Cardiovascular Pharmacotherapy
|
|
|
- Rafe Benson
- 5 years ago
- Views:
Transcription

1 Cardiovascular Pharmacotherapy
2 Overview Mechanism of cardiovascular drugs Indications and clinical use in cardiology


3 Renin-Angiotensin Inhibitors: Angiotensin-Converting Enzyme Inhibitors, Angiotensin Receptor Blockers

4 ACE-I, ARB
5 Cardiorenal Effects of ACE Inhibitors Vasodilation (arterial & venous) - reduce arterial & venous pressure - reduce ventricular afterload & preload Decrease blood volume - natriuretic - diuretic Depress sympathetic activity Inhibit cardiac and vascular hypertrophy
6 ACE-I, ARB Therapeutic Use: Hypertension Heart failure Post-myocardial infarction
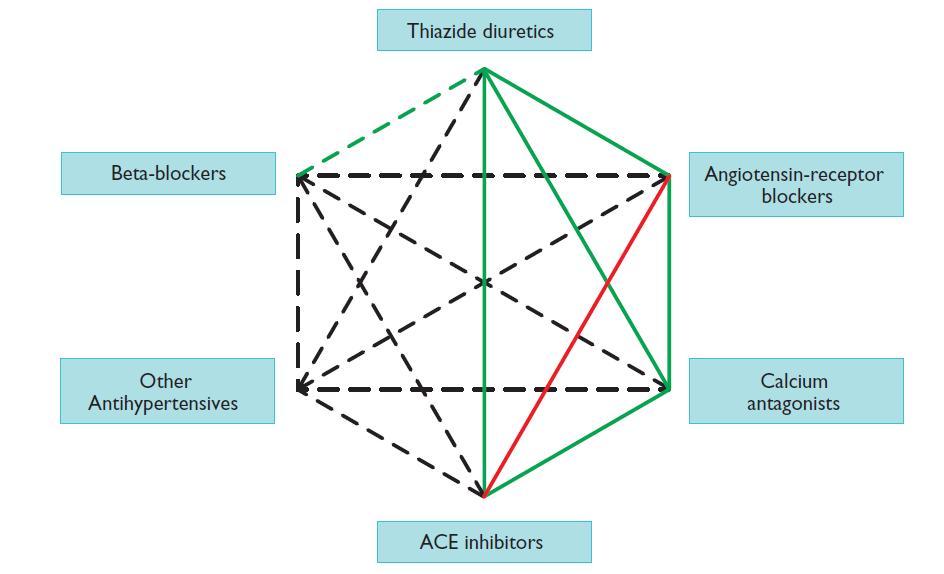
7 ACE-I, ARB à Hypertension RAS inhibitors are among the best tolerated of the antihypertensive drugs Reduce CV events and preventing deterioration of renal function in high-risk hypertensive patients Dual RAS blockade either with an ACEI plus an ARB is now contraindicated due to hypotension, acute kidney injury (AKI), and hyperkalemia As monotherapy, ACEIs are generally less effective in lowering BP in black patients and in older patients with low-renin hypertension, but they are quite effective in these groups when combined with a CCB or low-dose diuretic
8 ACE-I, ARB ARBs confer the same benefits as ACEIs in treating hypertension while avoiding the ACEI-related cough and angioedema ACEIs and ARBs have become standard first-line antihypertensive therapy for patients with diabetic and nondiabetic CKD, but evidence indicates that RAS inhibitors provide superior renal protection than do other antihypertensive agents, mainly for nondiabetic proteinuric CKD
9
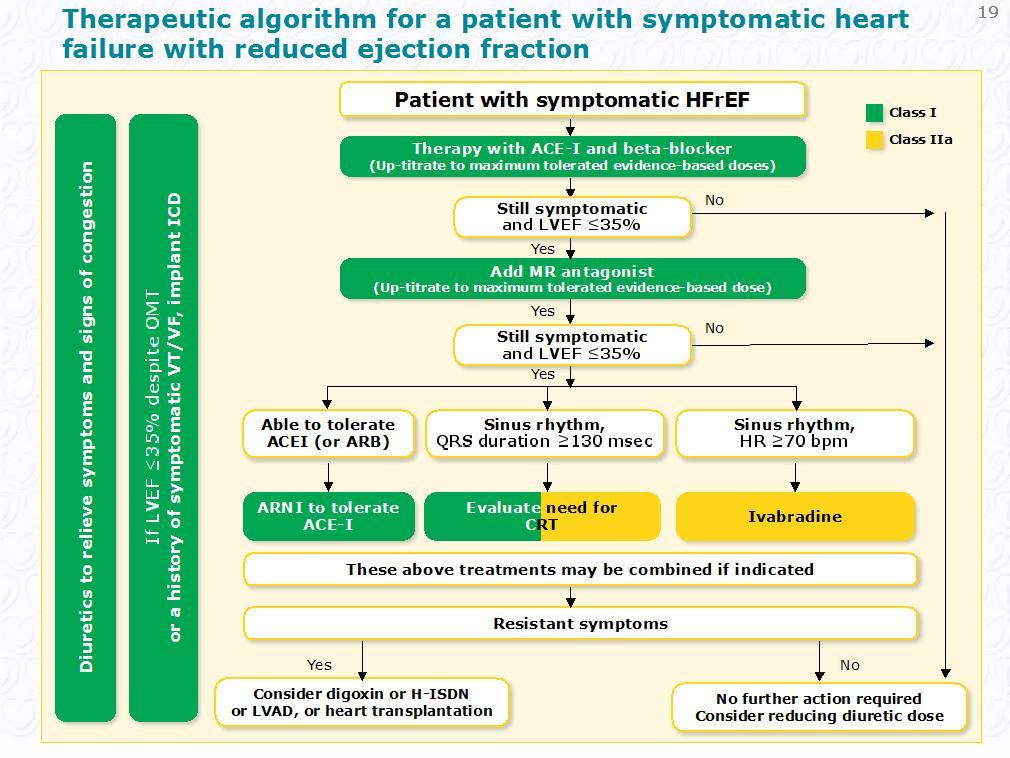
10 ACE-I, ARB à Heart failure There is overwhelming evidence that ACEIs should be used in symptomatic and asymptomatic patients with a reduced EF (<40%). ACEIs stabilize LV remodeling, improve patient symptoms, prevent hospitalization, and prolong life.
11
12
13 Side effects dry cough (ACE-I) angioedema (ACE-I) hyperkalemia ACEIs and ARBs can provoke hyperkalemia in the setting of CKD fetal renal agenesis and other birth defects (contraindicated in pregnancy )
14 Contrindication ACE inhibitors Pregnancy History of angioedema Bilateral renal artery stenosis Known allergic reaction/other adverse reaction (drug-specific)
15 Cautions/seek specialist advice: 1. Significant hyperkalemia (K+>5.0 mmol/l) 2. Significant renal disfunction (creatinine >2.5 mg/dl or GFR <30 ml/min/1,73m2). 3. Symptomatic or severe asymptomatic hypotension (systolic blood pressure <90 mmhg). 4. Drug interactions to look out for: o K+ supplements/ K+-sparing diuretics, e.g. amiloride and triamterene (beware combination preparations with furosemide). o MRAs. o Renin inhibitorsc. o NSAIDsd. o Trimethoprim/trimethoprim-sulfamethoxazole. o Low-salt substitutes with a high K+ content
 or membrane stabilizing activity (MSA).")
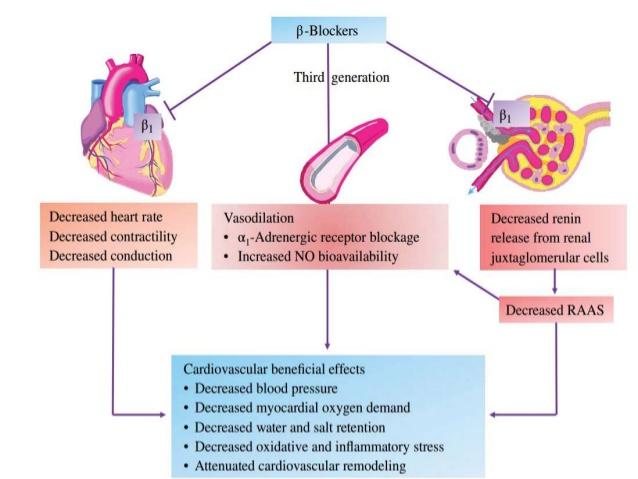
16 Beta-Adrenoceptor Antagonists (Beta-Blockers) bind to beta-adrenoceptors and block the binding of norepinephrine and epinephrine to these receptors sympatholytic drugs Some beta-blockers possess intrinsic sympathomimetic activity (ISA) or membrane stabilizing activity (MSA).
17 Beta-Adrenoceptor Antagonists (Beta-Blockers)
18
19 Therapeutic Indications Beta-Blockers - hypertension - angina - myocardial infarction - arrhythmias - heart failure
20 Beta-Blockers à Hypertension Reduce cardiac output Acute treatment with a beta-blocker is not very effective in reducing arterial pressure because of a compensatory increase in systemic vascular resistance. Chronic treatment with beta-blockers lowers arterial pressure possibly because of reduced renin release by the kidneys and effects of beta-blockade on central and peripheral nervous systems.
21 Angina and myocardial infarction B-blockers reduce oxygen demand by diminish heart rate, contractility, and arterial pressure relieve a patient of anginal pain decrease mortality in pts after myocardial infarction (improving the oxygen supply/demand ratio, reducing arrhythmias, and their ability to inhibit subsequent cardiac remodeling)
22 Arrhythmias B-blockers - class II antiarrhythmic drugs inhibit sympathetic influences on cardiac electrical activity sympathetic nerves increase: - sinoatrial node automaticity by increasing the pacemaker currents, which increases sinus rate. - conduction velocity (particularly at the atrioventricular node) - stimulates aberrant pacemaker activity (ectopic foci).
23 Heart failure Although it seems counterintuitive that cardioinhibitory drugs such as beta-blockers would be used in cases of systolic dysfunction, clinical studies have shown quite conclusively that some specific beta-blockers actually reduce mortality and morbidity in symptomatic patients with HFrEF reduce deleterious cardiac remodeling
24
25 Side effects of beta-blockers bradycardia reduced exercise capacity heart failure hypotension atrioventicular nodal conduction block bronchoconstriction (B2) mask the tachycardia that serves as a warning sign for insulin-induced hypoglycemia in diabetic patients
26 Contra-indications: 1. Second- or third-degree AV block (in the absence of a permanent pacemaker). 2. Critical limb ischaemia. 3. Asthma (relative contra-indication): if cardioselective beta-blockers are indicated, asthma is not necessarily an absolute contra-indication *COPD is not a contra-indication
27 Drug interactions to look out for (because of risk of bradycardia/atrioventricular block): Verapamil, diltiazem (should be discontinued).b Digoxin. Amiodarone. Ivabradine.
28
29 Mineralocorticoid receptor antagonists MRAs (spironolactone and eplerenone) block receptors that bind aldosterone and, with different degrees of affinity, other steroid hormone (e.g. corticosteroids, androgens) receptors.
30
31 MRAs Indication: Symptomatic patients (despite treatment with an ACEI and a beta-blocker) with HFrEF and LVEF 35% àreduce mortality and HF hospitalization
32
33 Inclusion criteria - the PARADIGM-HF trial symptomatic HFrEF with LVEF 35% elevated plasma NP levels (BNP 150 pg/ml or NT-proBNP 600 pg/ml) an estimated GFR (egfr) 30 ml/min/1.73 m2 of body surface area
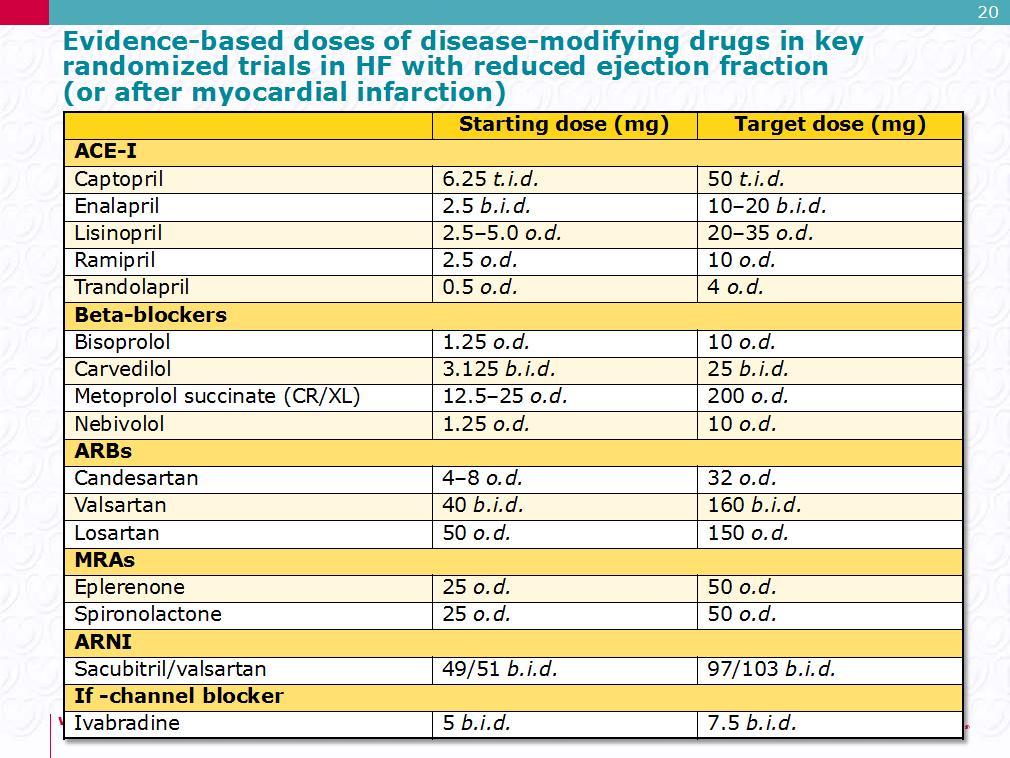
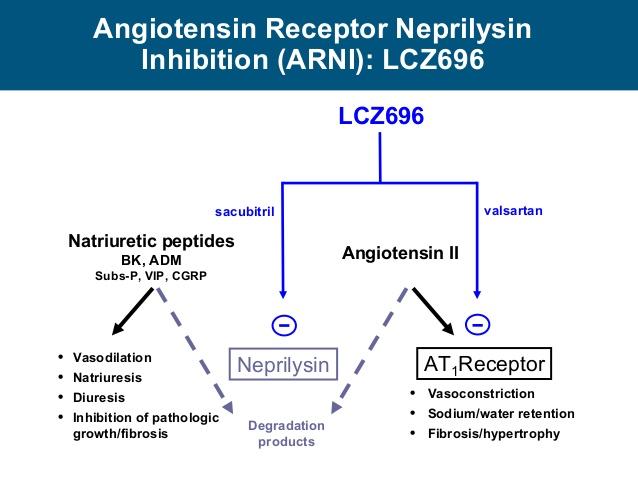
34 Conclusion - the PARADIGM-HF trial sacubitril/valsartan (97/103 mg b.i.d.) was superior to ACEI (enalapril 10mg b.i.d.) in reducing hospitalizations for worsening HF, cardiovascular mortality and overall mortality Side effects of ARNI: Symptomatic hypotension angioedema
35 Drugs for treatment of hypercholesterolaemia Statins Ezetymib PCSK9 inhibitors
36
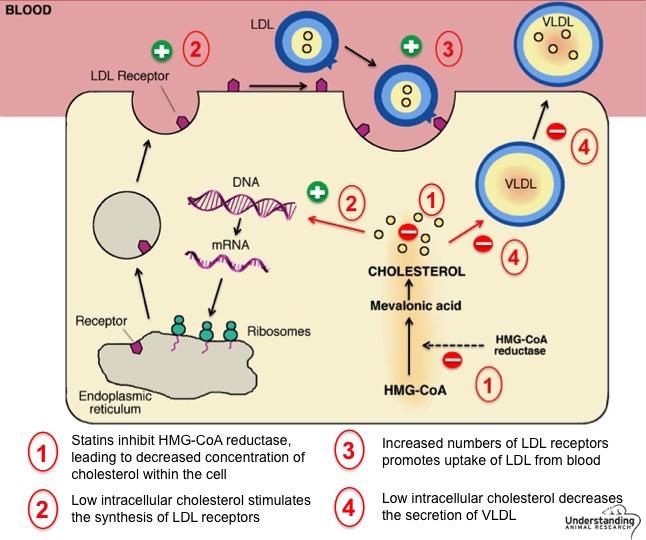
37 Statins -substantially reduce CV morbidity and mortality in both primary and secondary prevention, in both genders and in all age groups -have also been shown to slow the progression or even promote regression of coronary atherosclerosis

38 Recommendations for treatment goals for low-density lipoprotein-cholesterol
39 A80 R20 R30 R
40 Side effects of statins - muscular pain - statin-induced myopathy - rhabdomyolysis à severe muscular pain, muscle necrosis and myoglobinuria potentially leading to renal failure and death - elevation of alanine aminotransferase (ALT) - small increase in the incidence of diabetes

41 Statins + ezetymib (cholesterol absorption inhibitor)

42 PCSK9 inhibitors monoclonal antibodies that reduce LDL-C levels by 60%
43

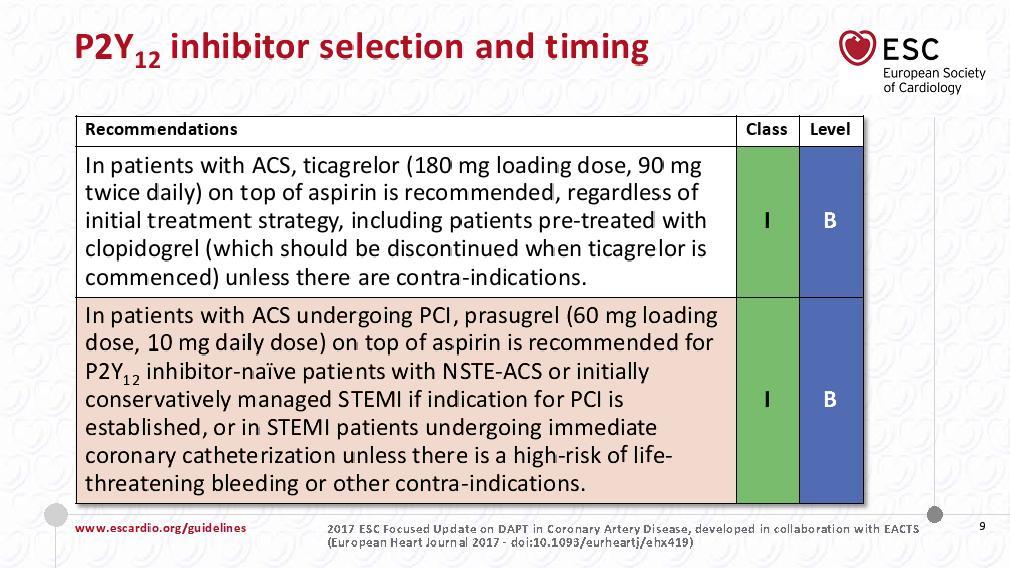
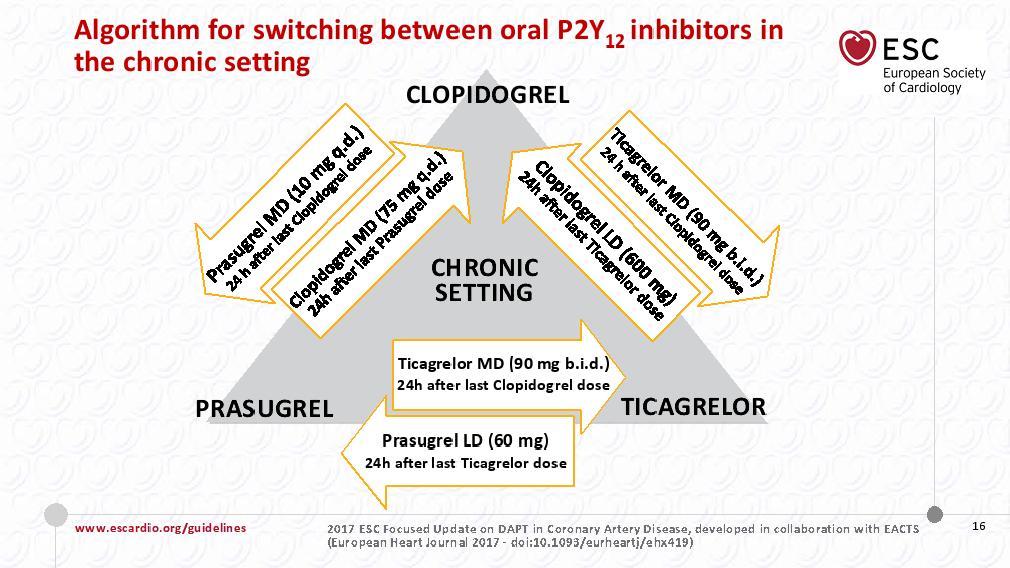
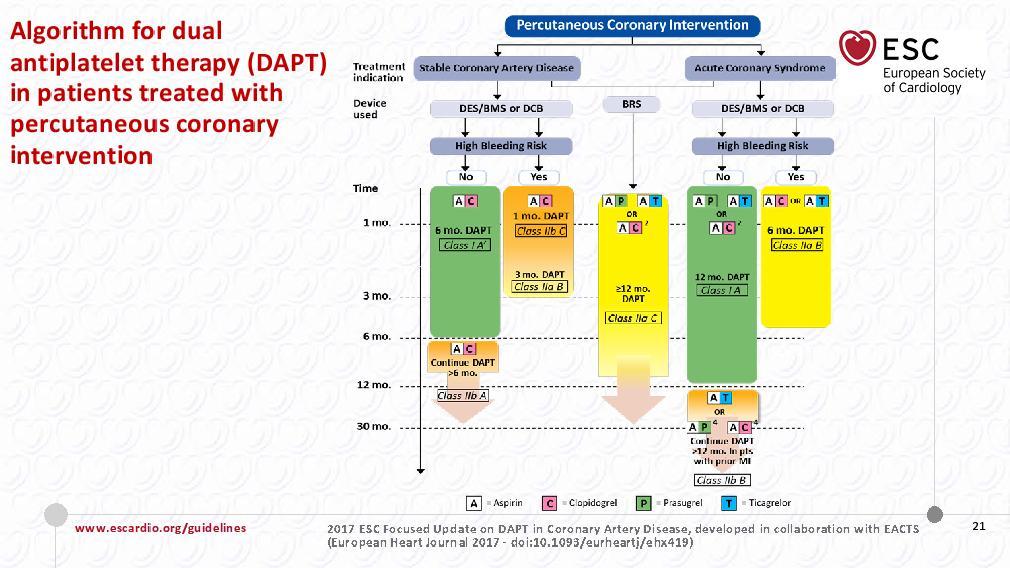
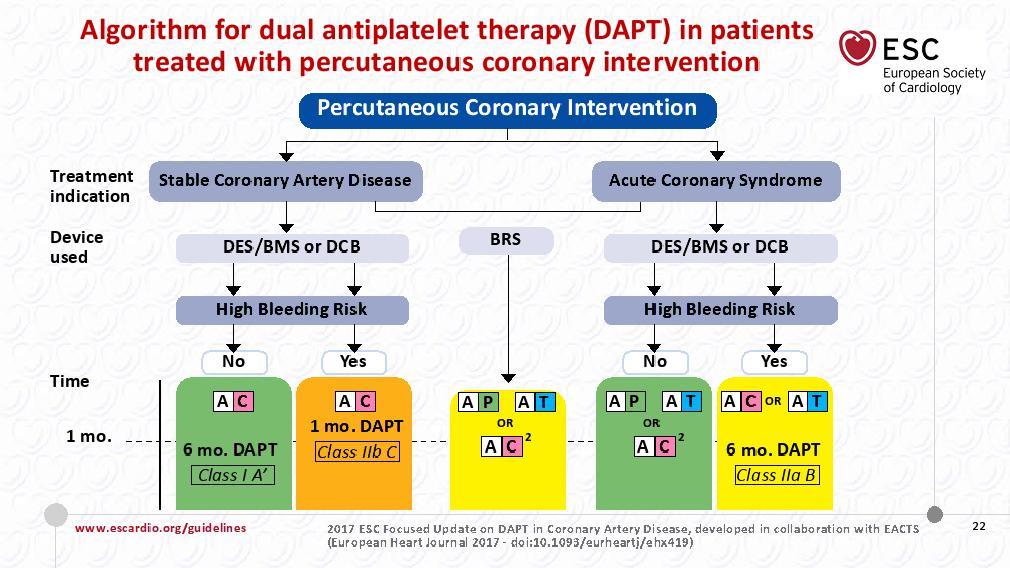
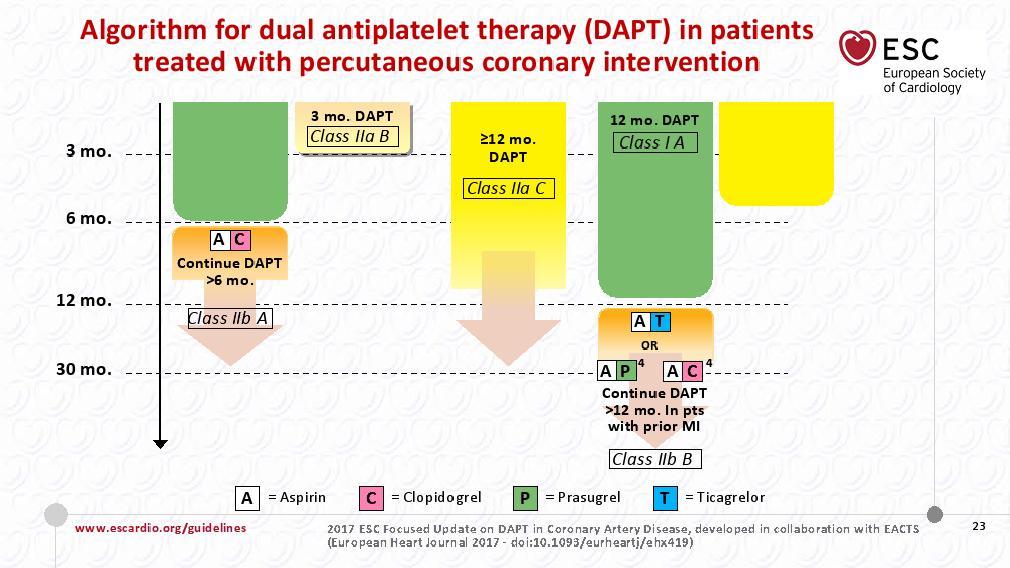
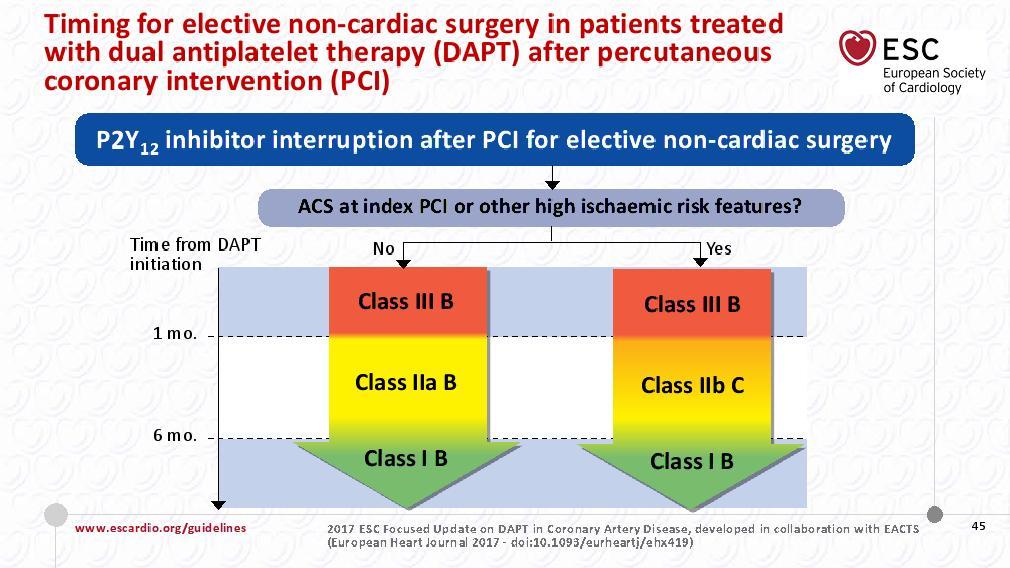
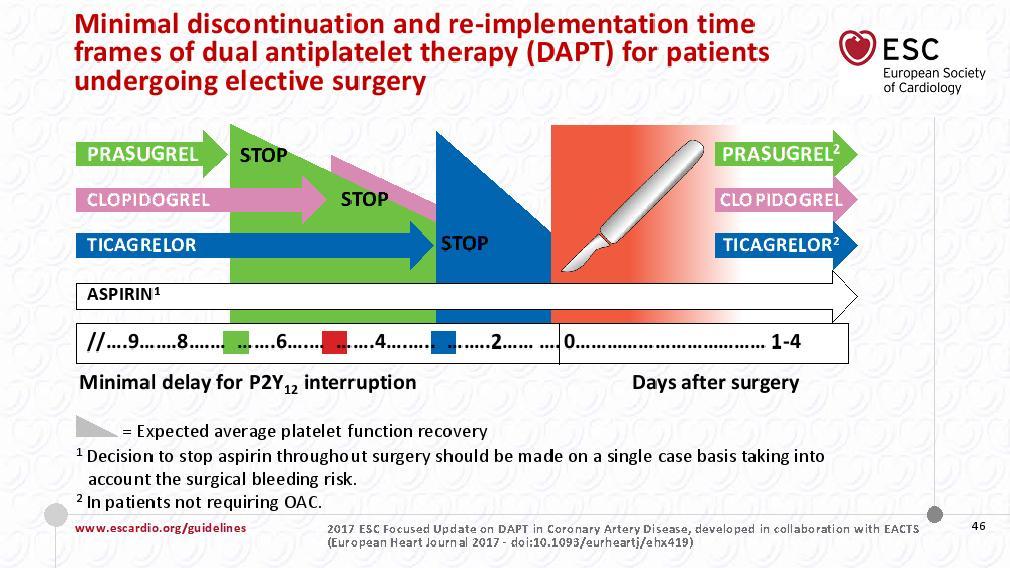
44 DAPT dual antiplatelet therapy Aspirin P2Y12 Inhibitor: clopidogrel prasugrel ticagrelor Indication for DAPT: coronary intervention myocardial infarction
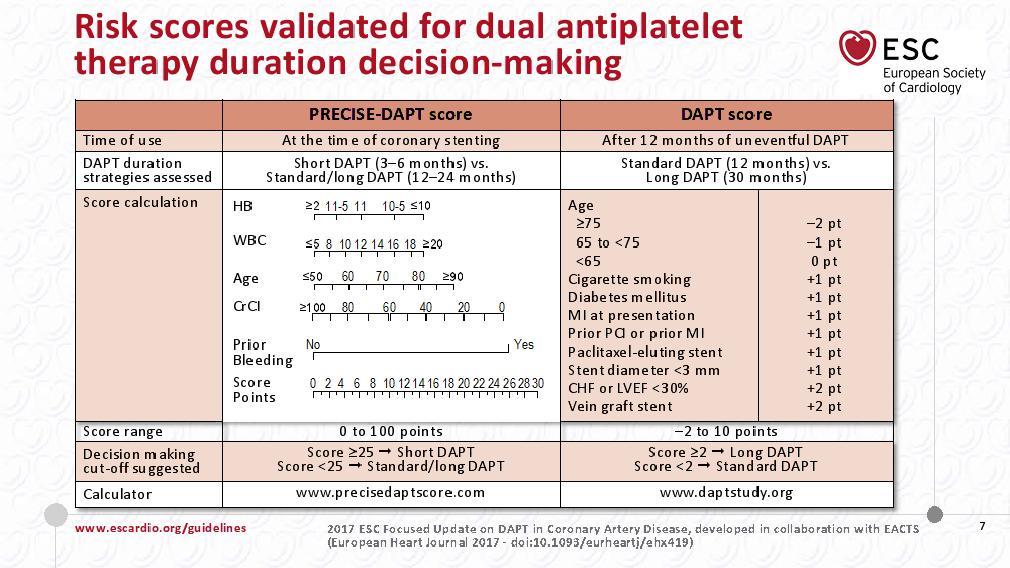
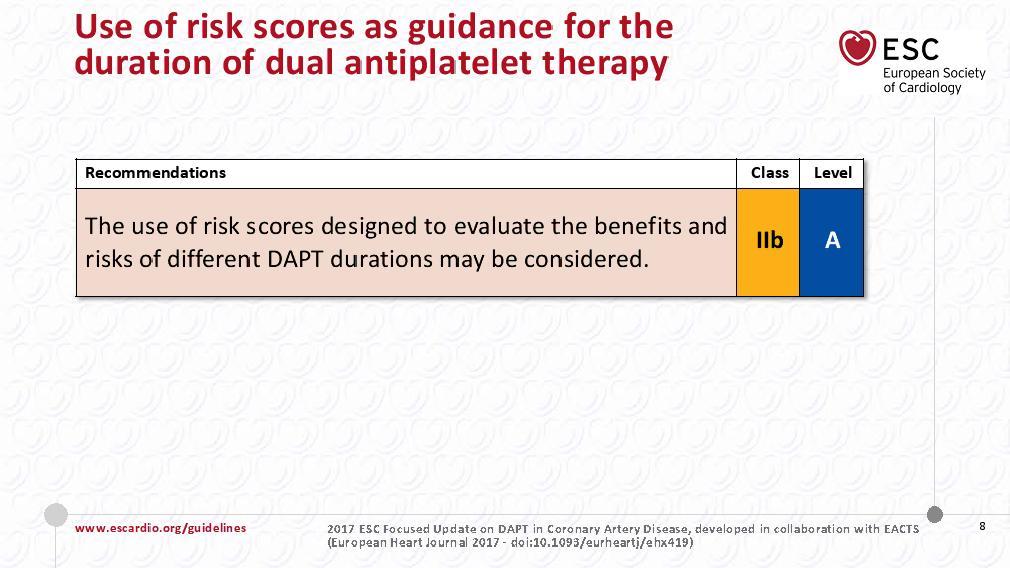
45 DAPT dual antiplatelet therapy Current evidence suggests that DAPT mitigates the risk of stent thrombosis across the whole spectrum, from acute to very late event ischaemic vs. bleeding risks for any given DAPT duration; the use of scores might prove useful to tailor DAPT duration in order to maximize ischaemic protection and minimiz bleeding risks in the individual patient
46
47
48
49
50
51
52
53
54
55
56
57
Heart Failure (HF) Treatment
 Treatment") Heart Failure (HF) Treatment Heart Failure (HF) Complex, progressive disorder. The heart is unable to pump sufficient blood to meet the needs of the body. Its cardinal symptoms are dyspnea, fatigue, and
Heart Failure (HF) Treatment Heart Failure (HF) Complex, progressive disorder. The heart is unable to pump sufficient blood to meet the needs of the body. Its cardinal symptoms are dyspnea, fatigue, and
LXIV: DRUGS: 4. RAS BLOCKADE
 LXIV: DRUGS: 4. RAS BLOCKADE ACE Inhibitors Components of RAS Actions of Angiotensin i II Indications for ACEIs Contraindications RAS blockade in hypertension RAS blockade in CAD RAS blockade in HF Limitations
LXIV: DRUGS: 4. RAS BLOCKADE ACE Inhibitors Components of RAS Actions of Angiotensin i II Indications for ACEIs Contraindications RAS blockade in hypertension RAS blockade in CAD RAS blockade in HF Limitations
Antihypertensive drugs SUMMARY Made by: Lama Shatat
 Antihypertensive drugs SUMMARY Made by: Lama Shatat Diuretic Thiazide diuretics The loop diuretics Potassium-sparing Diuretics *Hydrochlorothiazide *Chlorthalidone *Furosemide *Torsemide *Bumetanide Aldosterone
Antihypertensive drugs SUMMARY Made by: Lama Shatat Diuretic Thiazide diuretics The loop diuretics Potassium-sparing Diuretics *Hydrochlorothiazide *Chlorthalidone *Furosemide *Torsemide *Bumetanide Aldosterone
ARNI (Angiotensin Receptor blocker / Neprilysin Inhibitors [Sacubutril/Valsartan]) Heart Failure Medication Initiation and Titration
![ARNI (Angiotensin Receptor blocker / Neprilysin Inhibitors [Sacubutril/Valsartan]) Heart Failure Medication Initiation and Titration](/thumbs/77/76069192.jpg "ARNI (Angiotensin Receptor blocker / Neprilysin Inhibitors [Sacubutril/Valsartan]) Heart Failure Medication Initiation and Titration") ARNI (Angiotensin Receptor blocker / Neprilysin Inhibitors [Sacubutril/Valsartan]) Heart Failure Medication and Symptomatic HF despite ACEI/ARB and B-blocker therapy Bilateral renal artery stenosis Moderate/Severe
ARNI (Angiotensin Receptor blocker / Neprilysin Inhibitors [Sacubutril/Valsartan]) Heart Failure Medication and Symptomatic HF despite ACEI/ARB and B-blocker therapy Bilateral renal artery stenosis Moderate/Severe
M2 TEACHING UNDERSTANDING PHARMACOLOGY
 M2 TEACHING UNDERSTANDING PHARMACOLOGY USING CVS SYSTEM AS AN EXAMPLE NIGEL FONG 2 JAN 2014 TODAY S OBJECTIVE Pharmacology often seems like an endless list of mechanisms and side effects to memorize. To
M2 TEACHING UNDERSTANDING PHARMACOLOGY USING CVS SYSTEM AS AN EXAMPLE NIGEL FONG 2 JAN 2014 TODAY S OBJECTIVE Pharmacology often seems like an endless list of mechanisms and side effects to memorize. To
Beyond ACE-inhibitors for Heart Failure. Jacob Townsend, MD NCVH Birmingham 2015
 Beyond ACE-inhibitors for Heart Failure Jacob Townsend, MD NCVH Birmingham 2015 % Decrease in Mortality Current Therapy HFrEF 0% Angiotensin receptor blocker ACE inhibitor Beta blocker Mineralocorticoid
Beyond ACE-inhibitors for Heart Failure Jacob Townsend, MD NCVH Birmingham 2015 % Decrease in Mortality Current Therapy HFrEF 0% Angiotensin receptor blocker ACE inhibitor Beta blocker Mineralocorticoid
Byvalson. (nebivolol, valsartan) New Product Slideshow
 New Product Slideshow") Byvalson (nebivolol, valsartan) New Product Slideshow Introduction Brand name: Byvalson Generic name: Nebivolol, valsartan Pharmacological class: Beta-blocker + angiotensin II receptor blocker (ARB) Strength
Byvalson (nebivolol, valsartan) New Product Slideshow Introduction Brand name: Byvalson Generic name: Nebivolol, valsartan Pharmacological class: Beta-blocker + angiotensin II receptor blocker (ARB) Strength
Heart Failure: Current Management Strategies
 Heart Failure: Current Management Strategies CSHP Fall Education Session- September 30th, 2017 Carolyn MacKinnon & Tamara Matchett BscPharm, ACPR Candidates Objectives 1. Describe the pathophysiology &
Heart Failure: Current Management Strategies CSHP Fall Education Session- September 30th, 2017 Carolyn MacKinnon & Tamara Matchett BscPharm, ACPR Candidates Objectives 1. Describe the pathophysiology &
What s New in Heart Failure? Marie-France Gauthier, BSc, PharmD, ACPR Clinical Pharmacist at Montfort Hospital
 What s New in Heart Failure? Marie-France Gauthier, BSc, PharmD, ACPR Clinical Pharmacist at Montfort Hospital Disclosures I have no current or past relationships with commercial entities Learning objectives
What s New in Heart Failure? Marie-France Gauthier, BSc, PharmD, ACPR Clinical Pharmacist at Montfort Hospital Disclosures I have no current or past relationships with commercial entities Learning objectives
RAAS blocker + B Blocker Troubleshooting
 RAAS blocker + B Blocker Troubleshooting Heart Failure ECHO Clinic Virtual Heart Failure Consultation and Education Prof Ken McDonald & Dr. Patricia Campbell 13 th March 2017 HF activates 3 neurohormonal
RAAS blocker + B Blocker Troubleshooting Heart Failure ECHO Clinic Virtual Heart Failure Consultation and Education Prof Ken McDonald & Dr. Patricia Campbell 13 th March 2017 HF activates 3 neurohormonal
Cardiac Drugs: Chapter 9 Worksheet Cardiac Agents. 1. drugs affect the rate of the heart and can either increase its rate or decrease its rate.
 Complete the following. 1. drugs affect the rate of the heart and can either increase its rate or decrease its rate. 2. drugs affect the force of contraction and can be either positive or negative. 3.
Complete the following. 1. drugs affect the rate of the heart and can either increase its rate or decrease its rate. 2. drugs affect the force of contraction and can be either positive or negative. 3.
Neprilysin Inhibitor (Entresto ) Prior Authorization and Quantity Limit Program Summary
 Prior Authorization and Quantity Limit Program Summary") Neprilysin Inhibitor (Entresto ) Prior Authorization and Quantity Limit Program Summary FDA APPROVED INDICATIONS DOSAGE 1 Indication Entresto Reduce the risk of cardiovascular (sacubitril/valsartan) death
Neprilysin Inhibitor (Entresto ) Prior Authorization and Quantity Limit Program Summary FDA APPROVED INDICATIONS DOSAGE 1 Indication Entresto Reduce the risk of cardiovascular (sacubitril/valsartan) death
Heart Failure Clinician Guide JANUARY 2018
 Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Heart Failure Clinician Guide JANUARY 2018 Introduction This evidence-based guideline summary is based on the 2018 National Heart Failure Guideline.
Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Heart Failure Clinician Guide JANUARY 2018 Introduction This evidence-based guideline summary is based on the 2018 National Heart Failure Guideline.
Heart Failure. Subjective SOB (shortness of breath) Peripheral edema. Orthopnea (2-3 pillows) PND (paroxysmal nocturnal dyspnea)
 Peripheral edema. Orthopnea (2-3 pillows) PND (paroxysmal nocturnal dyspnea)") Pharmacology I. Definitions A. Heart Failure (HF) Heart Failure Ezra Levy, Pharm.D. HF Results when one or both ventricles are unable to pump sufficient blood to meet the body s needs There are 2 types
Pharmacology I. Definitions A. Heart Failure (HF) Heart Failure Ezra Levy, Pharm.D. HF Results when one or both ventricles are unable to pump sufficient blood to meet the body s needs There are 2 types
HYPERTENSION: Sustained elevation of arterial blood pressure above normal o Systolic 140 mm Hg and/or o Diastolic 90 mm Hg
 Lecture 39 Anti-Hypertensives B-Rod BLOOD PRESSURE: Systolic / Diastolic NORMAL: 120/80 Systolic = measure of pressure as heart is beating Diastolic = measure of pressure while heart is at rest between
Lecture 39 Anti-Hypertensives B-Rod BLOOD PRESSURE: Systolic / Diastolic NORMAL: 120/80 Systolic = measure of pressure as heart is beating Diastolic = measure of pressure while heart is at rest between
Estimated 5.7 million Americans with HF. 915, 000 new HF cases annually, HF incidence approaches
 Heart Failure: Management of a Chronic Disease Jenny Bauerly RN, CHFN, APRN-BC Heart Failure (HF) Definition A complex clinical syndrome that can result from any structural or functional cardiac disorder
Heart Failure: Management of a Chronic Disease Jenny Bauerly RN, CHFN, APRN-BC Heart Failure (HF) Definition A complex clinical syndrome that can result from any structural or functional cardiac disorder
Disclosures. Advances in Chronic Heart Failure Management 6/12/2017. Van N Selby, MD UCSF Advanced Heart Failure Program June 19, 2017
 Advances in Chronic Heart Failure Management Van N Selby, MD UCSF Advanced Heart Failure Program June 19, 2017 I have nothing to disclose Disclosures 1 Goal statement To review recently-approved therapies
Advances in Chronic Heart Failure Management Van N Selby, MD UCSF Advanced Heart Failure Program June 19, 2017 I have nothing to disclose Disclosures 1 Goal statement To review recently-approved therapies
Disclosure Statement. Heart Failure: Refreshers and Updates. Objectives. CHF: Chronic Heart Failure. Definitions. Definitions 2/19/2018
 Disclosure Statement Heart Failure: Refreshers and Updates Tracy K. Pettinger, PharmD Clinical Associate Professor College of Pharmacy The planners and presenter of this presentation have disclosed no
Disclosure Statement Heart Failure: Refreshers and Updates Tracy K. Pettinger, PharmD Clinical Associate Professor College of Pharmacy The planners and presenter of this presentation have disclosed no
New Winners in the World of Heart Failure. Laura Steffens PharmD Candidate 2016 CICU Presentation August 12, 2015
 New Winners in the World of Heart Failure Laura Steffens PharmD Candidate 2016 CICU Presentation August 12, 2015 Jessup 2014 Shaking Things Up 2003: FDA approved eplerenone for the treatment of heart failure
New Winners in the World of Heart Failure Laura Steffens PharmD Candidate 2016 CICU Presentation August 12, 2015 Jessup 2014 Shaking Things Up 2003: FDA approved eplerenone for the treatment of heart failure
Management of chronic heart failure: pharmacology. Giuseppe M.C. Rosano, MD, PhD, FHFA
 Management of chronic heart failure: pharmacology. Giuseppe M.C. Rosano, MD, PhD, FHFA Declaration of potential conflict of interests Type of job or financial support Salary Ordinary funds Position in
Management of chronic heart failure: pharmacology. Giuseppe M.C. Rosano, MD, PhD, FHFA Declaration of potential conflict of interests Type of job or financial support Salary Ordinary funds Position in
Heart Failure Clinician Guide JANUARY 2016
 Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Heart Failure Clinician Guide JANUARY 2016 Introduction This evidence-based guideline summary is based on the 2016 National Heart Failure Guideline.
Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Heart Failure Clinician Guide JANUARY 2016 Introduction This evidence-based guideline summary is based on the 2016 National Heart Failure Guideline.
Heart Failure New Drugs- Updated Guidelines
 Heart Failure New Drugs- Updated Guidelines Eileen Handberg, PhD, ANP-BC, FAHA, FACC Professor of Medicine Division of Cardiovascular Medicine University of Florida Disclosures 1. 3 2. 6 3. 8 4. 11 Dunlay
Heart Failure New Drugs- Updated Guidelines Eileen Handberg, PhD, ANP-BC, FAHA, FACC Professor of Medicine Division of Cardiovascular Medicine University of Florida Disclosures 1. 3 2. 6 3. 8 4. 11 Dunlay
Sacubitril/valsartan: A New Management Strategy for the Treatment of Heart Failure. Elizabeth Pogge, PharmD, MPH, BCPS, FASCP
 Sacubitril/valsartan: A New Management Strategy for the Treatment of Heart Failure Elizabeth Pogge, PharmD, MPH, BCPS, FASCP Disclosure Elizabeth Pogge reports no actual or potential conflicts of interest
Sacubitril/valsartan: A New Management Strategy for the Treatment of Heart Failure Elizabeth Pogge, PharmD, MPH, BCPS, FASCP Disclosure Elizabeth Pogge reports no actual or potential conflicts of interest
SGK 2016 Session: Postgraduate Course in Heart Failure Lausanne, 15. June 2016 Heart Failure Guidelines 2016
 SGK 2016 Session: Postgraduate Course in Heart Failure Lausanne, 15. June 2016 Heart Failure Guidelines 2016 Matthias Nägele, MD University Hospital Zurich Disclosures I have nothing to disclose. The new
SGK 2016 Session: Postgraduate Course in Heart Failure Lausanne, 15. June 2016 Heart Failure Guidelines 2016 Matthias Nägele, MD University Hospital Zurich Disclosures I have nothing to disclose. The new
Practical considerations for the use of ARNI in CHF: clinical cases. J. Parissis, Heart Failure Clinic, University of Athens, Athens, Greece
 Practical considerations for the use of ARNI in CHF: clinical cases J. Parissis, Heart Failure Clinic, University of Athens, Athens, Greece Disclosures: Research grants and honoraria for lectures from
Practical considerations for the use of ARNI in CHF: clinical cases J. Parissis, Heart Failure Clinic, University of Athens, Athens, Greece Disclosures: Research grants and honoraria for lectures from
Controversies in Cardiac Pharmacology
 Controversies in Cardiac Pharmacology Thomas D. Conley, MD FACC FSCAI Disclosures I have no relevant relationships with commercial interests to disclose. 1 Doc, do I really need to take all these medicines?
Controversies in Cardiac Pharmacology Thomas D. Conley, MD FACC FSCAI Disclosures I have no relevant relationships with commercial interests to disclose. 1 Doc, do I really need to take all these medicines?
Congestive Heart Failure: Outpatient Management
 The Chattanooga Heart Institute Cardiovascular Symposium Congestive Heart Failure: Outpatient Management E. Philip Lehman MD, MPP Disclosure No financial disclosures. Objectives Evidence-based therapy
The Chattanooga Heart Institute Cardiovascular Symposium Congestive Heart Failure: Outpatient Management E. Philip Lehman MD, MPP Disclosure No financial disclosures. Objectives Evidence-based therapy
Disclosures. Overview. Goal statement. Advances in Chronic Heart Failure Management 5/22/17
 Disclosures Advances in Chronic Heart Failure Management I have nothing to disclose Van N Selby, MD UCSF Advanced Heart Failure Program May 22, 2017 Goal statement To review recently-approved therapies
Disclosures Advances in Chronic Heart Failure Management I have nothing to disclose Van N Selby, MD UCSF Advanced Heart Failure Program May 22, 2017 Goal statement To review recently-approved therapies
Initiating New Medications in the Management of Heart Failure
 Initiating New Medications in the Management of Heart Failure Sandra Oliver-McNeil DNP, MSN, ACNP-BC, CHFN Associate Professor (Clinical) Wayne State University College of Nursing Objectives The participant
Initiating New Medications in the Management of Heart Failure Sandra Oliver-McNeil DNP, MSN, ACNP-BC, CHFN Associate Professor (Clinical) Wayne State University College of Nursing Objectives The participant
By Prof. Khaled El-Rabat
 What is The Optimum? By Prof. Khaled El-Rabat Professor of Cardiology - Benha Faculty of Medicine HT. Introduction Despite major worldwide efforts over recent decades directed at diagnosing and treating
What is The Optimum? By Prof. Khaled El-Rabat Professor of Cardiology - Benha Faculty of Medicine HT. Introduction Despite major worldwide efforts over recent decades directed at diagnosing and treating
Heart Failure Pharmacotherapy An Update
 Heart Failure Pharmacotherapy An Update Kenneth Mishler, PharmD, MBA Objectives Review the epidemiology of heart failure (HF) Review evidence based guidelines for the use of mediations used to treat HF
Heart Failure Pharmacotherapy An Update Kenneth Mishler, PharmD, MBA Objectives Review the epidemiology of heart failure (HF) Review evidence based guidelines for the use of mediations used to treat HF
Disclosures. This speaker has indicated there are no relevant financial relationships to be disclosed.
 Disclosures This speaker has indicated there are no relevant financial relationships to be disclosed. And the Beat Goes On: New Medications for Heart Failure Alison M. Walton, PharmD, BCPS The Case of
Disclosures This speaker has indicated there are no relevant financial relationships to be disclosed. And the Beat Goes On: New Medications for Heart Failure Alison M. Walton, PharmD, BCPS The Case of
Patient details GP details Specialist details Name GP Name Dr Specialist Name Dr R. Horton
 Rationale for Initiation, Continuation and Discontinuation (RICaD) Sacubitril/Valsartan (Entresto) For the treatment of symptomatic heart failure with reduced ejection fraction (NICE TA388) This document
Rationale for Initiation, Continuation and Discontinuation (RICaD) Sacubitril/Valsartan (Entresto) For the treatment of symptomatic heart failure with reduced ejection fraction (NICE TA388) This document
Summary/Key Points Introduction
 Summary/Key Points Introduction Scope of Heart Failure (HF) o 6.5 million Americans 20 years of age have HF o 960,000 new cases of HF diagnosed annually o 5-year survival rate for HF is ~50% Classification
Summary/Key Points Introduction Scope of Heart Failure (HF) o 6.5 million Americans 20 years of age have HF o 960,000 new cases of HF diagnosed annually o 5-year survival rate for HF is ~50% Classification
Drugs acting on the reninangiotensin-aldosterone
 Drugs acting on the reninangiotensin-aldosterone system John McMurray Eugene Braunwald Scholar in Cardiovascular Diseases, Brigham and Women s Hospital, Boston & Visiting Professor, Harvard Medical School
Drugs acting on the reninangiotensin-aldosterone system John McMurray Eugene Braunwald Scholar in Cardiovascular Diseases, Brigham and Women s Hospital, Boston & Visiting Professor, Harvard Medical School
Towards a Greater Understanding of Cardiac Medications Foundational Cardiac Concepts That Must Be Understood:
 Towards a Greater Understanding of Cardiac Medications Foundational Cardiac Concepts That Must Be Understood: Cardiac Output (CO) CO=SVxHR (stroke volume x heart rate) Cardiac output: The amount of blood
Towards a Greater Understanding of Cardiac Medications Foundational Cardiac Concepts That Must Be Understood: Cardiac Output (CO) CO=SVxHR (stroke volume x heart rate) Cardiac output: The amount of blood
Updates in Congestive Heart Failure
 Updates in Congestive Heart Failure GREGORY YOST, DO JOHNSTOWN CARDIOVASCULAR ASSOCIATES 1/28/2018 Disclosures Edwards speaker on Sapien3 valves (TAVR) Stages A-D and NYHA Classes I-IV Stage A: High risk
Updates in Congestive Heart Failure GREGORY YOST, DO JOHNSTOWN CARDIOVASCULAR ASSOCIATES 1/28/2018 Disclosures Edwards speaker on Sapien3 valves (TAVR) Stages A-D and NYHA Classes I-IV Stage A: High risk
Aldosterone Antagonism in Heart Failure: Now for all Patients?
 Aldosterone Antagonism in Heart Failure: Now for all Patients? Inder Anand, MD, FRCP, D Phil (Oxon.) Professor of Medicine, University of Minnesota, Director Heart Failure Program, VA Medical Center 111C
Aldosterone Antagonism in Heart Failure: Now for all Patients? Inder Anand, MD, FRCP, D Phil (Oxon.) Professor of Medicine, University of Minnesota, Director Heart Failure Program, VA Medical Center 111C
Hypertension. Penny Mosley MRPharmS
 Hypertension Penny Mosley MRPharmS Outline of presentation Introduction to hypertension Physiological control of arterial blood pressure What determines our bp? What determines the heart rate? What determines
Hypertension Penny Mosley MRPharmS Outline of presentation Introduction to hypertension Physiological control of arterial blood pressure What determines our bp? What determines the heart rate? What determines
Drugs Used in Heart Failure. Assistant Prof. Dr. Najlaa Saadi PhD pharmacology Faculty of Pharmacy University of Philadelphia
 Drugs Used in Heart Failure Assistant Prof. Dr. Najlaa Saadi PhD pharmacology Faculty of Pharmacy University of Philadelphia Heart Failure Heart failure (HF), occurs when cardiac output is inadequate to
Drugs Used in Heart Failure Assistant Prof. Dr. Najlaa Saadi PhD pharmacology Faculty of Pharmacy University of Philadelphia Heart Failure Heart failure (HF), occurs when cardiac output is inadequate to
2017 Summer MAOFP Update
 2017 Summer MAOFP Update. Cardiology Update 2017 Landmark Trials Change Practice Guidelines David J. Strobl, DO, FNLA Heart Failure: Epidemiology More than 4 million patients affected 400,000 new cases
2017 Summer MAOFP Update. Cardiology Update 2017 Landmark Trials Change Practice Guidelines David J. Strobl, DO, FNLA Heart Failure: Epidemiology More than 4 million patients affected 400,000 new cases
Management of Hypertension
 Clinical Practice Guidelines Management of Hypertension Definition and classification of blood pressure levels (mmhg) Category Systolic Diastolic Normal
Clinical Practice Guidelines Management of Hypertension Definition and classification of blood pressure levels (mmhg) Category Systolic Diastolic Normal
Treating HF Patients with ARNI s Why, When and How?
 Treating HF Patients with ARNI s Why, When and How? 19 th Annual San Diego Heart Failure Symposium for Primary Care Physicians January 11-12, 2019 La Jolla, CA Barry Greenberg M.D. Distinguished Professor
Treating HF Patients with ARNI s Why, When and How? 19 th Annual San Diego Heart Failure Symposium for Primary Care Physicians January 11-12, 2019 La Jolla, CA Barry Greenberg M.D. Distinguished Professor
DRUG CLASSES BETA-ADRENOCEPTOR ANTAGONISTS (BETA-BLOCKERS)
") DRUG CLASSES BETA-ADRENOCEPTOR ANTAGONISTS (BETA-BLOCKERS) Beta-blockers have been widely used in the management of angina, certain tachyarrhythmias and heart failure, as well as in hypertension. Examples
DRUG CLASSES BETA-ADRENOCEPTOR ANTAGONISTS (BETA-BLOCKERS) Beta-blockers have been widely used in the management of angina, certain tachyarrhythmias and heart failure, as well as in hypertension. Examples
Heart Failure. Dr. William Vosik. January, 2012
 Heart Failure Dr. William Vosik January, 2012 Questions for clinicians to ask Is this heart failure? What is the underlying cause? What are the associated disease processes? Which evidence-based treatment
Heart Failure Dr. William Vosik January, 2012 Questions for clinicians to ask Is this heart failure? What is the underlying cause? What are the associated disease processes? Which evidence-based treatment
Outline. Classification by LVEF Conventional Therapy New Therapies. Ivabradine Sacubitril/valsartan
 New Pharmacological Therapies for Heart Failure Mark Drazner, MD, MSc Clinical Chief of Cardiology Medical Director, CHF/VAD/Transplant James M. Wooten Chair in Cardiology UT Southwestern Medical Center
New Pharmacological Therapies for Heart Failure Mark Drazner, MD, MSc Clinical Chief of Cardiology Medical Director, CHF/VAD/Transplant James M. Wooten Chair in Cardiology UT Southwestern Medical Center
Akash Ghai MD, FACC February 27, No Disclosures
 Akash Ghai MD, FACC February 27, 2015 No Disclosures Epidemiology Lifetime risk is > 20% for American s older than 40 years old. > 650,000 new cases diagnosed each year. Incidence increases with age: 2%
Akash Ghai MD, FACC February 27, 2015 No Disclosures Epidemiology Lifetime risk is > 20% for American s older than 40 years old. > 650,000 new cases diagnosed each year. Incidence increases with age: 2%
1/4/18. Heart Failure Guideline Review and Update. Disclosure. Pharmacist Objectives. Pharmacy Technician Objectives. What is Heart Failure?
 Disclosure Heart Failure Guideline Review and Update I have had no financial relationship over the past 12 months with any commercial sponsor with a vested interest in this presentation. Natalie Beiter,
Disclosure Heart Failure Guideline Review and Update I have had no financial relationship over the past 12 months with any commercial sponsor with a vested interest in this presentation. Natalie Beiter,
The Failing Heart in Primary Care
 The Failing Heart in Primary Care Hamid Ikram How fares the Heart Failure Epidemic? 4357 patients, 57% women, mean age 74 years HFSA 2010 Practice Guideline (3.1) Heart Failure Prevention A careful and
The Failing Heart in Primary Care Hamid Ikram How fares the Heart Failure Epidemic? 4357 patients, 57% women, mean age 74 years HFSA 2010 Practice Guideline (3.1) Heart Failure Prevention A careful and
Antihypertensive Agents Part-2. Assistant Prof. Dr. Najlaa Saadi PhD Pharmacology Faculty of Pharmacy University of Philadelphia
 Antihypertensive Agents Part-2 Assistant Prof. Dr. Najlaa Saadi PhD Pharmacology Faculty of Pharmacy University of Philadelphia Agents that block production or action of angiotensin Angiotensin-converting
Antihypertensive Agents Part-2 Assistant Prof. Dr. Najlaa Saadi PhD Pharmacology Faculty of Pharmacy University of Philadelphia Agents that block production or action of angiotensin Angiotensin-converting
Heart Failure. Dr. Alia Shatanawi
 Heart Failure Dr. Alia Shatanawi Left systolic dysfunction secondary to coronary artery disease is the most common cause, account to 70% of all cases. Heart Failure Heart is unable to pump sufficient blood
Heart Failure Dr. Alia Shatanawi Left systolic dysfunction secondary to coronary artery disease is the most common cause, account to 70% of all cases. Heart Failure Heart is unable to pump sufficient blood
Beta-blockers in Patients with Mid-range Left Ventricular Ejection Fraction after AMI Improved Clinical Outcomes
 Beta-blockers in Patients with Mid-range Left Ventricular Ejection Fraction after AMI Improved Clinical Outcomes Seung-Jae Joo and other KAMIR-NIH investigators Department of Cardiology, Jeju National
Beta-blockers in Patients with Mid-range Left Ventricular Ejection Fraction after AMI Improved Clinical Outcomes Seung-Jae Joo and other KAMIR-NIH investigators Department of Cardiology, Jeju National
Medical Management of Acute Coronary Syndrome: The roles of a noncardiologist. Norbert Lingling D. Uy, MD Professor of Medicine UERMMMCI
 Medical Management of Acute Coronary Syndrome: The roles of a noncardiologist physician Norbert Lingling D. Uy, MD Professor of Medicine UERMMMCI Outcome objectives of the discussion: At the end of the
Medical Management of Acute Coronary Syndrome: The roles of a noncardiologist physician Norbert Lingling D. Uy, MD Professor of Medicine UERMMMCI Outcome objectives of the discussion: At the end of the
Chapter (9) Calcium Antagonists
 Calcium Antagonists") Chapter (9) Calcium Antagonists (CALCIUM CHANNEL BLOCKERS) Classification Mechanism of Anti-ischemic Actions Indications Drug Interaction with Verapamil Contraindications Adverse Effects Treatment of Drug
Chapter (9) Calcium Antagonists (CALCIUM CHANNEL BLOCKERS) Classification Mechanism of Anti-ischemic Actions Indications Drug Interaction with Verapamil Contraindications Adverse Effects Treatment of Drug
7/7/ CHD/MI LVH and LV dysfunction Dysrrhythmias Stroke PVD Renal insufficiency and failure Retinopathy. Normal <120 Prehypertension
 Prevalence of Hypertension Hypertension: Diagnosis and Management T. Villela, M.D. Program Director University of California, San Francisco-San Francisco General Hospital Family and Community Medicine
Prevalence of Hypertension Hypertension: Diagnosis and Management T. Villela, M.D. Program Director University of California, San Francisco-San Francisco General Hospital Family and Community Medicine
HEART FAILURE: PHARMACOTHERAPY UPDATE
 HEART FAILURE: PHARMACOTHERAPY UPDATE 3 HEART FAILURE REVIEW 1 5.1 million x1.25 = 6.375 million 40 years old = MICHAEL F. AKERS, PHARM.D. CLINICAL PHARMACIST CENTRACARE HEALTH, ST. CLOUD HOSPITAL HF Diagnosis
HEART FAILURE: PHARMACOTHERAPY UPDATE 3 HEART FAILURE REVIEW 1 5.1 million x1.25 = 6.375 million 40 years old = MICHAEL F. AKERS, PHARM.D. CLINICAL PHARMACIST CENTRACARE HEALTH, ST. CLOUD HOSPITAL HF Diagnosis
Angina pectoris due to coronary atherosclerosis : Atenolol is indicated for the long term management of patients with angina pectoris.
 Lonet Tablet Description Lonet contains Atenolol, a synthetic β1 selective (cardioselective) adrenoreceptor blocking agent without membrane stabilising or intrinsic sympathomimetic (partial agonist) activity.
Lonet Tablet Description Lonet contains Atenolol, a synthetic β1 selective (cardioselective) adrenoreceptor blocking agent without membrane stabilising or intrinsic sympathomimetic (partial agonist) activity.
Heart Failure CTSHP Fall Seminar
 Heart Failure CTSHP Fall Seminar Laurajo Ryan, PharmD, MSc, BCPS, CDE Pharmacist Learning Objectives Outline the pathophysiology of heart failure List triggers for decompensated heart failure Describe
Heart Failure CTSHP Fall Seminar Laurajo Ryan, PharmD, MSc, BCPS, CDE Pharmacist Learning Objectives Outline the pathophysiology of heart failure List triggers for decompensated heart failure Describe
8:30-10:30 WS #4: Cardiology :00-13:00 WS #11: Cardiology 101 (Repeated)
") Professor Ralph Stewart Cardiologist Auckland City Hospital Green Lane Cardiovascular Research Unit Auckland Heart Group Fiona Stewart Cardiologist Green Lane Hospital National Women's Hospital Professor
Professor Ralph Stewart Cardiologist Auckland City Hospital Green Lane Cardiovascular Research Unit Auckland Heart Group Fiona Stewart Cardiologist Green Lane Hospital National Women's Hospital Professor
Cardiovascular Health Practice Guideline Outpatient Management of Coronary Artery Disease 2003
 Authorized By: Medical Management Guideline Committee Approval Date: 12/13/01 Revision Date: 12/11/03 Beta-Blockers Nitrates Calcium Channel Blockers MEDICATIONS Indicated in post-mi, unstable angina,
Authorized By: Medical Management Guideline Committee Approval Date: 12/13/01 Revision Date: 12/11/03 Beta-Blockers Nitrates Calcium Channel Blockers MEDICATIONS Indicated in post-mi, unstable angina,
Hypertension diagnosis (see detail document) Diabetic. Target less than 130/80mmHg
 Diabetic. Target less than 130/80mmHg") Hypertension diagnosis (see detail document) Non-diabetic Diabetic Very elderly (older than 80 years) Target less than 140/90mmHg Target less than 130/80mmHg Consider SBP target less than 150mmHg Non-diabetic
Hypertension diagnosis (see detail document) Non-diabetic Diabetic Very elderly (older than 80 years) Target less than 140/90mmHg Target less than 130/80mmHg Consider SBP target less than 150mmHg Non-diabetic
Hypertension (JNC-8)
") Hypertension (JNC-8) Southern California University of Health Sciences Physician Assistant Program Management and Treatment of Hypertension April 17, 2018, presented by Ezra Levy, Pharm.D.! The 8 th Joint
Hypertension (JNC-8) Southern California University of Health Sciences Physician Assistant Program Management and Treatment of Hypertension April 17, 2018, presented by Ezra Levy, Pharm.D.! The 8 th Joint
sympatholytics sympatholytics sympatholytics
 sympatholytics sympatholytics sympatholytics CNS-ACTING SYMPATHOPLEGICS Sympathetic brain signals Doesn t affect baroreceptor reflex (no orthostatic hypotension) Methyldopa α-methylne crosses BBB (+) α-adrenoreceptors
sympatholytics sympatholytics sympatholytics CNS-ACTING SYMPATHOPLEGICS Sympathetic brain signals Doesn t affect baroreceptor reflex (no orthostatic hypotension) Methyldopa α-methylne crosses BBB (+) α-adrenoreceptors
Heart failure. Failure? blood supply insufficient for body needs. CHF = congestive heart failure. increased blood volume, interstitial fluid
 Failure? blood supply insufficient for body needs CHF = congestive heart failure increased blood volume, interstitial fluid Underlying causes/risk factors Ischemic heart disease (CAD) 70% hypertension
Failure? blood supply insufficient for body needs CHF = congestive heart failure increased blood volume, interstitial fluid Underlying causes/risk factors Ischemic heart disease (CAD) 70% hypertension
The ACC Heart Failure Guidelines
 The ACC Heart Failure Guidelines Fakhr Alayoubi, Msc,R Ph President of SCCP Cardiology Clinical Pharmacist Assistant Professor At King Saud University King Khalid University Hospital Riyadh-KSA 2017 ACC/AHA/HFSA
The ACC Heart Failure Guidelines Fakhr Alayoubi, Msc,R Ph President of SCCP Cardiology Clinical Pharmacist Assistant Professor At King Saud University King Khalid University Hospital Riyadh-KSA 2017 ACC/AHA/HFSA
β adrenergic blockade, a renal perspective Prof S O McLigeyo
 β adrenergic blockade, a renal perspective Prof S O McLigeyo Carvedilol Third generation β blocker (both β 1 and β 2 ) Possesses α 1 adrenergic blocking properties. β: α blocking ratio 7:1 to 3:1 Antioxidant
β adrenergic blockade, a renal perspective Prof S O McLigeyo Carvedilol Third generation β blocker (both β 1 and β 2 ) Possesses α 1 adrenergic blocking properties. β: α blocking ratio 7:1 to 3:1 Antioxidant
Incidence. 4.8 million in the United States. 400,000 new cases/year. 20 million patients with asymptomatic LV dysfunction
 Heart Failure Diagnosis According to the Working Group in Heart Failure, CHF is a syndrome where the diagnosis has the following essential components: A combination of: Symptoms, typically breathlessness
Heart Failure Diagnosis According to the Working Group in Heart Failure, CHF is a syndrome where the diagnosis has the following essential components: A combination of: Symptoms, typically breathlessness
Combination of renin-angiotensinaldosterone. how to choose?
 Combination of renin-angiotensinaldosterone system inhibitors how to choose? Karl Swedberg Professor of Medicine Sahlgrenska Academy University of Gothenburg karl.swedberg@gu.se Disclosures Research grants
Combination of renin-angiotensinaldosterone system inhibitors how to choose? Karl Swedberg Professor of Medicine Sahlgrenska Academy University of Gothenburg karl.swedberg@gu.se Disclosures Research grants
HYPERTENSION IN CKD. LEENA ONGAJYOOTH, M.D., Dr.med RENAL UNIT SIRIRAJ HOSPITAL
 HYPERTENSION IN CKD LEENA ONGAJYOOTH, M.D., Dr.med RENAL UNIT SIRIRAJ HOSPITAL Stages in Progression of Chronic Kidney Disease and Therapeutic Strategies Complications Normal Increased risk Damage GFR
HYPERTENSION IN CKD LEENA ONGAJYOOTH, M.D., Dr.med RENAL UNIT SIRIRAJ HOSPITAL Stages in Progression of Chronic Kidney Disease and Therapeutic Strategies Complications Normal Increased risk Damage GFR
Dose. Route. Units. Given. Special situations. Dose. Route. Units. Given. Special situations
 Chapter 3 Cardiology Georgia Woodfield ASPIRIN FONDAPARINUX 300 once only in acute MI 75 in primary/ secondary prevention of thrombus formation and thromboembolic disease or PR; can also be given via nasogastric
Chapter 3 Cardiology Georgia Woodfield ASPIRIN FONDAPARINUX 300 once only in acute MI 75 in primary/ secondary prevention of thrombus formation and thromboembolic disease or PR; can also be given via nasogastric
Long-Term Care Updates
 Long-Term Care Updates July 2015 By Amy Friedman Wilson, PharmD Heart failure (HF) is a clinical condition in which ventricular filling or ejection of blood is structurally or functionally impaired. 1
Long-Term Care Updates July 2015 By Amy Friedman Wilson, PharmD Heart failure (HF) is a clinical condition in which ventricular filling or ejection of blood is structurally or functionally impaired. 1
LCZ696 A First-in-Class Angiotensin Receptor Neprilysin Inhibitor
 The Angiotensin Receptor Neprilysin Inhibitor LCZ696 in Heart Failure with Preserved Ejection Fraction The Prospective comparison of ARNI with ARB on Management Of heart failure with preserved ejection
The Angiotensin Receptor Neprilysin Inhibitor LCZ696 in Heart Failure with Preserved Ejection Fraction The Prospective comparison of ARNI with ARB on Management Of heart failure with preserved ejection
Core Safety Profile. Pharmaceutical form(s)/strength: Film-coated tablets 1.25 mg, 2.5 mg, 3.75 mg, 5 mg, 7.5 mg and 10 mg. Date of FAR:
/strength: Film-coated tablets 1.25 mg, 2.5 mg, 3.75 mg, 5 mg, 7.5 mg and 10 mg. Date of FAR:") Core Safety Profile Active substance: Bisoprolol Pharmaceutical form(s)/strength: Film-coated tablets 1.25 mg, 2.5 mg, 3.75 mg, 5 mg, 7.5 mg and 10 mg P - RMS: FI/H/PSUR/0002/002 Date of FAR: 13.12.2011
Core Safety Profile Active substance: Bisoprolol Pharmaceutical form(s)/strength: Film-coated tablets 1.25 mg, 2.5 mg, 3.75 mg, 5 mg, 7.5 mg and 10 mg P - RMS: FI/H/PSUR/0002/002 Date of FAR: 13.12.2011
DISCLOSURES ACHIEVING SUCCESS THROUGH FAILURE: UPDATE ON HEART FAILURE WITH PRESERVED EJECTION FRACTION NONE
 ACHIEVING SUCCESS THROUGH FAILURE: UPDATE ON HEART FAILURE WITH PRESERVED EJECTION FRACTION Lori M. Tam, MD Providence Heart Institute DISCLOSURES NONE 1 OUTLINE Systolic vs. Diastolic Heart Failure New
ACHIEVING SUCCESS THROUGH FAILURE: UPDATE ON HEART FAILURE WITH PRESERVED EJECTION FRACTION Lori M. Tam, MD Providence Heart Institute DISCLOSURES NONE 1 OUTLINE Systolic vs. Diastolic Heart Failure New
Section 3, Lecture 2
 59-291 Section 3, Lecture 2 Diuretics: -increase in Na + excretion (naturesis) Thiazide and Related diuretics -decreased PVR due to decreases muscle contraction -an economical and effective treatment -protect
59-291 Section 3, Lecture 2 Diuretics: -increase in Na + excretion (naturesis) Thiazide and Related diuretics -decreased PVR due to decreases muscle contraction -an economical and effective treatment -protect
Updates in Heart Failure (HF) 2016: ACC / AHA and ESC
 2016: ACC / AHA and ESC") Updates in Heart Failure (HF) 2016: ACC / AHA and ESC Patrick McBride, MD, MPH Professor of Medicine & Family Medicine, UW School of Medicine and Public Health Special thanks to: Clyde W. Yancy, MD, MSc
Updates in Heart Failure (HF) 2016: ACC / AHA and ESC Patrick McBride, MD, MPH Professor of Medicine & Family Medicine, UW School of Medicine and Public Health Special thanks to: Clyde W. Yancy, MD, MSc
2/15/2017. Disclosures. Heart Failure = Big Problem. Heart Failure Update Reducing Hospitalizations and Improving Patient Outcomes 02/18/2017
 Heart Failure Update Reducing Hospitalizations and Improving Patient Outcomes 02/18/2017 Julio A. Barcena, M.D. South Miami Heart Specialists Disclosures I have no relevant commercial relationships to
Heart Failure Update Reducing Hospitalizations and Improving Patient Outcomes 02/18/2017 Julio A. Barcena, M.D. South Miami Heart Specialists Disclosures I have no relevant commercial relationships to
Update in Cardiology What s Hot in 2017?
 Update in Cardiology What s Hot in 2017? Mark R. Milunski, MD, FACC, FACP Chief, Cardiology Section Orlando Veterans Affairs Medical Center Associate Professor of Medicine University of Central Florida
Update in Cardiology What s Hot in 2017? Mark R. Milunski, MD, FACC, FACP Chief, Cardiology Section Orlando Veterans Affairs Medical Center Associate Professor of Medicine University of Central Florida
Introductory Clinical Pharmacology Chapter 41 Antihypertensive Drugs
 Introductory Clinical Pharmacology Chapter 41 Antihypertensive Drugs Blood Pressure Normal = sys
Introductory Clinical Pharmacology Chapter 41 Antihypertensive Drugs Blood Pressure Normal = sys
Coronary Artery Disease (CAD) Clinician Guide SEPTEMBER 2017
 Clinician Guide SEPTEMBER 2017") Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Coronary Artery Disease (CAD) Clinician Guide SEPTEMBER 2017 Introduction This Clinician Guide is based on the 2017 KP National Coronary Artery Disease
Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Coronary Artery Disease (CAD) Clinician Guide SEPTEMBER 2017 Introduction This Clinician Guide is based on the 2017 KP National Coronary Artery Disease
LITERATURE REVIEW: HEART FAILURE. Chief Residents
 LITERATURE REVIEW: HEART FAILURE Chief Residents Heart Failure EF 40% HFrEF Problem with contractility EF 40-50% HFmrEF EF > 50% HFpEF Problem with filling/relaxation RISK FACTORS Post MI HTN DM Obesity
LITERATURE REVIEW: HEART FAILURE Chief Residents Heart Failure EF 40% HFrEF Problem with contractility EF 40-50% HFmrEF EF > 50% HFpEF Problem with filling/relaxation RISK FACTORS Post MI HTN DM Obesity
Heart Failure: Combination Treatment Strategies
 Heart Failure: Combination Treatment Strategies M. McDonald MD, FRCP State of the Heart Symposium May 28, 2011 None Disclosures Case 69 F, prior MIs (LV ejection fraction 25%), HTN No demonstrable ischemia
Heart Failure: Combination Treatment Strategies M. McDonald MD, FRCP State of the Heart Symposium May 28, 2011 None Disclosures Case 69 F, prior MIs (LV ejection fraction 25%), HTN No demonstrable ischemia
HEART FAILURE. Heart Failure in the US. Heart Failure (HF) 3/2/2014
 3/2/2014") HEART FAILURE Martina Frost, PA-C Desert Cardiology of Tucson Northwest Medical Center March 2014 Heart Failure in the US Prevalence - ~5 million 650,000 new cases annually 300,000 deaths annually Leading
HEART FAILURE Martina Frost, PA-C Desert Cardiology of Tucson Northwest Medical Center March 2014 Heart Failure in the US Prevalence - ~5 million 650,000 new cases annually 300,000 deaths annually Leading
CKD Satellite Symposium
 CKD Satellite Symposium Recommended Therapy by Heart Failure Stage AHA/ACC Task Force on Practice Guideline 2001 Natural History of Heart Failure Patients surviving % Mechanism of death Sudden death 40%
CKD Satellite Symposium Recommended Therapy by Heart Failure Stage AHA/ACC Task Force on Practice Guideline 2001 Natural History of Heart Failure Patients surviving % Mechanism of death Sudden death 40%
Cardiology. Self Learning Package. Module 5: Pharmacology: Treatment of Acute Coronary. Prevention
 Cardiology Self Learning Package Module 5: Pharmacology: Treatment of Acute Coronary Syndromes, Module 5: Pharmacology: Hyperlipidaemia, Treatment of Acute Coronary Hypertension, Symdrome, Hyperlipidaemia,
Cardiology Self Learning Package Module 5: Pharmacology: Treatment of Acute Coronary Syndromes, Module 5: Pharmacology: Hyperlipidaemia, Treatment of Acute Coronary Hypertension, Symdrome, Hyperlipidaemia,
Management of Hypertension. M Misra MD MRCP (UK) Division of Nephrology University of Missouri School of Medicine
 Division of Nephrology University of Missouri School of Medicine") Management of Hypertension M Misra MD MRCP (UK) Division of Nephrology University of Missouri School of Medicine Disturbing Trends in Hypertension HTN awareness, treatment and control rates are decreasing
Management of Hypertension M Misra MD MRCP (UK) Division of Nephrology University of Missouri School of Medicine Disturbing Trends in Hypertension HTN awareness, treatment and control rates are decreasing
Dr. Vishaal Bhat. anti-adrenergic drugs
 Dr. Vishaal Bhat anti-adrenergic drugs Divisions of human nervous system Human Nervous system Central Nervous System Peripheral Nervous System Autonomic Nervous System Nervous system Includes neurons and
Dr. Vishaal Bhat anti-adrenergic drugs Divisions of human nervous system Human Nervous system Central Nervous System Peripheral Nervous System Autonomic Nervous System Nervous system Includes neurons and
Satish K Surabhi, MD.FACC,FSCAI,RPVI Medical Director, Cardiac Cath Labs AnMed Health Heart & Vascular Care
 Satish K Surabhi, MD.FACC,FSCAI,RPVI Medical Director, Cardiac Cath Labs AnMed Health Heart & Vascular Care None Fig. 1. Progression of Heart Failure.With each hospitalization for acute heart failure,
Satish K Surabhi, MD.FACC,FSCAI,RPVI Medical Director, Cardiac Cath Labs AnMed Health Heart & Vascular Care None Fig. 1. Progression of Heart Failure.With each hospitalization for acute heart failure,
Guideline-Directed Medical Therapy
 Guideline-Directed Medical Therapy Cardiovascular Outcomes Assessment of the MitraClip Percutaneous Therapy for Heart Failure Patients with Functional Mitral Regurgitation OPTIMAL THERAPY (As defined in
Guideline-Directed Medical Therapy Cardiovascular Outcomes Assessment of the MitraClip Percutaneous Therapy for Heart Failure Patients with Functional Mitral Regurgitation OPTIMAL THERAPY (As defined in
Combining Antihypertensives in People with Diabetes
 Combining ntihypertensives in People with Diabetes The majority of people with diabetes will develop hypertension and this subsequently increases the risk of microvascular and macrovascular complications.
Combining ntihypertensives in People with Diabetes The majority of people with diabetes will develop hypertension and this subsequently increases the risk of microvascular and macrovascular complications.
JNC Evidence-Based Guidelines for the Management of High Blood Pressure in Adults
 JNC 8 2014 Evidence-Based Guidelines for the Management of High Blood Pressure in Adults Table of Contents Why Do We Treat Hypertension? Blood Pressure Treatment Goals Initial Therapy Strength of Recommendation
JNC 8 2014 Evidence-Based Guidelines for the Management of High Blood Pressure in Adults Table of Contents Why Do We Treat Hypertension? Blood Pressure Treatment Goals Initial Therapy Strength of Recommendation
Disclosures for Presenter
 A Comparison of Angiotensin Receptor- Neprilysin Inhibition (ARNI) With ACE Inhibition in the Long-Term Treatment of Chronic Heart Failure With a Reduced Ejection Fraction Milton Packer, John J.V. McMurray,
A Comparison of Angiotensin Receptor- Neprilysin Inhibition (ARNI) With ACE Inhibition in the Long-Term Treatment of Chronic Heart Failure With a Reduced Ejection Fraction Milton Packer, John J.V. McMurray,
Introduction. Factors affecting blood pressure: 1-COP = HR X SV mainly affect SBP. 2-TPR = diameter of arterioles X viscosity of blood affect DBP
 Introduction Hypertension is a persistent elevation of blood pressure above 140 / 90 mmhg for more than three sitting. (0ptimal level
Introduction Hypertension is a persistent elevation of blood pressure above 140 / 90 mmhg for more than three sitting. (0ptimal level
Performance and Quality Measures 1. NQF Measure Number. Coronary Artery Disease Measure Set
 Unless indicated, the PINNACLE Registry measures are endorsed by the American College of Cardiology Foundation and the American Heart Association and may be used for purposes of health care insurance payer
Unless indicated, the PINNACLE Registry measures are endorsed by the American College of Cardiology Foundation and the American Heart Association and may be used for purposes of health care insurance payer
578 Index. Eplerenone, 7, 29, 119, 120, 126, 275, 276,
 Index A AC. See Adenylate cyclase (AC) ACEI. See Angiotensin converting enzyme inhibitors (ACEI) Adenosine, 179, 180, 182 184, 191, 196 198 Adenosine A1 receptor, 179 183, 186, 190 198 Adenylate cyclase
Index A AC. See Adenylate cyclase (AC) ACEI. See Angiotensin converting enzyme inhibitors (ACEI) Adenosine, 179, 180, 182 184, 191, 196 198 Adenosine A1 receptor, 179 183, 186, 190 198 Adenylate cyclase
HeFSSA Practitioners Program 2017 Theme The Patient Journey: Feel Good and Live Long. Case Study 2
 HeFSSA Practitioners Program 2017 Theme The Patient Journey: Feel Good and Live Long Case Study 2 HEART FAILURE WITH MID-RANGE EJECTION FRACTION TREATMENT OPTIONS CLINICAL CASE MEDICAL HISTORY 59-year-old
HeFSSA Practitioners Program 2017 Theme The Patient Journey: Feel Good and Live Long Case Study 2 HEART FAILURE WITH MID-RANGE EJECTION FRACTION TREATMENT OPTIONS CLINICAL CASE MEDICAL HISTORY 59-year-old
New Paradigms in Rx of Symptomati Heart Failure:Role of Ivabradine & Angiotensin Neprilysin Inhibition
 New Paradigms in Rx of Symptomati Heart Failure:Role of Ivabradine & Angiotensin Neprilysin Inhibition Prakash Deedwania, MD, FACC, FACP, FCCP, FAHA Professor of Medicine, UCSF School of Medicine, Director,
New Paradigms in Rx of Symptomati Heart Failure:Role of Ivabradine & Angiotensin Neprilysin Inhibition Prakash Deedwania, MD, FACC, FACP, FCCP, FAHA Professor of Medicine, UCSF School of Medicine, Director,
Antihypertensive Agents
 Antihypertensive Agents Southern California University of Health Sciences Physician Assistant Program Management and Treatment of Hypertension April 7, 08, presented by Ezra Levy, Pharm.D! Usual Dose,
Antihypertensive Agents Southern California University of Health Sciences Physician Assistant Program Management and Treatment of Hypertension April 7, 08, presented by Ezra Levy, Pharm.D! Usual Dose,
HEART FAILURE PHARMACOLOGY. University of Hawai i Hilo Pre- Nursing Program NURS 203 General Pharmacology Danita Narciso Pharm D
 HEART FAILURE PHARMACOLOGY University of Hawai i Hilo Pre- Nursing Program NURS 203 General Pharmacology Danita Narciso Pharm D 1 LEARNING OBJECTIVES Understand the effects of heart failure in the body
HEART FAILURE PHARMACOLOGY University of Hawai i Hilo Pre- Nursing Program NURS 203 General Pharmacology Danita Narciso Pharm D 1 LEARNING OBJECTIVES Understand the effects of heart failure in the body
Antihypertensives. Diagnostic category
 Measurement of blood pressure At first assessment, take both arms then choose the one with the higher reading. Beware of orthostatic hypotension. Measure BP in sitting position, and repeat after patient
Measurement of blood pressure At first assessment, take both arms then choose the one with the higher reading. Beware of orthostatic hypotension. Measure BP in sitting position, and repeat after patient