Cardiac evaluation for the noncardiac. Nathaen Weitzel MD University of Colorado Denver Dept of Anesthesiology
|
|
|
- Richard Kennedy
- 5 years ago
- Views:
Transcription
1 Cardiac evaluation for the noncardiac patient Nathaen Weitzel MD University of Colorado Denver Dept of Anesthesiology
2 Objectives! Review ACC / AHA guidelines as updated for 2009! Discuss new recommendations with!-blockers.! Discuss issues surrounding revascularization and stents in the perioperative setting
3
4
5 General approach:! Goal is not medical clearance for surgery.! Rather it is a discussion about cardiac risk for a given procedure and patient.! Ideally this allows for medical planning to minimize risk, and utilize maximal therapy prior to surgery.
6 Who should you worry about?! Patients with known CAD.! Patients with new symptoms indicating CAD! Asymptomatic patients over age 50:! This group is the reference in the Revised Cardiac Risk Index! More extensive evaluation may be warranted starting with focused cardiac history
7
8 What are the active cardiac conditions?
9 Active Cardiac Conditions: The Big Five 1. Unstable coronary syndromes! Unstable angina / recent MI (within 30 days) 2. Decompensated Heart Failure! Class IV or new onset 3. Significant Arrhythmias! High grade AV block, 3 rd degree block, symptomatic ventricular arrhythmias, SVT s without rate control, severe bradycardia, new VT
10 Active Cardiac Conditions: 4. Severe AS* 5. Severe MS*! Presence of Active Cardiac Conditions warrants further evaluation unless case is emergent. (Class I)! Non-invasive testing vs catheterization based on patient scenario and previous workup.
11 What s next-! Absence of the big five leads to the OR most of the time! Based on functional capacity and surgical risk.
12
13 Low Surgical Risk:! Combined incidence of cardiac death or nonfatal MI < 1%! Ambulatory surgery, Cataracts, Breast surgery, endoscopic procedures, superficial procedures! Noninvasive testing not useful in low risk surgery (Class III)
14 Intermediate Risk Surgery:! Cardiac Risk 1-5%! Orthopedic surgery, head and neck, carotid endarterectomy, prostate surgery, intraperitoneal surgery, & intrathoracic surgery.
15 High Risk Surgery! Cardiac risk reported > 5%.! Aortic and major vascular surgery along with peripheral vascular procedures.! Key point: For intermediate or high risk surgery, further testing should be based on clinical risk factors & undertaken only if it will change management. (Class IIa / IIb)
16
17 Step 5 is often the key! These patients fall into the unknown category.! Not clearly healthy, but not clearly unhealthy! Assesment based on physical ability, and clinical risk factors.
18
19 How about low activity or unclear activity patients?! Must rely on clinical risk factors to determine surgical risk


20 Clinical Risk Factors:! ACC / AHA guidelines used Revised Cardiac Risk Index as basis or recommendations.
21 Results:
22 Clinical Risk Factors! Ischemic heart disease:! Hx of MI, + treadmill, NTG use, current angina, Q waves on ECG**.! CHF! Hx of CHF, Pulm Edema, Bilateral Rales! Cerebrovascular Disease! TIA or full stroke
23 Clinical Risk factors:! Number of factors correlates to class, ie class I, II, III, IV.! History of MI or abnormal Q wave on ECG is a clinical risk factor.! Acute MI < 1 month is active cardiac condition! Class correlated with risk based on type of surgery
24 Using clinical factors! High risk surgery with 3 or more risk factors warrants testing IF management may be altered! (Class IIa)! Intermediate risk! regardless of clinical factors can proceed with optimal HR control or consider noninvasive testing IF management may be altered! (Class IIb)
25 How different from 2002:! Elimination of intermediate and minor clinical predictors! Use Revised cardiac risk index! Minor predictors not proven to independently increase cardiac risk perioperatively! Age, Abnl ECG, Rhythm not SR, HTN*! Goal to identify patients who may benefit from revascularization
26 Preoperative testing:! Active Cardiac Conditions warrant invasive testing most of the time! Resting LV function not a consistent predictor of ischemic events! ECG warranted within 30 days if: " Major surgery and at least 1 risk factor " Intermediate surgery and known CAD " Age > 50! Stress test! gives best information*
27 Problems with guidelines! Higher level of Class II evidence used! Reduced amount of Class I evidence (10%)! Places high importance on risk of surgery but increased endovascular therapies (AAA endografts etc) may alter classic risk groups
28 Case Scenario:! 58 yo female, SSO for elective hip replacement! Daughter tells you she had a heart attack 10 months prior they placed a stent in one of her coronary vessels! DM not on insulin! Patient is not active.! BP 185/ 95 in pre-op. Baseline 160 / 85
29 Assessment:! Intermediate Risk Surgery - Elective! Pre-op labs! Hct 42. Cr 1.1.! Review Medications! On B-Blockade, Statin therapy, ASA. Stopped Plavix 5 days prior.! Get ECG! Q waves in II / III
30 Case Scenario! Should we stress test the patient?! How about further revascularization?! What about her!-blockers?! What about her existing stent?

31 Basic changes are a discussion of the POISE trial and how this has impacted recommendations for -blocker therapy.

32 ! 8351 pts for non-cardiac surgery! Randomized to metoprolol extended release vs placebo! 190 hospitals, 23 countries.! Tx initiated 2-4 hours before surgery continued for 30 days.
33 Cardiac Events Myocardial Infarction! A primary outcome was composite of cardiac death, non-fatal MI, non-fatal cardiac arrest within 30 days.! B- Myocardial Infarction
34 Stroke Death C Stroke D - Death
35 Conclusions: Reduction in cardiac related events, but increased risk of stroke and overall increase in mortality using extended release Metoprolol.
36
37 What to do.! Class I: Continue!-blockade for pts on medication! Class IIa: Probably good to titrate!-blockade for high cardiac risk pts in both high and intermediate risk surgery, and for patients with > 1 clinical risk factor.! Class IIb: Use of!-blockade is uncertain in intermediate risk surgery and low / intermediate cardiac risk groups.
38 What not to do.! Class III: Don t give to patients with absolute contraindications to!-blockade! Based on POISE routine administration of!-blockade on day of surgery cannot be advocated
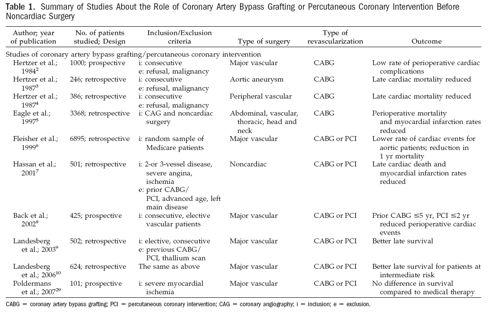
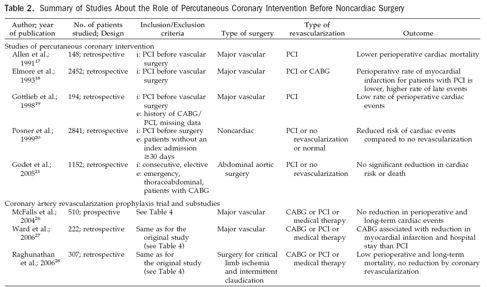
39 Revascularization! Multiple studies, some randomized, some not looking at both CABG and PCI! Entire lecture series! Multiple questions: CABG vs PCI, what type of testing best, which group of patients best..
40 Does Revascularization Matter??
41 ! 5859 pts for major vascular surgery! 510 Pts angiographically stable CAD! 1/3 with 3 vessel disease! 33% aortic, 66% peripheral vascular! Active Cardiac Conditions excluded! Randomized to intervention or not before surgery (CABG 41%, PCI 59%)
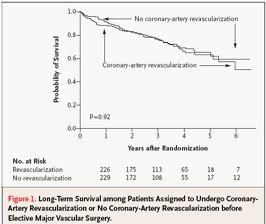
42 ! Of 510 pts studied:! 49% had 2 Clinical Risk Factors! 13% had 3 Clinical Risk Factors! 62% had nuclear perfusion scanning! Perfusion defect moderate or large in 226 patients! Mortality was final end point! One year follow-up minimum
43
44

45
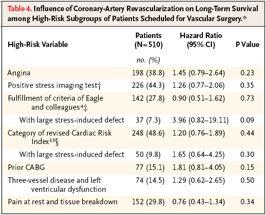
46 Principle finding of this study is that among patients with stable coronary artery disease, revascularization does not improve long term survival.
47 Revascularization: Poldermans - J AM Coll Cardiol 2007;49: ! Decrease V: Looked at value of preoperative revascularization! Screened patients with >3 risk factors! 1880 patients screened, 430 high risk patients found! 101 patients randomized with extensive ischemia after testing! End points were death or MI at 30 days and one year.
48 Results:! 43% vs 33% incidence, but not statistically significant between groups! Overall study was a pilot study, and underpowered.! Key point: High risk study group with relatively high complication rates! Aggressive medical management with ASA, and B- Blockade
49 CONCLUSIONS: In this randomized pilot study, designed to obtain efficacy and safety estimates, preoperative coronary revascularization in high-risk patients was not associated with an improved outcome.
50
51
52 Revascularization! Bottom Line:! CABG probably better than PCI overall! Only recommended if significant myocardium at risk.
 2009 by the")
53 But wait. (J Am Coll Cardiol 2009;54:989 96) 2009 by the American College of Cardiology Foundation
54 ! Study designed to determine impact of systematic coronary angiography on intermediate and long term outcomes in medium risk patients for vascular procedures.! Basically in between CARP and Decrease V.
55 ! 208 pts for elective Vascular surgery! Randomized Control group had invasive testing based on positive stress test (ACC guidelines strategy)! Study group had initial coronary angiography from start
56 ! Anti-platelet agents stopped and pts bridged with LMWH! If stents placed, BMS used. Surgery done in days. Plavix stopped for surgery, ASA maintained.! Surgical intervention by OPCAB if indicated
57
58
59 For patients at medium to high risk! First randomized study for medium risk patients demonstrating benefit for aggressive interventional approach for cardiac events presenting for elective vascular surgery, a systematic! Assumes maximal medical therapy along with anti-platelet therapy for stented patients angiographic approach guiding cardiac therapy confers a survival benefit.
60 What to do.! Class I: Revascularize pts with significant left main disease (CABG), 3 vessel disease, 2V disease + proximal LAD lesions, high risk unstable angina or with acute STelevation MI.
61 What not to do.! Class III, Level B: Due to elevated risk of re-stenosis, and lack of support by current clinical trials PCI is not routinely recommended unless patient has active cardiac condition amenable to intervention.! Class IIb: PCI not well established for pts with abnormal stress echocardiography (low or high risk).
62 What about surgery after Stenting?! Questions recently regarding use of bare metal stents vs drug eluting stents.! Elevated risk of thrombosis in BMS until endothelialization occurs at 6 weeks if anti-platelet therapy stopped! Risk of thrombosis elevated with DES for 12 months if anti-platelet drugs stopped (plavix)
63 Approach for previous PCI management
64 Need for stenting along with noncardiac surgery
65 Case Scenario:! Take effort to assess physical activity! If on Beta-blockade, ASA, and Statins then I would proceed after reducing BP in pre-op.! Stent: Assume DES could be justified in delaying surgery until 12 months out.! Definite increase risk in stopping Plavix with DES before 6 mos with low risk of stenosis after 12 months. No real data on patients months out.
66 Recommended reading:
67 Concluding thoughts:! Use published guidelines to guide decision making! Discuss risk with patient and outline potential options! Most of time the OR will be the answer given ideal medical therapy! Documentation of discussion is vital! Tight hemodynamic control is key in high risk cardiac patients
68 References: 1. Fleisher, L.A., et al., Circulation, (17): p Fleisher, L.A., et al., J Am Coll Cardiol, (22): p. e13-e Lee, T.H., et al., Circulation, (10): p McFalls, E.O., et al., N Engl J Med, (27): p Poldermans, D., et al., J Am Coll Cardiol, (17): p Devereaux, P.J., et al., Lancet, (9627): p Monaco, M., et al., J Am Coll Cardiol, (11): p Kertai, M.D., Anesth Analg, (3): p
Perioperative Cardiology Consultations for Noncardiac Surgery Ischemic Heart Disease
 2012 대한춘계심장학회 Perioperative Cardiology Consultations for Noncardiac Surgery Ischemic Heart Disease 울산의대울산대학병원심장내과이상곤 ECG CLASS IIb 1. Preoperative resting 12-lead ECG may be reasonable in patients with
2012 대한춘계심장학회 Perioperative Cardiology Consultations for Noncardiac Surgery Ischemic Heart Disease 울산의대울산대학병원심장내과이상곤 ECG CLASS IIb 1. Preoperative resting 12-lead ECG may be reasonable in patients with
Preoperative Cardiac Evaluation:
 Preoperative Cardiac Evaluation: The New Guidelines Hugo Quinny Cheng, MD Division of Hospital Medicine University of California, San Francisco Disclosures No financial relationships with pharmaceutical
Preoperative Cardiac Evaluation: The New Guidelines Hugo Quinny Cheng, MD Division of Hospital Medicine University of California, San Francisco Disclosures No financial relationships with pharmaceutical
Assessing Cardiac Risk in Noncardiac Surgery. Murali Sivarajan, M.D. Professor University of Washington Seattle, Washington
 Assessing Cardiac Risk in Noncardiac Surgery Murali Sivarajan, M.D. Professor University of Washington Seattle, Washington Disclosure None. I have no conflicts of interest, financial or otherwise. CME
Assessing Cardiac Risk in Noncardiac Surgery Murali Sivarajan, M.D. Professor University of Washington Seattle, Washington Disclosure None. I have no conflicts of interest, financial or otherwise. CME
Clinical Controversies in Perioperative Medicine
 Clinical Controversies in Perioperative Medicine Hugo Quinny Cheng, MD Division of Hospital Medicine University of California, San Francisco Cardiac Evaluation: New Guidelines A 70-y.o. man with progressive
Clinical Controversies in Perioperative Medicine Hugo Quinny Cheng, MD Division of Hospital Medicine University of California, San Francisco Cardiac Evaluation: New Guidelines A 70-y.o. man with progressive
Perioperative Cardiovascular Evaluation and Care for Noncardiac. Dr Mahmoud Ebrahimi Interventional cardiologist 91/9/30
 Perioperative Cardiovascular Evaluation and Care for Noncardiac Surgery Dr Mahmoud Ebrahimi Interventional cardiologist 91/9/30 Active Cardiac Conditions for Which the Patient Should Undergo Evaluation
Perioperative Cardiovascular Evaluation and Care for Noncardiac Surgery Dr Mahmoud Ebrahimi Interventional cardiologist 91/9/30 Active Cardiac Conditions for Which the Patient Should Undergo Evaluation
Clinical Controversies in Perioperative Medicine
 Clinical Controversies in Perioperative Medicine Hugo Quinny Cheng, MD Division of Hospital Medicine University of California, San Francisco Predicting & Managing Cardiac Risk A 70-y.o. man with progressive
Clinical Controversies in Perioperative Medicine Hugo Quinny Cheng, MD Division of Hospital Medicine University of California, San Francisco Predicting & Managing Cardiac Risk A 70-y.o. man with progressive
Guidelines PATHOLOGY: FATAL PERIOPERATIVE MI NON-PMI N = 25 PMI N = 42. Prominent Dutch Cardiovascular Researcher Fired for Scientific Misconduct
 PATHOLOGY: FATAL PERIOPERATIVE MI NON-PMI N = 25 PMI N = 42 Preoperative, Intraoperative, and Postoperative Factors Associated with Perioperative Cardiac Complications in Patients Undergoing Major Noncardiac
PATHOLOGY: FATAL PERIOPERATIVE MI NON-PMI N = 25 PMI N = 42 Preoperative, Intraoperative, and Postoperative Factors Associated with Perioperative Cardiac Complications in Patients Undergoing Major Noncardiac
8/28/2018. Pre-op Evaluation for non cardiac surgery. A quick review from 2007!! Disclosures. John Steuter, MD. None
 Pre-op Evaluation for non cardiac surgery John Steuter, MD Disclosures None A quick review from 2007!! Fliesheret al, ACC/AHA 2007 Guidelines on Perioperative Cardiovascular Evaluation and are for Noncardiac
Pre-op Evaluation for non cardiac surgery John Steuter, MD Disclosures None A quick review from 2007!! Fliesheret al, ACC/AHA 2007 Guidelines on Perioperative Cardiovascular Evaluation and are for Noncardiac
SESSION 5 2:20 3:35 pm
 SESSION 2:2 3:3 pm Strategies to Reduce Cardiac Risk for Noncardiac Surgery SPEAKER Lee A. Fleisher, MD Presenter Disclosure Information The following relationships exist related to this presentation:
SESSION 2:2 3:3 pm Strategies to Reduce Cardiac Risk for Noncardiac Surgery SPEAKER Lee A. Fleisher, MD Presenter Disclosure Information The following relationships exist related to this presentation:
Update on Perioperative Medicine. Update on Perioperative Medicine. Question 1: Clinical Risk Prediction. for the Office-based Practitioner
 Update on Perioperative Medicine Update on Perioperative Medicine for the Office-based Practitioner Hugo Quinny Cheng, MD Division of Hospital Medicine University of California, San Francisco Predicting
Update on Perioperative Medicine Update on Perioperative Medicine for the Office-based Practitioner Hugo Quinny Cheng, MD Division of Hospital Medicine University of California, San Francisco Predicting
Perioperative Cardiac Management. Emma Sargsyan, MD, FACP
 Perioperative Cardiac Management Emma Sargsyan, MD, FACP March 22-24, 2018 Outline Evaluation of cardiac risk prior to non-cardiac surgery Management of cardiac risk for non-cardiac surgery 2 Preop medical
Perioperative Cardiac Management Emma Sargsyan, MD, FACP March 22-24, 2018 Outline Evaluation of cardiac risk prior to non-cardiac surgery Management of cardiac risk for non-cardiac surgery 2 Preop medical
Preoperative Cardiac Risk Assessment: Approach & Guidelines
 Preoperative Cardiac Risk Assessment: Approach & Guidelines By, Liam Morris, MD., FACC (02/03/18) CPG : Clinical Practice Guidelines GDMT : Guidelines Directed Medical Therapy GWC : Guideline Writing Committee
Preoperative Cardiac Risk Assessment: Approach & Guidelines By, Liam Morris, MD., FACC (02/03/18) CPG : Clinical Practice Guidelines GDMT : Guidelines Directed Medical Therapy GWC : Guideline Writing Committee
Clinical Controversies in Perioperative Medicine
 Update on Perioperative Medicine Clinical Controversies in Perioperative Medicine Hugo Quinny Cheng, MD Division of Hospital Medicine University of California, San Francisco Cardiac Medications & Perioperative
Update on Perioperative Medicine Clinical Controversies in Perioperative Medicine Hugo Quinny Cheng, MD Division of Hospital Medicine University of California, San Francisco Cardiac Medications & Perioperative
Perioperative Medical Therapy: Beta Blockers, Statins, ACE-Inhibitors, ARB Effects on Mortality
 Perioperative Medical Therapy: Beta Blockers, Statins, ACE-Inhibitors, ARB Effects on Mortality Art Wallace, MD, PhD SF VAMC Chief of Anethesia and Vice Chair of Anesthesia and Perioperative Care UCSF
Perioperative Medical Therapy: Beta Blockers, Statins, ACE-Inhibitors, ARB Effects on Mortality Art Wallace, MD, PhD SF VAMC Chief of Anethesia and Vice Chair of Anesthesia and Perioperative Care UCSF
PERIOPERATIVE CARDIAC RISK ASSESSMENT. Divya Gollapudi, MD
 PERIOPERATIVE CARDIAC RISK ASSESSMENT Divya Gollapudi, MD Clinical Assistant Professor Hospital Medicine Program Division of General Internal Medicine Harborview Medical Center None Disclosures Objectives
PERIOPERATIVE CARDIAC RISK ASSESSMENT Divya Gollapudi, MD Clinical Assistant Professor Hospital Medicine Program Division of General Internal Medicine Harborview Medical Center None Disclosures Objectives
Cardiac Risk Assessment in the Preoperative period
 Cardiac Risk Assessment in the Preoperative period Catherine Curley, MD May, 2017 Disclosures I am not a cardiologist! 1 Case 1 78 yo man presenting to the ED after mechanical fall on his driveway. Found
Cardiac Risk Assessment in the Preoperative period Catherine Curley, MD May, 2017 Disclosures I am not a cardiologist! 1 Case 1 78 yo man presenting to the ED after mechanical fall on his driveway. Found
Evaluation and Management of the Patient with Cardiac Disease for Non-Cardiac Surgery WINTER CONFRENCE 2016 RONY GORGES, MD
 Evaluation and Management of the Patient with Cardiac Disease for Non-Cardiac Surgery WINTER CONFRENCE 2016 RONY GORGES, MD 67 yo man Asymptomatic carotid stenosis, CEA planned Golfs regularly, walks and
Evaluation and Management of the Patient with Cardiac Disease for Non-Cardiac Surgery WINTER CONFRENCE 2016 RONY GORGES, MD 67 yo man Asymptomatic carotid stenosis, CEA planned Golfs regularly, walks and
Timing of Surgery After Percutaneous Coronary Intervention
 Timing of Surgery After Percutaneous Coronary Intervention Deepak Talreja, MD, FACC Bayview/EVMS/Sentara Outline/Highlights Timing of elective surgery What to do with medications Stopping anti-platelet
Timing of Surgery After Percutaneous Coronary Intervention Deepak Talreja, MD, FACC Bayview/EVMS/Sentara Outline/Highlights Timing of elective surgery What to do with medications Stopping anti-platelet
COMPARISON OF 2014 ACCAHA VS. ESC GUIDELINES EDITORIAL
 COMPARISON OF 2014 ACCAHA VS. ESC GUIDELINES EDITORIAL Guidelines in review: Comparison of the 2014 ACC/AHA guidelines on perioperative cardiovascular evaluation and management of patients undergoing noncardiac
COMPARISON OF 2014 ACCAHA VS. ESC GUIDELINES EDITORIAL Guidelines in review: Comparison of the 2014 ACC/AHA guidelines on perioperative cardiovascular evaluation and management of patients undergoing noncardiac
Agenda. Perioperative Cardiac Risk Stratification circa Surgical Mortality: What is High Risk? Presenter Disclosure Information
 9:45 1:45 am Perioperative Evaluation and Management of the Cardiac Patient in Noncardiac Surgery SPEAKER Joshua A. Beckman, MD, MS Presenter Disclosure Information The following relationships exist related
9:45 1:45 am Perioperative Evaluation and Management of the Cardiac Patient in Noncardiac Surgery SPEAKER Joshua A. Beckman, MD, MS Presenter Disclosure Information The following relationships exist related
Pre-op Risk Assessment. Hal Blanks MD FACC
 Pre-op Risk Assessment Hal Blanks MD FACC Objectives: Identify and manage patients with known or suspected CAD and other cardiac diseases who are at risk of cardiac complications during noncardiac surgery.
Pre-op Risk Assessment Hal Blanks MD FACC Objectives: Identify and manage patients with known or suspected CAD and other cardiac diseases who are at risk of cardiac complications during noncardiac surgery.
Controversies in Perioperative Medicine
 Controversies in Perioperative Medicine Staying Abreast & Ahead of the Guidelines Hugo Quinny Cheng, MD Division of Hospital Medicine University of California, San Francisco Controversies in Perioperative
Controversies in Perioperative Medicine Staying Abreast & Ahead of the Guidelines Hugo Quinny Cheng, MD Division of Hospital Medicine University of California, San Francisco Controversies in Perioperative
Preoperative Evaluation Guidelines and Work up
 Preoperative Evaluation Guidelines and Work up Wesley Fiser, MD Disclosures: None 1 Case An 80 year old woman with osteoarthritis of the hip, DM, CKD (Cr 2.1), and HTN is diagnosed with an obstructing
Preoperative Evaluation Guidelines and Work up Wesley Fiser, MD Disclosures: None 1 Case An 80 year old woman with osteoarthritis of the hip, DM, CKD (Cr 2.1), and HTN is diagnosed with an obstructing
Conflicts of Interest. Evaluation of Cardiac and Pulmonary Risk in the Preop Patient. Introduction. Risk Assessment. Risk Assessment: RCRI
 Evaluation of Cardiac and Pulmonary Risk in the Preop Patient Conflicts of Interest I have no conflicts of interest to declare Adam Schaffer, MD Brigham and Women s Hospital July 20, 2012 Introduction
Evaluation of Cardiac and Pulmonary Risk in the Preop Patient Conflicts of Interest I have no conflicts of interest to declare Adam Schaffer, MD Brigham and Women s Hospital July 20, 2012 Introduction
Objectives. Old School. Preoperative Evaluation and Postoperative Complications: Where are the opportunities for risk reduction?
 Preoperative Evaluation and Postoperative Complications: Where are the opportunities for risk reduction? Jeffrey Carter, MD RMHMS October 5, 2010 Objectives Understand the preoperative cardiac evaluation
Preoperative Evaluation and Postoperative Complications: Where are the opportunities for risk reduction? Jeffrey Carter, MD RMHMS October 5, 2010 Objectives Understand the preoperative cardiac evaluation
2010, Metzler Helfried
 Perioperative Strategies in Patients on Dual Antiplatelet Drug Therapy: Noncardiac Surgery H. Metzler Department of Anaesthesiology and Intensive Care Medicine Medical University of Graz, Austria What
Perioperative Strategies in Patients on Dual Antiplatelet Drug Therapy: Noncardiac Surgery H. Metzler Department of Anaesthesiology and Intensive Care Medicine Medical University of Graz, Austria What
Pre-Operative Services Teaching Rounds 3 Jan 2011
 Pre-Operative Services Teaching Rounds 3 Jan 2011 Deborah Richman MBChB FFA(SA) Director Pre-Operative Services Department of Anesthesia Stony Brook University Medical Center, NY drichman@notes.cc.sunysb.edu
Pre-Operative Services Teaching Rounds 3 Jan 2011 Deborah Richman MBChB FFA(SA) Director Pre-Operative Services Department of Anesthesia Stony Brook University Medical Center, NY drichman@notes.cc.sunysb.edu
Agenda. Disclosures. Surgical Mortality: What is High Risk?
 Pre-Operative Cardiac Evaluation of the Vascular Patient: Updated AHA/ACC Guidelines Choosing Wisely UCSF Vascular Symposium 2015 Joshua A. Beckman, M.D., M.S. Brigham and Women s Hospital Consulting Merck
Pre-Operative Cardiac Evaluation of the Vascular Patient: Updated AHA/ACC Guidelines Choosing Wisely UCSF Vascular Symposium 2015 Joshua A. Beckman, M.D., M.S. Brigham and Women s Hospital Consulting Merck
PERIOPERATIVE EVALUATION AND ANESTHETIC MANAGEMENT OF PATIENTS WITH CARDIAC DISEASE FOR NON CARDIAC SURGERY
 PERIOPERATIVE EVALUATION AND ANESTHETIC MANAGEMENT OF PATIENTS WITH CARDIAC DISEASE FOR NON CARDIAC SURGERY WHICH PATIENT IS AT HIGHEST RISK? 1. 70 yo asymptomatic patient with history of heart failure
PERIOPERATIVE EVALUATION AND ANESTHETIC MANAGEMENT OF PATIENTS WITH CARDIAC DISEASE FOR NON CARDIAC SURGERY WHICH PATIENT IS AT HIGHEST RISK? 1. 70 yo asymptomatic patient with history of heart failure
Clinical Controversies in Perioperative Medicine!
 Clinical Controversies in Perioperative Medicine! Hugo Quinny Cheng, MD! Division of Hospital Medicine! University of California, San Francisco! Disclosures! Perioperative beta-blockade & statin therapy
Clinical Controversies in Perioperative Medicine! Hugo Quinny Cheng, MD! Division of Hospital Medicine! University of California, San Francisco! Disclosures! Perioperative beta-blockade & statin therapy
PERIOPERATIVE MYOCARDIAL INFARCTION THE ANAESTHESIOLOGIST'S VIEW
 PERIOPERATIVE MYOCARDIAL INFARCTION THE ANAESTHESIOLOGIST'S VIEW Bruce Biccard Perioperative Research Group, Department of Anaesthetics 18 June 2015 Disclosure Research funding received Medical Research
PERIOPERATIVE MYOCARDIAL INFARCTION THE ANAESTHESIOLOGIST'S VIEW Bruce Biccard Perioperative Research Group, Department of Anaesthetics 18 June 2015 Disclosure Research funding received Medical Research
Beta Blockade: Protection or Panacea
 Beta Blockade: Protection or Panacea Jason Axt Jason s Recommendations Perioperative β Blockade (BB) If on BB stay on If Vascular Sx + documented ischemia - start. 2+ risk factors - start Use in isolated
Beta Blockade: Protection or Panacea Jason Axt Jason s Recommendations Perioperative β Blockade (BB) If on BB stay on If Vascular Sx + documented ischemia - start. 2+ risk factors - start Use in isolated
Perioperative Medicine 2016 Some Answers, Even More Questions
 Learning Objectives Perioperative Medicine 2016 Some Answers, Even More Questions Kurt Pfeifer, MD, FACP, FHM Professor of Medicine Medical College of Wisconsin Outline changes to the ACC/AHA perioperative
Learning Objectives Perioperative Medicine 2016 Some Answers, Even More Questions Kurt Pfeifer, MD, FACP, FHM Professor of Medicine Medical College of Wisconsin Outline changes to the ACC/AHA perioperative
David A. Orsinelli, MD, FACC, FASE Professor, Internal Medicine The Ohio State University Division of Cardiovascular Medicine Columbus, Ohio
 1 STABLE ISCHEMIC HEART DISEASE: A NON-INVASIVE CARDIOLOGIST S PERSECTIVE 2018 Cardiovascular Course for Trainees and Early Career Physicians APRIL 20, 2018 David A. Orsinelli, MD, FACC, FASE Professor,
1 STABLE ISCHEMIC HEART DISEASE: A NON-INVASIVE CARDIOLOGIST S PERSECTIVE 2018 Cardiovascular Course for Trainees and Early Career Physicians APRIL 20, 2018 David A. Orsinelli, MD, FACC, FASE Professor,
Perioperative Medicine 2017 November 3, Disclosures
 Perioperative Medicine 2017 November 3, 2017 Scott Marsal, MD MSc FACP Chief, Medicine Division Medical Director, Quality & Patient Safety Providence St. Vincent Medical Center Disclosures No conflicts
Perioperative Medicine 2017 November 3, 2017 Scott Marsal, MD MSc FACP Chief, Medicine Division Medical Director, Quality & Patient Safety Providence St. Vincent Medical Center Disclosures No conflicts
Coronary Artery Disease: Revascularization (Teacher s Guide)
") Stephanie Chan, M.D. Updated 3/15/13 2008-2013, SCVMC (40 minutes) I. Objectives Coronary Artery Disease: Revascularization (Teacher s Guide) To review the evidence on whether percutaneous coronary intervention
Stephanie Chan, M.D. Updated 3/15/13 2008-2013, SCVMC (40 minutes) I. Objectives Coronary Artery Disease: Revascularization (Teacher s Guide) To review the evidence on whether percutaneous coronary intervention
Indications of Coronary Angiography Dr. Shaheer K. George, M.D Faculty of Medicine, Mansoura University 2014
 Indications of Coronary Angiography Dr. Shaheer K. George, M.D Faculty of Medicine, Mansoura University 2014 Indications for cardiac catheterization Before a decision to perform an invasive procedure such
Indications of Coronary Angiography Dr. Shaheer K. George, M.D Faculty of Medicine, Mansoura University 2014 Indications for cardiac catheterization Before a decision to perform an invasive procedure such
John B. Hill D.O. Department of Anesthesiology NORMAN ANESTHESIA PROVIDERS 03/05/2013
 Pre-op Assessment by Primary Providers What we really want to know John B. Hill D.O. Department of Anesthesiology NORMAN ANESTHESIA PROVIDERS 03/05/2013 Outline Discuss anesthesia specific risk Discuss
Pre-op Assessment by Primary Providers What we really want to know John B. Hill D.O. Department of Anesthesiology NORMAN ANESTHESIA PROVIDERS 03/05/2013 Outline Discuss anesthesia specific risk Discuss
by Brian Wolfe, MD Assistant Professor of Medicine, University of Colorado Denver
 Perioperative Cases by Brian Wolfe, MD Assistant Professor of Medicine, University of Colorado Denver 75 yo for left knee arthroplasty Problem List Social Hx: obesity uses a walker diabetes because of
Perioperative Cases by Brian Wolfe, MD Assistant Professor of Medicine, University of Colorado Denver 75 yo for left knee arthroplasty Problem List Social Hx: obesity uses a walker diabetes because of
Learning Objectives. Epidemiology of Acute Coronary Syndrome
 Cardiovascular Update: Antiplatelet therapy in acute coronary syndromes PHILLIP WEEKS, PHARM.D., BCPS-AQ CARDIOLOGY Learning Objectives Interpret guidelines as they relate to constructing an antiplatelet
Cardiovascular Update: Antiplatelet therapy in acute coronary syndromes PHILLIP WEEKS, PHARM.D., BCPS-AQ CARDIOLOGY Learning Objectives Interpret guidelines as they relate to constructing an antiplatelet
Anesthesia for Cardiac Patients for Non Cardiac Surgery. Kimberly Westra DNP, MSN, CRNA
 Anesthesia for Cardiac Patients for Non Cardiac Surgery Kimberly Westra DNP, MSN, CRNA Anesthesia for Cardiac Patients for Non Cardiac Surgery Heart Disease is a significant problem in the United States:
Anesthesia for Cardiac Patients for Non Cardiac Surgery Kimberly Westra DNP, MSN, CRNA Anesthesia for Cardiac Patients for Non Cardiac Surgery Heart Disease is a significant problem in the United States:
Optimal testing for coronary artery disease in symptomatic and asymptomatic patients
 Optimal testing for coronary artery disease in symptomatic and asymptomatic patients Alexandre C Ferreira, MD Clinical Chief of Cardiology Jackson Health System Director, Interventional Cardiology Training
Optimal testing for coronary artery disease in symptomatic and asymptomatic patients Alexandre C Ferreira, MD Clinical Chief of Cardiology Jackson Health System Director, Interventional Cardiology Training
Chest Pain: To Cath or Not? Part I
 Chest Pain: To Cath or Not? Part I Georgios Papaioannou, MD Ioannis Karavas, MD Newton-Wellesley Hospital 5/3/2000 1 A Typical Scenario... 57 year old female, Mrs. X., presents to your office with a 2
Chest Pain: To Cath or Not? Part I Georgios Papaioannou, MD Ioannis Karavas, MD Newton-Wellesley Hospital 5/3/2000 1 A Typical Scenario... 57 year old female, Mrs. X., presents to your office with a 2
An algorithmic approach to the very high risk surgical patient
 An algorithmic approach to the very high risk surgical patient Daniel A. Reuter Center of Anesthesiology and Intensive Care Medicine Hamburg-Eppendorf Universiy Medical Center Disclosures: Member of the
An algorithmic approach to the very high risk surgical patient Daniel A. Reuter Center of Anesthesiology and Intensive Care Medicine Hamburg-Eppendorf Universiy Medical Center Disclosures: Member of the
Preoperative Management. Presley Regional Trauma Center Department of Surgery University of Tennessee Health Science Center Memphis, Tennessee
 Preoperative Management Presley Regional Trauma Center Department of Surgery University of Tennessee Health Science Center Memphis, Tennessee Perioperative Care Consideration Medical care provided to prepare
Preoperative Management Presley Regional Trauma Center Department of Surgery University of Tennessee Health Science Center Memphis, Tennessee Perioperative Care Consideration Medical care provided to prepare
Perioperative Infarcts: Epidemiology, predictors and post-op monitoring
 Friday Nov 3rd, 2017 1pm Perioperative Infarcts: Epidemiology, predictors and post-op monitoring Dr Carol Chong Geriatrician Northern Health, Epping, Victoria, Australia How I became interested in this
Friday Nov 3rd, 2017 1pm Perioperative Infarcts: Epidemiology, predictors and post-op monitoring Dr Carol Chong Geriatrician Northern Health, Epping, Victoria, Australia How I became interested in this
21st Annual Contemporary Therapeutic Issues in Cardiovascular Disease
 21st Annual Contemporary Therapeutic Issues in Cardiovascular Disease Noninvasive Evaluation of Coronary Artery Disease: Anatomical, Functional, Clinical May 5, 2018 Mark Hansen MD FRCPC Cardiologist,
21st Annual Contemporary Therapeutic Issues in Cardiovascular Disease Noninvasive Evaluation of Coronary Artery Disease: Anatomical, Functional, Clinical May 5, 2018 Mark Hansen MD FRCPC Cardiologist,
Perioperative Assessment in the Older Adult. Sondra Vazirani, MD, MPH
 Perioperative Assessment in the Older Adult Sondra Vazirani, MD, MPH The Preoperative Evaluation in the Older Adult Sondra Vazirani, MD, MPH, FACP* 33 rd UCLA Intensive Course in Geriatric Medicine & Pharmacy,
Perioperative Assessment in the Older Adult Sondra Vazirani, MD, MPH The Preoperative Evaluation in the Older Adult Sondra Vazirani, MD, MPH, FACP* 33 rd UCLA Intensive Course in Geriatric Medicine & Pharmacy,
CCS Perioperative Guidelines When to order a BNP and What to do with a Positive Troponin
 Canadian Society of Internal Medicine Annual Meeting 2017 Toronto, ON CCS Perioperative Guidelines When to order a BNP and What to do with a Positive Troponin Dr. Vikas Tandon Associate Professor, Cardiology
Canadian Society of Internal Medicine Annual Meeting 2017 Toronto, ON CCS Perioperative Guidelines When to order a BNP and What to do with a Positive Troponin Dr. Vikas Tandon Associate Professor, Cardiology
Perioperative Management After Coronary Stenting: Risk Assessment Before Surgery. Christian Seiler No conflict of interest to declare.
 Perioperative Management After Coronary Stenting: Risk Assessment Before Surgery Christian Seiler No conflict of interest to declare PCI Long-Term Outcome Perioperative Management After Coronary Stenting:
Perioperative Management After Coronary Stenting: Risk Assessment Before Surgery Christian Seiler No conflict of interest to declare PCI Long-Term Outcome Perioperative Management After Coronary Stenting:
2018 David Stultz. The Consultant s Job
 The Consultant s Job Cardiac Pre-Operative Evaluation ACC 2014 Guidelines David Stultz, MD September 8, 2017 www.drstultz.com KPN Heart & Vascular Objectives of Conference Understand Cardiac Clearance
The Consultant s Job Cardiac Pre-Operative Evaluation ACC 2014 Guidelines David Stultz, MD September 8, 2017 www.drstultz.com KPN Heart & Vascular Objectives of Conference Understand Cardiac Clearance
Pre-operative Evaluations. Objectives. General Considerations. FP Consultation Considerations. CV Credits 7/24/2017. Brian Bachelder, MD Akron, Ohio
 Pre-operative Evaluations Brian Bachelder, MD Akron, Ohio Objectives Discuss the perioperative cardiopulmonary evaluation and management of patients undergoing non-cardiac surgery Objectively estimate
Pre-operative Evaluations Brian Bachelder, MD Akron, Ohio Objectives Discuss the perioperative cardiopulmonary evaluation and management of patients undergoing non-cardiac surgery Objectively estimate
A few years ago my team was consulted to clear a patient for surgery. I said OK, let s get a pre-op consult note on the chart.
 November 2016 A few years ago my team was consulted to clear a patient for surgery. I said OK, let s get a pre-op consult note on the chart. He consulted Cardiology. No attempt should be made to prognosticate
November 2016 A few years ago my team was consulted to clear a patient for surgery. I said OK, let s get a pre-op consult note on the chart. He consulted Cardiology. No attempt should be made to prognosticate
4/27/2015. Cardiac Events #1 cause of postoperative complications/ mortality- CHF, complete heart block, MI,
 Not intended for medical clearance Identify, document, and evaluate health conditions Medication Management Stratify Risks Optimize conditions within context of surgical illness Recommend measures that
Not intended for medical clearance Identify, document, and evaluate health conditions Medication Management Stratify Risks Optimize conditions within context of surgical illness Recommend measures that
VCU Pauley Heart Center: A 2009 US News Top 50 Heart and Heart Surgery Hospital
 VCU Pauley Heart Center: A 2009 US News Top 50 Heart and Heart Surgery Hospital Complex PCI: Multivessel Disease George W. Vetrovec, MD. Kimmerling Chair of Cardiology VCU Pauley Heart Center Virginia
VCU Pauley Heart Center: A 2009 US News Top 50 Heart and Heart Surgery Hospital Complex PCI: Multivessel Disease George W. Vetrovec, MD. Kimmerling Chair of Cardiology VCU Pauley Heart Center Virginia
Imaging ischemic heart disease: role of SPECT and PET. Focus on Patients with Known CAD
 Imaging ischemic heart disease: role of SPECT and PET. Focus on Patients with Known CAD Hein J. Verberne Academic Medical Center, University of Amsterdam, Amsterdam, Netherlands International Conference
Imaging ischemic heart disease: role of SPECT and PET. Focus on Patients with Known CAD Hein J. Verberne Academic Medical Center, University of Amsterdam, Amsterdam, Netherlands International Conference
I have no disclosures
 Preparing patients for out of hospital anesthesia BobbieJean Sweitzer, M.D. Director, Anesthesia Perioperative Medicine Clinic Professor of Anesthesia and Critical Care Professor of Medicine University
Preparing patients for out of hospital anesthesia BobbieJean Sweitzer, M.D. Director, Anesthesia Perioperative Medicine Clinic Professor of Anesthesia and Critical Care Professor of Medicine University
Update in Perioperative Medicine
 Update in Perioperative Medicine Linda Venner MD FACP March 2018 Agenda 1 2 3 4 5 Optimized not Cleared Identify red flags for cardiac and pulmonary complications Optimize management Prevent delirium Don
Update in Perioperative Medicine Linda Venner MD FACP March 2018 Agenda 1 2 3 4 5 Optimized not Cleared Identify red flags for cardiac and pulmonary complications Optimize management Prevent delirium Don
Evaluating the Heart before Non-Cardiac Surgery
 Evaluating the Heart before Non-Cardiac Surgery Dr Rob Stephens Anaesthetist UCLH + UCL the centre for Anaesthesia www.ucl.ac.uk/anaesthesia/people/stephens Google UCL Stephens www.ucl.ac.uk/anaesthesia/people/stephens
Evaluating the Heart before Non-Cardiac Surgery Dr Rob Stephens Anaesthetist UCLH + UCL the centre for Anaesthesia www.ucl.ac.uk/anaesthesia/people/stephens Google UCL Stephens www.ucl.ac.uk/anaesthesia/people/stephens
Perioperative Cardiovascular Evaluation and Care for Noncardiac Surgery
 Perioperative Cardiovascular Evaluation and Care for Noncardiac Surgery 2008 Update Plus Overview of the Guidelines Concept John Coyle, M.D. October 16, 2008 The History of Medicine As Mountaineering Feat
Perioperative Cardiovascular Evaluation and Care for Noncardiac Surgery 2008 Update Plus Overview of the Guidelines Concept John Coyle, M.D. October 16, 2008 The History of Medicine As Mountaineering Feat
Screening for Asymptomatic Coronary Artery Disease: When, How, and Why?
 Screening for Asymptomatic Coronary Artery Disease: When, How, and Why? Joseph S. Terlato, MD FACC Clinical Assistant Professor, Brown Medical School Coastal Medical Definition The presence of objective
Screening for Asymptomatic Coronary Artery Disease: When, How, and Why? Joseph S. Terlato, MD FACC Clinical Assistant Professor, Brown Medical School Coastal Medical Definition The presence of objective
Post Operative Troponin Leak: David Smyth Christchurch New Zealand
 Post Operative Troponin Leak: Does It Really Matter? David Smyth Christchurch New Zealand Life Was Simple Once Transmural Infarction Subendocardial Infarction But the Blood Tests Were n t Perfect Creatine
Post Operative Troponin Leak: Does It Really Matter? David Smyth Christchurch New Zealand Life Was Simple Once Transmural Infarction Subendocardial Infarction But the Blood Tests Were n t Perfect Creatine
Belinda Green, Cardiologist, SDHB, 2016
 Acute Coronary syndromes All STEMI ALL Non STEMI Unstable angina Belinda Green, Cardiologist, SDHB, 2016 Thrombus in proximal LAD Underlying pathophysiology Be very afraid for your patient Wellens
Acute Coronary syndromes All STEMI ALL Non STEMI Unstable angina Belinda Green, Cardiologist, SDHB, 2016 Thrombus in proximal LAD Underlying pathophysiology Be very afraid for your patient Wellens
Non ST Elevation-ACS. Michael W. Cammarata, MD
 Non ST Elevation-ACS Michael W. Cammarata, MD Case Presentation 65 year old man PMH: CAD s/p stent in 2008 HTN HLD Presents with chest pressure, substernally and radiating to the left arm and jaw, similar
Non ST Elevation-ACS Michael W. Cammarata, MD Case Presentation 65 year old man PMH: CAD s/p stent in 2008 HTN HLD Presents with chest pressure, substernally and radiating to the left arm and jaw, similar
An update on the management of UA / NSTEMI. Michael H. Crawford, MD
 An update on the management of UA / NSTEMI Michael H. Crawford, MD New ACC/AHA Guidelines 2007 What s s new in the last 5 years CT imaging advances Ascendancy of troponin and BNP Clarification of ACEI/ARB
An update on the management of UA / NSTEMI Michael H. Crawford, MD New ACC/AHA Guidelines 2007 What s s new in the last 5 years CT imaging advances Ascendancy of troponin and BNP Clarification of ACEI/ARB
Cardiovascular nuclear imaging employs non-invasive techniques to assess alterations in coronary artery flow, and ventricular function.
 National Imaging Associates, Inc. Clinical guidelines CARDIOVASCULAR NUCLEAR MEDICINE -MYOCARDIAL PERFUSION IMAGING -MUGA Original Date: October 2015 Page 1 of 9 FOR CMS (MEDICARE) MEMBERS ONLY CPT4 Codes:
National Imaging Associates, Inc. Clinical guidelines CARDIOVASCULAR NUCLEAR MEDICINE -MYOCARDIAL PERFUSION IMAGING -MUGA Original Date: October 2015 Page 1 of 9 FOR CMS (MEDICARE) MEMBERS ONLY CPT4 Codes:
MPS and Calcium Score in asymptomatic patient F. Mut, J. Vitola
 MPS and Calcium Score in asymptomatic patient F. Mut, J. Vitola Nuclear Medicine Service, Asociacion Española Montevideo, Uruguay Quanta Diagnostico Nuclear Curitiba, Brazil Clinical history Male 63 y.o.,
MPS and Calcium Score in asymptomatic patient F. Mut, J. Vitola Nuclear Medicine Service, Asociacion Española Montevideo, Uruguay Quanta Diagnostico Nuclear Curitiba, Brazil Clinical history Male 63 y.o.,
Asif Serajian DO FACC FSCAI
 Anticoagulation and Antiplatelet update: A case based approach Asif Serajian DO FACC FSCAI No disclosures relevant to this talk Objectives 1. Discuss the indication for antiplatelet therapy for cardiac
Anticoagulation and Antiplatelet update: A case based approach Asif Serajian DO FACC FSCAI No disclosures relevant to this talk Objectives 1. Discuss the indication for antiplatelet therapy for cardiac
Stable Angina: Indication for revascularization and best medical therapy
 Stable Angina: Indication for revascularization and best medical therapy Cardiology Basics and Updated Guideline 2018 Chang-Hwan Yoon, MD/PhD Cardiovascular Center, Department of Internal Medicine Bundang
Stable Angina: Indication for revascularization and best medical therapy Cardiology Basics and Updated Guideline 2018 Chang-Hwan Yoon, MD/PhD Cardiovascular Center, Department of Internal Medicine Bundang
Q: Do cardiac risk stratification indexes
 1-MINUTE CONSULT ROHAN MANDALIYA, MD, FACP Clinical Fellow, Division of Gastroenterology and Hepatology, Department of Medicine, Georgetown University Hospital, Washington, DC GENO MERLI, MD, MACP Professor
1-MINUTE CONSULT ROHAN MANDALIYA, MD, FACP Clinical Fellow, Division of Gastroenterology and Hepatology, Department of Medicine, Georgetown University Hospital, Washington, DC GENO MERLI, MD, MACP Professor
Preoperative Risk. Geoffrey C Zarrella DO FACC. Assessment
 Preoperative Risk Geoffrey C Zarrella DO FACC Assessment your late add ons keep calm use your tools stick to your guns PURPOSE OF THE PREOP EVAL ASSESS PERIOP RISK CAN INFORM DECISION TO PROCEED OR
Preoperative Risk Geoffrey C Zarrella DO FACC Assessment your late add ons keep calm use your tools stick to your guns PURPOSE OF THE PREOP EVAL ASSESS PERIOP RISK CAN INFORM DECISION TO PROCEED OR
5/2/2016. Outpatient Stroke Management Sheila Smith MD May 5, 2016
 Outpatient Stroke Management Sheila Smith MD May 5, 2016 1 Management of Outpatient Stroke Objectives Review blood pressure management post stroke Review antithrombotic therapy Review statin therapy Discuss
Outpatient Stroke Management Sheila Smith MD May 5, 2016 1 Management of Outpatient Stroke Objectives Review blood pressure management post stroke Review antithrombotic therapy Review statin therapy Discuss
Acute Coronary Syndrome. Sonny Achtchi, DO
 Acute Coronary Syndrome Sonny Achtchi, DO Objectives Understand evidence based and practice based treatments for stabilization and initial management of ACS Become familiar with ACS risk stratification
Acute Coronary Syndrome Sonny Achtchi, DO Objectives Understand evidence based and practice based treatments for stabilization and initial management of ACS Become familiar with ACS risk stratification
Evidence-Based Management of CAD: Last Decade Trials and Updated Guidelines
 Evidence-Based Management of CAD: Last Decade Trials and Updated Guidelines Enrico Ferrari, MD Cardiac Surgery Unit Cardiocentro Ticino Foundation Lugano, Switzerland Conflict of Interests No conflict
Evidence-Based Management of CAD: Last Decade Trials and Updated Guidelines Enrico Ferrari, MD Cardiac Surgery Unit Cardiocentro Ticino Foundation Lugano, Switzerland Conflict of Interests No conflict
Controversies in Cardiac Pharmacology
 Controversies in Cardiac Pharmacology Thomas D. Conley, MD FACC FSCAI Disclosures I have no relevant relationships with commercial interests to disclose. 1 Doc, do I really need to take all these medicines?
Controversies in Cardiac Pharmacology Thomas D. Conley, MD FACC FSCAI Disclosures I have no relevant relationships with commercial interests to disclose. 1 Doc, do I really need to take all these medicines?
Updates & Controversies in Perioperative Medicine
 Updates in Perioperative Medicine Updates & Controversies in Perioperative Medicine Hugo Quinny Cheng, MD Division of Hospital Medicine University of California, San Francisco New Guidelines for Perioperative
Updates in Perioperative Medicine Updates & Controversies in Perioperative Medicine Hugo Quinny Cheng, MD Division of Hospital Medicine University of California, San Francisco New Guidelines for Perioperative
PACT module High risk surgical patient. Intensive Care Training Program Radboud University Medical Centre Nijmegen
 PACT module High risk surgical patient Intensive Care Training Program Radboud University Medical Centre Nijmegen Intravascular volume effect of Ringer s lactate Double-tracer BV measurement Blood 1097
PACT module High risk surgical patient Intensive Care Training Program Radboud University Medical Centre Nijmegen Intravascular volume effect of Ringer s lactate Double-tracer BV measurement Blood 1097
FFR in Multivessel Disease
 FFR in Multivessel Disease April, 26 2013 Coronary Physiology in the Catheterization Laboratory Location: European Heart House, Nice, France Pim A.L. Tonino, MD, PhD Hartcentrum, Eindhoven, the Netherlands
FFR in Multivessel Disease April, 26 2013 Coronary Physiology in the Catheterization Laboratory Location: European Heart House, Nice, France Pim A.L. Tonino, MD, PhD Hartcentrum, Eindhoven, the Netherlands
Disclosures. Inpatient Management of Non-ST Elevation Acute Coronary Syndromes. Edward McNulty MD, FACC. None
 Inpatient Management of Non-ST Elevation Acute Coronary Syndromes Edward McNulty MD, FACC Assistant Clinical Professor UCSF Director, SF VAMC Cardiac Catheterization Laboratory Disclosures None New Guidelines
Inpatient Management of Non-ST Elevation Acute Coronary Syndromes Edward McNulty MD, FACC Assistant Clinical Professor UCSF Director, SF VAMC Cardiac Catheterization Laboratory Disclosures None New Guidelines
PCIs on Intermediate Lesions NCDR Cath-PCI Registry
 Practical Application Of Coronary Physiology in The Cath Lab Talal T Attar, MD, MBA, FACC PCIs on Intermediate Lesions NCDR Cath-PCI Registry Fraction of stenoses 50-70% treated with PCI without further
Practical Application Of Coronary Physiology in The Cath Lab Talal T Attar, MD, MBA, FACC PCIs on Intermediate Lesions NCDR Cath-PCI Registry Fraction of stenoses 50-70% treated with PCI without further
Cardiac Perioperative Risk Assessment American Heart Association Guidelines
 Cardiac Perioperative Risk Assessment American Heart Association Guidelines Dr Gary Liew, MBBS, PhD, FRACP US Board Certified in Cardiovascular CT Executive Committee, Cardiac Institute, Epworth Healthcare
Cardiac Perioperative Risk Assessment American Heart Association Guidelines Dr Gary Liew, MBBS, PhD, FRACP US Board Certified in Cardiovascular CT Executive Committee, Cardiac Institute, Epworth Healthcare
Updates & Controversies in Perioperative Medicine
 Updates & Controversies in Perioperative Medicine Hugo Quinny Cheng, MD Division of Hospital Medicine University of California, San Francisco Updates in Perioperative Medicine Estimating mortality in surgical
Updates & Controversies in Perioperative Medicine Hugo Quinny Cheng, MD Division of Hospital Medicine University of California, San Francisco Updates in Perioperative Medicine Estimating mortality in surgical
Patient characteristics Intervention Comparison Length of followup
 ISCHAEMIA TESTING CHAPTER TESTING FOR MYCOCARDIAL ISCHAEMIA VERSUS NOT TESTING FOR MYOCARDIAL ISCHAEMIA Ref ID: 4154 Reference Wienbergen H, Kai GA, Schiele R et al. Actual clinical practice exercise ing
ISCHAEMIA TESTING CHAPTER TESTING FOR MYCOCARDIAL ISCHAEMIA VERSUS NOT TESTING FOR MYOCARDIAL ISCHAEMIA Ref ID: 4154 Reference Wienbergen H, Kai GA, Schiele R et al. Actual clinical practice exercise ing
Canadian Antiplatelet Therapy Guidelines: 2014 Update James D. Douketis MD, FRCP(C)
") Canadian Antiplatelet Therapy Guidelines: 2014 Update James D. Douketis MD, FRCP(C) Department of Medicine, St. Joseph s Healthcare Hamilton and McMaster University, Hamilton, Canada Disclosures for: James
Canadian Antiplatelet Therapy Guidelines: 2014 Update James D. Douketis MD, FRCP(C) Department of Medicine, St. Joseph s Healthcare Hamilton and McMaster University, Hamilton, Canada Disclosures for: James
Διάρκεια διπλής αντιαιμοπεταλιακής αγωγής. Νικόλαος Γ.Πατσουράκος Καρδιολόγος, Επιμελητής Α ΕΣΥ Τζάνειο Γενικό Νοσοκομείο Πειραιά
 Διάρκεια διπλής αντιαιμοπεταλιακής αγωγής Νικόλαος Γ.Πατσουράκος Καρδιολόγος, Επιμελητής Α ΕΣΥ Τζάνειο Γενικό Νοσοκομείο Πειραιά International ACS guidelines: Recommendations on duration of dual
Διάρκεια διπλής αντιαιμοπεταλιακής αγωγής Νικόλαος Γ.Πατσουράκος Καρδιολόγος, Επιμελητής Α ΕΣΥ Τζάνειο Γενικό Νοσοκομείο Πειραιά International ACS guidelines: Recommendations on duration of dual
Surgery for patients with diffuse atherosclerotic disease
 Surgery for patients with diffuse atherosclerotic disease Special hospital for surgery Skopje Macedonia September, 2012 Mitrev Z, Anguseva T, E.Stoicovski, Hristov N, E.Idoski Oktomvri, 2008 Atherosclerosis
Surgery for patients with diffuse atherosclerotic disease Special hospital for surgery Skopje Macedonia September, 2012 Mitrev Z, Anguseva T, E.Stoicovski, Hristov N, E.Idoski Oktomvri, 2008 Atherosclerosis
ASA PLAVIX AND PREOPERATIVE OPTIMIZATION. John Hann, MD
 ASA PLAVIX AND PREOPERATIVE OPTIMIZATION John Hann, MD QUESTIONS: WHICH ANTI-PLATELETS DO YOU STOP AND WHEN? 1. 65 yo M with history of stroke on ASA PreOp eval for cataracts surgery 2. 65 yo M with RCRI
ASA PLAVIX AND PREOPERATIVE OPTIMIZATION John Hann, MD QUESTIONS: WHICH ANTI-PLATELETS DO YOU STOP AND WHEN? 1. 65 yo M with history of stroke on ASA PreOp eval for cataracts surgery 2. 65 yo M with RCRI
AMERICAN SOCIETY OF ANESTHESIOLOGISTS ANESTHESIA PRE OPERATIVE SCREENING ASA PHYSICAL STATUS CLASSIFICATION ANESTHESIOLOGISTS
 ANESTHESIA PRE OPERATIVE SCREENING CAPA S 37 TH ANNUAL CONFERENCE PALM SPRINGS OCTOBER 5, 2013 ROBERT F. KOPEL, MD, FACP, FCCP HOAG HOSPITAL ASSISTANT CLINICAL PROFESSOR UCLA SCHOOL OF MEDICINE AMERICAN
ANESTHESIA PRE OPERATIVE SCREENING CAPA S 37 TH ANNUAL CONFERENCE PALM SPRINGS OCTOBER 5, 2013 ROBERT F. KOPEL, MD, FACP, FCCP HOAG HOSPITAL ASSISTANT CLINICAL PROFESSOR UCLA SCHOOL OF MEDICINE AMERICAN
Management of Stable Ischemic Heart Disease. Vinay Madan MD February 10, 2018
 Management of Stable Ischemic Heart Disease Vinay Madan MD February 10, 2018 1 Disclosure No financial disclosure. 2 Overview of SIHD Diagnosis Outline of talk Functional vs. Anatomic assessment Management
Management of Stable Ischemic Heart Disease Vinay Madan MD February 10, 2018 1 Disclosure No financial disclosure. 2 Overview of SIHD Diagnosis Outline of talk Functional vs. Anatomic assessment Management
Quality Measures MIPS CV Specific
 Quality Measures MIPS CV Specific MEASURE NAME Atrial Fibrillation and Atrial Flutter: Chronic Anticoagulation Therapy CAHPS for MIPS Clinician/Group Survey Cardiac Rehabilitation Patient Referral from
Quality Measures MIPS CV Specific MEASURE NAME Atrial Fibrillation and Atrial Flutter: Chronic Anticoagulation Therapy CAHPS for MIPS Clinician/Group Survey Cardiac Rehabilitation Patient Referral from
Cardiovascular nuclear imaging employs non-invasive techniques to assess alterations in coronary artery flow, and ventricular function.
 National Imaging Associates, Inc. Clinical guidelines CARDIOVASCULAR NUCLEAR MEDICINE -MYOCARDIAL PERFUSION IMAGING -MUGA CPT4 Codes: Refer to pages 6-9 LCD ID Number: L33960 J 15 = KY, OH Responsible
National Imaging Associates, Inc. Clinical guidelines CARDIOVASCULAR NUCLEAR MEDICINE -MYOCARDIAL PERFUSION IMAGING -MUGA CPT4 Codes: Refer to pages 6-9 LCD ID Number: L33960 J 15 = KY, OH Responsible
PERIOPERATIVE ANESTHETIC RISK IN THE GERIATRIC PATIENT
 PERIOPERATIVE ANESTHETIC RISK IN THE GERIATRIC PATIENT Susan H. Noorily, M.D. Clinical Professor of Anesthesiology Medical Director University Preoperative Medicine Center IMPORTANCE Half of all currently
PERIOPERATIVE ANESTHETIC RISK IN THE GERIATRIC PATIENT Susan H. Noorily, M.D. Clinical Professor of Anesthesiology Medical Director University Preoperative Medicine Center IMPORTANCE Half of all currently
Risk Stratification for CAD for the Primary Care Provider
 Risk Stratification for CAD for the Primary Care Provider Shimoli Shah MD Assistant Professor of Medicine Directory, Ambulatory Cardiology Clinic Knight Cardiovascular Institute Oregon Health & Sciences
Risk Stratification for CAD for the Primary Care Provider Shimoli Shah MD Assistant Professor of Medicine Directory, Ambulatory Cardiology Clinic Knight Cardiovascular Institute Oregon Health & Sciences
CCS/CAIC/CSCS Position Statement on Revascularization Multi-vessel CAD. Teo et al, Canadian Journal of Cardiology 2014;30:
 CCS/CAIC/CSCS Position Statement on Revascularization Multi-vessel CAD Teo et al, Canadian Journal of Cardiology 2014;30: 1482-1491 Parallel Paper: Canadian Cardiovascular Society Guidelines for the Diagnosis
CCS/CAIC/CSCS Position Statement on Revascularization Multi-vessel CAD Teo et al, Canadian Journal of Cardiology 2014;30: 1482-1491 Parallel Paper: Canadian Cardiovascular Society Guidelines for the Diagnosis
Cardiac Risk Factors and Noninvasive Cardiac Diagnosis-ECG, ECHO, et al. Martin C. Burke, DO, FACOI ACOI IM Board Review Course 2018
 Cardiac Risk Factors and Noninvasive Cardiac Diagnosis-ECG, ECHO, et al. Martin C. Burke, DO, FACOI ACOI IM Board Review Course 2018 No Disclosures The American Heart Association Evidence-Based Scoring
Cardiac Risk Factors and Noninvasive Cardiac Diagnosis-ECG, ECHO, et al. Martin C. Burke, DO, FACOI ACOI IM Board Review Course 2018 No Disclosures The American Heart Association Evidence-Based Scoring
Coronary interventions
 Controversial issues in the management of ischemic heart failure Coronary interventions Maciej Lesiak Department of Cardiology, University Hospital in Poznan none DECLARATION OF CONFLICT OF INTEREST CHF
Controversial issues in the management of ischemic heart failure Coronary interventions Maciej Lesiak Department of Cardiology, University Hospital in Poznan none DECLARATION OF CONFLICT OF INTEREST CHF
Maria Angela S. Cruz-Anacleto, MD
 Maria Angela S. Cruz-Anacleto, MD 57/Female Menopausal Non-HTN, non-dm Hypothyroid (s/p RAI 1997) Levothyroxine 100 ug OD 5 Months PTA Chest discomfort Stress Echocardiography 5 Months PTA Chest discomfort
Maria Angela S. Cruz-Anacleto, MD 57/Female Menopausal Non-HTN, non-dm Hypothyroid (s/p RAI 1997) Levothyroxine 100 ug OD 5 Months PTA Chest discomfort Stress Echocardiography 5 Months PTA Chest discomfort
Choosing the Appropriate Stress Test: Brett C. Stoll, MD, FACC February 24, 2018
 Choosing the Appropriate Stress Test: Brett C. Stoll, MD, FACC February 24, 2018 Choosing the Appropriate Stress Test: Does it Really Matter? Brett C. Stoll, MD, FACC February 24, 2018 Conflicts of Interest
Choosing the Appropriate Stress Test: Brett C. Stoll, MD, FACC February 24, 2018 Choosing the Appropriate Stress Test: Does it Really Matter? Brett C. Stoll, MD, FACC February 24, 2018 Conflicts of Interest
Managing Cardiac & Pulmonary Risk in the Surgical Patient
 Managing Cardiac & Pulmonary Risk in the Surgical Patient Hugo Quinny Cheng, MD Division of Hospital Medicine University of California, San Francisco Preoperative Evaluation Guidelines Cardiac: Fleisher
Managing Cardiac & Pulmonary Risk in the Surgical Patient Hugo Quinny Cheng, MD Division of Hospital Medicine University of California, San Francisco Preoperative Evaluation Guidelines Cardiac: Fleisher
Coronary Artery Disease in the 21 st Century: An Integrated Approach Based on Science and Art
 Coronary Artery Disease in the 21 st Century: An Integrated Approach Based on Science and Art Harisios Boudoulas, MD, Dr, Dr. Hon. Professor, Honorary Professor, Academician Development of Coronary Artery
Coronary Artery Disease in the 21 st Century: An Integrated Approach Based on Science and Art Harisios Boudoulas, MD, Dr, Dr. Hon. Professor, Honorary Professor, Academician Development of Coronary Artery