Paula Wright, CPC, CPC I, CEMC, CPMA
|
|
|
- Curtis Wheeler
- 6 years ago
- Views:
Transcription

1 Paula Wright, CPC, CPC I, CEMC, CPMA
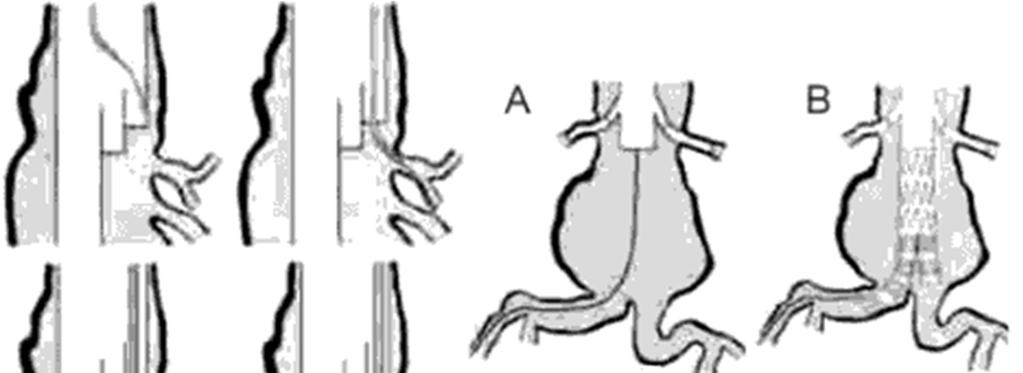
2 Abdominal Aortic Aneurysm Repairs Open direct or endovascular? Was there surgical exposure of an artery? Unilateral or bilateral access (endovascular)? Introduction of catheters? Type of device? 2

3 34800 Endovascular repair of infrarenal abdominal aortic aneurysm or dissection; using aorta aortic tube prosthesis 3
")
4 34802 Endovascular repair of infrarenal abdominal aortic aneurysm or dissection; using modular bifurcated prosthesis (1 docking limb) 4


5 34803 Endovascular repair of infrarenal abdominal aortic aneurysm or dissection; using modular bifurcated prosthesis (2 docking limbs) 5


6 34804 Endovascular repair of infrarenal abdominal aortic aneurysm or dissection; using unibody bifurcated prosthesis 6



7 34805 Endovascular repair of infrarenal abdominal aortic aneurysm or dissection; using aorto uniiliac or unifemoral prosthesis 7
8 34825 Placement of proximal or distal extension prosthesis for endovascular repair of infrarenal abdominal aortic or iliac aneurysm, false aneurysm, or dissection; initial vessel 8
9 Example She then had an Endurant main body device advanced without difficulty through a left sided approach using the Endurant 28x16x145 length device. The contralateral gate was then cannulated from the right side using a guidewire and glide catheter. A contralateral limb was then placed using a 16x16x124 cm length device just proximal to the iliac bifurcation on the right side. On the left she had a distal type 1 endoleak that required the placement of a distal extension limb. Using an Endurant 24x24x82 cm length device was deployed 34802,
10 1 Example This was done in both groins, and after that, a 12 French sheath was placed on the right groin, and on the left, we inserted directly an Endurant 23 rnrn proximal diameter, 166 length, 16 distal diameter Endograft. After confirming the position of the renal arteries and the left hypogastric artery, we deployed the Endograft according to instructions for use without any complications. Using the right groin access, we cannulated the contralateral gate, and after confirming intragraft placement of the wire, we advanced an introducer and then a right iliac limb, 16 proximal diameter, 13 distal diameter, 124 in length, and deployed making sure that the right hypogastric artery remained patent. Balloon angioplasty was then performed within the
11 2 Example..opened the groins surgically in a routine manner and put 5 frnech sheaths within at the level of the common femoral artery. Two superstiff wires went up. We brought the main body from the left side, and pigtailed in from the right side. We did our initial angiogram, at the level of the renals. We went up with the ipsilateral limb, got that into position, marked the level of the internal iliac arteries with an angiogram, deployed very nicely and then went up the contralateral limb and did an angiogram and marked the origin of the internal iliac on that side and deployed the contralateral limb , x2 11
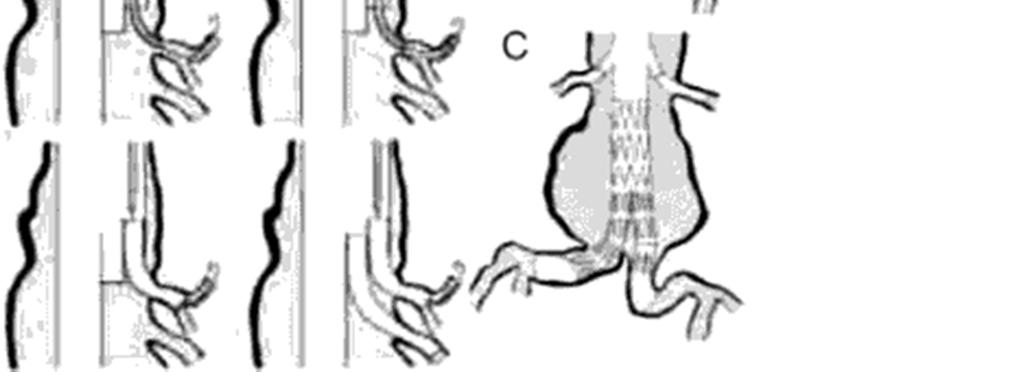
12 34830 Open repair of infrarenal aortic aneurysm or dissection, plus repair of associated arterial trauma, following unsuccessful endovascular repair; tube prosthesis aorto bi iliac prosthesis aorto bifemoral prosthesis 12

13 35081 Direct repair of aneurysm, pseudoaneurysm, or excision (partial or total) and graft insertion, with or without patch graft; for aneurysm, pseudoaneurysm, and associated occlusive disease, abdominal aorta. 13
 and graft insertion, with or without patch graft; for ruptured")
14 35082 Direct repair of aneurysm, pseudoaneurysm, or excision (partial or total) and graft insertion, with or without patch graft; for ruptured aneurysm 14
15 35091 Direct repair of aneurysm, pseudoaneurysm, or excision (partial or total) and graft insertion, with or without patch graft; for aneurysm, pseudoaneurysm, and associated occlusive disease, abdominal aorta involving visceral vessels (mesenteric, celiac, renal) for ruptured aneurysm, abdominal aorta involving visceral vessels (mesenteric, celiac, renal) 15
16 16
17 17
18 35102 Direct repair of aneurysm, pseudoaneurysm, or excision (partial or total) and graft insertion, with or without patch graft; for aneurysm, pseudoaneurysm, and associated occlusive disease, abdominal aorta involving iliac vessels (common, hypogastric, external) for ruptured aneurysm, abdominal aorta involving iliac vessels (common, hypogastric, external) 18

19 35301 Thromboendarterectomy, including patch, if performed; carotid, vertebral, subclavian, by neck incision 19
20 The physician makes an incision in the skin of the neck over the site of plaque or abnormal lining of the carotid, vertebral, or subclavian artery. The vessel is isolated and dissected from adjacent critical structures and vessel clamps are applied. A temporary vascular shunt may be placed, bypassing the area and allowing blood supply to continue uninterrupted during the procedure. The vessel is incised. Using a blunt, spatula like tool, the plaque and the vessel lining are separated from the artery and removed. The edge of the normal artery lining may be sutured to the artery wall to prevent separation when blood flow resumes. After the plaque and lining are removed, a patch graft taken from another portion of the patient's body, a cadaver, or a synthetic source may be applied and sutured to the vessel. This enlarges the diameter of the artery. The vessel clamps are removed and the skin incision is repaired with layered closure 20

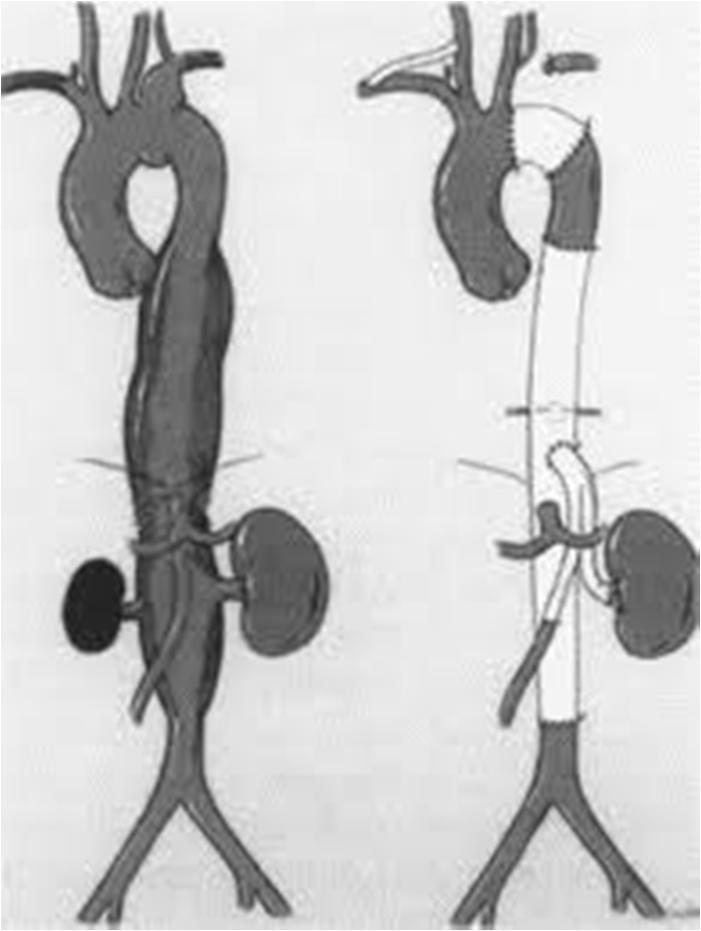
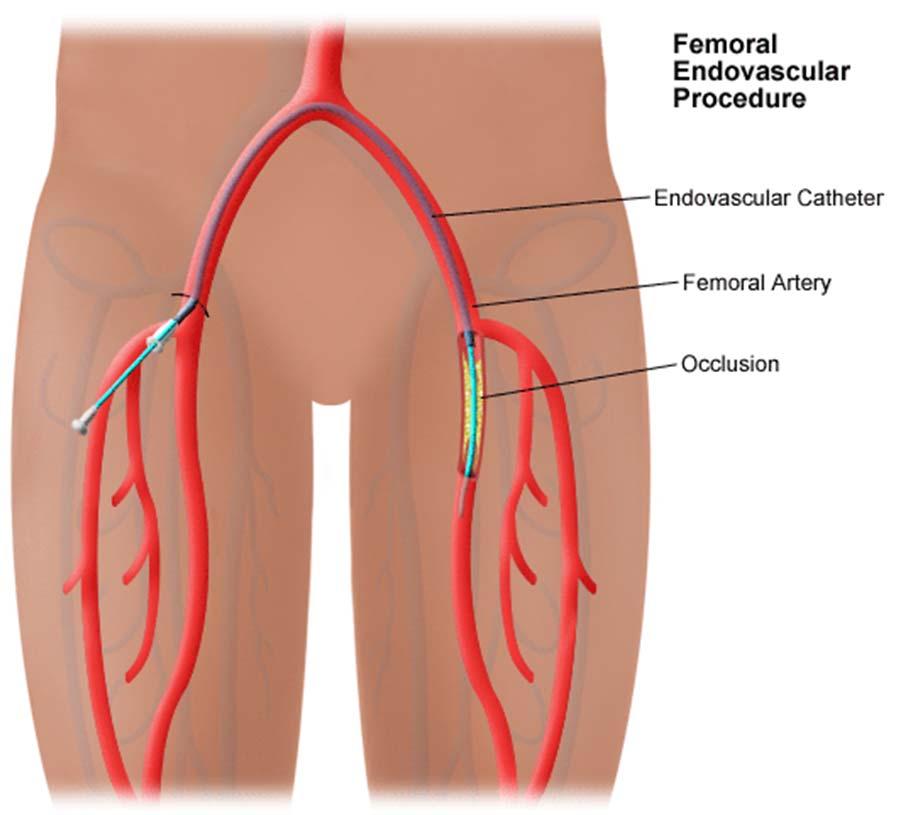
21 35556 Bypass graft, with vein; femoralpopliteal Bypass graft, with other than vein; femoral popliteal 21
22 Through incisions in the skin of the leg overlying the femoral and popliteal arteries, the physician isolates and dissects a section of artery that is damaged or blocked. The physician creates a bypass around the superficial femoral artery, using a harvested vein and one of two methods of repair. Once vessel clamps have been affixed above and below the defect, the superficial femoral artery may be cut through above the damaged or blocked area and sutured to one end of a harvested vein. The vein is passed through a tunnel down the thigh muscles and behind the knee and sutured to the popliteal artery. In the second method, the ends of the harvested vein are sutured into the side of the femoral and popliteal arterial walls, resulting in a bypass of the damaged area. When the clamps are removed, the section of vein forms a new path through which blood can easily bypass the blocked area. The blocked or damaged portion of artery is not removed. After the graft is complete, the skin incisions are repaired with layered closures. 22
23 35583 In situ vein bypass; femoral popliteal In situ vein bypass; femoral anterior tibial, posterior tibial, or peroneal artery In situ vein bypass; popliteal tibial, peroneal 23
24 Through an incision in the skin of the leg overlying the greater saphenous vein, the physician isolates and dissects the greater saphenous vein from adjacent critical structures from the upper thigh to the level of the knee. Vessel clamps are affixed above and below the site of the anastomosis to the femoral and popliteal arteries. All side branches of the saphenous vein are tied off. The vessel's valves are destroyed. The upper end of the saphenous vein is divided and sutured into the femoral artery end to end or end to side. The lower end is divided and sutured into the popliteal artery end to end or end to side. The clamps are removed, and blood flows backward toward the feet, as if the vein were an artery. 24

25 35566 Bypass graft, with vein; femoralanterior tibial, posterior tibial, peroneal artery or other distal vessels Other than vein 25
26 Through incisions in the skin of the leg overlying the superficial femoral artery, the physician isolates and dissects sections of the femoral and anterior tibial, posterior tibial, or peroneal arteries. The physician creates a bypass around the affected artery using a harvested vein. Once vessel clamps have been affixed above and below the defect, the superficial femoral artery may be cut through above the damaged area and sutured to one end of a harvested vein, which is passed through an intramuscular tunnel and sutured to the anterior tibial, posterior tibial, peroneal, or other distal vessel. In the second method, the ends of the harvested vein are sutured to the side of the femoral artery and anterior tibial, posterior tibial, peroneal, or other distal vessel wall, resulting in a bypass of the damaged area. When the clamps are removed, the section of vein forms a new path through which blood can easily bypass the blocked area. The blocked or damaged portion of artery is left in place and not removed. After the graft is complete, the skin incisions are repaired with layered closures. 26

27 35558 Bypass graft, with vein; femoralfemoral Bypass graft, with other than vein; femoral femoral 27
28 Through incisions in the skin of the upper thighs, the physician isolates and dissects a section of the femoral arteries. The physician creates a bypass using a harvested vein. Once vessel clamps have been affixed above and below the area of anastomosis, the femoral artery may be cut through below the damaged area and sutured to one end of a harvested vein, which is sutured to the femoral artery in the opposite leg, resulting in a bypass of the damaged or blocked area. When the clamps are removed, the section of vein forms a new path through which blood can easily bypass the blocked area. The blocked or damaged portion of the artery is not removed. After the graft is complete, the skin incisions are repaired with layered closures 28

29 35565 Bypass graft, with vein; iliofemoral Bypass graft, other Than vein; iliofemoral 29
30 Through incisions in the skin of the lower abdomen overlying the iliac artery and in the skin of the upper thigh overlying the femoral artery, the physician isolates and dissects a section of common iliac artery. The physician creates a bypass around the iliac artery, using a harvested vein and one of two methods of repair. Once vessel clamps have been affixed above and below the defect, the iliac artery may be cut or tied off with sutures above the damaged area and sutured to one end of a harvested vein. The graft is passed through a tunnel on the inside of the upper thigh and is sutured to the side of the femoral artery. In the second method, the end of the harvested vein is sutured to the side of the iliac artery. Either method results in a bypass of the damaged area. When the clamps are removed, the section of vein forms a new path through which blood can easily bypass the blocked area. After the graft is complete, the skin incisions are repaired with layered closures. 30
31 35571 Bypass graft, with vein; popliteal tibial, peroneal artery or other distal vessels other than vein 31
32 Through incisions in the skin of the leg overlying the popliteal arteries, the physician isolates and dissects a section of arteries from adjacent critical structures. The physician creates a bypass around the artery, using a harvested vein and one of two methods of repair. Once vessel clamps have been affixed above and below the defect, the popliteal artery may be cut through above the damaged area and sutured to one end of a harvested vein, which is sutured to the tibial, peroneal, or other distal artery. In the second method, the ends of the harvested vein are sutured into the side of the popliteal and the tibial or peroneal arterial wall resulting in a bypass of the damaged area. When the clamps are removed, the section of vein forms a new path through which blood can easily bypass the blocked area. After the graft is complete, the incisions are repaired with layered closures. 32

33 Bypass Graft Bypass graft, with other than vein; axillary femoral femoral 33
34 Through an incision in the skin of the axilla and both upper thighs, the physician creates a bypass around a section of lower aorta that is damaged or blocked, using a synthetic graft. Once vessel clamps have been affixed above and below the defect, the synthetic graft is sutured to the side of the axillary artery and passed through a subcutaneous tunnel to the upper thigh where it is sutured end to end or end to side to the femoral artery. A second synthetic graft is sutured end to side to the femoral artery and passed through another subcutaneous tunnel to the opposite thigh where it is sutured end to end or end to side to the femoral artery. The section of blocked artery is not removed. When the clamps are removed, the two synthetic grafted limbs form a new path through which blood can easily bypass the blocked area. After the graft is complete, the skin incisions are repaired with layered closures. 34
35 Carotid Artery Stenting Transcatheter placement of intravascular stent(s), cervical carotid artery, percutaneous; with distal embolic protection Transcatheter placement of intravascular stent(s), cervical carotid artery, percutaneous; without distal embolic protection 35

36 Carotid Artery Stenting 36
37 The physician places an intravascular stent percutaneously through a catheter into the cervical carotid artery. A needle is inserted through the skin into the access blood vessel, usually the brachial or femoral artery. A guidewire is threaded through the needle into the cervical carotid artery and the needle is removed. Long sheaths or guiding catheters are advanced into the stenosed cervical carotid artery. A filter protection device may be inserted distal to the stenosis to capture emboli. After filter opening, predilation of the stenosis with angioplasty balloons may be performed. A catheter with a stent transporting tip is threaded over the guidewire into the vessel, and the wire is extracted. The catheter travels to the point where the vessel needs additional support. The compressed stent is passed from the catheter out into the vessel, where it deploys, expanding to support the vessel walls. The catheter is removed and pressure is applied over the puncture site 37

38 35472 Transluminal balloon angioplasty, percutaneous; aortic 38
39 ENDOVASCULAR REVASCULARIZATION 39
40 ENDOVASCULAR REVASCULARIZATION Three arterial vascular territories Iliac Femoral/Popliteal Tibial/Peroneal»Angioplasty»Atherectomy»Stent placement 40

41 Iliac Territory Femoral/Popliteal Territory Tibial/Peroneal Territory 41

42 ENDOVASCULAR REVASCULARIZATION Iliac Territory Common Iliac Internal Iliac External Iliac 42
43 37220 Revascularization, endovascular, open or percutaneous, iliac artery, unilateral, initial vessel; with transluminal angioplasty with transluminal stent placement(s), includes angioplasty within same vessel, when performed Revascularization, endovascular, open or percutaneous, iliac artery, each additional ipsilateral vessel; with transluminal angioplasty with transluminal stent placement(s), includes angioplasty within same vessel, when performed 43
44 A patient with no prior angiograms is scheduled for angiography and possible intervention due to right leg pain. The physician punctures the left common femoral and performs an aortogram and bilateral extremity angiograms. These reveal stenosis of the right iliac vessels. The physician therefore performs angioplasty of the right common iliac and angioplasty and stent placement in the right external iliac (rt external iliac), (rt common iliac), 75625,
45 A patient with no prior catheter angiograms is scheduled for angiography and possible intervention. The physician punctures the right femoral artery and performs an abdominal aortogram and bilateral lower extremity angiograms. The angiograms reveal stenosis of the left common iliac and the right external iliac. The physician performs angioplasty and stent placement in the left common iliac and angioplasty in the right external iliac, all via the right common femoral access lt common iliac, rt external iliac, 75625,

46 ENDOVASCULAR REVASCULARIZATION Femoral/Popliteal Territory Common Femoral Lateral Circumflex Profunda Femoris Medial Descending Lateral Descending Perforating Branches Superficial Femoral Popliteal Geniculate 46
47 37224 Revascularization, endovascular, open or percutaneous, femoral/popliteal artery(s), unilateral, initial vessel; with transluminal angioplasty with atherectomy, includes angioplasty within the same vessel, when performed with transluminal stent placement(s), includes angioplasty within same vessel, when performed with transluminal stent placement(s) and atherectomy, includes angioplasty within same vessel, when performed 47
48 A patient with no prior angiograms undergoes an abdominal aortogram and bilateral lower extremity angiogram via right femoral access, which reveals stenosis of the left superficial femoral artery (SFA). The physician therefore performs angioplasty and stent placement in this vessel , 75625,
49 A patient with prior angiograms that showed lesions of the right SFA and popliteal. He returns for intervention. Via left femoral access, the physician performs a right lower extremity angiogram, followed by angioplasty and stent placement in the right SFA and angioplasty of the right popliteal
50 ENDOVASCULAR REVASCULARIZATION Tibial/Peroneal Territory Common Tibio peroneal Trunk Anterior Tibial Peroneal Posterior Tibial 50
51 37228 Revascularization, endovascular, open or percutaneous, tibial/peroneal artery, unilateral, initial vessel; with transluminal angioplasty with atherectomy, includes angioplasty within same vessel, when performed with transluminal stent placement(s), includes angioplasty within same vessel, when performed with transluminal stent placement and atherectomy, includes angioplasty within same vessel, when performed 51
52 37232 Revascularization, endovascular, open or percutaneous, tibial/peroneal, unilateral, each additional vessel; with transluminal angioplasty with atherectomy, includes angioplasty within the same vessel, when performed Revascularization, with transluminal endovascular, stent placement(s), open or includes percutaneous, angioplasty tibial/peroneal, within the unilateral, same vessel, each when performed additional vessel; with transluminal angioplasty with transluminal stent placement(s) and atherectomy, includes angioplasty within the same vessel, when performed 52
53 A patient has had prior angiograms showing severe disease of both lower legs and returns for intervention. The physician punctures the right common femoral artery and via antegrade approach, performs angioplasty of the anterior tibial artery and angioplasty and atherectomy of the posterior tibial artery. Then the physician punctures the left popliteal artery and via antegrade approach, performs angioplasty and stent placement in the left peroneal artery rt posterior tibial, lt peroneal, rt anterior tibial 53
54 A patient has had prior angiograms showing stenosis of the infrapopliteal vessels in the right leg. The physician punctures the right common femoral and deploys a drug eluting stent in the right tibioperoneal trunk. He also performs angioplasty of the right posterior tibial artery
55 3 Setup shots were done from the common femoral region demonstrating high grade disease in the popliteal of the left lower extremity. A wire was then placed down the posterior tibial and an SS Fox Hollow cutter was then utilized and multiple passes were made over below knee popliteal region with excellent results. Then attention was turned to the posterior tibial artery, which was done with the same cutter. Following this, a 3.0 x 100 balloon was utilized and the posterior tibial was ballooned at about 10 atmospheres. 55
56 3 Then attention turned to the peroneal artery. This was cut with the SS Fox Hollow cutter and then ballooned with a 2.5x 150 NanoCross balloon
57 Example A 7 French Ansel sheath was placed into the left common femoral region from the right groin. Catheter was placed in the popliteal, then an Xpeedior AngioJet catheter was utilized and at that time, we made multiple passes. Flow was restored in the vessel with stenotic tissue proximally and distally. We decided that we would stent over the remaining stenosis. A 6 x 20 balloon was then utilized to pre dilate that area where there was remaining stenosis and then a Supera stent was deployed extending past
58 Atherectomy 0234T Transluminal peripheral atherectomy, including radiological supervision and interpretation; renal artery 0235T visceral artery 0236T abdominal aorta 0237T brachiocephalic trunk and branches, each 0238T iliac artery, each vessel (above the inguinal ligaments 58

59 0238T Atherectomy provided in iliac above the inguinal ligament 59

60 60

61 Colectomy and Proctectomy 61

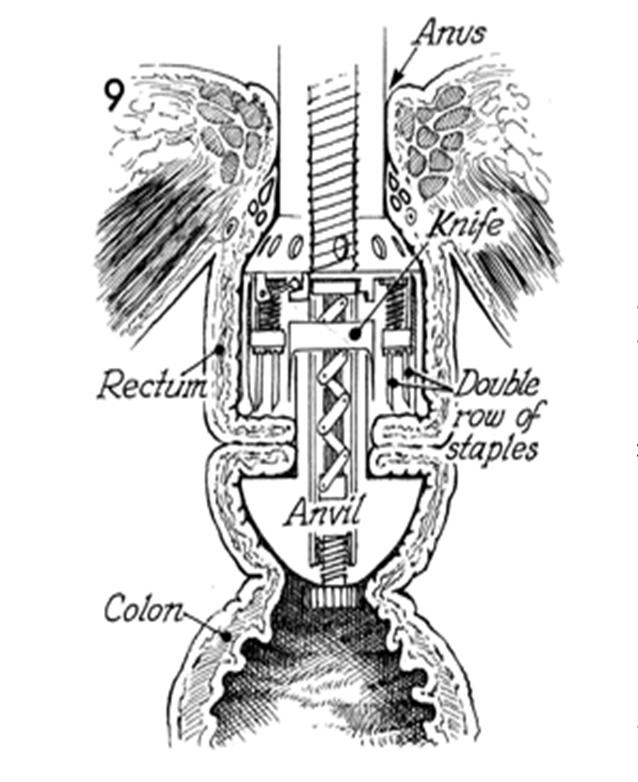
62 Stapler 62
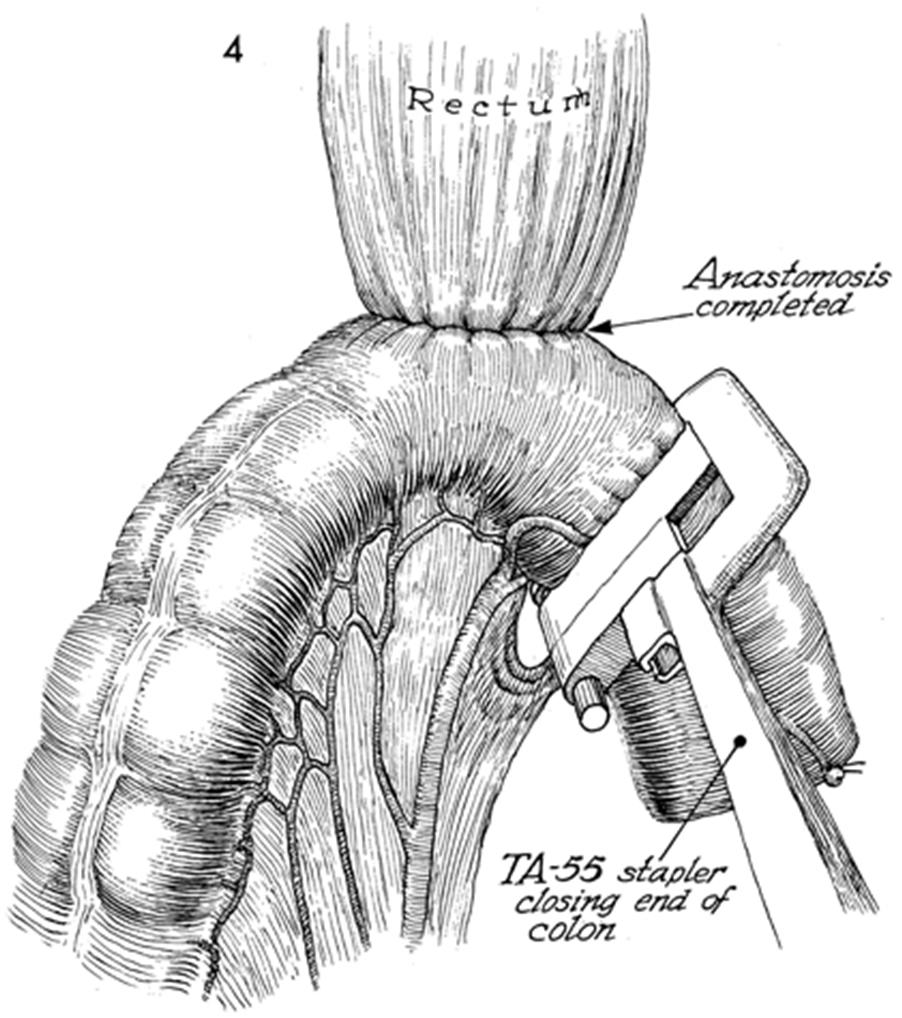
63 63

64 44140 Colectomy, partial; with anastomosis Laparoscopic 64
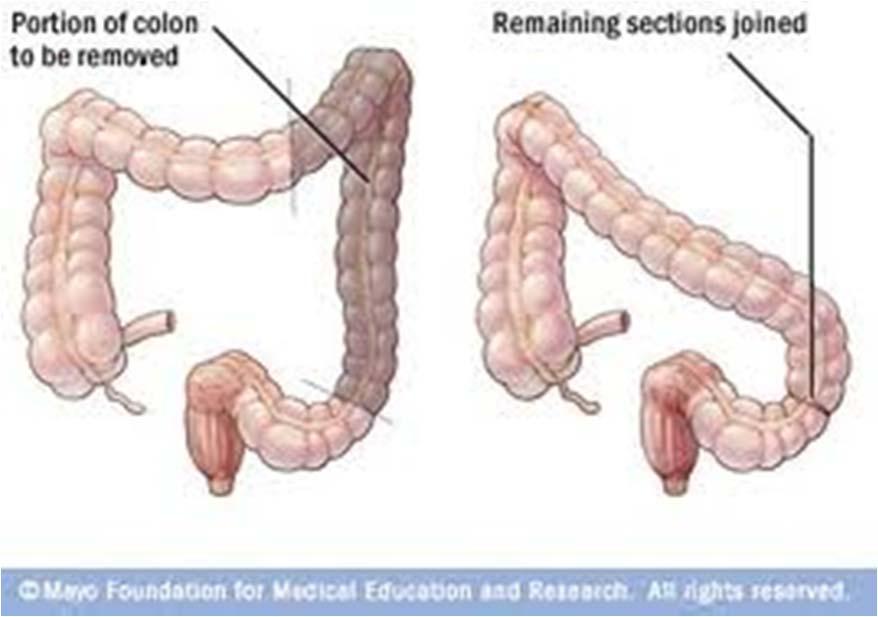
65 Hemicolectomy 65

66 Colectomy 66
67 I then took the left colon proximal and distal to the mass which allowed us a little bit of mobility, took the mesentery of the colon thus freeing the mass inferiorly. We were able to remove the mass intact. This brought the tranvserse colon to the descending colon, I performed a side toside hand sewn anastomosis with an outer layer of silk and an inner layer of Maxon

68 44141 Colectomy, partial; with skin level cecostomy or colostomy 68
69 The physician resects a segment of colon and brings the proximal end of colon through the abdominal wall onto the skin as a colostomy. The physician makes an abdominal incision. Next, the selected segment of colon is isolated and divided proximally and distally to the remaining colon and removed. The proximal end of colon is brought through a separate incision on the abdominal wall and onto the skin as a colostomy. Alternately, the remaining bowel ends may be reapproximated and a loop of colon proximal to the anastomosis brought through a separate incision on the abdominal wall onto the skin as a loop colostomy. 69
 44206 Laparoscopic")
70 44143 Colectomy, partial; with end colostomy and closure of distal segment (Hartmann type procedure) Laparoscopic 70
71 The physician resects a segment of colon and brings the proximal end of colon through the abdominal wall onto the skin as a colostomy. The physician makes an abdominal incision. Next, the selected segment of colon is isolated and divided proximally and distally to the remaining colon and removed. The proximal end of colon is brought through a separate incision on the abdominal wall onto the skin as a colostomy. The distal end of colon is closed with staples or sutures and left in the abdomen. The initial incision is closed 71


72 44144 Colectomy, partial; with resection, with colostomy or ileostomy and creation of mucofistula 72
73 The physician resects a segment of colon. The proximal and distal ends of colon are brought through the abdominal wall onto the skin as a colostomy and mucus fistula. The physician makes an abdominal incision. Next, the selected segment of colon is isolated and divided proximally and distally to the remaining colon and removed. The proximal end of colon or terminal ileum and the distal end of colon are brought through separate incisions on the abdominal wall onto the skin as an ileostomy or colostomy and mucus fistula. The initial abdominal incision is closed. 73
74 44145 Colectomy, partial; with coloproctostomy (low pelvic anastomosis) Laparoscopic 74
75 The physician resects a segment of distal colon or rectum and performs a low colorectal anastomosis in the pelvis. The physician makes an abdominal incision. Next, the distal colon and rectum are mobilized and the selected segment divided proximally and distally to the remaining colon. An anastomosis is created between the proximal colon and remaining rectum in the pelvis with staples or sutures. The incision is closed. 75
, with colostomy 44208 Laparoscopic")
76 44146 Colectomy, partial; with coloproctostomy (low pelvic anastomosis), with colostomy Laparoscopic 76
77 The physician resects a segment of distal colon or rectum and performs a low colorectal anastomosis in the pelvis and creates a proximal colostomy. The physician makes an abdominal incision. Next, the distal colon and rectum are mobilized and the selected segment of diseased colon and/or rectal tissue is removed. The new ends are brought together and an anastomosis is done between the colon and the rectum low in the pelvis with staples or sutures (coloproctostomy). A loop of colon above the newly sutured anastomosis is brought out through a separate incision in the abdominal wall and fixed there so the colon will empty through this artificial opening in the skin as a colostomy, usually temporary, to divert the fecal stream while the anastomosis heals. The initial incision is closed. 77

78 44147 Colectomy, partial; abdominal and transanal approach 78
79 The physician removes a segment of colon through a combined abdominal and transanal approach and reapproximates the remaining ends of the colon. The physician makes an abdominal incision. The distal colon and rectum are mobilized also by using a transanal approach. The segment of the colon to be eliminated is divided at the appropriate distal and proximal points and the remaining ends are anastomosed. The abdominal and transanal incisions are closed 79

80 44160 Colectomy, partial, with removal of terminal ileum with ileocolostomy Laprascopic 80
81 The physician makes an abdominal incision and removes a segment of the colon and terminal ileum and performs an anastomosis between the remaining ileum and colon. The physician makes an abdominal incision. Next, the selected segment of colon and terminal ileum are isolated and divided proximal and distal to the remaining bowel and removed. An anastomosis is created between the distal ileum and remaining colon with staples or sutures. The incision is closed. 81


82 44150 Colectomy, total, abdominal, without proctectomy; with ileostomy or ileoproctostomy Laparoscopic OR With rectum preserved 82
83 The physician removes the entire colon and performs an ileostomy or an anastomosis between the ileum and rectum. The physician makes an abdominal incision. Next, the colon is mobilized and the colorectal junction and terminal ileum is divided. The colon is removed. The terminal ileum is approximated to the rectum or brought out through a separate incision on the abdominal wall onto the skin as an ileostomy. The initial incision is closed. 83

84 44151 Colectomy, total, abdominal, without proctectomy; with continent ileostomy 84
85 The physician removes the entire colon and creates a reservoir of distal ileum (Kock pouch). The reservoir is brought out through the abdominal wall as a continent stoma. The physician makes an abdominal incision. Next, the colon is mobilized. The colorectal junction and terminal ileum is divided and the colon removed. The distal ileum is folded upon itself and approximated to form a pouch and valve. The distal end of the pouch is brought through a separate incision on the abdominal wall onto the skin as a continent ileostomy. The initial incision is closed. 85

86 44155 Colectomy, total, abdominal, with proctectomy; with ileostomy Laparoscopic 86
87 The physician removes the entire colon and rectum and brings the terminal ileum out through the abdominal wall onto the skin as an ileostomy. The physician makes an abdominal incision. Next, the colon and rectum are mobilized, the proximal rectum and distal ileum are divided, and the colon and proximal rectum are removed. The distal rectum is mobilized and removed through a perineal approach. The terminal ileum is brought out through a separate incision on the abdominal wall onto the skin as an ileostomy. The abdominal and perineal incisions are closed 87
88 44156 Colectomy, total, abdominal, with proctectomy; with continent ileostomy 88


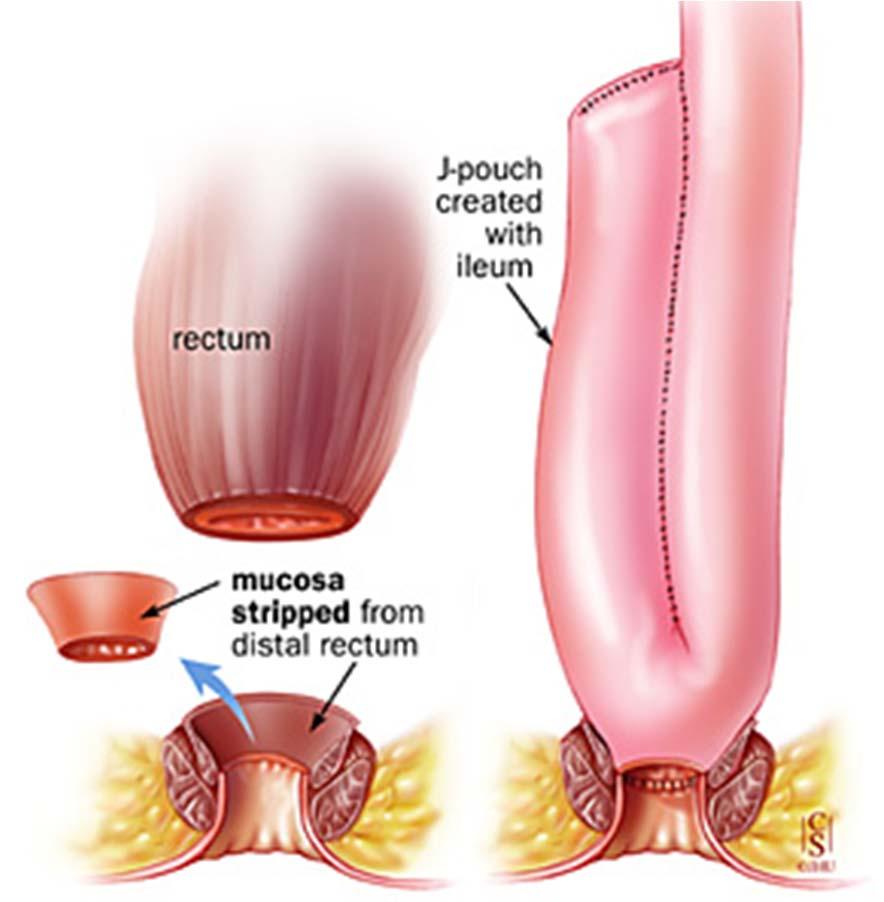
89 44157 Colectomy, total, abdominal, with proctectomy; with ileoanal anastomosis, includes loop ileostomy, and rectal mucosectomy, when performed 89
, includes loop ileostomy, and rectal mucosectomy, when performed 44211")
90 44158 Colectomy, total, abdominal, with proctectomy; with ileoanal anastomosis, creation of ileal reservoir (S or J), includes loop ileostomy, and rectal mucosectomy, when performed Laparoscopic 90
91 91

92 45110 Proctectomy; complete, combined abdominoperineal, with colostomy Laparoscopic 92
93 The physician removes the entire rectum and anus and forms a colostomy. The physician makes an abdominal incision. The proximal rectum is mobilized within the abdomen to the level of the sphincter muscles and the colon is divided above the pelvic brim. An incision is made around the anus from a perineal approach and the anus and distal rectum are dissected free of surrounding structures and the anus and rectum are removed. The proximal end of colon is brought out through a separate incision on the abdominal wall as a colostomy. The abdominal and perineal incisions are closed. 93

94 45111 Proctectomy; partial resection of rectum, transabdominal approach 94
95 The physician removes the proximal rectum. The physician makes an abdominal incision. The distal colon and rectum are mobilized and divided proximal and distal to the segment of interest. The colon and distal rectum may be reapproximated or the proximal end of colon may be brought out through a separate incision on the abdominal wall as a colostomy and the remaining rectum closed with staples or sutures. The initial incision is closed. 95


96 45112 Proctectomy, combined abdominoperineal, pull through procedure (eg, colo anal anastomosis) 96
97 The physician removes the rectum and performs an anastomosis between the colon and the anus. The physician makes an abdominal incision. The distal colon and rectum are mobilized within the abdomen to the level of the sphincter muscles. The colon is divided above the pelvic brim and the rectum at the level of the sphincter muscles and removed. The mucosa may be stripped from the remaining distal rectum from a perineal approach. The distal colon is pulled through the sphincter complex and approximated to the anus with sutures. The incision is closed. 97

, with or without")
98 45113 Proctectomy, partial, with rectal mucosectomy, ileoanal anastomosis, creation of ileal reservoir (S or J), with or without loop ileostomy 98
99 The physician removes the proximal rectum, strips the mucosa from the distal rectum and performs an anastomosis between an ileal pouch and the anus. The physician makes an abdominal incision. The distal colon and rectum are mobilized within the abdomen to the level of the sphincter muscles. The colon is divided above the pelvic brim and the rectum is divided above the sphincter muscles and removed. The mucosa of the distal rectum is stripped from a perineal approach. The distal ileum is folded upon itself and approximated in order to form a reservoir. The ileal pouch is pulled through the remaining muscular cuff of distal rectum and sutured to the anus. A loop ileostomy may be formed proximal to the anastomosis. The incision is closed. 99
100 45114 Proctectomy, partial, with anastomosis; abdominal and transsacral approach transsacral approach only (Kraske type) An incision is made posteriorly at the junction of the sacrum and coccyx. The coccyx is excised. Dissection is continued posteriorly to further mobilize the rectum. The rectum is divided distally and the excised segment is removed. The distal end of colon is approximated to the remaining rectal stump with sutures or staples. The incisions are closed. 100
101 45119 Proctectomy, combined abdominoperineal pull through procedure (eg, colo anal anastomosis), with creation of colonic reservoir (eg, J pouch), with diverting enterostomy when performed Laparoscopic 101
102 The physician surgically removes the rectum. The physician makes an abdominal incision, and the distal part of the diseased colon and rectum are mobilized down to the level of the anal sphincter muscles. The rectum is incised at the level of the sphincter muscles while the colon is incised above the pelvic brim where it is disease free. The diseased colon and rectum are removed. The free end of the distal colon is brought through the sphincter complex and approximated with the anus to form a colo anal anastomosis. The distal colon is folded and sutured in such a way as to create a colonic reservoir pouch. The physician may elect to bring a loop or end of the colon through a separate abdominal incision to create a stoma (enterostomy). 102
103 45120 Proctectomy, complete (for congenital megacolon), abdominal and perineal approach; with pullthrough procedure and anastomosis eg, Swenson, Duhamel, or Soave type operation) 103
104 The physician removes or bypasses the diseased rectal segment and performs an anastomosis of the colon and anus. The physician makes an abdominal incision. The rectum and distal colon are mobilized and the colon is divided just proximal to the diseased rectal segment. The rectal segment may be removed and the distal colon pulled through the sphincter complex and approximated to the anus with sutures from a perineal approach. Alternatively, the distal colon may be pulled down and approximated to the anus with sutures, bypassing the diseased rectal segment with a combined longitudinal anastomosis between the colon and the diseased rectal segment. The incision is closed. 104
105 45216 Pelvic exenteration for colorectal malignancy, with proctectomy (with or without colostomy), with removal of bladder and ureteral transplantations, and/or hysterectomy, or cervicectomy, with or without removal of tube(s), with or without removal of ovary(s), or any combination thereof 105

106 45130 Excision of rectal procidentia, with anastomosis; perineal approach abdominal & perineal approach 106
107 107
108 The physician removes a rectal prolapse through a perineal approach. The physician prolapses the rectum and colon through the anus. A circular incision is made through the distal rectum at the anorectal junction. The mesentery and blood supply to the prolapsed rectum is divided and the segment is telescoped out through the anus. The proximal rectum or colon is divided and the prolapsed segment is removed. The proximal end of rectum or colon is approximated to the anus with sutures or staples. 108
109 45160 Excision of rectal tumor by proctotomy, transsacral or transcoccygeal approach 109
110 The physician removes a rectal tumor through a transsacral or transcoccygeal approach. The physician makes an incision at the junction of the sacrum and coccyx. The coccyx is excised and dissection is continued posteriorly to mobilize the rectum. The tumor is identified, an incision is made in the rectum (proctotomy), and the tumor is excised. The rectum is closed with sutures or staples. The initial incision is closed. 110
, with sigmoid resection 45550 Open")
111 45402 Laparoscopy, surgical; proctopexy (for prolapse), with sigmoid resection Open 111
112 The physician completely mobilizes the rectum down to the pelvic floor and attaches the rectum to the sacrum using polypropylene mesh. The mesh is initially stapled to the sacral hollow and sutured on both sides of the rectum. The sigmoid resection is performed in conjunction with the proctopexy. Using a laparoscope, the physician mobilizes the sigmoid colon and rectum. The redundant segment of sigmoid colon and rectum are excised and an anastomosis is created between the remaining bowel ends with sutures or staples 112
2017 Cardiology Survival Guide
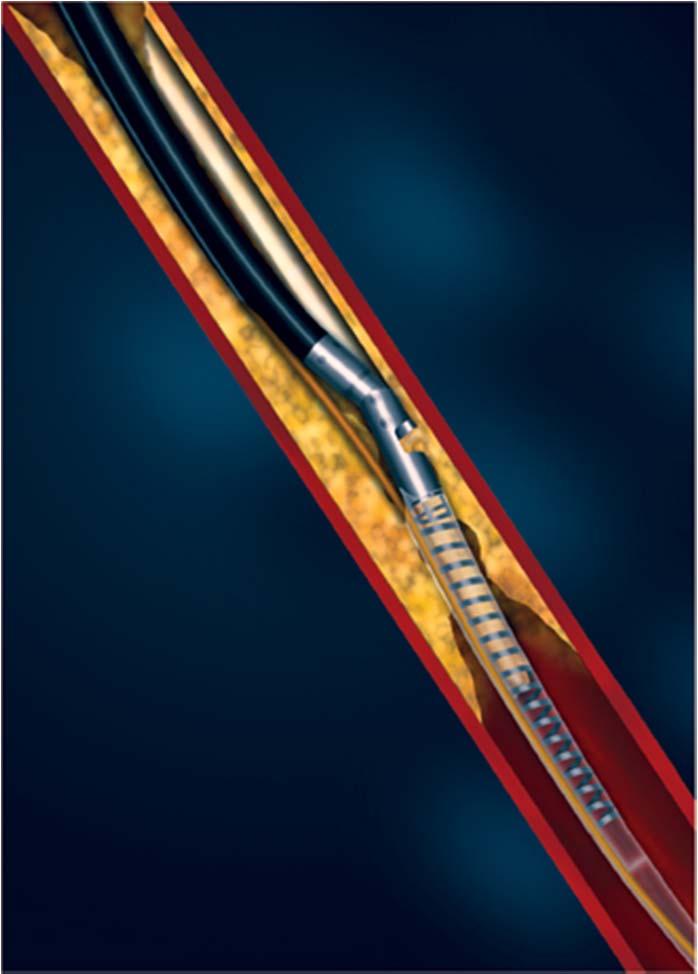
 2017 Cardiology Survival Guide Chapter 2: Angioplasty/Atherectomy/Stent The term angioplasty literally means "blood vessel repair." During an angioplasty procedure, the physician inserts a catheter, with
2017 Cardiology Survival Guide Chapter 2: Angioplasty/Atherectomy/Stent The term angioplasty literally means "blood vessel repair." During an angioplasty procedure, the physician inserts a catheter, with
Schedule of Benefits. for Professional Fees Vascular Procedures
 Schedule of Benefits for Professional Fees 2018 Vascular Procedures ANASTOMOSIS RULES 820 Arteriovenous anastomosis in arm 1453 Arteriovenous anastomosis, open by basilic vein transposition 1465 Splenorenal
Schedule of Benefits for Professional Fees 2018 Vascular Procedures ANASTOMOSIS RULES 820 Arteriovenous anastomosis in arm 1453 Arteriovenous anastomosis, open by basilic vein transposition 1465 Splenorenal
SAMPLE EDITION PELVIC AND LOWER EXTREMITY ARTERIES WITH ENDOVASCULAR REVASCULARIZATION. Cardiovascular Illustrations and Guidelines
 Cardiovascular Illustrations and Guidelines PELVIC AND LOWER EXTREMITY ARTERIES WITH ENDOVASCULAR REVASCULARIZATION ANGIOPLASTY INTRAVASCULAR STENT PLACEMENT ATHERECTOMY For Fem-Pop Territory Angioplasty
Cardiovascular Illustrations and Guidelines PELVIC AND LOWER EXTREMITY ARTERIES WITH ENDOVASCULAR REVASCULARIZATION ANGIOPLASTY INTRAVASCULAR STENT PLACEMENT ATHERECTOMY For Fem-Pop Territory Angioplasty
RadRx Your Prescription for Accurate Coding & Reimbursement Copyright All Rights Reserved.
 Interventional Radiology Coding Case Studies Prepared by Stacie L. Buck, RHIA, CCS-P, RCC, CIRCC, AAPC Fellow President & Senior Consultant Week of November 19, 2018 Abdominal Aortogram, Bilateral Runoff
Interventional Radiology Coding Case Studies Prepared by Stacie L. Buck, RHIA, CCS-P, RCC, CIRCC, AAPC Fellow President & Senior Consultant Week of November 19, 2018 Abdominal Aortogram, Bilateral Runoff
Morbidity Audit and Logbook Tool SNOMED Board Reporting Terms for SET and IMG Vascular Surgery AMPUTATION AORTA
 SNOMED s for SET and IMG Vascular Surgery AMPUTATION Amputation above-knee Amputation of leg through tibia and fibula Amputation of the foot Amputation of toe Through knee amputation Ray amputation of
SNOMED s for SET and IMG Vascular Surgery AMPUTATION Amputation above-knee Amputation of leg through tibia and fibula Amputation of the foot Amputation of toe Through knee amputation Ray amputation of
Primary to non-coronary IVUS
 codes 2018 2018 codes Primary to non-coronary IVUS Page 2 All coding, coverage, billing and payment information provided herein by Philips is gathered from third-party sources and is subject to change.
codes 2018 2018 codes Primary to non-coronary IVUS Page 2 All coding, coverage, billing and payment information provided herein by Philips is gathered from third-party sources and is subject to change.
RadRx Your Prescription for Accurate Coding & Reimbursement Copyright All Rights Reserved.
 Interventional Radiology Coding Case Studies Prepared by Stacie L. Buck, RHIA, CCS-P, RCC, CIRCC, AAPC Fellow President & Senior Consultant Week of June 4, 2018 Thrombolysis, Thrombectomy & Angioplasty
Interventional Radiology Coding Case Studies Prepared by Stacie L. Buck, RHIA, CCS-P, RCC, CIRCC, AAPC Fellow President & Senior Consultant Week of June 4, 2018 Thrombolysis, Thrombectomy & Angioplasty
RadRx Your Prescription for Accurate Coding & Reimbursement Copyright All Rights Reserved.
 Interventional Radiology Coding Case Studies Prepared by Stacie L. Buck, RHIA, CCS-P, RCC, CIRCC, AAPC Fellow President & Senior Consultant INDICATION: Abdominal aortic aneurysm. INTERVENTIONAL RADIOLOGIST:
Interventional Radiology Coding Case Studies Prepared by Stacie L. Buck, RHIA, CCS-P, RCC, CIRCC, AAPC Fellow President & Senior Consultant INDICATION: Abdominal aortic aneurysm. INTERVENTIONAL RADIOLOGIST:
Intro: Slide 1. Slide 2. Slide 3. Basic understanding of interventional radiology. Gain knowledge of key terms and phrases
 Slide 1 Intro: PRESENTED BY: Selena M. Moore, AAS, CCS, CPC HIMS Physician Liaison Coder This is a modified/updated presentation that was originally written by: Rosemary Waligorski, RHIT, CCS, RCC and
Slide 1 Intro: PRESENTED BY: Selena M. Moore, AAS, CCS, CPC HIMS Physician Liaison Coder This is a modified/updated presentation that was originally written by: Rosemary Waligorski, RHIT, CCS, RCC and
Sample page. POWER UP YOUR CODING with Optum360, your trusted coding partner for 32 years. Visit optum360coding.com.
 2018 Complete Guide for Interventional Radiology An in-depth guide to interventional radiology coding, billing, and reimbursement for facilities and physicians POWER UP YOUR CODING with Optum360, your
2018 Complete Guide for Interventional Radiology An in-depth guide to interventional radiology coding, billing, and reimbursement for facilities and physicians POWER UP YOUR CODING with Optum360, your
Reimbursement Guide Zenith Fenestrated AAA Endovascular Graft
 MEDICAL Reimbursement Guide Zenith Fenestrated AAA Endovascular Graft Disclaimer: The information provided herein reflects Cook s understanding of the procedure(s) and/or device(s) from sources that may
MEDICAL Reimbursement Guide Zenith Fenestrated AAA Endovascular Graft Disclaimer: The information provided herein reflects Cook s understanding of the procedure(s) and/or device(s) from sources that may
Arterial Map of the Thorax, Abdomen and Pelvis 2017 Edition
 Arterial Map of the Thorax, Abdomen and Pelvis Angiography 75605 (-26) Aortography, thoracic 75625 (-26) Aortography, abdominal by serialography 75630 (-26) Aortography, abdominal + bilat iliofemoral 75705
Arterial Map of the Thorax, Abdomen and Pelvis Angiography 75605 (-26) Aortography, thoracic 75625 (-26) Aortography, abdominal by serialography 75630 (-26) Aortography, abdominal + bilat iliofemoral 75705
2018 CPT CODING CHANGES
 17 2018 CPT coding changes by Samuel Smith, MD, FACS; Megan McNally, MD, FACS; and Jan Nagle, MS, RPh JAN 2018 BULLETIN American College of Surgeons 18 Significant changes in Current Procedural Terminology
17 2018 CPT coding changes by Samuel Smith, MD, FACS; Megan McNally, MD, FACS; and Jan Nagle, MS, RPh JAN 2018 BULLETIN American College of Surgeons 18 Significant changes in Current Procedural Terminology
Coding Changes for 2018
 Coding Changes for 2018 An overview of changes to interventional CPT coding that you need to know for practicing in 2018. BY KATHARINE L. KROL, MD, FSIR, FACR There are several coding changes for endovascular
Coding Changes for 2018 An overview of changes to interventional CPT coding that you need to know for practicing in 2018. BY KATHARINE L. KROL, MD, FSIR, FACR There are several coding changes for endovascular
! " " # $ " " # $ " % " # $ # $
 ! " "#$ " "#$ " % "# $ #$ Skin Replacement Surgery Grafts 15040 Harvest of skin for cultured autograft 100 sq cm or less 15110 Epidermal autograft, trunk, arms, legs; first 100 sq cm or 1% of children
! " "#$ " "#$ " % "# $ #$ Skin Replacement Surgery Grafts 15040 Harvest of skin for cultured autograft 100 sq cm or less 15110 Epidermal autograft, trunk, arms, legs; first 100 sq cm or 1% of children
An Overview- Vascular Coding. Caren J Swartz, CPC-I, COC, CPMA, CRC, CPB
 An Overview- Vascular Coding Caren J Swartz, CPC-I, COC, CPMA, CRC, CPB caren@practiceintegrity.com Objectives Understand Anatomy for Vascular Coding Review the Rules for Vascular Procedures Review ICD-10
An Overview- Vascular Coding Caren J Swartz, CPC-I, COC, CPMA, CRC, CPB caren@practiceintegrity.com Objectives Understand Anatomy for Vascular Coding Review the Rules for Vascular Procedures Review ICD-10
Lower Extremity Endovascular Revascularization Codes
 Lower Extremity Endovascular Update: AAPC National Long Beach, CA April 4, 2011 Presented by: David Zielske, MD, CIRCC, CPC H, CCC, CCS, RCC Lower Extremity Endovascular Revascularization Codes 37220 37235
Lower Extremity Endovascular Update: AAPC National Long Beach, CA April 4, 2011 Presented by: David Zielske, MD, CIRCC, CPC H, CCC, CCS, RCC Lower Extremity Endovascular Revascularization Codes 37220 37235
RadRx Your Prescription for Accurate Coding & Reimbursement Copyright All Rights Reserved.
 Interventional Radiology Coding Case Studies Prepared by Stacie L. Buck, RHIA, CCS-P, RCC, CIRCC, AAPC Fellow President & Senior Consultant Week of October 29, 2018 Mesenteric Arteriogram & Thrombectomy/Thrombolysis
Interventional Radiology Coding Case Studies Prepared by Stacie L. Buck, RHIA, CCS-P, RCC, CIRCC, AAPC Fellow President & Senior Consultant Week of October 29, 2018 Mesenteric Arteriogram & Thrombectomy/Thrombolysis
Surgical Privileges Form: Vascular Surgery
 Surgical Form: Vascular Surgery Clinical Request Applicant s Name:. License No. (If Any):... Date:... Scope of Practice:. Facility:.. Place of Work:. CATEGORY I: GENERAL PRIVILEGES 1. Admitting privileges
Surgical Form: Vascular Surgery Clinical Request Applicant s Name:. License No. (If Any):... Date:... Scope of Practice:. Facility:.. Place of Work:. CATEGORY I: GENERAL PRIVILEGES 1. Admitting privileges
CPT 2018 Radiology Code Changes
 CPT 2018 Radiology Code Changes CPT 2018 Radiology Code Changes The following is a listing of new Current Procedural Terminology (CPT ) codes and their descriptors as described in the CPT 2018 codebook.
CPT 2018 Radiology Code Changes CPT 2018 Radiology Code Changes The following is a listing of new Current Procedural Terminology (CPT ) codes and their descriptors as described in the CPT 2018 codebook.
2011 CPT Code Update. Diagnostic Radiology. Computed Tomography (CT), Abdomen and Pelvis. Deletion of Xeroradiography and Subtraction Codes
, Abdomen and Pelvis. Deletion of Xeroradiography and Subtraction Codes") 2011 CPT Code Update [The Health Insurance Portability and Accountability Act [HIPAA] transaction and code set rules require the use of the medical code set that is valid at the time a service is provided.
2011 CPT Code Update [The Health Insurance Portability and Accountability Act [HIPAA] transaction and code set rules require the use of the medical code set that is valid at the time a service is provided.
CY2017 Hospital Outpatient: Vascular Procedure APCs and Complexity Adjustments
 CY2017 Hospital Outpatient: Vascular Procedure APCs and Complexity Adjustments Comprehensive Ambulatory Payment Classifications (c-apcs) In CY2015 and in an effort to help pay providers for quality, not
CY2017 Hospital Outpatient: Vascular Procedure APCs and Complexity Adjustments Comprehensive Ambulatory Payment Classifications (c-apcs) In CY2015 and in an effort to help pay providers for quality, not
Bifurcated system Proximal suprarenal stent Modular (aortic main body and two iliac legs) Full thickness woven polyester graft material Fully
 Full thickness woven polyester graft material Fully") Physician Training Bifurcated system Proximal suprarenal stent Modular (aortic main body and two iliac legs) Full thickness woven polyester graft material Fully supported by self-expanding z-stents H&L-B
Physician Training Bifurcated system Proximal suprarenal stent Modular (aortic main body and two iliac legs) Full thickness woven polyester graft material Fully supported by self-expanding z-stents H&L-B
CY2015 Hospital Outpatient: Endovascular Procedure APCs and Complexity Adjustments
 CY2015 Hospital Outpatient: Endovascular Procedure APCs Complexity Adjustments Comprehensive Ambulatory Payment Classifications (c-apcs) CMS finalized the implementation of 25 Comprehensive APC to further
CY2015 Hospital Outpatient: Endovascular Procedure APCs Complexity Adjustments Comprehensive Ambulatory Payment Classifications (c-apcs) CMS finalized the implementation of 25 Comprehensive APC to further
Peripheral Arterial Disease: A Practical Approach
 Peripheral Arterial Disease: A Practical Approach Sanjoy Kundu BSc, MD, FRCPC, DABR, FASA, FCIRSE, FSIR The Scarborough Hospital Toronto Endovascular Centre The Vein Institute of Toronto Scarborough Vascular
Peripheral Arterial Disease: A Practical Approach Sanjoy Kundu BSc, MD, FRCPC, DABR, FASA, FCIRSE, FSIR The Scarborough Hospital Toronto Endovascular Centre The Vein Institute of Toronto Scarborough Vascular
DIGESTIVE SYSTEM SURGICAL PROCEDURES December 22, 2015 (effective March 1, 2016) INTESTINES (EXCEPT RECTUM) Asst Surg Anae
 INTESTINES (EXCEPT RECTUM) Asst Surg Anae") December 22, 2015 (effective March 1, 201) INTESTINES (EXCEPT RECTUM) Z513 Hydrostatic - Pneumatic dilatation of colon stricture(s) through colonoscope... 10.50 Z50 Fulguration of first polyp through colonoscope...
December 22, 2015 (effective March 1, 201) INTESTINES (EXCEPT RECTUM) Z513 Hydrostatic - Pneumatic dilatation of colon stricture(s) through colonoscope... 10.50 Z50 Fulguration of first polyp through colonoscope...
Disclaimer. Diagnostic Angiography & Therapeutic Interventions 6/8/2016. Deciphering Coding Rules for Complex Interventional Radiology Procedures
 Deciphering Coding Rules for Complex Interventional Radiology Procedures Presented by Stacie L. Buck, RHIA, CCS-P, CIRCC, RCC President & Senior Consultant RadRx July 19, 2016 FHIMA Annual Meeting Disclaimer
Deciphering Coding Rules for Complex Interventional Radiology Procedures Presented by Stacie L. Buck, RHIA, CCS-P, CIRCC, RCC President & Senior Consultant RadRx July 19, 2016 FHIMA Annual Meeting Disclaimer
Naviga&ng the Road Map of Vascular Families
 Naviga&ng the Road Map of Vascular Families AAPC Regional Conference Chicago, IL October 26, 2012 Presented by: David Dunn, MD, FACS CIRCC, CCVTC, CPC- H, CCC, CCS, RCC Na&onal Coding Standards Sources
Naviga&ng the Road Map of Vascular Families AAPC Regional Conference Chicago, IL October 26, 2012 Presented by: David Dunn, MD, FACS CIRCC, CCVTC, CPC- H, CCC, CCS, RCC Na&onal Coding Standards Sources
Basics of Interventional Radiology Coding 2017
 Basics of Interventional Radiology Coding 2017 Prepared and Published By: MedLearn Publishing A Division of Panacea Healthcare Solutions, Inc. 287 East Sixth Street, Suite 400 St. Paul, MN 55101 1-800-252-1578
Basics of Interventional Radiology Coding 2017 Prepared and Published By: MedLearn Publishing A Division of Panacea Healthcare Solutions, Inc. 287 East Sixth Street, Suite 400 St. Paul, MN 55101 1-800-252-1578
Free Esophageal Perforation Following Hybrid Visceral Debranching and Distal Endograft Extension to Repair a Ruptured Thoracoabdominal Aortic
 Free Esophageal Perforation Following Hybrid Visceral Debranching and Distal Endograft Extension to Repair a Ruptured Thoracoabdominal Aortic Aneurysm History A 56-year-old gentleman, who had been referred
Free Esophageal Perforation Following Hybrid Visceral Debranching and Distal Endograft Extension to Repair a Ruptured Thoracoabdominal Aortic Aneurysm History A 56-year-old gentleman, who had been referred
Basics of Interventional Radiology Coding 2018
 Basics of Interventional Radiology Coding 2018 Prepared and Published By: MedLearn Publishing A Division of MedLearn Media, Inc. 445 Minnesota Street, Suite 514 St. Paul, MN 55101 1-800-252-1578 medlearnmedia.com
Basics of Interventional Radiology Coding 2018 Prepared and Published By: MedLearn Publishing A Division of MedLearn Media, Inc. 445 Minnesota Street, Suite 514 St. Paul, MN 55101 1-800-252-1578 medlearnmedia.com
A Comprehensive Multi-disciplinary Approach to Improve Surgical Outcomes Following Elective Colon and Rectal Surgery
 A Comprehensive Multi-disciplinary Approach to Improve Surgical Outcomes Following Elective Colon and Rectal Surgery Tripurari Mishra MD, Deepa Bhat MD, Mina Saeed MD, Jan Kaminski MD, Mihaela Banulescu
A Comprehensive Multi-disciplinary Approach to Improve Surgical Outcomes Following Elective Colon and Rectal Surgery Tripurari Mishra MD, Deepa Bhat MD, Mina Saeed MD, Jan Kaminski MD, Mihaela Banulescu
Ancillary Components with Z-Trak Introduction System
 Ancillary Components with Z-Trak Introduction System Zenith Flex AAA Endovascular Graft Ancillary Components Converter Converters can be used to convert a bifurcated graft into an aortouniiliac graft if
Ancillary Components with Z-Trak Introduction System Zenith Flex AAA Endovascular Graft Ancillary Components Converter Converters can be used to convert a bifurcated graft into an aortouniiliac graft if
2019 ABBOTT REIMBURSEMENT GUIDE CMS Physician Fee Schedule
 ABBOTT REIMBURSEMENT GUIDE CMS Physician Fee Schedule This document and the information contained herein is for general information purposes only and is not intended and does not constitute legal, reimbursement,
ABBOTT REIMBURSEMENT GUIDE CMS Physician Fee Schedule This document and the information contained herein is for general information purposes only and is not intended and does not constitute legal, reimbursement,
Introduction What Causes Peripheral Vascular Disease? How Do Doctors Treat Peripheral Vascular Disease?... 9
 Patient Information Table of Contents Introduction... 3 What is Peripheral Vascular Disease?... 5 What Are Some of the Symptoms of Peripheral Vascular Disease?... 7 What Causes Peripheral Vascular Disease?...
Patient Information Table of Contents Introduction... 3 What is Peripheral Vascular Disease?... 5 What Are Some of the Symptoms of Peripheral Vascular Disease?... 7 What Causes Peripheral Vascular Disease?...
Introduction 3. What is Peripheral Vascular Disease? 5. What Are Some of the Symptoms of Peripheral Vascular Disease? 6
 Patient Information Table of Contents Introduction 3 What is Peripheral Vascular Disease? 5 What Are Some of the Symptoms of Peripheral Vascular Disease? 6 What Causes Peripheral Vascular Disease? 7 How
Patient Information Table of Contents Introduction 3 What is Peripheral Vascular Disease? 5 What Are Some of the Symptoms of Peripheral Vascular Disease? 6 What Causes Peripheral Vascular Disease? 7 How
Selected Operative Procedure Categories for KNHSS SSI Surveillance
 Selected Operative Procedure Categories for KNHSS SSI Surveillance Breast Surgery Excision of lesion or tissue of breast including radical, modified, or quadrant resection, lumpectomy, incisional biopsy,
Selected Operative Procedure Categories for KNHSS SSI Surveillance Breast Surgery Excision of lesion or tissue of breast including radical, modified, or quadrant resection, lumpectomy, incisional biopsy,
Re: CMS-1676-P Medicare Program; Revisions to Payment Policies under the Physician Fee Schedule and Other Revisions to Part B for CY 2018
 September 11, 2017 The Honorable Seema Verma Administrator Centers for Medicare & Medicaid Services U.S. Department of Health and Human Services Attention: CMS-1676 P P.O. Box 8016 Baltimore, MD 21244-1850
September 11, 2017 The Honorable Seema Verma Administrator Centers for Medicare & Medicaid Services U.S. Department of Health and Human Services Attention: CMS-1676 P P.O. Box 8016 Baltimore, MD 21244-1850
Cook Medical. Zenith Flex AAA Endovascular Graft with Z-Trak Introduction System Physician Training
 Cook Medical Zenith Flex AAA Endovascular Graft with Z-Trak Introduction System Physician Training Bifurcated system Proximal suprarenal stent Modular (aortic main body and two iliac legs) Full-thickness,
Cook Medical Zenith Flex AAA Endovascular Graft with Z-Trak Introduction System Physician Training Bifurcated system Proximal suprarenal stent Modular (aortic main body and two iliac legs) Full-thickness,
Complete Guide for Interventional Radiology
 2015 Complete Guide for Interventional Radiology Contents Introduction... 1 CPT Codes and Descriptions...1 Procedure Codes...2 Chapter 1: The Basics... 5 APC Basics Why Is This Important?...5 CCI Edits
2015 Complete Guide for Interventional Radiology Contents Introduction... 1 CPT Codes and Descriptions...1 Procedure Codes...2 Chapter 1: The Basics... 5 APC Basics Why Is This Important?...5 CCI Edits
Chapter 13 Worksheet Code It
 Class: Date: Chapter 13 Worksheet 3 2 1 Code It True/False Indicate whether the statement is true or false. 1. A cardiac catheterization diverts blood from the heart to the aorta. 2. Selective vascular
Class: Date: Chapter 13 Worksheet 3 2 1 Code It True/False Indicate whether the statement is true or false. 1. A cardiac catheterization diverts blood from the heart to the aorta. 2. Selective vascular
Robert F. Cuff, MD FACS SHMG Vascular Surgery
 Robert F. Cuff, MD FACS SHMG Vascular Surgery Objectives To become familiar with the commercially available fenestrated EVAR graft Discuss techniques to increase success Review available data to determine
Robert F. Cuff, MD FACS SHMG Vascular Surgery Objectives To become familiar with the commercially available fenestrated EVAR graft Discuss techniques to increase success Review available data to determine
Case #1. Case #1- Possible codes. Unraveling the -59 modifier. Principles of Interventional. CASE 1: Simple angioplasty
 Unraveling the -59 modifier Principles of Interventional Coding Donald Schon, MD, FACP Debra Lawson, CPC, PCS Distinct or independent from other services performed on the same day Normally not reported
Unraveling the -59 modifier Principles of Interventional Coding Donald Schon, MD, FACP Debra Lawson, CPC, PCS Distinct or independent from other services performed on the same day Normally not reported
Endovascular Repair of Combined Occluded Femoral and Popliteal Arteries
 MEET 2013 Endovascular Repair of Combined Occluded Femoral and Popliteal Arteries ALI AMIN MD, FACS,FACC, RVT CHIEF OF ENDOVASCULAR INTERVENTIONS READING HOSPITAL AND MEDICAL CENTER READING, PA USA Chronic
MEET 2013 Endovascular Repair of Combined Occluded Femoral and Popliteal Arteries ALI AMIN MD, FACS,FACC, RVT CHIEF OF ENDOVASCULAR INTERVENTIONS READING HOSPITAL AND MEDICAL CENTER READING, PA USA Chronic
How to manage TAVI related vascular complications. Paul TL Chiam MBBS, FRCP, FESC, FACC, FSCAI
 How to manage TAVI related vascular complications Paul TL Chiam MBBS, FRCP, FESC, FACC, FSCAI Definition VARC-2 consensus statement Complications caused by: Wire Catheter Anything related to vascular access
How to manage TAVI related vascular complications Paul TL Chiam MBBS, FRCP, FESC, FACC, FSCAI Definition VARC-2 consensus statement Complications caused by: Wire Catheter Anything related to vascular access
Artery 1 Head and Thoracic Arteries. Arrange the parts in the order blood flows through them.
 Artery 1 Head and Thoracic Arteries 1. Given the following parts of the aorta: 1. abdominal aorta 2. aortic arch 3. ascending aorta 4. thoracic aorta Arrange the parts in the order blood flows through
Artery 1 Head and Thoracic Arteries 1. Given the following parts of the aorta: 1. abdominal aorta 2. aortic arch 3. ascending aorta 4. thoracic aorta Arrange the parts in the order blood flows through
SANWICH TECHNIQUE TO REDUCE COMPLICATIONS WHEN TREATING BILATERAL INTERNAL ILIAC ARTERY
 SANWICH TECHNIQUE TO REDUCE COMPLICATIONS WHEN TREATING BILATERAL INTERNAL ILIAC ARTERY TRAN TRA GIANG.MD Interventional cardiovascular department Hanoi Heart Hospital, Hanoi, Viet Nam Nothing to Disclose
SANWICH TECHNIQUE TO REDUCE COMPLICATIONS WHEN TREATING BILATERAL INTERNAL ILIAC ARTERY TRAN TRA GIANG.MD Interventional cardiovascular department Hanoi Heart Hospital, Hanoi, Viet Nam Nothing to Disclose
BILLING BULLETIN. Re: Interventional Cardiology. Bulletin #: 1. Date Issued: November 10, Background
 BILLING BULLETIN Re: Interventional Cardiology Bulletin #: 1 Date Issued: November 10, 2016 Background This Billing Bulletin provides billing guidance when submitting claims to Manitoba Health, Seniors
BILLING BULLETIN Re: Interventional Cardiology Bulletin #: 1 Date Issued: November 10, 2016 Background This Billing Bulletin provides billing guidance when submitting claims to Manitoba Health, Seniors
The catheter-based treatment of valvular disease and aortic
 Access Issues in Abdominal/ Thoracic Endovascular Aortic Repair and Transcatheter Aortic Valve Replacement René Bombien, MD, PhD, and Ali Khoynezhad, MD, PhD The catheter-based treatment of valvular disease
Access Issues in Abdominal/ Thoracic Endovascular Aortic Repair and Transcatheter Aortic Valve Replacement René Bombien, MD, PhD, and Ali Khoynezhad, MD, PhD The catheter-based treatment of valvular disease
Appendix. Vascular Anastomosis Workshop PURPOSE DESCRIPTION WORKSHOP TOOLS
 Appendix Vascular Anastomosis Workshop PURPOSE The purpose of this workshop is to expose the participant to commonly used basic vascular reconstructions. The participant is expected to learn new skills
Appendix Vascular Anastomosis Workshop PURPOSE The purpose of this workshop is to expose the participant to commonly used basic vascular reconstructions. The participant is expected to learn new skills
Case Report 1. CTA head. (c) Tele3D Advantage, LLC
 Tele3D Advantage, LLC") Case Report 1 CTA head 1 History 82 YEAR OLD woman with signs and symptoms of increased intra cranial pressure in setting of SAH. CT Brain was performed followed by CT Angiography of head. 2 CT brain Extensive
Case Report 1 CTA head 1 History 82 YEAR OLD woman with signs and symptoms of increased intra cranial pressure in setting of SAH. CT Brain was performed followed by CT Angiography of head. 2 CT brain Extensive
ADDITIONS. The following codes have been added.
 ADDITIONS The following codes have been added. 99446 Interprofessional telephone/internet assessment and management service provided by treating/requesting physician or other qualified health care professional;
ADDITIONS The following codes have been added. 99446 Interprofessional telephone/internet assessment and management service provided by treating/requesting physician or other qualified health care professional;
Challenges. 1. Sizing. 2. Proximal landing zone 3. Distal landing zone 4. Access vessels 5. Spinal cord ischemia 6. Endoleak
 Disclosure I have the following potential conflicts of interest to report: Consulting: Medtronic, Gore Employment in industry Stockholder of a healthcare company Owner of a healthcare company Other(s)
Disclosure I have the following potential conflicts of interest to report: Consulting: Medtronic, Gore Employment in industry Stockholder of a healthcare company Owner of a healthcare company Other(s)
Acute dissections of the descending thoracic aorta (Debakey
 Endovascular Treatment of Acute Descending Thoracic Aortic Dissections Nimesh D. Desai, MD, PhD, and Joseph E. Bavaria, MD Acute dissections of the descending thoracic aorta (Debakey type III or Stanford
Endovascular Treatment of Acute Descending Thoracic Aortic Dissections Nimesh D. Desai, MD, PhD, and Joseph E. Bavaria, MD Acute dissections of the descending thoracic aorta (Debakey type III or Stanford
Disclosures. Tips and Tricks for Tibial Intervention. Tibial intervention overview
 Tips and Tricks for Tibial Intervention Donald L. Jacobs, MD C Rollins Hanlon Endowed Professor and Chair Chair of Surgery Saint Louis University SSM-STL Saint Louis University Hospital Disclosures Abbott
Tips and Tricks for Tibial Intervention Donald L. Jacobs, MD C Rollins Hanlon Endowed Professor and Chair Chair of Surgery Saint Louis University SSM-STL Saint Louis University Hospital Disclosures Abbott
2018 Endovascular Reimbursement Coding Fact Sheet
 The information contained in this document is provided for informational purposes only and represents no statement, promise, or guarantee by Cordis Corporation concerning levels of reimbursement, payment,
The information contained in this document is provided for informational purposes only and represents no statement, promise, or guarantee by Cordis Corporation concerning levels of reimbursement, payment,
Access (Antegrade, Retrograde, Pedal)
") Access (Antegrade, Retrograde, Pedal) ARCH St. Louis Craig M. Walker, MD, FACC, FACP Clinical Professor of Medicine Tulane University School of Medicine New Orleans, LA Clinical Professor of Medicine LSU
Access (Antegrade, Retrograde, Pedal) ARCH St. Louis Craig M. Walker, MD, FACC, FACP Clinical Professor of Medicine Tulane University School of Medicine New Orleans, LA Clinical Professor of Medicine LSU
Quick Reference Guide
 Quick Reference Guide Indications for Use The AFX Endovascular AAA System is indicated for endovascular treatment in patients with AAA. The devices are indicated for patients with suitable aneurysm morphology
Quick Reference Guide Indications for Use The AFX Endovascular AAA System is indicated for endovascular treatment in patients with AAA. The devices are indicated for patients with suitable aneurysm morphology
Colostomy & Ileostomy
 Colostomy & Ileostomy Indications, problems and preference By Waleed Omar Professor of Colorectal surgery, Mansoura University. Disclosure I have no disclosures. Presentation outline Stoma: Definition
Colostomy & Ileostomy Indications, problems and preference By Waleed Omar Professor of Colorectal surgery, Mansoura University. Disclosure I have no disclosures. Presentation outline Stoma: Definition
Colorectal Laparoscopic Standards and Coding Protocols July 2015 v2.0
 Laparoscopic Standards and Coding Protocols July 2015 v2.0 COLORECTAL LAPAROSCOPIC STANDARDS AND CODING PROTOCOLS Contents 1 Context... 3 2 Laparoscopic Standards... 3 3 Coding Protocols... 3 Appendix
Laparoscopic Standards and Coding Protocols July 2015 v2.0 COLORECTAL LAPAROSCOPIC STANDARDS AND CODING PROTOCOLS Contents 1 Context... 3 2 Laparoscopic Standards... 3 3 Coding Protocols... 3 Appendix
Intervention for Lower Extremity PAD: When, why and what?! Robert F Cuff, MD FACS RVT RPVI
 Intervention for Lower Extremity PAD: When, why and what?! Robert F Cuff, MD FACS RVT RPVI 1 Disclosures I have no financial disclosures related to this talk Objectives 1. Discuss indications for intervention
Intervention for Lower Extremity PAD: When, why and what?! Robert F Cuff, MD FACS RVT RPVI 1 Disclosures I have no financial disclosures related to this talk Objectives 1. Discuss indications for intervention
THE VESSELS OF BLOOD CIRCULATION
 THE VESSELS OF BLOOD CIRCULATION scientistcindy.com /the-vessels-of-blood-circulation.html NOTE: You should familiarize yourself with the anatomy of the heart and have a good understanding of the flow
THE VESSELS OF BLOOD CIRCULATION scientistcindy.com /the-vessels-of-blood-circulation.html NOTE: You should familiarize yourself with the anatomy of the heart and have a good understanding of the flow
Indications: following: embolization. artery that has diseases 5. The evaluation. of suspected. such entities. a cold hand. biopsy
 Peripheral Arterial Ultrasound Protocol Using Color and Spectral Doppler Reviewed by: Mark Yuhasz, MD Last Review Date: January 2015 Contact: (866) 761 4200, Option 1 Indications: The indications for peripheral
Peripheral Arterial Ultrasound Protocol Using Color and Spectral Doppler Reviewed by: Mark Yuhasz, MD Last Review Date: January 2015 Contact: (866) 761 4200, Option 1 Indications: The indications for peripheral
Colorectal procedure guide
 Colorectal procedure guide Illustrations by Lisa Clark Biodesign ADVANCED TISSUE REPAIR cookmedical.com 2 INDEX Anal fistula repair Using the Biodesign plug with no button.... 4 Anal fistula repair Using
Colorectal procedure guide Illustrations by Lisa Clark Biodesign ADVANCED TISSUE REPAIR cookmedical.com 2 INDEX Anal fistula repair Using the Biodesign plug with no button.... 4 Anal fistula repair Using
5F Devices with 0.035
 Ambulatory mamagement for PAD endovascular treatment 5F Devices with 0.035 Flavio Airoldi, MD Multmedica IRCCS Milan - ITALY flavio.airoldi@multimedica.it Is there a need for low profile delivery systems?
Ambulatory mamagement for PAD endovascular treatment 5F Devices with 0.035 Flavio Airoldi, MD Multmedica IRCCS Milan - ITALY flavio.airoldi@multimedica.it Is there a need for low profile delivery systems?
Adductor canal (Subsartorial) or Hunter s canal
 or Hunter s canal") Adductor canal (Subsartorial) or Hunter s canal John Hunter described the exposure and ligation of the femoral artery in this canal for aneurysm of the popliteal artery; this method has the advantage that
Adductor canal (Subsartorial) or Hunter s canal John Hunter described the exposure and ligation of the femoral artery in this canal for aneurysm of the popliteal artery; this method has the advantage that
The Whipple Operation Illustrations
 The Whipple Operation Illustrations Fig. 1. Illustration of the sixstep pancreaticoduodenectomy (Whipple operation) as described in a number of recent text books by Dr. Evans. The operation is divided
The Whipple Operation Illustrations Fig. 1. Illustration of the sixstep pancreaticoduodenectomy (Whipple operation) as described in a number of recent text books by Dr. Evans. The operation is divided
Perineum. done by : zaid al-ghnaneem
 Perineum done by : zaid al-ghnaneem Hello everyone, this sheet will talk about 2 nd Lecture which is Perineum but there are some slides and info from 1 st Lecture. Everything included Slides + Pics Let
Perineum done by : zaid al-ghnaneem Hello everyone, this sheet will talk about 2 nd Lecture which is Perineum but there are some slides and info from 1 st Lecture. Everything included Slides + Pics Let
Abdominal Aortic Aneurysms. A Surgeons Perspective Dr. Derek D. Muehrcke
 Abdominal Aortic Aneurysms A Surgeons Perspective Dr. Derek D. Muehrcke Aneurysm Definition The abnormal enlargement or bulging of an artery caused by an injury or weakness in the blood vessel wall A localized
Abdominal Aortic Aneurysms A Surgeons Perspective Dr. Derek D. Muehrcke Aneurysm Definition The abnormal enlargement or bulging of an artery caused by an injury or weakness in the blood vessel wall A localized
2017 FlexHD Abdominal Wall Reconstruction Reimbursement Coding Reference
 2017 FlexHD Abdominal Wall Reconstruction Reimbursement Coding Reference Most Commonly Reported ICD-10-CM Procedure Codes and Descriptors ICD-10-CM Description 0WUF0KZ Supplement Abdominal Wall with Nonautologous
2017 FlexHD Abdominal Wall Reconstruction Reimbursement Coding Reference Most Commonly Reported ICD-10-CM Procedure Codes and Descriptors ICD-10-CM Description 0WUF0KZ Supplement Abdominal Wall with Nonautologous
BC Vascular Day. Contents. November 3, Abdominal Aortic Aneurysm 2 3. Peripheral Arterial Disease 4 6. Deep Venous Thrombosis 7 8
 BC Vascular Day Contents Abdominal Aortic Aneurysm 2 3 November 3, 2018 Peripheral Arterial Disease 4 6 Deep Venous Thrombosis 7 8 Abdominal Aortic Aneurysm Conservative Management Risk factor modification
BC Vascular Day Contents Abdominal Aortic Aneurysm 2 3 November 3, 2018 Peripheral Arterial Disease 4 6 Deep Venous Thrombosis 7 8 Abdominal Aortic Aneurysm Conservative Management Risk factor modification
Anatomy of the Large Intestine
 Large intestine Anatomy of the Large Intestine 2 Large Intestine Extends from ileocecal valve to anus Length = 1.5-2.5m = 5 feet Regions Cecum = 2.5-3 inch Appendix= 3-5 inch Colon Ascending= 5 inch Transverse=
Large intestine Anatomy of the Large Intestine 2 Large Intestine Extends from ileocecal valve to anus Length = 1.5-2.5m = 5 feet Regions Cecum = 2.5-3 inch Appendix= 3-5 inch Colon Ascending= 5 inch Transverse=
Lower Extremity Arterial Disease
 Lower Extremity Arterial Disease Circulating the Facts About Peripheral Disease Brought to you by the Education Committee of the Society for 1 www.svnnet.org Peripheral Artery Disease (PAD) Many people
Lower Extremity Arterial Disease Circulating the Facts About Peripheral Disease Brought to you by the Education Committee of the Society for 1 www.svnnet.org Peripheral Artery Disease (PAD) Many people
1 Description. 2 Indications. 3 Warnings ASPIRATION CATHETER
 Page 1 of 5 ASPIRATION CATHETER Carefully read all instructions prior to use, observe all warnings and precautions noted throughout these instructions. Failure to do so may result in complications. STERILE.
Page 1 of 5 ASPIRATION CATHETER Carefully read all instructions prior to use, observe all warnings and precautions noted throughout these instructions. Failure to do so may result in complications. STERILE.
Abdominal Exam: The examination of the abdomen used by physicians to detect an abdominal aortic aneurysm.
 Glossary of Terms Abdominal Exam: The examination of the abdomen used by physicians to detect an abdominal aortic aneurysm. Angiogram: A diagnostic test requiring the insertion of a catheter into an artery
Glossary of Terms Abdominal Exam: The examination of the abdomen used by physicians to detect an abdominal aortic aneurysm. Angiogram: A diagnostic test requiring the insertion of a catheter into an artery
Billing and Coding in Practice: What Do I Need to Know and What Are My Resources? Sean P. Roddy, MD Albany, NY
 Billing and Coding in Practice: What Do I Need to Know and What Are My Resources? Sean P. Roddy, MD Albany, NY Nothing To Disclose What Do I Need to Know? Billing and Coding Overview Claim Diagnoses ICD-10
Billing and Coding in Practice: What Do I Need to Know and What Are My Resources? Sean P. Roddy, MD Albany, NY Nothing To Disclose What Do I Need to Know? Billing and Coding Overview Claim Diagnoses ICD-10
STOMA SITING & PARASTOMAL HERNIA MANAGEMENT
 STOMA SITING & PARASTOMAL HERNIA MANAGEMENT Professor Hany S. Tawfik Head of the Department of Surgery & Chairman of Colorectal Surgery Unit Benha University Disclosure No financial affiliation to disclose
STOMA SITING & PARASTOMAL HERNIA MANAGEMENT Professor Hany S. Tawfik Head of the Department of Surgery & Chairman of Colorectal Surgery Unit Benha University Disclosure No financial affiliation to disclose
Arteriovenostomy for renal dialysis 39.27, 39.42
 Surgery categories NHSN Surgery codes (Reference: NHSN Operative Procedure Category Mappings to ICD-9-CM Codes, October 2010 www.cdc.gov/nhsn/pdfs/pscmanual/9pscssicurrent.pdf) Operative aortic aneurysm
Surgery categories NHSN Surgery codes (Reference: NHSN Operative Procedure Category Mappings to ICD-9-CM Codes, October 2010 www.cdc.gov/nhsn/pdfs/pscmanual/9pscssicurrent.pdf) Operative aortic aneurysm
2017 ICD 10 PCS Code Updates
 2017 ICD 10 PCS Code Updates Kimberly Cunningham CPC, CIC, CCS Copyright/Disclaimer text No part of this presentation may be reproduced or transmitted in any form or by any means (graphically, electronically,
2017 ICD 10 PCS Code Updates Kimberly Cunningham CPC, CIC, CCS Copyright/Disclaimer text No part of this presentation may be reproduced or transmitted in any form or by any means (graphically, electronically,
YOU MUST BRING GLOVES FOR THIS ACTIVITY
 ACTIVITY 10: VESSELS AND CIRCULATION OBJECTIVES: 1) How to get ready: Read Chapter 23, McKinley et al., Human Anatomy, 5e. All text references are for this textbook. 2) Observe and sketch histology slide
ACTIVITY 10: VESSELS AND CIRCULATION OBJECTIVES: 1) How to get ready: Read Chapter 23, McKinley et al., Human Anatomy, 5e. All text references are for this textbook. 2) Observe and sketch histology slide
VESSELS: GROSS ANATOMY
 ACTIVITY 10: VESSELS AND CIRCULATION OBJECTIVES: 1) How to get ready: Read Chapter 23, McKinley et al., Human Anatomy, 4e. All text references are for this textbook. 2) Observe and sketch histology slide
ACTIVITY 10: VESSELS AND CIRCULATION OBJECTIVES: 1) How to get ready: Read Chapter 23, McKinley et al., Human Anatomy, 4e. All text references are for this textbook. 2) Observe and sketch histology slide
P Paraplegia abdominal aortic aneurysm repair, 52 paraparesis, 52 pathophysiology, 51 rates and endografts, 51 two-stage approach, 129
 A AAA. See Abdominal aortic aneurysm (AAA) Abdominal aortic aneurysm (AAA). See also Abdominal aortic pathologies advantage, IVUS, 20 asymptomatic infrarenal, 154 device selection and treatment, 19 20
A AAA. See Abdominal aortic aneurysm (AAA) Abdominal aortic aneurysm (AAA). See also Abdominal aortic pathologies advantage, IVUS, 20 asymptomatic infrarenal, 154 device selection and treatment, 19 20
2014 Deleted CPT Codes
 2014 Deleted CPT Codes Surgery 13150 - Repair, complex, eyelids, nose, ears and/or lips; 1.0 cm or less 19102 - Biopsy of breast; percutaneous, needle core, using imaging guidance 19103 - Biopsy of breast;
2014 Deleted CPT Codes Surgery 13150 - Repair, complex, eyelids, nose, ears and/or lips; 1.0 cm or less 19102 - Biopsy of breast; percutaneous, needle core, using imaging guidance 19103 - Biopsy of breast;
DEPARTMENT OF HEALTH & HUMAN SERVICES Public Health Service
 M AY. 6. 2011 10:37 A M F D A - C D R H - O D E - P M O N O. 4147 P. 1 DEPARTMENT OF HEALTH & HUMAN SERVICES Public Health Service Food and Drug Administration 10903 New Hampshire Avenue Document Control
M AY. 6. 2011 10:37 A M F D A - C D R H - O D E - P M O N O. 4147 P. 1 DEPARTMENT OF HEALTH & HUMAN SERVICES Public Health Service Food and Drug Administration 10903 New Hampshire Avenue Document Control
CARDIOVASCULAR DANIL HAMMOUDI.MD
 CARDIOVASCULAR DANIL HAMMOUDI.MD 18 Systemic Circulation Figure 19.19 Pulmonary Circulation Figure 19.18b 1. Thyroid gland 2. Trachea 3. Brachiocephalic 4. Common carotid 5. Internal jugular 6. Superior
CARDIOVASCULAR DANIL HAMMOUDI.MD 18 Systemic Circulation Figure 19.19 Pulmonary Circulation Figure 19.18b 1. Thyroid gland 2. Trachea 3. Brachiocephalic 4. Common carotid 5. Internal jugular 6. Superior
Anatomy of the Blood Vessels
 Biology 212: Anatomy and Physiology II Anatomy of the Blood Vessels References: Saladin, KS: Anatomy and Physiology, The Unity of Form and Function 8 th (2018). Required reading before beginning this lab:
Biology 212: Anatomy and Physiology II Anatomy of the Blood Vessels References: Saladin, KS: Anatomy and Physiology, The Unity of Form and Function 8 th (2018). Required reading before beginning this lab:
Diagnostic and interventional arterial procedures (lower extremity)
") 2017 Coding and Medicare payment guide Diagnostic and interventional arterial procedures (lower extremity) Page 2 All coding, coverage, billing and payment information provided herein by Philips Volcano
2017 Coding and Medicare payment guide Diagnostic and interventional arterial procedures (lower extremity) Page 2 All coding, coverage, billing and payment information provided herein by Philips Volcano
Access strategy for chronic total occlusions (CTOs) is crucial
 is crucial") Learn How Access Strategy Impacts Complex CTO Crossing Arthur C. Lee, MD The Cardiac & Vascular Institute, Gainesville, Florida VASCULAR DISEASE MANAGEMENT 2018;15(3):E19-E23. Key words: chronic total
Learn How Access Strategy Impacts Complex CTO Crossing Arthur C. Lee, MD The Cardiac & Vascular Institute, Gainesville, Florida VASCULAR DISEASE MANAGEMENT 2018;15(3):E19-E23. Key words: chronic total
There are multiple endovascular options for treatment
 Peripheral Rotablator Atherectomy: The Below-the-Knee Approach to Address Calcium Head On Peripheral Rotablator s front-cutting, diamond-tipped burr provides stable rotation in calcified lesions. BY SONYA
Peripheral Rotablator Atherectomy: The Below-the-Knee Approach to Address Calcium Head On Peripheral Rotablator s front-cutting, diamond-tipped burr provides stable rotation in calcified lesions. BY SONYA
PERPHERAL ARTERY ANEURYSM. By Pooja Sharma and Susanna Sebastianpillai
 PERPHERAL ARTERY ANEURYSM By Pooja Sharma and Susanna Sebastianpillai Defintions True Aneurysm Involves all three layers of the vessel. Have two basic shapes; Fusiform = symmetric widening of the vessels
PERPHERAL ARTERY ANEURYSM By Pooja Sharma and Susanna Sebastianpillai Defintions True Aneurysm Involves all three layers of the vessel. Have two basic shapes; Fusiform = symmetric widening of the vessels
Malperfusion Syndromes Type B Aortic Dissection with Malperfusion
 Malperfusion Syndromes Type B Aortic Dissection with Malperfusion Jade S. Hiramoto, MD, MAS April 27, 2012 Associated with early mortality Occurs when there is end organ ischemia secondary to aortic branch
Malperfusion Syndromes Type B Aortic Dissection with Malperfusion Jade S. Hiramoto, MD, MAS April 27, 2012 Associated with early mortality Occurs when there is end organ ischemia secondary to aortic branch
HEALTHMAN GENERAL SURGERY COSTING GUIDE 2014
 s s Consultations: See the Notes below for All s 0109 Hospital follow-up visit 15 531.30 35.423 180.40 12.027 254.10 16.937 251.80 16.785 259.10 17.276 0129 Prolonged first/follow-up consultation : 15
s s Consultations: See the Notes below for All s 0109 Hospital follow-up visit 15 531.30 35.423 180.40 12.027 254.10 16.937 251.80 16.785 259.10 17.276 0129 Prolonged first/follow-up consultation : 15
Summary of Operative Experience
 Summary of Operative Experience (Remarks: Programme Directors of respective Specialty Boards will conduct random check of the trainee s Logbook Summary and Logbook Summary Report against the operation
Summary of Operative Experience (Remarks: Programme Directors of respective Specialty Boards will conduct random check of the trainee s Logbook Summary and Logbook Summary Report against the operation
MedStar Health, Inc. POLICY AND PROCEDURE MANUAL Policy Number: MP.103.MH Last Review Date: 11/08/2018 Effective Date: 02/01/2019
 MedStar Health, Inc. POLICY AND PROCEDURE MANUAL This policy applies to the following lines of business: MedStar Employee (Select) MedStar CareFirst PPO MedStar Health considers Endovascular Repair/Stent
MedStar Health, Inc. POLICY AND PROCEDURE MANUAL This policy applies to the following lines of business: MedStar Employee (Select) MedStar CareFirst PPO MedStar Health considers Endovascular Repair/Stent
An Overview of Post-EVAR Endoleaks: Imaging Findings and Management. Ravi Shergill BSc Sean A. Kennedy MD Mark O. Baerlocher MD FRCPC
 An Overview of Post-EVAR Endoleaks: Imaging Findings and Management Ravi Shergill BSc Sean A. Kennedy MD Mark O. Baerlocher MD FRCPC Disclosure Slide Mark O. Baerlocher: Current: Consultant for Boston
An Overview of Post-EVAR Endoleaks: Imaging Findings and Management Ravi Shergill BSc Sean A. Kennedy MD Mark O. Baerlocher MD FRCPC Disclosure Slide Mark O. Baerlocher: Current: Consultant for Boston
CPT Code Details
 CPT Code 93572 Details Code Descriptor Intravascular Doppler velocity and/or pressure derived coronary flow reserve measurement (coronary vessel or graft) during coronary angiography including pharmacologically
CPT Code 93572 Details Code Descriptor Intravascular Doppler velocity and/or pressure derived coronary flow reserve measurement (coronary vessel or graft) during coronary angiography including pharmacologically
Large veins of the thorax Brachiocephalic veins
 Large veins of the thorax Brachiocephalic veins Right brachiocephalic vein: formed at the root of the neck by the union of the right subclavian & the right internal jugular veins. Left brachiocephalic
Large veins of the thorax Brachiocephalic veins Right brachiocephalic vein: formed at the root of the neck by the union of the right subclavian & the right internal jugular veins. Left brachiocephalic
Copyright HMP Communications
 Ocelot With Wildcat in a Complicated Superficial Femoral Artery Chronic Total Occlusion Soundos K. Moualla, MD, FACC, FSCAI; Richard R. Heuser, MD, FACC, FACP, FESC, FSCAI From Phoenix Heart Center, Phoenix,
Ocelot With Wildcat in a Complicated Superficial Femoral Artery Chronic Total Occlusion Soundos K. Moualla, MD, FACC, FSCAI; Richard R. Heuser, MD, FACC, FACP, FESC, FSCAI From Phoenix Heart Center, Phoenix,
3 Circulatory Pathways
 40 Chapter 3 Circulatory Pathways Systemic Arteries -Arteries carry blood away from the heart to the various organs of the body. -The aorta is the longest artery in the body; it branches to give rise to
40 Chapter 3 Circulatory Pathways Systemic Arteries -Arteries carry blood away from the heart to the various organs of the body. -The aorta is the longest artery in the body; it branches to give rise to
Treatment of Thoracoabdominal Aneurysms Is there a need for custom-made devices?
 : FETURED TECHNOLOGY: JOTEC E-XTR DESIGN ENGINEERING Treatment of Thoracoabdominal neurysms Is there a need for custom-made devices? INTERVIEW ND CSE PRESENTTIONS WITH DNIEL RNZN, MD, ND NDREJ SCHMIDT,
: FETURED TECHNOLOGY: JOTEC E-XTR DESIGN ENGINEERING Treatment of Thoracoabdominal neurysms Is there a need for custom-made devices? INTERVIEW ND CSE PRESENTTIONS WITH DNIEL RNZN, MD, ND NDREJ SCHMIDT,