Cardiac Biomarkers in Acute Chest Pain
|
|
|
- Warren Booth
- 5 years ago
- Views:
Transcription
1 Cardiac Biomarkers in Acute Chest Pain Dr. K. Shanthi Naidu, Prof & HOD & Dept of Biochemistry, CARE Hospitals, Banjara Hills, Hyderabad. Dr Maddury Jyotsna Prof & HOU-IV, Dept of Cardiology, Nizam s institute of medical sciences, Panjagutta, Hyderabad
2 Cardiac biomarkers are substances that are released into the blood when the heart is damaged or stressed.
3 The Ideal Biomarker Then Sensitive and specific Now Either highly sensitive (diagnosis) OR highly specific (treatment effect) Reflects disease severity Correlates with prognosis Should aid in clinical decision making Reflects abnormal Physiology/biochemistry Prognosis is most meaningful if level is clinically actionable Should be used as a basis for specific biomarker guided-therapy Level should decrease following effective therapy Bio-monitoring during treatment is an effective surrogate of improvement

4 Ischemia and reprefusion ECG GDF-15? Acute myocardial damage TnT, TnI, CK-MB Clinical background Renal Dysfunction Crea Cl Cystatin C Inflammatory Activity CRP, IL-6, Cd-40 lig Left ventricular Dysfunction BNP, NT-proBNP

5 Classification of Cardiac Biomarkers according to various stages during cardiac disease process
6 Blood Level of Marker Above Upper Limit of Normal Cardiac Markers Release Kinetics Cardiac Marker Specificity Appears At Peaks At Returns to Normal Myoglobin Non - specific 1-3 hours 9 hours 24 hours CK - MB Moderately specific 4-6 hours hours 72 hours Troponin I Specific 4-6 hours hours 10 days Myoglobin CK-MB Troponin I Time After Onset Post AMI (Hours)
7 Case capsule 1 54 yr old diabetic male, came to ED with chest pain for 15 minutes with normal ECG. Pt was hemodynamically stable. What biomarkers should be done?
8 Depends on time of arrival Within one hour Myoglobin > 2hrs CK MB/ Troponin
9 Myoglobin Small-size heme protein found in all tissues mainly assists in oxygen transport It is released from all damaged tissues Its level rises more rapidly than ctn and CK-MB. Released from damaged tissue within 1 hour Normal value: ng/ml Timing: Earliest Rise: Peak Return to normal: 1-4 hrs 6-9 hrs 12 hrs
10
11 The earliest expressions ( 30 min) were observed for connexin 43, JunB, and cytochrome c, followed by fibronectin ( 1 h), myoglobin ( 1 h), troponins I and T ( 1 h), TUNEL ( 1 h), and C5b- 9 ( 2 h). Early markers for myocardial ischemia and sudden cardiac death. Int J Legal Med Sep;130(5): Continuous immunosensing of myoglobin in human serum as potential companion diagnostics technique. Biosens Bioelectron Dec 15;62:
12
13 AIM Since limited numbers of studies have been conducted, in this study the utility of H-FABP as candidate markers for diagnosis of NSTE- ACS.
14 EXCLUSION CRITERIA Chest pain > 8 hours duration non cardiac chest pain recent injuries renal failure
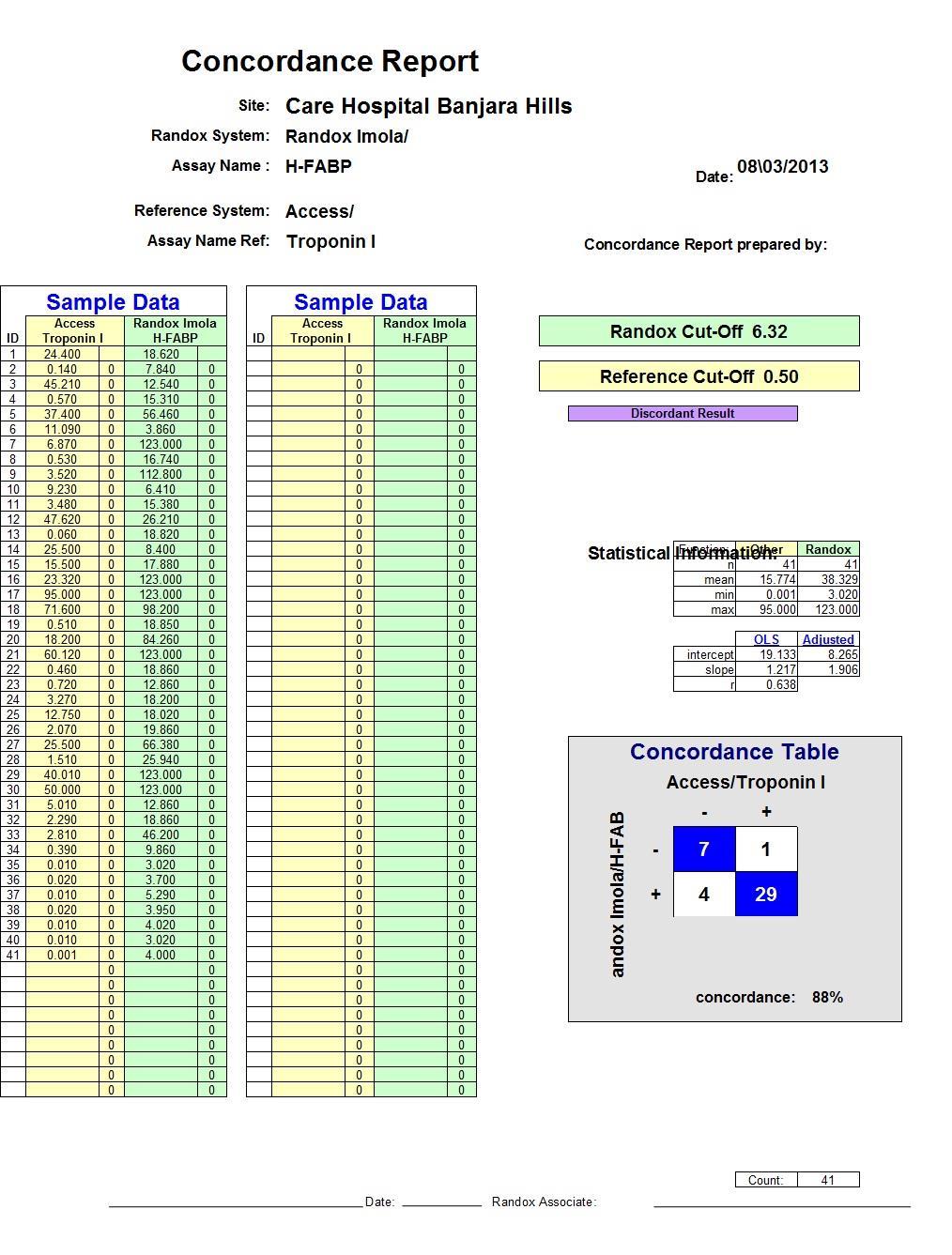
15 Laboratory Analysis Serum H-FABP : Quantitative immunoturbidimetric method (Randox Laboratories, Ltd. Co., Antrim, United Kingdom) cardiac Troponin T and Troponin I : Time resolved immunofluorescence method (AQT90 FLEX, Radiometer, Denmark). CK-MB : Quantitative immunoturbidimetric method (Roche)

16 Results
17 CARDIAC BIOMARKERS CARDIAC BIOMARKER CASES(N=30) CONTROLS(N=2 2) P VALUE HFABP(ng/ml) 40.42± ±1.52 <0.001 ctnt(ng/l) 370± ±0.5 <0.01 ctni(μg/l) 0.18± ±
18 Model CK-MB 0.59 ctnt 0.71 ctni H-FABP 0.79
19 Diagnostic Performance of Different Cardiac Biomarkers for NSTE-ACS Variable CK-MB ctnt ctni H-FABP Sensitivity 40% 47% 41% 58% Specificity 81% 100% 100% 100% AUC PPV 75% 100% 100% 100% NPV 50% 58% 55% 63% Cut-off 18IU/L 16ng/L 0.012μg/L 9.4ng/ml
20 DISCUSSION H-FABP was elevated (>9.4 ng/ml) in 17 of the 30 patients (57%). Among the cases, the mean level of H-FABP was 40 ng/ml, where as in controls it was 3.47ng/ml and the difference was statistically significant (p <0.001). In a number of studies, H-FABP has been reported to be particularly sensitive within the first few hours after the onset of coronary occlusion and symptoms. small molecular weight (15 kda) cytoplasmic unbound abundance rapid release from damaged myocardial cells. Kathrukha et al. proved in their study that H-FABP levels elevate earlier than ctni levels in patients with UA.
21 LIMITATIONS OF THE STUDY The sample size was small to allow for a generalization of the results. Hence, further larger studies are required to evaluate the diagnostic role of the novel biomarker. This work only studied the potential benefit from a single measurement of H-FABP at admission, sequential measurements were not performed. Take home message In order to decrease the risk of falsely excluded patients with on-going AMI, a combined measurement of two biomarkers, an early one such as H-FABP and a later marker such as troponins may provide the optimum diagnostic performance.
22 Creatinine Kinase - MB Prior to cardiac Troponins marker of choice CK-MB isoenzyme Criterion 2 serial elevations above diagnostic cut off/single result more than twice upper limit of normal Appearance 4 to 6 hours after symptom onset/normal 48 to 72 hours. Release kinetics assist in diagnosing reinfarction if rise follows decline.
23 CK-MB Relative Index = χ 100 Total CK The relative index allows the distinction between increased total CK due to myocardial damage and that due to skeletal or neural damage. Relative index calculated by ratio of CK-MB mass to Total CK assist in false positive elevations. The relative index is clinically useful when both CK and CKMB are increased.
24 CK-MB/CK relative index A relative index exceeding 3 is indicative of AMI Ratios between 3 and 5 represent a gray zone. No definitive diagnosis can be established without serial determinations to detect a rise. Note that the diagnosis of acute MI must not be based on an elevated relative index alone, because the relative index may be elevated in clinical settings when either the total CK or the CK-MB is within normal limits. The relative index is only clinically useful when both the total CK and the CK-MB levels are increased.
25 Testing strategy The American College of Emergency Physicians (ACEP) recommends 3 different testing strategies for ruling out NSTEMI in the ED. Strategy 1 - is to use a single negative CK-MB, TnI, or TnT measured 8-12 hours after symptom onset. Strategy 2 - is to use negative myoglobin in conjunction with a negative CK-MB mass or negative TnI measured at baseline and at 90 minutes in patients presenting less than 8 hours after symptom onset. Strategy 3 - is to use a negative 2-hour delta CK- MB in conjunction with a negative 2-hour delta TnI in patients presenting less than 8 hours after symptom onset.
26 Testing strategy ACEP s recommendations on the use of delta CK-MB and delta TnI are based on determining the change in the level of TnI or CK-MB on samples drawn 2 hours apart. However, the delta TnI evaluation is partially based on the use of older TnI assays and outdated WHO acute MI cutoffs in a retrospective study. Therefore, ACEP s recommendation to use a delta TnI in conjunction with a delta CK-MB may not be generalizable to other commercially available Troponin assays. The ACC/AHA guidelines for the treatment of patients with unstable angina and NSTEMI recommend a baseline sample upon ED arrival and a repeat sample 6-9 hours after presentation.
27 Case 1 follow up Immediate Trop I (POC) testing after arrival to ED was negative. But CK MB which was sent to lab came as elevated. How can we interpret this discordant Troponin and CK-MB results?
28 WHAT IS discordant Troponin and CK-MB results In the CRUSADE registry, a review of almost 30,000 patients revealed that discordant Troponin and CK-MB results occurred in 28% of patients. However, patients who were Troponin negative but CK-MB positive had in-hospital mortality rates that were not significantly increased from patients who were negative for both biomarkers. [30] Similarly, in a report of more than 10,000 patients with ACS from the multicenter GRACE registry, in-hospital mortality was highest when both Troponin and CK-MB were positive, intermediate in troponin-positive/ck-mb-negative patients, and lowest in patients in whom both markers were negative and in those who were troponin-negative/ck-mb-positive. [31] Thus, an isolated CK-MB elevation has limited prognostic value in patients with a non-st elevation ACS.
29 Troponins Generally undetectable in healthy patients??? Sensitive assays available Absolute abnormal value varies depending on the clinical setting Above 99 th percentile of healthy population as cut off using an assay in the acceptable precision
30 Features of serum markers of acute myocardial infarction Marker Time to appearance Duration of elevation Sensitivity at: 6hr 12hr Specificity Comments MB2 Isoform 2 6 hr 1 2 d 95% % 95% Not widely available Myoglobin 1 2 hr < 1 d 85% 90% 80% Slightly improved sensitivity early in AMI when added to troponin/ck-mb but not widely used due to low specificity AMI = acute myocardial infarction; CK=creatine kinase Courtesy: Cecil Textbook of Medicine, 22 nd ed., Chapter 69 St.Elevation Acute Myocardial Infarction and Complications of Myocardial Infarction
31 The recent developments in interpretation of Troponin Cardiac Troponin shows our understanding is still evolving Improved sensitivity Compared to prior markers Utilization by Clinicians debatable..laboratory understanding of these sensitive values is deter mental to help the physician Heterogeneity of cut off values MIXED MESSAGE in its usage, pushes in more individuals as AMI.. Not easy on the clinician, Hence the situation must be circumstance where the clinical signs, symptoms lead to a strong suspicion of AMI
32 Study from CARE hospital Materials and Methods 100 patients were analysed for cardiac markers 79 were studied for CK-MB and Troponin T serially up to 48 hours 23 patients were compared with Troponin T and Troponin I 20 patients were compared with Troponin and NT probnp Less than 15 were studied for myoglobin HsCRP was found not to be effective in analysis
33 Serial Measurement of Cardiac Markers after Chest pain Trop T ng/ml BASE 8hrs 16hrs 24hrs 9 CK-MB TROP-T CK-MB N= BASE 8hrs 16hrs 24hrs 0 U/L TROP-T CK-MB
34 Study in our Laboratory on changing over 50 samples were compared on Roche platform Elecsys 2010 between Troponin T and Hs Troponin T Assay showed concordance of 98% and Paired sample statistics p value 0.39 Inferring that the two assays did not differ significantly at 5% level Validation between Elecsys 2010 and Cobas e601 for Hs Troponin T had concordance of 100%
35 Features of serum markers of acute myocardial infarction Sensitivity at: Marker Time to appearance Duration of elevation 6hr 12hr Specificity Comments Troponin I 2 6 hr 5 10 d 75% % 98% Generally regarded as a test of choice Troponin T 2 6 hr 5 14 d 80% % 95% A test of choice. Less specific than Troponin I (elevated in renal insufficiency) CK-MB 3 6 hr 2 4 d 65% 95% 95% Test of choice for recurrent angina once Troponin elevated
36 Sensitivity, specificity and precision of commercial Troponin assays: Vary considerably due to Lack of standardization Use of different monoclonal antibodies Presence of modified Troponin in serum Variations in antibody Cross reactivity with degradation products
37 Study in our Laboratory on changing over 75 samples were validated Roche platform Elecsys 2010 and Beckman Coulter Access for Hs Troponin T and Hs Troponin I Assay showed concordance of 89% and Paired sample statistics p value Inferring that the two variables of instrumentation and methodology differ significantly at 5 % level. Validation between Elecsys 2010 and Cobas e601 for Hs Troponin T had concordance of 100% Cobose601 and Access 2 for 20 samples showed concordance 90%.
38 TROPONINS Troponins released in response to myocardial infarction regardless of cause Ischemia most common cardiac muscle damage Cytosolic pool small, muscular pool larger Cardiac injury severity release from both pools injury Initial small elevation cytosolic pool Diffuse across the sarcolemma in to the surrounding lymphatics and blood vessels and there by detectable in blood If injury persists and necrosis progresses further Troponins are released from the muscular pool
39 TROPONINS Levels of Troponin complex T & I Not present in serum unless-cardiac necrosis Cardiac specific Levels remain elevated from 3-14 days after MI, sensitivity high when other markers have returned to normal Adv: Delay in seeking medical advice Elevated levels are predictive of poor outcome in patients with acute coronary syndrome Disadvantage - Detection of Reinfarction - Less sensitive in early stages of infarction
40 TROPONINS 5 4? Ideal Marker Trop T 0.3 Trop I Normal Obtained Diagnostic Measurement Normal Trop T N=23 Trop I Troponin T Troponin I Normal < 0.01 ng/ml 0.03 ng/ml Cut off for AMI 0.1 ng/ml 0.5 ng/ml Measuredb Normal Obtained Diagnostic Measurement
41 Percentage increase in routine Cardiac Markers emphasizing best alternative Troponin: Sensitivity in the Emergency Department CK CK-MB TnI Admission CK CK-MB TnI + 4 hours Troponin I compared with CK activity and CK-MB concentration in patients with AMI on admission and 4 hours later. Reference: Hamm, Christian W., M.D., Braunwald Heart Disease Update 3.
42

43 Evolution of the cardiac Troponin (ctn) assays and their diagnostic cut-offs. Mahajan V S, Jarolim P Circulation 2011;124: Copyright American Heart Association
 population.")
44 Cardiac Troponin I (ctni) levels in a healthy reference population and in an acute coronary syndrome (ACS) population. Mahajan V S, Jarolim P Circulation 2011;124: Copyright American Heart Association
45 High sensitivity cardiac Troponin T (hsctnt) as an isolated marker in ED for chest pain evaluation Troponin-only Manchester Acute Coronary Syndromes (T-MACS) decision aid: single biomarker re-derivation and external validation in three cohorts At the 'rule out' threshold, in the derivation set (n=703), T-MACS had 99.3% (95% CI 97.3% to 99.9%) negative predictive value (NPV) and 98.7% (95.3%-99.8%) sensitivity for ACS, 'ruling out' 37.7% patients (specificity 47.6%, positive predictive value (PPV) 34.0%). In the validation set (n=1459), T-MACS had 99.3% (98.3%-99.8%) NPV and 98.1% (95.2%-99.5%) sensitivity, 'ruling out' 40.4% (n=590) patients (specificity 47.0%, PPV 23.9%). T-MACS would 'rule in' 10.1% and 4.7% patients in the respective sets, of which 100.0% and 91.3% had ACS. C- statistics for the original and refined rules were similar (T-MACS 0.91 vs MACS 0.90 on validation). CONCLUSIONS: T-MACS could 'rule out' ACS in 40% of patients, while 'ruling in' 5% at highest risk using a single hs-ctnt measurement on arrival. Emerg Med J Aug 26
46 Case capsule 2 63 years old female hypertensive patients with anterior STMI of 3 hours duration. No contraindications for thrombolysis. Hemodynamically stable. What biomarker we should use? Is there any difference in gender for biomarkers elevation timing and severity of elevation?
47 Are cardiac biomarkers are required for STMI? Note that cardiac markers are not necessary for the diagnosis of patients who present with ischemic chest pain and diagnostic ECGs with ST-segment elevation.
48 Clinical Effect of Sex-Specific Cutoff Values of High-Sensitivity Cardiac Troponin T in Suspected Myocardial Infarction. JAMA Cardiol 2016;Sep 21:[Epub ahead of print]. once using the uniform 99th percentile cutoff value level of 14 ng/l and once using sex-specific 99th percentile levels of hsctnt (women, 9 ng/l; men, 15.5 ng/l). The diagnosis in two women was upgraded from unstable angina to AMI, and the diagnosis in one man was downgraded from AMI to unstable angina. These diagnostic results were confirmed when using two alternative pairs of uniform and sexspecific cutoff values. Conclusions: The authors concluded that uniform 99th percentile should remain the standard of care when using hsctnt levels for the diagnosis of AMI.
49 Exceptions Simple markers can distinguish Takotsubo cardiomyopathy from ST segment elevation myocardial infarction. Int J Cardiol Sep 15;219: The concentration of NTproBNP was greater in pts with TTC than STEMI (4702pg/ml vs 2138pg/ml). The concentration of TnI and CKMB mass was greater in the STEMI group than in the TTC group (TnI: 2.1ng/ml and CK MB mass: 9.5ng/ml in pts with TTC vs TnI: 19ng/ml and CK MB mass: 73.3ng/ml in pts with STEMI). The NTproBNP/TnI ratio and NTproBNP/CKMB mass ratio were, respectively, and in pts with TTC and 81.6 and 27.5 in pts with STEMI (p<0.001). Moreover, the NTproBNP/EF ratio was also statistically significant (110.4 in TTC group and 39.4 in STEMI group). CONCLUSIONS: NTproBNP/TnI, NTproBNP/CKMB mass and NTproBNP/EF ratios can distinguish TTC from STEMI at an early stadium. The most accurate marker is the NTproBNP/TnI ratio.
50
51 Toll Like Receptor 4 in Acute Myocardial Infarction Background: Previous studies on Toll-like receptor 4 (TLR 4), which are identified as central innate immune receptors, were done for local (at plaque rupture site) and systemic expression of TLR 4 from mononuclear concentrate (MNC) in acute myocardial infarction (AMI) pts. TLR inhibition is considered as a emerging new therapeutic modality for LV remodeling. We want to study difference of expression of TLR 4 on MNC and plasma in AMI pts. Even though, for TLR 4 protein detection in plasma requires higher concentration on the lymphocytes and to be secreted into plasma, but still, if plasma detected TLR 4 has same prognostification importance as from TLR 4 of MNC then, TLR 4 detection from plasma may be used at bed side.
52 Methods We recruited acute MI pts who presented with in 48 hrs of onset of chest pain. TLR4 estimation was done with TLR4 ELISA kit from Cusabio at the time of admission. Group 1 are AMI pts with TLR 4 measured from MNC (Ficoll paque method) and Group 2 are AMI pts with TLR 4 measured from plasma. In two groups of Controls (Control A are volunteers without known CAD and coronary risk factors and Control B are pts with obvious sepsis), TLR4 was estimated in both plasma and from MNC. According to that kit standards TLR 4 concentration < or = 0.03 ng/dl is considered as negative. Killips class, adverse events in hospitals (including recurrent angina, LVF, ventricular arrhythmias and death) and CPK levels were correlated with TLR 4 levels.
53 Table 1: AMI Parameter AMI Controls Group 1 (MNC) Group 2(Plasma) A(no CAD+RF) B (Infection) Number TLR 4 pos. 14 (53.8%) 2(14.3%) 0 5(100%) Table 2: Parameter Variable Age (yrs) 54.1 ± 11.6 M:F 12:8 HTN 21 (52.5%) DM 10 (25%) Location of MI Inferior MI 11 (27.5%) Anterior MI 26 (65%) Extensive MI 3 (7.5%) Average Killips 1.7 ± 0.9 class CPK levels ± units/l Mean TLR ± 0.4 ng/dl
54 Table 3: Parameter TLR Positive TLR Negative P value Group 1 Average Killips class 2.4 ± ± o.4 < Average CPK level ± ± NS Primary VT 1 1 NS Death Group 2 Average Killips class 3 ± ± Average CPK level 1348 ± ± 45.7 NS Primary VT 1 1 NS Death
55 Conclusion In Group 1, & group 2 also there is no correlation to TLR 4 concentration and occurrence of primary VT and CPK levels but strong association with Killips class and death. Plasma TLR 4 detection was given same correlation with Killips class and dreaded prognostication of the patient ( that is mortality) in AMI like the TLR 4 detected from MNC. Therefore, kit to design using plasma of the AMI pt may be useful after larger AMI patients study.
56 Case capsule 3 44 year old gentleman admitted with road traffic accident developed chest pain. What would be the preferred marker for diagnosing infarction Road traffic accident with rhadomyolysis Trop
57 How we can standerdize the TnT assay Only one manufacturer produces the TnT assay, and its 99th percentile cutoffs and the 10% CV are well established. However, up to 20-fold variation has occurred in results obtained with the multitude of commercial TnI assays currently available, each with their own 99th percentile upper reference limits and 10% CV levels.
58 How we can standerdize the TnT assay In the GUSTO IV study, a relatively insensitive point-of-care TnI assay was used to screen patients for study eligibility. In a subsequent study, the blood samples were reanalyzed using the 99th percentile cutoff of a far more sensitive central laboratory TnT assay. The more sensitive 99th percentile cutoff of this TnT assay identified an additional 96 (28%) of 337 patients with a positive TnT result but negative point-of-care TnI; these patients had higher rates of death or MI at 30 days. [14] In a similar reanalysis of the TACTICS-TIMI 18 trial, 3 different TnI cutoffs were compared on 1821 patients to evaluate the 30-day risk of death or MI: the 99th percentile, 10% CV, and the World Health Organization (WHO) acute MI cutoffs. (The WHO cutoffs define acute MI using CK-MB and report troponin levels as either a higher acute MI level or a lower intermediate level that is correlated with leak or minor myocardial injury. ) Using the 10% CV cutoff identified, an additional 12% more cases were identified relative to the WHO acute MI cutoff. The 99th percentile cutoff identified an additional 10% of cases relative to the 10% CV cutoff, as well as a 22% increase in the number of cases over the WHO acute MI cutoff. Nevertheless, the odds ratios for the adverse cardiac event rates of death or MI at 30 days were similar for all 3 cutoffs, suggesting that the lower cutoffs detected more patients with cardiovascular risk without sacrificing specificity. [
59 How we can standerdize the TnT assay The National Academy of Clinical Biochemistry (NACB) working with the ACC/ESC guidelines has recommended adoption of the 99th percentile upper reference limit as the recommended cutoff for a positive troponin result. Ideally, the precision of the assay at this cutoff level should be measured by a CV that is less than 10%. However, most TnI assays are imprecise at the 99th percentile reference limit. [17] Some have therefore recommended that the cutoff level be raised to the slightly higher 10% CV level instead of the 99th percentile reference limit to ensure adequate assay precision.
60 Is Point-of-care assays are available? NACB recommendations specify that cardiac markers be available on an immediate basis 24 h/d, 7 d/wk, with a turnaround time of 1 hour. [18] Point-of-care (POC) devices that provide rapid results should be considered in hospitals whose laboratories cannot meet these guidelines. POC assays for CK-MB, myoglobin, and the cardiac troponins TnI and TnT are available. Only qualitative TnT assays are available as POC tests, but both quantitative and qualitative POC TnI assays are currently marketed.
61 Point-of-care assays In a multicenter trial, the time to positivity was significantly faster for the POC device than for the local laboratory (2.5 h vs 3.4 h). [19] In another multicenter study, which evaluated the i-stat POC TnI assay in comparison with the central laboratory in 2000 patients with suspected ACS, POC testing reduced the length of stay by approximately 25 minutes for patients who were discharged from the ED. [20, 21] The sensitivity of current POC assays coupled with the benefit of rapid turnaround time make the POC assays attractive clinical tools in the ED.
62 Point of care assays: NACB Cardiac markers to be available 24 hrs/day, 7 d/week Ideal turn around time 1 hour POC when labs cannot meet this guidelines Qualitative TnT assay Qualitative and Quantitative for TnI assay
63 Ultrasensitive and low-volume point-of-care diagnostics are available for trop T testing? Sci Rep Sep 16;6: Ultrasensitive and low-volume point-of-care diagnostics on flexible strips - a study with cardiac Troponin biomarkers. Shanmugam NR1, Muthukumar S2, Prasad S1. A flexible, mechanically stable, and disposable electrochemical sensor platform for monitoring cardiac Troponin through the detection and quantification of cardiac Troponin-T (ctnt). They designed and fabricated nanostructured zinc oxide (ZnO) sensing electrodes on flexible porous polyimide substrates.
64 Additive biomarkers in AMI
65 Potential Biomarker Targets in ACS ctnt, ctnl, Myo, CKMB, FABP Necrosis Ischemia IMA, uffa Plaque Rupture MMP s, PAPP scd40l, PIGF Arrhythmias Thrombosis PAI-1, scd40l, vwf, D dimer Neurohormone Activation BNP, NE Inflammation Hs-CRP, Ox LDL MCP-1, MPO. IL18 Endothelial Activation sicam, pselection
66 Midregional fragment of the N-terminal of pro-anp (MR-proANP) and 2 extracardiac biomarkers; the c-terminal provasopressin (copeptin) and the midregional portion of proadrenomedullin (MR-proADM).
67 Novel markers in ACS Cost effective Traditional markers CK/CK-MB/cTnI/cTnT/ Myglobin PAPPP-A Mettaloproteinate causes extracellular matrix degradation, activates insulin like growth factor IGF-1 (mediator of atherosclerosis) HsCRP Acute phase/prothrombotic/specificity? BNP Neurohormonal activity, risk stratification IL-6 Cytokine, indipendent marker for risk stratification Albumin Cobalt binding ischemic modified albumin?
68 Summary of studies using BNP or NTproBNP for risk stratification of AMI Study Pop N Endpoints Thresholds Odds ratio or Hazard Ratio ACS-TIMI16 2,525 Death (30 day, 10 months) HF(10 months) MI (10 months) Quartiles BNP > 80 pg/ml 1, 3.8, 4.0, 5.8 Approximately 2.7 Approximately 2 AMI 70 Death (18 months) Median (>59 pg/ml) Approximately 2.5 AMI-CONSENSUS 131 Death (one year) 75 th centile BNP 33.3 pmol/l Approximately 1.36 ACS 609 Death Median 2.4 NSTEACS 1,483 Death (in hosp) (180 days) BNP > 586 pg/ml (1.7) (1.67) FRISC-II 2,019 Death Top Tertile 4.1(invasive) vs 3.5(noninvasive) TACTICS-TIMI18 1,676 ACS 1,033 Death (six months) HF (30 days) Death (30 day) (six months) BNP > 80 pg/ml OR 3.3 OR 3.9 Quartiles (2.24) (1.84) AMI 473 Death Median OR 3.82
69 Novel markers in ACS Cost effective Glycogen Phosphorylase (GPBB) - Released early from injured Myocardial cells - Reflecting burst in Glycogenolysis associated with MI - Greater discriminating power than other markers Haemostatic - Fibrinopeptide A (FPA) - Ongoing Thrombin Activity - Thrombin Antithrombin Complex(TAT) - Thrombin Generation - Prothrombin Fragmen 1.2(F1.2)- Ongoing Haemostatic Activation
70 Summary of studies using GDF-15 for risk stratification of AMI Study Pop N Endpoints Thresholds Odds ratio or Hazard Ratio Ref GUSTOIV (NSTEACS) 2, Death (one year) Tertiles < 1,200 ng/l, 1,200 to 1,800 ng/l > 1,800 ng/l 1.5%, 5%, 14.1% [46] FRISC-II (invasive vs conservative) 2,079 Death or MI (2 yrs) Invasive at > 1,800 ng/l Invasive 1,200 to 1,800 ng/l Invasive < 1,200 or Trop -ve HR 0.49 (risk reduction) HR 0.68 No benefit [47] ASSENT-2/plus (STEMI) 741 Death (1 yr) Tertiles < 1,200, 1,200 to 1,800, > 1, %, 5.0%, 14% [48] AMI 1,142 Death or HF (1.5 yr) <1,470 ng/l, >1,470 ng/l HR 1.77 [49]
71 Comprehensive Metabolomic Characterization of Coronary Artery Diseases. A total of 89 differential metabolites were identified. The altered metabolic pathways included reduced phospholipid catabolism, increased amino acid metabolism, increased short-chain acylcarnitines, decrease in tricarboxylic acid cycle, and less biosynthesis of primary bile acid. Plasma metabolomics are powerful for characterizing metabolic disturbances. Differences in small-molecule metabolites may reflect underlying CAD and serve as biomarkers for CAD progression. J Am Coll Cardiol Sep 20;68(12):
72 Novel markers in ACS Cost effective -Plasma D-Dimer - Activation of coagulation/ fibrinolysis -S100 Protein- Levels at early & late ph? Continuous Release after injury? Future Marker

73

74 Ack. JAPI, Volume 63, June 2015


75 Hs Troponin Cut off point of 99% percentile highly sensitive for diagnosis of AMI, 2 hours after presentation Ack. JAPI, Volume 63, June 2015
76 Questions in thought process Diagnosing acute MI using high sensitive Troponin How to use high sensitive cardiac troponin in acute cardiac insult Groups with subclinical Ischemic heart disease and slightly elevated troponin Studies of diagnostic performance study design influences sensitivity and specificity Age cut off -? Elderly?? Cardiac Troponin A marker of Myocardial necrosis and not a specific marker of AMI Constant values without diagnosis changes are likely to be marker of chronic heart disease
77 The 10 commandments of troponin Collaborate with the laboratory and the emergency department Understand some analytical considerations Make the diagnosis of AMI based on ctn and the clinical scenario Rule out myocardial infarction differently than ruling it in Use common sense to interpret elevations of ctn in patients who are critically ill Do not be intimidated by elevations in patients with renal failure Take the baseline value of ctn into account with percutaneous coronary intervention It takes multiple parameters to make the diagnosis of AMI following bypass surgery Do not forget drug toxicities as an aetiology for ctn elevations Be cautious with ctn elevations post-exercise Heart 2011;97:
High Sensitivity Troponin Improves Management. But Not Yet
 High Sensitivity Troponin Improves Management But Not Yet Allan S. Jaffe, MD.* Consultant - Cardiology & Laboratory Medicine Professor of Medicine Chair, CCLS Division, Department of Laboratory Medicine
High Sensitivity Troponin Improves Management But Not Yet Allan S. Jaffe, MD.* Consultant - Cardiology & Laboratory Medicine Professor of Medicine Chair, CCLS Division, Department of Laboratory Medicine
Use of Biomarkers for Detection of Acute Myocardial Infarction
 Use of Biomarkers for Detection of Acute Myocardial Infarction Allan S. Jaffe, MD.* Consultant - Cardiology & Laboratory Medicine Professor of Medicine Chair, CCLS Division, Department of Laboratory Medicine
Use of Biomarkers for Detection of Acute Myocardial Infarction Allan S. Jaffe, MD.* Consultant - Cardiology & Laboratory Medicine Professor of Medicine Chair, CCLS Division, Department of Laboratory Medicine
Cardiac Troponin Testing and Chest Pain Patients: Exploring the Shades of Gray
 Cardiac Troponin Testing and Chest Pain Patients: Exploring the Shades of Gray Nichole Korpi-Steiner, PhD, DABCC, FACB University of North Carolina Chapel Hill, NC Learning Objectives Describe the acute
Cardiac Troponin Testing and Chest Pain Patients: Exploring the Shades of Gray Nichole Korpi-Steiner, PhD, DABCC, FACB University of North Carolina Chapel Hill, NC Learning Objectives Describe the acute
 Biomarkers in Acute Cardiac Disease Samir Arnaout, M.D.FESC Associate Professor of Medicine Internal Medicine i & Cardiology American University of Beirut Time course of the appearance of various markers
Biomarkers in Acute Cardiac Disease Samir Arnaout, M.D.FESC Associate Professor of Medicine Internal Medicine i & Cardiology American University of Beirut Time course of the appearance of various markers
Är dagens troponinmetoder tillräckligt känsliga?
 Är dagens troponinmetoder tillräckligt känsliga? Per Venge, MD PhD Professor Department of Medical Sciences Uppsala University and Department of Clinical Chemistry and Pharmacology University Hospital
Är dagens troponinmetoder tillräckligt känsliga? Per Venge, MD PhD Professor Department of Medical Sciences Uppsala University and Department of Clinical Chemistry and Pharmacology University Hospital
Troponin when is an assay high sensitive?
 Troponin when is an assay high sensitive? Professor P. O. Collinson MA MB BChir FRCPath FRCP edin MD FACB EurClin Chem Consultant Chemical Pathologist and Professor of Cardiovascular Biomarkers, Departments
Troponin when is an assay high sensitive? Professor P. O. Collinson MA MB BChir FRCPath FRCP edin MD FACB EurClin Chem Consultant Chemical Pathologist and Professor of Cardiovascular Biomarkers, Departments
Current Utilities of Cardiac Biomarker Testing at POC. June 24, 2010 Joe Pezzuto, MT (ASCP) Carolyn Kite, RN
 Carolyn Kite, RN") Current Utilities of Cardiac Biomarker Testing at POC June 24, 2010 Joe Pezzuto, MT (ASCP) Carolyn Kite, RN 1. Discuss challenges associated with diagnosing Acute Coronary Syndromes (ACS) and Heart Failure
Current Utilities of Cardiac Biomarker Testing at POC June 24, 2010 Joe Pezzuto, MT (ASCP) Carolyn Kite, RN 1. Discuss challenges associated with diagnosing Acute Coronary Syndromes (ACS) and Heart Failure
Biomarkers of myocardial infarction. Dr. Mamoun Ahram Cardiovascular system, 2013
 Biomarkers of myocardial infarction Dr. Mamoun Ahram Cardiovascular system, 2013 References This lecture Hand-outs Acute Myocardial Infarction A rapid development of myocardial necrosis caused by prolonged
Biomarkers of myocardial infarction Dr. Mamoun Ahram Cardiovascular system, 2013 References This lecture Hand-outs Acute Myocardial Infarction A rapid development of myocardial necrosis caused by prolonged
Mario Plebani University-Hospital of Padova, Italy
 Mario Plebani University-Hospital of Padova, Italy CK-MB mass assay CHF guidelines use BNP for rule out AST in AMI CK in AMI INH for CK-MB electrophoresis for CK and LD isoenzymes RIA for myoglobin WHO
Mario Plebani University-Hospital of Padova, Italy CK-MB mass assay CHF guidelines use BNP for rule out AST in AMI CK in AMI INH for CK-MB electrophoresis for CK and LD isoenzymes RIA for myoglobin WHO
High-Sensitivity Cardiac Troponin in Suspected ACS
 15 th Annual Biomarkers in Heart Failure and Acute Coronary Syndromes STATE-OF-THE-ART High-Sensitivity Cardiac Troponin in Suspected ACS David A. Morrow, MD, MPH Director, Levine Cardiac Intensive Care
15 th Annual Biomarkers in Heart Failure and Acute Coronary Syndromes STATE-OF-THE-ART High-Sensitivity Cardiac Troponin in Suspected ACS David A. Morrow, MD, MPH Director, Levine Cardiac Intensive Care
Measuring Natriuretic Peptides in Acute Coronary Syndromes
 Measuring Natriuretic Peptides in Acute Coronary Syndromes Peter A. McCullough, MD, MPH, FACC, FACP, FAHA, FCCP Consultant Cardiologist Chief Academic and Scientific Officer St. John Providence Health
Measuring Natriuretic Peptides in Acute Coronary Syndromes Peter A. McCullough, MD, MPH, FACC, FACP, FAHA, FCCP Consultant Cardiologist Chief Academic and Scientific Officer St. John Providence Health
About OMICS International
 About OMICS International OMICS International through its Open Access Initiative is committed to make genuine and reliable contributions to the scientific community. OMICS International hosts over 700
About OMICS International OMICS International through its Open Access Initiative is committed to make genuine and reliable contributions to the scientific community. OMICS International hosts over 700
Defining rise and fall of cardiac troponin values
 Defining rise and fall of cardiac troponin values Doable but Not Simple Allan S. Jaffe, MD.* Consultant - Cardiology & Laboratory Medicine Professor of Medicine Chair, CCLS Division, Department of Laboratory
Defining rise and fall of cardiac troponin values Doable but Not Simple Allan S. Jaffe, MD.* Consultant - Cardiology & Laboratory Medicine Professor of Medicine Chair, CCLS Division, Department of Laboratory
High Sensitivity Troponins. IT S TIME TO SAVE LIVES. Updates from the ESC 2015 Guidelines November 17th 2016 OPL CONGRESS Dr.
 High Sensitivity Troponins. IT S TIME TO SAVE LIVES. Updates from the ESC 2015 Guidelines November 17th 2016 OPL CONGRESS Dr. Marcel El Achkar Chairperson of Laboratory department Nini Hospital Lecturer
High Sensitivity Troponins. IT S TIME TO SAVE LIVES. Updates from the ESC 2015 Guidelines November 17th 2016 OPL CONGRESS Dr. Marcel El Achkar Chairperson of Laboratory department Nini Hospital Lecturer
Congreso Nacional del Laboratorio Clínico 2016
 Can biomarkers help us make a better use of cardiac imaging for myocardial ischaemia rule-out in the Emergency Department? Alessandro Sionis Director Acute and Intensive Cardiac Care Unit Hospital de la
Can biomarkers help us make a better use of cardiac imaging for myocardial ischaemia rule-out in the Emergency Department? Alessandro Sionis Director Acute and Intensive Cardiac Care Unit Hospital de la
EDUCATIONAL COMMENTARY CARDIAC FUNCTION: BIOCHEMICAL MARKERS UPDATE
 EDUCATIONAL COMMENTARY CARDIAC FUNCTION: BIOCHEMICAL MARKERS UPDATE Educational commentary is provided through our affiliation with the American Society for Clinical Pathology (ASCP). To obtain FREE CME/CMLE
EDUCATIONAL COMMENTARY CARDIAC FUNCTION: BIOCHEMICAL MARKERS UPDATE Educational commentary is provided through our affiliation with the American Society for Clinical Pathology (ASCP). To obtain FREE CME/CMLE
Troponin Assessment. Does it Carry Clinical Message? Stefan Blankenberg. University Heart Center Hamburg
 Biomarkers for Optimal Management of Heart Failure Troponin Assessment Does it Carry Clinical Message? Stefan Blankenberg University Heart Center Hamburg Congress of the European Society of Cardiology
Biomarkers for Optimal Management of Heart Failure Troponin Assessment Does it Carry Clinical Message? Stefan Blankenberg University Heart Center Hamburg Congress of the European Society of Cardiology
How will new high sensitive troponins affect the criteria?
 How will new high sensitive troponins affect the criteria? Hugo A Katus MD Abteilung Innere Medizin III Kardiologie, Angiologie, Pulmologie Universitätsklinikum Heidelberg Even more sensitive: The new
How will new high sensitive troponins affect the criteria? Hugo A Katus MD Abteilung Innere Medizin III Kardiologie, Angiologie, Pulmologie Universitätsklinikum Heidelberg Even more sensitive: The new
TROPONINS HAVE THEY CHANGED YOUR
 TROPONINS HAVE THEY CHANGED YOUR PRACTICE THIS WEEK? Harvey White John Neutze Scholar Green Lane Cardiovascular Service and Cardiovascular Research Unit Auckland City Hospital, Auckland, New Zealand Disclosure
TROPONINS HAVE THEY CHANGED YOUR PRACTICE THIS WEEK? Harvey White John Neutze Scholar Green Lane Cardiovascular Service and Cardiovascular Research Unit Auckland City Hospital, Auckland, New Zealand Disclosure
Acute coronary syndrome. Dr LM Murray Chemical Pathology Block SA
 Acute coronary syndrome Dr LM Murray Chemical Pathology Block SA13-2014 Acute myocardial infarction (MI) MI is still the leading cause of death in many countries It is characterized by severe chest pain,
Acute coronary syndrome Dr LM Murray Chemical Pathology Block SA13-2014 Acute myocardial infarction (MI) MI is still the leading cause of death in many countries It is characterized by severe chest pain,
10 Ways to Make the Use of High Sensitivity Cardiac Troponin Values Easier and Better
 10 Ways to Make the Use of High Sensitivity Cardiac Troponin Values Easier and Better Allan S. Jaffe, MD.* Consultant - Cardiology & Laboratory Medicine Professor of Medicine Chair, CCLS Division, Department
10 Ways to Make the Use of High Sensitivity Cardiac Troponin Values Easier and Better Allan S. Jaffe, MD.* Consultant - Cardiology & Laboratory Medicine Professor of Medicine Chair, CCLS Division, Department
New diagnostic markers for acute coronary syndromes
 New diagnostic markers for acute coronary syndromes - Nye diagnostiske markørerer for akutt iskemisk hjertesykdom Bertil Lindahl, Professor Cardiology, Uppsala University and Uppsala Clinical Research
New diagnostic markers for acute coronary syndromes - Nye diagnostiske markørerer for akutt iskemisk hjertesykdom Bertil Lindahl, Professor Cardiology, Uppsala University and Uppsala Clinical Research
Risk Stratification of ACS Patients. Frans Van de Werf, MD, PhD University of Leuven, Belgium
 Risk Stratification of ACS Patients Frans Van de Werf, MD, PhD University of Leuven, Belgium Which type of ACS patients are we talking about to day? 4/14/2011 STEMI and NSTEMI in the NRMI registry from
Risk Stratification of ACS Patients Frans Van de Werf, MD, PhD University of Leuven, Belgium Which type of ACS patients are we talking about to day? 4/14/2011 STEMI and NSTEMI in the NRMI registry from
hs-c Tn I high sensitivity troponin I <17 min
 hs-c Tn I high sensitivity troponin I IFCC & ESC compliant 0/ h NSTEMI rule-out / rule-in algorithm POCT whole blood/plasma Results in < 7 minutes
hs-c Tn I high sensitivity troponin I IFCC & ESC compliant 0/ h NSTEMI rule-out / rule-in algorithm POCT whole blood/plasma Results in < 7 minutes
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE Centre for Clinical Practice
 NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE Centre for Clinical Practice Review consultation document Review of Clinical Guideline (CG95) Chest pain of recent onset: Assessment and diagnosis
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE Centre for Clinical Practice Review consultation document Review of Clinical Guideline (CG95) Chest pain of recent onset: Assessment and diagnosis
Acute Coronary Syndrome. Sonny Achtchi, DO
 Acute Coronary Syndrome Sonny Achtchi, DO Objectives Understand evidence based and practice based treatments for stabilization and initial management of ACS Become familiar with ACS risk stratification
Acute Coronary Syndrome Sonny Achtchi, DO Objectives Understand evidence based and practice based treatments for stabilization and initial management of ACS Become familiar with ACS risk stratification
EARLY DIAGNOSIS AND RISK STRATIFICATION IN PATIENTS WITH SYMPTOMS SUGGESTIVE OF ACUTE CORONARY SYNDROME
 DEPARTMENT OF CLINICAL SCIENCE AND EDUCATION, SÖDERSJUKHUSET Karolinska Institutet, Stockholm, Sweden EARLY DIAGNOSIS AND RISK STRATIFICATION IN PATIENTS WITH SYMPTOMS SUGGESTIVE OF ACUTE CORONARY SYNDROME
DEPARTMENT OF CLINICAL SCIENCE AND EDUCATION, SÖDERSJUKHUSET Karolinska Institutet, Stockholm, Sweden EARLY DIAGNOSIS AND RISK STRATIFICATION IN PATIENTS WITH SYMPTOMS SUGGESTIVE OF ACUTE CORONARY SYNDROME
To estimate the serum level of N-terminal pro-brain natriuretic peptide levels in acute coronary syndrome
 Original Research Article To estimate the serum level of N-terminal pro-brain natriuretic peptide levels in acute coronary syndrome Mohamed Yasar Arafath 1, K. Babu Raj 2* 1 First Year Post Graduate, 2
Original Research Article To estimate the serum level of N-terminal pro-brain natriuretic peptide levels in acute coronary syndrome Mohamed Yasar Arafath 1, K. Babu Raj 2* 1 First Year Post Graduate, 2
DIAGNOSTICS ASSESSMENT PROGRAMME
 DIAGNOSTICS ASSESSMENT PROGRAMME Evidence overview Early rule out or diagnosis of acute myocardial infarction: High-sensitivity troponin tests (Elecsys troponin T high-sensitive, ARCHITECT STAT highsensitivity
DIAGNOSTICS ASSESSMENT PROGRAMME Evidence overview Early rule out or diagnosis of acute myocardial infarction: High-sensitivity troponin tests (Elecsys troponin T high-sensitive, ARCHITECT STAT highsensitivity
7/31/2018. Overview of Next Generation Cardiac Troponin T High Sensitivity. Disclosures. Course Objectives: high sensitive Troponin T assay
 Overview of Next Generation Cardiac Troponin T High Sensitivity Arleen Francis Medical & Scientific Liaison Roche Diagnostics 1 Disclosures Arleen Francis is an employee of Roche Diagnostics and a member
Overview of Next Generation Cardiac Troponin T High Sensitivity Arleen Francis Medical & Scientific Liaison Roche Diagnostics 1 Disclosures Arleen Francis is an employee of Roche Diagnostics and a member
Post Operative Troponin Leak: David Smyth Christchurch New Zealand
 Post Operative Troponin Leak: Does It Really Matter? David Smyth Christchurch New Zealand Life Was Simple Once Transmural Infarction Subendocardial Infarction But the Blood Tests Were n t Perfect Creatine
Post Operative Troponin Leak: Does It Really Matter? David Smyth Christchurch New Zealand Life Was Simple Once Transmural Infarction Subendocardial Infarction But the Blood Tests Were n t Perfect Creatine
Troponin = 35. Objectives. Low Risk Chest Pain. Does this patient have ACS? Does this patient have ACS? Objectives
 Objectives Low Risk Chest Pain Jeffrey Tabas, MD Professor of Emergency Medicine Office of CME UCSF School of Medicine Improve speed and accuracy in assessing patients with possible ACS! Avoid pitfalls
Objectives Low Risk Chest Pain Jeffrey Tabas, MD Professor of Emergency Medicine Office of CME UCSF School of Medicine Improve speed and accuracy in assessing patients with possible ACS! Avoid pitfalls
Undetectable High Sensitivity Cardiac Troponin T Level in the Emergency Department and Risk of Myocardial Infarction
 Undetectable High Sensitivity Cardiac Troponin T Level in the Emergency Department and Risk of Myocardial Infarction Nadia Bandstein, MD; Rickard Ljung, MD, PhD; Magnus Johansson, MD, PhD; Martin Holzmann,
Undetectable High Sensitivity Cardiac Troponin T Level in the Emergency Department and Risk of Myocardial Infarction Nadia Bandstein, MD; Rickard Ljung, MD, PhD; Magnus Johansson, MD, PhD; Martin Holzmann,
BIOCHEMICAL EXAMINATION OF ACUTE MYOCARDIAL INFARCTION. Written by Lenka Fialová, translated by Jan Pláteník
 BIOCHEMICAL EXAMINATION OF ACUTE MYOCARDIAL INFARCTION 1 Structure of heart muscle Written by Lenka Fialová, translated by Jan Pláteník Heart muscle (myocardium) is a particular form of striated muscle,
BIOCHEMICAL EXAMINATION OF ACUTE MYOCARDIAL INFARCTION 1 Structure of heart muscle Written by Lenka Fialová, translated by Jan Pláteník Heart muscle (myocardium) is a particular form of striated muscle,
Post-Procedural Myocardial Injury or Infarction
 Post-Procedural Myocardial Injury or Infarction Hugo A Katus MD & Evangelos Giannitsis MD Abteilung Innere Medizin III Kardiologie, Angiologie, Pulmologie Universitätsklinikum Heidelberg Conflict of Interest:
Post-Procedural Myocardial Injury or Infarction Hugo A Katus MD & Evangelos Giannitsis MD Abteilung Innere Medizin III Kardiologie, Angiologie, Pulmologie Universitätsklinikum Heidelberg Conflict of Interest:
Classification of lab tests useful in cardiac disease Biochemical markers in Acute Coronary Syndromes (ACS) Redefinition of Myocardial Infarction (MI)
 Redefinition of Myocardial Infarction (MI)") Biochemical Markers in Cardiac Injury Dr Sami Saeed Assistant Professor/Consultant Chemical Pathologist Foundation University Medical College Fauji Foundation Hospital Rawalpindi Email: drsami@comsats.net.pk
Biochemical Markers in Cardiac Injury Dr Sami Saeed Assistant Professor/Consultant Chemical Pathologist Foundation University Medical College Fauji Foundation Hospital Rawalpindi Email: drsami@comsats.net.pk
Impact of Troponin Performance on Patient Care
 Impact of Troponin Performance on Patient Care Linda C, Rogers PhD, DABCC, FACB Agenda Introduction Diagnosis of MI Guidelines Troponin Assay differences Classification of troponin assays Guideline acceptable
Impact of Troponin Performance on Patient Care Linda C, Rogers PhD, DABCC, FACB Agenda Introduction Diagnosis of MI Guidelines Troponin Assay differences Classification of troponin assays Guideline acceptable
Supplementary Online Content
 Supplementary Online Content Rubini Giménez M, Twerenbold R, Boeddinghaus J, et al. Clinical effect of sex-specific cutoff values of high-sensitivity cardiac troponin T in suspected myocardial infarction.
Supplementary Online Content Rubini Giménez M, Twerenbold R, Boeddinghaus J, et al. Clinical effect of sex-specific cutoff values of high-sensitivity cardiac troponin T in suspected myocardial infarction.
Continuing Medical Education Post-Test
 Continuing Medical Education Post-Test Based on the information presented in this monograph, please choose one correct response for each of the following questions or statements. Record your answers on
Continuing Medical Education Post-Test Based on the information presented in this monograph, please choose one correct response for each of the following questions or statements. Record your answers on
What can we learn from EQAs and audits for cardiac marker testing?
 What can we learn from EQAs and audits for cardiac marker testing? Dr P. O. Collinson MA MB BChir FRCPath MD FACB Consultant Chemical Pathologist and Director of Clinical Blood Sciences, Head of Vascular
What can we learn from EQAs and audits for cardiac marker testing? Dr P. O. Collinson MA MB BChir FRCPath MD FACB Consultant Chemical Pathologist and Director of Clinical Blood Sciences, Head of Vascular
TYPE II MI. KC ACDIS LOCAL CHAPTER March 8, 2016
 TYPE II MI KC ACDIS LOCAL CHAPTER March 8, 2016 TYPE 2 MI DEFINITION: Acute coronary syndrome (ACS) encompasses a continuum of myocardial ischemia and infarction, which can make the diagnostic and coding
TYPE II MI KC ACDIS LOCAL CHAPTER March 8, 2016 TYPE 2 MI DEFINITION: Acute coronary syndrome (ACS) encompasses a continuum of myocardial ischemia and infarction, which can make the diagnostic and coding
Peri-operative Troponin Measurements - Pathophysiology and Prognosis
 Peri-operative Troponin Measurements - Pathophysiology and Prognosis Allan S. Jaffe, MD.* Consultant - Cardiology & Laboratory Medicine Professor of Medicine Chair, CCLS Division, Department of Laboratory
Peri-operative Troponin Measurements - Pathophysiology and Prognosis Allan S. Jaffe, MD.* Consultant - Cardiology & Laboratory Medicine Professor of Medicine Chair, CCLS Division, Department of Laboratory
Patients presenting with symptoms suggestive. Using biomarkers to obtain mechanistic insight and guide management in acute coronary syndrome
 Original Article Heart Metab. (2015) 67:4-8 Using biomarkers to obtain mechanistic insight and guide management in acute coronary syndrome Kai C. Wollert, MD Division of Molecular and Translational Cardiology,
Original Article Heart Metab. (2015) 67:4-8 Using biomarkers to obtain mechanistic insight and guide management in acute coronary syndrome Kai C. Wollert, MD Division of Molecular and Translational Cardiology,
12/18/2009 Resting and Maxi Resting and Max mal Coronary Blood Flow 2
 Coronary Artery Pathophysiology ACS / AMI LeRoy E. Rabbani, MD Director, Cardiac Inpatient Services Director, Cardiac Intensive Care Unit Professor of Clinical Medicine Major Determinants of Myocardial
Coronary Artery Pathophysiology ACS / AMI LeRoy E. Rabbani, MD Director, Cardiac Inpatient Services Director, Cardiac Intensive Care Unit Professor of Clinical Medicine Major Determinants of Myocardial
Hit the road Jack! W. FRANK PEACOCK, MD, FACEP, FACC
 Hit the road Jack! W. FRANK PEACOCK, MD, FACEP, FACC Visits 130,000,000 annually 10.4 M chest pain (8.0%) 4.1 M sent home non-cardiac 6.24 M suspected or actual cardiac 50,000 MIs 3.1 M non-cardiac (50%)
Hit the road Jack! W. FRANK PEACOCK, MD, FACEP, FACC Visits 130,000,000 annually 10.4 M chest pain (8.0%) 4.1 M sent home non-cardiac 6.24 M suspected or actual cardiac 50,000 MIs 3.1 M non-cardiac (50%)
9/18/2017. Disclosures. Cardiac Troponin: ER Utilization and the Next Generation
 Disclosures Cardiac Troponin: ER Utilization and the Next Generation Joshua Soldo is an employee of Roche Diagnostics within the division of Medical Scientific Affairs. Data presented is intended for purely
Disclosures Cardiac Troponin: ER Utilization and the Next Generation Joshua Soldo is an employee of Roche Diagnostics within the division of Medical Scientific Affairs. Data presented is intended for purely
Serial Changes in Highly Sensitive Troponin I Assay and Early Diagnosis of Myocardial Infarction JAMA. 2011;306(24):
:") ORIGINAL CONTRIBUTION Serial Changes in Highly Sensitive Troponin I Assay and Early Diagnosis of Myocardial Infarction Till Keller, MD Tanja Zeller, PhD Francisco Ojeda, PhD Stergios Tzikas, MD Lars Lillpopp
ORIGINAL CONTRIBUTION Serial Changes in Highly Sensitive Troponin I Assay and Early Diagnosis of Myocardial Infarction Till Keller, MD Tanja Zeller, PhD Francisco Ojeda, PhD Stergios Tzikas, MD Lars Lillpopp
BioRemarkable Symposium
 BACC BioRemarkable Symposium Acute Myocardial infarction Stefan Blankenberg University Heart Center Hamburg London, September 7th, 2017 Universitätsklinikum Hamburg-Eppendorf Third Universal-Definition
BACC BioRemarkable Symposium Acute Myocardial infarction Stefan Blankenberg University Heart Center Hamburg London, September 7th, 2017 Universitätsklinikum Hamburg-Eppendorf Third Universal-Definition
Managing Quality of ACS Care in VHA The IDH Guideline Key Points and Metrics
 Managing Quality of ACS Care in VHA The IDH Guideline Key Points and Metrics Robert L. Jesse, MD, PhD National Program Director for Cardiology Veterans Health Administration Washington, DC Chief, Cardiology
Managing Quality of ACS Care in VHA The IDH Guideline Key Points and Metrics Robert L. Jesse, MD, PhD National Program Director for Cardiology Veterans Health Administration Washington, DC Chief, Cardiology
Diagnostics consultation document
 National Institute for Health and Care Excellence Diagnostics consultation document Myocardial infarction (acute): Early rule out using high-sensitivity troponin tests (Elecsys Troponin T high-sensitive,
National Institute for Health and Care Excellence Diagnostics consultation document Myocardial infarction (acute): Early rule out using high-sensitivity troponin tests (Elecsys Troponin T high-sensitive,
Biochemical risk assessment and invasive strategies for acute coronary syndromes without ST-segment elevation Riezebos, R.K.
 UvA-DARE (Digital Academic Repository) Biochemical risk assessment and invasive strategies for acute coronary syndromes without ST-segment elevation Riezebos, R.K. Link to publication Citation for published
UvA-DARE (Digital Academic Repository) Biochemical risk assessment and invasive strategies for acute coronary syndromes without ST-segment elevation Riezebos, R.K. Link to publication Citation for published
Waiting for High-Sensitivity POCT Cardiac Troponin Assays: Clinical and Analytical Needs I Have a Pain in My Chest That Hurts Very Bad
 Waiting for High-Sensitivity POCT Cardiac Troponin Assays: Clinical and Analytical Needs I Have a Pain in My Chest That Hurts Very Bad Fred Apple PhD Hennepin County Medical Center University of Minnesota
Waiting for High-Sensitivity POCT Cardiac Troponin Assays: Clinical and Analytical Needs I Have a Pain in My Chest That Hurts Very Bad Fred Apple PhD Hennepin County Medical Center University of Minnesota
Low Risk Chest Pain. Objectives. Disclosure. Case 1. Jeffrey Tabas, MD Professor of Emergency Medicine Office of CME UCSF School of Medicine
 Disclosure Low Risk Chest Pain No Financial Relationships to Disclose No significant investments or savings Unlimited Expenses Jeffrey Tabas, MD Professor of Emergency Medicine Office of CME UCSF School
Disclosure Low Risk Chest Pain No Financial Relationships to Disclose No significant investments or savings Unlimited Expenses Jeffrey Tabas, MD Professor of Emergency Medicine Office of CME UCSF School
Diagnostics guidance Published: 1 October 2014 nice.org.uk/guidance/dg15
 Myocardial infarction (acute): Early rule out using high-sensitivity troponin tests (Elecsys Troponin T high-sensitive, e, ARCHITECT STAT T High Sensitive Troponin-I and AccuTnI+3 assays) Diagnostics guidance
Myocardial infarction (acute): Early rule out using high-sensitivity troponin tests (Elecsys Troponin T high-sensitive, e, ARCHITECT STAT T High Sensitive Troponin-I and AccuTnI+3 assays) Diagnostics guidance
e356 Downloaded from by on October 4, 2018
 National Academy of Clinical Biochemistry Laboratory Medicine Practice Guidelines: Clinical Characteristics and Utilization of Biochemical Markers in Acute Coronary Syndromes NACB WRITING GROUP MEMBERS
National Academy of Clinical Biochemistry Laboratory Medicine Practice Guidelines: Clinical Characteristics and Utilization of Biochemical Markers in Acute Coronary Syndromes NACB WRITING GROUP MEMBERS
BIOCHEMICAL INVESTIGATIONS IN THE DIAGNOSTICS OF CARDIOVASCULAR DISORDERS. As. MARUSHCHAK M.I.
 BIOCHEMICAL INVESTIGATIONS IN THE DIAGNOSTICS OF CARDIOVASCULAR DISORDERS As. MARUSHCHAK M.I. Heart attack symptoms Acute MI Measurement of cardiac enzyme levels Measure cardiac enzyme levels at regular
BIOCHEMICAL INVESTIGATIONS IN THE DIAGNOSTICS OF CARDIOVASCULAR DISORDERS As. MARUSHCHAK M.I. Heart attack symptoms Acute MI Measurement of cardiac enzyme levels Measure cardiac enzyme levels at regular
Chest pain and troponins on the acute take. J N Townend Queen Elizabeth Hospital Birmingham
 Chest pain and troponins on the acute take J N Townend Queen Elizabeth Hospital Birmingham 3 rd Universal Definition of Myocardial Infarction Type 1: Spontaneous MI related to atherosclerotic plaque rupture
Chest pain and troponins on the acute take J N Townend Queen Elizabeth Hospital Birmingham 3 rd Universal Definition of Myocardial Infarction Type 1: Spontaneous MI related to atherosclerotic plaque rupture
Laboratory diagnosis of heart diseases: Cardiometabolic risk AMI Heart failure
 Laboratory diagnosis of heart diseases: 2017 Cardiometabolic risk AMI Heart failure 2 Suggested Risk Factors for CVD LDL Oxidation LDL-C Anti-OxLDL OxLDL LDL Oxid. Lag Time Negative LDL HDL-C Paraoxonase
Laboratory diagnosis of heart diseases: 2017 Cardiometabolic risk AMI Heart failure 2 Suggested Risk Factors for CVD LDL Oxidation LDL-C Anti-OxLDL OxLDL LDL Oxid. Lag Time Negative LDL HDL-C Paraoxonase
Essam Mahfouz, MD. Professor of Cardiology, Mansoura University
 By Essam Mahfouz, MD. Professor of Cardiology, Mansoura University Agenda Definitions Classifications Epidemiology Risk stratification What is new? What is MI? Myocardial infarction is the death of part
By Essam Mahfouz, MD. Professor of Cardiology, Mansoura University Agenda Definitions Classifications Epidemiology Risk stratification What is new? What is MI? Myocardial infarction is the death of part
ACCESS hstni SCIENTIFIC LITERATURE
 ACCESS hstni SCIENTIFIC LITERATURE 2017 2018 Table of contents Performance Evaluation of Access hstni A critical evaluation of the Beckman Coulter Access hstni: Analytical performance, reference interval
ACCESS hstni SCIENTIFIC LITERATURE 2017 2018 Table of contents Performance Evaluation of Access hstni A critical evaluation of the Beckman Coulter Access hstni: Analytical performance, reference interval
Rikshospitalet, University of Oslo
 Rikshospitalet, University of Oslo Preventing heart failure by preventing coronary artery disease progression European Society of Cardiology Dyslipidemia 29.08.2010 Objectives The trends in cardiovascular
Rikshospitalet, University of Oslo Preventing heart failure by preventing coronary artery disease progression European Society of Cardiology Dyslipidemia 29.08.2010 Objectives The trends in cardiovascular
What oral antiplatelet therapy would you choose? a) ASA alone b) ASA + Clopidogrel c) ASA + Prasugrel d) ASA + Ticagrelor
 ASA alone b) ASA + Clopidogrel c) ASA + Prasugrel d) ASA + Ticagrelor") 76 year old female Prior Hypertension, Hyperlipidemia, Smoking On Hydrochlorothiazide, Atorvastatin New onset chest discomfort; 2 episodes in past 24 hours Heart rate 122/min; BP 170/92 mm Hg, Killip Class
76 year old female Prior Hypertension, Hyperlipidemia, Smoking On Hydrochlorothiazide, Atorvastatin New onset chest discomfort; 2 episodes in past 24 hours Heart rate 122/min; BP 170/92 mm Hg, Killip Class
IFCC Task Force on Clinical Applications of Cardiac Biomarkers (TF-CB) Report to the General Conference 2016 Madrid
 Report to the General Conference 2016 Madrid") IFCC Task Force on Clinical Applications of Cardiac Biomarkers (TF-CB) Report to the General Conference 2016 Madrid 1 CREATED By the EB in 2011, following to the Committee on Standardization of Cardiac
IFCC Task Force on Clinical Applications of Cardiac Biomarkers (TF-CB) Report to the General Conference 2016 Madrid 1 CREATED By the EB in 2011, following to the Committee on Standardization of Cardiac
Fifty shades of Troponin. Dr Liam Penny The Queens Hotel, Cheltenham 4 th October 2012
 Fifty shades of Troponin Dr Liam Penny The Queens Hotel, Cheltenham 4 th October 2012 Plaque-fissure and intracoronary thrombus Courtesy Prof. MJ Davies Acute Coronary Syndromes Plaque-fissure and intracoronary
Fifty shades of Troponin Dr Liam Penny The Queens Hotel, Cheltenham 4 th October 2012 Plaque-fissure and intracoronary thrombus Courtesy Prof. MJ Davies Acute Coronary Syndromes Plaque-fissure and intracoronary
DIFFERENTIATING THE PATIENT WITH UNDIFFERENTIATED CHEST PAIN
 DIFFERENTIATING THE PATIENT WITH UNDIFFERENTIATED CHEST PAIN Objectives Gain competence in evaluating chest pain Recognize features of moderate risk unstable angina Review initial management of UA and
DIFFERENTIATING THE PATIENT WITH UNDIFFERENTIATED CHEST PAIN Objectives Gain competence in evaluating chest pain Recognize features of moderate risk unstable angina Review initial management of UA and
The Clinical Laboratory Working with Physicians to Improve Patient Care
 The Clinical Laboratory Working with Physicians to Improve Patient Care Michael A. Pesce, PhD Professor Emeritus Columbia University Medical Center Department of Pathology and Cell Biology Objectives Troponin
The Clinical Laboratory Working with Physicians to Improve Patient Care Michael A. Pesce, PhD Professor Emeritus Columbia University Medical Center Department of Pathology and Cell Biology Objectives Troponin
Undetectable High Sensitivity Cardiac Troponin T Level in the Emergency Department and Risk of Myocardial Infarction
 Undetectable High Sensitivity Cardiac Troponin T Level in the Emergency Department and Risk of Myocardial Infarction Nadia Bandstein, MD; Rickard Ljung, MD, PhD; Magnus Johansson, MD, PhD; Martin Holzmann,
Undetectable High Sensitivity Cardiac Troponin T Level in the Emergency Department and Risk of Myocardial Infarction Nadia Bandstein, MD; Rickard Ljung, MD, PhD; Magnus Johansson, MD, PhD; Martin Holzmann,
An update on the management of UA / NSTEMI. Michael H. Crawford, MD
 An update on the management of UA / NSTEMI Michael H. Crawford, MD New ACC/AHA Guidelines 2007 What s s new in the last 5 years CT imaging advances Ascendancy of troponin and BNP Clarification of ACEI/ARB
An update on the management of UA / NSTEMI Michael H. Crawford, MD New ACC/AHA Guidelines 2007 What s s new in the last 5 years CT imaging advances Ascendancy of troponin and BNP Clarification of ACEI/ARB
Cardiac Bio-Marker Testing in Acute Coronary Syndromes
 Cardiac Bio-Marker Testing in Acute Coronary Syndromes Dr. Zohair Alaseri, MD FRCPc, Emergency Medicine FRCPc, Critical Care Medicine Intensivest and Emergency Medicine Consultant Chairman, Department
Cardiac Bio-Marker Testing in Acute Coronary Syndromes Dr. Zohair Alaseri, MD FRCPc, Emergency Medicine FRCPc, Critical Care Medicine Intensivest and Emergency Medicine Consultant Chairman, Department
Pharmacologyonline 2: (2010) Newsletter Kakadiya and Shah
 Newsletter Kakadiya and Shah") ROLE OF CREATINE KINASE MB AND LACTATE DEHYDROGENASE IN CARDIAC FUNCTION A REVIEW Jagdish Kakadiya*, Nehal Shah Department of Pharmacology, Dharmaj Degree Pharmacy College, Petlad- Khambhat Road, Dharmaj,
ROLE OF CREATINE KINASE MB AND LACTATE DEHYDROGENASE IN CARDIAC FUNCTION A REVIEW Jagdish Kakadiya*, Nehal Shah Department of Pharmacology, Dharmaj Degree Pharmacy College, Petlad- Khambhat Road, Dharmaj,
TROPONIN POSITIVE 2/20/2015 WHAT DOES IT MEAN? When should a troponin level be obtained?
 TROPONIN POSITIVE WHAT DOES IT MEAN? Frequently Asked Questions Regarding the Use of Troponin in the Clinical Setting What does an elevated troponin level mean? Elevated troponin is a sensitive and specific
TROPONIN POSITIVE WHAT DOES IT MEAN? Frequently Asked Questions Regarding the Use of Troponin in the Clinical Setting What does an elevated troponin level mean? Elevated troponin is a sensitive and specific
ACUTE CORONARY SYNDROME PCI IN THE ELDERLY
 ACUTE CORONARY SYNDROME PCI IN THE ELDERLY G.KARABELA MD.PhD ATHENS NAVAL HOSPITAL INTERVENTIONAL CARDIOLOGY DEPARTMENT NO CONFLICT OF INTEREST TO DECLAIRE Risk stratification in Αcute Coronary Syndrome.
ACUTE CORONARY SYNDROME PCI IN THE ELDERLY G.KARABELA MD.PhD ATHENS NAVAL HOSPITAL INTERVENTIONAL CARDIOLOGY DEPARTMENT NO CONFLICT OF INTEREST TO DECLAIRE Risk stratification in Αcute Coronary Syndrome.
EDUCATIONAL COMMENTARY UNDERSTANDING THE BENEFITS AND CHALLENGES OF HIGH- SENSITIVITY TROPONIN TESTING IN CLINICAL AND PATHOLOGY SETTINGS
 SENSITIVITY TROPONIN TESTING IN CLINICAL AND PATHOLOGY SETTINGS Educational commentary is provided through our affiliation with the American Society for Clinical Pathology (ASCP). To obtain FREE CME/CMLE
SENSITIVITY TROPONIN TESTING IN CLINICAL AND PATHOLOGY SETTINGS Educational commentary is provided through our affiliation with the American Society for Clinical Pathology (ASCP). To obtain FREE CME/CMLE
FastTest. You ve read the book now test yourself
 FastTest You ve read the book...... now test yourself To ensure you have learned the key points that will improve your patient care, read the authors questions below. The answers will refer you back to
FastTest You ve read the book...... now test yourself To ensure you have learned the key points that will improve your patient care, read the authors questions below. The answers will refer you back to
Rapid exclusion of acute myocardial infarction in patients with undetectable troponin using a sensitive troponin I assay
 Original Article Annals of Clinical Biochemistry 2015, Vol. 52(5) 543 549! The Author(s) 2015 Reprints and permissions: sagepub.co.uk/journalspermissions.nav DOI: 10.1177/0004563215576976 acb.sagepub.com
Original Article Annals of Clinical Biochemistry 2015, Vol. 52(5) 543 549! The Author(s) 2015 Reprints and permissions: sagepub.co.uk/journalspermissions.nav DOI: 10.1177/0004563215576976 acb.sagepub.com
RESPONSES TO COMMENTS ON: Recommendations for Use of Point-of-Care (POC) Troponin Assays in Assessment of Acute Coronary Syndrome
 Troponin Assays in Assessment of Acute Coronary Syndrome") RESPONSES TO COMMENTS ON: Recommendations for Use of Point-of-Care (POC) Troponin Assays in Assessment of Acute Coronary Syndrome Page 1 Responses were received from: 1. Chemical Pathology Clinical Stream,
RESPONSES TO COMMENTS ON: Recommendations for Use of Point-of-Care (POC) Troponin Assays in Assessment of Acute Coronary Syndrome Page 1 Responses were received from: 1. Chemical Pathology Clinical Stream,
Multi-marker approach with the use of biochip cardiac array technology for early diagnosis in patients with acute coronary syndromes
 Multi-marker approach with the use of biochip cardiac array technology for early diagnosis in patients with acute coronary syndromes Marcin Sawicki, Grazyna Sypniewska, Magdalena Krintus, Marek Kozinski
Multi-marker approach with the use of biochip cardiac array technology for early diagnosis in patients with acute coronary syndromes Marcin Sawicki, Grazyna Sypniewska, Magdalena Krintus, Marek Kozinski
Acute Coronary Syndrome. Cindy Baker, MD FACC Director Peripheral Vascular Interventions Division of Cardiovascular Medicine
 Acute Coronary Syndrome Cindy Baker, MD FACC Director Peripheral Vascular Interventions Division of Cardiovascular Medicine Topics Timing is everything So many drugs to choose from What s a MINOCA? 2 Acute
Acute Coronary Syndrome Cindy Baker, MD FACC Director Peripheral Vascular Interventions Division of Cardiovascular Medicine Topics Timing is everything So many drugs to choose from What s a MINOCA? 2 Acute
Timing of angiography for high- risk ACS
 Timing of angiography for high- risk ACS Christian Spaulding, MD, PhD, FESC, FACC Cardiology Department Cochin Hospital, Inserm U 970 Paris Descartes University Paris, France A very old story. The Interventional
Timing of angiography for high- risk ACS Christian Spaulding, MD, PhD, FESC, FACC Cardiology Department Cochin Hospital, Inserm U 970 Paris Descartes University Paris, France A very old story. The Interventional
Quantitative Measurement of Emergency Biomarkers in Parallel
 Point-of-Care Immunoassay Analyzer Quantitative Measurement of Emergency Biomarkers in Parallel Troponin I, Myoglobin, CK-MB, D-Dimer, NTproBNP, hscrp Results in 17 minutes Direct measurement from whole
Point-of-Care Immunoassay Analyzer Quantitative Measurement of Emergency Biomarkers in Parallel Troponin I, Myoglobin, CK-MB, D-Dimer, NTproBNP, hscrp Results in 17 minutes Direct measurement from whole
DISCUSSION QUESTION - 1
 CASE PRESENTATION 87 year old male No past history of diabetes, HTN, dyslipidemia or smoking Very active Medications: omeprazole for heart burn Admitted because of increasing retrosternal chest pressure
CASE PRESENTATION 87 year old male No past history of diabetes, HTN, dyslipidemia or smoking Very active Medications: omeprazole for heart burn Admitted because of increasing retrosternal chest pressure
High-sensitivity Troponin T Predicts Recurrent Cardiovascular Events in Patients with Stable Coronary Heart Disease: KAROLA Study 8 Year FU
 ESC Congress 2011 Paris, France, August 27-31 KAROLA Session: Prevention: Are biomarkers worth their money? Abstract # 84698 High-sensitivity Troponin T Predicts Recurrent Cardiovascular Events in Patients
ESC Congress 2011 Paris, France, August 27-31 KAROLA Session: Prevention: Are biomarkers worth their money? Abstract # 84698 High-sensitivity Troponin T Predicts Recurrent Cardiovascular Events in Patients
Chest pain management. Ruvin Gabriel and Niels van Pelt August 2011
 Chest pain management Ruvin Gabriel and Niels van Pelt August 2011 Introduction Initial assessment Case 1 Case 2 and 3 Comparison of various diagnostic techniques Summary 1-2 % of GP consultations are
Chest pain management Ruvin Gabriel and Niels van Pelt August 2011 Introduction Initial assessment Case 1 Case 2 and 3 Comparison of various diagnostic techniques Summary 1-2 % of GP consultations are
Rapid detection of myocardial infarction with a sensitive troponin test Scharnhorst, V.; Krasznai, K.; van 't Veer, M.; Michels, R.
 Rapid detection of myocardial infarction with a sensitive troponin test Scharnhorst, V.; Krasznai, K.; van 't Veer, M.; Michels, R. Published in: American Journal of Clinical Pathology DOI: 10.1309/AJCPA4G8AQOYEKLD
Rapid detection of myocardial infarction with a sensitive troponin test Scharnhorst, V.; Krasznai, K.; van 't Veer, M.; Michels, R. Published in: American Journal of Clinical Pathology DOI: 10.1309/AJCPA4G8AQOYEKLD
Non ST Elevation-ACS. Michael W. Cammarata, MD
 Non ST Elevation-ACS Michael W. Cammarata, MD Case Presentation 65 year old man PMH: CAD s/p stent in 2008 HTN HLD Presents with chest pressure, substernally and radiating to the left arm and jaw, similar
Non ST Elevation-ACS Michael W. Cammarata, MD Case Presentation 65 year old man PMH: CAD s/p stent in 2008 HTN HLD Presents with chest pressure, substernally and radiating to the left arm and jaw, similar
Statistical analysis plan
 Statistical analysis plan Prepared and approved for the BIOMArCS 2 glucose trial by Prof. Dr. Eric Boersma Dr. Victor Umans Dr. Jan Hein Cornel Maarten de Mulder Statistical analysis plan - BIOMArCS 2
Statistical analysis plan Prepared and approved for the BIOMArCS 2 glucose trial by Prof. Dr. Eric Boersma Dr. Victor Umans Dr. Jan Hein Cornel Maarten de Mulder Statistical analysis plan - BIOMArCS 2
Adults With Diagnosed Diabetes
 Adults With Diagnosed Diabetes 1990 No data available Less than 4% 4%-6% Above 6% Mokdad AH, et al. Diabetes Care. 2000;23(9):1278-1283. Adults With Diagnosed Diabetes 2000 4%-6% Above 6% Mokdad AH, et
Adults With Diagnosed Diabetes 1990 No data available Less than 4% 4%-6% Above 6% Mokdad AH, et al. Diabetes Care. 2000;23(9):1278-1283. Adults With Diagnosed Diabetes 2000 4%-6% Above 6% Mokdad AH, et
Prehospital and Hospital Care of Acute Coronary Syndrome
 Ischemic Heart Diseases Prehospital and Hospital Care of Acute Coronary Syndrome JMAJ 46(8): 339 346, 2003 Katsuo KANMATSUSE* and Ikuyoshi WATANABE** * Professor, Second Internal Medicine, Nihon University,
Ischemic Heart Diseases Prehospital and Hospital Care of Acute Coronary Syndrome JMAJ 46(8): 339 346, 2003 Katsuo KANMATSUSE* and Ikuyoshi WATANABE** * Professor, Second Internal Medicine, Nihon University,
Long-term prognostic value of N-Terminal Pro-Brain Natriuretic Peptide (NT-proBNP) changes within one year in patients with coronary heart disease
 changes within one year in patients with coronary heart disease") Long-term prognostic value of N-Terminal Pro-Brain Natriuretic Peptide (NT-proBNP) changes within one year in patients with coronary heart disease D. Dallmeier 1, D. Rothenbacher 2, W. Koenig 1, H. Brenner
Long-term prognostic value of N-Terminal Pro-Brain Natriuretic Peptide (NT-proBNP) changes within one year in patients with coronary heart disease D. Dallmeier 1, D. Rothenbacher 2, W. Koenig 1, H. Brenner
Current and Future Imaging Trends in Risk Stratification for CAD
 Current and Future Imaging Trends in Risk Stratification for CAD Brian P. Griffin, MD FACC Department of Cardiovascular Medicine, Heart and Vascular Institute, Cleveland Clinic Disclosures: None Introduction
Current and Future Imaging Trends in Risk Stratification for CAD Brian P. Griffin, MD FACC Department of Cardiovascular Medicine, Heart and Vascular Institute, Cleveland Clinic Disclosures: None Introduction
Quantitative Measurement of Cardiac Biomarkers
 Cardiac Biomarker Analyzer Quantitative Measurement of Cardiac Biomarkers Troponin I, Myoglobin, CK-MB, D-Dimer, NTproBNP, hscrp Results in 17 minutes Direct measurement from whole blood samples 6 parallel
Cardiac Biomarker Analyzer Quantitative Measurement of Cardiac Biomarkers Troponin I, Myoglobin, CK-MB, D-Dimer, NTproBNP, hscrp Results in 17 minutes Direct measurement from whole blood samples 6 parallel
Evaluation of analytical quality of cardiac biomarkers in the emergency laboratory by sigma metrics
 r l a Re s e a r c h g i O in Evaluation of analytical quality of cardiac biomarkers in the emergency laboratory by sigma metrics Fatma Ceyla Eraldemir Department of Biochemistry, Kocaeli University School
r l a Re s e a r c h g i O in Evaluation of analytical quality of cardiac biomarkers in the emergency laboratory by sigma metrics Fatma Ceyla Eraldemir Department of Biochemistry, Kocaeli University School
Biomarkers in Heart Disease. Felix J. Rogers, DO, FACOI April 29, 2018
 Biomarkers in Heart Disease Felix J. Rogers, DO, FACOI April 29, 2018 Biomarkers NIH: A biomarker is a characteristic that is objectively measured and evaluated as an indicator of normal biological processes,
Biomarkers in Heart Disease Felix J. Rogers, DO, FACOI April 29, 2018 Biomarkers NIH: A biomarker is a characteristic that is objectively measured and evaluated as an indicator of normal biological processes,
Assays Pros and Cons AACB 2013 GOLD COAST QUEENSLAND AUSTRALIA
 Highly Sensitive Versus Sensitive Troponin Assays Pros and Cons AACB 2013 GOLD COAST QUEENSLAND AUSTRALIA Robert H. Christenson, Ph.D., DABCC, FACB 2013 AACC President Professor of Pathology Professor
Highly Sensitive Versus Sensitive Troponin Assays Pros and Cons AACB 2013 GOLD COAST QUEENSLAND AUSTRALIA Robert H. Christenson, Ph.D., DABCC, FACB 2013 AACC President Professor of Pathology Professor
Lnformation Coverage Guidance
 Lnformation Coverage Guidance Coverage Indications, Limitations, and/or Medical Necessity Abstract: B-type natriuretic peptide (BNP) is a cardiac neurohormone produced mainly in the left ventricle. It
Lnformation Coverage Guidance Coverage Indications, Limitations, and/or Medical Necessity Abstract: B-type natriuretic peptide (BNP) is a cardiac neurohormone produced mainly in the left ventricle. It
International Journal of Cardiology and Cardiovascular Research Vol. 4(2), pp , September, ISSN:
, pp , September, ISSN:") International Journal of Cardiology and Cardiovascular Research Vol. 4(2), pp. 072-078, September, 2018. www.premierpublishers.org, ISSN: 3102-9869 IJCCR Research Article Copeptin as a Novel Biomarker
International Journal of Cardiology and Cardiovascular Research Vol. 4(2), pp. 072-078, September, 2018. www.premierpublishers.org, ISSN: 3102-9869 IJCCR Research Article Copeptin as a Novel Biomarker
High-Sensitive Troponin in the Evaluation of patients with Acute Coronary Syndrome (High-STEACS): a stepped-wedge cluster-randomised controlled trial
: a stepped-wedge cluster-randomised controlled trial") EUROPEAN SOCIETY OF CARDIOLOGY CONGRESS 2018 High-Sensitive Troponin in the Evaluation of patients with Acute Coronary Syndrome (High-STEACS): a stepped-wedge cluster-randomised controlled trial Professor
EUROPEAN SOCIETY OF CARDIOLOGY CONGRESS 2018 High-Sensitive Troponin in the Evaluation of patients with Acute Coronary Syndrome (High-STEACS): a stepped-wedge cluster-randomised controlled trial Professor
Beta-blockers in Patients with Mid-range Left Ventricular Ejection Fraction after AMI Improved Clinical Outcomes
 Beta-blockers in Patients with Mid-range Left Ventricular Ejection Fraction after AMI Improved Clinical Outcomes Seung-Jae Joo and other KAMIR-NIH investigators Department of Cardiology, Jeju National
Beta-blockers in Patients with Mid-range Left Ventricular Ejection Fraction after AMI Improved Clinical Outcomes Seung-Jae Joo and other KAMIR-NIH investigators Department of Cardiology, Jeju National
Topic. Updates on Definition of Myocardial Infarction
 Topic Updates on Definition of Myocardial Infarction In the past, general consensus for MI? Definition of MI by WHO - Combination of 2 of 3 characteristics - 1. Typical Symptoms 2. Enzyme Rise 3. Typical
Topic Updates on Definition of Myocardial Infarction In the past, general consensus for MI? Definition of MI by WHO - Combination of 2 of 3 characteristics - 1. Typical Symptoms 2. Enzyme Rise 3. Typical
Does serial troponin measurement help identify acute ischemia/ischemic events?
 Does serial troponin measurement help identify acute ischemia/ischemic events? Allan S. Jaffe, MD.* Consultant - Cardiology & Laboratory Medicine Professor of Medicine and Laboratory Medicine & Pathology
Does serial troponin measurement help identify acute ischemia/ischemic events? Allan S. Jaffe, MD.* Consultant - Cardiology & Laboratory Medicine Professor of Medicine and Laboratory Medicine & Pathology