Long-term results (22 years) of the Ross Operation a single institutional experience
|
|
|
- Tyler Barnett
- 5 years ago
- Views:
Transcription




1 Long-term results (22 years) of the Ross Operation a single institutional experience Authors: Costa FDA, Schnorr GM, Veloso M,Calixto A, Colatusso D, Balbi EM, Torres R, Ferreira ADA, Colatusso C Department of Cardiovascular Surgery INC- Cardio

2
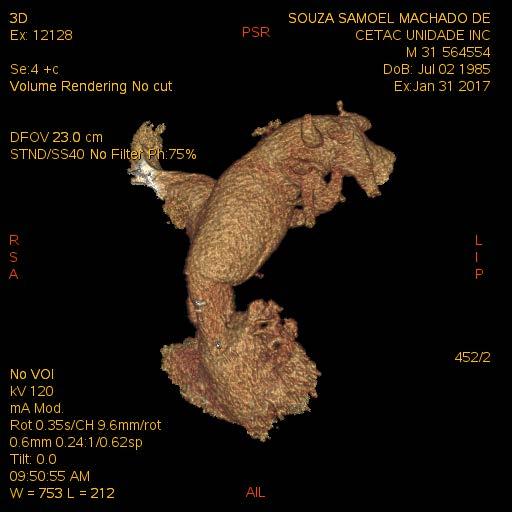
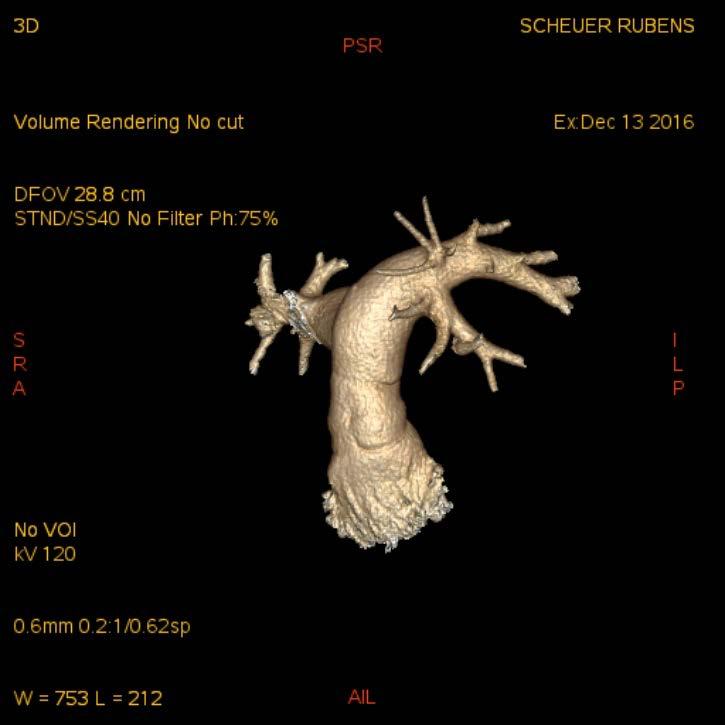
 Late functional evaluation of the RVOT allograft Department of Cardiovascular Surgery")
3 Ross Operation - 22 Years Results Evaluate the long-term results (22 Years) of the Ross Operation with emphasis on: Late survival Causes and incidence of reoperations Late functional evaluation of the Pulmonary Autograft (PA) Late functional evaluation of the RVOT allograft Department of Cardiovascular Surgery INC- Cardio
4 Ross Operation - 22 Years Results Study Period: May 1995 thru October 2017 Total experience 526 patients Patients: n = 477 (includes all consecutive patients operated at the author s official institution) Age: 31.1 ± 13.1 years (min = 3, max = 60) Sex: Male 351 (73.6%), Female 126 (26.3%). 38 with concomitant mitral valve disease 8 with Ascending Aortic Aneurysm 26 with Bacterial Endocarditis 5 with Coronary Insufficiency Department of Cardiovascular Surgery INC- Cardio
5 Ross Operation Patient Demographics Ross Operation - 22 Years Results Etiology Bicuspid/Unicuspid valves 264 (55,3) Rheumatic 138 (28,9) Degenerative 28 (5,9) Endocarditis (Native + Prosthetic Valves) 26 (5,5) Others 21 (4,4) Predominant aortic hemodynamics Stenosis 150 (31,4) Regurgitation 183 (38,4) Mixed lesion 144 (30,2) Rhythm Sinus 459 (97,6) Atrial fibrillation 8 (1,7) Pacemaker 9 (0,5) Complete AV block 1 (0,2) LV ejection fraction 50% 432 (90,6) 31% to 49% 40 (8,4) 30% 5 (1,0) NYHA functional class I 108 (22,7) II 211 (44,2) III 135 (28,3) IV 23 (4,8) Previous aortic valve interventions 67 (14,0)
 58 Myocardial Protection Intermittent Cold Blood")
 Department of Cardiovascular Surgery")
6 Ross Operation - 22 Years Results Total Root Replacement 419 Inclusion Technique (MiniRoot) 58 Myocardial Protection Intermittent Cold Blood Cardioplegia Cross Clamp Time 113 ± 26 min (min = 37, max = 226) ECC Bypass Time 138 ± 33 min (min = 58, max = 300) Department of Cardiovascular Surgery INC- Cardio
7 Ross Operation Operative Data Ross Operation - 22 Years Results Operative Technique Root Replacement 419 (87,8) Inclusion 58 (12,2) Additional Aortic Procedures External Annular Reduction 44 (9,2) Comissural Plication 9 (1,9) Mannouguian 9 (1,9) Konno 11 (2,3) Reduction Aortoplasty 59 (12,3) Concomitant Procedures Mitral Valve Repair 38 (8,0) CABG 15 (3,1) Congenital Anomalies Repair 10 (2,0) Ascending Aorta Replacement 8 (1,7) Aortic Annulus Diameter < 27mm 345 (72,3) 27mm 132 (27,6)


8 Ross Operation 22 Years Results RVOT Reconstrucion Group I Cryo Allografts Group II- Cryo + DOA Dcell valves...42 Group III Cryo + SDS Dcell Valves Group IV Fresh + SDS Dcell Valves Department of Cardiovascular Surgery INC- Cardio
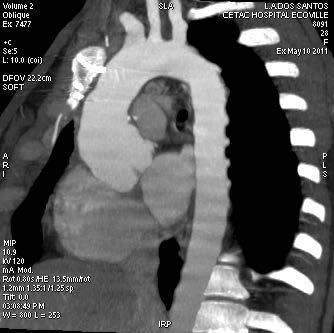
9 Ross Operation 22 Years Results Postoperative Evaluation Clinical Examination Echocardiography Before hospital discharge 6/12 months PO, annualy thereafter CT scan studies Follow-up Clinical Follow-up 451 patients (94,5% complete) Mean clinical follow-up time = 9,4 years (0,1 22,0) Mean echo follow-up time = 7,6 years (0,1 21,9) Department of Cardiovascular Surgery INC- Cardio
10 Ross Operation - 22Years Results Statistical Analysis Actuarial Survival and Event-Free Survival for Pulmonary Autograft or RVOT Allograft Dysfunction or Reoperation- Kaplan-Meier Method Time related events- Risk factors for Pulmonary Autograft and RVOT Allograft Dysfunctionunivariate analysis with the Log Rank Mantel Cox Test and multivariable analysis with Cox Regression models Department of Cardiovascular Surgery INC- Cardio
11 Ross Operation - 22 Years Results Results - Early Mortality 2,5% (12/477) Low Cardiac Output Syndrome 5 Intraoperative Hemorrhage 3 Intractable Ventricular Fibrillation 1 Anomalous Circumflex Artery Injury 1 First Septal Injury 1 Left Main Angulation 1 Last 150 cases 2 deaths = 1.3% mortality Department of Cardiovascular Surgery INC- Cardio
12 Ross Operation - 22 Years Results Results - Late Mortality 31 cases (31/451) 6,8% Valve-Related 10 Sudden death 7 Endocarditis PA and/or RVOT allograft 2 Stroke 1 Cardiac -Related 11 Progressive CHF 7 Acute Myocardial Infarction 2 Pulmonary Embolism 2 Non- cardiac causes 10 Car accident 2 HIV + Meningitis 1 Drowning 1 Acute Abdomen 1 Murder 1 Colon cancer 1 Unknown 3 Department of Cardiovascular Surgery INC- Cardio
13 Ross Operation Actuarial Survival Survival at 20 years = 81.6% (CI95% = %)
14 Ross Operation - 22 Years Results Clinical Follow-up Late Functional Status NYHA I patients NYHA II - 77 patients NYHA III - 12 patients NYHA IV 1 patient 11 cases of Thromboembolism 0,28%/patient-year 2 Major Bleeding 0,05%/patient-year 9 cases of Bacterial Endocarditis- 0,23%/patient-year Department of Cardiovascular Surgery INC- Cardio

15 Ross Operation - 22 Years Results Reoperations (n=65 patients, 70 procedures) Pulmonary Autograft (PA) 38 RVOT Allograft 14 Mitral Valve 9 Myocardial Revascularization 4 Department of Cardiovascular Surgery INC- Cardio
16
17 Indications for Reoperations on the Pulmonary Autograft Conservative Approach Severe Aortic Regurgitation Root Aneurysm 55 mm or with documented increase > 3mm/year Moderate AR + Root Size 50 mm Endocarditis with valvular lesion or nonresponsive to medical therapy Pseudo-aneurysms at suture lines Ross Operation 22 Years Results
18 Ross Operation 22 Years Results Indications for Reoperation on the Pulmonary Autograft (n=38) Root Dilatation + AI 17 Endocarditis 4 Pure AI 11 Quadricuspid pulmonary autograft 1 Proximal Pseudo-Aneurysm 2 Rheumatic involvement 1 Supra-aortic stenosis 1 Technical distortion 1
19 Mean time to reoperation = 7,8 years ( min =0,1 y max =21 years) Reoperative Mortality = 7,7% (Both in endocarditis cases) No Mortality in Elective Reoperations 20 Patients (52%) retained their original PA Reoperations on the PA Operations Performed Ross Operation 22 Years Results Ao Homograft 9 David/Yacoub 15 Valve repair 3 Ao Bioprosthesis 4 Fistula closure 2 Bentall operation 4 Supra-aortic repair 1



20 Aortic Valve Repair for Pulmonary Autograft Dilatation with AR
21
22
23 Table 5. Risk Factors for More than Mild AI at Late Follow-up Risk Factor Hazard Ratio (95% CI) p value Sex (male) 1,45 (0,79 to 2,69) 0,23 Age ,63 (0,35 to 1,13) 0,12 > 40 0,76 (0,39 to 1,47) 0,41 Valve Lesion AI 1,70 (0,87 to 3,33) 0,12 Mixed 1,29 (0,63 to 2,63) 0,47 Etiology Bicuspid (congenital) 1,14 (0,66 to 1,98) 0,63 Etiology Degenerative 1,30 (0,45 to 3,78) 0,63 Etiology Endocarditis 2,72 (0,93 to 7,96) 0,06 Etiology Others 1,16 (0,27 to 4,98) 0,83 Implantation Technique: inclusion 1,19 (0,57 to 2,53) 0.63 Aortic Annulus 27mm 2,00 (1,14 to 3,50) 0,01 Annulus Reduction 2,12 (1,10 to 4,07) 0,02 Aortoplasty 1,74 (0,82 to 3,69) 0,14 Previous Operation 1,08 (0,56 2,07) 0,81 Multivariable Cox Regression: Aortic Annulus > 27mm HR 1,76 95% CI 0,98-3,15: p= 0,05 Aortic Annulus Reduction HR 2,05 CI 1,02 4,09: p=0,04
24
25
26 Table 6. Risk Factors for Root Diameter 45mm at Late Follow-up Risk Factor Hazard Ratio (95% CI) p value Sex (males vs females) 9,09 (2,20 to 37,60) 0,0023 Age ,92 (0,44 to 1,89) 0,82 > 40 0,94 (0,40 to 2,18) 0,89 Valve Lesion AI 3,88 (1,33 to 11,28) 0,01 Mixed 3,41 (1,15 to 10,10) 0,02 Etiology Bicuspid (congenital) 1,48 (0,73 to 3,01) 0,27 Etiology Degenerative 4,55 (1,69 to 12,22) 0,026 Etiology Endocarditis 4,023 (1,19 to 15,05) 0,02 Etiology Others 2,85 (0,63 to 12,86) 0,17 Implantation Technique: inclusion 1,64 (0,50 to 5,33) 0,40 Aortic Annulus 27mm 10,30 (4,04 to 26,21) <0,0001 Annulus Reduction 3,20 (1,62 to 6,33) 0,0008 Aortoplasty 1,35 (0,47 to 3,82) 0,56 Previous Operation 1,35 (0,64 12,82) 0,41 Multivariable Cox Regression : Aortic Annulus > 27mm (HR % CI ; p=0.000) Males (HR % CI ; p=0.04) Aortic Insuf. (HR % CI ; p=0.08) Mixed (HR % CI ; p=0.06)
27 Ross Operation Risk Factors for Root Dilatation
28


29 FRESH DECELLULARIZED VERSUS STANDARD CRYOPRESERVED PULMONARY ALLOGRAFTS FOR RVOT RECONSTRUCTION DURING THE ROSS OPERATION A PROPENSITY MATCHED STUDY Authors: Jonathan Etnel, Paula H Suss, Danielle F. Collatusso, Eduardo M. Balbi Filho, Gabriela M. Schnorr, Myrian Wisniewski, Francisco Diniz Affonso da Costa
 GROUP SCA")
")
30 PATIENTS AND METHODS Ross Operations RVOT RECONSTRUCTION WITH DIFFERENT ALLOGRAFTS (EXCLUDED) GROUP SCA (N=202) Standard Cryopreserved Allografts GROUP DA (N=200) Fresh Decellularized Allografts PROPENSITY MATCHING GROUP SCA (N=130) GROUP DA (N=130)
 HR = 0.68, (95% CI: 0.32-1.44, p=0,311) Freedom from Dysfunction at 8 years DA = 87.1% ( 95%CI: 67.")
 Freedom from Dysfunction at 8 years DA = 86.7% (95%CI: 63.6-95.6) SCA = 87.")
31 Freedom from Allograft Dysfunction Unmatched Matched SCA = 43 events (1.82%/year) DA = 10 events (1.47%/year) HR = 0.68, (95% CI: , p=0,311) Freedom from Dysfunction at 8 years DA = 87.1% ( 95%CI: ) SCA = 84.4% ( 95%CI: ) SCA = 25 events (1.55%/year) DA = 7 events (1.28%/year) HR = 0.54, (95%CI: , p=0,09) Freedom from Dysfunction at 8 years DA = 86.7% (95%CI: ) SCA = 87.3%( 95%CI: )

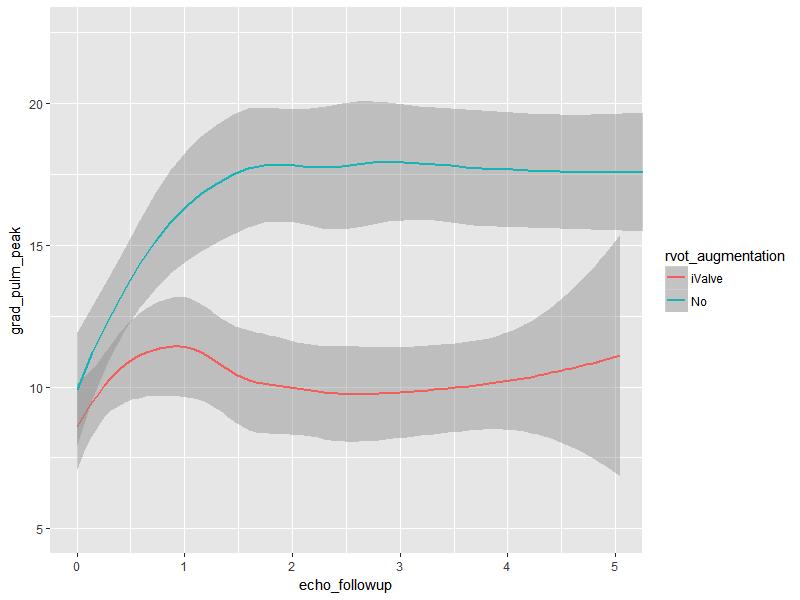
32 LONGITUDINAL ECHO ANALYSIS
33


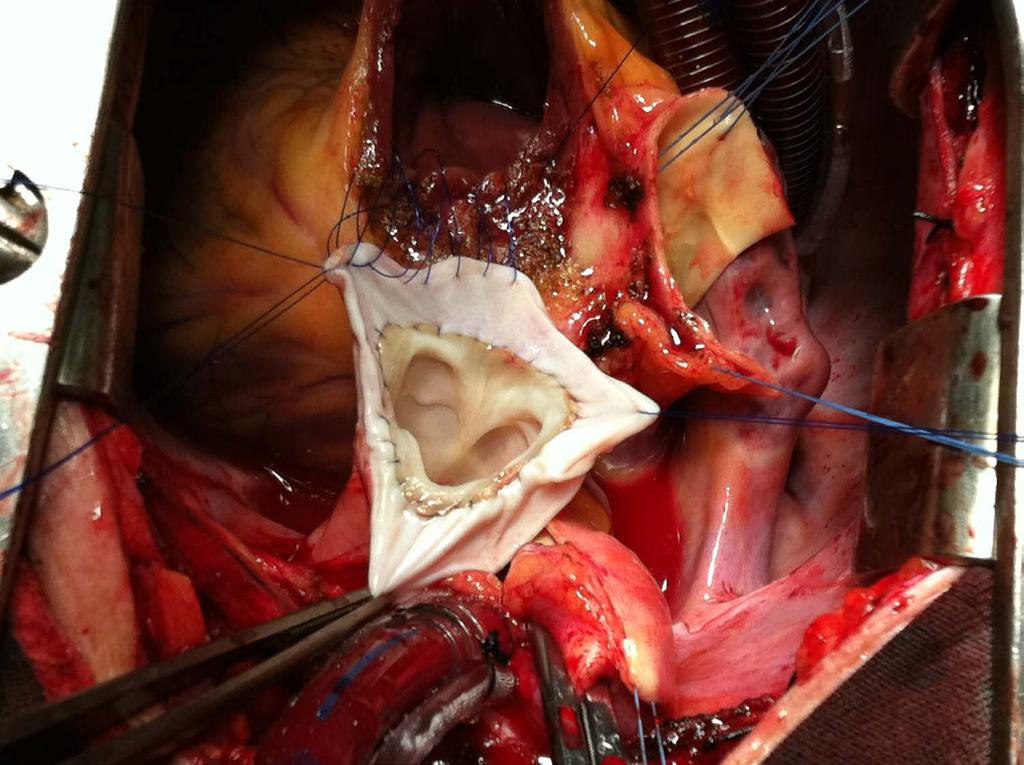
34 Decellularized Pulmonary Allograft with Decellularized Human Pericardium Extension Patent Pending

35
36

37
38
39
40 Ross Operation - 22Years Results The Ross Operation is associated with excellent functional recovery and long-term survival up to 20 years of followup. The Pulmonary Autograft, when implanted as a root replacement has acceptable durability, especially in patients with pure Aortic Stenosis. Males, with a dilated aortic annulus and preoperative diagnosis of AI are at incresead risk for developing late AI and root dilatation. Progressive AI/PA dilatation may indicate the need for future reoperations after the second decade of follow-up Technical Aspects/Patient Selection.

41 Ross Operation - 22 Years Results Although cryopreserved allografts provides good long-term results for the RVOT reconstruction, the incidence of elevated peak gradients is not negligible. The use of fresh decellularized allografts valves is emerging as a better alternative to RVOT reconstruction. Proximal Pericardium extension may improve RVOT allograft function even further.
The Role Of Decellularized Valve Prostheses In The Young Patient
 The Role Of Decellularized Valve Prostheses In The Young Patient Francisco Diniz Affonso da Costa Human Tissue Bank PUCPR - Brazil Disclosures Ownership and patent license of the SDS decellularization
The Role Of Decellularized Valve Prostheses In The Young Patient Francisco Diniz Affonso da Costa Human Tissue Bank PUCPR - Brazil Disclosures Ownership and patent license of the SDS decellularization
The Ross Procedure: Outcomes at 20 Years
 The Ross Procedure: Outcomes at 20 Years Tirone David Carolyn David Anna Woo Cedric Manlhiot University of Toronto Conflict of Interest None The Ross Procedure 1990 to 2004 212 patients: 66% 34% Mean age:
The Ross Procedure: Outcomes at 20 Years Tirone David Carolyn David Anna Woo Cedric Manlhiot University of Toronto Conflict of Interest None The Ross Procedure 1990 to 2004 212 patients: 66% 34% Mean age:
Decellularization of Aortic Homografts: South American and European Current Experience
 Department of Cardiac Surgery Instituto de Neurologia e Cardiologia de Curitiba (INC-Cardio) Decellularization of Aortic Homografts: South American and European Current Experience Francisco Diniz Affonso
Department of Cardiac Surgery Instituto de Neurologia e Cardiologia de Curitiba (INC-Cardio) Decellularization of Aortic Homografts: South American and European Current Experience Francisco Diniz Affonso
Bicuspid aortic root spared during ascending aorta surgery: an update of long-term results
 Short Communication Bicuspid aortic root spared during ascending aorta surgery: an update of long-term results Marco Russo, Guglielmo Saitto, Paolo Nardi, Fabio Bertoldo, Carlo Bassano, Antonio Scafuri,
Short Communication Bicuspid aortic root spared during ascending aorta surgery: an update of long-term results Marco Russo, Guglielmo Saitto, Paolo Nardi, Fabio Bertoldo, Carlo Bassano, Antonio Scafuri,
Case. 15-year-old boy with bicuspid AV Severe AR with moderate AS. Ross vs. AVR (or AVP)
") Case 15-year-old boy with bicuspid AV Severe AR with moderate AS Ross vs. AVR (or AVP) AMC case 14-year-old boy with bicuspid AV Severe AS with mild AR Body size Bwt: 55 kg, Ht: 154 cm, BSA: 1.53 m 2 Echocardiography
Case 15-year-old boy with bicuspid AV Severe AR with moderate AS Ross vs. AVR (or AVP) AMC case 14-year-old boy with bicuspid AV Severe AS with mild AR Body size Bwt: 55 kg, Ht: 154 cm, BSA: 1.53 m 2 Echocardiography
Presenter Disclosure. Patrick O. Myers, M.D. No Relationships to Disclose
 Presenter Disclosure Patrick O. Myers, M.D. No Relationships to Disclose Aortic Valve Repair by Cusp Extension for Rheumatic Aortic Insufficiency in Children Long term Results and Impact of Extension Material
Presenter Disclosure Patrick O. Myers, M.D. No Relationships to Disclose Aortic Valve Repair by Cusp Extension for Rheumatic Aortic Insufficiency in Children Long term Results and Impact of Extension Material
Expanding Relevance of Aortic Valve Repair Is Earlier Operation Indicated?
 Expanding Relevance of Aortic Valve Repair Is Earlier Operation Indicated? RM Suri, V Sharma, JA Dearani, HM Burkhart, RC Daly, LD Joyce, HV Schaff Division of Cardiovascular Surgery, Mayo Clinic, Rochester,
Expanding Relevance of Aortic Valve Repair Is Earlier Operation Indicated? RM Suri, V Sharma, JA Dearani, HM Burkhart, RC Daly, LD Joyce, HV Schaff Division of Cardiovascular Surgery, Mayo Clinic, Rochester,
Results of Aortic Valve Preservation and Repair
 Results of Aortic Valve Preservation and Repair Department of Cardiothoracic and Vascular Surgery Cliniques Universitaires St. Luc Brussels, Belgium Gebrine Elkhoury Institutional experience in AV preservation
Results of Aortic Valve Preservation and Repair Department of Cardiothoracic and Vascular Surgery Cliniques Universitaires St. Luc Brussels, Belgium Gebrine Elkhoury Institutional experience in AV preservation
CLINICAL COMMUNIQUE 16 YEAR RESULTS
 CLINICAL COMMUNIQUE 6 YEAR RESULTS Carpentier-Edwards PERIMOUNT Mitral Pericardial Bioprosthesis, Model 6900 Introduction The Carpentier-Edwards PERIMOUNT Mitral Pericardial Valve, Model 6900, was introduced
CLINICAL COMMUNIQUE 6 YEAR RESULTS Carpentier-Edwards PERIMOUNT Mitral Pericardial Bioprosthesis, Model 6900 Introduction The Carpentier-Edwards PERIMOUNT Mitral Pericardial Valve, Model 6900, was introduced
16 YEAR RESULTS Carpentier-Edwards PERIMOUNT Mitral Pericardial Bioprosthesis, Model 6900
 CLINICAL COMMUNIQUé 6 YEAR RESULTS Carpentier-Edwards PERIMOUNT Mitral Pericardial Bioprosthesis, Model 69 The Carpentier-Edwards PERIMOUNT Mitral Pericardial Valve, Model 69, was introduced into clinical
CLINICAL COMMUNIQUé 6 YEAR RESULTS Carpentier-Edwards PERIMOUNT Mitral Pericardial Bioprosthesis, Model 69 The Carpentier-Edwards PERIMOUNT Mitral Pericardial Valve, Model 69, was introduced into clinical
Long Term Outcomes of Aortic Root Operations for Marfan Syndrome: A Comparison of Bentall versus Aortic Valve-Sparing Procedures
 Long Term Outcomes of Aortic Root Operations for Marfan Syndrome: A Comparison of Bentall versus Aortic Valve-Sparing Procedures Joel Price, MD, J. Trent Magruder, MD, Allen Young, MPH, Joshua C. Grimm,
Long Term Outcomes of Aortic Root Operations for Marfan Syndrome: A Comparison of Bentall versus Aortic Valve-Sparing Procedures Joel Price, MD, J. Trent Magruder, MD, Allen Young, MPH, Joshua C. Grimm,
Long-term results of a strategy of aortic valve repair in the paediatric population: Should we avoid cusp extension?
 Long-term results of a strategy of aortic valve repair in the paediatric population: Should we avoid cusp extension? Y d Udekem, J Siddiqui, C Seaman, I Konstantinov, J Galati, M Cheung, C Brizard Royal
Long-term results of a strategy of aortic valve repair in the paediatric population: Should we avoid cusp extension? Y d Udekem, J Siddiqui, C Seaman, I Konstantinov, J Galati, M Cheung, C Brizard Royal
Management of Difficult Aortic Root, Old and New solutions
 Management of Difficult Aortic Root, Old and New solutions Hani K. Najm MD, Msc, FRCSC,, FACC, FESC Chairman, Pediatric and Congenital Heart Surgery Cleveland Clinic Conflict of Interest None Difficult
Management of Difficult Aortic Root, Old and New solutions Hani K. Najm MD, Msc, FRCSC,, FACC, FESC Chairman, Pediatric and Congenital Heart Surgery Cleveland Clinic Conflict of Interest None Difficult
TSDA Boot Camp September 13-16, Introduction to Aortic Valve Surgery. George L. Hicks, Jr., MD
 TSDA Boot Camp September 13-16, 2018 Introduction to Aortic Valve Surgery George L. Hicks, Jr., MD Aortic Valve Pathology and Treatment Valvular Aortic Stenosis in Adults Average Course (Post mortem data)
TSDA Boot Camp September 13-16, 2018 Introduction to Aortic Valve Surgery George L. Hicks, Jr., MD Aortic Valve Pathology and Treatment Valvular Aortic Stenosis in Adults Average Course (Post mortem data)
Minimally Invasive Aortic Surgery With Emphasis On Technical Aspects, Extracorporeal Circulation Management And Cardioplegic Techniques
 Minimally Invasive Aortic Surgery With Emphasis On Technical Aspects, Extracorporeal Circulation Management And Cardioplegic Techniques Konstadinos A Plestis, MD System Chief of Cardiothoracic and Vascular
Minimally Invasive Aortic Surgery With Emphasis On Technical Aspects, Extracorporeal Circulation Management And Cardioplegic Techniques Konstadinos A Plestis, MD System Chief of Cardiothoracic and Vascular
Experience with 500 Stentless Aortic Valve Replacements
 Experience with 500 Stentless Aortic Valve Replacements Dimitrios C. Iliopoulos, MD Cardiac Surgeon Ass. Professor of Surgery University of Athens, School of Medicine I declare no conflict of interest
Experience with 500 Stentless Aortic Valve Replacements Dimitrios C. Iliopoulos, MD Cardiac Surgeon Ass. Professor of Surgery University of Athens, School of Medicine I declare no conflict of interest
Adult Echocardiography Examination Content Outline
 Adult Echocardiography Examination Content Outline (Outline Summary) # Domain Subdomain Percentage 1 2 3 4 5 Anatomy and Physiology Pathology Clinical Care and Safety Measurement Techniques, Maneuvers,
Adult Echocardiography Examination Content Outline (Outline Summary) # Domain Subdomain Percentage 1 2 3 4 5 Anatomy and Physiology Pathology Clinical Care and Safety Measurement Techniques, Maneuvers,
Prof. Patrizio LANCELLOTTI, MD, PhD Heart Valve Clinic, University of Liège, CHU Sart Tilman, Liège, BELGIUM
 The Patient with Aortic Stenosis and Mitral Regurgitation Prof. Patrizio LANCELLOTTI, MD, PhD Heart Valve Clinic, University of Liège, CHU Sart Tilman, Liège, BELGIUM Aortic Stenosis + Mitral Regurgitation?
The Patient with Aortic Stenosis and Mitral Regurgitation Prof. Patrizio LANCELLOTTI, MD, PhD Heart Valve Clinic, University of Liège, CHU Sart Tilman, Liège, BELGIUM Aortic Stenosis + Mitral Regurgitation?
Ischemic mitral valve reconstruction and replacement: Comparison of long-term survival and complications
 Surgery for Acquired Cardiovascular Disease Ischemic mitral valve reconstruction and replacement: Comparison of long-term survival and complications Eugene A. Grossi, MD Judith D. Goldberg, ScD Angelo
Surgery for Acquired Cardiovascular Disease Ischemic mitral valve reconstruction and replacement: Comparison of long-term survival and complications Eugene A. Grossi, MD Judith D. Goldberg, ScD Angelo
Quality Outcomes Mitral Valve Repair
 Quality Outcomes Mitral Valve Repair Moving Beyond Reoperation Rakesh M. Suri, D.Phil. Professor of Surgery 2015 MFMER 3431548-1 Disclosure Mayo Clinic Division of Cardiovascular Surgery Research funding
Quality Outcomes Mitral Valve Repair Moving Beyond Reoperation Rakesh M. Suri, D.Phil. Professor of Surgery 2015 MFMER 3431548-1 Disclosure Mayo Clinic Division of Cardiovascular Surgery Research funding
Detailed Order Request Checklists for Cardiology
 Next Generation Solutions Detailed Order Request Checklists for Cardiology 8600 West Bryn Mawr Avenue South Tower Suite 800 Chicago, IL 60631 www.aimspecialtyhealth.com Appropriate.Safe.Affordable 2018
Next Generation Solutions Detailed Order Request Checklists for Cardiology 8600 West Bryn Mawr Avenue South Tower Suite 800 Chicago, IL 60631 www.aimspecialtyhealth.com Appropriate.Safe.Affordable 2018
Clinical material and methods. Copyright by ICR Publishers 2003
 Fourteen Years Experience with the CarboMedics Valve in Young Adults with Aortic Valve Disease Jan Aagaard 1, Jens Tingleff 2, Per V. Andersen 1, Christel N. Hansen 2 1 Department of Cardio-Thoracic and
Fourteen Years Experience with the CarboMedics Valve in Young Adults with Aortic Valve Disease Jan Aagaard 1, Jens Tingleff 2, Per V. Andersen 1, Christel N. Hansen 2 1 Department of Cardio-Thoracic and
Hani K. Najm MD, Msc, FRCSC FACC, FESC President Saudi Society for Cardiac Surgeons Associate Professor of Cardiothoracic Surgery King Abdulaziz
 Hani K. Najm MD, Msc, FRCSC FACC, FESC President Saudi Society for Cardiac Surgeons Associate Professor of Cardiothoracic Surgery King Abdulaziz Cardiac Centre Riyadh, Saudi Arabia Decision process for
Hani K. Najm MD, Msc, FRCSC FACC, FESC President Saudi Society for Cardiac Surgeons Associate Professor of Cardiothoracic Surgery King Abdulaziz Cardiac Centre Riyadh, Saudi Arabia Decision process for
SONOGRAPHER & NURSE LED VALVE CLINICS
 SONOGRAPHER & NURSE LED VALVE CLINICS Frequency of visits and alerts AORTIC STENOSIS V max > 4.0 m/s or EOA < 1.0 cm 2 V max 3.5 4.0 m/s + Ca+ V max 3.0 4.0 m/s or EOA 1.0-1.5 cm 2 V max 2.5 3.0 m/s every
SONOGRAPHER & NURSE LED VALVE CLINICS Frequency of visits and alerts AORTIC STENOSIS V max > 4.0 m/s or EOA < 1.0 cm 2 V max 3.5 4.0 m/s + Ca+ V max 3.0 4.0 m/s or EOA 1.0-1.5 cm 2 V max 2.5 3.0 m/s every
Paris, August 28 th Gian Paolo Ussia on behalf of the CoreValve Italian Registry Investigators
 Paris, August 28 th 2011 Is TAVI the definitive treatment in high risk patients? Impact Of Coronary Artery Disease In Elderly Patients Undergoing TAVI: Insight The Italian CoreValve Registry Gian Paolo
Paris, August 28 th 2011 Is TAVI the definitive treatment in high risk patients? Impact Of Coronary Artery Disease In Elderly Patients Undergoing TAVI: Insight The Italian CoreValve Registry Gian Paolo
Frozen Elephant Trunk procedure in patients with aortic dissection type B and concomitant aortic arch or ascending aortic pathology
 Frozen Elephant Trunk procedure in patients with aortic dissection type B and concomitant aortic arch or ascending aortic pathology Eduard Charchyan MD, PhD, Yurii Belov MD, PhD, Denis Breshenkov, Alexey
Frozen Elephant Trunk procedure in patients with aortic dissection type B and concomitant aortic arch or ascending aortic pathology Eduard Charchyan MD, PhD, Yurii Belov MD, PhD, Denis Breshenkov, Alexey
Indications and Late Results of Aortic Valve Repair
 Indications and Late Results of Aortic Valve Repair Prof. Gebrine El Khoury Department of Cardiovascular and Thoracic Surgery Cliniques St. Luc Brussels, Belgium Aortic Valve Repair Question # 1 Can the
Indications and Late Results of Aortic Valve Repair Prof. Gebrine El Khoury Department of Cardiovascular and Thoracic Surgery Cliniques St. Luc Brussels, Belgium Aortic Valve Repair Question # 1 Can the
Joseph E. Bavaria, M.D. Roberts Measy Professor and Vice Chief CardioVascular Surgery Director: Thoracic Aortic Surgery Program University of
 Joseph E. Bavaria, M.D. Roberts Measy Professor and Vice Chief CardioVascular Surgery Director: Thoracic Aortic Surgery Program University of Pennsylvania, USA North American Valve Repair, Philadelphia
Joseph E. Bavaria, M.D. Roberts Measy Professor and Vice Chief CardioVascular Surgery Director: Thoracic Aortic Surgery Program University of Pennsylvania, USA North American Valve Repair, Philadelphia
Kinsing Ko, Thom de Kroon, Najim Kaoui, Bart van Putte, Nabil Saouti. St. Antonius Hospital, Nieuwegein, The Netherlands
 Minimal Invasive Mitral Valve Surgery After Previous Sternotomy Without Aortic Clamping: Short- and Long Term Results of a Single Surgeon Single Institution Kinsing Ko, Thom de Kroon, Najim Kaoui, Bart
Minimal Invasive Mitral Valve Surgery After Previous Sternotomy Without Aortic Clamping: Short- and Long Term Results of a Single Surgeon Single Institution Kinsing Ko, Thom de Kroon, Najim Kaoui, Bart
Hani K. Najm MD, Msc, FRCSC, FRCS (Glasgow), FACC, FESC President of Saudi Heart Association King Abdulaziz Cardiac Centre Riyadh, Saudi Arabia.
, FACC, FESC President of Saudi Heart Association King Abdulaziz Cardiac Centre Riyadh, Saudi Arabia.") Hani K. Najm MD, Msc, FRCSC, FRCS (Glasgow), FACC, FESC President of Saudi Heart Association King Abdulaziz Cardiac Centre Riyadh, Saudi Arabia. Decision process for Management of any valve Timing Feasibility
Hani K. Najm MD, Msc, FRCSC, FRCS (Glasgow), FACC, FESC President of Saudi Heart Association King Abdulaziz Cardiac Centre Riyadh, Saudi Arabia. Decision process for Management of any valve Timing Feasibility
EACTS Adult Cardiac Database
 EACTS Adult Cardiac Database Quality Improvement Programme List of changes to Version 2.0, 13 th Dec 2018, compared to version 1.0, 1 st May 2014. INTRODUCTORY NOTES This document s purpose is to list
EACTS Adult Cardiac Database Quality Improvement Programme List of changes to Version 2.0, 13 th Dec 2018, compared to version 1.0, 1 st May 2014. INTRODUCTORY NOTES This document s purpose is to list
Joseph E. Bavaria, M.D. Roberts Measy Professor and Vice Chief CardioVascular Surgery Director: Thoracic Aortic Surgery Program University of
 Joseph E. Bavaria, M.D. Roberts Measy Professor and Vice Chief CardioVascular Surgery Director: Thoracic Aortic Surgery Program University of Pennsylvania, USA AVRS Philadelphia Sept 2016 Pictures courtesy
Joseph E. Bavaria, M.D. Roberts Measy Professor and Vice Chief CardioVascular Surgery Director: Thoracic Aortic Surgery Program University of Pennsylvania, USA AVRS Philadelphia Sept 2016 Pictures courtesy
Supplementary Online Content
 Supplementary Online Content Inohara T, Manandhar P, Kosinski A, et al. Association of renin-angiotensin inhibitor treatment with mortality and heart failure readmission in patients with transcatheter
Supplementary Online Content Inohara T, Manandhar P, Kosinski A, et al. Association of renin-angiotensin inhibitor treatment with mortality and heart failure readmission in patients with transcatheter
Clinical material and methods. Fukui Cardiovascular Center, Fukui, Japan
 Mitral Valve Regurgitation after Atrial Septal Defect Repair in Adults Shohei Yoshida, Satoshi Numata, Yasushi Tsutsumi, Osamu Monta, Sachiko Yamazaki, Hiroyuki Seo, Takaaki Samura, Hirokazu Ohashi Fukui
Mitral Valve Regurgitation after Atrial Septal Defect Repair in Adults Shohei Yoshida, Satoshi Numata, Yasushi Tsutsumi, Osamu Monta, Sachiko Yamazaki, Hiroyuki Seo, Takaaki Samura, Hirokazu Ohashi Fukui
Surgical AVR: Are there any contraindications? Pyowon Park Samsung Medical Center Seoul, Korea
 Surgical AVR: Are there any contraindications? Pyowon Park Samsung Medical Center Seoul, Korea Contents Decision making in surgical AVR in old age Clinical results of AVR with tissue valve Impact of 19mm
Surgical AVR: Are there any contraindications? Pyowon Park Samsung Medical Center Seoul, Korea Contents Decision making in surgical AVR in old age Clinical results of AVR with tissue valve Impact of 19mm
Reconstruction of the Aortic Valve and Root A Practical approach Why and when to repair the aortic valve. Diana Aicher. September 16 th - 18 th 2015
 Reconstruction of the Aortic Valve and Root A Practical approach Why and when to repair the aortic valve Diana Aicher September 16 th - 18 th 2015 Why repair the aortic valve? Aortic Valve Replacement
Reconstruction of the Aortic Valve and Root A Practical approach Why and when to repair the aortic valve Diana Aicher September 16 th - 18 th 2015 Why repair the aortic valve? Aortic Valve Replacement
Outcomes of Mitral Valve Repair for Mitral Regurgitation Due to Degenerative Disease
 Outcomes of Mitral Valve Repair for Mitral Regurgitation Due to Degenerative Disease TIRONE E. DAVID, MD ; SEMIN THORAC CARDIOVASC SURG 19:116-120c 2007 ELSEVIER INC. PRESENTED BY INTERN 許士盟 Mitral valve
Outcomes of Mitral Valve Repair for Mitral Regurgitation Due to Degenerative Disease TIRONE E. DAVID, MD ; SEMIN THORAC CARDIOVASC SURG 19:116-120c 2007 ELSEVIER INC. PRESENTED BY INTERN 許士盟 Mitral valve
Prosthetic valve dysfunction: stenosis or regurgitation
 Prosthetic valve dysfunction: stenosis or regurgitation Jean G. Dumesnil MD, FRCP(C), FACC, FASE(Hon) Quebec Heart and Lung Institute, Québec, Québec No disclosures Possible Causes of High Gradients in
Prosthetic valve dysfunction: stenosis or regurgitation Jean G. Dumesnil MD, FRCP(C), FACC, FASE(Hon) Quebec Heart and Lung Institute, Québec, Québec No disclosures Possible Causes of High Gradients in
Early and One-year Outcomes of Aortic Root Surgery in Marfan Syndrome Patients
 Early and One-year Outcomes of Aortic Root Surgery in Marfan Syndrome Patients A Prospective, Multi-Center, Comparative Study Joseph S. Coselli, Irina V. Volguina, Scott A. LeMaire, Thoralf M. Sundt, Elizabeth
Early and One-year Outcomes of Aortic Root Surgery in Marfan Syndrome Patients A Prospective, Multi-Center, Comparative Study Joseph S. Coselli, Irina V. Volguina, Scott A. LeMaire, Thoralf M. Sundt, Elizabeth
42yr Old Male with Severe AR Mild LV dysfunction s/p TOF -AV Replacement(tissue valve) or AoV plasty- Kyung-Hwan Kim
 or AoV plasty- Kyung-Hwan Kim") 42yr Old Male with Severe AR Mild LV dysfunction s/p TOF -AV Replacement(tissue valve) or AoV plasty- Kyung-Hwan Kim Current Guideline for AR s/p TOF Surgery is reasonable in adults with prior repair of
42yr Old Male with Severe AR Mild LV dysfunction s/p TOF -AV Replacement(tissue valve) or AoV plasty- Kyung-Hwan Kim Current Guideline for AR s/p TOF Surgery is reasonable in adults with prior repair of
The production of murmurs is due to 3 main factors:
 Heart murmurs The production of murmurs is due to 3 main factors: high blood flow rate through normal or abnormal orifices forward flow through a narrowed or irregular orifice into a dilated vessel or
Heart murmurs The production of murmurs is due to 3 main factors: high blood flow rate through normal or abnormal orifices forward flow through a narrowed or irregular orifice into a dilated vessel or
Indication, Timing, Assessment and Update on TAVI
 Indication, Timing, Assessment and Update on TAVI Swedish Heart and Vascular Institute Ming Zhang MD PhD Interventional Cardiology Structure Heart Disease Conflict of Interest None Starr- Edwards Mechanical
Indication, Timing, Assessment and Update on TAVI Swedish Heart and Vascular Institute Ming Zhang MD PhD Interventional Cardiology Structure Heart Disease Conflict of Interest None Starr- Edwards Mechanical
A Surgeon s Perspective Guidelines for the Management of Patients with Valvular Heart Disease Adapted from the 2006 ACC/AHA Guideline Revision
 A Surgeon s Perspective Guidelines for the Management of Patients with Valvular Heart Disease Adapted from the 2006 ACC/AHA Guideline Revision Prof. Pino Fundarò, MD Niguarda Hospital Milan, Italy Introduction
A Surgeon s Perspective Guidelines for the Management of Patients with Valvular Heart Disease Adapted from the 2006 ACC/AHA Guideline Revision Prof. Pino Fundarò, MD Niguarda Hospital Milan, Italy Introduction
The operative mortality rate after redo valvular operations
 Clinical Outcomes of Redo Valvular Operations: A 20-Year Experience Naoto Fukunaga, MD, Yukikatsu Okada, MD, Yasunobu Konishi, MD, Takashi Murashita, MD, Mitsuru Yuzaki, MD, Yu Shomura, MD, Hiroshi Fujiwara,
Clinical Outcomes of Redo Valvular Operations: A 20-Year Experience Naoto Fukunaga, MD, Yukikatsu Okada, MD, Yasunobu Konishi, MD, Takashi Murashita, MD, Mitsuru Yuzaki, MD, Yu Shomura, MD, Hiroshi Fujiwara,
CIPG Transcatheter Aortic Valve Replacement- When Is Less, More?
 CIPG 2013 Transcatheter Aortic Valve Replacement- When Is Less, More? James D. Rossen, M.D. Professor of Medicine and Neurosurgery Director, Cardiac Catheterization Laboratory and Interventional Cardiology
CIPG 2013 Transcatheter Aortic Valve Replacement- When Is Less, More? James D. Rossen, M.D. Professor of Medicine and Neurosurgery Director, Cardiac Catheterization Laboratory and Interventional Cardiology
Prosthesis-Patient Mismatch in High Risk Patients with Severe Aortic Stenosis in a Randomized Trial of a Self-Expanding Prosthesis
 Prosthesis-Patient Mismatch in High Risk Patients with Severe Aortic Stenosis in a Randomized Trial of a Self-Expanding Prosthesis George L. Zorn, III On Behalf of the CoreValve US Clinical Investigators
Prosthesis-Patient Mismatch in High Risk Patients with Severe Aortic Stenosis in a Randomized Trial of a Self-Expanding Prosthesis George L. Zorn, III On Behalf of the CoreValve US Clinical Investigators
Reconstruction of the Aortic Valve and Root A Practical approach Failures after aortic valve repair. Diana Aicher. September 16 th -18 th 2015
 Reconstruction of the Aortic Valve and Root A Practical approach Failures after aortic valve repair Diana Aicher September 16 th -18 th 2015 Classification of failures- root repair 51/810 acute/ intraoperative
Reconstruction of the Aortic Valve and Root A Practical approach Failures after aortic valve repair Diana Aicher September 16 th -18 th 2015 Classification of failures- root repair 51/810 acute/ intraoperative
Clinical outcomes of aortic root replacement after previous aortic root replacement
 Clinical outcomes of aortic root replacement after previous aortic root replacement Luis Garrido-Olivares, MD, MSc, Manjula Maganti, MSc, Susan Armstrong, MSc, and Tirone E. David, MD Objective: The study
Clinical outcomes of aortic root replacement after previous aortic root replacement Luis Garrido-Olivares, MD, MSc, Manjula Maganti, MSc, Susan Armstrong, MSc, and Tirone E. David, MD Objective: The study
Aortic root reconstructive surgery - new created technique for aortic stenosis
 Aortic root reconstructive surgery - new created technique for aortic stenosis Reconstructive surgery of the aortic root Academician d-r Zan Mitrev, T.Anguseva, E.Stoicovski, E Idoski Special hospital
Aortic root reconstructive surgery - new created technique for aortic stenosis Reconstructive surgery of the aortic root Academician d-r Zan Mitrev, T.Anguseva, E.Stoicovski, E Idoski Special hospital
-The Living Aortic Valve- Repair or Else? Ismail El-Hamamsy, MD PhD
 -The Living Aortic Valve- Repair or Else? Ismail El-Hamamsy, MD PhD Associate Professor Director, Aortic Surgery Division of Cardiac Surgery Montreal Heart Institute Université de Montreal PhD Thesis Imperial
-The Living Aortic Valve- Repair or Else? Ismail El-Hamamsy, MD PhD Associate Professor Director, Aortic Surgery Division of Cardiac Surgery Montreal Heart Institute Université de Montreal PhD Thesis Imperial
Candice Silversides, MD Toronto Congenital Cardiac Centre for Adults University of Toronto Toronto, Canada
 PVR Following Repair of TOF Now? When? Candice Silversides, MD Toronto Congenital Cardiac Centre for Adults University of Toronto Toronto, Canada Late Complications after TOF repair Repair will be necessary
PVR Following Repair of TOF Now? When? Candice Silversides, MD Toronto Congenital Cardiac Centre for Adults University of Toronto Toronto, Canada Late Complications after TOF repair Repair will be necessary
PPM: How to fit a big valve in a small heart
 PPM: How to fit a big valve in a small heart Hani K. Najm MD, Msc, FRCSC, FRCS (Glasgow), FACC, FESC King Abdulaziz Cardiac Centre National Guard Health Affairs Riyadh, Saudi Arabia GHA meeting Muscat
PPM: How to fit a big valve in a small heart Hani K. Najm MD, Msc, FRCSC, FRCS (Glasgow), FACC, FESC King Abdulaziz Cardiac Centre National Guard Health Affairs Riyadh, Saudi Arabia GHA meeting Muscat
The application of autologous pulmonary artery in surgical correction of complicated aortic arch anomaly
 Original Article The application of autologous pulmonary artery in surgical correction of complicated aortic arch anomaly Shusheng Wen, Jianzheng Cen, Jimei Chen, Gang Xu, Biaochuan He, Yun Teng, Jian
Original Article The application of autologous pulmonary artery in surgical correction of complicated aortic arch anomaly Shusheng Wen, Jianzheng Cen, Jimei Chen, Gang Xu, Biaochuan He, Yun Teng, Jian
Australia and New Zealand Source Registry Edwards Sapien Aortic Valve 30 day Outcomes
 Australia and New Zealand Source Registry Edwards Sapien Aortic Valve 30 day Outcomes A/ Professor Darren Walters On behalf of the ANZ Source Investigators Director of Cardiology Brisbane, Australia ANZ
Australia and New Zealand Source Registry Edwards Sapien Aortic Valve 30 day Outcomes A/ Professor Darren Walters On behalf of the ANZ Source Investigators Director of Cardiology Brisbane, Australia ANZ
Chapter 24: Diagnostic workup and evaluation: eligibility, risk assessment, FDA guidelines Ashwin Nathan, MD, Saif Anwaruddin, MD, FACC Penn Medicine
 Chapter 24: Diagnostic workup and evaluation: eligibility, risk assessment, FDA guidelines Ashwin Nathan, MD, Saif Anwaruddin, MD, FACC Penn Medicine Mitral regurgitation, regurgitant flow between the
Chapter 24: Diagnostic workup and evaluation: eligibility, risk assessment, FDA guidelines Ashwin Nathan, MD, Saif Anwaruddin, MD, FACC Penn Medicine Mitral regurgitation, regurgitant flow between the
Catheter-based mitral valve repair MitraClip System
 Percutaneous Mitral Valve Repair: Results of the EVEREST II Trial William A. Gray MD Director of Endovascular Services Associate Professor of Clinical Medicine Columbia University Medical Center The Cardiovascular
Percutaneous Mitral Valve Repair: Results of the EVEREST II Trial William A. Gray MD Director of Endovascular Services Associate Professor of Clinical Medicine Columbia University Medical Center The Cardiovascular
Emergency Intraoperative Echocardiography
 Emergency Intraoperative Echocardiography Justiaan Swanevelder Department of Anaesthesia, Glenfield Hospital University Hospitals of Leicester NHS Trust, UK Carl Gustav Jung (1875-1961) Your vision will
Emergency Intraoperative Echocardiography Justiaan Swanevelder Department of Anaesthesia, Glenfield Hospital University Hospitals of Leicester NHS Trust, UK Carl Gustav Jung (1875-1961) Your vision will
Effect of Valve Suture Technique on Incidence of Paraprosthetic Regurgitation and 10-Year Survival
 Effect of Valve Suture Technique on Incidence of Paraprosthetic Regurgitation and 10-Year Survival Sukumaran K. Nair, FRCS (C Th), Gauraang Bhatnagar, MBBS, Oswaldo Valencia, MD, and Venkatachalam Chandrasekaran,
Effect of Valve Suture Technique on Incidence of Paraprosthetic Regurgitation and 10-Year Survival Sukumaran K. Nair, FRCS (C Th), Gauraang Bhatnagar, MBBS, Oswaldo Valencia, MD, and Venkatachalam Chandrasekaran,
Aortic Valve Practice Guidelines: What Has Changed and What You Need to Know
 Aortic Valve Practice Guidelines: What Has Changed and What You Need to Know James F. Burke, MD Program Director Cardiovascular Disease Fellowship Lankenau Medical Center Disclosure Dr. Burke has no conflicts
Aortic Valve Practice Guidelines: What Has Changed and What You Need to Know James F. Burke, MD Program Director Cardiovascular Disease Fellowship Lankenau Medical Center Disclosure Dr. Burke has no conflicts
Department of Cardiothoracic Surgery, Heart and Lung Center, Lund University Hospital, Lund, Sweden
 Long-Term Outcome of the Mitroflow Pericardial Bioprosthesis in the Elderly after Aortic Valve Replacement Johan Sjögren, Tomas Gudbjartsson, Lars I. Thulin Department of Cardiothoracic Surgery, Heart
Long-Term Outcome of the Mitroflow Pericardial Bioprosthesis in the Elderly after Aortic Valve Replacement Johan Sjögren, Tomas Gudbjartsson, Lars I. Thulin Department of Cardiothoracic Surgery, Heart
Indications of Coronary Angiography Dr. Shaheer K. George, M.D Faculty of Medicine, Mansoura University 2014
 Indications of Coronary Angiography Dr. Shaheer K. George, M.D Faculty of Medicine, Mansoura University 2014 Indications for cardiac catheterization Before a decision to perform an invasive procedure such
Indications of Coronary Angiography Dr. Shaheer K. George, M.D Faculty of Medicine, Mansoura University 2014 Indications for cardiac catheterization Before a decision to perform an invasive procedure such
Severity of AS Degree of AV calcification (? Bicuspid AV), annulus size, & aortic root
, annulus size, & aortic root") The role of Cardiac Imaging modalities in evaluation & selection of patients for Trans-catheter Aortic Valve Implantation Dr.Saeed AL Ahmari Consultant Cardiologist Prince Sultan Cardaic Center, Riyadh
The role of Cardiac Imaging modalities in evaluation & selection of patients for Trans-catheter Aortic Valve Implantation Dr.Saeed AL Ahmari Consultant Cardiologist Prince Sultan Cardaic Center, Riyadh
Cardiac MRI in ACHD What We. ACHD Patients
 Cardiac MRI in ACHD What We Have Learned to Apply to ACHD Patients Faris Al Mousily, MBChB, FAAC, FACC Consultant, Pediatric Cardiology, KFSH&RC/Jeddah Adjunct Faculty, Division of Pediatric Cardiology
Cardiac MRI in ACHD What We Have Learned to Apply to ACHD Patients Faris Al Mousily, MBChB, FAAC, FACC Consultant, Pediatric Cardiology, KFSH&RC/Jeddah Adjunct Faculty, Division of Pediatric Cardiology
Outcomes of Surgical Aortic Valve Replacement in Moderate Risk Patients: Implications for Determination of Equipoise in the Transcatheter Era
 Outcomes of Surgical Aortic Valve Replacement in Moderate Risk Patients: Implications for Determination of Equipoise in the Transcatheter Era Sebastian A. Iturra, Rakesh M. Suri, Kevin L. Greason, John
Outcomes of Surgical Aortic Valve Replacement in Moderate Risk Patients: Implications for Determination of Equipoise in the Transcatheter Era Sebastian A. Iturra, Rakesh M. Suri, Kevin L. Greason, John
Focused. se with 2008 F. lar Heart Diseas. date. ents With Valvul. Upd. gement of Patie. lines for Manag. HA 2006 Guidel ACC/AH. Fig.
 ACC/AH HA 2006 Guidel nic severe AI (Fig. 4). ned by age, ay also be helpful nd echo. For AI, ollow up may be or MRI rather than mension; SD, end lines for Manag gement of Patie Upd ents With Valvul date
ACC/AH HA 2006 Guidel nic severe AI (Fig. 4). ned by age, ay also be helpful nd echo. For AI, ollow up may be or MRI rather than mension; SD, end lines for Manag gement of Patie Upd ents With Valvul date
14 Valvular Stenosis
 14 Valvular Stenosis 14-1. Valvular Stenosis unicuspid valve FIGUE 14-1. This photograph shows severe valvular stenosis as it occurs in a newborn. There is a unicuspid, horseshoe-shaped leaflet with a
14 Valvular Stenosis 14-1. Valvular Stenosis unicuspid valve FIGUE 14-1. This photograph shows severe valvular stenosis as it occurs in a newborn. There is a unicuspid, horseshoe-shaped leaflet with a
Gender Differences in Valvular Heart Disease. Linda D. Gillam, MD FESC Disclosure: Core Lab services Edwards Lifesciences
 Gender Differences in Valvular Heart Disease Linda D. Gillam, MD FESC Disclosure: Core Lab services Edwards Lifesciences Obstacles Interest in gender differences is a relatively new phenomenon Registries/RCT
Gender Differences in Valvular Heart Disease Linda D. Gillam, MD FESC Disclosure: Core Lab services Edwards Lifesciences Obstacles Interest in gender differences is a relatively new phenomenon Registries/RCT
State of the art in reconstruction of the ascending aorta with or without valve reconstruction
 State of the art in reconstruction of the ascending aorta with or without valve reconstruction PD Dr Diana Aicher Universitätskliniken des Saarlandes Homburg/Germany ESBV Straßbourg, May 10 2013 Background
State of the art in reconstruction of the ascending aorta with or without valve reconstruction PD Dr Diana Aicher Universitätskliniken des Saarlandes Homburg/Germany ESBV Straßbourg, May 10 2013 Background
Ejection across stenotic aortic valve requires a systolic pressure gradient between the LV and aorta. This places a pressure load on the LV.
 Valvular Heart Disease Etiology General Principles Cellular and molecular mechanism of valve damage Structural pathology Functional pathology - stenosis/regurgitation Loading conditions - pressure/volume
Valvular Heart Disease Etiology General Principles Cellular and molecular mechanism of valve damage Structural pathology Functional pathology - stenosis/regurgitation Loading conditions - pressure/volume
Durability and Outcome of Aortic Valve Replacement With Mitral Valve Repair Versus Double Valve Replacement
 Durability and Outcome of Aortic Valve Replacement With Mitral Valve Repair Versus Double Valve Replacement Masaki Hamamoto, MD, Ko Bando, MD, Junjiro Kobayashi, MD, Toshihiko Satoh, MD, MPH, Yoshikado
Durability and Outcome of Aortic Valve Replacement With Mitral Valve Repair Versus Double Valve Replacement Masaki Hamamoto, MD, Ko Bando, MD, Junjiro Kobayashi, MD, Toshihiko Satoh, MD, MPH, Yoshikado
DECISION MAKING DEL CARDIOCHIRURGO NELL INSUFFICIENZA MITRALICA: ISTRUZIONI D USO D CARDIOLOGO
 DECISION MAKING DEL CARDIOCHIRURGO NELL INSUFFICIENZA MITRALICA: ISTRUZIONI D USO D PER IL CARDIOLOGO GUIDELINES IN ASYMPTOMATIC MR ACC/AHA ESC Antonio Miceli Heart Hospital Monasterio Foundation NATURAL/
DECISION MAKING DEL CARDIOCHIRURGO NELL INSUFFICIENZA MITRALICA: ISTRUZIONI D USO D PER IL CARDIOLOGO GUIDELINES IN ASYMPTOMATIC MR ACC/AHA ESC Antonio Miceli Heart Hospital Monasterio Foundation NATURAL/
PROSTHETIC VALVE BOARD REVIEW
 PROSTHETIC VALVE BOARD REVIEW The correct answer D This two chamber view shows a porcine mitral prosthesis with the typical appearance of the struts although the leaflets are not well seen. The valve
PROSTHETIC VALVE BOARD REVIEW The correct answer D This two chamber view shows a porcine mitral prosthesis with the typical appearance of the struts although the leaflets are not well seen. The valve
Influence of Atrial Fibrillation on Outcome Following Mitral Valve Repair
 Influence of Atrial Fibrillation on Outcome Following Mitral Valve Repair Eric Lim, MBChB, MRCS; Clifford W. Barlow, DPhil, FRCS; A. Reza Hosseinpour, FRCS; Christopher Wisbey, BA; Kate Wilson, RN, BSc;
Influence of Atrial Fibrillation on Outcome Following Mitral Valve Repair Eric Lim, MBChB, MRCS; Clifford W. Barlow, DPhil, FRCS; A. Reza Hosseinpour, FRCS; Christopher Wisbey, BA; Kate Wilson, RN, BSc;
Mitral Gradients and Frequency of Recurrence of Mitral Regurgitation After Ring Annuloplasty for Ischemic Mitral Regurgitation
 Mitral Gradients and Frequency of Recurrence of Mitral Regurgitation After Ring Annuloplasty for Ischemic Mitral Regurgitation Matthew L. Williams, MD, Mani A. Daneshmand, MD, James G. Jollis, MD, John
Mitral Gradients and Frequency of Recurrence of Mitral Regurgitation After Ring Annuloplasty for Ischemic Mitral Regurgitation Matthew L. Williams, MD, Mani A. Daneshmand, MD, James G. Jollis, MD, John
The Bicuspid AV Surgical Conisiderations
 The Bicuspid AV Surgical Conisiderations Ehud Raanani, MD Cardiothoracic Surgery, Sheba Medical Center Sackler School of Medicine, Tel Aviv University MAY 15, 2014 Homburg BAV Repair Congenital variations
The Bicuspid AV Surgical Conisiderations Ehud Raanani, MD Cardiothoracic Surgery, Sheba Medical Center Sackler School of Medicine, Tel Aviv University MAY 15, 2014 Homburg BAV Repair Congenital variations
Clinical Outcome in Patients with Aortic Stenosis
 Clinical Outcome in Patients with Aortic Stenosis Is the Prognosis Worse in Patients with Low-Gradient Severe Aortic Stenosis? Yoel Angel BSc, Shemy Carasso MD, Diab Mutlak MD, Jonathan Lessick MD Dsc,
Clinical Outcome in Patients with Aortic Stenosis Is the Prognosis Worse in Patients with Low-Gradient Severe Aortic Stenosis? Yoel Angel BSc, Shemy Carasso MD, Diab Mutlak MD, Jonathan Lessick MD Dsc,
The production of murmurs is due to 3 main factors:
 Heart murmurs The production of murmurs is due to 3 main factors: high blood flow rate through normal or abnormal orifices forward flow through a narrowed or irregular orifice into a dilated vessel or
Heart murmurs The production of murmurs is due to 3 main factors: high blood flow rate through normal or abnormal orifices forward flow through a narrowed or irregular orifice into a dilated vessel or
Aortic valve repair: When and how to employ this novel approach?
 Aortic valve repair: When and how to employ this novel approach? Konstadinos A Plestis, MD System Chief of Cardiac Thoracic and Vascular Surgery Main Line Health Care System Professor Sidney Kimmel Medical
Aortic valve repair: When and how to employ this novel approach? Konstadinos A Plestis, MD System Chief of Cardiac Thoracic and Vascular Surgery Main Line Health Care System Professor Sidney Kimmel Medical
Percutaneous Mitral Valve Repair
 Percutaneous Mitral Valve Repair MitraClip: Procedure, Data, Patient Selection Chad Rammohan, MD FACC Director, Cardiac Cath Lab El Camino Hospital Mountain View, California Mitral Regurgitation MitraClip
Percutaneous Mitral Valve Repair MitraClip: Procedure, Data, Patient Selection Chad Rammohan, MD FACC Director, Cardiac Cath Lab El Camino Hospital Mountain View, California Mitral Regurgitation MitraClip
Strategies for the High Risk Redo in CHD
 Strategies for the High Risk Redo in CHD Joseph A. Dearani, MD AATS, Minneapolis 2013 Strategies for the High Risk Redo in CHD Joseph A. Dearani, MD AATS, Minneapolis 2013 No Disclosures 2011 MFMER slide-3
Strategies for the High Risk Redo in CHD Joseph A. Dearani, MD AATS, Minneapolis 2013 Strategies for the High Risk Redo in CHD Joseph A. Dearani, MD AATS, Minneapolis 2013 No Disclosures 2011 MFMER slide-3
Ejection across stenotic aortic valve requires a systolic pressure gradient between the LV and aorta. This places a pressure load on the LV.
 Valvular Heart Disease General Principles Etiology Cellular and molecular mechanism of valve damage Structural pathology Functional pathology - stenosis/regurgitation Loading conditions - pressure/volume
Valvular Heart Disease General Principles Etiology Cellular and molecular mechanism of valve damage Structural pathology Functional pathology - stenosis/regurgitation Loading conditions - pressure/volume
ACD. Tirone E. David, MD, Christopher M. Feindel, MD, Susan Armstrong, MSc, and Manjula Maganti, MSc
 Replacement of the ascending aorta with reduction of the diameter of the sinotubular junction to treat aortic insufficiency in patients with ascending aortic aneurysm Tirone E. David, MD, Christopher M.
Replacement of the ascending aorta with reduction of the diameter of the sinotubular junction to treat aortic insufficiency in patients with ascending aortic aneurysm Tirone E. David, MD, Christopher M.
An Update on the Edwards TAVR Results. Zvonimir Krajcer, MD Director, Peripheral Intervention Texas Heart Institute at St.
 An Update on the Edwards TAVR Results Zvonimir Krajcer, MD Director, Peripheral Intervention Texas Heart Institute at St. Luke s Hospital Disclosures On the speaker s bureau for Endologix, TriVascular,
An Update on the Edwards TAVR Results Zvonimir Krajcer, MD Director, Peripheral Intervention Texas Heart Institute at St. Luke s Hospital Disclosures On the speaker s bureau for Endologix, TriVascular,
Excellence in heart and lung care. Royal Brompton Hospital, Sydney Street, London SW3 6NP
 The Surgical Management of the Bicuspid Aortic Valve in Children Professor D.F Shore Royal Brompton & Harefield NHS Trust Excellence in heart and lung care Royal Brompton Hospital, Sydney Street, London
The Surgical Management of the Bicuspid Aortic Valve in Children Professor D.F Shore Royal Brompton & Harefield NHS Trust Excellence in heart and lung care Royal Brompton Hospital, Sydney Street, London
Ross introduced the replacement of a diseased aortic. The Ross Operation: An Evaluation of a Single Institution s Experience
 The Ross Operation: An Evaluation of a Single Institution s Experience Fabrizio Settepani, MD Abdullah Kaya, MD, Wim J. Morshuis, MD, PhD, Marc A. Schepens, MD, PhD, Robin H. Heijmen, MD, PhD, and Karl
The Ross Operation: An Evaluation of a Single Institution s Experience Fabrizio Settepani, MD Abdullah Kaya, MD, Wim J. Morshuis, MD, PhD, Marc A. Schepens, MD, PhD, Robin H. Heijmen, MD, PhD, and Karl
Risk Analysis of the Long-Term Outcomes of the Surgical Closure of Secundum Atrial Septal Defects
 Korean J Thorac Cardiovasc Surg 2017;50:78-85 ISSN: 2233-601X (Print) ISSN: 2093-6516 (Online) CLINICAL RESEARCH https://doi.org/10.5090/kjtcs.2017.50.2.78 Risk Analysis of the Long-Term Outcomes of the
Korean J Thorac Cardiovasc Surg 2017;50:78-85 ISSN: 2233-601X (Print) ISSN: 2093-6516 (Online) CLINICAL RESEARCH https://doi.org/10.5090/kjtcs.2017.50.2.78 Risk Analysis of the Long-Term Outcomes of the
Outcome of elderly patients with severe but asymptomatic aortic stenosis
 Outcome of elderly patients with severe but asymptomatic aortic stenosis Robert Zilberszac, Harald Gabriel, Gerald Maurer, Raphael Rosenhek Department of Cardiology Medical University of Vienna ESC Congress
Outcome of elderly patients with severe but asymptomatic aortic stenosis Robert Zilberszac, Harald Gabriel, Gerald Maurer, Raphael Rosenhek Department of Cardiology Medical University of Vienna ESC Congress
Valvular Heart Disease
 Valvular Heart Disease B K Singh, MD, FACC Disclosures: None 1 CARDIAC CYCLE S2 S2=A2P2 S1=M1T1 S4 S1 S3 2 JVP Carotid S1 Slitting of S2 S3 S4 Ejection click Opening snap Dynamic Auscultation What is the
Valvular Heart Disease B K Singh, MD, FACC Disclosures: None 1 CARDIAC CYCLE S2 S2=A2P2 S1=M1T1 S4 S1 S3 2 JVP Carotid S1 Slitting of S2 S3 S4 Ejection click Opening snap Dynamic Auscultation What is the
Reconstructive surgery of the aortic root
 Reconstructive surgery of the aortic root Reconstructive surgery of the aortic root Academician d-r Zan Mitrev MDFETCS Special hospital for surgery Fillip II Skopje - Macedonia february, 2011 Reconstructive
Reconstructive surgery of the aortic root Reconstructive surgery of the aortic root Academician d-r Zan Mitrev MDFETCS Special hospital for surgery Fillip II Skopje - Macedonia february, 2011 Reconstructive
Introducing the COAPT Trial
 physician INFORMATION Eligible patients Symptomatic functional mitral regurgitation 3+ Not suitable candidates for open mitral valve surgery NYHA functional class II, III, or ambulatory IV Introducing
physician INFORMATION Eligible patients Symptomatic functional mitral regurgitation 3+ Not suitable candidates for open mitral valve surgery NYHA functional class II, III, or ambulatory IV Introducing
The Bicuspid AV Surgical Considerations
 The Bicuspid AV Surgical Considerations Ehud Raanani, MD Cardiothoracic Surgery, Sheba Medical Center Sackler School of Medicine, Tel Aviv University September 12, 2014 Homburg BAV Repair Congenital variations
The Bicuspid AV Surgical Considerations Ehud Raanani, MD Cardiothoracic Surgery, Sheba Medical Center Sackler School of Medicine, Tel Aviv University September 12, 2014 Homburg BAV Repair Congenital variations
Pregnancy, Heart Disease and Imaging. Hemodynamics. Decreased systemic vascular resistance. Physiology anemia
 Pregnancy, Heart Disease and Imaging Sangeeta Shah, MD, FASE, FACC Associate Professor, Ochsner Clinical School of Medicine Advanced CV Imaging and Adult Congenital Heart Disease New Orleans, LA Hemodynamics
Pregnancy, Heart Disease and Imaging Sangeeta Shah, MD, FASE, FACC Associate Professor, Ochsner Clinical School of Medicine Advanced CV Imaging and Adult Congenital Heart Disease New Orleans, LA Hemodynamics
Carpentier-Edwards Pericardial Valve in the Aortic Position: 25-Years Experience
 SURGERY: The Annals of Thoracic Surgery CME Program is located online at http://www.annalsthoracicsurgery.org/cme/ home. To take the CME activity related to this article, you must have either an STS member
SURGERY: The Annals of Thoracic Surgery CME Program is located online at http://www.annalsthoracicsurgery.org/cme/ home. To take the CME activity related to this article, you must have either an STS member
Outline. EuroScore II. Society of Thoracic Surgeons Score. EuroScore II
 SURGICAL RISK IN VALVULAR HEART DISEASE: WHAT 2D AND 3D ECHO CAN TELL YOU AND WHAT THEY CAN'T Ernesto E Salcedo, MD Professor of Medicine University of Colorado School of Medicine Director of Echocardiography
SURGICAL RISK IN VALVULAR HEART DISEASE: WHAT 2D AND 3D ECHO CAN TELL YOU AND WHAT THEY CAN'T Ernesto E Salcedo, MD Professor of Medicine University of Colorado School of Medicine Director of Echocardiography
7. Echocardiography Appropriate Use Criteria (by Indication)
") Criteria for Echocardiography 1133 7. Echocardiography Criteria (by ) Table 1. TTE for General Evaluation of Cardiac Structure and Function Suspected Cardiac Etiology General With TTE 1. Symptoms or conditions
Criteria for Echocardiography 1133 7. Echocardiography Criteria (by ) Table 1. TTE for General Evaluation of Cardiac Structure and Function Suspected Cardiac Etiology General With TTE 1. Symptoms or conditions
Edwards Transcatheter AVR: Have the Outcomes Changed after CE Approval?
 Edwards Transcatheter AVR: Have the Outcomes Changed after CE Approval? Update from PARTNER EU and SOURCE Registries T. Lefèvre Disclosure Statement Cardiologist Interventional cardiologist 1 st PABV in
Edwards Transcatheter AVR: Have the Outcomes Changed after CE Approval? Update from PARTNER EU and SOURCE Registries T. Lefèvre Disclosure Statement Cardiologist Interventional cardiologist 1 st PABV in
MATRIX VHD FORM. State the name of the patient ( Product Recipient ) for whom you are providing the information contained in this form.
 for whom you are providing the information contained in this form.") MATRIX VHD FORM A. Patient Information State the name of the patient ( Product Recipient ) for whom you are providing the information contained in this form. (First Name) (Middle Initial) (Last Name) (Date
MATRIX VHD FORM A. Patient Information State the name of the patient ( Product Recipient ) for whom you are providing the information contained in this form. (First Name) (Middle Initial) (Last Name) (Date
Re-do aortic valve replacement after previous homograft aortic root replacement
 Re-do aortic valve replacement after previous homograft aortic root replacement Jullien Gaer, Toufan Bahrami, Fabio de Robertis, Ahmed Abdulsalam, John Pepper, NHS Foundation Trust, UK Professor Sir Magdi
Re-do aortic valve replacement after previous homograft aortic root replacement Jullien Gaer, Toufan Bahrami, Fabio de Robertis, Ahmed Abdulsalam, John Pepper, NHS Foundation Trust, UK Professor Sir Magdi
Annular Stabilization Techniques in the Context of Aortic Valve Repair
 Annular Stabilization Techniques in the Context of Aortic Valve Repair Prashanth Vallabhajosyula, MD MS University of Pennsylvania, Philadelphia, Pennsylvania 2 nd North American Aortic Valve Repair Symposium
Annular Stabilization Techniques in the Context of Aortic Valve Repair Prashanth Vallabhajosyula, MD MS University of Pennsylvania, Philadelphia, Pennsylvania 2 nd North American Aortic Valve Repair Symposium
TRANSCATHETER AORTIC VALVE IMPLANTATION: PSCC EXPERIENCE DR HUSSEIN ALAMRI PSCC RIYADH
 TRANSCATHETER AORTIC VALVE IMPLANTATION: PSCC EXPERIENCE DR HUSSEIN ALAMRI PSCC RIYADH Available systems: Edwards (TA and TF) and Core valve. INTRODUCTION 3 4% 0f > 65 y. 30 40% of elderly denied surgery,.
TRANSCATHETER AORTIC VALVE IMPLANTATION: PSCC EXPERIENCE DR HUSSEIN ALAMRI PSCC RIYADH Available systems: Edwards (TA and TF) and Core valve. INTRODUCTION 3 4% 0f > 65 y. 30 40% of elderly denied surgery,.