ECG Interpretation Made Easy
|
|
|
- Evan Daniels
- 5 years ago
- Views:
Transcription
1 ECG Interpretation Made Easy Dr. A Tageldien Abdellah, MSc MD EBSC Lecturer of Cardiology- Hull University Hull York Medical School
2 ECG Interpretation Made Easy Synopsis Benefits Objectives Process Disclaimer
3 Electrocardiogram (ECG)

4 Conductive System of the Heart
5 ECG and Conductive System



6 Electrical Conduction in the Heart Pacemaker Intrinsic Rate SAN bpm AVN bpm His Bundle bpm Purkinje Fibers bpm

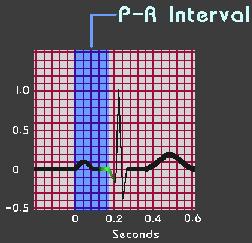
7 ECG Waves and Segments


8 ECG Waves and Segments

9 ECG Waves and Segments Bazett's formula: QT corrected = QT measured SQRT (RR interval)

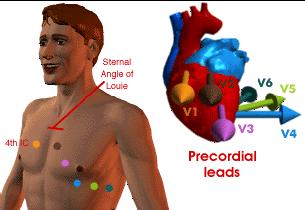
10 12-lead ECG

11 12-lead ECG
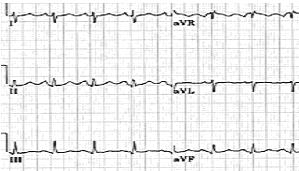
12 Normal ECG
13 Where ECG leads look at? Lateral Anterior/ Septal Anterior Inferior Lateral Anterior/ Septal Lateral Inferior Inferior Anterior Lateral
14 ECG Analysis Step 1: Is the Rhythm Regular or Irregular? Step 2: Are All QRS Complexes Similar and Narrow, and is ST segment is isoelectric? Step 3: Are All P Waves Similar and Are PR Intervals Normal? Step 4: Is the Rate Normal? Step 5: Do Waves and Complexes Proceed in Normal Sequence?
15 Systematic ECG Analysis 1. Check the patient details - is the ECG correctly labelled? 2. What is the rate? 3. Is this sinus rhythm? If not, what is going on? 4. What is the mean frontal plane QRS axis? 5. Are the P waves normal (Good places to look are II and V1)? 6. What is the PR interval? 7. Are the QRS complexes normal? 8. Are the ST segments normal, depressed or elevated? 9. Are the T waves normal? 10. What is the QT interval? 11. Are there abnormal U waves?

16 Systematic ECG Analysis: Heart Rate Estimation
17 Systematic ECG Analysis: Cardiac Axis
18 Systematic ECG Analysis: Cardiac Axis Three Easy steps 1- Estimate the overall deflection (positive or negative, and how much) of the QRS in standard lead I. 2- Do the same for avf. 3- Plot the vector on a system of axes, and estimate the angle. Normal QRS axis Normal axis = -30 to +120 degrees Left axis deviation is left of -30 degrees Right axis deviation is right of +120 degrees Axis is abnormal Lead II is more negative than positive. Lead III is more positive than lead II.


19 Systematic ECG Analysis: Cardiac Axis RAD LAD Intermediate Axis RAD LAD Intermediate Axis RAD LAD Intermediate Axis
20 Common ECG Abnormalities I- Abnormalities involving ECG waves and segments. II- Pacemaker Abnormalities. III- Conduction Abnormalities. IV- Ischemic Abnormalities. V- Miscellaneous Abnormalities.


21 I- Abnormalities of ECG Waves and Segments P Wave Abnormalities: left Atrial Enlargement Prolonged P wave duration of 0.12 seconds or more Notched upright P wave duration in leads I, II, V4 to V6 Deep, broad terminal negative deflection in V1 No significant shift in P wave axis Common in Mitral Stenosis and HTN


22 I- Abnormalities of ECG Waves and Segments P Wave Abnormalities: Right Atrial Enlargement Normal P wave duration Tall, peaked P waves with an amplitude greater than 2.5 mm in leads II, III, avf Positive deflection of the P wave in lead V1 or V2 is greater than 1.5 mm Common in Pulmonary Hypertension and COPD

23 I- Abnormalities of ECG Waves and Segments P Wave Abnormalities: Biatrial Enlargement Large biphasic P wave in V1 with initial positive portion of the P wave greater than 1.5 mm and terminal negative component up to 1 mm in depth and 0.04 seconds in duration Tall, peaked P wave greater than 1.5 mm in the right precordial leads (V1, V2) and a wide, notched P wave in the limb leads or leads (V5 and V6). Increase in both amplitude (2.5 mm or more) and duration (0.12 seconds or more) of the P wave in the limb leads.


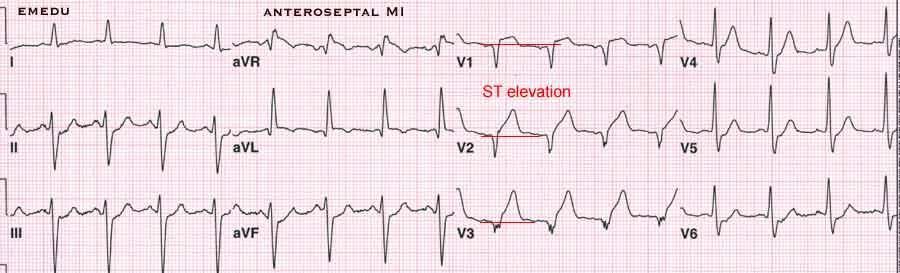
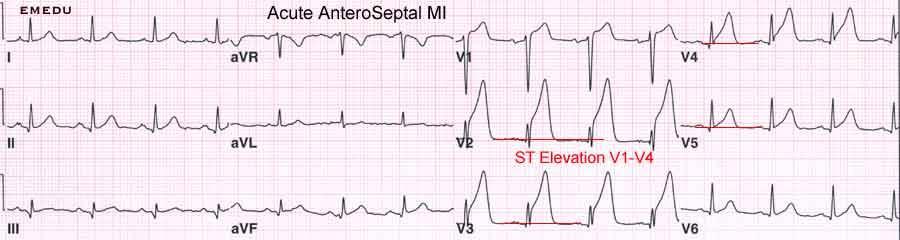
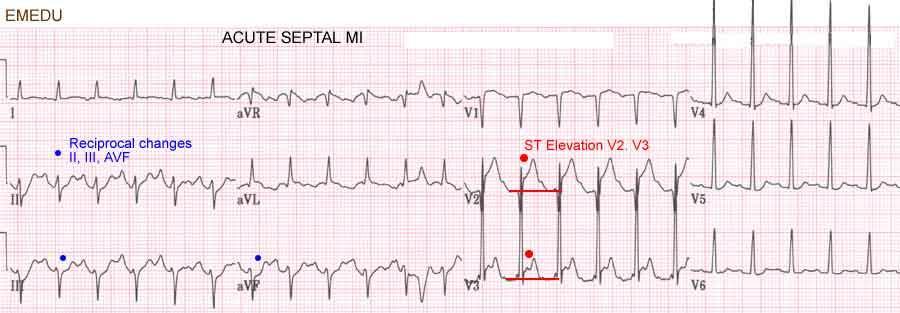
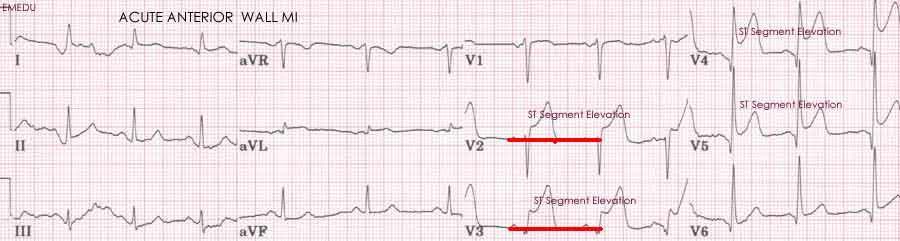
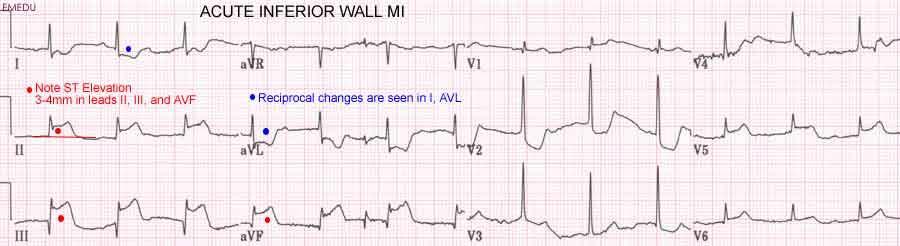
24 I- Abnormalities of ECG Waves and Segments QRS Abnormalities: Q Wave in Myocardial Infarction Septal Localizing Old Myocardial Infarction by Presence of Q-Wave V1, V2 Inferior MI Anterior Lateral Inferior V1, V2, V3, V4 I, avl, V5, V6 II, III, avf Antero-spetal MI
25 I- Abnormalities of ECG Waves and Segments QRS Changes in Ventricular Hypertrophy


26 I- Abnormalities of ECG Waves and Segments QRS Changes in Ventricular Hypertrophy RVH LVH


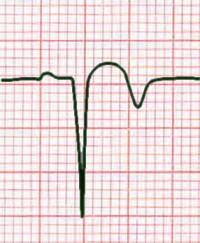
27 I- Abnormalities of ECG Waves and Segments T Wave abnormalities T wave abnormalities are common and often rather nonspecific. Ischaemia: T wave is inverted and symmetrical. It is very important to know the features of hypo/hyperkalaemia. Hyperkalaemia Hypokalaemia

28 I- Abnormalities of ECG Waves and Segments T Wave abnormalities in Hyperkaleamia Flattened P wave with 1 st * HB

29 II- Pacemaker Abnormalities

30 II- Pacemaker Abnormalities Supraventricular Abnormalities

31 II- Pacemaker Abnormalities Supraventricular Abnormalities

32 II- Pacemaker Abnormalities Supraventricular Abnormalities

33 II- Pacemaker Abnormalities Supraventricular Abnormalities

34 II- Pacemaker Abnormalities Supraventricular Abnormalities

35 II- Pacemaker Abnormalities Supraventricular Abnormalities
36 II- Pacemaker Abnormalities Supraventricular Tachycardia with Irregular Heart Rate Atrial Fibrillation Atrial Flutter with variable Atrio-Ventricular Block Multifocal (Chaotic) Atrial Tachycardia Multiple Premature Atrial Complexes


37 II- Pacemaker Abnormalities Supraventricular Tachycardia with Irregular Heart Rate *Atrial Fibrillation

38 II- Pacemaker Abnormalities Supraventricular Tachycardia with Irregular Heart Rate *Atrial Fibrillation (slow ventricular response)

39 II- Pacemaker Abnormalities Supraventricular Tachycardia with Irregular Heart Rate *Atrial Fibrillation (fast ventricular response)
 Atrial Tachycardia in")
40 II- Pacemaker Abnormalities Supraventricular Tachycardia with Irregular Heart Rate *Multifocal (Chaotic) Atrial Tachycardia in one lead

41 II- Pacemaker Abnormalities Supraventricular Tachycardia with Irregular Heart Rate *Multiple Premature Atrial Complexes


42 II- Pacemaker Abnormalities Supraventricular Tachycardia with Irregular Heart Rate Atrial Flutter with variable AtrioVentricular Conduction
43 II- Pacemaker Abnormalities Supraventricular Tachycardia with Regular Heart Rate Atrial Flutter with fixed (i.e. 2:1) AtrioVentricular Conduction Atrioventricular-Nodal Reenterant Tachycardia (AVNRT) Atrioventricular Reenterant Tachycardia (AVRT) Atrial Tachycardia (AT)


44 II- Pacemaker Abnormalities Supraventricular Tachycardia with Regular Heart Rate *Atrial Flutter with 2:1 AtrioVentricular Conduction
45 II- Pacemaker Abnormalities Supraventricular Tachycardia with Regular Heart Rate: *Atrioventricular-Nodal Reenterant Tachycardia (AVNRT) No Clearly Visible P Waves
46 II- Pacemaker Abnormalities Supraventricular Tachycardia with Regular Heart Rate: *Atrioventricular Reenterant Tachycardia (AVRT)

47 II- Pacemaker Abnormalities Supraventricular Tachycardia with Regular Heart Rate: *Atrial Tachycardia (AT)
48 II- Pacemaker Abnormalities Supraventricular Tachycardia with Regular Heart Rate Atrioventricular-Nodal Reenterant Tachycardia (AVNRT) Atrioventricular Reenterant Tachycardia (AVRT) Atrial Tachycardia (AT) P is not seen (and probably lost within the QRS) P is after the QRS, consider accessory pathway P is inscribed before the QRS with abnormal morphology A re-entrant circuit between slow and fast pathways of the AVN A re-entrant circuit via an accessory pathway P wave coming from ectopic atrial focus



49 II- Pacemaker Abnormalities Supraventricular Tachycardia with Regular Heart Rate Atrioventricular-Nodal Reenterant Tachycardia (AVNRT) Atrioventricular Reenterant Tachycardia (AVRT) Atrial Tachycardia (AT)
50 II- Pacemaker Abnormalities Supraventricular Tachycardia with Regular Heart Rate Atrioventricular-Nodal Reenterant Tachycardia (AVNRT) Atrioventricular Reenterant Tachycardia (AVRT) Atrial Tachycardia (AT)



51 II- Pacemaker Abnormalities Supraventricular Tachycardia with Regular Heart Rate Atrioventricular-Nodal Reenterant Tachycardia (AVNRT)
52 II- Pacemaker Abnormalities Supraventricular Tachycardia with Regular Heart Rate Atrioventricular-Nodal Reenterant Tachycardia (AVNRT) No Clearly Visible P Waves

53 II- Pacemaker Abnormalities Supraventricular Tachycardia with Regular Heart Rate AtrioVentricular Reenterant Tachycardia (AVRT)

54 Pacemaker/Conduction Abnormalities Accessory Pathway or Wolf Parkinson White (WPW) Syndrome Abnormal, congenital extra pathways between the atria and ventricles or/and conduction tissue, and can perforate the electrically insulating fibrous ring that normally separates the atrial and the ventricular chambers. Atrio-Ventricular conduction could be achieved bypassing the AV node. This means that fast Atrial rates (i.e. AF) could be conducted to ventricles at high rates causing serious tachycardia.

 The other way around (down accessory pathway, up AV node, termed antidromic tachycardia) WPW Syndrome")
55 Pacemaker/Conduction Abnormalities WPW Syndrome The WPW syndrome is a combination of the pre-excitation pattern, and tachycardia. The tachycardia may be due to impulse conduction down via the AV node and back up the accessory pathway (commonest, called orthodromic tachycardia) The other way around (down accessory pathway, up AV node, termed antidromic tachycardia) WPW Syndrome = short PR interval + Delta wave + Wide QRS complex + Tachycardia Pre-exited ECG = short PR interval + Delta wave + Wide QRS complex
56 Pacemaker Abnormalities Supraventricular Tachycardia with Regular Heart Rate AtrioVentricular Reenterant Tachycardia (AVRT)

57 Pacemaker/Conduction Abnormalities Pre Excited ECG


58 II- Pacemaker Abnormalities Ventricular Abnormalities Ventricular Extrasystoles
 lasting < 30s are subgrouped into salvos of 3 to 5 consecutive impulses and nonsustained VT of six or more impulses in")
59 II- Pacemaker Abnormalities Ventricular Abnormalities Nonsustained Ventricular Tachycardia Runs of repetitive premature ventricular impulses (rate > 100/m) lasting < 30s are subgrouped into salvos of 3 to 5 consecutive impulses and nonsustained VT of six or more impulses in duration.

60 II- Pacemaker Abnormalities Ventricular Abnormalities Sustaiend Ventricular Tachycardia Monomorphic Polymorphic Ventricular Tachycardia (Torsaed des Pointes)

61 II- Pacemaker Abnormalities Ventricular Abnormalities Ventricular Fibrillation and Asystole


62 II- Pacemaker Abnormalities Ventricular Abnormalities Ventricular Flutter Ventricular 'flutter' is a bizarre sine-wave like rhythm, and usually degenerates into ventricular fibrillation.

63 II- Pacemaker Abnormalities Ventricular Abnormalities Ventricular Fibrillation and Asystole
64 III- Conduction Abnormalities 1) Sino-Atrial Block 2) Atrio-Ventricular Block 3) Bundle Branch Block 4) WPW Syndrome (mentioned before in Pacemaker Abnormalities) 5) The Long QT Syndrome
65 III- Conduction Abnormalities Sino-Atrial Block

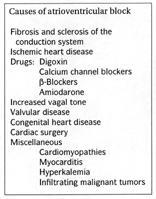
66 III- Conduction Abnormalities Atrio-Ventricular Block


67 III- Conduction Abnormalities Atrio-Ventricular Block First Degree Heart Block


68 III- Conduction Abnormalities Atrio-Ventricular Block Second Degree Heart Block (Mobitz I) or (Wenckebach)


69 III- Conduction Abnormalities Atrio-Ventricular Block Second Degree Heart Block (Mobitz II)


70 III- Conduction Abnormalities Atrio-Ventricular Block Third Degree Heart Block

71 III- Conduction Abnormalities Bundle Branch Block


72 III- Conduction Abnormalities Left Bundle Branch Block

73 III- Conduction Abnormalities Left Bundle Branch Block


74 III- Conduction Abnormalities Right Bundle Branch Block

75 III- Conduction Abnormalities Right Bundle Branch Block

76 III- Conduction Abnormalities Left Anterior Fascicular Block
77 III- Conduction Abnormalities The Long QT Syndrome Normally, the QT-interval is less than 50% of the preceding RR-interval. The long QT-interval symbolises a long ventricular systole. The ST-interval is simultaneous with the phase 2 plateau of the ventricular membrane action potential. The slow Ca2+ -Na+ - channels remain open for more than 300 ms as normally. The net influx of Ca2+ and Na+ is almost balanced by a net outflux of K+. Hereby, a long phase 2 plateau or isoelectric segment is formed. Long QT syndrome one of the common causes of unexplained sudden cardiac death (especially in young people) due to occurrence of fatal arrhythmia called (Torsades de pointes, i.e. polymorphic VT).

78 III- Conduction Abnormalities The Long QT Syndrome

79 III- Conduction Abnormalities The Long QT Syndrome
80 IV- Ischemic Abnormalities
81 IV- Ischemic Abnormalities
82 IV- Ischemic Abnormalities
83 IV- Ischemic Abnormalities
84 IV- Ischemic Abnormalities
85 IV- Ischemic Abnormalities
86 IV- Ischemic Abnormalities
87 IV- Ischemic Abnormalities
88 IV- Ischemic Abnormalities
89 IV- Ischemic Abnormalities
90 IV- Ischemic Abnormalities
91 IV- Ischemic Abnormalities
92 IV- Ischemic Abnormalities
93 IV- Ischemic Abnormalities
94 IV- Ischemic Abnormalities
95 IV- Ischemic Abnormalities
96 IV- Ischemic Abnormalities
Please check your answers with correct statements in answer pages after the ECG cases.
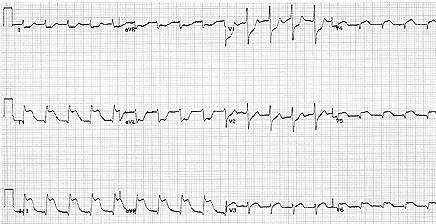
 ECG Cases ECG Case 1 Springer International Publishing AG, part of Springer Nature 2018 S. Okutucu, A. Oto, Interpreting ECGs in Clinical Practice, In Clinical Practice, https://doi.org/10.1007/978-3-319-90557-0
ECG Cases ECG Case 1 Springer International Publishing AG, part of Springer Nature 2018 S. Okutucu, A. Oto, Interpreting ECGs in Clinical Practice, In Clinical Practice, https://doi.org/10.1007/978-3-319-90557-0
Huseng Vefali MD St. Luke s University Health Network Department of Cardiology
 Huseng Vefali MD St. Luke s University Health Network Department of Cardiology Learning Objectives Establish Consistent Approach to Interpreting ECGs Review Essential Cases for Paramedics and first responders
Huseng Vefali MD St. Luke s University Health Network Department of Cardiology Learning Objectives Establish Consistent Approach to Interpreting ECGs Review Essential Cases for Paramedics and first responders
ELECTROCARDIOGRAPH. General. Heart Rate. Starship Children s Health Clinical Guideline
 General Heart Rate QRS Axis T Wave Axis PR Interval according to Heart Rate & Age P Wave Duration and Amplitude QRS Duration according to Age QT Interval R & S voltages according to Lead & Age R/S ratio
General Heart Rate QRS Axis T Wave Axis PR Interval according to Heart Rate & Age P Wave Duration and Amplitude QRS Duration according to Age QT Interval R & S voltages according to Lead & Age R/S ratio
Appendix D Output Code and Interpretation of Analysis
 Appendix D Output Code and Interpretation of Analysis 8 Arrhythmia Code No. Description 8002 Marked rhythm irregularity 8110 Sinus rhythm 8102 Sinus arrhythmia 8108 Marked sinus arrhythmia 8120 Sinus tachycardia
Appendix D Output Code and Interpretation of Analysis 8 Arrhythmia Code No. Description 8002 Marked rhythm irregularity 8110 Sinus rhythm 8102 Sinus arrhythmia 8108 Marked sinus arrhythmia 8120 Sinus tachycardia
ECG ABNORMALITIES D R. T AM A R A AL Q U D AH
 ECG ABNORMALITIES D R. T AM A R A AL Q U D AH When we interpret an ECG we compare it instantaneously with the normal ECG and normal variants stored in our memory; these memories are stored visually in
ECG ABNORMALITIES D R. T AM A R A AL Q U D AH When we interpret an ECG we compare it instantaneously with the normal ECG and normal variants stored in our memory; these memories are stored visually in
Basic electrocardiography reading. R3 lee wei-chieh
 Basic electrocardiography reading R3 lee wei-chieh The Normal Conduction System Lead Placement avf Limb Leads Precordial Leads Interpretation Rate Rhythm Interval Axis Chamber abnormality QRST change What
Basic electrocardiography reading R3 lee wei-chieh The Normal Conduction System Lead Placement avf Limb Leads Precordial Leads Interpretation Rate Rhythm Interval Axis Chamber abnormality QRST change What
If the P wave > 0.12 sec( 3 mm) usually in any lead. Notched P wave usually in lead I,aVl may be lead II Negative terminal portion of P wave in V1, 1
 usually in any lead. Notched P wave usually in lead I,aVl may be lead II Negative terminal portion of P wave in V1, 1") If the P wave > 0.12 sec( 3 mm) usually in any lead. Notched P wave usually in lead I,aVl may be lead II Negative terminal portion of P wave in V1, 1 mm depth and 3 mm width( most specific) Since Mitral
If the P wave > 0.12 sec( 3 mm) usually in any lead. Notched P wave usually in lead I,aVl may be lead II Negative terminal portion of P wave in V1, 1 mm depth and 3 mm width( most specific) Since Mitral
Cardiology Flash Cards
 Cardiology Flash Cards EKG in a nut shell www.brain101.info Conduction System www.brain101.info 2 Analyzing EKG Step by step Steps in Analyzing ECG'S 1. Rhythm: - Regular _ Sinus, Junctional or Ventricular.
Cardiology Flash Cards EKG in a nut shell www.brain101.info Conduction System www.brain101.info 2 Analyzing EKG Step by step Steps in Analyzing ECG'S 1. Rhythm: - Regular _ Sinus, Junctional or Ventricular.
Pennsylvania Academy of Family Physicians Foundation & UPMC 43rd Refresher Course in Family Medicine CME Conference March 10-13, 2016
 Pennsylvania Academy of Family Physicians Foundation & UPMC 43rd Refresher Course in Family Medicine CME Conference March 10-13, 2016 Disclosures: EKG Workshop Louis Mancano, MD Speaker has no disclosures
Pennsylvania Academy of Family Physicians Foundation & UPMC 43rd Refresher Course in Family Medicine CME Conference March 10-13, 2016 Disclosures: EKG Workshop Louis Mancano, MD Speaker has no disclosures
SIMPLY ECGs. Dr William Dooley
 SIMPLY ECGs Dr William Dooley Content Basic ECG interpretation pattern Some common (examined) abnormalities Presenting ECGs in context Setting up an ECG Setting up an ECG 1 V1-4 th Right intercostal space
SIMPLY ECGs Dr William Dooley Content Basic ECG interpretation pattern Some common (examined) abnormalities Presenting ECGs in context Setting up an ECG Setting up an ECG 1 V1-4 th Right intercostal space
12-Lead ECG Interpretation. Kathy Kuznar, RN, ANP
 12-Lead ECG Interpretation Kathy Kuznar, RN, ANP The 12-Lead ECG Objectives Identify the normal morphology and features of the 12- lead ECG. Perform systematic analysis of the 12-lead ECG. Recognize abnormalities
12-Lead ECG Interpretation Kathy Kuznar, RN, ANP The 12-Lead ECG Objectives Identify the normal morphology and features of the 12- lead ECG. Perform systematic analysis of the 12-lead ECG. Recognize abnormalities
DR QAZI IMTIAZ RASOOL OBJECTIVES
 PRACTICAL ELECTROCARDIOGRAPHY DR QAZI IMTIAZ RASOOL OBJECTIVES Recording of electrical events in heart Established electrode pattern results in specific tracing pattern Health of heart i. e. Anatomical
PRACTICAL ELECTROCARDIOGRAPHY DR QAZI IMTIAZ RASOOL OBJECTIVES Recording of electrical events in heart Established electrode pattern results in specific tracing pattern Health of heart i. e. Anatomical
The Electrocardiogram part II. Dr. Adelina Vlad, MD PhD
 The Electrocardiogram part II Dr. Adelina Vlad, MD PhD Basic Interpretation of the ECG 1) Evaluate calibration 2) Calculate rate 3) Determine rhythm 4) Determine QRS axis 5) Measure intervals 6) Analyze
The Electrocardiogram part II Dr. Adelina Vlad, MD PhD Basic Interpretation of the ECG 1) Evaluate calibration 2) Calculate rate 3) Determine rhythm 4) Determine QRS axis 5) Measure intervals 6) Analyze
Paediatric ECG Interpretation
 Paediatric ECG Interpretation Dr Sanj Fernando (thanks to http://lifeinthefastlane.com/ecg-library/paediatric-ecginterpretation/) 3 yo boy complaining of abdominal pain and chest pain Child ECG vs Adult
Paediatric ECG Interpretation Dr Sanj Fernando (thanks to http://lifeinthefastlane.com/ecg-library/paediatric-ecginterpretation/) 3 yo boy complaining of abdominal pain and chest pain Child ECG vs Adult
REtrive. REpeat. RElearn Design by. Test-Enhanced Learning based ECG practice E-book
 Test-Enhanced Learning Test-Enhanced Learning Test-Enhanced Learning Test-Enhanced Learning based ECG practice E-book REtrive REpeat RElearn Design by S I T T I N U N T H A N G J U I P E E R I Y A W A
Test-Enhanced Learning Test-Enhanced Learning Test-Enhanced Learning Test-Enhanced Learning based ECG practice E-book REtrive REpeat RElearn Design by S I T T I N U N T H A N G J U I P E E R I Y A W A
ECGs: Everything a finalist needs to know. Dr Amy Coulden As part of the Simply Finals series
 ECGs: Everything a finalist needs to know Dr Amy Coulden As part of the Simply Finals series Aims and objectives To be able to interpret basic ECG abnormalities To be able to recognise commonly tested
ECGs: Everything a finalist needs to know Dr Amy Coulden As part of the Simply Finals series Aims and objectives To be able to interpret basic ECG abnormalities To be able to recognise commonly tested
Family Medicine for English language students of Medical University of Lodz ECG. Jakub Dorożyński
 Family Medicine for English language students of Medical University of Lodz ECG Jakub Dorożyński Parts of an ECG The standard ECG has 12 leads: six of them are considered limb leads because they are placed
Family Medicine for English language students of Medical University of Lodz ECG Jakub Dorożyński Parts of an ECG The standard ECG has 12 leads: six of them are considered limb leads because they are placed
ECG CONVENTIONS AND INTERVALS
 1 ECG Waveforms and Intervals ECG waveforms labeled alphabetically P wave== represents atrial depolarization QRS complex=ventricular depolarization ST-T-U complex (ST segment, T wave, and U wave)== V repolarization.
1 ECG Waveforms and Intervals ECG waveforms labeled alphabetically P wave== represents atrial depolarization QRS complex=ventricular depolarization ST-T-U complex (ST segment, T wave, and U wave)== V repolarization.
CASE 10. What would the ST segment of this ECG look like? On which leads would you see this ST segment change? What does the T wave represent?
 CASE 10 A 57-year-old man presents to the emergency center with complaints of chest pain with radiation to the left arm and jaw. He reports feeling anxious, diaphoretic, and short of breath. His past history
CASE 10 A 57-year-old man presents to the emergency center with complaints of chest pain with radiation to the left arm and jaw. He reports feeling anxious, diaphoretic, and short of breath. His past history
UNDERSTANDING YOUR ECG: A REVIEW
 UNDERSTANDING YOUR ECG: A REVIEW Health professionals use the electrocardiograph (ECG) rhythm strip to systematically analyse the cardiac rhythm. Before the systematic process of ECG analysis is described
UNDERSTANDING YOUR ECG: A REVIEW Health professionals use the electrocardiograph (ECG) rhythm strip to systematically analyse the cardiac rhythm. Before the systematic process of ECG analysis is described
Chapter 16: Arrhythmias and Conduction Disturbances
 Complete the following. Chapter 16: Arrhythmias and Conduction Disturbances 1. Cardiac arrhythmias result from abnormal impulse, abnormal impulse, or both mechanisms together. 2. is the ability of certain
Complete the following. Chapter 16: Arrhythmias and Conduction Disturbances 1. Cardiac arrhythmias result from abnormal impulse, abnormal impulse, or both mechanisms together. 2. is the ability of certain
Supraventricular Arrhythmias. Reading Assignment. Chapter 5 (p17-30)
") Supraventricular Arrhythmias Reading Assignment Chapter 5 (p17-30) The Supraventricular Rhythms In Our Lives Site of Origin Single Events Slow Rates Intermediate Rates Fast Rates (>100 bpm) Sinus Sinus
Supraventricular Arrhythmias Reading Assignment Chapter 5 (p17-30) The Supraventricular Rhythms In Our Lives Site of Origin Single Events Slow Rates Intermediate Rates Fast Rates (>100 bpm) Sinus Sinus
ECGs and Arrhythmias: Family Medicine Board Review 2009
 Rate Rhythm Intervals Hypertrophy ECGs and Arrhythmias: Family Medicine Board Review 2009 Axis Jess (Fogler) Waldura, MD University of California, San Francisco walduraj@nccc.ucsf.edu Ischemia Overview
Rate Rhythm Intervals Hypertrophy ECGs and Arrhythmias: Family Medicine Board Review 2009 Axis Jess (Fogler) Waldura, MD University of California, San Francisco walduraj@nccc.ucsf.edu Ischemia Overview
Conduction Problems / Arrhythmias. Conduction
 Conduction Problems / Arrhythmias Conduction Wolf-Parkinson White Syndrome (WPW) and Lown-Ganong-Levine (LGL): Atrial impulses bypass the AV node through an accessory pathway or bypass tract (bundle of
Conduction Problems / Arrhythmias Conduction Wolf-Parkinson White Syndrome (WPW) and Lown-Ganong-Levine (LGL): Atrial impulses bypass the AV node through an accessory pathway or bypass tract (bundle of
SIMPLY ECGs. Dr William Dooley
 SIMPLY ECGs Dr William Dooley 1 No anatomy just interpretation 2 Setting up an ECG 3 Setting up an ECG 1 V1-4 th Right intercostal space at sternal border 2 V2-4 th Left intercostal space at sternal border
SIMPLY ECGs Dr William Dooley 1 No anatomy just interpretation 2 Setting up an ECG 3 Setting up an ECG 1 V1-4 th Right intercostal space at sternal border 2 V2-4 th Left intercostal space at sternal border
ECG (MCQs) In the fundamental rules of the ECG all the following are right EXCEP:
 In the fundamental rules of the ECG all the following are right EXCEP:") ECG (MCQs) 2010 1- In the fundamental rules of the ECG all the following are right EXCEP: a- It is a biphasic record of myocardial action potential fluctuations. b- Deflection record occurs only during
ECG (MCQs) 2010 1- In the fundamental rules of the ECG all the following are right EXCEP: a- It is a biphasic record of myocardial action potential fluctuations. b- Deflection record occurs only during
ECG pre-reading manual. Created for the North West Regional EMET training program
 ECG pre-reading manual Created for the North West Regional EMET training program Author:- Dr Juan Carlos Ascencio-Lane juan.ascencio-lane@ths.tas.gov.au 1 Disclaimer This handbook has been created for
ECG pre-reading manual Created for the North West Regional EMET training program Author:- Dr Juan Carlos Ascencio-Lane juan.ascencio-lane@ths.tas.gov.au 1 Disclaimer This handbook has been created for
Diploma in Electrocardiography
 The Society for Cardiological Science and Technology Diploma in Electrocardiography The Society makes this award to candidates who can demonstrate the ability to accurately record a resting 12-lead electrocardiogram
The Society for Cardiological Science and Technology Diploma in Electrocardiography The Society makes this award to candidates who can demonstrate the ability to accurately record a resting 12-lead electrocardiogram
Pathologic ECG. Adelina Vlad, MD PhD
 Pathologic ECG Adelina Vlad, MD PhD Basic Interpretation of the ECG 1) Evaluate calibration 2) Calculate rate 3) Determine rhythm 4) Determine QRS axis 5) Measure intervals 6) Analyze the morphology and
Pathologic ECG Adelina Vlad, MD PhD Basic Interpretation of the ECG 1) Evaluate calibration 2) Calculate rate 3) Determine rhythm 4) Determine QRS axis 5) Measure intervals 6) Analyze the morphology and
Introduction to ECG Gary Martin, M.D.
 Brief review of basic concepts Introduction to ECG Gary Martin, M.D. The electrical activity of the heart is caused by a sequence of rapid ionic movements across cell membranes resulting first in depolarization
Brief review of basic concepts Introduction to ECG Gary Martin, M.D. The electrical activity of the heart is caused by a sequence of rapid ionic movements across cell membranes resulting first in depolarization
ECG Interpretation Cat Williams, DVM DACVIM (Cardiology)
") ECG Interpretation Cat Williams, DVM DACVIM (Cardiology) Providing the best quality care and service for the patient, the client, and the referring veterinarian. GOAL: Reduce Anxiety about ECGs Back to
ECG Interpretation Cat Williams, DVM DACVIM (Cardiology) Providing the best quality care and service for the patient, the client, and the referring veterinarian. GOAL: Reduce Anxiety about ECGs Back to
-RHYTHM PRACTICE- By Dr.moanes Msc.cardiology Assistant Lecturer of Cardiology Al Azhar University. OBHG Education Subcommittee
 -RHYTHM PRACTICE- By Dr.moanes Msc.cardiology Assistant Lecturer of Cardiology Al Azhar University The Normal Conduction System Sinus Node Normal Sinus Rhythm (NSR) Sinus Bradycardia Sinus Tachycardia
-RHYTHM PRACTICE- By Dr.moanes Msc.cardiology Assistant Lecturer of Cardiology Al Azhar University The Normal Conduction System Sinus Node Normal Sinus Rhythm (NSR) Sinus Bradycardia Sinus Tachycardia
a lecture series by SWESEMJR
 Arrhythmias Automaticity- the ability to depolarize spontaneously. Pacemakers: Sinoatrial node: 70 bpm AV-nodal area: 40 bpm His-Purkinje: 20-40 bpm it Mechanisms of arrhythmias 1. Increased automaticity
Arrhythmias Automaticity- the ability to depolarize spontaneously. Pacemakers: Sinoatrial node: 70 bpm AV-nodal area: 40 bpm His-Purkinje: 20-40 bpm it Mechanisms of arrhythmias 1. Increased automaticity
ECG Interactive Session
 SA HEART 2018 PRE-CONGRESS WORKSHOP 4 OCTOBER 2018 ECG Interactive Session Ashley Chin Cardiologist/Electrophysiologist University of Cape Town Groote Schuur Hospital ECG 1 Which ONE of the following is
SA HEART 2018 PRE-CONGRESS WORKSHOP 4 OCTOBER 2018 ECG Interactive Session Ashley Chin Cardiologist/Electrophysiologist University of Cape Town Groote Schuur Hospital ECG 1 Which ONE of the following is
PAEDIATRIC ECG Dimosthenis Avramidis, MD.
 PAEDIATRIC ECG Dimosthenis Avramidis, MD. Consultant Mitera Children s Hospital Athens Greece S. Associate 1st Cardiology Dpt Evangelismos Hospital Athens Greece 5 y/o with sinus tach Background ECG changes
PAEDIATRIC ECG Dimosthenis Avramidis, MD. Consultant Mitera Children s Hospital Athens Greece S. Associate 1st Cardiology Dpt Evangelismos Hospital Athens Greece 5 y/o with sinus tach Background ECG changes
Return to Basics. ECG Rate and Rhythm. Management of the Hospitalized Patient September 25, 2009
 Management of the Hospitalized Patient September 25, 2009 ECG Refresher and Update 2009 Return to Basics Determine rate and rhythm Determine intervals and axes Define morphology of P-QRS-T-U Compare with
Management of the Hospitalized Patient September 25, 2009 ECG Refresher and Update 2009 Return to Basics Determine rate and rhythm Determine intervals and axes Define morphology of P-QRS-T-U Compare with
ECG Basics Sonia Samtani 7/2017 UCI Resident Lecture Series
 ECG Basics Sonia Samtani 7/2017 UCI Resident Lecture Series Agenda I. Introduction II.The Conduction System III.ECG Basics IV.Cardiac Emergencies V.Summary The Conduction System Lead Placement avf Precordial
ECG Basics Sonia Samtani 7/2017 UCI Resident Lecture Series Agenda I. Introduction II.The Conduction System III.ECG Basics IV.Cardiac Emergencies V.Summary The Conduction System Lead Placement avf Precordial
General Introduction to ECG. Reading Assignment (p2-16 in PDF Outline )
") General Introduction to ECG Reading Assignment (p2-16 in PDF Outline ) Objectives 1. Practice the 5-step Method 2. Differential Diagnosis: R & L axis deviation 3. Differential Diagnosis: Poor R-wave progression
General Introduction to ECG Reading Assignment (p2-16 in PDF Outline ) Objectives 1. Practice the 5-step Method 2. Differential Diagnosis: R & L axis deviation 3. Differential Diagnosis: Poor R-wave progression
Rate: The atrial and ventricular rates are equal; heart rate is greater than 100 bpm (usually between bpm).
.") Sinus Bradycardia Regularity: The R-R intervals are constant; the rhythm is regular. Rate: The atrial and ventricular rates are equal; heart rate is less than 60 bpm. P wave: There is a uniform P wave
Sinus Bradycardia Regularity: The R-R intervals are constant; the rhythm is regular. Rate: The atrial and ventricular rates are equal; heart rate is less than 60 bpm. P wave: There is a uniform P wave
Skin supplied by T1-4 (medial upper arm and neck) T5-9- epigastrium Visceral afferents from skin and heart are the same dorsal root ganglio
 T5-9- epigastrium Visceral afferents from skin and heart are the same dorsal root ganglio") Cardio 2 ECG... 3 Cardiac Remodelling... 11 Valvular Diseases... 13 Hypertension... 18 Aortic Coarctation... 24 Erythropoiesis... 27 Haemostasis... 30 Anaemia... 36 Atherosclerosis... 44 Angina... 48 Myocardial
Cardio 2 ECG... 3 Cardiac Remodelling... 11 Valvular Diseases... 13 Hypertension... 18 Aortic Coarctation... 24 Erythropoiesis... 27 Haemostasis... 30 Anaemia... 36 Atherosclerosis... 44 Angina... 48 Myocardial
1 st Degree Block Prolonged P-R interval caused by first degree heart block (lead II)
") AV Heart Blocks 1 st degree A condition of a rhythm, not a true rhythm Need to always state underlying rhythm 2 nd degree Type I - Wenckebach Type II Classic dangerous to the patient Can be variable (periodic)
AV Heart Blocks 1 st degree A condition of a rhythm, not a true rhythm Need to always state underlying rhythm 2 nd degree Type I - Wenckebach Type II Classic dangerous to the patient Can be variable (periodic)
Return to Basics. Normal Intervals & Axes. ECG Rate and Rhythm
 Return to Basics Management of the Hospitalized Patient October 15, 2010 ECG Refresher and Update 2010 Determine rate and rhythm Determine intervals and axes Define morphology of P-QRS-T-U Compare with
Return to Basics Management of the Hospitalized Patient October 15, 2010 ECG Refresher and Update 2010 Determine rate and rhythm Determine intervals and axes Define morphology of P-QRS-T-U Compare with
This presentation will deal with the basics of ECG description as well as the physiological basics of
 Snímka 1 Electrocardiography basics This presentation will deal with the basics of ECG description as well as the physiological basics of Snímka 2 Lecture overview 1. Cardiac conduction system functional
Snímka 1 Electrocardiography basics This presentation will deal with the basics of ECG description as well as the physiological basics of Snímka 2 Lecture overview 1. Cardiac conduction system functional
ECGs and Arrhythmias: Family Medicine Board Review 2012
 Overview ECGs and Arrhythmias: Family Medicine Board Review 2012 Jess Waldura, MD University of California, San Francisco walduraj@nccc.ucsf.edu Bundle branch blocks Quick review of ischemia Arrhythmias
Overview ECGs and Arrhythmias: Family Medicine Board Review 2012 Jess Waldura, MD University of California, San Francisco walduraj@nccc.ucsf.edu Bundle branch blocks Quick review of ischemia Arrhythmias
PATIENT S NAME, DATE/TIME,
 ECG and Arrhythmias Dec, 1 st 2014 Doctor Mohammad Jarrah References: - Lecture and Slides - ECG Made Easy - Davidson Principles of Medicine - First Aid Cases for the USMLE Step 1 - Mini-OSCE Archive ECG
ECG and Arrhythmias Dec, 1 st 2014 Doctor Mohammad Jarrah References: - Lecture and Slides - ECG Made Easy - Davidson Principles of Medicine - First Aid Cases for the USMLE Step 1 - Mini-OSCE Archive ECG
2017 EKG Workshop Advanced. Family Medicine Review Course Lou Mancano, MD, FAAFP Reading Health System Family and Community Medicine Reading, PA
 2017 EKG Workshop Advanced Family Medicine Review Course Lou Mancano, MD, FAAFP Reading Health System Family and Community Medicine Reading, PA Part II - Objective Describe a useful approach to interpreting
2017 EKG Workshop Advanced Family Medicine Review Course Lou Mancano, MD, FAAFP Reading Health System Family and Community Medicine Reading, PA Part II - Objective Describe a useful approach to interpreting
Study methodology for screening candidates to athletes risk
 1. Periodical Evaluations: each 2 years. Study methodology for screening candidates to athletes risk 2. Personal history: Personal history of murmur in childhood; dizziness, syncope, palpitations, intolerance
1. Periodical Evaluations: each 2 years. Study methodology for screening candidates to athletes risk 2. Personal history: Personal history of murmur in childhood; dizziness, syncope, palpitations, intolerance
HR: 50 bpm (Sinus) PR: 280 ms QRS: 120 ms QT: 490 ms Axis: -70. Sinus bradycardia with one ventricular escape (*)
 PR: 280 ms QRS: 120 ms QT: 490 ms Axis: -70. Sinus bradycardia with one ventricular escape (*)") 1? HR: 50 bpm (Sinus) PR: 280 ms QRS: 120 ms QT: 490 ms Axis: -70 1 Sinus P waves? 2 sinus cycles The pause (2 sinus cycles) suggests that the sinus fired (?) but did not conduct to the atria (i.e., missing
1? HR: 50 bpm (Sinus) PR: 280 ms QRS: 120 ms QT: 490 ms Axis: -70 1 Sinus P waves? 2 sinus cycles The pause (2 sinus cycles) suggests that the sinus fired (?) but did not conduct to the atria (i.e., missing
ELECTROCARDIOGRAPHY (III) THE ANALYSIS OF THE ELECTROCARDIOGRAM
 THE ANALYSIS OF THE ELECTROCARDIOGRAM") ELECTROCARDIOGRAPHY (III) THE ANALYSIS OF THE ELECTROCARDIOGRAM Scridon Alina, Șerban Răzvan Constantin Recording and analysis of the 12-lead ECG is part of the basic medical assessment performed for every
ELECTROCARDIOGRAPHY (III) THE ANALYSIS OF THE ELECTROCARDIOGRAM Scridon Alina, Șerban Răzvan Constantin Recording and analysis of the 12-lead ECG is part of the basic medical assessment performed for every
Step by step approach to EKG rhythm interpretation:
 Sinus Rhythms Normal sinus arrhythmia Small, slow variation of the R-R interval i.e. variation of the normal sinus heart rate with respiration, etc. Sinus Tachycardia Defined as sinus rhythm with a rate
Sinus Rhythms Normal sinus arrhythmia Small, slow variation of the R-R interval i.e. variation of the normal sinus heart rate with respiration, etc. Sinus Tachycardia Defined as sinus rhythm with a rate
Understanding basics of EKG
 Understanding basics of EKG By Alula A.(R III) www.le.ac.uk Topic for discussion Understanding of cellular electrophysiology Basics Rate Rhythm Axis Intervals P wave QRS ST/T wave Abnormal EKGs Understanding
Understanding basics of EKG By Alula A.(R III) www.le.ac.uk Topic for discussion Understanding of cellular electrophysiology Basics Rate Rhythm Axis Intervals P wave QRS ST/T wave Abnormal EKGs Understanding
ECG interpretation basics
 ECG interpretation basics Michał Walczewski, MD Krzysztof Ozierański, MD 21.03.18 Electrical conduction system of the heart Limb leads Precordial leads 21.03.18 Precordial leads Precordial leads 21.03.18
ECG interpretation basics Michał Walczewski, MD Krzysztof Ozierański, MD 21.03.18 Electrical conduction system of the heart Limb leads Precordial leads 21.03.18 Precordial leads Precordial leads 21.03.18
Electrocardiography Abnormalities (Arrhythmias) 7. Faisal I. Mohammed, MD, PhD
 7. Faisal I. Mohammed, MD, PhD") Electrocardiography Abnormalities (Arrhythmias) 7 Faisal I. Mohammed, MD, PhD 1 Causes of Cardiac Arrythmias Abnormal rhythmicity of the pacemaker Shift of pacemaker from sinus node Blocks at different
Electrocardiography Abnormalities (Arrhythmias) 7 Faisal I. Mohammed, MD, PhD 1 Causes of Cardiac Arrythmias Abnormal rhythmicity of the pacemaker Shift of pacemaker from sinus node Blocks at different
How To Think About Rhythms and Conduction
 How To Think About Rhythms and Conduction Frank Yanowitz, MD Professor of Medicine (Cardiology) University of Utah School of Medicine Medical Director, IHC ECG Services Intermountain Healthcare http://ecg.utah.edu
How To Think About Rhythms and Conduction Frank Yanowitz, MD Professor of Medicine (Cardiology) University of Utah School of Medicine Medical Director, IHC ECG Services Intermountain Healthcare http://ecg.utah.edu
Dr.Binoy Skaria 13/07/15
 Dr.Binoy Skaria binoyskaria@hotmail.com binoy.skaria@heartofengland.nhs.uk 13/07/15 Acknowledgement Medtronic, Google images & Elsevier for slides Natalie Ryan, Events Manager, HEFT- for organising the
Dr.Binoy Skaria binoyskaria@hotmail.com binoy.skaria@heartofengland.nhs.uk 13/07/15 Acknowledgement Medtronic, Google images & Elsevier for slides Natalie Ryan, Events Manager, HEFT- for organising the
ECG Practice Strips Discussion part 1:
 ECG Practice Strips Discussion part 1: The first 20 strips are for teaching various abnormalities of the morphology of the waves of the ECG. Strips 21 and following are for teaching some abnormalities
ECG Practice Strips Discussion part 1: The first 20 strips are for teaching various abnormalities of the morphology of the waves of the ECG. Strips 21 and following are for teaching some abnormalities
Lab Activity 24 EKG. Portland Community College BI 232
 Lab Activity 24 EKG Reference: Dubin, Dale. Rapid Interpretation of EKG s. 6 th edition. Tampa: Cover Publishing Company, 2000. Portland Community College BI 232 Graph Paper 1 second equals 25 little boxes
Lab Activity 24 EKG Reference: Dubin, Dale. Rapid Interpretation of EKG s. 6 th edition. Tampa: Cover Publishing Company, 2000. Portland Community College BI 232 Graph Paper 1 second equals 25 little boxes
Understanding the 12-lead ECG, part II
 Bundle-branch blocks Understanding the 12-lead ECG, part II Most common electrocardiogram (ECG) abnormality Appears as a wider than normal S complex Occurs when one of the two bundle branches can t conduct
Bundle-branch blocks Understanding the 12-lead ECG, part II Most common electrocardiogram (ECG) abnormality Appears as a wider than normal S complex Occurs when one of the two bundle branches can t conduct
402 Index. B β-blockers, 4, 5 Bradyarrhythmias, 76 77
 Index A Acquired immunodeficiency syndrome (AIDS), 126, 163 Action potentials, 1, 5, 27 Acute coronary syndromes, 123t, 129 Adenosine, intravenous, 277 Alcohol abuse, as T wave inversion cause, 199 Aneurysm,
Index A Acquired immunodeficiency syndrome (AIDS), 126, 163 Action potentials, 1, 5, 27 Acute coronary syndromes, 123t, 129 Adenosine, intravenous, 277 Alcohol abuse, as T wave inversion cause, 199 Aneurysm,
CRC 431 ECG Basics. Bill Pruitt, MBA, RRT, CPFT, AE-C
 CRC 431 ECG Basics Bill Pruitt, MBA, RRT, CPFT, AE-C Resources White s 5 th ed. Ch 6 Electrocardiography Einthoven s Triangle Chest leads and limb leads Egan s 10 th ed. Ch 17 Interpreting the Electrocardiogram
CRC 431 ECG Basics Bill Pruitt, MBA, RRT, CPFT, AE-C Resources White s 5 th ed. Ch 6 Electrocardiography Einthoven s Triangle Chest leads and limb leads Egan s 10 th ed. Ch 17 Interpreting the Electrocardiogram
Chapter 2 Practical Approach
 Chapter 2 Practical Approach There are beginners in electrocardiogram (ECG) analysis who are fascinated by a special pattern (e.g., a bundle-branch block or a striking Q wave) and thereby overlook other
Chapter 2 Practical Approach There are beginners in electrocardiogram (ECG) analysis who are fascinated by a special pattern (e.g., a bundle-branch block or a striking Q wave) and thereby overlook other
ABCs of ECGs. Shelby L. Durler
 ABCs of ECGs Shelby L. Durler Objectives Review the A&P of the cardiac conduction system Placement and obtaining 4-lead and 12-lead ECGs Overview of the basics of ECG rhythm interpretation Intrinsic
ABCs of ECGs Shelby L. Durler Objectives Review the A&P of the cardiac conduction system Placement and obtaining 4-lead and 12-lead ECGs Overview of the basics of ECG rhythm interpretation Intrinsic
You Don t Want to Miss This One! Focus on can t miss EKG tracings
 You Don t Want to Miss This One! Focus on can t miss EKG tracings Renaissance St. Louis Grand Hotel Convention Center October 23, 2014 David K. Tan, M.D., EMT-T, FAAEM EMS Section Chief, Division of Emergency
You Don t Want to Miss This One! Focus on can t miss EKG tracings Renaissance St. Louis Grand Hotel Convention Center October 23, 2014 David K. Tan, M.D., EMT-T, FAAEM EMS Section Chief, Division of Emergency
Electrical System Overview Electrocardiograms Action Potentials 12-Lead Positioning Values To Memorize Calculating Rates
 Electrocardiograms Electrical System Overview James Lamberg 2/ 74 Action Potentials 12-Lead Positioning 3/ 74 4/ 74 Values To Memorize Inherent Rates SA: 60 to 100 AV: 40 to 60 Ventricles: 20 to 40 Normal
Electrocardiograms Electrical System Overview James Lamberg 2/ 74 Action Potentials 12-Lead Positioning 3/ 74 4/ 74 Values To Memorize Inherent Rates SA: 60 to 100 AV: 40 to 60 Ventricles: 20 to 40 Normal
Proceedings of the World Small Animal Veterinary Association Sydney, Australia 2007
 Proceedings of the World Small Animal Sydney, Australia 2007 Hosted by: Next WSAVA Congress ECG INTERPRETATION Adrian Boswood MA VetMB DVC DECVIM-CA(Cardiology) MRCVS The Royal Veterinary College, Hawkshead
Proceedings of the World Small Animal Sydney, Australia 2007 Hosted by: Next WSAVA Congress ECG INTERPRETATION Adrian Boswood MA VetMB DVC DECVIM-CA(Cardiology) MRCVS The Royal Veterinary College, Hawkshead
Module 1: Introduction to ECG & Normal ECG
 Module 1: Introduction to ECG & Normal ECG Importance of Correct anatomical positions Measurements & Morphologies ONLY accurate if Precise anatomical positions adhered to Standardised techniques are used
Module 1: Introduction to ECG & Normal ECG Importance of Correct anatomical positions Measurements & Morphologies ONLY accurate if Precise anatomical positions adhered to Standardised techniques are used
2) Heart Arrhythmias 2 - Dr. Abdullah Sharif
 Heart Arrhythmias 2 - Dr. Abdullah Sharif") 2) Heart Arrhythmias 2 - Dr. Abdullah Sharif Rhythms from the Sinus Node Sinus Tachycardia: HR > 100 b/m Causes: o Withdrawal of vagal tone & Sympathetic stimulation (exercise, fight or flight) o Fever
2) Heart Arrhythmias 2 - Dr. Abdullah Sharif Rhythms from the Sinus Node Sinus Tachycardia: HR > 100 b/m Causes: o Withdrawal of vagal tone & Sympathetic stimulation (exercise, fight or flight) o Fever
Paroxysmal Supraventricular Tachycardia PSVT.
 Atrial Tachycardia; is the name for an arrhythmia caused by a disorder of the impulse generation in the atrium or the AV node. An area in the atrium sends out rapid signals, which are faster than those
Atrial Tachycardia; is the name for an arrhythmia caused by a disorder of the impulse generation in the atrium or the AV node. An area in the atrium sends out rapid signals, which are faster than those
Acute Coronary Syndromes. Disclosures
 Acute Coronary Syndromes Disclosures I work for Virginia Garcia Memorial Health Center, Beaverton, OR. Jon Tardiff, BS, PA-C OHSU Clinical Assistant Professor And I am a medical editor for Jones & Bartlett
Acute Coronary Syndromes Disclosures I work for Virginia Garcia Memorial Health Center, Beaverton, OR. Jon Tardiff, BS, PA-C OHSU Clinical Assistant Professor And I am a medical editor for Jones & Bartlett
at least 4 8 hours per week
 ECG IN ATHLETS An athlete is defined as an individual who engages in regular exercise or training for sport or general fitness, typically with a premium on performance, and often engaged in individual
ECG IN ATHLETS An athlete is defined as an individual who engages in regular exercise or training for sport or general fitness, typically with a premium on performance, and often engaged in individual
1 Cardiology Acute Care Day 22 April 2013 Arrhythmia Tutorial Course Material
 1 Cardiology Acute Care Day 22 April 2013 Arrhythmia Tutorial Course Material Arrhythmia recognition This tutorial builds on the ECG lecture and provides a framework for approaching any ECG to allow the
1 Cardiology Acute Care Day 22 April 2013 Arrhythmia Tutorial Course Material Arrhythmia recognition This tutorial builds on the ECG lecture and provides a framework for approaching any ECG to allow the
ECG Interpretation. Introduction to Cardiac Telemetry. Michael Peters, RN, CCRN, CFRN CALSTAR Air Medical Services
 ECG Interpretation Introduction to Cardiac Telemetry Michael Peters, RN, CCRN, CFRN CALSTAR Air Medical Services Disclosures Nothing to disclose Objectives Describe the electrical conduction pathway in
ECG Interpretation Introduction to Cardiac Telemetry Michael Peters, RN, CCRN, CFRN CALSTAR Air Medical Services Disclosures Nothing to disclose Objectives Describe the electrical conduction pathway in
Ekg pra pr c a tice D.HAMMOUDI.MD
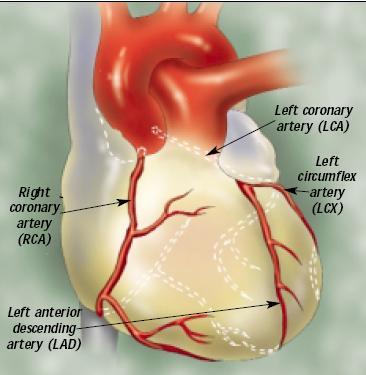
 Ekg practice D.HAMMOUDI.MD Anatomy Revisited RCA (Right Coronary Artery) Right ventricle Inferior wall of LV Posterior wall of LV (75%) SA Node (60%) AV Node (>80%) LCA (Left Coronary Artery) Septal wall
Ekg practice D.HAMMOUDI.MD Anatomy Revisited RCA (Right Coronary Artery) Right ventricle Inferior wall of LV Posterior wall of LV (75%) SA Node (60%) AV Node (>80%) LCA (Left Coronary Artery) Septal wall
Section V. Objectives
 Section V Landscape of an MI Objectives At the conclusion of this presentation the participant will be able to Outline a systematic approach to 12 lead ECG interpretation Demonstrate the process for determining
Section V Landscape of an MI Objectives At the conclusion of this presentation the participant will be able to Outline a systematic approach to 12 lead ECG interpretation Demonstrate the process for determining
EKG Abnormalities. Adapted from:
 EKG Abnormalities Adapted from: http://www.bem.fi/book/19/19.htm Some key terms: Arrhythmia-an abnormal rhythm or sequence of events in the EKG Flutter-rapid depolarizations (and therefore contractions)
EKG Abnormalities Adapted from: http://www.bem.fi/book/19/19.htm Some key terms: Arrhythmia-an abnormal rhythm or sequence of events in the EKG Flutter-rapid depolarizations (and therefore contractions)
WPW syndrome and AVRT
 WPW syndrome and AVRT Myung-Yong Lee, MD, PhD Division of Cardiology Department of Internal Medicine School of Medicine Dankook University, Cheonan, Korea Supraventricular tachycardia (SVT) Paroxysmal
WPW syndrome and AVRT Myung-Yong Lee, MD, PhD Division of Cardiology Department of Internal Medicine School of Medicine Dankook University, Cheonan, Korea Supraventricular tachycardia (SVT) Paroxysmal
Case-Based Practical ECG Interpretation for the Generalist
 Case-Based Practical ECG Interpretation for the Generalist Paul D. Varosy, MD, FACC, FAHA, FHRS Director of Cardiac Electrophysiology VA Eastern Colorado Health Care System Associate Professor of Medicine
Case-Based Practical ECG Interpretation for the Generalist Paul D. Varosy, MD, FACC, FAHA, FHRS Director of Cardiac Electrophysiology VA Eastern Colorado Health Care System Associate Professor of Medicine
Course Objectives. Proper Lead Placements. Review the ECG print paper. Review the mechanics of the Myocardium. Review basics of ECG Rhythms
 ECG Interpretations Course Objectives Proper Lead Placements Review the ECG print paper Review the mechanics of the Myocardium Review basics of ECG Rhythms How Leads Work The ECG Leads we use are Bipolar
ECG Interpretations Course Objectives Proper Lead Placements Review the ECG print paper Review the mechanics of the Myocardium Review basics of ECG Rhythms How Leads Work The ECG Leads we use are Bipolar
TACHYARRHYTHMIAs. Pawel Balsam, MD, PhD
 TACHYARRHYTHMIAs Pawel Balsam, MD, PhD SupraVentricular Tachycardia Atrial Extra Systole Sinus Tachycardia Focal A. Tachycardia AVRT AVNRT Atrial Flutter Atrial Fibrillation Ventricular Tachycardia Ventricular
TACHYARRHYTHMIAs Pawel Balsam, MD, PhD SupraVentricular Tachycardia Atrial Extra Systole Sinus Tachycardia Focal A. Tachycardia AVRT AVNRT Atrial Flutter Atrial Fibrillation Ventricular Tachycardia Ventricular
2017 EKG Workshop Basic. Family Medicine Review Course Lou Mancano, MD, FAAFP Reading Health System Family and Community Medicine Reading, PA
 2017 EKG Workshop Basic Family Medicine Review Course Lou Mancano, MD, FAAFP Reading Health System Family and Community Medicine Reading, PA Part I - Objectives Discuss a systematic approach to EKG interpretation
2017 EKG Workshop Basic Family Medicine Review Course Lou Mancano, MD, FAAFP Reading Health System Family and Community Medicine Reading, PA Part I - Objectives Discuss a systematic approach to EKG interpretation
Other 12-Lead ECG Findings
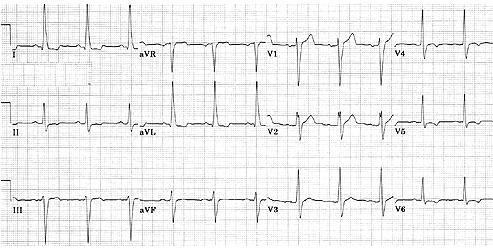
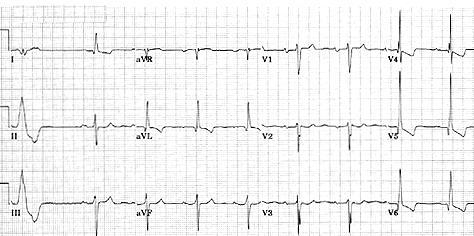
 Other 12-Lead ECG Findings Left Atrial Enlargement Left atrial enlargement is illustrated by increased P wave duration in lead II, top ECG, and by the prominent negative P terminal force in lead V1, bottom
Other 12-Lead ECG Findings Left Atrial Enlargement Left atrial enlargement is illustrated by increased P wave duration in lead II, top ECG, and by the prominent negative P terminal force in lead V1, bottom
I have no conflicts of interest relative to this lecture.
 PATHWAYS AROUND THE PITFALLS OF EKG RHYTHM INTERPRETATION Donald D. Brown, MD April 4, 2019 I have no conflicts of interest relative to this lecture. OBJECTIVES FOR PATHWAYS AROUND PITFALLS OF EKG RHYTHM
PATHWAYS AROUND THE PITFALLS OF EKG RHYTHM INTERPRETATION Donald D. Brown, MD April 4, 2019 I have no conflicts of interest relative to this lecture. OBJECTIVES FOR PATHWAYS AROUND PITFALLS OF EKG RHYTHM
By the end of this lecture, you will be able to: Understand the 12 lead ECG in relation to the coronary circulation and myocardium Perform an ECG
 By the end of this lecture, you will be able to: Understand the 12 lead ECG in relation to the coronary circulation and myocardium Perform an ECG recording Identify the ECG changes that occur in the presence
By the end of this lecture, you will be able to: Understand the 12 lead ECG in relation to the coronary circulation and myocardium Perform an ECG recording Identify the ECG changes that occur in the presence
ELECTROCARDIOGRAPHY KEVIN REBECK PA-C. For more presentations
 ELECTROCARDIOGRAPHY KEVIN REBECK PA-C For more presentations www.medicalppt.blogspot.com Objectives ECG History Pathophysiology Basics Case Historys Electrical activation of the heart In the heart
ELECTROCARDIOGRAPHY KEVIN REBECK PA-C For more presentations www.medicalppt.blogspot.com Objectives ECG History Pathophysiology Basics Case Historys Electrical activation of the heart In the heart
Miscellaneous Stuff Keep reading the Outline
 Miscellaneous Stuff Keep reading the Outline Welcome to the 5-Step Method ECG #: Mearurements: Rhythm (s): Conduction: Waveform: Interpretation: A= V= PR= QRS= QT= Axis= 1. Compute the 5 basic measurements:
Miscellaneous Stuff Keep reading the Outline Welcome to the 5-Step Method ECG #: Mearurements: Rhythm (s): Conduction: Waveform: Interpretation: A= V= PR= QRS= QT= Axis= 1. Compute the 5 basic measurements:
PATIENT WITH ARRHYTHMIA IN DENTIST S OFFICE. Małgorzata Kurpesa, MD., PhD. Chair&Department of Cardiology
 PATIENT WITH ARRHYTHMIA IN DENTIST S OFFICE Małgorzata Kurpesa, MD., PhD. Chair&Department of Cardiology Medical University of Łódź The heart is made up of four chambers Left Atrium Right Atrium Left Ventricle
PATIENT WITH ARRHYTHMIA IN DENTIST S OFFICE Małgorzata Kurpesa, MD., PhD. Chair&Department of Cardiology Medical University of Łódź The heart is made up of four chambers Left Atrium Right Atrium Left Ventricle
Blocks & Dissociations. Reading Assignment (p47-52 in Outline )
") Blocks & Dissociations Reading Assignment (p47-52 in Outline ) Objectives Who are Wenckebach and Mobitz? Review SA and AV Blocks AV Dissociations: learning who s the boss and why 2 nd degree SA Block:
Blocks & Dissociations Reading Assignment (p47-52 in Outline ) Objectives Who are Wenckebach and Mobitz? Review SA and AV Blocks AV Dissociations: learning who s the boss and why 2 nd degree SA Block:
EKG. Danil Hammoudi.MD
 EKG Danil Hammoudi.MD What is an EKG? The electrocardiogram (EKG) is a representation of the electrical events of the cardiac cycle. Each event has a distinctive waveform, the study of which can lead to
EKG Danil Hammoudi.MD What is an EKG? The electrocardiogram (EKG) is a representation of the electrical events of the cardiac cycle. Each event has a distinctive waveform, the study of which can lead to
12 Lead ECG Skills: Building Confidence for Clinical Practice. Presented By: Cynthia Webner, BSN, RN, CCRN-CMC. Karen Marzlin, BSN, RN,CCRN-CMC
 12 Lead ECG Skills: Building Confidence for Clinical Practice NTI 2009 Preconference Session 803 Presented By: Karen Marzlin, BSN, RN,CCRN-CMC 1 12 Lead ECG Fundamentals: The Starting Place for Linking
12 Lead ECG Skills: Building Confidence for Clinical Practice NTI 2009 Preconference Session 803 Presented By: Karen Marzlin, BSN, RN,CCRN-CMC 1 12 Lead ECG Fundamentals: The Starting Place for Linking
Ben Taylor, PhD, PA-C
 Ben Taylor, PhD, PA-C The patient is a 23-year-old white male with a history of polysubstance abuse who was found unresponsive, last seen the day before. Classic signs of systemic hypothermia with prominent
Ben Taylor, PhD, PA-C The patient is a 23-year-old white male with a history of polysubstance abuse who was found unresponsive, last seen the day before. Classic signs of systemic hypothermia with prominent
ECG Underwriting Puzzler Dr. Regina Rosace AVP & Medical Director
 December 2018 ECG Underwriting Puzzler Dr. Regina Rosace AVP & Medical Director To obtain best results Select Slide Show from the ribbon at the top of your PowerPoint screen Select From Beginning on the
December 2018 ECG Underwriting Puzzler Dr. Regina Rosace AVP & Medical Director To obtain best results Select Slide Show from the ribbon at the top of your PowerPoint screen Select From Beginning on the
Return to Basics. ECG Rate and Rhythm. Management of the Hospitalized Patient October 4, 2007
 Management of the Hospitalized Patient October 4, 2007 ECG Refresher for the Hospitalists Return to Basics Determine rate and rhythm Determine intervals and axes Define morphology of P-QRS-T-U Compare
Management of the Hospitalized Patient October 4, 2007 ECG Refresher for the Hospitalists Return to Basics Determine rate and rhythm Determine intervals and axes Define morphology of P-QRS-T-U Compare
Ronald J. Kanter, MD Director, Electrophysiology Miami Children s Hospital Professor Emeritus, Duke University Miami, Florida
 S306- Pediatric Electrocardiography: A Potpourri Ronald J. Kanter, MD Director, Electrophysiology Miami Children s Hospital Professor Emeritus, Duke University Miami, Florida Disclosure of Relevant Relationship
S306- Pediatric Electrocardiography: A Potpourri Ronald J. Kanter, MD Director, Electrophysiology Miami Children s Hospital Professor Emeritus, Duke University Miami, Florida Disclosure of Relevant Relationship
FLB s What Are Those Funny-Looking Beats?
 FLB s What Are Those Funny-Looking Beats? Reading Assignment (pages 27-45 in Outline ) The 5-Step Method ECG #: Mearurements: Rhythm (s): Conduction: Waveform: Interpretation: A= V= PR= QRS= QT= Axis=
FLB s What Are Those Funny-Looking Beats? Reading Assignment (pages 27-45 in Outline ) The 5-Step Method ECG #: Mearurements: Rhythm (s): Conduction: Waveform: Interpretation: A= V= PR= QRS= QT= Axis=
The Efficient and Smart Methods for Diagnosis of SVT 대구파티마병원순환기내과정병천
 The Efficient and Smart Methods for Diagnosis of SVT 대구파티마병원순환기내과정병천 Differentiation Supraventricular Origin from Ventricular Origin on ECG. QRS-Complex Width. 1. Narrow QRS-Complex Tachycardia (
The Efficient and Smart Methods for Diagnosis of SVT 대구파티마병원순환기내과정병천 Differentiation Supraventricular Origin from Ventricular Origin on ECG. QRS-Complex Width. 1. Narrow QRS-Complex Tachycardia (
2017 BDKA Review. Regularity Rate P waves PRI QRS Interpretation. Regularity Rate P waves PRI QRS Interpretation 1/1/2017
 1. 2017 BDKA Review 2. 3. 4. Interpretation 5. QT 6. 7. 8. 9. 10. QT 11. 12. 13. 14. 15. 16. 17. 18. QT 19. 20. QT 21. 22. QT 23. 24. Where are pacer spikes? Before the P wave or before the QRS complex?
1. 2017 BDKA Review 2. 3. 4. Interpretation 5. QT 6. 7. 8. 9. 10. QT 11. 12. 13. 14. 15. 16. 17. 18. QT 19. 20. QT 21. 22. QT 23. 24. Where are pacer spikes? Before the P wave or before the QRS complex?
Introduction to Electrocardiography
 Introduction to Electrocardiography Class Objectives: Introduction to ECG monitoring Discuss principles of interpretation Identify the components and measurements of the ECG ECG analysis ECG Monitoring
Introduction to Electrocardiography Class Objectives: Introduction to ECG monitoring Discuss principles of interpretation Identify the components and measurements of the ECG ECG analysis ECG Monitoring
Electrocardiography for Healthcare Professionals. Chapter 14 Basic 12-Lead ECG Interpretation
 Electrocardiography for Healthcare Professionals Chapter 14 Basic 12-Lead ECG Interpretation 2012 The Companies, Inc. All rights reserved. Learning Outcomes 14.1 Discuss the anatomic views seen on a 12-lead
Electrocardiography for Healthcare Professionals Chapter 14 Basic 12-Lead ECG Interpretation 2012 The Companies, Inc. All rights reserved. Learning Outcomes 14.1 Discuss the anatomic views seen on a 12-lead
Left posterior hemiblock (LPH)/
/") ECG OF THE MONTH Left Postero-inferior Depolarization Delay Keywords Electrocardiography Intraventricular conduction delay, Inferoposterior hemiblock, Left posterior fascicular block, Left posterior hemiblock
ECG OF THE MONTH Left Postero-inferior Depolarization Delay Keywords Electrocardiography Intraventricular conduction delay, Inferoposterior hemiblock, Left posterior fascicular block, Left posterior hemiblock
TEST BANK FOR ECGS MADE EASY 5TH EDITION BY AEHLERT
 Link download full: http://testbankair.com/download/test-bank-for-ecgs-made-easy-5thedition-by-aehlert/ TEST BANK FOR ECGS MADE EASY 5TH EDITION BY AEHLERT Chapter 5 TRUE/FALSE 1. The AV junction consists
Link download full: http://testbankair.com/download/test-bank-for-ecgs-made-easy-5thedition-by-aehlert/ TEST BANK FOR ECGS MADE EASY 5TH EDITION BY AEHLERT Chapter 5 TRUE/FALSE 1. The AV junction consists