Definition of Success and Surgical Results That Shouldn t Be a Hard Talk, Right?
|
|
|
- Melinda Davis
- 5 years ago
- Views:
Transcription
1 Definition of Success and Surgical Results That Shouldn t Be a Hard Talk, Right? Patrick M. McCarthy MD, FACC Executive Director of the Bluhm Cardiovascular Institute Chief of Cardiac Surgery Division Heller-Sacks Professor of Surgery in the Feinberg School of Medicine November 17, 2017 Session IV: Concomitant Ablation How I Do it and Why Nobu Eden Roc Hotel Miami Beach, Florida
2 Disclosures None
3 What is Success? statement recommends a 3 month blanking period during which recurrences are not counted. reaffirms the use of freedom from any atrial arrhythmia (e.g., AF, AT, AFL) greater than 30 seconds to be the gold standard for reporting the efficacy of AF ablation strict cutoff might underestimate the true benefit of ablation Heart Rhythm, 2017:10, in press





4 Heart Rhythm 2017;14:e275 e444
5 Heart Rhythm 2017;14:e275 e444 The writing group also believes that all trials should report single procedure, off AAD therapy efficacy for ablation with a minimum of 12 months follow-up. Slight variations in this endpoint have been used in several clinical trials, but ideally, all categories of recurrence should be reported transparently, such as freedom from AF separately from other atrial arrhythmia, one- and multiple-procedure success rates, and success on and off antiarrhythmic therapy. By reporting all of these variations, the reader can determine the most relevant outcome for themselves and can also easily compare results between clinical trials.
6 Trial vs Real World Atricure Post Approval Study Example
7 Challenges in the Non-Trial World (and for those who review my papers) Surgeons Don t Manage Meds Late After Surgery Referring Docs Don t Do Holter, Zio, TEE Patients feel fine and don t come back at 6, 12, 24 month etc intervals Sometimes you don t need a holter, zio and an EKG is enough (ie failure) How do we report single center non trial studies?

8 Ann Thorac Surg 2017;103:329-41

9 How to Monitor Success ECG: That s Not Enough Holter: Most Common PPM and Implantables may be Best
10 PPM Most Accurate Cardioversion Surgery Procedure Failure: 35 seconds of AF after 90 days
11 The EP/AF World is Different It s all about perspective If 4+ MR became trace after repair would that be a failure? Not to the surgeon or patient If 4+ MR became moderate (2+) after MitraClip would that be a success? Yes to IC, no to surgeon/fda, maybe to patient Is >30 seconds of VT/VF a failure of aa? Yes! To EP, surgeon, and the patient! Is >30 sec of PAF the same? Does it cause a stroke? No one knows


12 Monitor Options Zio and Reveal LINQ Water resistant 14 days continuous recording Phone app to log symptoms Receive/return via mail Implanted by injection 3 year battery Remote download of data
13 Ann Thorac Surg 2016;101:42 8
14 Ann Thorac Surg 2016;101:42 8
15 Conclusions ILR was equivalent at detecting ATAs when compared with Holter monitoring or ECG. However, the high rate of false-positive readings and the limited number of events available for review present barriers to broad implementation of this form of monitoring. Very few symptomatic events were AF on review. Ann Thorac Surg 2016;101:42 8
16 Should we Focus on Clinical Measures of Success? Free From Stroke; Cardioversion; Catheter Ablation; Coumadin
17 CHA 2 DS 2 -VASc Am J Medicine 2012;125(6): 603
18 Heart Rhythm2015;12: )
19 Heart Rhythm2015;12: )
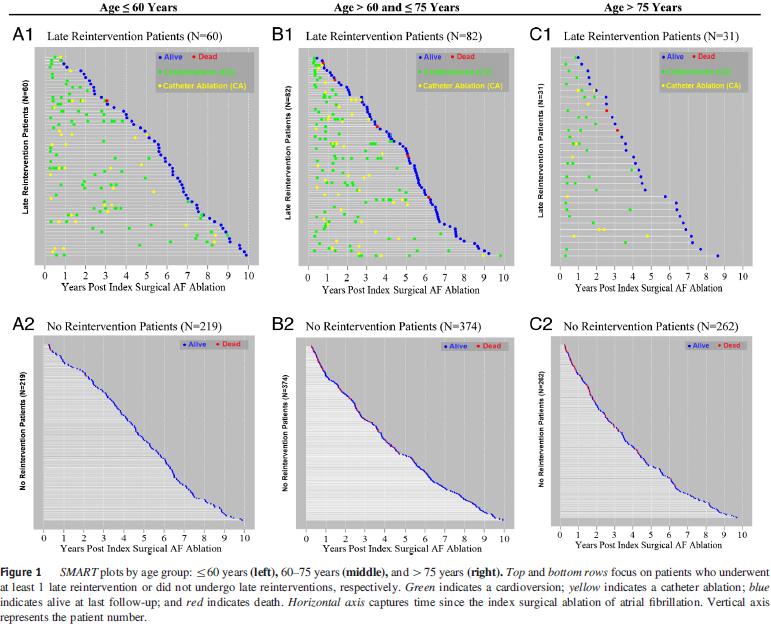
20 NMH: AF Ablation and Mitral Surgery June 06 to June MV patients 405 (71%) no intervention 169 (29%) intervention SR Fail CV CA Both 303 (53%) 102 (18%) % success 20% salvage SR 114 (67%)
21 Towards a Real World Approach to AF
22 What to Tell the Patient Before Surgery? Set Pre-op Expectations: Early AF recurrence is NOT a failure Meds; Monitoring (ppm, holter or zio); Frequency; Intervention (CV or CA) AF nurse ; printed materials for patient AND the referring cardiologist
23 Peri-op Meds Amiodarone 90% at DC Second Choice: The Prior AA Beta blocker: rate control 30% aren t on these due to bradycardia/heart block
24 Team Follow-up After Surgical Treatment of Atrial Fibrillation How do you make it happen? Develop care guidelines with all players - Cardiology, electrophysiology, cardiac surgery and patient - Based on the Expert Consensus Statement Communicate the plan Follow-up to keep the plan on track
25 Post AF Surgery Guidelines Phase I: DC to 3 months (Blanking Period) - Suppressive AAD and anticoagulation - Monitor for symptomatic arrhythmia and DCCV if needed - Phone follow-up with patient by AF nurse Phase II: 3-6 months (Cards?, EP?, You?) - H&P, ECG, extended cardiac monitoring - Consideration of discontinuing AAD at 3 months - Consideration of stopping anticoagulation (CHADS 2 or CHA 2 DS 2 VASc) - Phone follow-up by AF nurse
26 Post AF Surgery Guidelines Phase III: 1-2 years - At 6 months post-procedure and every 6 months for 2 years patients should have an ECG and a minimum of a Holter monitor - Phone follow-up with AF nurse Patients with Symptoms Suggestive of Arrhythmia - Patient activated cardiac event monitor - Referral for DCCV or catheter ablation if AF/AFL Patients with Implanted Cardiac Devices - Pacemaker, defibrillator, implanted cardiac monitor - Program to detect and store AHR to substitute external monitoring
27 Summary Failure is an OK term (still in AF and we all give up) Free from CV, CA Free from CVA, coumadin, aa Not AF at last follow-up (extended monitoring) Trials = strict timelines
28
29 Summary AF in the early post-operative period does not mean failure. Cardioversion or referral to EP for ablation can increase the success of procedure Monitoring is critical - Prior symptoms may no longer exist - Regular pulse may be controlled flutter
30 Summary Repeated CV after 6 months not usually useful. - Consider referral to EP for ablation - Consider re-initiation of suitable AAD Some patients who fail AF surgery are not appropriate to send for intervention - Stop the AAD they were discharged on - Evaluate appropriate anticoagulation
31

32 Peri-op Meds Amiodarone 90% at DC Second Choice: The Prior AA Beta blocker: rate control 30% aren t on these due to bradycardia/heart block
33 Team Follow-up After Surgical Treatment of Atrial Fibrillation How do you make it happen? Develop care guidelines with all players - Cardiology, electrophysiology, cardiac surgery and patient - Based on the Expert Consensus Statement Communicate the plan Follow-up to keep the plan on track
34 Summary AF in the early post-operative period does not mean failure. Cardioversion or referral to EP for ablation can increase the success of procedure Monitoring is critical - Prior symptoms may no longer exist - Regular pulse may be controlled flutter
35 Summary Repeated CV after 6 months not usually useful. - Consider referral to EP for ablation - Consider re-initiation of suitable AAD Some patients who fail AF surgery are not appropriate to send for intervention - Stop the AAD they were discharged on - Evaluate appropriate anticoagulation
36 CHA 2 DS 2 -VASc Am J Medicine 2012;125(6): 603

37 Ann Thorac Surg 2016;101:42 8

38 Ann Thorac Surg 2016;101:42 8
39 Conclusions ILR was equivalent at detecting ATAs when compared with Holter monitoring or ECG. However, the high rate of false-positive readings and the limited number of events available for review present barriers to broad implementation of this form of monitoring. Very few symptomatic events were AF on review. Ann Thorac Surg 2016;101:42 8
40 Monitor Options Zio and Reveal LINQ Water resistant 14 days continuous recording Phone app to log symptoms Receive/return via mail Implanted by injection 3 year battery Remote download of data
 intervention SR Fail CV CA Both 303 (53%) 102 (18%) 119 20 30 73% success 20% salvage SR 114")
41 NMH: AF Ablation and Mitral Surgery June 06 to June MV patients 405 (71%) no intervention 169 (29%) intervention SR Fail CV CA Both 303 (53%) 102 (18%) % success 20% salvage SR 114 (67%)

42 Monitoring ECG: That s Not Enough Holter: Most Common
43 PPM Most Accurate Cardioversion Surgery Procedure Failure: 35 seconds of AF after 90 days

44 What is Success? Free From AF Off Antiarrthymics 3 month blanking period.freedom from any atrial arrhythmia (e.g., AF, AT, AFL) greater than 30 seconds to be the gold standard for reporting the efficacy of AF ablation Heart Rhythm, 2017:10, in press
45 Freedom from AF statement recommends a 3 month blanking period during which recurrences are not counted. reaffirms the use of freedom from any atrial arrhythmia (e.g., AF, AT, AFL) greater than 30 seconds to be the gold standard for reporting the efficacy of AF ablation strict cutoff might underestimate the true benefit of ablation Heart Rhythm, 2017:10, in press
 greater than 30 seconds off antiarrhythmic therapy as the gold standard for reporting the efficacy of AF")
46 Heart Rhythm 2017;14:e275 e444 The consensus statement reaffirms the use of freedom from any atrial arrhythmia (e.g., AF, AT, or AFL) greater than 30 seconds off antiarrhythmic therapy as the gold standard for reporting the efficacy of AF ablation.
47 Heart Rhythm 2017;14:e275 e444 The writing group also believes that all trials should report single procedure, off AAD therapy efficacy for ablation with a minimum of 12 months follow-up. Slight variations in this endpoint have been used in several clinical trials, but ideally, all categories of recurrence should be reported transparently, such as freedom from AF separately from other atrial arrhythmia, one- and multiple-procedure success rates, and success on and off antiarrhythmic therapy. By reporting all of these variations, the reader can determine the most relevant outcome for themselves and can also easily compare results between clinical trials.
48 Heart Rhythm 2017;14:e275 e444

49 AF Management with Valve Surgery in 17 Latest Guidelines Why? What s the Evidence? How? Lesion sets; Technologies; LAA Outcomes? How to Measure them

50 Surgical ablation for atrial fibrillation (AF) can be performed without additional risk of operative mortality or major morbidity, and is recommended at the time of concomitant mitral operations to restore sinus rhythm. (Class I, Level A) Ann Thorac Surg 2017;103:

51 Heart Rhythm, 2017:10, in press
52 Ann Thorac Surg 2017;103:329-41
53 Why Such Strong Guidelines?
54 Prospective Randomized Trials of Permanent AF Ablation with Mitral Valve Surgery Number Control Treated Trials, Year of Pts Technology 12 Month * NSR 12 Month NSR Deneke et al., Unipolar Cooled RF 26.7% 80% (p < 0.01) Schuetz et al., Microwave 33.3% 80% (p = 0.036) Akpinar et al., Unipolar RF 9.4% 93.6% (p =0.0001) Abreu Filho et al., Unipolar Cooled RF 26.9% 79.4% (p = 0.001) Doukas et al., 2005 Blomström- Lunqvist 2007 Chevalier Unipolar RF 4.5% 44.4% (p = 0.001) 69 Cryoablation 42.9% 73.3%(p=0.013) 43 Unipolar RF 4% 57% (p=0.004) Gillinov Radiofrequency and cryo 29.4% 63.2% (p<0.001)

55 Conclusions: Contemporary utilization of SA is increasing across all operative categories. Performance of SA is accompanied by a 30-day reduction in mortality and stroke. These findings further refine our understanding of the role of SA in the treatment of AF. Ann Thorac Surg 2017;104:

56 Unmatched: Treated PAF, Untreated PAF and No history of AF P<

57 PS Matched Survival
58 Does AF Treatment Change the Curve?
59 Maze Surgery is Complicated Can It Be Effective and Efficient?
60 Prospective Randomized Trials of Permanent AF Ablation with Mitral Valve Surgery Number Control Treated Trials, Year of Pts Technology 12 Month * NSR 12 Month NSR Deneke et al., Unipolar Cooled RF 26.7% 80% (p < 0.01) Schuetz et al., Microwave 33.3% 80% (p = 0.036) Akpinar et al., Unipolar RF 9.4% 93.6% (p = ) Abreu Filho et al., Unipolar Cooled RF 26.9% 79.4% (p = 0.001) Doukas et al., 2005 Blomström- Lunqvist 2007 Chevalier Unipolar RF 4.5% 44.4% (p = 0.001) 69 Cryoablation 42.9% 73.3%(p=0.013) 43 Unipolar RF 4% 57% (p=0.004) Gillinov Radiofrequency and cryo 29.4% 63.2% (p<0.001)
61 AF with MR is NOT The Same as Lone AF Volume Overload: Corrected by Surgery Pressure Overload: Corrected by Surgery Atrial Fibrosis/myopathy/hypertrophy: Anatomically Scattered, not at PV/LA junction Lessons from Basic Science and Lone AF Patients are of Limited Use, or Irrelevant


62 Cox Maze Procedure Pulmonary Vein Box Lesion MV Annulus to Box Lesion SVC-IVC TV Annulus flutter lines X2 Excision of LAA


63


64 MV Annulus Lesion

65
66 Ann Thorac Surg, 103(6):
67

68 Cryoablation: Not Just for Reops Anymore

69
70 Propensity matched groups FFAF at last FU, p=0.10 FFAF at last FU off AA, p=.09 80% 80% 60% 40% 20% 70% 89/127 79% 98/124 60% 40% 20% 69% 82/119 79% 86/109 0% LA BA 0% LA BA Pre-discharge PPM, p=0.57 Annualized Stroke rate per 10 person/year, p= % 10% 5% 0% 10% 14/147 LA 12% 17/147 BA LA 0.08 BA
71 What About the Appendage?

72 The atrial appendage is the source of stroke in 91% of non-rheumatic AF and 57% in rheumatic AF


73 J Thorac Cardiovasc Surg 2016;152:


74 European Journal of Cardio-Thoracic Surgery 45 (2014) patients, serial CT imaging over 3 year follow-up CONCLUSION: This is the first prospective trial in which concomitant epicardial LAA occlusion using this novel epicardial LAA clip device is 100% effective, safe and durable in the long term. Closure of the LAA by epicardial clipping is applicable to all-comers regardless of LAA morphology. Minimal access epicardial LAA clip closure may become an interesting therapeutic option for patients in AF who are not amenable to anticoagulation and/or catheter closure. Further data are necessary to establish LAA occlusion as a true and viable therapy for stroke prevention.
. 97% Use with MV.")
75 Conclusions Not Only Safe, it May Reduce Peri-op Risk Effective Surgery Can Be Efficient, even with LA Only Lesions (RA Ablation is Easy if Needed). 97% Use with MV. Close or Excise Appendage
76
; Frequency;")
77 What to Tell the Patient Before Surgery? Set Pre-op Expectations: Early AF recurrence is NOT a failure Meds; Monitoring (ppm, holter or zio); Frequency; Intervention (CV or CA) AF nurse ; printed materials for patient AND the referring cardiologist

78 Post AF Surgery Guidelines Phase I: DC to 3 months (Blanking Period) - Suppressive AAD and anticoagulation - Monitor for symptomatic arrhythmia and DCCV if needed - Phone follow-up with patient by AF nurse Phase II: 3-6 months (Cards?, EP?, You?) - H&P, ECG, extended cardiac monitoring - Consideration of discontinuing AAD at 3 months - Consideration of stopping anticoagulation (CHADS 2 or CHA 2 DS 2 VASc) - Phone follow-up by AF nurse

79 Peri-op Meds Amiodarone 90% at DC Second Choice: The Prior AA Beta blocker: rate control 30% aren t on these due to bradycardia/heart block

80 J Thorac Cardiovasc Surg 2016;151:
81 If You Don t Detect AF is it Safe to Stop A/C? What s the Stroke Risk?
:")
82 CHA 2 DS 2 -VASc Am J Medicine 2012;125(6): 603

83 Ann Thorac Surg, 2017;104:
 off Coumadin Stroke rate 0.")
84 NM Freedom from Coumadin and Stroke At last follow-up, 496/935 patients (53%) off Coumadin Stroke rate 0.8%/year in AF Ablation MV surgery patients
85 Ann Thorac Surg 2017;103: After SA for AF, full anticoagulation therapy is common and reasonable until durable rhythm restoration is established, provided the patient otherwise meets criteria for the safe administration of systemic anticoagulant agents. Anticoagulation therapy is commonly continued until a stable sinus rhythm is documented by at least a 24-hour Holter monitor off all antiarrhythmic drugs, often between 2 and 6 months postoperatively. It is also common practice to obtain an echocardiogram before discontinuing anticoagulation to ensure adequate LA emptying by the absence of spontaneous LA echocardiography contrast.

86 Post AF Surgery Guidelines Phase III: 1-2 years - At 6 months post-procedure and every 6 months for 2 years patients should have an ECG and a minimum of a Holter monitor - Phone follow-up with AF nurse Patients with Symptoms Suggestive of Arrhythmia - Patient activated cardiac event monitor - Referral for DCCV or catheter ablation if AF/AFL Patients with Implanted Cardiac Devices - Pacemaker, defibrillator, implanted cardiac monitor - Program to detect and store AHR to substitute external monitoring
87 Post AF Surgery Guidelines 1 month 3 months 6 months 12 months 18 months 24 months H & P * * * * * * ECG * * * * * * Medication review Antiarrhythmic * STOP * * * * * Anticoagulation * * STOP Extended Monitoring Cardioversion Catheter Ablation * * * * * 6-8 weeks Consider
88 NMH AF Surgery (N=989) June 06 to June 16 60% 50% 40% 30% 20% 10% Left atrial Biatrial CM III PVI 0% Mitral Surgery All Other n=597 n=392
89 NMH AF Surgery (N=989) June 06 to June 16 60% 50% 40% 30% 20% 10% PAF Persistent LSP 0% Mitral Surgery All Others

90 Summary AF in the early post-operative period does not mean failure. Cardioversion or referral to EP for ablation can increase the success of procedure Monitoring is critical - Prior symptoms may no longer exist - Regular pulse may be controlled flutter

91 Summary Repeated CV after 6 months not usually useful. - Consider referral to EP for ablation - Consider re-initiation of suitable AAD Some patients who fail AF surgery are not appropriate to send for intervention - Stop the AAD they were discharged on - Evaluate appropriate anticoagulation
92

93 Team Follow-up After Surgical Treatment of Atrial Fibrillation How do you make it happen? Develop care guidelines with all players - Cardiology, electrophysiology, cardiac surgery and patient - Based on the Expert Consensus Statement Communicate the plan Follow-up to keep the plan on track


94 This important manuscript considers many of the factors that are important in the decision making process for the surgical treatment of atrial fibrillation. A clear treatment algorithm is offered which can help surgeons increase their success, to the obvious potential benefit for patients. Patrick M. McCarthy, et al. J. Thorac. Cardiovasc. Surg. Apr 01, 2010; 139:

95 Controversy About AF Ablation Lesion Set Strong proponents of Cox Maze IV Biatrial lesions 1, 2 Data Indicating Equal Efficacy of BA vs. LA lesions 3, 4 Increased Risk with Biatrial vs. Left Atrial Only 4,5 1 Henn MC, Lancaster TS, Miller JR, Sinn LA, Schuessler RB, Moon MR, et al. Late outcomes after the Cox maze IV procedure for atrial fibrillation. J Thorac Cardiovasc Surg. 2015;150(5): Ad N, Henry L, Massimiano P, Pritchard G, Holmes SD. The state of surgical ablation for atrial fibrillation in patients with mitral valve disease. Current opinion in cardiology. 2013;28(2): Gillinov AM, Gelijns AC, Parides MK, DeRose JJ, Jr., Moskowitz AJ, Voisine P, et al. Surgical ablation of atrial fibrillation during mitral-valve surgery. N Engl J Med. 2015;372(15): Phan K, Xie A, Tsai YC, Kumar N, La Meir M, Yan TD. Biatrial ablation vs. left atrial concomitant surgical ablation for treatment of atrial fibrillation: a meta-analysis. Europace: European pacing, arrhythmias, and cardiac electrophysiology : journal of the working groups on cardiac pacing, arrhythmias, and cardiac cellular electrophysiology of the European Society of Cardiology. 2015;17(1): Soni LK, Cedola SR, Cogan J, Jiang J, Yang J, Takayama H, et al. Right atrial lesions do not improve the efficacy of a complete left atrial lesion set in the surgical treatment of atrial fibrillation, but they do increase procedural morbidity. The Journal of thoracic and cardiovascular surgery. 2013;145(2):356-61

96 The Mechanism of AF in Our Surgical Patients is More Complicated than for Most Lone AF Patients and Experimental Studies And the Approach in Simple Patients Isn t All That Clear

97 J Am Coll Cardiol 2017;69:303-21

98 AF with MR is NOT The Same as Lone AF Volume Overload: Corrected by Surgery Pressure Overload: Corrected by Surgery Atrial Fibrosis/myopathy/hypertrophy: Anatomically Scattered, not at PV/LA junction Lessons from Basic Science and Lone AF Patients are of Limited Use, or Irrelevant
99 N Engl J Med 2015;372:
100 Treating The Mitral Treats the AF Adding Left Atrial Lesions (location of the Pathologic Change) Increases Success. For MR patients Do RA lesions Add Even More? Is There a Price for BA Lesions?

101 Ann Thorac Surg, in press 2017
 AF pre-op 724 (86%) ablation 616 (79%) BA or LA lesion sets with cryo")

102 Methods NMH 4-04 thru 6-14 Mitral surgery +/- other 2137 Mitral Surgery 838 (39%) AF pre-op 724 (86%) ablation 616 (79%) BA or LA lesion sets with cryo and/or bipolar RF available for analysis 359 (58%) LA lesion set 257 (42%) BA lesion set Lesion set was at discretion of surgeon based on patient characteristics
103 Characteristics of Original Groups Variable Left Only (N=359) Biatrial (N=257) P-value Age, years Ejection Fraction, Median (Q1, Q3) 55.0 (50.0, 61.0) 55.0 (45.0, 60.0) Cardiopulmonary Bypass time (min), median (Q1, Q3) (97.0, 154.0) (110.0, 156.0) 0.01 Repeat Sternotomy 86 (24%) 63 (25%) 0.87 Tricuspid Valve Surgery, No. (%) 92(26%) 158(61%) <.001 Mitral Valve repair 218 (61%) 145 (56%) 0.28 Mitral Valve Replacement 141 (39%) 112( 44%) 0.28 Mechanical valve 10 (7%) 4 (4% ) 0.28 AF duration, years 1.0 (0.5, 5.0) 4.0 (1.0, 10.5) <.001 Left Atrial Size, Median (Q1, Q3) 4.6 (4.1, 5.2) 4.8 (4.2, 5.3) Paroxysmal AF 223(62%) 86(33%) <.001 Post-Operative Length of Stay (Days), Median (Q1, Q3) 7.0 (6.0, 9.0) 8.0 (6.0, 10.0) Day Mortality, No. (%) 7 (2%) 7 (3%) 0.53
104 Characteristics of PS-Matched Groups Variable Left Only (N=147) Biatrial (N=147) P-value Age, years Ejection Fraction, Median (Q1, Q3) 55.0 (50.0, 60.0) 55.0 (45.0, 60.0) 0.75 Cardiopulmonary Bypass time (min), median (Q1, Q3) (110.0, 162.0) (110.0, 160.0) 0.83 Repeat Sternotomy 38 (26%) 36 (24%) 0.79 Tricuspid Valve Surgery, No. (%) 67(46%) 69(47%) 0.82 Mitral Valve repair 82 (56%) 82 (56%) 1.00 Mitral Valve Replacement 65 (44%) 65( 44%) 1.00 Mechanical valve 6 (9%) 4 (6% ) 0.74 AF duration, years 2.0 (0.5, 9.0) 3.0 (1.0, 8.0) 0.23 Left Atrial Size, Median (Q1, Q3) 4.9 (4.3, 5.4) 4.7 (4.2, 5.2) 0.12 Paroxysmal AF 62(42%) 63(43%) 0.78 Post-Operative Length of Stay (Days), Median (Q1, Q3) 7.0 (6.0, 10.0) 7.0 (5.0, 10.0) Day Mortality, No. (%) 4 (3%) 4 (3%) 1.00

105 Propensity matched groups FFAF at last FU, p=0.10 FFAF at last FU off AA, p=.09 80% 80% 60% 40% 20% 70% 89/127 79% 98/124 60% 40% 20% 69% 82/119 79% 86/109 0% LA BA 0% LA BA Pre-discharge PPM, p=0.57 Annualized Stroke rate per 10 person/year, p= % 10% 5% 0% 10% 14/147 LA 12% 17/147 BA LA 0.08 BA
106 Are There High Risk Subgroups Who May Benefit from BA, More Extensive Lesions?

107 No Difference in Matched High Risk Subgroups: FFAF off AA Last F/up LSP/Persistent: 71.4% BA vs. 66.2% LA; p=0.51 Increasing LA Size: OR=0.85; p=0.52 Increasing AF Duration: OR=0.96; p=0.13 Also No differences in CVA; Coumadin use; PPM

108 J Thorac Cardiovasc Surg 2010; 139:860-7 Failures Don t Often Come from the RA and, if so, are quick and easy to treat as an outpatient
109 What Have Others Found Recently?

110 Conclusions: PVI is associated with lower rhythm success than an extended left atrial lesion set. The addition of a right atrial lesion to an extended left atrial lesion set does not improve efficacy, but it does increase the rate of pacemaker placement for sinus dysfunction. Adding an LAA lesion may confer additional efficacy when added to a lesion set that includes PVI + MV. (J Thorac Cardiovasc Surg 2013;145:356-63)
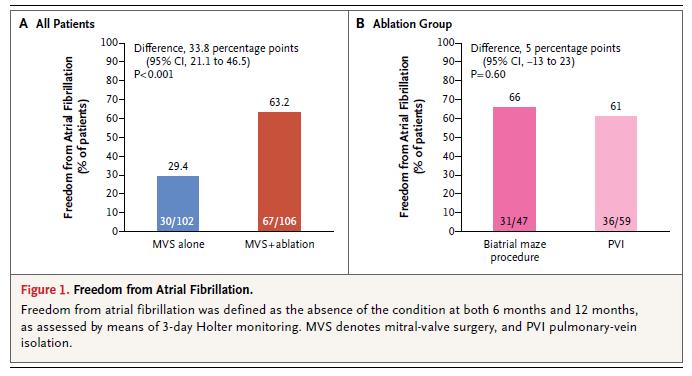
111 .There was no significant difference in the rate of freedom from atrial fibrillation between patients who underwent pulmonary-vein isolation and those who underwent the biatrial maze procedure (61.0% and 66.0%, respectively; P=0.60). N Eng J Med 2015;372(15):
112 532 patients with Maze IV 44 pts with left only lesions The success rates were reported for both the biatrial CMPIV and the left-sided CMPIV combined. The left sided CMPIV lesion set was included in the analysis because the success rates were observed to be similar to that of the biatrial CMPIV. However, this group of patients was highly selected. In our center, a left-sided CMPIV was chosen for patients with paroxysmal AF, left atrial size<5.0 cm, and no evidence of right atrial enlargement. In this selected group, late efficacy was good. J Thorac Cardiovasc Surg 2015;150(5):
, whereas a more extensive lesion set is referred to as a box lesion in combination with connecting lines to the LA")
113 800 patients in study 110 (14%) LA only and 682 Cox Maze LA-only ablation procedures included bilateral PVI (n = 82) with bipolar radiofrequency. A PVI-only procedure is referred to as bilateral PVI (or bilateral antral PVI), whereas a more extensive lesion set is referred to as a box lesion in combination with connecting lines to the LA appendage and the mitral valve isthmus endocardially and epicardially over the coronary sinus. PVI was accomplished with four to six repeated applications of bipolar radiofrequency. LA lesion set procedures (n = 28) were performed according to the Cox maze III/IV lesion scheme only on the left atrium by using either a combination of bipolar radiofrequency and cryothermal energy or cryothermal energy only. Ann Thorac Surg 2017;103:58-65
114 Ann Thorac Surg 2017;103:58-65 Propensity score matched outcomes LA-only (n= 93) Cox Maze (n=93) p value SR without AAD, 6M 80% 75% 0.41 SR without AAD, 12M 85% 83% 0.74 SR without AAD, 24M 75% 86% 0.13 Follow-up cardioversion 14% 17% 0.54 Folllow-up catheter ablation 7% 5% 0.76 Freedom from embolic stroke 95.1% 98.9% 0.21 Freedom from TIA 90.1% 93.0% 0.53

115 Europace (2015) 17, Biatrial and LA ablations produced comparable 30- day and late mortality but LA was associated with significantly reduced permanent pacemaker implantation rates. Biatrial ablation appeared to be more efficacious than LA ablation in achieving SR at 1 year, but this difference was not maintained beyond 1 year.


116 Permanent Pacemaker Implant 17.3% in ablation group vs. 5.5% in isolated Mitral Valve P= % in concomitant AVR vs. 5% in stand alone Cox Maze IV P=

117 Risk Factors for PPM Post-AF Ablation: Northwestern All Surgery
118 I d Rather Have a Pacemaker Than a Failed Ablation I d Rather Have a Late Right Side Ablation Than a Pacemaker the Rest of My Life!
119

120 Summary A Series Needs a Comparison: You Can t Say it only Works in Uncomplicated AF if you didn t use it in more Complex Patients
121 Why This Study? Northwestern Has Extensive Experience with Both Lesion Sets Hypothesis: - In mitral valve surgery patients, left atrial only (LA) and biatrial (BA) lesions result in similar outcomes Objectives: - Determine effectiveness of AF treatment with BA vs LA lesions - Determine postoperative complication rate in different lesion set groups - Determine possible subsets that may benefit

122 Ann Thorac Surg, in press 2016

123 Ann Thorac Surg 2017;103:58-65
124 Our study clearly demonstrates that early to intermediate success rates can be reasonably achieved with LA-only surgical ablation procedures in patients with no significant clinical predictors of failure. However, the results of the multivariate prediction models in this study should be evaluated with caution. Although these models provide initial evidence that ablation procedures confined to the LA may have reduced success in patients with traditional predictors of failure, the small sample size and event rate limit the generalizability and reliability of these results. Ann Thorac Surg 2017;103:58-65

125 Presented at The Society of Thoracic Surgeons 52 nd Annual Meeting, January 25, 2016, Phoenix, AZ Of 914 patients studied, 115 had LA only lesions
126 124 patients between undergoing AVR +/- CAB J Heart Valve Dis 2012;21:350-57

127 J Heart Valve Dis 2012;21:350-57
128




129 Unmatched groups FFAF at last FU, p=0.57 FFAF at last FU off AA, p= % 80% 60% 40% 20% 0% 75% 231/306 LA BA 73% 159/217 60% 40% 20% 0% 75% 210/280 LA 72% 143/198 BA Pre-discharge PMM, p=0.006 Stroke Rate per 10 person/year, p= % % 5% 0% 7% 24/359 LA 13% 34/257 BA LA BA
130 Long term survival of the original groups


131 Perioperative complications in propensity matched groups p=0.32 Left only Biatrial 44 30% 52 35% % 95 65% No complications Complications No complications Complications

132 Long term survival in propensity matched groups
Surgical Ablation: Which Lesion Set for Which Patient?
 Surgical Ablation: Which Lesion Set for Which Patient? Patrick M. McCarthy MD, FACC Director of the Bluhm Cardiovascular Institute Chief of Cardiac Surgery Division Heller-Sacks Professor of Surgery in
Surgical Ablation: Which Lesion Set for Which Patient? Patrick M. McCarthy MD, FACC Director of the Bluhm Cardiovascular Institute Chief of Cardiac Surgery Division Heller-Sacks Professor of Surgery in
Mitral Repair/AF Ablation Sternotomy Approach
 Mitral Repair/AF Ablation Sternotomy Approach Patrick M. McCarthy MD, FACC Executive Director of the Bluhm Cardiovascular Institute Chief of Cardiac Surgery Division Heller-Sacks Professor of Surgery in
Mitral Repair/AF Ablation Sternotomy Approach Patrick M. McCarthy MD, FACC Executive Director of the Bluhm Cardiovascular Institute Chief of Cardiac Surgery Division Heller-Sacks Professor of Surgery in
Should Paroxysmal Atrial Fibrillation be Treated During Cardiac Surgery?
 Should Paroxysmal Atrial Fibrillation be Treated During Cardiac Surgery? Patrick M. McCarthy MD, Adarsh Manjunath, BA, Jane Kruse, RN, BSN, Adin-Cristian Andrei, PhD, Zhi Li, MS, Edwin C. McGee, MD, S.
Should Paroxysmal Atrial Fibrillation be Treated During Cardiac Surgery? Patrick M. McCarthy MD, Adarsh Manjunath, BA, Jane Kruse, RN, BSN, Adin-Cristian Andrei, PhD, Zhi Li, MS, Edwin C. McGee, MD, S.
Surgical AF Ablation : Lesion Sets and Energy Sources. What are the data? Steven F Bolling, MD Cardiac Surgery University of Michigan
 Surgical AF Ablation : Lesion Sets and Energy Sources What are the data? Steven F Bolling, MD Cardiac Surgery University of Michigan Disclosures Consultant/Advisory Board: Abbott, Edwards Lifesciences
Surgical AF Ablation : Lesion Sets and Energy Sources What are the data? Steven F Bolling, MD Cardiac Surgery University of Michigan Disclosures Consultant/Advisory Board: Abbott, Edwards Lifesciences
Stand alone maze: when and how?
 Stand alone maze: when and how? Dong Seop Jeong Department of Thoracic and Cardiovascular Surgery, HVSI Samsung Medical Center Type of atrial fibrillation First diagnose AF Paroxysmal AF: self-terminating
Stand alone maze: when and how? Dong Seop Jeong Department of Thoracic and Cardiovascular Surgery, HVSI Samsung Medical Center Type of atrial fibrillation First diagnose AF Paroxysmal AF: self-terminating
AATS STARS Meeting Miami Beach November 17, 2017
 The New Surgical The Heart Ablation Hospital Guidelines AATS STARS Meeting Miami Beach November 17, 2017 The Heart Hospital Baylor Plano Plano, Texas James R. Edgerton, MD, FACS, FACC, FHRS Surgical Director
The New Surgical The Heart Ablation Hospital Guidelines AATS STARS Meeting Miami Beach November 17, 2017 The Heart Hospital Baylor Plano Plano, Texas James R. Edgerton, MD, FACS, FACC, FHRS Surgical Director
Surgical Ablation for Lone AF: What have we learned after 30 years?
 Surgical Ablation for Lone AF: What have we learned after 30 years? Ralph J. Damiano, Jr., MD Evarts A. Graham Professor of Surgery Chief of Cardiothoracic Surgery Vice Chairman, Department of Surgery
Surgical Ablation for Lone AF: What have we learned after 30 years? Ralph J. Damiano, Jr., MD Evarts A. Graham Professor of Surgery Chief of Cardiothoracic Surgery Vice Chairman, Department of Surgery
New Guidelines: Surgical Ablation of Atrial Fibrillation. Niv Ad, MD
 New Guidelines: Surgical Ablation of Atrial Fibrillation Niv Ad, MD Potential conflicts of interest Niv Ad, MD I have the following potential conflicts of interest to report: Atricure Inc.: Medtronic:
New Guidelines: Surgical Ablation of Atrial Fibrillation Niv Ad, MD Potential conflicts of interest Niv Ad, MD I have the following potential conflicts of interest to report: Atricure Inc.: Medtronic:
Biatrial Maze or PVI to Ablate Afib? Marc Gillinov, MD
 Biatrial Maze or PVI to Ablate Afib? Marc Gillinov, MD Disclosures Consultant/Speaker AtriCure Medtronic CryoLife Edwards Abbott Research Funding Abbott Equity Interest Clear Catheter Cleveland Clinic
Biatrial Maze or PVI to Ablate Afib? Marc Gillinov, MD Disclosures Consultant/Speaker AtriCure Medtronic CryoLife Edwards Abbott Research Funding Abbott Equity Interest Clear Catheter Cleveland Clinic
The Journal of Thoracic and Cardiovascular Surgery
 Accepted Manuscript Judgement Day: Should You Add Atrial Fibrillation Ablation? Dr. Patrick M. McCarthy, MD PII: S0022-5223(18)32917-9 DOI: https://doi.org/10.1016/j.jtcvs.2018.11.004 Reference: YMTC 13719
Accepted Manuscript Judgement Day: Should You Add Atrial Fibrillation Ablation? Dr. Patrick M. McCarthy, MD PII: S0022-5223(18)32917-9 DOI: https://doi.org/10.1016/j.jtcvs.2018.11.004 Reference: YMTC 13719
Clinical Practice Guidelines and the Under Treatment of Concomitant AF Vinay Badhwar, MD
 Clinical Practice Guidelines and the Under Treatment of Concomitant AF Vinay Badhwar, MD Gordon F. Murray Professor and Chairman Department of Cardiovascular & Thoracic Surgery WVU Heart and Vascular Institute
Clinical Practice Guidelines and the Under Treatment of Concomitant AF Vinay Badhwar, MD Gordon F. Murray Professor and Chairman Department of Cardiovascular & Thoracic Surgery WVU Heart and Vascular Institute
SURGICAL ABLATION OF ATRIAL FIBRILLATION DURING MITRAL VALVE SURGERY THE CARDIOTHORACIC SURGICAL TRIALS NETWORK
 SURGICAL ABLATION OF ATRIAL FIBRILLATION DURING MITRAL VALVE SURGERY THE CARDIOTHORACIC SURGICAL TRIALS NETWORK Marc Gillinov, M.D. For the CTSN Investigators ACC Late Breaking Clinical Trials March 16,
SURGICAL ABLATION OF ATRIAL FIBRILLATION DURING MITRAL VALVE SURGERY THE CARDIOTHORACIC SURGICAL TRIALS NETWORK Marc Gillinov, M.D. For the CTSN Investigators ACC Late Breaking Clinical Trials March 16,
Atrial Fibrillation Ablation: in Whom and How
 Update on Consensus Statement on Management of Atrial Fibrillation: EHRA 2012 Atrial Fibrillation Ablation: in Whom and How Update of HRS/EHRA AF/ECAS Ablation Document 2012 Anne M Gillis MD FHRS Professor
Update on Consensus Statement on Management of Atrial Fibrillation: EHRA 2012 Atrial Fibrillation Ablation: in Whom and How Update of HRS/EHRA AF/ECAS Ablation Document 2012 Anne M Gillis MD FHRS Professor
The EP Perspective: Should We Do Hybrid Ablation, and Who Should We Do It On?
 The EP Perspective: Should We Do Hybrid Ablation, and Who Should We Do It On? L. Pison, MD PhD FESC AATS Surgical Treatment of Arrhythmias and Rhythm Disorders November 17-18, 2017 Miami Beach, FL, USA
The EP Perspective: Should We Do Hybrid Ablation, and Who Should We Do It On? L. Pison, MD PhD FESC AATS Surgical Treatment of Arrhythmias and Rhythm Disorders November 17-18, 2017 Miami Beach, FL, USA
Atrial Fibrillation Procedures Data Summary. Participant STS Period Ending 12/31/2016
 Period Ending 12/31/2016 Number of Cases Preoperative Predominant Atrial Arrhythmia Type Paroxysmal Atrial Fibrillation... - - Persistent Atrial Fibrillation... - - Longstanding Persistent Atrial Fibrillation...
Period Ending 12/31/2016 Number of Cases Preoperative Predominant Atrial Arrhythmia Type Paroxysmal Atrial Fibrillation... - - Persistent Atrial Fibrillation... - - Longstanding Persistent Atrial Fibrillation...
New Guidelines: Surgical Ablation of Atrial Fibrillation. Niv Ad, MD West Virginia University Washington Adventist Hospital
 New Guidelines: Surgical Ablation of Atrial Fibrillation Niv Ad, MD West Virginia University Washington Adventist Hospital Disclosures Medtronic Inc. : Speaker LivaNova : Speaker and Proctor Atricure Inc.
New Guidelines: Surgical Ablation of Atrial Fibrillation Niv Ad, MD West Virginia University Washington Adventist Hospital Disclosures Medtronic Inc. : Speaker LivaNova : Speaker and Proctor Atricure Inc.
What s new in my specialty?
 What s new in my specialty? Jon Melman, MD Heart Rhythm Specialists McKay-Dee Hospital some would say some would say my specialty 1 some would say my specialty First pacemaker 1958 some would say my specialty
What s new in my specialty? Jon Melman, MD Heart Rhythm Specialists McKay-Dee Hospital some would say some would say my specialty 1 some would say my specialty First pacemaker 1958 some would say my specialty
Surgical Ablation of Atrial Fibrillation. Gregory D. Rushing, MD. Assistant Professor, Division of Cardiac Surgery
 Surgical Ablation of Atrial Fibrillation Gregory D. Rushing, MD Assistant Professor, Division of Cardiac Surgery Midwestern Conference on Optimizing Electrophysiology Patient Care and Procedural Success
Surgical Ablation of Atrial Fibrillation Gregory D. Rushing, MD Assistant Professor, Division of Cardiac Surgery Midwestern Conference on Optimizing Electrophysiology Patient Care and Procedural Success
Minimally Invasive Stand Alone Cox-Maze Procedure For Patients With Non-Paroxysmal Atrial Fibrillation
 Minimally Invasive Stand Alone Cox-Maze Procedure For Patients With Non-Paroxysmal Atrial Fibrillation Niv Ad, MD Chief, Cardiac Surgery Inova Heart and Vascular Institute Disclosures Niv Ad: Medtronic
Minimally Invasive Stand Alone Cox-Maze Procedure For Patients With Non-Paroxysmal Atrial Fibrillation Niv Ad, MD Chief, Cardiac Surgery Inova Heart and Vascular Institute Disclosures Niv Ad: Medtronic
AF ABLATION Concepts and Techniques
 AF ABLATION Concepts and Techniques Antony F Chu, M.D. Director of Complex Ablation Arrhythmia Services Section Division of Cardiology at the Rhode Island and Miriam Hospital HIGHLIGHTS The main indications
AF ABLATION Concepts and Techniques Antony F Chu, M.D. Director of Complex Ablation Arrhythmia Services Section Division of Cardiology at the Rhode Island and Miriam Hospital HIGHLIGHTS The main indications
AF :RHYTHM CONTROL BY DR-MOHAMMED SALAH ASSISSTANT LECTURER CARDIOLOGY DEPARTMENT
 AF :RHYTHM CONTROL BY DR-MOHAMMED SALAH ASSISSTANT LECTURER CARDIOLOGY DEPARTMENT 5-2014 Atrial Fibrillation therapeutic Approach Rhythm Control Thromboembolism Prevention: Recommendations Direct-Current
AF :RHYTHM CONTROL BY DR-MOHAMMED SALAH ASSISSTANT LECTURER CARDIOLOGY DEPARTMENT 5-2014 Atrial Fibrillation therapeutic Approach Rhythm Control Thromboembolism Prevention: Recommendations Direct-Current
The Emerging Atrial Fibrillation Epidemic: Treat It, Leave It or Burn It. Chandra Kumbar MD FACC FHRS The Heart Group, Evansville IN
 The Emerging Atrial Fibrillation Epidemic: Treat It, Leave It or Burn It Chandra Kumbar MD FACC FHRS The Heart Group, Evansville IN Disclosures Consultant Advisory Board, Medtronic Atrial fibrillation
The Emerging Atrial Fibrillation Epidemic: Treat It, Leave It or Burn It Chandra Kumbar MD FACC FHRS The Heart Group, Evansville IN Disclosures Consultant Advisory Board, Medtronic Atrial fibrillation
Atrial fibrillation (AF) is associated with increased morbidity
 is associated with increased morbidity") Ablation of Atrial Fibrillation with Concomitant Surgery Edward G. Soltesz, MD, MPH, and A. Marc Gillinov, MD Atrial fibrillation (AF) is associated with increased morbidity and mortality in coronary artery
Ablation of Atrial Fibrillation with Concomitant Surgery Edward G. Soltesz, MD, MPH, and A. Marc Gillinov, MD Atrial fibrillation (AF) is associated with increased morbidity and mortality in coronary artery
Manuel Castella MD PhD Hospital Clínic, University of
 Manuel Castella MD PhD Hospital Clínic, University of Barcelona mcaste@clinic.ub.es @mcastellamd www.escardio.org/guidelines European Heart Journal - doi:10.1093/eurheartj/ehw210 Providing integrated care
Manuel Castella MD PhD Hospital Clínic, University of Barcelona mcaste@clinic.ub.es @mcastellamd www.escardio.org/guidelines European Heart Journal - doi:10.1093/eurheartj/ehw210 Providing integrated care
Combined catheter ablation and left atrial appendage closure as a. treatment of atrial fibrillation
 Combined catheter ablation and left atrial appendage closure as a hybrid procedure for the treatment of atrial fibrillation Giulio Molon, MD FACC, FESC, Fellow ANMCO Card Dept, S.Cuore hospital Negrar
Combined catheter ablation and left atrial appendage closure as a hybrid procedure for the treatment of atrial fibrillation Giulio Molon, MD FACC, FESC, Fellow ANMCO Card Dept, S.Cuore hospital Negrar
2018 CODING AND REIMBURSEMENT FOR. Cardiac Surgical Ablation and Left Atrial Appendage Management
 2018 CODING AND REIMBURSEMENT FOR Cardiac Surgical Ablation and Left Atrial Appendage Management Introduction This information is shared for educational purposes and current as of January 2018. Healthcare
2018 CODING AND REIMBURSEMENT FOR Cardiac Surgical Ablation and Left Atrial Appendage Management Introduction This information is shared for educational purposes and current as of January 2018. Healthcare
Is cardioversion old hat? What is new in interventional treatment of AF symptoms?
 Is cardioversion old hat? What is new in interventional treatment of AF symptoms? Joseph de Bono Consultant Electrophysiologist University Hospitals Birmingham Atrial Fibrillation (AF) Affects 2% of the
Is cardioversion old hat? What is new in interventional treatment of AF symptoms? Joseph de Bono Consultant Electrophysiologist University Hospitals Birmingham Atrial Fibrillation (AF) Affects 2% of the
Outcomes of AF Ablation
 2017 춘계심혈관통합학술대회 AF Summit: Atrial Fibrillation Apr.21(Fri) 14:40-16:10 Rm.300B 15:00-15:10 Outcomes of AF Ablation Gi-Byoung Nam MD Asan Medical Center, UUCM 2017 Annual Spring Scientific Conference of
2017 춘계심혈관통합학술대회 AF Summit: Atrial Fibrillation Apr.21(Fri) 14:40-16:10 Rm.300B 15:00-15:10 Outcomes of AF Ablation Gi-Byoung Nam MD Asan Medical Center, UUCM 2017 Annual Spring Scientific Conference of
What s New in the Guidelines for Surgical Ablation for Atrial Fibrillation?
 What s New in the Guidelines for Surgical Ablation for Atrial Fibrillation? Vinay Badhwar, MD Gordon F. Murray Professor and Chairman Department of Cardiovascular & Thoracic Surgery West Virginia University
What s New in the Guidelines for Surgical Ablation for Atrial Fibrillation? Vinay Badhwar, MD Gordon F. Murray Professor and Chairman Department of Cardiovascular & Thoracic Surgery West Virginia University
Recurrent Stroke under Anticoagulation in Mild MS & AF
 Recurrent Stroke under Anticoagulation in Mild MS & AF - Minimal maze operation and LAA excision or exclusion- Seung Hyun Lee, M.D, Ph.D Division of Thoracic and Cardiovascular surgery Severance cardiovascular
Recurrent Stroke under Anticoagulation in Mild MS & AF - Minimal maze operation and LAA excision or exclusion- Seung Hyun Lee, M.D, Ph.D Division of Thoracic and Cardiovascular surgery Severance cardiovascular
Ablation Should Not Be Used as Primary Therapy for Treatment of Patients with Atrial Fibrillation
 Ablation Should Not Be Used as Primary Therapy for Treatment of Patients with Atrial Fibrillation 25 October 2008 Update in Electrocardiography and Arrhythmias Zian H. Tseng, M.D., M.A.S. Assistant Professor
Ablation Should Not Be Used as Primary Therapy for Treatment of Patients with Atrial Fibrillation 25 October 2008 Update in Electrocardiography and Arrhythmias Zian H. Tseng, M.D., M.A.S. Assistant Professor
Debate-STAR AF 2 study. PVI is not enough
 Debate-STAR AF 2 study PVI is not enough Debate about STAR AF 2 trial STAR AF trial Substrate and Trigger Ablation for Reduction of Atrial Fibrillation EHJ 2010 STAR-AF 2 trial One Size Fits All? PVI is
Debate-STAR AF 2 study PVI is not enough Debate about STAR AF 2 trial STAR AF trial Substrate and Trigger Ablation for Reduction of Atrial Fibrillation EHJ 2010 STAR-AF 2 trial One Size Fits All? PVI is
Hybrid Surgical Ablation in South America: Lesson Learned. Joao R. Breda
 Hybrid Surgical Ablation in South America: Lesson Learned Joao R. Breda DISCLOSURES NONE 2 How to treat Atrial Fibrillation (AF) Understanding of pathophysiology mechanisms Ablation approach Choice of
Hybrid Surgical Ablation in South America: Lesson Learned Joao R. Breda DISCLOSURES NONE 2 How to treat Atrial Fibrillation (AF) Understanding of pathophysiology mechanisms Ablation approach Choice of
Trial design and selection criteria
 Background Cox-MAZE open chest, cardiac surgery was a very successful invasive procedure for treatment of AF 1, but highly invasive Since the landmark trial by Haissaguerre et al. 2, PV isolation by catheter
Background Cox-MAZE open chest, cardiac surgery was a very successful invasive procedure for treatment of AF 1, but highly invasive Since the landmark trial by Haissaguerre et al. 2, PV isolation by catheter
Atrial Fibrillation: Rate vs. Rhythm. Michael Curley, MD Cardiac Electrophysiology
 Atrial Fibrillation: Rate vs. Rhythm Michael Curley, MD Cardiac Electrophysiology I have no relevant financial disclosures pertaining to this topic. A Fib Epidemiology #1 Most common heart rhythm disturbance
Atrial Fibrillation: Rate vs. Rhythm Michael Curley, MD Cardiac Electrophysiology I have no relevant financial disclosures pertaining to this topic. A Fib Epidemiology #1 Most common heart rhythm disturbance
Ablation of persistent AF Is it different than paroxysmal?
 Ablation of persistent AF Is it different than paroxysmal? Steven J. Kalbfleisch, MD Medical Director Electrophysiology Laboratory Ohio State University Wexner Medical Center Ross Heart Hospital Columbus,
Ablation of persistent AF Is it different than paroxysmal? Steven J. Kalbfleisch, MD Medical Director Electrophysiology Laboratory Ohio State University Wexner Medical Center Ross Heart Hospital Columbus,
Hybrid Ablation of AF in the Operating Room: Is There a Need? MAZE III Procedure. Spectrum of Atrial Fibrillation
 Hybrid Ablation of AF in the Operating Room: Is There a Need? MAZE III Procedure Paul J. Wang, MD Amin Al-Ahmad, MD Gan Dunnington, MD Stanford University Cox J, et al. Ann Thorac Surg. 1993;55:578-580.
Hybrid Ablation of AF in the Operating Room: Is There a Need? MAZE III Procedure Paul J. Wang, MD Amin Al-Ahmad, MD Gan Dunnington, MD Stanford University Cox J, et al. Ann Thorac Surg. 1993;55:578-580.
Atrial fibrillation and advanced age
 Atrial fibrillation and advanced age Prof. Fiorenzo Gaita Director of the Cardiology School University of Turin, Italy Prevalence of AF in the general population Prevalence and age distribution in patients
Atrial fibrillation and advanced age Prof. Fiorenzo Gaita Director of the Cardiology School University of Turin, Italy Prevalence of AF in the general population Prevalence and age distribution in patients
Κατάλυση παροξυσμικής κολπικής μαρμαρυγής Ποια τεχνολογία και σε ποιους ασθενείς; Χάρης Κοσσυβάκης Καρδιολογικό Τμήμα Γ.Ν.Α. «Γ.
 Κατάλυση παροξυσμικής κολπικής μαρμαρυγής Ποια τεχνολογία και σε ποιους ασθενείς; Χάρης Κοσσυβάκης Καρδιολογικό Τμήμα Γ.Ν.Α. «Γ. ΓΕΝΝΗΜΑΤΑΣ» Rhythm control antiarrhythmic drugs vs catheter ablation Summary
Κατάλυση παροξυσμικής κολπικής μαρμαρυγής Ποια τεχνολογία και σε ποιους ασθενείς; Χάρης Κοσσυβάκης Καρδιολογικό Τμήμα Γ.Ν.Α. «Γ. ΓΕΝΝΗΜΑΤΑΣ» Rhythm control antiarrhythmic drugs vs catheter ablation Summary
The multi purse string maze procedure: A new surgical technique to perform the full maze procedure without atriotomies
 Ad Evolving Technology The multi purse string maze procedure: A new surgical technique to perform the full maze procedure without atriotomies Niv Ad, MD Objective: The maze procedure is the most effective
Ad Evolving Technology The multi purse string maze procedure: A new surgical technique to perform the full maze procedure without atriotomies Niv Ad, MD Objective: The maze procedure is the most effective
Controversies in Atrial Fibrillation and HF
 Controversies in Atrial Fibrillation and HF Dr.Yahya Al Hebaishi Cardiac electrophysiology division, PSCC, Riyadh Atrial Fibrillation: Rate or Rhythm? HF and AF: the twin epidemic of cardiovascular disease.
Controversies in Atrial Fibrillation and HF Dr.Yahya Al Hebaishi Cardiac electrophysiology division, PSCC, Riyadh Atrial Fibrillation: Rate or Rhythm? HF and AF: the twin epidemic of cardiovascular disease.
Long-Term Outcome and Risks of Catheter Ablation for Atrial Fibrillation
 Long-Term Outcome and Risks of Catheter Ablation for Atrial Fibrillation Carlo Pappone, MD, PhD, FACC EP Director, Villa Maria Hospital Group How many times AF can increase mortality DO MORTALITY REALLY
Long-Term Outcome and Risks of Catheter Ablation for Atrial Fibrillation Carlo Pappone, MD, PhD, FACC EP Director, Villa Maria Hospital Group How many times AF can increase mortality DO MORTALITY REALLY
부정맥 3 Debaste 2. 08:30~10:00: 4 회의장
 부정맥 3 Debaste 2. 08:30~10:00: 4 회의장 130420 Sinus Node Dysfunction vs. Atrial Fibrillation 45 years old man, persistent AF, planned for MVR, LA 69mm, EF 70%: Does he need additional maze surgery? CON Hui-Nam
부정맥 3 Debaste 2. 08:30~10:00: 4 회의장 130420 Sinus Node Dysfunction vs. Atrial Fibrillation 45 years old man, persistent AF, planned for MVR, LA 69mm, EF 70%: Does he need additional maze surgery? CON Hui-Nam
What is Minimally Invasive Surgical Ablation?
 What is Minimally Invasive Surgical Ablation? ( and who might be suitable for it?) HRC October 2011 Mr. Jonathan Hyde Consultant Cardiac Surgeon Royal Sussex County Hospital, Brighton Introduction Atrial
What is Minimally Invasive Surgical Ablation? ( and who might be suitable for it?) HRC October 2011 Mr. Jonathan Hyde Consultant Cardiac Surgeon Royal Sussex County Hospital, Brighton Introduction Atrial
FDA Executive Summary. Prepared for the October 26, 2011 meeting of the Circulatory System Devices Panel
 FDA Executive Summary Prepared for the October 26, 2011 meeting of the Circulatory System Devices Panel P100046 AtriCure Synergy Ablation System AtriCure, Inc. Introduction This is the FDA Executive Summary
FDA Executive Summary Prepared for the October 26, 2011 meeting of the Circulatory System Devices Panel P100046 AtriCure Synergy Ablation System AtriCure, Inc. Introduction This is the FDA Executive Summary
ATRIAL FIBRILLATION: REVISITING CONTROVERSIES IN AN ERA OF INNOVATION
 ATRIAL FIBRILLATION: REVISITING CONTROVERSIES IN AN ERA OF INNOVATION Frederick Schaller, DO, MACOI,FACP Adjunct Clinical Professor Touro University Nevada DISCLOSURES I have no financial relationships
ATRIAL FIBRILLATION: REVISITING CONTROVERSIES IN AN ERA OF INNOVATION Frederick Schaller, DO, MACOI,FACP Adjunct Clinical Professor Touro University Nevada DISCLOSURES I have no financial relationships
Concurrent AF Ablation with Mitral Valve Surgery
 Concurrent AF Ablation with Mitral Valve Surgery James L. Cox, MD Surgical Director, Center for Heart Rhythm Disorders Bluhm Cardiovascular Institute Professor of Surgery Feinberg School of Medicine Northwestern
Concurrent AF Ablation with Mitral Valve Surgery James L. Cox, MD Surgical Director, Center for Heart Rhythm Disorders Bluhm Cardiovascular Institute Professor of Surgery Feinberg School of Medicine Northwestern
Seek and Ye Shall Find: Surprising Findings When Using the ILR-LINQ
 Seek and Ye Shall Find: Surprising Findings When Using the ILR-LINQ Suneet Mittal, MD, FACC, FHRS Director, Electrophysiology Laboratory Valley Health System www.arrhythmia.org; @drsuneet October 31, 2015
Seek and Ye Shall Find: Surprising Findings When Using the ILR-LINQ Suneet Mittal, MD, FACC, FHRS Director, Electrophysiology Laboratory Valley Health System www.arrhythmia.org; @drsuneet October 31, 2015
2015 Atrial Fibrillation Therapy Meds, Shock, or Ablate? D. Scott Kirby MD, FACC Cardiac Electrophysiologist
 2015 Atrial Fibrillation Therapy Meds, Shock, or Ablate? D. Scott Kirby MD, FACC Cardiac Electrophysiologist Todays Objectives Atrial Fibrillation evaluation and treatment from an EP perspective Multimodal
2015 Atrial Fibrillation Therapy Meds, Shock, or Ablate? D. Scott Kirby MD, FACC Cardiac Electrophysiologist Todays Objectives Atrial Fibrillation evaluation and treatment from an EP perspective Multimodal
Atrial Fibrillation New Approaches, Techniques, and Technology
 New Cardiovascular Horizons 2015 May 28, 2015 New Orleans, Louisiana Atrial Fibrillation New Approaches, Techniques, and Technology State of the Art - - 2015 Richard Abben, M D Director, Cardiac Arrhythmia
New Cardiovascular Horizons 2015 May 28, 2015 New Orleans, Louisiana Atrial Fibrillation New Approaches, Techniques, and Technology State of the Art - - 2015 Richard Abben, M D Director, Cardiac Arrhythmia
Devices to Protect Against Stroke in Atrial Fibrillation
 Devices to Protect Against Stroke in Atrial Fibrillation Jonathan C. Hsu, MD, MAS Associate Clinical Professor Division of Cardiology, Section of Cardiac Electrophysiology June 2, 2018 Disclosures Honoraria
Devices to Protect Against Stroke in Atrial Fibrillation Jonathan C. Hsu, MD, MAS Associate Clinical Professor Division of Cardiology, Section of Cardiac Electrophysiology June 2, 2018 Disclosures Honoraria
Manuel Castellá Cardiovascular Surgery Hospital Clínic, Universidad de
 When not to exclude the LAA Manuel Castellá Cardiovascular Surgery Hospital Clínic, Universidad de Barcelona mcaste@clinic.ub.es @mcastellamd Normal hearts Patient in sinus rhythm Patient in AF (with
When not to exclude the LAA Manuel Castellá Cardiovascular Surgery Hospital Clínic, Universidad de Barcelona mcaste@clinic.ub.es @mcastellamd Normal hearts Patient in sinus rhythm Patient in AF (with
Page 1. Current Trends in the Management of Atrial Fibrillation: Left Atrial Appendage Occlusion. Atrial fibrillation: Scope of the problem
 Current Trends in the Management of Atrial Fibrillation: Left Atrial Appendage Occlusion Benjamin A. D Souza, MD, FACC, FHRS Assistant Professor of Clinical Medicine Penn Presbyterian Medical Center Cardiac
Current Trends in the Management of Atrial Fibrillation: Left Atrial Appendage Occlusion Benjamin A. D Souza, MD, FACC, FHRS Assistant Professor of Clinical Medicine Penn Presbyterian Medical Center Cardiac
Contemporary Strategies for Catheter Ablation of Atrial Fibrillation
 Contemporary Strategies for Catheter Ablation of Atrial Fibrillation Suneet Mittal, MD Director, Electrophysiology Medical Director, Snyder Center for Atrial Fibrillation The Arrhythmia Institute at The
Contemporary Strategies for Catheter Ablation of Atrial Fibrillation Suneet Mittal, MD Director, Electrophysiology Medical Director, Snyder Center for Atrial Fibrillation The Arrhythmia Institute at The
Should hybrid ablation be the standard of care instead of transcatheter ablation techniques?
 Should hybrid ablation be the standard of care instead of transcatheter ablation techniques? Christian Shults, MD Assistant Professor, Georgetown University School of Medicine Cardiac Surgeon, Medstar
Should hybrid ablation be the standard of care instead of transcatheter ablation techniques? Christian Shults, MD Assistant Professor, Georgetown University School of Medicine Cardiac Surgeon, Medstar
Atrial Fibrillation Ablation Thinktank
 Atrial Fibrillation Ablation Thinktank Mitchell J. Magee, M.D. STS National Database Taskforce CRSTI Dallas, TX FDA, Silver Spring, MD April 27, 2009 STS National Database Current Status Update Adult Cardiac
Atrial Fibrillation Ablation Thinktank Mitchell J. Magee, M.D. STS National Database Taskforce CRSTI Dallas, TX FDA, Silver Spring, MD April 27, 2009 STS National Database Current Status Update Adult Cardiac
Post-ablation Management: Drug therapy, Anticoagulation and long-term Monitoring
 Catheter Ablation of Atrial Fibrillation: State of the Art Post-ablation Management: Drug therapy, Anticoagulation and long-term Monitoring Dipen Shah Service de Cardiologie Hospital Cantonal de Genève
Catheter Ablation of Atrial Fibrillation: State of the Art Post-ablation Management: Drug therapy, Anticoagulation and long-term Monitoring Dipen Shah Service de Cardiologie Hospital Cantonal de Genève
Ablation for atrial fibrillation during mitral valve surgery: 1-year results through continuous subcutaneous monitoring
 Interactive CardioVascular and Thoracic Surgery 15 (2012) 37 41 doi:10.1093/icvts/ivs053 Advance Access publication 18 April 2012 ORIGINAL ARTICLE - ADULT CARDIAC Ablation for atrial fibrillation during
Interactive CardioVascular and Thoracic Surgery 15 (2012) 37 41 doi:10.1093/icvts/ivs053 Advance Access publication 18 April 2012 ORIGINAL ARTICLE - ADULT CARDIAC Ablation for atrial fibrillation during
Thromboembolism During Sinus Rhythm in Patients with a History of Atrial Fibrillation
 48 th Annual New York Cardiovascular Symposium Thromboembolism During Sinus Rhythm in Patients with a History of Atrial Fibrillation Is Left Atrial Appendage Dysfunction Sufficient to Generate Clots? December
48 th Annual New York Cardiovascular Symposium Thromboembolism During Sinus Rhythm in Patients with a History of Atrial Fibrillation Is Left Atrial Appendage Dysfunction Sufficient to Generate Clots? December
Long-Term ECG Monitoring Using an ILR. Evgeny Pokushalov, MD, PhD
 Long-Term ECG Monitoring Using an ILR Evgeny Pokushalov, MD, PhD Long- Term ECG Monitoring Using an ILR Evgeny Pokushalov, MD, PhD, FESC State Research Ins;tute of Circula;on Pathology, Novosibirsk, Russia
Long-Term ECG Monitoring Using an ILR Evgeny Pokushalov, MD, PhD Long- Term ECG Monitoring Using an ILR Evgeny Pokushalov, MD, PhD, FESC State Research Ins;tute of Circula;on Pathology, Novosibirsk, Russia
In patients with an enlarged left atrium does left atrial size reduction improve maze surgery success?
 doi:10.1510/icvts.2011.275511 Interactive CardioVascular and Thoracic Surgery 13 (2011) 635-641 www.icvts.org Best evidence topic - Arrhythmia In patients with an enlarged left atrium does left atrial
doi:10.1510/icvts.2011.275511 Interactive CardioVascular and Thoracic Surgery 13 (2011) 635-641 www.icvts.org Best evidence topic - Arrhythmia In patients with an enlarged left atrium does left atrial
A Cryo Anatomical Procedure to Everyone? Saverio Iacopino, FACC, FESC
 A Cryo Anatomical Procedure to Everyone? Saverio Iacopino, FACC, FESC AF Clinical/Referral Challenge Asymptomatic 40% 3 Rx Effective 30% Failed Rx Ablation Atrial fibrillation (AF) is the most common Candidate
A Cryo Anatomical Procedure to Everyone? Saverio Iacopino, FACC, FESC AF Clinical/Referral Challenge Asymptomatic 40% 3 Rx Effective 30% Failed Rx Ablation Atrial fibrillation (AF) is the most common Candidate
Incidence and Predictors of Pacemaker Placement After Surgical Ablation for Atrial Fibrillation
 Incidence and Predictors of Pacemaker Placement After Surgical Ablation for Atrial Fibrillation Berhane Worku, MD, Sang-Woo Pak, MD, Faisal Cheema, MD, Mark Russo, MD, Brian Housman, BA, Danielle Van Patten,
Incidence and Predictors of Pacemaker Placement After Surgical Ablation for Atrial Fibrillation Berhane Worku, MD, Sang-Woo Pak, MD, Faisal Cheema, MD, Mark Russo, MD, Brian Housman, BA, Danielle Van Patten,
Atrial Fibrillation: Catheter Ablation with New Technologies, Improving Quality of Life and Outcomes in Various Disease States
 Atrial Fibrillation: Catheter Ablation with New Technologies, Improving Quality of Life and Outcomes in Various Disease States Srinivas R. Dukkipati, MD Co-Director, Cardiac Arrhythmia Service The Mount
Atrial Fibrillation: Catheter Ablation with New Technologies, Improving Quality of Life and Outcomes in Various Disease States Srinivas R. Dukkipati, MD Co-Director, Cardiac Arrhythmia Service The Mount
Papel da imagem na estratificac ão de risco e na predic ão do risco tromboemboĺico
 Imagiologia na Fibrilhac ão Auricular Papel da imagem na estratificac ão de risco e na predic ão do risco tromboemboĺico Mª João Andrade Diagnosis and timely detection of atrial fibrillation Echo-machines
Imagiologia na Fibrilhac ão Auricular Papel da imagem na estratificac ão de risco e na predic ão do risco tromboemboĺico Mª João Andrade Diagnosis and timely detection of atrial fibrillation Echo-machines
The HISTORIC-AF TRIAL
 European Prospective Multicenter Study of Hybrid Thoracoscopic and Transcatheter Ablation of Persistent Atrial Fibrillation: The HISTORIC-AF TRIAL Claudio Muneretto 1, Gianluigi Bisleri 1, Gianluca Polvani
European Prospective Multicenter Study of Hybrid Thoracoscopic and Transcatheter Ablation of Persistent Atrial Fibrillation: The HISTORIC-AF TRIAL Claudio Muneretto 1, Gianluigi Bisleri 1, Gianluca Polvani
Intraoperative Radiofrequency Ablation for the Treatment of Atrial Fibrillation During Concomitant Cardiac Surgery
 Intraoperative Radiofrequency Ablation for the Treatment of Atrial Fibrillation During Concomitant Cardiac Surgery Michael E. Halkos, MD, Joseph M. Craver, MD, Vinod H. Thourani, MD, Faraz Kerendi, MD,
Intraoperative Radiofrequency Ablation for the Treatment of Atrial Fibrillation During Concomitant Cardiac Surgery Michael E. Halkos, MD, Joseph M. Craver, MD, Vinod H. Thourani, MD, Faraz Kerendi, MD,
AF and arrhythmia management. Dr Rhys Beynon Consultant Cardiologist and Electrophysiologist University Hospital of North Staffordshire
 AF and arrhythmia management Dr Rhys Beynon Consultant Cardiologist and Electrophysiologist University Hospital of North Staffordshire Atrial fibrillation Paroxysmal AF recurrent AF (>2 episodes) that
AF and arrhythmia management Dr Rhys Beynon Consultant Cardiologist and Electrophysiologist University Hospital of North Staffordshire Atrial fibrillation Paroxysmal AF recurrent AF (>2 episodes) that
AF Today: W. For the majority of patients with atrial. are the Options? Chris Case
 AF Today: W hat are the Options? Management strategies for patients with atrial fibrillation should depend on the individual patient. Treatment with medications seems adequate for most patients with atrial
AF Today: W hat are the Options? Management strategies for patients with atrial fibrillation should depend on the individual patient. Treatment with medications seems adequate for most patients with atrial
Basics of Atrial Fibrillation. By Mini Thannikal NP-BC Mount Sinai St Luke s Hospital New York, NY
 Basics of Atrial Fibrillation By Mini Thannikal NP-BC Mount Sinai St Luke s Hospital New York, NY Atrial Fibrillation(AF) is a supraventricular tachyarrhythmia characterized by uncoordinated atrial activation
Basics of Atrial Fibrillation By Mini Thannikal NP-BC Mount Sinai St Luke s Hospital New York, NY Atrial Fibrillation(AF) is a supraventricular tachyarrhythmia characterized by uncoordinated atrial activation
Catheter Ablation of Atrial Fibrillation Strategy and Outcome Predictors Shih-Ann Chen MD
 Catheter Ablation of Atrial Fibrillation Strategy and Outcome Predictors Shih-Ann Chen MD Taipei Veterans General Hospital, Taiwan Outline of AF Ablation 1. Strategy for Catheter Ablation of AF 2. Substrate
Catheter Ablation of Atrial Fibrillation Strategy and Outcome Predictors Shih-Ann Chen MD Taipei Veterans General Hospital, Taiwan Outline of AF Ablation 1. Strategy for Catheter Ablation of AF 2. Substrate
Indicatie voor ablatie bij voorkamerfibrillatie. Andrea Sarkozy Cardiologie Universitair Ziekenhuis Antwerpen
 Indicatie voor ablatie bij voorkamerfibrillatie Andrea Sarkozy Cardiologie Universitair Ziekenhuis Antwerpen Definition and Classification of AF - Practical aspects Classification of AF Paroxysmal, persistent,
Indicatie voor ablatie bij voorkamerfibrillatie Andrea Sarkozy Cardiologie Universitair Ziekenhuis Antwerpen Definition and Classification of AF - Practical aspects Classification of AF Paroxysmal, persistent,
Arrhythmias and Heart Failure Dr Chris Lang Consultant Cardiologist and Electrophysiologist Royal Infirmary of Edinburgh
 Arrhythmias and Heart Failure Dr Chris Lang Consultant Cardiologist and Electrophysiologist Royal Infirmary of Edinburgh Arrhythmias and Heart Failure Ventricular Supraventricular VT/VF Primary prevention
Arrhythmias and Heart Failure Dr Chris Lang Consultant Cardiologist and Electrophysiologist Royal Infirmary of Edinburgh Arrhythmias and Heart Failure Ventricular Supraventricular VT/VF Primary prevention
Rebuttal. Jerónimo Farré MD 2010
 Rebuttal 1.We do not know what are the types of AF in which ablation is worthless or most effective 2.Waiting implies to consider the ablation at an older age and when the duration of the history of AF
Rebuttal 1.We do not know what are the types of AF in which ablation is worthless or most effective 2.Waiting implies to consider the ablation at an older age and when the duration of the history of AF
Treating Atrial Fibrillation. Richard Schilling. St Bartholomew's Hospital, Queen Mary s University of London
 Treating Atrial Fibrillation Richard Schilling St Bartholomew's Hospital, Queen Mary s University of London AF burden Framingham Lifetime risk of developing AF = 25% Mortality: SMR =1.9 1.5 NHS audit 1%
Treating Atrial Fibrillation Richard Schilling St Bartholomew's Hospital, Queen Mary s University of London AF burden Framingham Lifetime risk of developing AF = 25% Mortality: SMR =1.9 1.5 NHS audit 1%
» A new drug s trial
 » A new drug s trial A placebo-controlled, double-blind, parallel arm Trial to assess the efficacy of dronedarone 400 mg bid for the prevention of cardiovascular Hospitalization or death from any cause
» A new drug s trial A placebo-controlled, double-blind, parallel arm Trial to assess the efficacy of dronedarone 400 mg bid for the prevention of cardiovascular Hospitalization or death from any cause
Catheter Ablation of Atrial Fibrillation Persistent Atrial Fibrillation Catheter Ablation : where are we?
 Catheter Ablation of Atrial Fibrillation Persistent Atrial Fibrillation Catheter Ablation : where are we? F. HIDDEN-LUCET francoise.hidden-lucet@aphp.fr Pitié-Salpétrière APHP FRANCE Disclosure Statement
Catheter Ablation of Atrial Fibrillation Persistent Atrial Fibrillation Catheter Ablation : where are we? F. HIDDEN-LUCET francoise.hidden-lucet@aphp.fr Pitié-Salpétrière APHP FRANCE Disclosure Statement
Atrial Fibrillation Ablation in Patients with Heart Failure
 Atrial Fibrillation Ablation in Patients with Heart Failure Eleftherios M. Kallergis, MD, PhD, FESC Cardiology Department, Heraklion University Hospital Since auricular fibrillation so often complicates
Atrial Fibrillation Ablation in Patients with Heart Failure Eleftherios M. Kallergis, MD, PhD, FESC Cardiology Department, Heraklion University Hospital Since auricular fibrillation so often complicates
30 Seconds is the Proper Endpoint for AF Ablation YES. Hugh Calkins MD. Professor of Medicine
 30 Seconds is the Proper Endpoint for AF Ablation YES Hugh Calkins MD Professor of Medicine Director of Electrophysiology Johns Hopkins Medical Institutions COI Disclosures Dr Calkins is a consultant to
30 Seconds is the Proper Endpoint for AF Ablation YES Hugh Calkins MD Professor of Medicine Director of Electrophysiology Johns Hopkins Medical Institutions COI Disclosures Dr Calkins is a consultant to
Isolator Synergy Ablation System THE ONLY FDA-APPROVED SURGICAL DEVICE TO TREAT ATRIAL FIBRILLATION
 Isolator Synergy Ablation System THE ONLY FDA-APPROVED SURGICAL DEVICE TO TREAT ATRIAL FIBRILLATION WWW.ATRICURE.COM Why the Isolator Synergy Ablation System by AtriCure? / UNIQUE LESION FORMATION A lesion
Isolator Synergy Ablation System THE ONLY FDA-APPROVED SURGICAL DEVICE TO TREAT ATRIAL FIBRILLATION WWW.ATRICURE.COM Why the Isolator Synergy Ablation System by AtriCure? / UNIQUE LESION FORMATION A lesion
Catheter ablation of atrial fibrillation: Indications and tools for improvement of the success rate of the method. Konstantinos P.
 Ioannina 2015 Catheter ablation of atrial fibrillation: Indications and tools for improvement of the success rate of the method Konstantinos P. Letsas, MD, FESC SECOND DEPARTMENT OF CARDIOLOGY LABORATORY
Ioannina 2015 Catheter ablation of atrial fibrillation: Indications and tools for improvement of the success rate of the method Konstantinos P. Letsas, MD, FESC SECOND DEPARTMENT OF CARDIOLOGY LABORATORY
ΚΑΤΑΛΥΣΗ ΚΟΛΠΙΚΗΣ ΜΑΡΜΑΡΥΓΗΣ. ΥΠΕΡ. Michalis Efremidis MD Second Department of Cardiology Evangelismos General Hospital
 ΚΑΤΑΛΥΣΗ ΚΟΛΠΙΚΗΣ ΜΑΡΜΑΡΥΓΗΣ. ΥΠΕΡ. Michalis Efremidis MD Second Department of Cardiology Evangelismos General Hospital Rate control versus Rhythm control for Atrial Fibrillation AFFIRM N Engl J Med 2002;347:1825-33
ΚΑΤΑΛΥΣΗ ΚΟΛΠΙΚΗΣ ΜΑΡΜΑΡΥΓΗΣ. ΥΠΕΡ. Michalis Efremidis MD Second Department of Cardiology Evangelismos General Hospital Rate control versus Rhythm control for Atrial Fibrillation AFFIRM N Engl J Med 2002;347:1825-33
Linear Ablation Should Not Be a Standard Part of Ablation in Persistent AF. Disclosures. LA Ablation vs. Segmental Ostial Ablation With PVI for PAF
 Linear Ablation Should Not Be a Standard Part of Ablation in Persistent AF The CA Heart Rhythm Symposium September 7, 2012 Gregory K. Feld, MD Professor of Medicine Director, Cardiac EP Program University
Linear Ablation Should Not Be a Standard Part of Ablation in Persistent AF The CA Heart Rhythm Symposium September 7, 2012 Gregory K. Feld, MD Professor of Medicine Director, Cardiac EP Program University
Cardiac Electrophysiology
 Cardiac Electrophysiology Tamara Langeberg, CNP Minneapolis Heart Institute Cardiac Electrophysiology February 27, 2018 Disclosures None 2 Objectives Rhythm identification Identify indications for cardiac
Cardiac Electrophysiology Tamara Langeberg, CNP Minneapolis Heart Institute Cardiac Electrophysiology February 27, 2018 Disclosures None 2 Objectives Rhythm identification Identify indications for cardiac
Seminars in Cardiovascular Medicine, 2016; 22:1 6 e-issn
 Original paper Procedural arrhythmia termination during beating-heart, stand-alone surgical ablation and long-term outcome in patients with persistent atrial fibrillation Vilius Janušauskas a,b*, Lina
Original paper Procedural arrhythmia termination during beating-heart, stand-alone surgical ablation and long-term outcome in patients with persistent atrial fibrillation Vilius Janušauskas a,b*, Lina
Predictors for permanent pacemaker implantation after concomitant surgical ablation for atrial fibrillation
 Predictors for permanent pacemaker implantation after concomitant surgical ablation for atrial fibrillation Simon Pecha, MD, a Timm Sch afer, MD, a Yalin Yildirim, MD, a Teymour Ahmadzade, MD, a Stephan
Predictors for permanent pacemaker implantation after concomitant surgical ablation for atrial fibrillation Simon Pecha, MD, a Timm Sch afer, MD, a Yalin Yildirim, MD, a Teymour Ahmadzade, MD, a Stephan
Left Atrial Appendage Closure Devices. Atrial Fibrillation 10/11/2017
 Left Atrial Appendage Closure Devices Emile Daoud, MD Chief, Cardiac Electrophysiology Wexner Medical Center, The Ohio State University Atrial Fibrillation 1 Adjusted Annual Stroke Risk Using CHA 2 DS
Left Atrial Appendage Closure Devices Emile Daoud, MD Chief, Cardiac Electrophysiology Wexner Medical Center, The Ohio State University Atrial Fibrillation 1 Adjusted Annual Stroke Risk Using CHA 2 DS
EP WIRE on Management Preexcitation syndromes
 EP WIRE on Management Preexcitation syndromes 1. Is your Institution: A University Hospital 70.7% 41 A Private Hospital 13.8% 8 Other Type of Hospital 15.5% 9 Institution name: 50 answered question 58
EP WIRE on Management Preexcitation syndromes 1. Is your Institution: A University Hospital 70.7% 41 A Private Hospital 13.8% 8 Other Type of Hospital 15.5% 9 Institution name: 50 answered question 58
Cardiac Imaging in abnormal rhythm Role of MDCT
 Cardiac Imaging in abnormal rhythm Role of MDCT Cardiac Imaging in abnormal rhythm Role of MDCT Scope of the problem CT in Atrial Fibrillation CT and pacing Ventricular arrhythmia Other applications 1
Cardiac Imaging in abnormal rhythm Role of MDCT Cardiac Imaging in abnormal rhythm Role of MDCT Scope of the problem CT in Atrial Fibrillation CT and pacing Ventricular arrhythmia Other applications 1
NATIONAL INSTITUTE FOR CLINICAL EXCELLENCE
 271 NATIONAL INSTITUTE FOR CLINICAL EXCELLENCE INTERVENTIONAL PROCEDURES PROGRAMME Interventional procedures overview of cryoablation for atrial fibrillation as an associated procedure with other cardiac
271 NATIONAL INSTITUTE FOR CLINICAL EXCELLENCE INTERVENTIONAL PROCEDURES PROGRAMME Interventional procedures overview of cryoablation for atrial fibrillation as an associated procedure with other cardiac
Cost and Prevalence of A fib. Atrial Fibrillation: Guideline Directed Treatment. Prevalence of A Fib. Risk Factors for A Fib. Risk Factors for A Fib
 Atrial Fibrillation: Guideline Directed Treatment Melissa Wendell, FNP-C, MSN Heart Failure - Lead Nurse Practitioner, Aspirus Wausau Hospital and Aspirus Cardiology Cost and Prevalence of A fib 33.5 million
Atrial Fibrillation: Guideline Directed Treatment Melissa Wendell, FNP-C, MSN Heart Failure - Lead Nurse Practitioner, Aspirus Wausau Hospital and Aspirus Cardiology Cost and Prevalence of A fib 33.5 million
Index. cardiology.theclinics.com. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A AADs. See Antiarrhythmic drugs (AADs) ACE inhibitors. See Angiotensin-converting enzyme (ACE) inhibitors ACP in transseptal approach to
Index Note: Page numbers of article titles are in boldface type. A AADs. See Antiarrhythmic drugs (AADs) ACE inhibitors. See Angiotensin-converting enzyme (ACE) inhibitors ACP in transseptal approach to
Mid-Term Results of Intraoperative Radiofrequency Ablation
 Kitakanto Med J 37 2003 ; 53 : 37 `41 Mid-Term Results of Intraoperative Radiofrequency Ablation A new approach to atrial fibrillation Susumu Ishikawa,1 Jai S. Raman,1 Brian F. Buxton1 and Yasuo Morishita
Kitakanto Med J 37 2003 ; 53 : 37 `41 Mid-Term Results of Intraoperative Radiofrequency Ablation A new approach to atrial fibrillation Susumu Ishikawa,1 Jai S. Raman,1 Brian F. Buxton1 and Yasuo Morishita
ABLATION OF CHRONIC AF
 ABLATION OF CHRONIC AF A PISAPIA ST JOSEPH HOSPITAL MARSEILLE MEET 2008 Atrial Fibrillation The most common significant heart rhythm disturbance Incidence increases with age and the development of structural
ABLATION OF CHRONIC AF A PISAPIA ST JOSEPH HOSPITAL MARSEILLE MEET 2008 Atrial Fibrillation The most common significant heart rhythm disturbance Incidence increases with age and the development of structural
Options for my no option Patients Treating Heart Conditions Via a Tiny Catheter
 Options for my no option Patients Treating Heart Conditions Via a Tiny Catheter Nirat Beohar, MD Associate Professor of Medicine Director Cardiac Catheterization Laboratory, Medical Director Structural
Options for my no option Patients Treating Heart Conditions Via a Tiny Catheter Nirat Beohar, MD Associate Professor of Medicine Director Cardiac Catheterization Laboratory, Medical Director Structural
NATIONAL INSTITUTE FOR CLINICAL EXCELLENCE
 266 NATIONAL INSTITUTE FOR CLINICAL EXCELLENCE INTERVENTIONAL PROCEDURES PROGRAMME Interventional procedures overview of microwave ablation for atrial fibrillation as an associated procedure with other
266 NATIONAL INSTITUTE FOR CLINICAL EXCELLENCE INTERVENTIONAL PROCEDURES PROGRAMME Interventional procedures overview of microwave ablation for atrial fibrillation as an associated procedure with other
Percutaneous Epicardial LAA Closure: When Does it Make Sense?
 Percutaneous Epicardial LAA Closure: When Does it Make Sense? Petr Neuzil, MD,PhD, FESC Professor of Medicine Cardiology department Na Homolce Hospital, Prague, Czechia petr.neuzil@gmail.com Disclosures
Percutaneous Epicardial LAA Closure: When Does it Make Sense? Petr Neuzil, MD,PhD, FESC Professor of Medicine Cardiology department Na Homolce Hospital, Prague, Czechia petr.neuzil@gmail.com Disclosures
Atrial Fibrillation 2009
 Atrial Fibrillation 2009 Michael Glikson, MD Director of Pacing & Electrophysiology Leviev Heart Center Sheba medical Center Sheba Medical Center Tel Hashomer The Leviev Heart Center Rhythm vs rate control
Atrial Fibrillation 2009 Michael Glikson, MD Director of Pacing & Electrophysiology Leviev Heart Center Sheba medical Center Sheba Medical Center Tel Hashomer The Leviev Heart Center Rhythm vs rate control
Device detected AF and atrial high rate episodes
 Device detected AF and atrial high rate episodes Professor Paulus Kirchhof University of Birmingham Institute of Cardiovascular Sciences SWBH and UHB NHS trusts, Birmingham, UK Department of Cardiovascular
Device detected AF and atrial high rate episodes Professor Paulus Kirchhof University of Birmingham Institute of Cardiovascular Sciences SWBH and UHB NHS trusts, Birmingham, UK Department of Cardiovascular
Postoperative Management of Patients Following Surgical Ablation
 Postoperative Management of Patients Following Surgical Ablation Harold G. Roberts, Jr. Department of Cardiovascular and Thoracic Surgery West Virginia University Morgantown, WV None Disclosures Postop
Postoperative Management of Patients Following Surgical Ablation Harold G. Roberts, Jr. Department of Cardiovascular and Thoracic Surgery West Virginia University Morgantown, WV None Disclosures Postop