What is the role of Surgery for IBD State of the Art 2007
|
|
|
- Jeremy Stevens
- 5 years ago
- Views:
Transcription


1 What is the role of Surgery for IBD State of the Art 2007 Neil Mortensen MD FRCS Department of Surgery Radcliffe Hospital, Falk Meeting Istanbul 2007
2 Surgery for IBD Ulcerative colitis Crohns Disease When medicine fails..

3 Parks and Nicholls Proctocolectomy without ileostomy for ulcerative colitis BMJ 1978;2:65-8
4 Pouches around the World 2006 USA UK 3500 Sweden 2000 Canada 4500 Germany 2000 France 750 Australia 500 Estimated Total 25000



5 Pouch surgery the ecstasy


6 Pouch surgery the agony
7 Pouch technique convergence
8 Pelvic dissection Anastomosis Pouch ileostomy

9 Mesorectal plane or close rectal dissection Mesorectal plane now well known Less difficult More danger to pelvic nerves Bigger space Close rectal less familiar More difficult Less danger to pelvic nerves Less dead space
10 The pouch
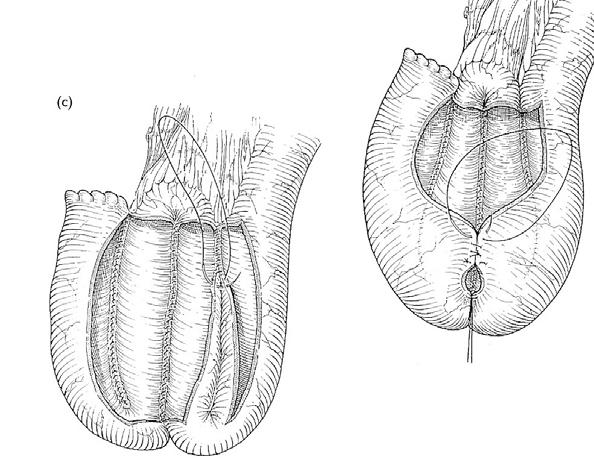
11 Size/configuration Rotation Mesentery Length/reach The pouch
12 Oversew the top staple line Angle of sorrow sutures
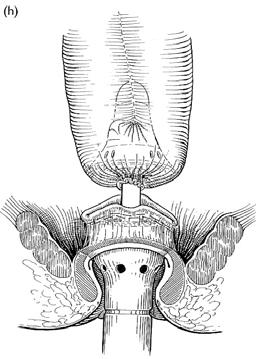
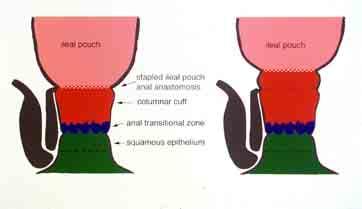
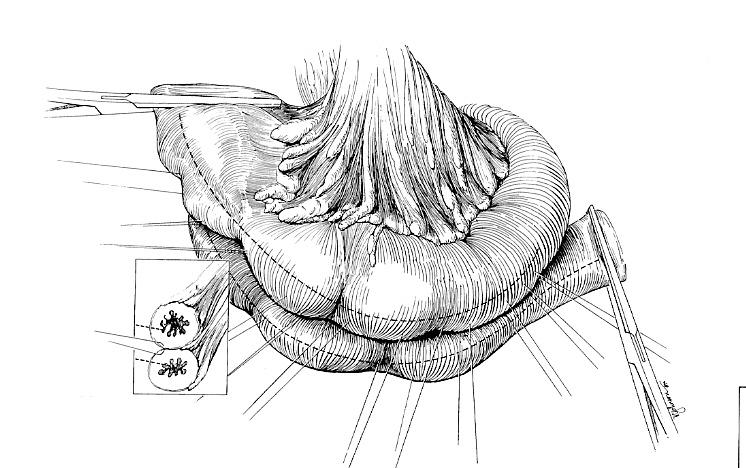
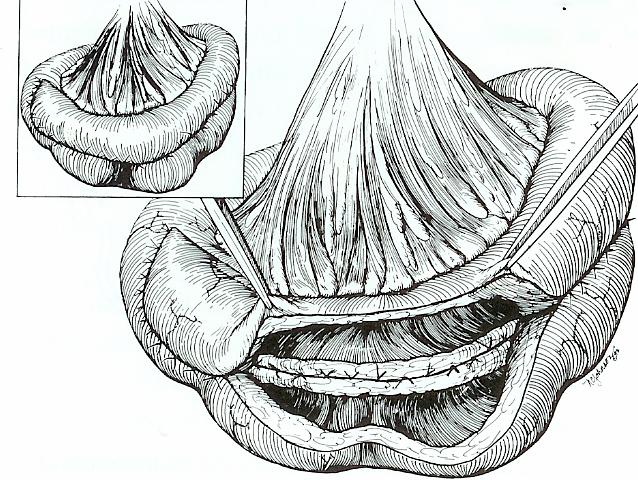
13 The anastomosis

14 Mucosectomy or no? Advantage theoretical improvement in disease control Disadvantage possible worse functional outcome and more difficult technically
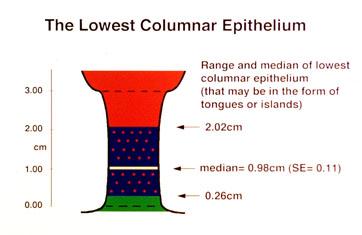
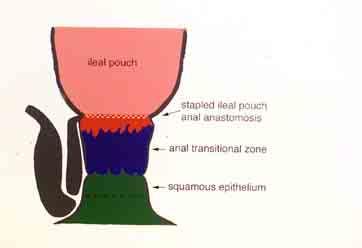
15 The 3 Components of the Anal Canal Mucosa great variation between individuals the anal transitional zone is narrower = av 0.45cm within the ATZ are islands of columnar epithelium Thompson-Fawcett et al Br J Surg1998
16
17
18
19 How to put the Anastomosis in the right place Visualise Parks et al BMJ 1978 Evert Regimbeau et al DCR 2004
20 How to put the anastomosis in the right place digitise To the pip joint
21 The risks of maintaining Columnar Cuff - Some 6-10% of the total anorectal mucosa is retained - risk of malignancy - risk of inflammation
22 Anal Manipulation/damage 153 patients Manipulation = mucosectomy, transanal pursestring, hand sewn pouch n=94 Less manipulation correlated with better resting pressure, continence and fewer pads Extent of smooth muscle resection during mucosectomy Tuckson et al, Am J Surg 1991 Becker et al DCR 1997




23 Pharmacological dilatation? Winter et al DCR 2004
24 Advantages of Stapling No anal dilatation No smooth muscle resection Sensation retained And its much easier Unless it misfires
25 Mucosectomy when? Consider in high grade rectal dysplasia or carcinoma complicating UC Consider in FAP with dense polyp burden in lower rectum Cuffitis requiring resection Re do pouch surgery with reanastomosis
26 Mucosectomy? Not very often
27 A brief history of defunctioning ileostomy always selective never
28 Are the consequences of an unprotected leak more serious?
29 One Stage Restorative Proctocolectomy without ileostomy 100 patients, randomised life threatening complications more frequent in those with no ileostomy 11 pelvic sepsis, 7 re-operation emergency operations in 11 v. 1 in those with ileostomy Williamson et al Dis Col Rect 1997
30 When is it reasonable to omit a defunctioning ileostomy? PATIENT no comorbidity non toxic low steroids female OPERATION elective perfect technique histology SURGEON experienced in town
31 ileostomy? usually
32 Laparoscopic Proctocolectomy and Pouch the US view One stage lap IPAA 32patients. No conversion, 3 reoperation Ky et al DCR2002
33 Laparoscopic Proctocolectomy and Pouch the European view Lap colon mobilisation and pfannensteil incision 54 patients, 5 conversions BMI 11 major complns and 9 needed secondary ileostomy Kienle Surg Endosc 2003
34 Pouch complications Pouch cutaneous fistula Pouch vaginal fistula Bleeding Infarction Peritonitis Anastomotic leak Stricture Small bowel stricture
35 Pouch Failure
36 Causes of Pouch Failure Toronto 49 (8.8%) of 551 pouches failed 9 (1.6%) defunctioned - 21 (39%) anastomotic leak - 13 (23%) poor function - 7 (12%) pouchitis - 7 (12%) pouch leakage - 7 (12%) perianal disease - 3 (5%) various MacRae et al DCR 1997
37 Incidence and Impact Pelvic Abscess after IPAA 73 of 1508 had pelvic abscess pouch failure 26% 55% need transabdominal salvage 8% local surgery 37% non surgical functional outcome poorer Farouk et al DCR 1998
38 Indications for Pouch Excision at St Mark s St Mark s n=996 Referred n=245 Total No patients Pelvic sepsis Pouch fistula Crohns Poor function Pouchitis other 58(5.6%) (4%) (48.5%) 24(35.2%) Karoui, Cohen, and Nicholls DCR 2004
39 Long Term Failure Rates from St Mark s Karoui Cohen and Nicholls DCR 2004
40 Restorative Proctocolectomy - Technique Get it right first time Spend quality time with your anastomosis!
41 Long Term Follow Up the issues Failure as defined by pouch excision Causes of failure Stability of function QOL data Fecundability Pregnancy and delivery The cancer bogey Pouchitis
42 0.5 Cumulative Risk of Pouchitis Proportion of risk overall chronic Follow up (m) Keranen et al Dis Col Rect 1997
43 Function and Quality of Life
44 Is pouch function stable with time? 1) 235 pouch patients studied in agreed to re-study median FU 12 y Bullard et al Dis Col Rect 2002
45 Is pouch function stable with time? 2) bowel frequency / v 6.8 night frequency 1.6 v 1.4 Bullard et al Dis Col Rect 2002
46 Is pouch function stable with time? 3) Continence Compared to 1992 major day major night minor day minor night Improved 1% 6% 9% 21% No change 82% 73% 59% 55% Worse 17% 21% 32% 24% Bullard et al Dis Col Rect 2002
47 Quality of Life- Age related Outcomes after IPAA 1895 patients, 4.1% failure Stratified into <45, 46-55, and >65 yrs Prospective assessment at 1,3 5, and 10yrs Minor diffs in QOL favouring <45s Acceptable function and QOL in patients of all ages Delaney et al Ann Surg 2003
48 Pregnancy and Fertility
49 Pregnancy and delivery before and after IPAA Mayo experience 236 pregnancies before and 232 after No diff in vag deliveries 59% before v 54% after Stool frequency up from 5.4 to 6.4 at 68m pp Occas incont up from 21% to 36% Hahnloser et al DCR 2003
50 Female Fecundity after IPAA for UC 290 patients Severe reduction in fecundity pre colect IPAA 12m 83% 18% 24m 85% 27% 60m 90% 36% Olsen KO et al Gastroenterology 2002
51 Female infertility after IPAA for UC Toronto experience Infertility rate 38.1% after IPAA v 13.3% non op No diff before and after diagnosis of UC 98% reduction in fertility after IPAA v before Johnson et al DCR 2004


52 Summary 10% lose pouch 10% have poor function but prefer to keep their pouch 80% report an excellent quality of life
53 But.. Some worries Increasing numbers of patients needing chronic ciproxin dosing Perianal disease being treated with infliximab
54 Surgery for Crohns Disease
55 Indications for Surgery in Crohn s Disease % Internal fistula and abscess Intestinal obstruction Perianal disease Failed medical therapy Acute colitis 0 Ileocolic Small bowel Colonic
56 Small bowel
57 Treatment of Crohn s Disease Radical Excision and lymph nodes Minimal Resections Bypass Limited Resections
58 Surgical Intervention in Crohn s Disease - the balance early surgery late surgery poor trial medical therapy disease recurs more technical problems more complications
59 Surgery for Obstruction Recurrent obstructive symptoms one is a warning two is an indication three is an indictment Alexander-Williams 1993
60 Resection for classical ileocaecal Crohn s disease patients 10y follow up 110 resection 114 fit and well 1 death from Crohn s disease Andrews et al 1991
61 SB Crohn s Surgery Effect of Resection Margins on Recurrence 131 in a randomised trial of limited v. extended resection Follow up median 56m Recurrence 25% limited v. 18% extended NS Microscopic disease at margins no effect Fazio et al Ann Surg 1996
62 Laparoscopic resection for ileocaecal Crohn s disease Lap assessment and ileocaecal mobilisation Extra corporeal anastomosis or strictureplasty Case selection
63 Laparoscopic resection for ileocaecal Crohn s disease problems with assessment Hand over hand with soft forceps Preop imaging will be the key small bowel enema being replaced by CT enteroclysis or MRI studies
64 Randomised trial of lap v open ileocaecal resection 60 patients randomised after lap assessment 6 exclusion for adhesions 2 conversions after randomisation Better pulmonary function and fewer complications in selected patients with ileocolic disease Milsom et al DCR 2001
65 Assessment at open surgery feel balloon characterisation on table enteroscopy inspect margins

66 Assessment of proximal margin of resection

67 Balloon impaction at strictures
68 Intra operative enteroscopy in Crohn s disease 33 exams in 31 patients 20 surgical decisions affected 14 more limited surgery External appearance less reliable than enteroscopy Smedh et al BJS 1993
69 What causes intestinal failure in Crohn s disease? Of 41 patients referred over 10y for permanent home TPN 7 due to Crohn s alone 34 due to repeated resection, 25 after multiple unplanned procedures 70 cm SB remaining Agwunobi DCR 2001

70 Who invented Strictureplasty? JAWS, Big Vic, or Mannie?

71 Strictureplasty in Crohn s Disease We have delayed reporting it widely in spite of the marked benefit obtained by a group of patients who present one of the most difficult problems of management in clinical medicine. Our particular worry was that the technique contravenes a widely held surgical view - that it is hazardous to anastomose bowel in which Crohn s inflammation is active Lee & Papaioannou 1982 Annals Royal Coll Surg Eng

72 Strictureplasty - diathermy transverse incision

73 Strictureplasty - suture vertically
74 Synchronous Resections acute phlegmon fistula perforation and abscess long stricture > 20 cm multiple strictures in a short segment
75 Strictureplasty: Experience 1978 to patients M:F 53: strictureplasties 151 operations mean follow-up 79.0 months (0.2 months to 19.5 years) Number of patients undergoing 1 or more SP operations
76 Complications not associated with: Patient Factors Medication Age > 50 years Weight loss > 5kg Hb < 10 Steroids Immunosuppressants Aminosalicylates Inflammatory Markers Surgical Factors WCC >10 ESR > 20 CRP > 20 Strictureplasties > 10 Previous anastomosis or strictureplasty site Concomitant resection
77 Complications: Associated Factors Nutritional status Albumin < 30 Perioperative TPN p < 0.01 p < p < number of patients Complications No complications no TPN TPN
78 Repeat Strictureplasty 39 strictured sites of previous anastomoses or strictureplasties were treated with strictureplasty Complication rate of 10.3% (vs 20.4% virgin site) 120 p = 0.46 number of operations Complications No complications 20 0 virgin site repeat site
79 Reported Strictureplasty Follow-up Authors Year Group Patients SPs Mean FU (range) months Spencer et al 1994 Mayo Clinic Serra et al 1995 Toronto (4 to 108) Stebbing et al (1 to 182) Hurst et al 1998 Chicago (3 to 95) Yamamoto et al 1999 Birmingham (3 to 206) Tonnelli & Ficaro 2000 Florence (3 to 132) Dietz et al 2001 Cleveland (1 to 192) Tichansky et al 2000 Meta-analysis analysis
80 Reported Strictureplasty Results Authors Patients SPs Complication Rate Recurrence or Reoperation Spencer et al % 20% at 3 years Serra et al % 32.6% reoperation Stebbing et al % 44% reoperation Hurst et al % 22% at 5 years Yamamoto et al % septic 54% at 8.9 years Tonnelli & Ficaro % 46% at 5 years Dietz et al % 34% at 7.5 years Tichansky et al % 25.5% further Sx
81 Michaelassi Strictureplasty Indication: short gut

82 Michaelassi strictureplasty Michelassi DCR 1996


83 Italian side to side Tonelli et : al DCR
84 Side to Side Strictureplasty 31 patients Average length 32cm (range 10-54) No morbidity or mortality At 26m follow up, 6 required reoperation, only one at a previous SP site Tonelli et al DCR 2004
85 Carcinoma and Strictureplasty 3 possible cases SB adenoca near a previous strictureplasty (Alexander Williams and Haynes World J Surg 1985) 70 yo with Crohn s and coeliac develops CA at strictureplasty site 7y later (Marchetti et al DCR 1996) 47 yo, CA at strictureplasty site 7y later, background 23y Crohn s (Jaskowiak and Michelassi DCR 2001)
86 Adhesions suspect an entero-enteric fistula until proven otherwise
87 Special Problems : severe adhesions back off, prolonged TPN painstakingly divide + sepra film
88 Special Problems- strategic inflammatory mass Inflammatory mass densely adherent to great vessels, ureters bypass, wait 3m painstakingly divide
89 Philosophy of Management in Crohn s Disease it is an incurable disease it has potential for pan-intestinal involvement surgery only overcomes the complications
90 Why do things go wrong? Wrong operation Wrong timing Wrong surgeon
91 Large bowel Segmental resections Ileoanal pouches
92 The Ideal Candidate * no SB disease * no anal disease * diffuse rectal and colonic involvement
93 The Typical Crohn s s Colitis * 25% have SB disease * anal disease common * rectal sparing
94 Perianal


95 Aetiology of anal lesions lymphoid aggregations around anal gland ducts retrograde lymphatic flow Narrow high pressure zone diarrhoea
96 Clinical Course of Perianal Fistula & Abscess 90 patients, median Fu 22m Risk of recurrence 48% at 1y, 59% at 2y Healing in 51% at 2y Re-opened in 44%, 18m after healing Best outcome with absent rectal disease and faecal diversion Makowiec et al Gut 1995
97 Emergency treatment of sepsis Incision and drainage Definitive treatment Fistulotomy Flap repair or glue Damage limitation Seton Defunctioning stoma Intestinal resection Proctectomy or proximal resection
98 What Surgery can Achieve drain abscess treat fistula dilate stricture defunction
99 What Surgery Cannot Achieve heal aggressive and atypical ulceration stop the inflammatory response prevent relapse success in the non healing perineum
100 Treatment of Fistula s in Crohn s Disease with Infliximab Randomised controlled trial, 94 patients, 90% perianal 55% multiple End point 50% or > reduction in number of draining fistulas 56-68% infliximab v 26% placebo success Present et al NEJ Med 1999
101 Does Infliximab heal fistula? Anal endosonography before and after although external tracks healed, ES changes remained Meuwissen DCR in press
102 Perianal Crohn s Disease Activity Index Score 0-4, worst case 20 discharge pain/restriction activity restriction sexual activity type perianal disease degree of induration Irvine et al J Clin Gastro 1995

103 A change in philosophy? Not so much to cure as to contain
104 Where will Infliximab fit in? reduction in inflammation prior to surgery prevention relapse after surgery the no hope case or instead of diversion
105 Combined seton, infliximab and maintenance immunosuppression 29 patients, 8 with rectovag fistula 67% complete response at 9m partial in 4 with decreased drainage or infliximab dependence Setons in 13 removed after 2 nd infusion Topstad et al DCR 2003
106 Unresolved issues with infliximab therapy How long should setons be left in place? When should they be removed, after 2 nd infusion? Can they be removed without any other intervention? What degree of continuing sepsis is acceptable? MRI or EUA? How long to continue with infliximab, every 8 weeks? (Sands et al NEJMed 2004)
107 Rectal Advancement Flap for Anorectal Crohn s Fistula number primary recurrence follow up failure months Moskowiez Jones Lewis Fry Joo Ozuner Kodner Total (11%) 28 (29%)
108 Perianal Crohn s Disease fibrin glue and other novel therapies fibrin glue results are poorer than for cryptogenic fistula Pharma treatment for fissure
109 Perianal Crohn s Disease - Philosophy of Management incurable damage limitation patient comfort and confidence share the pain with a physician


110 Joint medical-surgical management The aggressive physician The conservative surgeon
Ileoanal Pouch Solves the Problem
 Ileoanal Pouch Solves the Problem Bruce D George Department of Surgery John Radcliffe Hospital, Falk Symposium 2-3 May 2008 Ileoanal Pouch Solves the Problem? Sometimes Not always Key Issues in Pouch Surgery
Ileoanal Pouch Solves the Problem Bruce D George Department of Surgery John Radcliffe Hospital, Falk Symposium 2-3 May 2008 Ileoanal Pouch Solves the Problem? Sometimes Not always Key Issues in Pouch Surgery
Surgical Management of IBD in the Age of Biologics
 Surgical Management of IBD in the Age of Biologics Lisa S. Poritz, M.D Associate Professor of Surgery Division of Colon and Rectal Surgery Objectives Discuss surgical management of IBD When to operate
Surgical Management of IBD in the Age of Biologics Lisa S. Poritz, M.D Associate Professor of Surgery Division of Colon and Rectal Surgery Objectives Discuss surgical management of IBD When to operate
Homayoon Akbari, MD, PhD
 Recent Advances in IBD Surgery Homayoon M. Akbari, MD, PhD, FRCS(C), FACS Associate Professor of Surgery Virginia Commonwealth University Crohn s disease first described as a surgical condition, with the
Recent Advances in IBD Surgery Homayoon M. Akbari, MD, PhD, FRCS(C), FACS Associate Professor of Surgery Virginia Commonwealth University Crohn s disease first described as a surgical condition, with the
Surgery for Ulcerative Colitis 11/14/10. Colectomy for Ulcerative Colitis: What your patient should know. Surgery for Ulcerative Colitis
 Colectomy for Ulcerative Colitis: What your patient should know Madhulika G. Varma MD Associate Professor and Chief Section of Colorectal Surgery University of California, San Francisco Surgery for Ulcerative
Colectomy for Ulcerative Colitis: What your patient should know Madhulika G. Varma MD Associate Professor and Chief Section of Colorectal Surgery University of California, San Francisco Surgery for Ulcerative
Surgical Approach to Crohn s Colitis Segmental or Total Colectomy? Can We Avoid the Stoma?
 17 th Panhellenic IBD Congress Thessaloniki May 2018 Surgical Approach to Crohn s Colitis Segmental or Total Colectomy? Can We Avoid the Stoma? Janindra Warusavitarne Consultant Colorectal Surgeon, St
17 th Panhellenic IBD Congress Thessaloniki May 2018 Surgical Approach to Crohn s Colitis Segmental or Total Colectomy? Can We Avoid the Stoma? Janindra Warusavitarne Consultant Colorectal Surgeon, St
11/13/11. Biologics for CD and CUC: The Impact on Surgical Outcomes. Principles of Successful Intestinal Surgery
 Biologics for CD and CUC: The Impact on Surgical Outcomes Robert R. Cima, M.D., M.A. Associate Professor of Surgery Division of Colon and Rectal Surgery Overview Antibody based medications (biologics)
Biologics for CD and CUC: The Impact on Surgical Outcomes Robert R. Cima, M.D., M.A. Associate Professor of Surgery Division of Colon and Rectal Surgery Overview Antibody based medications (biologics)
Surgical Therapies for the Treatment of IBD!
 Surgical Therapies for the Treatment of IBD! Andrew A Shelton, MD Clinical Professor of Surgery Stanford Hospital and Clinics Section of Colon and Rectal Surgery! Ulcerative Colitis v. Crohn s! 30% of
Surgical Therapies for the Treatment of IBD! Andrew A Shelton, MD Clinical Professor of Surgery Stanford Hospital and Clinics Section of Colon and Rectal Surgery! Ulcerative Colitis v. Crohn s! 30% of
Ileal Pouch Anal Anastomosis: The Preferred Method of Reconstruction after Proctocolectomy in Children
 Ileal Pouch Anal Anastomosis: The Preferred Method of Reconstruction after Proctocolectomy in Children Stephanie Jones, D.O. Surgical Fellow March 21, 2011 Ulcerative Colitis Spectrum of inflammatory bowel
Ileal Pouch Anal Anastomosis: The Preferred Method of Reconstruction after Proctocolectomy in Children Stephanie Jones, D.O. Surgical Fellow March 21, 2011 Ulcerative Colitis Spectrum of inflammatory bowel
Inflammatory Bowel Disease and Surgery: What You Should Know
 Inflammatory Bowel Disease and Surgery: What You Should Know Ask the Experts March 9, 2019 Kristen Blaker, MD Colon and Rectal Surgery MetroHealth Medical Center Disclosures None Outline Who undergoes
Inflammatory Bowel Disease and Surgery: What You Should Know Ask the Experts March 9, 2019 Kristen Blaker, MD Colon and Rectal Surgery MetroHealth Medical Center Disclosures None Outline Who undergoes
Index. Note: Page numbers of article title are in boldface type.
 Index Note: Page numbers of article title are in boldface type. A Abscess(es) in Crohn s disease, 168 169 IPAA and, 110 114 as unexpected finding in colorectal surgery, 46 Adhesion(s) trocars-related laparoscopy
Index Note: Page numbers of article title are in boldface type. A Abscess(es) in Crohn s disease, 168 169 IPAA and, 110 114 as unexpected finding in colorectal surgery, 46 Adhesion(s) trocars-related laparoscopy
SURGERY FOR COLITIS THE BOTTOM LINE
 SURGERY FOR COLITIS THE BOTTOM LINE Speaker Declarations This presenter has the following declarations of relationship with industry None [Nov 2017] Surgeons just like to cut.. ABSOLUTE INDICATIONS Toxic
SURGERY FOR COLITIS THE BOTTOM LINE Speaker Declarations This presenter has the following declarations of relationship with industry None [Nov 2017] Surgeons just like to cut.. ABSOLUTE INDICATIONS Toxic
Surgical Management of IBD. Val Jefford Grand Rounds October 14, 2003
 Surgical Management of IBD Val Jefford Grand Rounds October 14, 2003 Introduction Important Features Clinical Presentation Evaluation Medical Treatment Surgical Treatment Cases Overview Introduction Two
Surgical Management of IBD Val Jefford Grand Rounds October 14, 2003 Introduction Important Features Clinical Presentation Evaluation Medical Treatment Surgical Treatment Cases Overview Introduction Two
Surgery for Inflammatory Bowel Disease
 Surgery for Inflammatory Bowel Disease Emily Steinhagen, MD Assistant Professor Department of Surgery, Division of Colorectal Surgery University Hospitals Cleveland Medical Center Common Questions Why
Surgery for Inflammatory Bowel Disease Emily Steinhagen, MD Assistant Professor Department of Surgery, Division of Colorectal Surgery University Hospitals Cleveland Medical Center Common Questions Why
Surgery and Crohn s. Crohn s Disease 70 % Why Operate? Complications of Disease. The Gastrointestinal Tract. Surgery for Inflammatory Bowel Disease
 The Gastrointestinal Tract Surgery for Inflammatory Bowel Disease Jonathan Chun, MD The regon Clinic Gastrointestinal and Minimally Invasive Surgery Crohn s Disease Can affect anywhere in the GI tract,
The Gastrointestinal Tract Surgery for Inflammatory Bowel Disease Jonathan Chun, MD The regon Clinic Gastrointestinal and Minimally Invasive Surgery Crohn s Disease Can affect anywhere in the GI tract,
Surgery in Inflammatory Bowel Disease. Rajesh Gupta MS, MCh Surgical Gastroenterology Division Dept of General Surgery PGIMER, Chandigarh
 Surgery in Inflammatory Bowel Disease Rajesh Gupta MS, MCh Surgical Gastroenterology Division Dept of General Surgery PGIMER, Chandigarh 1 Ulcerative colitis (UC) Ulcerative colitis (UC) characterized
Surgery in Inflammatory Bowel Disease Rajesh Gupta MS, MCh Surgical Gastroenterology Division Dept of General Surgery PGIMER, Chandigarh 1 Ulcerative colitis (UC) Ulcerative colitis (UC) characterized
Colorectal Surgery. Patient Care. Goals and Objectives
 Colorectal Surgery Patient Care 1) Interpret the results of clinical evaluations (history, physical examination) performed on patients with a) Hemorrhoids b) Perianal abscess/fistula c) Anal fissure d)
Colorectal Surgery Patient Care 1) Interpret the results of clinical evaluations (history, physical examination) performed on patients with a) Hemorrhoids b) Perianal abscess/fistula c) Anal fissure d)
Restorative Proctocolectomy For Ulcerative Colitis IN
 590540SJS0010.1177/1457496915590540Restorative proctocolectomyi. Helavirta, H. Huhtala, M. Hyöty, P. Collin, P. Aitola research-article2015 Original article Restorative Proctocolectomy For Ulcerative Colitis
590540SJS0010.1177/1457496915590540Restorative proctocolectomyi. Helavirta, H. Huhtala, M. Hyöty, P. Collin, P. Aitola research-article2015 Original article Restorative Proctocolectomy For Ulcerative Colitis
Poor Outcomes of Complicated Pouch-Related Fistulas after Ileal Pouch-Anal Anastomosis Surgery
 Syddansk Universitet Poor Outcomes of Complicated Pouch-Related Fistulas after Ileal Pouch-Anal Anastomosis Surgery Kjaer, M D; Kjeldsen, Jens; Qvist, Niels Published in: Scandinavian Journal of Surgery
Syddansk Universitet Poor Outcomes of Complicated Pouch-Related Fistulas after Ileal Pouch-Anal Anastomosis Surgery Kjaer, M D; Kjeldsen, Jens; Qvist, Niels Published in: Scandinavian Journal of Surgery
Inflammatory Bowel Disease: Updates and Controversies CASE #1 CASE #1 8/6/2015. What is the most likely diagnosis?
 Inflammatory Bowel Disease: Updates and Controversies Tehttp://192.185.93.102/~paulkeij/wpcontent/uploads/2013/07/collaboration.jpgxt August 7, 2015 Meagan M Costedio, MD; Colorectal Surgery; Cleveland
Inflammatory Bowel Disease: Updates and Controversies Tehttp://192.185.93.102/~paulkeij/wpcontent/uploads/2013/07/collaboration.jpgxt August 7, 2015 Meagan M Costedio, MD; Colorectal Surgery; Cleveland
Citation for published version (APA): Bartels, S. A. L. (2013). Laparoscopic colorectal surgery: beyond the short-term effects
: Bartels, S. A. L. (2013). Laparoscopic colorectal surgery: beyond the short-term effects") UvA-DARE (Digital Academic Repository) Laparoscopic colorectal surgery: beyond the short-term effects Bartels, S.A.L. Link to publication Citation for published version (APA): Bartels, S. A. L. (2013).
UvA-DARE (Digital Academic Repository) Laparoscopic colorectal surgery: beyond the short-term effects Bartels, S.A.L. Link to publication Citation for published version (APA): Bartels, S. A. L. (2013).
Pouchitis and Cuffitis A bloody mess. Sze-Lin Peng Colorectal Surgeon Counties Manukau District Health Board
 Pouchitis and Cuffitis A bloody mess Sze-Lin Peng Colorectal Surgeon Counties Manukau District Health Board Ileal-pouch anal anastomosis https://www.pennmedicine.org/for-health-care-professionals/for-physicians/physician-education-and-resources/clinicalbriefings/2018/february/total-proctocolectomy-with-jpouch-reconstruction-for-ulcerative-colitis
Pouchitis and Cuffitis A bloody mess Sze-Lin Peng Colorectal Surgeon Counties Manukau District Health Board Ileal-pouch anal anastomosis https://www.pennmedicine.org/for-health-care-professionals/for-physicians/physician-education-and-resources/clinicalbriefings/2018/february/total-proctocolectomy-with-jpouch-reconstruction-for-ulcerative-colitis
Ileo-rectal anastomosis for Crohn's disease of
 Ileo-rectal anastomosis for Crohn's disease of the colon W. N. W. BAKER From the Research Department, St Mark's Hospital, London Gut, 1971, 12, 427-431 SUMMARY Twenty-six cases of Crohn's disease of the
Ileo-rectal anastomosis for Crohn's disease of the colon W. N. W. BAKER From the Research Department, St Mark's Hospital, London Gut, 1971, 12, 427-431 SUMMARY Twenty-six cases of Crohn's disease of the
Perianal and Fistulizing Crohn s Disease: Tough Management Decisions. Jean-Paul Achkar, M.D. Kenneth Rainin Chair for IBD Research Cleveland Clinic
 Perianal and Fistulizing Crohn s Disease: Tough Management Decisions Jean-Paul Achkar, M.D. Kenneth Rainin Chair for IBD Research Cleveland Clinic Talk Overview Background Assessment and Classification
Perianal and Fistulizing Crohn s Disease: Tough Management Decisions Jean-Paul Achkar, M.D. Kenneth Rainin Chair for IBD Research Cleveland Clinic Talk Overview Background Assessment and Classification
Disclosure of Affiliations. The Way We Hope It Goes. Medicines and Surgery for IBD. None. Cases: Sweet and Not So Sweet
 Immunomodulators and Complications of Surgery for Inflammatory Bowel Disease Disclosure of Affiliations None Thomas E. Read, MD, FACS, FASCRS Professor of Surgery Tufts University School of Medicine Senior
Immunomodulators and Complications of Surgery for Inflammatory Bowel Disease Disclosure of Affiliations None Thomas E. Read, MD, FACS, FASCRS Professor of Surgery Tufts University School of Medicine Senior
SURGICAL MANAGEMENT OF ULCERATIVE COLITIS
 SURGICAL MANAGEMENT OF ULCERATIVE COLITIS Cary B. Aarons, MD Associate Professor of Surgery Division of Colon & Rectal Surgery University of Pennsylvania AGENDA Background Diagnosis/Work-up Medical Management
SURGICAL MANAGEMENT OF ULCERATIVE COLITIS Cary B. Aarons, MD Associate Professor of Surgery Division of Colon & Rectal Surgery University of Pennsylvania AGENDA Background Diagnosis/Work-up Medical Management
Angie Perrin Lead Nurse/Clinical Nurse Specialist Oxford Radcliffe Hospitals NHS Trust
 Angie Perrin Lead Nurse/Clinical Nurse Specialist Oxford Radcliffe Hospitals NHS Trust Background Late in 20th century saw revolutionary surgical advances within colorectal sphere 1978 Parks & Nicholls
Angie Perrin Lead Nurse/Clinical Nurse Specialist Oxford Radcliffe Hospitals NHS Trust Background Late in 20th century saw revolutionary surgical advances within colorectal sphere 1978 Parks & Nicholls
Colostomy & Ileostomy
 Colostomy & Ileostomy Indications, problems and preference By Waleed Omar Professor of Colorectal surgery, Mansoura University. Disclosure I have no disclosures. Presentation outline Stoma: Definition
Colostomy & Ileostomy Indications, problems and preference By Waleed Omar Professor of Colorectal surgery, Mansoura University. Disclosure I have no disclosures. Presentation outline Stoma: Definition
Epidemiology / Morbidity
 Perianal Crohn s Disease: Current Treatment Approach David A Schwartz, MD Director, Inflammatory Bowel Disease Center Vanderbilt University Medical Center Epidemiology / Morbidity Hellers et al, Gut 1980
Perianal Crohn s Disease: Current Treatment Approach David A Schwartz, MD Director, Inflammatory Bowel Disease Center Vanderbilt University Medical Center Epidemiology / Morbidity Hellers et al, Gut 1980
The Role of Surgery in Inflammatory Bowel Disease. Cory D Barrat, MD Colon and Rectal Surgeon Mercy Health
 The Role of Surgery in Inflammatory Bowel Disease Cory D Barrat, MD Colon and Rectal Surgeon Mercy Health THANKS FOR INVITING ME! I have no financial disclosures Outline - Who am I and what do I do? -
The Role of Surgery in Inflammatory Bowel Disease Cory D Barrat, MD Colon and Rectal Surgeon Mercy Health THANKS FOR INVITING ME! I have no financial disclosures Outline - Who am I and what do I do? -
Rectal Cancer. About the Colon and Rectum. Symptoms. Colorectal Cancer Screening
 Patient information regarding care and surgery associated with RECTAL CANCER by Robert K. Cleary, M.D., John C. Eggenberger, M.D., Amalia J. Stefanou., M.D. location: Michigan Heart and Vascular Institute,
Patient information regarding care and surgery associated with RECTAL CANCER by Robert K. Cleary, M.D., John C. Eggenberger, M.D., Amalia J. Stefanou., M.D. location: Michigan Heart and Vascular Institute,
Convegno Annuale Fondazione Rosa Gallo. Risultati chirurgici a lungo termine nelle IBD John Nicholls
 Convegno Annuale Fondazione Rosa Gallo Verona 23 24 novembre 2010 Risultati chirurgici a lungo termine nelle IBD John Nicholls MORTALITY IN IBD Roberts et al BMJ 2007 Record Linkage Study Oxford Region
Convegno Annuale Fondazione Rosa Gallo Verona 23 24 novembre 2010 Risultati chirurgici a lungo termine nelle IBD John Nicholls MORTALITY IN IBD Roberts et al BMJ 2007 Record Linkage Study Oxford Region
Fistulizing Crohn s Disease: The Aggressive Approach
 Fistulizing Crohn s Disease: The Aggressive Approach Bruce E. Sands, MD, MS MGH Crohn s and Colitis Center and Gastrointestinal Unit Massachusetts General Hospital Boston, USA Case Presentation: Summary
Fistulizing Crohn s Disease: The Aggressive Approach Bruce E. Sands, MD, MS MGH Crohn s and Colitis Center and Gastrointestinal Unit Massachusetts General Hospital Boston, USA Case Presentation: Summary
Index. Surg Clin N Am 87 (2007) Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type.") Surg Clin N Am 87 (2007) 787 796 Index Note: Page numbers of article titles are in boldface type. A Abscesses in anorectal Crohn s disease, 622 intra-abdominal, in Crohn s disease, 590 591 perirectal,
Surg Clin N Am 87 (2007) 787 796 Index Note: Page numbers of article titles are in boldface type. A Abscesses in anorectal Crohn s disease, 622 intra-abdominal, in Crohn s disease, 590 591 perirectal,
Chronic anastomotic sinus after low anterior resection: When can the defunctioning stoma be reversed?
 Received Date : 15-Oct-2009 Revised Date : 10-Dec-2009 Accepted Date : 14-Dec-2009 Article type : Original Article 547-2009.R1 Original Article Chronic anastomotic sinus after low anterior resection: When
Received Date : 15-Oct-2009 Revised Date : 10-Dec-2009 Accepted Date : 14-Dec-2009 Article type : Original Article 547-2009.R1 Original Article Chronic anastomotic sinus after low anterior resection: When
Mohamed EL-hemaly Gastro- intestinal surgical center, Mansoura University.
 Mohamed EL-hemaly Gastro- intestinal surgical center, Mansoura University. Chronic transmural inflammatory process of the bowel & affects any part of the gastro -intestinal tract from the mouth to the
Mohamed EL-hemaly Gastro- intestinal surgical center, Mansoura University. Chronic transmural inflammatory process of the bowel & affects any part of the gastro -intestinal tract from the mouth to the
Percent Cumulative. Probability. Penetrating. Inflammatory. Stricturing. Months Patients at risk N =
 Fistulizing Crohn s Disease Edward V. Loftus, Jr., M.D. Professor of Medicine Division of Gastroenterology & Hepatology Mayo Clinic Rochester, Minnesota, USA Outline Fistulizing Crohn s Etiology Incidence
Fistulizing Crohn s Disease Edward V. Loftus, Jr., M.D. Professor of Medicine Division of Gastroenterology & Hepatology Mayo Clinic Rochester, Minnesota, USA Outline Fistulizing Crohn s Etiology Incidence
Beyond Anti TNFs: positioning of other biologics for Crohn s disease. Christina Ha, MD Cedars Sinai Inflammatory Bowel Disease Center
 Beyond Anti TNFs: positioning of other biologics for Crohn s disease Christina Ha, MD Cedars Sinai Inflammatory Bowel Disease Center Objectives: To define high and low risk patient and disease features
Beyond Anti TNFs: positioning of other biologics for Crohn s disease Christina Ha, MD Cedars Sinai Inflammatory Bowel Disease Center Objectives: To define high and low risk patient and disease features
THE CUTTING EDGE SURGERY FOR CROHN S DISEASE & ULCERATIVE COLITIS. crohnsandcolitis.ca
 THE CUTTING EDGE SURGERY FOR CROHN S DISEASE & ULCERATIVE COLITIS crohnsandcolitis.ca There are many treatments that help manage Crohn s and colitis. Crohn s and Colitis Canada urges you to become knowledgeable
THE CUTTING EDGE SURGERY FOR CROHN S DISEASE & ULCERATIVE COLITIS crohnsandcolitis.ca There are many treatments that help manage Crohn s and colitis. Crohn s and Colitis Canada urges you to become knowledgeable
Surgical Treatment of Inflammatory Bowel Disease (IBD)
") Surgical Treatment of Inflammatory Bowel Disease (IBD) JMAJ 45(2): 55 62, 2002 Tetsuichiro MUTO Vice-Director, Cancer Institute Hospital Abstract: IBD, especially ulcerative colitis (UC) and Crohn s disease
Surgical Treatment of Inflammatory Bowel Disease (IBD) JMAJ 45(2): 55 62, 2002 Tetsuichiro MUTO Vice-Director, Cancer Institute Hospital Abstract: IBD, especially ulcerative colitis (UC) and Crohn s disease
The management and outcome of anastomotic leaks in colorectal surgery
 Original article doi:10.1111/j.1463-1318.2007.01417.x The management and outcome of anastomotic leaks in colorectal surgery A. A. Khan*, J. M. D. Wheeler, C. Cunningham, B. George, M. Kettlewell and N.
Original article doi:10.1111/j.1463-1318.2007.01417.x The management and outcome of anastomotic leaks in colorectal surgery A. A. Khan*, J. M. D. Wheeler, C. Cunningham, B. George, M. Kettlewell and N.
St Mark's Hospital from 1953 to 1968
 Gut, 1970, 11, 235-239 The results of ileorectal anastomosis at St Mark's Hospital from 1953 to 1968 W. N. W. BAKER From St Mark's Hospital, London SUMMARY The popular view of ileorectal anastomosis for
Gut, 1970, 11, 235-239 The results of ileorectal anastomosis at St Mark's Hospital from 1953 to 1968 W. N. W. BAKER From St Mark's Hospital, London SUMMARY The popular view of ileorectal anastomosis for
Operational Efficiency in Colon Surgery Enhanced Recovery Pathways: 23 hour laparoscopic colectomy
 Enhanced Recovery Pathways: 23 hour laparoscopic colectomy Conor P. Delaney MD MCh PhD Chairman, Digestive Disease Institute Professor of Surgery, Cleveland, Ohio Disclosure Slide Conor Delaney MD PhD
Enhanced Recovery Pathways: 23 hour laparoscopic colectomy Conor P. Delaney MD MCh PhD Chairman, Digestive Disease Institute Professor of Surgery, Cleveland, Ohio Disclosure Slide Conor Delaney MD PhD
Inflammatory Bowel Disease RTC 10/30/09
 Inflammatory Bowel Disease RTC 10/30/09 October 30, 1735 2nd President of the United States, John Adams, was born. Prior to becoming president he served 2 terms as Vice President under George Washington.
Inflammatory Bowel Disease RTC 10/30/09 October 30, 1735 2nd President of the United States, John Adams, was born. Prior to becoming president he served 2 terms as Vice President under George Washington.
Laparoscopic Resection Of Colon & Rectal Cancers. R Sim Centre for Advanced Laparoscopic Surgery, TTSH
 Laparoscopic Resection Of Colon & Rectal Cancers R Sim Centre for Advanced Laparoscopic Surgery, TTSH Feasibility and safety Adequacy - same radical surgery as open op. Efficacy short term benefits and
Laparoscopic Resection Of Colon & Rectal Cancers R Sim Centre for Advanced Laparoscopic Surgery, TTSH Feasibility and safety Adequacy - same radical surgery as open op. Efficacy short term benefits and
Index. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A Abdominal surgery prior as factor in laparoscopic colorectal surgery, 554 555 Abscess(es) CRC presenting as, 539 540 Adenocarcinoma of
Index Note: Page numbers of article titles are in boldface type. A Abdominal surgery prior as factor in laparoscopic colorectal surgery, 554 555 Abscess(es) CRC presenting as, 539 540 Adenocarcinoma of
Surgical Workload, Outcome and Research Database: V1.1
 Technical Guidance for Surgical Workload, Outcome and Research Database: V1.1 Contents 1. Standard Indicators... 5 1.1. Activity Volume... 5 1.2. Average Length of Stay (Days)... 5 1.3. 2/7/30 day Re-admission
Technical Guidance for Surgical Workload, Outcome and Research Database: V1.1 Contents 1. Standard Indicators... 5 1.1. Activity Volume... 5 1.2. Average Length of Stay (Days)... 5 1.3. 2/7/30 day Re-admission
Surgical Outcomes of Crohn s Disease: A Single Institutional Experience in Taiwan. [J Soc Colon Rectal Surgeon (Taiwan) 2009;20:1-6]
![Surgical Outcomes of Crohn s Disease: A Single Institutional Experience in Taiwan. [J Soc Colon Rectal Surgeon (Taiwan) 2009;20:1-6]](/thumbs/87/96356608.jpg "Surgical Outcomes of Crohn s Disease: A Single Institutional Experience in Taiwan. [J Soc Colon Rectal Surgeon (Taiwan) 2009;20:1-6]") J Soc Colon Rectal Surgeon (Taiwan) March 2009 Original Article Surgical Outcomes of Crohn s Disease: A Single Institutional Experience in Taiwan Ta-Wen Hsu 1,2 Feng-Fan Chiang 1 Hwei-Ming Wang 1 1 Division
J Soc Colon Rectal Surgeon (Taiwan) March 2009 Original Article Surgical Outcomes of Crohn s Disease: A Single Institutional Experience in Taiwan Ta-Wen Hsu 1,2 Feng-Fan Chiang 1 Hwei-Ming Wang 1 1 Division
Acute Care Surgery: Diverticulitis
 Acute Care Surgery: Diverticulitis Madhulika G. Varma, MD Associate Professor and Chief Section of Colorectal Surgery University of California, San Francisco Modern Treatment of Diverticular Disease Increasing
Acute Care Surgery: Diverticulitis Madhulika G. Varma, MD Associate Professor and Chief Section of Colorectal Surgery University of California, San Francisco Modern Treatment of Diverticular Disease Increasing
Bile Duct Injury during Lap Chole. Bile Duct Injury during cholecystectomy TOPICS. 1. Prevalence, mechanisms, prevention and diagnosis
 Bile Duct Injury during cholecystectomy Catherine HUBERT Jean-Fran François GIGOT Benoît t NAVEZ Division of Hepato-Biliary Biliary-Pancreatic Surgery Department of Abdominal Surgery and Transplantation
Bile Duct Injury during cholecystectomy Catherine HUBERT Jean-Fran François GIGOT Benoît t NAVEZ Division of Hepato-Biliary Biliary-Pancreatic Surgery Department of Abdominal Surgery and Transplantation
Complications and Functional Results after Ileoanal Pouch Formation in Obese Patients
 J Gastrointest Surg (2008) 12:668 674 DOI 10.1007/s11605-008-0465-3 Complications and Functional Results after Ileoanal Pouch Formation in Obese Patients R. P. Kiran & F. H. Remzi & V. W. Fazio & I. C.
J Gastrointest Surg (2008) 12:668 674 DOI 10.1007/s11605-008-0465-3 Complications and Functional Results after Ileoanal Pouch Formation in Obese Patients R. P. Kiran & F. H. Remzi & V. W. Fazio & I. C.
The role of Surgery and Stomas in IBD
 The role of Surgery and Stomas in IBD When do I need it? Can I avoid it? How do I live with it? Kyle G. Cologne, MD Assistant Professor of Surgery USC Division of Colorectal Surgery Topics Surgical Differences
The role of Surgery and Stomas in IBD When do I need it? Can I avoid it? How do I live with it? Kyle G. Cologne, MD Assistant Professor of Surgery USC Division of Colorectal Surgery Topics Surgical Differences
Posterior Deep Endometriosis. What is the best approach? Posterior Deep Endometriosis. Should we perform a routine excision of the vagina??
 Posterior Deep Endometriosis What is the best approach? Dept Gyn Obst Polyclinique Hotel Dieu CHU Clermont Ferrand France Posterior Deep Endometriosis Organs involved - Peritoneum - Uterine cervix -Rectum
Posterior Deep Endometriosis What is the best approach? Dept Gyn Obst Polyclinique Hotel Dieu CHU Clermont Ferrand France Posterior Deep Endometriosis Organs involved - Peritoneum - Uterine cervix -Rectum
Laparoscopic Surgical Approaches for Ulcerative Colitis
 Transcript Details This is a transcript of an educational program accessible on the ReachMD network. Details about the program and additional media formats for the program are accessible by visiting: https://reachmd.com/programs/medical-breakthroughs-from-penn-medicine/laparoscopic-surgicalapproaches-for-ulcerative-colitis/7261/
Transcript Details This is a transcript of an educational program accessible on the ReachMD network. Details about the program and additional media formats for the program are accessible by visiting: https://reachmd.com/programs/medical-breakthroughs-from-penn-medicine/laparoscopic-surgicalapproaches-for-ulcerative-colitis/7261/
Research Article Temporary Fecal Diversion in the Management of Colorectal and Perianal Crohn s Disease
 Hindawi Publishing Corporation Gastroenterology Research and Practice Volume 2015, Article ID 286315, 5 pages http://dx.doi.org/10.1155/2015/286315 Research Article Temporary Fecal Diversion in the Management
Hindawi Publishing Corporation Gastroenterology Research and Practice Volume 2015, Article ID 286315, 5 pages http://dx.doi.org/10.1155/2015/286315 Research Article Temporary Fecal Diversion in the Management
colorectal cancer Colorectal cancer hereditary sporadic Familial 1/12/2018
 colorectal cancer Adenocarcinoma of the colon and rectum is the third most common site of new cancer cases and deaths in men (following prostate and lung or bronchus cancer) and women (following breast
colorectal cancer Adenocarcinoma of the colon and rectum is the third most common site of new cancer cases and deaths in men (following prostate and lung or bronchus cancer) and women (following breast
World Journal of Colorectal Surgery
 World Journal of Colorectal Surgery Volume 5, Issue 1 2015 Article 1 Ileal U Pouch Reconstruction Proximal To Straight Sublevator Ileoanal Anastomosis Following Total Proctocolectomy For Low Rectal Cancer
World Journal of Colorectal Surgery Volume 5, Issue 1 2015 Article 1 Ileal U Pouch Reconstruction Proximal To Straight Sublevator Ileoanal Anastomosis Following Total Proctocolectomy For Low Rectal Cancer
Acute Diverticulitis. Andrew B. Peitzman, MD Mark M. Ravitch Professor of Surgery University of Pittsburgh
 Acute Diverticulitis Andrew B. Peitzman, MD Mark M. Ravitch Professor of Surgery University of Pittsburgh Focus today: when to operate n Recurrent, uncomplicated diverticulitis; after how many episodes?
Acute Diverticulitis Andrew B. Peitzman, MD Mark M. Ravitch Professor of Surgery University of Pittsburgh Focus today: when to operate n Recurrent, uncomplicated diverticulitis; after how many episodes?
, may spread caudally to present as a perianal abscess, laterally across the external sphincter to form an ischiorectal abscess or, rarely,
 ANORECTAL ABSCESSES , may spread caudally to present as a perianal abscess, laterally across the external sphincter to form an ischiorectal abscess or, rarely, superiorly above the anorectal junction
ANORECTAL ABSCESSES , may spread caudally to present as a perianal abscess, laterally across the external sphincter to form an ischiorectal abscess or, rarely, superiorly above the anorectal junction
Disclosures. I am a paid consultant for:
 Surgical Sub-specialization: Colorectal Specialist Peter W. Marcello, M.D. Vice Chairman, Department of Colon & Rectal Surgery Lahey Clinic Burlington, Massachusetts Disclosures I am a paid consultant
Surgical Sub-specialization: Colorectal Specialist Peter W. Marcello, M.D. Vice Chairman, Department of Colon & Rectal Surgery Lahey Clinic Burlington, Massachusetts Disclosures I am a paid consultant
Ein Leben nach tiefer Rektumresektion: Was erwartet unsere Patienten im Langzeitverlauf?
 Ein Leben nach tiefer Rektumresektion: Was erwartet unsere Patienten im Langzeitverlauf? Dieter Hahnloser Klinik für Viszeral- und Transplantationschirurgie UniverstätsSpital Zürich Low Rectal Resection
Ein Leben nach tiefer Rektumresektion: Was erwartet unsere Patienten im Langzeitverlauf? Dieter Hahnloser Klinik für Viszeral- und Transplantationschirurgie UniverstätsSpital Zürich Low Rectal Resection
Surgical strategies in paediatric inflammatory bowel disease
 Submit a Manuscript: http://www.wjgnet.com/esps/ Help Desk: http://www.wjgnet.com/esps/helpdesk.aspx DOI: 10.3748/wjg.v21.i20.6101 World J Gastroenterol 2015 May 28; 21(20): 6101-6116 ISSN 1007-9327 (print)
Submit a Manuscript: http://www.wjgnet.com/esps/ Help Desk: http://www.wjgnet.com/esps/helpdesk.aspx DOI: 10.3748/wjg.v21.i20.6101 World J Gastroenterol 2015 May 28; 21(20): 6101-6116 ISSN 1007-9327 (print)
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE
 NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE Centre for Clinical Practice SCOPE Clinical guideline title: Ulcerative colitis: the management of ulcerative colitis Quality standard title: Ulcerative
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE Centre for Clinical Practice SCOPE Clinical guideline title: Ulcerative colitis: the management of ulcerative colitis Quality standard title: Ulcerative
Endoscopic techniques for surveillance and treatment of FAP
 Endoscopic techniques for surveillance and treatment of FAP Evelien Dekker MD PhD Department of Gastroenterology & Hepatology Academic Medical Center Amsterdam The Netherlands FAP: endoscopic surveillance
Endoscopic techniques for surveillance and treatment of FAP Evelien Dekker MD PhD Department of Gastroenterology & Hepatology Academic Medical Center Amsterdam The Netherlands FAP: endoscopic surveillance
LONG TERM OUTCOME OF ELECTIVE SURGERY
 LONG TERM OUTCOME OF ELECTIVE SURGERY Roberto Persiani Associate Professor Mini-invasive Oncological Surgery Unit Institute of Surgical Pathology (Dir. prof. D. D Ugo) Dis Colon Rectum, March 2000 Dis
LONG TERM OUTCOME OF ELECTIVE SURGERY Roberto Persiani Associate Professor Mini-invasive Oncological Surgery Unit Institute of Surgical Pathology (Dir. prof. D. D Ugo) Dis Colon Rectum, March 2000 Dis
Perianal Fistula of Crohn s Disease
 Case 3 Perianal Fistula of Crohn s Disease A 16 year-old boy referred by surgeon due to perianal fistula since 6mo ago CC=perianal pain History of intermittent non-bloody diarrhea and mild abdominal pain
Case 3 Perianal Fistula of Crohn s Disease A 16 year-old boy referred by surgeon due to perianal fistula since 6mo ago CC=perianal pain History of intermittent non-bloody diarrhea and mild abdominal pain
Surgery and Stomas in IBD When do I need it? Can I avoid it? How do I live with it?
 Surgery and Stomas in IBD When do I need it? Can I avoid it? How do I live with it? Kyle G. Cologne, MD Assistant Professor of Surgery USC Division of Colorectal Surgery Topics Surgical Differences between
Surgery and Stomas in IBD When do I need it? Can I avoid it? How do I live with it? Kyle G. Cologne, MD Assistant Professor of Surgery USC Division of Colorectal Surgery Topics Surgical Differences between
Inflammatory Bowel Disease. Your Illness and Its Treatment
 Inflammatory Bowel Disease Your Illness and Its Treatment What Is Inflammatory Bowel Disease? Inflammatory bowel disease (IBD) is inflammation (irritation and swelling) of the digestive tract. Your digestive
Inflammatory Bowel Disease Your Illness and Its Treatment What Is Inflammatory Bowel Disease? Inflammatory bowel disease (IBD) is inflammation (irritation and swelling) of the digestive tract. Your digestive
Crohn s Disease. Resident Lecture 1/17/19
 Crohn s Disease Resident Lecture 1/17/19 Objectives Features/Classification of Crohn s Disease Medical Treatment Surgical Indications Surgical Considerations 2 Case 25 yo F presents to your office with
Crohn s Disease Resident Lecture 1/17/19 Objectives Features/Classification of Crohn s Disease Medical Treatment Surgical Indications Surgical Considerations 2 Case 25 yo F presents to your office with
Welcome to Week 2 of the Crohn s & Colitis Foundation of America (CCFA) Online Support Group.
 Online Support Group.") Welcome to Week 2 of the Crohn s & Colitis Foundation of America (CCFA) Online. Last week s material consisted of an overview of inflammatory bowel diseases (IBD), specifically Crohn s disease and ulcerative
Welcome to Week 2 of the Crohn s & Colitis Foundation of America (CCFA) Online. Last week s material consisted of an overview of inflammatory bowel diseases (IBD), specifically Crohn s disease and ulcerative
DIGESTIVE SYSTEM SURGICAL PROCEDURES December 22, 2015 (effective March 1, 2016) INTESTINES (EXCEPT RECTUM) Asst Surg Anae
 INTESTINES (EXCEPT RECTUM) Asst Surg Anae") December 22, 2015 (effective March 1, 201) INTESTINES (EXCEPT RECTUM) Z513 Hydrostatic - Pneumatic dilatation of colon stricture(s) through colonoscope... 10.50 Z50 Fulguration of first polyp through colonoscope...
December 22, 2015 (effective March 1, 201) INTESTINES (EXCEPT RECTUM) Z513 Hydrostatic - Pneumatic dilatation of colon stricture(s) through colonoscope... 10.50 Z50 Fulguration of first polyp through colonoscope...
Innovations in rectal cancer surgery TAMIS and transanal TME
 Innovations in rectal cancer surgery TAMIS and transanal TME A.D Hoore MD PhD, EBSQ CR Chair Departement of Abdominal Surgery University Hospitals Leuven, Belgium Actual treatment in rectal Early rectal
Innovations in rectal cancer surgery TAMIS and transanal TME A.D Hoore MD PhD, EBSQ CR Chair Departement of Abdominal Surgery University Hospitals Leuven, Belgium Actual treatment in rectal Early rectal
Laparoscopic vs Robotic Rectal Cancer Surgery: Making it better!
 Laparoscopic vs Robotic Rectal Cancer Surgery: Making it better! Francis Seow- Choen Medical Director Seow-Choen Colorectal Centre Singapore In all situations: We have to use the right tool for the job
Laparoscopic vs Robotic Rectal Cancer Surgery: Making it better! Francis Seow- Choen Medical Director Seow-Choen Colorectal Centre Singapore In all situations: We have to use the right tool for the job
Functional outcome and quality of life after restorative proctocolectomy and ileo-anal pouch anastomosis
 Original article Peer reviewed article SWISS MED WKLY 2009;139(13 14):193 197 www.smw.ch 193 Functional outcome and quality of life after restorative proctocolectomy and ileo-anal pouch anastomosis Philippe
Original article Peer reviewed article SWISS MED WKLY 2009;139(13 14):193 197 www.smw.ch 193 Functional outcome and quality of life after restorative proctocolectomy and ileo-anal pouch anastomosis Philippe
Ileal pouchyanal anastomosis (IPAA) is the procedure
 is the procedure") ORIGINAL CONTRIBUTION Proximal Diversion at the Time of Ileal Pouch Anal Anastomosis for Ulcerative Colitis: Current Practices of North American Colorectal Surgeons Sandra L. de Montbrun, M.D. & Paul M.
ORIGINAL CONTRIBUTION Proximal Diversion at the Time of Ileal Pouch Anal Anastomosis for Ulcerative Colitis: Current Practices of North American Colorectal Surgeons Sandra L. de Montbrun, M.D. & Paul M.
Challenges in IBD: The Post-Op IBD Patient: Preventing Pouchitis & Recurrence
 Challenges in IBD: The Post-Op IBD Patient: Preventing Pouchitis & Recurrence Sharon Dudley-Brown, PHD, FNP-BC, FAAN Assistant Professor Johns Hopkins University Baltimore, MD sdudley2@jhmi.edu Disclosures
Challenges in IBD: The Post-Op IBD Patient: Preventing Pouchitis & Recurrence Sharon Dudley-Brown, PHD, FNP-BC, FAAN Assistant Professor Johns Hopkins University Baltimore, MD sdudley2@jhmi.edu Disclosures
Positioning Biologics in Ulcerative Colitis
 Positioning Biologics in Ulcerative Colitis Bruce E. Sands, MD, MS Acting Chief, Gastrointestinal Unit Massachusetts General Hospital Associate Professor of Medicine Harvard Medical School Sequential Therapies
Positioning Biologics in Ulcerative Colitis Bruce E. Sands, MD, MS Acting Chief, Gastrointestinal Unit Massachusetts General Hospital Associate Professor of Medicine Harvard Medical School Sequential Therapies
Prevention, Diagnosis, and Treatment of Complications of the IPAA for Ulcerative Colitis
 RESIDENT S CORNER Prevention, Diagnosis, and Treatment of Complications of the IPAA for Ulcerative Colitis Stefan D. Holubar, M.D., M.S. Department of Colon & Rectal Surgery, Digestive Disease and Surgery
RESIDENT S CORNER Prevention, Diagnosis, and Treatment of Complications of the IPAA for Ulcerative Colitis Stefan D. Holubar, M.D., M.S. Department of Colon & Rectal Surgery, Digestive Disease and Surgery
Idiopathic inflammatory bowel disease is divided into 2 major disease processes, Crohn disease
 REVIEW ARTICLE Medical and Surgical Management of Chronic Ulcerative Colitis Robert R. Cima, MD; John H. Pemberton, MD Idiopathic inflammatory bowel disease is divided into 2 major disease processes, Crohn
REVIEW ARTICLE Medical and Surgical Management of Chronic Ulcerative Colitis Robert R. Cima, MD; John H. Pemberton, MD Idiopathic inflammatory bowel disease is divided into 2 major disease processes, Crohn
Grand Rounds Laparoscopic Colectomy. 3/12/2007 UCHSC, R.Durbin
 Grand Rounds Laparoscopic Colectomy 3/12/2007 UCHSC, R.Durbin DR 60 yo male with hx of Crohn s s for approx 15 yrs. Referred due to uncontrolled dz despite steroids with approx 10 bowel movements/day,
Grand Rounds Laparoscopic Colectomy 3/12/2007 UCHSC, R.Durbin DR 60 yo male with hx of Crohn s s for approx 15 yrs. Referred due to uncontrolled dz despite steroids with approx 10 bowel movements/day,
Case Report Squamous Cell Carcinoma Originating from a Crohn s Enterocutaneous Fistula
 Hindawi Case Reports in Surgery Volume 2017, Article ID 1929182, 4 pages https://doi.org/10.1155/2017/1929182 Case Report Squamous Cell Carcinoma Originating from a Crohn s Enterocutaneous Fistula Bogdan
Hindawi Case Reports in Surgery Volume 2017, Article ID 1929182, 4 pages https://doi.org/10.1155/2017/1929182 Case Report Squamous Cell Carcinoma Originating from a Crohn s Enterocutaneous Fistula Bogdan
Rectal Cancer. Madhulika G. Varma MD Associate Professor and Chief Section of Colorectal Surgery University of California, San Francisco
 Rectal Cancer Madhulika G. Varma MD Associate Professor and Chief Section of Colorectal Surgery University of California, San Francisco Modern Treatment for Rectal Cancer Improve Local Control Improved
Rectal Cancer Madhulika G. Varma MD Associate Professor and Chief Section of Colorectal Surgery University of California, San Francisco Modern Treatment for Rectal Cancer Improve Local Control Improved
Colorectal Cancer. Nimalan Pathma-Nathan
 Colorectal Cancer Nimalan Pathma-Nathan Introduction Rooms at HSS and Westmead Private Outpatients at Westmead Multidisciplinary clinic Westmead Surgery and scopes HSS Westmead Public, Private and Children
Colorectal Cancer Nimalan Pathma-Nathan Introduction Rooms at HSS and Westmead Private Outpatients at Westmead Multidisciplinary clinic Westmead Surgery and scopes HSS Westmead Public, Private and Children
The Role of Ultrasound in the Assessment of Inflammatory Bowel Disease
 The Role of Ultrasound in the Assessment of Inflammatory Bowel Disease Dr. Richard A. Beable Consultant Gastrointestinal Radiologist Queen Alexandra Hospital Portsmouth Hospitals NHS Trust Topics for Discussion
The Role of Ultrasound in the Assessment of Inflammatory Bowel Disease Dr. Richard A. Beable Consultant Gastrointestinal Radiologist Queen Alexandra Hospital Portsmouth Hospitals NHS Trust Topics for Discussion
Incidence and risk factors of anastomotic leaks. By: khaled Said Assistant professor of colorectal surgery Alexandria
 Incidence and risk factors of anastomotic leaks By: khaled Said Assistant professor of colorectal surgery Alexandria Anastomotic leakage after colorectal surgery is a major and potentially life-threatening
Incidence and risk factors of anastomotic leaks By: khaled Said Assistant professor of colorectal surgery Alexandria Anastomotic leakage after colorectal surgery is a major and potentially life-threatening
Considering whether to have ileal pouch surgery
 Considering whether to have ileal pouch surgery A guide for ulcerative colitis patients By Dr Andrew McCombie (Ulcerative Colitis Researcher and living with an ileal pouch) Co-authored by Associate Professor
Considering whether to have ileal pouch surgery A guide for ulcerative colitis patients By Dr Andrew McCombie (Ulcerative Colitis Researcher and living with an ileal pouch) Co-authored by Associate Professor
Case discussion. Anastomotic leakage. intern superviser
 Case discussion Anastomotic leakage intern superviser Basic data Name : XX ID: M101881671 Age:51 Y Gender: male Past history: Hospitalized for acute diverticulitis on 2004/7/17, 2005/5/28 controlled by
Case discussion Anastomotic leakage intern superviser Basic data Name : XX ID: M101881671 Age:51 Y Gender: male Past history: Hospitalized for acute diverticulitis on 2004/7/17, 2005/5/28 controlled by
Adult organisational audit
 Adult organisational audit Health Information Coding Responses for this section require data for the period between 1/12/13-30/11/14. [Infliximab was introduced for the treatment of ulcerative colitis
Adult organisational audit Health Information Coding Responses for this section require data for the period between 1/12/13-30/11/14. [Infliximab was introduced for the treatment of ulcerative colitis
Prof. Dr. Ahmed ElGeidie Professor of General surgery GEC Dr. Ahmed Abdelrafee
 Prof. Dr. Ahmed ElGeidie Professor of General surgery GEC Dr. Ahmed Abdelrafee Diverticulosis of the colon is the presence of pockets in the wall of the colon called diverticula which may, or may not,
Prof. Dr. Ahmed ElGeidie Professor of General surgery GEC Dr. Ahmed Abdelrafee Diverticulosis of the colon is the presence of pockets in the wall of the colon called diverticula which may, or may not,
UvA-DARE (Digital Academic Repository) Surgical treatment of perianal and rectal fistula van Koperen, P.J. Link to publication
 Surgical treatment of perianal and rectal fistula van Koperen, P.J. Link to publication") UvA-DARE (Digital Academic Repository) Surgical treatment of perianal and rectal fistula van Koperen, P.J. Link to publication Citation for published version (APA): van Koperen, P. J. (2010). Surgical
UvA-DARE (Digital Academic Repository) Surgical treatment of perianal and rectal fistula van Koperen, P.J. Link to publication Citation for published version (APA): van Koperen, P. J. (2010). Surgical
Treatment strategy of metastatic rectal cancer
 35.Schweizerische Koloproktologie-Tagung Treatment strategy of metastatic rectal cancer Gilles Mentha University hospital of Geneva Bern, January 18th, 2014 Colorectal cancer is the third most frequent
35.Schweizerische Koloproktologie-Tagung Treatment strategy of metastatic rectal cancer Gilles Mentha University hospital of Geneva Bern, January 18th, 2014 Colorectal cancer is the third most frequent
19th Annual International Colorectal Disease Symposium An International Exchange of Medical and Surgical Concepts
 Wednesday, February 13, 2008 7-9:00p Early Check-In / Registration (Grand Ballroom Foyer) Thursday, February 14, 2008 6:45 AM Breakfast (Caribbean Ballroom and Foyer) 7:00 AM Registration (Grand Ballroom
Wednesday, February 13, 2008 7-9:00p Early Check-In / Registration (Grand Ballroom Foyer) Thursday, February 14, 2008 6:45 AM Breakfast (Caribbean Ballroom and Foyer) 7:00 AM Registration (Grand Ballroom
Speaker Introduction
 Speaker Introduction Stephen B. Hanauer, MD Professor of Medicine and Clinical Pharmacology University of Chicago Pritzker School of Medicine Chief of Gastroenterology, Hepatology, and Nutrition University
Speaker Introduction Stephen B. Hanauer, MD Professor of Medicine and Clinical Pharmacology University of Chicago Pritzker School of Medicine Chief of Gastroenterology, Hepatology, and Nutrition University
ABC of Colorectal Diseases
 ABC of Colorectal Diseases NON-SPECIFIC INFLAMMATORY BOWEL DISEASE S Pettit, M H Irving Non-specific inflammatory bowel diseases are those for which there is no discernible aetiological agent. The two
ABC of Colorectal Diseases NON-SPECIFIC INFLAMMATORY BOWEL DISEASE S Pettit, M H Irving Non-specific inflammatory bowel diseases are those for which there is no discernible aetiological agent. The two
University of Groningen. Colorectal Anastomoses Bakker, Ilsalien
 University of Groningen Colorectal Anastomoses Bakker, Ilsalien IMPORTANT NOTE: You are advised to consult the publisher's version (publisher's PDF) if you wish to cite from it. Please check the document
University of Groningen Colorectal Anastomoses Bakker, Ilsalien IMPORTANT NOTE: You are advised to consult the publisher's version (publisher's PDF) if you wish to cite from it. Please check the document
COLORECTAL RESECTIONS
 COLORECTAL RESECTIONS What is a colorectal (bowel) resection? Surgery to remove a part of the large bowel is called a resection. Different parts of the colon require different operations and have different
COLORECTAL RESECTIONS What is a colorectal (bowel) resection? Surgery to remove a part of the large bowel is called a resection. Different parts of the colon require different operations and have different
Achieving Success in Ulcerative Colitis: the Role of Infliximab
 Achieving Success in Ulcerative Colitis: the Role of Infliximab Dr Gill Watermeyer IBD clinic Groote Schuur Hospital 17 th August 2012 Inflammatory Bowel Disease Crohn s disease and ulcerative colitis
Achieving Success in Ulcerative Colitis: the Role of Infliximab Dr Gill Watermeyer IBD clinic Groote Schuur Hospital 17 th August 2012 Inflammatory Bowel Disease Crohn s disease and ulcerative colitis
Surgical Management of Advanced Stage Colon Cancer. Nathan Huber, MD 6/11/14
 Surgical Management of Advanced Stage Colon Cancer Nathan Huber, MD 6/11/14 Colon Cancer Overview Approximately 50,000 attributable deaths per year Colorectal cancer is the 3 rd most common cause of cancer-related
Surgical Management of Advanced Stage Colon Cancer Nathan Huber, MD 6/11/14 Colon Cancer Overview Approximately 50,000 attributable deaths per year Colorectal cancer is the 3 rd most common cause of cancer-related
Complications of laparoscopic protective loop ileostomy in patients with colorectal cancer
 ISPUB.COM The Internet Journal of Surgery Volume 19 Number 2 Complications of laparoscopic protective loop ileostomy in patients with colorectal cancer F Puccio, M Solazzo, G Pandolfo, P Marcianò Citation
ISPUB.COM The Internet Journal of Surgery Volume 19 Number 2 Complications of laparoscopic protective loop ileostomy in patients with colorectal cancer F Puccio, M Solazzo, G Pandolfo, P Marcianò Citation
CLINICAL IMPACT OF SEPRAFILM SAFETY AND EFFICACY
 CLINICAL IMPACT OF Post-surgical ADHESIONS SEPRAFILM SAFETY AND EFFICACY Clinical Reviews Clinical studies contents OVERVIEW 3. REDUCED INCIDENCE AND SEVERITY OF ADHESIONS 3.1 Becker JM et al. (1996) 3.2
CLINICAL IMPACT OF Post-surgical ADHESIONS SEPRAFILM SAFETY AND EFFICACY Clinical Reviews Clinical studies contents OVERVIEW 3. REDUCED INCIDENCE AND SEVERITY OF ADHESIONS 3.1 Becker JM et al. (1996) 3.2
Can Robotics be useful to a General Surgeon Performing Colorectal Surgery? Curtis L. Peery MD April 27 th 2018 Throckmorton Surgical Society
 Can Robotics be useful to a General Surgeon Performing Colorectal Surgery? Curtis L. Peery MD April 27 th 2018 Throckmorton Surgical Society 1.Intuitive Surgical 2.C-Sats 3.Virtual Incision Study comparing
Can Robotics be useful to a General Surgeon Performing Colorectal Surgery? Curtis L. Peery MD April 27 th 2018 Throckmorton Surgical Society 1.Intuitive Surgical 2.C-Sats 3.Virtual Incision Study comparing