional Management of Acute Pulmonary Embolism
 Interventional Management of Acute Pulmonary Embolism Prof. Nils Kucher Angiology & Cardiology University Hospital Bern Inselspital nils.kucher@insel.ch DECLARATION OF CONFLICT OF INTEREST Consultant to
Interventional Management of Acute Pulmonary Embolism Prof. Nils Kucher Angiology & Cardiology University Hospital Bern Inselspital nils.kucher@insel.ch DECLARATION OF CONFLICT OF INTEREST Consultant to
Θεραπεία και Πρόληψη Θρομβώσεων και Πνευμονικών Εμβολών Τι μάθαμε το 2017; Τι περιμένουμε το 2018;
 Θεραπεία και Πρόληψη Θρομβώσεων και Πνευμονικών Εμβολών Τι μάθαμε το 2017; Τι περιμένουμε το 2018; Stavros V. Konstantinides, MD, PhD, FESC Professor of Cardiology Democritus University of Thrace, Greece
Θεραπεία και Πρόληψη Θρομβώσεων και Πνευμονικών Εμβολών Τι μάθαμε το 2017; Τι περιμένουμε το 2018; Stavros V. Konstantinides, MD, PhD, FESC Professor of Cardiology Democritus University of Thrace, Greece
Risk-Based Evaluation and Management of VTE
 12:50-1:50pm Risk-Based Evaluation and Management of VTE SPEAKER Gregory Piazza, MD, MS BRIGHAM AND WOMEN S HOSPITAL Risk-Based Evaluation and Management of VTE Gregory Piazza, MD, MS Assistant Professor
12:50-1:50pm Risk-Based Evaluation and Management of VTE SPEAKER Gregory Piazza, MD, MS BRIGHAM AND WOMEN S HOSPITAL Risk-Based Evaluation and Management of VTE Gregory Piazza, MD, MS Assistant Professor
Bilateral Central Pulmonary Embolism and Recent History of Ischemic Stroke
 WHAT WOULD YOU DO? Bilateral Central and Recent History of Ischemic Stroke MODERATOR: KEITH M. STERLING, MD PANEL: JAMES F. BENENATI, MD; NOAH J. JONES, MD, FACC, FSCAI; AND AKHILESH K. SISTA, MD, FSIR
WHAT WOULD YOU DO? Bilateral Central and Recent History of Ischemic Stroke MODERATOR: KEITH M. STERLING, MD PANEL: JAMES F. BENENATI, MD; NOAH J. JONES, MD, FACC, FSCAI; AND AKHILESH K. SISTA, MD, FSIR
Acute cardiogenic shock with standing-still heart
 Acute cardiogenic shock with standing-still heart Ga Yeon Lee April, 21, 2017 Division of cardiology, Department of Medicine, Heart Vascular Stroke Institute, Samsung Medical Center, Seoul, South Korea
Acute cardiogenic shock with standing-still heart Ga Yeon Lee April, 21, 2017 Division of cardiology, Department of Medicine, Heart Vascular Stroke Institute, Samsung Medical Center, Seoul, South Korea
Acute Management of Pulmonary Embolism
 Acute Management of Pulmonary Embolism Dr Alex West Respiratory Consultant Guy s and St Thomas Hospital London Declarations - none Order of Play Up date in Diagnostic Imaging - CTPA and V:Q SPECT Sub-massive
Acute Management of Pulmonary Embolism Dr Alex West Respiratory Consultant Guy s and St Thomas Hospital London Declarations - none Order of Play Up date in Diagnostic Imaging - CTPA and V:Q SPECT Sub-massive
Surgical Thrombectomy for PE: Is it Making a Comeback
 Surgical Thrombectomy for PE: Is it Making a Comeback Prashanth Vallabhajosyula, MD MS The University of Pennsylvania Health System Philadelphia, PA Case - 84 year old female presents with submassive right
Surgical Thrombectomy for PE: Is it Making a Comeback Prashanth Vallabhajosyula, MD MS The University of Pennsylvania Health System Philadelphia, PA Case - 84 year old female presents with submassive right
Heart Health ESC Guidelines on the diagnosis and management of acute pulmonary embolism
 Heart Health Open Access Received: Oct 22, 2014 Accepted: Dec 01, 2014 Published: Dec 05, 2014 http://dx.doi.org/10.14437/hhoa-1-105 Review Jiri Widimsky, Heart Health Open Access 2014, 1:1 2014 ESC Guidelines
Heart Health Open Access Received: Oct 22, 2014 Accepted: Dec 01, 2014 Published: Dec 05, 2014 http://dx.doi.org/10.14437/hhoa-1-105 Review Jiri Widimsky, Heart Health Open Access 2014, 1:1 2014 ESC Guidelines
Updates in Management of Pulmonary Embolism (PE) David Ming, MD Duke Hospital Medicine July 24, 2017 Hilton Head, SC
 David Ming, MD Duke Hospital Medicine July 24, 2017 Hilton Head, SC") Updates in Management of Pulmonary Embolism (PE) David Ming, MD Duke Hospital Medicine July 24, 2017 Hilton Head, SC Objectives Highlight clinical features and presentation of acute PE Analyze strategies
Updates in Management of Pulmonary Embolism (PE) David Ming, MD Duke Hospital Medicine July 24, 2017 Hilton Head, SC Objectives Highlight clinical features and presentation of acute PE Analyze strategies
Plasma MR-proADM is superior to NTproBNP for all-cause short term mortality prediction in acute pulmonary embolism.
 J. Pedowska-Wloszek, M. Kostrubiec, A. Labyk, S. Pacho, O. Dzikowska-Diduch, P. Bienias, B. Lichodziejewska, P. Palczewski, M. Ciurzynski, P. Pruszczyk Plasma MR-proADM is superior to NTproBNP for all-cause
J. Pedowska-Wloszek, M. Kostrubiec, A. Labyk, S. Pacho, O. Dzikowska-Diduch, P. Bienias, B. Lichodziejewska, P. Palczewski, M. Ciurzynski, P. Pruszczyk Plasma MR-proADM is superior to NTproBNP for all-cause
Is it safe to manage pulmonary embolism in Primary Care? Roopen Arya King s College Hospital
 Is it safe to manage pulmonary embolism in Primary Care? Roopen Arya King s College Hospital A few definitions Safe Avoid death, recurrent thrombosis, bleeding Manage Diagnosis + treatment Pulmonary embolism
Is it safe to manage pulmonary embolism in Primary Care? Roopen Arya King s College Hospital A few definitions Safe Avoid death, recurrent thrombosis, bleeding Manage Diagnosis + treatment Pulmonary embolism
Venous thromboembolic diseases: diagnosis, management and thrombophilia testing (2012) NICE guideline CG144
 NICE guideline CG144") Venous thromboembolic diseases: diagnosis, management and thrombophilia testing (2012) NICE guideline CG144 Appendix A: Summary of new evidence from Summary of evidence from previous year Diagnosis Diagnostic
Venous thromboembolic diseases: diagnosis, management and thrombophilia testing (2012) NICE guideline CG144 Appendix A: Summary of new evidence from Summary of evidence from previous year Diagnosis Diagnostic
SESSION 4 12:45 2:15 PM
 SESSION 4 12:45 2:15 PM Pulmonary Embolism Update SPEAKER Gregory Piazza, MD, MS Presenter Disclosure Information The following relationships exist related to this presentation: Gregory Piazza, MD, MS:
SESSION 4 12:45 2:15 PM Pulmonary Embolism Update SPEAKER Gregory Piazza, MD, MS Presenter Disclosure Information The following relationships exist related to this presentation: Gregory Piazza, MD, MS:
Acoustic Pulse Thrombolysis Treatment
 Acoustic Pulse Thrombolysis Treatment BTGVascular.com SETTING THE STANDARD FOR VASCULAR THERAPIES Quickly & safely dissolve thrombus with the EKOS System. The Acoustic Pulse Difference Acoustic Pulse Thrombolysis
Acoustic Pulse Thrombolysis Treatment BTGVascular.com SETTING THE STANDARD FOR VASCULAR THERAPIES Quickly & safely dissolve thrombus with the EKOS System. The Acoustic Pulse Difference Acoustic Pulse Thrombolysis
Timing of NT-pro-BNP sampling for predicting adverse outcome after acute pulmonary embolism
 7 Frederikus A. Klok Noortje van der Bijl Inge C.M. Mos Albert de Roos Lucia J. M. Kroft Menno V. Huisman Timing of NT-pro-BNP sampling for predicting adverse outcome after acute pulmonary embolism Letter
7 Frederikus A. Klok Noortje van der Bijl Inge C.M. Mos Albert de Roos Lucia J. M. Kroft Menno V. Huisman Timing of NT-pro-BNP sampling for predicting adverse outcome after acute pulmonary embolism Letter
EKOS. Interventional Vascular 3 February, Imagine where we can go.
 EKOS Interventional Vascular 3 February, 2015 Imagine where we can go. Forward-looking statement This presentation and information communicated verbally to you may contain certain projections and other
EKOS Interventional Vascular 3 February, 2015 Imagine where we can go. Forward-looking statement This presentation and information communicated verbally to you may contain certain projections and other
UC SF. Division of General Internal Medicine UNIVERSITY OF CALIFORNIA SAN FRANCISCO, DIVISION OF HOSPITAL MEDICINE
 Updates in the Management of Venous Thromboembolism Margaret C. Fang, MD, MPH Associate Professor of Medicine UCSF Division of Hospital Medicine Medical Director, Anticoagulation Clinic Venous Thromboembolism
Updates in the Management of Venous Thromboembolism Margaret C. Fang, MD, MPH Associate Professor of Medicine UCSF Division of Hospital Medicine Medical Director, Anticoagulation Clinic Venous Thromboembolism
National Institute for Health and Care Excellence
 National Institute for Health and Care Excellence IP1219 Ultrasound enhanced catheter-directed thrombolysis for deep vein thrombosis Consultation table IPAC date: Thursday 12 March 2015 Com. 1 3 NHS Professional
National Institute for Health and Care Excellence IP1219 Ultrasound enhanced catheter-directed thrombolysis for deep vein thrombosis Consultation table IPAC date: Thursday 12 March 2015 Com. 1 3 NHS Professional
Recent advances in the management of pulmonary embolism. Kodati Rakesh SR Pulmonary medicine
 Recent advances in the management of pulmonary embolism Kodati Rakesh SR Pulmonary medicine Clinical decision rules & D dimer Outpatient anticoagulation Thrombolysis Anticoagulation Catheter directed therapies
Recent advances in the management of pulmonary embolism Kodati Rakesh SR Pulmonary medicine Clinical decision rules & D dimer Outpatient anticoagulation Thrombolysis Anticoagulation Catheter directed therapies
Canadian Society of Internal Medicine Annual Meeting 2016 Montreal, QC
 Canadian Society of Internal Medicine Annual Meeting 2016 Montreal, QC 1 st workshop: update to VTE guidelines in 2016 2 nd workshop: VTE controversies + new horizons André Roussin MD, FRCP, CSPQ CHUM
Canadian Society of Internal Medicine Annual Meeting 2016 Montreal, QC 1 st workshop: update to VTE guidelines in 2016 2 nd workshop: VTE controversies + new horizons André Roussin MD, FRCP, CSPQ CHUM
Guideline for Thrombolysis Therapy in Pulmonary Embolism
 Guideline for Thrombolysis Therapy in Pulmonary Embolism Dr Jane Strong Consultant Haematologist Trust ref: B24/2016 1. Introduction / Scope All Patients with pulmonary embolism (PE) require rapid risk
Guideline for Thrombolysis Therapy in Pulmonary Embolism Dr Jane Strong Consultant Haematologist Trust ref: B24/2016 1. Introduction / Scope All Patients with pulmonary embolism (PE) require rapid risk
Pulmonary Embolectomy:
 Pulmonary Embolectomy: Recommendation for early surgical intervention Tomas A. Salerno, M.D. Professor of Surgery, University of Miami Miller School of Medicine and Jackson Memorial Hospital Epidemiology
Pulmonary Embolectomy: Recommendation for early surgical intervention Tomas A. Salerno, M.D. Professor of Surgery, University of Miami Miller School of Medicine and Jackson Memorial Hospital Epidemiology
Diagnosis and Treatment of Pulmonary Embolism: High-Tech versus Low- Tech, which way to go?
 Diagnosis and Treatment of Pulmonary Embolism: High-Tech versus Low- Tech, which way to go? Philip S. Wells MD, FRCPC, MSc Professor Chair and Chief, Department of Medicine, University of Ottawa DISCLOSURE
Diagnosis and Treatment of Pulmonary Embolism: High-Tech versus Low- Tech, which way to go? Philip S. Wells MD, FRCPC, MSc Professor Chair and Chief, Department of Medicine, University of Ottawa DISCLOSURE
Pulmonary Embolism Response to Fragmentation, Embolectomy, and Catheter Thrombolysis (PERFECT) Initial Results From a Prospective Multicenter Registry
 Initial Results From a Prospective Multicenter Registry") [ Original Research Pulmonary Vascular Disease ] Pulmonary Embolism Response to Fragmentation, Embolectomy, and Catheter Thrombolysis (PERFECT) Initial Results From a Prospective Multicenter Registry William
[ Original Research Pulmonary Vascular Disease ] Pulmonary Embolism Response to Fragmentation, Embolectomy, and Catheter Thrombolysis (PERFECT) Initial Results From a Prospective Multicenter Registry William
Recognizing the Need to Support A Failing Right Ventricular Role of Mechanical Support
 Recognizing the Need to Support A Failing Right Ventricular Role of Mechanical Support Mahir Elder, MD, FACC,SCAI Medical Direct of PERT program Medical Director of Endovascular medicine Clinical Professor
Recognizing the Need to Support A Failing Right Ventricular Role of Mechanical Support Mahir Elder, MD, FACC,SCAI Medical Direct of PERT program Medical Director of Endovascular medicine Clinical Professor
Emergency Pulmonary Embolectomy after Failed Thrombolysis in a Community Hospital: A Choice of Institutional Preference?
 ISPUB.COM The Internet Journal of Emergency Medicine Volume 5 Number 1 Emergency Pulmonary Embolectomy after Failed Thrombolysis in a Community Hospital: A Choice of F Vandy, G Fromm, P Guentert, W Halloran,
ISPUB.COM The Internet Journal of Emergency Medicine Volume 5 Number 1 Emergency Pulmonary Embolectomy after Failed Thrombolysis in a Community Hospital: A Choice of F Vandy, G Fromm, P Guentert, W Halloran,
Sachin Kumar Amruthlal Jain, 1 Brijesh Patel, 2 Wadie David, 2 Ayad Jazrawi, 1 and Patrick Alexander Introduction
 Hindawi Publishing Corporation Case Reports in Medicine Volume 2014, Article ID 297951, 8 pages http://dx.doi.org/10.1155/2014/297951 Case Report Unloading of Right Ventricle and Clinical Improvement after
Hindawi Publishing Corporation Case Reports in Medicine Volume 2014, Article ID 297951, 8 pages http://dx.doi.org/10.1155/2014/297951 Case Report Unloading of Right Ventricle and Clinical Improvement after
PE is a difficult diagnosis that may be missed because of non-specific clinical presentation.
 Pulmonary embolism (PE) is a relatively common cardiovascular emergency. By occluding the pulmonary arterial bed it may lead to acute life-threatening (3% early mortality rate), but potentially reversible
Pulmonary embolism (PE) is a relatively common cardiovascular emergency. By occluding the pulmonary arterial bed it may lead to acute life-threatening (3% early mortality rate), but potentially reversible
Τί κάνουμε όταν πάσχει η δεξιά κοιλία Οξεία πνευμονική εμβολή. Βασίλειος Σαχπεκίδης Επιμελητής Α Καρδιολογίας Γ.Ν.Θ. Παπαγεωργίου
 Τί κάνουμε όταν πάσχει η δεξιά κοιλία Οξεία πνευμονική εμβολή Βασίλειος Σαχπεκίδης Επιμελητής Α Καρδιολογίας Γ.Ν.Θ. Παπαγεωργίου No conflicts of interest RV anatomy Ho SY and Nihoyannopoulos P. Heart 2006;92
Τί κάνουμε όταν πάσχει η δεξιά κοιλία Οξεία πνευμονική εμβολή Βασίλειος Σαχπεκίδης Επιμελητής Α Καρδιολογίας Γ.Ν.Θ. Παπαγεωργίου No conflicts of interest RV anatomy Ho SY and Nihoyannopoulos P. Heart 2006;92
PE Pathway. The charts are listed as follows:
 PE Pathway This document comprises 6 simple flow charts to assist clinicians in the investigation and treatment of suspected or confirmed Acute Pulmonary Emboli. The pathway has been put together using
PE Pathway This document comprises 6 simple flow charts to assist clinicians in the investigation and treatment of suspected or confirmed Acute Pulmonary Emboli. The pathway has been put together using
Μακροχρόνια παρακολούθηση ασθενών με πνευμονική εμβολή
 Μακροχρόνια παρακολούθηση ασθενών με πνευμονική εμβολή Ευφροσύνη Δ. Μάναλη Λέκτορας Β Πανεπιστημιακή Πνευμονολογική Κλινική ΓΝΑ «Αττικόν» Εθνικό και Καποδιστριακό Πανεπιστήμιο Αθηνών Existing guidelines
Μακροχρόνια παρακολούθηση ασθενών με πνευμονική εμβολή Ευφροσύνη Δ. Μάναλη Λέκτορας Β Πανεπιστημιακή Πνευμονολογική Κλινική ΓΝΑ «Αττικόν» Εθνικό και Καποδιστριακό Πανεπιστήμιο Αθηνών Existing guidelines
Clinical Practice Statement. What is the Role of Thrombolysis in Intermediate Risk Pulmonary Embolism?
 Clinical Practice Statement What is the Role of Thrombolysis in Intermediate Risk Pulmonary Embolism? Co-Chairs: Authors: Steve Rosenbaum, MD FAAEM Michael Abraham, MD FAAEM David Pillus, MD FAAEM Eric
Clinical Practice Statement What is the Role of Thrombolysis in Intermediate Risk Pulmonary Embolism? Co-Chairs: Authors: Steve Rosenbaum, MD FAAEM Michael Abraham, MD FAAEM David Pillus, MD FAAEM Eric
Severe pulmonary embolism: surgical aspects. Oliver Reuthebuch Clinic for Cardiac Surgery University Hospital Basel Switzerland
 Severe pulmonary embolism: surgical aspects Oliver Reuthebuch Clinic for Cardiac Surgery University Hospital Basel Switzerland Severe pulmonary embolism Acute pulmonary embolism Chronic pulmonary thromboembolism
Severe pulmonary embolism: surgical aspects Oliver Reuthebuch Clinic for Cardiac Surgery University Hospital Basel Switzerland Severe pulmonary embolism Acute pulmonary embolism Chronic pulmonary thromboembolism
Pulmonary and Critical Care Year in Review
 Pulmonary and Critical Care Year in Review Heath E Latham, MD Assistant Professor University of Kansas Dept of Internal Medicine Division of Pulmonary and Critical Care None Disclosure Lung Cancer Screening
Pulmonary and Critical Care Year in Review Heath E Latham, MD Assistant Professor University of Kansas Dept of Internal Medicine Division of Pulmonary and Critical Care None Disclosure Lung Cancer Screening
Anjali Vaidya, MD, FACC, FASE, FACP Associate Director, Pulmonary Hypertension, Right Heart Failure, Pulmonary Thromboendarterectomy Program Advanced
 Anjali Vaidya, MD, FACC, FASE, FACP Associate Director, Pulmonary Hypertension, Right Heart Failure, Pulmonary Thromboendarterectomy Program Advanced Heart Failure & Cardiac Transplant Temple University
Anjali Vaidya, MD, FACC, FASE, FACP Associate Director, Pulmonary Hypertension, Right Heart Failure, Pulmonary Thromboendarterectomy Program Advanced Heart Failure & Cardiac Transplant Temple University
The Evidence Base for Treating Acute DVT
 The Evidence Base for Treating Acute DVT Mr Chung Sim Lim Consultant Vascular Surgeon and Honorary Lecturer Royal Free London NHS Foundation Trust and University College London NIHR UCLH Biomedical Research
The Evidence Base for Treating Acute DVT Mr Chung Sim Lim Consultant Vascular Surgeon and Honorary Lecturer Royal Free London NHS Foundation Trust and University College London NIHR UCLH Biomedical Research
Pulmonary Hypertension: When to Initiate Advanced Therapy. Jonathan D. Rich, MD Associate Professor of Medicine Northwestern University
 Pulmonary Hypertension: When to Initiate Advanced Therapy Jonathan D. Rich, MD Associate Professor of Medicine Northwestern University Disclosures Medtronic, Abbott: Consultant Hemodynamic Definition of
Pulmonary Hypertension: When to Initiate Advanced Therapy Jonathan D. Rich, MD Associate Professor of Medicine Northwestern University Disclosures Medtronic, Abbott: Consultant Hemodynamic Definition of
4/24/2017 CATHETER-DIRECTED THERAPIES FOR ACUTE PE THE GREY AREA OF SUBMASSIVE PE DISCLOSURES OBJECTIVES: INTRAVASCULAR LYTIC THERAPY
 THE GREY AREA OF SUBMASSIVE PE CATHETER-DIRECTED THERAPIES FOR ACUTE PE Submassive PE PE with RV strain Saad Farooqi, MD Pulmonary/Critical Care Fellow Fatal PE Concept borrowed from Jeffrey A. Kline,
THE GREY AREA OF SUBMASSIVE PE CATHETER-DIRECTED THERAPIES FOR ACUTE PE Submassive PE PE with RV strain Saad Farooqi, MD Pulmonary/Critical Care Fellow Fatal PE Concept borrowed from Jeffrey A. Kline,
Year in Review 2014: Critical Care Medicine
 Disclosures Year in Review 2014: Critical Care Medicine I receive laboratory support from CytoVale Diagnostics for research on early sepsis diagnostics Eric J. Seeley, M.D., F.C.C.P. Assistant Professor
Disclosures Year in Review 2014: Critical Care Medicine I receive laboratory support from CytoVale Diagnostics for research on early sepsis diagnostics Eric J. Seeley, M.D., F.C.C.P. Assistant Professor
Case Report Free Floating Right Heart Thrombus Associated with Acute Pulmonary Embolism: An Unsettled Therapeutic Difficulty
 Case Reports in Cardiology Volume 2015, Article ID 364780, 4 pages http://dx.doi.org/10.1155/2015/364780 Case Report Free Floating Right Heart Thrombus Associated with Acute Pulmonary Embolism: An Unsettled
Case Reports in Cardiology Volume 2015, Article ID 364780, 4 pages http://dx.doi.org/10.1155/2015/364780 Case Report Free Floating Right Heart Thrombus Associated with Acute Pulmonary Embolism: An Unsettled
Real life management of CTEPH: patient case
 2 nd International Congress on cardiovascular imaging in clinical practice k Real life management of CTEPH: patient case Anastasia Anthi Pulmonary Hypertension Clinic, Attikon University Hospital, Athens
2 nd International Congress on cardiovascular imaging in clinical practice k Real life management of CTEPH: patient case Anastasia Anthi Pulmonary Hypertension Clinic, Attikon University Hospital, Athens
Respiratory Review of 2014: Pulmonary Thromboembolism
 REVIEW http://dx.doi.org/10.4046/trd.2014.77.3.105 ISSN: 1738-3536(Print)/2005-6184(Online) Tuberc Respir Dis 2014;77:105-110 Respiratory Review of 2014: Pulmonary Thromboembolism Jae Seung Lee, M.D. Department
REVIEW http://dx.doi.org/10.4046/trd.2014.77.3.105 ISSN: 1738-3536(Print)/2005-6184(Online) Tuberc Respir Dis 2014;77:105-110 Respiratory Review of 2014: Pulmonary Thromboembolism Jae Seung Lee, M.D. Department
The shock index and the simplified PESI for identification of low-risk patients with acute pulmonary embolism
 Eur Respir J 211; 37: 762 766 DOI: 1.1183/931936.711 CopyrightßERS 211 The shock index and the simplified PESI for identification of low-risk patients with acute pulmonary embolism A. Sam*, D. Sánchez*,
Eur Respir J 211; 37: 762 766 DOI: 1.1183/931936.711 CopyrightßERS 211 The shock index and the simplified PESI for identification of low-risk patients with acute pulmonary embolism A. Sam*, D. Sánchez*,
Pulmonary Embolism Newer Concepts and Role of Thrombolysis
 CHAPTER 69 Pulmonary Embolism Newer Concepts and Role of Thrombolysis J. P. S. Sawhney, A. Bakhshi, B. Kandpal Introduction Pulmonary embolism (PE) is a common cardiovascular and cardiopulmonary illness
CHAPTER 69 Pulmonary Embolism Newer Concepts and Role of Thrombolysis J. P. S. Sawhney, A. Bakhshi, B. Kandpal Introduction Pulmonary embolism (PE) is a common cardiovascular and cardiopulmonary illness
Catheter Based Therapy for PE: Who and How?
 Catheter Based Therapy for PE: Who and How? Jay Giri, MD MPH Assistant Professor of Medicine Director, Pulmonary Embolism Response Team Associate Director, Penn Cardiovascular Quality, Outcomes & Evaluative
Catheter Based Therapy for PE: Who and How? Jay Giri, MD MPH Assistant Professor of Medicine Director, Pulmonary Embolism Response Team Associate Director, Penn Cardiovascular Quality, Outcomes & Evaluative
6 th Annual Scientific Sessions Georgia Vascular Society Reynolds Plantation, Lake Oconee 9/15/2018
 Current Outcomes of Management of Massive Pulmonary Embolism Achieved by a Multidisciplinary Pulmonary Embolism Response Team in a Quaternary Referral Center Presentation Sponsor: Charles B. Ross, M.D.,
Current Outcomes of Management of Massive Pulmonary Embolism Achieved by a Multidisciplinary Pulmonary Embolism Response Team in a Quaternary Referral Center Presentation Sponsor: Charles B. Ross, M.D.,
Acute pulmonary embolism: endovascular therapy
 Review Article Acute pulmonary embolism: endovascular therapy Stephen P. Reis 1, Ken Zhao 2, Noor Ahmad 3, Reginald S. Widemon 4, Christopher W. Root 5, Seth M. Toomay 6, James M. Horowitz 7, Akhilesh
Review Article Acute pulmonary embolism: endovascular therapy Stephen P. Reis 1, Ken Zhao 2, Noor Ahmad 3, Reginald S. Widemon 4, Christopher W. Root 5, Seth M. Toomay 6, James M. Horowitz 7, Akhilesh
ORIGINAL INVESTIGATION. Thrombolytic Therapy and Mortality in Patients With Acute Pulmonary Embolism
 ORIGINAL INVESTIGATION Thrombolytic Therapy and in Patients With Acute Pulmonary Embolism Said A. Ibrahim, MD, MPH; Roslyn A. Stone, PhD; D. Scott Obrosky, MSc; Ming Geng, MSc; Michael J. Fine, MD, MSc;
ORIGINAL INVESTIGATION Thrombolytic Therapy and in Patients With Acute Pulmonary Embolism Said A. Ibrahim, MD, MPH; Roslyn A. Stone, PhD; D. Scott Obrosky, MSc; Ming Geng, MSc; Michael J. Fine, MD, MSc;
Takotsubo syndrome. Ευτυχία Σμπαρούνη, FACC, FESC
 Takotsubo syndrome Ευτυχία Σμπαρούνη, FACC, FESC Definition Takotsubo Apical ballooning Broken heart syndrome Stress cardiomyopathy Cathecholaminergic cardiomyopathy Epidemiology 1990 first report by Japanese
Takotsubo syndrome Ευτυχία Σμπαρούνη, FACC, FESC Definition Takotsubo Apical ballooning Broken heart syndrome Stress cardiomyopathy Cathecholaminergic cardiomyopathy Epidemiology 1990 first report by Japanese
A 50-year-old woman with syncope
 Hira Shahzad 1, Ali Bin Sarwar Zubairi 2 1 Medical College, Aga Khan University Hospital, Karachi 2 Department of Medicine, Aga Khan University Hospital, Karachi, Pakistan Ali Bin Sarwar Zubairi Associate
Hira Shahzad 1, Ali Bin Sarwar Zubairi 2 1 Medical College, Aga Khan University Hospital, Karachi 2 Department of Medicine, Aga Khan University Hospital, Karachi, Pakistan Ali Bin Sarwar Zubairi Associate
Thrombolysis for submassive pulmonary embolus
 LITFL Google Search ABOUT BLOG ARCHIVE CONTACT LITFL Critical Care Compendium Thrombolysis for submassive pulmonary embolus Thrombolysis for submassive pulmonary embolus Tweet 0 Like 0 Share 0 Reviewed
LITFL Google Search ABOUT BLOG ARCHIVE CONTACT LITFL Critical Care Compendium Thrombolysis for submassive pulmonary embolus Thrombolysis for submassive pulmonary embolus Tweet 0 Like 0 Share 0 Reviewed
Pulmonary Embolism: Scope of the Problem
 Pulmonary Embolism: Scope of the Problem Rachel P. Rosovsky, MD, MPH Director, Thrombosis Research, Hematology, Massachusetts General Hospital Assistant Professor of Medicine, Harvard Medical School Disclosures
Pulmonary Embolism: Scope of the Problem Rachel P. Rosovsky, MD, MPH Director, Thrombosis Research, Hematology, Massachusetts General Hospital Assistant Professor of Medicine, Harvard Medical School Disclosures