Cardiac Critical Care Lance Cohen, MD MBBCh FCCP
|
|
|
- Easter Small
- 5 years ago
- Views:
Transcription
1 Cardiac Critical Care 2011 Lance Cohen, MD MBBCh FCCP
2 Open Heart Surgery Program Lance Cohen, MD MBBCh FCCP Medical Director - HSU
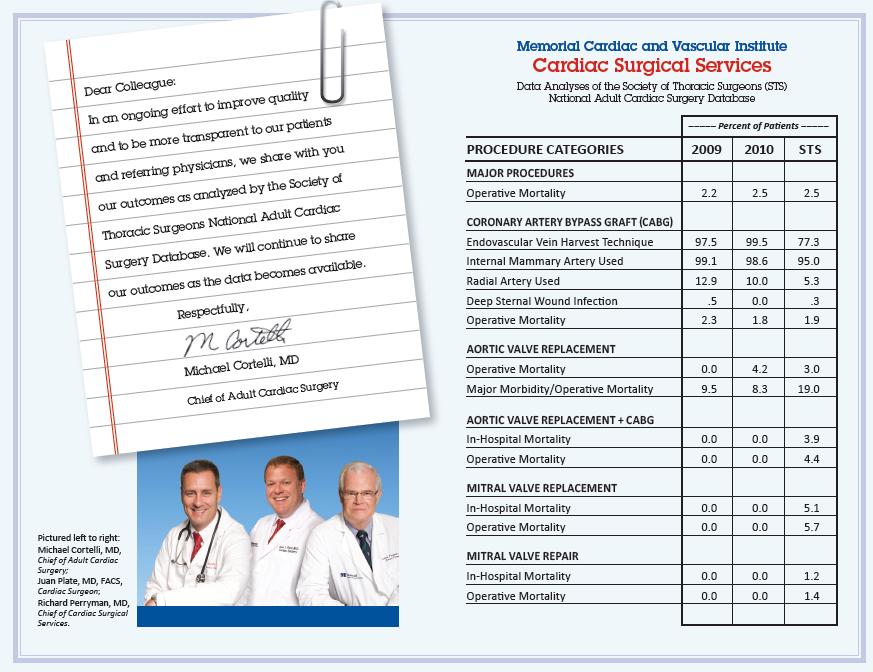
3 Open Heart Surgery Program Team Cardiac Surgeons Richard Perryman, MD Michael Cortelli, MD Juan Plate, MD
4 Open Heart Surgery Program Team Intensivists PA s NP s HSU nurses 6 North Nurses and team Dieticians PT Case Manager OR Team Anesthesiologists, Nurses, PA s Data team Pharmacy
 CABG Adult Congenital Mini")
5 Open Heart Surgery Program Services Aorta surgery Endovascular and open procedures. Cardiac Surgery : Valve (including minimally invasive) CABG Adult Congenital Mini Maze
6 Open Heart Surgery Program Services Team approach Daily team rounds / multidisciplinary Dedicated HSU Intensivist 3 star center top 13% in nation

7 Society Of Thoracic Surgeons (STS)
8 STS Founded in 1989, the Adult Cardiac Surgery Database is the largest cardiothoracic surgery outcomes and quality improvement program in the world. This database component contains more than 4.1 million surgical records, representing approximately 90 percent of all adult cardiac surgery centers throughout the U.S. More than 1,000 surgical groups, representing more than 3,000 surgeons, add new patient data four times each year.
9 STS Measures of CABG surgical quality, in four quality domains 1. Patient survival: Risk-adjusted 30- day operative mortality. 2. Optimal surgical technique: Use of at least one internal mammary artery graft.
10 STS 3. Absence of complications: Risk adjusted morbidity. Patients must avoid all 5: a. Kidney failure b. Deep sternal wound infection c. Re-operation for any cause d. Stroke e. Prolonged breathing support
11 STS 4. Recommended medications: Patient must receive all 4: a. Preoperative beta-blocker b. Discharge aspirin c. Discharge beta-blocker d. Discharge antilipid therapy
12 STS Other data looked at: 1. LOS 2. Intraop and Postop use of blood products 3. Cardiac rehab referal 4. Smoking cessation counceling
13 STS Other data looked at: day re-admission 2. Glucose control


14 HSU CABG Data 2010
15 HSU CABG DATA Mortality Rates 2.50% 2.30% 2.00% 1.50% 1.90% STS Benchmark 1.80% 1.00% 0.50% 0.00%
16 HSU CABG DATA Returns to OR 5.00% 4.50% 4.00% 4.60% STS Benchmark 3.50% 3.00% 2.50% 2.00% 1.50% 1.40% 1.00% 0.50% 0.00% %
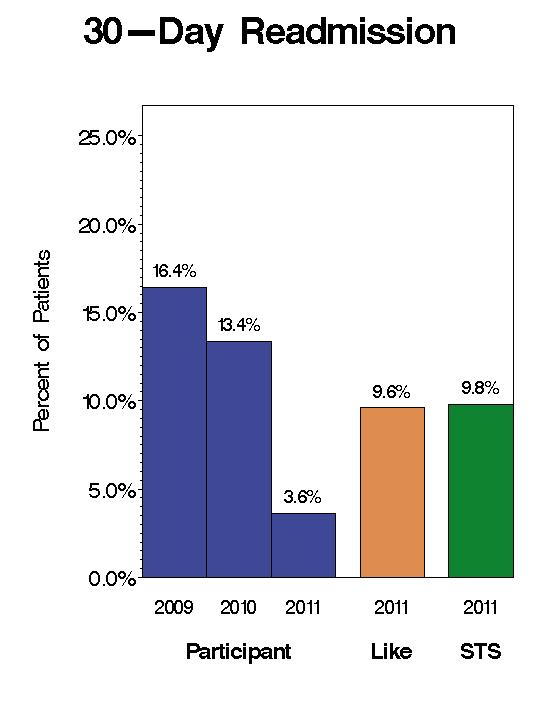
17 HSU CABG DATA Re-Admissions 18.00% 16.00% 15.70% 14.00% 12.00% 13% 10.00% 8.00% STS Benchmark 9.60% 6.00% 4.00% 2.00% 0.00%

18 30 Day Readmission Rate Discharge education lectures Discharge process by cardiac surgery team Follow up visit within 1 week of discharge by CTS team Phone call to patients by Medical Director and nursing staff within 72 hrs.
19 CAB
20 HSU CABG DATA Deep Sternal Wound Infections 2.00% 1.80% 1.80% 1.60% 1.40% 1.20% 1.00% 0.80% 0.60% 0.40% 0.20% STS Benchmark 0.40% 0.45% 0.00%
21 HSU CABG DATA Post OP CVA 2.50% 2.30% 2.00% 1.50% 1.00% 1.20% STS Benchmark 1.40% 0.50% 0.00%
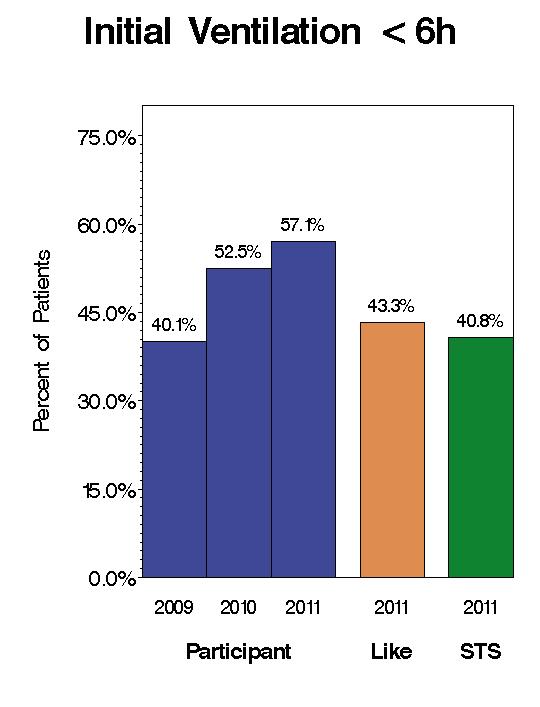
22 HSU CABG DATA Prolonged Intubation 14.00% 12.00% 10.00% 8.00% 12.00% 10.80% STS Benchmark 8.60% 6.00% 4.00% 2.00% 0.00%
23 HSU CABG DATA Acute Renal Failure 4.50% 4.00% 3.50% 3.00% 2.50% 2.00% 1.50% 4.10% 3.60% STS Benchmark 3.20% 1.00% 0.50% 0.00%
24 HSU CABG DATA 16.00% 14.00% 12.00% 10.00% 8.00% 6.00% 4.00% STS Benchmark % 0.00% Mortality Rates Returns to OR Re- Admissions Deep Sternal Wound Infections Post OP CVA Prolonged Intubation Acute Renal Failure
25 hours Reduction in LOS Length of Stay in HSU

26 STS Composite Quality Ratings Participant Rating * = Participant performance is significantly lower than the STS mean based on 99% Bayesian probability * * = Participant performance is not significantly different than the STS mean based on 99% Bayesian probability * * * = Participant performance is significantly higher than the STS mean based on 99% Bayesian probability
27 NQF Measures
28 NQF Measures
29 NQF Measures
30 NQF Measures
31 NQF Measures
32 NQF Measures
33 NQF Measures
34 NQF Measures
35 NQF Measures
36 NQF Measures
37 NQF Measures
38 NQF Measures
39 CAB
40 CAB
41
42
43
44
45 Therapeutic Hypothermia
46 Objectives: Scope of the Problem History, Current Evidence and AHA Recommendations Physiology of Cardiac Arrest Complications of Return of Spontaneous Circulation (ROSC) Physiology of Hypothermia Complications of Hypothermia Practical Aspects of Cooling
47 Scope of Problem Sudden cardiac arrest (SCA) is a leading cause of death in the US Approximately 330,000 deaths annually in ED and out of hospital from SCA 80% or more of initially comatose survivors will then die or suffer debilitating neurologic outcomes AHA 2005

48 1961 Research had not been favorable for temperatures C Mechanics not well controlled
49 History continued: 1980 s Cardiac Arrest with Dogs 1990 s Question? - Can we safely cool patients? - What is the best method? - We are still discovering the answer!

50 Current Evidence
51 So what do we mean by Good Outcomes? Glasgow-Pittsburgh Cerebral Performance Categories (CPC) 5 Levels Good Moderate Severe Coma, Vegetative State Death The Brain Resuscitation Clinical Trial II Study Group, Control Clin Trials 1991 Aug; 12 (4):
52 CPC Level 1 Conscious Alert Good Cerebral Performance Able to work and lead a normal life May have minor psychological or neurological deficits (mild dysphasia, nonincapacitating hemiparesis or minor cranial nerve abnormalities
53 CPC Level 2 Moderate Cerebral Disability Conscious Sufficient cerebral function for part-time work in sheltered environment or independent activities of daily life (dressing, traveling by public transportation and preparing food) May have hemiplegia, seizures, ataxia, dysarthria, dysphasia, or permanent memory or mental changes.
54 CPC Level 3 Conscious Severe Cerebral Disability Dependent on others for daily support At least limited cognition Includes a wide range of cerebral abnormalities from ambulatory with severe memory disturbance or dementia precluding independent existence to paralytic and able to communicate only with eyes, as in the locked in syndrome.
55 CPC Level 4 and 5 Level 4: Coma, Vegetative State Not conscious Unaware of surroundings, no cognition No verbal or psychological interactions with environment Level 5: Death Certified brain dead or dead by traditional criteria
56 Dr. Bernard s Study 77 patients - 43 hypothermia - 34 normothermia Results - 49% of hypothermia good outcome compared to 26% of normothermia (p=0.046) Bernard SA, et al. "Treatment of comatose survivors of out-of-hospital cardiac arrest with induced hypothermia." NEJM 2002; 346 (8):
57 European Study Multi -Center Trial 275 patients Hypothermia Normothermia Results - 55% Hypothermia group favorable outcome - 39% Normothermia group favorable outcome (p=0.009) The Hypothermia After Cardiac Arrest Study Group. "Mild therapeutic hypothermia to improve the neurologic outcome after cardiac arrest." NEJM 2002; 346 (8):
58 Bernard et al. Resuscitation 2003: 22 post cardiac arrest, comatose adults 30ml/kg LR at 4 C infused over 30 min via peripheral IV then temp maintained at 33 C Median temp decreased 1.6 C after bolus (P=<0.001) Median MAP increased 10 mmhg (P=0.012) No adverse outcomes Bernard SA, et al. Induced hypothermia using large volume, ice-cold intravenous fluid in comatose survivors of out-of-hospital cardiac arrest: a priliminary report. Resuscitation 2003: 56: 9-13
59 Oddo et al. Critical Care Medicine 2006: Implementation Study 109 comatose out of hospital arrests Retrospective Determined feasibility of Therapeutic Hypothermia (TH) to 33 C in "real life" clinical practice VF as initial rhythm Good outcomes: TH 56%, standard care 26% (P=0.004) TH safely applied to patients with initial rhythm of PEA and asystole. Outcomes were poor, though the subset was small (n=23) (P=NS) Oddo M, et al. from evidence to clinical practice: Effective implementation of therapeutic hypothermia to improve patient outcome after cardiac arrest. Critical Care medicine 2006; 34 (7):
60 Wolfrum et al. Critical Care Medicine 2008: Single center observational study with historical controls 33 comatose v-fib arrest patients with STEMI Initiated hypothermia with cold saline infusion and cold packs prior to PCI Showed that initiating hypothermia before PCI was feasible, safe Trend toward lower mortality (25% vs 35%, p=.71) and more CPC 1 or 2 (69% vs 47% p=.30)compared with historical controls Wolfrum S, et al: Mild therapeutic hypothermia in patients after out-of- hospital cardiac arrest due to acute ST-segment elevation myocardial infarction undergoing immediate percutaneous coronary intervention. Crit Care Med 2008; 36:
61 What Does This Mean? NNT: 4-6 NNT= statistical calculation of number of patients needed to treat to prevent one additional bad outcome, based on RCT s VF and pulseless VT patients may have better response to HACA, though PEA and asystole patients have not been adequately studied

62 HACA Recommendations American Heart Association 2005 ILCOR 2002
63 HACA Recommendations: 2005 AHA and 2002 ILCOR Unconscious adult patients with return of spontaneous circulation (ROSC) after out of hospital cardiac arrest should be cooled to C for hours when the initial rhythm is VF Such cooling may be beneficial for other rhythms or in-hospital cardiac arrest Hazinski MF, et al. Postresuscitation support. Circulation 2005: 112 (24): Nolan JP, et al. Therapeutic hypothermia after cardiac arrest: an advisory statement by the Advanced Life Support Task Force of the International Liaison Committee on Reusucitation. Circulation 2003; 108 (1):
64 Improving Postresuscitation Outcomes-Initial Goals 1. Optimize cardiopulmonary function and systemic perfusion especially to the brain 2. Transport victim to ED 3. Identify precipitating causes and institute measures to prevent recurrence 4. Institute measures that may improve long term neurologically intact survival AHA 2005
65 The Verdict Please? Induce Hypothermia
66 Life cycle of cardiac arrest ATP breakdown/anaerobic glycolysis Failure of energy dependent pumps and acidosis Excess calcium in cell oxygen free radical production and lipolysis Excess K+ and Na++ in cell Cerebral hypo-perfusion even with a good systemic blood pressure (for 24 hours or longer)
67 How to fix it? Decrease cerebral metabolism!!! Cool em!
68 Complications of Return of Spontaneous Circulation (ROSC): 1. Reperfusion Injury a. Increased oxygen free radical production with the presence of O2 contributes to apoptosis
69 Complications of ROSC 2. Initiates a Cascade of events a. Increased intracellular Ca++ continues. This contributes to an increase in glutamate increased intracellular Ca++ and the circle continues! 3. Inflammatory response a. Causes high levels of cytokines (can be elevated for up to 5 days post arrest). 4. Free radical production a. Increases after cardiac arrest and stays elevated for days.
70 Complications of ROSC 5. Coagulation cascade is activated a. This is true any time there is cell injury! 6. Ischemia/reperfusion injury cerebral edema a. Increased permeability of the blood brain barrier b. Increased permeability of the vasculature c. Increased permeability of the cell membranes 7. Hypoxia and reperfusion start all of these biochemical events but they can persist for hours to days
71 How do you prevent it? Cool em down Induce Hypothermia
72 Benefits of Therapeutic Induced Hypothermia Even if you start hours after ROSC (Return of Spontaneous Circulation) Decrease cerebral metabolism therefore decrease need for oxygen Hypothermia reduces the cellular levels of glutamate
73 Benefits of Therapeutic Induced Hypothermia (cont.) Reduces intracellular acidosis Decreases the inflammatory response and cytokinase release Protects the blood brain lipomembranes!
74 Okay - So we will cool them! Just give me the facts!
75 Witnessed Arrest Who got cooled in the RCT studies? Ventricular Tachycardia/Ventricular Fibrillation rhythm only Only 5-15 minutes from collapse to ACLS No more than 60 minutes from collapse to ROSC
76 WHO ARE WE COOLING? Patient is comatose after cardiac arrest Return of Spontaneous Circulation (ROSC) within 60 minutes of cardiac arrest Time of initiation of hypothermia less than 6 hours post cardiac arrest
77 Who Doesn t Get Cooled Temperature is already below 30 C Comatose before cardiac arrest resulting from drugs that depress the CNS Pregnancy Preexisting terminal illness Preexisting coagulopathy Recent major surgery within last 14 days Patients with major head trauma

78 How Can You Cool? Many methods Ice bags Fans Intravenous Cooling Mechanical Cooling Endovascular Cooling
79 Ice bags Pros Cons Inexpensive, widely Messy, difficult to available control temp Fans Inexpensive, widely Difficult to available control temp, limited ability to decrease temp quickly Intravenous Fluids Inexpensive, widely available Need to determine way to keep fluids cold
80 Mechanical Pros Fair control of patient temp, easy to use. Cons Variety of systems/costs, not easily transportable Endovascular Reliable control of patient temp Fast No risk of skin lesions Expensive, large invasive line concern for increase sepsis risk

81 Combination of methods 1. Intravenous cooling 2. Mechanical or endovascular cooling 3. Ice bags during induction
82 Keeping Track of Temperature Monitor every 15 minutes during induction until stabilized at goal temperature C Avoid temperature <30 C

83 MEDIVANCE ARCTIC SUN
84 Methods to Monitor Temperature Bladder Rectal PA Catheter Esophageal Tympanic Axilla Which is best?
85 Success with Induced Hypothermia Requires: Awareness of physiological effects hypothermia and pathophysiological mechanisms Understanding these concepts can prevent over-treatment, and insufficient treatment which could eliminate the protective, beneficial effects of hypothermia!
86 Physiological changes due to Mild to Moderate Hypothermia Temperature specific Influenced by age and co-morbidities - Especially cardiovascular disease
87 Physiological attempts to increase temperature Temperature C In awake patients: - Shivering - Peripheral vasoconstriction - Increased muscle activity - Increased oxygen consumption, increased metabolism Temperature <30 C Hibernation begins: - Shivering ceases - Decreased metabolic rate
88 Temp C Metabolic changes Oxygen consumption Carbon dioxide production Metabolism Fat metabolism Temp C Temp < 35 C Insulin sensitivity Insulin secretion Endocrine changes Levels of epinephrine and norepinephrine Levels of cortisol
89 Cardiovascular effects <36 >35 C Tachycardia <35 C Bradycardia <34 C Slight in blood pressure <33 C EKG changes: increased PR interval, widening of QRS, increased QT interval <32 C Mild arrhythmias in some patients <28 C High risk of tachyarrhythmias, <35 C beginning with atrial fibrillation CVP, Cardiac output
90 Renal changes Temp < 35 C Diuresis Tubular dysfunction Electrolyte loss Electrolyte disorders Hematological changes Platelet count < 35 C WBC, impaired leukocyte function < 33 C
91 GI Changes < 35 C Impaired bowel function Impaired intestinal motility Potential for ileus Mild pancreatitis (occurs frequently!) Liver enzymes Immune suppression < 35 C Impaired neutraphil and macrophage function Increased risk of infections (Pneumonia and wound infections)

92 Neurological Changes Consciousness Lethargy Coma Pharmacokinetics < 35 C Altered Clearance of various medications especially: Paralytics, Propofol, Fentanyl, Phenytoin, Verapamil! No effect on Gentamycin clearance
93 Lab Changes Amylase ( ) Platelet count ( k) Hyperglycemia K+, Mg++, Phos, Ca++ Mild Metabolic Acidosis Lactate Liver enzymes (SGOT, SGPT)
94 Pathophysiology of Hypothermia High risk of - Coagulopathy, increased bleeding time increased PTT, thrombocytopenia, - Impaired coagulation cascade - Electrolyte disorders - Hypovolemia - Rise in serum amylase - Changes in drug effects and drug metabolism - Insulin resistance
95 Pathophysiology of Hypothermia Low Risk - Manifest bleeding - Severe coagulation disorders - Airway infections - Wound infections - Myocardial ischemia
96 Pathophysiology of Hypothermia Rare risk - Manifest pancreatitis - Intracerebral bleeding

97 Phases of Induced Hypothermia
98 Three Phases of Therapeutic Induced Hypothermia Induction Get em cold Maintenance Keep em cold Re-warming Phase Warm em up slow
99 Induction Goal is to decrease temperature to 33 C Quickly Intravenous Cold Saline (kept at 1-4 C) Infuse rapidly ml/kg over a maximum of 30 minutes Mechanical cooling device or use of the endovascular cooling device and ice packs on! Quickly!!
100 Induction Avoid temperature overshoot Cold fluids through a peripheral or femoral line Expose and dampen the skin Cool the room to 62 F. Begin paralytics starting with bolus if indicated Ice Packs to axilla, groin and sides of neck if needed
101 Maintenance Phase Keep them cool between C for 24 hours! Only Minor fluctuations in temp C Don t overshoot the range Use the mechanical or endovasular cooling device Watch for side effects and complications of cooling
102 Maintenance Phase Fluid balance Electrolyte balance Glucose control Signs of infection Skin Care - Never Events! Central line infection Vent settings - frequent ABG s-maintain normocarbia Control shivering - using low dose continuous or prn paralytics (pancuronium or vercuronium) Control Seizures Watch for signs of bleeding

103 Re-warming Phase Goal to re-warm no more than C per hour Take Minimum of 12 hours to re-warm Be careful not to warm to fast. Slow re-warm

104 Re-warming Phase Discontinue any paralytics Watch for rises in electrolytes - especially K+ and Mg++ Watch for fluid shifts Maintain temp C
105 Post re-warming assessment Remember hypothermic pharmacokinetic effects Complete Neurological assessment at 96 hours post cardiac arrest.
106 DO HACA recommendations Initiated ASAP, at least by 6 hours after ROSC- TIME IS BRAIN!!! Initiate rapid cooling with a rapid infusion of cold (4 C) IV fluid, then use cooling vest, leg wraps, endovacular device, or ice packs to achieve/maintain C for 24 hours Avoid hypovolemia - cold fluids at induction phase
107 HACA recommendations (cont) Closely monitor Mg++ and K+ at least q 4 hours. Expect HYPOkalemia with cooling and HYPERkalemia with rewarming Strict Glucose control - Use IV insulin protocol Avoid infections - Early Goal Directed Therapy for SEPSIS
108 HACA Recommendations (cont) Appropriate sedation and analgesia and paralytics. SHIVERING MUST BE PREVENTED!! Paralytic protocol. Goal is no shivering, TOF is secondary and may be unreliable during hypothermia. Adjust ventilator settings to pco2 of 40 Consider enteral feeding
109 HACA Recommendations (cont.) Skin Care - Never Events. Gently rotate patient ASAP and skin checks q 4 hours Basic High Quality ICU Care - Hand washing, turning q2h, aseptic line care, etc. Use of β-blockers seems prudent for cardioprotection if there are no contraindications - Bradycardia
110 HACA Recommendations Maintain a normal or slightly elevated MAP Decrease ICP if elevated Treat witnessed seizures
111 Don t Don t overshoot the goal temperature Stay C Don t overtreat Bradycardia Mild Acidosis Don t use paralytics once rewarm is complete
112 Don t Don t re-warm to quickly
113 "A healthy brain and a functional patient are the primary goals of cardiopulmonary-cerebral resuscitation." AHA 2005
 shows that hypothermia can improve outcomes after cardiac arrest with VT/VF - Hypothermia should definitely be applied for these patients (Class IIA recommendation) Strong")
114 Dive In! Evidence (level 1) shows that hypothermia can improve outcomes after cardiac arrest with VT/VF - Hypothermia should definitely be applied for these patients (Class IIA recommendation) Strong evidence shows that hypothermia can improve outcomes with other presenting arrhythmias (Class IIB Recommendation) - Hypothermia should probably be applied for these patients AHA2005

115 Take the plunge! Follow the studies Use Cold Fluid for induction phase

116 MEMORIAL EXPERIENCE He just collapsed, says Tobin s wife, Angeline. I didn t know what to do. For about three weeks Tobin was on life support and was critically ill, They included the family in everything, Angeline says. At Memorial, they not only took care of my husband, they took care of all of us.

117 Thank you
118 Questions?
Post-Cardiac Arrest Syndrome. MICU Lecture Series
 Post-Cardiac Arrest Syndrome MICU Lecture Series Case 58 y/o female collapses at home, family attempts CPR, EMS arrives and notes VF, defibrillation x 3 with return of spontaneous circulation, brought
Post-Cardiac Arrest Syndrome MICU Lecture Series Case 58 y/o female collapses at home, family attempts CPR, EMS arrives and notes VF, defibrillation x 3 with return of spontaneous circulation, brought
INDUCED HYPOTHERMIA. F. Ben Housel, M.D.
 INDUCED HYPOTHERMIA F. Ben Housel, M.D. Historical Use of Induced Hypothermia 1950 s - Moderate hypothermia (30-32º C) in open heart surgery to protect brain against global ischemia 1960-1980 s - Use of
INDUCED HYPOTHERMIA F. Ben Housel, M.D. Historical Use of Induced Hypothermia 1950 s - Moderate hypothermia (30-32º C) in open heart surgery to protect brain against global ischemia 1960-1980 s - Use of
In-hospital Care of the Post-Cardiac Arrest Patient. David A. Pearson, MD, FACEP, FAAEM Associate Program Director Department of Emergency Medicine
 In-hospital Care of the Post-Cardiac Arrest Patient David A. Pearson, MD, FACEP, FAAEM Associate Program Director Department of Emergency Medicine Disclosures I have no financial interest, arrangement,
In-hospital Care of the Post-Cardiac Arrest Patient David A. Pearson, MD, FACEP, FAAEM Associate Program Director Department of Emergency Medicine Disclosures I have no financial interest, arrangement,
INDUCED HYPOTHERMIA A Hot Topic. R. Darrell Nelson, MD, FACEP Emergency Medicine Wake Forest University Health Sciences
 INDUCED HYPOTHERMIA A Hot Topic R. Darrell Nelson, MD, FACEP Emergency Medicine Wake Forest University Health Sciences Conflicts of Interest Sadly, we have no financial or industrial conflicts of interest
INDUCED HYPOTHERMIA A Hot Topic R. Darrell Nelson, MD, FACEP Emergency Medicine Wake Forest University Health Sciences Conflicts of Interest Sadly, we have no financial or industrial conflicts of interest
Case Presentation. Cooling. Case Presentation. New Developments in Cardiopulmonary Arrest: Therapeutic Hypothermia in Resuscitation
 New Developments in Cardiopulmonary Arrest: Therapeutic Hypothermia in Resuscitation Michael Sayre, MD Emergency Medicine and LeRoy Essig, MD Pulmonary/Critical Care Medicine Case Presentation 3:40 (+
New Developments in Cardiopulmonary Arrest: Therapeutic Hypothermia in Resuscitation Michael Sayre, MD Emergency Medicine and LeRoy Essig, MD Pulmonary/Critical Care Medicine Case Presentation 3:40 (+
Post-Resuscitation Care: Optimizing & Improving Outcomes after Cardiac Arrest. Objectives: U.S. stats
 Post-Resuscitation Care: Optimizing & Improving Outcomes after Cardiac Arrest Nicole L. Kupchik RN, MN, CCNS CCRN-CMC Clinical Nurse Specialist Harborview Medical Center Seattle, WA Objectives: At the
Post-Resuscitation Care: Optimizing & Improving Outcomes after Cardiac Arrest Nicole L. Kupchik RN, MN, CCNS CCRN-CMC Clinical Nurse Specialist Harborview Medical Center Seattle, WA Objectives: At the
Mild. Moderate. Severe. 32 to to and below
 Mohamud Daya MD, MS Mild 32 to 34 Moderate 28 to 32 Severe 28 and below Jon Rittenberger Shervin Ayati Protocol Development Committee Hypothermia Working Group Lynn Wittwer Jon Jui John Stouffer Scott
Mohamud Daya MD, MS Mild 32 to 34 Moderate 28 to 32 Severe 28 and below Jon Rittenberger Shervin Ayati Protocol Development Committee Hypothermia Working Group Lynn Wittwer Jon Jui John Stouffer Scott
The Evidence Base. Stephan A. Mayer, MD. Columbia University New York, NY
 Hypothermic for Cardiac Arrest The Evidence Base Stephan A. Mayer, MD Director, Neuro-ICU Columbia University New York, NY Disclosures Columbia University Clinical Trials Pilot Award Radiant Medical, Inc.
Hypothermic for Cardiac Arrest The Evidence Base Stephan A. Mayer, MD Director, Neuro-ICU Columbia University New York, NY Disclosures Columbia University Clinical Trials Pilot Award Radiant Medical, Inc.
CHILL OUT! Induced Hypothermia: Challenges & Successes in the
 CHILL OUT! Induced Hypothermia: Challenges & Successes in the ICU Colleen Bell RN, BS, CCRN, Donna Brault RN, BSN, CCRN, Cathy Patnode RN, BSN, CCRN Champlain Valley Physician Hospital November 2012 Objectives
CHILL OUT! Induced Hypothermia: Challenges & Successes in the ICU Colleen Bell RN, BS, CCRN, Donna Brault RN, BSN, CCRN, Cathy Patnode RN, BSN, CCRN Champlain Valley Physician Hospital November 2012 Objectives
Hypothermia: The Science and Recommendations (In-hospital and Out)
") Hypothermia: The Science and Recommendations (In-hospital and Out) L. Kristin Newby, MD, MHS Professor of Medicine Duke University Medical Center Chair, Council on Clinical Cardiology, AHA President, Society
Hypothermia: The Science and Recommendations (In-hospital and Out) L. Kristin Newby, MD, MHS Professor of Medicine Duke University Medical Center Chair, Council on Clinical Cardiology, AHA President, Society
Patient Case. Post cardiac arrest pathophysiology 10/19/2017. Disclosure. Objectives. Patient Case-TM
 Disclosure TARGETED TEMPERATURE MANAGEMENT POST CARDIAC ARREST I have nothing to disclose concerning possible financial or personal relationships with commercial entities that may have a direct or indirect
Disclosure TARGETED TEMPERATURE MANAGEMENT POST CARDIAC ARREST I have nothing to disclose concerning possible financial or personal relationships with commercial entities that may have a direct or indirect
Hypothermia After Cardiac Arrest: Where Are We Now?
 Hypothermia After Cardiac Arrest: Where Are We Now? David A. Pearson, MD, MS Associate Professor Director of Cardiac Arrest Resuscitation Carolinas HealthCare System Disclosures I have no financial interest,
Hypothermia After Cardiac Arrest: Where Are We Now? David A. Pearson, MD, MS Associate Professor Director of Cardiac Arrest Resuscitation Carolinas HealthCare System Disclosures I have no financial interest,
Curricullum Vitae. Dr. Isman Firdaus, SpJP (K), FIHA
, FIHA") Curricullum Vitae Dr. Isman Firdaus, SpJP (K), FIHA Email: ismanf@yahoo.com Qualification : o GP 2001 (FKUI) o Cardiologist 2007 (FKUI) o Cardiovascular Intensivist 2010 - present o Cardiovascular Intervensionist
Curricullum Vitae Dr. Isman Firdaus, SpJP (K), FIHA Email: ismanf@yahoo.com Qualification : o GP 2001 (FKUI) o Cardiologist 2007 (FKUI) o Cardiovascular Intensivist 2010 - present o Cardiovascular Intervensionist
Therapeutic Hypothermia. Jonas Cooper, MD MPH
 Therapeutic Hypothermia Jonas Cooper, MD MPH Hypothermia in Cardiology Early cardiac surgery included cooling to 15 C and stopping all blood flow for one hour while surgery proceeded Belsey RH et al. Profound
Therapeutic Hypothermia Jonas Cooper, MD MPH Hypothermia in Cardiology Early cardiac surgery included cooling to 15 C and stopping all blood flow for one hour while surgery proceeded Belsey RH et al. Profound
Induced Hypothermia for Cardiac Arrest. Heather Hand RN,CCRN,CNRN,ATCN,LNC
 Induced Hypothermia for Cardiac Arrest Heather Hand RN,CCRN,CNRN,ATCN,LNC Cardiac Arrest Epidemiology 400,000 arrests / year in U.S.A 3 / 4 Out-of-hospital 1 / 4 In-hospital survival to hospital 1-5% discharge
Induced Hypothermia for Cardiac Arrest Heather Hand RN,CCRN,CNRN,ATCN,LNC Cardiac Arrest Epidemiology 400,000 arrests / year in U.S.A 3 / 4 Out-of-hospital 1 / 4 In-hospital survival to hospital 1-5% discharge
POST-CARDIAC ARREST CARE: WHAT HAPPENS AFTER ROSC MATTERS! Emergency Nurses Association
 POST-CARDIAC ARREST CARE: WHAT HAPPENS AFTER ROSC MATTERS! Emergency Nurses Association - 2016 Nicole Kupchik MN, RN, CCNS, CCRN, PCCN, CMC Objectives Discuss the 2015 AHA Guideline Updates for Post- Arrest
POST-CARDIAC ARREST CARE: WHAT HAPPENS AFTER ROSC MATTERS! Emergency Nurses Association - 2016 Nicole Kupchik MN, RN, CCNS, CCRN, PCCN, CMC Objectives Discuss the 2015 AHA Guideline Updates for Post- Arrest
Therapeutic Hypothermia
 Objectives Overview Therapeutic Hypothermia Nerissa U. Ko, MD, MAS UCSF Department of Neurology Critical Care Medicine and Trauma June 4, 2011 Hypothermia as a neuroprotectant Proven indications: Adult
Objectives Overview Therapeutic Hypothermia Nerissa U. Ko, MD, MAS UCSF Department of Neurology Critical Care Medicine and Trauma June 4, 2011 Hypothermia as a neuroprotectant Proven indications: Adult
Outcomes of Therapeutic Hypothermia in Cardiac Arrest. Saad Mohammed Shariff, MBBS Aravind Herle, MD, FACC
 Outcomes of Therapeutic Hypothermia in Cardiac Arrest Saad Mohammed Shariff, MBBS Aravind Herle, MD, FACC https://my.americanheart.org/idc/groups/ahamah-public/@wcm/@sop/@scon/documents/downloadable/ucm_427331.pdf
Outcomes of Therapeutic Hypothermia in Cardiac Arrest Saad Mohammed Shariff, MBBS Aravind Herle, MD, FACC https://my.americanheart.org/idc/groups/ahamah-public/@wcm/@sop/@scon/documents/downloadable/ucm_427331.pdf
Therapeutic Hypothermia after Resuscitated Cardiac Arrest
 Therapeutic Hypothermia after Resuscitated Cardiac Arrest The purpose of this protocol is to improve the neurologic outcomes of patients who have experienced cardiac arrest and have been successfully resuscitated.
Therapeutic Hypothermia after Resuscitated Cardiac Arrest The purpose of this protocol is to improve the neurologic outcomes of patients who have experienced cardiac arrest and have been successfully resuscitated.
THERAPEUTIC HYPOTHERMIA POST CARDIAC ARREST
 THERAPEUTIC HYPOTHERMIA POST CARDIAC ARREST Heather Harrington RN, BScN, CNCC(c) Clinical Nurse Educator Sunnybrook Health Sciences Centre Objectives Define Therapeutic Hypothermia (TH) Describe current
THERAPEUTIC HYPOTHERMIA POST CARDIAC ARREST Heather Harrington RN, BScN, CNCC(c) Clinical Nurse Educator Sunnybrook Health Sciences Centre Objectives Define Therapeutic Hypothermia (TH) Describe current
Objectives. Trends in Resuscitation POST-CARDIAC ARREST CARE: WHAT S THE EVIDENCE?
 POST-CARDIAC ARREST CARE: WHAT S THE EVIDENCE? Nicole Kupchik RN, MN, CCNS, CCRN, PCCN, CMC Objectives Discuss the 2015 AHA Guideline Updates for Post- Arrest Care Discuss oxygenation & hemodynamic taregts
POST-CARDIAC ARREST CARE: WHAT S THE EVIDENCE? Nicole Kupchik RN, MN, CCNS, CCRN, PCCN, CMC Objectives Discuss the 2015 AHA Guideline Updates for Post- Arrest Care Discuss oxygenation & hemodynamic taregts
Post-Arrest Care: Beyond Hypothermia
 Post-Arrest Care: Beyond Hypothermia Damon Scales MD PhD Department of Critical Care Medicine Sunnybrook Health Sciences Centre University of Toronto Disclosures CIHR Physicians Services Incorporated Main
Post-Arrest Care: Beyond Hypothermia Damon Scales MD PhD Department of Critical Care Medicine Sunnybrook Health Sciences Centre University of Toronto Disclosures CIHR Physicians Services Incorporated Main
Therapeutic hypothermia following cardiac arrest
 TITLE: Therapeutic hypothermia following cardiac arrest AUTHOR: Jeffrey A. Tice, MD Assistant Professor of Medicine Division of General Internal Medicine Department of Medicine University of California
TITLE: Therapeutic hypothermia following cardiac arrest AUTHOR: Jeffrey A. Tice, MD Assistant Professor of Medicine Division of General Internal Medicine Department of Medicine University of California
Therapeutic Hypothermia: 2011 Research Update. Richard R. Riker MD, FCCM Chest Medicine Associates South Portland, Maine
 Therapeutic Hypothermia: 2011 Research Update Richard R. Riker MD, FCCM Chest Medicine Associates South Portland, Maine Agenda NMBA, Sedation, and Shivering Seizures Prognostication Early = Staging Late
Therapeutic Hypothermia: 2011 Research Update Richard R. Riker MD, FCCM Chest Medicine Associates South Portland, Maine Agenda NMBA, Sedation, and Shivering Seizures Prognostication Early = Staging Late
Update on Sudden Cardiac Death and Resuscitation
 Update on Sudden Cardiac Death and Resuscitation Ashish R. Panchal, MD, PhD Medical Director Center for Emergency Medical Services Assistant Professor Clinical Department of Emergency Medicine The Ohio
Update on Sudden Cardiac Death and Resuscitation Ashish R. Panchal, MD, PhD Medical Director Center for Emergency Medical Services Assistant Professor Clinical Department of Emergency Medicine The Ohio
ECG Changes in Patients Treated with Mild Hypothermia after Cardio-pulmonary Resuscitation for Out-of-hospital Cardiac Arrest
 ECG Changes in Patients Treated with Mild Hypothermia after Cardio-pulmonary Resuscitation for Out-of-hospital Cardiac Arrest R. Schneider, S. Zimmermann, W.G. Daniel, S. Achenbach Department of Internal
ECG Changes in Patients Treated with Mild Hypothermia after Cardio-pulmonary Resuscitation for Out-of-hospital Cardiac Arrest R. Schneider, S. Zimmermann, W.G. Daniel, S. Achenbach Department of Internal
Pathophysiology and Cardiac Insights for Targeted Temperature Management in Emergency Medicine and Critical Care
 Pathophysiology and Cardiac Insights for Targeted Temperature Management in Emergency Medicine and Critical Care LINDSAY LEWIS BSN, RN, CCCC Faculty Disclosure I AM CURRENTLY EMPLOYED AS A CLINICAL MANAGER
Pathophysiology and Cardiac Insights for Targeted Temperature Management in Emergency Medicine and Critical Care LINDSAY LEWIS BSN, RN, CCCC Faculty Disclosure I AM CURRENTLY EMPLOYED AS A CLINICAL MANAGER
TOO COOL OR NOT TOO COOL- THERAPEUTIC HYPOTHERMIA IN THE ICU SCCM TX 2017 TED WU MD PEDIATRIC CRITICAL CARE UNIVERSITY OF TEXAS HEALTH SAN ANTONIO
 TOO COOL OR NOT TOO COOL- THERAPEUTIC HYPOTHERMIA IN THE ICU SCCM TX 2017 TED WU MD PEDIATRIC CRITICAL CARE UNIVERSITY OF TEXAS HEALTH SAN ANTONIO DISCLOSURE I have no relationships with commercial companies
TOO COOL OR NOT TOO COOL- THERAPEUTIC HYPOTHERMIA IN THE ICU SCCM TX 2017 TED WU MD PEDIATRIC CRITICAL CARE UNIVERSITY OF TEXAS HEALTH SAN ANTONIO DISCLOSURE I have no relationships with commercial companies
CrackCast Episode 8 Brain Resuscitation
 CrackCast Episode 8 Brain Resuscitation Episode Overview: 1) Describe 6 therapeutic interventions for the post-arrest brain 2) List 5 techniques for initiating therapeutic hypothermia 3) List 4 mechanisms
CrackCast Episode 8 Brain Resuscitation Episode Overview: 1) Describe 6 therapeutic interventions for the post-arrest brain 2) List 5 techniques for initiating therapeutic hypothermia 3) List 4 mechanisms
Hypothermia Post Cardiac Arrest: An Update
 Hypothermia Post Cardiac Arrest: An Update Justin Lundbye, M.D., FACC Hospital of Central Connecticut Justin.Lundbye@HHCHealth.org Outline Background Whom to Cool How to Cool Post Cardiac Arrest Care Other
Hypothermia Post Cardiac Arrest: An Update Justin Lundbye, M.D., FACC Hospital of Central Connecticut Justin.Lundbye@HHCHealth.org Outline Background Whom to Cool How to Cool Post Cardiac Arrest Care Other
Post Cardiac Arrest Care 2015 American Heart Association Guideline Update for CPR and Emergency Cardiovascular Care
 Post Cardiac Arrest Care 2015 American Heart Association Guideline Update for CPR and Emergency Cardiovascular Care รศ.ดร.พญ.ต นหยง พ พานเมฆาภรณ ภาคว ชาว ส ญญ ว ทยา คณะแพทยศาสตร มหาว ทยาล ยเช ยงใหม System
Post Cardiac Arrest Care 2015 American Heart Association Guideline Update for CPR and Emergency Cardiovascular Care รศ.ดร.พญ.ต นหยง พ พานเมฆาภรณ ภาคว ชาว ส ญญ ว ทยา คณะแพทยศาสตร มหาว ทยาล ยเช ยงใหม System
Therapeutic hypothermia
 INDUCED HYPOTHERMIA Dr. Attilla Kiss M.D. Acting Medical Director Emergency Services EMS Medical Director St. John Medical Center OBJECTIVES Define and explain Induced Hypothermia Discuss both pre-hospital
INDUCED HYPOTHERMIA Dr. Attilla Kiss M.D. Acting Medical Director Emergency Services EMS Medical Director St. John Medical Center OBJECTIVES Define and explain Induced Hypothermia Discuss both pre-hospital
CRS Center for Resuscitation Science
 Therapeutic hypothermia after cardiac arrest and in critical care Speaker disclosures Research Funding: NIH NHLBI Philips Healthcare Doris Duke Foundation American Heart Association CRS Center for Resuscitation
Therapeutic hypothermia after cardiac arrest and in critical care Speaker disclosures Research Funding: NIH NHLBI Philips Healthcare Doris Duke Foundation American Heart Association CRS Center for Resuscitation
Post-Resuscitation Care. Prof. Wilhelm Behringer Center of Emergency Medicine University of Jena
 Post-Resuscitation Care Prof. Wilhelm Behringer Center of Emergency Medicine University of Jena Conflict of interest Emcools Shareholder and founder, honoraria Zoll: honoraria Bard: honoraria, nephew works
Post-Resuscitation Care Prof. Wilhelm Behringer Center of Emergency Medicine University of Jena Conflict of interest Emcools Shareholder and founder, honoraria Zoll: honoraria Bard: honoraria, nephew works
RACE CARS: Hospital Response. David A. Pearson, MD Department of Emergency Medicine Carolinas Medical Center February 23, 2012
 L MODULE 9 RACE CARS: Hospital Response David A. Pearson, MD Department of Emergency Medicine Carolinas Medical Center February 23, 2012 2 Objectives: Post-cardiac arrest syndrome Therapeutic hypothermia
L MODULE 9 RACE CARS: Hospital Response David A. Pearson, MD Department of Emergency Medicine Carolinas Medical Center February 23, 2012 2 Objectives: Post-cardiac arrest syndrome Therapeutic hypothermia
Targeted Temperature Management: An Evolving Therapy for Cardiac Arrest
 Targeted Temperature Management: An Evolving Therapy for Cardiac Arrest By Meagan Dunn, BScN, MSc,, RN, CNE NP Forum April 8, 2016 Objectives To understand: What Therapeutic Temperature Management (TTM)
Targeted Temperature Management: An Evolving Therapy for Cardiac Arrest By Meagan Dunn, BScN, MSc,, RN, CNE NP Forum April 8, 2016 Objectives To understand: What Therapeutic Temperature Management (TTM)
SUMMARY OF MAJOR CHANGES 2010 AHA GUIDELINES FOR CPR & ECC
 SUMMARY OF MAJOR CHANGES 2010 AHA GUIDELINES FOR CPR & ECC The following is a summary of the key issues and changes in the AHA 2010 Guidelines for Cardiopulmonary Resuscitation (CPR) and Emergency Cardiac
SUMMARY OF MAJOR CHANGES 2010 AHA GUIDELINES FOR CPR & ECC The following is a summary of the key issues and changes in the AHA 2010 Guidelines for Cardiopulmonary Resuscitation (CPR) and Emergency Cardiac
SYSTEM-WIDE POLICY & PROCEDURE MANUAL. Policy Title: Hypothermia Post Cardiac Arrest Policy Number: PC-124. President & CEO Page 1 of 9
 Approved By: President & CEO Date Page 1 of 9 POLICY: PURPOSE: To define and describe the implementation of induced hypothermia post cardiac arrest and the nursing assessment and interventions required
Approved By: President & CEO Date Page 1 of 9 POLICY: PURPOSE: To define and describe the implementation of induced hypothermia post cardiac arrest and the nursing assessment and interventions required
Update on Sudden Cardiac Death and Resuscitation
 Update on Sudden Cardiac Death and Resuscitation Ashish R. Panchal, MD, PhD Medical Director Center for Emergency Medical Services Assistant Professor Clinical Department of Emergency Medicine The Ohio
Update on Sudden Cardiac Death and Resuscitation Ashish R. Panchal, MD, PhD Medical Director Center for Emergency Medical Services Assistant Professor Clinical Department of Emergency Medicine The Ohio
New Therapeutic Hypothermia Techniques
 New Therapeutic Hypothermia Techniques Joseph P. Ornato, MD, FACP, FACC, FACEP Professor & Chairman, Emergency Medicine Virginia Commonwealth University Health System Richmond, VA Medical Director Richmond
New Therapeutic Hypothermia Techniques Joseph P. Ornato, MD, FACP, FACC, FACEP Professor & Chairman, Emergency Medicine Virginia Commonwealth University Health System Richmond, VA Medical Director Richmond
Samphant Ponvilawan Bumrungrad International
 Samphant Ponvilawan Bumrungrad International Definitions Artificial circulation using VA ECMO as an alternative to ventilation and external cardiac massage Indications Out-of-Hospital Cardiac Arrest (OHCA)
Samphant Ponvilawan Bumrungrad International Definitions Artificial circulation using VA ECMO as an alternative to ventilation and external cardiac massage Indications Out-of-Hospital Cardiac Arrest (OHCA)
CPR What Works, What Doesn t
 Resuscitation 2017 ECMO and ECLS April 1, 2017 Corey M. Slovis, M.D. Vanderbilt University Medical Center Metro Nashville Fire Department Nashville International Airport Nashville, TN Circulation 2013;128:417-35
Resuscitation 2017 ECMO and ECLS April 1, 2017 Corey M. Slovis, M.D. Vanderbilt University Medical Center Metro Nashville Fire Department Nashville International Airport Nashville, TN Circulation 2013;128:417-35
The ALS Algorithm and Post Resuscitation Care
 The ALS Algorithm and Post Resuscitation Care CET - Ballarat Health Services Valid from 1 st July 2018 to 30 th June 2020 2 Defibrillation Produces simultaneous mass depolarisation of myocardial cells
The ALS Algorithm and Post Resuscitation Care CET - Ballarat Health Services Valid from 1 st July 2018 to 30 th June 2020 2 Defibrillation Produces simultaneous mass depolarisation of myocardial cells
What s new in Therapeutic Hypothermia Ratchanee Lee, MD. Cardiology unit, Department of internal medicine Faculty of Medicine, Ramathibodi hospital
 What s new in Therapeutic Hypothermia Ratchanee Lee, MD. Cardiology unit, Department of internal medicine Faculty of Medicine, Ramathibodi hospital Scopes History & Evidence of TH Important physiologic
What s new in Therapeutic Hypothermia Ratchanee Lee, MD. Cardiology unit, Department of internal medicine Faculty of Medicine, Ramathibodi hospital Scopes History & Evidence of TH Important physiologic
Targeted temperature management after post-anoxic brain insult: where do we stand?
 Targeted temperature management after post-anoxic brain insult: where do we stand? Alain Cariou Intensive Care Unit Cochin University Hospital Paris Descartes University INSERM U970 (France) COI Disclosure
Targeted temperature management after post-anoxic brain insult: where do we stand? Alain Cariou Intensive Care Unit Cochin University Hospital Paris Descartes University INSERM U970 (France) COI Disclosure
Cardiopulmonary Resuscitation in Adults
 Cardiopulmonary Resuscitation in Adults Fatma Özdemir, MD Emergency Deparment of Uludag University Faculty of Medicine OVERVIEW Introduction Pathophysiology BLS algorithm ALS algorithm Post resuscitation
Cardiopulmonary Resuscitation in Adults Fatma Özdemir, MD Emergency Deparment of Uludag University Faculty of Medicine OVERVIEW Introduction Pathophysiology BLS algorithm ALS algorithm Post resuscitation
Emergency Preservation and Resuscitation
 Emergency Preservation and Resuscitation Samuel A. Tisherman, MD, FACS, FCCM Director, Center for Critical Care and Trauma Education Director, SICU RA Cowley Shock Trauma Center Disclosures Co-author of
Emergency Preservation and Resuscitation Samuel A. Tisherman, MD, FACS, FCCM Director, Center for Critical Care and Trauma Education Director, SICU RA Cowley Shock Trauma Center Disclosures Co-author of
CARES Targeted Temperature Management (TTM) Module
 Module") CARES Targeted Temperature Management (TTM) Module OHCA Data Dictionary June 2014 1 CASE NUMBER This is the number assigned to the patient by the hospital. The case number is the number the hospital assigns
CARES Targeted Temperature Management (TTM) Module OHCA Data Dictionary June 2014 1 CASE NUMBER This is the number assigned to the patient by the hospital. The case number is the number the hospital assigns
IN HOSPITAL CARDIAC ARREST AND SEPSIS
 IN HOSPITAL CARDIAC ARREST AND SEPSIS MARGARET DISSELKAMP, MD OVERVIEW Background Epidemiology of in hospital cardiac arrest (IHCA) Use a case scenario to introduce new guidelines Review surviving sepsis
IN HOSPITAL CARDIAC ARREST AND SEPSIS MARGARET DISSELKAMP, MD OVERVIEW Background Epidemiology of in hospital cardiac arrest (IHCA) Use a case scenario to introduce new guidelines Review surviving sepsis
Cardiothoracic Fellow Expectations Division of Cardiac Anesthesia, Beth Israel Deaconess Medical Center
 The fellowship in Cardiothoracic Anesthesia at the Beth Israel Deaconess Medical Center is intended to provide the foundation for a career as either an academic cardiothoracic anesthesiologist or clinical
The fellowship in Cardiothoracic Anesthesia at the Beth Israel Deaconess Medical Center is intended to provide the foundation for a career as either an academic cardiothoracic anesthesiologist or clinical
Post Cardiac Arrest Care. From : 2010 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care
 Post Cardiac Arrest Care From : 2010 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Initial Objectives of Post cardiac Arrest Care Optimize cardiopulmonary
Post Cardiac Arrest Care From : 2010 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Initial Objectives of Post cardiac Arrest Care Optimize cardiopulmonary
CORONARY ARTERY BYPASS GRAFT (CABG) MEASURES GROUP OVERVIEW
 MEASURES GROUP OVERVIEW") CONARY ARTERY BYPASS GRAFT (CABG) MEASURES GROUP OVERVIEW 2015 PQRS OPTIONS F MEASURES GROUPS: 2015 PQRS MEASURES IN CONARY ARTERY BYPASS GRAFT (CABG) MEASURES GROUP: #43 Coronary Artery Bypass Graft (CABG):
CONARY ARTERY BYPASS GRAFT (CABG) MEASURES GROUP OVERVIEW 2015 PQRS OPTIONS F MEASURES GROUPS: 2015 PQRS MEASURES IN CONARY ARTERY BYPASS GRAFT (CABG) MEASURES GROUP: #43 Coronary Artery Bypass Graft (CABG):
Tina Yoo, PharmD Clinical Pharmacist Alameda Health System Highland Hospital
 Tina Yoo, PharmD Clinical Pharmacist Alameda Health System Highland Hospital 1 Review changes in the 2015 AHA ACLS guidelines with emphasis on changes in therapeutic hypothermia Provide overview of ACLS
Tina Yoo, PharmD Clinical Pharmacist Alameda Health System Highland Hospital 1 Review changes in the 2015 AHA ACLS guidelines with emphasis on changes in therapeutic hypothermia Provide overview of ACLS
-Blood Warming- A Hot topic?
 -Blood Warming- A Hot topic? Blaine Kent, MD, FRCPC Associate Professor of Anesthesia Director, Peri-Operative Blood Management Chief, Cardiac Anesthesia Objectives To learn / review the deleterious systemic
-Blood Warming- A Hot topic? Blaine Kent, MD, FRCPC Associate Professor of Anesthesia Director, Peri-Operative Blood Management Chief, Cardiac Anesthesia Objectives To learn / review the deleterious systemic
Objectives. Design: Setting &Patients: Patients. Measurements and Main Results: Common. Adverse events VS Mortality
 ADVERSE EVENTS AND THEIR RELATION TO MORTALITY IN OUT-OF-HOSPITAL CARDIAC ARREST PATIENTS TREATED WITH THERAPEUTIC HYPOTHERMIA Reporter R1 吳志華 Supervisor VS 王瑞芳 100.04.02 Niklas Nielsen, MD, PhD; Kjetil
ADVERSE EVENTS AND THEIR RELATION TO MORTALITY IN OUT-OF-HOSPITAL CARDIAC ARREST PATIENTS TREATED WITH THERAPEUTIC HYPOTHERMIA Reporter R1 吳志華 Supervisor VS 王瑞芳 100.04.02 Niklas Nielsen, MD, PhD; Kjetil
Enhancing 5 th Chain TTM after Cardiac Arrest
 Enhancing 5 th Chain TTM after Cardiac Arrest Seoul St. Mary s Hospital Department of Emergency Medicine Chun Song Youn Agenda Past Current Future First study, 1958 2002, Two landmark paper HACA Trial
Enhancing 5 th Chain TTM after Cardiac Arrest Seoul St. Mary s Hospital Department of Emergency Medicine Chun Song Youn Agenda Past Current Future First study, 1958 2002, Two landmark paper HACA Trial
Hanna K. Al-Makhamreh, M.D., FACC Interventional Cardiologist
 Hanna K. Al-Makhamreh, M.D., FACC Interventional Cardiologist Introduction. Basic Life Support (BLS). Advanced Cardiac Life Support (ACLS). Cardiovascular diseases (CVDs) are the number one cause of death
Hanna K. Al-Makhamreh, M.D., FACC Interventional Cardiologist Introduction. Basic Life Support (BLS). Advanced Cardiac Life Support (ACLS). Cardiovascular diseases (CVDs) are the number one cause of death
Hypothermia in Neonates with HIE TARA JENDZIO, DNP(C), RN, RNC-NIC
, RN, RNC-NIC") Hypothermia in Neonates with HIE TARA JENDZIO, DNP(C), RN, RNC-NIC Objectives 1. Define Hypoxic-Ischemic Encephalopathy (HIE) 2. Identify the criteria used to determine if an infant qualifies for therapeutic
Hypothermia in Neonates with HIE TARA JENDZIO, DNP(C), RN, RNC-NIC Objectives 1. Define Hypoxic-Ischemic Encephalopathy (HIE) 2. Identify the criteria used to determine if an infant qualifies for therapeutic
(31189) Hypothermia Initiation Phase One
 Hypothermia Initiation Phase One") Hypothermia Initiation Phase One Diagnosis Allergies For hypothermia tracking purposes only. Please do not uncheck.- Required Cardiac Emergency Tracking For hypothermia tracking purposes only. Consults
Hypothermia Initiation Phase One Diagnosis Allergies For hypothermia tracking purposes only. Please do not uncheck.- Required Cardiac Emergency Tracking For hypothermia tracking purposes only. Consults
Stayin Alive: Pediatric Advanced Life Support (PALS) Updated Guidelines
 Updated Guidelines") Stayin Alive: Pediatric Advanced Life Support (PALS) Updated Guidelines Margaret Oates, PharmD, BCPPS Pediatric Critical Care Specialist GSHP Summer Meeting July 16, 2016 Disclosures I have nothing to
Stayin Alive: Pediatric Advanced Life Support (PALS) Updated Guidelines Margaret Oates, PharmD, BCPPS Pediatric Critical Care Specialist GSHP Summer Meeting July 16, 2016 Disclosures I have nothing to
Disclosures. Pediatrician Financial: none Volunteer :
 Brain Resuscitation Neurocritical Care Monitoring & Therapies CCCF November 2, 2016 Anne-Marie Guerguerian Critical Care Medicine, The Hospital for Sick Children University of Toronto Disclosures Pediatrician
Brain Resuscitation Neurocritical Care Monitoring & Therapies CCCF November 2, 2016 Anne-Marie Guerguerian Critical Care Medicine, The Hospital for Sick Children University of Toronto Disclosures Pediatrician
Hypothermic Resuscitation 1 st Intercontinental Emergency Medicine Congress, Belek-Antalya 2014
 Hypothermic Resuscitation 1 st Intercontinental Emergency Medicine Congress, Belek-Antalya 2014 Jasmin Arrich Department of Emergency Medicine Medical University of Vienna jasmin.arrich@meduniwien.ac.at
Hypothermic Resuscitation 1 st Intercontinental Emergency Medicine Congress, Belek-Antalya 2014 Jasmin Arrich Department of Emergency Medicine Medical University of Vienna jasmin.arrich@meduniwien.ac.at
Advanced Resuscitation - Child
 C02C Resuscitation 2017-03-23 1 up to 10 years Office of the Medical Director Advanced Resuscitation - Child Intermediate Advanced Critical From PRIMARY ASSESSMENT Known or suspected hypothermia Algorithm
C02C Resuscitation 2017-03-23 1 up to 10 years Office of the Medical Director Advanced Resuscitation - Child Intermediate Advanced Critical From PRIMARY ASSESSMENT Known or suspected hypothermia Algorithm
Advanced Resuscitation - Adult
 C02A Resuscitation 2017-03-23 17 years & older Office of the Medical Director Advanced Resuscitation - Adult Intermediate Advanced Critical From PRIMARY ASSESSMENT Known or suspected hypothermia Algorithm
C02A Resuscitation 2017-03-23 17 years & older Office of the Medical Director Advanced Resuscitation - Adult Intermediate Advanced Critical From PRIMARY ASSESSMENT Known or suspected hypothermia Algorithm
Therapeutic Hypothermia ANZCA 2013
 Therapeutic Hypothermia ANZCA 2013 Stephen Bernard MD Therapeutic Hypothermia-Indications Anoxic brain injury (cardiac arrest) Severe traumatic brain injury Spinal cord injury Why not Therapeutic Hypothermia?
Therapeutic Hypothermia ANZCA 2013 Stephen Bernard MD Therapeutic Hypothermia-Indications Anoxic brain injury (cardiac arrest) Severe traumatic brain injury Spinal cord injury Why not Therapeutic Hypothermia?
1) According to ILCOR guidelines, to what temperature should patients be cooled? a ºC b ºC c ºC d ºC
 According to ILCOR guidelines, to what temperature should patients be cooled? a ºC b ºC c ºC d ºC") MANAGEMENT OF OUT-OF-HOSPITAL CARDIAC ARRESTS WITH INDUCED HYPOTHERMIA ANAESTHESIA TUTORIAL OF THE WEEK 206 22 ND NOVEMBER 2010 Dr Clare Attwood, Specialist Trainee in Anaesthesia Royal Devon and Exeter
MANAGEMENT OF OUT-OF-HOSPITAL CARDIAC ARRESTS WITH INDUCED HYPOTHERMIA ANAESTHESIA TUTORIAL OF THE WEEK 206 22 ND NOVEMBER 2010 Dr Clare Attwood, Specialist Trainee in Anaesthesia Royal Devon and Exeter
DECLARATION OF CONFLICT OF INTEREST. Research grants: Sanofi-Aventis
 DECLARATION OF CONFLICT OF INTEREST Research grants: Sanofi-Aventis Invasive management after cardiac arrest Nikolaos I Nikolaou FESC, FERC Athens, Greece Survival (%) Survival from Out of Hospital Cardiac
DECLARATION OF CONFLICT OF INTEREST Research grants: Sanofi-Aventis Invasive management after cardiac arrest Nikolaos I Nikolaou FESC, FERC Athens, Greece Survival (%) Survival from Out of Hospital Cardiac
Prehospital Post Arrest Care AHA Strive to Revive 2017 November 3, 2017
 Prehospital Post Arrest Care AHA Strive to Revive 2017 November 3, 2017 Jon Rittenberger, MD, MS Department of University of Pittsburgh Employers: Disclosures - Rittenberger University of Pittsburgh UPMC
Prehospital Post Arrest Care AHA Strive to Revive 2017 November 3, 2017 Jon Rittenberger, MD, MS Department of University of Pittsburgh Employers: Disclosures - Rittenberger University of Pittsburgh UPMC
PUZZLE. EARLY IMPACT ALS Jamie Syrett, MD Director of Prehospital Care Rochester General Health System PUZZLE THINKING OUTSIDE THE BOX! EARLY IMPACT?
 PUZZLE EARLY IMPACT ALS Jamie Syrett, MD Director of Prehospital Care Rochester General Health System PUZZLE THINKING OUTSIDE THE BOX! EARLY IMPACT? IV ACCESS? What things do we do that make a difference?
PUZZLE EARLY IMPACT ALS Jamie Syrett, MD Director of Prehospital Care Rochester General Health System PUZZLE THINKING OUTSIDE THE BOX! EARLY IMPACT? IV ACCESS? What things do we do that make a difference?
ACLS Prep. Preparation is key to a successful ACLS experience. Please complete the ACLS Pretest and Please complete this ACLS Prep.
 November, 2013 ACLS Prep Preparation is key to a successful ACLS experience. Please complete the ACLS Pretest and Please complete this ACLS Prep. ACLS Prep Preparation is key to a successful ACLS experience.
November, 2013 ACLS Prep Preparation is key to a successful ACLS experience. Please complete the ACLS Pretest and Please complete this ACLS Prep. ACLS Prep Preparation is key to a successful ACLS experience.
2015 AHA Guidelines: Pediatric Updates
 2015 AHA Guidelines: Pediatric Updates Advances in Pediatric Emergency Medicine December 9, 2016 Karen O Connell, MD, MEd Associate Professor of Pediatrics and Emergency Medicine Emergency Medicine and
2015 AHA Guidelines: Pediatric Updates Advances in Pediatric Emergency Medicine December 9, 2016 Karen O Connell, MD, MEd Associate Professor of Pediatrics and Emergency Medicine Emergency Medicine and
Update of CPR AHA Guidelines
 Update of CPR AHA Guidelines Donald Hal Shaffner Course objective is to have an updated understanding of the American Heart Association s treatment algorithms for the management of cardiac decompensation
Update of CPR AHA Guidelines Donald Hal Shaffner Course objective is to have an updated understanding of the American Heart Association s treatment algorithms for the management of cardiac decompensation
ACLS Review. Pulse Oximetry to be between 94 99% to avoid hyperoxia (high oxygen tension can lead to tissue death
 ACLS Review BLS CPR BLS CPR changed in 2010. The primary change is from the ABC format to CAB. After establishing unresponsiveness and calling for a code, check for a pulse less than 10 seconds then begin
ACLS Review BLS CPR BLS CPR changed in 2010. The primary change is from the ABC format to CAB. After establishing unresponsiveness and calling for a code, check for a pulse less than 10 seconds then begin
Advanced Cardiac Life Support (ACLS) Science Update 2015
 Science Update 2015") 1 2 3 4 5 6 7 8 9 Advanced Cardiac Life Support (ACLS) Science Update 2015 What s New in ACLS for 2015? Adult CPR CPR remains (Compressions, Airway, Breathing Chest compressions has priority over all other
1 2 3 4 5 6 7 8 9 Advanced Cardiac Life Support (ACLS) Science Update 2015 What s New in ACLS for 2015? Adult CPR CPR remains (Compressions, Airway, Breathing Chest compressions has priority over all other
Drowning is a leading cause of death and loss of years of life with over 90% of cases occurring in lower- and middle-income countries.
 Chapter 145 Drowning Episode Overview: 1) List risk factors for drowning 2) List 5 variables that portend poor outcome 3) Describe the diving reflex 4) Describe the management of a drowning patient with
Chapter 145 Drowning Episode Overview: 1) List risk factors for drowning 2) List 5 variables that portend poor outcome 3) Describe the diving reflex 4) Describe the management of a drowning patient with
H Alex Choi, MD MSc Assistant Professor of Neurology and Neurosurgery The University of Texas Health Science Center Mischer Neuroscience Institute
 H Alex Choi, MD MSc Assistant Professor of Neurology and Neurosurgery The University of Texas Health Science Center Mischer Neuroscience Institute Memorial Hermann- Texas Medical Center Learning Objectives
H Alex Choi, MD MSc Assistant Professor of Neurology and Neurosurgery The University of Texas Health Science Center Mischer Neuroscience Institute Memorial Hermann- Texas Medical Center Learning Objectives
Current status of temperature management in the neuro-icu
 Current status of temperature management in the neuro-icu Gregor Brössner, MD Neurologic Intensiv Care Unit Innsbruck, Austria Disclosures: Gregor Brössner has recieved an unrestricted Grant by Alsius
Current status of temperature management in the neuro-icu Gregor Brössner, MD Neurologic Intensiv Care Unit Innsbruck, Austria Disclosures: Gregor Brössner has recieved an unrestricted Grant by Alsius
PRACTICE GUIDELINE. DEFINITIONS: Mild head injury: Glasgow Coma Scale* (GCS) score Moderate head injury: GCS 9-12 Severe head injury: GCS 3-8
 score Moderate head injury: GCS 9-12 Severe head injury: GCS 3-8") PRACTICE GUIDELINE Effective Date: 9-1-2012 Manual Reference: Deaconess Trauma Services TITLE: TRAUMATIC BRAIN INJURY GUIDELINE OBJECTIVE: To provide practice management guidelines for traumatic brain
PRACTICE GUIDELINE Effective Date: 9-1-2012 Manual Reference: Deaconess Trauma Services TITLE: TRAUMATIC BRAIN INJURY GUIDELINE OBJECTIVE: To provide practice management guidelines for traumatic brain
Out-of-Hospital Cardiac Arrest In North Carolina. Christopher Granger, M.D. Director, Duke CCU
 Out-of-Hospital Cardiac Arrest In North Carolina Christopher Granger, M.D. Director, Duke CCU Disclosure Research contracts: AstraZeneca, Novartis, GSK, Sanofi-Aventis, BMS, The Medicines Company, Astellas,
Out-of-Hospital Cardiac Arrest In North Carolina Christopher Granger, M.D. Director, Duke CCU Disclosure Research contracts: AstraZeneca, Novartis, GSK, Sanofi-Aventis, BMS, The Medicines Company, Astellas,
Emergency Cardiovascular Care: EMT-Intermediate Treatment Algorithms. Introduction to the Algorithms
 Emergency Cardiovascular Care: EMT-Intermediate Treatment Algorithms Introduction to the Algorithms Cardiac Arrest Algorithms Prehospital Medication Profiles Perspective regarding the EMT- Intermediate
Emergency Cardiovascular Care: EMT-Intermediate Treatment Algorithms Introduction to the Algorithms Cardiac Arrest Algorithms Prehospital Medication Profiles Perspective regarding the EMT- Intermediate
Cardiac Arrest January 2017 CPR /3/ Day to Survival Propensity Matched
 Cardiac Arrest January 217 Corey M. Slovis, M.D. Vanderbilt University Medical Center Metro Nashville Fire Department Nashville International Airport Nashville, TN CPR 217 Used data based on protocol that
Cardiac Arrest January 217 Corey M. Slovis, M.D. Vanderbilt University Medical Center Metro Nashville Fire Department Nashville International Airport Nashville, TN CPR 217 Used data based on protocol that
Epinephrine Cardiovascular Emergencies Symposium 2018
 Epinephrine Cardiovascular Emergencies Symposium 218 Corey M. Slovis, M.D. Vanderbilt University Medical Center Metro Nashville Fire Department Nashville International Airport Nashville, TN High Quality
Epinephrine Cardiovascular Emergencies Symposium 218 Corey M. Slovis, M.D. Vanderbilt University Medical Center Metro Nashville Fire Department Nashville International Airport Nashville, TN High Quality
Any man s death diminishes me, because I am involved in mankind. - John Donne
 Any man s death diminishes me, because I am involved in mankind - John Donne Cardiac Arrest in 2011 Where are we? Or where should we be? Michael W. Dailey, MD FACEP Associate Professor of Emergency Medicine
Any man s death diminishes me, because I am involved in mankind - John Donne Cardiac Arrest in 2011 Where are we? Or where should we be? Michael W. Dailey, MD FACEP Associate Professor of Emergency Medicine
JUST SAY NO? THE LATEST LOOK AT ACLS MEDICATIONS BRIDGETTE SVANCAREK, MD
 JUST SAY NO? THE LATEST LOOK AT ACLS MEDICATIONS BRIDGETTE SVANCAREK, MD OBJECTIVES Review the progression of the American Heart Association s ACLS cardiac arrest medication guidelines Identify the latest
JUST SAY NO? THE LATEST LOOK AT ACLS MEDICATIONS BRIDGETTE SVANCAREK, MD OBJECTIVES Review the progression of the American Heart Association s ACLS cardiac arrest medication guidelines Identify the latest
Post Resuscitation Care
 Princess Margaret Hospital f Children PAEDIATRIC ACUTE CARE GUIDELINE Post Resuscitation Care Scope (Staff): Scope (Area): All Emergency Department Clinicians Emergency Department This document should
Princess Margaret Hospital f Children PAEDIATRIC ACUTE CARE GUIDELINE Post Resuscitation Care Scope (Staff): Scope (Area): All Emergency Department Clinicians Emergency Department This document should
Adenosine. poison/drug induced. flushing, chest pain, transient asystole. Precautions: tachycardia. fibrillation, atrial flutter. Indications: or VT
 Adenosine Indications: 1. Narrow complex PSVT 2. Does not convert atrial fibrillation, atrial flutter or VT 1. Side effects include flushing, chest pain, transient asystole 2. May deteriorate widecomplex
Adenosine Indications: 1. Narrow complex PSVT 2. Does not convert atrial fibrillation, atrial flutter or VT 1. Side effects include flushing, chest pain, transient asystole 2. May deteriorate widecomplex
Chapter 9. Learning Objectives. Learning Objectives 9/11/2012. Cardiac Arrhythmias. Define electrical therapy
 Chapter 9 Cardiac Arrhythmias Learning Objectives Define electrical therapy Explain why electrical therapy is preferred initial therapy over drug administration for cardiac arrest and some arrhythmias
Chapter 9 Cardiac Arrhythmias Learning Objectives Define electrical therapy Explain why electrical therapy is preferred initial therapy over drug administration for cardiac arrest and some arrhythmias
Hypothermia Short Set-Critical Care HYPOTHERMIA SS- CRITICAL CARE
 Hypothermia Short Set-Critical Care HYPOTHERMIA SS- CRITICAL CARE Inclusion Criteria all must be present Cardiac arrest with return of spontaneous circulation (ROSC) ROSC within 60 mins of witnessed arrest;
Hypothermia Short Set-Critical Care HYPOTHERMIA SS- CRITICAL CARE Inclusion Criteria all must be present Cardiac arrest with return of spontaneous circulation (ROSC) ROSC within 60 mins of witnessed arrest;
Ischemic Heart Disease Interventional Treatment
 Ischemic Heart Disease Interventional Treatment Cardiac Catheterization Laboratory Procedures (N = 89) is a regional and national referral center for percutaneous coronary intervention (PCI). A total of
Ischemic Heart Disease Interventional Treatment Cardiac Catheterization Laboratory Procedures (N = 89) is a regional and national referral center for percutaneous coronary intervention (PCI). A total of
PEDIATRIC POST CARDIAC ARREST
 PEDIATRIC POST CARDIAC ARREST ALGORITHM Cardiac arrest with ROSC CPR > 1 min Initial neurologic exam Assess level of consciousness Evaluate for asymmetric neurologic exam (consider early brain CT if exam
PEDIATRIC POST CARDIAC ARREST ALGORITHM Cardiac arrest with ROSC CPR > 1 min Initial neurologic exam Assess level of consciousness Evaluate for asymmetric neurologic exam (consider early brain CT if exam
Care of the Deteriorating Patient in Recovery NADIA TICEHURST : CLINICAL NURSE EDUCATOR PERI ANAESTHETICS BENDIGO HEALTH
 Care of the Deteriorating Patient in Recovery NADIA TICEHURST : CLINICAL NURSE EDUCATOR PERI ANAESTHETICS BENDIGO HEALTH Intended learning outcomes Describe the components of a comprehensive clinician
Care of the Deteriorating Patient in Recovery NADIA TICEHURST : CLINICAL NURSE EDUCATOR PERI ANAESTHETICS BENDIGO HEALTH Intended learning outcomes Describe the components of a comprehensive clinician
Acid-base management during hypothermic CPB alpha-stat and ph-stat models of blood gas interpretation
 Acid-base management during hypothermic CPB alpha-stat and ph-stat models of blood gas interpretation Michael Kremke Department of Anaesthesiology and Intensive Care Aarhus University Hospital, Denmark
Acid-base management during hypothermic CPB alpha-stat and ph-stat models of blood gas interpretation Michael Kremke Department of Anaesthesiology and Intensive Care Aarhus University Hospital, Denmark
University of Bristol - Explore Bristol Research
 Rogers, C., Capoun, R., Scott, L., Taylor, J., Angelini, G., Narayan, P.,... Ascione, R. (2017). Shortening cardioplegic arrest time in patients undergoing combined coronary and valve surgery: results
Rogers, C., Capoun, R., Scott, L., Taylor, J., Angelini, G., Narayan, P.,... Ascione, R. (2017). Shortening cardioplegic arrest time in patients undergoing combined coronary and valve surgery: results
Standardize comprehensive care of the patient with severe traumatic brain injury
 Trauma Center Practice Management Guideline Iowa Methodist Medical Center Des Moines Management of Patients with Severe Traumatic Brain Injury (GCS < 9) ADULT Practice Management Guideline Contact: Trauma
Trauma Center Practice Management Guideline Iowa Methodist Medical Center Des Moines Management of Patients with Severe Traumatic Brain Injury (GCS < 9) ADULT Practice Management Guideline Contact: Trauma
No conflicts of interest
 Robert M. Rodriguez, MD FAAEM Clinical Professor of Medicine and Emergency Medicine, UCSF No conflicts of interest Major Points Most ICU patients start in ED Chain of critical care starting in field and
Robert M. Rodriguez, MD FAAEM Clinical Professor of Medicine and Emergency Medicine, UCSF No conflicts of interest Major Points Most ICU patients start in ED Chain of critical care starting in field and
Use of Blood Lactate Measurements in the Critical Care Setting
 Use of Blood Lactate Measurements in the Critical Care Setting John G Toffaletti, PhD Director of Blood Gas and Clinical Pediatric Labs Professor of Pathology Duke University Medical Center Chief, VAMC
Use of Blood Lactate Measurements in the Critical Care Setting John G Toffaletti, PhD Director of Blood Gas and Clinical Pediatric Labs Professor of Pathology Duke University Medical Center Chief, VAMC
2010 ACLS Guidelines. Primary goals of therapy for patients
 2010 ACLS Guidelines Part 10: Acute Coronary Syndrome Present : 內科 R1 鍾伯欣 Supervisor: F1 吳亮廷 991110 Primary goals of therapy for patients of ACS Reduce the amount of myocardial necrosis that occurs in
2010 ACLS Guidelines Part 10: Acute Coronary Syndrome Present : 內科 R1 鍾伯欣 Supervisor: F1 吳亮廷 991110 Primary goals of therapy for patients of ACS Reduce the amount of myocardial necrosis that occurs in
DELINEATION OF CLINICAL PRIVILEGES SURGERY - THORACIC AND CARDIOVASCULAR SURGERY
 Basic Education: MD or DO (Applicants must meet the following criteria) Be certified by or be currently qualified to take the board certification examination of a board recognized by the American Board
Basic Education: MD or DO (Applicants must meet the following criteria) Be certified by or be currently qualified to take the board certification examination of a board recognized by the American Board
Scene Safety First always first, your safety is above everything else, hands only CPR (use pocket
 BLS BASICS: Scene Safety First always first, your safety is above everything else, hands only CPR (use pocket facemask or AMBU bag) Adults call it in, start CPR, get AED Child CPR First, Phone call second
BLS BASICS: Scene Safety First always first, your safety is above everything else, hands only CPR (use pocket facemask or AMBU bag) Adults call it in, start CPR, get AED Child CPR First, Phone call second
Kiehl EL, 1,2 Parker AM, 1 Matar RM, 2 Gottbrecht M, 1 Johansen MC, 1 Adams MP, 1 Griffiths LA, 2 Bidwell KL, 1 Menon V, 2 Enfield KB, 1 Gimple LW 1
 C-GRApH: A Validated Scoring System For The Early Risk Stratification Of Neurologic Outcomes After Out-of-hospital Cardiac Arrest Treated With Therapeutic Hypothermia Kiehl EL, 1,2 Parker AM, 1 Matar RM,
C-GRApH: A Validated Scoring System For The Early Risk Stratification Of Neurologic Outcomes After Out-of-hospital Cardiac Arrest Treated With Therapeutic Hypothermia Kiehl EL, 1,2 Parker AM, 1 Matar RM,