Chronic anastomotic sinus after low anterior resection: When can the defunctioning stoma be reversed?
|
|
|
- Gregory Smith
- 6 years ago
- Views:
Transcription
1 Received Date : 15-Oct-2009 Revised Date : 10-Dec-2009 Accepted Date : 14-Dec-2009 Article type : Original Article R1 Original Article Chronic anastomotic sinus after low anterior resection: When can the defunctioning stoma be reversed? Sau Shung, FONG, MBBS (S pore), MMED (Surg) (S pore), MRCS (Edin) Institution: Tan Tock Seng Hospital, 11 Jalan Tan Tock Seng, Singapore Contribution: Design; Acquisition of data; Analysis and interpretation of data; Drafting of manuscript Kenneth, CHEN, MBBS (S pore) Institution: Tan Tock Seng Hospital, 11 Jalan Tan Tock Seng, Singapore Contribution: Acquisition of data; Analysis and interpretation of data Richard, SIM, MBBS (S pore), FRCS (Glas, Edin) Institution: Tan Tock Seng Hospital, 11 Jalan Tan Tock Seng, Singapore Contribution: Conception and design; Revision of manuscript; Final approval of manuscript This is an Accepted Article that has been peer-reviewed and approved for publication in the Colorectal Disease, but has yet to undergo copy-editing and proof correction. Please cite this article as an Accepted Article ; doi: /j x
2 Corresponding Author: Sau Shung, FONG Contact details: Mobile Tel: , Office Tel (Secretary): Address: Tan Tock Seng Hospital Dept of Surgery 11 Jalan Tan Tock Seng Singapore Abstract Aim: Anastomotic leakage after low anterior resections may incompletely resolve, resulting in sinus tracts that persist on repeated contrast studies. This case series evaluates the factors that may contribute to sinus healing or safe reversal of the defunctioning ileostomy. Methods: All patients (n = 8) who developed an anastomotic sinus after low anterior resections over a 8 year period were identified from a prospective database Results: All had low anterior resections with defunctioning stomas for rectal carcinoma (median follow up 43.5 (13-84) months).two patients with an unhealed subclinical leak had the stoma reversed successfully. Of the six patients with clinical leakage, two healed spontaneously. one healed after application of fibrin glue. one developed an anastomotic stricture successfully treated by dilatation with, subsequent stoma reversal and one developed recurrent cancer and was not reversed. Onepatient underwent reversal despite persistence of the sinus, followed by rectal perforation requiring laparotomy and faecal diversion Bowel function was satisfactory where the sinus healed spontaneously, but poor where reversal was carried out without sinus healing.
3 Conclusion: Tracks that persist more than one year are unlikely to heal but the stoma can be reversed if there had been a subclinical leak previously. A persistent anastomotic sinus leading to a cavity may not be suitable for stoma closure. Introduction Anastomotic leakage after anterior resection may be subclinical or clinical. Failure of healing results in persistence of the dehiscence, with formation of a chronic sinus tract.some may appear to have healed on subsequent contrast studies, but others persist. The patient therefore continues to suffer the significant morbidity of an ileostomy as reversal may bring about the undesired consequence of pelvic sepsis requiring operation. Management of the chronic sinus is difficult. Many methods have been described for their treatment, including deroofing mucosal advancement, resection and anastomosis, resection and permanent stoma and sealing of the track with tissue glue [1,2],. This case series reports patients who developed a persistent chronic anastomotic sinus after anterior resection and attempts to determine, the factors that may contribute to successful reversal of the covering stoma Method A retrospective review of all patients with low anterior resections performed from Jan 2001 to Feb 2008 in a single institution (Tan Tock Seng Hospital, Singapore) was carried out to indentify those with a chronic anastomotic sinus detected on contrast enema prior to stoma closure. Of 193 low anterior resections there were eight patients who met the inclusion criteria. Data on age, race, gender, stage of tumour, distance from anal verge, histological
4 grade and CEA levels were collected. The modality used to diagnose the leak was considered and both the ASA and POSSUM grading [3] ) were reviewed to evaluate the patient s preoperative physiological condition. Contrast enema studies of the sinus tract were reviewed individually to determine the morphology of the track and recorded according to a classification previously described by Lim et al [4]. Figures 1a, 1b and 1c demonstrate the typical contrast enema findings of the three morphologies encountered during this study (simple posterior, long linear posterior and cavity). All resections were performed by two senior colorectal surgeons. Total meso-rectal excisions were performed in all patients with an anastomosis using the double stapler technique. All patients were managed post operatively using a pre-determined clinical pathway. Anastomotic leakage was divided into clinical and subclinical. The former were defined by clinical sepsis, computer tomographic (CT) evidence of a peri-anastomotic collection or active extravasation of contrast during a contrast enema study and evidence of a contained leak on a subsequent water soluble contrast enema study performed at least 3 months later. A subclinical leak was defined by the absence of clinical sepsis but with evidence of sinus formation on a water soluble contrast enema study at least 3 months later. During the study period, routine contrast enemas were performed before stoma closure. All patients were followed by six monthly (or more frequent) water soluble contrast enemas. Spontaneous healing was defined as the absence of a previously noted anastomotic sinus on subsequent water soluble contrast enemas without
5 intervention. Where the ileostomy was closed, the surgeon s decision to reverse it was reviewed. Any major morbidity and mortality during the period of review were recorded. Results The patient demographic data are shown in table 1. Table 2 summarizes the presentation of the leak, the modality used for diagnosis, morphology of the track, details relating to sinus healing as well as eventual bowel function of all eight patients. Of the 8 patients identified, two presented sub-clinically (patients 1 and 2). Both sinuses failed to heal spontaneously but the stoma was reversed nevertheless at 11 and 15 months. Both patients recovered well from surgery but bowel function was poor.six patients presented with clinical leakage. two sinuses (patient 3 and 4) closed spontaneously at 10 and 11 months. The defunctioning stoma was reversed one month later. Subsequent bowel function was good. These were the only sinuses in this series, to show a long and linear morphology. Of the four remaining sinuses which presented with clinical leaage and failed to close spontaneously, one (patient 5) underwent the instillation of fibrin glue into the sinus at 25 months (figure 2). This resulted in successful closure. Stoma reversal was performed 1 month later with good bowel function and no recurrence of the sinus..another sinus (patient 6) failed to heal in a patient who developed anastomotic stricture. This was dilated successfully and the ileostomy reversed at 42 months after surgery. Bowel function was poor. Another sinus failed to heal but the stoma was reversed at 13 months (patient 7). This was followed by pelvic sepsis from a rectal perforation two years later and the patient underwent Hartmann s procedure with recreation of a stoma.. The radiological morphology
6 of this sinus had been that of a cavity in the initial contrast study. Finally in patient 8 the sinus failed to heal and the stoma was not reversed owing to recurrence of the tumour. Discussion The natural history of anastomotic sinuses is difficult to ascertain due to the rarity of the condition. Its exact incidence is not known, but approximately 4-8% of patients who do not have a clinically evident leak are found to have an anastomotic sinus on routine post operative water soluble contrast enema [1,4,5,6]. This rate is not reduced when inflammatory bowel disease is excluded [4,6]. After ileal pouch-anal anastomoses (IPAA), the literature suggests that reversal of the ileostomy in the presence of a subclinical sinus is not followed by a high complication rate [7,8]. The incidence of the condition in the present series is 4% And the data in the international literature are limited. This series is one of the largest to have been published. The main limitation of this paper is its retrospective nature and the small numbersof patients studied. Furthermore the duration of follow up was short for some patients. The data should therefore be interpreted with caution. There was no obvious evidence that development of a sinus was related to the POSSUM score or to other patient or disease-related factors (table 1), The case series has however shown that the defunctioning stoma can be reversed despite persistence of an anastomotic sinus. This was the case with the patients with a subclinical
7 leak where both patients had a good outcome despite a persisting sinus. In another study, on the other hand, a greater proportion of patients with a subclinical leak in the study of Lim et al healed spontaneously (7 out of 10, within 5 months). It is possible that the greater proportion of subclinical leaks that healed spontaneously in Lim s paper was due to the shorter interval between discharge and the diagnosing water soluble contrast enema. Both sinuses that healed spontaneously occurred within a year, as also noted by Arumainayagam et al (9). A year may therefore be a reasonable time frame to wait for spontaneous healing, beyond which, it is unlikely to occur. Both sinuses in our series that spontaneously healed were of the long and linear variety. We postulate that a narrow, long track would be a natural barrier to the passage of rectal contents and is analogous to the spontaneous closure of a T-tube track or a low output entero-cutaneous fistula, although a long and linear track had no effect on healing in the experience of Lim et al (4). The only morbidity occurred when reversal of ileostomy was performed despite radiological evidence of a persistent sinus. It is unlikely that the track could have healed spontaneously given more time. Lim et al [4] described only 4 out of 13 patients with clinical leakage that eventually healed. There is no convincing literature that delaying stoma reversal might be associated with greater success The morphological feature of a cavity in this patient probably contributed to failure of healing and the pelvic sepsis which resulted after stoma closure. A sinus with this morphology may therefore benefit from a definitive surgical procedure such as Whitlow s operation of deroofing [1], mucosal advancement, resection and reanastomosis, resection and permanent stoma or sealing the track with tissue glue.
8 Mucinous adenocarcinoma can arise from anorectal fistula and sinus tracks [9, [10,11,12]. In the present series, the single patient with recurrence developed this within a year of surgery and was probably derived form the disease(stage IIIC). In summary, the case series suggests that spontaneous healing of an anastomotic sinus can occur but may take up to a year.it is p ossible safely to reverse the ileostomy if the sinus is sub-clinical. Bowel function may be poor in reversed patients with a persistent sinus. Closure of the stoma when there is a persisting sinus leading to a cavity may not be advisable. References 1. Whitlow CB, Opelka FG, Gathright JB, Beck DE. Treatment of Colorectal and Ileoanal anastomotic sinuses. Dis Colon Retum. 1997;40(7): Swain BT, Ellis CN. Fibrin glue treatment of low rectal and pouch-anal anastomotic sinuses. Dis Col Rectum. 2004;47: Copeland GP, Jones D, Walters M. POSSUM: a scoring system for surgical audit. Br J Surg. 1991;78(3): Lim M, Akhtar S, Sasapu K, Harris K, Burke D, Sagar P, Finan P. Clinical and subclinical leaks after low colorectal anastomosis: a clinical and radiologic study. Dis Colon Rectum. 2006;49(10): Beart RW. Ulcerative colitis: complications of pelvic pouch. In: Fazio VW, ed. Current therapy in colon and rectal surgery. Toronto: BC Decker, 1990: Khair G, Alhamarneh O, Avery J, Cast J, Gunn J, Monson JR, Hartley J. Routine use of gastrograffin enema prior to the reversal of a loop ileostomy. Dig Surg. 2007;24(5): Akbari RP, Madoff RD, Parker SC, Hagerman G, Minami S, Bullard Dunn KM, Mellgren AF. Anastomotic sinuses after ileoanal pouch construction: incidence, management, and outcome. Dis Colon Rectum. 2009;52(3):452-5.
9 8. Nyam DC, Wolff BG, Dozois RR, Pemberton JH, Mathison SM. Does the presence of a pre-ileostomy closure asymptomatic pouch-anastomotic sinus tract affect the success of ileal pouch-anal anastomosis? J Gastrointest Surg. 1997;1(3): Arumainayagam N, Chadwick M, Roe A. The fate of anastomotic sinuses after total mesorectal excision (TME) for rectal cancer. Colorectal Dis. 2009;11(3): Cruickshank AH, McConnel EM, Miller DG. Malignancy in scars, chronic ulcers and sinuses. J Clin pathol. 1963;16: McCune WS, Thistlethwaite JR. Fistula cancer. Ann Surg. 1959;149: Skir I. Mucinous carcinoma associated with fistulas of long standing. Am J Surg. 1948;75:
10 Factor Results (n = 8) Age (median) (years) 56.6 (33 70) Gender (M : F) 7 : 1 Differentiation All moderately differentiated adenocarcinomas Distance from anal verge (median) (cm) 8 (4 10) Stage Stage 1: 1/8 Stage 3: 7/8 Tumour dimension (longest) (cm) 6 (4 12) Lymph nodes harvested (median) 16 (9 34)* ASA grade Grade 1: 1/8 Grade 2: 7/8 POSSUM Score Expected mortality < 10%: 6/7 Expected morbidity < 30%: 4/7 Duration of follow up (median) (months) 47 (13 84) Table 1: Patient and tumour characteristics.
11 Table 2: Details of patients with persistent anastomotic sinus N o. Days to Leak 1 NA (Subcli nical) 2 NA (Subcli Presentation of Leak NA (Subclinical) NA (Subclinical) nical) 3 29 Readmision for abdominal pain, Perrectal bleeding Modality used to detect Leak NA NA CT Morphology Simple posterior Simple posterior Long linear posterior 4 7 Prolonged ileus CT Long linear, posterior 5 5 Sepsis CT Simple posterior 6 10 Readmission CT Simple for abdominal posterior pain, perrectal bleeding 7 7 Readmission for intestinal obstruction CT Simple posterior, cavity 8 5 Sepsis CT Simple posterior Months to sinus healing Months to ileostomy reversal Function Status (length of follow up in months) Not healed 15 Diarrhoea NED (73) Not healed 11 Diarrhoea NED (84) Good NED (60) Good NED (47) 25 (fibrin glue 26 Good NED (35) applied) Not healed 42 Diarrhoea NED (47) After dilatation of stricture Not healed 13 Emergency laparotomy for rectal perforation 2 years later Incontinence Stoma* NED (40) Not healed Not reversed Stoma AWD (13) AWD: alive with disease. NED: no evidence of disease. Diarrhoea= frequency >4/24 hr Good function= no incontinence, frequency 3/24hr Figure 1a: Simple posterior sinus

12


13 Figure 1b: Long linear sinus


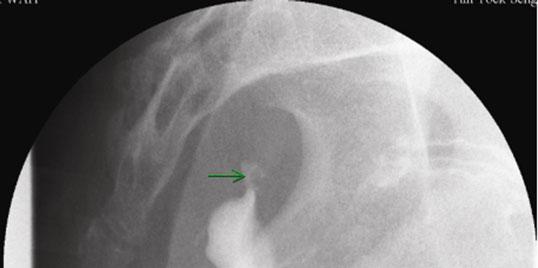
14 Figure 1c: Sinus with cavity


15 Figure 2: Endoscopic view of sinus prior to fibrin glue injection



16 Figure 3: Flowchart demonstrating outcome of 8 patients with anastomotic sinuses.
UvA-DARE (Digital Academic Repository) Surgical treatment of perianal and rectal fistula van Koperen, P.J. Link to publication
 Surgical treatment of perianal and rectal fistula van Koperen, P.J. Link to publication") UvA-DARE (Digital Academic Repository) Surgical treatment of perianal and rectal fistula van Koperen, P.J. Link to publication Citation for published version (APA): van Koperen, P. J. (2010). Surgical
UvA-DARE (Digital Academic Repository) Surgical treatment of perianal and rectal fistula van Koperen, P.J. Link to publication Citation for published version (APA): van Koperen, P. J. (2010). Surgical
The management and outcome of anastomotic leaks in colorectal surgery
 Original article doi:10.1111/j.1463-1318.2007.01417.x The management and outcome of anastomotic leaks in colorectal surgery A. A. Khan*, J. M. D. Wheeler, C. Cunningham, B. George, M. Kettlewell and N.
Original article doi:10.1111/j.1463-1318.2007.01417.x The management and outcome of anastomotic leaks in colorectal surgery A. A. Khan*, J. M. D. Wheeler, C. Cunningham, B. George, M. Kettlewell and N.
World Journal of Colorectal Surgery
 World Journal of Colorectal Surgery Volume 5, Issue 1 2015 Article 1 Ileal U Pouch Reconstruction Proximal To Straight Sublevator Ileoanal Anastomosis Following Total Proctocolectomy For Low Rectal Cancer
World Journal of Colorectal Surgery Volume 5, Issue 1 2015 Article 1 Ileal U Pouch Reconstruction Proximal To Straight Sublevator Ileoanal Anastomosis Following Total Proctocolectomy For Low Rectal Cancer
Index. Note: Page numbers of article title are in boldface type.
 Index Note: Page numbers of article title are in boldface type. A Abscess(es) in Crohn s disease, 168 169 IPAA and, 110 114 as unexpected finding in colorectal surgery, 46 Adhesion(s) trocars-related laparoscopy
Index Note: Page numbers of article title are in boldface type. A Abscess(es) in Crohn s disease, 168 169 IPAA and, 110 114 as unexpected finding in colorectal surgery, 46 Adhesion(s) trocars-related laparoscopy
Restorative Proctocolectomy For Ulcerative Colitis IN
 590540SJS0010.1177/1457496915590540Restorative proctocolectomyi. Helavirta, H. Huhtala, M. Hyöty, P. Collin, P. Aitola research-article2015 Original article Restorative Proctocolectomy For Ulcerative Colitis
590540SJS0010.1177/1457496915590540Restorative proctocolectomyi. Helavirta, H. Huhtala, M. Hyöty, P. Collin, P. Aitola research-article2015 Original article Restorative Proctocolectomy For Ulcerative Colitis
Poor Outcomes of Complicated Pouch-Related Fistulas after Ileal Pouch-Anal Anastomosis Surgery
 Syddansk Universitet Poor Outcomes of Complicated Pouch-Related Fistulas after Ileal Pouch-Anal Anastomosis Surgery Kjaer, M D; Kjeldsen, Jens; Qvist, Niels Published in: Scandinavian Journal of Surgery
Syddansk Universitet Poor Outcomes of Complicated Pouch-Related Fistulas after Ileal Pouch-Anal Anastomosis Surgery Kjaer, M D; Kjeldsen, Jens; Qvist, Niels Published in: Scandinavian Journal of Surgery
Colostomy & Ileostomy
 Colostomy & Ileostomy Indications, problems and preference By Waleed Omar Professor of Colorectal surgery, Mansoura University. Disclosure I have no disclosures. Presentation outline Stoma: Definition
Colostomy & Ileostomy Indications, problems and preference By Waleed Omar Professor of Colorectal surgery, Mansoura University. Disclosure I have no disclosures. Presentation outline Stoma: Definition
Homayoon Akbari, MD, PhD
 Recent Advances in IBD Surgery Homayoon M. Akbari, MD, PhD, FRCS(C), FACS Associate Professor of Surgery Virginia Commonwealth University Crohn s disease first described as a surgical condition, with the
Recent Advances in IBD Surgery Homayoon M. Akbari, MD, PhD, FRCS(C), FACS Associate Professor of Surgery Virginia Commonwealth University Crohn s disease first described as a surgical condition, with the
Citation for published version (APA): Bartels, S. A. L. (2013). Laparoscopic colorectal surgery: beyond the short-term effects
: Bartels, S. A. L. (2013). Laparoscopic colorectal surgery: beyond the short-term effects") UvA-DARE (Digital Academic Repository) Laparoscopic colorectal surgery: beyond the short-term effects Bartels, S.A.L. Link to publication Citation for published version (APA): Bartels, S. A. L. (2013).
UvA-DARE (Digital Academic Repository) Laparoscopic colorectal surgery: beyond the short-term effects Bartels, S.A.L. Link to publication Citation for published version (APA): Bartels, S. A. L. (2013).
Colorectal Surgery. Patient Care. Goals and Objectives
 Colorectal Surgery Patient Care 1) Interpret the results of clinical evaluations (history, physical examination) performed on patients with a) Hemorrhoids b) Perianal abscess/fistula c) Anal fissure d)
Colorectal Surgery Patient Care 1) Interpret the results of clinical evaluations (history, physical examination) performed on patients with a) Hemorrhoids b) Perianal abscess/fistula c) Anal fissure d)
Ileoanal Pouch Solves the Problem
 Ileoanal Pouch Solves the Problem Bruce D George Department of Surgery John Radcliffe Hospital, Falk Symposium 2-3 May 2008 Ileoanal Pouch Solves the Problem? Sometimes Not always Key Issues in Pouch Surgery
Ileoanal Pouch Solves the Problem Bruce D George Department of Surgery John Radcliffe Hospital, Falk Symposium 2-3 May 2008 Ileoanal Pouch Solves the Problem? Sometimes Not always Key Issues in Pouch Surgery
The Binational Colorectal Cancer Audit. A/Prof Paul McMurrick Head, Cabrini Monash University Dept of Surgery 2017
 The Binational Colorectal Cancer Audit A/Prof Paul McMurrick Head, Cabrini Monash University Dept of Surgery 2017 Binational Colorectal Cancer Database 2010 First Patient 2011 Contract between CMUDS and
The Binational Colorectal Cancer Audit A/Prof Paul McMurrick Head, Cabrini Monash University Dept of Surgery 2017 Binational Colorectal Cancer Database 2010 First Patient 2011 Contract between CMUDS and
Ileo-rectal anastomosis for Crohn's disease of
 Ileo-rectal anastomosis for Crohn's disease of the colon W. N. W. BAKER From the Research Department, St Mark's Hospital, London Gut, 1971, 12, 427-431 SUMMARY Twenty-six cases of Crohn's disease of the
Ileo-rectal anastomosis for Crohn's disease of the colon W. N. W. BAKER From the Research Department, St Mark's Hospital, London Gut, 1971, 12, 427-431 SUMMARY Twenty-six cases of Crohn's disease of the
Complications of laparoscopic protective loop ileostomy in patients with colorectal cancer
 ISPUB.COM The Internet Journal of Surgery Volume 19 Number 2 Complications of laparoscopic protective loop ileostomy in patients with colorectal cancer F Puccio, M Solazzo, G Pandolfo, P Marcianò Citation
ISPUB.COM The Internet Journal of Surgery Volume 19 Number 2 Complications of laparoscopic protective loop ileostomy in patients with colorectal cancer F Puccio, M Solazzo, G Pandolfo, P Marcianò Citation
Surgical Therapies for the Treatment of IBD!
 Surgical Therapies for the Treatment of IBD! Andrew A Shelton, MD Clinical Professor of Surgery Stanford Hospital and Clinics Section of Colon and Rectal Surgery! Ulcerative Colitis v. Crohn s! 30% of
Surgical Therapies for the Treatment of IBD! Andrew A Shelton, MD Clinical Professor of Surgery Stanford Hospital and Clinics Section of Colon and Rectal Surgery! Ulcerative Colitis v. Crohn s! 30% of
Incidence and risk factors of anastomotic leaks. By: khaled Said Assistant professor of colorectal surgery Alexandria
 Incidence and risk factors of anastomotic leaks By: khaled Said Assistant professor of colorectal surgery Alexandria Anastomotic leakage after colorectal surgery is a major and potentially life-threatening
Incidence and risk factors of anastomotic leaks By: khaled Said Assistant professor of colorectal surgery Alexandria Anastomotic leakage after colorectal surgery is a major and potentially life-threatening
Motility Disorders. Pelvic Floor. Colorectal Center for Functional Bowel Disorders (N = 701) January 2010 November 2011
 January 2010 November 2011") Motility Disorders Pelvic Floor Colorectal Center for Functional Bowel Disorders (N = 71) January 21 November 211 New Patients 35 3 25 2 15 1 5 Constipation Fecal Incontinence Rectal Prolapse Digestive-Genital
Motility Disorders Pelvic Floor Colorectal Center for Functional Bowel Disorders (N = 71) January 21 November 211 New Patients 35 3 25 2 15 1 5 Constipation Fecal Incontinence Rectal Prolapse Digestive-Genital
11/13/11. Biologics for CD and CUC: The Impact on Surgical Outcomes. Principles of Successful Intestinal Surgery
 Biologics for CD and CUC: The Impact on Surgical Outcomes Robert R. Cima, M.D., M.A. Associate Professor of Surgery Division of Colon and Rectal Surgery Overview Antibody based medications (biologics)
Biologics for CD and CUC: The Impact on Surgical Outcomes Robert R. Cima, M.D., M.A. Associate Professor of Surgery Division of Colon and Rectal Surgery Overview Antibody based medications (biologics)
University of Groningen. Colorectal Anastomoses Bakker, Ilsalien
 University of Groningen Colorectal Anastomoses Bakker, Ilsalien IMPORTANT NOTE: You are advised to consult the publisher's version (publisher's PDF) if you wish to cite from it. Please check the document
University of Groningen Colorectal Anastomoses Bakker, Ilsalien IMPORTANT NOTE: You are advised to consult the publisher's version (publisher's PDF) if you wish to cite from it. Please check the document
Surgical Approach to Crohn s Colitis Segmental or Total Colectomy? Can We Avoid the Stoma?
 17 th Panhellenic IBD Congress Thessaloniki May 2018 Surgical Approach to Crohn s Colitis Segmental or Total Colectomy? Can We Avoid the Stoma? Janindra Warusavitarne Consultant Colorectal Surgeon, St
17 th Panhellenic IBD Congress Thessaloniki May 2018 Surgical Approach to Crohn s Colitis Segmental or Total Colectomy? Can We Avoid the Stoma? Janindra Warusavitarne Consultant Colorectal Surgeon, St
Surgical Management of IBD. Val Jefford Grand Rounds October 14, 2003
 Surgical Management of IBD Val Jefford Grand Rounds October 14, 2003 Introduction Important Features Clinical Presentation Evaluation Medical Treatment Surgical Treatment Cases Overview Introduction Two
Surgical Management of IBD Val Jefford Grand Rounds October 14, 2003 Introduction Important Features Clinical Presentation Evaluation Medical Treatment Surgical Treatment Cases Overview Introduction Two
Management of Pancreatic Fistulae
 Management of Pancreatic Fistulae Jose Ramos University of the Witwatersrand Donald Gordon Medical Centre Fistula definition A Fistula is a permanent abnormal passageway between two organs (epithelial
Management of Pancreatic Fistulae Jose Ramos University of the Witwatersrand Donald Gordon Medical Centre Fistula definition A Fistula is a permanent abnormal passageway between two organs (epithelial
St Mark's Hospital from 1953 to 1968
 Gut, 1970, 11, 235-239 The results of ileorectal anastomosis at St Mark's Hospital from 1953 to 1968 W. N. W. BAKER From St Mark's Hospital, London SUMMARY The popular view of ileorectal anastomosis for
Gut, 1970, 11, 235-239 The results of ileorectal anastomosis at St Mark's Hospital from 1953 to 1968 W. N. W. BAKER From St Mark's Hospital, London SUMMARY The popular view of ileorectal anastomosis for
11/21/13 CEA: 1.7 WNL
 Case Scenario 1 A 70 year-old white male presented to his primary care physician with a recent history of rectal bleeding. He was referred for imaging and a colonoscopy and was found to have adenocarcinoma.
Case Scenario 1 A 70 year-old white male presented to his primary care physician with a recent history of rectal bleeding. He was referred for imaging and a colonoscopy and was found to have adenocarcinoma.
CLINICAL IMPACT OF SEPRAFILM SAFETY AND EFFICACY
 CLINICAL IMPACT OF Post-surgical ADHESIONS SEPRAFILM SAFETY AND EFFICACY Clinical Reviews Clinical studies contents OVERVIEW 3. REDUCED INCIDENCE AND SEVERITY OF ADHESIONS 3.1 Becker JM et al. (1996) 3.2
CLINICAL IMPACT OF Post-surgical ADHESIONS SEPRAFILM SAFETY AND EFFICACY Clinical Reviews Clinical studies contents OVERVIEW 3. REDUCED INCIDENCE AND SEVERITY OF ADHESIONS 3.1 Becker JM et al. (1996) 3.2
PROCARE FINAL FEEDBACK Definitions
 1 PROCARE FINAL FEEDBACK 2006-2014 Definitions Version 0.2 29/10/2015 2 Table of Contents Introduction... 3 Part 1: PROCARE indicators 2006-2014... 4 1.1. Methods... 4 1.1.1. Descriptive numbers... 4 1.1.2.
1 PROCARE FINAL FEEDBACK 2006-2014 Definitions Version 0.2 29/10/2015 2 Table of Contents Introduction... 3 Part 1: PROCARE indicators 2006-2014... 4 1.1. Methods... 4 1.1.1. Descriptive numbers... 4 1.1.2.
Chapter I 7. Laparoscopic versus open elective sigmoid resection in diverticular disease: six months follow-up of the randomized control Sigma-trial
 Chapter I 7 Laparoscopic versus open elective sigmoid resection in diverticular disease: six months follow-up of the randomized control Sigma-trial Bastiaan R. Klarenbeek Roberto Bergamaschi Alexander
Chapter I 7 Laparoscopic versus open elective sigmoid resection in diverticular disease: six months follow-up of the randomized control Sigma-trial Bastiaan R. Klarenbeek Roberto Bergamaschi Alexander
Comparison of Loop Ileostomy and Loop Colostomy as Defunctioning Stoma in Low Rectal Cancer Surgery NCI Experience
 Kasr El Aini Journal of Surgery VOL., 12, NO 1 January 2011 75 Comparison of Loop Ileostomy and Loop Colostomy as Defunctioning Stoma in Low Rectal Cancer Surgery NCI Experience Ahmed Abbas, MD MRCS General
Kasr El Aini Journal of Surgery VOL., 12, NO 1 January 2011 75 Comparison of Loop Ileostomy and Loop Colostomy as Defunctioning Stoma in Low Rectal Cancer Surgery NCI Experience Ahmed Abbas, MD MRCS General
Inflammatory Bowel Disease and Surgery: What You Should Know
 Inflammatory Bowel Disease and Surgery: What You Should Know Ask the Experts March 9, 2019 Kristen Blaker, MD Colon and Rectal Surgery MetroHealth Medical Center Disclosures None Outline Who undergoes
Inflammatory Bowel Disease and Surgery: What You Should Know Ask the Experts March 9, 2019 Kristen Blaker, MD Colon and Rectal Surgery MetroHealth Medical Center Disclosures None Outline Who undergoes
Ileal Pouch Anal Anastomosis: The Preferred Method of Reconstruction after Proctocolectomy in Children
 Ileal Pouch Anal Anastomosis: The Preferred Method of Reconstruction after Proctocolectomy in Children Stephanie Jones, D.O. Surgical Fellow March 21, 2011 Ulcerative Colitis Spectrum of inflammatory bowel
Ileal Pouch Anal Anastomosis: The Preferred Method of Reconstruction after Proctocolectomy in Children Stephanie Jones, D.O. Surgical Fellow March 21, 2011 Ulcerative Colitis Spectrum of inflammatory bowel
Surgical Outcomes of Crohn s Disease: A Single Institutional Experience in Taiwan. [J Soc Colon Rectal Surgeon (Taiwan) 2009;20:1-6]
![Surgical Outcomes of Crohn s Disease: A Single Institutional Experience in Taiwan. [J Soc Colon Rectal Surgeon (Taiwan) 2009;20:1-6]](/thumbs/87/96356608.jpg "Surgical Outcomes of Crohn s Disease: A Single Institutional Experience in Taiwan. [J Soc Colon Rectal Surgeon (Taiwan) 2009;20:1-6]") J Soc Colon Rectal Surgeon (Taiwan) March 2009 Original Article Surgical Outcomes of Crohn s Disease: A Single Institutional Experience in Taiwan Ta-Wen Hsu 1,2 Feng-Fan Chiang 1 Hwei-Ming Wang 1 1 Division
J Soc Colon Rectal Surgeon (Taiwan) March 2009 Original Article Surgical Outcomes of Crohn s Disease: A Single Institutional Experience in Taiwan Ta-Wen Hsu 1,2 Feng-Fan Chiang 1 Hwei-Ming Wang 1 1 Division
Case discussion. Anastomotic leakage. intern superviser
 Case discussion Anastomotic leakage intern superviser Basic data Name : XX ID: M101881671 Age:51 Y Gender: male Past history: Hospitalized for acute diverticulitis on 2004/7/17, 2005/5/28 controlled by
Case discussion Anastomotic leakage intern superviser Basic data Name : XX ID: M101881671 Age:51 Y Gender: male Past history: Hospitalized for acute diverticulitis on 2004/7/17, 2005/5/28 controlled by
Surgical Management of IBD in the Age of Biologics
 Surgical Management of IBD in the Age of Biologics Lisa S. Poritz, M.D Associate Professor of Surgery Division of Colon and Rectal Surgery Objectives Discuss surgical management of IBD When to operate
Surgical Management of IBD in the Age of Biologics Lisa S. Poritz, M.D Associate Professor of Surgery Division of Colon and Rectal Surgery Objectives Discuss surgical management of IBD When to operate
Surgery for Inflammatory Bowel Disease
 Surgery for Inflammatory Bowel Disease Emily Steinhagen, MD Assistant Professor Department of Surgery, Division of Colorectal Surgery University Hospitals Cleveland Medical Center Common Questions Why
Surgery for Inflammatory Bowel Disease Emily Steinhagen, MD Assistant Professor Department of Surgery, Division of Colorectal Surgery University Hospitals Cleveland Medical Center Common Questions Why
DIGESTIVE SYSTEM SURGICAL PROCEDURES May 1, 2015 INTESTINES (EXCEPT RECTUM) Asst Surg Anae
 Asst Surg Anae") ENDOSCOPY Z50 Duodenoscopy (not to be claimed if Z399 and/or Z00 performed on same patient within 3 months)... 92.10 Z9 Subsequent procedure (within three months following previous endoscopic procedure)...
ENDOSCOPY Z50 Duodenoscopy (not to be claimed if Z399 and/or Z00 performed on same patient within 3 months)... 92.10 Z9 Subsequent procedure (within three months following previous endoscopic procedure)...
Outcomes of Colostomy Reversal Procedures in Two Teaching Hospitals in Addis Ababa, Ethiopia A. Bekele, B. Kotisso, H. Biluts Correspondence to
 East and Central African Journal of Surgery http://www.bioline.org.br/js 9 Outcomes of Colostomy Reversal Procedures in Two Teaching Hospitals in Addis Ababa, Ethiopia A. Bekele, B. Kotisso, H. Biluts
East and Central African Journal of Surgery http://www.bioline.org.br/js 9 Outcomes of Colostomy Reversal Procedures in Two Teaching Hospitals in Addis Ababa, Ethiopia A. Bekele, B. Kotisso, H. Biluts
Complications and Functional Results after Ileoanal Pouch Formation in Obese Patients
 J Gastrointest Surg (2008) 12:668 674 DOI 10.1007/s11605-008-0465-3 Complications and Functional Results after Ileoanal Pouch Formation in Obese Patients R. P. Kiran & F. H. Remzi & V. W. Fazio & I. C.
J Gastrointest Surg (2008) 12:668 674 DOI 10.1007/s11605-008-0465-3 Complications and Functional Results after Ileoanal Pouch Formation in Obese Patients R. P. Kiran & F. H. Remzi & V. W. Fazio & I. C.
Incidence of Colorectal Cancers- Australia. Anterior Resection 5/23/2018. What spurs us to investigate?
 Incidence of Colorectal Cancers- Australia 17,000 Colorectal cancers in 2018 20% of Colorectal cancers are in the Rectum 12.3% of all new cancers Anterior Resection Syndrome (ARS) Lisa Wilson. Colorectal
Incidence of Colorectal Cancers- Australia 17,000 Colorectal cancers in 2018 20% of Colorectal cancers are in the Rectum 12.3% of all new cancers Anterior Resection Syndrome (ARS) Lisa Wilson. Colorectal
Preoperative adjuvant radiotherapy
 Preoperative adjuvant radiotherapy Dr John Hay Radiation Oncology Program BC Cancer Agency Vancouver Cancer Centre The key question for the surgeon Do you think that this tumour can be resected with clear
Preoperative adjuvant radiotherapy Dr John Hay Radiation Oncology Program BC Cancer Agency Vancouver Cancer Centre The key question for the surgeon Do you think that this tumour can be resected with clear
Rectal Cancer. About the Colon and Rectum. Symptoms. Colorectal Cancer Screening
 Patient information regarding care and surgery associated with RECTAL CANCER by Robert K. Cleary, M.D., John C. Eggenberger, M.D., Amalia J. Stefanou., M.D. location: Michigan Heart and Vascular Institute,
Patient information regarding care and surgery associated with RECTAL CANCER by Robert K. Cleary, M.D., John C. Eggenberger, M.D., Amalia J. Stefanou., M.D. location: Michigan Heart and Vascular Institute,
Is the routine use of a water-soluble contrast enema prior to closure of a loop ileostomy necessary? A review of a single institution experience
 Dimitriou et al. World Journal of Surgical Oncology (2015) 13:331 DOI 10.1186/s12957-015-0742-z RESEARCH Open Access Is the routine use of a water-soluble contrast enema prior to closure of a loop ileostomy
Dimitriou et al. World Journal of Surgical Oncology (2015) 13:331 DOI 10.1186/s12957-015-0742-z RESEARCH Open Access Is the routine use of a water-soluble contrast enema prior to closure of a loop ileostomy
Surgical Management of Advanced Stage Colon Cancer. Nathan Huber, MD 6/11/14
 Surgical Management of Advanced Stage Colon Cancer Nathan Huber, MD 6/11/14 Colon Cancer Overview Approximately 50,000 attributable deaths per year Colorectal cancer is the 3 rd most common cause of cancer-related
Surgical Management of Advanced Stage Colon Cancer Nathan Huber, MD 6/11/14 Colon Cancer Overview Approximately 50,000 attributable deaths per year Colorectal cancer is the 3 rd most common cause of cancer-related
DIGESTIVE SYSTEM SURGICAL PROCEDURES December 22, 2015 (effective March 1, 2016) INTESTINES (EXCEPT RECTUM) Asst Surg Anae
 INTESTINES (EXCEPT RECTUM) Asst Surg Anae") December 22, 2015 (effective March 1, 201) INTESTINES (EXCEPT RECTUM) Z513 Hydrostatic - Pneumatic dilatation of colon stricture(s) through colonoscope... 10.50 Z50 Fulguration of first polyp through colonoscope...
December 22, 2015 (effective March 1, 201) INTESTINES (EXCEPT RECTUM) Z513 Hydrostatic - Pneumatic dilatation of colon stricture(s) through colonoscope... 10.50 Z50 Fulguration of first polyp through colonoscope...
Laparoscopic Resection Of Colon & Rectal Cancers. R Sim Centre for Advanced Laparoscopic Surgery, TTSH
 Laparoscopic Resection Of Colon & Rectal Cancers R Sim Centre for Advanced Laparoscopic Surgery, TTSH Feasibility and safety Adequacy - same radical surgery as open op. Efficacy short term benefits and
Laparoscopic Resection Of Colon & Rectal Cancers R Sim Centre for Advanced Laparoscopic Surgery, TTSH Feasibility and safety Adequacy - same radical surgery as open op. Efficacy short term benefits and
COLORECTAL CANCER FAISALGHANISIDDIQUI MBBS; FCPS; PGDIP-BIOETHICS; MCPS-HPE
 COLORECTAL CANCER FAISALGHANISIDDIQUI MBBS; FCPS; PGDIP-BIOETHICS; MCPS-HPE PROFESSOR OF SURGERY & DIRECTOR, PROFESSIONAL DEVELOPMENT CENTRE J I N N A H S I N D H M E D I C A L U N I V E R S I T Y faisal.siddiqui@jsmu.edu.pk
COLORECTAL CANCER FAISALGHANISIDDIQUI MBBS; FCPS; PGDIP-BIOETHICS; MCPS-HPE PROFESSOR OF SURGERY & DIRECTOR, PROFESSIONAL DEVELOPMENT CENTRE J I N N A H S I N D H M E D I C A L U N I V E R S I T Y faisal.siddiqui@jsmu.edu.pk
UvA-DARE (Digital Academic Repository) Surgical treatment of perianal and rectal fistula van Koperen, P.J. Link to publication
 Surgical treatment of perianal and rectal fistula van Koperen, P.J. Link to publication") UvA-DARE (Digital Academic Repository) Surgical treatment of perianal and rectal fistula van Koperen, P.J. Link to publication Citation for published version (APA): van Koperen, P. J. (2010). Surgical
UvA-DARE (Digital Academic Repository) Surgical treatment of perianal and rectal fistula van Koperen, P.J. Link to publication Citation for published version (APA): van Koperen, P. J. (2010). Surgical
Repeat Single Incision Laparoscopic Surgery after Primary Single Incision Laparoscopic Surgery for Colorectal Disease
 ORIGINAL ARTICLE pissn 2234-778X eissn 2234-5248 J Minim Invasive Surg 2018;21(1):38-42 Journal of Minimally Invasive Surgery Repeat Single Incision Laparoscopic Surgery after Primary Single Incision Laparoscopic
ORIGINAL ARTICLE pissn 2234-778X eissn 2234-5248 J Minim Invasive Surg 2018;21(1):38-42 Journal of Minimally Invasive Surgery Repeat Single Incision Laparoscopic Surgery after Primary Single Incision Laparoscopic
Nikki Damen,* Katrina Spilsbury, Michael Levitt,* Gregory Makin,* Paul Salama,* Patrick Tan,* Cheryl Penter* and Cameron Platell* Abstract
 COLORECTAL ANZJSurg.com Anastomotic leaks in colorectal surgery Nikki Damen,* Katrina Spilsbury, Michael Levitt,* Gregory Makin,* Paul Salama,* Patrick Tan,* Cheryl Penter* and Cameron Platell* *Colorectal
COLORECTAL ANZJSurg.com Anastomotic leaks in colorectal surgery Nikki Damen,* Katrina Spilsbury, Michael Levitt,* Gregory Makin,* Paul Salama,* Patrick Tan,* Cheryl Penter* and Cameron Platell* *Colorectal
Risk Factors of Permanent Stomas in Patients with Rectal Cancer after Low Anterior Resection with Temporary Stomas
 Original Article http://dx.doi.org/10.3349/ymj.2015.56.2.447 pissn: 0513-5796, eissn: 1976-2437 Yonsei Med J 56(2):447-453, 2015 Risk Factors of Permanent Stomas in Patients with Rectal Cancer after Low
Original Article http://dx.doi.org/10.3349/ymj.2015.56.2.447 pissn: 0513-5796, eissn: 1976-2437 Yonsei Med J 56(2):447-453, 2015 Risk Factors of Permanent Stomas in Patients with Rectal Cancer after Low
ANZ Emergency Laparotomy Audit Quality Improvement (ANZELA-QI) Pilot Collaboration between RACS, ANZCA, GSA, NZAGS, ASA, NZSA, ACEM, CICM
 Pilot Collaboration between RACS, ANZCA, GSA, NZAGS, ASA, NZSA, ACEM, CICM") ANZ Emergency Laparotomy Audit Quality Improvement (ANZELA-QI) Pilot Collaboration between RACS, ANZCA, GSA, NZAGS, ASA, NZSA, ACEM, CICM DATA COLLECTION FORM Most Australian hospitals contribute data
ANZ Emergency Laparotomy Audit Quality Improvement (ANZELA-QI) Pilot Collaboration between RACS, ANZCA, GSA, NZAGS, ASA, NZSA, ACEM, CICM DATA COLLECTION FORM Most Australian hospitals contribute data
Laparoscopic vs Robotic Rectal Cancer Surgery: Making it better!
 Laparoscopic vs Robotic Rectal Cancer Surgery: Making it better! Francis Seow- Choen Medical Director Seow-Choen Colorectal Centre Singapore In all situations: We have to use the right tool for the job
Laparoscopic vs Robotic Rectal Cancer Surgery: Making it better! Francis Seow- Choen Medical Director Seow-Choen Colorectal Centre Singapore In all situations: We have to use the right tool for the job
Index. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A Abdominal surgery prior as factor in laparoscopic colorectal surgery, 554 555 Abscess(es) CRC presenting as, 539 540 Adenocarcinoma of
Index Note: Page numbers of article titles are in boldface type. A Abdominal surgery prior as factor in laparoscopic colorectal surgery, 554 555 Abscess(es) CRC presenting as, 539 540 Adenocarcinoma of
The role of Surgery and Stomas in IBD
 The role of Surgery and Stomas in IBD When do I need it? Can I avoid it? How do I live with it? Kyle G. Cologne, MD Assistant Professor of Surgery USC Division of Colorectal Surgery Topics Surgical Differences
The role of Surgery and Stomas in IBD When do I need it? Can I avoid it? How do I live with it? Kyle G. Cologne, MD Assistant Professor of Surgery USC Division of Colorectal Surgery Topics Surgical Differences
Management of Perforated Colon Cancers
 Management of Perforated Colon Cancers Introduction Colon and rectal cancers are the most common gastrointestinal cancers. They are 3 rd most common and 2 nd most common causes of cancer deaths among men
Management of Perforated Colon Cancers Introduction Colon and rectal cancers are the most common gastrointestinal cancers. They are 3 rd most common and 2 nd most common causes of cancer deaths among men
Gastrointestinal Imaging Original Research
 Contrast Enema for Detecting nastomotic Strictures Gastrointestinal Imaging Original Research David Dolinsky 1 Marc S. Levine 1 Stephen E. Rubesin 1 Igor Laufer 1 John L. Rombeau 2 Dolinsky D, Levine MS,
Contrast Enema for Detecting nastomotic Strictures Gastrointestinal Imaging Original Research David Dolinsky 1 Marc S. Levine 1 Stephen E. Rubesin 1 Igor Laufer 1 John L. Rombeau 2 Dolinsky D, Levine MS,
Large polyps: EMR, ESD, TEM and segmental resection. Terry Phang 2017 SON fall update
 Large polyps: EMR, ESD, TEM and segmental resection Terry Phang 2017 SON fall update Key Points: Large polyps No RCT re: Recurrence, complications Piecemeal vs en bloc: EMR vs ESD Partial vs full-thickness:
Large polyps: EMR, ESD, TEM and segmental resection Terry Phang 2017 SON fall update Key Points: Large polyps No RCT re: Recurrence, complications Piecemeal vs en bloc: EMR vs ESD Partial vs full-thickness:
Surgery and Crohn s. Crohn s Disease 70 % Why Operate? Complications of Disease. The Gastrointestinal Tract. Surgery for Inflammatory Bowel Disease
 The Gastrointestinal Tract Surgery for Inflammatory Bowel Disease Jonathan Chun, MD The regon Clinic Gastrointestinal and Minimally Invasive Surgery Crohn s Disease Can affect anywhere in the GI tract,
The Gastrointestinal Tract Surgery for Inflammatory Bowel Disease Jonathan Chun, MD The regon Clinic Gastrointestinal and Minimally Invasive Surgery Crohn s Disease Can affect anywhere in the GI tract,
Treatment strategy of metastatic rectal cancer
 35.Schweizerische Koloproktologie-Tagung Treatment strategy of metastatic rectal cancer Gilles Mentha University hospital of Geneva Bern, January 18th, 2014 Colorectal cancer is the third most frequent
35.Schweizerische Koloproktologie-Tagung Treatment strategy of metastatic rectal cancer Gilles Mentha University hospital of Geneva Bern, January 18th, 2014 Colorectal cancer is the third most frequent
Management of colorectal anastomotic leakage: differences between salvage and anastomotic takedown
 The American Journal of Surgery (2012) 204, 671 676 Clinical Science Management of colorectal anastomotic leakage: differences between salvage and anastomotic takedown Domenico Fraccalvieri, M.D., Sebastiano
The American Journal of Surgery (2012) 204, 671 676 Clinical Science Management of colorectal anastomotic leakage: differences between salvage and anastomotic takedown Domenico Fraccalvieri, M.D., Sebastiano
UNDERSTANDING X-RAYS: ABDOMINAL IMAGING THE ABDOMEN
 UNDERSTANDING X-RAYS: ABDOMINAL IMAGING THE ABDOMEN Radiology Enterprises radiologyenterprises@gmail.com www.radiologyenterprises.com STOMACH AND SMALL BOWEL STOMACH AND SMALL BOWEL Swallowed air is a
UNDERSTANDING X-RAYS: ABDOMINAL IMAGING THE ABDOMEN Radiology Enterprises radiologyenterprises@gmail.com www.radiologyenterprises.com STOMACH AND SMALL BOWEL STOMACH AND SMALL BOWEL Swallowed air is a
Hester Cheung Memorial Lecture
 Hester Cheung Memorial Lecture STEVEN D WEXNER, MD, PHD (HON),FACS, FRCS, FRCS(ED) Director, Digestive Disease Center; Chairman, Department of Colorectal Surgery; Cleveland Clinic Florida Professor of
Hester Cheung Memorial Lecture STEVEN D WEXNER, MD, PHD (HON),FACS, FRCS, FRCS(ED) Director, Digestive Disease Center; Chairman, Department of Colorectal Surgery; Cleveland Clinic Florida Professor of
The effect of rectal washout on local recurrence following rectal cancer surgery
 COLORECTAL SURGERY Ann R Coll Surg Engl 208; 00: 46 5 doi 0.308/rcsann.207.0202 The effect of rectal washout on local recurrence following rectal cancer surgery SR Moosvi, K Manley, J Hernon Norfolk and
COLORECTAL SURGERY Ann R Coll Surg Engl 208; 00: 46 5 doi 0.308/rcsann.207.0202 The effect of rectal washout on local recurrence following rectal cancer surgery SR Moosvi, K Manley, J Hernon Norfolk and
Ileal pouchyanal anastomosis (IPAA) is the procedure
 is the procedure") ORIGINAL CONTRIBUTION Proximal Diversion at the Time of Ileal Pouch Anal Anastomosis for Ulcerative Colitis: Current Practices of North American Colorectal Surgeons Sandra L. de Montbrun, M.D. & Paul M.
ORIGINAL CONTRIBUTION Proximal Diversion at the Time of Ileal Pouch Anal Anastomosis for Ulcerative Colitis: Current Practices of North American Colorectal Surgeons Sandra L. de Montbrun, M.D. & Paul M.
PROCARE FINAL FEEDBACK
 1 PROCARE FINAL FEEDBACK General report 2006-2014 Version 2.1 08/12/2015 PROCARE indicators 2006-2014... 3 Demographic Data... 3 Diagnosis and staging... 4 Time to first treatment... 6 Neoadjuvant treatment...
1 PROCARE FINAL FEEDBACK General report 2006-2014 Version 2.1 08/12/2015 PROCARE indicators 2006-2014... 3 Demographic Data... 3 Diagnosis and staging... 4 Time to first treatment... 6 Neoadjuvant treatment...
Surgery and Stomas in IBD When do I need it? Can I avoid it? How do I live with it?
 Surgery and Stomas in IBD When do I need it? Can I avoid it? How do I live with it? Kyle G. Cologne, MD Assistant Professor of Surgery USC Division of Colorectal Surgery Topics Surgical Differences between
Surgery and Stomas in IBD When do I need it? Can I avoid it? How do I live with it? Kyle G. Cologne, MD Assistant Professor of Surgery USC Division of Colorectal Surgery Topics Surgical Differences between
Short and longterm outcomes after endoscopic resection of malignant polyps.
 Short and longterm outcomes after endoscopic resection of malignant polyps. Short and longterm outcomes High risk features Lymph node metastasis Lymph node metastases sm1 sm2 sm3 Son 2008 3.1 % 14.9% 25.0
Short and longterm outcomes after endoscopic resection of malignant polyps. Short and longterm outcomes High risk features Lymph node metastasis Lymph node metastases sm1 sm2 sm3 Son 2008 3.1 % 14.9% 25.0
Colorectal non-inflammatory emergencies
 Colorectal non-inflammatory emergencies Prof. Hesham Amer Professor of general surgery, Kasr Alainy hospital, Cairo university Dr. Doaa Mansour Dr. Ahmed Nabil Dr. Ahmed Abdel-Salam Lecturers of general
Colorectal non-inflammatory emergencies Prof. Hesham Amer Professor of general surgery, Kasr Alainy hospital, Cairo university Dr. Doaa Mansour Dr. Ahmed Nabil Dr. Ahmed Abdel-Salam Lecturers of general
SURGERY FOR COLITIS THE BOTTOM LINE
 SURGERY FOR COLITIS THE BOTTOM LINE Speaker Declarations This presenter has the following declarations of relationship with industry None [Nov 2017] Surgeons just like to cut.. ABSOLUTE INDICATIONS Toxic
SURGERY FOR COLITIS THE BOTTOM LINE Speaker Declarations This presenter has the following declarations of relationship with industry None [Nov 2017] Surgeons just like to cut.. ABSOLUTE INDICATIONS Toxic
Safety of short stay Hospitalization in Reversal of Loop Ileostomy
 Original Article Safety of short stay Hospitalization in Reversal of Loop Ileostomy Tayyab Abbas, Abid Nazir, Muhammad Lateef, Faisal Rauf, Zafar Ali Choudhary Abstract Study Design: Prospective, randomized
Original Article Safety of short stay Hospitalization in Reversal of Loop Ileostomy Tayyab Abbas, Abid Nazir, Muhammad Lateef, Faisal Rauf, Zafar Ali Choudhary Abstract Study Design: Prospective, randomized
Structured Follow-Up after Colorectal Cancer Resection: Overrated. R. Taylor Ripley University of Colorado Grand Rounds April 23, 2007
 Structured Follow-Up after Colorectal Cancer Resection: Overrated R. Taylor Ripley University of Colorado Grand Rounds April 23, 2007 Guidelines for Colonoscopy Production: Surveillance US Multi-Society
Structured Follow-Up after Colorectal Cancer Resection: Overrated R. Taylor Ripley University of Colorado Grand Rounds April 23, 2007 Guidelines for Colonoscopy Production: Surveillance US Multi-Society
DIVERTICULAR DISEASE. Dr. Irina Murray Casanova PGY IV
 DIVERTICULAR DISEASE Dr. Irina Murray Casanova PGY IV Diverticular Disease Colonoscopy Abdpelvic CT Scan Surgical Indications Overall, approximately 20% of patients with diverticulitis require surgical
DIVERTICULAR DISEASE Dr. Irina Murray Casanova PGY IV Diverticular Disease Colonoscopy Abdpelvic CT Scan Surgical Indications Overall, approximately 20% of patients with diverticulitis require surgical
R Sim, D Cheong, KS Wong, B Lee, QY Liew Tan Tock Seng Hospital Singapore
 Prospective randomized, double-blind, placebo-controlled study of pre- and postoperative administration of a COX-2- specific inhibitor as opioid-sparing analgesia in major colorectal resections R Sim,
Prospective randomized, double-blind, placebo-controlled study of pre- and postoperative administration of a COX-2- specific inhibitor as opioid-sparing analgesia in major colorectal resections R Sim,
Rectal Prolapse: A 10-Year Experience
 24 The Ochsner Journal Volume 7, Number 1, Spring 2007 25 Rectal Prolapse: A 10-Year Experience Figure 2. Physical examination. A. Concentric folds of prolapsed rectum. B. Radial folds of hemorrhoids (mucosal
24 The Ochsner Journal Volume 7, Number 1, Spring 2007 25 Rectal Prolapse: A 10-Year Experience Figure 2. Physical examination. A. Concentric folds of prolapsed rectum. B. Radial folds of hemorrhoids (mucosal
WHAT IS LARS? LOW ANTERIOR RESECTIONSYNDROME. Sophie Pilkington. Colorectal Surgeon University Hospital Southampton
 WHAT IS LARS? LOW ANTERIOR RESECTIONSYNDROME Sophie Pilkington Colorectal Surgeon University Hospital Southampton INTRODUCTION UK Bowel cancer 2013 41,100 new cases INTRODUCTION UK Bowel cancer 2013 41,100
WHAT IS LARS? LOW ANTERIOR RESECTIONSYNDROME Sophie Pilkington Colorectal Surgeon University Hospital Southampton INTRODUCTION UK Bowel cancer 2013 41,100 new cases INTRODUCTION UK Bowel cancer 2013 41,100
COLORECTAL CARCINOMA
 QUICK REFERENCE FOR HEALTHCARE PROVIDERS MANAGEMENT OF COLORECTAL CARCINOMA Ministry of Health Malaysia Malaysian Society of Colorectal Surgeons Malaysian Society of Gastroenterology & Hepatology Malaysian
QUICK REFERENCE FOR HEALTHCARE PROVIDERS MANAGEMENT OF COLORECTAL CARCINOMA Ministry of Health Malaysia Malaysian Society of Colorectal Surgeons Malaysian Society of Gastroenterology & Hepatology Malaysian
The impact of adhesions on operations and postoperative recovery in colon cancer surgery
 The American Journal of Surgery (2013) -, - - The impact of adhesions on operations and postoperative recovery in colon cancer surgery Ramzi Amri, M.Sc., Hannah C. den Boon, B.Sc., Liliana G. Bordeianou,
The American Journal of Surgery (2013) -, - - The impact of adhesions on operations and postoperative recovery in colon cancer surgery Ramzi Amri, M.Sc., Hannah C. den Boon, B.Sc., Liliana G. Bordeianou,
National Emergency Laparotomy Audit. Help Box Text
 National Emergency Laparotomy Audit Help Box Text Version Control Version 1.1 06/12/13 1.2 13/12/13 1.3 20/12/13 1.4 20/01/14 1.5 30/01/14 1.6 13/03/14 1.7 07/04/14 1.8 01/12/14 1.9 05/05/15 1.10 02/07/15
National Emergency Laparotomy Audit Help Box Text Version Control Version 1.1 06/12/13 1.2 13/12/13 1.3 20/12/13 1.4 20/01/14 1.5 30/01/14 1.6 13/03/14 1.7 07/04/14 1.8 01/12/14 1.9 05/05/15 1.10 02/07/15
Acute Diverticulitis. Andrew B. Peitzman, MD Mark M. Ravitch Professor of Surgery University of Pittsburgh
 Acute Diverticulitis Andrew B. Peitzman, MD Mark M. Ravitch Professor of Surgery University of Pittsburgh Focus today: when to operate n Recurrent, uncomplicated diverticulitis; after how many episodes?
Acute Diverticulitis Andrew B. Peitzman, MD Mark M. Ravitch Professor of Surgery University of Pittsburgh Focus today: when to operate n Recurrent, uncomplicated diverticulitis; after how many episodes?
CHAPTER 7 Concluding remarks and implications for further research
 CONCLUDING REMARKS AND IMPLICATIONS FOR FURTHER RESEARCH CHAPTER 7 Concluding remarks and implications for further research 111 CHAPTER 7 Molecular staging of large sessile rectal tumors In this thesis,
CONCLUDING REMARKS AND IMPLICATIONS FOR FURTHER RESEARCH CHAPTER 7 Concluding remarks and implications for further research 111 CHAPTER 7 Molecular staging of large sessile rectal tumors In this thesis,
Innovations in Rectal Cancer Surgery
 Innovations in Rectal Cancer Surgery A. D Hoore MD PhD, EBSQ-CR, (hon)fascrs A. Wolthuis MD PhD, EBSQ-CR, FACS G. Bislenghi MD Departement of Abdominal Surgery University Hospitals Leuven, Belgium invasiveness
Innovations in Rectal Cancer Surgery A. D Hoore MD PhD, EBSQ-CR, (hon)fascrs A. Wolthuis MD PhD, EBSQ-CR, FACS G. Bislenghi MD Departement of Abdominal Surgery University Hospitals Leuven, Belgium invasiveness
Assessment by Using a Water-Soluble Contrast Enema Study of Radiologic Leakage in Lower Rectal Cancer Patients With Sphincter-Saving Surgery
 Original Article http://dx.doi.org/10.3393/ac.2015.31.4.131 pissn 2287-9714 eissn 2287-9722 Assessment by Using a Water-Soluble Contrast Enema Study of Radiologic Leakage in Lower Rectal Cancer Patients
Original Article http://dx.doi.org/10.3393/ac.2015.31.4.131 pissn 2287-9714 eissn 2287-9722 Assessment by Using a Water-Soluble Contrast Enema Study of Radiologic Leakage in Lower Rectal Cancer Patients
Department of Surgery, Aizu Central Hospital, Fukushima
 Case Reports Resection of Asynchronous Quadruple Advanced Colonic Carcinomas Followed by Reconstruction with Ileal Interposition between the Transverse Colon and Rectum Sho Mineta 1, Kimiyoshi Shimanuki
Case Reports Resection of Asynchronous Quadruple Advanced Colonic Carcinomas Followed by Reconstruction with Ileal Interposition between the Transverse Colon and Rectum Sho Mineta 1, Kimiyoshi Shimanuki
Laparoscopic Bladder-Preserving Surgery for Enterovesical Fistula Complicated with Benign Gastrointestinal Disease
 This is an Open Access article licensed under the terms of the Creative Commons Attribution-NonCommercial-NoDerivs 3.0 License (www.karger.com/oa-license), applicable to the online version of the article
This is an Open Access article licensed under the terms of the Creative Commons Attribution-NonCommercial-NoDerivs 3.0 License (www.karger.com/oa-license), applicable to the online version of the article
Influence of multiple stapler firings used for rectal division on colorectal anastomotic leak rate
 Surg Endosc (2017) 31:5318 5326 DOI 10.1007/s00464-017-5611-0 and Other Interventional Techniques Influence of multiple stapler firings used for rectal division on colorectal anastomotic leak rate Tamara
Surg Endosc (2017) 31:5318 5326 DOI 10.1007/s00464-017-5611-0 and Other Interventional Techniques Influence of multiple stapler firings used for rectal division on colorectal anastomotic leak rate Tamara
Innovations in rectal cancer surgery TAMIS and transanal TME
 Innovations in rectal cancer surgery TAMIS and transanal TME A.D Hoore MD PhD, EBSQ CR Chair Departement of Abdominal Surgery University Hospitals Leuven, Belgium Actual treatment in rectal Early rectal
Innovations in rectal cancer surgery TAMIS and transanal TME A.D Hoore MD PhD, EBSQ CR Chair Departement of Abdominal Surgery University Hospitals Leuven, Belgium Actual treatment in rectal Early rectal
Transanal Endoscopic Microsurgery
 Transanal Endoscopic Microsurgery Dana R. Sands, MD, FACS, FASCRS Director, Colorectal Physiology Center Staff Surgeon Department of Colorectal Surgery Cleveland Clinic Florida What is TEM? Minimally invasive
Transanal Endoscopic Microsurgery Dana R. Sands, MD, FACS, FASCRS Director, Colorectal Physiology Center Staff Surgeon Department of Colorectal Surgery Cleveland Clinic Florida What is TEM? Minimally invasive
Colorectal Clinical Pathways: A Method of Improving Clinical Outcome?
 Original Article Colorectal Clinical Pathways: A Method of Improving Clinical Outcome? Jane J.Y. Tan, Angel Y.Z. Foo and Denis M.O. Cheong, Department of General Surgery, Tan Tock Seng Hospital, Singapore.
Original Article Colorectal Clinical Pathways: A Method of Improving Clinical Outcome? Jane J.Y. Tan, Angel Y.Z. Foo and Denis M.O. Cheong, Department of General Surgery, Tan Tock Seng Hospital, Singapore.
NOVA SCOTIA RECTAL CANCER PROJECT: A POPULATION-BASED ASSESSMENT OF RECTAL CANCER CARE AND OUTCOMES. Devon Paula Richardson
 NOVA SCOTIA RECTAL CANCER PROJECT: A POPULATION-BASED ASSESSMENT OF RECTAL CANCER CARE AND OUTCOMES by Devon Paula Richardson Submitted in partial fulfilment of the requirements for the degree of Master
NOVA SCOTIA RECTAL CANCER PROJECT: A POPULATION-BASED ASSESSMENT OF RECTAL CANCER CARE AND OUTCOMES by Devon Paula Richardson Submitted in partial fulfilment of the requirements for the degree of Master
Mohamed EL-hemaly Gastro- intestinal surgical center, Mansoura University.
 Mohamed EL-hemaly Gastro- intestinal surgical center, Mansoura University. Chronic transmural inflammatory process of the bowel & affects any part of the gastro -intestinal tract from the mouth to the
Mohamed EL-hemaly Gastro- intestinal surgical center, Mansoura University. Chronic transmural inflammatory process of the bowel & affects any part of the gastro -intestinal tract from the mouth to the
This is the portion of the intestine which lies between the small intestine and the outlet (Anus).
.") THE COLON This is the portion of the intestine which lies between the small intestine and the outlet (Anus). 3 4 5 This part is responsible for formation of stool. The large intestine (colon- coloured
THE COLON This is the portion of the intestine which lies between the small intestine and the outlet (Anus). 3 4 5 This part is responsible for formation of stool. The large intestine (colon- coloured
Long-term efficacy of vacuum-assisted therapy (Endo-SPONGE ) in large anastomotic leakages following anterior rectal resection
 in large anastomotic leakages following anterior rectal resection") ORIGINAL ARTICLE Annals of Gastroenterology (2017) 30, 1-5 Long-term efficacy of vacuum-assisted therapy (Endo-SPONGE ) in large anastomotic leakages following anterior rectal resection Alessandro Mussetto
ORIGINAL ARTICLE Annals of Gastroenterology (2017) 30, 1-5 Long-term efficacy of vacuum-assisted therapy (Endo-SPONGE ) in large anastomotic leakages following anterior rectal resection Alessandro Mussetto
preparing for surgery
 preparing for surgery Facing the news that you need to have a stoma is very difficult but with thousands of people having stoma surgery each year, it is important to remember that you are not alone and
preparing for surgery Facing the news that you need to have a stoma is very difficult but with thousands of people having stoma surgery each year, it is important to remember that you are not alone and
Preoperative Data Colorectal Cancer Database
 Preoperative Data Please place patient label here Patient Information Patient s Last Name First Middle Initial UR MH MP Birth Date Sex Post Code / / M F ECOG (see codes below) Date of Diagnosis Consultant
Preoperative Data Please place patient label here Patient Information Patient s Last Name First Middle Initial UR MH MP Birth Date Sex Post Code / / M F ECOG (see codes below) Date of Diagnosis Consultant
Temporary Diverting Stoma Improves Recovery of Anastomotic Leakage after Anterior Resection for Rectal Cancer
 www.nature.com/scientificreports Received: 5 April 2017 Accepted: 7 November 2017 Published: xx xx xxxx OPEN Temporary Diverting Stoma Improves Recovery of Anastomotic Leakage after Anterior Resection
www.nature.com/scientificreports Received: 5 April 2017 Accepted: 7 November 2017 Published: xx xx xxxx OPEN Temporary Diverting Stoma Improves Recovery of Anastomotic Leakage after Anterior Resection
Surgery for Ulcerative Colitis 11/14/10. Colectomy for Ulcerative Colitis: What your patient should know. Surgery for Ulcerative Colitis
 Colectomy for Ulcerative Colitis: What your patient should know Madhulika G. Varma MD Associate Professor and Chief Section of Colorectal Surgery University of California, San Francisco Surgery for Ulcerative
Colectomy for Ulcerative Colitis: What your patient should know Madhulika G. Varma MD Associate Professor and Chief Section of Colorectal Surgery University of California, San Francisco Surgery for Ulcerative
LONG TERM OUTCOME OF ELECTIVE SURGERY
 LONG TERM OUTCOME OF ELECTIVE SURGERY Roberto Persiani Associate Professor Mini-invasive Oncological Surgery Unit Institute of Surgical Pathology (Dir. prof. D. D Ugo) Dis Colon Rectum, March 2000 Dis
LONG TERM OUTCOME OF ELECTIVE SURGERY Roberto Persiani Associate Professor Mini-invasive Oncological Surgery Unit Institute of Surgical Pathology (Dir. prof. D. D Ugo) Dis Colon Rectum, March 2000 Dis
Considering whether to have ileal pouch surgery
 Considering whether to have ileal pouch surgery A guide for ulcerative colitis patients By Dr Andrew McCombie (Ulcerative Colitis Researcher and living with an ileal pouch) Co-authored by Associate Professor
Considering whether to have ileal pouch surgery A guide for ulcerative colitis patients By Dr Andrew McCombie (Ulcerative Colitis Researcher and living with an ileal pouch) Co-authored by Associate Professor
, may spread caudally to present as a perianal abscess, laterally across the external sphincter to form an ischiorectal abscess or, rarely,
 ANORECTAL ABSCESSES , may spread caudally to present as a perianal abscess, laterally across the external sphincter to form an ischiorectal abscess or, rarely, superiorly above the anorectal junction
ANORECTAL ABSCESSES , may spread caudally to present as a perianal abscess, laterally across the external sphincter to form an ischiorectal abscess or, rarely, superiorly above the anorectal junction
Management of pt1 polyps. Maria Pellise
 Management of pt1 polyps Maria Pellise Early colorectal cancer Malignant polyp Screening programmes SM Invasive adenocar cinoma Advances in diagnostic & therapeutic endoscopy pt1 polyps 0.75 5.6% of large-bowel
Management of pt1 polyps Maria Pellise Early colorectal cancer Malignant polyp Screening programmes SM Invasive adenocar cinoma Advances in diagnostic & therapeutic endoscopy pt1 polyps 0.75 5.6% of large-bowel
DATA REPORT. August 2014
 AUDIT DATA REPORT August 2014 Prepared for the Australian and New Zealand Gastric and Oesophageal Surgical Association by the Royal Australasian College of Surgeons 199 Ward St, North Adelaide, SA 5006
AUDIT DATA REPORT August 2014 Prepared for the Australian and New Zealand Gastric and Oesophageal Surgical Association by the Royal Australasian College of Surgeons 199 Ward St, North Adelaide, SA 5006