Young high risk patients the role of statins Dr. Mohamed Jeilan
|
|
|
- Steven Stewart
- 5 years ago
- Views:
Transcription
1 Young high risk patients the role of statins Dr. Mohamed Jeilan KCS Congress: Impact through collaboration CONTACT: Tel Web:
2 Disclosures Conflict of Interests Astra Zeneca Honoraria
3 Disclaimer AstraZeneca does not advocate the use of its products in any manner unless as indicated in the registered prescribing information. The information contained in this material is not intended or implied to be a substitute for professional medical advice, diagnosis or treatment. AstraZeneca makes no representation and assumes no responsibility for the accuracy of the information contained on this material. AstraZeneca is not responsible for any liability, loss, risk, personal or otherwise which is or may be incurred as a consequence, directly or indirectly, of the use and application of any of the information contained in this material.
4 A 60 yr. old man is referred because of hypercholesterolaemia (total cholesterol 240mg/dL). His HDL is 45mg/dL and his systolic blood pressure is 135. He is a smoker who cannot quit and he has a family history of coronary artery disease. He has no other risk factors.
5 How should he be treated? 10 yr. risk (ASCVD calculator) 19%
6 A 30 yr. old man is referred because of hypercholesterolaemia (total cholesterol 240mg/dL). His HDL risk is 45mg/dL and his systolic blood pressure is 135. He is a smoker who cannot quit and he has a family history of coronary artery disease. He has no other risk factors.
7 Should he receive a statin? 10 yr. risk 6% (Framingham) Lifetime risk 67% (Framingham)


8
9 Most MI s in Africa occur in young patients 01 Most Africans are young true 02 But when did they get the disease?
10 A 27 yr. old male patient presents with chest pain and ST depression.
11
12
13 The fatty streak is the father of atherosclerosis JAMA 1999 Pathological Determinants of Atherosclerosis in the Young is seen in 30% of Korean war veterans in (mean age 22) is seen in 37% of organ donors age has the same risk factor profile as those that predict INFARCTION in adults (cholesterol, HTN, cigarettes)
14 Bogalusa Heart Study NEJM % of children and 85% of adults have fatty streaks Fibrous plaques increase from 8% to 69% as you progress from childhood to third decade Strong correlation with cholesterol (LDL) concentration Rise in obesity, T2DM and hypertension in young adults and children
15 CV Risk factors in children Rise in obesity, T2DM and hypertension in young adults and children
:2823-8.")
16 Continuous, graded, strong relationship between serum cholesterol and sixyear age-adjusted CHD death rate JAMA Nov 28;256(20):
 NHLBI updated this guidance in 2011 When (at what age)?")
17 Childhood dyslipidaemia is on the rise and is increasingly understood as a risk factor for atherosclerotic disease American Academy of Paediatrics recommend screening for this condition (2008) NHLBI updated this guidance in 2011 When (at what age)?
18
19
20 Age 2 to 8 Age 12 to 20 Positive FHx of premature ASCVD BMI > 95 th percentile, hypertension (>95th percentile), smoking, diabetes
21 Screening what are the guidelines? Issuing Organization Year Populations to be Screened Screening Measurement Screening Interval USPSTF [23] 2008 (update in progress) Men 35 years: Universal screening Men years: if at increased risk for coronary heart disease (CHD) Women 20 years: if at increased risk for CHD Fasting or non-fasting lipid panel Uncertain; every 5 years, with shorter intervals for individuals with elevated lipid levels and longer intervals for those not at increased risk with normal lipid levels ACC/AHA [24] 2013 Adults years None given Every 4-6 years if free of ASCVD ESC/EAS [28] 2011 Adults with any of the following risk factors: Type 2 diabetes Obesity Hypertension Smoker Chronic inflammatory disease Chronic kidney disease Family history of premature cardiovascular disease (CVD) or familial dyslipidemia Men 40 years and Women 50 years or post-menopausal: Consider screening Fasting lipid panel with calculation of non-hdl-c and TC/HDL-C ratio; apob or apob/apoa1 ratio considered alternate risk factors None given
22 Screening what are the guidelines? Issuing Organization Year Populations to be Screened Screening Measurement Screening Interval USPSTF [23] 2008 (update in progress) Men 35 years: Universal screening Men years: if at increased risk for coronary heart disease (CHD) Women 20 years: if at increased risk for CHD Fasting or non-fasting lipid panel Uncertain; every 5 years, with shorter intervals for individuals with elevated lipid levels and longer intervals for those not at increased risk with normal lipid levels ACC/AHA [24] 2013 Adults >21 years None given Every 4-6 years if free of ASCVD ESC/EAS [28] 2011 Adults with any of the following risk factors: Type 2 diabetes Obesity Hypertension Smoker Chronic inflammatory disease Chronic kidney disease Family history of premature cardiovascular disease (CVD) or familial dyslipidemia Men 40 years and Women 50 years or post-menopausal: Consider screening Fasting lipid panel with calculation of non-hdl-c and TC/HDL-C ratio; apob or apob/apoa1 ratio considered alternate risk factors None given
23 The interventions Diet Lifestyle modifications including activity and exercise Smoking cessation Statin Aspirin
24 The interventions Diet how effective is it? Lifestyle modifications including activity and exercise Smoking cessation Statin Aspirin
25 The interventions Diet how effective is it? Lifestyle modifications including activity and exercise Smoking cessation Statin Aspirin
 and 0.56 (95 percent confidence interval, 0.33 to 0.93), respectively")
26 Cox proportional-hazards regression showed that for men who consumed 35 g or more of fish daily as compared with those who consumed none, the relative risks of death from coronary heart disease and from sudden or nonsudden myocardial infarction were 0.62 (95 percent confidence interval, 0.40 to 0.94) and 0.56 (95 percent confidence interval, 0.33 to 0.93), respectively

27 Mediterranean Diet PREDIMED Study
28 PREDIMED Study The traditional Mediterranean diet is characterized by a high intake of olive oil, fruit, nuts, vegetables, and cereals; a moderate intake of fish and poultry; a low intake of dairy products, red meat, processed meats, and sweets; and wine in moderation, consumed with meals parallel-group, multicenter, randomized trial men (55 to 80 years of age) and women (60 to 80 years of age) with no cardiovascular disease at enrollment, who had either type 2 diabetes mellitus or at least three major risk factors Ramdomize to one of three diets: a Mediterranean diet supplemented with extra-virgin olive oil, a Mediterranean diet supplemented with mixed nuts, or a control diet (advice to reduce dietary fat)
29
30 PREDIMED Study The multivariable-adjusted hazard ratios were 0.70 (95% confidence interval [CI], 0.54 to 0.92) and 0.72 (95% CI, 0.54 to 0.96) for the group assigned to a Mediterranean diet with extra-virgin olive oil Conclusion: Among persons at high cardiovascular risk, a Mediterranean diet supplemented with extra-virgin olive oil or nuts reduced the incidence of major cardiovascular events
31 Lifestyle modification Critical component of ASCVD risk reduction Prior to, and in concert with cholesterol lowering drugs adhering to a heart healthy diet limiting intake of dietary trans-fats, carbohydrates. Increase intake of fruits, vegetables, nuts and legumes reduce excessive body weight regular exercise habits avoidance of tobacco products

32 Lifestyle Modification A summary
33
34 So who to treat with Statin? Children < 8 years LDL >500mg/dL
35 Familial hypercholesterolaemia Heterozygous most studied 1 in 500 worldwide LDL > 240mg/DL Tendon xanthomas, TC >600mg/dL associated with MI in childhood Homozygous most powerful Case series of 7 patients
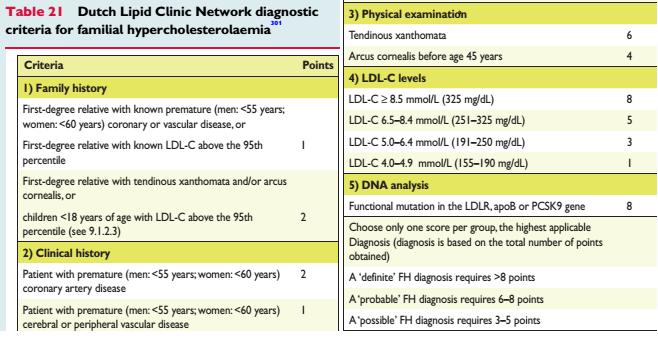
36 Familial Hypercholesterolemia
37
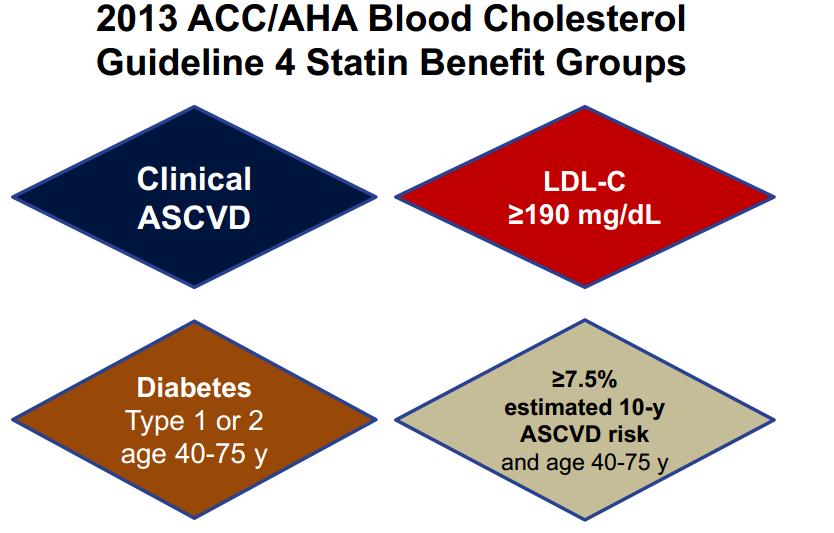
38 ACC / AHA
39 JUPITER TRIAL

40 The Evidence: Risk reduction with LDL-C lowering

41 2,884,260 patients with a qualifying lipid analysis 3.8% with LDL-C level > 190 mg/dl. Statins - 32% of patients in their 30s. LDL-C >250 mg/dl 25% not prescribed a statin

42 Discussion
43 Therapeutic Equivalence of Statins
44 What about safety and tolerability? Short term studies. Myalgia, arthritis, arthralgia, rhabdomyolysis, liver dysfunction, myositis Diabetes?

45
46 Conclusions We have a serious epidemic of cardiovascular disease on our hands The disease process starts in the very young Risk calculating models are reasonable for predicting risk in older patients but may underestimate the risk and benefit of early intervention A dearth of data on efficacy of interventions at the younger age groups. Lifestyle interventions provide a powerful tool Statins should be considered in the highest risk populations


47 It s never too late OBESITY AFRICA The next big thing November 2017
48 Thank you
49
50
51
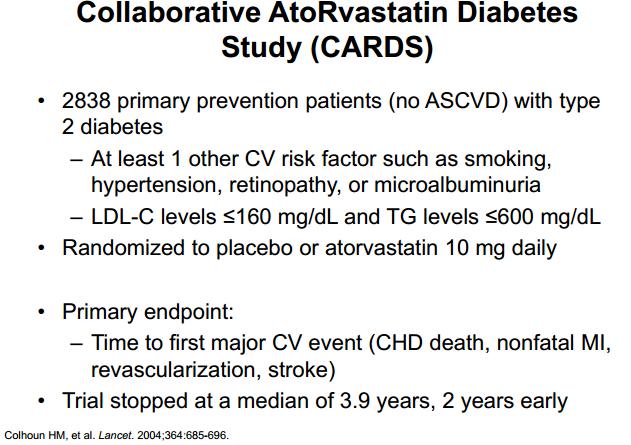
52 Primary prevention using statin therapy (when should we start?)
53 What do the guidelines tell us?
54 ASCVD Risk

55 The Profile: Components and Numbers
56
57
58 Dyslipidemia Guidelines American College of Cardiology (ACC)/American Heart Association(AHA) American Association of Clinical Endocrinologists (AACE) National Lipid Association (NLA) Department of Veteran s Affairs (VA)/Department of Defense (DOD) International Atherosclerosis Society (IAS) European Society of Cardiology (ESC)/European Atherosclerosis Society (EAS)

59 Risk reduction seems independent of method used
60 Lets take a look at the guidelines
61 ACC/AHA 2013 Risk Algorithm Intervention Population Treatment Goal Intervention ACC/AHA- ASCVD Adults 21 years old in any of the following risk groups: 1.Known ASCVD 2.LDL-C >190 mg/dl years old, with diabetes and LDL-C levels mg/dl and no ASCVD % 10 year ASCVD risk with LDL-C levels mg/dl By Risk Group Counsel on healthy lifestyle habits 1.: 50% reduction in LDL-C High-intensity statin therapy for most patients in groups 1 and 2, 2. 50% reduction in LDL-C and for group 3 patients if 7.5% 10- year ASCVD risk; consider for group % reduction in LDL- C % reduction in LDL- C Moderate-intensity statins for group 1-2 patients >75 years or with statin-associated adverse events, and for most group 3-4 patients
62 ESC 2016

63 ESC Treatment Targets
64 International Atherosclerosis Society (IAS) 2014 Risk Algorithm Intervention Population Treatment Goal Intervention Lifestyle changes(first line): Lifetime-FRS (preferred) or QRISK2 Non-HDL-C 130 mg/dl LDL-C 100 mg/dl LDL-C <100 mg/dl Non-HDL-C <130 mg/dl is an alternative target Nutrition counseling, physical activity, smoking cessation and weight loss. Pharmacologic Therapy in addition to lifestyle changes: Moderate to high intensity statin adjusted to absolute risk
65 Components of treatment
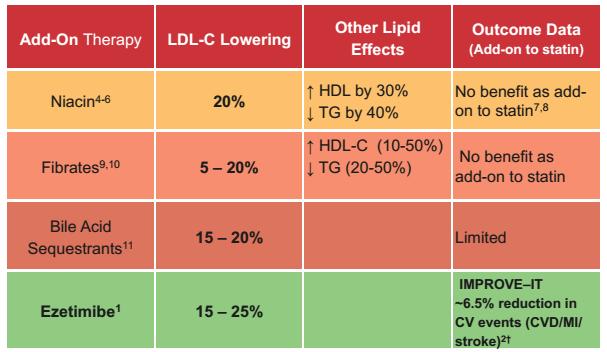
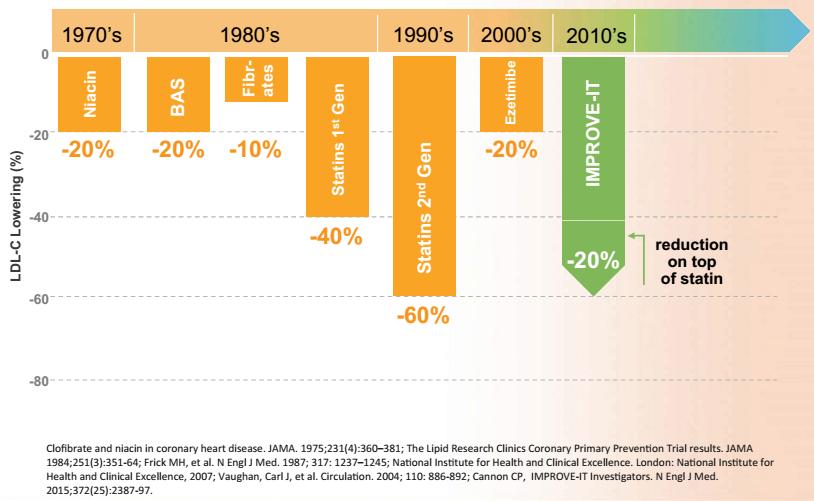
66 Drugs for reducing LDL-C Statins Non Statin lipid modifying drugs Ezetimibe Bile Acid Sequestrants: Cholestyramine, colestipol Cholesterol absorption Inhibitors: Ezetimibe Fibrates Niacin Novel drugs PCSK9 inhibitors
67 Statins Moderate-intensity Lovastatin 40 mg Pravastatin 40 mg Simvastatin 40 mg Atorvastatin 10 to 20 mg Rosuvastatin 5 to 10 mg High-intensity Atorvastatin 40 to 80 mg Rosuvastatin 20 to 40 mg

68 Jupiter Trial 17,802 healthy men and women LDL < 130 mg per deciliter (3.4 mmol per liter) and hscrp levels of 2.0 mg per liter or higher Rosuvastatin 20 mg daily or placebo combined primary end point of MI, stroke, arterial revascularization, hospitalization for unstable angina, or death from cardiovascular causes.
69 Jupiter Trial - Results Stopped after a median follow-up of 1.9 years (maximum, 5.0). Rosuvastatin reduced LDL cholesterol levels by 50% and highsensitivity C-reactive protein levels by 37% The rates of the primary end point were 0.77 and 1.36 per 100 person-years of follow-up in the rosuvastatin and placebo groups, respectively (HR 0.56; 95% confidence interval [CI], 0.46 to 0.69; P< )
70 JUPITER TRIAL
 compared with placebo 1 Diabetes subgroup analysis: 20% RRR in total CV events and procedures in nondiabetic patients was similar to the 23% RRR seen in the diabetic group 2 Incidence of")
71 Cumulative incidence (%) Group 4: Primary prevention ASCOT-LLA: Atorvastatin 10 mg provided a 36% RRR of the primary endpoint of non-fatal MI and fatal CHD (p=0.0005) compared with placebo 1 Diabetes subgroup analysis: 20% RRR in total CV events and procedures in nondiabetic patients was similar to the 23% RRR seen in the diabetic group 2 Incidence of non-fatal MI and fatal CHD Placebo (n=5137); final LDL-C=126 mg/dl Atorvastatin 10 mg (n=5168); final LDL-C=90 mg/dl 36% RRR HR= % CI ) (p=0.0005) ARR=1.1% Time (years) 1. Reprinted from The Lancet, 361, Sever et al, Prevention of coronary and stroke events with atorvastatin in hypertensive patients who have average or lower-than-average cholesterol concentrations, in the Anglo-Scandinavian Cardiac Outcomes Trial Lipid Lowering Arm (ASCOT-LLA): a multicentre randomised controlled trial, , Copyright (2003), with permission from Elsevier 2. Sever PS, et al. Diabetes Care 2005;28:
72
73
74 Therapeutic Equivalence of Statins
75 Non-Statins
76 Thank you
77
78 AAP AHA No CVD risk factors. Treat when LDL > 190mg/dL after 6 months of diet therapy Diabetes Consider treating when LDL > 130mg/dL after 6 months of diet therapy FHx of CAD or >2 addition risk factors present? Treat when LDL > 160mg/dL after 6 months of diet therapy Treat when LDL > 190mg/dL Treat when LDL > 190mg/dL after 6 months of diet therapy
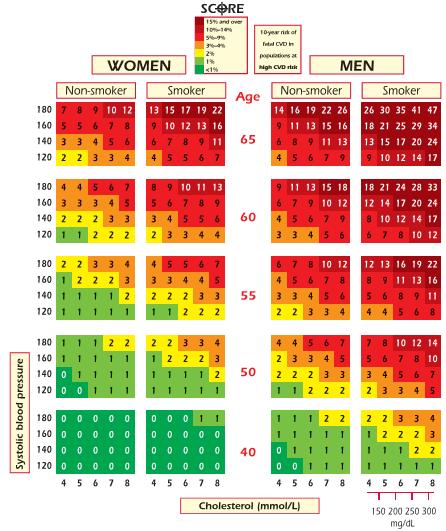
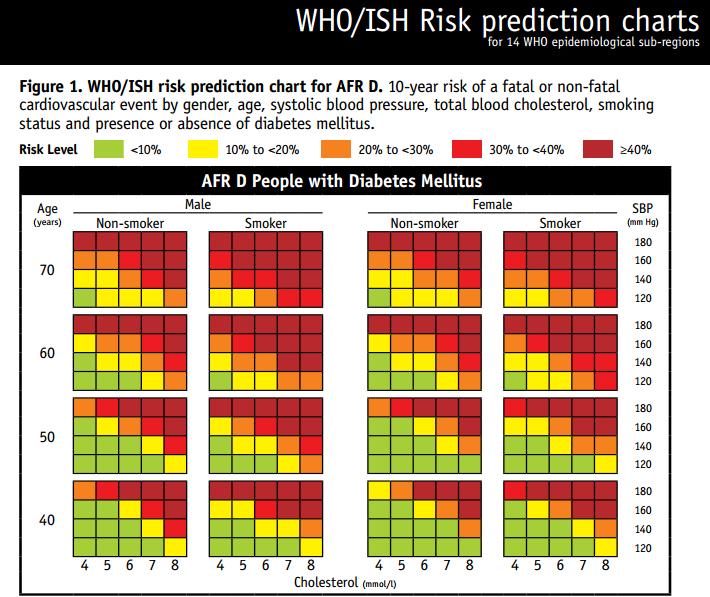
79 Use of Risk prediction models United States Framingham Risk Score (FRS; multiple adaptations) Reynolds Risk Score (RRS) American College of Cardiology/American Heart Association (AC/AHA- ASCVD) European population cohorts Systematic Coronary Risk Evaluation (SCORE) QRisk2 WHO risk charts

80 Novel drugs: PCSK9 Inhibitors
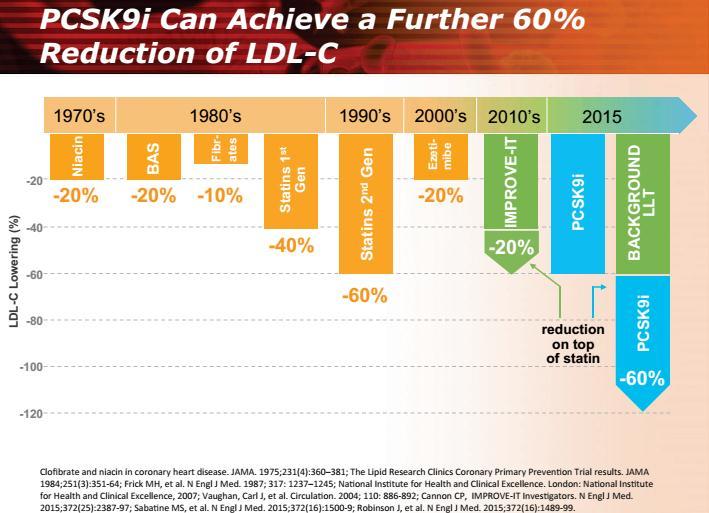
81
82 Proprotein convertase subtilisin kexin 9 (PCSK9) inhibitors Not been adequately evaluated in primary prevention in patients without familial hypercholesterolemia Their effects in secondary prevention suggest that they could be expected to reduce cardiovascular outcomes to a similar degree, as is seen with statin therapy However, their cost, the requirement for injections, and the lack of long-term safety data would make them an option only in the highestrisk primary prevention patients who are unable to tolerate statin therapy
83 Conclusions The processes leading to atherosclerosis begin early in life The rationale for activities focused on LDL-C reduction is based upon epidemiologic data documenting a continuous, positive, graded relationship between LDL-C concentration and CVD events and mortality Lowering LDL-C with statin therapy for primary prevention is effective at reducing CVD events (mostly myocardial infarction) over a wide range of baseline LDL-C levels and lipid profiles Lifestyle modification is a critical component of ASCVD risk reduction
How would you manage Ms. Gold
 How would you manage Ms. Gold 32 yo Asian woman with dyslipidemia Current medications: Simvastatin 20mg QD Most recent lipid profile: TC = 246, TG = 100, LDL = 176, HDL = 50 What about Mr. Williams? 56
How would you manage Ms. Gold 32 yo Asian woman with dyslipidemia Current medications: Simvastatin 20mg QD Most recent lipid profile: TC = 246, TG = 100, LDL = 176, HDL = 50 What about Mr. Williams? 56
Dyslipidemia in the light of Current Guidelines - Do we change our Practice?
 Dyslipidemia in the light of Current Guidelines - Do we change our Practice? Dato Dr. David Chew Soon Ping Senior Consultant Cardiologist Institut Jantung Negara Atherosclerotic Cardiovascular Disease
Dyslipidemia in the light of Current Guidelines - Do we change our Practice? Dato Dr. David Chew Soon Ping Senior Consultant Cardiologist Institut Jantung Negara Atherosclerotic Cardiovascular Disease
ATP IV: Predicting Guideline Updates
 Disclosures ATP IV: Predicting Guideline Updates Daniel M. Riche, Pharm.D., BCPS, CDE Speaker s Bureau Merck Janssen Boehringer-Ingelheim Learning Objectives Describe at least two evidence-based recommendations
Disclosures ATP IV: Predicting Guideline Updates Daniel M. Riche, Pharm.D., BCPS, CDE Speaker s Bureau Merck Janssen Boehringer-Ingelheim Learning Objectives Describe at least two evidence-based recommendations
No relevant financial relationships
 MANAGEMENT OF LIPID DISORDERS Balancing Benefits and harms Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial relationships baron@medicine.ucsf.edu
MANAGEMENT OF LIPID DISORDERS Balancing Benefits and harms Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial relationships baron@medicine.ucsf.edu
Review of guidelines for management of dyslipidemia in diabetic patients
 2012 international Conference on Diabetes and metabolism (ICDM) Review of guidelines for management of dyslipidemia in diabetic patients Nan Hee Kim, MD, PhD Department of Internal Medicine, Korea University
2012 international Conference on Diabetes and metabolism (ICDM) Review of guidelines for management of dyslipidemia in diabetic patients Nan Hee Kim, MD, PhD Department of Internal Medicine, Korea University
CLINICAL OUTCOME Vs SURROGATE MARKER
 CLINICAL OUTCOME Vs SURROGATE MARKER Statin Real Experience Dr. Mostafa Sherif Senior Medical Manager Pfizer Egypt & Sudan Objective Difference between Clinical outcome and surrogate marker Proper Clinical
CLINICAL OUTCOME Vs SURROGATE MARKER Statin Real Experience Dr. Mostafa Sherif Senior Medical Manager Pfizer Egypt & Sudan Objective Difference between Clinical outcome and surrogate marker Proper Clinical
Modern Lipid Management:
 Modern Lipid Management: New Drugs, New Targets, New Hope Kirk U. Knowlton, M.D Director of Cardiovascular Research Co Chief of Cardiology Why lower LDL C in those without evidence of CAD (primary prevention)
Modern Lipid Management: New Drugs, New Targets, New Hope Kirk U. Knowlton, M.D Director of Cardiovascular Research Co Chief of Cardiology Why lower LDL C in those without evidence of CAD (primary prevention)
Conflict of Interest Disclosure. Learning Objectives. Learning Objectives. Guidelines. Update on Lifestyle Guidelines
 Conflict of Interest Disclosure Updates for the Ambulatory Care Pharmacist: Dyslipidemia and CV Risk Assessment No conflicts of interest to disclose 2014 Updates to the Updates in Ambulatory Care Pharmacy
Conflict of Interest Disclosure Updates for the Ambulatory Care Pharmacist: Dyslipidemia and CV Risk Assessment No conflicts of interest to disclose 2014 Updates to the Updates in Ambulatory Care Pharmacy
Learning Objectives. Patient Case
 Joseph Saseen, Pharm.D., FASHP, FCCP, BCPS Professor and Vice Chair, Department of Clinical Pharmacy University of Colorado Anschutz Medical Campus Learning Objectives Identify the 4 patient populations
Joseph Saseen, Pharm.D., FASHP, FCCP, BCPS Professor and Vice Chair, Department of Clinical Pharmacy University of Colorado Anschutz Medical Campus Learning Objectives Identify the 4 patient populations
Placebo-Controlled Statin Trials MANAGEMENT OF HIGH BLOOD CHOLESTEROL MANAGEMENT OF HIGH BLOOD CHOLESTEROL: IMPLICATIONS OF THE NEW GUIDELINES
 MANAGEMENT OF HIGH BLOOD CHOLESTEROL: IMPLICATIONS OF THE NEW GUIDELINES Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest
MANAGEMENT OF HIGH BLOOD CHOLESTEROL: IMPLICATIONS OF THE NEW GUIDELINES Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest
Lipid Management C. Samuel Ledford, MD Interventional Cardiology Chattanooga Heart Institute
 Lipid Management 2018 C. Samuel Ledford, MD Interventional Cardiology Chattanooga Heart Institute Disclosures No Financial Disclosures Disclosures I am an Interventional Cardiologist I put STENTS in for
Lipid Management 2018 C. Samuel Ledford, MD Interventional Cardiology Chattanooga Heart Institute Disclosures No Financial Disclosures Disclosures I am an Interventional Cardiologist I put STENTS in for
Disclosure. No relevant financial relationships. Placebo-Controlled Statin Trials
 MANAGEMENT OF HYPERLIPIDEMIA AND CARDIOVASCULAR RISK IN WOMEN: Balancing Benefits and Harms Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial
MANAGEMENT OF HYPERLIPIDEMIA AND CARDIOVASCULAR RISK IN WOMEN: Balancing Benefits and Harms Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial
HYPERLIPIDEMIA IN THE OLDER POPULATION NICOLE SLATER, PHARMD, BCACP AUBURN UNIVERSITY, HARRISON SCHOOL OF PHARMACY JULY 16, 2016
 HYPERLIPIDEMIA IN THE OLDER POPULATION NICOLE SLATER, PHARMD, BCACP AUBURN UNIVERSITY, HARRISON SCHOOL OF PHARMACY JULY 16, 2016 NOTHING TO DISCLOSE I, Nicole Slater, have no actual or potential conflict
HYPERLIPIDEMIA IN THE OLDER POPULATION NICOLE SLATER, PHARMD, BCACP AUBURN UNIVERSITY, HARRISON SCHOOL OF PHARMACY JULY 16, 2016 NOTHING TO DISCLOSE I, Nicole Slater, have no actual or potential conflict
1. Which one of the following patients does not need to be screened for hyperlipidemia:
 Questions: 1. Which one of the following patients does not need to be screened for hyperlipidemia: a) Diabetes mellitus b) Hypertension c) Family history of premature coronary disease (first degree relatives:
Questions: 1. Which one of the following patients does not need to be screened for hyperlipidemia: a) Diabetes mellitus b) Hypertension c) Family history of premature coronary disease (first degree relatives:
Placebo-Controlled Statin Trials Prevention Of CVD in Women"
 MANAGEMENT OF HIGH BLOOD CHOLESTEROL: IMPLICATIONS OF THE NEW GUIDELINES Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest
MANAGEMENT OF HIGH BLOOD CHOLESTEROL: IMPLICATIONS OF THE NEW GUIDELINES Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest
Cholesterol Management Roy Gandolfi, MD
 Cholesterol Management 2017 Roy Gandolfi, MD Goals Interpreting cholesterol guidelines Cholesterol treatment in diabetics Statin use and side effects therapy Reporting- Comparison data among physicians
Cholesterol Management 2017 Roy Gandolfi, MD Goals Interpreting cholesterol guidelines Cholesterol treatment in diabetics Statin use and side effects therapy Reporting- Comparison data among physicians
Treatment of Cardiovascular Risk Factors. Kevin M Hayes D.O. F.A.C.C. First Coast Heart and Vascular Center
 Treatment of Cardiovascular Risk Factors Kevin M Hayes D.O. F.A.C.C. First Coast Heart and Vascular Center Disclosures: None Objectives What do risk factors tell us What to check and when Does treatment
Treatment of Cardiovascular Risk Factors Kevin M Hayes D.O. F.A.C.C. First Coast Heart and Vascular Center Disclosures: None Objectives What do risk factors tell us What to check and when Does treatment
Lipid Management 2013 Statin Benefit Groups
 Clinical Integration Steering Committee Clinical Integration Chronic Disease Management Work Group Lipid Management 2013 Statin Benefit Groups Approved by Board Chair Signature Name (Please Print) Date
Clinical Integration Steering Committee Clinical Integration Chronic Disease Management Work Group Lipid Management 2013 Statin Benefit Groups Approved by Board Chair Signature Name (Please Print) Date
CVD risk assessment using risk scores in primary and secondary prevention
 CVD risk assessment using risk scores in primary and secondary prevention Raul D. Santos MD, PhD Heart Institute-InCor University of Sao Paulo Brazil Disclosure Honoraria for consulting and speaker activities
CVD risk assessment using risk scores in primary and secondary prevention Raul D. Santos MD, PhD Heart Institute-InCor University of Sao Paulo Brazil Disclosure Honoraria for consulting and speaker activities
New Guidelines in Dyslipidemia Management
 The Fourth IAS-OSLA Course on Lipid Metabolism and Cardiovascular Risk Muscat, Oman, February 2018 New Guidelines in Dyslipidemia Management Dr. Khalid Al-Waili, MD, FRCPC, DABCL Senior Consultant Medical
The Fourth IAS-OSLA Course on Lipid Metabolism and Cardiovascular Risk Muscat, Oman, February 2018 New Guidelines in Dyslipidemia Management Dr. Khalid Al-Waili, MD, FRCPC, DABCL Senior Consultant Medical
Disclosures. Overview 9/30/ ACC/AHA Guidelines on the Treatment of Blood Cholesterol to Reduce Atherosclerotic Cardiovascular Risk in Adults
 2013 ACC/AHA Guidelines on the Treatment of Blood Cholesterol to Reduce Atherosclerotic Cardiovascular Risk in Adults 2014 AAHP Fall Seminar Sherry Myatt, PharmD, BCPS Assistant Director of Pharmacy for
2013 ACC/AHA Guidelines on the Treatment of Blood Cholesterol to Reduce Atherosclerotic Cardiovascular Risk in Adults 2014 AAHP Fall Seminar Sherry Myatt, PharmD, BCPS Assistant Director of Pharmacy for
New Guidelines in Dyslipidemia Management
 The Third IAS-OSLA Course on Lipid Metabolism and Cardiovascular Risk Muscat, Oman, February 2017 New Guidelines in Dyslipidemia Management Dr. Khalid Al-Waili, MD, FRCPC, DABCL Senior Consultant Medical
The Third IAS-OSLA Course on Lipid Metabolism and Cardiovascular Risk Muscat, Oman, February 2017 New Guidelines in Dyslipidemia Management Dr. Khalid Al-Waili, MD, FRCPC, DABCL Senior Consultant Medical
Drug Class Monograph
 Drug Class Monograph Class: Proprotein Convertase Subtilisin/Kexin Type 9 (PCSK9) Inhibitor Drugs: Praluent (alirocumab), Repatha (evolocumab) Line of Business: Medi-Cal Effective Date: February 17, 2016
Drug Class Monograph Class: Proprotein Convertase Subtilisin/Kexin Type 9 (PCSK9) Inhibitor Drugs: Praluent (alirocumab), Repatha (evolocumab) Line of Business: Medi-Cal Effective Date: February 17, 2016
4 th and Goal To Go How Low Should We Go? :
 4 th and Goal To Go How Low Should We Go? : Evaluating New Lipid Lowering Therapies Catherine Bourg Rebitch, PharmD, BCACP Clinical Associate Professor Disclosure The presenter has nothing to disclose
4 th and Goal To Go How Low Should We Go? : Evaluating New Lipid Lowering Therapies Catherine Bourg Rebitch, PharmD, BCACP Clinical Associate Professor Disclosure The presenter has nothing to disclose
What do the guidelines say about combination therapy?
 What do the guidelines say about combination therapy? Christie M. Ballantyne, MD Center for Cardiovascular Disease Prevention Methodist DeBakey Heart & Vascular Center Baylor College of Medicine Houston,
What do the guidelines say about combination therapy? Christie M. Ballantyne, MD Center for Cardiovascular Disease Prevention Methodist DeBakey Heart & Vascular Center Baylor College of Medicine Houston,
Pharmacy Management Drug Policy
 SUBJECT: ; Praluent (alirocumab), Repatha (evolocumab) POLICY NUMBER: Pharmacy-61 EFFECTIVE DATE: 8/15 LAST REVIEW DATE: 9/22/2017 If the member s subscriber contract excludes coverage for a specific service
SUBJECT: ; Praluent (alirocumab), Repatha (evolocumab) POLICY NUMBER: Pharmacy-61 EFFECTIVE DATE: 8/15 LAST REVIEW DATE: 9/22/2017 If the member s subscriber contract excludes coverage for a specific service
LDL cholesterol and cardiovascular outcomes?
 LDL cholesterol and cardiovascular outcomes? Prof Kausik Ray, BSc (hons), MBChB, FRCP, MD, MPhil (Cantab), FACC, FESC Professor of Cardiovascular Disease Prevention St Georges University of London Honorary
LDL cholesterol and cardiovascular outcomes? Prof Kausik Ray, BSc (hons), MBChB, FRCP, MD, MPhil (Cantab), FACC, FESC Professor of Cardiovascular Disease Prevention St Georges University of London Honorary
The JUPITER trial: What does it tell us? Alice Y.Y. Cheng, MD, FRCPC January 24, 2009
 The JUPITER trial: What does it tell us? Alice Y.Y. Cheng, MD, FRCPC January 24, 2009 Learning Objectives 1. Understand the role of statin therapy in the primary and secondary prevention of stroke 2. Explain
The JUPITER trial: What does it tell us? Alice Y.Y. Cheng, MD, FRCPC January 24, 2009 Learning Objectives 1. Understand the role of statin therapy in the primary and secondary prevention of stroke 2. Explain
Introduction. Objective. Critical Questions Addressed
 Introduction Objective To provide a strong evidence-based foundation for the treatment of cholesterol for the primary and secondary prevention of ASCVD in women and men Critical Questions Addressed CQ1:
Introduction Objective To provide a strong evidence-based foundation for the treatment of cholesterol for the primary and secondary prevention of ASCVD in women and men Critical Questions Addressed CQ1:
PCSK9 Agents Drug Class Prior Authorization Protocol
 PCSK9 Agents Drug Class Prior Authorization Protocol Line of Business: Medicaid P & T Approval Date: February 21, 2018 Effective Date: April 1, 2018 This policy has been developed through review of medical
PCSK9 Agents Drug Class Prior Authorization Protocol Line of Business: Medicaid P & T Approval Date: February 21, 2018 Effective Date: April 1, 2018 This policy has been developed through review of medical
An update on lipidology and cardiovascular risk management. Lipids, Metabolism & Vascular Risk Section - Royal Society of Medicine
 An update on lipidology and cardiovascular risk management Lipids, Metabolism & Vascular Risk Section - Royal Society of Medicine National and international lipid modification guidelines: A critical appraisal
An update on lipidology and cardiovascular risk management Lipids, Metabolism & Vascular Risk Section - Royal Society of Medicine National and international lipid modification guidelines: A critical appraisal
Landmark Clinical Trials.
 Landmark Clinical Trials 1 Learning Objectives Discuss clinical trials and their role in lipid and lipoprotein treatment in cardiovascular prevention. Review the clinical trials of lipid-altering drug
Landmark Clinical Trials 1 Learning Objectives Discuss clinical trials and their role in lipid and lipoprotein treatment in cardiovascular prevention. Review the clinical trials of lipid-altering drug
Lipid Guidelines Who, What, and How Low. Anita Ralstin, MS, CNP Next Step Health Consultant, LLC New Mexico Heart Institute
 Lipid Guidelines Who, What, and How Low Anita Ralstin, MS, CNP Next Step Health Consultant, LLC New Mexico Heart Institute Disclosures! None Objectives! List factors used in screening for dyslipidemia
Lipid Guidelines Who, What, and How Low Anita Ralstin, MS, CNP Next Step Health Consultant, LLC New Mexico Heart Institute Disclosures! None Objectives! List factors used in screening for dyslipidemia
Inflammation and and Heart Heart Disease in Women Inflammation and Heart Disease
 Inflammation and Heart Disease in Women Inflammation and Heart Disease What is the link between een inflammation and atherosclerotic disease? What is the role of biomarkers in predicting cardiovascular
Inflammation and Heart Disease in Women Inflammation and Heart Disease What is the link between een inflammation and atherosclerotic disease? What is the role of biomarkers in predicting cardiovascular
Dyslipedemia New Guidelines
 Dyslipedemia New Guidelines New ACC/AHA Prevention Guidelines on Blood Cholesterol November 12, 2013 Mohammed M Abd El Ghany Professor of Cardiology Cairo Universlty 1 1 0 Cholesterol Management Pharmacotherapy
Dyslipedemia New Guidelines New ACC/AHA Prevention Guidelines on Blood Cholesterol November 12, 2013 Mohammed M Abd El Ghany Professor of Cardiology Cairo Universlty 1 1 0 Cholesterol Management Pharmacotherapy
UnitedHealthcare Pharmacy Clinical Pharmacy Programs
 UnitedHealthcare Pharmacy Clinical Pharmacy Programs Program Number 2017 P 2062-8 Program Prior Authorization/Medical Necessity Medication Praluent (alirocumab) P&T Approval Date 5/2015, 8/2015, 9/2015,
UnitedHealthcare Pharmacy Clinical Pharmacy Programs Program Number 2017 P 2062-8 Program Prior Authorization/Medical Necessity Medication Praluent (alirocumab) P&T Approval Date 5/2015, 8/2015, 9/2015,
Andrew Cohen, MD and Neil S. Skolnik, MD INTRODUCTION
 2 Hyperlipidemia Andrew Cohen, MD and Neil S. Skolnik, MD CONTENTS INTRODUCTION RISK CATEGORIES AND TARGET LDL-CHOLESTEROL TREATMENT OF LDL-CHOLESTEROL SPECIAL CONSIDERATIONS OLDER AND YOUNGER ADULTS ADDITIONAL
2 Hyperlipidemia Andrew Cohen, MD and Neil S. Skolnik, MD CONTENTS INTRODUCTION RISK CATEGORIES AND TARGET LDL-CHOLESTEROL TREATMENT OF LDL-CHOLESTEROL SPECIAL CONSIDERATIONS OLDER AND YOUNGER ADULTS ADDITIONAL
Placebo-Controlled Statin Trials EXPLAINING THE DECREASE IN DEATHS FROM CHD! PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN EXPLAINING THE DECREASE IN
 PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest EXPLAINING THE DECREASE
PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest EXPLAINING THE DECREASE
David Y. Gaitonde, MD, FACP Endocrinology DDEAMC, Fort Gordon
 David Y. Gaitonde, MD, FACP Endocrinology DDEAMC, Fort Gordon I have no actual or potential conflicts of interest in relation to this program or presentation. Raphael School of Athens, 1509-1511 Apply
David Y. Gaitonde, MD, FACP Endocrinology DDEAMC, Fort Gordon I have no actual or potential conflicts of interest in relation to this program or presentation. Raphael School of Athens, 1509-1511 Apply
PCSK9 Inhibitors: Promise or Pitfall?
 PCSK9 Inhibitors: Promise or Pitfall? Tracy Harlan, PharmD PGY2 Ambulatory Care Resident University of Iowa Hospitals and Clinics tracy harlan@uiowa.edu Tracy Harlan does not have any actual or potential
PCSK9 Inhibitors: Promise or Pitfall? Tracy Harlan, PharmD PGY2 Ambulatory Care Resident University of Iowa Hospitals and Clinics tracy harlan@uiowa.edu Tracy Harlan does not have any actual or potential
UnitedHealthcare Pharmacy Clinical Pharmacy Programs
 UnitedHealthcare Pharmacy Clinical Pharmacy Programs Program Number 2017 P 2063-8 Program Prior Authorization/Medical Necessity Medication Repatha (evolocumab) P&T Approval Date 5/2015, 9/2015, 11/2015,
UnitedHealthcare Pharmacy Clinical Pharmacy Programs Program Number 2017 P 2063-8 Program Prior Authorization/Medical Necessity Medication Repatha (evolocumab) P&T Approval Date 5/2015, 9/2015, 11/2015,
Case Presentation. Rafael Bitzur The Bert W Strassburger Lipid Center Sheba Medical Center Tel Hashomer
 Case Presentation Rafael Bitzur The Bert W Strassburger Lipid Center Sheba Medical Center Tel Hashomer Case Presentation 50 YO man NSTEMI treated with PCI 1 month ago Medical History: Obesity: BMI 32,
Case Presentation Rafael Bitzur The Bert W Strassburger Lipid Center Sheba Medical Center Tel Hashomer Case Presentation 50 YO man NSTEMI treated with PCI 1 month ago Medical History: Obesity: BMI 32,
NEW GUIDELINES FOR CHOLESTEROL
 NEW GUIDELINES FOR CHOLESTEROL NEW CHOLESTEROL GUIDELINES 2013 Recently updated guidelines for the treatment of high blood cholesterol levels is a major update since 2002. The news media have trumpeted
NEW GUIDELINES FOR CHOLESTEROL NEW CHOLESTEROL GUIDELINES 2013 Recently updated guidelines for the treatment of high blood cholesterol levels is a major update since 2002. The news media have trumpeted
Prevention of Heart Disease: The New Guidelines
 Prevention of Heart Disease: The New Guidelines Nisha I. Parikh MD MPH Assistant Professor of Medicine Division of Cardiology Department of Medicine University of California San Francisco May 18 th 2015
Prevention of Heart Disease: The New Guidelines Nisha I. Parikh MD MPH Assistant Professor of Medicine Division of Cardiology Department of Medicine University of California San Francisco May 18 th 2015
Lipid Management: A Case-Based Approach. Overview. Simple Lipid Therapy Approach. Patients have lipid disorders of:
 Lipid Management: A Case-Based Approach Patrick E. McBride, M.D., M.P.H. Professor of Medicine, Cardiovascular Medicine Associate Director, Preventive Cardiology Program UW School of Medicine and Public
Lipid Management: A Case-Based Approach Patrick E. McBride, M.D., M.P.H. Professor of Medicine, Cardiovascular Medicine Associate Director, Preventive Cardiology Program UW School of Medicine and Public
Lipid Panel Management Refresher Course for the Family Physician
 Lipid Panel Management Refresher Course for the Family Physician Objectives Understand the evidence that was evaluated to develop the 2013 ACC/AHA guidelines Discuss the utility and accuracy of the new
Lipid Panel Management Refresher Course for the Family Physician Objectives Understand the evidence that was evaluated to develop the 2013 ACC/AHA guidelines Discuss the utility and accuracy of the new
No relevant financial relationships
 MANAGEMENT OF LIPID DISORDERS: WHERE DO WE STAND WITH THE NEW PRACTICE GUIDELINES? Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Disclosure No relevant financial relationships
MANAGEMENT OF LIPID DISORDERS: WHERE DO WE STAND WITH THE NEW PRACTICE GUIDELINES? Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Disclosure No relevant financial relationships
Statins for Cardiovascular Disease Prevention in Women: Review of the Evidence
 Statins for Cardiovascular Disease Prevention in Women: Review of the Evidence Karen E. Aspry, M.D., M.S., ABCL, FACC Assistant Professor of Medicine (Clinical) Alpert Medical School of Brown University
Statins for Cardiovascular Disease Prevention in Women: Review of the Evidence Karen E. Aspry, M.D., M.S., ABCL, FACC Assistant Professor of Medicine (Clinical) Alpert Medical School of Brown University
Latest Guidelines for Lipid Management
 Latest Guidelines for Lipid Management Goals Recognize the differences between different guidelines Understand the effective strategies to tailor lipid lowering therapies based on evidence and guideline
Latest Guidelines for Lipid Management Goals Recognize the differences between different guidelines Understand the effective strategies to tailor lipid lowering therapies based on evidence and guideline
How to Reduce Residual Risk in Primary Prevention
 How to Reduce Residual Risk in Primary Prevention Helene Glassberg, MD Assistant Professor of Medicine Section of Cardiology Hospital of the University of Pennsylvania Philadelphia, PA USA Patients with
How to Reduce Residual Risk in Primary Prevention Helene Glassberg, MD Assistant Professor of Medicine Section of Cardiology Hospital of the University of Pennsylvania Philadelphia, PA USA Patients with
Update on Lipid Management in Cardiovascular Disease: How to Understand and Implement the New ACC/AHA Guidelines
 Update on Lipid Management in Cardiovascular Disease: How to Understand and Implement the New ACC/AHA Guidelines Paul Mahoney, MD Sentara Cardiology Specialists Lipid Management in Cardiovascular Disease
Update on Lipid Management in Cardiovascular Disease: How to Understand and Implement the New ACC/AHA Guidelines Paul Mahoney, MD Sentara Cardiology Specialists Lipid Management in Cardiovascular Disease
4/7/ The stats on heart disease. + Deaths & Age-Adjusted Death Rates for
 + Update on Lipid Management Stacey Gardiner, MD Assistant Professor Division of Cardiovascular Medicine Medical College of Wisconsin + The stats on heart disease Over the past 10 years for which statistics
+ Update on Lipid Management Stacey Gardiner, MD Assistant Professor Division of Cardiovascular Medicine Medical College of Wisconsin + The stats on heart disease Over the past 10 years for which statistics
Conflicts of interest. What's the Skinny on the Lipid Guidelines? Key Differences. Are you applying the new ACC/AHA Lipid guidelines in your practice?
 Conflicts of interest What's the Skinny on the Lipid Guidelines? The presenter has no relevant conflicts of interest to disclose. Kathleen Vest, PharmD, CDE, BCACP At the end of this presentation, pharmacist
Conflicts of interest What's the Skinny on the Lipid Guidelines? The presenter has no relevant conflicts of interest to disclose. Kathleen Vest, PharmD, CDE, BCACP At the end of this presentation, pharmacist
Cardiovascular Complications of Diabetes
 VBWG Cardiovascular Complications of Diabetes Nicola Abate, M.D., F.N.L.A. Professor and Chief Division of Endocrinology and Metabolism The University of Texas Medical Branch Galveston, Texas Coronary
VBWG Cardiovascular Complications of Diabetes Nicola Abate, M.D., F.N.L.A. Professor and Chief Division of Endocrinology and Metabolism The University of Texas Medical Branch Galveston, Texas Coronary
The Mediterranean Diet: The Optimal Diet for Cardiovascular Health
 The Mediterranean Diet: The Optimal Diet for Cardiovascular Health Vasanti Malik, ScD Research Scientist Department of Nutrition Harvard School of Public Health Cardiovascular Disease Prevention International
The Mediterranean Diet: The Optimal Diet for Cardiovascular Health Vasanti Malik, ScD Research Scientist Department of Nutrition Harvard School of Public Health Cardiovascular Disease Prevention International
Disclosure. No relevant financial relationships. Placebo-Controlled Statin Trials
 PREVENTING CARDIOVASCULAR DISEASE IN WOMEN: Current Guidelines for Hypertension, Lipids and Aspirin Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial
PREVENTING CARDIOVASCULAR DISEASE IN WOMEN: Current Guidelines for Hypertension, Lipids and Aspirin Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial
Helen Williams Consultant Pharmacist for CV Disease - South London
 Helen Williams Consultant Pharmacist for CV Disease - South London CVD remains the leading cause of death in the UK Accounts for a third of all deaths 46,000 deaths in people < 75 years (70% of these
Helen Williams Consultant Pharmacist for CV Disease - South London CVD remains the leading cause of death in the UK Accounts for a third of all deaths 46,000 deaths in people < 75 years (70% of these
LIST OF ABBREVIATIONS
 Diabetes & Endocrinology 2005 Royal College of Physicians of Edinburgh Diabetes and lipids 1 G Marshall, 2 M Fisher 1 Research Fellow, Department of Cardiology, Glasgow Royal Infirmary, Glasgow, Scotland,
Diabetes & Endocrinology 2005 Royal College of Physicians of Edinburgh Diabetes and lipids 1 G Marshall, 2 M Fisher 1 Research Fellow, Department of Cardiology, Glasgow Royal Infirmary, Glasgow, Scotland,
Overview. The Mediterranean Diet: The Optimal Diet for Cardiovascular Health. No conflicts of interest or disclosures
 The Mediterranean Diet: The Optimal Diet for Cardiovascular Health No conflicts of interest or disclosures Vasanti Malik, ScD Research Scientist Department of Nutrition Harvard School of Public Health
The Mediterranean Diet: The Optimal Diet for Cardiovascular Health No conflicts of interest or disclosures Vasanti Malik, ScD Research Scientist Department of Nutrition Harvard School of Public Health
Disclosures. Prevention of Heart Disease: The New Guidelines. Summary of Talk. Four guidelines. No relevant disclosures.
 Disclosures Prevention of Heart Disease: The New Guidelines No relevant disclosures Nisha I. Parikh MD MPH Assistant Professor of Medicine Division of Cardiology Department of Medicine University of California
Disclosures Prevention of Heart Disease: The New Guidelines No relevant disclosures Nisha I. Parikh MD MPH Assistant Professor of Medicine Division of Cardiology Department of Medicine University of California
Pharmacy Drug Class Review
 Pharmacy Drug Class Review January 22, 2014 Authored By: Christina Manciocchi, Pharm.D. BCACP Disclaimer: Specific agents may have variations Edited By: Richard J. Kraft, Pharm.D.BCPS NEW CHOLESTEROL GUIDELINES
Pharmacy Drug Class Review January 22, 2014 Authored By: Christina Manciocchi, Pharm.D. BCACP Disclaimer: Specific agents may have variations Edited By: Richard J. Kraft, Pharm.D.BCPS NEW CHOLESTEROL GUIDELINES
Is Lower Better for LDL or is there a Sweet Spot
 Is Lower Better for LDL or is there a Sweet Spot ALAN S BROWN MD, FACC FNLA FAHA FASPC DIRECTOR, DIVISION OF CARDIOLOGY ADVOCATE LUTHERAN GENERAL HOSPITAL, PARK RIDGE, ILLINOIS DIRECTOR OF CARDIOLOGY,
Is Lower Better for LDL or is there a Sweet Spot ALAN S BROWN MD, FACC FNLA FAHA FASPC DIRECTOR, DIVISION OF CARDIOLOGY ADVOCATE LUTHERAN GENERAL HOSPITAL, PARK RIDGE, ILLINOIS DIRECTOR OF CARDIOLOGY,
2013 ACC/AHA Guidelines on the Assessment of Atherosclerotic Cardiovascular Risk: Overview and Commentary
 2013 ACC/AHA Guidelines on the Assessment of Atherosclerotic Cardiovascular Risk: Overview and Commentary The Johns Hopkins Ciccarone Center for the Prevention of Heart Disease Becky McKibben, MPH; Seth
2013 ACC/AHA Guidelines on the Assessment of Atherosclerotic Cardiovascular Risk: Overview and Commentary The Johns Hopkins Ciccarone Center for the Prevention of Heart Disease Becky McKibben, MPH; Seth
Disclosures. Diabetes and Cardiovascular Risk Management. Learning Objectives. Atherosclerotic Cardiovascular Disease
 Disclosures Diabetes and Cardiovascular Risk Management Tony Hampton, MD, MBA Medical Director Advocate Aurora Operating System Advocate Aurora Healthcare Downers Grove, IL No conflicts or disclosures
Disclosures Diabetes and Cardiovascular Risk Management Tony Hampton, MD, MBA Medical Director Advocate Aurora Operating System Advocate Aurora Healthcare Downers Grove, IL No conflicts or disclosures
Review current guideline recommendations for lipid-lowering therapy
 Breakout Session #3 New Paradigms in the Management of Dyslipidemia Review current guideline recommendations for lipid-lowering therapy Dr Meral KAYIKCIOGLU Ege University Medical School, Cardiology Dept,
Breakout Session #3 New Paradigms in the Management of Dyslipidemia Review current guideline recommendations for lipid-lowering therapy Dr Meral KAYIKCIOGLU Ege University Medical School, Cardiology Dept,
New ACC/AHA Guidelines on Lipids: Are PCSK9 Inhibitors Poised for a Breakthrough?
 New ACC/AHA Guidelines on Lipids: Are PCSK9 Inhibitors Poised for a Breakthrough? Sidney C. Smith, Jr. MD, FACC, FAHA Professor of Medicine/Cardiology University of North Carolina at Chapel Hill Immediate
New ACC/AHA Guidelines on Lipids: Are PCSK9 Inhibitors Poised for a Breakthrough? Sidney C. Smith, Jr. MD, FACC, FAHA Professor of Medicine/Cardiology University of North Carolina at Chapel Hill Immediate
Royal Wolverhampton Hospital Adult Lipid Lowering Therapy Guidelines Lipid Lowering Therapy for the Prevention of Cardiovascular Disease
 Royal Wolverhampton Hospital Adult Lipid Lowering Therapy Guidelines 1 This guideline is intended to assist rational and cost-effective prescribing of lipid regulating medications across both primary and
Royal Wolverhampton Hospital Adult Lipid Lowering Therapy Guidelines 1 This guideline is intended to assist rational and cost-effective prescribing of lipid regulating medications across both primary and
2013 ACC AHA LIPID GUIDELINE JAY S. FONTE, MD
 2013 ACC AHA LIPID GUIDELINE JAY S. FONTE, MD How do you interpret my blood test results? What are our targets for these tests? Before the ACC/AHA Lipid Guidelines A1c:
2013 ACC AHA LIPID GUIDELINE JAY S. FONTE, MD How do you interpret my blood test results? What are our targets for these tests? Before the ACC/AHA Lipid Guidelines A1c:
APPENDIX 2F Management of Cholesterol
 Patients with established CVD: Coronary heart disease Cerebrovascular disease Peripheral vascular disease APPEDIX 2F Management of Cholesterol Patients at high risk of cardiovascular events: Chronic kidney
Patients with established CVD: Coronary heart disease Cerebrovascular disease Peripheral vascular disease APPEDIX 2F Management of Cholesterol Patients at high risk of cardiovascular events: Chronic kidney
Case Discussions: Treatment Strategies for High Risk Populations. Most Common Reasons for Referral to the Baylor Lipid Clinic
 Case Discussions: Treatment Strategies for High Risk Populations Peter H. Jones MD, FNLA Associate Professor Methodist DeBakey Heart and Vascular Center Baylor College of Medicine Most Common Reasons for
Case Discussions: Treatment Strategies for High Risk Populations Peter H. Jones MD, FNLA Associate Professor Methodist DeBakey Heart and Vascular Center Baylor College of Medicine Most Common Reasons for
Marshall Tulloch-Reid, MD, MPhil, DSc, FACE Epidemiology Research Unit Tropical Medicine Research Institute The University of the West Indies, Mona,
 Marshall Tulloch-Reid, MD, MPhil, DSc, FACE Epidemiology Research Unit Tropical Medicine Research Institute The University of the West Indies, Mona, Jamaica At the end of this presentation the participant
Marshall Tulloch-Reid, MD, MPhil, DSc, FACE Epidemiology Research Unit Tropical Medicine Research Institute The University of the West Indies, Mona, Jamaica At the end of this presentation the participant
Contemporary management of Dyslipidemia
 Contemporary management of Dyslipidemia Todd Anderson Feb 2018 Disclosure Statement Within the past two years: I have not had an affiliation (financial or otherwise) with a commercial organization that
Contemporary management of Dyslipidemia Todd Anderson Feb 2018 Disclosure Statement Within the past two years: I have not had an affiliation (financial or otherwise) with a commercial organization that
Advances in Lipid Management
 Advances in Lipid Management Kavita Sharma, MD Assistant Professor of Medicine, Division of Cardiology Clinical Director of the Lipid Management Clinics, The Ohio State University Wexner Medical Center
Advances in Lipid Management Kavita Sharma, MD Assistant Professor of Medicine, Division of Cardiology Clinical Director of the Lipid Management Clinics, The Ohio State University Wexner Medical Center
Dyslipidemia: Lots of Good Evidence, Less Good Interpretation.
 Dyslipidemia: Lots of Good Evidence, Less Good Interpretation. G Michael Allan Evidence & CPD Program, ACFP Associate Professor, Dept of Family, U of A. CFPC CoI Templates: Slide 1 Faculty/Presenter Disclosure
Dyslipidemia: Lots of Good Evidence, Less Good Interpretation. G Michael Allan Evidence & CPD Program, ACFP Associate Professor, Dept of Family, U of A. CFPC CoI Templates: Slide 1 Faculty/Presenter Disclosure
Antiplatelet Therapy in Primary CVD Prevention and Stable Coronary Artery Disease. Καρακώστας Γεώργιος Διευθυντής Καρδιολογικής Κλινικής, Γ.Ν.
 Antiplatelet Therapy in Primary CVD Prevention and Stable Coronary Artery Disease Καρακώστας Γεώργιος Διευθυντής Καρδιολογικής Κλινικής, Γ.Ν.Κιλκίς Primary CVD Prevention A co-ordinated set of actions,
Antiplatelet Therapy in Primary CVD Prevention and Stable Coronary Artery Disease Καρακώστας Γεώργιος Διευθυντής Καρδιολογικής Κλινικής, Γ.Ν.Κιλκίς Primary CVD Prevention A co-ordinated set of actions,
Acute Coronary Syndromes (ACS)
") Sally A. Arif, Pharm.D., BCPS (AQ Cardiology) Assistant Professor of Pharmacy Practice Midwestern University, Chicago College of Pharmacy Cardiology Clinical Specialist, Rush University Medical Center
Sally A. Arif, Pharm.D., BCPS (AQ Cardiology) Assistant Professor of Pharmacy Practice Midwestern University, Chicago College of Pharmacy Cardiology Clinical Specialist, Rush University Medical Center
John J.P. Kastelein MD PhD Professor of Medicine Dept. of Vascular Medicine Academic Medial Center / University of Amsterdam
 Latest Insights from the JUPITER Study John J.P. Kastelein MD PhD Professor of Medicine Dept. of Vascular Medicine Academic Medial Center / University of Amsterdam Inflammation, hscrp, and Vascular Prevention
Latest Insights from the JUPITER Study John J.P. Kastelein MD PhD Professor of Medicine Dept. of Vascular Medicine Academic Medial Center / University of Amsterdam Inflammation, hscrp, and Vascular Prevention
Lipid Therapy: Statins and Beyond. Ivan Anderson, MD RIHVH Cardiology
 Lipid Therapy: Statins and Beyond Ivan Anderson, MD RIHVH Cardiology Outline The cholesterol hypothesis and lipid metabolism The Guidelines 4 Groups that Benefit from Lipid therapy Initiation and monitoring
Lipid Therapy: Statins and Beyond Ivan Anderson, MD RIHVH Cardiology Outline The cholesterol hypothesis and lipid metabolism The Guidelines 4 Groups that Benefit from Lipid therapy Initiation and monitoring
Confusion about guidelines: How should we treat lipids?
 Confusion about guidelines: How should we treat lipids? Anne Carol Goldberg, MD, FACP, FAHA, FNLA Professor of Medicine Washington University School of Medicine American College of Physicians Missouri
Confusion about guidelines: How should we treat lipids? Anne Carol Goldberg, MD, FACP, FAHA, FNLA Professor of Medicine Washington University School of Medicine American College of Physicians Missouri
SIGN 149 Risk estimation and the prevention of cardiovascular disease. Quick Reference Guide July Evidence
 SIGN 149 Risk estimation and the prevention of cardiovascular disease Quick Reference Guide July 2017 Evidence ESTIMATING CARDIOVASCULAR RISK R Individuals with the following risk factors should be considered
SIGN 149 Risk estimation and the prevention of cardiovascular disease Quick Reference Guide July 2017 Evidence ESTIMATING CARDIOVASCULAR RISK R Individuals with the following risk factors should be considered
A New Age of Dyslipidemia Treatment: Role of Non- Statin Therapies
 A New Age of Dyslipidemia Treatment: Role of Non- Statin Therapies BRODY MAACK, PHARMD, BCACP, CTTS Objectives 1. Review current guidelines regarding use of statin medications in the treatment and prevention
A New Age of Dyslipidemia Treatment: Role of Non- Statin Therapies BRODY MAACK, PHARMD, BCACP, CTTS Objectives 1. Review current guidelines regarding use of statin medications in the treatment and prevention
Lipid Management: The Next Level How Will the New ACC/AHA Guidelines Change My Practice
 Lipid Management: The Next Level How Will the New ACC/AHA Guidelines Change My Practice Vera Bittner, MD, MSPH Professor of Medicine Section Head, Preventive Cardiology Medical Director, Cardiac Rehabilitation
Lipid Management: The Next Level How Will the New ACC/AHA Guidelines Change My Practice Vera Bittner, MD, MSPH Professor of Medicine Section Head, Preventive Cardiology Medical Director, Cardiac Rehabilitation
Heart Disease Genesis
 Heart Disease Genesis The Ultimate Lecture on CAD origins Petr Polasek MD FRCPC FACC Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored,
Heart Disease Genesis The Ultimate Lecture on CAD origins Petr Polasek MD FRCPC FACC Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored,
American Osteopathic College of Occupational and Preventive Medicine 2012 Mid-Year Educational Conference St. Petersburg, Florida
 The 21 st Century Paradigm Shift: Prevention Rather Than Intervention for the Treatment of Stable CHD The Economic Burden of Cardiovascular Diseases Basil Margolis MD, FACC, FRCP Director, Preventive Cardiology
The 21 st Century Paradigm Shift: Prevention Rather Than Intervention for the Treatment of Stable CHD The Economic Burden of Cardiovascular Diseases Basil Margolis MD, FACC, FRCP Director, Preventive Cardiology
When Statins Aren t Enough: Appropriate Therapies for High-Risk Patients with Diabetes
 When Statins Aren t Enough: Appropriate Therapies for High-Risk Patients with Diabetes Kim K. Birtcher, MS, PharmD, AACC, FNLA, CLS, BCPS (AQ-Cardiology), CDE Clinical Professor University of Houston College
When Statins Aren t Enough: Appropriate Therapies for High-Risk Patients with Diabetes Kim K. Birtcher, MS, PharmD, AACC, FNLA, CLS, BCPS (AQ-Cardiology), CDE Clinical Professor University of Houston College
Sanger Heart & Vascular Institute Symposium 2015
 Sanger Heart & Vascular Institute Symposium 2015 Cardiovascular Update For Primary Care Physicians William E. Downey, MD FACC FSCAI Medical Director, Interventional Cardiology Sanger Heart & Vascular Institute
Sanger Heart & Vascular Institute Symposium 2015 Cardiovascular Update For Primary Care Physicians William E. Downey, MD FACC FSCAI Medical Director, Interventional Cardiology Sanger Heart & Vascular Institute
Cardiovascular Risk Reduction and Other Co-Morbidities in Type 2 Diabetes
 Cardiovascular Risk Reduction and Other Co-Morbidities in Type 2 Diabetes Following this presentation, you will be able to: Describe the relationship between major CV risk factors and CVD outcomes Select
Cardiovascular Risk Reduction and Other Co-Morbidities in Type 2 Diabetes Following this presentation, you will be able to: Describe the relationship between major CV risk factors and CVD outcomes Select
9/18/2017 DISCLOSURES. Consultant: RubiconMD. Research: Amgen, NHLBI OUTLINE OBJECTIVES. Review current CV risk assessment tools.
 UW MEDICINE UW MEDICINE UCSF ASIAN TITLE HEALTH OR EVENT SYMPOSIUM 2017 DISCLOSURES Consultant: RubiconMD ESTIMATING CV RISK IN ASIAN AMERICANS AND PREVENTION OF CVD Research: Amgen, NHLBI EUGENE YANG,
UW MEDICINE UW MEDICINE UCSF ASIAN TITLE HEALTH OR EVENT SYMPOSIUM 2017 DISCLOSURES Consultant: RubiconMD ESTIMATING CV RISK IN ASIAN AMERICANS AND PREVENTION OF CVD Research: Amgen, NHLBI EUGENE YANG,
Update on Dyslipidemia and Recent Data on Treating the Statin Intolerant Patient
 Update on Dyslipidemia and Recent Data on Treating the Statin Intolerant Patient Steven E. Nissen MD Chairman, Department of Cardiovascular Medicine Cleveland Clinic Disclosure Consulting: Many pharmaceutical
Update on Dyslipidemia and Recent Data on Treating the Statin Intolerant Patient Steven E. Nissen MD Chairman, Department of Cardiovascular Medicine Cleveland Clinic Disclosure Consulting: Many pharmaceutical
Disclosures No relationships (not even to an employer) No off-label uses. Cholesterol Lowering Guidelines: What now?
 No off-label uses. Cholesterol Lowering Guidelines: What now?") Disclosures No relationships (not even to an employer) No off-label uses Cholesterol Lowering Guidelines: What now?, FACP 1 2 65-year-old white woman Total cholesterol 175mg/dL HDL 54 mg/dl LDL 96 mg/dl
Disclosures No relationships (not even to an employer) No off-label uses Cholesterol Lowering Guidelines: What now?, FACP 1 2 65-year-old white woman Total cholesterol 175mg/dL HDL 54 mg/dl LDL 96 mg/dl
New Cholesterol Guidelines What the LDL are we supposed to do now?!
 New Cholesterol Guidelines What the LDL are we supposed to do now?! Michael D. Shapiro Assistant Professor of Medicine and Radiology Knight Cardiovascular Institute Oregon Health & Science University 2013
New Cholesterol Guidelines What the LDL are we supposed to do now?! Michael D. Shapiro Assistant Professor of Medicine and Radiology Knight Cardiovascular Institute Oregon Health & Science University 2013
JUPITER NEJM Poll. Panel Discussion: Literature that Should Have an Impact on our Practice: The JUPITER Study
 Panel Discussion: Literature that Should Have an Impact on our Practice: The Study Kaiser COAST 11 th Annual Conference Maui, August 2009 Robert Blumberg, MD, FACC Ralph Brindis, MD, MPH, FACC Primary
Panel Discussion: Literature that Should Have an Impact on our Practice: The Study Kaiser COAST 11 th Annual Conference Maui, August 2009 Robert Blumberg, MD, FACC Ralph Brindis, MD, MPH, FACC Primary
Joslin Diabetes Center Advances in Diabetes and Thyroid Disease 2013 Consensus and Controversy in Diabetic Dyslipidemia
 Consensus and Controversy in Diabetes and Dyslipidemia Om P. Ganda MD Director, Lipid Clinic Joslin diabetes Center Boston, MA, USA CVD Outcomes in DM vs non- DM 102 Prospective studies; 698, 782 people,
Consensus and Controversy in Diabetes and Dyslipidemia Om P. Ganda MD Director, Lipid Clinic Joslin diabetes Center Boston, MA, USA CVD Outcomes in DM vs non- DM 102 Prospective studies; 698, 782 people,
See Important Reminder at the end of this policy for important regulatory and legal information.
 Clinical Policy: (Repatha) Reference Number: HIM.PA.SP46 Effective Date: 01.01.18 Last Review Date: Line of Business: Health Insurance Marketplace Revision Log See Important Reminder at the end of this
Clinical Policy: (Repatha) Reference Number: HIM.PA.SP46 Effective Date: 01.01.18 Last Review Date: Line of Business: Health Insurance Marketplace Revision Log See Important Reminder at the end of this
Treatment of Cholesterol in 2018: Time to Level Up. Most Important Slide. Three Things Learned that Will be Applied
 Treatment of Cholesterol in 2018: Time to Level Up 1. Most Important Slide Three Things Learned that Will be Applied 2. 3. 2013 Top Ten Points 1. Expert committee. Evidence used. 2. Four groups identified
Treatment of Cholesterol in 2018: Time to Level Up 1. Most Important Slide Three Things Learned that Will be Applied 2. 3. 2013 Top Ten Points 1. Expert committee. Evidence used. 2. Four groups identified
CVD Risk Assessment. Lipid Management in Women: Lessons Learned. Conflict of Interest Disclosure
 Lipid Management in Women: Lessons Learned Conflict of Interest Disclosure Emma A. Meagher, MD has no conflicts to disclose Emma A. Meagher, MD Associate Professor, Medicine and Pharmacology University
Lipid Management in Women: Lessons Learned Conflict of Interest Disclosure Emma A. Meagher, MD has no conflicts to disclose Emma A. Meagher, MD Associate Professor, Medicine and Pharmacology University
Disclosures. Choosing a Statin/New Therapies. Case. How else would you do to treat him? LDL-C Reduction with Different Statin Strategies
 Disclosures I have no disclosures relevant to this talk Choosing a Statin/New Therapies Aryan Aiyer, MD Assistant Professor of Medicine University of Pittsburgh School of Medicine UPMC Heart and Vascular
Disclosures I have no disclosures relevant to this talk Choosing a Statin/New Therapies Aryan Aiyer, MD Assistant Professor of Medicine University of Pittsburgh School of Medicine UPMC Heart and Vascular
B. Patient has not reached the percentage reduction goal with statin therapy
 Managing Cardiovascular Risk: The Importance of Lowering LDL Cholesterol and Reaching Treatment Goals for LDL Cholesterol The Role of the Pharmacist Learning Objectives 1. Review the role of lipid levels
Managing Cardiovascular Risk: The Importance of Lowering LDL Cholesterol and Reaching Treatment Goals for LDL Cholesterol The Role of the Pharmacist Learning Objectives 1. Review the role of lipid levels
Cholesterol Treatment Update
 Cholesterol Treatment Update Patrick E. McBride, M.D., M.P.H. Professor of Medicine, Cardiovascular Medicine Associate Director, Preventive Cardiology Program UW School of Medicine and Public Health Disclosure:
Cholesterol Treatment Update Patrick E. McBride, M.D., M.P.H. Professor of Medicine, Cardiovascular Medicine Associate Director, Preventive Cardiology Program UW School of Medicine and Public Health Disclosure:
Index. cardiology.theclinics.com. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A ACC/AHA. See American College of Cardiology/ ACE inhibitors. See Angiotensin-converting enzyme (ACE) inhibitors American College of Cardiology/American
Index Note: Page numbers of article titles are in boldface type. A ACC/AHA. See American College of Cardiology/ ACE inhibitors. See Angiotensin-converting enzyme (ACE) inhibitors American College of Cardiology/American