Prof. Patrizio LANCELLOTTI, MD, PhD Heart Valve Clinic, University of Liège, CHU Sart Tilman, Liège, BELGIUM
|
|
|
- Kristina Jefferson
- 5 years ago
- Views:
Transcription


1 The Patient with Aortic Stenosis and Mitral Regurgitation Prof. Patrizio LANCELLOTTI, MD, PhD Heart Valve Clinic, University of Liège, CHU Sart Tilman, Liège, BELGIUM



2 Aortic Stenosis + Mitral Regurgitation?
3
4 Etiology of MR in patients with significant aortic valve disease Functional LV dysfunction «Ischemic» MR or not Mixed Organic Intrinsic MV dysfunction Rheumatic heart disease Myxomatous degeneration Chordal/papillary muscle rupture Calcifications of mitral leaflets or annulus Undetermined
5 Pathophysiology LV remodelling Mitral valve deformation LV pressure LV-LA pressure gradient Aortic stenosis Mitral regurgitation Functional tolerance Atrial fibrillation Diagnostic challenge Low flow low gradient aortic stenosis forward stroke volume Impedes detection of subclinical myocardial dysfunction EF Unger et al. Heart 2010;96:9-14
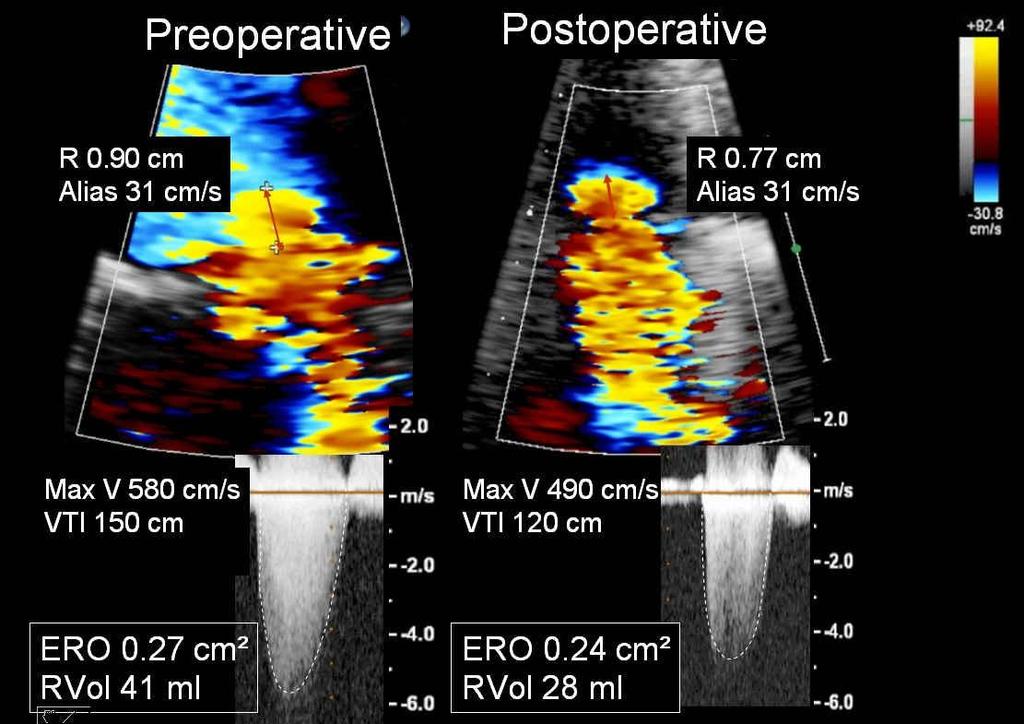
 LVOT diameter 2,2")
6 AVA 0.65 cm² (0,34 cm²/m²) LVOT diameter 2,2 cm Stroke volume 35 ml (18 ml/m²)

7 Prevalence 10% of all cardiac procedures 5% of all AVR +/-1000/yr STS database
8 Prevalence of MR in patients undergoing isolated AVR Authors, Year Tunick Am J Cardiol 1990 Adams Am J Cardiol studies Tassan-Mangina Clin Cardiol 2003 Moazami J Card Surg 2004 Barreiro Circulation 2005 Ruel Circulation 2006 Caballero-Borrego Eur J Cardiothor Surg 2008 Waisbren Ann Thor Surg 2008 Number of patients Exclusion criteria Method of MR assessment Percentage of patients with preoperative MR 44 None Colour flow mapping 61% with mild MR 56* None Pulsed wave Doppler mapping 82% with 1+ MR 30 Severe AR Unstable haemodynamic state Arrhythmia 250 Organic mitral valve disease Previous sternotomy or mitral valve surgery N=2550 Variable 408 Need for concomitant bypass surgery Age > 70 y 848 Organic mitral valve disease Patients who did not survive the operation 577 Organic mitral valve disease Predominant AR Predominant coronary artery disease Type A aortic dissection MR secondary to SAM 227 Organic mitral valve disease Combined procedure (CABG) Endocarditis Right heart valve procedure Moderate or severe AR Colour flow mapping Colour flow mapping Colour flow mapping 2003 American Society of organic MVD (4) Echocardiography recommendations moderate AR (3) CAD/CABG (4) Qualitative or semi-quantitative Colour flow and pulsed wave Doppler mapping, pulmonary vein flow Vena contracta width 90% with mild MR 78% with mild MR 17.2% with moderate MR mild: 12.6% with 60-80% 2+ MR moderate: ±15% 26.5% with non-severe MR 74% with moderate MR

9 Risk associated with double valve replacement STS database
10 Euro Heart Survey Operative mortality and morbidity of interventions according to the underlying valve disease Aortic stenosis n=512 Multiple valve disease n=185 Aortic stenosis n= Multiple valve dis % mponnade Embolism Mediastinitis 0 Mortality Major bleeding Tamponnade Embolism Mediastinitis Iung et al. Eur Heart J 2003; 24:1231
11 Long-term outcome after aortic + mitral valve replacement Independent predictors of late outcome: Age LVEF Additional tricuspid surgery NYHA class CAD requiring CABG Turina, J. et al. Circulation 1999;100:II-48-II-53
12 Survival (%)l Mitral valve repair with AV replacement is 100 superior to double valve replacement % P= years Repair: N=295 Replacement: N=518 Mean follow-up 6.9±5.9 yrs Gillinov AM, et al. J Thorac Cardiovasc Surg 2003; 125: 1372
13 AVR + MV repair vs AVR + AVR replacement/ event-free survival AVR + MV repair p < AVR + MVR Talwar S, et al Ann Thorac Surg. 2007:84:1219
14 Prognostic impact of MR in patients undergoing isolated AVR Functional MR First author, Year Absil, Eur J Cardiothoracic Surgery 2003 Number of patients with MR 2 Aetiology of MR Prognostic value 58 Functional No significant prognostic value Ruel, Circulation Functional No significant effect on mortality Wan, JTCVS Functional No independent prognostic value Caballero-Borrego, Eur J Cardiothoracic Surgery Functional Independent risk factor for mortality and morbidity Age, diabetes, renal failure, LV dysfunction, Atrial fibrillation
15 Prognostic impact of MR in patients undergoing isolated AVR Organic MR First author, Year Number of patients with Aetiology of MR Prognostic value MR 2 Barreiro, Circulation 2005 Takeda, Eur J Cardio Surg 70 Organic (2/3) Functional (1/3) 59 Organic (2/3) Functional (1/3) Independent risk factor for longterm mortality Independent risk factor for longterm morbidity
16 Independent Predictors of Late Mortality as Determined by Multivariate Statistical Analysis Barreiro, C. J. et al. Circulation 2005;112:I-443-I-447
17 First author, Year Tunick studies Adams 1990 Aetiology of MR Functional Organic Organic Functional Number of patients Timing of the postoperative echo examination Method of MR assessment % of patients with improvement in MR N = 27 with mild MR 58 days CFM 67% N = 46 with mild MR 6 months PW Doppler mapping 27% Harris 1997 Functional N=28 with mild MR 2.5 months CFM 82% Brasch 2000 N = 16 with moderate MR Christenson 2000 Functional N = 58 with mild MR 1 week and 5 months Tassan-Mangina 2003 Functional in all except 2 patients 2.2 months CFM 44% CFM 46% and 60% N = 23 with mild MR 19 days CFM 61% Moazami 2004 Functional N = 80 with mild MR > 60 days CFM 45% Barreiro 2005 Organic Functional N = 70 with moderate MR Early postoperative CFM 82% if functional 35% if organic Ruel 2006 Functional N = 107 with 2+ MR 18 months 2003 ASE recommendations Vanden Eynden 2007 Caballero-Borrego 2008 Waisbren 2008 Impact of isolated AVR on MR Functional: 8 Organic Functional + Functional organic: 5 Organic Functional Functional Functional No CABG 1014 patients mild or moderate MR N = 80 with moderate MR N =153 with non-severe MR N = 60 mild MR N = 167 moderate MR Wan 2009 Functional N=159 with moderate MR From OR up to 18 months 1 year CFM and PW Doppler mapping, PV flow Before hospital discharge CFM and PW Doppler mapping, PV flow 44-74% 35% 72% Intraoperative Vena contracta width 66% of preop. moderate MR Discharge Qualitative or ½ quantitative studies All retrospective studies except one 2003 ASE recommendations 65-75% (27-82%) 76%
18 Quantitative changes in MR after isolated AVR Unger P et al. Am J Cardiol. 2008; 102:
19 postop reduction (%) Quantitative changes in MR after AVR P< vs ERO P=0.034 vs ERO 0 ERO Reg Vol Reg jet/la area Unger P et al. Am J Cardiol. 2008; 102:
20
21 Predictors of MR down-grading after isolated AVR First author, Year Aetiology of MR Preoperative predictive factors of MR improvement Tunick Am J Cardiol 1990 Functional + organic MR severity Adams Am J Cardiol 1990 Functional + organic None Harris Am J Cardiol 1997 Functional Low LV fractional area Large left atrial size Brasch Am J Cardiol 2000 Functional + organic LV mass Christenson, Tex Heart Inst J 2000 Functional Presence of coronary artery disease Tassan-Mangina Clin Cardiol 2003 Functional in all except 2 patients Peak velocity of tricuspid regurgitant jet Indexed Functional LV mass etiology Moazami J Cardiac Surg 2004 Functional History of previous myocardial infarction Barreiro Circulation 2005 Functional + organic Functional MR 14 studies Ruel Circulation 2006 Functional No enlarged left atrium (>5cm), no chronic AF No low preoperative peak aortic pressure gradient (< 60 mm Hg) Vanden Eynden Ann Thor Surg 2007 Functional + organic Functional (including ischaemic) MR Caballero-Borrego Eur J CT Surg 2008 Functional Presence of CAD, absence of diabetes and of PHT Waisbren Ann Thor Surg 2008 Functional: n=8 Organic + funct: n=6 Functional No CABG MR severity, trace or mild aortic insufficiency Left atrial size < 4.5cm Congestive heart failure Unger Am J Cardiol 2008 Functional + organic MR severity Mitral coaptation height Improvement Low EF, CHF Lower grade of MR under anesthesia Less MV deformation Less/no improvement Organic etiology Enlarged atrium AFib Pulmonary HT Wan JTCVS 2009 Functional Lesser preop TR, lower MR grade under anesthesia No cerebrovasc disease Lower EF
22 Changes in hemodynamic and echocardiographic data according to mitral regurgitation etiology Functional MR Organic MR P value Variables (n=20, 48%) (n=22, 52%) LV geometry and function Indexed LVED volume, ml 12±13 4± Indexed LVES volume, ml 9±12 4±6 NS Indexed LV mass, g.m -2 9±25 5±26 NS LV ejection fraction, % -4±11-5±8 NS Mitral regurgitation Effective regurgitant orifice, mm 2 5.8± ± Regurgitant volume, ml 14.5±7 9.3±

23 Preop Predictors of Persistent Functional MR >1.4 cm² 0.7 cm 9.7 cm² Matsumura Y et al. Am J Cardiol. 2010; 106:
24 Relationship between postoperative changes in mitral tenting area and reduction in mitral regurgitation in patients with functional MR 25 Changes in ERO (pre-post), mm 2 35 Changes in RV (pre-post), ml r=0.51 p= r=0.55 p= Postoperative changes in mitral tenting area, cm 2
25 Postoperative improvement Postoperative changes in MR according to the presence/absence of patient/prosthesis mismatch PPM: postop indexed AVA < 0.85 cm²/m² in ERO, mm ±4.0 p= ± No PPM (n=19, 45%) PPM (n=23, 55%) Unger P et al. (Abstract) Circulation. 2009;120:S768
26 Relationship between aortic projected indexed EOA and reduction in ERO (preop minus postop value) 20 A Postoperative changes in ERO (pre-post), mm r=0.14, p=ns r=0.14, p=ns Projected indexed EOA, cm 2.m -2 r=0.70, p= r=0.70, p= r=0.44, p=0.01 Functional MR MR Organic Organic MR MR
27 When is double-valve surgery indicated? ACC/AHA 2006 Guidelines for the Management of Patients With Valvular Heart Disease «Remarkably few data exist to objectively guide the management of mixed valve disease Hence, each case must be consider individually the committee has developed no specific recommendations.» 2007 ESC Guidelines on the Management of Valvular Heart Disease «Data on multiple valve diseases are lacking and do not allow for evidence-based recommendations.»
28 When is double-valve surgery indicated? If MR is severe however, There are data on 40 patients with severe MR who did not undergo surgical mitral valve intervention 90% of them had an improvement of at least one grade When is MR considered severe?
29 Threshold of MR severity? Ischaemic (functional) MR 20 mm² (1) Organic MR 40 mm² (2) frequent downgrading after AVR less frequent downgrading risk of future reoperation 30 mm² 1. Lancellotti et al. Circulation Enriquez-Sarano M. et al. N Engl J Med 2005
30 When is double-valve surgery (not) indicated? Assessment of MR severity (ERO) Knowledge of functional or organic aetiology Suitability for MV repair Operative risk and comorbidities
31 Surgical Risk ERO < 20 mm² Symptomatic Aortic Stenosis + MR ERO mm² ERO 30 mm² Functional MR Organic MR PASP > 50 mmhg LAD > 50 mm Atrial fibrillation PPM MV deformation No No mitral valve surgery Yes Low AVR + mitral valve surgery (preferably repair) Operative risk+comorbidities Intermediate Isolated AVR High Percutaneous aortic valve implantation Low Intermediate High
Aortic stenosis with concomitant mitral regurgitation
 Challenges in the evaluation and management of aortic stenosis Aortic stenosis with concomitant mitral regurgitation S1 Philippe Unger, M.D., FESC Erasme Hospital - Université Libre de Bruxelles Brussels,
Challenges in the evaluation and management of aortic stenosis Aortic stenosis with concomitant mitral regurgitation S1 Philippe Unger, M.D., FESC Erasme Hospital - Université Libre de Bruxelles Brussels,
Primary Mitral Regurgitation
 EURO VALVE Madrid News from Valves Guidelines 2012: What s new and Why? Primary Mitral Regurgitation Luc A. Pierard, MD, PhD Professor of Medicine Head of the Department of Cardiology Heart Valve Clinic,
EURO VALVE Madrid News from Valves Guidelines 2012: What s new and Why? Primary Mitral Regurgitation Luc A. Pierard, MD, PhD Professor of Medicine Head of the Department of Cardiology Heart Valve Clinic,
How does Pulmonary Hypertension Affect the Decision to Intervene in Mitral Valve Disease? NO DISCLOSURE
 How does Pulmonary Hypertension Affect the Decision to Intervene in Mitral Valve Disease? Prof. Patrizio LANCELLOTTI, MD, PhD GIGA Cardiovascular Sciences, Heart Valve Clinic, University of Liège, CHU
How does Pulmonary Hypertension Affect the Decision to Intervene in Mitral Valve Disease? Prof. Patrizio LANCELLOTTI, MD, PhD GIGA Cardiovascular Sciences, Heart Valve Clinic, University of Liège, CHU
Ioannis Alexanian, MD, PhD Department of Cardiology General Hospital of Chest Diseases Sotiria Athens
 MITRAL REGURGITATION IN PATIENT WITH SEVERE AORTIC VALVE STENOSIS Ioannis Alexanian, MD, PhD Department of Cardiology General Hospital of Chest Diseases Sotiria Athens I HAVE NOTHING TO DECLARE Management
MITRAL REGURGITATION IN PATIENT WITH SEVERE AORTIC VALVE STENOSIS Ioannis Alexanian, MD, PhD Department of Cardiology General Hospital of Chest Diseases Sotiria Athens I HAVE NOTHING TO DECLARE Management
How to assess ischaemic MR?
 ESC 2012 How to assess ischaemic MR? Luc A. Pierard, MD, PhD, FESC, FACC Professor of Medicine Head, Department of Cardiology University Hospital Sart Tilman, Liège ESC 2012 No conflict of interest Luc
ESC 2012 How to assess ischaemic MR? Luc A. Pierard, MD, PhD, FESC, FACC Professor of Medicine Head, Department of Cardiology University Hospital Sart Tilman, Liège ESC 2012 No conflict of interest Luc
Echocardiographic changes after aortic valve replacement: Does the failure rate of mitral valve change? Original Article
 Echocardiographic changes after aortic valve replacement: Does the failure rate of mitral valve change? Abstract Arezoo Khosravi (1), Hadi Sheykhloo (2), Reza Karbasi-Afshar (1), Amin Saburi (3) Original
Echocardiographic changes after aortic valve replacement: Does the failure rate of mitral valve change? Abstract Arezoo Khosravi (1), Hadi Sheykhloo (2), Reza Karbasi-Afshar (1), Amin Saburi (3) Original
Clinical Outcome of Tricuspid Regurgitation. David Messika-Zeitoun
 Clinical Outcome of Tricuspid Regurgitation David Messika-Zeitoun I have financial relationships to disclose Consultant for: Edwards, Symetis and Valtech Tricuspid Regurgitation is a Common Finding Tricuspid
Clinical Outcome of Tricuspid Regurgitation David Messika-Zeitoun I have financial relationships to disclose Consultant for: Edwards, Symetis and Valtech Tricuspid Regurgitation is a Common Finding Tricuspid
Guidelines in perspective?
 EuroValve 2016 Challenges in the management Secondary MR Guidelines in perspective? Luc A. Pierard, MD, PhD Professor of Medicine Head of the Department of Cardiology, Liège, Belgium Heart Valve Clinic,
EuroValve 2016 Challenges in the management Secondary MR Guidelines in perspective? Luc A. Pierard, MD, PhD Professor of Medicine Head of the Department of Cardiology, Liège, Belgium Heart Valve Clinic,
Natural History and Echo Evaluation of Aortic Stenosis
 Natural History and Echo Evaluation of Aortic Stenosis Prof. Patrizio LANCELLOTTI, MD, PhD Heart Valve Clinic, University of Liège, CHU Sart Tilman, Liège, BELGIUM AORTIC STENOSIS First valvular disease
Natural History and Echo Evaluation of Aortic Stenosis Prof. Patrizio LANCELLOTTI, MD, PhD Heart Valve Clinic, University of Liège, CHU Sart Tilman, Liège, BELGIUM AORTIC STENOSIS First valvular disease
Effect of Aortic Valve Replacement for Aortic Stenosis on Severity of Mitral Regurgitation
 ORIGINAL ARTICLES: ADULT CARDIAC SURGERY: The Annals of Thoracic Surgery CME Program is located online at http://cme.ctsnetjournals.org. To take the CME activity related to this article, you must have
ORIGINAL ARTICLES: ADULT CARDIAC SURGERY: The Annals of Thoracic Surgery CME Program is located online at http://cme.ctsnetjournals.org. To take the CME activity related to this article, you must have
Valvular Regurgitation: Can We Do Better Than Colour Doppler?
 Valvular Regurgitation: Can We Do Better Than Colour Doppler? A/Prof David Prior St Vincent s Hospital Melbourne Sports Cardiology Valvular Regurgitation Valve regurgitation volume loads the ventricles
Valvular Regurgitation: Can We Do Better Than Colour Doppler? A/Prof David Prior St Vincent s Hospital Melbourne Sports Cardiology Valvular Regurgitation Valve regurgitation volume loads the ventricles
Χειρουργική Αντιμετώπιση της Ανεπάρκειας της Μιτροειδούς Βαλβίδας
 Χειρουργική Αντιμετώπιση της Ανεπάρκειας της Μιτροειδούς Βαλβίδας Dr Χρήστος ΑΛΕΞΙΟΥ MD, PhD, FRCS(Glasgow), FRCS(CTh), CCST(UK) Consultant Cardiothoracic Surgeon Normal Mitral Valve Function Mitral Regurgitation
Χειρουργική Αντιμετώπιση της Ανεπάρκειας της Μιτροειδούς Βαλβίδας Dr Χρήστος ΑΛΕΞΙΟΥ MD, PhD, FRCS(Glasgow), FRCS(CTh), CCST(UK) Consultant Cardiothoracic Surgeon Normal Mitral Valve Function Mitral Regurgitation
A Surgeon s Perspective Guidelines for the Management of Patients with Valvular Heart Disease Adapted from the 2006 ACC/AHA Guideline Revision
 A Surgeon s Perspective Guidelines for the Management of Patients with Valvular Heart Disease Adapted from the 2006 ACC/AHA Guideline Revision Prof. Pino Fundarò, MD Niguarda Hospital Milan, Italy Introduction
A Surgeon s Perspective Guidelines for the Management of Patients with Valvular Heart Disease Adapted from the 2006 ACC/AHA Guideline Revision Prof. Pino Fundarò, MD Niguarda Hospital Milan, Italy Introduction
Load and Function - Valvular Heart Disease. Tom Marwick, Cardiovascular Imaging Cleveland Clinic
 Load and Function - Valvular Heart Disease Tom Marwick, Cardiovascular Imaging Cleveland Clinic Indications for surgery in common valve lesions Risks Operative mortality Failed repair - to MVR Operative
Load and Function - Valvular Heart Disease Tom Marwick, Cardiovascular Imaging Cleveland Clinic Indications for surgery in common valve lesions Risks Operative mortality Failed repair - to MVR Operative
The Changing Epidemiology of Valvular Heart Disease: Implications for Interventional Treatment Alternatives. Martin B. Leon, MD
 The Changing Epidemiology of Valvular Heart Disease: Implications for Interventional Treatment Alternatives Martin B. Leon, MD Columbia University Medical Center Cardiovascular Research Foundation New
The Changing Epidemiology of Valvular Heart Disease: Implications for Interventional Treatment Alternatives Martin B. Leon, MD Columbia University Medical Center Cardiovascular Research Foundation New
SONOGRAPHER & NURSE LED VALVE CLINICS
 SONOGRAPHER & NURSE LED VALVE CLINICS Frequency of visits and alerts AORTIC STENOSIS V max > 4.0 m/s or EOA < 1.0 cm 2 V max 3.5 4.0 m/s + Ca+ V max 3.0 4.0 m/s or EOA 1.0-1.5 cm 2 V max 2.5 3.0 m/s every
SONOGRAPHER & NURSE LED VALVE CLINICS Frequency of visits and alerts AORTIC STENOSIS V max > 4.0 m/s or EOA < 1.0 cm 2 V max 3.5 4.0 m/s + Ca+ V max 3.0 4.0 m/s or EOA 1.0-1.5 cm 2 V max 2.5 3.0 m/s every
Exercise Testing/Echocardiography in Asymptomatic AS
 Exercise Testing/Echocardiography in Asymptomatic AS Raluca Dulgheru, MD Heart Valve Clinic, University of Liège, CHU Sart Tilman, BELGIUM Disclosure related to this presentation: None VALVULAR HEART DISEASE
Exercise Testing/Echocardiography in Asymptomatic AS Raluca Dulgheru, MD Heart Valve Clinic, University of Liège, CHU Sart Tilman, BELGIUM Disclosure related to this presentation: None VALVULAR HEART DISEASE
Disclosures. ESC Munich 2012 Bernard Iung, MD Consultancy: Abbott Boehringer Ingelheim Bayer Servier Valtech
 Disclosures ESC Munich 2012 Bernard Iung, MD Consultancy: Abbott Boehringer Ingelheim Bayer Servier Valtech Speaker s fee Edwards Lifesciences Sanofi-Aventis Decision Making in Patients with Multivalvular
Disclosures ESC Munich 2012 Bernard Iung, MD Consultancy: Abbott Boehringer Ingelheim Bayer Servier Valtech Speaker s fee Edwards Lifesciences Sanofi-Aventis Decision Making in Patients with Multivalvular
Severe left ventricular dysfunction and valvular heart disease: should we operate?
 Severe left ventricular dysfunction and valvular heart disease: should we operate? Laurie SOULAT DUFOUR Hôpital Saint Antoine Service de cardiologie Pr A. COHEN JESFC 16 janvier 2016 Disclosure : No conflict
Severe left ventricular dysfunction and valvular heart disease: should we operate? Laurie SOULAT DUFOUR Hôpital Saint Antoine Service de cardiologie Pr A. COHEN JESFC 16 janvier 2016 Disclosure : No conflict
ECHO HAWAII. Role of Stress Echo in Valvular Heart Disease. Not only ischemia! Cardiomyopathy. Prosthetic Valve. Diastolic Dysfunction
 Role of Stress Echo in Valvular Heart Disease ECHO HAWAII January 15 19, 2018 Kenya Kusunose, MD, PhD, FASE Tokushima University Hospital Japan Not only ischemia! Cardiomyopathy Prosthetic Valve Diastolic
Role of Stress Echo in Valvular Heart Disease ECHO HAWAII January 15 19, 2018 Kenya Kusunose, MD, PhD, FASE Tokushima University Hospital Japan Not only ischemia! Cardiomyopathy Prosthetic Valve Diastolic
Late secondary TR after left sided heart disease correction: is it predictibale and preventable
 Late secondary TR after left sided heart disease correction: is it predictibale and preventable Gilles D. Dreyfus Professor of Cardiothoracic surgery Nath J, et al. JACC 2004 PREDICT Incidence of secondary
Late secondary TR after left sided heart disease correction: is it predictibale and preventable Gilles D. Dreyfus Professor of Cardiothoracic surgery Nath J, et al. JACC 2004 PREDICT Incidence of secondary
The Ross Procedure: Outcomes at 20 Years
 The Ross Procedure: Outcomes at 20 Years Tirone David Carolyn David Anna Woo Cedric Manlhiot University of Toronto Conflict of Interest None The Ross Procedure 1990 to 2004 212 patients: 66% 34% Mean age:
The Ross Procedure: Outcomes at 20 Years Tirone David Carolyn David Anna Woo Cedric Manlhiot University of Toronto Conflict of Interest None The Ross Procedure 1990 to 2004 212 patients: 66% 34% Mean age:
Echocardiographic variables associated with mitral regurgitation after aortic valve replacement for aortic valve stenosis
 The Egyptian Heart Journal (2013) 65, 135 139 Egyptian Society of Cardiology The Egyptian Heart Journal www.elsevier.com/locate/ehj www.sciencedirect.com ORIGINAL ARTICLE Echocardiographic variables associated
The Egyptian Heart Journal (2013) 65, 135 139 Egyptian Society of Cardiology The Egyptian Heart Journal www.elsevier.com/locate/ehj www.sciencedirect.com ORIGINAL ARTICLE Echocardiographic variables associated
Outcome of elderly patients with severe but asymptomatic aortic stenosis
 Outcome of elderly patients with severe but asymptomatic aortic stenosis Robert Zilberszac, Harald Gabriel, Gerald Maurer, Raphael Rosenhek Department of Cardiology Medical University of Vienna ESC Congress
Outcome of elderly patients with severe but asymptomatic aortic stenosis Robert Zilberszac, Harald Gabriel, Gerald Maurer, Raphael Rosenhek Department of Cardiology Medical University of Vienna ESC Congress
Spotlight on Valvular Heart Disease Guidelines
 Spotlight on Valvular Heart Disease Guidelines Aortic Valve Disease Raphael Rosenhek Department of Cardiology Medical University of Vienna Palermo, April 26 th 2018 1998 2002 2006 2007 2008 2012 2014 2017
Spotlight on Valvular Heart Disease Guidelines Aortic Valve Disease Raphael Rosenhek Department of Cardiology Medical University of Vienna Palermo, April 26 th 2018 1998 2002 2006 2007 2008 2012 2014 2017
Advanced Evaluation of Left Ventricular Function in Degenerative MR. Dr Julien Magne, PhD University of Liege, CHU Sart Tilman, Liege, Belgium
 Advanced Evaluation of Left Ventricular Function in Degenerative MR Dr Julien Magne, PhD University of Liege, CHU Sart Tilman, Liege, Belgium Conflict of Interest Disclosure None Case Clinical data Previous
Advanced Evaluation of Left Ventricular Function in Degenerative MR Dr Julien Magne, PhD University of Liege, CHU Sart Tilman, Liege, Belgium Conflict of Interest Disclosure None Case Clinical data Previous
Management of Difficult Aortic Root, Old and New solutions
 Management of Difficult Aortic Root, Old and New solutions Hani K. Najm MD, Msc, FRCSC,, FACC, FESC Chairman, Pediatric and Congenital Heart Surgery Cleveland Clinic Conflict of Interest None Difficult
Management of Difficult Aortic Root, Old and New solutions Hani K. Najm MD, Msc, FRCSC,, FACC, FESC Chairman, Pediatric and Congenital Heart Surgery Cleveland Clinic Conflict of Interest None Difficult
The FORMA Early Feasibility Study: 30-Day Outcomes of Transcatheter Tricuspid Valve Therapy in Patients with Severe Secondary Tricuspid Regurgitation
 The FORMA Early Feasibility Study: 30-Day Outcomes of Transcatheter Tricuspid Valve Therapy in Patients with Severe Secondary Tricuspid Regurgitation Susheel Kodali, MD Director, Structural Heart & Valve
The FORMA Early Feasibility Study: 30-Day Outcomes of Transcatheter Tricuspid Valve Therapy in Patients with Severe Secondary Tricuspid Regurgitation Susheel Kodali, MD Director, Structural Heart & Valve
Aortic Stenosis: UPDATE Anjan Sinha, MD Krannert Institute of Cardiology
 Aortic Stenosis: UPDATE 2010 Anjan Sinha, MD Krannert Institute of Cardiology None Disclosures 67-Year-Old Male Dyspnea and angina Class III heart failure No PND or orthopnea 3/6 late peak SEM Diminished
Aortic Stenosis: UPDATE 2010 Anjan Sinha, MD Krannert Institute of Cardiology None Disclosures 67-Year-Old Male Dyspnea and angina Class III heart failure No PND or orthopnea 3/6 late peak SEM Diminished
What is the Role of Surgical Repair in 2012
 What is the Role of Surgical Repair in 2012 The Long-Term Results of Surgery Raphael Rosenhek Department of Cardiology Medical University of Vienna European Society of Cardiology 2012 Munich, August 27th
What is the Role of Surgical Repair in 2012 The Long-Term Results of Surgery Raphael Rosenhek Department of Cardiology Medical University of Vienna European Society of Cardiology 2012 Munich, August 27th
Chronic Primary Mitral Regurgitation
 Chronic Primary Mitral Regurgitation The Case For Early Surgical Intervention William K. Freeman, MD, FACC, FASE DISCLOSURES Relevant Financial Relationship(s) None Off Label Usage None Watchful Waiting......
Chronic Primary Mitral Regurgitation The Case For Early Surgical Intervention William K. Freeman, MD, FACC, FASE DISCLOSURES Relevant Financial Relationship(s) None Off Label Usage None Watchful Waiting......
Does Patient-Prosthesis Mismatch Affect Long-term Results after Mitral Valve Replacement?
 Original Article Does Patient-Prosthesis Mismatch Affect Long-term Results after Mitral Valve Replacement? Hiroaki Sakamoto, MD, PhD, and Yasunori Watanabe, MD, PhD Background: Recently, some articles
Original Article Does Patient-Prosthesis Mismatch Affect Long-term Results after Mitral Valve Replacement? Hiroaki Sakamoto, MD, PhD, and Yasunori Watanabe, MD, PhD Background: Recently, some articles
Degenerative Mitral Regurgitation: Etiology and Natural History of Disease and Triggers for Intervention
 Degenerative Mitral Regurgitation: Etiology and Natural History of Disease and Triggers for Intervention John N. Hamaty D.O. FACC, FACOI November 17 th 2017 I have no financial disclosures Primary Mitral
Degenerative Mitral Regurgitation: Etiology and Natural History of Disease and Triggers for Intervention John N. Hamaty D.O. FACC, FACOI November 17 th 2017 I have no financial disclosures Primary Mitral
Επιδιόπθωζη μιηποειδικήρ ζςζκεςήρ ζε ππόπηωζη ή πήξη γλωσίνων. Βαζίλειορ Σασπεκίδηρ Επιμεληηήρ Β Καπδιολογίαρ Γ.Ν. Παπαγεωπγίος
 Επιδιόπθωζη μιηποειδικήρ ζςζκεςήρ ζε ππόπηωζη ή πήξη γλωσίνων Βαζίλειορ Σασπεκίδηρ Επιμεληηήρ Β Καπδιολογίαρ Γ.Ν. Παπαγεωπγίος MV anatomy Otto C. NEJM 2001 Leaflets anatomy 2% of population Etiology Terminology
Επιδιόπθωζη μιηποειδικήρ ζςζκεςήρ ζε ππόπηωζη ή πήξη γλωσίνων Βαζίλειορ Σασπεκίδηρ Επιμεληηήρ Β Καπδιολογίαρ Γ.Ν. Παπαγεωπγίος MV anatomy Otto C. NEJM 2001 Leaflets anatomy 2% of population Etiology Terminology
Percutaneous Mitral Valve Repair: What Can We Treat and What Should We Treat
 Percutaneous Mitral Valve Repair: What Can We Treat and What Should We Treat Innovative Procedures, Devices & State of the Art Care for Arrhythmias, Heart Failure & Structural Heart Disease October 8-10,
Percutaneous Mitral Valve Repair: What Can We Treat and What Should We Treat Innovative Procedures, Devices & State of the Art Care for Arrhythmias, Heart Failure & Structural Heart Disease October 8-10,
Asymptomatic Valvular Disease:
 Asymptomatic Valvular Disease: Can Echocardiography Help You Decide When to Intervene? Neil J. Weissman, MD MedStar Health Research Inst at MedStar Washington Hospital Center & Professor of Medicine Georgetown
Asymptomatic Valvular Disease: Can Echocardiography Help You Decide When to Intervene? Neil J. Weissman, MD MedStar Health Research Inst at MedStar Washington Hospital Center & Professor of Medicine Georgetown
Which Type of Secondary Tricuspid Regurgitation Accompanying Mitral Valve Disease Should Be Surgically Treated?
 Ann Thorac Cardiovasc Surg 2013; 19: 428 434 Online January 31, 2013 doi: 10.5761/atcs.oa.12.01929 Original Article Which Type of Secondary Tricuspid Regurgitation Accompanying Mitral Valve Disease Should
Ann Thorac Cardiovasc Surg 2013; 19: 428 434 Online January 31, 2013 doi: 10.5761/atcs.oa.12.01929 Original Article Which Type of Secondary Tricuspid Regurgitation Accompanying Mitral Valve Disease Should
Valve Disease in Patients With Heart Failure TAVI or Surgery? Miguel Sousa Uva Hospital Cruz Vermelha Lisbon, Portugal
 Valve Disease in Patients With Heart Failure TAVI or Surgery? Miguel Sousa Uva Hospital Cruz Vermelha Lisbon, Portugal I have nothing to disclose. Wide Spectrum Stable vs Decompensated NYHA II IV? Ejection
Valve Disease in Patients With Heart Failure TAVI or Surgery? Miguel Sousa Uva Hospital Cruz Vermelha Lisbon, Portugal I have nothing to disclose. Wide Spectrum Stable vs Decompensated NYHA II IV? Ejection
Valvular Intervention
 Valvular Intervention Outline Introduction Aortic Stenosis Mitral Regurgitation Conclusion Calcific Aortic Stenosis Deformed Eccentric Calcified Nodular Rigid HOSTILE TARGET difficult to displace prone
Valvular Intervention Outline Introduction Aortic Stenosis Mitral Regurgitation Conclusion Calcific Aortic Stenosis Deformed Eccentric Calcified Nodular Rigid HOSTILE TARGET difficult to displace prone
Exercise Pulmonary Hypertension predicts the Occurrence of Symptoms in Asymptomatic Degenerative Mitral Regurgitation
 Exercise Pulmonary Hypertension predicts the Occurrence of Symptoms in Asymptomatic Degenerative Mitral Regurgitation Julien Magne, PhD, Kim O Connor, MD, Giuseppe Romano, MD, Marie Moonen, MD, Luc A.
Exercise Pulmonary Hypertension predicts the Occurrence of Symptoms in Asymptomatic Degenerative Mitral Regurgitation Julien Magne, PhD, Kim O Connor, MD, Giuseppe Romano, MD, Marie Moonen, MD, Luc A.
Stress Testing in Valvular Disease
 2017 ASE Florida Orlando, FL October 10, 2017 2:40 2:50 PM 10 min Grand Harbor Ballroom South Stress Testing in Valvular Disease Muhamed Sarić MD, PhD, MPA Director of Noninvasive Cardiology Echo Lab Associate
2017 ASE Florida Orlando, FL October 10, 2017 2:40 2:50 PM 10 min Grand Harbor Ballroom South Stress Testing in Valvular Disease Muhamed Sarić MD, PhD, MPA Director of Noninvasive Cardiology Echo Lab Associate
Aortic Valve Practice Guidelines: What Has Changed and What You Need to Know
 Aortic Valve Practice Guidelines: What Has Changed and What You Need to Know James F. Burke, MD Program Director Cardiovascular Disease Fellowship Lankenau Medical Center Disclosure Dr. Burke has no conflicts
Aortic Valve Practice Guidelines: What Has Changed and What You Need to Know James F. Burke, MD Program Director Cardiovascular Disease Fellowship Lankenau Medical Center Disclosure Dr. Burke has no conflicts
Long-term results (22 years) of the Ross Operation a single institutional experience
 of the Ross Operation a single institutional experience") Long-term results (22 years) of the Ross Operation a single institutional experience Authors: Costa FDA, Schnorr GM, Veloso M,Calixto A, Colatusso D, Balbi EM, Torres R, Ferreira ADA, Colatusso C Department
Long-term results (22 years) of the Ross Operation a single institutional experience Authors: Costa FDA, Schnorr GM, Veloso M,Calixto A, Colatusso D, Balbi EM, Torres R, Ferreira ADA, Colatusso C Department
Candice Silversides, MD Toronto Congenital Cardiac Centre for Adults University of Toronto Toronto, Canada
 PVR Following Repair of TOF Now? When? Candice Silversides, MD Toronto Congenital Cardiac Centre for Adults University of Toronto Toronto, Canada Late Complications after TOF repair Repair will be necessary
PVR Following Repair of TOF Now? When? Candice Silversides, MD Toronto Congenital Cardiac Centre for Adults University of Toronto Toronto, Canada Late Complications after TOF repair Repair will be necessary
Experience with 500 Stentless Aortic Valve Replacements
 Experience with 500 Stentless Aortic Valve Replacements Dimitrios C. Iliopoulos, MD Cardiac Surgeon Ass. Professor of Surgery University of Athens, School of Medicine I declare no conflict of interest
Experience with 500 Stentless Aortic Valve Replacements Dimitrios C. Iliopoulos, MD Cardiac Surgeon Ass. Professor of Surgery University of Athens, School of Medicine I declare no conflict of interest
What echo measurements are key prior to MitraClip?
 APHP CHU Bichat - Claude Bernard What echo measurements are key prior to MitraClip? Eric Brochet,MD Cardiology Department Hopital Bichat Paris France No disclosure Conflict of interest Case 69 y.o man
APHP CHU Bichat - Claude Bernard What echo measurements are key prior to MitraClip? Eric Brochet,MD Cardiology Department Hopital Bichat Paris France No disclosure Conflict of interest Case 69 y.o man
Valvular Heart Disease
 Valvular Heart Disease B K Singh, MD, FACC Disclosures: None 1 CARDIAC CYCLE S2 S2=A2P2 S1=M1T1 S4 S1 S3 2 JVP Carotid S1 Slitting of S2 S3 S4 Ejection click Opening snap Dynamic Auscultation What is the
Valvular Heart Disease B K Singh, MD, FACC Disclosures: None 1 CARDIAC CYCLE S2 S2=A2P2 S1=M1T1 S4 S1 S3 2 JVP Carotid S1 Slitting of S2 S3 S4 Ejection click Opening snap Dynamic Auscultation What is the
Prosthetic valve dysfunction: stenosis or regurgitation
 Prosthetic valve dysfunction: stenosis or regurgitation Jean G. Dumesnil MD, FRCP(C), FACC, FASE(Hon) Quebec Heart and Lung Institute, Québec, Québec No disclosures Possible Causes of High Gradients in
Prosthetic valve dysfunction: stenosis or regurgitation Jean G. Dumesnil MD, FRCP(C), FACC, FASE(Hon) Quebec Heart and Lung Institute, Québec, Québec No disclosures Possible Causes of High Gradients in
Prosthesis-Patient Mismatch or Prosthetic Valve Stenosis?
 EuroValves 2015, Nice Prosthesis-Patient Mismatch or Prosthetic Valve Stenosis? Philippe Pibarot, DVM, PhD, FACC, FAHA, FASE FESC Canada Research Chair in Valvular Heart Diseases Université LAVAL Disclosure
EuroValves 2015, Nice Prosthesis-Patient Mismatch or Prosthetic Valve Stenosis? Philippe Pibarot, DVM, PhD, FACC, FAHA, FASE FESC Canada Research Chair in Valvular Heart Diseases Université LAVAL Disclosure
Valvular Guidelines: The Past, the Present, the Future
 Valvular Guidelines: The Past, the Present, the Future Robert O. Bonow, MD, MS Northwestern University Feinberg School of Medicine Bluhm Cardiovascular Institute Northwestern Memorial Hospital Editor-in-Chief,
Valvular Guidelines: The Past, the Present, the Future Robert O. Bonow, MD, MS Northwestern University Feinberg School of Medicine Bluhm Cardiovascular Institute Northwestern Memorial Hospital Editor-in-Chief,
Bicuspid aortic root spared during ascending aorta surgery: an update of long-term results
 Short Communication Bicuspid aortic root spared during ascending aorta surgery: an update of long-term results Marco Russo, Guglielmo Saitto, Paolo Nardi, Fabio Bertoldo, Carlo Bassano, Antonio Scafuri,
Short Communication Bicuspid aortic root spared during ascending aorta surgery: an update of long-term results Marco Russo, Guglielmo Saitto, Paolo Nardi, Fabio Bertoldo, Carlo Bassano, Antonio Scafuri,
Functional Mitral Regurgitation
 Club 35 - The best in heart valve disease - Functional Mitral Regurgitation Steven Droogmans, MD, PhD UZ Brussel, Jette, Belgium 08-12-2011 Euroecho & other Imaging Modalities 2011 No conflicts of interest
Club 35 - The best in heart valve disease - Functional Mitral Regurgitation Steven Droogmans, MD, PhD UZ Brussel, Jette, Belgium 08-12-2011 Euroecho & other Imaging Modalities 2011 No conflicts of interest
HOW IMPORTANT ARE THESE ECHO MEASUREMENTS ANYWAY?
 HOW IMPORTANT ARE THESE ECHO MEASUREMENTS ANYWAY? John D. Carroll, MD Professor, Director of Interventional Cardiology and Co-Medical Director of the Cardiac and Vascular Center, University of Colorado
HOW IMPORTANT ARE THESE ECHO MEASUREMENTS ANYWAY? John D. Carroll, MD Professor, Director of Interventional Cardiology and Co-Medical Director of the Cardiac and Vascular Center, University of Colorado
Ischemic Mitral Regurgitation
 Ischemic Mitral Regurgitation Jean-Louis J. Vanoverschelde, MD, PhD Université catholique de Louvain Brussels, Belgium Definition Ischemic mitral regurgitation is mitral regurgitation due to complications
Ischemic Mitral Regurgitation Jean-Louis J. Vanoverschelde, MD, PhD Université catholique de Louvain Brussels, Belgium Definition Ischemic mitral regurgitation is mitral regurgitation due to complications
ECHOCARDIOGRAPHY DATA REPORT FORM
 Patient ID Patient Study ID AVM - - Date of form completion / / 20 Initials of person completing the form mm dd yyyy Study period Preoperative Postoperative Operative 6-month f/u 1-year f/u 2-year f/u
Patient ID Patient Study ID AVM - - Date of form completion / / 20 Initials of person completing the form mm dd yyyy Study period Preoperative Postoperative Operative 6-month f/u 1-year f/u 2-year f/u
Aortic Regurgitation and Aortic Aneurysm - Epidemiology and Guidelines -
 Reconstruction of the Aortic Valve and Root - A Practical Approach - Aortic Regurgitation and Aortic Aneurysm Wednesday 14 th September - 9.45 Practice must always be founded on sound theory. Leonardo
Reconstruction of the Aortic Valve and Root - A Practical Approach - Aortic Regurgitation and Aortic Aneurysm Wednesday 14 th September - 9.45 Practice must always be founded on sound theory. Leonardo
Ann Thorac Cardiovasc Surg 2015; 21: Online April 18, 2014 doi: /atcs.oa Original Article
 Ann Thorac Cardiovasc Surg 2015; 21: 53 58 Online April 18, 2014 doi: 10.5761/atcs.oa.13-00364 Original Article The Impact of Preoperative and Postoperative Pulmonary Hypertension on Long-Term Surgical
Ann Thorac Cardiovasc Surg 2015; 21: 53 58 Online April 18, 2014 doi: 10.5761/atcs.oa.13-00364 Original Article The Impact of Preoperative and Postoperative Pulmonary Hypertension on Long-Term Surgical
Ejection across stenotic aortic valve requires a systolic pressure gradient between the LV and aorta. This places a pressure load on the LV.
 Valvular Heart Disease Etiology General Principles Cellular and molecular mechanism of valve damage Structural pathology Functional pathology - stenosis/regurgitation Loading conditions - pressure/volume
Valvular Heart Disease Etiology General Principles Cellular and molecular mechanism of valve damage Structural pathology Functional pathology - stenosis/regurgitation Loading conditions - pressure/volume
Quality Outcomes Mitral Valve Repair
 Quality Outcomes Mitral Valve Repair Moving Beyond Reoperation Rakesh M. Suri, D.Phil. Professor of Surgery 2015 MFMER 3431548-1 Disclosure Mayo Clinic Division of Cardiovascular Surgery Research funding
Quality Outcomes Mitral Valve Repair Moving Beyond Reoperation Rakesh M. Suri, D.Phil. Professor of Surgery 2015 MFMER 3431548-1 Disclosure Mayo Clinic Division of Cardiovascular Surgery Research funding
What are the best diagnostic tools to quantify aortic regurgitation?
 What are the best diagnostic tools to quantify aortic regurgitation? Agnès Pasquet, MD, PhD Pôle de Recherche Cardiovasculaire Institut de Recherche Expérimentale et Clinique Université catholique de Louvain
What are the best diagnostic tools to quantify aortic regurgitation? Agnès Pasquet, MD, PhD Pôle de Recherche Cardiovasculaire Institut de Recherche Expérimentale et Clinique Université catholique de Louvain
Aortic Stenosis: Interventional Choice for a 70-year old- SAVR, TAVR or BAV? Interventional Choice for a 90-year old- SAVR, TAVR or BAV?
 Aortic Stenosis: Interventional Choice for a 70-year old- SAVR, TAVR or BAV? Interventional Choice for a 90-year old- SAVR, TAVR or BAV? Samin K Sharma, MD, FACC, FSCAI Director Clinical & Interventional
Aortic Stenosis: Interventional Choice for a 70-year old- SAVR, TAVR or BAV? Interventional Choice for a 90-year old- SAVR, TAVR or BAV? Samin K Sharma, MD, FACC, FSCAI Director Clinical & Interventional
TAVR-Update Andrzej Boguszewski MD, FACC, FSCAI Vice Chairman, Cardiology Mid-Michigan Health Associate Professor Michigan State University, Central
 TAVR-Update Andrzej Boguszewski MD, FACC, FSCAI Vice Chairman, Cardiology Mid-Michigan Health Associate Professor Michigan State University, Central Michigan University 1 Disclosure Chiesi Pharma- Consultant
TAVR-Update Andrzej Boguszewski MD, FACC, FSCAI Vice Chairman, Cardiology Mid-Michigan Health Associate Professor Michigan State University, Central Michigan University 1 Disclosure Chiesi Pharma- Consultant
APOLLO TMVR Trial Update: Case Presentation
 APOLLO TMVR Trial Update: Case Presentation Anelechi Anyanwu, MD, MSc, FRCS-CTh Professor and Vice-Chairman Department of Cardiovascular Surgery Icahn School of Medicine at Mount Sinai New York, NY Disclosure
APOLLO TMVR Trial Update: Case Presentation Anelechi Anyanwu, MD, MSc, FRCS-CTh Professor and Vice-Chairman Department of Cardiovascular Surgery Icahn School of Medicine at Mount Sinai New York, NY Disclosure
«Paradoxical» low-flow, low-gradient AS with preserved LV function: A Silent Killer
 «Paradoxical» low-flow, low-gradient AS with preserved LV function: A Silent Killer Philippe Pibarot, DVM, PhD, FACC, FAHA, FESC, FASE Canada Research Chair in Valvular Heart Diseases Université LAVAL
«Paradoxical» low-flow, low-gradient AS with preserved LV function: A Silent Killer Philippe Pibarot, DVM, PhD, FACC, FAHA, FESC, FASE Canada Research Chair in Valvular Heart Diseases Université LAVAL
Coronary Artery Bypass Graft: Monitoring Patients and Detecting Complications
 Coronary Artery Bypass Graft: Monitoring Patients and Detecting Complications Madhav Swaminathan, MD, FASE Professor of Anesthesiology Division of Cardiothoracic Anesthesia & Critical Care Duke University
Coronary Artery Bypass Graft: Monitoring Patients and Detecting Complications Madhav Swaminathan, MD, FASE Professor of Anesthesiology Division of Cardiothoracic Anesthesia & Critical Care Duke University
Disclosures Rebecca T. Hahn, MD, FASE
 The New ASE Guidelines for Native Valvular Regurgitation Mitral Regurgitation The New ASE Guidelines: Role of 2D/3D and CMR (With caveats and comments from R. Hahn) William A. Zoghbi MD, FASE, MACC Professor
The New ASE Guidelines for Native Valvular Regurgitation Mitral Regurgitation The New ASE Guidelines: Role of 2D/3D and CMR (With caveats and comments from R. Hahn) William A. Zoghbi MD, FASE, MACC Professor
Ejection across stenotic aortic valve requires a systolic pressure gradient between the LV and aorta. This places a pressure load on the LV.
 Valvular Heart Disease General Principles Etiology Cellular and molecular mechanism of valve damage Structural pathology Functional pathology - stenosis/regurgitation Loading conditions - pressure/volume
Valvular Heart Disease General Principles Etiology Cellular and molecular mechanism of valve damage Structural pathology Functional pathology - stenosis/regurgitation Loading conditions - pressure/volume
Hemodynamic Assessment. Assessment of Systolic Function Doppler Hemodynamics
 Hemodynamic Assessment Matt M. Umland, RDCS, FASE Aurora Medical Group Milwaukee, WI Assessment of Systolic Function Doppler Hemodynamics Stroke Volume Cardiac Output Cardiac Index Tei Index/Index of myocardial
Hemodynamic Assessment Matt M. Umland, RDCS, FASE Aurora Medical Group Milwaukee, WI Assessment of Systolic Function Doppler Hemodynamics Stroke Volume Cardiac Output Cardiac Index Tei Index/Index of myocardial
Ischemic Mitral Regurgitation
 Ischemic Mitral Regurgitation 1 / 6 2 / 6 3 / 6 Ischemic Mitral Regurgitation Background Myocardial infarction (MI) can directly cause (IMR), which has been touted as an indicator of poor prognosis in
Ischemic Mitral Regurgitation 1 / 6 2 / 6 3 / 6 Ischemic Mitral Regurgitation Background Myocardial infarction (MI) can directly cause (IMR), which has been touted as an indicator of poor prognosis in
Minimally Invasive Aortic Surgery With Emphasis On Technical Aspects, Extracorporeal Circulation Management And Cardioplegic Techniques
 Minimally Invasive Aortic Surgery With Emphasis On Technical Aspects, Extracorporeal Circulation Management And Cardioplegic Techniques Konstadinos A Plestis, MD System Chief of Cardiothoracic and Vascular
Minimally Invasive Aortic Surgery With Emphasis On Technical Aspects, Extracorporeal Circulation Management And Cardioplegic Techniques Konstadinos A Plestis, MD System Chief of Cardiothoracic and Vascular
The difficult patient with mitral regurgitation
 Clinical pathways The difficult patient with mitral regurgitation Stress echo can be the best tool Challenging cases Maria João Andrade, Lisbon PT Management of Severe Chronic Organic MR Echo Exercise
Clinical pathways The difficult patient with mitral regurgitation Stress echo can be the best tool Challenging cases Maria João Andrade, Lisbon PT Management of Severe Chronic Organic MR Echo Exercise
Les valvulopathies en sourdine: la valve mitrale Quoi faire devant une régurgitation mitrale sévère asymptomatique de type dégénérative?
 Réunion d automne de la SSC à Lucerne le 24.11.2011 Incertitudes dans le travail cardiologique quotidien Les valvulopathies en sourdine: la valve mitrale Quoi faire devant une régurgitation mitrale sévère
Réunion d automne de la SSC à Lucerne le 24.11.2011 Incertitudes dans le travail cardiologique quotidien Les valvulopathies en sourdine: la valve mitrale Quoi faire devant une régurgitation mitrale sévère
Prosthesis-Patient Mismatch in High Risk Patients with Severe Aortic Stenosis in a Randomized Trial of a Self-Expanding Prosthesis
 Prosthesis-Patient Mismatch in High Risk Patients with Severe Aortic Stenosis in a Randomized Trial of a Self-Expanding Prosthesis George L. Zorn, III On Behalf of the CoreValve US Clinical Investigators
Prosthesis-Patient Mismatch in High Risk Patients with Severe Aortic Stenosis in a Randomized Trial of a Self-Expanding Prosthesis George L. Zorn, III On Behalf of the CoreValve US Clinical Investigators
Severe aortic stenosis should be operated before symptom onset CONTRA. Helmut Baumgartner
 Severe aortic stenosis should be operated before symptom onset CONTRA Helmut Baumgartner Westfälische Wilhelms-Universität Münster Adult Congenital and Valvular Heart Disease Center Dept. of Cardiology
Severe aortic stenosis should be operated before symptom onset CONTRA Helmut Baumgartner Westfälische Wilhelms-Universität Münster Adult Congenital and Valvular Heart Disease Center Dept. of Cardiology
Understanding the guidelines for Interventions in MR. Ali AlMasood
 Understanding the guidelines for Interventions in MR Ali AlMasood Mitral regurgitation The most diverse from all acquired valve diseases About 50% of patients with an LVEF 35 percent had moderate to severe
Understanding the guidelines for Interventions in MR Ali AlMasood Mitral regurgitation The most diverse from all acquired valve diseases About 50% of patients with an LVEF 35 percent had moderate to severe
Emergency Intraoperative Echocardiography
 Emergency Intraoperative Echocardiography Justiaan Swanevelder Department of Anaesthesia, Glenfield Hospital University Hospitals of Leicester NHS Trust, UK Carl Gustav Jung (1875-1961) Your vision will
Emergency Intraoperative Echocardiography Justiaan Swanevelder Department of Anaesthesia, Glenfield Hospital University Hospitals of Leicester NHS Trust, UK Carl Gustav Jung (1875-1961) Your vision will
Mitral Valve Disease, When to Intervene
 Mitral Valve Disease, When to Intervene Swedish Heart and Vascular Institute Ming Zhang MD PhD Interventional Cardiology Structure Heart Disease Conflict of Interest None Current ACC/AHA guideline Stages
Mitral Valve Disease, When to Intervene Swedish Heart and Vascular Institute Ming Zhang MD PhD Interventional Cardiology Structure Heart Disease Conflict of Interest None Current ACC/AHA guideline Stages
The best in heart valve disease Aortic valve stenosis
 The best in heart valve disease Aortic valve stenosis Marie Moonen, MD, PhD Heart Valve Clinic, University of Liège, CHU Sart Tilman, BELGIUM My declaration of interest : I have nothing to declare Prevalence
The best in heart valve disease Aortic valve stenosis Marie Moonen, MD, PhD Heart Valve Clinic, University of Liège, CHU Sart Tilman, BELGIUM My declaration of interest : I have nothing to declare Prevalence
Michigan Society of Echocardiography 30 th Year Jubilee
 Michigan Society of Echocardiography 30 th Year Jubilee Stress Echocardiography in Valvular Heart Disease Moving Beyond CAD Karthik Ananthasubramaniam, MD FRCP (Glas) FACC FASE FASNC Associate Professor
Michigan Society of Echocardiography 30 th Year Jubilee Stress Echocardiography in Valvular Heart Disease Moving Beyond CAD Karthik Ananthasubramaniam, MD FRCP (Glas) FACC FASE FASNC Associate Professor
MITRAL VALVE PATHOLOGY WITH TRICUSPID REGURGITATION (AND PHT)
") UNIVERSITY OF PADUA, SCHOOL OF MEDICINE Department of Cardiac,Thoracic and Vascular Sciences Padua, Italy MITRAL VALVE PATHOLOGY WITH TRICUSPID REGURGITATION (AND PHT) Luigi P. Badano**, MD, PhD, FESC,
UNIVERSITY OF PADUA, SCHOOL OF MEDICINE Department of Cardiac,Thoracic and Vascular Sciences Padua, Italy MITRAL VALVE PATHOLOGY WITH TRICUSPID REGURGITATION (AND PHT) Luigi P. Badano**, MD, PhD, FESC,
Options for my no option Patients Treating Heart Conditions Via a Tiny Catheter
 Options for my no option Patients Treating Heart Conditions Via a Tiny Catheter Nirat Beohar, MD Associate Professor of Medicine Director Cardiac Catheterization Laboratory, Medical Director Structural
Options for my no option Patients Treating Heart Conditions Via a Tiny Catheter Nirat Beohar, MD Associate Professor of Medicine Director Cardiac Catheterization Laboratory, Medical Director Structural
Μαρία Μπόνου Διευθύντρια ΕΣΥ, ΓΝΑ Λαϊκό
 Μαρία Μπόνου Διευθύντρια ΕΣΥ, ΓΝΑ Λαϊκό Diastolic HF DD: Diastolic Dysfunction DHF: Diastolic HF HFpEF: HF with preserved EF DD Pathophysiologic condition: impaired relaxation, LV compliance, LV filling
Μαρία Μπόνου Διευθύντρια ΕΣΥ, ΓΝΑ Λαϊκό Diastolic HF DD: Diastolic Dysfunction DHF: Diastolic HF HFpEF: HF with preserved EF DD Pathophysiologic condition: impaired relaxation, LV compliance, LV filling
TSDA Boot Camp September 13-16, Introduction to Aortic Valve Surgery. George L. Hicks, Jr., MD
 TSDA Boot Camp September 13-16, 2018 Introduction to Aortic Valve Surgery George L. Hicks, Jr., MD Aortic Valve Pathology and Treatment Valvular Aortic Stenosis in Adults Average Course (Post mortem data)
TSDA Boot Camp September 13-16, 2018 Introduction to Aortic Valve Surgery George L. Hicks, Jr., MD Aortic Valve Pathology and Treatment Valvular Aortic Stenosis in Adults Average Course (Post mortem data)
Surgical AVR: Are there any contraindications? Pyowon Park Samsung Medical Center Seoul, Korea
 Surgical AVR: Are there any contraindications? Pyowon Park Samsung Medical Center Seoul, Korea Contents Decision making in surgical AVR in old age Clinical results of AVR with tissue valve Impact of 19mm
Surgical AVR: Are there any contraindications? Pyowon Park Samsung Medical Center Seoul, Korea Contents Decision making in surgical AVR in old age Clinical results of AVR with tissue valve Impact of 19mm
Hani K. Najm MD, Msc, FRCSC FACC, FESC President Saudi Society for Cardiac Surgeons Associate Professor of Cardiothoracic Surgery King Abdulaziz
 Hani K. Najm MD, Msc, FRCSC FACC, FESC President Saudi Society for Cardiac Surgeons Associate Professor of Cardiothoracic Surgery King Abdulaziz Cardiac Centre Riyadh, Saudi Arabia Decision process for
Hani K. Najm MD, Msc, FRCSC FACC, FESC President Saudi Society for Cardiac Surgeons Associate Professor of Cardiothoracic Surgery King Abdulaziz Cardiac Centre Riyadh, Saudi Arabia Decision process for
Assessing the Impact on the Right Ventricle
 Advances in Tricuspid Regurgitation Congress of the European Society of Cardiology (ESC) Munich, August 25-29, 2012 Assessing the Impact on the Right Ventricle Stephan Rosenkranz, MD Clinic III for Internal
Advances in Tricuspid Regurgitation Congress of the European Society of Cardiology (ESC) Munich, August 25-29, 2012 Assessing the Impact on the Right Ventricle Stephan Rosenkranz, MD Clinic III for Internal
TAVI- Is Stroke Risk the Achilles Heel of Percutaneous Aortic Valve Repair?
 TAVI- Is Stroke Risk the Achilles Heel of Percutaneous Aortic Valve Repair? Elaine E. Tseng, MD and Marlene Grenon, MD Department of Surgery Divisions of Adult Cardiothoracic and Vascular and Endovascular
TAVI- Is Stroke Risk the Achilles Heel of Percutaneous Aortic Valve Repair? Elaine E. Tseng, MD and Marlene Grenon, MD Department of Surgery Divisions of Adult Cardiothoracic and Vascular and Endovascular
Aortic stenosis aetiology: morphology of calcific AS,
 How to improve patient selection in aortic stenosis? Fausto J. Pinto, FESC Aortic stenosis aetiology: morphology of calcific AS, bicuspid valve, and rheumatic AS (Adapted from C. Otto, Principles of
How to improve patient selection in aortic stenosis? Fausto J. Pinto, FESC Aortic stenosis aetiology: morphology of calcific AS, bicuspid valve, and rheumatic AS (Adapted from C. Otto, Principles of
TRANSCATHETER AORTIC VALVE IMPLANTATION: PSCC EXPERIENCE DR HUSSEIN ALAMRI PSCC RIYADH
 TRANSCATHETER AORTIC VALVE IMPLANTATION: PSCC EXPERIENCE DR HUSSEIN ALAMRI PSCC RIYADH Available systems: Edwards (TA and TF) and Core valve. INTRODUCTION 3 4% 0f > 65 y. 30 40% of elderly denied surgery,.
TRANSCATHETER AORTIC VALVE IMPLANTATION: PSCC EXPERIENCE DR HUSSEIN ALAMRI PSCC RIYADH Available systems: Edwards (TA and TF) and Core valve. INTRODUCTION 3 4% 0f > 65 y. 30 40% of elderly denied surgery,.
Index. B B-type natriuretic peptide (BNP), 76
, 76") Index A ACCESS-EU registry, 158 159 Acute kidney injury (AKI), 76, 88 Annular enlargement, RV, 177 178 Annuloplasty chordal cutting, 113 complete ring, 99 etiology-specific ring, 100 evolution, 98 flexible
Index A ACCESS-EU registry, 158 159 Acute kidney injury (AKI), 76, 88 Annular enlargement, RV, 177 178 Annuloplasty chordal cutting, 113 complete ring, 99 etiology-specific ring, 100 evolution, 98 flexible
Expanding Relevance of Aortic Valve Repair Is Earlier Operation Indicated?
 Expanding Relevance of Aortic Valve Repair Is Earlier Operation Indicated? RM Suri, V Sharma, JA Dearani, HM Burkhart, RC Daly, LD Joyce, HV Schaff Division of Cardiovascular Surgery, Mayo Clinic, Rochester,
Expanding Relevance of Aortic Valve Repair Is Earlier Operation Indicated? RM Suri, V Sharma, JA Dearani, HM Burkhart, RC Daly, LD Joyce, HV Schaff Division of Cardiovascular Surgery, Mayo Clinic, Rochester,
Potential conflicts of interest
 Potential conflicts of interest Speaker's name: Petros Dardas MEDTRONIC proctor for TAVI Intermediate risk 83 FEMALE COAD SEVERE AS NYHA III Mean gradient 35 mmhg, AVA 0.45cm2, SVI 21ml/m2 Paradoxical
Potential conflicts of interest Speaker's name: Petros Dardas MEDTRONIC proctor for TAVI Intermediate risk 83 FEMALE COAD SEVERE AS NYHA III Mean gradient 35 mmhg, AVA 0.45cm2, SVI 21ml/m2 Paradoxical
Assessing Function by Echocardiography in VHD Asymptomatic Severe Organic MR. Dr. Julien Magne, PhD Sart Tilman Liège, BELGIUM
 Assessing Function by Echocardiography in VHD Asymptomatic Severe Organic MR Dr. Julien Magne, PhD Sart Tilman Liège, BELGIUM Conflict of Interest Disclosure None Why to assess LV function in asymptomatic
Assessing Function by Echocardiography in VHD Asymptomatic Severe Organic MR Dr. Julien Magne, PhD Sart Tilman Liège, BELGIUM Conflict of Interest Disclosure None Why to assess LV function in asymptomatic
Comprehensive Echo Assessment of Aortic Stenosis
 Comprehensive Echo Assessment of Aortic Stenosis Smonporn Boonyaratavej, MD, MSc King Chulalongkorn Memorial Hospital Bangkok, Thailand Management of Valvular AS Medical and interventional approaches to
Comprehensive Echo Assessment of Aortic Stenosis Smonporn Boonyaratavej, MD, MSc King Chulalongkorn Memorial Hospital Bangkok, Thailand Management of Valvular AS Medical and interventional approaches to
Echocardiography. Guidelines for Valve and Chamber Quantification. In partnership with
 Echocardiography Guidelines for Valve and Chamber Quantification In partnership with Explanatory note & references These guidelines have been developed by the Education Committee of the British Society
Echocardiography Guidelines for Valve and Chamber Quantification In partnership with Explanatory note & references These guidelines have been developed by the Education Committee of the British Society
22/06/2017. Oxford City. Transcatheter aortic valve replacement 2017 guidelines. 1. First time I have heard about it. 2.
 Oxford City Transcatheter aortic valve replacement 2017 guidelines Monday 19 th June Jim Newton Oxford Oxford University Hospitals NHS FT How familiar are you with TAVR? 1. First time I have heard about
Oxford City Transcatheter aortic valve replacement 2017 guidelines Monday 19 th June Jim Newton Oxford Oxford University Hospitals NHS FT How familiar are you with TAVR? 1. First time I have heard about
ESC/EACTS Guidelines for the Management of Valvular Heart Disease
 ES/EATS Guidelines for the Management of Valvular Heart Disease European Journal of ardio-thoracic Surgery 2012 - Why do we need new guidelines on the management of valvular disease? New evidence has been
ES/EATS Guidelines for the Management of Valvular Heart Disease European Journal of ardio-thoracic Surgery 2012 - Why do we need new guidelines on the management of valvular disease? New evidence has been
Reverse left atrium and left ventricle remodeling after aortic valve interventions
 Reverse left atrium and left ventricle remodeling after aortic valve interventions Alexandra Gonçalves, Cristina Gavina, Carlos Almeria, Pedro Marcos-Alberca, Gisela Feltes, Rosanna Hernández-Antolín,
Reverse left atrium and left ventricle remodeling after aortic valve interventions Alexandra Gonçalves, Cristina Gavina, Carlos Almeria, Pedro Marcos-Alberca, Gisela Feltes, Rosanna Hernández-Antolín,
25 different brand names >44 different models Sizes mm
 Types of Prosthetic Valves BIOLOGIC STENTED Porcine xenograft Pericardial xenograft STENTLESS Porcine xenograft Pericardial xenograft Homograft (allograft) Autograft PERCUTANEOUS MECHANICAL Bileaflet Single
Types of Prosthetic Valves BIOLOGIC STENTED Porcine xenograft Pericardial xenograft STENTLESS Porcine xenograft Pericardial xenograft Homograft (allograft) Autograft PERCUTANEOUS MECHANICAL Bileaflet Single
Catheter-based mitral valve repair MitraClip System
 Percutaneous Mitral Valve Repair: Results of the EVEREST II Trial William A. Gray MD Director of Endovascular Services Associate Professor of Clinical Medicine Columbia University Medical Center The Cardiovascular
Percutaneous Mitral Valve Repair: Results of the EVEREST II Trial William A. Gray MD Director of Endovascular Services Associate Professor of Clinical Medicine Columbia University Medical Center The Cardiovascular