Disclosures. Objectives 10/11/17. Short Term Mechanical Circulatory Support for Advanced Cardiogenic Shock. I have no disclosures to report
|
|
|
- Charla Atkins
- 5 years ago
- Views:
Transcription
1 Short Term Mechanical Circulatory Support for Advanced Cardiogenic Shock Christopher K. Gordon MSN, ACNP-BC Disclosures I have no disclosures to report 1. Pathophysiology 2. Epidemiology 3. Assessment 4. Management 1. Medical 2. Mechanical Objectives 1
2 Heart Failure A condition in which there is insufficient cardiac output to meet the metabolic demands of the body. Can be caused by a variety of conditions that decrease the ability of the heart muscle to pump blood; either by damaging and/or overloading Heart Failure Estimated 5.7 million people in the United States have heart failure. Heart Failure expected to increase to > 8 million by Acute Coronary Syndrome affecting nearly 700,000 people annually One of the most frequent causes of unscheduled hospital admissions Eargle, K., Ochsner Journal, 16: Heart Failure Divided into multiple sub-categories Left sided Right sided Bi-Ventricular Acute Chronic Acute on Chronic Systolic Diastolic 2
3 Acute Heart Failure (AHF) Can occur with either impaired or preserved ejection fraction Heart failure is categorized as a heart disorder but can lead to a systemic disorder affecting all vital organs Mechanisms of dysfunction: Congestion and hypo-perfusion Management of AHF Needs to be efficient, rapid and organized Multidisciplinary Care: Intensivists, Heart Failure Cardiologist, Interventional Cardiologist, Cardiac Surgeon, Advance practice provider, Nurse, Respiratory therapist Goals of care Restoring Cardiac Output Identifying and treating the etiology Clinical Presentation of AHF Importance of physical exam Jugular Vein Distension (JVD) Hepatomegaly Peripheral Edema Tachypnea Rales Orthopnea Gallops (S 3 ) Heart Murmurs Tachycardia Pulsus alternans Cool Extremities Restlessness and/or confusion 3

4 Diagnostic Evaluation Blood laboratory tests: Brain natriuretic peptide (BNP) Troponins Renal Function Liver Function Lactic acid Blood gas analysis Studies: Electrocardiogram (ECG) Echocardiogram Chest X-rays Early cardiac catheterization If indicated Hemodynamic Profile Warm & Wet Diuretics Loop Diuretics are typical first line Furosemide bolus (0.5 mg/kg) Thiazide Diuretics, combination therapy or 2 nd line Diuril 250 mg to 500mg IV bolus Vasodilators Nitrates Nitroglycerin (10-20 mcg/min, up to 200 mcg/min) Nitroprusside (0.3 mcg/kg/min, up to 5 mcg/kg/min) 4
5 Oxygen Warm & Wet Often needed secondary to hypoxia related to pulmonary edema Use of Non Invasive Ventilation Pulmonary edema often times can rapidly progress Due to flooding of the alveoli secondary to increase in hydrostatic capillary pressure with the lung Morphine Opiate that can help with anxiety related to air hunger Can lead to increased rates of intubation Cold & Wet Cardiogenic Shock Clinically presents as hypotension with evidence of organ hypo-perfusion Altered Mental Status Cold, clammy skin and/or extremities (mottling) Oliguria ( < 0.5 ml/kg/hr or < 30 ml/hr) Respiratory distress in the form of pulmonary congestion Cardiogenic Shock The most severe form of acute heart failure Commonly a direct sequelae of acute coronary syndrome Complicating ~ 5%-8% of acute myocardial infarctions Non-ischemic Etiologies less common (1%) Acute on chronic decompensations Myocarditis Takotsubo cardiomyopathy Acute valvular disease Eargle, K., Ochsner Journal, 16:
6 Cardiogenic Shock Hemodynamically defined as: Persistent hypotension with systolic blood pressure < 90 mmhg or mean arterial blood pressure 30 mmhg below baseline Inadequate Cardiac Output/Cardiac Index (CI < 2.2L/min/m 2 ) despite normal or elevated pre-load Pulmonary capillary wedge pressure > or = to 18 mmhg Central venous pressure > or = to 10 mmhg Medical Management Goal is to restore Cardiac Output and reverse end-organ dysfunction Hemodynamic Evaluation Echocardiograms Arterial line Serial Labs Lactic acid Blood gases Liver function Renal function Central Venous Access (SVC vs PAC) ScvO 2 and CVP SvO 2, CVP, PCWP, PVR, SVR, Stroke volume Inotropes Intravenous medications used to improve cardiac contractility Use for the shortest duration and at the lowest dose to maintain perfusion Adverse Risks: Increased risk of atrial and ventricular arrhythmias Systemic Hypotension Increased Myocardial Oxygen Demand 6
7 Dobutamine Synthetic catecholamine that stimulates Beta 1 receptors Does not increase blood pressure; can stimulate peripheral Beta 2 receptors that can lead to hypotension Frequently associated with: Tachycardia Arrhythmias: supraventricular and ventricular Increased myocardial oxygen demand Dosing: 2 to 20 mcg/kg/min Short half life Milrinone Phosphodiesterase inhibitor Increases cyclic AMP levels thus increasing intracellular calcium levels Net result is increased inotropy Vasodilation of both pulmonary and systemic circulatory systems Often require combination vasopressor support No significant chronotropic affects Can lead to arrhythmias due to increase in myocardial oxygen demand Dose: to 0.75 mcg/kg/min Long half life (2-6 hours) Renally cleared Epinephrine Catecholamine: non specific agonist of all adrenergic receptors Beta 1,2,3, Alpha 1,2 dose dependent Frequently associated with: Tachycardia Hypertension Arrhythmias: supraventricular and ventricular Increased myocardial oxygen demand Dosing: 0.02 to 0.2 mcg/kg/min Short half life 7
8 Vasopressors Intravenous medications used to improve blood pressure Use for the shortest duration and at the lowest dose to maintain perfusion Adverse Risks: Decreased peripheral tissue perfusion Decreased microcirculation Lead to tissue necrosis Norepinephrine Catecholamine: potent vasoconstrictor Alpha 1 agonist Frequently associated with: Bradycardia Hypertension Arrhythmias: supraventricular and ventricular Limb Ischemia Dosing: 0.02 to 0.2 mcg/kg/min (higher doses used in sepsis) Short half life Dopamine Catecholamine: non specific agonist of all adrenergic receptors Beta 1,2,3, Alpha 1,2, Dopa dose dependent Frequently associated with: Tachycardia Arrhythmias: supraventricular and ventricular Increased myocardial oxygen demand Dosing: 2 to 20 mcg/kg/min Short half life 8
9 Failure of Medical Management Persistent hypotension & hypo-perfusion despite use of 2 or more inotropic and/or vasopressor agents Rising lactic acid Evolving organ dysfunction Short Term MCS Devices 1. Intra Aortic Balloon Pump (IABP) 2. Impella 3. Tandem Heart 4. Extra Corporeal Membrane Oxygenation (ECMO) Short Term MCS Optimal timing / early initiation of mechanical support Optimal level of support to restore adequate perfusion of end organs Optimal prevention and management of potential device related complicates 9
 Can increase Cardiac Output ~ 0.")

")
10 IABP Helium filled balloon Inflates during diastole / Deflates during Systole Volume shifting ~ 40ml per heart beat (inc. SV) Can increase Cardiac Output ~ 0.5 to 1L During Diastole Increase Coronary Perfusion Improved reperfusion after intervention During Systole Hallmark is afterload reduction Reduction in LV end-diastolic pressure Reduction in pulmonary capillary wedge pressure Decrease in LV wall stress and myocardial oxygen demand IABP Percutaneously placed via the femoral artery or left axillary artery (7 to 8 French) Placed in the descending thoracic aorta Can be placed at the bedside, cath lab or OR Quick initiation Complications Bleeding Hemolysis Risk of limb ischemia Vascular compromise (dissection) Management Low complexity Trigger / Timing is automatic (1:1,1:2,1:3) Anticoagulation Heparin drip (PTT goal 40-50) Vascular checks 10


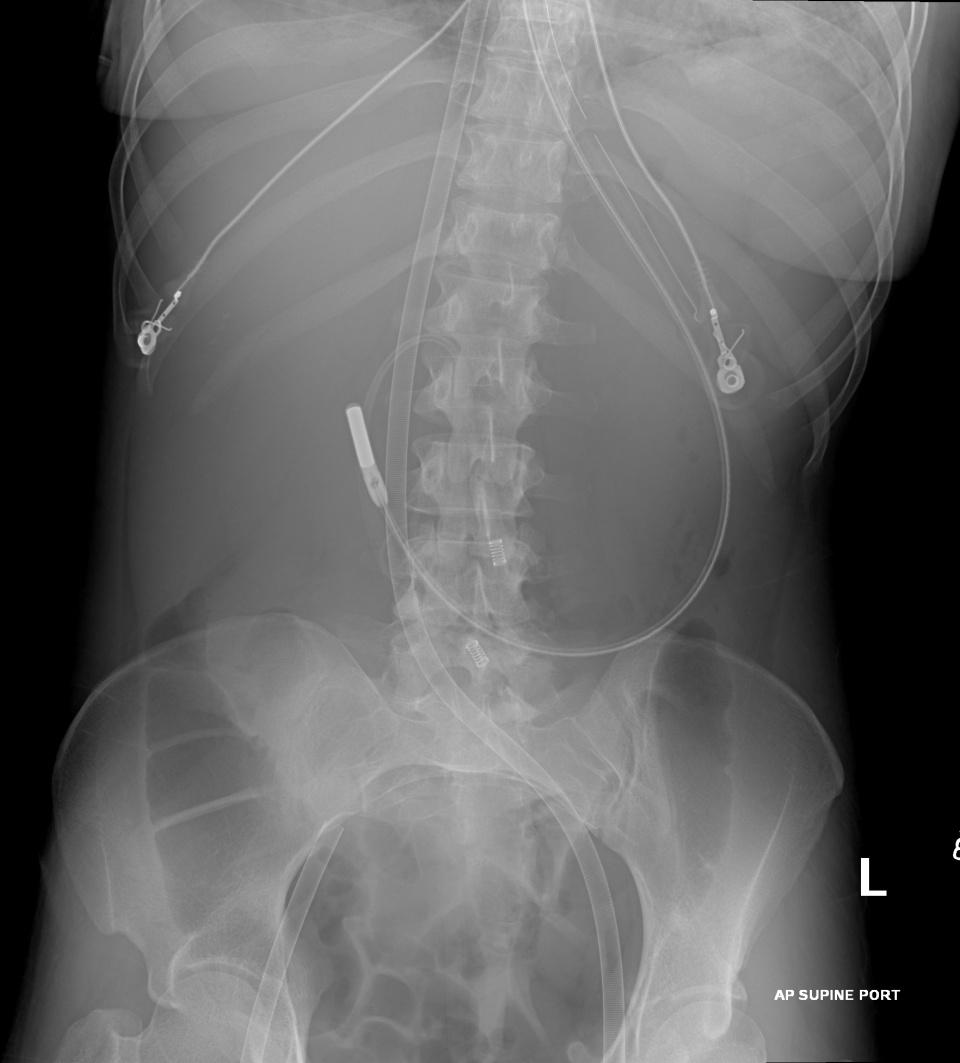
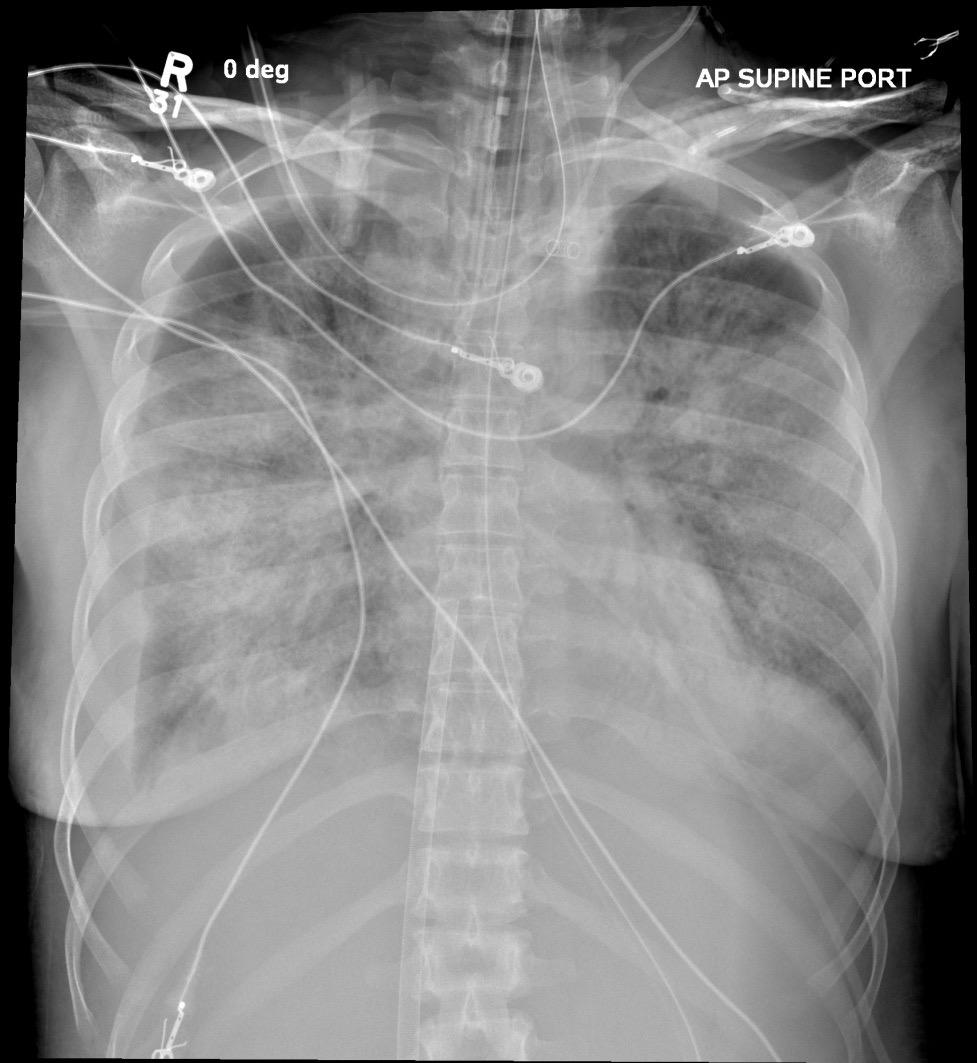
11 Tandem Heart A continuous flow centrifugal pump Can supply up to 4L/min cardiac output Percutaneously placed via the femoral vessels: 21 Fr inflow cannula: left atrium via femoral vein and then trans-septal puncture Fr outflow in the femoral artery Placed in the cardiac cath lab Tandem Heart 11
12 Tandem Heart Superior to the IABP in improving hemodynamic endpoints: Greater increase in cardiac output/cardiac index Greater increase in mean arterial pressure Greater decrease in cardiac filling pressures Reduced PCWP, CVP, PAP Reduced cardiac workload and oxygen demand Tandem Heart Complexity of insertion limits the use Complications Vascular compromise Malposition of cannula Can cause intra cardiac shunt Bleeding / Coagulopathies Insertion site GIB Limb Ischemia Infection SIRS/Sepsis Stroke Management Higher level of training required Nursing, advanced practice providers, physicians Anticoagulation PTT Vascular checks Device placement X-ray and Echocardiograms 12
13 Impella Continuous Axial Flow Pump Positioned across the aortic valve via access from the femoral artery Typically placed in the Cath Lab or OR Fluoroscopy and Echocardiogram guided Interventional Cardiology and/or Surgeon 3 Impella Devices: Impella 1. Imeplla Fr cannula percutaneously placed 12Fr mirco-axial catheter pump Can provide up to 2.5 LPM cardiac output 2. Impella CP Percutaneously placed 14Fr mirco-axial catheter pump Can provide up to 4.0 LPM cardiac output 3. Impella 5.0 Impella 22 Fr cannula placed by cut down of the femoral artery 21 Fr micro-axial catheter pump Can provide up to 5.0 LPM cardiac output Needs Surgical repair for removal Can also be placed via axillary artery 13




14 Bleeding Hemolysis Risk of limb ischemia Aortic Insufficiency Complications Management Anticoagulation Vascular checks Placement Echocardiogram and x-ray Vascular compromise (dissection) Malposition 14


15 ECMO: Extracorporeal membrane oxygenation (ECMO) A technique of providing cardiac and/or respiratory support to patients whose heart and lungs are unable to function appropriately. Works by removing blood from the body, artificially removing carbon dioxide, and reoxygenating red blood cells prior to returning blood back to the body. 15

 Bypasses/rests the")


 Circuit CentriMag Magnetically levitated,")

16 Basic Principles of ECMO Support for the failing heart and/or lungs Must meet metabolic demands: Cardiac output (VA) Adequate oxygenation and CO2 regulation Veno-arterial (VA) Bypasses/rests the heart & lungs Drains blood from venous system, returns oxygenated blood to arterial circulation Veno-venous (VV) Rests the lungs, relying on native cardiac circulation Drains blood from venous system, returns oxygenated blood to venous system (right atrium) Circuit CentriMag Magnetically levitated, centrifugal pump 2-10LPM Oxygenator & Blood pump are separate Circuit CardioHelp Centrifugal pump 2-10LPM Blood pump & oxygenator are 1 piece 16
 Leading to increased myocardial wall stress Decreased LV Pre-load")
17 ECMO Percutaneous placement by any trained provider in any location: Intensivist, Cardiologist, Surgeon, Emergency Room Arterial Access: 15 to 19 Fr Venous Access: 21 to 27 Fr Limb Perfusion catheter: 5 to 7 Fr Typical Flow 4-6 LPM Provides both cardiac and pulmonary support to the patient Can increase Afterload (No AI) Leading to increased myocardial wall stress Decreased LV Pre-load Decreased PCWP Decreased myocardial oxygen demand Management Bedside Nurse vs Perfusion Arterial blood returned in retrograde direction 2 Perfusion circuits Native vs ECMO Harlequin Syndrome --> need to monitor oxygenation from right radial artery Anticoagulation Heparin drip with PTT goal Hemorrhage vs embolic events vs hemolysis Vascular Checks Complications Bleeding Hemolysis Limb ischemia Vascular compromise (dissection) Thromboembolic events Aortic Insufficiency 17


18 18


19 Summary Cardiogenic Shock continues to carry a high in-hospital mortality rate, 40-50% despite advances in early revascularization Early identification and initiation of therapy is paramount in preventing development of multi-system organ dysfunction Hallmark therapies with inotropes/vasopressor and early revascularization have led to the reduction of mortality, but rates remain high Advances in mechanical circulatory support offer innovative ways to restore circulation and rest the heart but further research is needed Werdan, K., European Heart Journal, 35: Shah, P., Crit Care Clin, 30: Thank You 19
Management of Cardiogenic Shock. Dr Stephen Pettit, Consultant Cardiologist
 Dr Stephen Pettit, Consultant Cardiologist Cardiogenic shock Management of Cardiogenic Shock Outline Definition, INTERMACS classification Medical management of cardiogenic shock PA catheters and haemodynamic
Dr Stephen Pettit, Consultant Cardiologist Cardiogenic shock Management of Cardiogenic Shock Outline Definition, INTERMACS classification Medical management of cardiogenic shock PA catheters and haemodynamic
Cath Lab Essentials : LV Assist Devices for Hemodynamic Support (IABP, Impella, Tandem Heart, ECMO)
") Cath Lab Essentials : LV Assist Devices for Hemodynamic Support (IABP, Impella, Tandem Heart, ECMO) Michael A. Gibson, MD Assistant Professor of Medicine University of California, Irvine Division of Cardiology
Cath Lab Essentials : LV Assist Devices for Hemodynamic Support (IABP, Impella, Tandem Heart, ECMO) Michael A. Gibson, MD Assistant Professor of Medicine University of California, Irvine Division of Cardiology
Protocol Identifier Subject Identifier Visit Description. [Y] Yes [N] No. [Y] Yes [N] N. If Yes, admission date and time: Day Month Year
![Protocol Identifier Subject Identifier Visit Description. [Y] Yes [N] No. [Y] Yes [N] N. If Yes, admission date and time: Day Month Year](/thumbs/76/74263761.jpg "Protocol Identifier Subject Identifier Visit Description. [Y] Yes [N] No. [Y] Yes [N] N. If Yes, admission date and time: Day Month Year") PAST MEDICAL HISTORY Has the subject had a prior episode of heart failure? o Does the subject have a prior history of exposure to cardiotoxins, such as anthracyclines? URGENT HEART FAILURE VISIT Did heart
PAST MEDICAL HISTORY Has the subject had a prior episode of heart failure? o Does the subject have a prior history of exposure to cardiotoxins, such as anthracyclines? URGENT HEART FAILURE VISIT Did heart
Percutaneous Mechanical Circulatory Support for Cardiogenic Shock. 24 th Annual San Diego Heart Failure Symposium Ryan R Reeves, MD FSCAI
 Percutaneous Mechanical Circulatory Support for Cardiogenic Shock 24 th Annual San Diego Heart Failure Symposium Ryan R Reeves, MD FSCAI The Need for Circulatory Support Basic Pathophysiologic Problems:
Percutaneous Mechanical Circulatory Support for Cardiogenic Shock 24 th Annual San Diego Heart Failure Symposium Ryan R Reeves, MD FSCAI The Need for Circulatory Support Basic Pathophysiologic Problems:
Medical Management of Acute Heart Failure
 Critical Care Medicine and Trauma Medical Management of Acute Heart Failure Mary O. Gray, MD, FAHA Associate Professor of Medicine University of California, San Francisco Staff Cardiologist and Training
Critical Care Medicine and Trauma Medical Management of Acute Heart Failure Mary O. Gray, MD, FAHA Associate Professor of Medicine University of California, San Francisco Staff Cardiologist and Training
Management of Acute Shock and Right Ventricular Failure
 Management of Acute Shock and Right Ventricular Failure Nader Moazami, MD Department of Thoracic and Cardiovascular Surgery and Biomedical Engineering, Cleveland Clinic NONE Disclosures CARDIOGENIC SHOCK
Management of Acute Shock and Right Ventricular Failure Nader Moazami, MD Department of Thoracic and Cardiovascular Surgery and Biomedical Engineering, Cleveland Clinic NONE Disclosures CARDIOGENIC SHOCK
Introduction. Invasive Hemodynamic Monitoring. Determinants of Cardiovascular Function. Cardiovascular System. Hemodynamic Monitoring
 Introduction Invasive Hemodynamic Monitoring Audis Bethea, Pharm.D. Assistant Professor Therapeutics IV January 21, 2004 Hemodynamic monitoring is necessary to assess and manage shock Information obtained
Introduction Invasive Hemodynamic Monitoring Audis Bethea, Pharm.D. Assistant Professor Therapeutics IV January 21, 2004 Hemodynamic monitoring is necessary to assess and manage shock Information obtained
Medical Treatment for acute Decompensated Heart Failure. Vlasis Ninios Cardiologist St. Luke s s Hospital Thessaloniki 2011
 Medical Treatment for acute Decompensated Heart Failure Vlasis Ninios Cardiologist St. Luke s s Hospital Thessaloniki 2011 2010 HFSA guidelines for ADHF 2009 focused update of the 2005 American College
Medical Treatment for acute Decompensated Heart Failure Vlasis Ninios Cardiologist St. Luke s s Hospital Thessaloniki 2011 2010 HFSA guidelines for ADHF 2009 focused update of the 2005 American College
Complications of Acute Myocardial Infarction
 Acute Myocardial Infarction Complications of Acute Myocardial Infarction Diagnosis and Treatment JMAJ 45(4): 149 154, 2002 Hiroshi NONOGI Director, Division of Cardiology and Emergency Medicine, National
Acute Myocardial Infarction Complications of Acute Myocardial Infarction Diagnosis and Treatment JMAJ 45(4): 149 154, 2002 Hiroshi NONOGI Director, Division of Cardiology and Emergency Medicine, National
DIAGNOSIS AND MANAGEMENT OF ACUTE HEART FAILURE
 DIAGNOSIS AND MANAGEMENT OF ACUTE HEART FAILURE Mefri Yanni, MD Bagian Kardiologi dan Kedokteran Vaskular RS.DR.M.Djamil Padang The 3rd Symcard Padang, Mei 2013 Outline Diagnosis Diagnosis Treatment options
DIAGNOSIS AND MANAGEMENT OF ACUTE HEART FAILURE Mefri Yanni, MD Bagian Kardiologi dan Kedokteran Vaskular RS.DR.M.Djamil Padang The 3rd Symcard Padang, Mei 2013 Outline Diagnosis Diagnosis Treatment options
Diagnosis & Management of Heart Failure. Abena A. Osei-Wusu, M.D. Medical Fiesta
 Diagnosis & Management of Heart Failure Abena A. Osei-Wusu, M.D. Medical Fiesta Learning Objectives: 1) Become familiar with pathogenesis of congestive heart failure. 2) Discuss clinical manifestations
Diagnosis & Management of Heart Failure Abena A. Osei-Wusu, M.D. Medical Fiesta Learning Objectives: 1) Become familiar with pathogenesis of congestive heart failure. 2) Discuss clinical manifestations
Management of acute decompensated heart failure and cardiogenic shock. Arintaya Phrommintikul Department of Medicine CMU
 Management of acute decompensated heart failure and cardiogenic shock Arintaya Phrommintikul Department of Medicine CMU Acute heart failure: spectrum Case 64 y/o M with Hx of non-ischemic DCM (LVEF=25-30%)
Management of acute decompensated heart failure and cardiogenic shock Arintaya Phrommintikul Department of Medicine CMU Acute heart failure: spectrum Case 64 y/o M with Hx of non-ischemic DCM (LVEF=25-30%)
Mechanics of Cath Lab Support Devices
 Mechanics of Cath Lab Support Devices Issam D. Moussa, MD Professor of Medicine Mayo Clinic College of Medicine Chair, Division of Cardiovascular Diseases Mayo Clinic Jacksonville, Florida DISCLOSURE Presenter:
Mechanics of Cath Lab Support Devices Issam D. Moussa, MD Professor of Medicine Mayo Clinic College of Medicine Chair, Division of Cardiovascular Diseases Mayo Clinic Jacksonville, Florida DISCLOSURE Presenter:
Mechanics of Cath Lab Support Devices
 Mechanics of Cath Lab Support Devices Issam D. Moussa, MD Chief Medical Officer First Coast Cardiovascular Institute, Jacksonville, FL Professor of Medicine, UCF, Orlando, FL None DISCLOSURE Percutaneous
Mechanics of Cath Lab Support Devices Issam D. Moussa, MD Chief Medical Officer First Coast Cardiovascular Institute, Jacksonville, FL Professor of Medicine, UCF, Orlando, FL None DISCLOSURE Percutaneous
Mechanical circulatory support in cardiogenic shock The Cardiologist s view ACCA Masterclass 2017
 Mechanical circulatory support in cardiogenic shock The Cardiologist s view ACCA Masterclass 2017 Pascal Vranckx MD, PhD. Medical director Cardiac Critical Care Services Hartcentrum Hasselt Belgium Disclosure
Mechanical circulatory support in cardiogenic shock The Cardiologist s view ACCA Masterclass 2017 Pascal Vranckx MD, PhD. Medical director Cardiac Critical Care Services Hartcentrum Hasselt Belgium Disclosure
Hemodynamic Monitoring and Circulatory Assist Devices
 Hemodynamic Monitoring and Circulatory Assist Devices Speaker: Jana Ogden Learning Unit 2: Hemodynamic Monitoring and Circulatory Assist Devices Hemodynamic monitoring refers to the measurement of pressure,
Hemodynamic Monitoring and Circulatory Assist Devices Speaker: Jana Ogden Learning Unit 2: Hemodynamic Monitoring and Circulatory Assist Devices Hemodynamic monitoring refers to the measurement of pressure,
The Role of Mechanical Circulatory Support in Cardiogenic Shock: When to Utilize
 The Role of Mechanical Circulatory Support in Cardiogenic Shock: Presented by Nancy Scroggins ACNP, CNS-CC CV Surgery ACNP Bayshore Medical Center The Role of Mechanical Circulatory Support in Cardiogenic
The Role of Mechanical Circulatory Support in Cardiogenic Shock: Presented by Nancy Scroggins ACNP, CNS-CC CV Surgery ACNP Bayshore Medical Center The Role of Mechanical Circulatory Support in Cardiogenic
Percutaneous Mechanical Circulatory Support Devices
 Percutaneous Mechanical Circulatory Support Devices Daniel Vazquez RN, RCIS Miami Cardiac & Vascular Institute FINANCIAL DISCLOSURES none CASE STUDY CASE STUDY 52 year old gentlemen Complaining of dyspnea
Percutaneous Mechanical Circulatory Support Devices Daniel Vazquez RN, RCIS Miami Cardiac & Vascular Institute FINANCIAL DISCLOSURES none CASE STUDY CASE STUDY 52 year old gentlemen Complaining of dyspnea
Mechanical Cardiac Support in Acute Heart Failure. Michael Felker, MD, MHS Associate Professor of Medicine Director of Heart Failure Research
 Mechanical Cardiac Support in Acute Heart Failure Michael Felker, MD, MHS Associate Professor of Medicine Director of Heart Failure Research Disclosures Research Support and/or Consulting NHLBI Amgen Cytokinetics
Mechanical Cardiac Support in Acute Heart Failure Michael Felker, MD, MHS Associate Professor of Medicine Director of Heart Failure Research Disclosures Research Support and/or Consulting NHLBI Amgen Cytokinetics
SHOCK. Emergency pediatric PICU division Pediatric Department Medical Faculty, University of Sumatera Utara H. Adam Malik Hospital
 SHOCK Emergency pediatric PICU division Pediatric Department Medical Faculty, University of Sumatera Utara H. Adam Malik Hospital 1 Definition Shock is an acute, complex state of circulatory dysfunction
SHOCK Emergency pediatric PICU division Pediatric Department Medical Faculty, University of Sumatera Utara H. Adam Malik Hospital 1 Definition Shock is an acute, complex state of circulatory dysfunction
Swans and Pressors. Vanderbilt Surgery Summer School Ricky Shinall
 Swans and Pressors Vanderbilt Surgery Summer School Ricky Shinall Shock, Swans, Pressors in 15 minutes 4 Reasons for Shock 4 Swan numbers to know 7 Pressors =15 things to know 4 Reasons for Shock Not enough
Swans and Pressors Vanderbilt Surgery Summer School Ricky Shinall Shock, Swans, Pressors in 15 minutes 4 Reasons for Shock 4 Swan numbers to know 7 Pressors =15 things to know 4 Reasons for Shock Not enough
Swans and Pressors. Vanderbilt Surgery Summer School Ricky Shinall
 Swans and Pressors Vanderbilt Surgery Summer School Ricky Shinall SHOCK Hypotension SHOCK Hypotension SHOCK=Reduction of systemic tissue perfusion, resulting in decreased oxygen delivery to the tissues.
Swans and Pressors Vanderbilt Surgery Summer School Ricky Shinall SHOCK Hypotension SHOCK Hypotension SHOCK=Reduction of systemic tissue perfusion, resulting in decreased oxygen delivery to the tissues.
Post-Cardiac Surgery Evaluation
 Post-Cardiac Surgery Evaluation 20th Annual Heart Conference October 15, 2016 Gary A Mayman PROFESSOR PEDIATRICS UNIVERSITY OF NEVADA Look Touch Listen Temperature, pulse, respiratory rate, & blood pressure
Post-Cardiac Surgery Evaluation 20th Annual Heart Conference October 15, 2016 Gary A Mayman PROFESSOR PEDIATRICS UNIVERSITY OF NEVADA Look Touch Listen Temperature, pulse, respiratory rate, & blood pressure
Acute heart failure: ECMO Cardiology & Vascular Medicine 2012
 Acute heart failure: ECMO Cardiology & Vascular Medicine 2012 Lucia Jewbali cardiologist-intensivist 14 beds/8 ICU beds Acute coronary syndromes Heart failure/ Cardiogenic shock Post cardiotomy Heart
Acute heart failure: ECMO Cardiology & Vascular Medicine 2012 Lucia Jewbali cardiologist-intensivist 14 beds/8 ICU beds Acute coronary syndromes Heart failure/ Cardiogenic shock Post cardiotomy Heart
AllinaHealthSystem 1
 : Definition End-organ hypoperfusion secondary to cardiac failure Venoarterial ECMO: Patient Selection Michael A. Samara, MD FACC Advanced Heart Failure, Cardiac Transplant & Mechanical Circulatory Support
: Definition End-organ hypoperfusion secondary to cardiac failure Venoarterial ECMO: Patient Selection Michael A. Samara, MD FACC Advanced Heart Failure, Cardiac Transplant & Mechanical Circulatory Support
Rhondalyn C. McLean. 2 ND YEAR RESEARCH ELECTIVE RESIDENT S JOURNAL Volume VII, A. Study Purpose and Rationale
 A Randomized Clinical Study To Compare The Intra-Aortic Balloon Pump To A Percutaneous Left Atrial-To-Femoral Arterial Bypass Device For Treatment Of Cardiogenic Shock Following Acute Myocardial Infarction.
A Randomized Clinical Study To Compare The Intra-Aortic Balloon Pump To A Percutaneous Left Atrial-To-Femoral Arterial Bypass Device For Treatment Of Cardiogenic Shock Following Acute Myocardial Infarction.
University of Wisconsin - Madison Cardiovascular Medicine Fellowship Program UW CICU Rotation Goals and Objectives
 Background: The field of critical care cardiology has evolved considerably over the past 2 decades. Contemporary critical care cardiology is increasingly focused on the management of patients with advanced
Background: The field of critical care cardiology has evolved considerably over the past 2 decades. Contemporary critical care cardiology is increasingly focused on the management of patients with advanced
Topics to be Covered. Cardiac Measurements. Distribution of Blood Volume. Distribution of Pulmonary Ventilation & Blood Flow
 Topics to be Covered MODULE F HEMODYNAMIC MONITORING Cardiac Output Determinants of Stroke Volume Hemodynamic Measurements Pulmonary Artery Catheterization Control of Blood Pressure Heart Failure Cardiac
Topics to be Covered MODULE F HEMODYNAMIC MONITORING Cardiac Output Determinants of Stroke Volume Hemodynamic Measurements Pulmonary Artery Catheterization Control of Blood Pressure Heart Failure Cardiac
Hemodynamic Monitoring
 Perform Procedure And Interpret Results Hemodynamic Monitoring Tracheal Tube Cuff Pressure Dean R. Hess PhD RRT FAARC Hemodynamic Monitoring Cardiac Rate and Rhythm Arterial Blood Pressure Central Venous
Perform Procedure And Interpret Results Hemodynamic Monitoring Tracheal Tube Cuff Pressure Dean R. Hess PhD RRT FAARC Hemodynamic Monitoring Cardiac Rate and Rhythm Arterial Blood Pressure Central Venous
LV Distension and ECLS Lungs
 LV Distension and ECLS Lungs Kevin W. Hatton, MD, FCCM Interim Vice-Chair for Anesthesiology Research Division Chief, Anesthesiology Critical Care Medicine Program Director, Anesthesiology Critical Care
LV Distension and ECLS Lungs Kevin W. Hatton, MD, FCCM Interim Vice-Chair for Anesthesiology Research Division Chief, Anesthesiology Critical Care Medicine Program Director, Anesthesiology Critical Care
ECMO as a bridge to durable LVAD therapy. Jonathan Haft, MD Department of Cardiac Surgery University of Michigan
 ECMO as a bridge to durable LVAD therapy Jonathan Haft, MD Department of Cardiac Surgery University of Michigan Systolic Heart Failure Prevalence 4.8 million U.S. 287,000 deaths per year $39 billion spent
ECMO as a bridge to durable LVAD therapy Jonathan Haft, MD Department of Cardiac Surgery University of Michigan Systolic Heart Failure Prevalence 4.8 million U.S. 287,000 deaths per year $39 billion spent
DAY1_CARDIOVASCULAR PRACTICE QUESTIONS
 DAY1_CARDIOVASCULAR PRACTICE QUESTIONS 1 P age 1. A 59-year-old male is admitted complaining of chest pain and dyspnea. ST elevation and T-wave inversion were seen on the ECG in V2, V3, and V4. IV thrombolytic
DAY1_CARDIOVASCULAR PRACTICE QUESTIONS 1 P age 1. A 59-year-old male is admitted complaining of chest pain and dyspnea. ST elevation and T-wave inversion were seen on the ECG in V2, V3, and V4. IV thrombolytic
Relax and Learn At the Farm 2012
 Relax and Learn At the Farm Session 9: Invasive Hemodynamic Assessment and What to Do with the Data Carol Jacobson RN, MN Cardiovascular Nursing Education Associates Function of CV system is to deliver
Relax and Learn At the Farm Session 9: Invasive Hemodynamic Assessment and What to Do with the Data Carol Jacobson RN, MN Cardiovascular Nursing Education Associates Function of CV system is to deliver
Cardiogenic shock: Current management
 Cardiogenic shock: Current management Janine Pöss Universitätsklinikum des Saarlandes Klinik für Innere Medizin III Kardiologie, Angiologie und internistische Intensivmedizin Homburg/Saar I have nothing
Cardiogenic shock: Current management Janine Pöss Universitätsklinikum des Saarlandes Klinik für Innere Medizin III Kardiologie, Angiologie und internistische Intensivmedizin Homburg/Saar I have nothing
Bridging With Percutaneous Devices: Tandem Heart and Impella
 Bridging With Percutaneous Devices: Tandem Heart and Impella DAVID A. BARAN, MD, FACC, FSCAI SYSTEM DIRECTOR, ADVANCED HEART FAILURE, TX AND MCS SENTARA HEART HOSPITAL NORFOLK, VA PROFESSOR OF MEDICINE
Bridging With Percutaneous Devices: Tandem Heart and Impella DAVID A. BARAN, MD, FACC, FSCAI SYSTEM DIRECTOR, ADVANCED HEART FAILURE, TX AND MCS SENTARA HEART HOSPITAL NORFOLK, VA PROFESSOR OF MEDICINE
Heart Failure Dr ahmed almutairi Assistant professor internal medicin dept
 Heart Failure Dr ahmed almutairi Assistant professor internal medicin dept (MBBS)(SBMD) Introduction Epidemiology Pathophysiology diastolic/systolic Risk factors Signs and symptoms Classification of HF
Heart Failure Dr ahmed almutairi Assistant professor internal medicin dept (MBBS)(SBMD) Introduction Epidemiology Pathophysiology diastolic/systolic Risk factors Signs and symptoms Classification of HF
AATS/Cardiothoracic Critical Care Symposium
 AATS/Cardiothoracic Critical Care Symposium Balancing Pharmacologic and Mechanical Support Robert L Kormos MD, FACS, FRCS(C), FAHA I have no disclosures and will not discuss off label use of drugs or devices
AATS/Cardiothoracic Critical Care Symposium Balancing Pharmacologic and Mechanical Support Robert L Kormos MD, FACS, FRCS(C), FAHA I have no disclosures and will not discuss off label use of drugs or devices
Myocardial Infarction: Left Ventricular Failure
 CARDIOVASCULAR PHYSIOLOGY 93 Case 17 Myocardial Infarction: Left Ventricular Failure Marvin Zimmerman is a 52-year-old construction manager who is significantly overweight. Despite his physician's repeated
CARDIOVASCULAR PHYSIOLOGY 93 Case 17 Myocardial Infarction: Left Ventricular Failure Marvin Zimmerman is a 52-year-old construction manager who is significantly overweight. Despite his physician's repeated
Extra Corporeal Life Support for Acute Heart failure
 Extra Corporeal Life Support for Acute Heart failure Benjamin Medalion, MD Director Heart and Lung Transplantation Department of Cardiothoracic Surgery Rabin Medical Center, Beilinson Campus, Israel Mechanical
Extra Corporeal Life Support for Acute Heart failure Benjamin Medalion, MD Director Heart and Lung Transplantation Department of Cardiothoracic Surgery Rabin Medical Center, Beilinson Campus, Israel Mechanical
Copyright 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc. Normal Cardiac Anatomy
 Mosby,, an affiliate of Elsevier Normal Cardiac Anatomy Impaired cardiac pumping Results in vasoconstriction & fluid retention Characterized by ventricular dysfunction, reduced exercise tolerance, diminished
Mosby,, an affiliate of Elsevier Normal Cardiac Anatomy Impaired cardiac pumping Results in vasoconstriction & fluid retention Characterized by ventricular dysfunction, reduced exercise tolerance, diminished
Echo assessment of patients with an ECMO device
 Echo assessment of patients with an ECMO device Evangelos Leontiadis Cardiologist 1st Cardiology Dept. Onassis Cardiac Surgery Center Athens, Greece Gibbon HLM 1953 Goldstein DJ et al, NEJM 1998; 339:1522
Echo assessment of patients with an ECMO device Evangelos Leontiadis Cardiologist 1st Cardiology Dept. Onassis Cardiac Surgery Center Athens, Greece Gibbon HLM 1953 Goldstein DJ et al, NEJM 1998; 339:1522
Intravenous Inotropic Support an Overview
 Intravenous Inotropic Support an Overview Shaul Atar, MD Western Galilee Medical Center, Nahariya Affiliated with the Faculty of Medicine of the Galilee, Safed, Israel INOTROPES in Acute HF (not vasopressors)
Intravenous Inotropic Support an Overview Shaul Atar, MD Western Galilee Medical Center, Nahariya Affiliated with the Faculty of Medicine of the Galilee, Safed, Israel INOTROPES in Acute HF (not vasopressors)
Mechanical Circulatory Support (MCS): What Every Pharmacist Needs to Know!
: What Every Pharmacist Needs to Know!") Mechanical Circulatory Support (MCS): What Every Pharmacist Needs to Know! Matthew A. Wanat, PharmD, BCPS, BCCCP, FCCM Clinical Assistant Professor University of Houston College of Pharmacy Clinical Pharmacy
Mechanical Circulatory Support (MCS): What Every Pharmacist Needs to Know! Matthew A. Wanat, PharmD, BCPS, BCCCP, FCCM Clinical Assistant Professor University of Houston College of Pharmacy Clinical Pharmacy
CARDIOGENIC SHOCK. Antonio Pesenti. Università degli Studi di Milano Bicocca Azienda Ospedaliera San Gerardo Monza (MI)
") CARDIOGENIC SHOCK Antonio Pesenti Università degli Studi di Milano Bicocca Azienda Ospedaliera San Gerardo Monza (MI) Primary myocardial dysfunction resulting in the inability of the heart to mantain an
CARDIOGENIC SHOCK Antonio Pesenti Università degli Studi di Milano Bicocca Azienda Ospedaliera San Gerardo Monza (MI) Primary myocardial dysfunction resulting in the inability of the heart to mantain an
Chapter 10. Learning Objectives. Learning Objectives 9/11/2012. Congestive Heart Failure
 Chapter 10 Congestive Heart Failure Learning Objectives Explain concept of polypharmacy in treatment of congestive heart failure Explain function of diuretics Learning Objectives Discuss drugs used for
Chapter 10 Congestive Heart Failure Learning Objectives Explain concept of polypharmacy in treatment of congestive heart failure Explain function of diuretics Learning Objectives Discuss drugs used for
Recognizing the Need to Support A Failing Right Ventricular Role of Mechanical Support
 Recognizing the Need to Support A Failing Right Ventricular Role of Mechanical Support Mahir Elder, MD, FACC,SCAI Medical Direct of PERT program Medical Director of Endovascular medicine Clinical Professor
Recognizing the Need to Support A Failing Right Ventricular Role of Mechanical Support Mahir Elder, MD, FACC,SCAI Medical Direct of PERT program Medical Director of Endovascular medicine Clinical Professor
Cardiogenic Shock Protocol
 Cardiogenic Shock Protocol Impella Devices Best Practices in AMI Cardiogenic Shock Identify 1-3 SBP < 90 mmhg or on inotropes /pressors Cold, clammy, tachycardia Lactate elevated > 2 mmoi /L Stabilize
Cardiogenic Shock Protocol Impella Devices Best Practices in AMI Cardiogenic Shock Identify 1-3 SBP < 90 mmhg or on inotropes /pressors Cold, clammy, tachycardia Lactate elevated > 2 mmoi /L Stabilize
CVICU EXAM. Mrs. Jennings is a 71-year-old post-op CABG x5 with an IABP in her left femoral artery
 CVICU EXAM 1111 North 3rd Street Mrs. Jennings is a 71-year-old post-op CABG x5 with an IABP in her left femoral artery 1. Nursing standards for a patient on an IABP device include: a. Know results of
CVICU EXAM 1111 North 3rd Street Mrs. Jennings is a 71-year-old post-op CABG x5 with an IABP in her left femoral artery 1. Nursing standards for a patient on an IABP device include: a. Know results of
Circulatory Support: From IABP to LVAD
 Circulatory Support: From IABP to LVAD Howard A Cohen, MD, FACC, FSCAI Director Division of Cardiovascular Intervention Co Director Cardiovascular Interventional ti Laboratories Lenox Hill Heart & Vascular
Circulatory Support: From IABP to LVAD Howard A Cohen, MD, FACC, FSCAI Director Division of Cardiovascular Intervention Co Director Cardiovascular Interventional ti Laboratories Lenox Hill Heart & Vascular
A case of post myocardial infarction ventricular septal rupture CHRISTOFOROS KOBOROZOS, MD
 A case of post myocardial infarction ventricular septal rupture CHRISTOFOROS KOBOROZOS, MD NAVAL HOSPITAL OF ATHENS case presentation Female, 81yo Hx: diabetes mellitus, hypertension, chronic anaemia presented
A case of post myocardial infarction ventricular septal rupture CHRISTOFOROS KOBOROZOS, MD NAVAL HOSPITAL OF ATHENS case presentation Female, 81yo Hx: diabetes mellitus, hypertension, chronic anaemia presented
Assist Devices in STEMI- Intra-aortic Balloon Pump
 Assist Devices in STEMI- Intra-aortic Balloon Pump Ioannis Iakovou, MD, PhD Onassis Cardiac Surgery Center Athens, Greece Cardiogenic shock 5-10% of pts after a heart attack 60000-70000 pts in Europe/year
Assist Devices in STEMI- Intra-aortic Balloon Pump Ioannis Iakovou, MD, PhD Onassis Cardiac Surgery Center Athens, Greece Cardiogenic shock 5-10% of pts after a heart attack 60000-70000 pts in Europe/year
Cardiovascular Practice Quiz
 Cardiovascular Practice Quiz 1. When caring for a patient following a cardiac catheterization with coronary angiography, which of the following findings would be of most concern to the nurse? a. Swelling
Cardiovascular Practice Quiz 1. When caring for a patient following a cardiac catheterization with coronary angiography, which of the following findings would be of most concern to the nurse? a. Swelling
Case year old female nursing home resident with a hx CAD, PUD, recent hip fracture Transferred to ED with decreased mental status BP in ED 80/50
 Case 1 65 year old female nursing home resident with a hx CAD, PUD, recent hip fracture Transferred to ED with decreased mental status BP in ED 80/50 Case 1 65 year old female nursing home resident with
Case 1 65 year old female nursing home resident with a hx CAD, PUD, recent hip fracture Transferred to ED with decreased mental status BP in ED 80/50 Case 1 65 year old female nursing home resident with
Right Ventricular Failure: Prediction, Prevention and Treatment
 Right Ventricular Failure: Prediction, Prevention and Treatment 3 rd European Training Symposium for Heart Failure Cardiologists and Cardiac Surgeons University Hospital Bern June 24-25, 2016 Disclosures:
Right Ventricular Failure: Prediction, Prevention and Treatment 3 rd European Training Symposium for Heart Failure Cardiologists and Cardiac Surgeons University Hospital Bern June 24-25, 2016 Disclosures:
Acute Mechanical Circulatory Support Right Ventricular Support Devices
 Acute Mechanical Circulatory Support Right Ventricular Support Devices Navin K. Kapur, MD, FACC, FSCAI, FAHA Associate Professor, Department of Medicine Interventional Cardiology & Advanced Heart Failure
Acute Mechanical Circulatory Support Right Ventricular Support Devices Navin K. Kapur, MD, FACC, FSCAI, FAHA Associate Professor, Department of Medicine Interventional Cardiology & Advanced Heart Failure
Definition. Low-cardiac-output state resulting in life threatening end-organ hypoperfusion. Criteria: MAP 30 mm Hg lower than baseline)
") Definition Low-cardiac-output state resulting in life threatening end-organ hypoperfusion Criteria: 1. Persistent hypotension (SBP
Definition Low-cardiac-output state resulting in life threatening end-organ hypoperfusion Criteria: 1. Persistent hypotension (SBP
Cardiogenic Shock. Carlos Cafri,, MD
 Cardiogenic Shock Carlos Cafri,, MD SHOCK= Inadequate Tissue Mechanisms: Perfusion Inadequate oxygen delivery Release of inflammatory mediators Further microvascular changes, compromised blood flow and
Cardiogenic Shock Carlos Cafri,, MD SHOCK= Inadequate Tissue Mechanisms: Perfusion Inadequate oxygen delivery Release of inflammatory mediators Further microvascular changes, compromised blood flow and
Intraaortic Balloon Counterpulsation- Supportive Data for a Role in Cardiogenic Shock ( Be Still My Friend )
") Intraaortic Balloon Counterpulsation- Supportive Data for a Role in Cardiogenic Shock ( Be Still My Friend ) Stephen G. Ellis, MD Section Head, Interventional Cardiology Professor of Medicine Cleveland
Intraaortic Balloon Counterpulsation- Supportive Data for a Role in Cardiogenic Shock ( Be Still My Friend ) Stephen G. Ellis, MD Section Head, Interventional Cardiology Professor of Medicine Cleveland
8th Emirates Cardiac Society Congress in collaboration with ACC Middle East Conference Dubai: October Acute Coronary Syndromes
 8th Emirates Cardiac Society Congress in collaboration with ACC Middle East Conference 2017 OSPEDALE Dubai: 19-21 October 2017 Acute Coronary Syndromes Antonio Colombo Centro Cuore Columbus and S. Raffaele
8th Emirates Cardiac Society Congress in collaboration with ACC Middle East Conference 2017 OSPEDALE Dubai: 19-21 October 2017 Acute Coronary Syndromes Antonio Colombo Centro Cuore Columbus and S. Raffaele
Planned, Short-Term RVAD During Durable LVAD Implant: Indications and Management
 Planned, Short-Term RVAD During Durable LVAD Implant: Indications and Management Yoshifumi Naka, MD, PhD Columbia University Medical Center New York, NY Disclosure Abbott/St. Jude Med./Thoratec Consultant
Planned, Short-Term RVAD During Durable LVAD Implant: Indications and Management Yoshifumi Naka, MD, PhD Columbia University Medical Center New York, NY Disclosure Abbott/St. Jude Med./Thoratec Consultant
Impedance Cardiography (ICG) Application of ICG in Intensive Care and Emergency
 Application of ICG in Intensive Care and Emergency") Impedance Cardiography (ICG) Application of ICG in Intensive Care and Emergency Aim of haemodynamic monitoring in ICU and ED Detection and therapy of insufficient organ perfusion Answers to common cardiovascular
Impedance Cardiography (ICG) Application of ICG in Intensive Care and Emergency Aim of haemodynamic monitoring in ICU and ED Detection and therapy of insufficient organ perfusion Answers to common cardiovascular
Useful diagnostic measures: chest x ray to check pulmonary edema, ECG and ECHO to detect cardiac abnormalities (1).
.") Cardiogenic shock Etiology The most common cause of cardiogenic shock is LV dysfunction and necrosis as a result of acute myocardial infarction (AMI) (1). Acute valvular insufficiency or stenosis prevents
Cardiogenic shock Etiology The most common cause of cardiogenic shock is LV dysfunction and necrosis as a result of acute myocardial infarction (AMI) (1). Acute valvular insufficiency or stenosis prevents
FUNDAMENTALS OF HEMODYNAMICS, VASOACTIVE DRUGS AND IABP IN THE FAILING HEART
 FUNDAMENTALS OF HEMODYNAMICS, VASOACTIVE DRUGS AND IABP IN THE FAILING HEART CINDY BITHER, MSN, ANP, ANP, AACC, CHFN CHIEF NP, ADV HF PROGRAM MEDSTAR WASHINGTON HOSPITAL CENTER CONFLICTS OF INTEREST NONE
FUNDAMENTALS OF HEMODYNAMICS, VASOACTIVE DRUGS AND IABP IN THE FAILING HEART CINDY BITHER, MSN, ANP, ANP, AACC, CHFN CHIEF NP, ADV HF PROGRAM MEDSTAR WASHINGTON HOSPITAL CENTER CONFLICTS OF INTEREST NONE
ACUTE HEART FAILURE. Julie Gorchynski MD, MSc, FACEP, FAAEM. Department of Emergency Medicine Emergency Residency Program UTHSC, San Antonio TCEP 2014
 ACUTE HEART FAILURE Julie Gorchynski MD, MSc, FACEP, FAAEM Department of Emergency Medicine Emergency Residency Program UTHSC, San Antonio TCEP 2014 No disclosures Objectives Overview Cases Current Therapy
ACUTE HEART FAILURE Julie Gorchynski MD, MSc, FACEP, FAAEM Department of Emergency Medicine Emergency Residency Program UTHSC, San Antonio TCEP 2014 No disclosures Objectives Overview Cases Current Therapy
Rationale for Prophylactic Support During Percutaneous Coronary Intervention
 Rationale for Prophylactic Support During Percutaneous Coronary Intervention Navin K. Kapur, MD, FACC, FSCAI Assistant Director, Interventional Cardiology Director, Interventional Research Laboratories
Rationale for Prophylactic Support During Percutaneous Coronary Intervention Navin K. Kapur, MD, FACC, FSCAI Assistant Director, Interventional Cardiology Director, Interventional Research Laboratories
Impedance Cardiography (ICG) Method, Technology and Validity
 Method, Technology and Validity") Method, Technology and Validity Hemodynamic Basics Cardiovascular System Cardiac Output (CO) Mean arterial pressure (MAP) Variable resistance (SVR) Aortic valve Left ventricle Elastic arteries / Aorta
Method, Technology and Validity Hemodynamic Basics Cardiovascular System Cardiac Output (CO) Mean arterial pressure (MAP) Variable resistance (SVR) Aortic valve Left ventricle Elastic arteries / Aorta
Ray Matthews MD Professor of Clinical Medicine Chief of Cardiology University of Southern California
 High Risk PCI Making Possible the Impossible Ray Matthews MD Professor of Clinical Medicine Chief of Cardiology University of Southern California Disclosures Abiomed Research Support Consulting Agreement
High Risk PCI Making Possible the Impossible Ray Matthews MD Professor of Clinical Medicine Chief of Cardiology University of Southern California Disclosures Abiomed Research Support Consulting Agreement
Nothing to Disclose. Severe Pulmonary Hypertension
 Severe Ronald Pearl, MD, PhD Professor and Chair Department of Anesthesiology Stanford University Rpearl@stanford.edu Nothing to Disclose 65 year old female Elective knee surgery NYHA Class 3 Aortic stenosis
Severe Ronald Pearl, MD, PhD Professor and Chair Department of Anesthesiology Stanford University Rpearl@stanford.edu Nothing to Disclose 65 year old female Elective knee surgery NYHA Class 3 Aortic stenosis
Images have been removed from the PowerPoint slides in this handout due to copyright restrictions.
 Percutaneous Coronary Intervention https://www.youtube.com/watch?v=bssqnhylvma Types of PCI Procedures Balloon Angioplasty Rotational Atherectomy Coronary Stent Balloon Inflation Rotational Atherectomy
Percutaneous Coronary Intervention https://www.youtube.com/watch?v=bssqnhylvma Types of PCI Procedures Balloon Angioplasty Rotational Atherectomy Coronary Stent Balloon Inflation Rotational Atherectomy
Hemodynamic improvement upon levosimendan treatment in low cardiac output patients following coronary artery bypass graft
 Hemodynamic improvement upon levosimendan treatment in low cardiac output patients following coronary artery bypass graft M. Buerke, K. Krohe, M. Russ, C. Schneider, H. Lemm, R. Prondzinsky, I. Friedrich,
Hemodynamic improvement upon levosimendan treatment in low cardiac output patients following coronary artery bypass graft M. Buerke, K. Krohe, M. Russ, C. Schneider, H. Lemm, R. Prondzinsky, I. Friedrich,
Medical Management of Acutely Decompensated Heart Failure. William T. Abraham, MD Director, Division of Cardiovascular Medicine
 Medical Management of Acutely Decompensated Heart Failure William T. Abraham, MD Director, Division of Cardiovascular Medicine Orlando, Florida October 7-9, 2011 Goals of Acute Heart Failure Therapy Alleviate
Medical Management of Acutely Decompensated Heart Failure William T. Abraham, MD Director, Division of Cardiovascular Medicine Orlando, Florida October 7-9, 2011 Goals of Acute Heart Failure Therapy Alleviate
Index of subjects. effect on ventricular tachycardia 30 treatment with 101, 116 boosterpump 80 Brockenbrough phenomenon 55, 125
 145 Index of subjects A accessory pathways 3 amiodarone 4, 5, 6, 23, 30, 97, 102 angina pectoris 4, 24, 1l0, 137, 139, 140 angulation, of cavity 73, 74 aorta aortic flow velocity 2 aortic insufficiency
145 Index of subjects A accessory pathways 3 amiodarone 4, 5, 6, 23, 30, 97, 102 angina pectoris 4, 24, 1l0, 137, 139, 140 angulation, of cavity 73, 74 aorta aortic flow velocity 2 aortic insufficiency
Section 6 Intra Aortic Balloon Pump
 Section 6 Intra Aortic Balloon Pump The Intra Aortic Balloon Pump (IABP) The balloon is synthetic and is made for single use only. It is threaded into the aorta, usually via a femoral approach. The balloon
Section 6 Intra Aortic Balloon Pump The Intra Aortic Balloon Pump (IABP) The balloon is synthetic and is made for single use only. It is threaded into the aorta, usually via a femoral approach. The balloon
The Pharmacology of Hypotension: Vasopressor Choices for HIE patients. Keliana O Mara, PharmD August 4, 2018
 The Pharmacology of Hypotension: Vasopressor Choices for HIE patients Keliana O Mara, PharmD August 4, 2018 Objectives Review the pathophysiology of hypotension in neonates Discuss the role of vasopressors
The Pharmacology of Hypotension: Vasopressor Choices for HIE patients Keliana O Mara, PharmD August 4, 2018 Objectives Review the pathophysiology of hypotension in neonates Discuss the role of vasopressors
Titrating Critical Care Medications
 Titrating Critical Care Medications Chad Johnson, MSN (NED), RN, CNCC(C), CNS-cc Clinical Nurse Specialist: Critical Care and Neurosurgical Services E-mail: johnsoc@tbh.net Copyright 2017 1 Learning Objectives
Titrating Critical Care Medications Chad Johnson, MSN (NED), RN, CNCC(C), CNS-cc Clinical Nurse Specialist: Critical Care and Neurosurgical Services E-mail: johnsoc@tbh.net Copyright 2017 1 Learning Objectives
Index. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A Acute coronary syndrome(s), anticoagulant therapy in, 706, 707 antiplatelet therapy in, 702 ß-blockers in, 703 cardiac biomarkers in,
Index Note: Page numbers of article titles are in boldface type. A Acute coronary syndrome(s), anticoagulant therapy in, 706, 707 antiplatelet therapy in, 702 ß-blockers in, 703 cardiac biomarkers in,
MANAGEMENT OF CARDIOGENIC SHOCK
 MANAGEMENT OF CARDIOGENIC SHOCK CASE PRESENTATION 37 year old Dutch female No known coronary artery disease risk factors 1 week post partum at time of presentation (G3P3) after an uncomplicated normal
MANAGEMENT OF CARDIOGENIC SHOCK CASE PRESENTATION 37 year old Dutch female No known coronary artery disease risk factors 1 week post partum at time of presentation (G3P3) after an uncomplicated normal
TOPIC : Cardiogenic Shock
 University of Ferrara Department of Morphology, Surgery and Experimental Medicine. Section of Anaesthesia and Intensive Care Medicine TOPIC : Cardiogenic Shock What is shock? Shock is a condition of inadequate
University of Ferrara Department of Morphology, Surgery and Experimental Medicine. Section of Anaesthesia and Intensive Care Medicine TOPIC : Cardiogenic Shock What is shock? Shock is a condition of inadequate
How to do Primary Angioplasty. - Patients with Cardiogenic Shock
 How to do Primary Angioplasty - Patients with Cardiogenic Shock Advanced Cardiovascular Intervention 2011 Dan Blackman Leeds General Infirmary MY CONFLICTS OF INTEREST ARE: Research Grants Medicines Company
How to do Primary Angioplasty - Patients with Cardiogenic Shock Advanced Cardiovascular Intervention 2011 Dan Blackman Leeds General Infirmary MY CONFLICTS OF INTEREST ARE: Research Grants Medicines Company
Shock Quiz! By Clare Di Bona
 Shock Quiz! By Clare Di Bona Test Question What is Mr Burns full legal name? Answer Charles Montgomery Plantagenet Schicklgruber Burns. (Season 22, episode 11) Question 1. What is the definition of shock?
Shock Quiz! By Clare Di Bona Test Question What is Mr Burns full legal name? Answer Charles Montgomery Plantagenet Schicklgruber Burns. (Season 22, episode 11) Question 1. What is the definition of shock?
HOW LOW CAN YOU GO? HYPOTENSION AND THE ANESTHETIZED PATIENT.
 HOW LOW CAN YOU GO? HYPOTENSION AND THE ANESTHETIZED PATIENT. Donna M. Sisak, CVT, LVT, VTS (Anesthesia/Analgesia) Seattle Veterinary Specialists Kirkland, WA dsisak@svsvet.com THE ANESTHETIZED PATIENT
HOW LOW CAN YOU GO? HYPOTENSION AND THE ANESTHETIZED PATIENT. Donna M. Sisak, CVT, LVT, VTS (Anesthesia/Analgesia) Seattle Veterinary Specialists Kirkland, WA dsisak@svsvet.com THE ANESTHETIZED PATIENT
CASE DISCUSSION. Dr JAYASREE VEERABOINA 2nd yr PG MS OBG
 CASE DISCUSSION Dr JAYASREE VEERABOINA 2nd yr PG MS OBG Normal Cardiovascular changes in Pregnancy CARDIAC OUTPUT 5 th wk -- starts 12 wks -- 30-35% 30-32 wks -- 40% During labour -- 50% After delivery
CASE DISCUSSION Dr JAYASREE VEERABOINA 2nd yr PG MS OBG Normal Cardiovascular changes in Pregnancy CARDIAC OUTPUT 5 th wk -- starts 12 wks -- 30-35% 30-32 wks -- 40% During labour -- 50% After delivery
Heart Failure. Cardiac Anatomy. Functions of the Heart. Cardiac Cycle/Hemodynamics. Determinants of Cardiac Output. Cardiac Output
 Cardiac Anatomy Heart Failure Professor Qing ZHANG Department of Cardiology, West China Hospital www.blaufuss.org Cardiac Cycle/Hemodynamics Functions of the Heart Essential functions of the heart to cover
Cardiac Anatomy Heart Failure Professor Qing ZHANG Department of Cardiology, West China Hospital www.blaufuss.org Cardiac Cycle/Hemodynamics Functions of the Heart Essential functions of the heart to cover
CENTRAL ECMO WHEN AND HOW? RANJIT JOHN, MD UNIVERSITY OF MINESOTA
 CENTRAL ECMO WHEN AND HOW? RANJIT JOHN, MD UNIVERSITY OF MINESOTA Background How to do Case reports When to do Managing complications Post operative management strategies CASE PRESENTATION 46 year old
CENTRAL ECMO WHEN AND HOW? RANJIT JOHN, MD UNIVERSITY OF MINESOTA Background How to do Case reports When to do Managing complications Post operative management strategies CASE PRESENTATION 46 year old
Admission of patient CVICU and hemodynamic monitoring
 Admission of patient CVICU and hemodynamic monitoring Prepared by: Rami AL-Khatib King Fahad Medical City Pi Prince Salman Heart tcentre CVICU-RN Admission patient to CVICU Introduction All the patients
Admission of patient CVICU and hemodynamic monitoring Prepared by: Rami AL-Khatib King Fahad Medical City Pi Prince Salman Heart tcentre CVICU-RN Admission patient to CVICU Introduction All the patients
Intravenous Infusions
 Intravenous Infusions 1) An IV insulin infusion can be used for patients: a) with out of control diabetes b) with DKA (Diabetic Ketoacidosis) c) after a heart attack 2) Hyperglycemia is an adaptive response
Intravenous Infusions 1) An IV insulin infusion can be used for patients: a) with out of control diabetes b) with DKA (Diabetic Ketoacidosis) c) after a heart attack 2) Hyperglycemia is an adaptive response
Keynote Address II Managing Acute Heart Failure: What Can We Do to Improve Outcomes?
 Keynote Address II Managing Acute Heart Failure: What Can We Do to Improve Outcomes? 24 th Annual San Diego Heart Failure Symposium June 1-2, 2018 La Jolla, CA Barry Greenberg, MD Distinguished Professor
Keynote Address II Managing Acute Heart Failure: What Can We Do to Improve Outcomes? 24 th Annual San Diego Heart Failure Symposium June 1-2, 2018 La Jolla, CA Barry Greenberg, MD Distinguished Professor
Shock and Vasopressors. Nina E. Glass, MD TACS Fellow SICU Didactic Curriculum 9/24/14
 Shock and Vasopressors Nina E. Glass, MD TACS Fellow SICU Didactic Curriculum 9/24/14 Review Question Unilaterally diminished breath sounds A. Figure 1 B. Figure 2 C. Both D. Neither Related Specialties
Shock and Vasopressors Nina E. Glass, MD TACS Fellow SICU Didactic Curriculum 9/24/14 Review Question Unilaterally diminished breath sounds A. Figure 1 B. Figure 2 C. Both D. Neither Related Specialties
Cardiogenic Shock in Acute MI
 Cardiogenic Shock in Acute MI Mark Sheldon, MD UNMH Interventional Cardiology Objectives Overview Treatment Definition Shock profiles Causes Medical Mechanical Illustrative case Questions? Revascularization
Cardiogenic Shock in Acute MI Mark Sheldon, MD UNMH Interventional Cardiology Objectives Overview Treatment Definition Shock profiles Causes Medical Mechanical Illustrative case Questions? Revascularization
Drs. Rottman, Salloum, Campbell, Muldowney, Hong, Bagai, Kronenberg
 Rotation: or: Faculty: Coronary Care Unit (CVICU) Dr. Jeff Rottman Drs. Rottman, Salloum, Campbell, Muldowney, Hong, Bagai, Kronenberg Duty Hours: Mon Fri, 7 AM to 7 PM, weekend call shared with consult
Rotation: or: Faculty: Coronary Care Unit (CVICU) Dr. Jeff Rottman Drs. Rottman, Salloum, Campbell, Muldowney, Hong, Bagai, Kronenberg Duty Hours: Mon Fri, 7 AM to 7 PM, weekend call shared with consult
Ventricular Assisting Devices in the Cathlab. Unrestricted
 Ventricular Assisting Devices in the Cathlab Unrestricted What is a VAD? A single system device that is surgically attached to the left ventricle of the heart and to the aorta for left ventricular support
Ventricular Assisting Devices in the Cathlab Unrestricted What is a VAD? A single system device that is surgically attached to the left ventricle of the heart and to the aorta for left ventricular support
To ECMO Or Not To ECMO Challenges of venous arterial ECMO. Dr Emily Granger St Vincent s Hospital Darlinghurst NSW
 To ECMO Or Not To ECMO Challenges of venous arterial ECMO Dr Emily Granger St Vincent s Hospital Darlinghurst NSW The Start: 1972 St Vincent s Hospital The Turning Point ECMO program restarted in 2004
To ECMO Or Not To ECMO Challenges of venous arterial ECMO Dr Emily Granger St Vincent s Hospital Darlinghurst NSW The Start: 1972 St Vincent s Hospital The Turning Point ECMO program restarted in 2004
Index. K Knobology, TTE artifact, image resolution, ultrasound, 14
 A Acute aortic regurgitation (AR), 124 128 Acute aortic syndrome (AAS) classic aortic dissection diagnosis, 251 263 evolutive patterns, 253 255 pathology, 250 251 classifications, 247 248 incomplete aortic
A Acute aortic regurgitation (AR), 124 128 Acute aortic syndrome (AAS) classic aortic dissection diagnosis, 251 263 evolutive patterns, 253 255 pathology, 250 251 classifications, 247 248 incomplete aortic
Cardiovascular Nursing Practice: A Comprehensive Resource Manual and Study Guide for Clinical Nurses 2 nd Edition
 Cardiovascular Nursing Practice: A Comprehensive Resource Manual and Study Guide for Clinical Nurses 2 nd Edition Table of Contents Volume 1 Chapter 1: Cardiovascular Anatomy and Physiology Basic Cardiac
Cardiovascular Nursing Practice: A Comprehensive Resource Manual and Study Guide for Clinical Nurses 2 nd Edition Table of Contents Volume 1 Chapter 1: Cardiovascular Anatomy and Physiology Basic Cardiac
Introduction to Acute Mechanical Circulatory Support
 Introduction to Acute Mechanical Circulatory Support Navin K. Kapur, MD, FACC, FSCAI, FAHA Associate Professor, Department of Medicine Interventional Cardiology & Advanced Heart Failure Programs Executive
Introduction to Acute Mechanical Circulatory Support Navin K. Kapur, MD, FACC, FSCAI, FAHA Associate Professor, Department of Medicine Interventional Cardiology & Advanced Heart Failure Programs Executive
Taking the shock factor out of shock
 Taking the shock factor out of shock Julie Antonellis, BS, LVT, VTS (ECC) Northern Virginia Regional Director for the VALVT Technician Supervisor VCA Animal Emergency Critical Care Business owner Antonellis
Taking the shock factor out of shock Julie Antonellis, BS, LVT, VTS (ECC) Northern Virginia Regional Director for the VALVT Technician Supervisor VCA Animal Emergency Critical Care Business owner Antonellis
Technique. Technique. Technique. Monitoring 1. Local anesthetic? Aseptic technique Hyper-extend (if radial)
") Critical Care Monitoring Hemodynamic Monitoring Arterial Blood Pressure Cannulate artery Uses 2 Technique Sites Locate artery, prep 3 1 Technique Local anesthetic? Aseptic technique Hyper-extend (if radial)
Critical Care Monitoring Hemodynamic Monitoring Arterial Blood Pressure Cannulate artery Uses 2 Technique Sites Locate artery, prep 3 1 Technique Local anesthetic? Aseptic technique Hyper-extend (if radial)
DECLARATION OF CONFLICT OF INTEREST
 DECLARATION OF CONFLICT OF INTEREST Cardiogenic Shock Mechanical Support Eulàlia Roig FESC Heart Failure and HT Unit Hospital Sant Pau - UAB Barcelona. Spain No conflics of interest Mechanical Circulatory
DECLARATION OF CONFLICT OF INTEREST Cardiogenic Shock Mechanical Support Eulàlia Roig FESC Heart Failure and HT Unit Hospital Sant Pau - UAB Barcelona. Spain No conflics of interest Mechanical Circulatory
Case - Advanced HF and Shock (INTERMACS 1)
") Case - Advanced HF and Shock (INTERMACS 1) Navin K. Kapur, MD, FACC, FSCAI, FAHA Associate Professor, Department of Medicine Interventional Cardiology & Advanced Heart Failure Programs Executive Director,
Case - Advanced HF and Shock (INTERMACS 1) Navin K. Kapur, MD, FACC, FSCAI, FAHA Associate Professor, Department of Medicine Interventional Cardiology & Advanced Heart Failure Programs Executive Director,
Pheochromocytoma Crisis Presenting as Fulminant Cardiopulmonary Failure: A Case Report
 170 Pheochromocytoma Crisis Presenting as Fulminant Cardiopulmonary Failure: A Case Report Chun-Wen Chiu 1, Cheng-Hsiung Chen 2 Fulminant cardiopulmonary failure in a patient with pheochromocytoma is a
170 Pheochromocytoma Crisis Presenting as Fulminant Cardiopulmonary Failure: A Case Report Chun-Wen Chiu 1, Cheng-Hsiung Chen 2 Fulminant cardiopulmonary failure in a patient with pheochromocytoma is a