Intravascular Ultrasound for Complex Cases
|
|
|
- Linette Francis
- 5 years ago
- Views:
Transcription
1 Intravascular Ultrasound for Complex Cases The Practical Value of IVUS Shigeru Nakamura M.D.
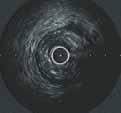
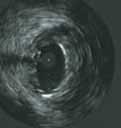
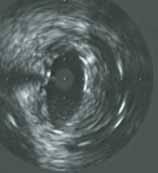
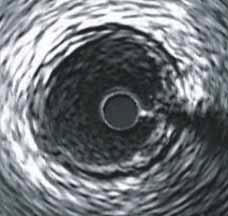
2 Intravascular ultrasound imaging provides short axis information about the vessel. Image quality is not as clear as for angiography, which perhaps explains why the majority of interventional cardiologists don t like it, but reviewing the IVUS tapes enables you to see what you missed under angiography and you can learn lot from IVUS. An operator trying to improve his/her coronary interventional skills must be familiar with IVUS.. What IVUS gives us: Lumen area Vessel Plaque (soft?, calcified?, location?)
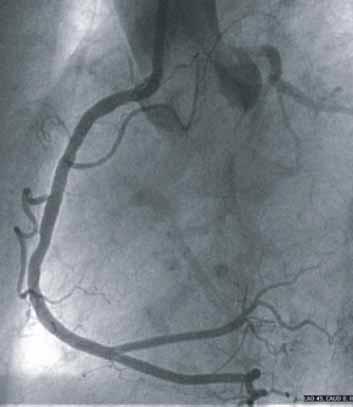
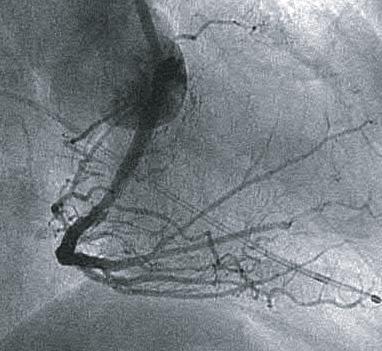
3 (1) Using IVUS to find lesions Angiography provides longitudinal information, and sometimes misses very short lesions ( napkin ring stenosis).

4 Intermediate stenosis by angiography RAO caudal projection Straight caudal projection


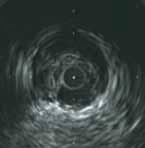

5 LAO caudal view IVUS Movie.1 Angioscopy Movie.2 Lesion


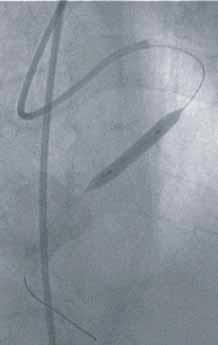
6 Lesion treated with a 9.0x 3.5mm NIR stent 15atm 18atm 1 st dilatation at 15atm, then IVUS, then 2 nd dilatation up to 18atm.


7 Final angiography Angioscopy Movie.3 RAO caudal


8 POBA Straight caudal LAO caudal
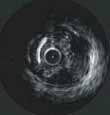
9 Angiography merely shows intermediate stenosis while IVUS reveals critical eccentric low hypo-echoic plaque. Angioscopy showed yellow eccentric plaque. A short 3.5mm NIR stent was implanted at 15atm. IVUS showed poor stent-expansion. Inflation pressure increased to 18 atm. Final angiography suggested a good result; IVUS revealed plaque is still not adequately compressed. Angioscopy showed protrusion from the stent struts.
10 (2) Which is the true lumen? The patient had undergone rotablation and balloon dilatation 3 months previously. There is a parallel channel in the mid RCA. Before stenting, we made sure the wire was in the true lumen. Also there is an eccentric stenosis at the RCA ostium, which we stented with a 3.5mm Multilink at 18atm. The mid RCA was stented with a 3.5mmx 24mm S670 at 12atm.


11 3 Months After Rota + Balloon Which is the true lumen? RAO LAO






12 cardiac atrium apex eccentric ostial stenosis pericardial Connectio site Guidewire in place Pseudolumen RAO cranial Connection site








13 Edge dissection but lumen paten t Stented site 3.5x 15mm Multilink stent at 18 atm. 3.5x 24mm S670 at 12 atm. Distal to the sten t 3month s follow up of dist al PTCA site. The lesion open due to horse shoe plaque disruption
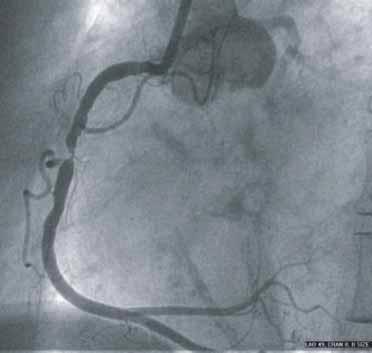
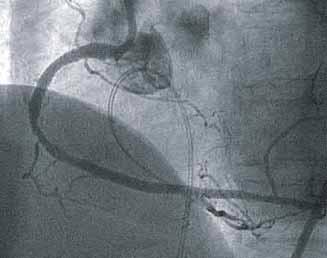
14 (3) Dissection In this case, we lost the guiding catheter and system following recanalization of a CTO in the proximal RCA. There was a large spiral dissection from proximal to distal. In order to ensure successful re-crossing with a guide wire, we have to make sure the wire in the true lumen.


15 Are you in the true lumen? Baseline Post-recanalization spiral dissection




16 White arrow shows the pseudo-lumen. The sharp marginal branch lumen take-off, seen by IVUS, shows the wire is in the true lumen. pseudolume n AM branch
17 The lesion was successfully treated with two long stents. When you need to re-cross a spiral dissection, you can use IVUS to check whether or not your wire is in the true lumen.
18 (4) Stenting Constricted Lesions A simple lesion in the mid RCA, with vessel shrinkage or constriction.

19 Baseline angiography LAO RAO




20 A: Proximal reference B: Lesion C: Constriction site D: Distal reference A B C D

21 Pre-dilatation Side-branch dilatation Wire kept in the RV Post-dilatation 2.5mm, 10atm. 2.5mm, 10atm. For RV branch Multilink plus. 3.5mm,9atm 3.5mm,14atm

22 Final angiogram LAO RAO



23 Pre Post
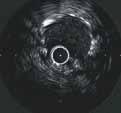
24 (5) Negative Contrast Method The recently-developed Atlantis catheter gives 40MHz imaging that picks up red blood-cell reflections. It can be difficult however to recognize the lumen surface. In this situation, using contrast injection or saline flush should provide a clearer image.

25 Proximal LAD lesion RAO caudal LAO cranial

26 Tightest Site of lesion Standard image Saline flush CVIS Atlantis IVUS catheter


27 LAO caudal Flexi-Cut L
28 LAO cranial RAO caudal Post-DCA by Flexi-Cut L LAO caudal


29 Final IVUS Image of Lesion Standard image Saline flush Movie.4
30 When using negative contrast, catheter position is sometimes affected by the force of the flushing motion. To avoid this problem, hold the IVUS catheter.
31 (6) Stent-edge dissection Stent-edge dissection can be very difficult to be treat.

32 Stenting a CTO in a diffusely-diseased RCA LAO After stenting


33 Visible edge-dissection between stents A B RAO view




34 Follow up angiography shows stent-restenosis at 3 months A B


35 Distal-edge dissection Dissection extending to the neo-intima. At follow up, enlarged vessel size reveals vessel remodeling. (1) (2) (3) noontime * : proliferatio n Remodeling *
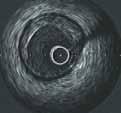
36 (7) IVUS-guided Stent Implantation Key points for IVUS-guided stenting 1) Complete apposition of stent struts to the vessel wall. 2) Stent-lumen CSA larger than the distal reference lumen area. 3) Symmetric expansion. But how do you get symmetric expansion?






37 Irregular lumen surface Baseline IVUS imaging Proximal ref. Distal ref. Lesion



38 Stent Implantation stent proximal stent center Multilink stent 4.0mm at 10atm. stent distal

. 4.0mm at 16atm.")
39 IUVS showed asymmetric stent-expansion. Higher pressure deployed (16atm). 4.0mm at 16atm. Still insufficient expansion



40 Additional inflation with short non-compliant balloon. 4.0x 9.0mm non-compliant balloon at 18atm. Worse expansion than before





41 Balloon downsized to improve symmetry of expansion 3.5mm at 20atm.


42 Final angiogram Spider view shows indentation at the stented site. RAO caudal shows good dilation



43 6 months follow up angiography



44 Pre- ML 4.0mm,10atm 4.0mm,16atm 4.0mm, 18atm 3.5mm, 20atm 6 months f/u
45 Baseline IVUS shows eccentric non-calcified plaque. 4.0mm Multilink stent implanted at 10atm resulted in asymmetric expansion and poor luminal area. Use of a 4.0 non-compliant balloon at 18 atm only resulted in worse symmetry. A 4.5mm balloon would risk a perforation. Downsizing the balloon and increasing the pressure improves stent symmetry but not the lumen area. This is the step-back method of eccentric expansion. Follow up angiography showed no restenosis. IVUS showed neo-intimal proliferation.
46 IVUS-guided DCA (8) Understanding plaque location in the LAD
47 How to use IVUS Guidance IVUS imaging gives a view along the artery from proximal to distal. The upper side of the IVUS image is not necessarily the surface of the heart. The image may be upside-down or rotated. Anatomical landmarks (side branches) are very important for understanding plaque location. Understanding the theory of branching is crucial for DCA.
48 Anatomical Theory of Branching in the Left Coronary Artery If image top is the pericardium site, Cx : 7 to 8 o clock diagonal : about 9 o clock septal: 4 to 5 o clock branching off diagonal circumflex septal
49 The pericardial site is not always at the top of the IVUS image. The operator must rotate his/her own mental image to match rotation of the IVUS image. Picture the diagonal branch at 9 o clock. diagonal Circumflex septal Circumflex septal diagona l
50 Key IVUS Image in the LCA is the diagonal branch. The diagonal and the LAD branch off along the same geometric plane. This plane is almost parallel to the pericardium. Orient the diagonal ostium at 9 o clock in your mind and for all other IVUS imaging. Now the pericardium is at the top, the cardiac site is at the bottom, RV on the right, and LV on the left. Pericardium site diagonal LV RV circumflex septal

51 Stenosis in the mid LAD but where exactly is the plaque?
52 Rotated images left coronary artery diagonal circumflex septal
53 LV site circumflex pericardium site RV site diagonal Key image In t Plaque location is at a 130 o (clockwise) rotation from the diagonal branch. he same direction as the septal branch. Cha mber site 8 o clock 9 o clock Image the diagonal branch at 9 o clock. lesion septal 5 o clock

54 RAO 30 cranial 30 lesion septal The plaque is on the septal side


55 LAO 45 cranial 30 diagonal lesion Plaque is opposite the diagonal

56 Plaque is opposite the diagonal LAO 60 caudal 30
57 IVUS-guided DCA (9) Understanding IVUS guidance in the RCA
58 Anatomical Theory of Branching in the Right Coronary Artery Distal RCA turning round tow ards the ostiu m According to anatomy, imaging the upside of the artery will necessitate a different direction from coronary angiography LAO 50
59 Using Key Branches The posterior descending (PD) branch usually branches off almost perpendicular to the distal RCA. The PD is coming towards you when you image the RCA using the LAO projection on the angio-monitor.

60 Key Image of the RCA atrium apex Pericardium RAO view PD branching direction
61 Rotate the PD to 3 o clock in your mind and for all IVUS images. After rotation, the cardiac side is on top, the pericardium on the bottom, right apex on the right, and the atrium on the left

62 Different Directions of RV branches RV branches Sinus node artery Posterior descending branch LAO 140 cranial




63 Rotated image with PD branch set to 3o clock pericardiu m atrium apex pericardiu m pericardiu m

64 Plaque is at the pericardial site LAO 50

65 RAO 30


66 Orient the cutter-window towards the lateral branch. That is your start-position. Rotate 90 o clockwise. Also rotate 90 o anti-clockwise rotation from start-position. LAO 50 LAO 50


67 Post-DCA Pre- Post-DCA LAO 50
68 For DCA in the RCA, the support wire can alter artery shape. Make sure you re-check the lesion using contrast.
69 (10) DCA in the ostial LAD Severely-angled CX branches

70

71 RAO 30 Caudal 25
72 LAO 60 Caudal 30

73 Pre DCA LAO 45 Cranial 30


74 Anti-clock wise rotation from the CX 60 o anti-clock wise rotation from the CX 120 o anti-clock wise rotation from the CX 180 o counter clock wise rotation from the CX
75 RAO 30 caudal 25 First DCA

76 Repeat IVUS and repeat atherectomy Face the cutter-window towards the circumflex and rotate anti-clockwise for 180 o.

77 RAO 30caudal 25 LAO 60 caudal 30





78 IVUS Guidance enhances plaque removal. ostial LAD plaque Pre 1 st. DCA 2 nd DCA Final LAD and Cx
79 IVUS will usually be used >3 times during your DCA procedure to check the evolving vessel situation. IVUS is useful for verifying plaque removal and the direction of any additional atherectomy. The new Flexi-Cut system removes more plaque than previous devices. One point of caution, however, is that it is harder to feel the plaque being cut, so be on your guard against coronary perforation.
80 Summary IVUS is not necessary for all coronary interventions. But there is no question that it helps you understand what is happening during coronary intervention. It really does take you beyond angiography.
Effectiveness of IVUS in Complex Cases
 Effectiveness of IVUS in Complex Cases Satoru Sumituji,M.D. Rinku General Medical Center IVUS is can provide images of the vessel wall and the tissue around the vessel which cannot be viewed by angiography.
Effectiveness of IVUS in Complex Cases Satoru Sumituji,M.D. Rinku General Medical Center IVUS is can provide images of the vessel wall and the tissue around the vessel which cannot be viewed by angiography.
PCI for Ostial Lesion
 PCI for Ostial Lesion ii) LAD ostial Osamu Katoh,M.D. kyoto Katsura Hospital Cardiovascular Center PCI for a LAD ostial lesion is well-known to be associated with a high restenosis rate because of excessive
PCI for Ostial Lesion ii) LAD ostial Osamu Katoh,M.D. kyoto Katsura Hospital Cardiovascular Center PCI for a LAD ostial lesion is well-known to be associated with a high restenosis rate because of excessive
Coronary Artery Perforation Angioplasty Summit Seoul April 30, 2005
 Coronary Artery Perforation Angioplasty Summit Seoul April 30, 2005 James R. Margolis, M.D. Miami International Cardiology Consultants Miami, Florida USA Introduction In the stent era, coronary artery
Coronary Artery Perforation Angioplasty Summit Seoul April 30, 2005 James R. Margolis, M.D. Miami International Cardiology Consultants Miami, Florida USA Introduction In the stent era, coronary artery
Radiation Safety Abbott Vascular. All rights reserved.
 Radiation Safety More and more complex cases are performed Complexity Index and Fluoroscopy Time 2 3 Collimators / Distances The intensity of scattered radiation is a function of exposed field size Use
Radiation Safety More and more complex cases are performed Complexity Index and Fluoroscopy Time 2 3 Collimators / Distances The intensity of scattered radiation is a function of exposed field size Use
Optimal assessment observation of intravascular ultrasound
 Optimal assessment observation of intravascular ultrasound Katsutoshi Kawamura and Atsunori Okamura Division of Radiology Cardiovascular Center Sakurabashi Watanabe Hospital SAKURABASHI WATANABE Hospital
Optimal assessment observation of intravascular ultrasound Katsutoshi Kawamura and Atsunori Okamura Division of Radiology Cardiovascular Center Sakurabashi Watanabe Hospital SAKURABASHI WATANABE Hospital
For Personal Use. Copyright HMP 2013
 Case Report J INVASIVE CARDIOL 2013;25(2):E39-E41 A Case With Successful Retrograde Stent Delivery via AC Branch for Tortuous Right Coronary Artery Yoshiki Uehara, MD, PhD, Mitsuyuki Shimizu, MD, PhD,
Case Report J INVASIVE CARDIOL 2013;25(2):E39-E41 A Case With Successful Retrograde Stent Delivery via AC Branch for Tortuous Right Coronary Artery Yoshiki Uehara, MD, PhD, Mitsuyuki Shimizu, MD, PhD,
Bifurcation stenting with BVS
 Bifurcation stenting with BVS Breaking the limits or just breaking the struts? Maciej Lesiak Department of Cardiology University Hospital in Poznan, Poland Disclosure Speaker s name: Maciej Lesiak I have
Bifurcation stenting with BVS Breaking the limits or just breaking the struts? Maciej Lesiak Department of Cardiology University Hospital in Poznan, Poland Disclosure Speaker s name: Maciej Lesiak I have
CTO Angioplasty Lessons from the Summit
 CTO Angioplasty Lessons from the Summit Gregg W. Stone, MD Columbia University Medical Center The Cardiovascular Research Foundation New York City The 1 st International CTO Summit January 2004 47 faculty
CTO Angioplasty Lessons from the Summit Gregg W. Stone, MD Columbia University Medical Center The Cardiovascular Research Foundation New York City The 1 st International CTO Summit January 2004 47 faculty
Solving the Dilemma of Ostial Stenting: A Case Series Illustrating the Flash Ostial System
 Volume 1, Issue 1 Case Report Solving the Dilemma of Ostial Stenting: A Case Series Illustrating the Flash Ostial System Robert F. Riley * and Bill Lombardi University of Washington Medical Center, Division
Volume 1, Issue 1 Case Report Solving the Dilemma of Ostial Stenting: A Case Series Illustrating the Flash Ostial System Robert F. Riley * and Bill Lombardi University of Washington Medical Center, Division
Excimer Laser for Coronary Intervention: Case Study RADIAL APPROACH: CORONARY LASER ATHERECTOMY FOR CTO OF THE LAD FOLLOWED BY PTCA NO STENTING
 Excimer Laser for Coronary Intervention: Case Study RADIAL APPROACH: CORONARY LASER ATHERECTOMY FOR CTO OF THE LAD FOLLOWED BY PTCA NO STENTING 1 2013 Spectranetics. All Rights Reserved. Approved for External
Excimer Laser for Coronary Intervention: Case Study RADIAL APPROACH: CORONARY LASER ATHERECTOMY FOR CTO OF THE LAD FOLLOWED BY PTCA NO STENTING 1 2013 Spectranetics. All Rights Reserved. Approved for External
Basics of Angiographic Interpretation Analysis of Angiography
 Basics of Angiographic Interpretation Analysis of Angiography Young-Hak Kim, MD, PhD Cardiac Center, University of Ulsan College of Medicine, Seoul, Korea What made us nervous Supervisors Stent Contrast
Basics of Angiographic Interpretation Analysis of Angiography Young-Hak Kim, MD, PhD Cardiac Center, University of Ulsan College of Medicine, Seoul, Korea What made us nervous Supervisors Stent Contrast
Management of Non-protected Left-Main Bifurcation without Drug Eluting Stent. Masahiko Ochiai MD, FACC, FESC, FSCAI
 Management of Non-protected Left-Main Bifurcation without Drug Eluting Stent Masahiko Ochiai MD, FACC, FESC, FSCAI Division of Cardiology and Cardiovascular Surgery Showa University Northern Yokohama Hospital
Management of Non-protected Left-Main Bifurcation without Drug Eluting Stent Masahiko Ochiai MD, FACC, FESC, FSCAI Division of Cardiology and Cardiovascular Surgery Showa University Northern Yokohama Hospital
PCI for Left Anterior Descending Artery Ostial Stenosis
 PCI for Left Anterior Descending Artery Ostial Stenosis Why do you hesitate PCI for LAD ostial stenosis? LAD Ostial Lesion Limitations of PCI High elastic recoil Involvement of the distal left main coronary
PCI for Left Anterior Descending Artery Ostial Stenosis Why do you hesitate PCI for LAD ostial stenosis? LAD Ostial Lesion Limitations of PCI High elastic recoil Involvement of the distal left main coronary
Elements of CTO PCI. Ashish Pershad, MD FACC Heart and Vascular Center of AZ & Banner Good Samaritan Medical Center
 Elements of CTO PCI Ashish Pershad, MD FACC Heart and Vascular Center of AZ & Banner Good Samaritan Medical Center Disclosures Consultant- Bridgepoint Medical Systems Speakers Honorarium- WL Gore Inc.
Elements of CTO PCI Ashish Pershad, MD FACC Heart and Vascular Center of AZ & Banner Good Samaritan Medical Center Disclosures Consultant- Bridgepoint Medical Systems Speakers Honorarium- WL Gore Inc.
Effect of Intravascular Ultrasound- Guided vs. Angiography-Guided Everolimus-Eluting Stent Implantation: the IVUS-XPL Randomized Clinical Trial
 Effect of Intravascular Ultrasound- Guided vs. Angiography-Guided Everolimus-Eluting Stent Implantation: the IVUS-XPL Randomized Clinical Trial Myeong-Ki Hong, MD. PhD on behalf of the IVUS-XPL trial investigators
Effect of Intravascular Ultrasound- Guided vs. Angiography-Guided Everolimus-Eluting Stent Implantation: the IVUS-XPL Randomized Clinical Trial Myeong-Ki Hong, MD. PhD on behalf of the IVUS-XPL trial investigators
MULTIVESSEL PCI. IN DRUG-ELUTING STENT RESTENOSIS DUE TO STENT FRACTURE, TREATED WITH REPEAT DES IMPLANTATION
 MULTIVESSEL PCI. IN DRUG-ELUTING STENT RESTENOSIS DUE TO STENT FRACTURE, TREATED WITH REPEAT DES IMPLANTATION C. Graidis, D. Dimitriadis, A. Ntatsios, V. Karasavvides Euromedica Kyanous Stavros, Thessaloniki.
MULTIVESSEL PCI. IN DRUG-ELUTING STENT RESTENOSIS DUE TO STENT FRACTURE, TREATED WITH REPEAT DES IMPLANTATION C. Graidis, D. Dimitriadis, A. Ntatsios, V. Karasavvides Euromedica Kyanous Stavros, Thessaloniki.
IVUS Analysis. Myeong-Ki. Hong, MD, PhD. Cardiac Center, Asan Medical Center University of Ulsan College of Medicine, Seoul, Korea
 IVUS Analysis Myeong-Ki Hong, MD, PhD Cardiac Center, Asan Medical Center University of Ulsan College of Medicine, Seoul, Korea Intimal disease (plaque) is dense and will appear white Media is made of
IVUS Analysis Myeong-Ki Hong, MD, PhD Cardiac Center, Asan Medical Center University of Ulsan College of Medicine, Seoul, Korea Intimal disease (plaque) is dense and will appear white Media is made of
Intravascular Ultrasound
 May 2008 Beth Israel Deaconess Medical Center Harvard Medical School Intravascular Ultrasound Matthew Altman, HMS III Gillian Lieberman, MD BIDMC Department of Radiology Presentation Overview 1. Patient
May 2008 Beth Israel Deaconess Medical Center Harvard Medical School Intravascular Ultrasound Matthew Altman, HMS III Gillian Lieberman, MD BIDMC Department of Radiology Presentation Overview 1. Patient
J Am Coll Cardiol 1995; 25: 1479
 Complex PCI: IVUS-Guided PCI Junko Honye Fuchu Keijinkai Hospital, Tokyo Gifu Heart Center, Gifu Japan Roles of IVUS during PCI 1. IVUS before PCI (automatic pullback) Device selection: direct stenting?
Complex PCI: IVUS-Guided PCI Junko Honye Fuchu Keijinkai Hospital, Tokyo Gifu Heart Center, Gifu Japan Roles of IVUS during PCI 1. IVUS before PCI (automatic pullback) Device selection: direct stenting?
The Case of the successful PCI for the ostium CTO lesion of the RCA by the retrograde approach
 The Case of the successful PCI for the ostium CTO lesion of the RCA by the retrograde approach NAGOYA KYORITSU HOSPITAL DAISUKE KAMOI K.KAWASHIMA, Y.KAWAMURA, M.TANAKA T.AOYAMA Case : 58y.o. Male CC: CCSⅡ
The Case of the successful PCI for the ostium CTO lesion of the RCA by the retrograde approach NAGOYA KYORITSU HOSPITAL DAISUKE KAMOI K.KAWASHIMA, Y.KAWAMURA, M.TANAKA T.AOYAMA Case : 58y.o. Male CC: CCSⅡ
Flexibility of the COMBO Dual Therapy Stent
 TM CaseSpotlight Flexibility of the COMBO Dual Therapy Stent Doctor Peter den Heijer is an of the Catheterization Laboratory at the Department of Cardiology of the Amphia Ziekenhuis, Breda, The Netherlands.
TM CaseSpotlight Flexibility of the COMBO Dual Therapy Stent Doctor Peter den Heijer is an of the Catheterization Laboratory at the Department of Cardiology of the Amphia Ziekenhuis, Breda, The Netherlands.
Crossing the Long SFA CTO
 Crossing the Long SFA CTO Techniques and Variables You need to Know Kyoto Katsura Hospital Cardiovascular Center Shigeru Nakamura M.D. Korea Soul 2011.4.28 28 Back ground Superficial femoral artery (SFA)
Crossing the Long SFA CTO Techniques and Variables You need to Know Kyoto Katsura Hospital Cardiovascular Center Shigeru Nakamura M.D. Korea Soul 2011.4.28 28 Back ground Superficial femoral artery (SFA)
Modified Reverse CART technique in a near-ostial
 Modified Reverse CART technique in a near-ostial RCA CTO Dr. Vincent O.H. Kwok MB BS (HK) FRCP (Lond( Lond, Edin, Glasg) ) FACC FSCAI Consultant Cardiologist & Director Cardiac Catheterization & Intervention
Modified Reverse CART technique in a near-ostial RCA CTO Dr. Vincent O.H. Kwok MB BS (HK) FRCP (Lond( Lond, Edin, Glasg) ) FACC FSCAI Consultant Cardiologist & Director Cardiac Catheterization & Intervention
Basic Coronary Angiography DAVID SHAVELLE MD
 Basic Coronary Angiography DAVID SHAVELLE MD Basic Coronary Angiography: Take Home Points Cardiovascular Medicine Boards and Clinical Practice Understand normal coronary anatomy Understand different imaging
Basic Coronary Angiography DAVID SHAVELLE MD Basic Coronary Angiography: Take Home Points Cardiovascular Medicine Boards and Clinical Practice Understand normal coronary anatomy Understand different imaging
EBC London 2013 Provisional SB stenting strategy with kissing balloon with Absorb
 EBC London 2013 Provisional SB stenting strategy with kissing balloon with Absorb A. Medina Servicio de Cardiología Hospital Universitario de Gran Canaria Dr. Negrín Islas Canarias (Spain) Provisional
EBC London 2013 Provisional SB stenting strategy with kissing balloon with Absorb A. Medina Servicio de Cardiología Hospital Universitario de Gran Canaria Dr. Negrín Islas Canarias (Spain) Provisional
Making the difference with Live Image Guidance
 Interventional Cardiology AlluraClarity Making the difference with Live Image Guidance Diagnosis and treatment of coronary artery diseases and atherosclerosis Where/who The First Bethune Hospital of Jilin
Interventional Cardiology AlluraClarity Making the difference with Live Image Guidance Diagnosis and treatment of coronary artery diseases and atherosclerosis Where/who The First Bethune Hospital of Jilin
NC EMERGE TM PTCA Dilatation Catheter
 LEARN MORE Indications, contraindications, warnings and instructions for use can be found in the product labeling supplied with each device. Information for use only in countries with applicable health
LEARN MORE Indications, contraindications, warnings and instructions for use can be found in the product labeling supplied with each device. Information for use only in countries with applicable health
Innovation by design. Technology that sets a new standard
 Innovation by design Technology that sets a new standard Flexible nitinol scoring element with three rectangular spiral struts works in tandem with a semi-compliant balloon to score the target lesion Balloon
Innovation by design Technology that sets a new standard Flexible nitinol scoring element with three rectangular spiral struts works in tandem with a semi-compliant balloon to score the target lesion Balloon
Percutaneous Intervention of Unprotected Left Main Disease
 Percutaneous Intervention of Unprotected Left Main Disease Technical feasibility and Clinical outcomes Seung-Jung Park, MD, PhD, FACC Professor of Internal Medicine Asan Medical Center, Seoul, Korea Unprotected
Percutaneous Intervention of Unprotected Left Main Disease Technical feasibility and Clinical outcomes Seung-Jung Park, MD, PhD, FACC Professor of Internal Medicine Asan Medical Center, Seoul, Korea Unprotected
Rationale and algorithm for below-the-knee acute gain optimization
 Leipzig, 01 Feb. 2018 Rationale and algorithm for below-the-knee acute gain optimization Flavio Airoldi, MD Flavio Airoldi Multimedica IRCCS Milan ITALY flavio.airoldi@multimedica.it Rationale Restenosis
Leipzig, 01 Feb. 2018 Rationale and algorithm for below-the-knee acute gain optimization Flavio Airoldi, MD Flavio Airoldi Multimedica IRCCS Milan ITALY flavio.airoldi@multimedica.it Rationale Restenosis
OCT GUIDED TREATMENT OF CALCIFIED LESIONS RICHARD SHLOFMITZ, MD CHAIRMAN OF DEPT. OF CARDIOLOGY ST. FRANCIS HOSPITAL ROSLYN, NEW YORK
 OCT GUIDED TREATMENT OF CALCIFIED LESIONS RICHARD SHLOFMITZ, MD CHAIRMAN OF DEPT. OF CARDIOLOGY ST. FRANCIS HOSPITAL ROSLYN, NEW YORK Disclosure Statement of Financial Interest Within the past 12 months,
OCT GUIDED TREATMENT OF CALCIFIED LESIONS RICHARD SHLOFMITZ, MD CHAIRMAN OF DEPT. OF CARDIOLOGY ST. FRANCIS HOSPITAL ROSLYN, NEW YORK Disclosure Statement of Financial Interest Within the past 12 months,
Dr Aniket Puri. OCT guided BVS for LMCA to LAD : Optimising the 'Pot'
 OCT guided BVS for LMCA to LAD : Optimising the 'Pot' Dr Aniket Puri MD,DM,FRACP, FACC, FSCAI, FAPSIC Consultant Interventional Cardiologist Christchurch Hospital and Canterbury DHB(Univ of Otago) Christchurch,New
OCT guided BVS for LMCA to LAD : Optimising the 'Pot' Dr Aniket Puri MD,DM,FRACP, FACC, FSCAI, FAPSIC Consultant Interventional Cardiologist Christchurch Hospital and Canterbury DHB(Univ of Otago) Christchurch,New
Form 4: Coronary Evaluation
 Patient Details Hidden Show Show/Hide Annotations Form : Coronary Evaluation Print this Form t Started Date of Coronary Evaluation Coronary Evaluation Indication for Coronary Evaluation Check only one.
Patient Details Hidden Show Show/Hide Annotations Form : Coronary Evaluation Print this Form t Started Date of Coronary Evaluation Coronary Evaluation Indication for Coronary Evaluation Check only one.
Case Report Coronary Artery Perforation and Regrowth of a Side Branch Occluded by a Polytetrafluoroethylene-Covered Stent Implantation
 International Scholarly Research Network Volume 2011, Article ID 212851, 4 pages doi:10.5402/2011/212851 Case Report Coronary Artery Perforation and Regrowth of a Side Branch Occluded by a Polytetrafluoroethylene-Covered
International Scholarly Research Network Volume 2011, Article ID 212851, 4 pages doi:10.5402/2011/212851 Case Report Coronary Artery Perforation and Regrowth of a Side Branch Occluded by a Polytetrafluoroethylene-Covered
Analysis of macrophage accumulation using optical coherence tomography one year after sirolimus, paclitaxel and zotarolimus-eluting stent
 Analysis of macrophage accumulation using optical coherence tomography one year after sirolimus, paclitaxel and zotarolimus-eluting stent implantation. Department of Cardiology, Ehime Prefectural Imabari
Analysis of macrophage accumulation using optical coherence tomography one year after sirolimus, paclitaxel and zotarolimus-eluting stent implantation. Department of Cardiology, Ehime Prefectural Imabari
ACVP s RCIS Review Course: Coronary and Vascular Anatomy, Physiology, Imaging Patrick Hoier, BS, RCIS, FSICP
 ACVP s RCIS Review Course: Coronary and Vascular Anatomy, Physiology, Imaging Patrick Hoier, BS, RCIS, FSICP Invasive Cardiovascular Technology Program Director Southeast Technical Institute Sioux Falls,
ACVP s RCIS Review Course: Coronary and Vascular Anatomy, Physiology, Imaging Patrick Hoier, BS, RCIS, FSICP Invasive Cardiovascular Technology Program Director Southeast Technical Institute Sioux Falls,
Form 4: Coronary Evaluation
 Form : Coronary Evaluation Print this Form t Started Date of Coronary Evaluation Coronary Evaluation Indication for Coronary Evaluation Check only one. Angio NOT DONE: n invasive test performed Followup
Form : Coronary Evaluation Print this Form t Started Date of Coronary Evaluation Coronary Evaluation Indication for Coronary Evaluation Check only one. Angio NOT DONE: n invasive test performed Followup
Bailout technique to rescue the abruptly occluded side branch with collapsed true lumen after main vessel stenting
 Cardiovasc Interv and Ther (2017) 32:87 91 DOI 10.1007/s12928-015-0376-7 CASE REPORT Bailout technique to rescue the abruptly occluded side branch with collapsed true lumen after main vessel stenting Atsushi
Cardiovasc Interv and Ther (2017) 32:87 91 DOI 10.1007/s12928-015-0376-7 CASE REPORT Bailout technique to rescue the abruptly occluded side branch with collapsed true lumen after main vessel stenting Atsushi
STENTYS for Le, Main Sten2ng. Carlo Briguori, MD, PhD Clinica Mediterranea Naples, Italy
 STENTYS for Le, Main Sten2ng Carlo Briguori, MD, PhD Clinica Mediterranea Naples, Italy Disclosure Statement of Financial Interest I, Carlo Briguori DO NOT have a financial interest/ arrangement or affilia2on
STENTYS for Le, Main Sten2ng Carlo Briguori, MD, PhD Clinica Mediterranea Naples, Italy Disclosure Statement of Financial Interest I, Carlo Briguori DO NOT have a financial interest/ arrangement or affilia2on
Successful revascularization of LCX-CTO via a underlying
 IPS/CTO LIVE 2012 ;@ Asan Medical Center, Seoul, Korea Successful revascularization of LCX-CTO via a underlying collateral l channel The Department of Cardiology, Daini i Okamoto general hospital Masaki
IPS/CTO LIVE 2012 ;@ Asan Medical Center, Seoul, Korea Successful revascularization of LCX-CTO via a underlying collateral l channel The Department of Cardiology, Daini i Okamoto general hospital Masaki
Lessons for Successful Subintimal Angioplasty in SFA CTO
 Lessons for Successful Subintimal Angioplasty in SFA CTO John R. Laird Professor of Medicine Medical Director of the Vascular Center UC Davis Medical Center CTOs in the Periphery Presence of Total Occlusion
Lessons for Successful Subintimal Angioplasty in SFA CTO John R. Laird Professor of Medicine Medical Director of the Vascular Center UC Davis Medical Center CTOs in the Periphery Presence of Total Occlusion
Fighting Through a Heavy Calcified RCA-CTO; Required Retrograde Approach Two Times in the Difficulty of Passing Devices Through
 Fighting Through a Heavy Calcified RCA-CTO; Required Retrograde Approach Two Times in the Difficulty of Passing Devices Through The Department of Cardiology Dai-ni Okamoto General Hospital Masaki Tanabe
Fighting Through a Heavy Calcified RCA-CTO; Required Retrograde Approach Two Times in the Difficulty of Passing Devices Through The Department of Cardiology Dai-ni Okamoto General Hospital Masaki Tanabe
Technical considerations in the Treatment of Left Main Lesions Ioannis Iakovou, MD, PhD
 Technical considerations in the Treatment of Left Main Lesions Ioannis Iakovou, MD, PhD Onassis Cardiac Surgery Center, Athens, Greece Critical issues in LM PCI Anatomic variability Techniques Variability
Technical considerations in the Treatment of Left Main Lesions Ioannis Iakovou, MD, PhD Onassis Cardiac Surgery Center, Athens, Greece Critical issues in LM PCI Anatomic variability Techniques Variability
FFR and intravascular imaging, which of which?
 FFR and intravascular imaging, which of which? Ayman Khairy MD, PhD, FESC Associate professor of Cardiovascular Medicine Vice Director of Assiut University Hospitals Assiut, Egypt Diagnostic assessment
FFR and intravascular imaging, which of which? Ayman Khairy MD, PhD, FESC Associate professor of Cardiovascular Medicine Vice Director of Assiut University Hospitals Assiut, Egypt Diagnostic assessment
Side Branch Occlusion
 Side Branch Occlusion Mechanism, Outcome, and How to avoid it From COBIS II Registry Hyeon-Cheol Gwon Cardiac&Vascular Center, Samsung Medical Center Sungkyunkwan University School of Medicine SB occlusion
Side Branch Occlusion Mechanism, Outcome, and How to avoid it From COBIS II Registry Hyeon-Cheol Gwon Cardiac&Vascular Center, Samsung Medical Center Sungkyunkwan University School of Medicine SB occlusion
Cardiologic history. Anamnesis. Female BD Risk factors HTN, DM, Dyslipidaemia. Cardiologic Long history. Last admission Heart failure
 Anamnesis Cardiologic history Female BD 29.7.1939 Risk factors HTN, DM, Dyslipidaemia Cardiologic Long history Last admission Heart failure 2004 NSTEMI CX stenosis DES on CX 2012 Acute Pulmonary Oedema
Anamnesis Cardiologic history Female BD 29.7.1939 Risk factors HTN, DM, Dyslipidaemia Cardiologic Long history Last admission Heart failure 2004 NSTEMI CX stenosis DES on CX 2012 Acute Pulmonary Oedema
Guide Wires design and selection Abbott Vascular. All rights reserved.
 Guide Wires design and selection the cardiac catheter was...the key in the lock Cournand AF, Nobel lecture December 11, 1956; nowadays, the coronary guidewire is the master key to all locks Colombo et
Guide Wires design and selection the cardiac catheter was...the key in the lock Cournand AF, Nobel lecture December 11, 1956; nowadays, the coronary guidewire is the master key to all locks Colombo et
Calcium Removal and Plaque Modification in the Era of DEB and Contemporary Stenting for Femoro- Popliteal Disease
 Calcium Removal and Plaque Modification in the Era of DEB and Contemporary Stenting for Femoro- Popliteal Disease Thomas M. Shimshak, MD Heart and Vascular Center Florida Hospital Heartland Medical Center
Calcium Removal and Plaque Modification in the Era of DEB and Contemporary Stenting for Femoro- Popliteal Disease Thomas M. Shimshak, MD Heart and Vascular Center Florida Hospital Heartland Medical Center
What Coronary Specialists Teach The Vascular Community About Vessel Prep? Tony Das, MD Texas Health, Dallas Dallas, Texas
 What Coronary Specialists Teach The Vascular Community About Vessel Prep? Tony Das, MD Texas Health, Dallas Dallas, Texas Stent Era Lessons on Vessel Preparation Under expanded stent consequences Abrupt
What Coronary Specialists Teach The Vascular Community About Vessel Prep? Tony Das, MD Texas Health, Dallas Dallas, Texas Stent Era Lessons on Vessel Preparation Under expanded stent consequences Abrupt
LM stenting - Cypher
 LM stenting - Cypher Left main stenting with BMS Since 1995 Issues in BMS era AMC Restenosis and TLR (%) 3 27 TLR P=.282 Restenosis P=.71 28 2 1 15 12 Ostium 5 4 Shaft Bifurcation Left main stenting with
LM stenting - Cypher Left main stenting with BMS Since 1995 Issues in BMS era AMC Restenosis and TLR (%) 3 27 TLR P=.282 Restenosis P=.71 28 2 1 15 12 Ostium 5 4 Shaft Bifurcation Left main stenting with
Blood supply of the Heart & Conduction System. Dr. Nabil Khouri
 Blood supply of the Heart & Conduction System Dr. Nabil Khouri Arterial supply of Heart Right coronary artery Left coronary artery 3 Introduction: Coronary arteries - VASAVASORUM arising from aortic sinuses
Blood supply of the Heart & Conduction System Dr. Nabil Khouri Arterial supply of Heart Right coronary artery Left coronary artery 3 Introduction: Coronary arteries - VASAVASORUM arising from aortic sinuses
A Case of Recoiling of Everolimus - eluting Stent at the Ostium of the Right Coronary Artery by Out - stent Plaque Progression
 Jikeikai Med J 2016 ; 63 : 71-6 Case Report A Case of Recoiling of Everolimus - eluting Stent at the Ostium of the Right Coronary Artery by Out - stent Plaque Progression Haruka Kimura, Tetsuya Ishikawa,
Jikeikai Med J 2016 ; 63 : 71-6 Case Report A Case of Recoiling of Everolimus - eluting Stent at the Ostium of the Right Coronary Artery by Out - stent Plaque Progression Haruka Kimura, Tetsuya Ishikawa,
Utility of Image-Guided Atherectomy for Optimal Treatment of Ambiguous Lesions by Angiography
 Utility of Image-Guided Atherectomy for Optimal Treatment of Ambiguous Lesions by Angiography Jon C. George, MD; Vincent Varghese, DO From the Deborah Heart and Lung Center, Browns Mills, New Jersey. ABSTRACT:
Utility of Image-Guided Atherectomy for Optimal Treatment of Ambiguous Lesions by Angiography Jon C. George, MD; Vincent Varghese, DO From the Deborah Heart and Lung Center, Browns Mills, New Jersey. ABSTRACT:
Le# main treatment with Stentys stent. Carlo Briguori, MD, PhD Clinica Mediterranea Naples, Italy
 Le# main treatment with Stentys stent Carlo Briguori, MD, PhD Clinica Mediterranea Naples, Italy Disclosure Statement of Financial Interest I, Carlo Briguori DO NOT have a financial interest/ arrangement
Le# main treatment with Stentys stent Carlo Briguori, MD, PhD Clinica Mediterranea Naples, Italy Disclosure Statement of Financial Interest I, Carlo Briguori DO NOT have a financial interest/ arrangement
Appropriate Device Selection for Endovascular Procedures
 Appropriate Device Selection for Endovascular Procedures Thomas M. Shimshak, MD Florida Hospital Heartland Medical Center Sebring, Florida Disclosures Speaker s Bureau: Abbott Vascular Boston Scientific
Appropriate Device Selection for Endovascular Procedures Thomas M. Shimshak, MD Florida Hospital Heartland Medical Center Sebring, Florida Disclosures Speaker s Bureau: Abbott Vascular Boston Scientific
Dr Felix Keng. Imaging of the heart is technically difficult because: Role of Cardiac MSCT. Current: Cardiac Motion Respiratory Motion
 Siemens Philips Dr Felix Keng GE Toshiba Role of Cardiac MSCT Current: Structural / congenital heart imaging Extra-cardiac / Great vessel imaging Volumes and ejection fractions (cine + gating) Calcium
Siemens Philips Dr Felix Keng GE Toshiba Role of Cardiac MSCT Current: Structural / congenital heart imaging Extra-cardiac / Great vessel imaging Volumes and ejection fractions (cine + gating) Calcium
When Aspiration Thrombectomy Does Not Work? A A R O N W O N G N A T I O N A L H E A R T C E N T R E S I N G A P O R E
 When Aspiration Thrombectomy Does Not Work? A A R O N W O N G N A T I O N A L H E A R T C E N T R E S I N G A P O R E Thrombus in STEMI Over 70% of STEMI patients has angiographic evidence of thrombus
When Aspiration Thrombectomy Does Not Work? A A R O N W O N G N A T I O N A L H E A R T C E N T R E S I N G A P O R E Thrombus in STEMI Over 70% of STEMI patients has angiographic evidence of thrombus
IVUS-Guided d Provisional i Stenting: Plaque or Carina Shift. Soo-Jin Kang, MD., PhD.
 Left Main and Bifurcation Summit IVUS-Guided d Provisional i Stenting: ti Plaque or Carina Shift Soo-Jin Kang, MD., PhD. Department of Cardiology, University of Ulsan College of Medicine Asan Medical Center,
Left Main and Bifurcation Summit IVUS-Guided d Provisional i Stenting: ti Plaque or Carina Shift Soo-Jin Kang, MD., PhD. Department of Cardiology, University of Ulsan College of Medicine Asan Medical Center,
Access strategy for chronic total occlusions (CTOs) is crucial
 is crucial") Learn How Access Strategy Impacts Complex CTO Crossing Arthur C. Lee, MD The Cardiac & Vascular Institute, Gainesville, Florida VASCULAR DISEASE MANAGEMENT 2018;15(3):E19-E23. Key words: chronic total
Learn How Access Strategy Impacts Complex CTO Crossing Arthur C. Lee, MD The Cardiac & Vascular Institute, Gainesville, Florida VASCULAR DISEASE MANAGEMENT 2018;15(3):E19-E23. Key words: chronic total
So-Yeon Choi, MD., PhD. Department of Cardiology Ajou University School of Medicine, Korea
 So-Yeon Choi, MD., PhD. Department of Cardiology Ajou University School of Medicine, Korea Anatomical vs Functional Significance? Coronary Angiogram Treadmill Test Tc-99m-MIBI SPECT MDCT Coronary Angiogram
So-Yeon Choi, MD., PhD. Department of Cardiology Ajou University School of Medicine, Korea Anatomical vs Functional Significance? Coronary Angiogram Treadmill Test Tc-99m-MIBI SPECT MDCT Coronary Angiogram
PCI for In-Stent Restenosis. CardioVascular Research Foundation
 PCI for In-Stent Restenosis ISR of BMS Patterns of In-Stent Restenosis Pattern I : Focal Type IA: Articulation / Gap Type IB: Marginal Type IC: Focal body Type ID: Multifocal Pattern II,III,IV : Diffuse
PCI for In-Stent Restenosis ISR of BMS Patterns of In-Stent Restenosis Pattern I : Focal Type IA: Articulation / Gap Type IB: Marginal Type IC: Focal body Type ID: Multifocal Pattern II,III,IV : Diffuse
INTEGRATING ECHOCARDIOGRAPHY WITH CATHETER INTERVENTIONS FOR CONGENITAL HEART DISEASE. Krishna Kumar SevenHills Hospital, Mumbai, India
 INTEGRATING ECHOCARDIOGRAPHY WITH CATHETER INTERVENTIONS FOR CONGENITAL HEART DISEASE Krishna Kumar SevenHills Hospital, Mumbai, India Why talk about it? What is the big deal? Are we not stating the obvious?
INTEGRATING ECHOCARDIOGRAPHY WITH CATHETER INTERVENTIONS FOR CONGENITAL HEART DISEASE Krishna Kumar SevenHills Hospital, Mumbai, India Why talk about it? What is the big deal? Are we not stating the obvious?
Two dislodged and crushed coronary stents: treatment of two simultaneously dislodged stents using crushing techniques
 CASE REPORT Korean J Intern Med 2013;28:718-723 Two dislodged and crushed coronary stents: treatment of two simultaneously dislodged stents using crushing techniques Dong-Hyeok Yang, Seong-Ill Woo, Dae-Hyeok
CASE REPORT Korean J Intern Med 2013;28:718-723 Two dislodged and crushed coronary stents: treatment of two simultaneously dislodged stents using crushing techniques Dong-Hyeok Yang, Seong-Ill Woo, Dae-Hyeok
Why I try to avoid side branch dilatation
 Why I try to avoid side branch dilatation Hyeon-Cheol Gwon Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea Why I don t kiss? I kiss! I prefer to discuss SB ballooning rather
Why I try to avoid side branch dilatation Hyeon-Cheol Gwon Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea Why I don t kiss? I kiss! I prefer to discuss SB ballooning rather
Transcatheter Aortic Valve Implantation Management of risks and complications
 Transcatheter Aortic Valve Implantation Management of risks and complications TAVI Summit, Seoul, Korea, Spetember 3rd, 2011 Alain Cribier University of Rouen, France Complications of TAVI Depending on
Transcatheter Aortic Valve Implantation Management of risks and complications TAVI Summit, Seoul, Korea, Spetember 3rd, 2011 Alain Cribier University of Rouen, France Complications of TAVI Depending on
THE PROXIMAL LAD VIA SVG IN PATIENT AFTER CABG. Cardiovascular department Tokyo, Japan
 SUCCESSFUL RECANALIZATION OF CTO IN THE PROXIMAL LAD VIA SVG IN PATIENT AFTER CABG St. Lukes International Hospital Cardiovascular department Tokyo, Japan Hitoshi Anzai MD M.D. Present illness 64 YRS-OLD
SUCCESSFUL RECANALIZATION OF CTO IN THE PROXIMAL LAD VIA SVG IN PATIENT AFTER CABG St. Lukes International Hospital Cardiovascular department Tokyo, Japan Hitoshi Anzai MD M.D. Present illness 64 YRS-OLD
ANGIOPLASY SUMMIT 2007 TCT ASIA PACIFIC. Seoul, Korea: April Session: Left mains & bifurcation intervention
 ANGIOPLASY SUMMIT 2007 TCT ASIA PACIFIC Seoul, Korea: 25-27 27 April 2007 Session: Left mains & bifurcation intervention An integrated approach to bifurcation lesions: lessons from years of randomized
ANGIOPLASY SUMMIT 2007 TCT ASIA PACIFIC Seoul, Korea: 25-27 27 April 2007 Session: Left mains & bifurcation intervention An integrated approach to bifurcation lesions: lessons from years of randomized
Ping-Pong Guide Catheter Technique for Retrograde Intervention of a Chronic Total Occlusion Through an Ipsilateral Collateral
 Catheterization and Cardiovascular Interventions 78:395 399 (2011) Case Reports Ping-Pong Guide Catheter Technique for Retrograde Intervention of a Chronic Total Occlusion Through an Ipsilateral Collateral
Catheterization and Cardiovascular Interventions 78:395 399 (2011) Case Reports Ping-Pong Guide Catheter Technique for Retrograde Intervention of a Chronic Total Occlusion Through an Ipsilateral Collateral
There are multiple endovascular options for treatment
 Peripheral Rotablator Atherectomy: The Below-the-Knee Approach to Address Calcium Head On Peripheral Rotablator s front-cutting, diamond-tipped burr provides stable rotation in calcified lesions. BY SONYA
Peripheral Rotablator Atherectomy: The Below-the-Knee Approach to Address Calcium Head On Peripheral Rotablator s front-cutting, diamond-tipped burr provides stable rotation in calcified lesions. BY SONYA
Making the difference with Philips Live Image Guidance. Philips Interventional tools for Allura Cath Lab Systems
 Making the difference with Philips Live Image Guidance Philips Interventional tools for Allura Cath Lab Systems Making the difference with 2 Philips Live Image Guidance Together we make the difference
Making the difference with Philips Live Image Guidance Philips Interventional tools for Allura Cath Lab Systems Making the difference with 2 Philips Live Image Guidance Together we make the difference
DK Crush,Culotte,SKS,T or TAP. Subhash Chandra, MD,DM,FACC Chairman,Cardiac Sciences BLK Super Speciality Hospital, Pusa Road, New Delhi
 PCI for Bifurcations: Which is the best strategy DK Crush,Culotte,SKS,T or TAP Subhash Chandra, MD,DM,FACC Chairman,Cardiac Sciences BLK Super Speciality Hospital, Pusa Road, New Delhi CSI 2018 Selection
PCI for Bifurcations: Which is the best strategy DK Crush,Culotte,SKS,T or TAP Subhash Chandra, MD,DM,FACC Chairman,Cardiac Sciences BLK Super Speciality Hospital, Pusa Road, New Delhi CSI 2018 Selection
CARDIOLOGY SYMPOSIUM 2015 CAROLINA CARDIOLOGY CONSULTANTS OF GHS
 CARDIOLOGY SYMPOSIUM 2015 CAROLINA CARDIOLOGY CONSULTANTS OF GHS STENT, OPERATE, OR MEDICATE? DIFFERING PERSPECTIVES ON CORONARY REVASCULARIZATION JIM BAUCUM, MD FACC SCOTT JOHNSON, MD JANUARY 24, 2015
CARDIOLOGY SYMPOSIUM 2015 CAROLINA CARDIOLOGY CONSULTANTS OF GHS STENT, OPERATE, OR MEDICATE? DIFFERING PERSPECTIVES ON CORONARY REVASCULARIZATION JIM BAUCUM, MD FACC SCOTT JOHNSON, MD JANUARY 24, 2015
Angioplasty Summit TCTAP Technical Aspects of Overview in CTO-PCI Toyohashi Heart Center Takahiko Suzuki, M.D
 Angioplasty Summit TCTAP 2010 Technical Aspects of Overview in CTO-PCI Toyohashi Heart Center Takahiko Suzuki, M.D Introduction CTO-PCI has been technically and technologically evolved over the past two
Angioplasty Summit TCTAP 2010 Technical Aspects of Overview in CTO-PCI Toyohashi Heart Center Takahiko Suzuki, M.D Introduction CTO-PCI has been technically and technologically evolved over the past two
Coronary artery Dissection. Dr TP Singh MD,DM
 Coronary artery Dissection Dr TP Singh MD,DM 52 M,Non HT, Non DM,Acute IWMI lysed within 4 hours D2 Coronary angiography RCA mid 90% discrete hazy stenosis LAD non significant ifi disease, LCx Normal Taken
Coronary artery Dissection Dr TP Singh MD,DM 52 M,Non HT, Non DM,Acute IWMI lysed within 4 hours D2 Coronary angiography RCA mid 90% discrete hazy stenosis LAD non significant ifi disease, LCx Normal Taken
Complex PCI. Your partner in complex PCI: In-stent restenosis (ISR)
") Comple PCI Your partner in comple PCI: Your partner in comple PCI: Philips provides a portfolio of specialty coronary diagnostic and therapy devices that enable safe and effective treatment of a wide variety
Comple PCI Your partner in comple PCI: Your partner in comple PCI: Philips provides a portfolio of specialty coronary diagnostic and therapy devices that enable safe and effective treatment of a wide variety
Shockwave Intravascular Lithotripsy System treatment of calcified lesions: Intravascular OCT analysis
 Shockwave Intravascular Lithotripsy System treatment of calcified lesions: Intravascular OCT analysis Andrew Holden, MBChB, FRANZCR, EBIR Director of Interventional Radiology Auckland, New Zealand LINC
Shockwave Intravascular Lithotripsy System treatment of calcified lesions: Intravascular OCT analysis Andrew Holden, MBChB, FRANZCR, EBIR Director of Interventional Radiology Auckland, New Zealand LINC
Antegrade techniques for CTO recanalization. Dr. George Karavolias, MD, PhD, FESC, FACC Interventional Cardiologist
 Antegrade techniques for CTO recanalization Dr. George Karavolias, MD, PhD, FESC, FACC Interventional Cardiologist can CTOs be reliably opened by PCI? Meta-Analysis of 18,061 Patients Patel V, J Am Coll
Antegrade techniques for CTO recanalization Dr. George Karavolias, MD, PhD, FESC, FACC Interventional Cardiologist can CTOs be reliably opened by PCI? Meta-Analysis of 18,061 Patients Patel V, J Am Coll
Culprit Lesion Remodeling and Long-term (> 5years) Prognosis in Patients with Acute Coronary Syndrome
 Prognosis in Patients with Acute Coronary Syndrome") Culprit Lesion Remodeling and Long-term (> 5years) Prognosis in Patients with Acute Coronary Syndrome Hiroyuki Okura*, MD; Nobuya Matsushita**,MD Kenji Shimeno**, MD; Hiroyuki Yamaghishi**, MD Iku Toda**,
Culprit Lesion Remodeling and Long-term (> 5years) Prognosis in Patients with Acute Coronary Syndrome Hiroyuki Okura*, MD; Nobuya Matsushita**,MD Kenji Shimeno**, MD; Hiroyuki Yamaghishi**, MD Iku Toda**,
PCI for Chronic Total Occlusions
 PCI for Chronic Total Occlusions Chronic Total Occlusions Why not Medical Treatment? Medical Treatment CTO in 891 pts over 24 years High 10% Mortality Low 2 % 1 year 10 years Puma JA, et al. JACC 1994;23:390A
PCI for Chronic Total Occlusions Chronic Total Occlusions Why not Medical Treatment? Medical Treatment CTO in 891 pts over 24 years High 10% Mortality Low 2 % 1 year 10 years Puma JA, et al. JACC 1994;23:390A
I have nothing to disclose.
 I have nothing to disclose. ESC congress of cardiology, 25-29th August 2012, Munich, Germany Minsk-Village 6, August 26 th, 2:22 PM Session: The grey zone of coronary interventions: The real bifurcation
I have nothing to disclose. ESC congress of cardiology, 25-29th August 2012, Munich, Germany Minsk-Village 6, August 26 th, 2:22 PM Session: The grey zone of coronary interventions: The real bifurcation
DEB experience in Gachon Universtiy Gil Hospital (in ISR) Soon Yong Suh MD., PhD. Heart Center Gachon University Gil Hospital Seoul, Korea.
 Soon Yong Suh MD., PhD. Heart Center Gachon University Gil Hospital Seoul, Korea.") DEB experience in Gachon Universtiy Gil Hospital (in ISR) Soon Yong Suh MD., PhD. Heart Center Gachon University Gil Hospital Seoul, Korea. In-stent restenosis (ISR) Remains important issue even in the
DEB experience in Gachon Universtiy Gil Hospital (in ISR) Soon Yong Suh MD., PhD. Heart Center Gachon University Gil Hospital Seoul, Korea. In-stent restenosis (ISR) Remains important issue even in the
A Novel Low Pressure Self Expanding Nitinol Coronary Stent (vprotect): Device Design and FIH Experience
: Device Design and FIH Experience") A Novel Low Pressure Self Expanding Nitinol Coronary Stent (vprotect): Device Design and FIH Experience Juan F. Granada, MD Medical Director, Skirball Center for Cardiovascular Research The Cardiovascular
A Novel Low Pressure Self Expanding Nitinol Coronary Stent (vprotect): Device Design and FIH Experience Juan F. Granada, MD Medical Director, Skirball Center for Cardiovascular Research The Cardiovascular
Left main coronary artery (LMCA): The proximal segment
: The proximal segment") Anatomy and Pathology of Left main coronary artery G Nakazawa Tokai Univ. Kanagawa, Japan 1 Anatomy Difinition Left main coronary artery (LMCA): The proximal segment RCA AV LAD LM LCX of the left coronary
Anatomy and Pathology of Left main coronary artery G Nakazawa Tokai Univ. Kanagawa, Japan 1 Anatomy Difinition Left main coronary artery (LMCA): The proximal segment RCA AV LAD LM LCX of the left coronary
September Peter Barlis. Royal Brompton Hospital, London, UK
 3rd EBC Meeting European Bifurcation Club September 2007 PALAU DE LA MUSICA, SalaRodrigo VALENCIA, SPAIN Culotte Technique in Left Main Disease Peter Barlis Carlo DiMario Royal Brompton Hospital, London,
3rd EBC Meeting European Bifurcation Club September 2007 PALAU DE LA MUSICA, SalaRodrigo VALENCIA, SPAIN Culotte Technique in Left Main Disease Peter Barlis Carlo DiMario Royal Brompton Hospital, London,
Complex Coronary Interventions: Bifurcations. John M. Lasala MD PhD Professor of Medicine Washington University St Louis, Missouri
 Complex Coronary Interventions: Bifurcations John M. Lasala MD PhD Professor of Medicine Washington University St Louis, Missouri Disclosures Advisory Board Boston Scientific, St. Jude Medical Speaker-
Complex Coronary Interventions: Bifurcations John M. Lasala MD PhD Professor of Medicine Washington University St Louis, Missouri Disclosures Advisory Board Boston Scientific, St. Jude Medical Speaker-
Journal of the American College of Cardiology Vol. 34, No. 4, by the American College of Cardiology ISSN /99/$20.
 Journal of the American College of Cardiology Vol. 34, No. 4, 1999 1999 by the American College of Cardiology ISSN 0735-1097/99/$20.00 Published by Elsevier Science Inc. PII S0735-1097(99)00324-1 Final
Journal of the American College of Cardiology Vol. 34, No. 4, 1999 1999 by the American College of Cardiology ISSN 0735-1097/99/$20.00 Published by Elsevier Science Inc. PII S0735-1097(99)00324-1 Final
Department of Internal Medicine, Saitama Citizens Medical Center, Saitama , Japan
 Case Reports in Cardiology Volume 2016, Article ID 8790347, 5 pages http://dx.doi.org/10.1155/2016/8790347 Case Report GuideLiner Catheter Use for Percutaneous Intervention Involving Anomalous Origin of
Case Reports in Cardiology Volume 2016, Article ID 8790347, 5 pages http://dx.doi.org/10.1155/2016/8790347 Case Report GuideLiner Catheter Use for Percutaneous Intervention Involving Anomalous Origin of
HKSTENT 2012: 2012/3/3-4 11:47 12:17 CTO Complication
 HKSTENT 2012: 2012/3/3-4 11:47 12:17 CTO Complication SATORU SUMITSUJI MD. FACC. Specially Appointed Associate Professor Advanced Cardiovascular Therapeutics, Osaka University Director of Heart Center,
HKSTENT 2012: 2012/3/3-4 11:47 12:17 CTO Complication SATORU SUMITSUJI MD. FACC. Specially Appointed Associate Professor Advanced Cardiovascular Therapeutics, Osaka University Director of Heart Center,
Form 4: Coronary Evaluation
 Page of 7 Patient Details Hidden Show Show/Hide Annotations Stickies: Toggle All Toggle Open Toggle Resolved Form : Coronary Evaluation Print this Form t Started Date of Coronary Evaluation Coronary Evaluation
Page of 7 Patient Details Hidden Show Show/Hide Annotations Stickies: Toggle All Toggle Open Toggle Resolved Form : Coronary Evaluation Print this Form t Started Date of Coronary Evaluation Coronary Evaluation
ΣΥΜΠΛΟΚΕΣ ΑΓΓΕΙΟΠΛΑΣΤΙΚΕΣ ΑΓΓΕΙΟΠΛΑΣΤΙΚΗ ΔΙΧΑΣΜΩΝ
 ΣΥΜΠΛΟΚΕΣ ΑΓΓΕΙΟΠΛΑΣΤΙΚΕΣ ΑΓΓΕΙΟΠΛΑΣΤΙΚΗ ΔΙΧΑΣΜΩΝ DR ΝΙΚΟΛΑΟΣ ΚΑΥΚΑΣ MD, FESC Διευθυντής, Υπεύθυνος Αιμοδ/κού Εργαστηρίου Καρδιολογική Κλινική Γεν. Νοσοκομείο ΚΑΤ-ΕΚΑ PCI in Coronary Bifurcations Bifurcations
ΣΥΜΠΛΟΚΕΣ ΑΓΓΕΙΟΠΛΑΣΤΙΚΕΣ ΑΓΓΕΙΟΠΛΑΣΤΙΚΗ ΔΙΧΑΣΜΩΝ DR ΝΙΚΟΛΑΟΣ ΚΑΥΚΑΣ MD, FESC Διευθυντής, Υπεύθυνος Αιμοδ/κού Εργαστηρίου Καρδιολογική Κλινική Γεν. Νοσοκομείο ΚΑΤ-ΕΚΑ PCI in Coronary Bifurcations Bifurcations
Stents selection and optimal implantation: sizes, design, deployment Abbott Vascular. All rights reserved.
 Stents selection and optimal implantation: sizes, design, deployment Stent classification: Mechanism of expansion - Self-expanding - Balloon expandable Design - Mesh structure - Coil - Slotted tube - Ring
Stents selection and optimal implantation: sizes, design, deployment Stent classification: Mechanism of expansion - Self-expanding - Balloon expandable Design - Mesh structure - Coil - Slotted tube - Ring
CARDIAC AND CORONARY ARTERY ANATOMY NO DISCLOSURES. Axial Anatomy of Heart. Axial Anatomy of Heart. Axial Anatomy of Heart
 CARDIAC AND CORONARY ARTERY ANATOMY NO DISCLOSURES NASCI MEETING, ORLANDO FLORIDA 2009 KOSTAKI G. BIS, MD, FACR DEPARTMENT OF RADIOLOGY WILLIAM BEAUMONT HOSPITAL Royal Oak, Michigan OBJECTIVES CARDIAC
CARDIAC AND CORONARY ARTERY ANATOMY NO DISCLOSURES NASCI MEETING, ORLANDO FLORIDA 2009 KOSTAKI G. BIS, MD, FACR DEPARTMENT OF RADIOLOGY WILLIAM BEAUMONT HOSPITAL Royal Oak, Michigan OBJECTIVES CARDIAC
Procedure of PCI. Tangshan Gongren Hospital. Hebei Medical University
 Spiral Dissection of RCA in Procedure of PCI Side branch guided to find out the true lumen Tangshan Gongren Hospital 唐山工人医院 Hebei Medical University Zheng Ji, MD History Male, 60y Chief complain:paroxysmal
Spiral Dissection of RCA in Procedure of PCI Side branch guided to find out the true lumen Tangshan Gongren Hospital 唐山工人医院 Hebei Medical University Zheng Ji, MD History Male, 60y Chief complain:paroxysmal
Kurdistan Technique for the Treatment of Unprotected Trifurcation Left Main Stem Coronary Artery Lesion: Case Report
 World Journal of Cardiovascular Diseases, 2014, 4, 483-491 Published Online August 2014 in SciRes. http://www.scirp.org/journal/wjcd http://dx.doi.org/10.4236/wjcd.2014.49058 Kurdistan Technique for the
World Journal of Cardiovascular Diseases, 2014, 4, 483-491 Published Online August 2014 in SciRes. http://www.scirp.org/journal/wjcd http://dx.doi.org/10.4236/wjcd.2014.49058 Kurdistan Technique for the
(EU), FACC (USA), FSCAI (USA)
, FACC (USA), FSCAI (USA)") How to reduce vascular complications of TAVI Paul TL Chiam MBBS (S pore), MMed, MRCP (UK), FAMS FRCP (Edin), FESC (EU), FACC (USA), FSCAI (USA) Cardiologist Mount Elizabeth Hospital Singapore Definition
How to reduce vascular complications of TAVI Paul TL Chiam MBBS (S pore), MMed, MRCP (UK), FAMS FRCP (Edin), FESC (EU), FACC (USA), FSCAI (USA) Cardiologist Mount Elizabeth Hospital Singapore Definition
JETSTREAM Atherectomy System DELIVERING VERSATILITY TO RESTORE FLOW
 JETSTREAM Atherectomy System DELIVERING VERSATILITY TO RESTORE FLOW DISCOVER THE VALUE OF VERSATILITY Versatility means not having to guess the morphology! Peripheral arterial lesions can present with
JETSTREAM Atherectomy System DELIVERING VERSATILITY TO RESTORE FLOW DISCOVER THE VALUE OF VERSATILITY Versatility means not having to guess the morphology! Peripheral arterial lesions can present with
Patient. Clinical data Indications: Operation date. Comorbidities: Patient code Birth date: / /
 Patient Patient code Birth date: / / Sex: Male Height (cm): Female Weight (kg): Risk Factors: Family history of coronary disease: Hypertension Dyslipidemia Peripheral disease Diabetes Comorbidities: No
Patient Patient code Birth date: / / Sex: Male Height (cm): Female Weight (kg): Risk Factors: Family history of coronary disease: Hypertension Dyslipidemia Peripheral disease Diabetes Comorbidities: No
Coronary angiography and PCI
 Coronary arteries Coronary angiography and PCI Samo Granda, Franjo Naji Department of Cardiology Clinical department of internal medicine University clinical centre Maribor Coronary arteries Atherosclerosis
Coronary arteries Coronary angiography and PCI Samo Granda, Franjo Naji Department of Cardiology Clinical department of internal medicine University clinical centre Maribor Coronary arteries Atherosclerosis
PCI for Left Main Coronary Artery Stenosis. Jean Fajadet Clinique Pasteur, Toulouse, France
 PCI for Left Main Coronary Artery Stenosis Jean Fajadet Clinique Pasteur, Toulouse, France Athens, October 19, 2018 Left Main Coronary Artery Disease Significant unprotected left main coronary artery disease
PCI for Left Main Coronary Artery Stenosis Jean Fajadet Clinique Pasteur, Toulouse, France Athens, October 19, 2018 Left Main Coronary Artery Disease Significant unprotected left main coronary artery disease
Catheter induced left main coronary artery stenosis: A rare complication of percutaneous coronary intervention
 Siddiqui et al. 5 CASE SERIES OPEN ACCESS Catheter induced left main coronary artery stenosis: A rare complication of percutaneous coronary intervention Muhammad Shamim Siddiqui, Syed Muhammad Faisal Hussain,
Siddiqui et al. 5 CASE SERIES OPEN ACCESS Catheter induced left main coronary artery stenosis: A rare complication of percutaneous coronary intervention Muhammad Shamim Siddiqui, Syed Muhammad Faisal Hussain,