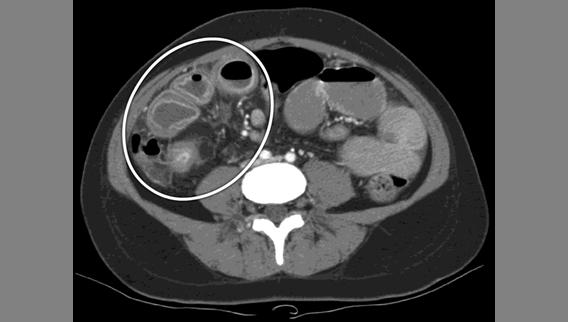
Inflammatory Bowel Disease RTC 10/30/09
|
|
|
- Ashlee Williams
- 5 years ago
- Views:
Transcription
1 Inflammatory Bowel Disease RTC 10/30/09

2 October 30, nd President of the United States, John Adams, was born. Prior to becoming president he served 2 terms as Vice President under George Washington. If we do not lay out ourselves in the service of mankind whom should we serve?
3 Objectives Review of pathology and clinical characteristics of Crohn s disease and Ulcerative Colitis Discuss common medical management strategies Understand surgical evaluation of patients with inflammatory bowel disease Crohn s disease Fulminant Ulcerative Colitis Understand indications for surgical treatment and rationale for specific procedures
4 CROHN S DISEASE ULCERATIVE COLITIS Thickened Wall/Mesentery +4 0 Creeping fat +4 0 Segmental disease +4 0 Transmural +4 0 Granulomas present +3 0 Bleeding per rectum Diarrhea Obstruction Anal/Peri-anal Disease +4 Rare Small Bowel Disease +4 0 Malignancy Risk GROSS MICROSCOPIC CLINICAL FEATURES
5 CROHN S DISEASE ULCERATIVE COLITIS Distribution Discontinuous Continuous Rectal Disease Longitudinal Ulcers +4 0 Aphthous Ulcers +4 0 Cobblestoning +4 0 Friability Pseudopolyps COLONOSCOPIC

6 Ulcerative colitis Fulminant
7 ulcerative colitis Criteria for evaluating severity of UC Variable Mild Disease Severe Disease Fulminant Disease Stools <4/day >6/day >10/day Blood in stool Intermittent Frequent Continuous Temperature Normal >37.5 >37.5 Pulse Normal >90 >90 Hgb Normal <75% normal Transfusion required ESR <30 >30 >30 Xray Features --- Air, edematous wall Dilatation Clinical Signs --- Tenderness Tenderness/Distension
8 Clinical evaluation History and Physical Duration of symptoms, medical therapy, etc. Labwork CBC, electrolytes, nutrition labs Stool for c.difficile, e.coli, CMV Imaging Plain films (abdomen; CXR) CT scan Endoscopy - diagnostic
9 Medical management Induction of remission: Corticosteroids/Cyclosporine I.V. Corticosteroid Therapy Response rate ~50-60% when given over 5-7 days Considered failure if no improvement Symptomatic colitis recurs in ~40-50% of patients Transition to maintenance therapy Purine analogues or immunosalicylates Cyclosporine Used when steroids fail > 50% response rate < 25% recurrence rate with maintenance therapy Renal insufficiency, opportunistic infections, seizures
10 Surgical indications Perforation - peritonitis Often masked by immunosuppression Severe GI hemorrhage Toxic megacolon Septic physiology with colon dilatation Associated with impending perforation Refractory to conservative measures No clinical improvement with corticosteroids or cyclosporine
11 Pre-Op Obtain enterostomal therapist consult Prophylactic antibiotics Anaerobic and Gram (-) coverage Stress steroids IV hydrocortisone
12 Operative Strategies Ultimate goal: Proctocolectomy and ileoanal anastomosis Physiologic state of the patient determines plan Options: 1) Colectomy with Hartmann s pouch or mucous fistula. Delayed proctocolectomy and ileoanal anastomosis 2) Immediate proctocolectomy with ileoanal anastomosis Advantage of 1) Recovery from acute illness Wean from immunosuppressives Maximize nutrition
13 Operative technique Standard Colectomy Wide mesenteric resection unnecessary Hartmann pouch Length is critical proximal end at sacral promontory Preservation of terminal IMA branches Evaluate for disease at planned site of resection Long Hartmann pouch proximal bowel in subq Mucous fistula Requires longer segment of distal colon Increased incidence of bleeding Laparoscopic


14 Fulminant UC

15 October 30, 1953 General George C. Marshall was awarded the Noble Peace Prize. He helped formulate the Marshall Plan for the rebuilding of Western Europe post-wwii and the expulsion of communism. When a thing is done, it s done. Don t look back.


16 Crohn s disease
17 Medical management Medical therapy is first line of defense Exceptions: perforation, obstruction, cancer, dysplasia Re-operation rate ~ 34% at 10 years1 Category Example Probiotics Lactobacillus Antibiotics Metronidazole, Ciprofloxacin Anti-inflammatory Sulfasalazine, 5-ASA s Immunosuppressives Corticosteroids, Cyclosporine Antimetabolites, Methotrexate Biologics Infliximab Michelassi F. Ann Surg 1991
18 Surgical indications No response to medical therapy Intolerance of side effects Prednisone (cataracts, aseptic necrosis, weigh gain) Antimetabolites (pancreatitis, neutropenia, infection) Obstruction Symptomatic fistulas Associated with obstruction/abscess Disabling rectovaginal or enterocutaneous fistulas Ileosigmoid fistula Abscess Not amenable to CT drainage Malignancy relative risk increased x3

19 Operative treatment Esophageal, Gastric, Duodenal Uncommon locations for disease Surgical treatment limited to duodenum Degree of obstruction best assessed w/contrast study Endoscopic diagnosis: noncaseating granulomas Gastrojejunostomy with vagotomy preferred treatment
20 Operative treatment Small bowel (jejunum, ileum) Small bowel associated with highest recurrence Most commonly presents as obstruction Concern for short bowel syndrome Segmental resection Reserved for long areas of stricture Resected segment should be as short as possible Palpate mesenteric margin of bowel Inspect entire bowel!
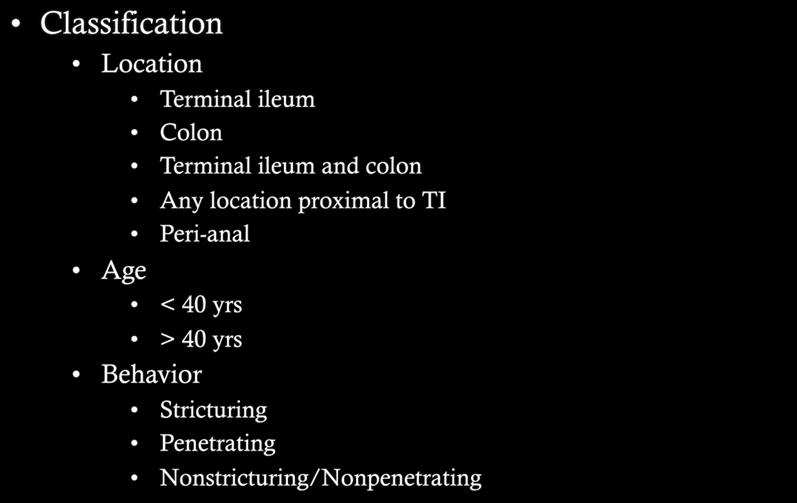
21 Operative treatment Stricturoplasty Useful for short, isolated strictures causing obstruction Saves bowel length 2 major techniques: Heineke Mikulicz (5-7cm) Finney (10-15cm) Rare incidence of adenocarcinoma at stricture site Biopsy active ulcer on mesenteric side Contraindicated in the presence of abscess, phlegmon, or fistula
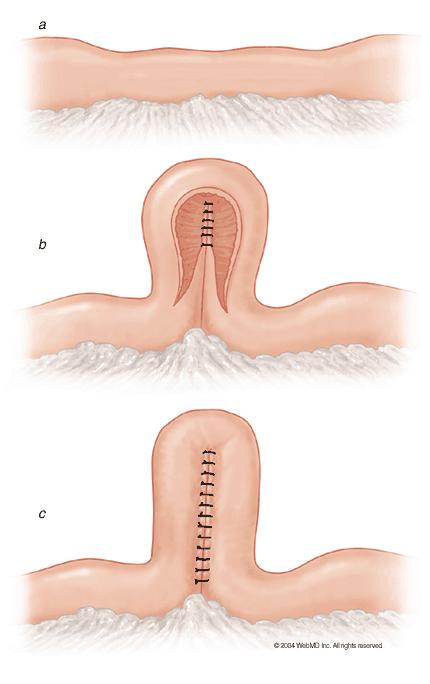
22 Stricturoplasty Heineke-Mikulicz Finney
23 Operative treatment Ileocolic Disease Most common location (~50% Crohn s pts) Resection, End-to-end anastomosis Colonoscopy for post-op surveillance The wider the better Often associated with intra-abdominal abscess/fistula Most common associated fistula is ileosigmoid Externalize anastomosis as loop ileostomy in the presence of abscess Disease recurrence increases with # resections Post-op recurrence Decreased with mesalamine Increased with tobacco use

24 Operative treatment Colonic Disease Present in 30-45% of Crohn s patients Often difficult to distinguish from UC Similar to UC endoscopically and macroscopically Increased frequency of pyoderma gangrenosum

 Toxic megacolon Segmental vs.")
25 Operative treatment Colonic disease Indications for surgical treatment Obstruction/stricture Malignancy Side effects or failure of medical therapy Growth retardation in children (bone age, IGF-1) Toxic megacolon Segmental vs. Pancolonic disease Recurrence risk
26 Operative treatment Operative Procedures Total proctocolectomy with end-ileostomy Traditional treatment for Crohn s colitis Ideal in patients with anal/rectal disease Intersphincteric approach 8-15% recurrence in proximal bowel Subtotal colectomy w/ileorectal or ileosigmoidostomy An option in absence of rectal/anal disease Avoids ostomy 70% recurrence rate Segmental resection Ideal for limited disease with obstructing stricture Some associated controversy

27 Operative treatment Anal Disease With Stenosis from stricture Poor response to medical therapy Ongoing fistulas and suppurative disease Usually extends proximally Ultimate need for fecal diversion Without stenosis Favorable response to medical therapy Protect sphincter is general rule Setons to prevent abscess Rectovaginal fistula
28 Postoperative Post-op chemoprophylaxis Reduces recurrence (~30-40%) Mesalamine 6-mercaptopurine Azathioprine Surveillance No clear guidelines With remaining colon scope every 2 years Risk reduction Tobacco use associated with 1/3 higher recurrence rate Appears to be dose-dependent

29 October 30, 1938 Orson Welles' "The War of the Worlds" aired on CBS radio. Many listeners believed that the radio dramatization was a live news event about a real Martian invasion
30 Questions Which of the following statements about inflammatory conditions of the colon is TRUE? A) The risk of malignancy with pancolonic UC is 1% to 2% per year B) UC is a mucosal disease that is associated with the development of strictures despite medical therapy C) Perianal lesions are relatively common in severe UC, but the rectum is usually spared D) NSAIDS are effective in the treatment of UC E) OCP s are associated with the development of inflammation of the colon that mimics UC histologically.
31 Questions A 45 y/o female with active Crohn s proctitis has a symptomatic anterior transphincteric ano-vaginal fistula. The most appropriate management is: A) a draining seton B) saucerization C) fibrin glue D) a cutting seton E) an endorectal advancement flap
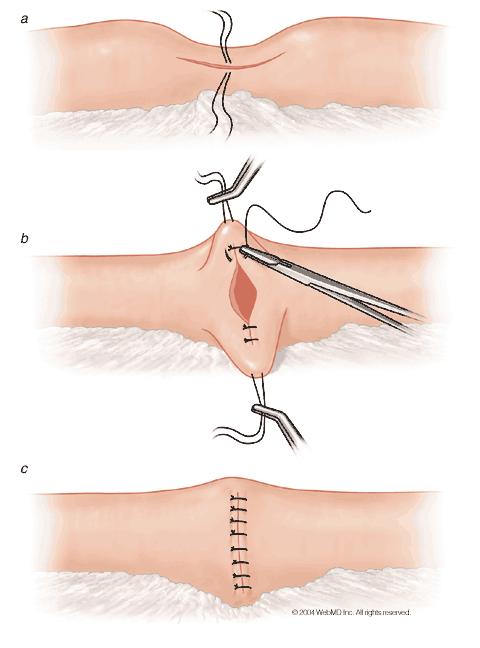
32 Questions A 28 y/o female arrives in the ED with a 72hr h/o diffuse abdominal pain, n/v. She can tolerate only minimal oral intake without emesis. A CT is obtained:

33 CT
34 Questions A 28 y/o female arrives in the ED with a 72hr h/o diffuse abdominal pain, n/v. She can tolerate only minimal oral intake without emesis. A CT is obtained. All of the following would be indicated except: A) insertion of NG tube B) endoscopy C) corticosteroids D) enteral nutrition E) exploratory laparotomy
35 Questions A 52 y/o female with Crohn s and 4-month h/o RLQ discomfort is seeking a 2nd opinion. 3 weeks ago she had an extensive work-up elsewhere. Colonoscopy and small-bowel follow through were normal. This xray was obtained 24hr ago.

36 Xray
37 Questions A 52 y/o female with Crohn s and 4-month h/o RLQ discomfort is seeking a 2nd opinion. 3 weeks ago she had an extensive work-up elsewhere. Colonoscopy and small-bowel follow through were normal. This xray was obtined 24hr ago. Best management would now be: A) elective laparotomy if her condition doesn t improve B) urgent ex-lap C) capsule endoscopy D) CT of abd/pel E) diagnostic laparoscopy
38 Questions Use of a seton should be considered in the management of anorectal fistulas associated with any of the following characteristics except: A) those tracking > 30% to 50% of the external sphincter B) anterior fistulas in women C) recurrent fistulas D) those associated with crohn s disease E) intersphincteric fistulas
39 questions 45 y/o male with crohn s has an asymptomatic intersphincteric fistula-in-ano. The most appropriate management would be: A) observation B) fibrin glue injection C) cutting seton D) fistulotomy E) botulinum toxin

40 questions 56 y/o female with h/o UC develops a painful area inferior to her ileostomy, as shown.
41 questions 56 y/o female with h/o UC develops a painful area inferior to her ileostomy, as shown. The most appropriate management would be: A) cholestyramine powder and reduction of the size of the ileostomy appliance opening B) antifungal powder C) high-dose systemic corticosteroids D) debridement followed by wound vac closures E) wide local excision with stoma relocation.
Surgical Management of IBD. Val Jefford Grand Rounds October 14, 2003
 Surgical Management of IBD Val Jefford Grand Rounds October 14, 2003 Introduction Important Features Clinical Presentation Evaluation Medical Treatment Surgical Treatment Cases Overview Introduction Two
Surgical Management of IBD Val Jefford Grand Rounds October 14, 2003 Introduction Important Features Clinical Presentation Evaluation Medical Treatment Surgical Treatment Cases Overview Introduction Two
Crohn s Disease. Resident Lecture 1/17/19
 Crohn s Disease Resident Lecture 1/17/19 Objectives Features/Classification of Crohn s Disease Medical Treatment Surgical Indications Surgical Considerations 2 Case 25 yo F presents to your office with
Crohn s Disease Resident Lecture 1/17/19 Objectives Features/Classification of Crohn s Disease Medical Treatment Surgical Indications Surgical Considerations 2 Case 25 yo F presents to your office with
Index. Surg Clin N Am 87 (2007) Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type.") Surg Clin N Am 87 (2007) 787 796 Index Note: Page numbers of article titles are in boldface type. A Abscesses in anorectal Crohn s disease, 622 intra-abdominal, in Crohn s disease, 590 591 perirectal,
Surg Clin N Am 87 (2007) 787 796 Index Note: Page numbers of article titles are in boldface type. A Abscesses in anorectal Crohn s disease, 622 intra-abdominal, in Crohn s disease, 590 591 perirectal,
Surgery in Inflammatory Bowel Disease. Rajesh Gupta MS, MCh Surgical Gastroenterology Division Dept of General Surgery PGIMER, Chandigarh
 Surgery in Inflammatory Bowel Disease Rajesh Gupta MS, MCh Surgical Gastroenterology Division Dept of General Surgery PGIMER, Chandigarh 1 Ulcerative colitis (UC) Ulcerative colitis (UC) characterized
Surgery in Inflammatory Bowel Disease Rajesh Gupta MS, MCh Surgical Gastroenterology Division Dept of General Surgery PGIMER, Chandigarh 1 Ulcerative colitis (UC) Ulcerative colitis (UC) characterized
Ileal Pouch Anal Anastomosis: The Preferred Method of Reconstruction after Proctocolectomy in Children
 Ileal Pouch Anal Anastomosis: The Preferred Method of Reconstruction after Proctocolectomy in Children Stephanie Jones, D.O. Surgical Fellow March 21, 2011 Ulcerative Colitis Spectrum of inflammatory bowel
Ileal Pouch Anal Anastomosis: The Preferred Method of Reconstruction after Proctocolectomy in Children Stephanie Jones, D.O. Surgical Fellow March 21, 2011 Ulcerative Colitis Spectrum of inflammatory bowel
Inflammatory Bowel Disease and Surgery: What You Should Know
 Inflammatory Bowel Disease and Surgery: What You Should Know Ask the Experts March 9, 2019 Kristen Blaker, MD Colon and Rectal Surgery MetroHealth Medical Center Disclosures None Outline Who undergoes
Inflammatory Bowel Disease and Surgery: What You Should Know Ask the Experts March 9, 2019 Kristen Blaker, MD Colon and Rectal Surgery MetroHealth Medical Center Disclosures None Outline Who undergoes
Surgical Management of IBD in the Age of Biologics
 Surgical Management of IBD in the Age of Biologics Lisa S. Poritz, M.D Associate Professor of Surgery Division of Colon and Rectal Surgery Objectives Discuss surgical management of IBD When to operate
Surgical Management of IBD in the Age of Biologics Lisa S. Poritz, M.D Associate Professor of Surgery Division of Colon and Rectal Surgery Objectives Discuss surgical management of IBD When to operate
Homayoon Akbari, MD, PhD
 Recent Advances in IBD Surgery Homayoon M. Akbari, MD, PhD, FRCS(C), FACS Associate Professor of Surgery Virginia Commonwealth University Crohn s disease first described as a surgical condition, with the
Recent Advances in IBD Surgery Homayoon M. Akbari, MD, PhD, FRCS(C), FACS Associate Professor of Surgery Virginia Commonwealth University Crohn s disease first described as a surgical condition, with the
Patho Basic Chronic Inflammatory Bowel Diseases. Jürg Vosbeck Pathology
 Patho Basic Chronic Inflammatory Bowel Diseases Jürg Vosbeck Pathology General Group of chronic relapsing diseases with chronic bloody or watery diarrhea Usually ulcerative colitis (UC) or Crohn s disease
Patho Basic Chronic Inflammatory Bowel Diseases Jürg Vosbeck Pathology General Group of chronic relapsing diseases with chronic bloody or watery diarrhea Usually ulcerative colitis (UC) or Crohn s disease
Mohamed EL-hemaly Gastro- intestinal surgical center, Mansoura University.
 Mohamed EL-hemaly Gastro- intestinal surgical center, Mansoura University. Chronic transmural inflammatory process of the bowel & affects any part of the gastro -intestinal tract from the mouth to the
Mohamed EL-hemaly Gastro- intestinal surgical center, Mansoura University. Chronic transmural inflammatory process of the bowel & affects any part of the gastro -intestinal tract from the mouth to the
SURGICAL MANAGEMENT OF ULCERATIVE COLITIS
 SURGICAL MANAGEMENT OF ULCERATIVE COLITIS Cary B. Aarons, MD Associate Professor of Surgery Division of Colon & Rectal Surgery University of Pennsylvania AGENDA Background Diagnosis/Work-up Medical Management
SURGICAL MANAGEMENT OF ULCERATIVE COLITIS Cary B. Aarons, MD Associate Professor of Surgery Division of Colon & Rectal Surgery University of Pennsylvania AGENDA Background Diagnosis/Work-up Medical Management
Treatment of Inflammatory Bowel Disease. Michael Weiss MD, FACG
 Treatment of Inflammatory Bowel Disease Michael Weiss MD, FACG What is IBD? IBD is an immune-mediated chronic intestinal disorder, characterized by chronic or relapsing inflammation within the GI tract.
Treatment of Inflammatory Bowel Disease Michael Weiss MD, FACG What is IBD? IBD is an immune-mediated chronic intestinal disorder, characterized by chronic or relapsing inflammation within the GI tract.
Perianal Fistula of Crohn s Disease
 Case 3 Perianal Fistula of Crohn s Disease A 16 year-old boy referred by surgeon due to perianal fistula since 6mo ago CC=perianal pain History of intermittent non-bloody diarrhea and mild abdominal pain
Case 3 Perianal Fistula of Crohn s Disease A 16 year-old boy referred by surgeon due to perianal fistula since 6mo ago CC=perianal pain History of intermittent non-bloody diarrhea and mild abdominal pain
Inflammatory Bowel Disease: Updates and Controversies CASE #1 CASE #1 8/6/2015. What is the most likely diagnosis?
 Inflammatory Bowel Disease: Updates and Controversies Tehttp://192.185.93.102/~paulkeij/wpcontent/uploads/2013/07/collaboration.jpgxt August 7, 2015 Meagan M Costedio, MD; Colorectal Surgery; Cleveland
Inflammatory Bowel Disease: Updates and Controversies Tehttp://192.185.93.102/~paulkeij/wpcontent/uploads/2013/07/collaboration.jpgxt August 7, 2015 Meagan M Costedio, MD; Colorectal Surgery; Cleveland
Inflammatory Bowel Disease When is diarrhea not just diarrhea?
 Inflammatory Bowel Disease When is diarrhea not just diarrhea? Jackie Kazik, MA, PA C CME Resources CAPA Annual Conference, 2011 Inflammatory Bowel Disease Objectives Discuss what is known about the pathophysiology
Inflammatory Bowel Disease When is diarrhea not just diarrhea? Jackie Kazik, MA, PA C CME Resources CAPA Annual Conference, 2011 Inflammatory Bowel Disease Objectives Discuss what is known about the pathophysiology
An Unusual Complication of Crohn s Disease. Dr Gerald Busuttil Mr Debono s Firm Surgical Grand Round 25 th November 2008
 An Unusual Complication of Crohn s Disease Dr Gerald Busuttil Mr Debono s Firm Surgical Grand Round 25 th November 2008 Case Presentation 70 year old lady k/c of Crohns disease h/o of Hartmann s procedure
An Unusual Complication of Crohn s Disease Dr Gerald Busuttil Mr Debono s Firm Surgical Grand Round 25 th November 2008 Case Presentation 70 year old lady k/c of Crohns disease h/o of Hartmann s procedure
Surgery for Inflammatory Bowel Disease
 Surgery for Inflammatory Bowel Disease Emily Steinhagen, MD Assistant Professor Department of Surgery, Division of Colorectal Surgery University Hospitals Cleveland Medical Center Common Questions Why
Surgery for Inflammatory Bowel Disease Emily Steinhagen, MD Assistant Professor Department of Surgery, Division of Colorectal Surgery University Hospitals Cleveland Medical Center Common Questions Why
Surgical Treatment of Inflammatory Bowel Disease (IBD)
") Surgical Treatment of Inflammatory Bowel Disease (IBD) JMAJ 45(2): 55 62, 2002 Tetsuichiro MUTO Vice-Director, Cancer Institute Hospital Abstract: IBD, especially ulcerative colitis (UC) and Crohn s disease
Surgical Treatment of Inflammatory Bowel Disease (IBD) JMAJ 45(2): 55 62, 2002 Tetsuichiro MUTO Vice-Director, Cancer Institute Hospital Abstract: IBD, especially ulcerative colitis (UC) and Crohn s disease
Pouchitis and Cuffitis A bloody mess. Sze-Lin Peng Colorectal Surgeon Counties Manukau District Health Board
 Pouchitis and Cuffitis A bloody mess Sze-Lin Peng Colorectal Surgeon Counties Manukau District Health Board Ileal-pouch anal anastomosis https://www.pennmedicine.org/for-health-care-professionals/for-physicians/physician-education-and-resources/clinicalbriefings/2018/february/total-proctocolectomy-with-jpouch-reconstruction-for-ulcerative-colitis
Pouchitis and Cuffitis A bloody mess Sze-Lin Peng Colorectal Surgeon Counties Manukau District Health Board Ileal-pouch anal anastomosis https://www.pennmedicine.org/for-health-care-professionals/for-physicians/physician-education-and-resources/clinicalbriefings/2018/february/total-proctocolectomy-with-jpouch-reconstruction-for-ulcerative-colitis
The Role of Surgery in Inflammatory Bowel Disease. Cory D Barrat, MD Colon and Rectal Surgeon Mercy Health
 The Role of Surgery in Inflammatory Bowel Disease Cory D Barrat, MD Colon and Rectal Surgeon Mercy Health THANKS FOR INVITING ME! I have no financial disclosures Outline - Who am I and what do I do? -
The Role of Surgery in Inflammatory Bowel Disease Cory D Barrat, MD Colon and Rectal Surgeon Mercy Health THANKS FOR INVITING ME! I have no financial disclosures Outline - Who am I and what do I do? -
The role of Surgery and Stomas in IBD
 The role of Surgery and Stomas in IBD When do I need it? Can I avoid it? How do I live with it? Kyle G. Cologne, MD Assistant Professor of Surgery USC Division of Colorectal Surgery Topics Surgical Differences
The role of Surgery and Stomas in IBD When do I need it? Can I avoid it? How do I live with it? Kyle G. Cologne, MD Assistant Professor of Surgery USC Division of Colorectal Surgery Topics Surgical Differences
Colorectal Surgery. Patient Care. Goals and Objectives
 Colorectal Surgery Patient Care 1) Interpret the results of clinical evaluations (history, physical examination) performed on patients with a) Hemorrhoids b) Perianal abscess/fistula c) Anal fissure d)
Colorectal Surgery Patient Care 1) Interpret the results of clinical evaluations (history, physical examination) performed on patients with a) Hemorrhoids b) Perianal abscess/fistula c) Anal fissure d)
Crohn's disease CAUSES COURSE OF CROHN'S DISEASE TREATMENT. Sulfasalazine
 Crohn's disease Crohn's disease is an inflammatory condition of the digestive tract that affects children and adults. Common features of Crohn's disease include mouth sores, diarrhea, abdominal pain, weight
Crohn's disease Crohn's disease is an inflammatory condition of the digestive tract that affects children and adults. Common features of Crohn's disease include mouth sores, diarrhea, abdominal pain, weight
Surgical Approach to Crohn s Colitis Segmental or Total Colectomy? Can We Avoid the Stoma?
 17 th Panhellenic IBD Congress Thessaloniki May 2018 Surgical Approach to Crohn s Colitis Segmental or Total Colectomy? Can We Avoid the Stoma? Janindra Warusavitarne Consultant Colorectal Surgeon, St
17 th Panhellenic IBD Congress Thessaloniki May 2018 Surgical Approach to Crohn s Colitis Segmental or Total Colectomy? Can We Avoid the Stoma? Janindra Warusavitarne Consultant Colorectal Surgeon, St
Understanding Inflammatory Bowel Diseases (IBD):
:") Understanding Inflammatory Bowel Diseases (IBD): What Every Patient Needs to Know William H Holderman, MD Digestive Health Specialists Tacoma, WA Today s Objectives Define IBD, its potential causes and
Understanding Inflammatory Bowel Diseases (IBD): What Every Patient Needs to Know William H Holderman, MD Digestive Health Specialists Tacoma, WA Today s Objectives Define IBD, its potential causes and
Treating Crohn s and Colitis in the ASC
 Treating Crohn s and Colitis in the ASC Kimberly M Persley, MD Texas Digestive Disease consultants TASC Meeting Outline IBD 101 Diagnosis Treatment Burden of Disease Role of ASC Inflammatory Bowel Disease
Treating Crohn s and Colitis in the ASC Kimberly M Persley, MD Texas Digestive Disease consultants TASC Meeting Outline IBD 101 Diagnosis Treatment Burden of Disease Role of ASC Inflammatory Bowel Disease
3/22/2011. Inflammatory Bowel Disease. Inflammatory Bowel Disease Objectives: Appendicitis. Lemone and Burke Chapter 26
 Inflammatory Bowel Disease Lemone and Burke Chapter 26 Inflammatory Bowel Disease Objectives: Discuss etiology, patho and clinical manifestations of Appendicitis Peritonitis Ulcerative Colitis Crohn s
Inflammatory Bowel Disease Lemone and Burke Chapter 26 Inflammatory Bowel Disease Objectives: Discuss etiology, patho and clinical manifestations of Appendicitis Peritonitis Ulcerative Colitis Crohn s
Crohn's Disease. What causes Crohn s disease? What are the symptoms?
 Crohn's Disease Crohn s disease is an ongoing disorder that causes inflammation of the digestive tract, also referred to as the gastrointestinal (GI) tract. Crohn s disease can affect any area of the GI
Crohn's Disease Crohn s disease is an ongoing disorder that causes inflammation of the digestive tract, also referred to as the gastrointestinal (GI) tract. Crohn s disease can affect any area of the GI
Surgery and Stomas in IBD When do I need it? Can I avoid it? How do I live with it?
 Surgery and Stomas in IBD When do I need it? Can I avoid it? How do I live with it? Kyle G. Cologne, MD Assistant Professor of Surgery USC Division of Colorectal Surgery Topics Surgical Differences between
Surgery and Stomas in IBD When do I need it? Can I avoid it? How do I live with it? Kyle G. Cologne, MD Assistant Professor of Surgery USC Division of Colorectal Surgery Topics Surgical Differences between
INFLAMMATORY BOWEL DISEASE
 National University Faculty of Medicine INFLAMMATORY BOWEL DISEASE Gehan M. Osman, MD. MBBS Pediatrician Jaffar Ibn Auf Specialized Hospital EDUCATIONAL OBJECTIVES Definitions and spectrum of (IBD) Epidemiology
National University Faculty of Medicine INFLAMMATORY BOWEL DISEASE Gehan M. Osman, MD. MBBS Pediatrician Jaffar Ibn Auf Specialized Hospital EDUCATIONAL OBJECTIVES Definitions and spectrum of (IBD) Epidemiology
DIGESTIVE SYSTEM SURGICAL PROCEDURES December 22, 2015 (effective March 1, 2016) INTESTINES (EXCEPT RECTUM) Asst Surg Anae
 INTESTINES (EXCEPT RECTUM) Asst Surg Anae") December 22, 2015 (effective March 1, 201) INTESTINES (EXCEPT RECTUM) Z513 Hydrostatic - Pneumatic dilatation of colon stricture(s) through colonoscope... 10.50 Z50 Fulguration of first polyp through colonoscope...
December 22, 2015 (effective March 1, 201) INTESTINES (EXCEPT RECTUM) Z513 Hydrostatic - Pneumatic dilatation of colon stricture(s) through colonoscope... 10.50 Z50 Fulguration of first polyp through colonoscope...
What is Crohn's disease?
 What is Crohn's disease? Crohn's disease is a chronic inflammatory disorder that causes inflammation of the digestive tract. It can affect any area of the GI tract, from the mouth to the anus, but it most
What is Crohn's disease? Crohn's disease is a chronic inflammatory disorder that causes inflammation of the digestive tract. It can affect any area of the GI tract, from the mouth to the anus, but it most
Disclosure of Affiliations. The Way We Hope It Goes. Medicines and Surgery for IBD. None. Cases: Sweet and Not So Sweet
 Immunomodulators and Complications of Surgery for Inflammatory Bowel Disease Disclosure of Affiliations None Thomas E. Read, MD, FACS, FASCRS Professor of Surgery Tufts University School of Medicine Senior
Immunomodulators and Complications of Surgery for Inflammatory Bowel Disease Disclosure of Affiliations None Thomas E. Read, MD, FACS, FASCRS Professor of Surgery Tufts University School of Medicine Senior
Surgical Therapies for the Treatment of IBD!
 Surgical Therapies for the Treatment of IBD! Andrew A Shelton, MD Clinical Professor of Surgery Stanford Hospital and Clinics Section of Colon and Rectal Surgery! Ulcerative Colitis v. Crohn s! 30% of
Surgical Therapies for the Treatment of IBD! Andrew A Shelton, MD Clinical Professor of Surgery Stanford Hospital and Clinics Section of Colon and Rectal Surgery! Ulcerative Colitis v. Crohn s! 30% of
Surgery and Crohn s. Crohn s Disease 70 % Why Operate? Complications of Disease. The Gastrointestinal Tract. Surgery for Inflammatory Bowel Disease
 The Gastrointestinal Tract Surgery for Inflammatory Bowel Disease Jonathan Chun, MD The regon Clinic Gastrointestinal and Minimally Invasive Surgery Crohn s Disease Can affect anywhere in the GI tract,
The Gastrointestinal Tract Surgery for Inflammatory Bowel Disease Jonathan Chun, MD The regon Clinic Gastrointestinal and Minimally Invasive Surgery Crohn s Disease Can affect anywhere in the GI tract,
Year 2002 Paper two: Questions supplied by Jo 1
 Year 2002 Paper two: Questions supplied by Jo 1 29) A 54 year old man with colonic Crohn s disease is in remission following an 8 week course of prednisolone. Which one of the following medications is
Year 2002 Paper two: Questions supplied by Jo 1 29) A 54 year old man with colonic Crohn s disease is in remission following an 8 week course of prednisolone. Which one of the following medications is
My Child Has Inflammatory Bowel Disease : Why? What now? What s next?
 My Child Has Inflammatory Bowel Disease : Why? What now? What s next? George M. Zacur, M.D., M.S. Clinical Assistant Professor Department of Pediatrics and Communicable Diseases Division of Gastroenterology
My Child Has Inflammatory Bowel Disease : Why? What now? What s next? George M. Zacur, M.D., M.S. Clinical Assistant Professor Department of Pediatrics and Communicable Diseases Division of Gastroenterology
Index. Note: Page numbers of article title are in boldface type.
 Index Note: Page numbers of article title are in boldface type. A Abscess(es) in Crohn s disease, 168 169 IPAA and, 110 114 as unexpected finding in colorectal surgery, 46 Adhesion(s) trocars-related laparoscopy
Index Note: Page numbers of article title are in boldface type. A Abscess(es) in Crohn s disease, 168 169 IPAA and, 110 114 as unexpected finding in colorectal surgery, 46 Adhesion(s) trocars-related laparoscopy
11/13/11. Biologics for CD and CUC: The Impact on Surgical Outcomes. Principles of Successful Intestinal Surgery
 Biologics for CD and CUC: The Impact on Surgical Outcomes Robert R. Cima, M.D., M.A. Associate Professor of Surgery Division of Colon and Rectal Surgery Overview Antibody based medications (biologics)
Biologics for CD and CUC: The Impact on Surgical Outcomes Robert R. Cima, M.D., M.A. Associate Professor of Surgery Division of Colon and Rectal Surgery Overview Antibody based medications (biologics)
Colostomy & Ileostomy
 Colostomy & Ileostomy Indications, problems and preference By Waleed Omar Professor of Colorectal surgery, Mansoura University. Disclosure I have no disclosures. Presentation outline Stoma: Definition
Colostomy & Ileostomy Indications, problems and preference By Waleed Omar Professor of Colorectal surgery, Mansoura University. Disclosure I have no disclosures. Presentation outline Stoma: Definition
Perianal and Fistulizing Crohn s Disease: Tough Management Decisions. Jean-Paul Achkar, M.D. Kenneth Rainin Chair for IBD Research Cleveland Clinic
 Perianal and Fistulizing Crohn s Disease: Tough Management Decisions Jean-Paul Achkar, M.D. Kenneth Rainin Chair for IBD Research Cleveland Clinic Talk Overview Background Assessment and Classification
Perianal and Fistulizing Crohn s Disease: Tough Management Decisions Jean-Paul Achkar, M.D. Kenneth Rainin Chair for IBD Research Cleveland Clinic Talk Overview Background Assessment and Classification
Inflammatory Bowel Disease
 Inflammatory Bowel Disease Objectives: NOT FOUND. Team Members: Shrouq alsomali + Basel almeflh + Alaa alaqeel + Raneem alghamdi Team Leader: Haneen Alsubki Revised By: Maha AlGhamdi Resources: 435 team
Inflammatory Bowel Disease Objectives: NOT FOUND. Team Members: Shrouq alsomali + Basel almeflh + Alaa alaqeel + Raneem alghamdi Team Leader: Haneen Alsubki Revised By: Maha AlGhamdi Resources: 435 team
Welcome to Week 2 of the Crohn s & Colitis Foundation of America (CCFA) Online Support Group.
 Online Support Group.") Welcome to Week 2 of the Crohn s & Colitis Foundation of America (CCFA) Online. Last week s material consisted of an overview of inflammatory bowel diseases (IBD), specifically Crohn s disease and ulcerative
Welcome to Week 2 of the Crohn s & Colitis Foundation of America (CCFA) Online. Last week s material consisted of an overview of inflammatory bowel diseases (IBD), specifically Crohn s disease and ulcerative
What is ulcerative colitis?
 What is ulcerative colitis? Ulcerative colitis is a disease that causes inflammation and sores, called ulcers, in the lining of the rectum and colon. Ulcers form where inflammation has killed the cells
What is ulcerative colitis? Ulcerative colitis is a disease that causes inflammation and sores, called ulcers, in the lining of the rectum and colon. Ulcers form where inflammation has killed the cells
WHAT IS ULCERATIVE COLITIS?
 235 60th Street, West New York, NJ 07093 T: (201) 854-4646 F: (201) 854-4647 810 Main Street, Hackensack, NJ 07601 T: (201) 488-0095 Ulcerative Colitis WHAT IS ULCERATIVE COLITIS? Ulcerative colitis is
235 60th Street, West New York, NJ 07093 T: (201) 854-4646 F: (201) 854-4647 810 Main Street, Hackensack, NJ 07601 T: (201) 488-0095 Ulcerative Colitis WHAT IS ULCERATIVE COLITIS? Ulcerative colitis is
IBD 101. Ronen Stein, MD Assistant Professor of Clinical Pediatrics Division of Gastroenterology, Hepatology, and Nutrition
 IBD 101 Ronen Stein, MD Assistant Professor of Clinical Pediatrics Division of Gastroenterology, Hepatology, and Nutrition Objectives Identify factors involved in the development of inflammatory bowel
IBD 101 Ronen Stein, MD Assistant Professor of Clinical Pediatrics Division of Gastroenterology, Hepatology, and Nutrition Objectives Identify factors involved in the development of inflammatory bowel
An Update on the Biologic Treatment for Patients with Inflammatory Bowel Disease. David A. Schwartz, MD
 An Update on the Biologic Treatment for Patients with Inflammatory Bowel Disease David A. Schwartz, MD Director, Inflammatory Bowel Disease Center Associate Professor of Medicine Vanderbilt University
An Update on the Biologic Treatment for Patients with Inflammatory Bowel Disease David A. Schwartz, MD Director, Inflammatory Bowel Disease Center Associate Professor of Medicine Vanderbilt University
Case Presentations #2 Saturday November 13, Case #1 HPI 11/14/10. Uma Mahadevan-Velayos MD. Complicated Crohn s Pregnancy
 Case Presentations #2 Saturday November 13, 2010 Uma Mahadevan-Velayos MD Case #1 Complicated Crohn s Pregnancy HPI 34 yo F with Crohn s disease presents to office 18 weeks pregnant, moved back to SF from
Case Presentations #2 Saturday November 13, 2010 Uma Mahadevan-Velayos MD Case #1 Complicated Crohn s Pregnancy HPI 34 yo F with Crohn s disease presents to office 18 weeks pregnant, moved back to SF from
Chapter 14: Training in Radiology. DDSEP Chapter 1: Question 12
 DDSEP Chapter 1: Question 12 A 52-year-old white male presents for evaluation of sudden onset of abdominal pain and shoulder pain. His past medical history is notable for a history of coronary artery disease,
DDSEP Chapter 1: Question 12 A 52-year-old white male presents for evaluation of sudden onset of abdominal pain and shoulder pain. His past medical history is notable for a history of coronary artery disease,
Diarrhoea for the Acute Physician
 Diarrhoea for the Acute Physician STEPHEN INNS GASTROENTEROLOGIST AND PHYSICIAN HUTT VALLEY DHB August 2013 Outline Case History 1 Initial assessment of acute diarrhoea Management of fulminant UC Management
Diarrhoea for the Acute Physician STEPHEN INNS GASTROENTEROLOGIST AND PHYSICIAN HUTT VALLEY DHB August 2013 Outline Case History 1 Initial assessment of acute diarrhoea Management of fulminant UC Management
How do I choose amongst medicines for inflammatory bowel disease. Maria T. Abreu, MD
 How do I choose amongst medicines for inflammatory bowel disease Maria T. Abreu, MD Overview of IBD Pathogenesis Bacterial Products Moderately Acutely Inflamed Chronic Inflammation = IBD Normal Gut Mildly
How do I choose amongst medicines for inflammatory bowel disease Maria T. Abreu, MD Overview of IBD Pathogenesis Bacterial Products Moderately Acutely Inflamed Chronic Inflammation = IBD Normal Gut Mildly
ULCERATIVE COLITIS. Sean Lynch, MD and Richard Bloomfeld, MD Wake Forest University School of Medicine Winston-Salem, NC
 ULCERATIVE COLITIS Sean Lynch, MD and Richard Bloomfeld, MD Wake Forest University School of Medicine Winston-Salem, NC What is Ulcerative Colitis? Ulcerative colitis (UC) is a disease marked by inflammation
ULCERATIVE COLITIS Sean Lynch, MD and Richard Bloomfeld, MD Wake Forest University School of Medicine Winston-Salem, NC What is Ulcerative Colitis? Ulcerative colitis (UC) is a disease marked by inflammation
Acute Diverticulitis. Andrew B. Peitzman, MD Mark M. Ravitch Professor of Surgery University of Pittsburgh
 Acute Diverticulitis Andrew B. Peitzman, MD Mark M. Ravitch Professor of Surgery University of Pittsburgh Focus today: when to operate n Recurrent, uncomplicated diverticulitis; after how many episodes?
Acute Diverticulitis Andrew B. Peitzman, MD Mark M. Ravitch Professor of Surgery University of Pittsburgh Focus today: when to operate n Recurrent, uncomplicated diverticulitis; after how many episodes?
Modern Management of Perianal Fistulas in Crohn s Disease (PFCD): Future Directions
: Future Directions") Modern Management of Perianal Fistulas in Crohn s Disease (PFCD): Future Directions Rami Ismail, Pharm.D., BCPS, BCCCP, CACP Lead Clinical staff Pharmacist, Cleveland Clinic Abu Dhabi Disclosure Information
Modern Management of Perianal Fistulas in Crohn s Disease (PFCD): Future Directions Rami Ismail, Pharm.D., BCPS, BCCCP, CACP Lead Clinical staff Pharmacist, Cleveland Clinic Abu Dhabi Disclosure Information
Diseases of the Colon. Jack Bragg, D.O., F.A.C.O.I.
 Diseases of the Colon Jack Bragg, D.O., F.A.C.O.I. I have no disclosures I work for the Curators of the University of Missouri Inflammatory Bowel Disease ULCERATIVE COLITIS CROHN S DISEASE Transmural Inflammation
Diseases of the Colon Jack Bragg, D.O., F.A.C.O.I. I have no disclosures I work for the Curators of the University of Missouri Inflammatory Bowel Disease ULCERATIVE COLITIS CROHN S DISEASE Transmural Inflammation
Index. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A Abdominal surgery prior as factor in laparoscopic colorectal surgery, 554 555 Abscess(es) CRC presenting as, 539 540 Adenocarcinoma of
Index Note: Page numbers of article titles are in boldface type. A Abdominal surgery prior as factor in laparoscopic colorectal surgery, 554 555 Abscess(es) CRC presenting as, 539 540 Adenocarcinoma of
Garrick Brown, MD. Digestive Health Specialists Tacoma Gig Harbor
 Garrick Brown, MD Digestive Health Specialists Tacoma Gig Harbor Today s Objectives Define IBD, its potential causes and diagnosis Discuss management and treatment Discuss complementary and alternative
Garrick Brown, MD Digestive Health Specialists Tacoma Gig Harbor Today s Objectives Define IBD, its potential causes and diagnosis Discuss management and treatment Discuss complementary and alternative
DIVERTICULOSIS MEDICAL AND SURGICAL MANAGEMENT. Simon Radley Consultant Surgeon March 2013
 DIVERTICULOSIS MEDICAL AND SURGICAL MANAGEMENT Simon Radley Consultant Surgeon March 2013 Definitions Diverticulosis: presence of diverticulae Diverticular disease: diverticulae associated with symptoms
DIVERTICULOSIS MEDICAL AND SURGICAL MANAGEMENT Simon Radley Consultant Surgeon March 2013 Definitions Diverticulosis: presence of diverticulae Diverticular disease: diverticulae associated with symptoms
Fistulizing Crohn s Disease: The Aggressive Approach
 Fistulizing Crohn s Disease: The Aggressive Approach Bruce E. Sands, MD, MS MGH Crohn s and Colitis Center and Gastrointestinal Unit Massachusetts General Hospital Boston, USA Case Presentation: Summary
Fistulizing Crohn s Disease: The Aggressive Approach Bruce E. Sands, MD, MS MGH Crohn s and Colitis Center and Gastrointestinal Unit Massachusetts General Hospital Boston, USA Case Presentation: Summary
Surgical Workload, Outcome and Research Database: V1.1
 Technical Guidance for Surgical Workload, Outcome and Research Database: V1.1 Contents 1. Standard Indicators... 5 1.1. Activity Volume... 5 1.2. Average Length of Stay (Days)... 5 1.3. 2/7/30 day Re-admission
Technical Guidance for Surgical Workload, Outcome and Research Database: V1.1 Contents 1. Standard Indicators... 5 1.1. Activity Volume... 5 1.2. Average Length of Stay (Days)... 5 1.3. 2/7/30 day Re-admission
Management of the Hospitalized IBD Patient. Drew DuPont MD
 Management of the Hospitalized IBD Patient Drew DuPont MD Ulcerative Colitis: Indications for Admission Severe ulcerative colitis Frequent loose bloody stools ( 6 per day) Severe cramps Systemic toxicity:
Management of the Hospitalized IBD Patient Drew DuPont MD Ulcerative Colitis: Indications for Admission Severe ulcerative colitis Frequent loose bloody stools ( 6 per day) Severe cramps Systemic toxicity:
The Spectrum of IBD. Inflammatory Bowel Disease. Symptoms. Epidemiology. Tests for IBD. CD or UC? Inflamatory Bowel Disease. Fernando Vega, M.D.
 The Spectrum of IBD Inflammatory Bowel Disease Fernando Vega, M.D. Epidemiology CD and UC together 1:400 UC Prevalence 1:500 UC Incidence 6-12K/annum CD Prevalence 1:1000 CD Incidence 3-6K/annum Symptoms
The Spectrum of IBD Inflammatory Bowel Disease Fernando Vega, M.D. Epidemiology CD and UC together 1:400 UC Prevalence 1:500 UC Incidence 6-12K/annum CD Prevalence 1:1000 CD Incidence 3-6K/annum Symptoms
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE
 NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE Centre for Clinical Practice SCOPE Clinical guideline title: Ulcerative colitis: the management of ulcerative colitis Quality standard title: Ulcerative
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE Centre for Clinical Practice SCOPE Clinical guideline title: Ulcerative colitis: the management of ulcerative colitis Quality standard title: Ulcerative
ABC of Colorectal Diseases
 ABC of Colorectal Diseases NON-SPECIFIC INFLAMMATORY BOWEL DISEASE S Pettit, M H Irving Non-specific inflammatory bowel diseases are those for which there is no discernible aetiological agent. The two
ABC of Colorectal Diseases NON-SPECIFIC INFLAMMATORY BOWEL DISEASE S Pettit, M H Irving Non-specific inflammatory bowel diseases are those for which there is no discernible aetiological agent. The two
Definitions. Clinical remission: Resolution of symptoms (stool frequency 3/day, no bleeding and no urgency)
") CROHN S DISEASE Definitions Clinical remission: Resolution of symptoms (stool frequency 3/day, no bleeding and no urgency) Recurrence: The reappearance of lesions after surgical resection Endoscopic remission:
CROHN S DISEASE Definitions Clinical remission: Resolution of symptoms (stool frequency 3/day, no bleeding and no urgency) Recurrence: The reappearance of lesions after surgical resection Endoscopic remission:
Case Report Successful Long-Term Use of Infliximab in Refractory Pouchitis in an Adolescent
 Gastroenterology Research and Practice Volume 2010, Article ID 860394, 4 pages doi:10.1155/2010/860394 Case Report Successful Long-Term Use of Infliximab in Refractory Pouchitis in an Adolescent Jessica
Gastroenterology Research and Practice Volume 2010, Article ID 860394, 4 pages doi:10.1155/2010/860394 Case Report Successful Long-Term Use of Infliximab in Refractory Pouchitis in an Adolescent Jessica
Top 10 Things you need to know about IBD. Suresh Pola, MD Kaiser San Diego
 Top 10 Things you need to know about IBD Suresh Pola, MD Kaiser San Diego Top 10 Things to Know: IBD What you can eat How to treat the pain Not all diarrhea is a flare Ways to reduce your risk of getting
Top 10 Things you need to know about IBD Suresh Pola, MD Kaiser San Diego Top 10 Things to Know: IBD What you can eat How to treat the pain Not all diarrhea is a flare Ways to reduce your risk of getting
CCFA. Crohns Disease vs UC: What is the best treatment for me? November
 CCFA Crohns Disease vs UC: What is the best treatment for me? November 8 2009 Ellen J. Scherl,, MD, FACP,AGAF Roberts Inflammatory Bowel Disease Center Weill Medical College Cornell University New York
CCFA Crohns Disease vs UC: What is the best treatment for me? November 8 2009 Ellen J. Scherl,, MD, FACP,AGAF Roberts Inflammatory Bowel Disease Center Weill Medical College Cornell University New York
Inflammatory Bowel Disease
 Inflammatory Bowel Disease William Sonnenberg, MD Titusville, PA Disclosure Dr. William Sonnenberg has no conflict of interest, financial agreement, or working affiliation with any group or organization.
Inflammatory Bowel Disease William Sonnenberg, MD Titusville, PA Disclosure Dr. William Sonnenberg has no conflict of interest, financial agreement, or working affiliation with any group or organization.
What do we need for diagnosis of IBD
 What do we need for diagnosis of IBD Kaichun Wu Dept. of Gastroenterology, Xijing Hospital Fourth Military Medical University Xi an an,, China In China UC 11.6/10 5,CD 1.4/10 5 Major cause of chronic diarrhea
What do we need for diagnosis of IBD Kaichun Wu Dept. of Gastroenterology, Xijing Hospital Fourth Military Medical University Xi an an,, China In China UC 11.6/10 5,CD 1.4/10 5 Major cause of chronic diarrhea
Indications for use of Infliximab
 Indications for use of Infliximab Moscow, June 10 th 2006 Prof. Dr. Dr. Gerhard Rogler Klinik und Poliklinik für Innere Medizin I Universität Regensburg Case report 1989: Diagnosis of Crohn s disease of
Indications for use of Infliximab Moscow, June 10 th 2006 Prof. Dr. Dr. Gerhard Rogler Klinik und Poliklinik für Innere Medizin I Universität Regensburg Case report 1989: Diagnosis of Crohn s disease of
Ali Keshavarzian MD Rush University Medical Center
 Treatment: Step Up or Top Down? Ali Keshavarzian MD Rush University Medical Center Questions What medication should IBD be treated with? Can we predict which patients with IBD are high risk? Is starting
Treatment: Step Up or Top Down? Ali Keshavarzian MD Rush University Medical Center Questions What medication should IBD be treated with? Can we predict which patients with IBD are high risk? Is starting
What is Crohn's disease?
 What is Crohn's disease? Crohn s disease is an ongoing disorder that causes inflammation of the digestive tract, also referred to as the gastrointestinal (GI) tract. Crohn s disease can affect any area
What is Crohn's disease? Crohn s disease is an ongoing disorder that causes inflammation of the digestive tract, also referred to as the gastrointestinal (GI) tract. Crohn s disease can affect any area
8/29/2016 DIVERTICULAR DISEASE: WHAT EVERY NURSE PRACTITIONER SHOULD KNOW. LENORE LAMANNA Ed.D, ANP-C LEARNING OBJECTIVES
 DIVERTICULAR DISEASE: WHAT EVERY NURSE PRACTITIONER SHOULD KNOW LENORE LAMANNA Ed.D, ANP-C LEARNING OBJECTIVES Define Diverticular Disease Discuss Epidemiology and Pathophysiology of Diverticular disease
DIVERTICULAR DISEASE: WHAT EVERY NURSE PRACTITIONER SHOULD KNOW LENORE LAMANNA Ed.D, ANP-C LEARNING OBJECTIVES Define Diverticular Disease Discuss Epidemiology and Pathophysiology of Diverticular disease
Deep Enteroscopy Methods to Diagnose Small Bowel IBD
 Deep Enteroscopy Methods to Diagnose Small Bowel IBD Name: Institution: Peter Draganov University of Florida, Gainesville, FL Overview Types of enteroscopy Enteroscopy equipment Enetoscopy do and don'ts
Deep Enteroscopy Methods to Diagnose Small Bowel IBD Name: Institution: Peter Draganov University of Florida, Gainesville, FL Overview Types of enteroscopy Enteroscopy equipment Enetoscopy do and don'ts
INFLAMMATORY BOWEL DISEASE (IBD): CROHN S DISEASE
: CROHN S DISEASE") INFLAMMATORY BOWEL DISEASE (IBD): CROHN S DISEASE Symptoms The symptoms of Crohn s disease can vary from person to person, based on where the disease is in the body and how bad the inflammation is. The
INFLAMMATORY BOWEL DISEASE (IBD): CROHN S DISEASE Symptoms The symptoms of Crohn s disease can vary from person to person, based on where the disease is in the body and how bad the inflammation is. The
Lower GI bleeding. Aliu Sanni, MD Long Island College Hospital 17 th June, 2010
 Lower GI bleeding Aliu Sanni, MD Long Island College Hospital 17 th June, 2010 Case Presentation CC: Hematochezia HPI: 28yr old male presents with 1 day episode of bloody stools. Denies any abdominal pain.
Lower GI bleeding Aliu Sanni, MD Long Island College Hospital 17 th June, 2010 Case Presentation CC: Hematochezia HPI: 28yr old male presents with 1 day episode of bloody stools. Denies any abdominal pain.
Idiopathic inflammatory bowel disease is divided into 2 major disease processes, Crohn disease
 REVIEW ARTICLE Medical and Surgical Management of Chronic Ulcerative Colitis Robert R. Cima, MD; John H. Pemberton, MD Idiopathic inflammatory bowel disease is divided into 2 major disease processes, Crohn
REVIEW ARTICLE Medical and Surgical Management of Chronic Ulcerative Colitis Robert R. Cima, MD; John H. Pemberton, MD Idiopathic inflammatory bowel disease is divided into 2 major disease processes, Crohn
ULCERATIVE COLITIS DEFINITION
 DR R DE LACY ULCERATIVE COLITIS DEFINITION Inflammation of the lining of the large bowel (colon and rectum) Aetiology is poorly understood Genetic factors - aggregation in families - identical twin concordance
DR R DE LACY ULCERATIVE COLITIS DEFINITION Inflammation of the lining of the large bowel (colon and rectum) Aetiology is poorly understood Genetic factors - aggregation in families - identical twin concordance
Endoscopy in IBD. F.Hartmann K.Kasper-Kliniken (St.Marienkrankenhaus) Frankfurt/M.
 Frankfurt/M.") F.Hartmann K.Kasper-Kliniken (St.Marienkrankenhaus) Frankfurt/M. F.Hartmann@em.uni-frankfurt.de Indications for endoscopy Diagnosis Management Surveillance Diagnosis Single most valuable tool: ileocolonoscopy
F.Hartmann K.Kasper-Kliniken (St.Marienkrankenhaus) Frankfurt/M. F.Hartmann@em.uni-frankfurt.de Indications for endoscopy Diagnosis Management Surveillance Diagnosis Single most valuable tool: ileocolonoscopy
Spectrum of Diverticular Disease. Outline
 Spectrum of Disease ACG Postgraduate Course January 24, 2015 Lisa Strate, MD, MPH Associate Professor of Medicine University of Washington, Seattle, WA Outline Traditional theories and updated perspectives
Spectrum of Disease ACG Postgraduate Course January 24, 2015 Lisa Strate, MD, MPH Associate Professor of Medicine University of Washington, Seattle, WA Outline Traditional theories and updated perspectives
STOMA SITING & PARASTOMAL HERNIA MANAGEMENT
 STOMA SITING & PARASTOMAL HERNIA MANAGEMENT Professor Hany S. Tawfik Head of the Department of Surgery & Chairman of Colorectal Surgery Unit Benha University Disclosure No financial affiliation to disclose
STOMA SITING & PARASTOMAL HERNIA MANAGEMENT Professor Hany S. Tawfik Head of the Department of Surgery & Chairman of Colorectal Surgery Unit Benha University Disclosure No financial affiliation to disclose
Understanding Learning is the first step to getting help.
 Understanding Inflammatory Bowel Disease (IBD) Learning is the first step to getting help. This booklet has been created through an educational grant provided by Fulford India Ltd., A subsidiary of Schering-Plough
Understanding Inflammatory Bowel Disease (IBD) Learning is the first step to getting help. This booklet has been created through an educational grant provided by Fulford India Ltd., A subsidiary of Schering-Plough
To help protect your privacy, PowerPoint prevented this external picture from being automatically downloaded. To download and display this picture,
 To help protect your privacy, PowerPoint prevented this external picture from being automatically downloaded. To download and display this picture, click Options in the Message Bar, and then click Enable
To help protect your privacy, PowerPoint prevented this external picture from being automatically downloaded. To download and display this picture, click Options in the Message Bar, and then click Enable
Pitfalls in the Diagnosis of Inflammatory Bowel Disease
 Pitfalls in the Diagnosis of Inflammatory Bowel Disease Robert H Riddell MD Mt Sinai Hospital Toronto Prof of Lab. Medicine and Pathobiology University of Toronto Atypical gross / endoscopic distribution
Pitfalls in the Diagnosis of Inflammatory Bowel Disease Robert H Riddell MD Mt Sinai Hospital Toronto Prof of Lab. Medicine and Pathobiology University of Toronto Atypical gross / endoscopic distribution
Medical therapies and IBD
 Medical therapies and IBD Although there is no cure for IBD, there are many treatment options available. There is no standard treatment for IBD that is effective in all situations or for all patients,
Medical therapies and IBD Although there is no cure for IBD, there are many treatment options available. There is no standard treatment for IBD that is effective in all situations or for all patients,
Ileo-rectal anastomosis for Crohn's disease of
 Ileo-rectal anastomosis for Crohn's disease of the colon W. N. W. BAKER From the Research Department, St Mark's Hospital, London Gut, 1971, 12, 427-431 SUMMARY Twenty-six cases of Crohn's disease of the
Ileo-rectal anastomosis for Crohn's disease of the colon W. N. W. BAKER From the Research Department, St Mark's Hospital, London Gut, 1971, 12, 427-431 SUMMARY Twenty-six cases of Crohn's disease of the
Surgery for Ulcerative Colitis 11/14/10. Colectomy for Ulcerative Colitis: What your patient should know. Surgery for Ulcerative Colitis
 Colectomy for Ulcerative Colitis: What your patient should know Madhulika G. Varma MD Associate Professor and Chief Section of Colorectal Surgery University of California, San Francisco Surgery for Ulcerative
Colectomy for Ulcerative Colitis: What your patient should know Madhulika G. Varma MD Associate Professor and Chief Section of Colorectal Surgery University of California, San Francisco Surgery for Ulcerative
INFLAMMATORY BOWEL DISEASE. Jean-Paul Achkar, MD Center for Inflammatory Bowel Disease Cleveland Clinic
 INFLAMMATORY BOWEL DISEASE Jean-Paul Achkar, MD Center for Inflammatory Bowel Disease Cleveland Clinic WHAT IS INFLAMMATORY BOWEL DISEASE (IBD)? Chronic inflammation of the intestinal tract Two related
INFLAMMATORY BOWEL DISEASE Jean-Paul Achkar, MD Center for Inflammatory Bowel Disease Cleveland Clinic WHAT IS INFLAMMATORY BOWEL DISEASE (IBD)? Chronic inflammation of the intestinal tract Two related
PEDIATRIC INFLAMMATORY BOWEL DISEASE
 PEDIATRIC INFLAMMATORY BOWEL DISEASE Alexis Rodriguez, MD Pediatric Gastroenterology Advocate Children s Hospital Disclosers Abbott Nutrition - Speaker Inflammatory Bowel Disease Chronic inflammatory disease
PEDIATRIC INFLAMMATORY BOWEL DISEASE Alexis Rodriguez, MD Pediatric Gastroenterology Advocate Children s Hospital Disclosers Abbott Nutrition - Speaker Inflammatory Bowel Disease Chronic inflammatory disease
Guideline scope Diverticular disease: diagnosis and management
 NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Guideline scope Diverticular disease: diagnosis and management The Department of Health in England has asked NICE to develop a clinical guideline on diverticular
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Guideline scope Diverticular disease: diagnosis and management The Department of Health in England has asked NICE to develop a clinical guideline on diverticular
Listed below are some of the words that you might come across concerning diseases and conditions of the bowels.
 Listed below are some of the words that you might come across concerning diseases and conditions of the bowels. Abscess A localised collection of pus in a cavity that is formed by the decay of diseased
Listed below are some of the words that you might come across concerning diseases and conditions of the bowels. Abscess A localised collection of pus in a cavity that is formed by the decay of diseased
LARGE BOWEL OBSTRUCTION MARCUS BURNSTEIN
 LARGE BOWEL OBSTRUCTION MARCUS BURNSTEIN MCQ A 78 yr. old man (HT, DM, 2 coronary stents) has 3 mos. of irregular bowel habits and 72 hrs. of LBO. Distended, non-tender. Normal blood work. Plain xray,
LARGE BOWEL OBSTRUCTION MARCUS BURNSTEIN MCQ A 78 yr. old man (HT, DM, 2 coronary stents) has 3 mos. of irregular bowel habits and 72 hrs. of LBO. Distended, non-tender. Normal blood work. Plain xray,
Surgical Outcomes of Crohn s Disease: A Single Institutional Experience in Taiwan. [J Soc Colon Rectal Surgeon (Taiwan) 2009;20:1-6]
![Surgical Outcomes of Crohn s Disease: A Single Institutional Experience in Taiwan. [J Soc Colon Rectal Surgeon (Taiwan) 2009;20:1-6]](/thumbs/87/96356608.jpg "Surgical Outcomes of Crohn s Disease: A Single Institutional Experience in Taiwan. [J Soc Colon Rectal Surgeon (Taiwan) 2009;20:1-6]") J Soc Colon Rectal Surgeon (Taiwan) March 2009 Original Article Surgical Outcomes of Crohn s Disease: A Single Institutional Experience in Taiwan Ta-Wen Hsu 1,2 Feng-Fan Chiang 1 Hwei-Ming Wang 1 1 Division
J Soc Colon Rectal Surgeon (Taiwan) March 2009 Original Article Surgical Outcomes of Crohn s Disease: A Single Institutional Experience in Taiwan Ta-Wen Hsu 1,2 Feng-Fan Chiang 1 Hwei-Ming Wang 1 1 Division
Clinical guideline Published: 10 October 2012 nice.org.uk/guidance/cg152
 Crohn's disease: management Clinical guideline Published: 10 October 2012 nice.org.uk/guidance/cg152 NICE 2018. All rights reserved. Subject to Notice of rights (https://www.nice.org.uk/terms-and-conditions#notice-ofrights).
Crohn's disease: management Clinical guideline Published: 10 October 2012 nice.org.uk/guidance/cg152 NICE 2018. All rights reserved. Subject to Notice of rights (https://www.nice.org.uk/terms-and-conditions#notice-ofrights).
Mucosal Healing in Crohn s Disease. Geert D Haens MD, PhD University Hospital Gasthuisberg University of Leuven Leuven, Belgium
 Mucosal Healing in Crohn s Disease Geert D Haens MD, PhD University Hospital Gasthuisberg University of Leuven Leuven, Belgium Mucosal Lesions in CD: General Features CD can affect the entire GI tract
Mucosal Healing in Crohn s Disease Geert D Haens MD, PhD University Hospital Gasthuisberg University of Leuven Leuven, Belgium Mucosal Lesions in CD: General Features CD can affect the entire GI tract
Slide 1 Medications in inflammatory bowel disease a primer for health care providers. Slide 2. Slide 3 Theory of pathogenesis. IBD - epidemiology
 Slide 1 Medications in inflammatory bowel disease a primer for health care providers Athos Bousvaros, MD Associate director Inflammatory Bowel Disease Center Boston Children s Hospital 617 355 2962 Slide
Slide 1 Medications in inflammatory bowel disease a primer for health care providers Athos Bousvaros, MD Associate director Inflammatory Bowel Disease Center Boston Children s Hospital 617 355 2962 Slide
Inflammatory Bowel Disease
 Inflammatory Bowel Disease Ali J. Olyaei, PharmD, BCPS Associate Professor of Medicine Director, Clinical Research Nephrology and Hypertension Associate Professor of Pharmacology School of Nursing Oregon
Inflammatory Bowel Disease Ali J. Olyaei, PharmD, BCPS Associate Professor of Medicine Director, Clinical Research Nephrology and Hypertension Associate Professor of Pharmacology School of Nursing Oregon
Case Report Squamous Cell Carcinoma Originating from a Crohn s Enterocutaneous Fistula
 Hindawi Case Reports in Surgery Volume 2017, Article ID 1929182, 4 pages https://doi.org/10.1155/2017/1929182 Case Report Squamous Cell Carcinoma Originating from a Crohn s Enterocutaneous Fistula Bogdan
Hindawi Case Reports in Surgery Volume 2017, Article ID 1929182, 4 pages https://doi.org/10.1155/2017/1929182 Case Report Squamous Cell Carcinoma Originating from a Crohn s Enterocutaneous Fistula Bogdan