LUTS & Cancer pathway. Mr Francis Thomas Urology Consultant DRI &BDGH
|
|
|
- Baldwin Wood
- 5 years ago
- Views:
Transcription
1 LUTS & Cancer pathway Mr Francis Thomas Urology Consultant DRI &BDGH
2 Topics Male and female LUTS Urinary retention Post void Residual urine Referral pathway LUTS Raised PSA Hematuria Services in community


3 Causes of LUTS in men BPE Life style habits Detrusor muscle weakness or overactivity, Prostate inflammation, UTI Prostate cancer Neurological diseases Medical causes Medications Renal BOO Pituitary LUTS Cardiac CNS BPE
4
5 Initial assessment History Predominant symptoms Life style General medical history Drug history Physical examination Abdomen DRE Genitalia IPSS score Urine dipstick
6 Initial assessment PSA- Abnormal prostate Patient concerns Serum creatinine- Suspect renal impairment Palpable bladder Nocturnal eneuresis Recurrent UTI H/o Renal stones USS KUB Suspecting renal failure

7 Conservative Management Reassurance and further information Life style interventions- mainly for storage symptoms Fluid balance Decrease tea/coffee/ alcohol/fizzy drinks Decrease night time drinks Bladder training Treat bowel constipation Reduce weight
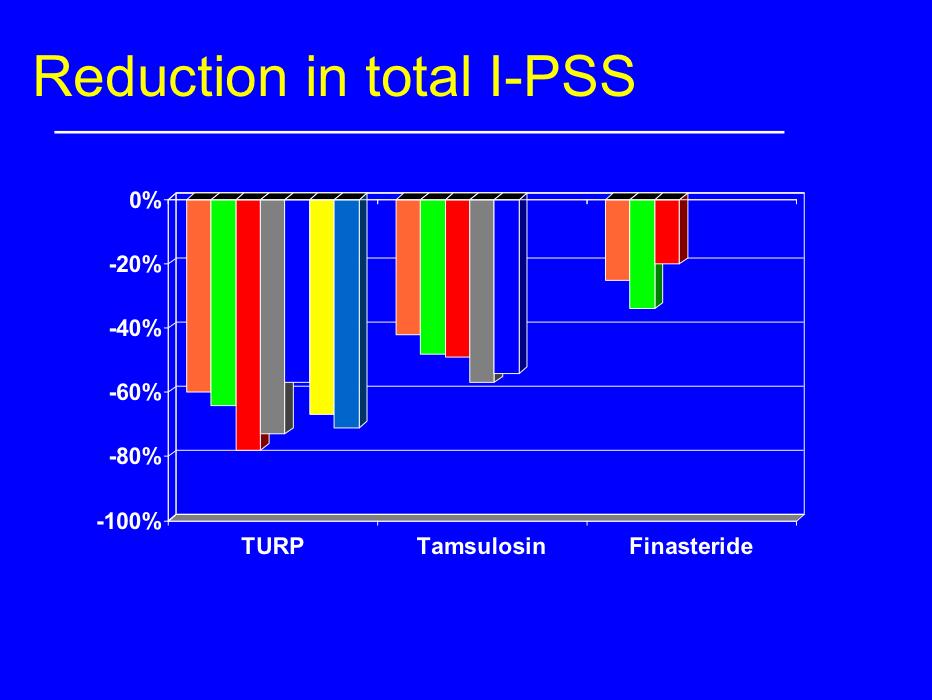
8 Drug treatment Alpha blocker for moderate to severe LUTS ( eg: Tamsulosin, Alfuzosin) Anticholinergics for OAB (Solifenacin, Tolteridine etc) 5 alpha reductase (Finasteride, Dutasteride) Prostate >30gm PSA >1.4ng/ml High risk for progression Combination therapy (alpha blocker+5 alpha reductase) Bothersome moderate to severe LUTS Prostate >30gm PSA >1.4ng/ml High risk for progression Alpha blocker+ Anticholinergic Persistent storage symptoms after treatment with alpha blocker alone
9 % Improvement in max Flow Improvement in Flow Q max Prazosin, Alfuzosin, Tamsulosin, Terazosin Buzelin 93 Buzelin 97 Lee 97 Na 98
10

11 Effect of finasteride on prostate volume Effect&of&finasteride&on&prostate&volume 20% 32% N"Engl"J"Med"
12

13 Mainly Voiding symptoms Mainly storage symptoms Voiding +storage symptoms Voiding symptoms +Erectile dysfunction Alpha blocker Life style advise Alpha blocker + anticholinergic+/- life style advise Alpha blocker + PDE5 inhibitor Large prostate PSA>1.4 Symptoms not improved Anticholinergics Alpha blocker + 5 alpha reductase
14 SCENARIOS 60 YEAR OLD MAN presenting with Slow stream, hesistancy, frequency Urinalysis negative PSA- 0.4 PR- moderate size BPE
15 55 year old man with urgency, frequency, hesitancy Urine positive for Nonvisible hematuria PR- moderate size bpe
16 Review after 4-6 weeks Continue active monitoring (reassurance and lifestyle modifications) Active intervention Drug therapy Referral to specialist
17 Referral Bothersome LUTS Not responded to drug treatment Complicated LUTS UTI Retention Renal impairment Lower urinary tract dysfunction Suspected malignancy Hematuria Abnormal prostate Raised PSA
18 Nocturia Waking to pass urine during the main sleep period Causes Nocturnal polyuria (It is defined as passing more than one third of your 24-hour urine output at night ) BPE UTI Medications Medical causes- cardiac failure Sleep apnoea-sleep disturbances
19 Nocturia-assessment History- Identify causative factors Lifestyle habits Fluid intake Assess with Frequency volume chart Urinalysis
20 Nocturia Lifestyle modifications Less fluid intake after 6 pm Reduce salt and sugar in diet Simple evening leg elevation or compression stockings can redistribute third space fluid Continuous positive airway pressure (CPAP) Alpha blockers- for BPE Anticholinergics-minimal effect Afternoon diuretics Desmopressin- oral or nasal spray ( monitor Sodium)
21 Retention of urine Acute retention < 1000 ml urine Painful Acute on chronic retention >1litre urine Painful Chronic retention RV>1 L, Palpable bladder painless High pressure chronic retention Painful or painless Renal failure, Hydroureteronephrosis (on USS KUB) Investigations +assessment Prostate examination Check U&E USS KUB if renal failure Management Acute retention Catheterise- GP practice/rdash/hospital Alpha blocker before TWOC (after 48hrs) C/C retention with symptoms ISC catheter Surgery C/C retention without symptoms (not catheterised) Active surveillance- monitor PV RV USS kidneys Serum creatinine
22 Retention of urine High pressure chronic retention Renal failure, Hydroureteronephrosis RX Catheterise Admit in hospital for monitoring LTC/Surgery
23 Effect of medical therapy on the development of AUR Effect&of&medical&therapy&on&the& development&of&aur Incidence:of:AUR/100:patient: years /1503 7/134 4/252 *14/1513 1/172 3/237 *1/126 2/179 0/249 4/811 placebo finasteride alpha7blocker PLESS ALF ALFIN PREDICT TAM Michel&MC.&Drugs&Today&2000J36(Suppl.F):11P13
24 75 year old man presents with difficulty passing urine through out night. Fit and well O/E palpable bladder
25 AUR/TWOC Community pathway -RDASH AUR in community DRI Urology Department Patient presenting with AUR in communityrefer to unplanned care services for catheterisation and then seen in RDASH clinic for assessment /TWOC and further referral to Urology Patients discharged from hospitals with catheter referred to RDASH clinic for TWOC or for further catheter care Patients given clear advise and support with catheter passport and contact details of RDASH clinic TWOC from community RDASH/ UNPLANNED CARE ISC/CATHETER PROBLEMS TWOC from hospital
26 Post void scans /USS KUB Post void residuals No minimal or maximum values Take into consideration Symptoms UTI Renal function Treatment depends on whether symptomatic or not Renal function
27 Surgery- mainly storage symptoms Failed conservative and drug treatment Urodynamic studies to assess bladder Botulinum toxin injection Sacral nerve neuromodulation Cystoplasty Willing and able to self catheterize Detrusor overactivity Small capacity bladder Artificial sphincter- stress UI Urinary diversion Failed cystoplasty Failed sacral nerve stimulation
28 Surgery- voiding symptoms -Severe voiding symptoms -Failed drug and conservative treatment TURP Monopolar/bipolar Green light Prostate embolisation HoLEP Uro-lift Aqua ablation Open prostatectomy-> gm prostate
29 Female LUTS Mr Francis Thomas Consultant Urologist DRI &BDGH
30 Definitions Urgency -a sudden compelling desire to urinate that is difficult to delay Urgency UI is involuntary urine leakage accompanied or immediately preceded by urgency Stress UI is involuntary urine leakage on effort or exertion or on sneezing or coughing. Mixed UI is involuntary urine leakage associated with both urgency and exertion, effort, sneezing or coughing. Overactive bladder (OAB) is defined as urgency that occurs with or without urgency UI and usually with frequency and nocturia. OAB that occurs with incontinence is known as OAB wet OAB that occurs without incontinence is known as 'OAB dry

31 History Duration Type of incontinence Triggering factors- uti, stress Obstructive symptoms Pads usage numbers, size, wetness Lifestyle factors-caffeine, smoking, alcohol Menstural/obstetric Bowel habits Previous pelvic surgery/radiotherapy Drugs Medical problems diabetes etc

32 Assessment Frequency volume chart Minimum of 3 days to include rest days and working days Fluid dairy Urinalysis Post void residuals Pelvic and speculum examination Cough test USS pelvis
33 Specialist opinion Haematuria Recurrent UTI Persisting bladder or urethral pain Pelvic mass/palpable bladder Urogenital fistula Previous continence surgery Fecal incontinence Neurological disease Previous Pelvic cancer Previous pelvic radiotherapy
34 Treatment Categorise the symptoms and diagnose the type of incontinence SUI,UI,MIXED OR OAB Treat the predisposing and precipitating factors UTI, Constipation, Loose weight (BMI>30) Lifestyle advice Reduce caffeine/fizzydrinks/smoking Fluid intake 1.5-2litres Bladder training exercises Pelvic floor exercises If mixed incontinence start treating the predominant symptom SUI with OAB Treat OAB symptoms prior to treatment of SUI Prolapse that is symptomatic and is visible and or below the introitus should be treated
35 Treatment-Conservative measures BLADDER TRAINING -6 weeks-3 months There are many different regimes, but they all involve suppressing the feelings of urinary urgency. Require a few months training to reach its full potential. Timed voiding Pelvic floor muscle training(pfmt) Assess pelvic muscle tone Supervised PFMT- 3months 8 contractions each held for 8 seconds three times a day RDASH clinic and physiotherapy department- offers bladder training and PFMT advice
36 Treatment PADS/CATHETERS/URINALS -Use them only as Coping strategy pending assessment and treatment An adjunct to ongoing treatment When all treatment options have been explored and failed
37 Medications Start with one with low acquisition cost Most of anticholinergics have same side effect profile Oxybutynin-(not in elderly) Tolteridine - Darifenacin- Solifenacin- Trospium chloride Fesoteridine Mirabegron- beta 3 agonist Mirabegron +anticholinergic Topical oestrogens for vaginal atrophy-6 weeks to 3months OAB DRUGS Counsel about success and associated common side effects Some side effects indicate that the treatment is starting to have an effect May take up to 4 weeks for medicines to start working Need to continue with bladder training /PFMT along with OAB drugs 4 week review and then 6month review Try atleast two drugs before referral to specialist centres
38 Referral- &secondary care If OAB symptoms, SUI/mixed incontinence not responding to bladder training, PFMT and OAB drugs OAB MDT Urodynamics Intravesical Botulinum toxin Posterior tibial nerve stimulation Sacral neuro modulation Augmentation cystoplasty Urinary diversion-ileal conduit SUI MDT Urodynamics Rectus fascial slings Colposuspension Urethral bulking agents Artificial sphincters Urinary diversion


39 Hospital pathway Women with bladder symptoms Community pathway- RDASH Urinalysis GP Urinalysis Clinical examination & medications Urology clinic Flow rate & bladder scan Pelvic floor exercise RDASH clinic Flow rate & bladder scan Fluid and dietary advise Clinical examination & medications Fluid and dietary advise Referred for Pelvic floor exercises Referred to Gynaecologist if prolapse etc-- Referred to Urology/Gynaecology MDT as appropriate Discharged if symptoms resolved Clinic revisit 6-8 weeks
40 Clinical scenarios 40 year old lady presenting with frequency,urgency, incontinence for 3 months. Otherwise fit and well.
41 40 year old lady presenting with frequency,urgency, incontinence for 3 months. Otherwise fit and well. Already on medications (anticholinergic) for 2 months but symptoms not better.
42 65 year old lady with frequency, urgency and hesitancy, otherwise fit and well. O/E microscopic hematuria, vaginal atrophy.
43 Cancer 2 WW Pathways
44 Hematuria referral 2 ww referral >45 yrs of age hematuria without UTI Non visible hematuria (NVH) >60 yrs and have either dysuria or raised WBC count Non urgent referral Visible hematuria <45 yrs of age Non visible hematuria <60 yrs Recurrent UTI NVH with proteinuria / renal failure Refer renal physician
45 3 CLINIC VISITS Current pathway Abnormal PSA One stop PSA clinic Abnormal PSA Seen in clinic- 2WW MRI PROSTATE One stop PSA clinic 2WW MRI done and reported same day PROSTATE BIOPSY- same day MRI MDT PROSTATE BIOPSY MDT ONCOLOGY ONCOLOGY MDT CLINIC CLINIC
46 South Yorkshire, Bassetlaw and North Derbyshire Cancer Alliance Urology Fast Track Referral 2 Week Wait
47 Prostate Cancer All Patients should have PSA and U&E/eGFR blood tests, urine dipstick and Digital Rectal Examination (DRE) 1. Asymptomatic patient requesting PSA test Require two blood tests, at least 4 weeks apart Informed consent: e.g. Prostate Cancer Risk Management Programme (PCRMP) leaflet Refer as 2ww if: Both PSA >3.0 (for all ages) (For raised PSA in men with significant co-morbidities, performance status >3 or life expectancy <10 years, consider discussion with patient/family/carers and/or a specialist before urgent referral.)
48 Prostate Cancer All Patients should have PSA and U&E/eGFR blood tests, urine dipstick and Digital Rectal Examination (DRE) 2. Symptomatic patient: Prostatic symptoms/luts Please Wait atleast 6 weeks following treated UTI before undertaking PSA test. Refer if: Abnormal DRE Or Both PSA >3.0 (Obtain two PSA tests, at least 4 weeks apart) (For raised PSA in men with significant co-morbidities, performance status >3 or life expectancy <10 years, consider discussion with patient/family/carers and/or a specialist before urgent referral.) Informed consent: e.g. (PCRMP) leaflet provided
49 Prostate Cancer All Patients should have PSA and U&E/eGFR blood tests, urine dipstick and Digital Rectal Examination (DRE) 3. Symptomatic patient: Suspected distant metastases Refer: If abnormal DRE Or a single PSA >20 In this group of patients if PSA result is between suggest repeat and review in 4 weeks with second PSA test. If repeat PSA level <10 Constitutional symptoms are unlikely to be directly due to prostate cancer but consider criteria above.
50 Prostate Cancer All Patients should have PSA and U&E/eGFR blood tests, urine dipstick and Digital Rectal Examination (DRE) 4. Prostate feels malignant (Firm, hard, nodular or craggy) on (DRE) One PSA is sufficient, Any PSA value
Lower Urinary Tract Symptoms K Kuruvilla Zachariah Associate Specialist
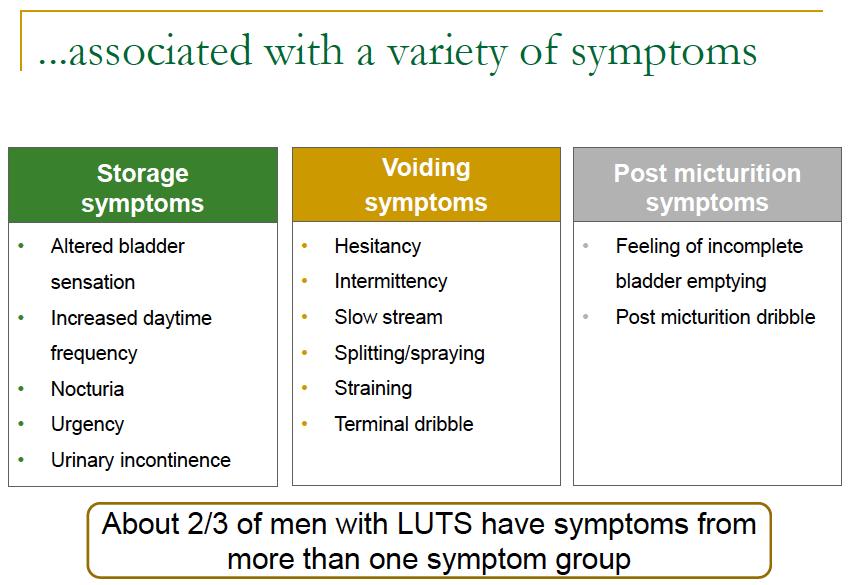
 Lower Urinary Tract Symptoms K Kuruvilla Zachariah Associate Specialist Lower Urinary Tract Symptoms Storage Symptoms Frequency, urgency, incontinence, Nocturia Voiding Symptoms Hesitancy, poor flow, intermittency,
Lower Urinary Tract Symptoms K Kuruvilla Zachariah Associate Specialist Lower Urinary Tract Symptoms Storage Symptoms Frequency, urgency, incontinence, Nocturia Voiding Symptoms Hesitancy, poor flow, intermittency,
Policy for Prostatism/Lower Urinary Tract Symptoms in men
 NHS Halton Clinical Commissioning Group NHS Liverpool Clinical Commissioning Group NHS St Helens Clinical Commissioning Group NHS South Sefton Clinical Commissioning Group NHS Southport and Formby Clinical
NHS Halton Clinical Commissioning Group NHS Liverpool Clinical Commissioning Group NHS St Helens Clinical Commissioning Group NHS South Sefton Clinical Commissioning Group NHS Southport and Formby Clinical
Case studies: LUTS. Case 1 history. Case 1 - questions. Case 1 - outcome. Case 2 - history. Case 1 learning point 14/07/2015 DR JON REES
 Case 1 history Case studies: LUTS DR JON REES A 49 year old male comes to see you he has had gradual deterioration of his flow over the last few years- he saw a colleague of yours 6 weeks ago who recorded
Case 1 history Case studies: LUTS DR JON REES A 49 year old male comes to see you he has had gradual deterioration of his flow over the last few years- he saw a colleague of yours 6 weeks ago who recorded
Clinical guideline Published: 23 May 2010 nice.org.uk/guidance/cg97
 Lower urinary tract symptoms in men: management Clinical guideline Published: 23 May 2010 nice.org.uk/guidance/cg97 NICE 2017. All rights reserved. Subject to Notice of rights (https://www.nice.org.uk/terms-and-conditions#notice-ofrights).
Lower urinary tract symptoms in men: management Clinical guideline Published: 23 May 2010 nice.org.uk/guidance/cg97 NICE 2017. All rights reserved. Subject to Notice of rights (https://www.nice.org.uk/terms-and-conditions#notice-ofrights).
Overactive Bladder Syndrome
 Overactive Bladder Syndrome behavioural modifications to pharmacological and surgical treatments Dr Jos Jayarajan Urologist Austin Health, Eastern Health Warringal Private, Northpark Private, Epworth Overactive
Overactive Bladder Syndrome behavioural modifications to pharmacological and surgical treatments Dr Jos Jayarajan Urologist Austin Health, Eastern Health Warringal Private, Northpark Private, Epworth Overactive
BPH / LUTS. Prevalence. Prevalence of BPH. It is abnormal NOT to have benign growth of the prostate with increasing age. Prevalence.
 BPH / LUTS Dr Jonny Coxon MA MD MRCS MRCGP DRCOG FECSM Beaconsfield Medical Practice, Brighton & Brighton & Sussex Universities NHS Trust As man draws near the common goal Can anything be sadder Than he
BPH / LUTS Dr Jonny Coxon MA MD MRCS MRCGP DRCOG FECSM Beaconsfield Medical Practice, Brighton & Brighton & Sussex Universities NHS Trust As man draws near the common goal Can anything be sadder Than he
Male Lower Urinary Tract Symptoms: Management in primary care and beyond. Daniel Cohen PhD FRCS(Urol) Consultant Urological Surgeon
 Consultant Urological Surgeon") Male Lower Urinary Tract Symptoms: Management in primary care and beyond Daniel Cohen PhD FRCS(Urol) Consultant Urological Surgeon 1 LUTS Very common: 1/3 men over age of 50 have moderate to severe LUTS
Male Lower Urinary Tract Symptoms: Management in primary care and beyond Daniel Cohen PhD FRCS(Urol) Consultant Urological Surgeon 1 LUTS Very common: 1/3 men over age of 50 have moderate to severe LUTS
As man draws near the common goal Can anything be sadder Than he who, master of his soul Is servant to his bladder LUTS 2. Prevalence of BPH LUTS 5
 BPH / LUTS Dr Jonny Coxon MA MD MRCS MRCGP DRCOG Beaconsfield Medical Practice, Brighton As man draws near the common goal Can anything be sadder Than he who, master of his soul Is servant to his bladder
BPH / LUTS Dr Jonny Coxon MA MD MRCS MRCGP DRCOG Beaconsfield Medical Practice, Brighton As man draws near the common goal Can anything be sadder Than he who, master of his soul Is servant to his bladder
URINARY INCONTINENCE. Urology Division, Surgery Department Medical Faculty, University of Sumatera Utara
 URINARY INCONTINENCE Urology Division, Surgery Department Medical Faculty, University of Sumatera Utara Definition The involuntary loss of urine May denote a symptom, a sign or a condition Symptom the
URINARY INCONTINENCE Urology Division, Surgery Department Medical Faculty, University of Sumatera Utara Definition The involuntary loss of urine May denote a symptom, a sign or a condition Symptom the
Various Types. Ralph Boling, DO, FACOG
 Various Types Ralph Boling, DO, FACOG The goal of this lecture is to increase assessment and treatment abilities for physicians managing urinary incontinence (UI) patients. 1. Effectively communicate with
Various Types Ralph Boling, DO, FACOG The goal of this lecture is to increase assessment and treatment abilities for physicians managing urinary incontinence (UI) patients. 1. Effectively communicate with
Priorities Forum Statement GUIDANCE
 Priorities Forum Statement Number 61 Subject The management of female incontinence Date of decision May 2016 Date refreshed May 2017 Date of review May 2019 Introduction: GUIDANCE Urinary incontinence
Priorities Forum Statement Number 61 Subject The management of female incontinence Date of decision May 2016 Date refreshed May 2017 Date of review May 2019 Introduction: GUIDANCE Urinary incontinence
MANAGING BENIGN PROSTATIC HYPERTROPHY IN PRIMARY CARE DR GEORGE G MATHEW CONSULTANT FAMILY PHYSICIAN FELLOW IN SEXUAL & REPRODUCTIVE HEALTH
 MANAGING BENIGN PROSTATIC HYPERTROPHY IN PRIMARY CARE DR GEORGE G MATHEW CONSULTANT FAMILY PHYSICIAN FELLOW IN SEXUAL & REPRODUCTIVE HEALTH INTRODUCTION (1) Part of male sexual reproductive organ Size
MANAGING BENIGN PROSTATIC HYPERTROPHY IN PRIMARY CARE DR GEORGE G MATHEW CONSULTANT FAMILY PHYSICIAN FELLOW IN SEXUAL & REPRODUCTIVE HEALTH INTRODUCTION (1) Part of male sexual reproductive organ Size
Management of LUTS. Simon Woodhams February 2012
 Management of LUTS Simon Woodhams February 2012 The management of lower urinary tract symptoms (LUTS) in men Implementing NICE guidance May 2010 NICE clinical guideline 97 Background Lower urinary tract
Management of LUTS Simon Woodhams February 2012 The management of lower urinary tract symptoms (LUTS) in men Implementing NICE guidance May 2010 NICE clinical guideline 97 Background Lower urinary tract
Urinary Incontinence. Lora Keeling and Byron Neale
 Urinary Incontinence Lora Keeling and Byron Neale Not life threatening. Introduction But can have a huge impact on quality of life. Two main types of urinary incontinence (UI). Stress UI leakage on effort,
Urinary Incontinence Lora Keeling and Byron Neale Not life threatening. Introduction But can have a huge impact on quality of life. Two main types of urinary incontinence (UI). Stress UI leakage on effort,
LUTS A plea for a holistic approach. HUBERT GALLAGHER, MCh; FRCSI, FRCSI(Urol) Head of Urology Beacon Hospital
 Head of Urology Beacon Hospital") LUTS A plea for a holistic approach. HUBERT GALLAGHER, MCh; FRCSI, FRCSI(Urol) Head of Urology Beacon Hospital LUTS- Classification Men LUTS can be divided into: Storage Voiding Frequency Nocturia Urgency
LUTS A plea for a holistic approach. HUBERT GALLAGHER, MCh; FRCSI, FRCSI(Urol) Head of Urology Beacon Hospital LUTS- Classification Men LUTS can be divided into: Storage Voiding Frequency Nocturia Urgency
Lower Urinary Tract Symptoms (LUTS) and Nurse-Led Clinics. Sean Diver Urology Advanced Nurse Practitioner candidate Letterkenny University Hospital
 and Nurse-Led Clinics. Sean Diver Urology Advanced Nurse Practitioner candidate Letterkenny University Hospital") Lower Urinary Tract Symptoms (LUTS) and Nurse-Led Clinics Sean Diver Urology Advanced Nurse Practitioner candidate Letterkenny University Hospital 01/02/2018 Lower Urinary Tract Symptoms LUTS - one of
Lower Urinary Tract Symptoms (LUTS) and Nurse-Led Clinics Sean Diver Urology Advanced Nurse Practitioner candidate Letterkenny University Hospital 01/02/2018 Lower Urinary Tract Symptoms LUTS - one of
Bladder dysfunction in ALD and AMN
 Bladder dysfunction in ALD and AMN Sara Simeoni, MD Department of Uro-Neurology National Hospital for Neurology and Neurosurgery Queen Square, London 10:15 Dr Sara Simeoni- Bladder issues for AMN patients
Bladder dysfunction in ALD and AMN Sara Simeoni, MD Department of Uro-Neurology National Hospital for Neurology and Neurosurgery Queen Square, London 10:15 Dr Sara Simeoni- Bladder issues for AMN patients
Voiding Dysfunction Block lecture, 5 th year student. Choosak Pripatnanont, Department of Surgery, PSU.
 Voiding Dysfunction 2009 Block lecture, 5 th year student. Choosak Pripatnanont, Department of Surgery, PSU. Objectives Understand and explain physiologic function and dysfunction of lower urinary tract.
Voiding Dysfunction 2009 Block lecture, 5 th year student. Choosak Pripatnanont, Department of Surgery, PSU. Objectives Understand and explain physiologic function and dysfunction of lower urinary tract.
Disclosures. Geriatric Incontinence and Voiding Dysfunction. Agenda. Agenda. UI: a Geriatric Syndrome. Geriatric Syndromes 9/7/2018.
 Disclosures Geriatric Incontinence and Voiding Dysfunction None Shachi Tyagi MD, MS Assistant Professor Division of Geriatric Medicine University of Pittsburgh Medical Center UI: a Geriatric Syndrome Geriatric
Disclosures Geriatric Incontinence and Voiding Dysfunction None Shachi Tyagi MD, MS Assistant Professor Division of Geriatric Medicine University of Pittsburgh Medical Center UI: a Geriatric Syndrome Geriatric
Urogynecology in EDS. Joan L. Blomquist, MD Greater Baltimore Medical Center August 2018
 Urogynecology in EDS Joan L. Blomquist, MD Greater Baltimore Medical Center August 2018 One in three like me Voiding Issues Frequency/Urgency Urinary Incontinence neurogenic bladder Neurologic supply
Urogynecology in EDS Joan L. Blomquist, MD Greater Baltimore Medical Center August 2018 One in three like me Voiding Issues Frequency/Urgency Urinary Incontinence neurogenic bladder Neurologic supply
Mr. GIT KAH ANN. Pakar Klinikal Urologi Hospital Kuala Lumpur.
 Mr. GIT KAH ANN Pakar Klinikal Urologi Hospital Kuala Lumpur drgitka@yahoo.com 25 Jan 2007 HIGHLIGHTS Introduction ICS Definition Making a Diagnosis Voiding Chart Investigation Urodynamics Ancillary Investigations
Mr. GIT KAH ANN Pakar Klinikal Urologi Hospital Kuala Lumpur drgitka@yahoo.com 25 Jan 2007 HIGHLIGHTS Introduction ICS Definition Making a Diagnosis Voiding Chart Investigation Urodynamics Ancillary Investigations
Management of Female Stress Incontinence
 Management of Female Stress Incontinence Dr. Arvind Goyal Associate Professor (Urology& Renal Transplant) Dayanand Medical College & Hospital, Ludhiana, Punjab, India Stress Incontinence Involuntary loss
Management of Female Stress Incontinence Dr. Arvind Goyal Associate Professor (Urology& Renal Transplant) Dayanand Medical College & Hospital, Ludhiana, Punjab, India Stress Incontinence Involuntary loss
Primary Care management of Overactive Bladder (OAB)
") DERBYSHIRE JOINT AREA PRESCRIBING COMMITTEE (JAPC) Primary Care management of Overactive Bladder (OAB) Prescribing Tips All medicines for OAB have similar dose-related efficacy. More than one agent (up
DERBYSHIRE JOINT AREA PRESCRIBING COMMITTEE (JAPC) Primary Care management of Overactive Bladder (OAB) Prescribing Tips All medicines for OAB have similar dose-related efficacy. More than one agent (up
Content. Terminology Anatomy Aetiology Presentation Classification Management
 Prolapse Content Terminology Anatomy Aetiology Presentation Classification Management Terminology Prolapse Descent of pelvic organs into the vagina Cystocele ant. vaginal wall involving bladder Uterine
Prolapse Content Terminology Anatomy Aetiology Presentation Classification Management Terminology Prolapse Descent of pelvic organs into the vagina Cystocele ant. vaginal wall involving bladder Uterine
Management of OAB. Lynsey McHugh. Consultant Urological Surgeon. Lancashire Teaching Hospitals
 Management of OAB Lynsey McHugh Consultant Urological Surgeon Lancashire Teaching Hospitals Summary Physiology Epidemiology Definitions NICE guidelines Evaluation Conservative management Medical management
Management of OAB Lynsey McHugh Consultant Urological Surgeon Lancashire Teaching Hospitals Summary Physiology Epidemiology Definitions NICE guidelines Evaluation Conservative management Medical management
All about the Prostate
 MEN S HEALTH Dr Nick Pendleton January 16 th 2018 All about the Prostate 1 What does it do? Functions of the Prostate 1. Secretes Prostatic Fluid slightly alkaline fluid, 30% of volume of seminal fluid,
MEN S HEALTH Dr Nick Pendleton January 16 th 2018 All about the Prostate 1 What does it do? Functions of the Prostate 1. Secretes Prostatic Fluid slightly alkaline fluid, 30% of volume of seminal fluid,
Objectives. Prevalence of Urinary Incontinence URINARY INCONTINENCE: EVALUATION AND CURRENT TREATMENT OPTIONS
 URINARY INCONTINENCE: EVALUATION AND CURRENT TREATMENT OPTIONS Lisa S Pair, MSN, CRNP Division of Urogynecology and Pelvic Reconstructive Surgery Department of Obstetrics and Gynecology University of Alabama
URINARY INCONTINENCE: EVALUATION AND CURRENT TREATMENT OPTIONS Lisa S Pair, MSN, CRNP Division of Urogynecology and Pelvic Reconstructive Surgery Department of Obstetrics and Gynecology University of Alabama
John Laughlin 4 th year Cardiff University Medical Student
 John Laughlin 4 th year Cardiff University Medical Student Prolapse/incontinence You need to know: Pelvic floor anatomy in relation to uterovaginal support and continence The classification of uterovaginal
John Laughlin 4 th year Cardiff University Medical Student Prolapse/incontinence You need to know: Pelvic floor anatomy in relation to uterovaginal support and continence The classification of uterovaginal
Diagnosis and Mangement of Nocturia in Adults
 Diagnosis and Mangement of Nocturia in Adults Christopher Chapple Professor of Urology Sheffield Teaching Hospitals University of Sheffield Sheffield Hallam University UK 23 rd October 2015 Terminology
Diagnosis and Mangement of Nocturia in Adults Christopher Chapple Professor of Urology Sheffield Teaching Hospitals University of Sheffield Sheffield Hallam University UK 23 rd October 2015 Terminology
Urogynaecology. Colm McAlinden
 Urogynaecology Colm McAlinden Definitions Urinary incontinence compliant of any involuntary leakage of urine with many different causes Two main types: Stress Urge Definitions Nocturia: More than a single
Urogynaecology Colm McAlinden Definitions Urinary incontinence compliant of any involuntary leakage of urine with many different causes Two main types: Stress Urge Definitions Nocturia: More than a single
Patient Information. Basic Information on Overactive Bladder Symptoms. pubic bone. urethra. scrotum. bladder. vaginal canal
 Patient Information English Basic Information on Overactive Bladder Symptoms The underlined terms are listed in the glossary. What is the bladder? pubic bone bladder seminal vesicles prostate rectum The
Patient Information English Basic Information on Overactive Bladder Symptoms The underlined terms are listed in the glossary. What is the bladder? pubic bone bladder seminal vesicles prostate rectum The
Overactive bladder syndrome (OAB)
") Service: Urology Overactive bladder syndrome (OAB) Exceptional healthcare, personally delivered What is OAB? An overactive bladder or OAB is where a person regularly gets a sudden and compelling need or
Service: Urology Overactive bladder syndrome (OAB) Exceptional healthcare, personally delivered What is OAB? An overactive bladder or OAB is where a person regularly gets a sudden and compelling need or
Management of male LUTS in general practice
 17 Management of male LUTS in general practice MARK J. SPEAKMAN AND FAITH MCMEEKIN The initial management of lower urinary tract symptoms in men is usually carried out in primary care. The authors explain
17 Management of male LUTS in general practice MARK J. SPEAKMAN AND FAITH MCMEEKIN The initial management of lower urinary tract symptoms in men is usually carried out in primary care. The authors explain
Urinary Incontinence. Vibhash Mishra Consultant Urological Surgeon Royal Free Hospital
 Urinary Incontinence Vibhash Mishra Consultant Urological Surgeon Royal Free Hospital Affects women of all ages Impacts physical, psychological & social wellbeing Impact on families & carers Costs the
Urinary Incontinence Vibhash Mishra Consultant Urological Surgeon Royal Free Hospital Affects women of all ages Impacts physical, psychological & social wellbeing Impact on families & carers Costs the
Diagnostic approach to LUTS in men. Prof Dato Dr. Zulkifli Md Zainuddin Consultant Urologist / Head Of Urology Unit UKM Medical Center
 Diagnostic approach to LUTS in men Prof Dato Dr. Zulkifli Md Zainuddin Consultant Urologist / Head Of Urology Unit UKM Medical Center Classification of LUTS Storage symptoms Voiding symptoms Post micturition
Diagnostic approach to LUTS in men Prof Dato Dr. Zulkifli Md Zainuddin Consultant Urologist / Head Of Urology Unit UKM Medical Center Classification of LUTS Storage symptoms Voiding symptoms Post micturition
EAU GUIDELINES ON URINARY INCONTINENCE
 EU GUIDELINES ON URINRY INONTINENE (Limited text update March 2017) F.. urkhard (hair), J.L.H.R. osch, F. ruz, G.E. Lemack,.K. Nambiar, N. Thiruchelvam,. Tubaro Guidelines ssociates: D. mbühl, D. edretdinova,
EU GUIDELINES ON URINRY INONTINENE (Limited text update March 2017) F.. urkhard (hair), J.L.H.R. osch, F. ruz, G.E. Lemack,.K. Nambiar, N. Thiruchelvam,. Tubaro Guidelines ssociates: D. mbühl, D. edretdinova,
AUCKLAND REGIONAL UROLOGY GUIDELINES AND REFERRAL RECOMMENDATIONS
 AUCKLAND REGIONAL UROLOGY GUIDELINES AND REFERRAL RECOMMENDATIONS This document outlines the urological conditions currently funded at Auckland District Health Board (ADHB), Counties Manukau District Health
AUCKLAND REGIONAL UROLOGY GUIDELINES AND REFERRAL RECOMMENDATIONS This document outlines the urological conditions currently funded at Auckland District Health Board (ADHB), Counties Manukau District Health
The management of lower urinary tract symptoms in men
 The management of lower urinary tract symptoms in men NICE guideline Draft for consultation, August 2009 If you wish to comment on this version of the guideline, please be aware that all the supporting
The management of lower urinary tract symptoms in men NICE guideline Draft for consultation, August 2009 If you wish to comment on this version of the guideline, please be aware that all the supporting
Newcastle upon Tyne, Gateshead and Northumbria Urology guidelines
 Newcastle upon Tyne, Gateshead and Northumbria Urology guidelines INTRODUCTION This document is an update of the NORTH OF TYNE AND GATESHEAD GUIDELINES FOR MANAGEMENT OF COMMON UROLOGICAL CONDITIONS IN
Newcastle upon Tyne, Gateshead and Northumbria Urology guidelines INTRODUCTION This document is an update of the NORTH OF TYNE AND GATESHEAD GUIDELINES FOR MANAGEMENT OF COMMON UROLOGICAL CONDITIONS IN
LUTS after TURP: How come and how to manage? Matthias Oelke
 LUTS after TURP: How come and how to manage? Matthias Oelke Department of Urology Global Congress on LUTD, Rome, 26 th June 2015 Disclosures Consultant, speaker, trial participant and/or research grants
LUTS after TURP: How come and how to manage? Matthias Oelke Department of Urology Global Congress on LUTD, Rome, 26 th June 2015 Disclosures Consultant, speaker, trial participant and/or research grants
NEUROGENIC BLADDER. Dr Harriet Grubb Dr Alison Seymour Dr Alexander Joseph
 NEUROGENIC BLADDER Dr Harriet Grubb Dr Alison Seymour Dr Alexander Joseph OUTLINE Definition Anatomy and physiology of bladder function Types of neurogenic bladder Assessment and management Complications
NEUROGENIC BLADDER Dr Harriet Grubb Dr Alison Seymour Dr Alexander Joseph OUTLINE Definition Anatomy and physiology of bladder function Types of neurogenic bladder Assessment and management Complications
EAU GUIDELINES ON URINARY INCONTINENCE
 EU GUIDELINES ON URINRY INONTINENE (Partial text update March 2016) F.. urkhard (hair), M.G. Lucas, L.. erghmans, J.L.H.R. osch, F. ruz, G.E. Lemack,.K. Nambiar,.G. Nilsson, R. Pickard,. Tubaro Guidelines
EU GUIDELINES ON URINRY INONTINENE (Partial text update March 2016) F.. urkhard (hair), M.G. Lucas, L.. erghmans, J.L.H.R. osch, F. ruz, G.E. Lemack,.K. Nambiar,.G. Nilsson, R. Pickard,. Tubaro Guidelines
Overview. Urology Dine and Learn: Erectile Dysfunction & Benign Prostatic Hyperplasia. Iain McAuley September 15, 2014
 Urology Dine and Learn: Erectile Dysfunction & Benign Prostatic Hyperplasia Iain McAuley September 15, 2014 Overview Review of the most recent guidelines for ED and BPH ED Guidelines CUA 2006 AUA 2011
Urology Dine and Learn: Erectile Dysfunction & Benign Prostatic Hyperplasia Iain McAuley September 15, 2014 Overview Review of the most recent guidelines for ED and BPH ED Guidelines CUA 2006 AUA 2011
NON-Neurogenic Chronic Urinary Retention AUA White Paper
 NON-Neurogenic Chronic Urinary Retention AUA White Paper Great Lakes SUNA Inside Urology March 16, 2018 Michelle J. Lajiness FNP-BC Nurse Practitioner DMC Urology Incidence Really unknown Lack consensus
NON-Neurogenic Chronic Urinary Retention AUA White Paper Great Lakes SUNA Inside Urology March 16, 2018 Michelle J. Lajiness FNP-BC Nurse Practitioner DMC Urology Incidence Really unknown Lack consensus
Overactive Bladder: Diagnosis and Approaches to Treatment
 Overactive Bladder: Diagnosis and Approaches to Treatment A Hidden Condition* Many Many patients self-manage by voiding frequently, reducing fluid intake, and wearing pads Nearly Nearly two-thirds thirds
Overactive Bladder: Diagnosis and Approaches to Treatment A Hidden Condition* Many Many patients self-manage by voiding frequently, reducing fluid intake, and wearing pads Nearly Nearly two-thirds thirds
Diagnosis and treatment of overactive bladder (non-neurogenic) in adults: AUA/SUFU guideline.
 in adults: AUA/SUFU guideline.") Diagnosis and treatment of overactive bladder (non-neurogenic) in adults: AUA/SUFU guideline. TARGET POPULATION Eligibility Decidable (Y or N) Inclusion Criterion non-neurogenic OAB Exclusion Criterion
Diagnosis and treatment of overactive bladder (non-neurogenic) in adults: AUA/SUFU guideline. TARGET POPULATION Eligibility Decidable (Y or N) Inclusion Criterion non-neurogenic OAB Exclusion Criterion
Overactive bladder can result from one or more of the following causes:
 Overactive bladder can affect people of any age; however, it is more common in older people. Effective treatments are available and seeing your doctor for symptoms of overactive bladder often results in
Overactive bladder can affect people of any age; however, it is more common in older people. Effective treatments are available and seeing your doctor for symptoms of overactive bladder often results in
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE SCOPE
 NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE 1 Guideline title SCOPE Urinary incontinence in women: the management of urinary incontinence in women 1.1 Short title Urinary incontinence in women
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE 1 Guideline title SCOPE Urinary incontinence in women: the management of urinary incontinence in women 1.1 Short title Urinary incontinence in women
Prolapse and Urogynae Incontinence. Lucy Tiffin and Hannah Wheldon-Holmes
 Prolapse and Urogynae Incontinence Lucy Tiffin and Hannah Wheldon-Holmes 66 year old woman with incontinence PC: 7 year Hx of urgency, frequency, nocturia (incl. incontinence at night), and stress incontinence
Prolapse and Urogynae Incontinence Lucy Tiffin and Hannah Wheldon-Holmes 66 year old woman with incontinence PC: 7 year Hx of urgency, frequency, nocturia (incl. incontinence at night), and stress incontinence
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Centre for Clinical Practice Surveillance Programme
 NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Centre for Clinical Practice Surveillance Programme Clinical guideline CG97: The management of lower urinary tract symptoms in men Publication date May
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Centre for Clinical Practice Surveillance Programme Clinical guideline CG97: The management of lower urinary tract symptoms in men Publication date May
Telford and Wrekin Clinical Commissioning Group
 Telford and Wrekin Clinical Commissioning Group Agenda Item 9.2 CLINICAL COMMISSIONING GROUP GOVERNANCE BOARD EXECUTIVE SUMMARY DATE: 9 th April 2013 TITLE OF PAPER: Continence pathway and Referral letter
Telford and Wrekin Clinical Commissioning Group Agenda Item 9.2 CLINICAL COMMISSIONING GROUP GOVERNANCE BOARD EXECUTIVE SUMMARY DATE: 9 th April 2013 TITLE OF PAPER: Continence pathway and Referral letter
Overactive bladder. Information for patients from Urogynaecology
 Overactive bladder Information for patients from Urogynaecology An overactive bladder (OAB) is a very common problem. It can cause distressing symptoms that are difficult to control. These can include
Overactive bladder Information for patients from Urogynaecology An overactive bladder (OAB) is a very common problem. It can cause distressing symptoms that are difficult to control. These can include
INCONTINENCE. Continence and Pelvic Floor Rehabilitation TYPES OF INCONTINENCE STRESS INCONTINENCE STRESS INCONTINENCE STRESS INCONTINENCE 11/08/2015
 INCONTINENCE Continence and Pelvic Floor Rehabilitation Dr Irmina Nahon PhD Pelvic Floor Physiotherapist www.nahonpfed.com.au Defined as the accidental and inappropriate passage of urine or faeces (ICI
INCONTINENCE Continence and Pelvic Floor Rehabilitation Dr Irmina Nahon PhD Pelvic Floor Physiotherapist www.nahonpfed.com.au Defined as the accidental and inappropriate passage of urine or faeces (ICI
Management of LUTS after TURP and MIT
 Management of LUTS after TURP and MIT Hong Sup Kim Konkuk University TURP & MIT TURP : Gold standard MIT TUIP TUNA TUMT HIFU LASER Nd:YAG, ILC, HoLRP, KTP LUTS after TURP and MIT Improved : about 70% Persistent
Management of LUTS after TURP and MIT Hong Sup Kim Konkuk University TURP & MIT TURP : Gold standard MIT TUIP TUNA TUMT HIFU LASER Nd:YAG, ILC, HoLRP, KTP LUTS after TURP and MIT Improved : about 70% Persistent
SELF CARE IN URINARY INCONTINENCE
 O P I N I O N SelfCare 2011;2(6):160-166 Advancing the study&understanding of self-care JULIAN SPINKS General Practitioner, Medway Primary Care Trust ABSTRACT Urinary incontinence and its associated urinary
O P I N I O N SelfCare 2011;2(6):160-166 Advancing the study&understanding of self-care JULIAN SPINKS General Practitioner, Medway Primary Care Trust ABSTRACT Urinary incontinence and its associated urinary
Urology Case Study Workbook - Questions
 Urology Case Study Workbook - Questions Developed in Partnership with the CME tutors for the CME Network Facilitated by an educational grant by GlaxoSmithKline Date of Preparation. September 5th 2011 IE/DUTT/0025/11
Urology Case Study Workbook - Questions Developed in Partnership with the CME tutors for the CME Network Facilitated by an educational grant by GlaxoSmithKline Date of Preparation. September 5th 2011 IE/DUTT/0025/11
21/03/2016. The urogynaecologist approach. Urinary continence management in women: a multidisciplinary approach. Dr Anna Rosamillia
 Urinary continence management in women: a multidisciplinary approach The urogynaecologist approach Dr Anna Rosamillia What is normal bladder function? Incontinence is not normal Normal voiding is 7-8 times
Urinary continence management in women: a multidisciplinary approach The urogynaecologist approach Dr Anna Rosamillia What is normal bladder function? Incontinence is not normal Normal voiding is 7-8 times
URGE MOTOR INCONTINENCE
 URGE MOTOR INCONTINENCE URGE INCONTINENCE COMMONEST TYPE IN ELDERLY WOMEN Causes: 1 - Defects in CNS regulation Stroke Parkinson s disease Dementia (Alzheimer s and other types) Normopressure hydrocephalus
URGE MOTOR INCONTINENCE URGE INCONTINENCE COMMONEST TYPE IN ELDERLY WOMEN Causes: 1 - Defects in CNS regulation Stroke Parkinson s disease Dementia (Alzheimer s and other types) Normopressure hydrocephalus
25-Feb-16 MANAGEMENT OF URINARY INCONTINENCE IN WOMEN.
 Female Urinary Incontinence: GP resources MANAGEMENT OF URINARY INCONTINENCE IN WOMEN Dr Marcus Carey 20 February 2016 www.thewomens.org.au Clinical Practice Guidelines GP management of female urinary
Female Urinary Incontinence: GP resources MANAGEMENT OF URINARY INCONTINENCE IN WOMEN Dr Marcus Carey 20 February 2016 www.thewomens.org.au Clinical Practice Guidelines GP management of female urinary
Victoria Sharp, MD, MBA, FAAFP. Clinical Professor of Urology and Family Medicine
 Victoria Sharp, MD, MBA, FAAFP Clinical Professor of Urology and Family Medicine Victoria Sharp, MD, MBA, FAAFP Market Chief Medial Officer AmeriHealth Caritas Family of Companies Office phone: (515) 330-3740
Victoria Sharp, MD, MBA, FAAFP Clinical Professor of Urology and Family Medicine Victoria Sharp, MD, MBA, FAAFP Market Chief Medial Officer AmeriHealth Caritas Family of Companies Office phone: (515) 330-3740
Dr Jonathan Evans Paediatric Nephrologist
 How do I manage a patient with intractable daytime wetting: Dr Jonathan Evans Paediatric Nephrologist Of 107 children aged 11-12 with day-wetting 91 (85%) were dry at 15-16 yr Swithinbank et al BJU 1998
How do I manage a patient with intractable daytime wetting: Dr Jonathan Evans Paediatric Nephrologist Of 107 children aged 11-12 with day-wetting 91 (85%) were dry at 15-16 yr Swithinbank et al BJU 1998
Urinary Incontinence for the Primary Care Provider
 Urinary Incontinence for the Primary Care Provider Diana J Scott FNP-BC https://youtu.be/gmzaue1ojn4 1 Assessment of Urinary Incontinence Urge Stress Mixed Other overflow, postural, continuous, insensible,
Urinary Incontinence for the Primary Care Provider Diana J Scott FNP-BC https://youtu.be/gmzaue1ojn4 1 Assessment of Urinary Incontinence Urge Stress Mixed Other overflow, postural, continuous, insensible,
CONTINENCE MODULE 1 MIMIMUM STANDARDS FOR THE SPECIALIST ASSESSMENT & CONSERVATIVE MANAGEMENT OF FEMALE LOWER URINARY TRACT SYMPTOMS
 CONTINENCE MODULE 1 MIMIMUM STANDARDS FOR THE SPECIALIST ASSESSMENT & CONSERVATIVE MANAGEMENT OF FEMALE LOWER URINARY TRACT SYMPTOMS The minimum standards required to initiate specialised conservative
CONTINENCE MODULE 1 MIMIMUM STANDARDS FOR THE SPECIALIST ASSESSMENT & CONSERVATIVE MANAGEMENT OF FEMALE LOWER URINARY TRACT SYMPTOMS The minimum standards required to initiate specialised conservative
NICE guideline Published: 2 April 2019 nice.org.uk/guidance/ng123
 Urinary incontinence and pelvic organ prolapse in women: management NICE guideline Published: 2 April 2019 nice.org.uk/guidance/ng123 NICE 2019. All rights reserved. Subject to Notice of rights (https://www.nice.org.uk/terms-and-conditions#notice-ofrights).
Urinary incontinence and pelvic organ prolapse in women: management NICE guideline Published: 2 April 2019 nice.org.uk/guidance/ng123 NICE 2019. All rights reserved. Subject to Notice of rights (https://www.nice.org.uk/terms-and-conditions#notice-ofrights).
Geriatric Urinary Incontinence
 Geriatric Urinary Incontinence Neil M. Resnick, MD Thomas Detre Professor of Medicine Chief, Division of Geriatric Medicine University of Pittsburgh/UPMC UI: The Problem Prevalence in elderly 33% Morbidity
Geriatric Urinary Incontinence Neil M. Resnick, MD Thomas Detre Professor of Medicine Chief, Division of Geriatric Medicine University of Pittsburgh/UPMC UI: The Problem Prevalence in elderly 33% Morbidity
NATIONAL INSTITUTE FOR CLINICAL EXCELLENCE SCOPE. Urinary incontinence: the management of urinary incontinence in women
 NATIONAL INSTITUTE FOR CLINICAL EXCELLENCE 1 Guideline title SCOPE Urinary incontinence: the management of urinary incontinence in women 1.1 Short title Urinary incontinence 2 Background a) The National
NATIONAL INSTITUTE FOR CLINICAL EXCELLENCE 1 Guideline title SCOPE Urinary incontinence: the management of urinary incontinence in women 1.1 Short title Urinary incontinence 2 Background a) The National
Incontinence in neurological disease
 nice bulletin Incontinence in neurological disease NICE provided the content for this booklet which is independent of any company or product advertised NICE Bulletin - Incontinence in neurological disease.indd
nice bulletin Incontinence in neurological disease NICE provided the content for this booklet which is independent of any company or product advertised NICE Bulletin - Incontinence in neurological disease.indd
Management, Evaluation, and Treatment of Overactive Bladder and Urinary Incontinence
 Management, Evaluation, and Treatment of Overactive Bladder and Urinary Incontinence Arthur Mourtzinos, MD, MBA Co-Vice Chair, Institute of Urology Director, Continence Center Assistant Professor of Urology,
Management, Evaluation, and Treatment of Overactive Bladder and Urinary Incontinence Arthur Mourtzinos, MD, MBA Co-Vice Chair, Institute of Urology Director, Continence Center Assistant Professor of Urology,
GUIDELINES ON URINARY INCONTINENCE
 GUIDELINES ON URINRY INONTINENE (Text update pril 2014) M.G. Lucas (chair), D. edretdinova, J.L.H.R. osch, F. urkhard, F. ruz, D.J.M.K. de Ridder,. Nambiar,.G. Nilsson,. Tubaro, R.S. Pickard This pocket
GUIDELINES ON URINRY INONTINENE (Text update pril 2014) M.G. Lucas (chair), D. edretdinova, J.L.H.R. osch, F. urkhard, F. ruz, D.J.M.K. de Ridder,. Nambiar,.G. Nilsson,. Tubaro, R.S. Pickard This pocket
Pelvic Floor Therapy for the Neurologic Client Carina Siracusa, PT, DPT, WCS
 Pelvic Floor Therapy for the Neurologic Client Carina Siracusa, PT, DPT, WCS OhioHealth, Columbus Ohio Disclosures I have nothing to disclose Objectives Describe the role of a pelvic floor therapist in
Pelvic Floor Therapy for the Neurologic Client Carina Siracusa, PT, DPT, WCS OhioHealth, Columbus Ohio Disclosures I have nothing to disclose Objectives Describe the role of a pelvic floor therapist in
The Management of Female Urinary Incontinence. Part 1: Aetiology and Investigations
 The Management of Female Urinary Incontinence Part 1: Aetiology and Investigations Dr Oseka Onuma Gynaecologist and Pelvic Reconstructive Surgeon 4 Robe Terrace Medindie SA 5081 Urinary incontinence has
The Management of Female Urinary Incontinence Part 1: Aetiology and Investigations Dr Oseka Onuma Gynaecologist and Pelvic Reconstructive Surgeon 4 Robe Terrace Medindie SA 5081 Urinary incontinence has
PROSTATIC ARTERY EMBOLISATION (PAE) FOR BENIGN PROSTATIC HYPERPLASIA. A Minimally Invasive Innovative Treatment
 FOR BENIGN PROSTATIC HYPERPLASIA. A Minimally Invasive Innovative Treatment") PROSTATIC ARTERY EMBOLISATION (PAE) FOR BENIGN PROSTATIC HYPERPLASIA A Minimally Invasive Innovative Treatment What is the prostate? The prostate is an accessory organ of the male reproductive system.
PROSTATIC ARTERY EMBOLISATION (PAE) FOR BENIGN PROSTATIC HYPERPLASIA A Minimally Invasive Innovative Treatment What is the prostate? The prostate is an accessory organ of the male reproductive system.
Benign Prostatic Hyperplasia. Jay Lee, MD, FRCSC Clinical Associate Professor University of Calgary
 Benign Prostatic Hyperplasia Jay Lee, MD, FRCSC Clinical Associate Professor University of Calgary Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied,
Benign Prostatic Hyperplasia Jay Lee, MD, FRCSC Clinical Associate Professor University of Calgary Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied,
Stress Incontinence. Susannah Elvy Urogynaecology CNS
 Stress Incontinence Susannah Elvy Urogynaecology CNS Definitions Prevalence Assessment Investigation Treatment Surgery Men International Continence Society define as the complaint of any involuntary leakage
Stress Incontinence Susannah Elvy Urogynaecology CNS Definitions Prevalence Assessment Investigation Treatment Surgery Men International Continence Society define as the complaint of any involuntary leakage
The Royal Marsden. Prostate case study. Presented by Mr Alan Thompson Consultant Urological Surgeon
 Prostate case study Presented by Mr Alan Thompson Consultant Urological Surgeon 2 Part one Initial presentation A 62 year old male solicitor attends your GP surgery. He has rarely seen you over the last
Prostate case study Presented by Mr Alan Thompson Consultant Urological Surgeon 2 Part one Initial presentation A 62 year old male solicitor attends your GP surgery. He has rarely seen you over the last
Overactive Bladder in Clinical Practice
 Overactive Bladder in Clinical Practice Alan J. Wein Christopher Chapple Overactive Bladder in Clinical Practice Authors Alan J. Wein Division of Urology University of Pennsylvania Health System Philadelphia
Overactive Bladder in Clinical Practice Alan J. Wein Christopher Chapple Overactive Bladder in Clinical Practice Authors Alan J. Wein Division of Urology University of Pennsylvania Health System Philadelphia
GUIDELINES ON NON-NEUROGENIC MALE LUTS INCLUDING BENIGN PROSTATIC OBSTRUCTION
 GUIDELINES ON NON-NEUROGENIC MLE LUTS INCLUDING BENIGN PROSTTIC OBSTRUCTION (Text update March 2015) S. Gravas (Chair), T. Bach,. Bachmann, M. Drake, M. Gacci, C. Gratzke, S. Madersbacher, C. Mamoulakis,
GUIDELINES ON NON-NEUROGENIC MLE LUTS INCLUDING BENIGN PROSTTIC OBSTRUCTION (Text update March 2015) S. Gravas (Chair), T. Bach,. Bachmann, M. Drake, M. Gacci, C. Gratzke, S. Madersbacher, C. Mamoulakis,
Prostate Disease. Chad Baxter, MD
 Prostate Disease Chad Baxter, MD Managing BPH and LUTS Chad Baxter, MD Department of Urology cbaxter@mednet.ucla.edu 33 nd Annual UCLA Intensive Course in Geriatric Medicine & Board Review Prevalence of
Prostate Disease Chad Baxter, MD Managing BPH and LUTS Chad Baxter, MD Department of Urology cbaxter@mednet.ucla.edu 33 nd Annual UCLA Intensive Course in Geriatric Medicine & Board Review Prevalence of
Diane K. Newman DNP, ANP-BC, PCB-PMD, FAAN
 Diane K. Newman DNP, ANP-BC, PCB-PMD, FAAN Diane K. Newman, DNP is a Biofeedback Certified Continence Specialist. With over 35-years experience, she is an expert in the assessment and management of pelvic-floor
Diane K. Newman DNP, ANP-BC, PCB-PMD, FAAN Diane K. Newman, DNP is a Biofeedback Certified Continence Specialist. With over 35-years experience, she is an expert in the assessment and management of pelvic-floor
Ambulatory Emergency Care Pathways. Acute Painful Bladder Outflow Obstruction
 Ambulatory Emergency Care Pathways Acute Painful Bladder Outflow Obstruction Effective Date: November 2011 Content Summary Ref Title Description 1 Condition Details Identifies pathway details and clinical
Ambulatory Emergency Care Pathways Acute Painful Bladder Outflow Obstruction Effective Date: November 2011 Content Summary Ref Title Description 1 Condition Details Identifies pathway details and clinical
NICE Pathways bring together all NICE guidance, quality standards and other NICE information on a specific topic.
 bring together all NICE guidance, quality standards and other NICE information on a specific topic. are interactive and designed to be used online. They are updated regularly as new NICE guidance is published.
bring together all NICE guidance, quality standards and other NICE information on a specific topic. are interactive and designed to be used online. They are updated regularly as new NICE guidance is published.
GUIDELINES ON NON-NEUROGENIC MALE LUTS INCLUDING BENIGN PROSTATIC OBSTRUCTION (BPO)
") GUIDELINES ON NON-NEUROGENIC MLE LUTS INCLUDING BENIGN PROSTTIC OBSTRUCTION (BPO) (Text update pril 2014) S. Gravas (chair),. Bachmann,. Descazeaud, M. Drake, C. Gratzke, S. Madersbacher, C. Mamoulakis,
GUIDELINES ON NON-NEUROGENIC MLE LUTS INCLUDING BENIGN PROSTTIC OBSTRUCTION (BPO) (Text update pril 2014) S. Gravas (chair),. Bachmann,. Descazeaud, M. Drake, C. Gratzke, S. Madersbacher, C. Mamoulakis,
Information for Patients. Overactive bladder syndrome (OAB) English
 English") Information for Patients Overactive bladder syndrome (OAB) English Table of contents What is the bladder?... 3 What are overactive bladder symptoms?... 3 What causes overactive bladder symptoms?... 3 Diagnosis
Information for Patients Overactive bladder syndrome (OAB) English Table of contents What is the bladder?... 3 What are overactive bladder symptoms?... 3 What causes overactive bladder symptoms?... 3 Diagnosis
Lower urinary tract symptoms
 Issue date: May 2010 Lower urinary tract symptoms The management of lower urinary tract symptoms in men NICE clinical guideline 97 Developed by the National Clinical Guideline Centre: Acute and Chronic
Issue date: May 2010 Lower urinary tract symptoms The management of lower urinary tract symptoms in men NICE clinical guideline 97 Developed by the National Clinical Guideline Centre: Acute and Chronic
Managing Female Urinary Incontinence Within Primary Care
 Managing Female Urinary Incontinence Within Primary Care Angela Patterson Lead Clinical Nurse Specialist in Bladder and Bowel Dysfunction. South Eastern HSCT Background More than 14 million in the UK affected
Managing Female Urinary Incontinence Within Primary Care Angela Patterson Lead Clinical Nurse Specialist in Bladder and Bowel Dysfunction. South Eastern HSCT Background More than 14 million in the UK affected
Managing lower urinary tract symptoms in men
 Managing lower urinary tract symptoms in men MacKenzie KR, Aning JJ. Managing lower urinary tract symptoms in men. Practitioner 6; 6(79):-6 Mr Kenneth R MacKenzie MBChB MRCS (Ed) Core Trainee in Urology
Managing lower urinary tract symptoms in men MacKenzie KR, Aning JJ. Managing lower urinary tract symptoms in men. Practitioner 6; 6(79):-6 Mr Kenneth R MacKenzie MBChB MRCS (Ed) Core Trainee in Urology
Incontinence: The silent scourge of the young and old. The International Continence Society has. In this article:
 Focus on CME at the University of Toronto Incontinence: The silent scourge of the young and old By Sender Herschorn, BSc, MDCM, FRCSC In this article: 1. What is the workup for urinary incontinence? 2.
Focus on CME at the University of Toronto Incontinence: The silent scourge of the young and old By Sender Herschorn, BSc, MDCM, FRCSC In this article: 1. What is the workup for urinary incontinence? 2.
EAU GUIDELINES ON NON- NEUROGENIC MALE LUTS INCLUDING BENIGN PROSTATIC OBSTRUCTION
 EAU GUIDELINES ON NON- NEUROGENIC MALE LUTS INCLUDING BENIGN PROSTATIC OBSTRUCTION (Text update March 2017) S. Gravas (Chair), T. Bach, M. Drake, M. Gacci, C. Gratzke, T.R.W. Herrmann, S. Madersbacher,
EAU GUIDELINES ON NON- NEUROGENIC MALE LUTS INCLUDING BENIGN PROSTATIC OBSTRUCTION (Text update March 2017) S. Gravas (Chair), T. Bach, M. Drake, M. Gacci, C. Gratzke, T.R.W. Herrmann, S. Madersbacher,
Disease Management. Incontinence Care. Chan Sau Kuen Continence Nurse Consultant United Christian Hospital 14/11/09
 Disease Management in Incontinence Care Chan Sau Kuen Continence Nurse Consultant United Christian Hospital 14/11/09 What is incontinence? Definition of Incontinence - Is the compliant of any involuntary
Disease Management in Incontinence Care Chan Sau Kuen Continence Nurse Consultant United Christian Hospital 14/11/09 What is incontinence? Definition of Incontinence - Is the compliant of any involuntary
R. Matthew Smith M.D. Stacy Pohlman, ARNP Jessica Gengler, PT, DPT Mercy Urology
 R. Matthew Smith M.D. Stacy Pohlman, ARNP Jessica Gengler, PT, DPT Mercy Urology Disclosures Matt Smith None Stacy Pohlman None Jessica Gengler None Topics Clinical Pathway Development Prostate Cancer
R. Matthew Smith M.D. Stacy Pohlman, ARNP Jessica Gengler, PT, DPT Mercy Urology Disclosures Matt Smith None Stacy Pohlman None Jessica Gengler None Topics Clinical Pathway Development Prostate Cancer
LUTS in the modern era. Dr Jon Rees Tyntesfield Medical Group
 LUTS in the modern era Dr Jon Rees Tyntesfield Medical Group In the past! Man with urinary symptoms = PROSTATISM Prostatism = TURP TURP unsuccessful = REDO TURP Redo TURP unsuccessful = can t help you!
LUTS in the modern era Dr Jon Rees Tyntesfield Medical Group In the past! Man with urinary symptoms = PROSTATISM Prostatism = TURP TURP unsuccessful = REDO TURP Redo TURP unsuccessful = can t help you!
Diagnosis and Treatment of Urinary Incontinence. Urinary Incontinence
 Diagnosis and Treatment of Urinary Incontinence Leslee L. Subak, MD Professor Obstetrics, Gynecology & RS Epidemiology, Urology University of California, San Francisco Urinary Incontinence Common - 25%
Diagnosis and Treatment of Urinary Incontinence Leslee L. Subak, MD Professor Obstetrics, Gynecology & RS Epidemiology, Urology University of California, San Francisco Urinary Incontinence Common - 25%
Urinary incontinence in women & men
 Urinary incontinence in women & men Dr. Blayne Welk Assistant Professor, Western University, London, ON, Canada Part 1: INCONTINENCE IN WOMEN Urinary incontinence is common. About 1 in 4 young women, and
Urinary incontinence in women & men Dr. Blayne Welk Assistant Professor, Western University, London, ON, Canada Part 1: INCONTINENCE IN WOMEN Urinary incontinence is common. About 1 in 4 young women, and
Urinary dysfunction assessment tool (care home)
") Addressograph label CHI:... Name:... Address:...... Urinary dysfunction assessment tool (care home) Past medical history: Is the patient on medications which can affect bladder function? If, please list
Addressograph label CHI:... Name:... Address:...... Urinary dysfunction assessment tool (care home) Past medical history: Is the patient on medications which can affect bladder function? If, please list
Urinary tract disorders
 Urinary tract disorders Medicines Formulary Contents: 1. Urinary retention 1 2. Urinary incontinence 2 3. Urethral pain prevention during catheterisation 3 4. Indwelling catheters maintenance of patency
Urinary tract disorders Medicines Formulary Contents: 1. Urinary retention 1 2. Urinary incontinence 2 3. Urethral pain prevention during catheterisation 3 4. Indwelling catheters maintenance of patency
The Management of Overactive Bladder Syndrome with Antimuscarinic Drugs
 The Management of Overactive Bladder Syndrome with Antimuscarinic Drugs Author Version Date Consultation Date of Ratification By JPG Shaista Hussain Joint Formulary Pharmacist V2 16.09.2014 Homerton University
The Management of Overactive Bladder Syndrome with Antimuscarinic Drugs Author Version Date Consultation Date of Ratification By JPG Shaista Hussain Joint Formulary Pharmacist V2 16.09.2014 Homerton University
Benign Prostatic Hyperplasia (BPH):
:") Benign Prostatic Hyperplasia (BPH): Evidence Based Guidelines for Primary Care Providers Jeanne Martin, DNP, ANP-BC Objectives 1. Understand the pathophysiology and prevalence of BPH 2. Select the appropriate
Benign Prostatic Hyperplasia (BPH): Evidence Based Guidelines for Primary Care Providers Jeanne Martin, DNP, ANP-BC Objectives 1. Understand the pathophysiology and prevalence of BPH 2. Select the appropriate
Physiology & Neurophysiology of lower U.T.
 Physiology & Neurophysiology of lower U.T. Classification of voiding dysfunction Evaluation of a child with voiding dysfunction Management Storage Ø Adequate volume of urine Ø At LOW pressure Ø With NO
Physiology & Neurophysiology of lower U.T. Classification of voiding dysfunction Evaluation of a child with voiding dysfunction Management Storage Ø Adequate volume of urine Ø At LOW pressure Ø With NO
Dr. Aso Urinary Symptoms
 Haematuria The presence of blood in the urine (haematuria) is always abnormal and may be the only indication of pathology in the urinary tract. False positive stick tests and the discolored urine caused
Haematuria The presence of blood in the urine (haematuria) is always abnormal and may be the only indication of pathology in the urinary tract. False positive stick tests and the discolored urine caused
Geriatric Giants Lecture Series: Urinary incontinence
 Geriatric Giants Lecture Series: Urinary incontinence Learning objectives To demonstrate an understanding of : definition of urinary incontinence physiological control of the micturition cycle changes
Geriatric Giants Lecture Series: Urinary incontinence Learning objectives To demonstrate an understanding of : definition of urinary incontinence physiological control of the micturition cycle changes