Reverse (fluid) resuscitation Should we be doing it? NAHLA IRTIZA ISMAIL
|
|
|
- Antony Garrison
- 5 years ago
- Views:
Transcription
1 Reverse (fluid) resuscitation Should we be doing it? NAHLA IRTIZA ISMAIL
2 65 Male, 60 kg D1 in ICU Admitted from OT intubated Diagnosis : septic shock secondary to necrotising fasciitis of the R lower limb Patient was given 3.5 L of fluid since admission On Noradrenaline infusion Urine output : mls/ hr I/O : l
3 D2 in ICU Still requires Noradrenaline infusion Doubling of Serum Creatinine Already started on feeding and on maintenance drip Given boluses of crystalloid Urine output :30 40 mls/ hr I/O positive l
4 D3 in ICU Able to taper Noradrenaline infusion further On low ventilator setting Creatinine static I/O l The wife updated regarding progress


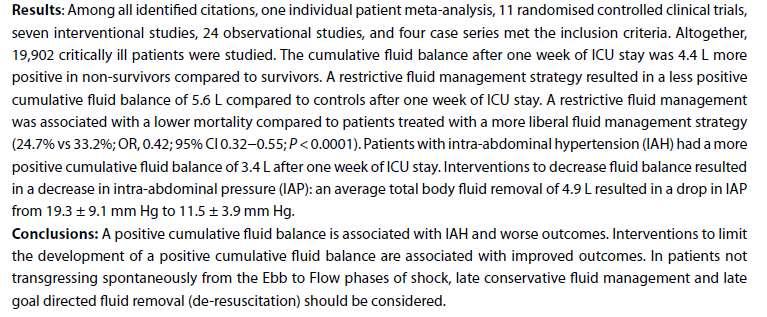
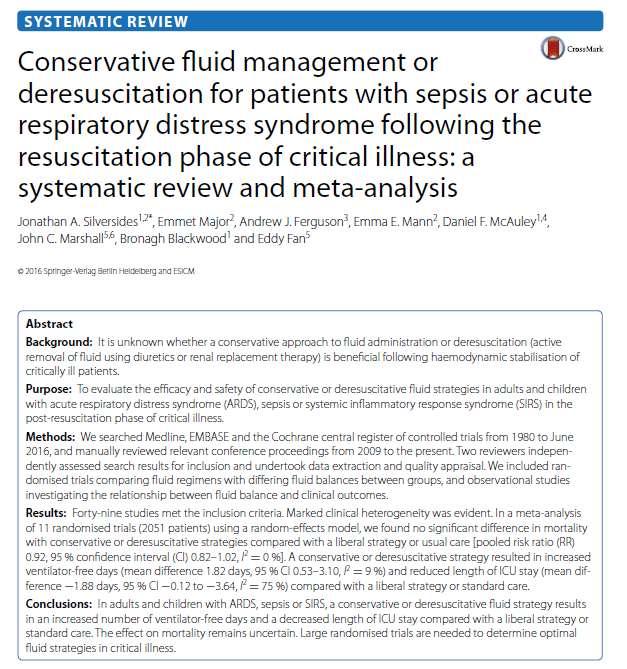
5 At this point cumulative balance is already +5.5 l for the past 3 days since admission.
6 Since patient was already started on feeding perhaps we should have cut down the IVD further. Should we allow for smaller positive balance or maybe even balance? Can we aim for a negative fluid balance? The kidney? Maybe we should give some frusemide now? Perhaps we should have done it earlier?
7 Is positive fluid balance harmful?
8 Why do we need to give our patient fluids? Shock
9 Aim of administrating fluid Optimisation of intravascular volume status increase cardiac output improvement in global oxygen delivery
10 Phases of fluid therapy RESCUE OPTIMIZATION STABILIZATION DEESCALATION Vincent JL et al. NEJM 2013; 369(18): Hoste E et al BJA 2014;113(5):740-7
11 Rescue Optimization Stabilization Deresuscitation/ Deescelation Principles Life saving Organ rescue Organ support Organ recovery Goals Correct shock Optimize tissue perfusion Aim for even or-ve fluid balance Mobilize accumulated fluid Time frame Min Hours Days Days weeks Phenotype Shock Unstable Stable Recovering Fluid therapy Bolus Fluid Titration Fluid challenge Conservative fluid Avoid unnecessary fluid
12 Resuscitation Administration of fluid for immediate management of life threatening conditions associated with impaired tissue perfusion
13 Opposite Reverse resuscitation Deresuscitation Deescalation Late Goal Directed Fluid Removal
14 Reverse (fluid)resuscitation more aggressive and active fluid removal by means of diuretics and renal replacement therapy with net ultrafiltration Malbrain et al, Anaesthesiology Intensive Therapy 2014
15 What are the problems with fluid administration? Increased capillary permeability Accumulation of large volumes of fluid in the interstitium Impaired oxygen delivery at the cellular level

16 Is this all?

17 Respiratory System Pulmonary oedema Pleural effusion Altered pulmonary and chest wall elastance Impaired gas exchange PaCO2 increased PaO2 reduced Extravascular lung water increase Lung volumes Prolonged ventilation Difficult weaning Hepatic system Hepatic congestion Impaired synthetic function Increase cholestasis Hepatic compartment syndrome GIT system Ascites Gut oedema Malabsorption Ileus Abdominal perfusion pressure reduce Reduce bowel contractility Increase Intra-abdominal Hypertension Reduce successful enteral feeding Increase intestinal permeability Increase bacterial translocation CNS Increase ICP, CPP, IOP Cerebral oedema Delirium CVS Increase in CVP and PAOP Reduce venous return Reduce stroke volume and CO Myocardial depression Pericardial effussion Myocardial oedema Conduction disturbance Renal System Renal interstitial oedema Renal blood flow decrease Glomerular filtration rate reduce Uremia increase Salt and water retention Renal compartment syndrome Abdominal wall Tissue oedema increase Impaired lymphatic drainage Poor wound healing Wound infection Pressure ulcers Skin oedema Abdominal compliance reduce
18
19
20

21
22
23
24 Deresuscitation Should we be doing it? When should we do it? How to do it? When should we stop?
25 Aim : A goal of zero to negative fluid balance by day 3 Keep cumulative fluid balance as low as possible Deresuscitation should be considered when fluid overload and fluid accumulation negatively impact end-organ function such as: P/F ratio < 200 EVLWI > 12 ml/kg PBW Increase IAP
26 PAL - treatment P A L high PEEP for 30 minutes (= to IAP) to drive fluid from the alveoli into the interstitium Albumin administration 2 x 100 ml 20% albumin over 60 minutes on Day 1, then titrated to albumin >30 g/l) to pull fluid from the interstitium into the circulation Frusemide ( Lasix ) infusion started 60 minutes after albumin at 60 mg/h for 4 hours, o then titrated between 5-20 mg/h to maintain UO >100 ml/h Cordemans C et al. Ann Intensive Care.Suppl 1:S15, 2012
27 Deresuscitation In anuric patient may consider RRT with ultrafiltration
28 When should we stop? Overzealous fluid removal hypoperfusion and tissue hypoxia Monitor organ function
29 Summary Fluid resuscitation is core in the management of shock but there are consequences Positive fluid balance is harmful May consider deresuscitation when fluid overload and fluid accumulation negatively impact end-organ function
30 Thank you
L : Line and Tube อ นตรายป องก นได จากการให สารน า
 L : Line and Tube อ นตรายป องก นได จากการให สารน า รศ.นพ.กว ศ กด จ ตตว ฒนร ตน ภาคว ชาศ ลยศาสตร คณะแพทยศาสตร มหาว ทยาล ยเช ยงใหม 3 rd Mini Conference: ความปลอดภ ยในผ ป วย ร วมด วย ช วยได ท กคน ว นท 13-14
L : Line and Tube อ นตรายป องก นได จากการให สารน า รศ.นพ.กว ศ กด จ ตตว ฒนร ตน ภาคว ชาศ ลยศาสตร คณะแพทยศาสตร มหาว ทยาล ยเช ยงใหม 3 rd Mini Conference: ความปลอดภ ยในผ ป วย ร วมด วย ช วยได ท กคน ว นท 13-14
Fluid balance in Critical Care
 Fluid balance in Critical Care By Dr HP Shum Nephrologist and Critical Care Physician Department of Intensive Care, PYNEH Fluid therapy is a critical aspect of initial acute resuscitation in critically
Fluid balance in Critical Care By Dr HP Shum Nephrologist and Critical Care Physician Department of Intensive Care, PYNEH Fluid therapy is a critical aspect of initial acute resuscitation in critically
SHOCK and the Trauma Victim. JP Pretorius Department of Surgery & SICU Steve Biko Academic Hospital.
 SHOCK and the Trauma Victim JP Pretorius Department of Surgery & SICU Steve Biko Academic Hospital. Classification of Shock Cardiogenic - Myopathic Arrythmic Mechanical Hypovolaemic - Haemorrhagic Non-haemorrhagic
SHOCK and the Trauma Victim JP Pretorius Department of Surgery & SICU Steve Biko Academic Hospital. Classification of Shock Cardiogenic - Myopathic Arrythmic Mechanical Hypovolaemic - Haemorrhagic Non-haemorrhagic
Wet Lungs Dry lungs Impact on Outcome in ARDS. Charlie Phillips MD Division of PCCM OHSU 2009
 Wet Lungs Dry lungs Impact on Outcome in ARDS Charlie Phillips MD Division of PCCM OHSU 2009 Today s talk Pathophysiology of ARDS The case for dry Targeting EVLW Disclosures Advisor for Pulsion Medical
Wet Lungs Dry lungs Impact on Outcome in ARDS Charlie Phillips MD Division of PCCM OHSU 2009 Today s talk Pathophysiology of ARDS The case for dry Targeting EVLW Disclosures Advisor for Pulsion Medical
Presented by: Indah Dwi Pratiwi
 Presented by: Indah Dwi Pratiwi Normal Fluid Requirements Resuscitation Fluids Goals of Resuscitation Maintain normal body temperature In most cases, elevate the feet and legs above the level of the heart
Presented by: Indah Dwi Pratiwi Normal Fluid Requirements Resuscitation Fluids Goals of Resuscitation Maintain normal body temperature In most cases, elevate the feet and legs above the level of the heart
INTRODUCTION The effect of CPAP works on lung mechanics to improve oxygenation (PaO 2
 2 Effects of CPAP INTRODUCTION The effect of CPAP works on lung mechanics to improve oxygenation (PaO 2 ). The effect on CO 2 is only secondary to the primary process of improvement in lung volume and
2 Effects of CPAP INTRODUCTION The effect of CPAP works on lung mechanics to improve oxygenation (PaO 2 ). The effect on CO 2 is only secondary to the primary process of improvement in lung volume and
Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock: 2016
 Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock: 2016 Mitchell M. Levy MD, MCCM Professor of Medicine Chief, Division of Pulmonary, Sleep, and Critical Care
Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock: 2016 Mitchell M. Levy MD, MCCM Professor of Medicine Chief, Division of Pulmonary, Sleep, and Critical Care
Fluids in Sepsis: How much and what type? John Fowler, MD, FACEP Kent Hospital, İzmir Eisenhower Medical Center, USA American Hospital Dubai, UAE
 Fluids in Sepsis: How much and what type? John Fowler, MD, FACEP Kent Hospital, İzmir Eisenhower Medical Center, USA American Hospital Dubai, UAE In critically ill patients: too little fluid Low preload,
Fluids in Sepsis: How much and what type? John Fowler, MD, FACEP Kent Hospital, İzmir Eisenhower Medical Center, USA American Hospital Dubai, UAE In critically ill patients: too little fluid Low preload,
Nurse Driven Fluid Optimization Using Dynamic Assessments
 Nurse Driven Fluid Optimization Using Dynamic Assessments 2016 1 WHAT WE BELIEVE We believe that clinicians make vital fluid and drug decisions every day with limited and inconclusive information Cheetah
Nurse Driven Fluid Optimization Using Dynamic Assessments 2016 1 WHAT WE BELIEVE We believe that clinicians make vital fluid and drug decisions every day with limited and inconclusive information Cheetah
Fluid Resuscitation in Critically Ill Patients with Acute Kidney Injury (AKI)
") Fluid Resuscitation in Critically Ill Patients with Acute Kidney Injury (AKI) Robert W. Schrier, MD University of Colorado School of Medicine Denver, Colorado USA Prevalence of acute renal failure in Intensive
Fluid Resuscitation in Critically Ill Patients with Acute Kidney Injury (AKI) Robert W. Schrier, MD University of Colorado School of Medicine Denver, Colorado USA Prevalence of acute renal failure in Intensive
Rounds in the ICU. Eran Segal, MD Director General ICU Sheba Medical Center
 Rounds in the ICU Eran Segal, MD Director General ICU Sheba Medical Center Real Clinical cases (including our mistakes) Emphasis on hemodynamic monitoring Usually no single correct answer We will conduct
Rounds in the ICU Eran Segal, MD Director General ICU Sheba Medical Center Real Clinical cases (including our mistakes) Emphasis on hemodynamic monitoring Usually no single correct answer We will conduct
Cardiorenal syndrome. Sofie Gevaert. Ghent University Hospital, Belgium
 Cardiorenal syndrome Sofie Gevaert Ghent University Hospital, Belgium Disclosures Consultancy Astra Zeneca Boegringer MSD Novartis 68 y old man, ADHF ICMP, ejection fraction 35 %: progressive dyspnea,
Cardiorenal syndrome Sofie Gevaert Ghent University Hospital, Belgium Disclosures Consultancy Astra Zeneca Boegringer MSD Novartis 68 y old man, ADHF ICMP, ejection fraction 35 %: progressive dyspnea,
Causes of Edema That Result From an Increased Capillary Pressure. Student Name. Institution Affiliation
 Running Head: CAUSES OF EDEMA 1 Causes of Edema That Result From an Increased Capillary Pressure Student Name Institution Affiliation CAUSES OF EDEMA 2 Causes of Edema That Result From an Increased Capillary
Running Head: CAUSES OF EDEMA 1 Causes of Edema That Result From an Increased Capillary Pressure Student Name Institution Affiliation CAUSES OF EDEMA 2 Causes of Edema That Result From an Increased Capillary
Effects of mechanical ventilation on organ function. Masterclass ICU nurses
 Effects of mechanical ventilation on organ function Masterclass ICU nurses Case Male, 60 - No PMH - L 1.74 m and W 85 kg Pneumococcal pneumonia Stable hemodynamics - No AKI MV in prone position (PEEP 16
Effects of mechanical ventilation on organ function Masterclass ICU nurses Case Male, 60 - No PMH - L 1.74 m and W 85 kg Pneumococcal pneumonia Stable hemodynamics - No AKI MV in prone position (PEEP 16
Purist? or Pragmatist? Assessment & Management of ICU Volume Status
 Assessment & Management of ICU Volume Status 9 th Annual Rocky Mountain Hospital Medicine Symposium Denver, Colorado Paula Dennen, MD Assistant Professor of Medicine Nephrology and Critical Care Medicine
Assessment & Management of ICU Volume Status 9 th Annual Rocky Mountain Hospital Medicine Symposium Denver, Colorado Paula Dennen, MD Assistant Professor of Medicine Nephrology and Critical Care Medicine
Fluids in Sepsis Less is more. Dr Anand Senthi Joondalup Health Campus ED MBBS, MAppFin, GradCertPubHlth,
 Fluids in Sepsis Less is more Dr Anand Senthi Joondalup Health Campus ED MBBS, MAppFin, GradCertPubHlth, FRACGP @drsenthi Summary Discussion of the evidence for/against fluid resuscitation in septic shock
Fluids in Sepsis Less is more Dr Anand Senthi Joondalup Health Campus ED MBBS, MAppFin, GradCertPubHlth, FRACGP @drsenthi Summary Discussion of the evidence for/against fluid resuscitation in septic shock
Dr. Nai Shun Tsoi Department of Paediatric and Adolescent Medicine Queen Mary Hospital Hong Kong SAR
 Dr. Nai Shun Tsoi Department of Paediatric and Adolescent Medicine Queen Mary Hospital Hong Kong SAR A very important aspect in paediatric intensive care and deserve more attention Basic principle is to
Dr. Nai Shun Tsoi Department of Paediatric and Adolescent Medicine Queen Mary Hospital Hong Kong SAR A very important aspect in paediatric intensive care and deserve more attention Basic principle is to
Surviving Sepsis Campaign. Guidelines for Management of Severe Sepsis/Septic Shock. An Overview
 Surviving Sepsis Campaign Guidelines for Management of Severe Sepsis/Septic Shock An Overview Mechanical Ventilation of Sepsis-Induced ALI/ARDS ARDSnet Mechanical Ventilation Protocol Results: Mortality
Surviving Sepsis Campaign Guidelines for Management of Severe Sepsis/Septic Shock An Overview Mechanical Ventilation of Sepsis-Induced ALI/ARDS ARDSnet Mechanical Ventilation Protocol Results: Mortality
Fluid Treatments in Sepsis: Meta-Analyses
 Fluid Treatments in Sepsis: Recent Trials and Meta-Analyses Lauralyn McIntyre MD, FRCP(C), MSc Scientist, Ottawa Hospital Research Institute Assistant Professor, University of Ottawa Department of Epidemiology
Fluid Treatments in Sepsis: Recent Trials and Meta-Analyses Lauralyn McIntyre MD, FRCP(C), MSc Scientist, Ottawa Hospital Research Institute Assistant Professor, University of Ottawa Department of Epidemiology
Acute Liver Failure: Supporting Other Organs
 Acute Liver Failure: Supporting Other Organs Michael A. Gropper, MD, PhD Professor of Anesthesia and Physiology Director, Critical Care Medicine University of California San Francisco Acute Liver Failure
Acute Liver Failure: Supporting Other Organs Michael A. Gropper, MD, PhD Professor of Anesthesia and Physiology Director, Critical Care Medicine University of California San Francisco Acute Liver Failure
R2R: Severe sepsis/septic shock. Surat Tongyoo Critical care medicine Siriraj Hospital
 R2R: Severe sepsis/septic shock Surat Tongyoo Critical care medicine Siriraj Hospital Diagnostic criteria ACCP/SCCM consensus conference 1991 SCCM/ESICM/ACCP/ATS/SIS International Sepsis Definitions Conference
R2R: Severe sepsis/septic shock Surat Tongyoo Critical care medicine Siriraj Hospital Diagnostic criteria ACCP/SCCM consensus conference 1991 SCCM/ESICM/ACCP/ATS/SIS International Sepsis Definitions Conference
The Septic Patient. Dr Arunraj Navaratnarajah. Renal SpR Imperial College NHS Healthcare Trust
 The Septic Patient Dr Arunraj Navaratnarajah Renal SpR Imperial College NHS Healthcare Trust Objectives of this session Define SIRS / sepsis / severe sepsis / septic shock Early recognition of Sepsis The
The Septic Patient Dr Arunraj Navaratnarajah Renal SpR Imperial College NHS Healthcare Trust Objectives of this session Define SIRS / sepsis / severe sepsis / septic shock Early recognition of Sepsis The
Managing Patients with Sepsis
 Managing Patients with Sepsis Diagnosis; Initial Resuscitation; ARRT Initiation Prof. Achim Jörres, M.D. Dept. of Nephrology and Medical Intensive Care Charité University Hospital Campus Virchow Klinikum
Managing Patients with Sepsis Diagnosis; Initial Resuscitation; ARRT Initiation Prof. Achim Jörres, M.D. Dept. of Nephrology and Medical Intensive Care Charité University Hospital Campus Virchow Klinikum
ICU treatment of the trauma patient. Intensive Care Training Program Radboud University Medical Centre Nijmegen
 ICU treatment of the trauma patient Intensive Care Training Program Radboud University Medical Centre Nijmegen Christian Kleber Surgical Intensive Care Unit - The trauma surgery Perspective Langenbecks
ICU treatment of the trauma patient Intensive Care Training Program Radboud University Medical Centre Nijmegen Christian Kleber Surgical Intensive Care Unit - The trauma surgery Perspective Langenbecks
Fluid responsiveness and extravascular lung water
 Fluid responsiveness and extravascular lung water Prof. Jean-Louis TEBOUL Medical ICU Bicetre hospital University Paris-South France Conflicts of interest Member of the Medical Advisory Board of Maquet/Pulsion
Fluid responsiveness and extravascular lung water Prof. Jean-Louis TEBOUL Medical ICU Bicetre hospital University Paris-South France Conflicts of interest Member of the Medical Advisory Board of Maquet/Pulsion
Abdominal Compartment Syndrome. Jeff Johnson, MD
 Abdominal Compartment Syndrome Jeff Johnson, MD Acute Care Surgeon, Denver Health Associate Professor of Surgery, University of Colorado Denver The Abdomen A Forgotten Closed Compartment Early Animal Models
Abdominal Compartment Syndrome Jeff Johnson, MD Acute Care Surgeon, Denver Health Associate Professor of Surgery, University of Colorado Denver The Abdomen A Forgotten Closed Compartment Early Animal Models
Sepsis: Identification and Management in an Acute Care Setting
 Sepsis: Identification and Management in an Acute Care Setting Dr. Barbara M. Mills DNP Director Rapid Response Team/ Code Resuscitation Stony Brook University Medical Center SEPSIS LECTURE NPA 2018 OBJECTIVES
Sepsis: Identification and Management in an Acute Care Setting Dr. Barbara M. Mills DNP Director Rapid Response Team/ Code Resuscitation Stony Brook University Medical Center SEPSIS LECTURE NPA 2018 OBJECTIVES
Post Resuscitation Care
 Princess Margaret Hospital f Children PAEDIATRIC ACUTE CARE GUIDELINE Post Resuscitation Care Scope (Staff): Scope (Area): All Emergency Department Clinicians Emergency Department This document should
Princess Margaret Hospital f Children PAEDIATRIC ACUTE CARE GUIDELINE Post Resuscitation Care Scope (Staff): Scope (Area): All Emergency Department Clinicians Emergency Department This document should
SHOCK. Emergency pediatric PICU division Pediatric Department Medical Faculty, University of Sumatera Utara H. Adam Malik Hospital
 SHOCK Emergency pediatric PICU division Pediatric Department Medical Faculty, University of Sumatera Utara H. Adam Malik Hospital 1 Definition Shock is an acute, complex state of circulatory dysfunction
SHOCK Emergency pediatric PICU division Pediatric Department Medical Faculty, University of Sumatera Utara H. Adam Malik Hospital 1 Definition Shock is an acute, complex state of circulatory dysfunction
IV fluid administration in sepsis. Dr David Inwald Consultant in PICU St Mary s Hospital, London CATS, London
 IV fluid administration in sepsis Dr David Inwald Consultant in PICU St Mary s Hospital, London CATS, London The talk What is septic shock? What are the recommendations? What is the evidence? Do we follow
IV fluid administration in sepsis Dr David Inwald Consultant in PICU St Mary s Hospital, London CATS, London The talk What is septic shock? What are the recommendations? What is the evidence? Do we follow
Fluid balance in the critically ill child with dengue Too much too little? Professor Lucy Lum Universiti Malaya ASMIC Sept
 Fluid balance in the critically ill child with dengue Too much too little? Professor Lucy Lum Universiti Malaya ASMIC 2018 21-23 Sept CFR 0.22 in 2017 0.15 in 2018 2 Lecture Contents: Dynamic disease Self-limiting
Fluid balance in the critically ill child with dengue Too much too little? Professor Lucy Lum Universiti Malaya ASMIC 2018 21-23 Sept CFR 0.22 in 2017 0.15 in 2018 2 Lecture Contents: Dynamic disease Self-limiting
Hyperemia, Congestion, and Edema
 Hyperemia, Congestion, and Edema Hyperemia Acute, actively increased blood flow Tissues look red (erythema) Congestion Chronic, passively reduced outflow Tissues look pale or blue (cyanosis) Edema Water
Hyperemia, Congestion, and Edema Hyperemia Acute, actively increased blood flow Tissues look red (erythema) Congestion Chronic, passively reduced outflow Tissues look pale or blue (cyanosis) Edema Water
Abdominal Compartment Syndrome. Jeff Johnson, MD
 Abdominal Compartment Syndrome Jeff Johnson, MD Acute Care Surgeon, Denver Health Associate Professor of Surgery, University of Colorado Denver The Abdomen A Forgotten Closed Compartment Early Animal Models
Abdominal Compartment Syndrome Jeff Johnson, MD Acute Care Surgeon, Denver Health Associate Professor of Surgery, University of Colorado Denver The Abdomen A Forgotten Closed Compartment Early Animal Models
INTENSIVE CARE MEDICINE CPD EVENING. Dr Alastair Morgan Wednesday 13 th September 2017
 INTENSIVE CARE MEDICINE CPD EVENING Dr Alastair Morgan Wednesday 13 th September 2017 WHAT IS NEW IN ICU? (RELEVANT TO ANAESTHETISTS) Not much! SURVIVING SEPSIS How many deaths in England were thought
INTENSIVE CARE MEDICINE CPD EVENING Dr Alastair Morgan Wednesday 13 th September 2017 WHAT IS NEW IN ICU? (RELEVANT TO ANAESTHETISTS) Not much! SURVIVING SEPSIS How many deaths in England were thought
Norepinephrine in septic shock
 Norepinephrine in septic shock Prof. Zsolt Molnár zsoltmolna@gmail.com Department of Anaesthesia and Intensive Therapy University of Szeged, Hungary A few months ago should we give it earlier? (Courtesy
Norepinephrine in septic shock Prof. Zsolt Molnár zsoltmolna@gmail.com Department of Anaesthesia and Intensive Therapy University of Szeged, Hungary A few months ago should we give it earlier? (Courtesy
Medical Treatment for acute Decompensated Heart Failure. Vlasis Ninios Cardiologist St. Luke s s Hospital Thessaloniki 2011
 Medical Treatment for acute Decompensated Heart Failure Vlasis Ninios Cardiologist St. Luke s s Hospital Thessaloniki 2011 2010 HFSA guidelines for ADHF 2009 focused update of the 2005 American College
Medical Treatment for acute Decompensated Heart Failure Vlasis Ninios Cardiologist St. Luke s s Hospital Thessaloniki 2011 2010 HFSA guidelines for ADHF 2009 focused update of the 2005 American College
SHOCK AETIOLOGY OF SHOCK (1) Inadequate circulating blood volume ) Loss of Autonomic control of the vasculature (3) Impaired cardiac function
 Inadequate circulating blood volume ) Loss of Autonomic control of the vasculature (3) Impaired cardiac function") SHOCK Shock is a condition in which the metabolic needs of the body are not met because of an inadequate cardiac output. If tissue perfusion can be restored in an expeditious fashion, cellular injury may
SHOCK Shock is a condition in which the metabolic needs of the body are not met because of an inadequate cardiac output. If tissue perfusion can be restored in an expeditious fashion, cellular injury may
Burn Resuscitation Formulas. John P. Sabra, MD Seton Surgical Group Department of Surgery Dell Medical School Austin, TX
 Burn Resuscitation Formulas John P. Sabra, MD Seton Surgical Group Department of Surgery Dell Medical School Austin, TX BURN INJURY % Physiologic Change % TBSA burn Stasis BURN VASCULAR PERMEABILITY
Burn Resuscitation Formulas John P. Sabra, MD Seton Surgical Group Department of Surgery Dell Medical School Austin, TX BURN INJURY % Physiologic Change % TBSA burn Stasis BURN VASCULAR PERMEABILITY
Rationale for renal replacement therapy in ICU: indications, approaches and outcomes. Richard Beale
 Rationale for renal replacement therapy in ICU: indications, approaches and outcomes Richard Beale RIFLE classification (ADQI group) 2004 Outcome AKIN classification Definition: Abrupt (within 48 hrs)
Rationale for renal replacement therapy in ICU: indications, approaches and outcomes Richard Beale RIFLE classification (ADQI group) 2004 Outcome AKIN classification Definition: Abrupt (within 48 hrs)
Critical Care Treatment Guidelines
 Critical Care Treatment Guidelines West Virginia Office of Emergency Medical Services CCT Guidelines CCT Guidelines TABLE OF CONTENTS Preface Acknowledgments Using the Guidelines INITIAL TREATMENT / UNIVERSAL
Critical Care Treatment Guidelines West Virginia Office of Emergency Medical Services CCT Guidelines CCT Guidelines TABLE OF CONTENTS Preface Acknowledgments Using the Guidelines INITIAL TREATMENT / UNIVERSAL
Impact of Fluids in Children with Acute Lung Injury
 Impact of Fluids in Children with Acute Lung Injury Canadian Critical Care Forum Toronto, Canada October 27 th, 2015 Adrienne G. Randolph, MD, MSc Critical Care Division, Department of Anesthesia, Perioperative
Impact of Fluids in Children with Acute Lung Injury Canadian Critical Care Forum Toronto, Canada October 27 th, 2015 Adrienne G. Randolph, MD, MSc Critical Care Division, Department of Anesthesia, Perioperative
Bedside assessment of fluid status
 Bedside assessment of fluid status 2nd AKI Academy October 18 th 2014 David Treacher Guy s & St Thomas NHS Trust Assessing the circulation - the 3 key questions v Is my patient adequately filled? v What
Bedside assessment of fluid status 2nd AKI Academy October 18 th 2014 David Treacher Guy s & St Thomas NHS Trust Assessing the circulation - the 3 key questions v Is my patient adequately filled? v What
ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) Rv
 Rv") ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) Rv.8.18.18 ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) SUDDEN PROGRESSIVE FORM OF ACUTE RESPIRATORY FAILURE ALVEOLAR CAPILLARY MEMBRANE BECOMES DAMAGED AND MORE
ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) Rv.8.18.18 ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) SUDDEN PROGRESSIVE FORM OF ACUTE RESPIRATORY FAILURE ALVEOLAR CAPILLARY MEMBRANE BECOMES DAMAGED AND MORE
ARDS and Lung Protection
 ARDS and Lung Protection Kristina Sullivan, MD Associate Professor University of California, San Francisco Department of Anesthesia and Perioperative Care Division of Critical Care Medicine Overview Low
ARDS and Lung Protection Kristina Sullivan, MD Associate Professor University of California, San Francisco Department of Anesthesia and Perioperative Care Division of Critical Care Medicine Overview Low
TACO CASE STUDIES RTC JUNE Kerry Dowling Blood Transfusion Laboratory Manager Jonathan Ricks Blood Transfusion Nurse Practitioner
 TACO CASE STUDIES RTC JUNE 2017 Kerry Dowling Blood Transfusion Laboratory Manager Jonathan Ricks Blood Transfusion Nurse Practitioner RISK FACTORS - TACO Age over 70 years although also seen in younger
TACO CASE STUDIES RTC JUNE 2017 Kerry Dowling Blood Transfusion Laboratory Manager Jonathan Ricks Blood Transfusion Nurse Practitioner RISK FACTORS - TACO Age over 70 years although also seen in younger
ICU management and referral guidelines for severe hypoxic respiratory failure
 Aim: ICU management and referral guidelines for severe hypoxic respiratory failure 1) To provide a concise management plan Non ventilatory Ventilatory 2) Timeline for referring patient with refractory
Aim: ICU management and referral guidelines for severe hypoxic respiratory failure 1) To provide a concise management plan Non ventilatory Ventilatory 2) Timeline for referring patient with refractory
Sepsis overview. Dr. Tsang Hin Hung MBBS FHKCP FRCP
 Sepsis overview Dr. Tsang Hin Hung MBBS FHKCP FRCP Epidemiology Sepsis, severe sepsis, septic shock Pathophysiology of sepsis Recent researches and advances From bench to bedside Sepsis bundle Severe sepsis
Sepsis overview Dr. Tsang Hin Hung MBBS FHKCP FRCP Epidemiology Sepsis, severe sepsis, septic shock Pathophysiology of sepsis Recent researches and advances From bench to bedside Sepsis bundle Severe sepsis
Fluid assessment, monitoring and therapy for the acute nurse
 Fluid assessment, monitoring and therapy for the acute nurse Kelly Wright Lead Nurse for AKI King s College Hospital Aims and objectives Aims and objectives Why do we worry about volume assessment? Completing
Fluid assessment, monitoring and therapy for the acute nurse Kelly Wright Lead Nurse for AKI King s College Hospital Aims and objectives Aims and objectives Why do we worry about volume assessment? Completing
Care of the Deteriorating Patient in Recovery NADIA TICEHURST : CLINICAL NURSE EDUCATOR PERI ANAESTHETICS BENDIGO HEALTH
 Care of the Deteriorating Patient in Recovery NADIA TICEHURST : CLINICAL NURSE EDUCATOR PERI ANAESTHETICS BENDIGO HEALTH Intended learning outcomes Describe the components of a comprehensive clinician
Care of the Deteriorating Patient in Recovery NADIA TICEHURST : CLINICAL NURSE EDUCATOR PERI ANAESTHETICS BENDIGO HEALTH Intended learning outcomes Describe the components of a comprehensive clinician
Sepsis: Management ANUPOL PANITCHOTE, MD. Division of Critical Care Medicine Department of Medicine, Khon Kaen University, Thailand
 Sepsis: Management ANUPOL PANITCHOTE, MD. Division of Critical Care Medicine Department of Medicine, Khon Kaen University, Thailand Vital signs Symptoms LAB BT > 38.3 or < 36 ๐ C HR > 90 bpm RR > 20 /min
Sepsis: Management ANUPOL PANITCHOTE, MD. Division of Critical Care Medicine Department of Medicine, Khon Kaen University, Thailand Vital signs Symptoms LAB BT > 38.3 or < 36 ๐ C HR > 90 bpm RR > 20 /min
Sepsis Story At Intermountain Healthcare Intensive Medicine Clinical Program
 Sepsis Story At Intermountain Healthcare 2004-2012 Intensive Medicine Clinical Program The International Surviving Sepsis Campaign Was Organized In 2002 During The ESICM International Meeting In Barcelona,
Sepsis Story At Intermountain Healthcare 2004-2012 Intensive Medicine Clinical Program The International Surviving Sepsis Campaign Was Organized In 2002 During The ESICM International Meeting In Barcelona,
Intraoperative Fluid Management. David G Hovord BA MB BChir FRCA Clinical Assistant Professor University of Michigan
 Intraoperative Fluid Management David G Hovord BA MB BChir FRCA Clinical Assistant Professor University of Michigan Objectives Examine impact of perioperative renal failure, and discuss structure and function
Intraoperative Fluid Management David G Hovord BA MB BChir FRCA Clinical Assistant Professor University of Michigan Objectives Examine impact of perioperative renal failure, and discuss structure and function
Surviving Sepsis Campaign Guidelines 2012 & Update for David E. Tannehill, DO Critical Care Medicine Mercy Hospital St.
 Surviving Sepsis Campaign Guidelines 2012 & Update for 2015 David E. Tannehill, DO Critical Care Medicine Mercy Hospital St. Louis Be appropriately aggressive the longer one delays aggressive metabolic
Surviving Sepsis Campaign Guidelines 2012 & Update for 2015 David E. Tannehill, DO Critical Care Medicine Mercy Hospital St. Louis Be appropriately aggressive the longer one delays aggressive metabolic
Sepsis Combine experience and Evidence. Eran Segal, MD Director General ICU, Sheba Medical Center, Israel
 Sepsis Combine experience and Evidence Eran Segal, MD Director General ICU, Sheba Medical Center, Israel The Science of Sepsis A complex and diverse clinical entity Outcome is affected by: Infecting organism
Sepsis Combine experience and Evidence Eran Segal, MD Director General ICU, Sheba Medical Center, Israel The Science of Sepsis A complex and diverse clinical entity Outcome is affected by: Infecting organism
SEPSIS SYNDROME
 INTRODUCTION Sepsis has been defined as a life threatening condition that arises when the body s response to an infection injures its own tissues and organs. Sepsis may lead to shock, multiple organ failure
INTRODUCTION Sepsis has been defined as a life threatening condition that arises when the body s response to an infection injures its own tissues and organs. Sepsis may lead to shock, multiple organ failure
Fluid Management in Critically Ill AKI Patients
 Fluid Management in Critically Ill AKI Patients Sang Kyung Jo, MD, PhD Department of Internal Medicine Korea University Medical College KO/MG31/15-0017 Outline Fluid balance in critically ill patients:
Fluid Management in Critically Ill AKI Patients Sang Kyung Jo, MD, PhD Department of Internal Medicine Korea University Medical College KO/MG31/15-0017 Outline Fluid balance in critically ill patients:
TBSA Burn Estimation Chart Adult Major Burn Clinical Practice Guideline
 TBSA Burn Estimation Chart Adult Major Burn Clinical Practice Guideline Patient Label Anatomical Subunit Percent Total Percent One Side Anterior Posterior Injury Subtotal 3.5% 2nd and 3rd degree burns
TBSA Burn Estimation Chart Adult Major Burn Clinical Practice Guideline Patient Label Anatomical Subunit Percent Total Percent One Side Anterior Posterior Injury Subtotal 3.5% 2nd and 3rd degree burns
Salty Solutions or Salty Problems? Outline. Outline 29/04/2013
 Salty Solutions or Salty Problems? 18 th October 2012 Richard Seigne Anaesthetist 1 - Non fluid 40% T o t a l b o d y f l u i d 60% NaCl NaCl Intra-cellular fluid 2/3 KCl Interstitial fluid 3/4 of ECF
Salty Solutions or Salty Problems? 18 th October 2012 Richard Seigne Anaesthetist 1 - Non fluid 40% T o t a l b o d y f l u i d 60% NaCl NaCl Intra-cellular fluid 2/3 KCl Interstitial fluid 3/4 of ECF
Cardiopulmonary System
 Dana Oakes, BA, RRT NPS Author/Speaker Cardiopulmonary System Main Purpose Main Function Main Goal Oxygen Delivery Adequate Perfusion (deliver adequate oxygen and nutrients; remove metabolic waste) Tissue
Dana Oakes, BA, RRT NPS Author/Speaker Cardiopulmonary System Main Purpose Main Function Main Goal Oxygen Delivery Adequate Perfusion (deliver adequate oxygen and nutrients; remove metabolic waste) Tissue
M5 BOARD REVIEW. Q s. Q s. Q s. Q s. Q s. Equations. Be Brilliant Today. Respiratory ( ) Alveolar Gas Equation. Dead Space (Bohr Equation)
 Alveolar Gas Equation. Dead Space (Bohr Equation)") Be Brilliant Today Respiratory Alveolar Gas Equation Dead Space (Bohr Equation) PA O2 FI O2 ( P ATM P H2 O ) Pa CO2 / RQ V D V T P a P ECO CO2 2 P a CO 2 PA O2 Alveolar partial pressure of oxygen P a CO
Be Brilliant Today Respiratory Alveolar Gas Equation Dead Space (Bohr Equation) PA O2 FI O2 ( P ATM P H2 O ) Pa CO2 / RQ V D V T P a P ECO CO2 2 P a CO 2 PA O2 Alveolar partial pressure of oxygen P a CO
Printed copies of this document may not be up to date, obtain the most recent version from
 Children s Acute Transport Service Clinical Guidelines Septic Shock Document Control Information Author Shruti Dholakia L Chigaru Author Position Fellow CATS Consultant Document Owner E. Polke Document
Children s Acute Transport Service Clinical Guidelines Septic Shock Document Control Information Author Shruti Dholakia L Chigaru Author Position Fellow CATS Consultant Document Owner E. Polke Document
Case year old female nursing home resident with a hx CAD, PUD, recent hip fracture Transferred to ED with decreased mental status BP in ED 80/50
 Case 1 65 year old female nursing home resident with a hx CAD, PUD, recent hip fracture Transferred to ED with decreased mental status BP in ED 80/50 Case 1 65 year old female nursing home resident with
Case 1 65 year old female nursing home resident with a hx CAD, PUD, recent hip fracture Transferred to ED with decreased mental status BP in ED 80/50 Case 1 65 year old female nursing home resident with
Albumina nel paziente critico. Savona 18 aprile 2007
 Albumina nel paziente critico Savona 18 aprile 2007 What Is Unique About Critical Care RCTs patients eligibility is primarily defined by location of care in the ICU rather than by the presence of a specific
Albumina nel paziente critico Savona 18 aprile 2007 What Is Unique About Critical Care RCTs patients eligibility is primarily defined by location of care in the ICU rather than by the presence of a specific
INTRODUCTION. Dengue is one of the ten leading. Globally 20 million cases/yr. 24,000 deaths/yr. It is important to know the typical and atypical
 DENGUE IN CHILDREN INTRODUCTION Dengue is one of the ten leading causes of hospitalization and death in children. Globally 20 million cases/yr. 24,000 deaths/yr. It is important to know the typical and
DENGUE IN CHILDREN INTRODUCTION Dengue is one of the ten leading causes of hospitalization and death in children. Globally 20 million cases/yr. 24,000 deaths/yr. It is important to know the typical and
Sepsis is an important issue. Clinician s decision-making capability. Guideline recommendations
 Surviving Sepsis Campaign: International Guidelines for Management of Severe Sepsis and Septic Shock: 2012 Clinicians decision-making capability Guideline recommendations Sepsis is an important issue 8.7%
Surviving Sepsis Campaign: International Guidelines for Management of Severe Sepsis and Septic Shock: 2012 Clinicians decision-making capability Guideline recommendations Sepsis is an important issue 8.7%
Septic Shock. Rontgene M. Solante, MD, FPCP,FPSMID
 Septic Shock Rontgene M. Solante, MD, FPCP,FPSMID Learning Objectives Identify situations wherein high or low BP are hemodynamically significant Recognize complications arising from BP emergencies Manage
Septic Shock Rontgene M. Solante, MD, FPCP,FPSMID Learning Objectives Identify situations wherein high or low BP are hemodynamically significant Recognize complications arising from BP emergencies Manage
Dengue Fever & Dengue Shock Syndrome. 07-May-18 PLES / SLCP 1
 Dengue Fever & Dengue Shock Syndrome 07-May-18 PLES / SLCP 1 Objectives Early diagnosis Pathophysiology of DHF Proper management How to avoid complications Case 07-May-18 PLES / SLCP 2 Febrile Phase High
Dengue Fever & Dengue Shock Syndrome 07-May-18 PLES / SLCP 1 Objectives Early diagnosis Pathophysiology of DHF Proper management How to avoid complications Case 07-May-18 PLES / SLCP 2 Febrile Phase High
Over- and underfill: not all nephrotic states are equal. Detlef Bockenhauer
 Over- and underfill: not all nephrotic states are equal Detlef Bockenhauer Objectives Review pathophysiology of oedema: undervs overfill Treatment options The clinical setting: case 1 A6-y old girl with
Over- and underfill: not all nephrotic states are equal Detlef Bockenhauer Objectives Review pathophysiology of oedema: undervs overfill Treatment options The clinical setting: case 1 A6-y old girl with
Fluid Resuscitation and Monitoring in Sepsis. Deepa Gotur, MD, FCCP Anne Rain T. Brown, PharmD, BCPS
 Fluid Resuscitation and Monitoring in Sepsis Deepa Gotur, MD, FCCP Anne Rain T. Brown, PharmD, BCPS Learning Objectives Compare and contrast fluid resuscitation strategies in septic shock Discuss available
Fluid Resuscitation and Monitoring in Sepsis Deepa Gotur, MD, FCCP Anne Rain T. Brown, PharmD, BCPS Learning Objectives Compare and contrast fluid resuscitation strategies in septic shock Discuss available
Staging Sepsis for the Emergency Department: Physician
 Staging Sepsis for the Emergency Department: Physician Sepsis Continuum 1 Sepsis Continuum SIRS = 2 or more clinical criteria, resulting in Systemic Inflammatory Response Syndrome Sepsis = SIRS + proven/suspected
Staging Sepsis for the Emergency Department: Physician Sepsis Continuum 1 Sepsis Continuum SIRS = 2 or more clinical criteria, resulting in Systemic Inflammatory Response Syndrome Sepsis = SIRS + proven/suspected
Chapter 5: Sepsis Stephen Lo
 Chapter 5: Sepsis Stephen Lo Introduction Sepsis and its consequence are the bread and butter of intensive care medicine and management of it is time critical. This chapter will discuss the definitions,
Chapter 5: Sepsis Stephen Lo Introduction Sepsis and its consequence are the bread and butter of intensive care medicine and management of it is time critical. This chapter will discuss the definitions,
Update in Critical Care Medicine
 Update in Critical Care Medicine Michael A. Gropper, MD, PhD Professor and Executive Vice Chair Department of Anesthesia and Perioperative Care Director, Critical Care Medicine UCSF Disclosure None Update
Update in Critical Care Medicine Michael A. Gropper, MD, PhD Professor and Executive Vice Chair Department of Anesthesia and Perioperative Care Director, Critical Care Medicine UCSF Disclosure None Update
Initial Resuscitation of Sepsis & Septic Shock
 Initial Resuscitation of Sepsis & Septic Shock Dr. Fatema Ahmed MD (Critical Care Medicine) FCPS (Medicine) Associate professor Dept. of Critical Care Medicine BIRDEM General Hospital Is Sepsis a known
Initial Resuscitation of Sepsis & Septic Shock Dr. Fatema Ahmed MD (Critical Care Medicine) FCPS (Medicine) Associate professor Dept. of Critical Care Medicine BIRDEM General Hospital Is Sepsis a known
The Art and Science of Diuretic therapy
 The Art and Science of Diuretic therapy Dr. Fayez EL Shaer Associate Professour of cardiology Consultant cardiologist MD, MSc, PhD, CBNC, NBE FESC, ACCP, FASNC,HFA KKUH, KFCC Heart failure: fluid overload
The Art and Science of Diuretic therapy Dr. Fayez EL Shaer Associate Professour of cardiology Consultant cardiologist MD, MSc, PhD, CBNC, NBE FESC, ACCP, FASNC,HFA KKUH, KFCC Heart failure: fluid overload
Sepsis. From EMS to ER to ICU. What we need to be doing
 Sepsis From EMS to ER to ICU What we need to be doing NEHAL BHATT, MD ATHENS PULMONARY, CRITICAL CARE AND SLEEP Objectives 1. Define the changes to the definition of Sepsis 2. Describe the assessment,
Sepsis From EMS to ER to ICU What we need to be doing NEHAL BHATT, MD ATHENS PULMONARY, CRITICAL CARE AND SLEEP Objectives 1. Define the changes to the definition of Sepsis 2. Describe the assessment,
Visit ESICM LIVES 2015
 B COVER STORY: the Brain THE OFFICIAL MANAGEMENT AND PRACTICE JOURNAL VOLUME 15 - ISSUE 3 - AUTUMN 2015 Visit us @ ESICM LIVES 2015 stand 21 Plus Infections in the Immunosuppressed and Immunocompromised
B COVER STORY: the Brain THE OFFICIAL MANAGEMENT AND PRACTICE JOURNAL VOLUME 15 - ISSUE 3 - AUTUMN 2015 Visit us @ ESICM LIVES 2015 stand 21 Plus Infections in the Immunosuppressed and Immunocompromised
How and why I give IV fluid Disclosures SCA Fluids and public health 4/1/15. Andrew Shaw MB FRCA FCCM FFICM
 How and why I give IV fluid Andrew Shaw MB FRCA FCCM FFICM Professor and Chief Cardiothoracic Anesthesiology Vanderbilt University Medical Center 2015 Disclosures Consultant for Grifols manufacturer of
How and why I give IV fluid Andrew Shaw MB FRCA FCCM FFICM Professor and Chief Cardiothoracic Anesthesiology Vanderbilt University Medical Center 2015 Disclosures Consultant for Grifols manufacturer of
Fluids: occult effects. S Magder Department of Critical Care, McGill University Health Centre
 Fluids: occult effects S Magder Department of Critical Care, McGill University Health Centre Why is volume important? 1. Water is essential to dissolve substances and allow them to diffuse 2. Necessary
Fluids: occult effects S Magder Department of Critical Care, McGill University Health Centre Why is volume important? 1. Water is essential to dissolve substances and allow them to diffuse 2. Necessary
IV Fluids. I.V. Fluid Osmolarity Composition 0.9% NaCL (Normal Saline Solution, NSS) Uses/Clinical Considerations
 Uses/Clinical Considerations") IV Fluids When administering IV fluids, the type and amount of fluid may influence patient outcomes. Make sure to understand the differences between fluid products and their effects. Crystalloids Crystalloid
IV Fluids When administering IV fluids, the type and amount of fluid may influence patient outcomes. Make sure to understand the differences between fluid products and their effects. Crystalloids Crystalloid
John Park, MD Assistant Professor of Medicine
 John Park, MD Assistant Professor of Medicine Faculty photo will be placed here park.john@mayo.edu 2015 MFMER 3543652-1 Sepsis Out with the Old, In with the New Mayo School of Continuous Professional Development
John Park, MD Assistant Professor of Medicine Faculty photo will be placed here park.john@mayo.edu 2015 MFMER 3543652-1 Sepsis Out with the Old, In with the New Mayo School of Continuous Professional Development
10. Severe traumatic brain injury also see flow chart Appendix 5
 10. Severe traumatic brain injury also see flow chart Appendix 5 Introduction Severe traumatic brain injury (TBI) is the leading cause of death in children in the UK, accounting for 15% of deaths in 1-15
10. Severe traumatic brain injury also see flow chart Appendix 5 Introduction Severe traumatic brain injury (TBI) is the leading cause of death in children in the UK, accounting for 15% of deaths in 1-15
THE KIDNEY IN HYPOTENSIVE STATES. Benita S. Padilla, M.D.
 THE KIDNEY IN HYPOTENSIVE STATES Benita S. Padilla, M.D. Objectives To discuss what happens when the kidney encounters low perfusion To discuss new developments and clinical application points in two scenarios
THE KIDNEY IN HYPOTENSIVE STATES Benita S. Padilla, M.D. Objectives To discuss what happens when the kidney encounters low perfusion To discuss new developments and clinical application points in two scenarios
Vasopressors in septic shock
 Vasopressors in septic shock Prof. Jean-Louis TEBOUL Medical ICU Bicetre hospital University Paris-South France Questions 1- Why do we use vasopressors in septic shock? 2- Which first-line agent? 3- When
Vasopressors in septic shock Prof. Jean-Louis TEBOUL Medical ICU Bicetre hospital University Paris-South France Questions 1- Why do we use vasopressors in septic shock? 2- Which first-line agent? 3- When
Shock Quiz! By Clare Di Bona
 Shock Quiz! By Clare Di Bona Test Question What is Mr Burns full legal name? Answer Charles Montgomery Plantagenet Schicklgruber Burns. (Season 22, episode 11) Question 1. What is the definition of shock?
Shock Quiz! By Clare Di Bona Test Question What is Mr Burns full legal name? Answer Charles Montgomery Plantagenet Schicklgruber Burns. (Season 22, episode 11) Question 1. What is the definition of shock?
The Use of Dynamic Parameters in Perioperative Fluid Management
 The Use of Dynamic Parameters in Perioperative Fluid Management Gerard R. Manecke Jr., M.D. Chief, Cardiac Anesthesia UCSD Medical Center San Diego, CA, USA Thanks to Tom Higgins, M.D. 1 Goals of today
The Use of Dynamic Parameters in Perioperative Fluid Management Gerard R. Manecke Jr., M.D. Chief, Cardiac Anesthesia UCSD Medical Center San Diego, CA, USA Thanks to Tom Higgins, M.D. 1 Goals of today
How can the PiCCO improve protocolized care?
 How can the PiCCO improve protocolized care? Azriel Perel Professor and Chairman Department of Anesthesiology and Intensive Care Sheba Medical Center, Tel Aviv University, Israel ESICM, Vienna 2009 Disclosure
How can the PiCCO improve protocolized care? Azriel Perel Professor and Chairman Department of Anesthesiology and Intensive Care Sheba Medical Center, Tel Aviv University, Israel ESICM, Vienna 2009 Disclosure
SEPSIS: Seeing Through the. W. Graham Carlos MD, MSCR, ATSF, FACP
 SEPSIS: Seeing Through the W. Graham Carlos MD, MSCR, ATSF, FACP Objectives Forget everything you have known about sepsis Learn new things Objectives Define sepsis Explain why Early Goal Directed Therapy
SEPSIS: Seeing Through the W. Graham Carlos MD, MSCR, ATSF, FACP Objectives Forget everything you have known about sepsis Learn new things Objectives Define sepsis Explain why Early Goal Directed Therapy
Management of Nephrotic Syndrome
 Management of Nephrotic Syndrome 1. Introduction Incidence 2-4/100,000. Boys > girls 3:2; age of onset 2-6 years 80% of cases in children is due to minimal change (MCD) of which 80% will respond to steroid
Management of Nephrotic Syndrome 1. Introduction Incidence 2-4/100,000. Boys > girls 3:2; age of onset 2-6 years 80% of cases in children is due to minimal change (MCD) of which 80% will respond to steroid
-Cardiogenic: shock state resulting from impairment or failure of myocardium
 Shock chapter Shock -Condition in which tissue perfusion is inadequate to deliver oxygen, nutrients to support vital organs, cellular function -Affects all body systems -Classic signs of early shock: Tachycardia,tachypnea,restlessness,anxiety,
Shock chapter Shock -Condition in which tissue perfusion is inadequate to deliver oxygen, nutrients to support vital organs, cellular function -Affects all body systems -Classic signs of early shock: Tachycardia,tachypnea,restlessness,anxiety,
Fluids and electrolytes: the basics
 Fluids and electrolytes: the basics This document is based on the handout from the Surgery for Finals course. The notes provided here summarise key aspects, focusing on areas that are popular in clinical
Fluids and electrolytes: the basics This document is based on the handout from the Surgery for Finals course. The notes provided here summarise key aspects, focusing on areas that are popular in clinical
Fluids in ICU. JMO teaching 5th July 2016
 Fluids in ICU JMO teaching 5th July 2016 Objectives Physiology of fluid infusion History of fluid resuscitation Physiology of fluid resuscitation Types of resuscitation fluid The ideal resuscitation fluid
Fluids in ICU JMO teaching 5th July 2016 Objectives Physiology of fluid infusion History of fluid resuscitation Physiology of fluid resuscitation Types of resuscitation fluid The ideal resuscitation fluid
Childhood nephrotic syndrome practice guidelines
 Childhood nephrotic syndrome practice guidelines Dr Shuman Haq Consultant Paediatric Nephrologist Southampton Children s Hospital Definitions Nephrotic syndrome Proteinuria Urine protein : creatinine >200
Childhood nephrotic syndrome practice guidelines Dr Shuman Haq Consultant Paediatric Nephrologist Southampton Children s Hospital Definitions Nephrotic syndrome Proteinuria Urine protein : creatinine >200
How to resuscitate the patient in early sepsis? A physiological approach. J.G. van der Hoeven, Nijmegen
 How to resuscitate the patient in early sepsis? A physiological approach J.G. van der Hoeven, Nijmegen Disclosure interests speaker (potential) conflict of interest Potentially relevant relationships with
How to resuscitate the patient in early sepsis? A physiological approach J.G. van der Hoeven, Nijmegen Disclosure interests speaker (potential) conflict of interest Potentially relevant relationships with
Inpatient Quality Reporting Program
 SEP-1 Early Management Bundle, Severe Sepsis/Septic Shock Part II Questions and Answers Moderator: Candace Jackson, RN Inpatient Quality Reporting (IQR) Program Lead Hospital Inpatient Value, Incentives,
SEP-1 Early Management Bundle, Severe Sepsis/Septic Shock Part II Questions and Answers Moderator: Candace Jackson, RN Inpatient Quality Reporting (IQR) Program Lead Hospital Inpatient Value, Incentives,
PHYSIOLOGY AND MANAGEMENT OF THE SEPTIC PATIENT
 PHYSIOLOGY AND MANAGEMENT OF THE SEPTIC PATIENT Melanie Sanchez, RN, MSNE, OCN, CCRN Clinical Nurse III City of Hope National Medical Center HOW THE EXPERTS TREAT HEMATOLOGIC MALIGNANCIES LAS VEGAS, NV
PHYSIOLOGY AND MANAGEMENT OF THE SEPTIC PATIENT Melanie Sanchez, RN, MSNE, OCN, CCRN Clinical Nurse III City of Hope National Medical Center HOW THE EXPERTS TREAT HEMATOLOGIC MALIGNANCIES LAS VEGAS, NV
Admissions with severe sepsis in adult, general critical care units in England, Wales and Northern Ireland
 Admissions with severe sepsis in adult, general critical care units in England, Wales and Northern Ireland Question For all admissions to adult, general critical care units in the Case Mix Programme Database
Admissions with severe sepsis in adult, general critical care units in England, Wales and Northern Ireland Question For all admissions to adult, general critical care units in the Case Mix Programme Database
Fluid restriction is superior in acute lung injury and ARDS
 TAKE-HOME POINTS FROM LECTURES BY CLEVELAND CLINIC AND VISITING FACULTY MEDICAL GRAND ROUNDS CME CREDIT HERBERT P. WIEDEMANN, MD Chairman, Department of Pulmonary, Allergy, and Critical Care Medicine,
TAKE-HOME POINTS FROM LECTURES BY CLEVELAND CLINIC AND VISITING FACULTY MEDICAL GRAND ROUNDS CME CREDIT HERBERT P. WIEDEMANN, MD Chairman, Department of Pulmonary, Allergy, and Critical Care Medicine,
Sepsis Update: Focus on Early Recognition and Intervention. Disclosures
 Sepsis Update: Focus on Early Recognition and Intervention Jessie Roske, MD October 2017 Disclosures I have no actual or potential conflict of interest in relation to this program/presentation. I will
Sepsis Update: Focus on Early Recognition and Intervention Jessie Roske, MD October 2017 Disclosures I have no actual or potential conflict of interest in relation to this program/presentation. I will
Admission of patient CVICU and hemodynamic monitoring
 Admission of patient CVICU and hemodynamic monitoring Prepared by: Rami AL-Khatib King Fahad Medical City Pi Prince Salman Heart tcentre CVICU-RN Admission patient to CVICU Introduction All the patients
Admission of patient CVICU and hemodynamic monitoring Prepared by: Rami AL-Khatib King Fahad Medical City Pi Prince Salman Heart tcentre CVICU-RN Admission patient to CVICU Introduction All the patients
Printed copies of this document may not be up to date, obtain the most recent version from
 Children s Acute Transport Service Clinical Guidelines Septic Shock Document Control Information Author Claire Fraser P.Ramnarayan Author Position tanp CATS Consultant Document Owner E. Polke Document
Children s Acute Transport Service Clinical Guidelines Septic Shock Document Control Information Author Claire Fraser P.Ramnarayan Author Position tanp CATS Consultant Document Owner E. Polke Document