Anatomy & Physiology
|
|
|
- Alannah Simpson
- 5 years ago
- Views:
Transcription



1 1
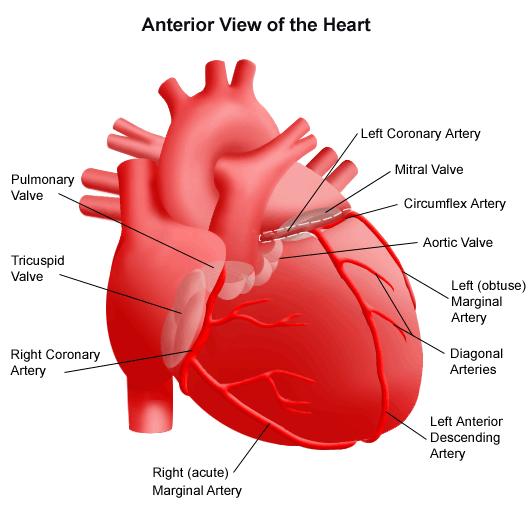
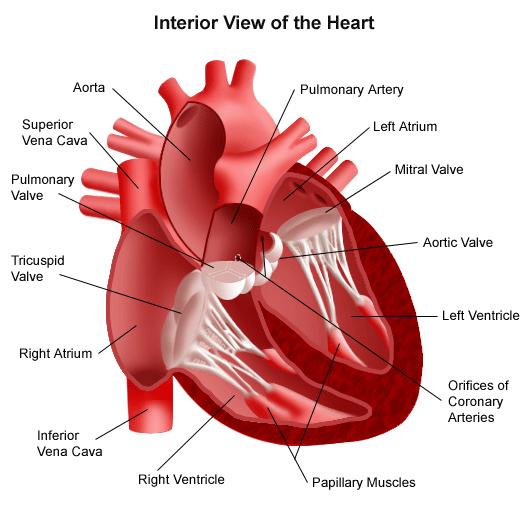
2 Anatomy & Physiology Heart is divided into four chambers, two atrias & two ventricles. Atrioventricular valves (tricuspid & mitral) separate the atria from ventricles. they open & close to control flow of blood into ventricles. The simelunar valve (pulmonary & aortic), they open & close to prevent the backflow of blood to ventricles. The pulmonary artery carry deoxygenated blood from right ventricle to lungs, after process of gas exchange occur, oxygenated blood is transmitted again into left atrium by pulmonary veins and through mitral valve to the left ventricle. And then to the body by aorta. 2
3 3
4 4
5 5
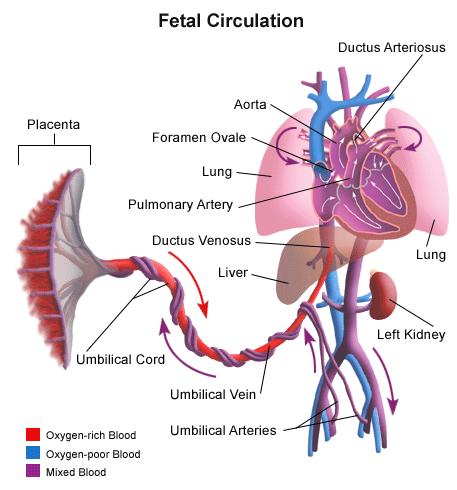
6 Fetal Circulation During pregnancy blood is transferred from placenta through umbilical vein into the ductus venosus (opining into the inferior vena cava). Then blood is carried to the right atrium in which is forced into the left atrium by an opining between the two atriums called foramen ovale. Blood is transferred into the left ventricles and to the whole body through aorta. Some blood pass into the right ventricle, in which it moved to the lungs by the pulmonary artery. But, the majority of this blood pass into the aorta by an opining between aorta & pulmonary artery called ductus atreriousus. 6
7 7
8 After birth, the newborn start breathing which increase the lung expansion, helping in shifting of blood into the lungs by the pulmonary artery not into the aorta by the ductus arteriosus as during pregnancy. This will lead to increase pulmonary blood flow & decrease pulmonary vascular resistance. Also leading to increase blood returned to the left atrium through pulmonary veins & this leads to increase pressure in the left atrium. The increasing pressure stimulate the closure of the foramen ovale and. Ductus arteriosus close in response to increase O2 saturation after hours and permanently after days. 8 Transition from fetal to pulmonary circulation
9 Pediatric differences 1- Cardiac functioning: The heart s muscle fibers are less develops & less organized, resulting in limited functional capacity. The heart muscle is fully developed at 5 years of age & the heart muscle fiber at 9 years of age. The heart weight increase by six times at one year. Heart rate is high due to increase metabolic rate & O2 requirements. 9
10 Laboratory tests 1. Cardiac catheterization. 2. Chest radiograph study. 3. Echocardiogram. 4. ECG 5. MRI 6. Arterial blood gases. 7. CBC 10
11 Congenital Heart Diseases Refer to a defect in the heart or great vessels or persistence of a fetal structure after birth. Most of the CHD develops during the first 8 weeks of gestation. Some genetic or environmental factors found to be related to the CHD, such as: 1. Fetal exposure to drugs such as warfarin, lithium, alcohol. 2. Maternal viral infection such as rubella. 3. Genetic factors. 4. Chromosomal abnormalities such as Down syndrome. 5. Maternal complication during pregnancy. 11
12 Classifications CHD previously were categorized as to whether the child have or did not have cyanosis (cyanotic or acyanotic). But now they are classified according to their pathophysiology & hemodynamics. Theses categories include The following: 1. Increase pulmonary blood flow 2. Decreased pulmonary blood flow. 3. Obstructed systemic blood flow. 4. Mixed defects in which infant survival is dependent upon mixing of systemic & pulmonary blood. 12
13 CHD that increase pulmonary blood flow These defects includes: 1. Patent ductus arteriosus. 2. Atrial septal defect 3. Ventricular septal defect 13
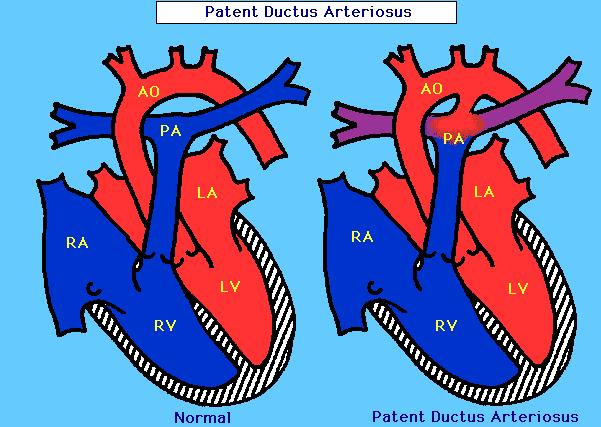
14 Patent ductus arteriosus (PDA) Pathophysiology: In this anomaly, the ductus arteriosus does not close after birth. Leading blood to shift from aorta to the pulmonary artery ( because the pressure in the aorta is higher than it in the pulmonary artery). Leading to increase blood shunted into the lungs and increased pulmonary vascular resistance & pulmonary blood pressure in response. This will leads to right ventricular hypertrophy to overcome the increasing pulmonary vascular resistance & deliver the blood to the lungs. 14
15 15
16 It is a common problem in preterm infants & present in nearly all preterm infant less than 27 weeks gestation Clinical manifestations: Dyspnea; tachycardia; full, bounding pulse; hypotension, crackles. Intercostal retractions & growth retardation. Contentious murmur in diastole & systole. Diagnostic procedure: Chest radiograph; ECG; will show left & right ventricular hypertrophy. 16

17 Clinical Therapy Surgical ligation of PDA. Intravenous indomethacin often stimulate the closure of the ductus atreriosus. Thranscatheter closure by obstructive device is needed in children over 18 months. Prognosis: No long term interventions if treated before pulmonary vascular disease develops. 17
18 Arterial Septal Defect (ASD) It is an opening in the atrial septum that permits left to right shunting of blood. It can be small as when the foramen ovale fail to close, or large as when the septum may be completely absent. As the pressure in the left atrium is higher than in the right atrium; blood will shifts from the left to the right atrium. Leading to increase pressure on pulmonary system & right sided hypertrophy. 18
19 19
20 Clinical manifestations: Infant & young children may have no symptoms, small to moderate size ASDs may not be diagnosed until preschool years or later. CHF, easy tiring, poor growth in large ASDs. Diagnostic procedure: Echocardiogram identified dilated right ventricle. Radiograph & ECG reviles right sided hypertrophy. 20

21 Clinical Therapy Spontaneous closure occur within the first 4 years of life. surgery is needed when symptoms of CHF occur. Prognosis: if not treated, person may develop signs of CHF. 21
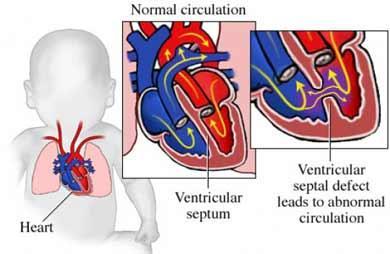
22 Ventricular Septal Defect (VSD) An opening in the ventricular septum leads blood to shunts from the left ventricle to the right ventricle. Leading to increase pressure in the right side of the heart, hypertrophy occur in response. Clinical manifestations: Only large VSDs causes symptoms of CHF. Systolic murmur is heard. 22
23 23

24 Diagnostic procedures: Echocardiogram identified dilated right ventricle. Radiograph & ECG reviles right & left sided hypertrophy. Treatment: Small VSDs lose within 6 months of life. Surgical patch is used when poor growth is evident. Closure of VSD by catheterization. Prognosis: Highest risk associated with surgical repair in the few months of life. 24
25 Nursing interventions for defects that increase pulmonary blood flow Psychological assessment. Assess parents needs. Psychosocial support. Genetic counseling for future pregnancy Pain management ( after surgery), e.g. use a pillow or stuffed animal held against the chest to reduce the pain from coughing & deep breathing. Promote respiratory function. Chest physiotherapy. Mange fluid & nutrition, encourage parents to bring favored food to the child if he tolerate it. 25

26 CHD that decreased pulmonary blood flow & mixed defects ## defects that decrease pulmonary flow: 1. Pulmonic stenosis. 2. Tetrology of fallot. 3. Tricuspid atresia. 4. Pulmonary atresia. ## Mixed defects: 1. Coarctation of aorta. 2. Aortic stenosis. 3. Mitral stenosis. 26
27 Pathophysiology: Pulmonic stenosis. Stenosis in the pulmonic valve. The stenosis can be at the valve area, above or below it. The stenosis obstruct the blood flow into the pulmonary artery leading to increased preload (the volume of blood in ventricles at the end of diastole). leading to right ventricle hypertrophy. 27

28 Pulmonary stenosis 28

29 Normal valve Pulmonary stenosis 29
30 Clinical manifestations: Children with mild stenosis have no symptoms. In moderate stenosis, dyspnea & fatigue occur on exertion. In sever cases, heart failure & chest pain occur with exertion. Load systolic murmur is heard. Thrill is felt in the pulmonic area. Diagnostic tests: Chest radiograph show an enlarged pulmonary artery with normal heart size. The ECG show right sided hypertrophy. 30

31 Clinical Therapy Dilation by balloon valvuloplasty, performed during cardiac catheterization. Surgical valvotomy is used with other defects presents such as VSD. Prognosis: It does not increase in severity, lifelong infective endocarditis prophylaxis is necessary. 31
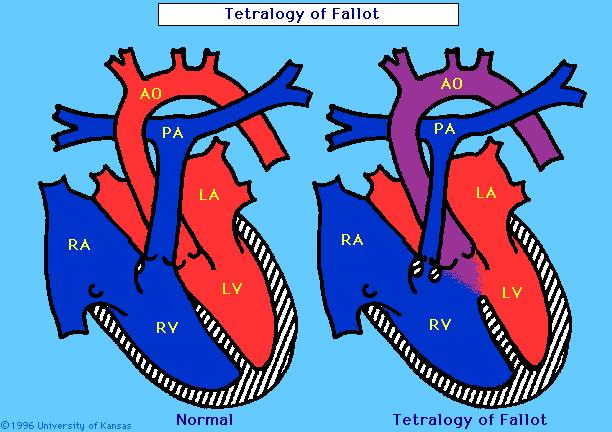
32 Tetrology of fallot It consists of four defects: pulmonary stenosis, right ventricular hypertrophy, ventricular septal defect (VSD), & overriding of the aorta. Some children have fifth defect, an open foramen ovale. Presence of VSD leads blood to shunt from left ventricle to the right ventricle increase pressure in right ventricle hypertrophy. Presence of pulmonary stenosis leads to increase accumulation of blood in right ventricle increase pressure in right ventricle hypertrophy. 32
33 33

34 Tetrology of fallot 34
35 Clinical Manifestation Hypoxia; cyanosis. Systolic murmur is heard in the pulmonic area. Thrill is palpated in the palmonic area. poor growth. Clubbing nail. Hypoxia episodes. Metabolic acidosis. Toddler with uncorrected or partially corrected defect, assume knee to chest position to decrease venous return. 35
36 Diagnostic tests: Chest radiograph. The ECG shows right ventricular hypertrophy. The echocardiogram shows the VSD, the size of the pulmonary artery. Cardiac catheterization provides details about the anatomic defects. Clinical therapy: Treating he cyanotic episodes by placing the child on knee-chest position, giving oxygen. Total repair performed before the age of 6 months when the infant has hypercyanotic episode. 36
CONGENITAL HEART DISEASE (CHD)
") CONGENITAL HEART DISEASE (CHD) DEFINITION It is the result of a structural or functional abnormality of the cardiovascular system at birth GENERAL FEATURES OF CHD Structural defects due to specific disturbance
CONGENITAL HEART DISEASE (CHD) DEFINITION It is the result of a structural or functional abnormality of the cardiovascular system at birth GENERAL FEATURES OF CHD Structural defects due to specific disturbance
Congenital heart disease. By Dr Saima Ali Professor of pediatrics
 Congenital heart disease By Dr Saima Ali Professor of pediatrics What is the most striking clinical finding in this child? Learning objectives By the end of this lecture, final year student should be able
Congenital heart disease By Dr Saima Ali Professor of pediatrics What is the most striking clinical finding in this child? Learning objectives By the end of this lecture, final year student should be able
Uptofate Study Summary
 CONGENITAL HEART DISEASE Uptofate Study Summary Acyanotic Atrial septal defect Ventricular septal defect Patent foramen ovale Patent ductus arteriosus Aortic coartation Pulmonary stenosis Cyanotic Tetralogy
CONGENITAL HEART DISEASE Uptofate Study Summary Acyanotic Atrial septal defect Ventricular septal defect Patent foramen ovale Patent ductus arteriosus Aortic coartation Pulmonary stenosis Cyanotic Tetralogy
Paediatric Cardiology. Acyanotic CHD. Prof F F Takawira
 Paediatric Cardiology Acyanotic CHD Prof F F Takawira Aetiology Chromosomal Down syndrome, T13, T18 Genetic syndromes (gene defects) Velo-Cardio-facial (22 del) Genetic syndromes (undefined aetiology)
Paediatric Cardiology Acyanotic CHD Prof F F Takawira Aetiology Chromosomal Down syndrome, T13, T18 Genetic syndromes (gene defects) Velo-Cardio-facial (22 del) Genetic syndromes (undefined aetiology)
By Dickens ATURWANAHO & ORIBA DAN LANGOYA MAKchs, MBchB CONGENTAL HEART DISEASE
 By Dickens ATURWANAHO & ORIBA DAN LANGOYA MAKchs, MBchB CONGENTAL HEART DISEASE Introduction CHDs are abnormalities of the heart or great vessels that are present at birth. Common type of heart disease
By Dickens ATURWANAHO & ORIBA DAN LANGOYA MAKchs, MBchB CONGENTAL HEART DISEASE Introduction CHDs are abnormalities of the heart or great vessels that are present at birth. Common type of heart disease
Congenital Heart Disease: Physiology and Common Defects
 Congenital Heart Disease: Physiology and Common Defects Jamie S. Sutherell, M.D, M.Ed. Associate Professor, Pediatrics Division of Cardiology Director, Medical Student Education in Pediatrics Director,
Congenital Heart Disease: Physiology and Common Defects Jamie S. Sutherell, M.D, M.Ed. Associate Professor, Pediatrics Division of Cardiology Director, Medical Student Education in Pediatrics Director,
Large Arteries of Heart
 Cardiovascular System (Part A-2) Module 5 -Chapter 8 Overview Arteries Capillaries Veins Heart Anatomy Conduction System Blood pressure Fetal circulation Susie Turner, M.D. 1/5/13 Large Arteries of Heart
Cardiovascular System (Part A-2) Module 5 -Chapter 8 Overview Arteries Capillaries Veins Heart Anatomy Conduction System Blood pressure Fetal circulation Susie Turner, M.D. 1/5/13 Large Arteries of Heart
Heart and Lungs. LUNG Coronal section demonstrates relationship of pulmonary parenchyma to heart and chest wall.
 Heart and Lungs Normal Sonographic Anatomy THORAX Axial and coronal sections demonstrate integrity of thorax, fetal breathing movements, and overall size and shape. LUNG Coronal section demonstrates relationship
Heart and Lungs Normal Sonographic Anatomy THORAX Axial and coronal sections demonstrate integrity of thorax, fetal breathing movements, and overall size and shape. LUNG Coronal section demonstrates relationship
Pathophysiology: Left To Right Shunts
 Pathophysiology: Left To Right Shunts Daphne T. Hsu, MD dh17@columbia.edu Learning Objectives Learn the relationships between pressure, blood flow, and resistance Review the transition from fetal to mature
Pathophysiology: Left To Right Shunts Daphne T. Hsu, MD dh17@columbia.edu Learning Objectives Learn the relationships between pressure, blood flow, and resistance Review the transition from fetal to mature
Screening for Critical Congenital Heart Disease
 Screening for Critical Congenital Heart Disease Caroline K. Lee, MD Pediatric Cardiology Disclosures I have no relevant financial relationships or conflicts of interest 1 Most Common Birth Defect Most
Screening for Critical Congenital Heart Disease Caroline K. Lee, MD Pediatric Cardiology Disclosures I have no relevant financial relationships or conflicts of interest 1 Most Common Birth Defect Most
Slide 1. Slide 2. Slide 3 CONGENITAL HEART DISEASE. Papworth Hospital NHS Trust INTRODUCTION. Jakub Kadlec/Catherine Sudarshan INTRODUCTION
 Slide 1 CONGENITAL HEART DISEASE Jakub Kadlec/Catherine Sudarshan NHS Trust Slide 2 INTRODUCTION Most common congenital illness in the newborn Affects about 4 9 / 1000 full-term live births in the UK 1.5
Slide 1 CONGENITAL HEART DISEASE Jakub Kadlec/Catherine Sudarshan NHS Trust Slide 2 INTRODUCTION Most common congenital illness in the newborn Affects about 4 9 / 1000 full-term live births in the UK 1.5
Paediatrics Revision Session Cardiology. Emma Walker 7 th May 2016
 Paediatrics Revision Session Cardiology Emma Walker 7 th May 2016 Cardiovascular Examination! General:! Make it fun!! Change how you act depending on their age! Introduction! Introduce yourself & check
Paediatrics Revision Session Cardiology Emma Walker 7 th May 2016 Cardiovascular Examination! General:! Make it fun!! Change how you act depending on their age! Introduction! Introduce yourself & check
Pathophysiology: Left To Right Shunts
 Pathophysiology: Left To Right Shunts Daphne T. Hsu, MD dh17@columbia.edu Learning Objectives Learn the relationships between pressure, blood flow, and resistance Review the transition from fetal to mature
Pathophysiology: Left To Right Shunts Daphne T. Hsu, MD dh17@columbia.edu Learning Objectives Learn the relationships between pressure, blood flow, and resistance Review the transition from fetal to mature
5.8 Congenital Heart Disease
 5.8 Congenital Heart Disease Congenital heart diseases (CHD) refer to structural or functional heart diseases, which are present at birth. Some of these lesions may be discovered later. prevalence of Chd
5.8 Congenital Heart Disease Congenital heart diseases (CHD) refer to structural or functional heart diseases, which are present at birth. Some of these lesions may be discovered later. prevalence of Chd
Congenital Heart Defects
 Normal Heart Congenital Heart Defects 1. Patent Ductus Arteriosus The ductus arteriosus connects the main pulmonary artery to the aorta. In utero, it allows the blood leaving the right ventricle to bypass
Normal Heart Congenital Heart Defects 1. Patent Ductus Arteriosus The ductus arteriosus connects the main pulmonary artery to the aorta. In utero, it allows the blood leaving the right ventricle to bypass
PATENT DUCTUS ARTERIOSUS (PDA)
") PATENT DUCTUS ARTERIOSUS (PDA) It is a channel that connect the pulmonary artery with the descending aorta (isthumus part). It results from the persistence of patency of the fetal ductus arteriosus after
PATENT DUCTUS ARTERIOSUS (PDA) It is a channel that connect the pulmonary artery with the descending aorta (isthumus part). It results from the persistence of patency of the fetal ductus arteriosus after
Index. cardiology.theclinics.com. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A ACHD. See Adult congenital heart disease (ACHD) Adult congenital heart disease (ACHD), 503 512 across life span prevalence of, 504 506
Index Note: Page numbers of article titles are in boldface type. A ACHD. See Adult congenital heart disease (ACHD) Adult congenital heart disease (ACHD), 503 512 across life span prevalence of, 504 506
Congenital heart disease: When to act and what to do?
 Leading Article Congenital heart disease: When to act and what to do? Duminda Samarasinghe 1 Sri Lanka Journal of Child Health, 2010; 39: 39-43 (Key words: Congenital heart disease) Congenital heart disease
Leading Article Congenital heart disease: When to act and what to do? Duminda Samarasinghe 1 Sri Lanka Journal of Child Health, 2010; 39: 39-43 (Key words: Congenital heart disease) Congenital heart disease
2) VSD & PDA - Dr. Aso
 VSD & PDA - Dr. Aso") 2) VSD & PDA - Dr. Aso Ventricular Septal Defect (VSD) Most common cardiac malformation 25-30 % Types of VSD: According to position perimembranous, inlet, muscular. According to size small, medium, large.
2) VSD & PDA - Dr. Aso Ventricular Septal Defect (VSD) Most common cardiac malformation 25-30 % Types of VSD: According to position perimembranous, inlet, muscular. According to size small, medium, large.
Absent Pulmonary Valve Syndrome
 Absent Pulmonary Valve Syndrome Fact sheet on Absent Pulmonary Valve Syndrome In this condition, which has some similarities to Fallot's Tetralogy, there is a VSD with narrowing at the pulmonary valve.
Absent Pulmonary Valve Syndrome Fact sheet on Absent Pulmonary Valve Syndrome In this condition, which has some similarities to Fallot's Tetralogy, there is a VSD with narrowing at the pulmonary valve.
Nursing Care of Children and their Families: Alterations in Cardiac Function
 Nursing Care of Children and their Families: Alterations in Cardiac Function Congenital Heart Disease Incidence 4-10 per live births Extra cardiac defects: TE fistula, renal agenesis and diaphragmatic
Nursing Care of Children and their Families: Alterations in Cardiac Function Congenital Heart Disease Incidence 4-10 per live births Extra cardiac defects: TE fistula, renal agenesis and diaphragmatic
Cardiovascular Pathophysiology: Right to Left Shunts aka Cyanotic Lesions
 Cardiovascular Pathophysiology: Right to Left Shunts aka Cyanotic Lesions Ismee A. Williams, MD, MS iib6@columbia.edu Pediatric Cardiology Learning Objectives To discuss the hemodynamic significance of
Cardiovascular Pathophysiology: Right to Left Shunts aka Cyanotic Lesions Ismee A. Williams, MD, MS iib6@columbia.edu Pediatric Cardiology Learning Objectives To discuss the hemodynamic significance of
Cardiovascular Pathophysiology: Right to Left Shunts aka Cyanotic Lesions Ismee A. Williams, MD, MS Pediatric Cardiology
 Cardiovascular Pathophysiology: Right to Left Shunts aka Cyanotic Lesions Ismee A. Williams, MD, MS iib6@columbia.edu Pediatric Cardiology Learning Objectives To discuss the hemodynamic significance of
Cardiovascular Pathophysiology: Right to Left Shunts aka Cyanotic Lesions Ismee A. Williams, MD, MS iib6@columbia.edu Pediatric Cardiology Learning Objectives To discuss the hemodynamic significance of
Adult Echocardiography Examination Content Outline
 Adult Echocardiography Examination Content Outline (Outline Summary) # Domain Subdomain Percentage 1 2 3 4 5 Anatomy and Physiology Pathology Clinical Care and Safety Measurement Techniques, Maneuvers,
Adult Echocardiography Examination Content Outline (Outline Summary) # Domain Subdomain Percentage 1 2 3 4 5 Anatomy and Physiology Pathology Clinical Care and Safety Measurement Techniques, Maneuvers,
Patent ductus arteriosus PDA
 Patent ductus arteriosus PDA Is connecting between the aortic end just distal to the origin of the LT sub clavian artery& the pulmonary artery at its bifurcation. Female/male ratio is 2:1 and it is more
Patent ductus arteriosus PDA Is connecting between the aortic end just distal to the origin of the LT sub clavian artery& the pulmonary artery at its bifurcation. Female/male ratio is 2:1 and it is more
Congenital Heart Disease
 Congenital Heart Disease Mohammed Alghamdi, MD, FRCPC, FAAP, FACC Associate Professor and Consultant Pediatric Cardiology, Cardiac Science King Fahad Cardiac Centre King Saud University INTRODUCTION CHD
Congenital Heart Disease Mohammed Alghamdi, MD, FRCPC, FAAP, FACC Associate Professor and Consultant Pediatric Cardiology, Cardiac Science King Fahad Cardiac Centre King Saud University INTRODUCTION CHD
CongHeartDis.doc. Андрій Миколайович Лобода
 CongHeartDis.doc Андрій Миколайович Лобода 2015 Зміст 3 Зміст Зміст 4 A child with tetralogy of Fallot is most likely to exhibit: -Increased pulmonary blood flow -Increased pressure in the right ventricle
CongHeartDis.doc Андрій Миколайович Лобода 2015 Зміст 3 Зміст Зміст 4 A child with tetralogy of Fallot is most likely to exhibit: -Increased pulmonary blood flow -Increased pressure in the right ventricle
When is Risky to Apply Oxygen for Congenital Heart Disease 부천세종병원 소아청소년과최은영
 When is Risky to Apply Oxygen for Congenital Heart Disease 부천세종병원 소아청소년과최은영 The Korean Society of Cardiology COI Disclosure Eun-Young Choi The author have no financial conflicts of interest to disclose
When is Risky to Apply Oxygen for Congenital Heart Disease 부천세종병원 소아청소년과최은영 The Korean Society of Cardiology COI Disclosure Eun-Young Choi The author have no financial conflicts of interest to disclose
Notes by Sandra Dankwa 2009 HF- Heart Failure DS- Down Syndrome IE- Infective Endocarditis ET- Exercise Tolerance. Small VSD Symptoms -asymptomatic
 Congenital Heart Disease: Notes. Condition Pathology PC Ix Rx Ventricular septal defect (VSD) L R shuntsdefect anywhere in the ventricle, usually perimembranous (next to the tricuspid valve) 30% 1)small
Congenital Heart Disease: Notes. Condition Pathology PC Ix Rx Ventricular septal defect (VSD) L R shuntsdefect anywhere in the ventricle, usually perimembranous (next to the tricuspid valve) 30% 1)small
Cardiac Emergencies in Infants. Michael Luceri, DO
 Cardiac Emergencies in Infants Michael Luceri, DO October 7, 2017 I have no financial obligations or conflicts of interest to disclose. Objectives Understand the scope of congenital heart disease Recognize
Cardiac Emergencies in Infants Michael Luceri, DO October 7, 2017 I have no financial obligations or conflicts of interest to disclose. Objectives Understand the scope of congenital heart disease Recognize
ECHOCARDIOGRAPHIC APPROACH TO CONGENITAL HEART DISEASE: THE UNOPERATED ADULT
 ECHOCARDIOGRAPHIC APPROACH TO CONGENITAL HEART DISEASE: THE UNOPERATED ADULT Karen Stout, MD, FACC Divisions of Cardiology University of Washington Medical Center Seattle Children s Hospital NO DISCLOSURES
ECHOCARDIOGRAPHIC APPROACH TO CONGENITAL HEART DISEASE: THE UNOPERATED ADULT Karen Stout, MD, FACC Divisions of Cardiology University of Washington Medical Center Seattle Children s Hospital NO DISCLOSURES
HISTORY. Question: What category of heart disease is suggested by this history? CHIEF COMPLAINT: Heart murmur present since early infancy.
 HISTORY 18-year-old man. CHIEF COMPLAINT: Heart murmur present since early infancy. PRESENT ILLNESS: Although normal at birth, a heart murmur was heard at the six week check-up and has persisted since
HISTORY 18-year-old man. CHIEF COMPLAINT: Heart murmur present since early infancy. PRESENT ILLNESS: Although normal at birth, a heart murmur was heard at the six week check-up and has persisted since
بسم هللا الرحمن الرحيم. The cardio vascular system By Dr.Rawa Younis Mahmood
 بسم هللا الرحمن الرحيم The cardio vascular system By Dr.Rawa Younis Mahmood Introduction Evaluation of the cardio vascular system depend on history and physical examination by : Asking about cyanosis,blueness
بسم هللا الرحمن الرحيم The cardio vascular system By Dr.Rawa Younis Mahmood Introduction Evaluation of the cardio vascular system depend on history and physical examination by : Asking about cyanosis,blueness
Pediatric Echocardiography Examination Content Outline
 Pediatric Echocardiography Examination Content Outline (Outline Summary) # Domain Subdomain Percentage 1 Anatomy and Physiology Normal Anatomy and Physiology 10% 2 Abnormal Pathology and Pathophysiology
Pediatric Echocardiography Examination Content Outline (Outline Summary) # Domain Subdomain Percentage 1 Anatomy and Physiology Normal Anatomy and Physiology 10% 2 Abnormal Pathology and Pathophysiology
Cardiology Competency Based Goals and Objectives
 Cardiology Competency Based Goals and Objectives COMPETENCY 1. Patient Care. Provide family centered patient care that is developmentally and age appropriate, compassionate, and effective for the treatment
Cardiology Competency Based Goals and Objectives COMPETENCY 1. Patient Care. Provide family centered patient care that is developmentally and age appropriate, compassionate, and effective for the treatment
HISTORY. Question: What type of heart disease is suggested by this history? CHIEF COMPLAINT: Decreasing exercise tolerance.
 HISTORY 15-year-old male. CHIEF COMPLAINT: Decreasing exercise tolerance. PRESENT ILLNESS: A heart murmur was noted in childhood, but subsequent medical care was sporadic. Easy fatigability and slight
HISTORY 15-year-old male. CHIEF COMPLAINT: Decreasing exercise tolerance. PRESENT ILLNESS: A heart murmur was noted in childhood, but subsequent medical care was sporadic. Easy fatigability and slight
The sinus venosus represent the venous end of the heart It receives 3 veins: 1- Common cardinal vein body wall 2- Umbilical vein from placenta 3-
 1 2 The sinus venosus represent the venous end of the heart It receives 3 veins: 1- Common cardinal vein body wall 2- Umbilical vein from placenta 3- Vitelline vein from yolk sac 3 However!!!!! The left
1 2 The sinus venosus represent the venous end of the heart It receives 3 veins: 1- Common cardinal vein body wall 2- Umbilical vein from placenta 3- Vitelline vein from yolk sac 3 However!!!!! The left
Congenital Heart Disease. Mohamed Waheed Elsharief.
 Congenital Heart Disease Mohamed Waheed Elsharief. Objectives l By the end of this lecture you should be able to Fetal Circulation l For the fetus the placenta is the oxygenator so the lungs do little
Congenital Heart Disease Mohamed Waheed Elsharief. Objectives l By the end of this lecture you should be able to Fetal Circulation l For the fetus the placenta is the oxygenator so the lungs do little
Ummeenatrbilaoiasetptiwmsaiiri
 atrial This This atrial CIRCULATORY CHANGES My My pressure In the foetus the left atrial is low as relatively Ummeenatrbilaoiasetptiwmsaiiri ze@fgffmftheyubsidtritupyeiirieminfyifjjtajefjjieiminylntentiiiarmmnitnteimiiiinc1udingfromthepl9centaj
atrial This This atrial CIRCULATORY CHANGES My My pressure In the foetus the left atrial is low as relatively Ummeenatrbilaoiasetptiwmsaiiri ze@fgffmftheyubsidtritupyeiirieminfyifjjtajefjjieiminylntentiiiarmmnitnteimiiiinc1udingfromthepl9centaj
CYANOTIC CONGENITAL HEART DISEASES. PRESENTER: DR. Myra M. Koech Pediatric cardiologist MTRH/MU
 CYANOTIC CONGENITAL HEART DISEASES PRESENTER: DR. Myra M. Koech Pediatric cardiologist MTRH/MU DEFINITION Congenital heart diseases are defined as structural and functional problems of the heart that are
CYANOTIC CONGENITAL HEART DISEASES PRESENTER: DR. Myra M. Koech Pediatric cardiologist MTRH/MU DEFINITION Congenital heart diseases are defined as structural and functional problems of the heart that are
Pathological physiology of cardiovascular system Congenital heart diseases
 Pathological physiology of cardiovascular system Congenital heart diseases Rácz Oliver, Sedláková Eva Institute of Pathological Physiology, Medical School, P.J. Šafárik University Oliver Rácz, Eva Sedláková
Pathological physiology of cardiovascular system Congenital heart diseases Rácz Oliver, Sedláková Eva Institute of Pathological Physiology, Medical School, P.J. Šafárik University Oliver Rácz, Eva Sedláková
APPROACH TO CARDIAC HISTORY TAKING. Index
 Christopher Cheung APPROACH TO CARDIAC HISTORY TAKING Index General Presentation...1 2 Table 1 Congenital Heart Conditions...2 Questions to Ask...2 Table 2 PQRSTAAA Mnemonic Approach to Chest Pain...3
Christopher Cheung APPROACH TO CARDIAC HISTORY TAKING Index General Presentation...1 2 Table 1 Congenital Heart Conditions...2 Questions to Ask...2 Table 2 PQRSTAAA Mnemonic Approach to Chest Pain...3
CONGENITAL HEART LESIONS ((C.H.L
 CONGENITAL HEART LESIONS ((C.H.L BY THE BOOKS: 0.8 IN FACT: 3-5% INCLUDING: - BICUSPID AORTIC VALVE MITRAL VALVE PROLAPSE LATE DIAGNOSIS - :INCREASED INCIDENCE IN ADULTS BETTER DIAGNOSIS IN INFANCY BETTER
CONGENITAL HEART LESIONS ((C.H.L BY THE BOOKS: 0.8 IN FACT: 3-5% INCLUDING: - BICUSPID AORTIC VALVE MITRAL VALVE PROLAPSE LATE DIAGNOSIS - :INCREASED INCIDENCE IN ADULTS BETTER DIAGNOSIS IN INFANCY BETTER
Introduction. Pediatric Cardiology. General Appearance. Tools of Assessment. Auscultation. Vital Signs
 Introduction Pediatric Cardiology An introduction to the pediatric patient with heart disease: M-III Lecture Douglas R. Allen, M.D. Assistant Professor and Director of Community Pediatric Cardiology at
Introduction Pediatric Cardiology An introduction to the pediatric patient with heart disease: M-III Lecture Douglas R. Allen, M.D. Assistant Professor and Director of Community Pediatric Cardiology at
How to Recognize a Suspected Cardiac Defect in the Neonate
 Neonatal Nursing Education Brief: How to Recognize a Suspected Cardiac Defect in the Neonate https://www.seattlechildrens.org/healthcareprofessionals/education/continuing-medical-nursing-education/neonatalnursing-education-briefs/
Neonatal Nursing Education Brief: How to Recognize a Suspected Cardiac Defect in the Neonate https://www.seattlechildrens.org/healthcareprofessionals/education/continuing-medical-nursing-education/neonatalnursing-education-briefs/
Coarctation of the aorta
 T H E P E D I A T R I C C A R D I A C S U R G E R Y I N Q U E S T R E P O R T Coarctation of the aorta In the normal heart, blood flows to the body through the aorta, which connects to the left ventricle
T H E P E D I A T R I C C A R D I A C S U R G E R Y I N Q U E S T R E P O R T Coarctation of the aorta In the normal heart, blood flows to the body through the aorta, which connects to the left ventricle
SPECIFIC HEART DEFECTS
 A. Acyanotic Defects 1. Ventricular Septal Defect (VSD): SPECIFIC HEART DEFECTS Which side of the heart is stronger? Left This is when there is an opening between the left and right ventricle (in the septum)
A. Acyanotic Defects 1. Ventricular Septal Defect (VSD): SPECIFIC HEART DEFECTS Which side of the heart is stronger? Left This is when there is an opening between the left and right ventricle (in the septum)
Journal of American Science 2014;10(9) Congenital Heart Disease in Pediatric with Down's Syndrome
 Congenital Heart Disease in Pediatric with Down's Syndrome") Journal of American Science 2014;10(9) http://www.jofamericanscience.org Congenital Heart Disease in Pediatric with Down's Syndrome Jawaher Khalid Almaimani; Maryam Faisal Zafir; Hanan Yousif Abbas and
Journal of American Science 2014;10(9) http://www.jofamericanscience.org Congenital Heart Disease in Pediatric with Down's Syndrome Jawaher Khalid Almaimani; Maryam Faisal Zafir; Hanan Yousif Abbas and
"Lecture Index. 1) Heart Progenitors. 2) Cardiac Tube Formation. 3) Valvulogenesis and Chamber Formation. 4) Epicardium Development.
 Heart Progenitors. 2) Cardiac Tube Formation. 3) Valvulogenesis and Chamber Formation. 4) Epicardium Development.") "Lecture Index 1) Heart Progenitors. 2) Cardiac Tube Formation. 3) Valvulogenesis and Chamber Formation. 4) Epicardium Development. 5) Septation and Maturation. 6) Changes in Blood Flow during Development.
"Lecture Index 1) Heart Progenitors. 2) Cardiac Tube Formation. 3) Valvulogenesis and Chamber Formation. 4) Epicardium Development. 5) Septation and Maturation. 6) Changes in Blood Flow during Development.
Heart and Soul Evaluation of the Fetal Heart
 Heart and Soul Evaluation of the Fetal Heart Ivana M. Vettraino, M.D., M.B.A. Clinical Associate Professor, Michigan State University College of Human Medicine Objectives Review the embryology of the formation
Heart and Soul Evaluation of the Fetal Heart Ivana M. Vettraino, M.D., M.B.A. Clinical Associate Professor, Michigan State University College of Human Medicine Objectives Review the embryology of the formation
HISTORY. Question: What category of heart disease is suggested by the fact that a murmur was heard at birth?
 HISTORY 23-year-old man. CHIEF COMPLAINT: Decreasing exercise tolerance of several years duration. PRESENT ILLNESS: The patient is the product of an uncomplicated term pregnancy. A heart murmur was discovered
HISTORY 23-year-old man. CHIEF COMPLAINT: Decreasing exercise tolerance of several years duration. PRESENT ILLNESS: The patient is the product of an uncomplicated term pregnancy. A heart murmur was discovered
Surgical Management Of TAPVR. Daniel A. Velez, M.D. Congenital Cardiac Surgeon Phoenix Children s Hospital
 Surgical Management Of TAPVR Daniel A. Velez, M.D. Congenital Cardiac Surgeon Phoenix Children s Hospital No Disclosures Goals Review the embryology and anatomy Review Surgical Strategies for repair Discuss
Surgical Management Of TAPVR Daniel A. Velez, M.D. Congenital Cardiac Surgeon Phoenix Children s Hospital No Disclosures Goals Review the embryology and anatomy Review Surgical Strategies for repair Discuss
Pediatric Board Review Congenital Heart Disease. Steven H. Todman, M.D. Pediatric Cardiologist Louisiana State University
 Pediatric Board Review Congenital Heart Disease Steven H. Todman, M.D. Pediatric Cardiologist Louisiana State University Our Mission To discuss various types of congenital heart disease that are commonly
Pediatric Board Review Congenital Heart Disease Steven H. Todman, M.D. Pediatric Cardiologist Louisiana State University Our Mission To discuss various types of congenital heart disease that are commonly
Echocardiography in Adult Congenital Heart Disease
 Echocardiography in Adult Congenital Heart Disease Michael Vogel Kinderherz-Praxis München CHD missed in childhood Subsequent lesions after repaired CHD Follow-up of cyanotic heart disease CHD missed in
Echocardiography in Adult Congenital Heart Disease Michael Vogel Kinderherz-Praxis München CHD missed in childhood Subsequent lesions after repaired CHD Follow-up of cyanotic heart disease CHD missed in
The blue baby. Case 4
 Case 4 The blue baby Mrs Smith has brought her baby to A&E because she says he has started turning blue. What are your immediate differential diagnoses? 1 Respiratory causes: Congenital respiratory disorder.
Case 4 The blue baby Mrs Smith has brought her baby to A&E because she says he has started turning blue. What are your immediate differential diagnoses? 1 Respiratory causes: Congenital respiratory disorder.
Notes: 1)Membranous part contribute in the formation of small portion in the septal cusp.
Membranous part contribute in the formation of small portion in the septal cusp.") Embryology 9 : Slide 16 : There is a sulcus between primitive ventricular and bulbis cordis that will disappear gradually and lead to the formation of one chamber which is called bulboventricular chamber.
Embryology 9 : Slide 16 : There is a sulcus between primitive ventricular and bulbis cordis that will disappear gradually and lead to the formation of one chamber which is called bulboventricular chamber.
Adult Congenital Heart Disease: What All Echocardiographers Should Know Sharon L. Roble, MD, FACC Echo Hawaii 2016
 1 Adult Congenital Heart Disease: What All Echocardiographers Should Know Sharon L. Roble, MD, FACC Echo Hawaii 2016 DISCLOSURES I have no disclosures relevant to today s talk 2 Why should all echocardiographers
1 Adult Congenital Heart Disease: What All Echocardiographers Should Know Sharon L. Roble, MD, FACC Echo Hawaii 2016 DISCLOSURES I have no disclosures relevant to today s talk 2 Why should all echocardiographers
Foetal Cardiology: How to predict perinatal problems. Prof. I.Witters Prof.M.Gewillig UZ Leuven
 Foetal Cardiology: How to predict perinatal problems Prof. I.Witters Prof.M.Gewillig UZ Leuven Cardiopathies Incidence : 8-12 / 1000 births ( 1% ) Most frequent - Ventricle Septum Defect 20% - Atrium Septum
Foetal Cardiology: How to predict perinatal problems Prof. I.Witters Prof.M.Gewillig UZ Leuven Cardiopathies Incidence : 8-12 / 1000 births ( 1% ) Most frequent - Ventricle Septum Defect 20% - Atrium Septum
DORV: The Great Chameleon. Heart Conference October 15, 2016 Tina Kwan, MD
 DORV: The Great Chameleon Heart Conference October 15, 2016 Tina Kwan, MD Kenneth Maehara, Ph.D. May 7, 1942 - August 26, 2013 A.R. A classic case of broken heart 38 week AGA F born at an OSH to
DORV: The Great Chameleon Heart Conference October 15, 2016 Tina Kwan, MD Kenneth Maehara, Ph.D. May 7, 1942 - August 26, 2013 A.R. A classic case of broken heart 38 week AGA F born at an OSH to
The Physiology of the Fetal Cardiovascular System
 The Physiology of the Fetal Cardiovascular System Jeff Vergales, MD, MS Department of Pediatrics Division of Pediatric Cardiology jvergales@virginia.edu Disclosures I serve as the medical director for
The Physiology of the Fetal Cardiovascular System Jeff Vergales, MD, MS Department of Pediatrics Division of Pediatric Cardiology jvergales@virginia.edu Disclosures I serve as the medical director for
PAEDIATRIC EMQs. Andrew A Mallick Paediatrics.info.
 PAEDIATRIC EMQs Andrew A Mallick Paediatrics.info www.paediatrics.info Paediatric EMQs Paediatrics.info First published in the United Kingdom in 2012. While the advice and information in this book is believed
PAEDIATRIC EMQs Andrew A Mallick Paediatrics.info www.paediatrics.info Paediatric EMQs Paediatrics.info First published in the United Kingdom in 2012. While the advice and information in this book is believed
A. Incorrect! Think of a therapy that reduces prostaglandin synthesis. B. Incorrect! Think of a therapy that reduces prostaglandin synthesis.
 USMLE Step 1 - Problem Drill 02: Embryology Question No. 1 of 10 1. A premature infant is born with a patent ductus arteriosis. Which of the following treatments may be used as part of the treatment regimen?
USMLE Step 1 - Problem Drill 02: Embryology Question No. 1 of 10 1. A premature infant is born with a patent ductus arteriosis. Which of the following treatments may be used as part of the treatment regimen?
AORTIC COARCTATION. Synonyms: - Coarctation of the aorta
 AORTIC COARCTATION Synonyms: - Coarctation of the aorta Definition: Aortic coarctation is a congenital narrowing of the aorta, usually located after the left subclavian artery, near the ductus or the ligamentum
AORTIC COARCTATION Synonyms: - Coarctation of the aorta Definition: Aortic coarctation is a congenital narrowing of the aorta, usually located after the left subclavian artery, near the ductus or the ligamentum
Neonatal Cardiac Assessment and Congenial Heart Disease compiled by Violet Stephens based on the works of Patricia Hartley
 Neonatal Cardiac Assessment and Congenial Heart Disease compiled by Violet Stephens based on the works of Patricia Hartley Course Contents Purpose Objectives Introduction Fetal Circulation Neonatal Circulation
Neonatal Cardiac Assessment and Congenial Heart Disease compiled by Violet Stephens based on the works of Patricia Hartley Course Contents Purpose Objectives Introduction Fetal Circulation Neonatal Circulation
Neonatal Cardiac Anomalies
 Objectives Neonatal Cardiac Anomalies Karen Knuth, RNC, MN, NNP-BC, ARNP Seattle Childrens Hospital What is CHD? Normal anatomy and circulation Clinical presentation: signs and symptoms Diagnostics Common
Objectives Neonatal Cardiac Anomalies Karen Knuth, RNC, MN, NNP-BC, ARNP Seattle Childrens Hospital What is CHD? Normal anatomy and circulation Clinical presentation: signs and symptoms Diagnostics Common
Critical Heart Disease in the Newborn. What you need to know
 Critical Heart Disease in the Newborn What you need to know DISCLOSURES Nothing to report OBJECTIVES DESCRIBE NEONATAL CARDIOVASCULAR PHYSIOLOGY RECOGNIZE NEONATAL CARDIAC EMERGENCIES FORMULATE TREATMENT
Critical Heart Disease in the Newborn What you need to know DISCLOSURES Nothing to report OBJECTIVES DESCRIBE NEONATAL CARDIOVASCULAR PHYSIOLOGY RECOGNIZE NEONATAL CARDIAC EMERGENCIES FORMULATE TREATMENT
Surgical Treatment of Congenital Heart Disease
 Surgical Treatment of Congenital Heart Disease The Evaluation of Diagnostic Data JAMES V. MALONEY, JR., M.D., and PIERCE J. FLYNN, M.D., Los Angeles THE TASK OF THE CARDIOLOGIST in diagnosing congenital
Surgical Treatment of Congenital Heart Disease The Evaluation of Diagnostic Data JAMES V. MALONEY, JR., M.D., and PIERCE J. FLYNN, M.D., Los Angeles THE TASK OF THE CARDIOLOGIST in diagnosing congenital
Objectives Part 1. Objectives Part 2. Fetal Circulation Transition to Postnatal Circulation Normal Cardiac Anatomy Ductal Dependence and use of PGE1
 Cardiac Physiology Gia Marzano, AC PNP Pediatric Cardiac Surgery Rush Center for Congenital Heart Disease Rush University Medical Center Objectives Part 1 Fetal Circulation Transition to Postnatal Circulation
Cardiac Physiology Gia Marzano, AC PNP Pediatric Cardiac Surgery Rush Center for Congenital Heart Disease Rush University Medical Center Objectives Part 1 Fetal Circulation Transition to Postnatal Circulation
Pearson's Comprehensive Medical Assisting Administrative and Clinical Competencies
 Pearson's Comprehensive Medical Assisting Administrative and Clinical Competencies THIRD EDITION CHAPTER 27 The Cardiovascular System Lesson 1: Overview of the Cardiovascular System Lesson Objectives Upon
Pearson's Comprehensive Medical Assisting Administrative and Clinical Competencies THIRD EDITION CHAPTER 27 The Cardiovascular System Lesson 1: Overview of the Cardiovascular System Lesson Objectives Upon
Ch.15 Cardiovascular System Pgs {15-12} {15-13}
 Ch.15 Cardiovascular System Pgs {15-12} {15-13} E. Skeleton of the Heart 1. The skeleton of the heart is composed of rings of dense connective tissue and other masses of connective tissue in the interventricular
Ch.15 Cardiovascular System Pgs {15-12} {15-13} E. Skeleton of the Heart 1. The skeleton of the heart is composed of rings of dense connective tissue and other masses of connective tissue in the interventricular
MEDICAL MANAGEMENT WITH CAVEATS 1. In one study of 50 CHARGE patients with CHD, 75% required surgery. 2. Children with CHARGE may be resistant to chlo
 CARDIOLOGY IN CHARGE SYNDROME: FOR THE PHYSICIAN Angela E. Lin, M.D. Teratology Program/Active Malformation Surveillance, Brigham and Women's Hospital, Old PBBH-B501, 75 Francis St., Boston, MA 02115 alin@partners.org
CARDIOLOGY IN CHARGE SYNDROME: FOR THE PHYSICIAN Angela E. Lin, M.D. Teratology Program/Active Malformation Surveillance, Brigham and Women's Hospital, Old PBBH-B501, 75 Francis St., Boston, MA 02115 alin@partners.org
PedsCases Podcast Scripts
 PedsCases Podcast Scripts This is a text version of a podcast from Pedscases.com on Acyanotic Congenital Heart Lesions. These podcasts are designed to give medical students an overview of key topics in
PedsCases Podcast Scripts This is a text version of a podcast from Pedscases.com on Acyanotic Congenital Heart Lesions. These podcasts are designed to give medical students an overview of key topics in
Common Defects With Expected Adult Survival:
 Common Defects With Expected Adult Survival: Bicuspid aortic valve :Acyanotic Mitral valve prolapse Coarctation of aorta Pulmonary valve stenosis Atrial septal defect Patent ductus arteriosus (V.S.D.)
Common Defects With Expected Adult Survival: Bicuspid aortic valve :Acyanotic Mitral valve prolapse Coarctation of aorta Pulmonary valve stenosis Atrial septal defect Patent ductus arteriosus (V.S.D.)
Congenital Heart Disease An Approach for Simple and Complex Anomalies
 Congenital Heart Disease An Approach for Simple and Complex Anomalies Michael D. Pettersen, MD Director, Echocardiography Rocky Mountain Hospital for Children Denver, CO None Disclosures 1 ASCeXAM Contains
Congenital Heart Disease An Approach for Simple and Complex Anomalies Michael D. Pettersen, MD Director, Echocardiography Rocky Mountain Hospital for Children Denver, CO None Disclosures 1 ASCeXAM Contains
Data Collected: June 17, Reported: June 30, Survey Dates 05/24/ /07/2010
 Job Task Analysis for ARDMS Pediatric Echocardiography Data Collected: June 17, 2010 Reported: Analysis Summary For: Pediatric Echocardiography Exam Survey Dates 05/24/2010-06/07/2010 Invited Respondents
Job Task Analysis for ARDMS Pediatric Echocardiography Data Collected: June 17, 2010 Reported: Analysis Summary For: Pediatric Echocardiography Exam Survey Dates 05/24/2010-06/07/2010 Invited Respondents
Congenital Heart Disease: Cyanotic Lesions. Amitesh Aggarwal
 Congenital Heart Disease: Cyanotic Lesions Amitesh Aggarwal 12 y/o male admitted because of dyspnea and cyanosis Patient has been cyanotic since few months after birth Has episodes of tachypnea and worsening
Congenital Heart Disease: Cyanotic Lesions Amitesh Aggarwal 12 y/o male admitted because of dyspnea and cyanosis Patient has been cyanotic since few months after birth Has episodes of tachypnea and worsening
Definitions. N24 Pediatrics: Alterations in Cardiovascular Function. May C. Madsen RN, MSN 1. Congestive Heart Failure
 Definitions C.O.= volume of blood ejected by heart in 1 minute Cardiac output = HR x stroke volume S.V.: preload, afterload, contractility Flow = pressure gradient resistance 1 Congestive Heart Failure
Definitions C.O.= volume of blood ejected by heart in 1 minute Cardiac output = HR x stroke volume S.V.: preload, afterload, contractility Flow = pressure gradient resistance 1 Congestive Heart Failure
September 26, 2012 Philip Stockwell, MD Lifespan CVI Assistant Professor of Medicine (Clinical)
") September 26, 2012 Philip Stockwell, MD Lifespan CVI Assistant Professor of Medicine (Clinical) Advances in cardiac surgery have created a new population of adult patients with repaired congenital heart
September 26, 2012 Philip Stockwell, MD Lifespan CVI Assistant Professor of Medicine (Clinical) Advances in cardiac surgery have created a new population of adult patients with repaired congenital heart
Circulatory System Notes
 Circulatory System Notes Functions of Circulatory System A. Transports B. Transports C. Transports D. Transports E. of fluids F. G. Regulate temperature H. Blood clotting Characteristics of various blood
Circulatory System Notes Functions of Circulatory System A. Transports B. Transports C. Transports D. Transports E. of fluids F. G. Regulate temperature H. Blood clotting Characteristics of various blood
COMBINED CONGENITAL SUBAORTIC STENOSIS AND INFUNDIBULAR PULMONARY STENOSIS*
 COMBINED CONGENITAL SUBAORTIC STENOSIS AND INFUNDIBULAR PULMONARY STENOSIS* BY HENRY N. NEUFELD,t PATRICK A. ONGLEY, AND JESSE E. EDWARDS From the Sections of Pa?diatrics and Pathological Anatomy, Mayo
COMBINED CONGENITAL SUBAORTIC STENOSIS AND INFUNDIBULAR PULMONARY STENOSIS* BY HENRY N. NEUFELD,t PATRICK A. ONGLEY, AND JESSE E. EDWARDS From the Sections of Pa?diatrics and Pathological Anatomy, Mayo
: Provide cardiovascular preventive counseling to parents and patients with specific cardiac diseases about:
 Children s Hospital & Research Center Oakland Cardiology Primary Goals for this Rotation 5.13 GOAL: Prevention, Counseling and Screening (Cardiovascular). Understand the role of the pediatrician in preventing
Children s Hospital & Research Center Oakland Cardiology Primary Goals for this Rotation 5.13 GOAL: Prevention, Counseling and Screening (Cardiovascular). Understand the role of the pediatrician in preventing
BLOOD I. Composition and Function of Blood
 BLOOD I. Composition and Function of Blood A. Components 1. Blood is the only fluid tissue 2. Has living blood cells and nonliving fluid matrix 3. Breakdown of blood sample a. Formed elements b. Plasma
BLOOD I. Composition and Function of Blood A. Components 1. Blood is the only fluid tissue 2. Has living blood cells and nonliving fluid matrix 3. Breakdown of blood sample a. Formed elements b. Plasma
Pathology. Congenital heart disease. congenital heart diseases. congenital heart diseases - etiology. lecture 7
 Pathology lecture 7 prof hab. n. med. Andrzej Marszałek Congenital heart disease congenital heart diseases Def.: anatomical anomalies present at delivery ambnormal embryogenesis 3. and 8. week of gestation
Pathology lecture 7 prof hab. n. med. Andrzej Marszałek Congenital heart disease congenital heart diseases Def.: anatomical anomalies present at delivery ambnormal embryogenesis 3. and 8. week of gestation
Heart Development and Congenital Heart Disease
 Heart Development and Congenital Heart Disease Sally Dunwoodie s.dunwoodie@victorchang.edu.au Developmental and Stem Cell Biology Division Victor Chang Cardiac Research Institute for the heart of Australia...
Heart Development and Congenital Heart Disease Sally Dunwoodie s.dunwoodie@victorchang.edu.au Developmental and Stem Cell Biology Division Victor Chang Cardiac Research Institute for the heart of Australia...
The Chest X-ray for Cardiologists
 Mayo Clinic & British Cardiovascular Society at the Royal College of Physicians, London : 21-23-October 2013 Cases-Controversies-Updates 2013 The Chest X-ray for Cardiologists Michael Rubens Royal Brompton
Mayo Clinic & British Cardiovascular Society at the Royal College of Physicians, London : 21-23-October 2013 Cases-Controversies-Updates 2013 The Chest X-ray for Cardiologists Michael Rubens Royal Brompton
Clinicians and Facilities: RESOURCES WHEN CARING FOR WOMEN WITH ADULT CONGENITAL HEART DISEASE OR OTHER FORMS OF CARDIOVASCULAR DISEASE!!
 Clinicians and Facilities: RESOURCES WHEN CARING FOR WOMEN WITH ADULT CONGENITAL HEART DISEASE OR OTHER FORMS OF CARDIOVASCULAR DISEASE!! Abha'Khandelwal,'MD,'MS' 'Stanford'University'School'of'Medicine'
Clinicians and Facilities: RESOURCES WHEN CARING FOR WOMEN WITH ADULT CONGENITAL HEART DISEASE OR OTHER FORMS OF CARDIOVASCULAR DISEASE!! Abha'Khandelwal,'MD,'MS' 'Stanford'University'School'of'Medicine'
Systematic approach to Fetal Echocardiography. Objectives. Introduction 11/2/2015
 Systematic approach to Fetal Echocardiography. Pediatric Echocardiography Conference, JCMCH November 7, 2015 Rajani Anand Objectives Fetal cardiology pre-test Introduction Embryology and Physiology of
Systematic approach to Fetal Echocardiography. Pediatric Echocardiography Conference, JCMCH November 7, 2015 Rajani Anand Objectives Fetal cardiology pre-test Introduction Embryology and Physiology of
DEVELOPMENT OF THE CIRCULATORY SYSTEM L E C T U R E 5
 DEVELOPMENT OF THE CIRCULATORY SYSTEM L E C T U R E 5 REVIEW OF CARDIAC ANATOMY Heart 4 chambers Base and apex Valves Pericardial sac 3 layers: epi, myo, endo cardium Major blood vessels Aorta and its
DEVELOPMENT OF THE CIRCULATORY SYSTEM L E C T U R E 5 REVIEW OF CARDIAC ANATOMY Heart 4 chambers Base and apex Valves Pericardial sac 3 layers: epi, myo, endo cardium Major blood vessels Aorta and its
Chapter 2 Cardiac Interpretation of Pediatric Chest X-Ray
 Chapter 2 Cardiac Interpretation of Pediatric Chest X-Ray Ra-id Abdulla and Douglas M. Luxenberg Key Facts The cardiac silhouette occupies 50 55% of the chest width on an anterior posterior chest X-ray
Chapter 2 Cardiac Interpretation of Pediatric Chest X-Ray Ra-id Abdulla and Douglas M. Luxenberg Key Facts The cardiac silhouette occupies 50 55% of the chest width on an anterior posterior chest X-ray
Patent Ductus Arteriosus (PDA)
") Patent Ductus Arteriosus (PDA) How does the heart work? The heart is the organ responsible for pumping blood to and from all tissues of the body. The heart is divided into right and left sides. The job
Patent Ductus Arteriosus (PDA) How does the heart work? The heart is the organ responsible for pumping blood to and from all tissues of the body. The heart is divided into right and left sides. The job
The Heart. Happy Friday! #takeoutyournotes #testnotgradedyet
 The Heart Happy Friday! #takeoutyournotes #testnotgradedyet Introduction Cardiovascular system distributes blood Pump (heart) Distribution areas (capillaries) Heart has 4 compartments 2 receive blood (atria)
The Heart Happy Friday! #takeoutyournotes #testnotgradedyet Introduction Cardiovascular system distributes blood Pump (heart) Distribution areas (capillaries) Heart has 4 compartments 2 receive blood (atria)
3/14/2011 MANAGEMENT OF NEWBORNS CARDIAC INTENSIVE CARE CONFERENCE FOR HEALTH PROFESSIONALS IRVINE, CA. MARCH 7, 2011 WITH HEART DEFECTS
 CONFERENCE FOR HEALTH PROFESSIONALS IRVINE, CA. MARCH 7, 2011 MANAGEMENT OF NEWBORNS WITH HEART DEFECTS A NTHONY C. CHANG, MD, MBA, MPH M E D I C AL D I RE C T OR, HEART I N S T I T U T E C H I LDRE N
CONFERENCE FOR HEALTH PROFESSIONALS IRVINE, CA. MARCH 7, 2011 MANAGEMENT OF NEWBORNS WITH HEART DEFECTS A NTHONY C. CHANG, MD, MBA, MPH M E D I C AL D I RE C T OR, HEART I N S T I T U T E C H I LDRE N
THE HEART. Unit 3: Transportation and Respiration
 THE HEART Unit 3: Transportation and Respiration The Circulatory System Also called the Cardiovascular System Circulates blood in the body Transports nutrients, oxygen, carbon dioxide, hormones, and blood
THE HEART Unit 3: Transportation and Respiration The Circulatory System Also called the Cardiovascular System Circulates blood in the body Transports nutrients, oxygen, carbon dioxide, hormones, and blood
The production of murmurs is due to 3 main factors:
 Heart murmurs The production of murmurs is due to 3 main factors: high blood flow rate through normal or abnormal orifices forward flow through a narrowed or irregular orifice into a dilated vessel or
Heart murmurs The production of murmurs is due to 3 main factors: high blood flow rate through normal or abnormal orifices forward flow through a narrowed or irregular orifice into a dilated vessel or
Upon completion of this presentation, the participant will be able to:
 B12 Neonatal Cardiology Review Nicole Bowie, NNP-/BC, PNP Neonatal Nurse Practitioner Jackson Memorial Hospital, Miami, FL The speaker has signed a disclosure form and indicated she has no significant
B12 Neonatal Cardiology Review Nicole Bowie, NNP-/BC, PNP Neonatal Nurse Practitioner Jackson Memorial Hospital, Miami, FL The speaker has signed a disclosure form and indicated she has no significant
Approach to a baby with cyanosis
 Approach to a baby with cyanosis Objectives Cyanosis : types Differentials: cardiac vs. non cardiac Approach Case scenarios Cyanosis Greek word kuaneos meaning dark blue Bluish discolouration of skin,
Approach to a baby with cyanosis Objectives Cyanosis : types Differentials: cardiac vs. non cardiac Approach Case scenarios Cyanosis Greek word kuaneos meaning dark blue Bluish discolouration of skin,
The production of murmurs is due to 3 main factors:
 Heart murmurs The production of murmurs is due to 3 main factors: high blood flow rate through normal or abnormal orifices forward flow through a narrowed or irregular orifice into a dilated vessel or
Heart murmurs The production of murmurs is due to 3 main factors: high blood flow rate through normal or abnormal orifices forward flow through a narrowed or irregular orifice into a dilated vessel or
Cardiovascular System
 Cardiovascular System Heart: hollow muscular organ, pumps blood full of nutrients throughout the body Arteries: carry blood away from the heart Capillaries: smaller vessels, microscopic, exchange of nutrients
Cardiovascular System Heart: hollow muscular organ, pumps blood full of nutrients throughout the body Arteries: carry blood away from the heart Capillaries: smaller vessels, microscopic, exchange of nutrients
9/8/2009 < 1 1,2 3,4 5,6 7,8 9,10 11,12 13,14 15,16 17,18 > 18. Tetralogy of Fallot. Complex Congenital Heart Disease.
 Current Indications for Pediatric CTA S Bruce Greenberg Professor of Radiology Arkansas Children s Hospital University of Arkansas for Medical Sciences greenbergsbruce@uams.edu 45 40 35 30 25 20 15 10
Current Indications for Pediatric CTA S Bruce Greenberg Professor of Radiology Arkansas Children s Hospital University of Arkansas for Medical Sciences greenbergsbruce@uams.edu 45 40 35 30 25 20 15 10
More History. Organization. Maternal Cardiac Disease: a historical perspective. The Parturient with Cardiac Disease 9/21/2012
 The Parturient with Cardiac Disease Pamela Flood M.D. Professor of Anesthesia and Perioperative Care Obstetrics, Gynecology and Reproductive Sciences University of California, San Francisco Maternal Cardiac
The Parturient with Cardiac Disease Pamela Flood M.D. Professor of Anesthesia and Perioperative Care Obstetrics, Gynecology and Reproductive Sciences University of California, San Francisco Maternal Cardiac