The Future of EMS as Revealed through Research. A Window into the Near Future
|
|
|
- Cordelia Russell
- 5 years ago
- Views:
Transcription

1 The Future of EMS as Revealed through Research A Window into the Near Future
2 Raymond L. Fowler, M.D., FACEP Co-Principal Investigator National Institutes of Health Resuscitation Outcomes Consortium Joint Investigator National Heart, Lung, and Blood Institute IMMEDIATE Trial Medical Director of Douglas County Fire Department and Mid Georgia Ambulance Service Deputy Medical Director Dallas Area BioTel System
3

4 The emerging of a subspecialty: EMS Medicine
5 Approaching the Patient
6 See what you see! People look, but they don t t see A. Fowler, Jr.

7 Alertness? Level of distress? Noises? Respirations? The pulse rate? Skin? Obvious things (bleeding)

8 Our pulse can only go so fast under sympathetic stimulation: 220 minus age
9 Baby = (220 0) = 220 Snerd = (220 53) = 167 Aunt Minnie = (220 70) = 150

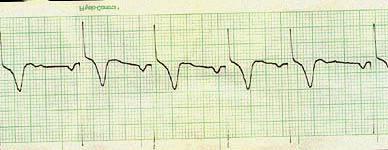
10 What is this rhythm? = 165 Correct answer: It COULD be sinus tach

11 What is this rhythm? = 160 Correct answer: This HAS to be an arrhythmia
12 If you forget everything else that I say: Remember that patients having near maximum sinus tachycardia at rest are dying!
13 A physiological response
14 Hemorrhagic Something shock Sepsis mobilizing a Tension massive Tamponade Ruptured aorta Ruptured ectopic Massive P.E. physiological response
15 Your job is to determine if a rapid rhythm MAY be sinus tach If it is, you must take action



16 Speaking of Adenosine
17 Because so many EMS courses are too long, too boring, and teach difficult concepts to medics who will never use that information

18

19
20 Airway Breathing Circulation Drugs Disaster Electrocardiography
21 Airway
22 It is not at all clear what the best airway devices are now or what they will be
23
24
25

26
27
28
29
30
31
32
33
34
35
36
37 What does all of this mean?
38 Endotracheal intubation in the field may be rarely indicated
39 Endotracheal intubation in the field may be harmful indeed, if you tracked your own survival data, you would likely find that people were less likely to survive with Field ETI
40 Why?
41 Field ETI Prolonged attempts Hypoxia during attempts Multiple attempts Aspiration during attempts Hyperventilation AFTER intubation Instrumenting the airway in critical patients
42 Example Medic reports to Medical Director that an elderly patient in respiratory distress was cared for in the field, given nebs and oxygen, improved to GCS 8 On arrival to ED, Doc takes one look at her and makes 8 attempts to intubate her, during which she bradys down and dies
43 Example What does that mean? Did that patient need to be intubated who was improving with oxygen and supportive care?
44 Fowler s Maxim The First Five Minutes
45 Fowler s Maxim In some patients you have to act right now: Airway obstruction Exsanguination Cardiac Arrest Profound respiratory distress Shock
46 Fowler s Maxim In most patients, you have five minutes The patient who seems stable for the moment, with a decent pressure, with a decent pulse ox, whose airway is not immediately threatened TAKE A MINUTE OR TWO TO THINK
47 Delaney s Corollary If it took them a couple of days or more to get sick, then you probably have at least five minutes to stop and think While you re getting oxygen, IV s, other supportive care, arranging for transport to the appropriate facility
48 The Airway of the future will be fast, effective, and virtually hazard free Avoiding airway trauma Virtually always goes in Easy to train Easy to remember
49 The Easy Tube
50 The Easy Tube
51 The Airway of the future will be fast, effective, and virtually hazard free
52 Breathing and Circulation
53 Resuscitation Outcomes Consortium A consortium of ten cities and states across North America designated by the National Institutes of Health to be the largest EMS research group in the history of medicine
54 Resuscitation Outcomes Consortium Will be initially looking at hypertonic saline infusions for traumatic brain injury and hemorrhagic shock due to trauma Already in use in the military, just not studied in large civilian populations
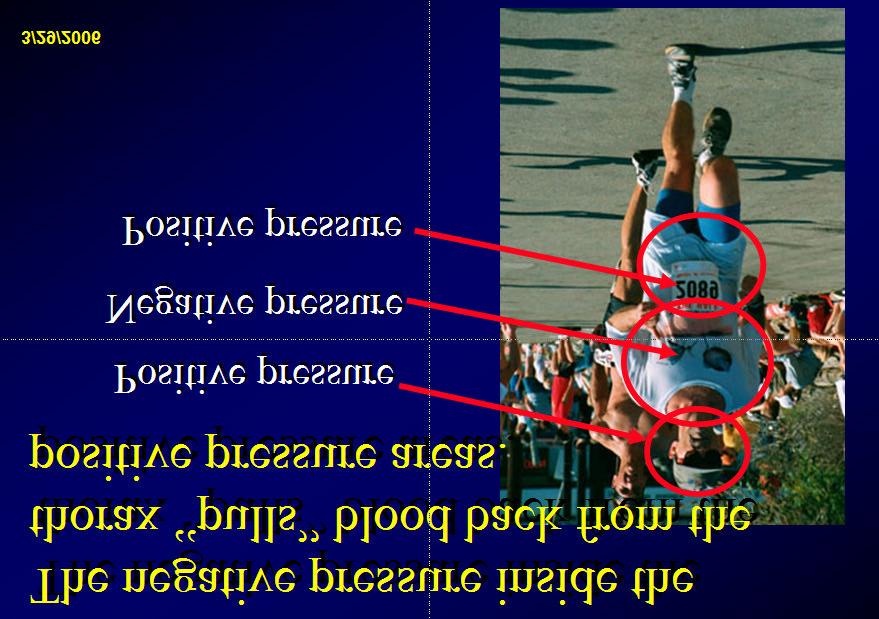
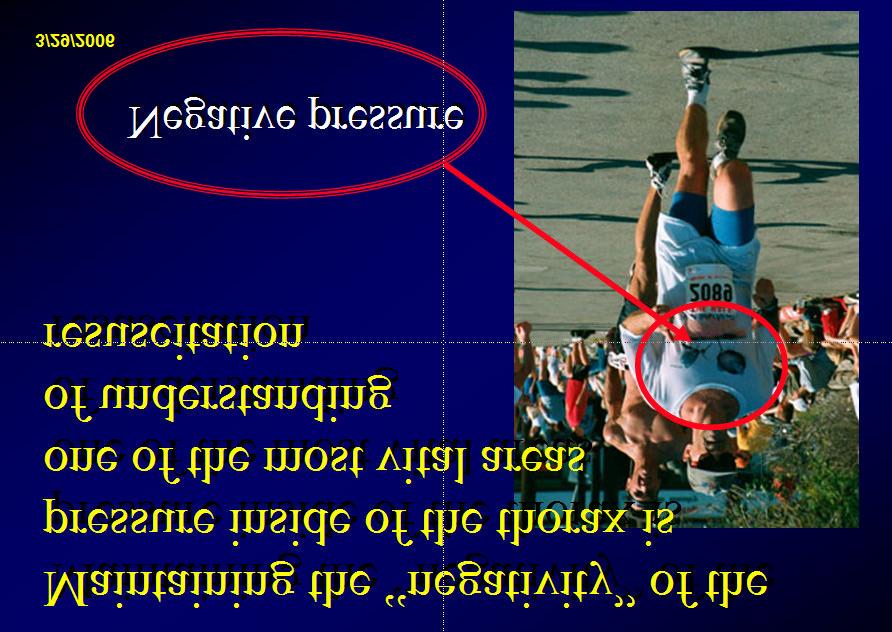
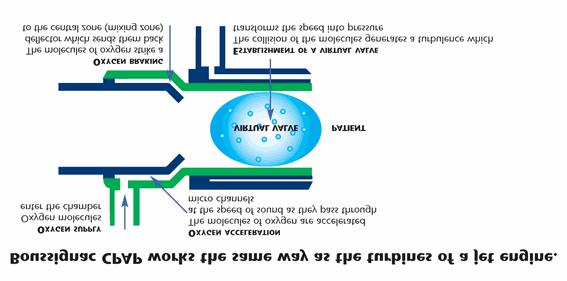
55 Resuscitation Outcomes Consortium Will next look at the Impedance Threshold Device to improve negative intrathoracic pressure during cardiac compressions
56 Resuscitation Outcomes Consortium Impedance Threshold Device Turns chest compressions from a one stroke engine to a two stroke engine
57 Resuscitation Outcomes Consortium Impedance Threshold Device Makes use of chest recoil with tiny, momentary airway occlusion to increase venous return
58 Resuscitation Outcomes Consortium Impedance Threshold Device Essentially normalizes blood pressure during chest compressions
59

60

61
62
63
64
65 Signs of Shock Early Late Weak, thirsty, lightheaded Pale, then sweaty Tachycardia Tachypnea Diminished urinary output Hypotension Altered LOC Cardiac arrest Death

66 What does a low blood pressure mean? Either... Loss of of volume Low Or a cardiac combination output Increased of any of vascular these space from BTLS, editions 2, 3, 4, and 5 Fowler et al
67 Shock Cardiogenic Rapid pulse Distended neck veins Cyanosis Volume Loss Rapid pulse Flat neck veins Pale Vasodilatory Variable pulse Flat neck veins Pale or or pink
68 We have been overventilating patients in circulatory collapse to death for years, without knowing it After all, if a little oxygen is GOOD, more is better, right?
69 WRONG!
70 Overventilation raises intrathoracic pressure, decreasing venous return, and dropping cardiac output

71
72 If you drop venous return, cardiac output drops That is, if the pump can t fill, then the pump can t pump
73 Research is clear on the fact that medics (and all providers) bag patients too fast with too big of a squeeze and too fast on the squeeze
74 Slow down the rate of ventilation until capnography begins to rise Maintain a minute ventilation of approximately five liters and see where capnography goes from there One hand squeeze every 8 seconds

75 CPAP
76

77
78 What about the AutoPulse?
79 Drugs and ECG s
80 Drugs It is clear that overventilation has changed patient outcomes over the years and prevented us from seeing what drugs could
81 Which Drugs to Revisit? Antiarrhythmics in arrest Pressors during arrest
82 Future Drugs Artificial hemoglobins? Vasopressin?

83 but just when we thought life was getting easier
84 Electrocardiography 12 Lead Interpretation by medics is now the standard of care even if the 12 lead is NOT on your rig
85 ECG Interpretation Anatomically speaking...
86 SA Bundle of His AV Bundle Branches
87

88 Multifocal Atrial Tachycardia
89 IMMEDIATE Trial
90 IMMEDIATE Trial Medic identifies the Acute Coronary Syndrome through patient History and Physical and through 12 Lead Interpretation Medic gets consent Medic initiates an infusion of Glucose, Insulin, and Potassium in the field to limit incidence of sudden death and infarct size
91 IMMEDIATE Trial Over time EMS will likely be giving medication to limit infarct size and incidence of sudden death This will ultimately increase survival from acute coronary syndrome and decrease the burden of CHF post infarct to patients and the community
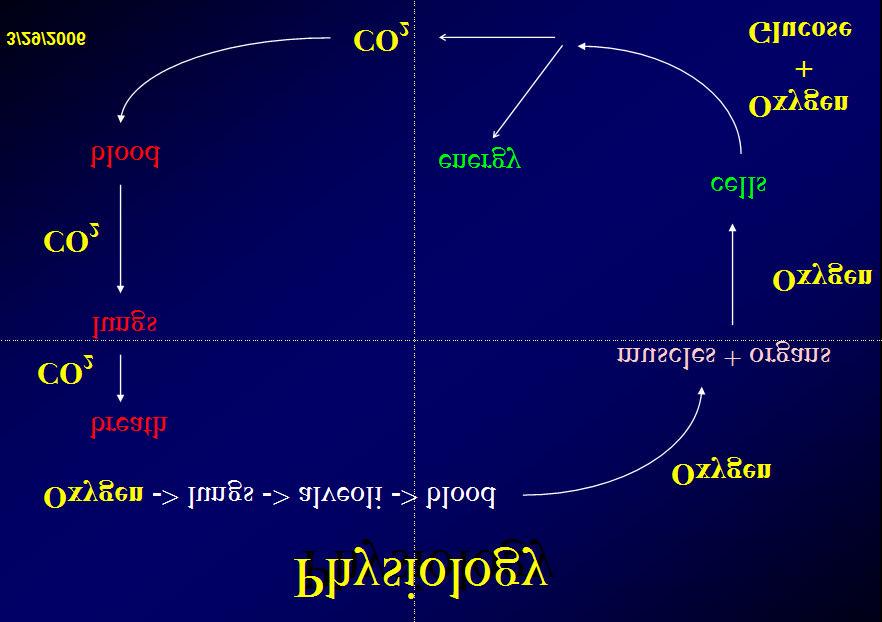
92 IMMEDIATE Trial Turns out that sick tissue likes a little extra insulin around Insulin turns off fat metabolism and turns on carbohydrate metabolism, giving more energy per gram of substrate to sick cells This has been know for over 40 years

93 What is the patient s blood pressure?



94 A 15 year old AA male is is found confused, sweaty, with a respiratory rate of of 36, a systolic pressure of of 80, and this EKG rhythm strip What is is the working impression and what do you think might be the cause of of his problem?
95 60 year old Aunt Minnie presents with systolic of 90 and no cardiac history She has been ill for two days
96 60 year old with rate of = 160 What statement can you make?
97 60 year old with rate of = 160 Does she need Adenosine?

98 Synthesis

99 So, Who s Foolin Who??
100 EMS professionals are primary members of the emergency medical team. The scope of practice of these EMS professionals continues to grow with passing years
101 Let us then apply our best efforts to monitor emerging research with the sharpened focus of clarity and simplification, pooling our individual creativities for the greater good of those we serve.
102 This Talk may be found at

103 ... and Good Morning! Questions or comments?
104
Ruminations about the Past, Present, and Future
 Ruminations about the Past, Present, and Future Raymond L. Fowler, MD, FACEP, DABEMS Professor and Chief Division of Emergency Medical Services Department of Emergency Medicine UT Southwestern Medical
Ruminations about the Past, Present, and Future Raymond L. Fowler, MD, FACEP, DABEMS Professor and Chief Division of Emergency Medical Services Department of Emergency Medicine UT Southwestern Medical
ACLS Prep. Preparation is key to a successful ACLS experience. Please complete the ACLS Pretest and Please complete this ACLS Prep.
 November, 2013 ACLS Prep Preparation is key to a successful ACLS experience. Please complete the ACLS Pretest and Please complete this ACLS Prep. ACLS Prep Preparation is key to a successful ACLS experience.
November, 2013 ACLS Prep Preparation is key to a successful ACLS experience. Please complete the ACLS Pretest and Please complete this ACLS Prep. ACLS Prep Preparation is key to a successful ACLS experience.
Advanced Cardiac Life Support (ACLS) Science Update 2015
 Science Update 2015") 1 2 3 4 5 6 7 8 9 Advanced Cardiac Life Support (ACLS) Science Update 2015 What s New in ACLS for 2015? Adult CPR CPR remains (Compressions, Airway, Breathing Chest compressions has priority over all other
1 2 3 4 5 6 7 8 9 Advanced Cardiac Life Support (ACLS) Science Update 2015 What s New in ACLS for 2015? Adult CPR CPR remains (Compressions, Airway, Breathing Chest compressions has priority over all other
FAILURE. Matt Beecroft, MD
 FAILURE Matt Beecroft, MD 64 yo male with no real PMH Sitting on couch when sudden onset SOB Says he s been sweaty FIRST PATIENT OF THE WEEKEND HR 131, RR 28, 132/96, 93% RE-EXAM BP 229/130, HR 180s
FAILURE Matt Beecroft, MD 64 yo male with no real PMH Sitting on couch when sudden onset SOB Says he s been sweaty FIRST PATIENT OF THE WEEKEND HR 131, RR 28, 132/96, 93% RE-EXAM BP 229/130, HR 180s
3. D Objective: Chapter 4, Objective 4 Page: 79 Rationale: A carbon dioxide level below 35 mmhg indicates hyperventilation.
 1. A Objective: Chapter 1, Objective 3 Page: 14 Rationale: The sudden increase in acceleration produces posterior displacement of the occupants and possible hyperextension of the cervical spine if the
1. A Objective: Chapter 1, Objective 3 Page: 14 Rationale: The sudden increase in acceleration produces posterior displacement of the occupants and possible hyperextension of the cervical spine if the
Prehospital Resuscitation for the 21 st Century Simulation Case. VF/Asystole
 Prehospital Resuscitation for the 21 st Century Simulation Case VF/Asystole Case History 1 (hypovolemic cardiac arrest secondary to massive upper GI bleed) 56 year-old male patient who fainted in the presence
Prehospital Resuscitation for the 21 st Century Simulation Case VF/Asystole Case History 1 (hypovolemic cardiac arrest secondary to massive upper GI bleed) 56 year-old male patient who fainted in the presence
Hypotension / Shock. Adult Medical Section Protocols. Protocol 30
 Hypotension / Shock History Blood loss - vaginal or gastrointestinal bleeding, AAA, ectopic Fluid loss - vomiting, diarrhea, fever nfection Cardiac ischemia (M, CHF) Medications Allergic reaction regnancy
Hypotension / Shock History Blood loss - vaginal or gastrointestinal bleeding, AAA, ectopic Fluid loss - vomiting, diarrhea, fever nfection Cardiac ischemia (M, CHF) Medications Allergic reaction regnancy
Written 01/09/17 Rewritten 3/29/17 for Interior Regional EMS Symposium
 Written 01/09/17 Rewritten 3/29/17 for Interior Regional EMS Symposium MARIA E. MANDICH MD Fairbanks Memorial Hospital Emergency Department Attending Physician Interior Region EMS Council Medical Director
Written 01/09/17 Rewritten 3/29/17 for Interior Regional EMS Symposium MARIA E. MANDICH MD Fairbanks Memorial Hospital Emergency Department Attending Physician Interior Region EMS Council Medical Director
1 Pediatric Advanced Life Support Science Update What s New for 2010? 3 CPR. 4 4 Steps of BLS Survey 5 CPR 6 CPR.
 1 Pediatric Advanced Life Support Science Update 2010 2 What s New for 2010? 3 CPR Take no longer than seconds for pulse check Rate at least on per minute (instead of around 100 per minute ) Depth change:
1 Pediatric Advanced Life Support Science Update 2010 2 What s New for 2010? 3 CPR Take no longer than seconds for pulse check Rate at least on per minute (instead of around 100 per minute ) Depth change:
Algorithm Focus. Emergency Cardiovascular Care: EMT-Intermediate Treatment Algorithms. Perspective regarding the EMT- Intermediate algorithms
 Emergency Cardiovascular Care: EMT-Intermediate Treatment Algorithms Algorithms for the Conscious Patient Prehospital Medication Profiles Algorithm Focus Bradycardia Acute Pulmonary Edema and Shock Hypothermia
Emergency Cardiovascular Care: EMT-Intermediate Treatment Algorithms Algorithms for the Conscious Patient Prehospital Medication Profiles Algorithm Focus Bradycardia Acute Pulmonary Edema and Shock Hypothermia
SHOCK AETIOLOGY OF SHOCK (1) Inadequate circulating blood volume ) Loss of Autonomic control of the vasculature (3) Impaired cardiac function
 Inadequate circulating blood volume ) Loss of Autonomic control of the vasculature (3) Impaired cardiac function") SHOCK Shock is a condition in which the metabolic needs of the body are not met because of an inadequate cardiac output. If tissue perfusion can be restored in an expeditious fashion, cellular injury may
SHOCK Shock is a condition in which the metabolic needs of the body are not met because of an inadequate cardiac output. If tissue perfusion can be restored in an expeditious fashion, cellular injury may
Michigan Pediatric Cardiac Protocols. Date: November 15, 2012 Page 1 of 1 TABLE OF CONTENTS
 Date: November 15, 2012 Page 1 of 1 TABLE OF CONTENTS Pediatric Asystole Section 4-1 Pediatric Bradycardia Section 4-2 Pediatric Cardiac Arrest General Section 4-3 Pediatric Narrow Complex Tachycardia
Date: November 15, 2012 Page 1 of 1 TABLE OF CONTENTS Pediatric Asystole Section 4-1 Pediatric Bradycardia Section 4-2 Pediatric Cardiac Arrest General Section 4-3 Pediatric Narrow Complex Tachycardia
Cardiac Emergencies. A Review of Cardiac Compromise. Lawrence L. Lambert
 Cardiac Emergencies A Review of Cardiac Compromise Lawrence L. Lambert 1 Cardiac Emergencies Objectives: Following successful completion of this training session, the student should be able to: 1. Describe
Cardiac Emergencies A Review of Cardiac Compromise Lawrence L. Lambert 1 Cardiac Emergencies Objectives: Following successful completion of this training session, the student should be able to: 1. Describe
Surgical Care at the District Hospital. EMERGENCY & ESSENTIAL SURGICAL CARE
 Surgical Care at the District Hospital 1 13 Resuscitation and Preparation for Anesthesia & Surgery Key Points 2 13.1 Management of Emergencies and Cardiopulmonary Resuscitation The emergency measures that
Surgical Care at the District Hospital 1 13 Resuscitation and Preparation for Anesthesia & Surgery Key Points 2 13.1 Management of Emergencies and Cardiopulmonary Resuscitation The emergency measures that
ACLS Review. Pulse Oximetry to be between 94 99% to avoid hyperoxia (high oxygen tension can lead to tissue death
 ACLS Review BLS CPR BLS CPR changed in 2010. The primary change is from the ABC format to CAB. After establishing unresponsiveness and calling for a code, check for a pulse less than 10 seconds then begin
ACLS Review BLS CPR BLS CPR changed in 2010. The primary change is from the ABC format to CAB. After establishing unresponsiveness and calling for a code, check for a pulse less than 10 seconds then begin
Scene Safety First always first, your safety is above everything else, hands only CPR (use pocket
 BLS BASICS: Scene Safety First always first, your safety is above everything else, hands only CPR (use pocket facemask or AMBU bag) Adults call it in, start CPR, get AED Child CPR First, Phone call second
BLS BASICS: Scene Safety First always first, your safety is above everything else, hands only CPR (use pocket facemask or AMBU bag) Adults call it in, start CPR, get AED Child CPR First, Phone call second
ITLS Advanced Pre-Test Annotated Key 8 th Edition
 1. A Objective: Chapter 1, Objective 3 Page: 14 Rationale: The sudden increase in acceleration produces posterior displacement of the occupants and possible hyperextension of the cervical spine if the
1. A Objective: Chapter 1, Objective 3 Page: 14 Rationale: The sudden increase in acceleration produces posterior displacement of the occupants and possible hyperextension of the cervical spine if the
Cardiovascular Disorders. Heart Disorders. Diagnostic Tests for CV Function. Bio 375. Pathophysiology
 Cardiovascular Disorders Bio 375 Pathophysiology Heart Disorders Heart disease is ranked as a major cause of death in the U.S. Common heart diseases include: Congenital heart defects Hypertensive heart
Cardiovascular Disorders Bio 375 Pathophysiology Heart Disorders Heart disease is ranked as a major cause of death in the U.S. Common heart diseases include: Congenital heart defects Hypertensive heart
PALS Case Scenario Testing Checklist Respiratory Case Scenario 1 Upper Airway Obstruction
 Respiratory Case Scenario 1 Upper Airway Obstruction Directs administration of 100% oxygen or supplementary oxygen as needed to support oxygenation Identifies signs and symptoms of upper airway obstruction
Respiratory Case Scenario 1 Upper Airway Obstruction Directs administration of 100% oxygen or supplementary oxygen as needed to support oxygenation Identifies signs and symptoms of upper airway obstruction
Shock Kills! By the time you see it, it is probably too late! Contact Information. Overview
 Contact Information Tim Hillier, EMT-P Director of Professional Development M.D. Ambulance Saskatoon, SK (306) 975-8825 (Office) t.hillier@mdambulance.com Tim Hillier, EMT-P Shock Kills! By the time you
Contact Information Tim Hillier, EMT-P Director of Professional Development M.D. Ambulance Saskatoon, SK (306) 975-8825 (Office) t.hillier@mdambulance.com Tim Hillier, EMT-P Shock Kills! By the time you
ETCO2 MONITORING NON-INTUBATED PATIENTS
 Although the standard of care in ETC02 is well established for intubated patients, there has been little emphasis on the use of capnography in nonintubated patients till now. In addition to confirming
Although the standard of care in ETC02 is well established for intubated patients, there has been little emphasis on the use of capnography in nonintubated patients till now. In addition to confirming
Pediatric Assessment Triangle
 Pediatric Assessment Triangle Katherine Remick, MD, FAAP Associate Medical Director Austin Travis County EMS Pediatric Emergency Medicine Dell Children s Medical Center Objectives 1. Discuss why the Pediatric
Pediatric Assessment Triangle Katherine Remick, MD, FAAP Associate Medical Director Austin Travis County EMS Pediatric Emergency Medicine Dell Children s Medical Center Objectives 1. Discuss why the Pediatric
Michigan Pediatric Cardiac Protocols. Date: November 15, 2012 Page 1 of 1 TABLE OF CONTENTS
 Date: November 15, 2012 Page 1 of 1 TABLE OF CONTENTS Pediatric Asystole Section 4-1 Pediatric Bradycardia Section 4-2 Pediatric Cardiac Arrest General Section 4-3 Pediatric Narrow Complex Tachycardia
Date: November 15, 2012 Page 1 of 1 TABLE OF CONTENTS Pediatric Asystole Section 4-1 Pediatric Bradycardia Section 4-2 Pediatric Cardiac Arrest General Section 4-3 Pediatric Narrow Complex Tachycardia
TEACHING BASIC LIFE SUPPORT (& ALS)
") TEACHING BASIC LIFE SUPPORT (& ALS) Anton Koželj, R.N., B. Sc., lecturer Faculty of Health Sciences, University of Maribor Žitna ulica 15, 2000 Maribor, Slovenia Fact s To know-how to perform basic life
TEACHING BASIC LIFE SUPPORT (& ALS) Anton Koželj, R.N., B. Sc., lecturer Faculty of Health Sciences, University of Maribor Žitna ulica 15, 2000 Maribor, Slovenia Fact s To know-how to perform basic life
Chapter 11 - The Primary Assessment
 Introduction to Emergency Medical Care 1 OBJECTIVES 11.1 Define key terms introduced in this chapter. Slides 11 12, 14, 19 21, 28 11.2 Explain the purpose of the primary assessment. Slides 11 13 OBJECTIVES
Introduction to Emergency Medical Care 1 OBJECTIVES 11.1 Define key terms introduced in this chapter. Slides 11 12, 14, 19 21, 28 11.2 Explain the purpose of the primary assessment. Slides 11 13 OBJECTIVES
INSTITUTE FOR MEDICAL SIMULATION & EDUCATION ACLS PRACTICAL SCENARIOS
 Practical Teaching for Respiratory Arrest with a Pulse (Case 1) You are a medical officer doing a pre-operative round when 60-year old patient started coughing violently and becomes unconscious. Fortunately
Practical Teaching for Respiratory Arrest with a Pulse (Case 1) You are a medical officer doing a pre-operative round when 60-year old patient started coughing violently and becomes unconscious. Fortunately
Prehospital Care Bundles
 Prehospital s The MLREMS Prehospital s have been created to provide a simple framework to help EMS providers identify the most critical elements when caring for a patient. These bundles do not replace
Prehospital s The MLREMS Prehospital s have been created to provide a simple framework to help EMS providers identify the most critical elements when caring for a patient. These bundles do not replace
Hanna K. Al-Makhamreh, M.D., FACC Interventional Cardiologist
 Hanna K. Al-Makhamreh, M.D., FACC Interventional Cardiologist Introduction. Basic Life Support (BLS). Advanced Cardiac Life Support (ACLS). Cardiovascular diseases (CVDs) are the number one cause of death
Hanna K. Al-Makhamreh, M.D., FACC Interventional Cardiologist Introduction. Basic Life Support (BLS). Advanced Cardiac Life Support (ACLS). Cardiovascular diseases (CVDs) are the number one cause of death
Resuscitation Checklist
 Resuscitation Checklist Actions if multiple responders are on scene Is resuscitation appropriate? Conditions incompatible with life Advanced decision in place Based on the information available, the senior
Resuscitation Checklist Actions if multiple responders are on scene Is resuscitation appropriate? Conditions incompatible with life Advanced decision in place Based on the information available, the senior
Preparing for your upcoming PALS course
 IU Health PALS Study Guide Preparing for your upcoming PALS course UPDATED November 2016 Course Curriculum: 2015 American Heart Association (AHA) Guidelines for Pediatric Advanced Life Support (PALS) AHA
IU Health PALS Study Guide Preparing for your upcoming PALS course UPDATED November 2016 Course Curriculum: 2015 American Heart Association (AHA) Guidelines for Pediatric Advanced Life Support (PALS) AHA
Handling Common Problems & Pitfalls During. Oxygen desaturation in patients receiving mechanical ventilation ACUTE SEVERE RESPIRATORY FAILURE
 Handling Common Problems & Pitfalls During ACUTE SEVERE RESPIRATORY FAILURE Pravit Jetanachai, MD QSNICH Oxygen desaturation in patients receiving mechanical ventilation Causes of oxygen desaturation 1.
Handling Common Problems & Pitfalls During ACUTE SEVERE RESPIRATORY FAILURE Pravit Jetanachai, MD QSNICH Oxygen desaturation in patients receiving mechanical ventilation Causes of oxygen desaturation 1.
ACLS. Advanced Cardiac Life Support Practice Test Questions. 1. The following is included in the ACLS Survey?
 1. The following is included in the ACLS Survey? a. Airway, Breathing, Circulation, Differential Diagnosis b. Airway, Breathing, Circulation, Defibrillation c. Assessment, Breathing, Circulation, Defibrillation
1. The following is included in the ACLS Survey? a. Airway, Breathing, Circulation, Differential Diagnosis b. Airway, Breathing, Circulation, Defibrillation c. Assessment, Breathing, Circulation, Defibrillation
MASTER SYLLABUS
 A. Academic Division: Health Sciences B. Discipline: Respiratory Care MASTER SYLLABUS 2018-2019 C. Course Number and Title: RESP 2330 Advanced Life Support Procedures D. Course Coordinator: Tricia Winters,
A. Academic Division: Health Sciences B. Discipline: Respiratory Care MASTER SYLLABUS 2018-2019 C. Course Number and Title: RESP 2330 Advanced Life Support Procedures D. Course Coordinator: Tricia Winters,
Chest Trauma.
 Chest Trauma www.fisiokinesiterapia.biz Objectives Anatomy of Thorax Main Causes of Chest Injuries S/S of Chest Injuries Different Types of Chest Injuries Treatments of Chest Injuries Anatomy of the chest
Chest Trauma www.fisiokinesiterapia.biz Objectives Anatomy of Thorax Main Causes of Chest Injuries S/S of Chest Injuries Different Types of Chest Injuries Treatments of Chest Injuries Anatomy of the chest
Student Guide Module 4: Pediatric Trauma
 Student Guide Module 4: Pediatric Trauma Problem based learning exercise objectives Understand how to manage traumatic injuries in mass casualty events. Discuss the features and the approach to pediatric
Student Guide Module 4: Pediatric Trauma Problem based learning exercise objectives Understand how to manage traumatic injuries in mass casualty events. Discuss the features and the approach to pediatric
Maternal Collapse Guideline
 Maternal Collapse Guideline Guideline Number: 664 Supersedes: Classification Clinical Version No: Date of EqIA: Approved by: Date Approved: Date made active: Review Date: 1 Obstetric Written Documentation
Maternal Collapse Guideline Guideline Number: 664 Supersedes: Classification Clinical Version No: Date of EqIA: Approved by: Date Approved: Date made active: Review Date: 1 Obstetric Written Documentation
UNITED STATES MARINE CORPS FIELD MEDICAL TRAINING BATTALION Camp Lejeune, NC
 UNITED STATES MARINE CORPS FIELD MEDICAL TRAINING BATTALION Camp Lejeune, NC 28542-0042 FMST 406 Manage Shock Casualties TERMINAL LEARNING OBJECTIVES 1. Given a casualty in an operational environment,
UNITED STATES MARINE CORPS FIELD MEDICAL TRAINING BATTALION Camp Lejeune, NC 28542-0042 FMST 406 Manage Shock Casualties TERMINAL LEARNING OBJECTIVES 1. Given a casualty in an operational environment,
Pediatric Shock. Hypovolemia. Sepsis. Most common cause of pediatric shock Small blood volumes (80cc/kg)
") Critical Concepts: Shock Inadequate peripheral perfusion where oxygen delivery does not meet metabolic demand Adult vs Pediatric Shock - Same causes/different frequencies Pediatric Shock Hypovolemia Most
Critical Concepts: Shock Inadequate peripheral perfusion where oxygen delivery does not meet metabolic demand Adult vs Pediatric Shock - Same causes/different frequencies Pediatric Shock Hypovolemia Most
Nassau Regional Emergency Medical Services. Advanced Life Support Pediatric Protocol Manual
 Nassau Regional Emergency Medical Services Advanced Life Support Pediatric Protocol Manual 2014 PEDIATRIC ADVANCED LIFE SUPPORT PROTOCOLS TABLE OF CONTENTS Approved Effective Newborn Resuscitation P 1
Nassau Regional Emergency Medical Services Advanced Life Support Pediatric Protocol Manual 2014 PEDIATRIC ADVANCED LIFE SUPPORT PROTOCOLS TABLE OF CONTENTS Approved Effective Newborn Resuscitation P 1
The student guide to simulation
 CETL 2008 1 The following guide will introduce you to what the simulators can do But firstly a few words on communication Please verbally and non-verbally communicate with the simulator as if it were a
CETL 2008 1 The following guide will introduce you to what the simulators can do But firstly a few words on communication Please verbally and non-verbally communicate with the simulator as if it were a
physiology 6 Mohammed Jaafer Turquoise team
 15 physiology 6 Mohammed Jaafer 22-3-2016 Turquoise team Cardiac Arrhythmias and Their Electrocardiographic Interpretation Today, we are going to talk about the abnormal excitation. As we said before,
15 physiology 6 Mohammed Jaafer 22-3-2016 Turquoise team Cardiac Arrhythmias and Their Electrocardiographic Interpretation Today, we are going to talk about the abnormal excitation. As we said before,
Advanced Resuscitation - Child
 C02C Resuscitation 2017-03-23 1 up to 10 years Office of the Medical Director Advanced Resuscitation - Child Intermediate Advanced Critical From PRIMARY ASSESSMENT Known or suspected hypothermia Algorithm
C02C Resuscitation 2017-03-23 1 up to 10 years Office of the Medical Director Advanced Resuscitation - Child Intermediate Advanced Critical From PRIMARY ASSESSMENT Known or suspected hypothermia Algorithm
TASERS and EMS. Separating Truth from Fancy
 TASERS and EMS Separating Truth from Fancy Raymond L. Fowler, M.D., FACEP Associate Professor of Emergency Medicine, Surgery, and Allied Health and Co-Chair Chair of the Section on EMS, Disaster Medicine,
TASERS and EMS Separating Truth from Fancy Raymond L. Fowler, M.D., FACEP Associate Professor of Emergency Medicine, Surgery, and Allied Health and Co-Chair Chair of the Section on EMS, Disaster Medicine,
Mesa County EMS Protocol Test 2016
 Mesa County EMS Protocol Test 2016 1. Which of the following is incorrect? a. Each EMS and Fire agency should have protocols in place for evaluation of personnel involved in fire suppression operations
Mesa County EMS Protocol Test 2016 1. Which of the following is incorrect? a. Each EMS and Fire agency should have protocols in place for evaluation of personnel involved in fire suppression operations
Index. Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type. A Abdomen, and aorta, as causes of shock, point-of-care ultrasonography in assessment of, 915 917 Abdominal compartment syndrome, trauma patient
Note: Page numbers of article titles are in boldface type. A Abdomen, and aorta, as causes of shock, point-of-care ultrasonography in assessment of, 915 917 Abdominal compartment syndrome, trauma patient
ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) Rv
 Rv") ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) Rv.8.18.18 ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) SUDDEN PROGRESSIVE FORM OF ACUTE RESPIRATORY FAILURE ALVEOLAR CAPILLARY MEMBRANE BECOMES DAMAGED AND MORE
ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) Rv.8.18.18 ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) SUDDEN PROGRESSIVE FORM OF ACUTE RESPIRATORY FAILURE ALVEOLAR CAPILLARY MEMBRANE BECOMES DAMAGED AND MORE
Emergency Room Resuscitation of the Unstable Trauma Patient
 Emergency Room Resuscitation of the Unstable Trauma Patient Goals of trauma resuscitation Maintain: Systemic oxygenation Systemic perfusion Neurologic function Approach to unstable trauma patient Primary
Emergency Room Resuscitation of the Unstable Trauma Patient Goals of trauma resuscitation Maintain: Systemic oxygenation Systemic perfusion Neurologic function Approach to unstable trauma patient Primary
Surgical Care at the District Hospital. EMERGENCY & ESSENTIAL SURGICAL CARE
 Surgical Care at the District Hospital 1 14 Practical Anesthesia Key Points 2 14.1 General Anesthesia Have a clear plan before starting anesthesia Never use an unfamiliar anesthetic technique in an emergency
Surgical Care at the District Hospital 1 14 Practical Anesthesia Key Points 2 14.1 General Anesthesia Have a clear plan before starting anesthesia Never use an unfamiliar anesthetic technique in an emergency
Lesson 4-3: Cardiac Emergencies. CARDIAC EMERGENCIES Angina, AMI, CHF and AED
 Lesson 4-3: Cardiac Emergencies CARDIAC EMERGENCIES Angina, AMI, CHF and AED THREE FAMILIAR CARDIAC CONDITIONS Angina Pectoris Acute Myocardial Infarction Congestive Heart Failure ANGINA PECTORIS Chest
Lesson 4-3: Cardiac Emergencies CARDIAC EMERGENCIES Angina, AMI, CHF and AED THREE FAMILIAR CARDIAC CONDITIONS Angina Pectoris Acute Myocardial Infarction Congestive Heart Failure ANGINA PECTORIS Chest
Advanced Cardiac Life Support ACLS
 Essential Medical Training, LLC Providing Quality, Professional Training Advanced Cardiac Life Support ACLS Course Study Guide and Agenda 772-781-9249 office 772-382-0607 fax Email: treasurecoastcpr@gmail.com
Essential Medical Training, LLC Providing Quality, Professional Training Advanced Cardiac Life Support ACLS Course Study Guide and Agenda 772-781-9249 office 772-382-0607 fax Email: treasurecoastcpr@gmail.com
McHenry Western Lake County EMS System Optional CE for EMT-B, Paramedics and PHRN s Bradycardia and Treatments Optional #7 2018
 McHenry Western Lake County EMS System Optional CE for EMT-B, Paramedics and PHRN s Bradycardia and Treatments Optional #7 2018 This month we will be looking at a specific ECG Rhythm and its treatments
McHenry Western Lake County EMS System Optional CE for EMT-B, Paramedics and PHRN s Bradycardia and Treatments Optional #7 2018 This month we will be looking at a specific ECG Rhythm and its treatments
EMS System for Metropolitan Oklahoma City and Tulsa 2017 Medical Control Board Treatment Protocols
 S O EMT EMT-INTERMEDIATE 85 ADVANCED EMT PARAMEDIC 3H WAVEFORM CAPNOGRAPHY ADULT & PEDIATRIC Indications: 1. Medical General Assessment/General Supportive Care. 2. Trauma General Assessment/Trauma & Hypovolemic
S O EMT EMT-INTERMEDIATE 85 ADVANCED EMT PARAMEDIC 3H WAVEFORM CAPNOGRAPHY ADULT & PEDIATRIC Indications: 1. Medical General Assessment/General Supportive Care. 2. Trauma General Assessment/Trauma & Hypovolemic
Wake County EMS System Peer Review/Clinical Data/System Performance
 P a g e 1 Wake County EMS System Peer Review/Clinical Data/System Performance Explanations and Definitions for Reports Wake County EMS engages in regular external review. The System makes quarterly reports
P a g e 1 Wake County EMS System Peer Review/Clinical Data/System Performance Explanations and Definitions for Reports Wake County EMS engages in regular external review. The System makes quarterly reports
New and Future Trends in EMS. Ron Brown, MD, FACEP Paramedic Lecture Series 2018
 New and Future Trends in EMS Ron Brown, MD, FACEP Paramedic Lecture Series 2018 New technologies and protocols DSD Mechanical Compression ITD BiPAP Ultrasound Double Sequential Defibrillation Two defibrillators
New and Future Trends in EMS Ron Brown, MD, FACEP Paramedic Lecture Series 2018 New technologies and protocols DSD Mechanical Compression ITD BiPAP Ultrasound Double Sequential Defibrillation Two defibrillators
Post Resuscitation (ROSC) Care
 Care") Standard Operating Procedure 2.10 Post Resuscitation (ROSC) Care Position Responsible: Medical Director Approved: Clinical Governance Committee Related Documents: This document is the intellectual property
Standard Operating Procedure 2.10 Post Resuscitation (ROSC) Care Position Responsible: Medical Director Approved: Clinical Governance Committee Related Documents: This document is the intellectual property
COUNTY OF SACRAMENTO EMERGENCY MEDICAL SERVICES AGENCY
 COUNTY OF SACRAMENTO EMERGENCY MEDICAL SERVICES AGENCY Document # 8024.31 PROGRAM DOCUMENT: Initial Date: 10/26/94 Cardiac Dysrhythmias Last Approval Date: 11/01/16 Effective Date: 11/01/18 Next Review
COUNTY OF SACRAMENTO EMERGENCY MEDICAL SERVICES AGENCY Document # 8024.31 PROGRAM DOCUMENT: Initial Date: 10/26/94 Cardiac Dysrhythmias Last Approval Date: 11/01/16 Effective Date: 11/01/18 Next Review
Cardiovascular Emergencies. Chapter 12
 Cardiovascular Emergencies Chapter 12 Cardiovascular Emergencies Cardiovascular disease (CVD) claimed 931,108 lives in the US during 2001. 2,551 per day Almost two people per minute! CVD accounts for 38.5%
Cardiovascular Emergencies Chapter 12 Cardiovascular Emergencies Cardiovascular disease (CVD) claimed 931,108 lives in the US during 2001. 2,551 per day Almost two people per minute! CVD accounts for 38.5%
Z19.2 Cross Reference to Patient Care Maps & Clinical Care Procedures
 2017-04-07 Old version G1 Code of Ethics G2 Scope and Function G3 Scene Assessment G4 Triage G5 Primary Survey G6 Shock G7 Load and Go G8 Secondary Survey G9 Unconscious Patient G10A Obstructed Airway
2017-04-07 Old version G1 Code of Ethics G2 Scope and Function G3 Scene Assessment G4 Triage G5 Primary Survey G6 Shock G7 Load and Go G8 Secondary Survey G9 Unconscious Patient G10A Obstructed Airway
Condensed version.
 I m Stu 3 Condensed version smcvicar@uwhealth.org Listen 1. Snoring 2. Gurgling 3. Hoarseness 4. Stridor (inspiratory/expiratory) 5. Wheezing 6. Grunting Listen Crackles Wheezing Stridor Absent Crackles
I m Stu 3 Condensed version smcvicar@uwhealth.org Listen 1. Snoring 2. Gurgling 3. Hoarseness 4. Stridor (inspiratory/expiratory) 5. Wheezing 6. Grunting Listen Crackles Wheezing Stridor Absent Crackles
Cardiovascular and Respiratory Disorders
 Cardiovascular and Respiratory Disorders Blood Pressure Normal blood pressure is 120/80 mmhg (millimeters of mercury) Hypertension is when the resting blood pressure is too high Systolic BP is 140 mmhg
Cardiovascular and Respiratory Disorders Blood Pressure Normal blood pressure is 120/80 mmhg (millimeters of mercury) Hypertension is when the resting blood pressure is too high Systolic BP is 140 mmhg
Therapeutic hypothermia
 INDUCED HYPOTHERMIA Dr. Attilla Kiss M.D. Acting Medical Director Emergency Services EMS Medical Director St. John Medical Center OBJECTIVES Define and explain Induced Hypothermia Discuss both pre-hospital
INDUCED HYPOTHERMIA Dr. Attilla Kiss M.D. Acting Medical Director Emergency Services EMS Medical Director St. John Medical Center OBJECTIVES Define and explain Induced Hypothermia Discuss both pre-hospital
FIRST AID WRITTEN EXAM. Team Name: 1. Participation in a critical incident stress debriefing (CISD) is mandatory. a. TRUE b. FALSE
 is mandatory. a. TRUE b. FALSE") 2015 NEW IBERIA MINE RESCUE CONTEST FIRST AID WRITTEN EXAM Name: Date: 1. Participation in a critical incident stress debriefing (CISD) is mandatory. 2. The use of accessory muscles in the chest, abdomen
2015 NEW IBERIA MINE RESCUE CONTEST FIRST AID WRITTEN EXAM Name: Date: 1. Participation in a critical incident stress debriefing (CISD) is mandatory. 2. The use of accessory muscles in the chest, abdomen
CENTRAL CALIFORNIA EMERGENCY MEDICAL SERVICES A Division of the Fresno County Department of Public Health
 CENTRAL CALIFORNIA EMERGENCY MEDICAL SERVICES A Division of the Fresno County Department of Public Health Manual Subject Emergency Medical Services Administrative Policies and Procedures Table of Contents
CENTRAL CALIFORNIA EMERGENCY MEDICAL SERVICES A Division of the Fresno County Department of Public Health Manual Subject Emergency Medical Services Administrative Policies and Procedures Table of Contents
Pediatric Advanced Life Support
 Pediatric Advanced Life Support Pediatric Chain of Survival Berg M D et al. Circulation 2010;122:S862-S875 Prevention Early cardiopulmonary resuscitation (CPR) Prompt access to the emergency response system
Pediatric Advanced Life Support Pediatric Chain of Survival Berg M D et al. Circulation 2010;122:S862-S875 Prevention Early cardiopulmonary resuscitation (CPR) Prompt access to the emergency response system
CHANGES FOR DECEMBER 2008 PREHOSPITAL CARE MANUAL
 CHANGES FOR DECEMBER 2008 PREHOSPITAL CARE MANUAL Item Changed Airway Management Procedure Oral Intubation Procedure Tube Confirmation and Monitoring Procedure C10 Chest Pain/ACS M2 Allergic Reaction/Anaphylaxis
CHANGES FOR DECEMBER 2008 PREHOSPITAL CARE MANUAL Item Changed Airway Management Procedure Oral Intubation Procedure Tube Confirmation and Monitoring Procedure C10 Chest Pain/ACS M2 Allergic Reaction/Anaphylaxis
ITLS Pediatric Provider Course Advanced Pre-Test
 ITLS Pediatric Provider Course Advanced Pre-Test 1. You arrive at the scene of a motor vehicle crash and are directed to evaluate a child who was in one of the vehicles. The patient appears to be a child
ITLS Pediatric Provider Course Advanced Pre-Test 1. You arrive at the scene of a motor vehicle crash and are directed to evaluate a child who was in one of the vehicles. The patient appears to be a child
SHOCK. can contribute to one of the four kinds of shock. Sometimes the cause of shock is multi-factorial.
 SHOCK GENERAL CONSIDERATIONS A. Hypoperfusion (shock) is the inadequate delivery of vital oxygen and nutrients to body tissues, which left unchecked will result in organ system failure and death. B. No
SHOCK GENERAL CONSIDERATIONS A. Hypoperfusion (shock) is the inadequate delivery of vital oxygen and nutrients to body tissues, which left unchecked will result in organ system failure and death. B. No
Electrocardiography for Healthcare Professionals
 Electrocardiography for Healthcare Professionals Kathryn A. Booth Thomas O Brien Chapter 5: Rhythm Strip Interpretation and Sinus Rhythms Learning Outcomes 5.1 Explain the process of evaluating ECG tracings
Electrocardiography for Healthcare Professionals Kathryn A. Booth Thomas O Brien Chapter 5: Rhythm Strip Interpretation and Sinus Rhythms Learning Outcomes 5.1 Explain the process of evaluating ECG tracings
EMT. Chapter 14 Review
 EMT Chapter 14 Review Review 1. All of the following are common signs and symptoms of cardiac ischemia, EXCEPT: A. headache. B. chest pressure. C. shortness of breath. D. anxiety or restlessness. Review
EMT Chapter 14 Review Review 1. All of the following are common signs and symptoms of cardiac ischemia, EXCEPT: A. headache. B. chest pressure. C. shortness of breath. D. anxiety or restlessness. Review
CSI Skills Lab #5: Arrhythmia Interpretation and Treatment
 CSI 202 - Skills Lab #5: Arrhythmia Interpretation and Treatment Origins of the ACLS Approach: CSI 202 - Skills Lab 5 Notes ACLS training originated in Nebraska in the early 1970 s. Its purpose was to
CSI 202 - Skills Lab #5: Arrhythmia Interpretation and Treatment Origins of the ACLS Approach: CSI 202 - Skills Lab 5 Notes ACLS training originated in Nebraska in the early 1970 s. Its purpose was to
GETTING TO THE HEART OF THE MATTER. Ritu Sahni, MD, MPH Lake Oswego Fire Department Washington County EMS Clackamas County EMS
 GETTING TO THE HEART OF THE MATTER Ritu Sahni, MD, MPH Lake Oswego Fire Department Washington County EMS Clackamas County EMS TAKE HOME POINTS CPR is the most important thing Train like we fight Measure
GETTING TO THE HEART OF THE MATTER Ritu Sahni, MD, MPH Lake Oswego Fire Department Washington County EMS Clackamas County EMS TAKE HOME POINTS CPR is the most important thing Train like we fight Measure
Resuscitation Patient Management Tool May 2015 MET Event
 OPTIONAL: Local Event ID: Date/Time MET was activated: Time Not Documented MET 2.1 Pre-Event Pre-Event Tab Was patient discharged from an Intensive Care Unit (ICU) at any point during this admission and
OPTIONAL: Local Event ID: Date/Time MET was activated: Time Not Documented MET 2.1 Pre-Event Pre-Event Tab Was patient discharged from an Intensive Care Unit (ICU) at any point during this admission and
MICHIGAN. State Protocols. Pediatric Cardiac Table of Contents 6.1 General Pediatric Cardiac Arrest 6.2 Bradycardia 6.
 MICHIGAN State Protocols Protocol Number Protocol Name Pediatric Cardiac Table of Contents 6.1 General Pediatric Cardiac Arrest 6.2 Bradycardia 6.3 Tachycardia PEDIATRIC CARDIAC PEDIATRIC CARDIAC ARREST
MICHIGAN State Protocols Protocol Number Protocol Name Pediatric Cardiac Table of Contents 6.1 General Pediatric Cardiac Arrest 6.2 Bradycardia 6.3 Tachycardia PEDIATRIC CARDIAC PEDIATRIC CARDIAC ARREST
Admission of patient CVICU and hemodynamic monitoring
 Admission of patient CVICU and hemodynamic monitoring Prepared by: Rami AL-Khatib King Fahad Medical City Pi Prince Salman Heart tcentre CVICU-RN Admission patient to CVICU Introduction All the patients
Admission of patient CVICU and hemodynamic monitoring Prepared by: Rami AL-Khatib King Fahad Medical City Pi Prince Salman Heart tcentre CVICU-RN Admission patient to CVICU Introduction All the patients
Final Written Exam ASHI ACLS
 Final Written Exam ASHI ACLS Instructions: Identify the choice that best completes the statement or answers the question. Questions 1 and 2 pertain to the following scenario: A 54-year-old man has experienced
Final Written Exam ASHI ACLS Instructions: Identify the choice that best completes the statement or answers the question. Questions 1 and 2 pertain to the following scenario: A 54-year-old man has experienced
San Benito County EMS Agency Section 700: Patient Care Procedures
 Purpose: To outline the steps EMTs & paramedics will take to manage possible life threats in any child or adult patient they encounter. This policy is in effect for all treatment protocols & is to be referred
Purpose: To outline the steps EMTs & paramedics will take to manage possible life threats in any child or adult patient they encounter. This policy is in effect for all treatment protocols & is to be referred
Capnography for Pediatric Procedural Sedation Learning Module Last revised: February 18, 2014
 Capnography for Pediatric Procedural Sedation Learning Module Last revised: February 18, 2014 Capnography 40 Non-invasive device that continually monitors EtCO 2 While pulse oximetry measures oxygen saturation,
Capnography for Pediatric Procedural Sedation Learning Module Last revised: February 18, 2014 Capnography 40 Non-invasive device that continually monitors EtCO 2 While pulse oximetry measures oxygen saturation,
Capnography (ILS/ALS)
") Capnography (ILS/ALS) Clinical Indications: 1. Capnography shall be used as soon as possible in conjunction with any airway management adjunct, including endotracheal, Blind Insertion Airway Devices (BIAD)
Capnography (ILS/ALS) Clinical Indications: 1. Capnography shall be used as soon as possible in conjunction with any airway management adjunct, including endotracheal, Blind Insertion Airway Devices (BIAD)
Adult Basic Life Support
 Adult Basic Life Support UNRESPONSIVE? Shout for help Open airway NOT BREATHING NORMALLY? Call 112* 30 chest compressions 2 rescue breaths 30 compressions *or national emergency number Fig 1.2_Adult BLS
Adult Basic Life Support UNRESPONSIVE? Shout for help Open airway NOT BREATHING NORMALLY? Call 112* 30 chest compressions 2 rescue breaths 30 compressions *or national emergency number Fig 1.2_Adult BLS
Routine Patient Care Guidelines - Adult
 Routine Patient Care Guidelines - Adult All levels of provider will complete an initial & focused assessment on every patient, and as standing order, use necessary and appropriate skills and procedures
Routine Patient Care Guidelines - Adult All levels of provider will complete an initial & focused assessment on every patient, and as standing order, use necessary and appropriate skills and procedures
Major Points. The ED-ICU Interface. Chain of Survival. It usually starts here
 Major Points The ED-ICU Interface Robert M. Rodriguez, MD FAAEM Most ICU patients start in ED Chain of critical care starting in field and ED Collaborate, develop protocols (define roles), communicate
Major Points The ED-ICU Interface Robert M. Rodriguez, MD FAAEM Most ICU patients start in ED Chain of critical care starting in field and ED Collaborate, develop protocols (define roles), communicate
SHOCK Susanna Hilda Hutajulu, MD, PhD
 SHOCK Susanna Hilda Hutajulu, MD, PhD Div Hematology and Medical Oncology Department of Internal Medicine Universitas Gadjah Mada Yogyakarta Outline Definition Epidemiology Physiology Classes of Shock
SHOCK Susanna Hilda Hutajulu, MD, PhD Div Hematology and Medical Oncology Department of Internal Medicine Universitas Gadjah Mada Yogyakarta Outline Definition Epidemiology Physiology Classes of Shock
Chapter 29 - Chest_and_Abdominal_Trauma
 Introduction to Emergency Medical Care 1 OBJECTIVES 29.1 Define key terms introduced in this chapter. Slides 11, 15, 18, 27 29.2 Describe mechanisms of injury commonly associated with chest injuries. Slides
Introduction to Emergency Medical Care 1 OBJECTIVES 29.1 Define key terms introduced in this chapter. Slides 11, 15, 18, 27 29.2 Describe mechanisms of injury commonly associated with chest injuries. Slides
Purpose This Operating Procedure provides guidance on the management of blunt thoracic traumatic injury
 Blunt Thoracic Trauma HELI.CLI.09 Purpose This Operating Procedure provides guidance on the management of blunt thoracic traumatic injury Procedure Management of Blunt Thoracic Traumatic Injury For Review
Blunt Thoracic Trauma HELI.CLI.09 Purpose This Operating Procedure provides guidance on the management of blunt thoracic traumatic injury Procedure Management of Blunt Thoracic Traumatic Injury For Review
County of Santa Clara Emergency Medical Services System
 County of Santa Clara Emergency Medical Services System Policy #700-M12: Continuous Positive Airway Pressure CONTINUOUS POSITIVE AIRWAY PRESSURE Effective: February 8, 2013TBD Replaces: NewFebruary 8,
County of Santa Clara Emergency Medical Services System Policy #700-M12: Continuous Positive Airway Pressure CONTINUOUS POSITIVE AIRWAY PRESSURE Effective: February 8, 2013TBD Replaces: NewFebruary 8,
Advanced Resuscitation - Adult
 C02A Resuscitation 2017-03-23 17 years & older Office of the Medical Director Advanced Resuscitation - Adult Intermediate Advanced Critical From PRIMARY ASSESSMENT Known or suspected hypothermia Algorithm
C02A Resuscitation 2017-03-23 17 years & older Office of the Medical Director Advanced Resuscitation - Adult Intermediate Advanced Critical From PRIMARY ASSESSMENT Known or suspected hypothermia Algorithm
6. Knowledge and Skill Comparison (Paramedic)
") 6. Knowledge and Skill Comparison (Paramedic) The order of content is not meant to imply the order of delivery. a. Paramedic: New Course Considerations When planning and conducting a new Paramedic course,
6. Knowledge and Skill Comparison (Paramedic) The order of content is not meant to imply the order of delivery. a. Paramedic: New Course Considerations When planning and conducting a new Paramedic course,
Appendix (i) The ABCDE approach to the sick patient
 The ABCDE approach to the sick patient") Appendix (i) The ABCDE approach to the sick patient This appendix and the one following provide guidance on the initial approach and management of common medical emergencies which may arise in general
Appendix (i) The ABCDE approach to the sick patient This appendix and the one following provide guidance on the initial approach and management of common medical emergencies which may arise in general
Dr. Rami M. Adil Al-Hayali Assistant Professor in Medicine
 Dr. Rami M. Adil Al-Hayali Assistant Professor in Medicine Venous thromboembolism: pulmonary embolism (PE) deep vein thrombosis (DVT) 1% of all patients admitted to hospital 5% of in-hospital mortality
Dr. Rami M. Adil Al-Hayali Assistant Professor in Medicine Venous thromboembolism: pulmonary embolism (PE) deep vein thrombosis (DVT) 1% of all patients admitted to hospital 5% of in-hospital mortality
Core Subject Part 4. Identify the principles of approaching the sick patient.
 The Role of The Dental Care Professional During a Medical Emergency: General Dental Council Standards and The Management of The Collapsed Patient Using the ABCDE Approach Aims: Core Subject Part 4 To provide
The Role of The Dental Care Professional During a Medical Emergency: General Dental Council Standards and The Management of The Collapsed Patient Using the ABCDE Approach Aims: Core Subject Part 4 To provide
Learning Station Competency Checklists
 Learning Station Competency Checklists Cardiac Arrest: Shockable Rhythm Team Dynamics Practice Demonstrates effective team dynamics (see, below) Performs manual maneuvers to open airway* Initiates assisted
Learning Station Competency Checklists Cardiac Arrest: Shockable Rhythm Team Dynamics Practice Demonstrates effective team dynamics (see, below) Performs manual maneuvers to open airway* Initiates assisted
Chapter 29 - Chest Injuries
 1 2 3 4 5 6 7 8 9 National EMS Education Standard Competencies (1 of 5) Trauma Applies fundamental knowledge to provide basic emergency care and transportation based on assessment findings for an acutely
1 2 3 4 5 6 7 8 9 National EMS Education Standard Competencies (1 of 5) Trauma Applies fundamental knowledge to provide basic emergency care and transportation based on assessment findings for an acutely
Shifts 28, 29, 30 Quizzes
 Shifts 28, 29, 30 Quizzes Name: Score: Date: 1. You are on the scene of a 4 year old in cardiac arrest. CPR is initiated and an E.T. tube has been placed, an I.V. has been established. What is the correct
Shifts 28, 29, 30 Quizzes Name: Score: Date: 1. You are on the scene of a 4 year old in cardiac arrest. CPR is initiated and an E.T. tube has been placed, an I.V. has been established. What is the correct
Taking the shock factor out of shock
 Taking the shock factor out of shock Julie Antonellis, BS, LVT, VTS (ECC) Northern Virginia Regional Director for the VALVT Technician Supervisor VCA Animal Emergency Critical Care Business owner Antonellis
Taking the shock factor out of shock Julie Antonellis, BS, LVT, VTS (ECC) Northern Virginia Regional Director for the VALVT Technician Supervisor VCA Animal Emergency Critical Care Business owner Antonellis
1. Which of the following organs is contained in the retroperitoneal region of the abdomen? A. Stomach B. Liver C. Kidney D.
 1. Which of the following organs is contained in the retroperitoneal region of the abdomen? A. Stomach B. Liver C. Kidney D. Uterus 2. What is Sellick's maneuver? A. A method allowing the rescuer to hold
1. Which of the following organs is contained in the retroperitoneal region of the abdomen? A. Stomach B. Liver C. Kidney D. Uterus 2. What is Sellick's maneuver? A. A method allowing the rescuer to hold
Julie Zimmerman, MSN, RN, CCRN Clinical Nurse Specialist
 Julie Zimmerman, MSN, RN, CCRN Clinical Nurse Specialist Objectives Define capnography vs. end tidal CO2 (EtCO 2 ) Identify what normal vs. abnormal EtCO2 values mean and what to do Understand when to
Julie Zimmerman, MSN, RN, CCRN Clinical Nurse Specialist Objectives Define capnography vs. end tidal CO2 (EtCO 2 ) Identify what normal vs. abnormal EtCO2 values mean and what to do Understand when to
June 2011 Bill Streett-Training Section Chief
 Capnography 102 June 2011 Bill Streett-Training Section Chief Terminology Capnography: the measurement and numerical display of end-tidal CO2 concentration, at the patient s airway, during a respiratory
Capnography 102 June 2011 Bill Streett-Training Section Chief Terminology Capnography: the measurement and numerical display of end-tidal CO2 concentration, at the patient s airway, during a respiratory
4. Which survey program does your facility use to get your program designated by the state?
 TRAUMA SURVEY Please complete one survey for each TCD designation you have in your facility. There would be a maximum of three surveys completed if your facility was designated as a trauma, stroke and
TRAUMA SURVEY Please complete one survey for each TCD designation you have in your facility. There would be a maximum of three surveys completed if your facility was designated as a trauma, stroke and
STROKE INTRODUCTION OBJECTIVES. When the student has finished this module, he/she will be able to:
 STROKE INTRODUCTION Stroke is the medical term for a specific type of neurological event that causes damage to the brain. There are two types of stroke, but both types of stroke cause the same type of
STROKE INTRODUCTION Stroke is the medical term for a specific type of neurological event that causes damage to the brain. There are two types of stroke, but both types of stroke cause the same type of
Pediatric Advanced Life Support Overview Judy Haluka BS, RCIS, EMT-P
 Pediatric Advanced Life Support Overview 2006 Judy Haluka BS, RCIS, EMT-P General Our Database is lacking in pediatrics Pediatrics are DIFFERENT than Adults not just smaller The same procedure may require
Pediatric Advanced Life Support Overview 2006 Judy Haluka BS, RCIS, EMT-P General Our Database is lacking in pediatrics Pediatrics are DIFFERENT than Adults not just smaller The same procedure may require