Disclosure: Investigator in industry sponsored trials by Novartis
|
|
|
- Suzan Morgan
- 5 years ago
- Views:
Transcription
1 Disclosure: Investigator in industry sponsored trials by Novartis

2 Update in the Management of Chronic Heart Failure Family Medicine Grand Rounds November 14, 2017 Arunima Misra, MD Baylor College of Medicine Harris Health System
3 Demographics Diagnosis Treatment Referrals Review OBJECTIVES
4 HF prevalence has increased from 5 7 million (2009 to 2012) to 6 5 million (2011 to 2014) in Americans 20 years of age Five-year survival of HF diagnosis after an MI has also improved in 2001 to 2010 versus 1990 to 2000, from 54% to 61% Of incident hospitalized HF events, 53% had HF with reduced ejection fraction and 47% had preserved ejection fraction Black males had the highest proportion of hospitalized HF with reduced ejection fraction (70%); white females had the highest proportion of hospitalized HF with preserved ejection fraction (59%) Projections show prevalence will increase by 46% from 2012 to 2030 resulting in more than 8 million people 18 years of age and older with HF YOU WILL BE SEEING THESE PATIENTS! CURRENT FACTS ON HF
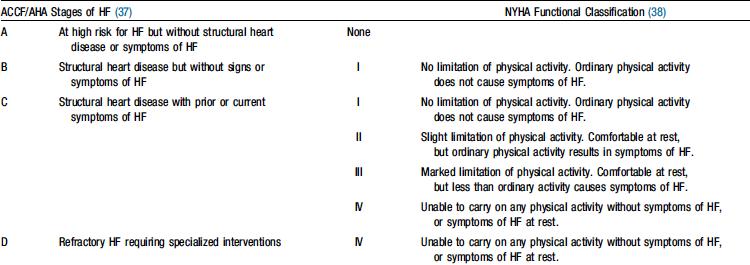
5 HF Classification
6 Approach to the Classification of New Approach to the Classification ofheart HeartFailure Failure Stage Patient Description A High risk for developing heart failure (HF) B Asymptomatic HF Previous MI LV systolic dysfunction Asymptomatic valvular disease C Symptomatic HF Known structural heart disease Shortness of breath and fatigue Reduced exercise tolerance D Refractory end-stage HF Marked symptoms at rest despite maximal medical therapy (eg, those who are recurrently hospitalized or cannot be safely discharged from the hospital without specialized interventions) Hypertension CAD Diabetes mellitus Family history of cardiomyopathy Carvedilol is indicated for use in patients with mild to severe chronic HF and in patients with HTN. Hunt SA et al. J Am Coll Cardiol. 2001;38:
7 Target treatment earlier to prevent HF Make patients aware of the importance of goals of therapy for HTN, DM Catch CAD earlier if pt has symptoms or has RF, treat RF such as HLD, HTN and DM more aggressively Screen for HF using BNP Stage A Hypertension and lipid disorders should be controlled in accordance with contemporary guidelines to lower the risk of HF Other conditions that may lead to or contribute to HF, such as obesity, diabetes mellitus, tobacco use, and known cardiotoxic agents, should be controlled or avoided. Provide or Reinforce Lifestyle Interventions: Diet,Exercise, Weight Loss, and Smoking Cessation!! WHY IS STAGE IMPORTANT
8 HYPERTENSION Nearly one fourth of the adult population of the U.S. has hypertension and (BP) lowering in patients with hypertension produces robust reductions in cardiovascular risk. The < 140/90 mm Hg BP target is reasonable in patients with hypertension and CAD. A lower target BP of < 130/80 mm Hg may be appropriate in some individuals with CAD or those with previous myocardial infarction (MI), stroke, or transient ischemic attack, or CAD risk equivalents (carotid artery disease, peripheral arterial disease, or abdominal aortic aneurysm). New goal in new guidelines. A BP goal of < 150/90 mm Hg is recommended in those who are > 80 years of age. Target of < 140/90 mm Hg for the 65- to 79-year age group. Decreases in diastolic BP < 60 mm Hg should be made with caution in any patient with diabetes mellitus or who is > 60 years of age. Goals of Therapy J Am Coll Cardiol. 2015;doi: /j.jacc
9 Beta-blockade in those patients with angina, prior MI, or heart failure with reduced ejection fraction. Angiotensin-converting enzyme inhibitor or angiotensin-receptor blocker if there is prior MI, left ventricular systolic dysfunction, diabetes mellitus, or chronic kidney disease. Thiazide or thiazide-like diuretic may be also added. Drugs to avoid in patients with hypertension and HF with reduced ejection fraction: non-dihydropyridine calcium channel blockers (such as verapamil or diltiazem), clonidine, and hydralazine without a nitrate. Avoid hypotension. HYPERTENSION What treatment to use
10 Diet modification HgbA1C <7% Avoid hypoglycemia DIABETES MELLITUS Contraindicated meds in HF: only if concomitant significant renal failure, then avoid metformin, sulfonylureas and flozins Empagliflozin shows Improved cardiovascular and total mortality, and decreased hospitalization for heart failure in high risk patients Goals for DM Treatment to Prevent CV Disease Circulation. 2016;133:

11 STAGE B Treatment of Stage B

12 STAGE C Noninvasive Imaging
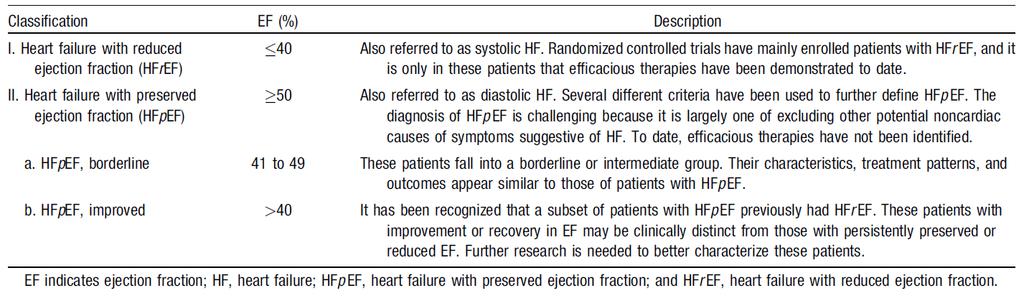
13 Classification Based on EF
14 Suspected Heart Failure because of SYMPTOMS and/or SIGNS Assess presence of CARDIAC DISEASE by ECG, CXR and BNP And VENTRICULAR FUNCTION Imaging by ECHO Doppler (preferred), Nuclear angiography or MRI if available Tests abnormal Heart Failure: (Reduced or Preserved) Identify etiology, evaluate severity, choose therapy ESC HF guidelines 2001, modified from AHA NORMAL No Heart Failure
15 Identify heart disease and RF for cardiac disease Assess functional capacity (NYHA Class, 6 min walk, or other) Assess volume status: (edema, rales, JVP, hepatomegaly, body weight) Lab assessment: routine: electrolytes, renal funct., BNP, repeat ECHO, RX only if significant changes in functional status Assess prognosis Initial and Ongoing Diagnosis
16 71 yo man with obesity, HTN, DM, paroxysmal afib, HIV presents with DOE. He denies CP, orthopnea, PND. Has some edema. No SOB at rest; only when he goes up stairs or lifts something heavy. Case 1
17 Vitals: HR 85 BP 119/75 mm Hg Cardiovascular: Irregular rhythm. S1 and S2, no S3 or S4. No murmur noted Respiratory: CTAB. GI: Soft, nontender, nondistended, bowel sounds present Extremities: +1-2 pitting edema BLE left more than right Physical Exam
18 Sodium 142 Potassium 4.0 Chloride 102 CO Urea Nitrogen 24 (H) Creatinine 1.43 (H) Glucose 156 (H) Hgb A1c 6.7 (H) TSH 2.02 BNP 327 (H) Labs
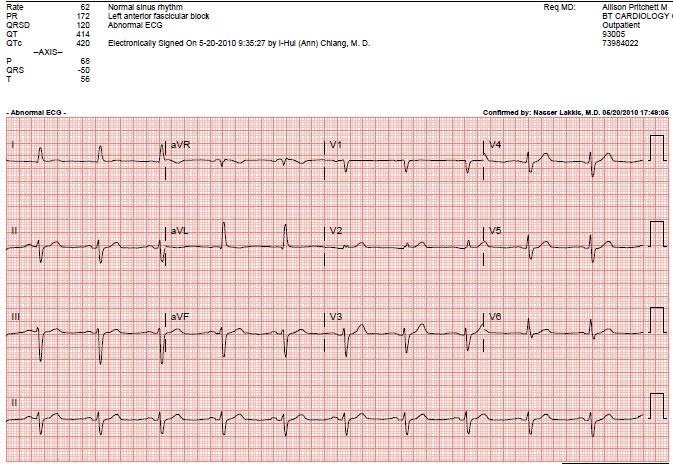
19 ECG

20 CXR
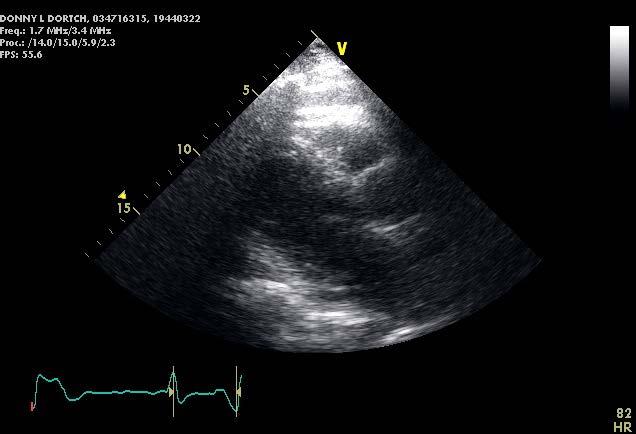
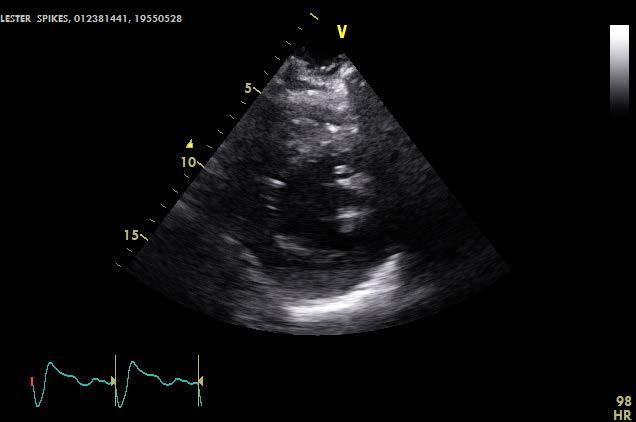
21 ECHO
 Management includes control of comorbid conditions such as hypertension, CAD, DM, CKD, etc.")
22 HFpEF Not well studied Prevalence and morbidity and mortality similar to HFrEF Therapies for HFrEF may prevent further decline in EF or clinical status No positive RCT to support use of any pharmacotherapy (neg trials including nitrates, phosphodiesterase inhibitors, spironolactone) Management includes control of comorbid conditions such as hypertension, CAD, DM, CKD, etc. HFpEF Review of standard of care
23 Evaluate for CAD and treat If atrial fibrillation, control rhythm or rate Use of BB or ACEI/ARB is reasonable for BP control In select patients with HFpEF (with EF 45%, elevated BNP levels or HF admission within 1 year, GFR>30 ml/min, creat <2.5 mg/dl, K <5.0 meq/l), aldosterone receptor antagonists might be considered to decrease hospitalizations. Use of ARBs might be considered to decrease hospitalizations for patients with HFpEF. Treatment of HFpEF
24 Did nuclear stress test that showed scar in RCA territory: he did not want cath (unclear if SOB is angina since improved with nitrates) Meds: Metoprolol succinate 25 mg daily Furosemide 80 mg daily Not on ACEI/ARB or spironolactone Isosorbide mononitrate 30 mg daily On Doxazosin (for BPH and not willing to change) DM meds HLD meds Potassium HIV meds Next step and meds
25 Case 2
26 58yo male w/ HTN now presents with 1 week history of worsening SOB and cough productive of clear and blood-tinged sputum associated with BLE edema. PMH: HTN FH: not reported History
27 BP 186/128 Pulse 104 Temp(Src) 98.4 F (36.9 C) Resp 30 SpO2 97% Cardiovascular: Regular rhythm, normal heart sounds and intact distal pulses. Tachycardia present. Exam reveals no gallop and no friction rub. No murmur heard. Pulmonary/Chest: Tachypnea noted. He is in respiratory distress. He has no wheezes. He has rales in the right lower field and the left lower field. He exhibits no tenderness. Abdominal: Soft. Bowel sounds are normal. He exhibits no distension. There is no tenderness. There is no rebound and no guarding. Musculoskeletal: Normal range of motion. He exhibits edema (1+ BLE). He exhibits no tenderness. Physical
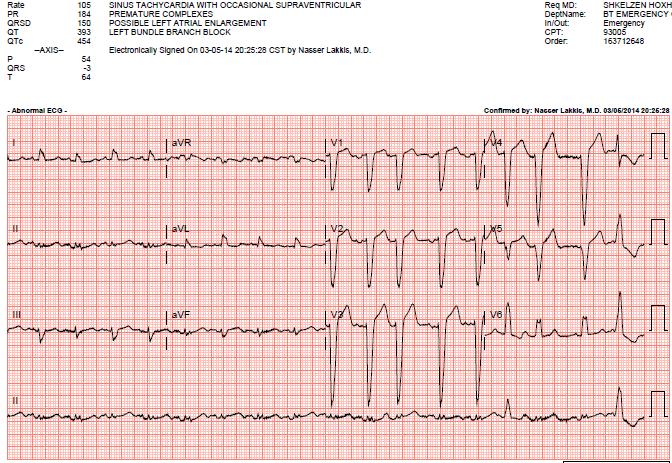
28 ECG
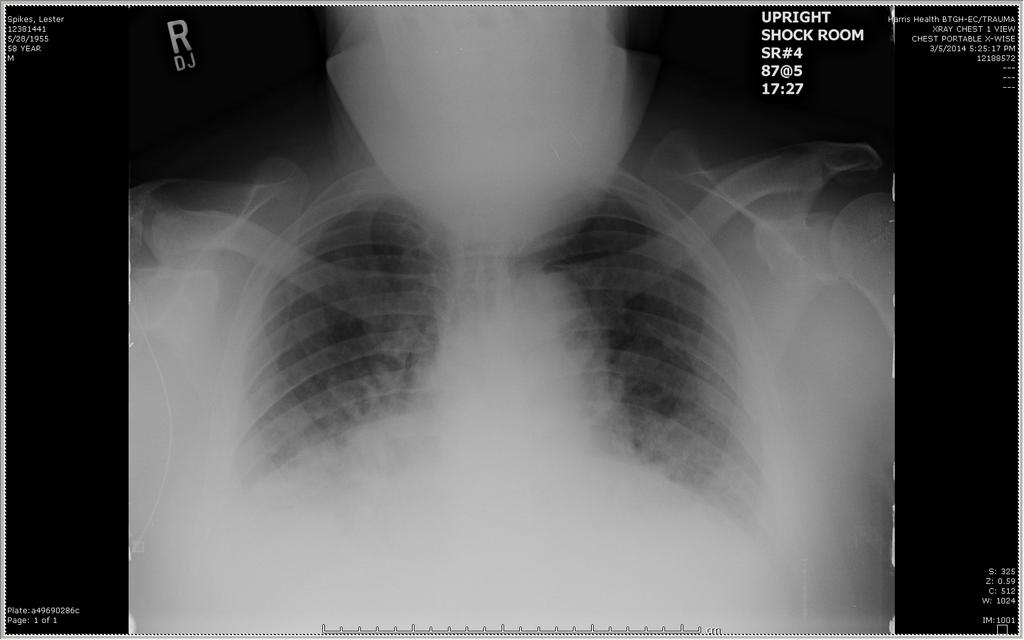
29 CXR
30 BNP 930 HgbA1C 6.1 % Cholesterol 179 Triglyceride 117 HDL 43 LDL 113 TSH 2.02 Sodium 145 Potassium 3.9 Chloride 106 CO2 31 Urea Nitrogen 24 (H) Creatinine 1.9 (H) Glucose 84 LABS
31 32-amino acid protein that is secreted by the ventricles in response to wall stress Levels >100 pg/ml are considered abnormal; usually >>150 in heart failure Systolic HF >>>> Diastolic HF in women compared to men May be in obesity Initially used in ER setting to improve identification of HF as cause of SOB (Breathing Not Properly study) Brain Natriuretic Peptide (BNP) Circulation 106: , 2002

32 How to Use BNP
33 Echo
34 Etiology is important: either need nuclear stress test, dobutamine stress echo or cardiac catheterization especially in patients who have risk factors for CAD Etiologies that are reversible include valvular disease, thyroid disease, some infiltrative diseases REFER to cardiologist sooner than later Further Testing
35 IMPRESSIONS No evidence of ischemia or infarction. Reduced left ventricular function with ejection fraction of 44%. Dilated LV. Nuclear
36 Eligible for revascularization are HF patients presenting with: angina or significant ischemia (Class I) Chest pain (Class IIa) Known or suspected CAD (Class IIa) Indications for Cardiac Catheterization and Revascularization
37 A At high risk for heart failure, but no structural heart disease B Evidence of structural heart disease, but asymptomatic C Structural heart disease with prior or current heart failure symptoms D Refractory heart failure requiring specialized interventions What Stage of HF is our patient
38 I: Experience symptoms at levels of exertion that would limit normal individuals II: III: IV: I get SOB walking from the elevator to the clinic Symptoms with ordinary exertion Symptoms with less than ordinary exertion Symptoms at rest NYHA Functional Class
39 Survival Morbidity Exercise capacity Quality of life Neurohormonal changes Progression of CHF Symptoms Treatment Objectives
40 For All HF Patients Control of risk factors Life style modification Treat etiologic cause / comorbid conditions Drug therapy Personal care Team work For Select Patients Revascularization for obstructive CAD ICD (Implantable Cardiac Defibrillator) Cardiac resynchronization Ventricular assist devices Heart transplant Artificial heart Neoangiogenesis, Gene therapy (experimental) Treatment
41 ACE inhibitors ARBs Beta blockers Diuretics Spironolactone Hydralazine/Nitrates Neprolysin/ARB (ARNIs) Ivabradine Digoxin? Pharmacologic Therapy




42 Renin Angiotensinogen Angiotensin I ACE enzyme Angiotensin II Aldosterone ACE INHIBITORS ARB SPIRONO BETA-BLOCKERS Vasoconstriction Catecholamines Sodium retention Cardiac fibrosis Neurohormonal Activation

43 NEP: neprilysin inhibitor VALSARTAN How neprilysin or sacubitril works along with valsartan June 2016Br J Cardiol 2016;23(suppl 1):S1

44 IVABRADINE Blocks the If current and lowers heart rate at the SA node level How Ivabradine works


45 Medication Initial Dose Goal Dose Enalapril 2.5 mg daily mg bid Lisinopril mg daily mg daily Captopril 6.25 mg tid Up to 50 mg tid Main side effects: cough, hyperkalemia and serious angioedema; not to use in pregnancy ACE Inhibitors

46 Medication Properties Initial Dose Goal Dose Carvedilol Metoprolol XL Bisoprolol β1 β mg Vasodilatory bid Antioxidant β mg daily 1.25 mg daily 25 mg bid 50 mg bid if >85 kg 200 mg daily 10 mg daily Main side effects: fatigue, bradycardia, sexual dysfunction Beta-Blockers
47 Indicated in patients who are intolerant of ACE inhibitors due to cough (or angioedema) Valsartan and Candesartan have been most studied in HF Patients who develop angioedema with ACE inhibitors may have a similar response to ARBs although uncommon Losartan mg 150 mg Valsartan 40 mg BID 160 mg BID Candesartan 4-8 mg 32 mg Angiotensin Receptor Blockers (ARBs)
 GFR 31-49 12.")
48 Sprinolactone: Side Effects: Hyperkalemia, Gynecomastia, Impotence, Oligomenorrhea (due to androgen / progesterone receptor binding) Eplerenone: EF <40%, CHF AFTER MI Side effects: Hyperkalemia Spironolactone GFR > mg 25 mg (50 mg) GFR mg QD OR QOD Eplerenone GFR > mg 50 mg (100 mg) GFR mg QOD Aldosterone Antagonists
49 May be used in patient who cannot take an ACE inhibitor or ARB such as hyperkalemia (Class IIb) A-Heft Trial: African-Americans with HF were randomized to conventional therapy + / - this combination (Class IIa) Isosorbide dinitrate plus hydralazine Without ACE-I/ARB Isosorbide dinitrate mg QID 40 mg QID Hydralazine mg QID 75 mg QID With ACE-I/ARB Isosorbide dinitrate mg 3 TID 40 mg TID Hydralazine mg 3 TID 75 mg TID Nitrates / Hydralazine A-Heft: NEJM 351: , 2004
50 Can use in patients who remain symptomatic on standard therapy of BB, ACEI/ARB and aldosterone antagonist Must use INSTEAD of ACEI or ARB not in addition to Contraindication in patients with angioedema Must wait 36hrs for ACEI to washout to avoid risk of angioedema ARNI 24mg/26mg bid 97mg/103mg bid Sacubitril/Valsartan
51 HF readmissions occur more commonly in patients with HR >70 Can use this SA nodal blocking agent in the setting of HR that is high even after tolerated BB dose has been optimized Has prospective data compared to digoxin with retrospective data Ivabradine 2.5 mg bid 7.5 mg bid Ivabradine

52 a Standardized to 12 months. b Benefit of ARNI therapy incremental to that achieved with ACEI therapy. For the other medications shown, the benefits are based on comparisons to placebo control. RISK REDUCTION OF THERAPIES JAMA Cardiol. 2016;1(6):

53 All ICDs have pacemaker capabilities Patients should carry device ID card and have device checked q 3 months Average device cost: $17-20,000 Defibrillators or ICDs
:")
54 3 lead devices: RA RV LV via coronary sinus Indications (Class IIa): NYHA III or IV Receiving optimal medical Rx Sinus rhythm QRS >120 msec Reasonable expectations to survive >1 year BiVentricular ICDs JACC 48(5):
55 Carvedilol 25 mg bid Losartan 25 mg daily Furosemide 120 mg bid Spironolactone 25 mg daily +/- Metolazone as needed Amiodarone 200 mg daily for PAF Rivaroxaban Optimization complicated by continued sx of fatigue and dizziness and multiple HF admissions Vitals: BP 115/80, HR 100Creat 1.9 ECG with sinus tachy with LBBB TTE f/u LVEF <20% What is the next step? Patient s Meds


56 HF REDUCED EF????? JACC Volume 70, Issue 6, August 2017
57 Lack contemporary data However, in 2013 Guidelines, remains Class IIa indication In pts with high HR and on tolerated optimal dose of BB, in particular with afib, digoxin can be used (narrow window of therapy and do not use in pts with CKD) Amiodarone is more effective in afib HR control To add Digoxin?
58 Indications for Warfarin in HF Atrial fibrillation Previous thrombotic events Intraventricular thrombi Indications for Aspirin in HF 2 Prevention of Atherothrombotic events Atrial fibrillation when warfarin or NOAC is contraindicated
59 <2000 mg sodium / day Culprit foods: Canned soup / vegetables Bacon / ham Pickles / BBQ sauces / Salad dressings Fast food Microwave meals / Spice packets in meal kits Spaghetti Sauce CAUTION: Some salt substitutes contain potassium! Low Salt Diet
60 HF-ACTION Multi-center, randomized trial of 3000 patients Exercise regimen: 30 min 3x / week to 40 min 5x / week No mortality or hospitalization After adjusting for other differences, exercise was associated with a 11% in death or hospitalization. Exercise appears safe Exercise and HF Am J of Med 116(10): , 2004

61 Treatment for Prevention of HF
62 Educate patient about salt diet and medication compliance Titrate ACE inhibitors and beta-blockers to target or maximally tolerated doses Remember to add aldosterone antagonist and/or hydralazine/nitrates to those who qualify Refer to cardiology those with continued symptoms for novel pharmacotherapy (not on formulary yet), frequent admissions, and for device assessment and potential further referral to advanced heart failure center Take Home Points for Treating HF
63 Thank You!!
Heart Failure Clinician Guide JANUARY 2016
 Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Heart Failure Clinician Guide JANUARY 2016 Introduction This evidence-based guideline summary is based on the 2016 National Heart Failure Guideline.
Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Heart Failure Clinician Guide JANUARY 2016 Introduction This evidence-based guideline summary is based on the 2016 National Heart Failure Guideline.
Heart Failure Clinician Guide JANUARY 2018
 Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Heart Failure Clinician Guide JANUARY 2018 Introduction This evidence-based guideline summary is based on the 2018 National Heart Failure Guideline.
Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Heart Failure Clinician Guide JANUARY 2018 Introduction This evidence-based guideline summary is based on the 2018 National Heart Failure Guideline.
Congestive Heart Failure: Outpatient Management
 The Chattanooga Heart Institute Cardiovascular Symposium Congestive Heart Failure: Outpatient Management E. Philip Lehman MD, MPP Disclosure No financial disclosures. Objectives Evidence-based therapy
The Chattanooga Heart Institute Cardiovascular Symposium Congestive Heart Failure: Outpatient Management E. Philip Lehman MD, MPP Disclosure No financial disclosures. Objectives Evidence-based therapy
1/4/18. Heart Failure Guideline Review and Update. Disclosure. Pharmacist Objectives. Pharmacy Technician Objectives. What is Heart Failure?
 Disclosure Heart Failure Guideline Review and Update I have had no financial relationship over the past 12 months with any commercial sponsor with a vested interest in this presentation. Natalie Beiter,
Disclosure Heart Failure Guideline Review and Update I have had no financial relationship over the past 12 months with any commercial sponsor with a vested interest in this presentation. Natalie Beiter,
Guideline-Directed Medical Therapy
 Guideline-Directed Medical Therapy Cardiovascular Outcomes Assessment of the MitraClip Percutaneous Therapy for Heart Failure Patients with Functional Mitral Regurgitation OPTIMAL THERAPY (As defined in
Guideline-Directed Medical Therapy Cardiovascular Outcomes Assessment of the MitraClip Percutaneous Therapy for Heart Failure Patients with Functional Mitral Regurgitation OPTIMAL THERAPY (As defined in
DISCLAIMER: ECHO Nevada emphasizes patient privacy and asks participants to not share ANY Protected Health Information during ECHO clinics.
 DISCLAIMER: Video will be taken at this clinic and potentially used in Project ECHO promotional materials. By attending this clinic, you consent to have your photo taken and allow Project ECHO to use this
DISCLAIMER: Video will be taken at this clinic and potentially used in Project ECHO promotional materials. By attending this clinic, you consent to have your photo taken and allow Project ECHO to use this
State-of-the-Art Management of Chronic Systolic Heart Failure
 State-of-the-Art Management of Chronic Systolic Heart Failure Michael McCulloch, MD 17 th Annual Cardiovascular Update Intermountain Medical Center December 16, 2017 Disclosures: I have no financial disclosures
State-of-the-Art Management of Chronic Systolic Heart Failure Michael McCulloch, MD 17 th Annual Cardiovascular Update Intermountain Medical Center December 16, 2017 Disclosures: I have no financial disclosures
Checklist for Treating Heart Failure. Alan M. Kaneshige MD, FACC, FASE Oklahoma Heart Institute
 Checklist for Treating Heart Failure Alan M. Kaneshige MD, FACC, FASE Oklahoma Heart Institute Novartis Disclosure Heart Failure (HF) a complex clinical syndrome that arises secondary to abnormalities
Checklist for Treating Heart Failure Alan M. Kaneshige MD, FACC, FASE Oklahoma Heart Institute Novartis Disclosure Heart Failure (HF) a complex clinical syndrome that arises secondary to abnormalities
HEART FAILURE: PHARMACOTHERAPY UPDATE
 HEART FAILURE: PHARMACOTHERAPY UPDATE 3 HEART FAILURE REVIEW 1 5.1 million x1.25 = 6.375 million 40 years old = MICHAEL F. AKERS, PHARM.D. CLINICAL PHARMACIST CENTRACARE HEALTH, ST. CLOUD HOSPITAL HF Diagnosis
HEART FAILURE: PHARMACOTHERAPY UPDATE 3 HEART FAILURE REVIEW 1 5.1 million x1.25 = 6.375 million 40 years old = MICHAEL F. AKERS, PHARM.D. CLINICAL PHARMACIST CENTRACARE HEALTH, ST. CLOUD HOSPITAL HF Diagnosis
Heart Failure. Dr. William Vosik. January, 2012
 Heart Failure Dr. William Vosik January, 2012 Questions for clinicians to ask Is this heart failure? What is the underlying cause? What are the associated disease processes? Which evidence-based treatment
Heart Failure Dr. William Vosik January, 2012 Questions for clinicians to ask Is this heart failure? What is the underlying cause? What are the associated disease processes? Which evidence-based treatment
The ACC Heart Failure Guidelines
 The ACC Heart Failure Guidelines Fakhr Alayoubi, Msc,R Ph President of SCCP Cardiology Clinical Pharmacist Assistant Professor At King Saud University King Khalid University Hospital Riyadh-KSA 2017 ACC/AHA/HFSA
The ACC Heart Failure Guidelines Fakhr Alayoubi, Msc,R Ph President of SCCP Cardiology Clinical Pharmacist Assistant Professor At King Saud University King Khalid University Hospital Riyadh-KSA 2017 ACC/AHA/HFSA
Definition of Congestive Heart Failure
 Heart Failure Definition of Congestive Heart Failure A clinical syndrome of signs & symptoms resulting from the heart s inability to supply adequate tissue perfusion. CHF Epidemiology Affects 4.7 million
Heart Failure Definition of Congestive Heart Failure A clinical syndrome of signs & symptoms resulting from the heart s inability to supply adequate tissue perfusion. CHF Epidemiology Affects 4.7 million
Difficult to Treat Hypertension
 Difficult to Treat Hypertension According to Goldilocks JNC 8 Blood Pressure Goals (2014) BP Goal 60 years old and greater*- systolic < 150 and diastolic < 90. (Grade A)** BP Goal 18-59 years old* diastolic
Difficult to Treat Hypertension According to Goldilocks JNC 8 Blood Pressure Goals (2014) BP Goal 60 years old and greater*- systolic < 150 and diastolic < 90. (Grade A)** BP Goal 18-59 years old* diastolic
Cardiovascular Clinical Practice Guideline Pilot Implementation
 Cardiovascular Clinical Practice Guideline Pilot Implementation Pharmacologic Management of Chronic Heart Failure Sept 15, 2004 Angela Allerman, PharmD, BCPS DoD Pharmacoeconomic Center Promoting high
Cardiovascular Clinical Practice Guideline Pilot Implementation Pharmacologic Management of Chronic Heart Failure Sept 15, 2004 Angela Allerman, PharmD, BCPS DoD Pharmacoeconomic Center Promoting high
Estimated 5.7 million Americans with HF. 915, 000 new HF cases annually, HF incidence approaches
 Heart Failure: Management of a Chronic Disease Jenny Bauerly RN, CHFN, APRN-BC Heart Failure (HF) Definition A complex clinical syndrome that can result from any structural or functional cardiac disorder
Heart Failure: Management of a Chronic Disease Jenny Bauerly RN, CHFN, APRN-BC Heart Failure (HF) Definition A complex clinical syndrome that can result from any structural or functional cardiac disorder
Nora Goldschlager, M.D. SFGH Division of Cardiology UCSF
 CLASSIFICATION OF HEART FAILURE Nora Goldschlager, M.D. SFGH Division of Cardiology UCSF DISCLOSURES: NONE CLASSIFICATION C OF HEART FAILURE NYHA I IV New paradigm Stage A: Pts at high risk of developing
CLASSIFICATION OF HEART FAILURE Nora Goldschlager, M.D. SFGH Division of Cardiology UCSF DISCLOSURES: NONE CLASSIFICATION C OF HEART FAILURE NYHA I IV New paradigm Stage A: Pts at high risk of developing
Heart Failure: Guideline-Directed Management and Therapy
 Heart Failure: Guideline-Directed Management and Therapy Guideline-Directed Management and Therapy (GDMT) was developed by the American College of Cardiology and American Heart Association to define the
Heart Failure: Guideline-Directed Management and Therapy Guideline-Directed Management and Therapy (GDMT) was developed by the American College of Cardiology and American Heart Association to define the
HEART FAILURE. Heart Failure in the US. Heart Failure (HF) 3/2/2014
 3/2/2014") HEART FAILURE Martina Frost, PA-C Desert Cardiology of Tucson Northwest Medical Center March 2014 Heart Failure in the US Prevalence - ~5 million 650,000 new cases annually 300,000 deaths annually Leading
HEART FAILURE Martina Frost, PA-C Desert Cardiology of Tucson Northwest Medical Center March 2014 Heart Failure in the US Prevalence - ~5 million 650,000 new cases annually 300,000 deaths annually Leading
Outline. Chronic Heart Failure: Update on Effective Monitoring and Treatment. Heart Failure Epidemiology. Michael G.
 Chronic Heart Failure: Update on Effective Monitoring and Treatment Michael G. Shlipak, MD, MPH Professor of Medicine, UCSF Chief, Division of General Internal Medicine, SFVA Medical Center Scientific
Chronic Heart Failure: Update on Effective Monitoring and Treatment Michael G. Shlipak, MD, MPH Professor of Medicine, UCSF Chief, Division of General Internal Medicine, SFVA Medical Center Scientific
Introduction to Heart Failure. Mauricio Velez, M.D. Transplant Cardiologist APACVS 2018 April 5-7 Miami, FL
 Introduction to Heart Failure Mauricio Velez, M.D. Transplant Cardiologist APACVS 2018 April 5-7 Miami, FL Disclosures No relevant financial relationships to disclose Objectives and Outline Define heart
Introduction to Heart Failure Mauricio Velez, M.D. Transplant Cardiologist APACVS 2018 April 5-7 Miami, FL Disclosures No relevant financial relationships to disclose Objectives and Outline Define heart
Management Strategies for Advanced Heart Failure
 Management Strategies for Advanced Heart Failure Mary Norine Walsh, MD, FACC Medical Director, HF and Cardiac Transplantation St Vincent Heart Indianapolis, IN USA President American College of Cardiology
Management Strategies for Advanced Heart Failure Mary Norine Walsh, MD, FACC Medical Director, HF and Cardiac Transplantation St Vincent Heart Indianapolis, IN USA President American College of Cardiology
Chronic. Congestive^ Heart Failure: Update on Effective Monitoring and Treatment. Michael G. Shlipak, MD, MPH
 Chronic Congestive^ Heart Failure: Update on Effective Monitoring and Treatment Michael G. Shlipak, MD, MPH Professor of Medicine, UCSF Chief, Division of General Internal Medicine, SFVA Medical Center
Chronic Congestive^ Heart Failure: Update on Effective Monitoring and Treatment Michael G. Shlipak, MD, MPH Professor of Medicine, UCSF Chief, Division of General Internal Medicine, SFVA Medical Center
ESC Guidelines for the Diagnosis and Treatment of Acute and Chronic Heart Failure
 Patients t with acute heart failure frequently develop chronic heart failure Patients with chronic heart failure frequently decompensate acutely ESC Guidelines for the Diagnosis and A clinical response
Patients t with acute heart failure frequently develop chronic heart failure Patients with chronic heart failure frequently decompensate acutely ESC Guidelines for the Diagnosis and A clinical response
Update in Congestive Hear Failure DRAGOS VESBIANU MD
 Update in Congestive Hear Failure DRAGOS VESBIANU MD Case 58 yo AAM c/o shortness of breath for 3 weeks. Used to walk one mile per day and now he has noticed that he gets short of breath after 2 blocks.
Update in Congestive Hear Failure DRAGOS VESBIANU MD Case 58 yo AAM c/o shortness of breath for 3 weeks. Used to walk one mile per day and now he has noticed that he gets short of breath after 2 blocks.
From PARADIGM-HF to Clinical Practice. Waleed AlHabeeb, MD, MHA Associate Professor of Medicine President of the Saudi Heart Failure Group
 From PARADIGM-HF to Clinical Practice Waleed AlHabeeb, MD, MHA Associate Professor of Medicine President of the Saudi Heart Failure Group PARADIGM-HF: Inclusion Criteria Chronic HF NYHA FC II IV with LVEF
From PARADIGM-HF to Clinical Practice Waleed AlHabeeb, MD, MHA Associate Professor of Medicine President of the Saudi Heart Failure Group PARADIGM-HF: Inclusion Criteria Chronic HF NYHA FC II IV with LVEF
Contemporary Management of Heart Failure. Keerthy K Narisetty, MD Comprehensive Heart Failure Management Program BHHI Primary Care Symposium
 Contemporary Management of Heart Failure Keerthy K Narisetty, MD Comprehensive Heart Failure Management Program BHHI Primary Care Symposium Disclosures I have no relevant relationships with commercial
Contemporary Management of Heart Failure Keerthy K Narisetty, MD Comprehensive Heart Failure Management Program BHHI Primary Care Symposium Disclosures I have no relevant relationships with commercial
Chronic. Outline. Congestive^ Heart Failure: Update on Effective Monitoring and Treatment. Heart Failure Epidemiology. Michael G.
 Chronic Congestive^ Heart Failure: Update on Effective Monitoring and Treatment Michael G. Shlipak, MD, MPH Professor of Medicine, UCSF Chief, Division of General Internal Medicine, SFVA Medical Center
Chronic Congestive^ Heart Failure: Update on Effective Monitoring and Treatment Michael G. Shlipak, MD, MPH Professor of Medicine, UCSF Chief, Division of General Internal Medicine, SFVA Medical Center
2016 Update to Heart Failure Clinical Practice Guidelines
 2016 Update to Heart Failure Clinical Practice Guidelines Mitchell T. Saltzberg, MD, FACC, FAHA, FHFSA Medical Director of Advanced Heart Failure Froedtert & Medical College of Wisconsin Stages, Phenotypes
2016 Update to Heart Failure Clinical Practice Guidelines Mitchell T. Saltzberg, MD, FACC, FAHA, FHFSA Medical Director of Advanced Heart Failure Froedtert & Medical College of Wisconsin Stages, Phenotypes
Hypertension (JNC-8)
") Hypertension (JNC-8) Southern California University of Health Sciences Physician Assistant Program Management and Treatment of Hypertension April 17, 2018, presented by Ezra Levy, Pharm.D.! The 8 th Joint
Hypertension (JNC-8) Southern California University of Health Sciences Physician Assistant Program Management and Treatment of Hypertension April 17, 2018, presented by Ezra Levy, Pharm.D.! The 8 th Joint
CLINICAL PRACTICE GUIDELINE
 CLINICAL PRACTICE GUIDELINE Procedure: Congestive Heart Failure Guideline Review Cycle: Biennial Reviewed By: Amish Purohit, MD, MHA, CPE, FACHE Review Date: November 2014 Committee Approval Date: 11/12/2014
CLINICAL PRACTICE GUIDELINE Procedure: Congestive Heart Failure Guideline Review Cycle: Biennial Reviewed By: Amish Purohit, MD, MHA, CPE, FACHE Review Date: November 2014 Committee Approval Date: 11/12/2014
Updates in Congestive Heart Failure
 Updates in Congestive Heart Failure GREGORY YOST, DO JOHNSTOWN CARDIOVASCULAR ASSOCIATES 1/28/2018 Disclosures Edwards speaker on Sapien3 valves (TAVR) Stages A-D and NYHA Classes I-IV Stage A: High risk
Updates in Congestive Heart Failure GREGORY YOST, DO JOHNSTOWN CARDIOVASCULAR ASSOCIATES 1/28/2018 Disclosures Edwards speaker on Sapien3 valves (TAVR) Stages A-D and NYHA Classes I-IV Stage A: High risk
HFpEF. April 26, 2018
 HFpEF April 26, 2018 (J Am Coll Cardiol 2017;70:2476 86) HFpEF 50% or more (40-71%) of patients with CHF have preserved LV systolic function. HFpEF is an increasingly frequent hospital discharge. Outcomes
HFpEF April 26, 2018 (J Am Coll Cardiol 2017;70:2476 86) HFpEF 50% or more (40-71%) of patients with CHF have preserved LV systolic function. HFpEF is an increasingly frequent hospital discharge. Outcomes
Heart Failure: Current Management Strategies
 Heart Failure: Current Management Strategies CSHP Fall Education Session- September 30th, 2017 Carolyn MacKinnon & Tamara Matchett BscPharm, ACPR Candidates Objectives 1. Describe the pathophysiology &
Heart Failure: Current Management Strategies CSHP Fall Education Session- September 30th, 2017 Carolyn MacKinnon & Tamara Matchett BscPharm, ACPR Candidates Objectives 1. Describe the pathophysiology &
Case 1. Case 2. What do you think about reducing or discontinuing some of the above now that his LVEF has normalized?
 Case 1 A primary care colleague inquires what to do with a patient (HFrEF in NSR) who has a digoxin level of 2.8ng/ml. Level was obtained at 10am, patient takes all medications at one time upon arising
Case 1 A primary care colleague inquires what to do with a patient (HFrEF in NSR) who has a digoxin level of 2.8ng/ml. Level was obtained at 10am, patient takes all medications at one time upon arising
ARNI (Angiotensin Receptor blocker / Neprilysin Inhibitors [Sacubutril/Valsartan]) Heart Failure Medication Initiation and Titration
![ARNI (Angiotensin Receptor blocker / Neprilysin Inhibitors [Sacubutril/Valsartan]) Heart Failure Medication Initiation and Titration](/thumbs/77/76069192.jpg "ARNI (Angiotensin Receptor blocker / Neprilysin Inhibitors [Sacubutril/Valsartan]) Heart Failure Medication Initiation and Titration") ARNI (Angiotensin Receptor blocker / Neprilysin Inhibitors [Sacubutril/Valsartan]) Heart Failure Medication and Symptomatic HF despite ACEI/ARB and B-blocker therapy Bilateral renal artery stenosis Moderate/Severe
ARNI (Angiotensin Receptor blocker / Neprilysin Inhibitors [Sacubutril/Valsartan]) Heart Failure Medication and Symptomatic HF despite ACEI/ARB and B-blocker therapy Bilateral renal artery stenosis Moderate/Severe
Summary/Key Points Introduction
 Summary/Key Points Introduction Scope of Heart Failure (HF) o 6.5 million Americans 20 years of age have HF o 960,000 new cases of HF diagnosed annually o 5-year survival rate for HF is ~50% Classification
Summary/Key Points Introduction Scope of Heart Failure (HF) o 6.5 million Americans 20 years of age have HF o 960,000 new cases of HF diagnosed annually o 5-year survival rate for HF is ~50% Classification
The Failing Heart in Primary Care
 The Failing Heart in Primary Care Hamid Ikram How fares the Heart Failure Epidemic? 4357 patients, 57% women, mean age 74 years HFSA 2010 Practice Guideline (3.1) Heart Failure Prevention A careful and
The Failing Heart in Primary Care Hamid Ikram How fares the Heart Failure Epidemic? 4357 patients, 57% women, mean age 74 years HFSA 2010 Practice Guideline (3.1) Heart Failure Prevention A careful and
Chronic. Outline. Congestive^ Heart Failure: Update on Effective Monitoring and Treatment. Heart Failure Epidemiology
 Chronic Congestive^ Heart Failure: Update on Effective Monitoring and Treatment Michael G. Shlipak, MD, MPH Professor of Medicine, UCSF Chief, Division of General Internal Medicine, SFVA Medical Center
Chronic Congestive^ Heart Failure: Update on Effective Monitoring and Treatment Michael G. Shlipak, MD, MPH Professor of Medicine, UCSF Chief, Division of General Internal Medicine, SFVA Medical Center
Heart Failure A Disease for the Internist?
 Heart Failure A Disease for the Internist? Dr Chris Davidson Sussex Cardiac Centre BRIGHTON UK Hot Topics in Heart Failure Drug treatments Valsartan / neprilysin inhib Investigations BNP and others Devices
Heart Failure A Disease for the Internist? Dr Chris Davidson Sussex Cardiac Centre BRIGHTON UK Hot Topics in Heart Failure Drug treatments Valsartan / neprilysin inhib Investigations BNP and others Devices
Heart Failure: Combination Treatment Strategies
 Heart Failure: Combination Treatment Strategies M. McDonald MD, FRCP State of the Heart Symposium May 28, 2011 None Disclosures Case 69 F, prior MIs (LV ejection fraction 25%), HTN No demonstrable ischemia
Heart Failure: Combination Treatment Strategies M. McDonald MD, FRCP State of the Heart Symposium May 28, 2011 None Disclosures Case 69 F, prior MIs (LV ejection fraction 25%), HTN No demonstrable ischemia
LITERATURE REVIEW: HEART FAILURE. Chief Residents
 LITERATURE REVIEW: HEART FAILURE Chief Residents Heart Failure EF 40% HFrEF Problem with contractility EF 40-50% HFmrEF EF > 50% HFpEF Problem with filling/relaxation RISK FACTORS Post MI HTN DM Obesity
LITERATURE REVIEW: HEART FAILURE Chief Residents Heart Failure EF 40% HFrEF Problem with contractility EF 40-50% HFmrEF EF > 50% HFpEF Problem with filling/relaxation RISK FACTORS Post MI HTN DM Obesity
Neprilysin Inhibitor (Entresto ) Prior Authorization and Quantity Limit Program Summary
 Prior Authorization and Quantity Limit Program Summary") Neprilysin Inhibitor (Entresto ) Prior Authorization and Quantity Limit Program Summary FDA APPROVED INDICATIONS DOSAGE 1 Indication Entresto Reduce the risk of cardiovascular (sacubitril/valsartan) death
Neprilysin Inhibitor (Entresto ) Prior Authorization and Quantity Limit Program Summary FDA APPROVED INDICATIONS DOSAGE 1 Indication Entresto Reduce the risk of cardiovascular (sacubitril/valsartan) death
Heart Failure 101 The Basic Principles of Diagnosis & Management
 Heart Failure 101 The Basic Principles of Diagnosis & Management Bill Tran, MD Non Invasive Cardiologist February 24, 2018 What the eye does not see and the mind does not know, does not exist. DH Lawrence
Heart Failure 101 The Basic Principles of Diagnosis & Management Bill Tran, MD Non Invasive Cardiologist February 24, 2018 What the eye does not see and the mind does not know, does not exist. DH Lawrence
HEART FAILURE. Heart Failure in the US. Heart Failure (HF) 10/5/2015. Martina Frost, PA-C Desert Cardiology of Tucson Northwest Medical Center
 10/5/2015. Martina Frost, PA-C Desert Cardiology of Tucson Northwest Medical Center") HEART FAILURE Martina Frost, PA-C Desert Cardiology of Tucson Northwest Medical Center Heart Failure in the US Prevalence - ~5 million 650,000 new cases annually 300,000 deaths annually Leading DRG among
HEART FAILURE Martina Frost, PA-C Desert Cardiology of Tucson Northwest Medical Center Heart Failure in the US Prevalence - ~5 million 650,000 new cases annually 300,000 deaths annually Leading DRG among
A patient with decompensated HF
 A patient with decompensated HF Professor Michel KOMAJDA University Pierre & Marie Curie Pitie Salpetriere Hospital Department of Cardiology Paris (France) Declaration Of Interest 2010 Speaker : Servier,
A patient with decompensated HF Professor Michel KOMAJDA University Pierre & Marie Curie Pitie Salpetriere Hospital Department of Cardiology Paris (France) Declaration Of Interest 2010 Speaker : Servier,
Antialdosterone treatment in heart failure
 Update on the Treatment of Chronic Heart Failure 2012 Antialdosterone treatment in heart failure 전남의대윤현주 Chronic Heart Failure Prognosis of Heart failure Cecil, Text book of Internal Medicine, 22 th edition
Update on the Treatment of Chronic Heart Failure 2012 Antialdosterone treatment in heart failure 전남의대윤현주 Chronic Heart Failure Prognosis of Heart failure Cecil, Text book of Internal Medicine, 22 th edition
Heart Failure Management. Waleed AlHabeeb, MD, MHA Assistant Professor of Medicine Consultant Heart Failure Cardiologist
 Heart Failure Management Waleed AlHabeeb, MD, MHA Assistant Professor of Medicine Consultant Heart Failure Cardiologist Heart failure prevalence is expected to continue to increase¹ 21 MILLION ADULTS WORLDWIDE
Heart Failure Management Waleed AlHabeeb, MD, MHA Assistant Professor of Medicine Consultant Heart Failure Cardiologist Heart failure prevalence is expected to continue to increase¹ 21 MILLION ADULTS WORLDWIDE
DISCLOSURES ACHIEVING SUCCESS THROUGH FAILURE: UPDATE ON HEART FAILURE WITH PRESERVED EJECTION FRACTION NONE
 ACHIEVING SUCCESS THROUGH FAILURE: UPDATE ON HEART FAILURE WITH PRESERVED EJECTION FRACTION Lori M. Tam, MD Providence Heart Institute DISCLOSURES NONE 1 OUTLINE Systolic vs. Diastolic Heart Failure New
ACHIEVING SUCCESS THROUGH FAILURE: UPDATE ON HEART FAILURE WITH PRESERVED EJECTION FRACTION Lori M. Tam, MD Providence Heart Institute DISCLOSURES NONE 1 OUTLINE Systolic vs. Diastolic Heart Failure New
HEART FAILURE. Heart Failure in the US. Heart Failure (HF) 2/20/2017. Martina Frost, PA-C Desert Cardiology of Tucson Northwest Medical Center
 2/20/2017. Martina Frost, PA-C Desert Cardiology of Tucson Northwest Medical Center") HEART FAILURE Martina Frost, PA-C Desert Cardiology of Tucson Northwest Medical Center Heart Failure in the US Prevalence - ~5 million 650,000 new cases annually 300,000 deaths annually Leading DRG among
HEART FAILURE Martina Frost, PA-C Desert Cardiology of Tucson Northwest Medical Center Heart Failure in the US Prevalence - ~5 million 650,000 new cases annually 300,000 deaths annually Leading DRG among
Incidence. 4.8 million in the United States. 400,000 new cases/year. 20 million patients with asymptomatic LV dysfunction
 Heart Failure Diagnosis According to the Working Group in Heart Failure, CHF is a syndrome where the diagnosis has the following essential components: A combination of: Symptoms, typically breathlessness
Heart Failure Diagnosis According to the Working Group in Heart Failure, CHF is a syndrome where the diagnosis has the following essential components: A combination of: Symptoms, typically breathlessness
Congestive Heart Failure 2015
 Definition Congestive Heart Failure 215 JP Mehegan/ Mercy Cardiology n Cardiac failure; Congestive heart failure; Chronic heart failure (synonyms) n When the heart is unable to pump sufficiently and at
Definition Congestive Heart Failure 215 JP Mehegan/ Mercy Cardiology n Cardiac failure; Congestive heart failure; Chronic heart failure (synonyms) n When the heart is unable to pump sufficiently and at
Heart Failure. Subjective SOB (shortness of breath) Peripheral edema. Orthopnea (2-3 pillows) PND (paroxysmal nocturnal dyspnea)
 Peripheral edema. Orthopnea (2-3 pillows) PND (paroxysmal nocturnal dyspnea)") Pharmacology I. Definitions A. Heart Failure (HF) Heart Failure Ezra Levy, Pharm.D. HF Results when one or both ventricles are unable to pump sufficient blood to meet the body s needs There are 2 types
Pharmacology I. Definitions A. Heart Failure (HF) Heart Failure Ezra Levy, Pharm.D. HF Results when one or both ventricles are unable to pump sufficient blood to meet the body s needs There are 2 types
Heart Failure. Jay Shavadia
 Heart Failure Jay Shavadia Definition Clinical syndrome characterized by: Symptoms: breathlessness at rest or on exercise, fatigue, tiredness or ankle swelling AND Signs: tachycardia, tachypnea, pulmonary
Heart Failure Jay Shavadia Definition Clinical syndrome characterized by: Symptoms: breathlessness at rest or on exercise, fatigue, tiredness or ankle swelling AND Signs: tachycardia, tachypnea, pulmonary
Heart Failure. Disclosures. Objectives: 8/28/2017. This is not a virus. It doesn t go away. none
 Heart Failure This is not a virus. It doesn t go away Shelley Wojtaszczyk, FNP-C, CHFN Heart Failure Program Coordinator Mercy Hospital of Buffalo none Disclosures Objectives: Defining and identifying
Heart Failure This is not a virus. It doesn t go away Shelley Wojtaszczyk, FNP-C, CHFN Heart Failure Program Coordinator Mercy Hospital of Buffalo none Disclosures Objectives: Defining and identifying
Long-Term Care Updates
 Long-Term Care Updates July 2015 By Amy Friedman Wilson, PharmD Heart failure (HF) is a clinical condition in which ventricular filling or ejection of blood is structurally or functionally impaired. 1
Long-Term Care Updates July 2015 By Amy Friedman Wilson, PharmD Heart failure (HF) is a clinical condition in which ventricular filling or ejection of blood is structurally or functionally impaired. 1
What s New in Heart Failure? Marie-France Gauthier, BSc, PharmD, ACPR Clinical Pharmacist at Montfort Hospital
 What s New in Heart Failure? Marie-France Gauthier, BSc, PharmD, ACPR Clinical Pharmacist at Montfort Hospital Disclosures I have no current or past relationships with commercial entities Learning objectives
What s New in Heart Failure? Marie-France Gauthier, BSc, PharmD, ACPR Clinical Pharmacist at Montfort Hospital Disclosures I have no current or past relationships with commercial entities Learning objectives
Heart Failure Update. Bibiana Cujec MD May 2015
 Heart Failure Update Bibiana Cujec MD May 2015 Disclosures Participation in clinical trial GUIDE IT (BNP in management of HF) Plan Review of new trials/ccs guidelines Management of heart failure: cases
Heart Failure Update Bibiana Cujec MD May 2015 Disclosures Participation in clinical trial GUIDE IT (BNP in management of HF) Plan Review of new trials/ccs guidelines Management of heart failure: cases
Heart Failure (HF) Treatment
 Treatment") Heart Failure (HF) Treatment Heart Failure (HF) Complex, progressive disorder. The heart is unable to pump sufficient blood to meet the needs of the body. Its cardinal symptoms are dyspnea, fatigue, and
Heart Failure (HF) Treatment Heart Failure (HF) Complex, progressive disorder. The heart is unable to pump sufficient blood to meet the needs of the body. Its cardinal symptoms are dyspnea, fatigue, and
Therapeutic Targets and Interventions
 Therapeutic Targets and Interventions Ali Valika, MD, FACC Advanced Heart Failure and Pulmonary Hypertension Advocate Medical Group Midwest Heart Foundation Disclosures: 1. Novartis: Speaker Honorarium
Therapeutic Targets and Interventions Ali Valika, MD, FACC Advanced Heart Failure and Pulmonary Hypertension Advocate Medical Group Midwest Heart Foundation Disclosures: 1. Novartis: Speaker Honorarium
Combination of renin-angiotensinaldosterone. how to choose?
 Combination of renin-angiotensinaldosterone system inhibitors how to choose? Karl Swedberg Professor of Medicine Sahlgrenska Academy University of Gothenburg karl.swedberg@gu.se Disclosures Research grants
Combination of renin-angiotensinaldosterone system inhibitors how to choose? Karl Swedberg Professor of Medicine Sahlgrenska Academy University of Gothenburg karl.swedberg@gu.se Disclosures Research grants
Objectives. Outline 4/3/2014
 Jessica Litke PGY1 ISHP Spring Meeting April 12, 2014 Objectives Appreciate the significance of heart failure (HF) to a patient and to the health care system Understand 2013 ACCF/AHA guidelines for the
Jessica Litke PGY1 ISHP Spring Meeting April 12, 2014 Objectives Appreciate the significance of heart failure (HF) to a patient and to the health care system Understand 2013 ACCF/AHA guidelines for the
Disclosure Statement. Heart Failure: Refreshers and Updates. Objectives. CHF: Chronic Heart Failure. Definitions. Definitions 2/19/2018
 Disclosure Statement Heart Failure: Refreshers and Updates Tracy K. Pettinger, PharmD Clinical Associate Professor College of Pharmacy The planners and presenter of this presentation have disclosed no
Disclosure Statement Heart Failure: Refreshers and Updates Tracy K. Pettinger, PharmD Clinical Associate Professor College of Pharmacy The planners and presenter of this presentation have disclosed no
Disclosures. This speaker has indicated there are no relevant financial relationships to be disclosed.
 Disclosures This speaker has indicated there are no relevant financial relationships to be disclosed. And the Beat Goes On: New Medications for Heart Failure Alison M. Walton, PharmD, BCPS The Case of
Disclosures This speaker has indicated there are no relevant financial relationships to be disclosed. And the Beat Goes On: New Medications for Heart Failure Alison M. Walton, PharmD, BCPS The Case of
Performance and Quality Measures 1. NQF Measure Number. Coronary Artery Disease Measure Set
 Unless indicated, the PINNACLE Registry measures are endorsed by the American College of Cardiology Foundation and the American Heart Association and may be used for purposes of health care insurance payer
Unless indicated, the PINNACLE Registry measures are endorsed by the American College of Cardiology Foundation and the American Heart Association and may be used for purposes of health care insurance payer
Chronic. Outline. Congestive^ Heart Failure: Update on Effective Monitoring and Treatment. Heart Failure Epidemiology. Michael G.
 Chronic Congestive^ Heart Failure: Update on Effective Monitoring and Treatment Michael G. Shlipak, MD, MPH Professor of Medicine, UCSF Chief, Division of General Internal Medicine, SFVA Medical Center
Chronic Congestive^ Heart Failure: Update on Effective Monitoring and Treatment Michael G. Shlipak, MD, MPH Professor of Medicine, UCSF Chief, Division of General Internal Medicine, SFVA Medical Center
MEDICAL MANAGEMENT OF PATIENTS WITH HEART FAILURE AND REDUCED EJECTION FRACTION
 MEDICAL MANAGEMENT OF PATIENTS WITH HEART FAILURE AND REDUCED EJECTION FRACTION FRANCIS X. CELIS, D.O. OPSO FALL CONFERENCE PORTLAND, OR 16 SEPTEMBER 2017 OVERVIEW What are the ACC/AHA Stages of HF? What
MEDICAL MANAGEMENT OF PATIENTS WITH HEART FAILURE AND REDUCED EJECTION FRACTION FRANCIS X. CELIS, D.O. OPSO FALL CONFERENCE PORTLAND, OR 16 SEPTEMBER 2017 OVERVIEW What are the ACC/AHA Stages of HF? What
Heart Failure Medical and Surgical Treatment
 Heart Failure Medical and Surgical Treatment Daniel S. Yip, M.D. Medical Director, Heart Failure and Transplantation Mayo Clinic Second Annual Lakeland Regional Health Cardiovascular Symposium February
Heart Failure Medical and Surgical Treatment Daniel S. Yip, M.D. Medical Director, Heart Failure and Transplantation Mayo Clinic Second Annual Lakeland Regional Health Cardiovascular Symposium February
Heart Failure A Team Approach Background, recognition, diagnosis and management
 Heart Failure A Team Approach Background, recognition, diagnosis and management Speaker bureau: Novartis At the conclusion of this activity, participants will be able to: Recognize signs and symptoms of
Heart Failure A Team Approach Background, recognition, diagnosis and management Speaker bureau: Novartis At the conclusion of this activity, participants will be able to: Recognize signs and symptoms of
Optimizing CHF Therapy: The Role of Digoxin, Diuretics, and Aldosterone Antagonists
 Optimizing CHF Therapy: The Role of Digoxin, Diuretics, and Aldosterone Antagonists Old Drugs for an Old Problem Jay Geoghagan, MD, FACC BHHI Primary Care Symposium February 28, 2014 None. Financial disclosures
Optimizing CHF Therapy: The Role of Digoxin, Diuretics, and Aldosterone Antagonists Old Drugs for an Old Problem Jay Geoghagan, MD, FACC BHHI Primary Care Symposium February 28, 2014 None. Financial disclosures
The NEW Heart Failure Guidelines
 The NEW Heart Failure Guidelines Daily Practice HF scenario of the Case Presentations HF as a complex and heterogeneous syndrome Several proposed pathophysiological mechanisms involving the heart and the
The NEW Heart Failure Guidelines Daily Practice HF scenario of the Case Presentations HF as a complex and heterogeneous syndrome Several proposed pathophysiological mechanisms involving the heart and the
New PINNACLE Measures The below measures for PINNACLE will be added as new measures to the outcomes reporting starting with Version 2.0.
 New PINNACLE Measures The below measures for PINNACLE will be added as new measures to the outcomes reporting starting with Version 2.0. Measure Steward Measure Name Measure Description Rationale for Adding
New PINNACLE Measures The below measures for PINNACLE will be added as new measures to the outcomes reporting starting with Version 2.0. Measure Steward Measure Name Measure Description Rationale for Adding
Images have been removed from the PowerPoint slides in this handout due to copyright restrictions.
 Heart Failure Heart Failure Introduction and History AHA 2015 Statistics About 6 million Americans 870,000 new cases each year 1 in 9 deaths related to HF Almost 1 million hospitalizations each year (cost
Heart Failure Heart Failure Introduction and History AHA 2015 Statistics About 6 million Americans 870,000 new cases each year 1 in 9 deaths related to HF Almost 1 million hospitalizations each year (cost
SGK 2016 Session: Postgraduate Course in Heart Failure Lausanne, 15. June 2016 Heart Failure Guidelines 2016
 SGK 2016 Session: Postgraduate Course in Heart Failure Lausanne, 15. June 2016 Heart Failure Guidelines 2016 Matthias Nägele, MD University Hospital Zurich Disclosures I have nothing to disclose. The new
SGK 2016 Session: Postgraduate Course in Heart Failure Lausanne, 15. June 2016 Heart Failure Guidelines 2016 Matthias Nägele, MD University Hospital Zurich Disclosures I have nothing to disclose. The new
Heart Failure New Drugs- Updated Guidelines
 Heart Failure New Drugs- Updated Guidelines Eileen Handberg, PhD, ANP-BC, FAHA, FACC Professor of Medicine Division of Cardiovascular Medicine University of Florida Disclosures 1. 3 2. 6 3. 8 4. 11 Dunlay
Heart Failure New Drugs- Updated Guidelines Eileen Handberg, PhD, ANP-BC, FAHA, FACC Professor of Medicine Division of Cardiovascular Medicine University of Florida Disclosures 1. 3 2. 6 3. 8 4. 11 Dunlay
Heart Failure Background, recognition, diagnosis and management
 Heart Failure Background, recognition, diagnosis and management Speaker bureau: Novartis At the conclusion of this activity, participants will be able to: Recognize signs and symptoms of heart failure
Heart Failure Background, recognition, diagnosis and management Speaker bureau: Novartis At the conclusion of this activity, participants will be able to: Recognize signs and symptoms of heart failure
Heart Failure Update John Coyle, M.D.
 Heart Failure Update 2011 John Coyle, M.D. Causes of Heart Failure Anderson,B.Am Heart J 1993;126:632-40 It It is now well-established that at least one-half of the patients presenting with symptoms and
Heart Failure Update 2011 John Coyle, M.D. Causes of Heart Failure Anderson,B.Am Heart J 1993;126:632-40 It It is now well-established that at least one-half of the patients presenting with symptoms and
Introductory Clinical Pharmacology Chapter 41 Antihypertensive Drugs
 Introductory Clinical Pharmacology Chapter 41 Antihypertensive Drugs Blood Pressure Normal = sys
Introductory Clinical Pharmacology Chapter 41 Antihypertensive Drugs Blood Pressure Normal = sys
Disclosures. Advances in Chronic Heart Failure Management 6/12/2017. Van N Selby, MD UCSF Advanced Heart Failure Program June 19, 2017
 Advances in Chronic Heart Failure Management Van N Selby, MD UCSF Advanced Heart Failure Program June 19, 2017 I have nothing to disclose Disclosures 1 Goal statement To review recently-approved therapies
Advances in Chronic Heart Failure Management Van N Selby, MD UCSF Advanced Heart Failure Program June 19, 2017 I have nothing to disclose Disclosures 1 Goal statement To review recently-approved therapies
New Advances in the Diagnosis and Management of Acute and Chronic Heart Failure
 New Advances in the Diagnosis and Management of Acute and Chronic Heart Failure Deborah Budge, MD Intermountain Healthcare Heart Failure Cardiologist Objectives: State the updates from the ACC 2013 HF
New Advances in the Diagnosis and Management of Acute and Chronic Heart Failure Deborah Budge, MD Intermountain Healthcare Heart Failure Cardiologist Objectives: State the updates from the ACC 2013 HF
Why guess when you could know? Gold Standard. Cardiac catheterization (Angiogram) Invasive Risks: Infection, hematoma, death
 Invasive Risks: Infection, hematoma, death") Why guess when you could know? Gold Standard Cardiac catheterization (Angiogram) Invasive Risks: Infection, hematoma, death PCI decisions Number of vessels involved Surgeon experience level The anatomic
Why guess when you could know? Gold Standard Cardiac catheterization (Angiogram) Invasive Risks: Infection, hematoma, death PCI decisions Number of vessels involved Surgeon experience level The anatomic
Disclosures. Overview. Goal statement. Advances in Chronic Heart Failure Management 5/22/17
 Disclosures Advances in Chronic Heart Failure Management I have nothing to disclose Van N Selby, MD UCSF Advanced Heart Failure Program May 22, 2017 Goal statement To review recently-approved therapies
Disclosures Advances in Chronic Heart Failure Management I have nothing to disclose Van N Selby, MD UCSF Advanced Heart Failure Program May 22, 2017 Goal statement To review recently-approved therapies
Aldosterone Antagonism in Heart Failure: Now for all Patients?
 Aldosterone Antagonism in Heart Failure: Now for all Patients? Inder Anand, MD, FRCP, D Phil (Oxon.) Professor of Medicine, University of Minnesota, Director Heart Failure Program, VA Medical Center 111C
Aldosterone Antagonism in Heart Failure: Now for all Patients? Inder Anand, MD, FRCP, D Phil (Oxon.) Professor of Medicine, University of Minnesota, Director Heart Failure Program, VA Medical Center 111C
VA/DoD Clinical Practice Guideline for the Diagnosis and Management of Hypertension - Pocket Guide Update 2004 Revision July 2005
 VA/DoD Clinical Practice Guideline for the Diagnosis and Management of Hypertension - Pocket Guide Update 2004 Revision July 2005 1 Any adult in the health care system 2 Obtain blood pressure (BP) (Reliable,
VA/DoD Clinical Practice Guideline for the Diagnosis and Management of Hypertension - Pocket Guide Update 2004 Revision July 2005 1 Any adult in the health care system 2 Obtain blood pressure (BP) (Reliable,
Contemporary Advanced Heart Failure Therapy
 Contemporary Advanced Heart Failure Therapy Andrew Boyle, MD Professor of Medicine Medical Director of Advanced Heart Failure Thomas Jefferson University Philadelphia, PA Audience Response Question 40
Contemporary Advanced Heart Failure Therapy Andrew Boyle, MD Professor of Medicine Medical Director of Advanced Heart Failure Thomas Jefferson University Philadelphia, PA Audience Response Question 40
Management of Hypertension
 Clinical Practice Guidelines Management of Hypertension Definition and classification of blood pressure levels (mmhg) Category Systolic Diastolic Normal
Clinical Practice Guidelines Management of Hypertension Definition and classification of blood pressure levels (mmhg) Category Systolic Diastolic Normal
Cardiovascular Health Practice Guideline Outpatient Management of Coronary Artery Disease 2003
 Authorized By: Medical Management Guideline Committee Approval Date: 12/13/01 Revision Date: 12/11/03 Beta-Blockers Nitrates Calcium Channel Blockers MEDICATIONS Indicated in post-mi, unstable angina,
Authorized By: Medical Management Guideline Committee Approval Date: 12/13/01 Revision Date: 12/11/03 Beta-Blockers Nitrates Calcium Channel Blockers MEDICATIONS Indicated in post-mi, unstable angina,
Initiating New Medications in the Management of Heart Failure
 Initiating New Medications in the Management of Heart Failure Sandra Oliver-McNeil DNP, MSN, ACNP-BC, CHFN Associate Professor (Clinical) Wayne State University College of Nursing Objectives The participant
Initiating New Medications in the Management of Heart Failure Sandra Oliver-McNeil DNP, MSN, ACNP-BC, CHFN Associate Professor (Clinical) Wayne State University College of Nursing Objectives The participant
CT Academy of Family Physicians Scientific Symposium October 2012 Amit Pursnani, MD
 CT Academy of Family Physicians Scientific Symposium October 2012 Amit Pursnani, MD Clinical syndrome resulting from a structural or functional cardiac disorder that impairs the ability of the heart to
CT Academy of Family Physicians Scientific Symposium October 2012 Amit Pursnani, MD Clinical syndrome resulting from a structural or functional cardiac disorder that impairs the ability of the heart to
Outline. Classification by LVEF Conventional Therapy New Therapies. Ivabradine Sacubitril/valsartan
 New Pharmacological Therapies for Heart Failure Mark Drazner, MD, MSc Clinical Chief of Cardiology Medical Director, CHF/VAD/Transplant James M. Wooten Chair in Cardiology UT Southwestern Medical Center
New Pharmacological Therapies for Heart Failure Mark Drazner, MD, MSc Clinical Chief of Cardiology Medical Director, CHF/VAD/Transplant James M. Wooten Chair in Cardiology UT Southwestern Medical Center
Cardiovascular Pharmacotherapy
 Cardiovascular Pharmacotherapy Overview Mechanism of cardiovascular drugs Indications and clinical use in cardiology Renin-Angiotensin Inhibitors: Angiotensin-Converting Enzyme Inhibitors, Angiotensin
Cardiovascular Pharmacotherapy Overview Mechanism of cardiovascular drugs Indications and clinical use in cardiology Renin-Angiotensin Inhibitors: Angiotensin-Converting Enzyme Inhibitors, Angiotensin
Balanced information for better care. Heart failure: Managing risk and improving patient outcomes
 Balanced information for better care Heart failure: Managing risk and improving patient outcomes Heart failure increases hospitalization Heart failure is the most common medical reason for hospitalization
Balanced information for better care Heart failure: Managing risk and improving patient outcomes Heart failure increases hospitalization Heart failure is the most common medical reason for hospitalization
2017 CCS HF Guidelines Medical Therapy for HFrEF When What Order and How Much?
 2017 CCS HF Guidelines Medical Therapy for HFrEF When What Order and How Much? Dr. Shelley Zieroth University of Manitoba @ShelleyZieroth @CanHFSociety Disclosures Consulting/Advisory Board: Amgen, Astra
2017 CCS HF Guidelines Medical Therapy for HFrEF When What Order and How Much? Dr. Shelley Zieroth University of Manitoba @ShelleyZieroth @CanHFSociety Disclosures Consulting/Advisory Board: Amgen, Astra
Heart Failure CTSHP Fall Seminar
 Heart Failure CTSHP Fall Seminar Laurajo Ryan, PharmD, MSc, BCPS, CDE Pharmacist Learning Objectives Outline the pathophysiology of heart failure List triggers for decompensated heart failure Describe
Heart Failure CTSHP Fall Seminar Laurajo Ryan, PharmD, MSc, BCPS, CDE Pharmacist Learning Objectives Outline the pathophysiology of heart failure List triggers for decompensated heart failure Describe
8:30-10:30 WS #4: Cardiology :00-13:00 WS #11: Cardiology 101 (Repeated)
") Professor Ralph Stewart Cardiologist Auckland City Hospital Green Lane Cardiovascular Research Unit Auckland Heart Group Fiona Stewart Cardiologist Green Lane Hospital National Women's Hospital Professor
Professor Ralph Stewart Cardiologist Auckland City Hospital Green Lane Cardiovascular Research Unit Auckland Heart Group Fiona Stewart Cardiologist Green Lane Hospital National Women's Hospital Professor
Sara O. Weiss, MD Director, Heart Failure Services Virginia Mason Medical Center September 8, 2012
 Sara O. Weiss, MD Director, Heart Failure Services Virginia Mason Medical Center September 8, 2012 Disclosure: Dr. Weiss has no significant financial interest in any of the products or manufacturers mentioned.
Sara O. Weiss, MD Director, Heart Failure Services Virginia Mason Medical Center September 8, 2012 Disclosure: Dr. Weiss has no significant financial interest in any of the products or manufacturers mentioned.
Beyond ACE-inhibitors for Heart Failure. Jacob Townsend, MD NCVH Birmingham 2015
 Beyond ACE-inhibitors for Heart Failure Jacob Townsend, MD NCVH Birmingham 2015 % Decrease in Mortality Current Therapy HFrEF 0% Angiotensin receptor blocker ACE inhibitor Beta blocker Mineralocorticoid
Beyond ACE-inhibitors for Heart Failure Jacob Townsend, MD NCVH Birmingham 2015 % Decrease in Mortality Current Therapy HFrEF 0% Angiotensin receptor blocker ACE inhibitor Beta blocker Mineralocorticoid
ESC Guidelines for the Diagnosis and Treatment of Chronic Heart Failure
 ESC Guidelines for the Diagnosis and Treatment of Chronic Heart Failure - 2005 Karl Swedberg Professor of Medicine Department of Medicine Sahlgrenska University Hospital/Östra Göteborg University Göteborg
ESC Guidelines for the Diagnosis and Treatment of Chronic Heart Failure - 2005 Karl Swedberg Professor of Medicine Department of Medicine Sahlgrenska University Hospital/Östra Göteborg University Göteborg
Evaluation and Management of Acute Decompensated Heart Failure (HF) with Reduced Ejection Fraction Systolic Heart Failure (HFrEF)(EF<40%
 with Reduced Ejection Fraction Systolic Heart Failure (HFrEF)(EF<40%") Evaluation and Management of Acute Decompensated Heart Failure (HF) with Reduced Ejection Fraction Systolic Heart Failure (HFrEF)(EF
Evaluation and Management of Acute Decompensated Heart Failure (HF) with Reduced Ejection Fraction Systolic Heart Failure (HFrEF)(EF
7/7/ CHD/MI LVH and LV dysfunction Dysrrhythmias Stroke PVD Renal insufficiency and failure Retinopathy. Normal <120 Prehypertension
 Prevalence of Hypertension Hypertension: Diagnosis and Management T. Villela, M.D. Program Director University of California, San Francisco-San Francisco General Hospital Family and Community Medicine
Prevalence of Hypertension Hypertension: Diagnosis and Management T. Villela, M.D. Program Director University of California, San Francisco-San Francisco General Hospital Family and Community Medicine