Congenital Heart Disease
|
|
|
- Madlyn Gilmore
- 5 years ago
- Views:
Transcription
1 Congenital Heart Disease Mohammed Alghamdi, MD, FRCPC, FAAP, FACC Associate Professor and Consultant Pediatric Cardiology, Cardiac Science King Fahad Cardiac Centre King Saud University
2 INTRODUCTION CHD ~ 0.8% of live births. Major CHD: Ventricular Septal Defect: 35% Atrial Septal Defect: 7 % Patent Ductus Ateriosus: 7 % Coarctation of Aorta: 6 % Tetralogy of Fallot: 6 % Pulmonary valve stenosis: 6 % Aortic valve stenosis: 5 % D-Transposition of great arteries: 4 %
3 Congenital Heart Disease Etiology: Mostly unknown Chromosomal abnormalities can cause Trisomy 21: AVSD Trisomy 18: VSD Trismoy 13: PDA, VSD, ASD DiGeorge Syndrome: Arch, Conotruncal abnormalities Turner syndrome: Coarctation of Aorta Williams Syndrome: Supra-aortic stenosis, PA stenosis Noonan Syndrome: Dysplastic pulmonary valve
4 Classification of CHD Divided into 2 major groups: Cyanotic heart diseases. Acyanotic heart diseases. Subdivided further according to: Physical Finding Chest X-ray finding ECG finding Diagnosis is confirmed by: Echo, Cardiac CT/MRI or Cardiac Catheterization.
5 Classification of CHD Cyanotic Heart Disease Decreased pulmonary flow: Tetralogy of Fallot Tricuspid atresia Other univentricular heart with pulmonary stenosis. Increased pulmonary flow: Transposition of great arteries Total anomalous pulmonary venous return. Acyanotic Heart Disease Left Right shunt lesions: Ventricular septal defect Atrial Septal Defect Atrio-ventricular Septal Defect Patent Ductus Arteriosus Obstructive lesions: Aortic stenosis Pulmonary valve stenosis Coarctation of Aorta
6 Acyanotic Heart Disease Left to- Right Shunt lesions
7 Left to- Right Shunt lesions VSD PDA ASD
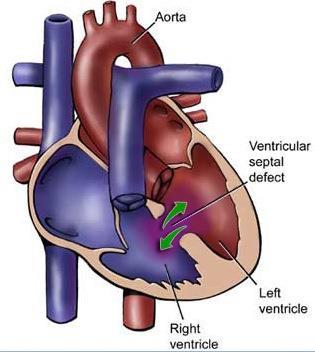
8 VSD
9 ASD
10 PDA
11 PATHOPHYSIOLOGY: L-R SHUNT L-R shunt toward pulmonary circulation. Increased Qp:Qs ratio Increased cardiac output to the pulmonary circulation (Qp) Reduced of cardiac output to the systemic circulation (Qs)
12 PATHOPHYSIOLOGY: L-R SHUNT VSD L-R shunt at ventricular level: Dilated LA and LV Enlarged pulmonary arteries ASD L-R shunt at atrial level: Dilated RA and RV Enlarged pulmonary arteries PDA L-R shunt at artery level: Dilated LA and LV
13 SYMPTOM: L-R SHUNT VSD Small VSD: Asymptomatic Moderate to large VSD: CHF ASD Usually asymptomatic Older children: Activity related SOB & Fatigability Rare: CHF, FTT PDA Small PDA: Asymptomatic Moderate to large PDA: CHF
14 CONGESTIVE HEART FAILURE SYMPTOMS Diaphoresis Poor feeding Failure to thrive Shortness of breath Recurrent chest infection Exercise intolerance SIGNS Tachypnia Tachycardia Cardiomegally Hepatomegally Active precordium
15 VSD No symptom during neonatal period due to high pulmonary vascular resistance Symptoms of CHF started ~ 2/12 of age diaphoresis, poor feeding, and failure to thrive. shortness of breath, recurrent chest infection. exercise intolerance.
16 EXAMINATION: L-R SHUNT VSD Holosystolic murmur Large: mid-diastolic murmur Small muscular: ejection systolic murmur ASD Fixed Widely splitted second heart sound Ejection systolic murmur Large: mid-diastolic murmur PDA Small PDA: Silent Large PDA: Continuous machinery murmur Large PDA: Widened pulse pressure
17 INVESTIGATION: L-R SHUNT Diagnosis: Chest X-ray: Increased pulmonary vascular marking +/- cardiomegally ECG: Small lesion: Normal Mod to large: chambers enlargement ECHO: Confirm Diagnosis Cardiac Cath: not required for Dx
18 MEDICAL Rx: L-R SHUNT Medical Mgx Anti-congestive therapy: Diuretics Digoxin. After load reducing agents Nutritional support ASD: usually no medication needed
19 INTERVENSION: L-R SHUNT VSD Surgical closure 4-8 months Some types in older children can be closed by device via CATH. ASD Most closed by device via CATH around 3-6 years Some types need surgical closure. PDA Most closed by device via CATH Surgery needed in premature baby and symptomtic neonate less than 6 kg.
20 PROGNOSIS: L-R SHUNT Untreated VSD and PDA beyond infancy: Eisenmenger s syndrome Sign and symptom of CHF will disappear Patient will become cyanotic R-L shunt
21 PROGNOSIS: L-R SHUNT Untreated ASD: complication happened during adult Life: Eisenmenger s syndrome Atrial arrhythmias Paradoxical embolism (rare)
22 AVSD

23 AVSD Incidence: 4 % of all CHD Associated with Down Syndrome (50%) Divided into: Complete AVSD ASD primum/ inlet VSD / common AV valve Balanced vs. Unbalanced AVSD Partial AVSD ASD primum No VSD
24 AVSD Pathophysiology: Similar to VSD and ASD left to right shunt across the atrial level Left to right shunt at and ventricular level In addition: AV valve regurgitation Significant L-R shunting: Pulmonary over-circulation Increase Qp:Qs ratio.
25 AVSD Clinical Features: Usually asymptomatic at neonatal period Due to high pulmonary vascular resistance Baby may have slightly lower oxygen saturation Symptoms of CHF started at few months of age Diaphoresis Poor feeding Failure to thrive. Shortness of breath Recurrent chest infection. Exercise intolerance.
26 AVSD Clinical Features: Physical Examination: Feature of Down Syndrome Tachypnia Tachycardia Active precordium Murmur: Pan-systolic (holosystolic) murmur Hepatomegaly
27 AVSD Diagnosis: Chest X-ray: Increased pulmonary vascular marking Cardiomegaly ECG: Left Axis deviation with RVH is very suggestive of AVSD ECHO: Confirm Diagnosis Cardiac Cath: not required for Dx
28 AVSD Treatment: Medical Rx: Anti-congestive therapy: Nutritional suppor Surgical closure for complete VSD: Usually done before 6 months of age to ovoid development of Eisenmenger s syndrome. Balanced AVSD: Biventricular repair Unbalanced AVSD: may need single ventricular repair
29 Acyanotic Heart Disease obstructive lesion

30 Coarctation of Aorta (CoA)
31 Coarctation of Aorta (CoA) Incidence: 5-7 % of all CHD Associated with Turner syndrome in female Arch interruption: seen in DiGeorge syndrom Can be: Discrete or Diffuse Can be mild to severe
32 PATHOPHYSIOLOGY: CoA CRTICAL CoA Spontaneous PDA closure Obstruction of blood flow to distal arch Hypotension and Shock Acute increase of LV afterload LV dysfunction DUCT DEPENDENT CHD MILD CoA Collateral vessels develop overtime Flow maintained between proximal and distal aorta Present later on life
33 CLINICAL PRESENTATION: CoA CRTICAL CoA Presented 2-3 wks of life Sign of CHF Circulatory collapse Shock Death DUCT DEPENDENT CHD MILD CoA Present later on life Murmur Chronic hypertension Headache Fatigue Stroke» Rupture cerebral aneurysm
34 Clinical Features: CoA Physical Examination: Differential cyanosis (severe CoA in newborn) Signs of cardiac shock Reduced or absent femoral pulses Brachio- femoral delay BP in lower limb lower than upper Limb BP Murmur: Ejection systolic murmur at the back Continues murmur due to collateral at the back


35 DIAGNOSIS: CoA Chest X-ray: Cardiomegaly Prominent aortic knob Rib notching» Due to d of collateral vessels» Rarely seen before age of 10 years ECG: Neonate: RV hypertrophy Older children: LV hypertrophy ECHO: Usually will establish the diagnosis May need Cardiac CT /MRI
36 TREATMENT: CoA Critical CoA Duct Dependent CHD Prostaglandin E2 to keep PDA open Surgery is the primary intervension Trans-catheter balloon angioplasty +/- stent: Recurrent CoA Primary intervention: Discrete CoA in older children

37 Pulmonary Valve Stenosis
38 Aortic Valve Stenosis
39 Cyanotic Heart Disease
40 Tetralogy of Fallot

41 Tetralogy of Fallot Most common cyanotic CHD Incidence: 6 % of all CHD Can be associated with DiGeorge Syndrome
42 Tetralogy of Fallot Four basic components Large VSD Pulmonary stenosis (PS) Overriding aorta RV hypertrophy
43 CLINICAL FEATURES: TOF Depend on the severity of PS Most newborn: Asymptomatic Ejection systolic murmur on routine discharge exam Initially have mild cyanosis which progress with time: Might present with hypercyanotic spells tet spell if delayed intervention
44 CLINICAL FEATURES: TET SPELL Usually occur around 9-12 months of age Episodes of acute and severe cyanosis RX: Medical emergency Reduced anxiety Keep child in his mother lab Knee-to-chest position Give oxygen Sedation with morphine IV fluid Beta Blocker Phenylephrine Might require emergency surgical intervention
45 CLINICAL FEATURES: TOF Newborn with severe PS or pulmonary atresia Severe cyanosis when PDA close Duct dependent CHD Need IV prostaglandin E2

46 INVESTIGATION: TOF CHEST X-RAY: boot-shaped heart ECG: RVH ECHO: confirm diagnosis CT/MRI rarely needed
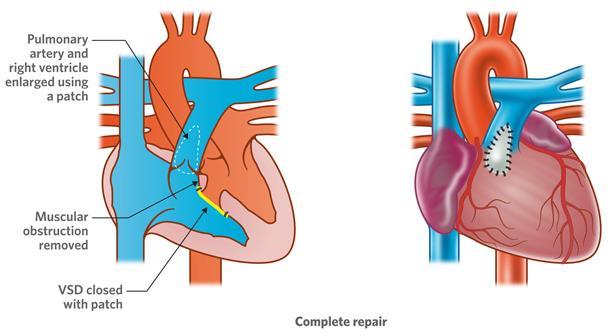
47 TREATMENT: TOF

48 Transposition of the Great Arteries
49 D-TGA Incidence: 4 % of all CHD Most common CHD presented with cyanosis at birth. More common in male Higher incidence in infant of diabetic mother
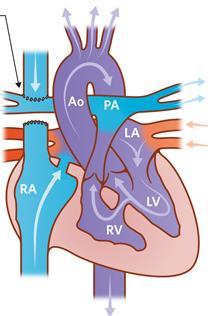
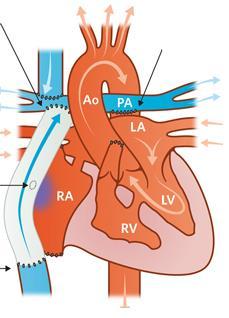
50 PATHOPHYSIOLOGY: D-TGA In Normal heart: Pulmonary and systemic circulations are in series In D-TGA: Pulmonary and systemic circulations are in parallel
51 PATHOPHYSIOLOGY: D-TGA Mixing of oxygenated and deoxygenated blood can occur at three levels: Atrial level via ASD/PFO (most important) Great arteries level via PDA Ventricular level via VSD (if present)
52 PRESENTATION: D-TGA Severely Cyanosis after birth Duct Dependent CHD Reverse differential cyanosis if Pulm HTN No signs of respiratory distress Single second heart sound Typically: no murmur Hyperoxic test: FAIL

53 INVESTIGATION: D-TGA Chest X-ray: egg on a string appearance ECG: Typically normal ECHO: confirm diagnosis Cardiac Cath: For septestomy +/- coronary arteries anatomy
54 MANAGEMENT: D-TGA Supportive: Prostaglandin E2 Balloon atrial septostomy (for better mixing)
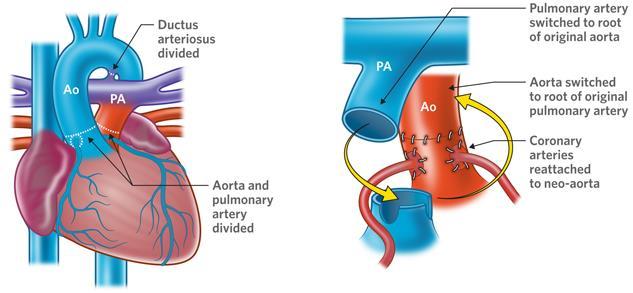
55 MANAGEMENT: D-TGA

56 Total Anomalous Pulmonary Venous Return : TAPVD
 Infracardiac (20%) Mixed (5%) Can be: Obstructed TAPVR Non-obstructed")
57 TAPVD All 4 pulmonary veins returns to the right atrium Can be: Supracardiac (50%) Cardiac (25%) Infracardiac (20%) Mixed (5%) Can be: Obstructed TAPVR Non-obstructed TAPVR


58 PRESENTATION: TAPVD Clinical Feature: Cyanosis at birth Diagnosis: Chest X-ray: Increased pulmonary vascualr markings Figure of eight in obstructed supracardiac TAPVR ECG: RVH ECHO: Confirm Dx Cardiac CT/MI: may be need

59 Hypoplastic Left Heart Syndrome
60 HLHS HLHS: one of the most severe form of CHD High morbidity and mortality Incidence: 1-2 % of all CHD multiple level of obstruction at left heart structures. Mitral stenosis to mitral atresia Variable degree of LV hypoplasia Aortic stenosis to aortic atresia Variable degree of ascending aorta hypoplasia

61 PATHOPHYSIOLOGY: HLHS No adequate flow across aortic valve to ascending aorta Relies on retrograde PDA flow to: Brain Coronary arteries Need ASD/PFO to shunt blood from LA to RA.
62 PRESENTATION: HLHS At birth: Cyanosis At 2-4 week of life: Respiratory distress Poor pulses/perfusion Signs of cardiac shock
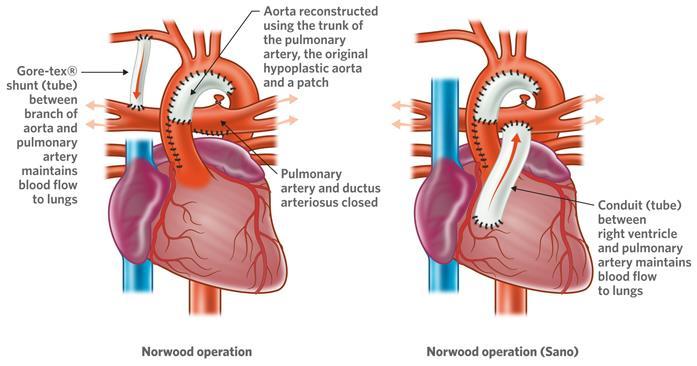
63 TREATMENT: HLHS

64 Tricuspid Atresia

65 Single Ventricle

66 STAGED SURGERY UNIVENTRICULAR HEART BT SHUNT GLENN FONTAN
67 Truncus Arteriosus


68 Ebstein s Anomaly
69 END
Notes by Sandra Dankwa 2009 HF- Heart Failure DS- Down Syndrome IE- Infective Endocarditis ET- Exercise Tolerance. Small VSD Symptoms -asymptomatic
 Congenital Heart Disease: Notes. Condition Pathology PC Ix Rx Ventricular septal defect (VSD) L R shuntsdefect anywhere in the ventricle, usually perimembranous (next to the tricuspid valve) 30% 1)small
Congenital Heart Disease: Notes. Condition Pathology PC Ix Rx Ventricular septal defect (VSD) L R shuntsdefect anywhere in the ventricle, usually perimembranous (next to the tricuspid valve) 30% 1)small
Congenital Heart Disease: Physiology and Common Defects
 Congenital Heart Disease: Physiology and Common Defects Jamie S. Sutherell, M.D, M.Ed. Associate Professor, Pediatrics Division of Cardiology Director, Medical Student Education in Pediatrics Director,
Congenital Heart Disease: Physiology and Common Defects Jamie S. Sutherell, M.D, M.Ed. Associate Professor, Pediatrics Division of Cardiology Director, Medical Student Education in Pediatrics Director,
Cardiovascular Pathophysiology: Right to Left Shunts aka Cyanotic Lesions
 Cardiovascular Pathophysiology: Right to Left Shunts aka Cyanotic Lesions Ismee A. Williams, MD, MS iib6@columbia.edu Pediatric Cardiology Learning Objectives To discuss the hemodynamic significance of
Cardiovascular Pathophysiology: Right to Left Shunts aka Cyanotic Lesions Ismee A. Williams, MD, MS iib6@columbia.edu Pediatric Cardiology Learning Objectives To discuss the hemodynamic significance of
Cardiovascular Pathophysiology: Right to Left Shunts aka Cyanotic Lesions Ismee A. Williams, MD, MS Pediatric Cardiology
 Cardiovascular Pathophysiology: Right to Left Shunts aka Cyanotic Lesions Ismee A. Williams, MD, MS iib6@columbia.edu Pediatric Cardiology Learning Objectives To discuss the hemodynamic significance of
Cardiovascular Pathophysiology: Right to Left Shunts aka Cyanotic Lesions Ismee A. Williams, MD, MS iib6@columbia.edu Pediatric Cardiology Learning Objectives To discuss the hemodynamic significance of
CONGENITAL HEART DISEASE (CHD)
") CONGENITAL HEART DISEASE (CHD) DEFINITION It is the result of a structural or functional abnormality of the cardiovascular system at birth GENERAL FEATURES OF CHD Structural defects due to specific disturbance
CONGENITAL HEART DISEASE (CHD) DEFINITION It is the result of a structural or functional abnormality of the cardiovascular system at birth GENERAL FEATURES OF CHD Structural defects due to specific disturbance
Paediatrics Revision Session Cardiology. Emma Walker 7 th May 2016
 Paediatrics Revision Session Cardiology Emma Walker 7 th May 2016 Cardiovascular Examination! General:! Make it fun!! Change how you act depending on their age! Introduction! Introduce yourself & check
Paediatrics Revision Session Cardiology Emma Walker 7 th May 2016 Cardiovascular Examination! General:! Make it fun!! Change how you act depending on their age! Introduction! Introduce yourself & check
Slide 1. Slide 2. Slide 3 CONGENITAL HEART DISEASE. Papworth Hospital NHS Trust INTRODUCTION. Jakub Kadlec/Catherine Sudarshan INTRODUCTION
 Slide 1 CONGENITAL HEART DISEASE Jakub Kadlec/Catherine Sudarshan NHS Trust Slide 2 INTRODUCTION Most common congenital illness in the newborn Affects about 4 9 / 1000 full-term live births in the UK 1.5
Slide 1 CONGENITAL HEART DISEASE Jakub Kadlec/Catherine Sudarshan NHS Trust Slide 2 INTRODUCTION Most common congenital illness in the newborn Affects about 4 9 / 1000 full-term live births in the UK 1.5
Anatomy & Physiology
 1 Anatomy & Physiology Heart is divided into four chambers, two atrias & two ventricles. Atrioventricular valves (tricuspid & mitral) separate the atria from ventricles. they open & close to control flow
1 Anatomy & Physiology Heart is divided into four chambers, two atrias & two ventricles. Atrioventricular valves (tricuspid & mitral) separate the atria from ventricles. they open & close to control flow
When is Risky to Apply Oxygen for Congenital Heart Disease 부천세종병원 소아청소년과최은영
 When is Risky to Apply Oxygen for Congenital Heart Disease 부천세종병원 소아청소년과최은영 The Korean Society of Cardiology COI Disclosure Eun-Young Choi The author have no financial conflicts of interest to disclose
When is Risky to Apply Oxygen for Congenital Heart Disease 부천세종병원 소아청소년과최은영 The Korean Society of Cardiology COI Disclosure Eun-Young Choi The author have no financial conflicts of interest to disclose
By Dickens ATURWANAHO & ORIBA DAN LANGOYA MAKchs, MBchB CONGENTAL HEART DISEASE
 By Dickens ATURWANAHO & ORIBA DAN LANGOYA MAKchs, MBchB CONGENTAL HEART DISEASE Introduction CHDs are abnormalities of the heart or great vessels that are present at birth. Common type of heart disease
By Dickens ATURWANAHO & ORIBA DAN LANGOYA MAKchs, MBchB CONGENTAL HEART DISEASE Introduction CHDs are abnormalities of the heart or great vessels that are present at birth. Common type of heart disease
5.8 Congenital Heart Disease
 5.8 Congenital Heart Disease Congenital heart diseases (CHD) refer to structural or functional heart diseases, which are present at birth. Some of these lesions may be discovered later. prevalence of Chd
5.8 Congenital Heart Disease Congenital heart diseases (CHD) refer to structural or functional heart diseases, which are present at birth. Some of these lesions may be discovered later. prevalence of Chd
Congenital heart disease. By Dr Saima Ali Professor of pediatrics
 Congenital heart disease By Dr Saima Ali Professor of pediatrics What is the most striking clinical finding in this child? Learning objectives By the end of this lecture, final year student should be able
Congenital heart disease By Dr Saima Ali Professor of pediatrics What is the most striking clinical finding in this child? Learning objectives By the end of this lecture, final year student should be able
Patent ductus arteriosus PDA
 Patent ductus arteriosus PDA Is connecting between the aortic end just distal to the origin of the LT sub clavian artery& the pulmonary artery at its bifurcation. Female/male ratio is 2:1 and it is more
Patent ductus arteriosus PDA Is connecting between the aortic end just distal to the origin of the LT sub clavian artery& the pulmonary artery at its bifurcation. Female/male ratio is 2:1 and it is more
PATENT DUCTUS ARTERIOSUS (PDA)
") PATENT DUCTUS ARTERIOSUS (PDA) It is a channel that connect the pulmonary artery with the descending aorta (isthumus part). It results from the persistence of patency of the fetal ductus arteriosus after
PATENT DUCTUS ARTERIOSUS (PDA) It is a channel that connect the pulmonary artery with the descending aorta (isthumus part). It results from the persistence of patency of the fetal ductus arteriosus after
Pediatric Board Review Congenital Heart Disease. Steven H. Todman, M.D. Pediatric Cardiologist Louisiana State University
 Pediatric Board Review Congenital Heart Disease Steven H. Todman, M.D. Pediatric Cardiologist Louisiana State University Our Mission To discuss various types of congenital heart disease that are commonly
Pediatric Board Review Congenital Heart Disease Steven H. Todman, M.D. Pediatric Cardiologist Louisiana State University Our Mission To discuss various types of congenital heart disease that are commonly
Congenital heart disease: When to act and what to do?
 Leading Article Congenital heart disease: When to act and what to do? Duminda Samarasinghe 1 Sri Lanka Journal of Child Health, 2010; 39: 39-43 (Key words: Congenital heart disease) Congenital heart disease
Leading Article Congenital heart disease: When to act and what to do? Duminda Samarasinghe 1 Sri Lanka Journal of Child Health, 2010; 39: 39-43 (Key words: Congenital heart disease) Congenital heart disease
Uptofate Study Summary
 CONGENITAL HEART DISEASE Uptofate Study Summary Acyanotic Atrial septal defect Ventricular septal defect Patent foramen ovale Patent ductus arteriosus Aortic coartation Pulmonary stenosis Cyanotic Tetralogy
CONGENITAL HEART DISEASE Uptofate Study Summary Acyanotic Atrial septal defect Ventricular septal defect Patent foramen ovale Patent ductus arteriosus Aortic coartation Pulmonary stenosis Cyanotic Tetralogy
Cardiac Emergencies in Infants. Michael Luceri, DO
 Cardiac Emergencies in Infants Michael Luceri, DO October 7, 2017 I have no financial obligations or conflicts of interest to disclose. Objectives Understand the scope of congenital heart disease Recognize
Cardiac Emergencies in Infants Michael Luceri, DO October 7, 2017 I have no financial obligations or conflicts of interest to disclose. Objectives Understand the scope of congenital heart disease Recognize
Congenital Heart Defects
 Normal Heart Congenital Heart Defects 1. Patent Ductus Arteriosus The ductus arteriosus connects the main pulmonary artery to the aorta. In utero, it allows the blood leaving the right ventricle to bypass
Normal Heart Congenital Heart Defects 1. Patent Ductus Arteriosus The ductus arteriosus connects the main pulmonary artery to the aorta. In utero, it allows the blood leaving the right ventricle to bypass
ECHOCARDIOGRAPHIC APPROACH TO CONGENITAL HEART DISEASE: THE UNOPERATED ADULT
 ECHOCARDIOGRAPHIC APPROACH TO CONGENITAL HEART DISEASE: THE UNOPERATED ADULT Karen Stout, MD, FACC Divisions of Cardiology University of Washington Medical Center Seattle Children s Hospital NO DISCLOSURES
ECHOCARDIOGRAPHIC APPROACH TO CONGENITAL HEART DISEASE: THE UNOPERATED ADULT Karen Stout, MD, FACC Divisions of Cardiology University of Washington Medical Center Seattle Children s Hospital NO DISCLOSURES
Paediatric Cardiology. Acyanotic CHD. Prof F F Takawira
 Paediatric Cardiology Acyanotic CHD Prof F F Takawira Aetiology Chromosomal Down syndrome, T13, T18 Genetic syndromes (gene defects) Velo-Cardio-facial (22 del) Genetic syndromes (undefined aetiology)
Paediatric Cardiology Acyanotic CHD Prof F F Takawira Aetiology Chromosomal Down syndrome, T13, T18 Genetic syndromes (gene defects) Velo-Cardio-facial (22 del) Genetic syndromes (undefined aetiology)
Screening for Critical Congenital Heart Disease
 Screening for Critical Congenital Heart Disease Caroline K. Lee, MD Pediatric Cardiology Disclosures I have no relevant financial relationships or conflicts of interest 1 Most Common Birth Defect Most
Screening for Critical Congenital Heart Disease Caroline K. Lee, MD Pediatric Cardiology Disclosures I have no relevant financial relationships or conflicts of interest 1 Most Common Birth Defect Most
2) VSD & PDA - Dr. Aso
 VSD & PDA - Dr. Aso") 2) VSD & PDA - Dr. Aso Ventricular Septal Defect (VSD) Most common cardiac malformation 25-30 % Types of VSD: According to position perimembranous, inlet, muscular. According to size small, medium, large.
2) VSD & PDA - Dr. Aso Ventricular Septal Defect (VSD) Most common cardiac malformation 25-30 % Types of VSD: According to position perimembranous, inlet, muscular. According to size small, medium, large.
Congenital Heart Disease An Approach for Simple and Complex Anomalies
 Congenital Heart Disease An Approach for Simple and Complex Anomalies Michael D. Pettersen, MD Director, Echocardiography Rocky Mountain Hospital for Children Denver, CO None Disclosures 1 ASCeXAM Contains
Congenital Heart Disease An Approach for Simple and Complex Anomalies Michael D. Pettersen, MD Director, Echocardiography Rocky Mountain Hospital for Children Denver, CO None Disclosures 1 ASCeXAM Contains
Pathophysiology: Left To Right Shunts
 Pathophysiology: Left To Right Shunts Daphne T. Hsu, MD dh17@columbia.edu Learning Objectives Learn the relationships between pressure, blood flow, and resistance Review the transition from fetal to mature
Pathophysiology: Left To Right Shunts Daphne T. Hsu, MD dh17@columbia.edu Learning Objectives Learn the relationships between pressure, blood flow, and resistance Review the transition from fetal to mature
3/14/2011 MANAGEMENT OF NEWBORNS CARDIAC INTENSIVE CARE CONFERENCE FOR HEALTH PROFESSIONALS IRVINE, CA. MARCH 7, 2011 WITH HEART DEFECTS
 CONFERENCE FOR HEALTH PROFESSIONALS IRVINE, CA. MARCH 7, 2011 MANAGEMENT OF NEWBORNS WITH HEART DEFECTS A NTHONY C. CHANG, MD, MBA, MPH M E D I C AL D I RE C T OR, HEART I N S T I T U T E C H I LDRE N
CONFERENCE FOR HEALTH PROFESSIONALS IRVINE, CA. MARCH 7, 2011 MANAGEMENT OF NEWBORNS WITH HEART DEFECTS A NTHONY C. CHANG, MD, MBA, MPH M E D I C AL D I RE C T OR, HEART I N S T I T U T E C H I LDRE N
How to Recognize a Suspected Cardiac Defect in the Neonate
 Neonatal Nursing Education Brief: How to Recognize a Suspected Cardiac Defect in the Neonate https://www.seattlechildrens.org/healthcareprofessionals/education/continuing-medical-nursing-education/neonatalnursing-education-briefs/
Neonatal Nursing Education Brief: How to Recognize a Suspected Cardiac Defect in the Neonate https://www.seattlechildrens.org/healthcareprofessionals/education/continuing-medical-nursing-education/neonatalnursing-education-briefs/
Pathophysiology: Left To Right Shunts
 Pathophysiology: Left To Right Shunts Daphne T. Hsu, MD dh17@columbia.edu Learning Objectives Learn the relationships between pressure, blood flow, and resistance Review the transition from fetal to mature
Pathophysiology: Left To Right Shunts Daphne T. Hsu, MD dh17@columbia.edu Learning Objectives Learn the relationships between pressure, blood flow, and resistance Review the transition from fetal to mature
Congenital Heart Disease. Mohamed Waheed Elsharief.
 Congenital Heart Disease Mohamed Waheed Elsharief. Objectives l By the end of this lecture you should be able to Fetal Circulation l For the fetus the placenta is the oxygenator so the lungs do little
Congenital Heart Disease Mohamed Waheed Elsharief. Objectives l By the end of this lecture you should be able to Fetal Circulation l For the fetus the placenta is the oxygenator so the lungs do little
Foetal Cardiology: How to predict perinatal problems. Prof. I.Witters Prof.M.Gewillig UZ Leuven
 Foetal Cardiology: How to predict perinatal problems Prof. I.Witters Prof.M.Gewillig UZ Leuven Cardiopathies Incidence : 8-12 / 1000 births ( 1% ) Most frequent - Ventricle Septum Defect 20% - Atrium Septum
Foetal Cardiology: How to predict perinatal problems Prof. I.Witters Prof.M.Gewillig UZ Leuven Cardiopathies Incidence : 8-12 / 1000 births ( 1% ) Most frequent - Ventricle Septum Defect 20% - Atrium Septum
Cardiac Catheterization Cases Primary Cardiac Diagnoses Facility 12 month period from to PRIMARY DIAGNOSES (one per patient)
") PRIMARY DIAGNOSES (one per patient) Septal Defects ASD (Atrial Septal Defect) PFO (Patent Foramen Ovale) ASD, Secundum ASD, Sinus venosus ASD, Coronary sinus ASD, Common atrium (single atrium) VSD (Ventricular
PRIMARY DIAGNOSES (one per patient) Septal Defects ASD (Atrial Septal Defect) PFO (Patent Foramen Ovale) ASD, Secundum ASD, Sinus venosus ASD, Coronary sinus ASD, Common atrium (single atrium) VSD (Ventricular
Congenital Heart Disease: Cyanotic Lesions. Amitesh Aggarwal
 Congenital Heart Disease: Cyanotic Lesions Amitesh Aggarwal 12 y/o male admitted because of dyspnea and cyanosis Patient has been cyanotic since few months after birth Has episodes of tachypnea and worsening
Congenital Heart Disease: Cyanotic Lesions Amitesh Aggarwal 12 y/o male admitted because of dyspnea and cyanosis Patient has been cyanotic since few months after birth Has episodes of tachypnea and worsening
Absent Pulmonary Valve Syndrome
 Absent Pulmonary Valve Syndrome Fact sheet on Absent Pulmonary Valve Syndrome In this condition, which has some similarities to Fallot's Tetralogy, there is a VSD with narrowing at the pulmonary valve.
Absent Pulmonary Valve Syndrome Fact sheet on Absent Pulmonary Valve Syndrome In this condition, which has some similarities to Fallot's Tetralogy, there is a VSD with narrowing at the pulmonary valve.
Adult Congenital Heart Disease: What All Echocardiographers Should Know Sharon L. Roble, MD, FACC Echo Hawaii 2016
 1 Adult Congenital Heart Disease: What All Echocardiographers Should Know Sharon L. Roble, MD, FACC Echo Hawaii 2016 DISCLOSURES I have no disclosures relevant to today s talk 2 Why should all echocardiographers
1 Adult Congenital Heart Disease: What All Echocardiographers Should Know Sharon L. Roble, MD, FACC Echo Hawaii 2016 DISCLOSURES I have no disclosures relevant to today s talk 2 Why should all echocardiographers
Children with Single Ventricle Physiology: The Possibilities
 Children with Single Ventricle Physiology: The Possibilities William I. Douglas, M.D. Pediatric Cardiovascular Surgery Children s Memorial Hermann Hospital The University of Texas Health Science Center
Children with Single Ventricle Physiology: The Possibilities William I. Douglas, M.D. Pediatric Cardiovascular Surgery Children s Memorial Hermann Hospital The University of Texas Health Science Center
Debate in Management of native COA; Balloon Versus Surgery
 Debate in Management of native COA; Balloon Versus Surgery Dr. Amira Esmat, El Tantawy, MD Professor of Pediatrics Consultant Pediatric Cardiac Interventionist Faculty of Medicine Cairo University 23/2/2017
Debate in Management of native COA; Balloon Versus Surgery Dr. Amira Esmat, El Tantawy, MD Professor of Pediatrics Consultant Pediatric Cardiac Interventionist Faculty of Medicine Cairo University 23/2/2017
Critical Heart Disease in the Newborn. What you need to know
 Critical Heart Disease in the Newborn What you need to know DISCLOSURES Nothing to report OBJECTIVES DESCRIBE NEONATAL CARDIOVASCULAR PHYSIOLOGY RECOGNIZE NEONATAL CARDIAC EMERGENCIES FORMULATE TREATMENT
Critical Heart Disease in the Newborn What you need to know DISCLOSURES Nothing to report OBJECTIVES DESCRIBE NEONATAL CARDIOVASCULAR PHYSIOLOGY RECOGNIZE NEONATAL CARDIAC EMERGENCIES FORMULATE TREATMENT
Adults with Congenital Heart Disease
 Adults with Congenital Heart Disease Edward K. Rhee, MD, FACC Director, Pediatric-Adult Congenital Arrhythmia Service SJHMC Disclosures & Disclaimer I have no lucrative financial relationships with industry
Adults with Congenital Heart Disease Edward K. Rhee, MD, FACC Director, Pediatric-Adult Congenital Arrhythmia Service SJHMC Disclosures & Disclaimer I have no lucrative financial relationships with industry
Introduction. Pediatric Cardiology. General Appearance. Tools of Assessment. Auscultation. Vital Signs
 Introduction Pediatric Cardiology An introduction to the pediatric patient with heart disease: M-III Lecture Douglas R. Allen, M.D. Assistant Professor and Director of Community Pediatric Cardiology at
Introduction Pediatric Cardiology An introduction to the pediatric patient with heart disease: M-III Lecture Douglas R. Allen, M.D. Assistant Professor and Director of Community Pediatric Cardiology at
Objectives Part 1. Objectives Part 2. Fetal Circulation Transition to Postnatal Circulation Normal Cardiac Anatomy Ductal Dependence and use of PGE1
 Cardiac Physiology Gia Marzano, AC PNP Pediatric Cardiac Surgery Rush Center for Congenital Heart Disease Rush University Medical Center Objectives Part 1 Fetal Circulation Transition to Postnatal Circulation
Cardiac Physiology Gia Marzano, AC PNP Pediatric Cardiac Surgery Rush Center for Congenital Heart Disease Rush University Medical Center Objectives Part 1 Fetal Circulation Transition to Postnatal Circulation
Common Defects With Expected Adult Survival:
 Common Defects With Expected Adult Survival: Bicuspid aortic valve :Acyanotic Mitral valve prolapse Coarctation of aorta Pulmonary valve stenosis Atrial septal defect Patent ductus arteriosus (V.S.D.)
Common Defects With Expected Adult Survival: Bicuspid aortic valve :Acyanotic Mitral valve prolapse Coarctation of aorta Pulmonary valve stenosis Atrial septal defect Patent ductus arteriosus (V.S.D.)
Ummeenatrbilaoiasetptiwmsaiiri
 atrial This This atrial CIRCULATORY CHANGES My My pressure In the foetus the left atrial is low as relatively Ummeenatrbilaoiasetptiwmsaiiri ze@fgffmftheyubsidtritupyeiirieminfyifjjtajefjjieiminylntentiiiarmmnitnteimiiiinc1udingfromthepl9centaj
atrial This This atrial CIRCULATORY CHANGES My My pressure In the foetus the left atrial is low as relatively Ummeenatrbilaoiasetptiwmsaiiri ze@fgffmftheyubsidtritupyeiirieminfyifjjtajefjjieiminylntentiiiarmmnitnteimiiiinc1udingfromthepl9centaj
ADULT CONGENITAL HEART DISEASE. Stuart Lilley
 ADULT CONGENITAL HEART DISEASE Stuart Lilley More adults than children have congenital heart disease Huge variety of congenital lesions from minor to major Heart failure, re-operation and arrhythmia are
ADULT CONGENITAL HEART DISEASE Stuart Lilley More adults than children have congenital heart disease Huge variety of congenital lesions from minor to major Heart failure, re-operation and arrhythmia are
Chapter 2 Cardiac Interpretation of Pediatric Chest X-Ray
 Chapter 2 Cardiac Interpretation of Pediatric Chest X-Ray Ra-id Abdulla and Douglas M. Luxenberg Key Facts The cardiac silhouette occupies 50 55% of the chest width on an anterior posterior chest X-ray
Chapter 2 Cardiac Interpretation of Pediatric Chest X-Ray Ra-id Abdulla and Douglas M. Luxenberg Key Facts The cardiac silhouette occupies 50 55% of the chest width on an anterior posterior chest X-ray
9/8/2009 < 1 1,2 3,4 5,6 7,8 9,10 11,12 13,14 15,16 17,18 > 18. Tetralogy of Fallot. Complex Congenital Heart Disease.
 Current Indications for Pediatric CTA S Bruce Greenberg Professor of Radiology Arkansas Children s Hospital University of Arkansas for Medical Sciences greenbergsbruce@uams.edu 45 40 35 30 25 20 15 10
Current Indications for Pediatric CTA S Bruce Greenberg Professor of Radiology Arkansas Children s Hospital University of Arkansas for Medical Sciences greenbergsbruce@uams.edu 45 40 35 30 25 20 15 10
Echocardiography in Adult Congenital Heart Disease
 Echocardiography in Adult Congenital Heart Disease Michael Vogel Kinderherz-Praxis München CHD missed in childhood Subsequent lesions after repaired CHD Follow-up of cyanotic heart disease CHD missed in
Echocardiography in Adult Congenital Heart Disease Michael Vogel Kinderherz-Praxis München CHD missed in childhood Subsequent lesions after repaired CHD Follow-up of cyanotic heart disease CHD missed in
Index. cardiology.theclinics.com. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A ACHD. See Adult congenital heart disease (ACHD) Adult congenital heart disease (ACHD), 503 512 across life span prevalence of, 504 506
Index Note: Page numbers of article titles are in boldface type. A ACHD. See Adult congenital heart disease (ACHD) Adult congenital heart disease (ACHD), 503 512 across life span prevalence of, 504 506
CongHeartDis.doc. Андрій Миколайович Лобода
 CongHeartDis.doc Андрій Миколайович Лобода 2015 Зміст 3 Зміст Зміст 4 A child with tetralogy of Fallot is most likely to exhibit: -Increased pulmonary blood flow -Increased pressure in the right ventricle
CongHeartDis.doc Андрій Миколайович Лобода 2015 Зміст 3 Зміст Зміст 4 A child with tetralogy of Fallot is most likely to exhibit: -Increased pulmonary blood flow -Increased pressure in the right ventricle
Neonatal Cardiac Anomalies
 Objectives Neonatal Cardiac Anomalies Karen Knuth, RNC, MN, NNP-BC, ARNP Seattle Childrens Hospital What is CHD? Normal anatomy and circulation Clinical presentation: signs and symptoms Diagnostics Common
Objectives Neonatal Cardiac Anomalies Karen Knuth, RNC, MN, NNP-BC, ARNP Seattle Childrens Hospital What is CHD? Normal anatomy and circulation Clinical presentation: signs and symptoms Diagnostics Common
بسم هللا الرحمن الرحيم. The cardio vascular system By Dr.Rawa Younis Mahmood
 بسم هللا الرحمن الرحيم The cardio vascular system By Dr.Rawa Younis Mahmood Introduction Evaluation of the cardio vascular system depend on history and physical examination by : Asking about cyanosis,blueness
بسم هللا الرحمن الرحيم The cardio vascular system By Dr.Rawa Younis Mahmood Introduction Evaluation of the cardio vascular system depend on history and physical examination by : Asking about cyanosis,blueness
Born Blue. Anesthesia and CHD. Kristine Faust, CRNA, MS, MBA, DNAP
 Born Blue Anesthesia and CHD Kristine Faust, CRNA, MS, MBA, DNAP Disclosures Disclosures None to Report Objectives Review all congenital defects in which the patient is blue Describe physiology of the
Born Blue Anesthesia and CHD Kristine Faust, CRNA, MS, MBA, DNAP Disclosures Disclosures None to Report Objectives Review all congenital defects in which the patient is blue Describe physiology of the
Upon completion of this presentation, the participant will be able to:
 B12 Neonatal Cardiology Review Nicole Bowie, NNP-/BC, PNP Neonatal Nurse Practitioner Jackson Memorial Hospital, Miami, FL The speaker has signed a disclosure form and indicated she has no significant
B12 Neonatal Cardiology Review Nicole Bowie, NNP-/BC, PNP Neonatal Nurse Practitioner Jackson Memorial Hospital, Miami, FL The speaker has signed a disclosure form and indicated she has no significant
FANNP 28TH NATIONAL NNP SYMPOSIUM: CLINICAL UPDATE AND REVIEW OCTOBER 17-21, 2017
 Neonatal Cardiology Review Nicole Bowie, NNP/BC, PNP Neonatal Nurse Practitioner Jackson Memorial Hospital, Miami, FL B12 The speaker has signed a disclosure statement indicating that she has no significant
Neonatal Cardiology Review Nicole Bowie, NNP/BC, PNP Neonatal Nurse Practitioner Jackson Memorial Hospital, Miami, FL B12 The speaker has signed a disclosure statement indicating that she has no significant
Echocardiographic assessment in Adult Patients with Congenital Heart Diseases
 Echocardiographic assessment in Adult Patients with Congenital Heart Diseases Athanasios Koutsakis Cardiologist, Cl. Research Fellow George Giannakoulas Ass. Professor in Cardiology 1st Cardiology Department,
Echocardiographic assessment in Adult Patients with Congenital Heart Diseases Athanasios Koutsakis Cardiologist, Cl. Research Fellow George Giannakoulas Ass. Professor in Cardiology 1st Cardiology Department,
CYANOTIC CONGENITAL HEART DISEASES. PRESENTER: DR. Myra M. Koech Pediatric cardiologist MTRH/MU
 CYANOTIC CONGENITAL HEART DISEASES PRESENTER: DR. Myra M. Koech Pediatric cardiologist MTRH/MU DEFINITION Congenital heart diseases are defined as structural and functional problems of the heart that are
CYANOTIC CONGENITAL HEART DISEASES PRESENTER: DR. Myra M. Koech Pediatric cardiologist MTRH/MU DEFINITION Congenital heart diseases are defined as structural and functional problems of the heart that are
"Lecture Index. 1) Heart Progenitors. 2) Cardiac Tube Formation. 3) Valvulogenesis and Chamber Formation. 4) Epicardium Development.
 Heart Progenitors. 2) Cardiac Tube Formation. 3) Valvulogenesis and Chamber Formation. 4) Epicardium Development.") "Lecture Index 1) Heart Progenitors. 2) Cardiac Tube Formation. 3) Valvulogenesis and Chamber Formation. 4) Epicardium Development. 5) Septation and Maturation. 6) Changes in Blood Flow during Development.
"Lecture Index 1) Heart Progenitors. 2) Cardiac Tube Formation. 3) Valvulogenesis and Chamber Formation. 4) Epicardium Development. 5) Septation and Maturation. 6) Changes in Blood Flow during Development.
MEDICAL MANAGEMENT WITH CAVEATS 1. In one study of 50 CHARGE patients with CHD, 75% required surgery. 2. Children with CHARGE may be resistant to chlo
 CARDIOLOGY IN CHARGE SYNDROME: FOR THE PHYSICIAN Angela E. Lin, M.D. Teratology Program/Active Malformation Surveillance, Brigham and Women's Hospital, Old PBBH-B501, 75 Francis St., Boston, MA 02115 alin@partners.org
CARDIOLOGY IN CHARGE SYNDROME: FOR THE PHYSICIAN Angela E. Lin, M.D. Teratology Program/Active Malformation Surveillance, Brigham and Women's Hospital, Old PBBH-B501, 75 Francis St., Boston, MA 02115 alin@partners.org
PedsCases Podcast Scripts
 PedsCases Podcast Scripts This is a text version of a podcast from Pedscases.com on Acyanotic Congenital Heart Lesions. These podcasts are designed to give medical students an overview of key topics in
PedsCases Podcast Scripts This is a text version of a podcast from Pedscases.com on Acyanotic Congenital Heart Lesions. These podcasts are designed to give medical students an overview of key topics in
Hypoplastic Left Heart Syndrome: Echocardiographic Assessment
 Hypoplastic Left Heart Syndrome: Echocardiographic Assessment Craig E Fleishman, MD, FACC, FASE Director, Non-invasive Cardiac Imaging The Hear Center at Arnold Palmer Hospital for Children, Orlando SCAI
Hypoplastic Left Heart Syndrome: Echocardiographic Assessment Craig E Fleishman, MD, FACC, FASE Director, Non-invasive Cardiac Imaging The Hear Center at Arnold Palmer Hospital for Children, Orlando SCAI
Approach to a baby with cyanosis
 Approach to a baby with cyanosis Objectives Cyanosis : types Differentials: cardiac vs. non cardiac Approach Case scenarios Cyanosis Greek word kuaneos meaning dark blue Bluish discolouration of skin,
Approach to a baby with cyanosis Objectives Cyanosis : types Differentials: cardiac vs. non cardiac Approach Case scenarios Cyanosis Greek word kuaneos meaning dark blue Bluish discolouration of skin,
Cardiology Competency Based Goals and Objectives
 Cardiology Competency Based Goals and Objectives COMPETENCY 1. Patient Care. Provide family centered patient care that is developmentally and age appropriate, compassionate, and effective for the treatment
Cardiology Competency Based Goals and Objectives COMPETENCY 1. Patient Care. Provide family centered patient care that is developmentally and age appropriate, compassionate, and effective for the treatment
Data Collected: June 17, Reported: June 30, Survey Dates 05/24/ /07/2010
 Job Task Analysis for ARDMS Pediatric Echocardiography Data Collected: June 17, 2010 Reported: Analysis Summary For: Pediatric Echocardiography Exam Survey Dates 05/24/2010-06/07/2010 Invited Respondents
Job Task Analysis for ARDMS Pediatric Echocardiography Data Collected: June 17, 2010 Reported: Analysis Summary For: Pediatric Echocardiography Exam Survey Dates 05/24/2010-06/07/2010 Invited Respondents
SPECIFIC HEART DEFECTS
 A. Acyanotic Defects 1. Ventricular Septal Defect (VSD): SPECIFIC HEART DEFECTS Which side of the heart is stronger? Left This is when there is an opening between the left and right ventricle (in the septum)
A. Acyanotic Defects 1. Ventricular Septal Defect (VSD): SPECIFIC HEART DEFECTS Which side of the heart is stronger? Left This is when there is an opening between the left and right ventricle (in the septum)
The Chest X-ray for Cardiologists
 Mayo Clinic & British Cardiovascular Society at the Royal College of Physicians, London : 21-23-October 2013 Cases-Controversies-Updates 2013 The Chest X-ray for Cardiologists Michael Rubens Royal Brompton
Mayo Clinic & British Cardiovascular Society at the Royal College of Physicians, London : 21-23-October 2013 Cases-Controversies-Updates 2013 The Chest X-ray for Cardiologists Michael Rubens Royal Brompton
AORTIC COARCTATION. Synonyms: - Coarctation of the aorta
 AORTIC COARCTATION Synonyms: - Coarctation of the aorta Definition: Aortic coarctation is a congenital narrowing of the aorta, usually located after the left subclavian artery, near the ductus or the ligamentum
AORTIC COARCTATION Synonyms: - Coarctation of the aorta Definition: Aortic coarctation is a congenital narrowing of the aorta, usually located after the left subclavian artery, near the ductus or the ligamentum
What is the Definition of Small Systemic Ventricle. Hong Ryang Kil, MD Department of Pediatrics, College of Medicine, Chungnam National University
 What is the Definition of Small Systemic Ventricle Hong Ryang Kil, MD Department of Pediatrics, College of Medicine, Chungnam National University Contents Introduction Aortic valve stenosis Aortic coarctation
What is the Definition of Small Systemic Ventricle Hong Ryang Kil, MD Department of Pediatrics, College of Medicine, Chungnam National University Contents Introduction Aortic valve stenosis Aortic coarctation
Cardiac MRI in ACHD What We. ACHD Patients
 Cardiac MRI in ACHD What We Have Learned to Apply to ACHD Patients Faris Al Mousily, MBChB, FAAC, FACC Consultant, Pediatric Cardiology, KFSH&RC/Jeddah Adjunct Faculty, Division of Pediatric Cardiology
Cardiac MRI in ACHD What We Have Learned to Apply to ACHD Patients Faris Al Mousily, MBChB, FAAC, FACC Consultant, Pediatric Cardiology, KFSH&RC/Jeddah Adjunct Faculty, Division of Pediatric Cardiology
Pediatric Echocardiography Examination Content Outline
 Pediatric Echocardiography Examination Content Outline (Outline Summary) # Domain Subdomain Percentage 1 Anatomy and Physiology Normal Anatomy and Physiology 10% 2 Abnormal Pathology and Pathophysiology
Pediatric Echocardiography Examination Content Outline (Outline Summary) # Domain Subdomain Percentage 1 Anatomy and Physiology Normal Anatomy and Physiology 10% 2 Abnormal Pathology and Pathophysiology
Heart and Lungs. LUNG Coronal section demonstrates relationship of pulmonary parenchyma to heart and chest wall.
 Heart and Lungs Normal Sonographic Anatomy THORAX Axial and coronal sections demonstrate integrity of thorax, fetal breathing movements, and overall size and shape. LUNG Coronal section demonstrates relationship
Heart and Lungs Normal Sonographic Anatomy THORAX Axial and coronal sections demonstrate integrity of thorax, fetal breathing movements, and overall size and shape. LUNG Coronal section demonstrates relationship
Heart and Soul Evaluation of the Fetal Heart
 Heart and Soul Evaluation of the Fetal Heart Ivana M. Vettraino, M.D., M.B.A. Clinical Associate Professor, Michigan State University College of Human Medicine Objectives Review the embryology of the formation
Heart and Soul Evaluation of the Fetal Heart Ivana M. Vettraino, M.D., M.B.A. Clinical Associate Professor, Michigan State University College of Human Medicine Objectives Review the embryology of the formation
Adult Congenital Heart Disease for the Internist
 Adult Congenital Heart Disease for the Internist Saurabh Rajpal, MBBS, MD Assistant Professor Department of Internal Medicine Division of Cardiovascular Medicine The Ohio State University Wexner Medical
Adult Congenital Heart Disease for the Internist Saurabh Rajpal, MBBS, MD Assistant Professor Department of Internal Medicine Division of Cardiovascular Medicine The Ohio State University Wexner Medical
Adult Congenital Heart Disease for the Internist
 Adult Congenital Heart Disease for the Internist Saurabh Rajpal, MBBS, MD Assistant Professor Department of Internal Medicine Division of Cardiovascular Medicine The Ohio State University Wexner Medical
Adult Congenital Heart Disease for the Internist Saurabh Rajpal, MBBS, MD Assistant Professor Department of Internal Medicine Division of Cardiovascular Medicine The Ohio State University Wexner Medical
Miscellaneous Cardiology Topics pregnancy - congenital - myocarditis - pericardial disease. Pregnancy and Cardiovascular Disease MCQ
 Miscellaneous Cardiology Topics pregnancy - congenital - myocarditis - pericardial disease Maan Jokhadar, MD, FACC Emory Center for Advanced Heart Failure Therapy Emory Adult Congenital Heart Center Pregnancy
Miscellaneous Cardiology Topics pregnancy - congenital - myocarditis - pericardial disease Maan Jokhadar, MD, FACC Emory Center for Advanced Heart Failure Therapy Emory Adult Congenital Heart Center Pregnancy
The blue baby. Case 4
 Case 4 The blue baby Mrs Smith has brought her baby to A&E because she says he has started turning blue. What are your immediate differential diagnoses? 1 Respiratory causes: Congenital respiratory disorder.
Case 4 The blue baby Mrs Smith has brought her baby to A&E because she says he has started turning blue. What are your immediate differential diagnoses? 1 Respiratory causes: Congenital respiratory disorder.
PAEDIATRIC EMQs. Andrew A Mallick Paediatrics.info.
 PAEDIATRIC EMQs Andrew A Mallick Paediatrics.info www.paediatrics.info Paediatric EMQs Paediatrics.info First published in the United Kingdom in 2012. While the advice and information in this book is believed
PAEDIATRIC EMQs Andrew A Mallick Paediatrics.info www.paediatrics.info Paediatric EMQs Paediatrics.info First published in the United Kingdom in 2012. While the advice and information in this book is believed
HISTORY. Question: What category of heart disease is suggested by this history? CHIEF COMPLAINT: Heart murmur present since early infancy.
 HISTORY 18-year-old man. CHIEF COMPLAINT: Heart murmur present since early infancy. PRESENT ILLNESS: Although normal at birth, a heart murmur was heard at the six week check-up and has persisted since
HISTORY 18-year-old man. CHIEF COMPLAINT: Heart murmur present since early infancy. PRESENT ILLNESS: Although normal at birth, a heart murmur was heard at the six week check-up and has persisted since
The Blue Baby. Network Stabilisation of the Term Infant Study Day 15 th March 2017 Joanna Behrsin
 The Blue Baby Network Stabilisation of the Term Infant Study Day 15 th March 2017 Joanna Behrsin Session Structure Definitions and assessment of cyanosis Causes of blue baby Structured approach to assessing
The Blue Baby Network Stabilisation of the Term Infant Study Day 15 th March 2017 Joanna Behrsin Session Structure Definitions and assessment of cyanosis Causes of blue baby Structured approach to assessing
Most common fetal cardiac anomalies
 Most common fetal cardiac anomalies Common congenital heart defects CHD % of cardiac defects Chromosomal Infants Fetuses anomaly (%) 22q11 deletion (%) VSD 30 5~10 20~40 10 PS 9 5 (PA w/ VSD) HLHS 7~9
Most common fetal cardiac anomalies Common congenital heart defects CHD % of cardiac defects Chromosomal Infants Fetuses anomaly (%) 22q11 deletion (%) VSD 30 5~10 20~40 10 PS 9 5 (PA w/ VSD) HLHS 7~9
Index. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A Acute coronary syndrome(s), anticoagulant therapy in, 706, 707 antiplatelet therapy in, 702 ß-blockers in, 703 cardiac biomarkers in,
Index Note: Page numbers of article titles are in boldface type. A Acute coronary syndrome(s), anticoagulant therapy in, 706, 707 antiplatelet therapy in, 702 ß-blockers in, 703 cardiac biomarkers in,
DORV: The Great Chameleon. Heart Conference October 15, 2016 Tina Kwan, MD
 DORV: The Great Chameleon Heart Conference October 15, 2016 Tina Kwan, MD Kenneth Maehara, Ph.D. May 7, 1942 - August 26, 2013 A.R. A classic case of broken heart 38 week AGA F born at an OSH to
DORV: The Great Chameleon Heart Conference October 15, 2016 Tina Kwan, MD Kenneth Maehara, Ph.D. May 7, 1942 - August 26, 2013 A.R. A classic case of broken heart 38 week AGA F born at an OSH to
Survival Rates of Children with Congenital Heart Disease continue to improve.
 DOROTHY RADFORD Survival Rates of Children with Congenital Heart Disease continue to improve. 1940-20% 1960-40% 1980-70% 2010->90% Percentage of children with CHD reaching age of 18 years 1938 First Patent
DOROTHY RADFORD Survival Rates of Children with Congenital Heart Disease continue to improve. 1940-20% 1960-40% 1980-70% 2010->90% Percentage of children with CHD reaching age of 18 years 1938 First Patent
Adult Echocardiography Examination Content Outline
 Adult Echocardiography Examination Content Outline (Outline Summary) # Domain Subdomain Percentage 1 2 3 4 5 Anatomy and Physiology Pathology Clinical Care and Safety Measurement Techniques, Maneuvers,
Adult Echocardiography Examination Content Outline (Outline Summary) # Domain Subdomain Percentage 1 2 3 4 5 Anatomy and Physiology Pathology Clinical Care and Safety Measurement Techniques, Maneuvers,
The complications of cardiac surgery:
 The complications of cardiac surgery: a walk on the Dark Side? Prof Rik De Decker Red Cross Children s Hospital CME Nov/Dec 2011 http://www.cmej.org.za Why should you care? You are about to leave your
The complications of cardiac surgery: a walk on the Dark Side? Prof Rik De Decker Red Cross Children s Hospital CME Nov/Dec 2011 http://www.cmej.org.za Why should you care? You are about to leave your
Cases in Adult Congenital Heart Disease
 Cases in Adult Congenital Heart Disease Sabrina Phillips, MD FACC FASE Associate Professor of Medicine The University of Oklahoma Health Sciences Center No Disclosures I Have Palpitations 18 Year old Man
Cases in Adult Congenital Heart Disease Sabrina Phillips, MD FACC FASE Associate Professor of Medicine The University of Oklahoma Health Sciences Center No Disclosures I Have Palpitations 18 Year old Man
September 26, 2012 Philip Stockwell, MD Lifespan CVI Assistant Professor of Medicine (Clinical)
") September 26, 2012 Philip Stockwell, MD Lifespan CVI Assistant Professor of Medicine (Clinical) Advances in cardiac surgery have created a new population of adult patients with repaired congenital heart
September 26, 2012 Philip Stockwell, MD Lifespan CVI Assistant Professor of Medicine (Clinical) Advances in cardiac surgery have created a new population of adult patients with repaired congenital heart
SURGICAL TREATMENT AND OUTCOME OF CONGENITAL HEART DISEASE
 SURGICAL TREATMENT AND OUTCOME OF CONGENITAL HEART DISEASE Mr. W. Brawn Birmingham Children s Hospital. Aims of surgery The aim of surgery in congenital heart disease is to correct or palliate the heart
SURGICAL TREATMENT AND OUTCOME OF CONGENITAL HEART DISEASE Mr. W. Brawn Birmingham Children s Hospital. Aims of surgery The aim of surgery in congenital heart disease is to correct or palliate the heart
APPROACH TO CARDIAC HISTORY TAKING. Index
 Christopher Cheung APPROACH TO CARDIAC HISTORY TAKING Index General Presentation...1 2 Table 1 Congenital Heart Conditions...2 Questions to Ask...2 Table 2 PQRSTAAA Mnemonic Approach to Chest Pain...3
Christopher Cheung APPROACH TO CARDIAC HISTORY TAKING Index General Presentation...1 2 Table 1 Congenital Heart Conditions...2 Questions to Ask...2 Table 2 PQRSTAAA Mnemonic Approach to Chest Pain...3
Notes: 1)Membranous part contribute in the formation of small portion in the septal cusp.
Membranous part contribute in the formation of small portion in the septal cusp.") Embryology 9 : Slide 16 : There is a sulcus between primitive ventricular and bulbis cordis that will disappear gradually and lead to the formation of one chamber which is called bulboventricular chamber.
Embryology 9 : Slide 16 : There is a sulcus between primitive ventricular and bulbis cordis that will disappear gradually and lead to the formation of one chamber which is called bulboventricular chamber.
Total Anomalous Pulmonary Venous Connections: Anatomy and Diagnostic Imaging
 Total Anomalous Pulmonary Venous Connections: Anatomy and Diagnostic Imaging Timothy Slesnick, MD March 12, 2015 Congenital Cardiac Anesthesia Society Annual Meeting Disclosures I will discuss the use
Total Anomalous Pulmonary Venous Connections: Anatomy and Diagnostic Imaging Timothy Slesnick, MD March 12, 2015 Congenital Cardiac Anesthesia Society Annual Meeting Disclosures I will discuss the use
How to Assess and Treat Obstructive Lesions
 How to Assess and Treat Obstructive Lesions Erwin Oechslin, MD, FESC, FRCPC, Director, Congenital Cardiac Centre for Adults Peter Munk Cardiac Centre University Health Network/Toronto General Hospital
How to Assess and Treat Obstructive Lesions Erwin Oechslin, MD, FESC, FRCPC, Director, Congenital Cardiac Centre for Adults Peter Munk Cardiac Centre University Health Network/Toronto General Hospital
Complex Congenital Heart Disease in Adults
 Complex Congenital Heart Disease in Adults Linda B. Haramati, MD Disclosures Complex Congenital Heart Disease in Adults Linda B. Haramati MD, MS Jeffrey M. Levsky MD, PhD Meir Scheinfeld MD, PhD Department
Complex Congenital Heart Disease in Adults Linda B. Haramati, MD Disclosures Complex Congenital Heart Disease in Adults Linda B. Haramati MD, MS Jeffrey M. Levsky MD, PhD Meir Scheinfeld MD, PhD Department
Surgical Procedures. Direct suture of small ASDs Patch repair Transcatheter closure with a prosthetic device called occluder
 PEDIATRIC Review Surgical Procedures Atrial Septal Defect repair: Direct suture of small ASDs Patch repair Transcatheter closure with a prosthetic device called occluder Balloon atrial septostomy (Rashkind)
PEDIATRIC Review Surgical Procedures Atrial Septal Defect repair: Direct suture of small ASDs Patch repair Transcatheter closure with a prosthetic device called occluder Balloon atrial septostomy (Rashkind)
Nursing Care of Children and their Families: Alterations in Cardiac Function
 Nursing Care of Children and their Families: Alterations in Cardiac Function Congenital Heart Disease Incidence 4-10 per live births Extra cardiac defects: TE fistula, renal agenesis and diaphragmatic
Nursing Care of Children and their Families: Alterations in Cardiac Function Congenital Heart Disease Incidence 4-10 per live births Extra cardiac defects: TE fistula, renal agenesis and diaphragmatic
Pattern of Congenital Heart Disease A Hospital-Based Study *Sadiq Mohammed Al-Hamash MBChB, FICMS
 Pattern of Congenital Heart Disease A Hospital-Based Study *Sadiq Mohammed Al-Hamash MBChB, FICMS ABSTRACT Background: The congenital heart disease occurs in 0,8% of live births and they have a wide spectrum
Pattern of Congenital Heart Disease A Hospital-Based Study *Sadiq Mohammed Al-Hamash MBChB, FICMS ABSTRACT Background: The congenital heart disease occurs in 0,8% of live births and they have a wide spectrum
: Provide cardiovascular preventive counseling to parents and patients with specific cardiac diseases about:
 Children s Hospital & Research Center Oakland Cardiology Primary Goals for this Rotation 5.13 GOAL: Prevention, Counseling and Screening (Cardiovascular). Understand the role of the pediatrician in preventing
Children s Hospital & Research Center Oakland Cardiology Primary Goals for this Rotation 5.13 GOAL: Prevention, Counseling and Screening (Cardiovascular). Understand the role of the pediatrician in preventing
Anomalous Systemic Venous Connection Systemic venous anomaly
 World Database for Pediatric and Congenital Heart Surgery Appendix B: Diagnosis (International Paediatric and Congenital Cardiac Codes (IPCCC) and definitions) Anomalous Systemic Venous Connection Systemic
World Database for Pediatric and Congenital Heart Surgery Appendix B: Diagnosis (International Paediatric and Congenital Cardiac Codes (IPCCC) and definitions) Anomalous Systemic Venous Connection Systemic
MEDICAL SCIENCES Vol.I -Adult Congenital Heart Disease: A Challenging Population - Khalid Aly Sorour
 ADULT CONGENITAL HEART DISEASE: A CHALLENGING POPULATION Khalid Aly Sorour Cairo University, Kasr elaini Hospital, Egypt Keywords: Congenital heart disease, adult survival, specialized care centers. Contents
ADULT CONGENITAL HEART DISEASE: A CHALLENGING POPULATION Khalid Aly Sorour Cairo University, Kasr elaini Hospital, Egypt Keywords: Congenital heart disease, adult survival, specialized care centers. Contents
CONGENITAL HEART LESIONS ((C.H.L
 CONGENITAL HEART LESIONS ((C.H.L BY THE BOOKS: 0.8 IN FACT: 3-5% INCLUDING: - BICUSPID AORTIC VALVE MITRAL VALVE PROLAPSE LATE DIAGNOSIS - :INCREASED INCIDENCE IN ADULTS BETTER DIAGNOSIS IN INFANCY BETTER
CONGENITAL HEART LESIONS ((C.H.L BY THE BOOKS: 0.8 IN FACT: 3-5% INCLUDING: - BICUSPID AORTIC VALVE MITRAL VALVE PROLAPSE LATE DIAGNOSIS - :INCREASED INCIDENCE IN ADULTS BETTER DIAGNOSIS IN INFANCY BETTER
NCC Review Cardiac 8/22/12. Intrauterine Blood Flow. Topics
 NCC Review Cardiac Tracey Buckley MSN,RNC, NNP-BC Cape Fear Valley Health System Topics Transition to Extrauterine Life Cyanosis Congenital Heart Disease (CHD) Clinical Manifestations of CHD Therapeutic
NCC Review Cardiac Tracey Buckley MSN,RNC, NNP-BC Cape Fear Valley Health System Topics Transition to Extrauterine Life Cyanosis Congenital Heart Disease (CHD) Clinical Manifestations of CHD Therapeutic
Case submission for CSI Asia-Pacific Case 2
 Case submission for CSI Asia-Pacific 2018- Case 2 Title Page Case category: Coarctation and ducts, valves Title: Simultaneous balloon aortic valvuloplasty with transcatheter closure of large hypertensive
Case submission for CSI Asia-Pacific 2018- Case 2 Title Page Case category: Coarctation and ducts, valves Title: Simultaneous balloon aortic valvuloplasty with transcatheter closure of large hypertensive