Bladder Cancer: Overview, diagnosis and treatment with a focus on outpatient clinical issues
|
|
|
- Raymond George
- 5 years ago
- Views:
Transcription

1 Bladder Cancer: Overview, diagnosis and treatment with a focus on outpatient clinical issues William F. Santis, M.D. Concord Hospital Center for Urologic Care September 28, 2013
2 Goals: Overview of bladder cancer Treatment options for various stages of bladder cancer Surgical options for patients requiring cystectomy and urinary diversion including post operative care Keep you awake Ask me questions throughout this talk! Audience composition?
3 Epidemiology: 72,570 new cases of bladder cancer in the U.S.A. each year 15,210 deaths each year in U.S.A. 2.7x more common in men Smoking related 4 th most common cancer in men Lung, prostate and colorectal 8 th most common cancer in women
4 Pathology: Transition cell carcinoma (>90%) Squamous cell carcinoma (1%) Adenocarcinoma (2%) Urachal carcinoma Metastatic adenocarcinoma From rectum, prostate, endometrium, breast and ovary




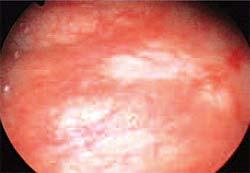
5 Name the location?
6 Etiology: Cigarette Smoking Lung blood urine bladder Specific agent unclear (nitrosamines, 2- naphthaline) implicated At least 50-52% CaBladder smoking related Increased risk >4 times Related to duration/amount smoking, and degree of inhalation Smoking Smoking and and chemical chemical exposure exposure history history important important in in evaluation evaluation of of hematuria hematuria patient patient
7 Etiology: Occupational exposures: 25-30% cases Aniline dyes (to color clothing), benzidine, xenylamine and many others Higher risk in auto workers, painters, drivers, machine workers, dry cleaners, paper and clothing workers? Color hair> each 6 wks Chlorinated H2O increases risk fold (byproduct Trihalomethanes as cause) Consumption of Chinese herbs that contain aristolochic acid or prescription of aristolochic
8 Etiology: Cyclophosphomide Phenacetin, Thiazolidinediones,?HPV, Chronic cystitis: Squamous cell carcinoma Longstanding bladder calculi Schistosoma haemotobium Indwelling catheters 2-10% SCI pts with indwelling catheter Any Any patient patient with with LE>10 LE>10 yrs yrs who who has has a chronic chronic catheter..ask catheter..ask why? why?
9 54 yo man with 4d gross/painless hematuria No flank pain/some difficulty completely emptying/no fever. PMH: COPD, HTN, Nephrolithiasis, ED PSH: Appy, Chole, RIH Meds: HCTZ, Albuterol NKDA SH: 0-2 EtOH/d, 40 pack yrs, mechanic in machine shop What do you want to look for in the office? What will trigger an admission?
10 54 yo man with 4d gross/painless hematuria Retention Need for cath? Need for CBI Infection Anemia Colic/Pain control Hematuria w/u with cysto/cytol/ct
11 Signs/Symptoms: Painless hematuria 85% of patients Flank pain Ureteral obstruction Lower extremity edema Weight loss, abdominal or bone pain Signs of advanced disease
12 Diagnosis: Hematuria Evaluation Flexible or rigid cystoscopy Urine cytology Upper urinary tract studies Hematuria CT best study IVP Ultrasound not adequate

13 Name the Red Sox Player?



14
15 Staging: Resection of bladder tumor Determine depth of invasion and grade Can be curative in superficial disease Random biopsies to rule out CIS Muscle must be included Consideration of single dose Mitomycin CT Scan Chest imaging Bone scan Usually not necessary if alkaline phosphatase is wnl

16


17
18 Post TURBT complications: Infection Clot retention Perforation TUR syndrome LUTS Ureteral obstruction

19 Pathology: Stage Tis=CIS Tis=CIS Ta: Non-invasive T1: Lamina propria invasion T2a: Muscle invasion/superficial T2b: Muscle invasion/deep T3a: Perivesical fat invasion T4: invasion continuous organs
20 Pathology: Grade Low grade: usually papillary High grade: Papillary or solid 50% muscle invasive Evil Often associated with CIS Stage is where it is, grade is the cellular aggressiveness

21 Superficial v. Invasive Bladder Cancer: Massive difference in behavior and treatment Patients die from invasive disease that becomes metastatic
22 Natural history: 70% are low grade superficial tumors Greater than 25% will recur Usually from other sites in bladder (field defect) 10-15% pts with superficial disease develop invasive disease 30% pts present with muscle invasive disease 50% of these pts already have distant mets



23
24 CIS
25 Treatment: Cis Intravesical therapy: immuno or chemotherapy Baccillus Calmette-Guerin (BCG) Attenuated mycobacterium bovis Stimulates immune response Can be used in conjunction with alpha interferon Consider SWOG maintenance regiment Mitomycin, adriamycin, thiotepa Dysuria, frequency, infection, BCG systemic absorbtion
26 Treatment: Ta/T1 TURBT 10-15% will require more aggressive tx High rate of recurrent lesions Intravesical BCG will decrease frequency of recurrence Consider SWOG 3yr maintenance Follow up cystoscopy, cytology and IVP Surveillance for recurrent bladder tumors 2-5% will develop upper tract tumors
27 Treatment Grade 3/T1: Grade 3/T1 may have as high as 46% chance of developing muscle invasion Reasonable to consider cystectomy especially if CIS present Reresection to assure no understaging If TURBT/BCG Follow up critical Maintenance BCG





28
29 CT: Muscle invasive CaBladder

30





31
32 Treatment: Muscle invasive disease Standard treatment: Radical cystectomy with urinary diversion Consider neoadjuvant chemotherapy Distal ureteral margin frozen section +/- urethrectomy Men: cystoprostatectomy with LND Women: anterior pelvic exenteration Removal of uterus, fallopian tubes, ovaries, and anterior wall of vagina
33 Invasive disease Time from resection to cystectomy will impact survival curves (RN navigator) Preop cardiology and pulmonary evaluation Teaching regarding options for diversion Enterostomal therapist visit Staging and oncology consultation regarding possible neoadjuvant chemo
34 Radical cystectomy: Complications 25-30% complication rate Wound infections (10%) Intestinal obstruction Hemorrhage Cardiopulmonary complications Rectal injury 1-2% mortality You You guys guys see see all all of of this! this!
35 Radical Cystectomy: Open v. Robotic Robotic assisted laparoscopic surgery will have less blood loss, smaller incisions and less negative influence on bowel function Prostatectomy experience has allowed us to perform cystectomies robotically Diversion can be done lap or open Difficult if multiple prior surgery



36
37 Urinary Diversion: Bladder removed/need divert urine Use of intestinal segments results in metabolic abnormalities Use of intestinal segment with stoma Most successful Diversion to the urethra Continent cutaneous urinary diversion
38 Urinary Diversion: Ileal conduit Most common form of urinary diversion Isolated ileal segment to right lower quadrant stoma Ureteroileal anastamosis Complications: Ureterointestinal stenosis Bowel obstruction/anastamotic leakage Post Post op: op: Diversion Diversion stents stents out out of of stoma stoma and and 2 JP JP drains drains

39 Ileal Conduit: Ureteroileal anastamosis

40 Ileal conduit: Stoma
41 Urinary Diversion: ileal conduit + - Rapid Low complication rate Good stoma Low reoperation rate Urostomy/Bag Self image

42 Name this athlete?


43
44 Urinary Diversion: Non-ileal conduits In selected cases other segments of bowel must be used Transverse colon Sigmoid colon Jejunal conduit Ileocecal conduit
45 Urinary diversion to the urethra: Neobladders No evidence of disease at bladder neck or urethra (no CIS?) Young, motivated patient Pt informed of increased complication rate. 5% chance of urethral recurrence Retention: Pt must be willing to self catheterize as needed Nocturnal enuresis (25% or more)
46 Studer neobladder: This This is is the the most most common common neobladder neobladder performed performed
47 Tube Tube fiesta!!! fiesta!!! Post Post op op nursing nursing care care critical critical
48 Post operative care Regular irrigation of neobladder to assure no mucous accumulating and drainage of urine This is through and through with outflow open All tubes must remain secure Failure of above could result in Prolonged neobladder urine leak Loss of tube across anastamosis or stent requiring re-exploration Never Never hesitate hesitate to to call call surgeon. surgeon. We We would would rather rather have have a question question answered answered than than have have a mistake mistake made made
49 Post discharge care Patient usually discharged with SP tube/urethral catheter and stents internal Pt on self irrigation regiment SP tube removed while urethral foley still in in place Urethral catheter removed after cystogram shows no leak Pt taugh CIC and irrigation Pt weans CIC over time if residual wnl Neobladder enlargens over first post op year
50 Neobladder: Sample of complications that present to the office Retention Neobladder perforation Infection Ureteral obstruction Bowel obstruction Urine leak Bowel leak Incontinence

51



52
53 Continent cutaneous urinary diversion Reservoir for urine storage Abdominal stoma for catheterization of continent mechanism No appliance Continence achieved via: Ileocecal valve Imbrication, Tapering or Intussusception Appendix
54 Continent cutaneous urinary diversion Koch, Mainz, UCLA, Indiana, Florida Need to have manual dexterity Complication rate >10% Failure of continence mechanism Continent at low volume, not at high

55 Indiana pouch: You You will will see see some some types types of of reconstructions reconstructions similar similar to to this this with with Dr. Dr. Triaca s Triaca s neurogenic neurogenic bladder bladder patients patients
56 Case 1: 81 yo woman with dysuria Cystoscopy: large, flat based tumor TURBT: T2a, Grade III Staging: Bone scan -, CT -, CXR Plan? Radical Cystectomy Ileal conduit urinary diversion Muscle invasive high grade disease
57 Case 2: 52 yo man with gross hematuria Cystoscopy: Single posterior large mass TURBT: T2a, Grade III, random bx Staging: Bone scan -, CXR -, CT Radical cystectomy Ileal neobladder




58
59 Case 3: 78 yo man with gross hematuria Cysto: multiple papillary lesions TURBT: Ta/Grade I IVP: WNL Plan? Surveillance with q3mos cystoscopy, cytology and yearly IVP Superficial low grade disease
60 Case 4: 45 you woman with microscopic hematuria Cystoscopy: Few erythematous patches Bladder biopsy: Multifocal CIS Plan? Treatment: Intravesical BCG qwk x 6wks Follow up: Bladder biopsy, repeat cytology, IVP Strongly suggest maintenance BCG per SWOG protocol
61 Thank you!
Joseph H. Williams, MD Idaho Urologic Institute St. Alphonsus Regional Medical Center September 22, 2016
 BLADDER CANCER Joseph H. Williams, MD Idaho Urologic Institute St. Alphonsus Regional Medical Center September 22, 2016 BLADDER CANCER = UROTHELIAL CANCER Antiquated term is Transitional Cell Carcinoma
BLADDER CANCER Joseph H. Williams, MD Idaho Urologic Institute St. Alphonsus Regional Medical Center September 22, 2016 BLADDER CANCER = UROTHELIAL CANCER Antiquated term is Transitional Cell Carcinoma
BLADDER CANCER: PATIENT INFORMATION
 BLADDER CANCER: PATIENT INFORMATION The bladder is the balloon like organ located in the pelvis that stores and empties urine. Urine is produced by the kidneys, is conducted to the bladder by the ureters,
BLADDER CANCER: PATIENT INFORMATION The bladder is the balloon like organ located in the pelvis that stores and empties urine. Urine is produced by the kidneys, is conducted to the bladder by the ureters,
URINARY DIVERSIONS. Winter 2016 Dr P. O Malley
 URINARY DIVERSIONS Winter 2016 Dr P. O Malley OVERVIEW Who gets diversions? What s involved with cystectomy? What are the different types of diversions? What are the problems with various diversions? How
URINARY DIVERSIONS Winter 2016 Dr P. O Malley OVERVIEW Who gets diversions? What s involved with cystectomy? What are the different types of diversions? What are the problems with various diversions? How
Carcinoma of the Urinary Bladder Histopathology
 Carcinoma of the Urinary Bladder Histopathology Reporting Proforma (Radical & Partial Cystectomy, Cystoprostatectomy) Includes the International Collaboration on Cancer reporting dataset denoted by * Family
Carcinoma of the Urinary Bladder Histopathology Reporting Proforma (Radical & Partial Cystectomy, Cystoprostatectomy) Includes the International Collaboration on Cancer reporting dataset denoted by * Family
Bladder Cancer Guidelines
 Bladder Cancer Guidelines Agreed by Urology CSG: October 2011 Review Date: September 2013 Bladder Cancer 1. Referral Guidelines The following patients should be considered as potentially having bladder
Bladder Cancer Guidelines Agreed by Urology CSG: October 2011 Review Date: September 2013 Bladder Cancer 1. Referral Guidelines The following patients should be considered as potentially having bladder
Bladder replacement in men and women: when and when not? Outline. Continent Diversion History
 1 Bladder replacement in men and women: when and when not? Eila C. Skinner, MD Professor of Clinical Urology Keck USC School of Medicine Outline 1) Selection criteria for orthotopic diversion: Tumor-related
1 Bladder replacement in men and women: when and when not? Eila C. Skinner, MD Professor of Clinical Urology Keck USC School of Medicine Outline 1) Selection criteria for orthotopic diversion: Tumor-related
MUSCLE - INVASIVE AND METASTATIC BLADDER CANCER
 10 MUSCLE - INVASIVE AND METASTATIC BLADDER CANCER Recommendations from the EAU Working Party on Muscle Invasive and Metastatic Bladder Cancer G. Jakse (chairman), F. Algaba, S. Fossa, A. Stenzl, C. Sternberg
10 MUSCLE - INVASIVE AND METASTATIC BLADDER CANCER Recommendations from the EAU Working Party on Muscle Invasive and Metastatic Bladder Cancer G. Jakse (chairman), F. Algaba, S. Fossa, A. Stenzl, C. Sternberg
Urological Tumours 1 Kidney tumours 2 Bladder tumours
 Urological Tumours 1 Kidney tumours 2 Bladder tumours Tim Bracey SpR Histopathology Derriford Hospital Kidney tumours What are we going to talk about?! Anatomy of urinary tract! Types of kidney tumours!
Urological Tumours 1 Kidney tumours 2 Bladder tumours Tim Bracey SpR Histopathology Derriford Hospital Kidney tumours What are we going to talk about?! Anatomy of urinary tract! Types of kidney tumours!
Cystectomies and bladder preservation: What you need to know
 Cystectomies and bladder preservation: What you need to know Robin Morash RN, BNSc, MHS Bladder Cancer Canada November 21, 2018 Presentation goals Review the options for treatment of muscle-invasive bladder
Cystectomies and bladder preservation: What you need to know Robin Morash RN, BNSc, MHS Bladder Cancer Canada November 21, 2018 Presentation goals Review the options for treatment of muscle-invasive bladder
3.1 Investigations for Patients Presenting with Haematuria Table 1
 3.1 Investigations for Patients Presenting with Haematuria Table 1 Patients at risk of bacterial endocarditis should be given antibiotic prophylaxis as per local guidelines. Patients with heart valve replacements
3.1 Investigations for Patients Presenting with Haematuria Table 1 Patients at risk of bacterial endocarditis should be given antibiotic prophylaxis as per local guidelines. Patients with heart valve replacements
MUSCLE-INVASIVE AND METASTATIC BLADDER CANCER
 MUSCLE-INVASIVE AND METASTATIC BLADDER CANCER (Text update March 2008) A. Stenzl (chairman), N.C. Cowan, M. De Santis, G. Jakse, M. Kuczyk, A.S. Merseburger, M.J. Ribal, A. Sherif, J.A. Witjes Introduction
MUSCLE-INVASIVE AND METASTATIC BLADDER CANCER (Text update March 2008) A. Stenzl (chairman), N.C. Cowan, M. De Santis, G. Jakse, M. Kuczyk, A.S. Merseburger, M.J. Ribal, A. Sherif, J.A. Witjes Introduction
MEDitorial March Bladder Cancer
 MEDitorial March 2010 Bladder Cancer Last month, my article addressed the issue of blood in the urine ( hematuria ). A concerning cause of hematuria is bladder cancer, a variably malignant tumor starting
MEDitorial March 2010 Bladder Cancer Last month, my article addressed the issue of blood in the urine ( hematuria ). A concerning cause of hematuria is bladder cancer, a variably malignant tumor starting
UNDERSTANDING BLADDER CANCER
 UNDERSTANDING BLADDER CANCER Learn About Your Treatment Options After Your Diagnosis If your doctor has told you that you have bladder cancer, you likely have many questions and concerns. Learning about
UNDERSTANDING BLADDER CANCER Learn About Your Treatment Options After Your Diagnosis If your doctor has told you that you have bladder cancer, you likely have many questions and concerns. Learning about
Management of High Grade, T1 Bladder Cancer Douglas S. Scherr, M.D.
 Management of High Grade, T1 Bladder Cancer Douglas S. Scherr, M.D. Assistant Professor of Urology Clinical Director, Urologic Oncology Weill Medical College-Cornell University Estimated new cancer cases.
Management of High Grade, T1 Bladder Cancer Douglas S. Scherr, M.D. Assistant Professor of Urology Clinical Director, Urologic Oncology Weill Medical College-Cornell University Estimated new cancer cases.
Bladder Cancer in Primary Care. Dr Penny Kehagioglou Consultant Clinical Oncologist
 Bladder Cancer in Primary Care Dr Penny Kehagioglou Consultant Clinical Oncologist Objectives Patient presentation in primary care Investigating bladder cancer Management of bladder cancer Differential
Bladder Cancer in Primary Care Dr Penny Kehagioglou Consultant Clinical Oncologist Objectives Patient presentation in primary care Investigating bladder cancer Management of bladder cancer Differential
Bladder Cancer Canada November 21st, Bladder Cancer 2018: A brighter light at the end of the cystoscope
 Bladder Cancer Canada November 21st, 2018 Bladder Cancer 2018: A brighter light at the end of the cystoscope Chris Morash MD FRCSC Associate Professor, University of Ottawa Head, Urological Oncology Bladder
Bladder Cancer Canada November 21st, 2018 Bladder Cancer 2018: A brighter light at the end of the cystoscope Chris Morash MD FRCSC Associate Professor, University of Ottawa Head, Urological Oncology Bladder
Radical Cystectomy A Patient s Guide
 Radical Cystectomy A Patient s Guide Introduction The urinary system, which includes the bladder, urethra, ureters, and kidneys, helps maintain stable chemical conditions in the body, stores, and eliminates
Radical Cystectomy A Patient s Guide Introduction The urinary system, which includes the bladder, urethra, ureters, and kidneys, helps maintain stable chemical conditions in the body, stores, and eliminates
Guidelines for the Management of Bladder Cancer West Midlands Expert Advisory Group for Urological Cancer
 Guidelines for the Management of Bladder Cancer West Midlands Expert Advisory Group for Urological Cancer West Midlands Clinical Networks and Clinical Senate Coversheet for Network Expert Advisory Group
Guidelines for the Management of Bladder Cancer West Midlands Expert Advisory Group for Urological Cancer West Midlands Clinical Networks and Clinical Senate Coversheet for Network Expert Advisory Group
Management of Superficial Bladder Cancer Douglas S. Scherr, M.D.
 Management of Superficial Bladder Cancer Douglas S. Scherr, M.D. Assistant Professor of Urology Clinical Director, Urologic Oncology Weill Medical College-Cornell University Estimated new cancer cases.
Management of Superficial Bladder Cancer Douglas S. Scherr, M.D. Assistant Professor of Urology Clinical Director, Urologic Oncology Weill Medical College-Cornell University Estimated new cancer cases.
Case 1. Receives induction BCG weekly x 6 without significant toxicity Next step should be:
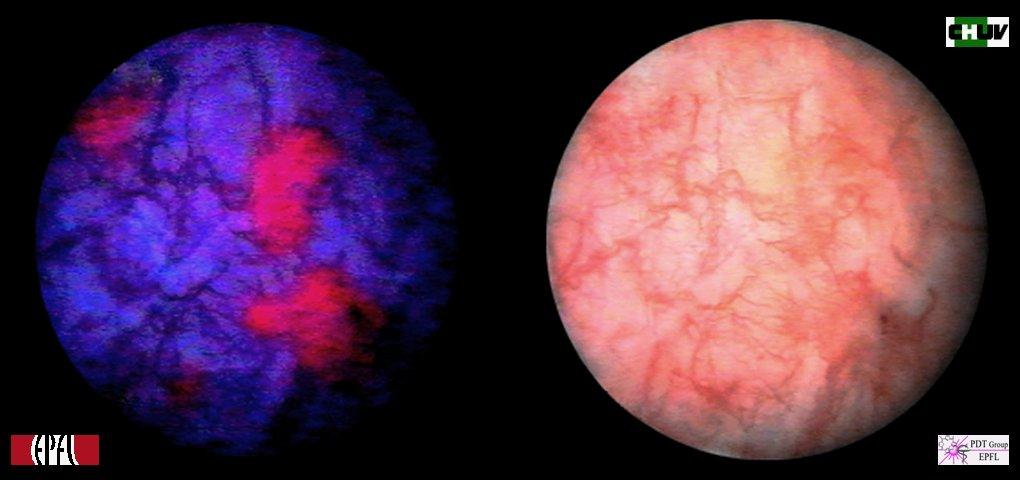
 Case 1 89 year old male with initial occurrence of gross hematuria Office flexible cystoscopy shows two papillary tumors with some surface necrosis Complete TURBT into muscle Florescence cysto shows two
Case 1 89 year old male with initial occurrence of gross hematuria Office flexible cystoscopy shows two papillary tumors with some surface necrosis Complete TURBT into muscle Florescence cysto shows two
A patient with recurrent bladder cancer presents with the following history:
 MP/H Quiz A patient with recurrent bladder cancer presents with the following history: 9/23/06 TURB 1/12/07 TURB 4/1/07 TURB 7/12/07 TURB 11/14/07 Non-invasive papillary transitional cell carcinoma from
MP/H Quiz A patient with recurrent bladder cancer presents with the following history: 9/23/06 TURB 1/12/07 TURB 4/1/07 TURB 7/12/07 TURB 11/14/07 Non-invasive papillary transitional cell carcinoma from
Attachment #2 Overview of Follow-up
 Attachment #2 Overview of Follow-up Provided below is a general overview of follow-up and this may vary based on specific patient or cancer characteristics. Of note, Labs and imaging can be performed closer
Attachment #2 Overview of Follow-up Provided below is a general overview of follow-up and this may vary based on specific patient or cancer characteristics. Of note, Labs and imaging can be performed closer
Part II: Treatment. A Woman-to-Woman Talk with Dr. Armine Smith. Wednesday, March 8, Presented by
 Women & Bladder Cancer A Woman-to-Woman Talk with Dr. Armine Smith Wednesday, March 8, 2017 Part II: Treatment Presented by Dr. Smith is an Assistant Professor of Urology at Johns Hopkins University and
Women & Bladder Cancer A Woman-to-Woman Talk with Dr. Armine Smith Wednesday, March 8, 2017 Part II: Treatment Presented by Dr. Smith is an Assistant Professor of Urology at Johns Hopkins University and
Attachment #2 Overview of Follow-up
 Attachment #2 Overview of Follow-up Provided below is a general overview of follow-up and this may vary based on specific patient or cancer characteristics. Of note, Labs and imaging can be performed closer
Attachment #2 Overview of Follow-up Provided below is a general overview of follow-up and this may vary based on specific patient or cancer characteristics. Of note, Labs and imaging can be performed closer
When to Integrate Surgery for Metatstatic Urothelial Cancers
 When to Integrate Surgery for Metatstatic Urothelial Cancers Wade J. Sexton, M.D. Senior Member and Professor Department of Genitourinary Oncology Moffitt Cancer Center Case Presentation #1 67 yo male
When to Integrate Surgery for Metatstatic Urothelial Cancers Wade J. Sexton, M.D. Senior Member and Professor Department of Genitourinary Oncology Moffitt Cancer Center Case Presentation #1 67 yo male
Understanding Women's Sexuality after Bladder Cancer webinar. Part I: The Physical Impact
 Understanding Women's Sexuality after Bladder Cancer webinar Tuesday, December 1, 2015 Part I: The Physical Impact Presented by LaShon Day received her Masters of Science as a Physician s Assistant at
Understanding Women's Sexuality after Bladder Cancer webinar Tuesday, December 1, 2015 Part I: The Physical Impact Presented by LaShon Day received her Masters of Science as a Physician s Assistant at
Hey Doc, there s blood in my urine Evaluation of hematuria. Christian S. Kuhr, MD FACS May 4, 2018
 Hey Doc, there s blood in my urine Evaluation of hematuria Christian S. Kuhr, MD FACS May 4, 2018 Objectives Understand the algorithm for hematuria evaluation Know the differential diagnosis for hematuria
Hey Doc, there s blood in my urine Evaluation of hematuria Christian S. Kuhr, MD FACS May 4, 2018 Objectives Understand the algorithm for hematuria evaluation Know the differential diagnosis for hematuria
Staging and Grading Last Updated Friday, 14 November 2008
 Staging and Grading Last Updated Friday, 14 November 2008 There is a staging graph below Blood in the urine is the most common indication that something is wrong. Often one will experience pain or difficulty
Staging and Grading Last Updated Friday, 14 November 2008 There is a staging graph below Blood in the urine is the most common indication that something is wrong. Often one will experience pain or difficulty
Panel: A Case-based Approach to the Management of Bladder Cancer
 Panel: A Case-based Approach to the Management of Bladder Cancer ~ Moderator: Robert Donohue, MD Panel: David C. Beyer, MD E. David Crawford, MD Donald L. Lamm, MD Paul D. Maroni, MD TCC Cases Robert E.
Panel: A Case-based Approach to the Management of Bladder Cancer ~ Moderator: Robert Donohue, MD Panel: David C. Beyer, MD E. David Crawford, MD Donald L. Lamm, MD Paul D. Maroni, MD TCC Cases Robert E.
 A Personal History NIH CWRU U of TN U of Miami Animal Model for Bladder Cancer Carcinogen induced FANFT Three Models Primary tumors individual tumors, simulates clinical scenario of locally advanced cancer
A Personal History NIH CWRU U of TN U of Miami Animal Model for Bladder Cancer Carcinogen induced FANFT Three Models Primary tumors individual tumors, simulates clinical scenario of locally advanced cancer
3. Urinary Catheters. Indications. Methods of Bladder Catheterization. Hashim Hashim
 3. Urinary Catheters Hashim Hashim Indications Urinary catheters are used to drain urine from the bladder. The main indications are: A. Diagnostic Measure post-void residual in the absence of ultrasound
3. Urinary Catheters Hashim Hashim Indications Urinary catheters are used to drain urine from the bladder. The main indications are: A. Diagnostic Measure post-void residual in the absence of ultrasound
GUIDELINES ON NON-MUSCLE- INVASIVE BLADDER CANCER
 GUIDELINES ON NON-MUSCLE- INVASIVE BLADDER CANCER (Limited text update December 21) M. Babjuk, W. Oosterlinck, R. Sylvester, E. Kaasinen, A. Böhle, J. Palou, M. Rouprêt Eur Urol 211 Apr;59(4):584-94 Introduction
GUIDELINES ON NON-MUSCLE- INVASIVE BLADDER CANCER (Limited text update December 21) M. Babjuk, W. Oosterlinck, R. Sylvester, E. Kaasinen, A. Böhle, J. Palou, M. Rouprêt Eur Urol 211 Apr;59(4):584-94 Introduction
Case by Case: Critical Issues in Superficial Bladder Cancer Management 5/24/05 13:46 1
 Case by Case: Critical Issues in Superficial Bladder Cancer Management 5/24/05 13:46 1 Case Study 1 A 22-year-old man with a history of gross total painless hematuria: two times in two months, both after
Case by Case: Critical Issues in Superficial Bladder Cancer Management 5/24/05 13:46 1 Case Study 1 A 22-year-old man with a history of gross total painless hematuria: two times in two months, both after
Bladder Cancer Basics For the Newly Diagnosed
 Bladder Cancer Basics For the Newly Diagnosed Bladder Cancer Advocacy Network The information in this patient guide is not intended to take the place of medical care or the advice of your doctor. Please
Bladder Cancer Basics For the Newly Diagnosed Bladder Cancer Advocacy Network The information in this patient guide is not intended to take the place of medical care or the advice of your doctor. Please
Pathology Driving Decisions
 Pathology Driving Decisions Part I: Understanding Your Diagnosis and Your Treatment Options May 7, 2018 Presented by: Dr. Matthew Mossanen completed his college and medical school training at UCLA. He
Pathology Driving Decisions Part I: Understanding Your Diagnosis and Your Treatment Options May 7, 2018 Presented by: Dr. Matthew Mossanen completed his college and medical school training at UCLA. He
URINARY DIVERSIONS. Susan Hilton, MD and Nicholas Papanicolaou, MD Co-Chiefs, CT Section Hospital of the University of Pennsylvania
 URINARY DIVERSIONS Susan Hilton, MD and Nicholas Papanicolaou, MD Co-Chiefs, CT Section Hospital of the University of Pennsylvania Neither of us has any financial relationships with commercial interests
URINARY DIVERSIONS Susan Hilton, MD and Nicholas Papanicolaou, MD Co-Chiefs, CT Section Hospital of the University of Pennsylvania Neither of us has any financial relationships with commercial interests
Non-Muscle Invasive Bladder Cancer BCG Failures: University of Iowa Hospitals and Clinics Experience. Paul Gellhaus Assistant Clinical Professor
 Non-Muscle Invasive Bladder Cancer BCG Failures: University of Iowa Hospitals and Clinics Experience Paul Gellhaus Assistant Clinical Professor Iowa??? none Disclosures Caveats Dr. Michael O Donnell
Non-Muscle Invasive Bladder Cancer BCG Failures: University of Iowa Hospitals and Clinics Experience Paul Gellhaus Assistant Clinical Professor Iowa??? none Disclosures Caveats Dr. Michael O Donnell
BLADDER HEALTH. Muscle Invasive Bladder Cancer: A Patient Guide
 BLADDER HEALTH Muscle Invasive Bladder Cancer: A Patient Guide Table of Contents Bladder Cancer Expert Panel Mike's Story: A Patient Story.... Introduction.... GET THE FACTS What is bladder cancer?....
BLADDER HEALTH Muscle Invasive Bladder Cancer: A Patient Guide Table of Contents Bladder Cancer Expert Panel Mike's Story: A Patient Story.... Introduction.... GET THE FACTS What is bladder cancer?....
Advanced Pathophysiology Unit 7: Renal-Urologic Page 1 of 6
 Advanced Pathophysiology Unit 7: Renal-Urologic Page 1 of 6 Learning Objectives for this File: 1. Understand how clinical presentation drives the diagnostic workup 2. Recognize how patient education is
Advanced Pathophysiology Unit 7: Renal-Urologic Page 1 of 6 Learning Objectives for this File: 1. Understand how clinical presentation drives the diagnostic workup 2. Recognize how patient education is
Information for Patients. Primary urethral cancer. English
 Information for Patients Primary urethral cancer English Table of contents What is primary urethral cancer?... 3 Risk factors... 3 Symptoms... 4 Diagnosis... 4 Clinical examination... 4 Urinary cytology...
Information for Patients Primary urethral cancer English Table of contents What is primary urethral cancer?... 3 Risk factors... 3 Symptoms... 4 Diagnosis... 4 Clinical examination... 4 Urinary cytology...
Muscle-invasive bladder cancer
 Patient Information English 4 Muscle-invasive bladder cancer The underlined terms are listed in the glossary. What is muscle-invasive bladder cancer? About a quarter of patients diagnosed with bladder
Patient Information English 4 Muscle-invasive bladder cancer The underlined terms are listed in the glossary. What is muscle-invasive bladder cancer? About a quarter of patients diagnosed with bladder
Glossary of Terms Primary Urethral Cancer
 Patient Information English Glossary of Terms Primary Urethral Cancer Advanced cancer A tumour that grows into deeper layers of tissue, adjacent organs, or surrounding muscles. Anaesthesia (general, spinal,
Patient Information English Glossary of Terms Primary Urethral Cancer Advanced cancer A tumour that grows into deeper layers of tissue, adjacent organs, or surrounding muscles. Anaesthesia (general, spinal,
Q&A. Fabulous Prizes. Collecting Cancer Data: Bladder, Renal Pelvis, and Ureter 5/2/13. NAACCR Webinar Series
 Collecting Cancer Data Bladder & Renal Pelvis NAACCR 2012 2013 Webinar Series Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching
Collecting Cancer Data Bladder & Renal Pelvis NAACCR 2012 2013 Webinar Series Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching
BCAN Fall Series: Survivorship
 BCAN Fall Series: Survivorship The New Normal after Bladder Removal and Urinary Diversion Vashti Livingston RN, MS, CNS, CWOCN Ambulatory Urology MSKCC NYC livingsv@mskcc.org Disclosure None BCAN Volunteer
BCAN Fall Series: Survivorship The New Normal after Bladder Removal and Urinary Diversion Vashti Livingston RN, MS, CNS, CWOCN Ambulatory Urology MSKCC NYC livingsv@mskcc.org Disclosure None BCAN Volunteer
Non Muscle Invasive Bladder Cancer. Primary and Recurrent TCC 4/10/2010. Two major consequences: Strategies: High-Risk NMI TCC
 Intravesical Therapy 2010-When, with What, When to Stop Friday, April 9, 2010 Ralph de VereWhite, MD Director, UC Davis Cancer Center Associate Dean for Cancer Programs Professor, Department of Urolgoy
Intravesical Therapy 2010-When, with What, When to Stop Friday, April 9, 2010 Ralph de VereWhite, MD Director, UC Davis Cancer Center Associate Dean for Cancer Programs Professor, Department of Urolgoy
Bladder Trauma Data Collection Sheet
 Bladder Trauma Data Collection Sheet If there was no traumatic injury with PENETRATION of the bladder DO NOT proceed Date of injury: / / Time of injury: Date of hospital arrival: / / Time of hospital arrival:
Bladder Trauma Data Collection Sheet If there was no traumatic injury with PENETRATION of the bladder DO NOT proceed Date of injury: / / Time of injury: Date of hospital arrival: / / Time of hospital arrival:
Bladder Case 1 SURGICAL PATHOLOGY REPORT. Procedure: Cystoscopy, transurethral resection of bladder tumor (TURBT)
") Bladder Case 1 February 17, 2007 Specimen (s) received: Bladder Tumor Pre-operative Diagnosis: Bladder Cancer Post operative Diagnosis: Bladder Cancer Procedure: Cystoscopy, transurethral resection of
Bladder Case 1 February 17, 2007 Specimen (s) received: Bladder Tumor Pre-operative Diagnosis: Bladder Cancer Post operative Diagnosis: Bladder Cancer Procedure: Cystoscopy, transurethral resection of
Index. Surg Oncol Clin N Am 14 (2005) Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type.") Surg Oncol Clin N Am 14 (2005) 433 439 Index Note: Page numbers of article titles are in boldface type. A Abdominosacral resection, of recurrent rectal cancer, 202 215 Ablative techniques, image-guided,
Surg Oncol Clin N Am 14 (2005) 433 439 Index Note: Page numbers of article titles are in boldface type. A Abdominosacral resection, of recurrent rectal cancer, 202 215 Ablative techniques, image-guided,
Diagnosis and classification
 Patient Information English 2 Diagnosis and classification The underlined terms are listed in the glossary. Signs and symptoms Blood in the urine is the most common symptom when a bladder tumour is present.
Patient Information English 2 Diagnosis and classification The underlined terms are listed in the glossary. Signs and symptoms Blood in the urine is the most common symptom when a bladder tumour is present.
Urethral Carcinoma Recurrence in Ileal Orthotopic Neobladder: Urethrectomy and Conversion in a Continent Pouch with Abdominal Stoma
 Case Report Urol Int 1999;62:213 216 Received: June 19, 1998 Accepted after revision: March 8, 1999 Urethral Carcinoma Recurrence in Ileal Orthotopic Neobladder: Urethrectomy and Conversion in a Continent
Case Report Urol Int 1999;62:213 216 Received: June 19, 1998 Accepted after revision: March 8, 1999 Urethral Carcinoma Recurrence in Ileal Orthotopic Neobladder: Urethrectomy and Conversion in a Continent
Reviewing Immunotherapy for Bladder Carcinoma In Situ
 Reviewing Immunotherapy for Bladder Carcinoma In Situ Samir Bidnur Dept of Urologic Sciences, Grand Rounds March 1 st, 2017 Checkpoint Inhibition and Bladder Cancer, an evolving story with immunotherapy
Reviewing Immunotherapy for Bladder Carcinoma In Situ Samir Bidnur Dept of Urologic Sciences, Grand Rounds March 1 st, 2017 Checkpoint Inhibition and Bladder Cancer, an evolving story with immunotherapy
Haematuria and Bladder Cancer
 Haematuria and Bladder Cancer Dr Pardeep Kumar Consultant Urological Surgeon Haematuria 3 Haematuria Macroscopic vs Microscopic Painful vs Painless Concurrent abdo pain/urinary symptoms Previous testing?
Haematuria and Bladder Cancer Dr Pardeep Kumar Consultant Urological Surgeon Haematuria 3 Haematuria Macroscopic vs Microscopic Painful vs Painless Concurrent abdo pain/urinary symptoms Previous testing?
URETHRAL CANCER EPIDEMIOLOGY - 1
 URETHRAL CANCER Diagnosis & Management Case Conferences Jennie Mickelson Grand Rounds November 15, 2006 EPIDEMIOLOGY - 1 RARE 2200 reported cases F:M - 4:1 1 FEMALE URETHRAL CA any age but >60 most common
URETHRAL CANCER Diagnosis & Management Case Conferences Jennie Mickelson Grand Rounds November 15, 2006 EPIDEMIOLOGY - 1 RARE 2200 reported cases F:M - 4:1 1 FEMALE URETHRAL CA any age but >60 most common
Clinical Commissioning Policy Proposition: Robotic Assisted Surgery for Bladder Cancer
 Clinical Commissioning Policy Proposition: Robotic Assisted Surgery for Bladder Cancer Reference: NHS England B14X08 Information Reader Box (IRB) to be inserted on inside front cover for documents of 6
Clinical Commissioning Policy Proposition: Robotic Assisted Surgery for Bladder Cancer Reference: NHS England B14X08 Information Reader Box (IRB) to be inserted on inside front cover for documents of 6
Open Radical Cystectomy Tips and Tricks in Males and Females
 Open Radical Cystectomy Tips and Tricks in Males and Females Seth P. Lerner, MD, FACS Professor of Urology Beth and Dave Swalm Chair in Urologic Oncology Scott Department of Urology Baylor College of Medicine
Open Radical Cystectomy Tips and Tricks in Males and Females Seth P. Lerner, MD, FACS Professor of Urology Beth and Dave Swalm Chair in Urologic Oncology Scott Department of Urology Baylor College of Medicine
Glossary of terms Urinary Incontinence
 Patient Information English Glossary of terms Urinary Incontinence Anaesthesia (general, spinal, or local) Before a procedure you will get medication to make sure that you don t feel pain. Under general
Patient Information English Glossary of terms Urinary Incontinence Anaesthesia (general, spinal, or local) Before a procedure you will get medication to make sure that you don t feel pain. Under general
Hong Kong College of Surgical Nursing
 Hong Kong College of Surgical Nursing Higher Surgical Nursing Training: Part B Specialty - Urological Nursing Curriculum TABLE OF CONTENTS No. Contents Page. Introduction. Aims. Learning Objectives 4.
Hong Kong College of Surgical Nursing Higher Surgical Nursing Training: Part B Specialty - Urological Nursing Curriculum TABLE OF CONTENTS No. Contents Page. Introduction. Aims. Learning Objectives 4.
NMIBC. Piotr Jarzemski. Department of Urology Jan Biziel University Hospital Bydgoszcz, Poland
 NMIBC Piotr Jarzemski Department of Urology Jan Biziel University Hospital Bydgoszcz, Poland 71 year old male patient was admitted to the Department of Urology First TURBT - 2 months prior to the hospitalisation.
NMIBC Piotr Jarzemski Department of Urology Jan Biziel University Hospital Bydgoszcz, Poland 71 year old male patient was admitted to the Department of Urology First TURBT - 2 months prior to the hospitalisation.
Bladder cancer - suspected
 Background information Information resources for patients and carers Updates to this care map Bladder cancer - clinical presentation History Examination Consider differential diagnoses Clinical indications
Background information Information resources for patients and carers Updates to this care map Bladder cancer - clinical presentation History Examination Consider differential diagnoses Clinical indications
Bladder Cancer Handbook
 Bladder Cancer Handbook Table of Contents Overview Page Numbers Understanding Your Diagnosis Page 4 About this Handbook What To Do Before Your Doctor Visit Page 5 Page 6 Important Phone Numbers Page 7
Bladder Cancer Handbook Table of Contents Overview Page Numbers Understanding Your Diagnosis Page 4 About this Handbook What To Do Before Your Doctor Visit Page 5 Page 6 Important Phone Numbers Page 7
Bladder cancer (BC) is the fifth most commonly diagnosed malignancy in the United
 is the fifth most commonly diagnosed malignancy in the United") 1 Chapter 1: Background 1.1 Bladder Cancer Incidence and Etiology Bladder cancer (BC) is the fifth most commonly diagnosed malignancy in the United States, with more than 70,000 new cases and more than
1 Chapter 1: Background 1.1 Bladder Cancer Incidence and Etiology Bladder cancer (BC) is the fifth most commonly diagnosed malignancy in the United States, with more than 70,000 new cases and more than
Bladder Cancer. Clinical Case Conference
 Bladder Cancer Clinical Case Conference Clinical Case 89 yo M with gross hematuria Labs: Chem: BUN/Cr increased 22/1.27 CBC: H/H 13/36, WBCs wnl UA: >50 RBCs, otherwise wnl UCx: No growth Cystoscopy at
Bladder Cancer Clinical Case Conference Clinical Case 89 yo M with gross hematuria Labs: Chem: BUN/Cr increased 22/1.27 CBC: H/H 13/36, WBCs wnl UA: >50 RBCs, otherwise wnl UCx: No growth Cystoscopy at
10/23/2012 CASE STUDIES: RENAL AND UROLOGIC IMPAIRMENTS. 1) Are there any clues from this history that suggest a particular diagnosis?
 Are there any clues from this history that suggest a particular diagnosis?") Case # 1 An underwriter enters your office, hands you a sheet of paper, and asks What do you think? Can we make an offer? You look at the paper and see it s lab results on a 60 year male looking for $500,000
Case # 1 An underwriter enters your office, hands you a sheet of paper, and asks What do you think? Can we make an offer? You look at the paper and see it s lab results on a 60 year male looking for $500,000
Carcinoma of the Renal Pelvis and Ureter Histopathology
 Carcinoma of the Renal Pelvis and Ureter Histopathology Reporting Proforma (NEPHROURETERECTOMY AND URETERECTOMY) Includes the International Collaboration on Cancer reporting dataset denoted by * Family
Carcinoma of the Renal Pelvis and Ureter Histopathology Reporting Proforma (NEPHROURETERECTOMY AND URETERECTOMY) Includes the International Collaboration on Cancer reporting dataset denoted by * Family
Understanding Bladder Cancer
 Understanding Bladder Cancer A guide for people with cancer, their families and friends Cancer information www.cancercouncil.com.au Understanding Bladder Cancer A guide for people with cancer, their families
Understanding Bladder Cancer A guide for people with cancer, their families and friends Cancer information www.cancercouncil.com.au Understanding Bladder Cancer A guide for people with cancer, their families
Collection of Recorded Radiotherapy Seminars
 IAEA Human Health Campus Collection of Recorded Radiotherapy Seminars http://humanhealth.iaea.org Conservative Treatment of Invasive Bladder Cancer Luis Souhami, MD Professor Department of Radiation Oncology
IAEA Human Health Campus Collection of Recorded Radiotherapy Seminars http://humanhealth.iaea.org Conservative Treatment of Invasive Bladder Cancer Luis Souhami, MD Professor Department of Radiation Oncology
Surgery for Inflammatory Bowel Disease
 Surgery for Inflammatory Bowel Disease Emily Steinhagen, MD Assistant Professor Department of Surgery, Division of Colorectal Surgery University Hospitals Cleveland Medical Center Common Questions Why
Surgery for Inflammatory Bowel Disease Emily Steinhagen, MD Assistant Professor Department of Surgery, Division of Colorectal Surgery University Hospitals Cleveland Medical Center Common Questions Why
Symptoms, Diagnosis and Classification
 Patient Information English 2 Symptoms, Diagnosis and Classification The underlined terms are listed in the glossary. Signs and symptoms Blood in the urine is the most common symptom when a bladder tumour
Patient Information English 2 Symptoms, Diagnosis and Classification The underlined terms are listed in the glossary. Signs and symptoms Blood in the urine is the most common symptom when a bladder tumour
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES GYNECOLOGIC CANCER CERVIX
 PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES GYNECOLOGIC CANCER CERVIX Site Group: Gynecology Cervix Author: Dr. Stephane Laframboise 1. INTRODUCTION 3 2. PREVENTION 3 3. SCREENING AND
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES GYNECOLOGIC CANCER CERVIX Site Group: Gynecology Cervix Author: Dr. Stephane Laframboise 1. INTRODUCTION 3 2. PREVENTION 3 3. SCREENING AND
Sara Schaenzer Grand Rounds January 24 th, 2018
 Sara Schaenzer Grand Rounds January 24 th, 2018 Bladder Anatomy Ureter Anatomy Areas of Injury Bladder: Posterior bladder wall above trigone Ureter Crosses beneath uterine vessels At pelvic brim when ligating
Sara Schaenzer Grand Rounds January 24 th, 2018 Bladder Anatomy Ureter Anatomy Areas of Injury Bladder: Posterior bladder wall above trigone Ureter Crosses beneath uterine vessels At pelvic brim when ligating
Care of bladder cancer patients diagnosed in Northern Ireland 2010 & 2011 (Summary)
") Care of bladder cancer patients diagnosed in 2010 & 2011 (Summary) Bannon, F., Ranaghan, L., & Gavin, A. (2014). Care of bladder cancer patients diagnosed in 2010 & 2011 (Summary). N. Cancer Registry,
Care of bladder cancer patients diagnosed in 2010 & 2011 (Summary) Bannon, F., Ranaghan, L., & Gavin, A. (2014). Care of bladder cancer patients diagnosed in 2010 & 2011 (Summary). N. Cancer Registry,
Cystectomy and Bladder Reconstruction (Continent Urinary Diversion) Department of Urology Information for patients
 Department of Urology Information for patients") Cystectomy and Bladder Reconstruction (Continent Urinary Diversion) Department of Urology Information for patients i Introduction You and your consultant have decided that you need a cystectomy (removal
Cystectomy and Bladder Reconstruction (Continent Urinary Diversion) Department of Urology Information for patients i Introduction You and your consultant have decided that you need a cystectomy (removal
Bladder Cancer. Patient. in the Neurogenic. Anne P. Cameron MD FRCSC. Assistant Professor, University of Michigan
 Bladder Cancer in the Neurogenic Patient Anne P. Cameron MD FRCSC Assistant Professor, University of Michigan Outline Incidence Pathology Risk factors Diagnosis Screening Treatment Case: Emily injection
Bladder Cancer in the Neurogenic Patient Anne P. Cameron MD FRCSC Assistant Professor, University of Michigan Outline Incidence Pathology Risk factors Diagnosis Screening Treatment Case: Emily injection
Appendix 4 Urology Care Pathways
 Appendix 4 Urology Care Pathways Cancer Care Pathways outline the steps and stages in the patient journey from referral through to diagnostics, staging, treatment, follow up, rehabilitation and if applicable
Appendix 4 Urology Care Pathways Cancer Care Pathways outline the steps and stages in the patient journey from referral through to diagnostics, staging, treatment, follow up, rehabilitation and if applicable
5/26/16: CT scan of the abdomen showed a multinodular liver disease highly suspicious for metastasis and hydronephrosis of the right kidney.
 Bladder Case Scenario 1 History 5/23/16: A 52-year-old male, smoker was admitted to our hospital with a 3-month history of right pelvic pain, multiple episodes of gross hematuria, dysuria, and extreme
Bladder Case Scenario 1 History 5/23/16: A 52-year-old male, smoker was admitted to our hospital with a 3-month history of right pelvic pain, multiple episodes of gross hematuria, dysuria, and extreme
Neoplasms of the Prostate and Bladder
 Neoplasms of the Prostate and Bladder 2015-2016 FCDS Educational Webcast Series Steven Peace, BS, CTR September 19, 2015 2015 Focus o Anatomy o SSS 2000 o MPH Rules o AJCC TNM 1 CDC & Florida DOH Attribution
Neoplasms of the Prostate and Bladder 2015-2016 FCDS Educational Webcast Series Steven Peace, BS, CTR September 19, 2015 2015 Focus o Anatomy o SSS 2000 o MPH Rules o AJCC TNM 1 CDC & Florida DOH Attribution
Radical Cystectomy Often Too Late? Yes, But...
 european urology 50 (2006) 1129 1138 available at www.sciencedirect.com journal homepage: www.europeanurology.com Editorial 50th Anniversary Radical Cystectomy Often Too Late? Yes, But... Urs E. Studer
european urology 50 (2006) 1129 1138 available at www.sciencedirect.com journal homepage: www.europeanurology.com Editorial 50th Anniversary Radical Cystectomy Often Too Late? Yes, But... Urs E. Studer
Male genital tract tumors. SiCA. Division of Urology, Department of Surgery, Faculty of Medicine Siriraj Hospital.
 Male genital tract tumors Division of Urology, Department of Surgery, Faculty of Medicine Siriraj Hospital. adenocarcinoma Prostate Cancer most common male cancer in western countries more detected in
Male genital tract tumors Division of Urology, Department of Surgery, Faculty of Medicine Siriraj Hospital. adenocarcinoma Prostate Cancer most common male cancer in western countries more detected in
Point-Counterpoint: Radiation & Bladder Cancer
 Radiation Plays a Major Role in Certain Stages of Bladder Cancer ~ David C. Beyer, MD Radiation Therapy; no role in management of bladder cancer Robert E. Donohue M.D. Denver VAMC University of Colorado
Radiation Plays a Major Role in Certain Stages of Bladder Cancer ~ David C. Beyer, MD Radiation Therapy; no role in management of bladder cancer Robert E. Donohue M.D. Denver VAMC University of Colorado
The pathology of bladder cancer
 1 The pathology of bladder cancer Charles Jameson Introduction Carcinoma of the bladder is the seventh most common cancer worldwide [1]. It comprises 3.2% of all cancers, with an estimated 260 000 new
1 The pathology of bladder cancer Charles Jameson Introduction Carcinoma of the bladder is the seventh most common cancer worldwide [1]. It comprises 3.2% of all cancers, with an estimated 260 000 new
Upper Tract Tcc. Mohan Arianayagam FRACS (Urology)
") Upper Tract Tcc Mohan Arianayagam FRACS (Urology) Epidemiology Peak incidence 75 to 79 years 2x more common in men 7% of all renal tumours 5% of all urothelial tumours Synchronous bilateral is rare ~ 1.6%
Upper Tract Tcc Mohan Arianayagam FRACS (Urology) Epidemiology Peak incidence 75 to 79 years 2x more common in men 7% of all renal tumours 5% of all urothelial tumours Synchronous bilateral is rare ~ 1.6%
Citation International journal of urology (2. Right which has been published in final f
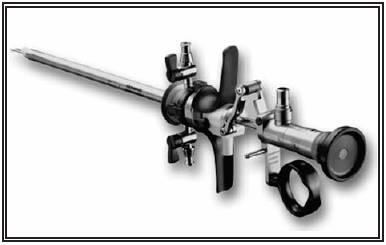
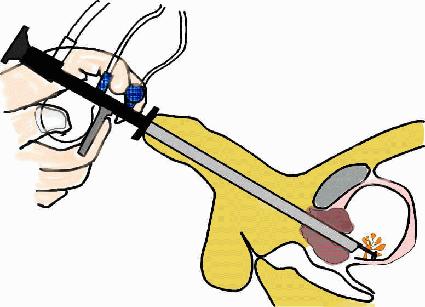
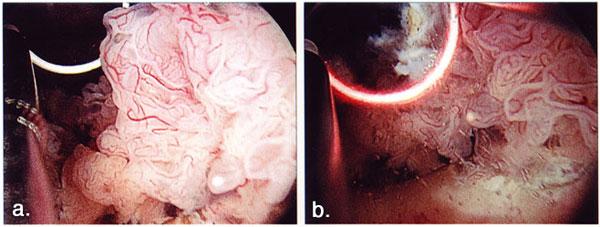
 Title Novel constant-pressure irrigation of renal pelvic tumors after ipsila Nakamura, Kenji; Terada, Naoki; Sug Author(s) Toshinori; Matsui, Yoshiyuki; Imamu Kazutoshi; Kamba, Tomomi; Yoshimura Citation
Title Novel constant-pressure irrigation of renal pelvic tumors after ipsila Nakamura, Kenji; Terada, Naoki; Sug Author(s) Toshinori; Matsui, Yoshiyuki; Imamu Kazutoshi; Kamba, Tomomi; Yoshimura Citation
Arieh L. Shalhav Is There a Risk in Robotic Nephroureterectomy?
 Arieh L. Shalhav Is There a Risk in Robotic Nephroureterectomy? 80 patients LNU (n = 40) or ONU (n = 40) CSS (p = 0.2), BRFS (p = 0.86), MFS (p = 0.12) similar for the entire cohort Subgroups of pt3 UTUC
Arieh L. Shalhav Is There a Risk in Robotic Nephroureterectomy? 80 patients LNU (n = 40) or ONU (n = 40) CSS (p = 0.2), BRFS (p = 0.86), MFS (p = 0.12) similar for the entire cohort Subgroups of pt3 UTUC
CHEMO-RADIOTHERAPY FOR BLADDER CANCER. Dr Darren Mitchell Consultant Clinical Oncologist Northern Ireland Cancer Centre
 CHEMO-RADIOTHERAPY FOR BLADDER CANCER Dr Darren Mitchell Consultant Clinical Oncologist Northern Ireland Cancer Centre AIMS Muscle invasive disease Current Gold-Standard Rationale behind Chemo-Radiotherapy
CHEMO-RADIOTHERAPY FOR BLADDER CANCER Dr Darren Mitchell Consultant Clinical Oncologist Northern Ireland Cancer Centre AIMS Muscle invasive disease Current Gold-Standard Rationale behind Chemo-Radiotherapy
Koji Ichihara Hiroshi Kitamura Naoya Masumori Fumimasa Fukuta Taiji Tsukamoto
 Int J Clin Oncol (2013) 18:75 80 DOI 10.1007/s10147-011-0346-8 ORIGINAL ARTICLE Transurethral prostate biopsy before radical cystectomy remains clinically relevant for decision-making on urethrectomy in
Int J Clin Oncol (2013) 18:75 80 DOI 10.1007/s10147-011-0346-8 ORIGINAL ARTICLE Transurethral prostate biopsy before radical cystectomy remains clinically relevant for decision-making on urethrectomy in
Trimodality Therapy for Muscle Invasive Bladder Cancer
 Trimodality Therapy for Muscle Invasive Bladder Cancer Brita Danielson, MD, FRCPC Radiation Oncologist, Cross Cancer Institute Assistant Professor, Department of Oncology University of Alberta Edmonton,
Trimodality Therapy for Muscle Invasive Bladder Cancer Brita Danielson, MD, FRCPC Radiation Oncologist, Cross Cancer Institute Assistant Professor, Department of Oncology University of Alberta Edmonton,
THE operation of reimplantation of the ureter into the bladder has undergone
 REIMPLANTATION OF THE URETER INTO THE BLADDER J. G. WARDEN, M.D., and C. C. HIGGINS, M.D. Department of Urology THE operation of reimplantation of the ureter into the bladder has undergone a stormy course
REIMPLANTATION OF THE URETER INTO THE BLADDER J. G. WARDEN, M.D., and C. C. HIGGINS, M.D. Department of Urology THE operation of reimplantation of the ureter into the bladder has undergone a stormy course
AUA Guidelines for Invasive Bladder Cancer: What s New?
 AUA Guidelines for Invasive Bladder Cancer: What s New? Michael S. Cookson, MD, MMHC Professor and Chairman Department of Urology, University of Oklahoma History 1999: AUA guidelines Panel Non-muscle invasive
AUA Guidelines for Invasive Bladder Cancer: What s New? Michael S. Cookson, MD, MMHC Professor and Chairman Department of Urology, University of Oklahoma History 1999: AUA guidelines Panel Non-muscle invasive
Bladder Tumours Urology Patient Information Leaflet
 Bladder Tumours Urology Patient Information Leaflet Page 1 Bladder Tumours You have just been informed that you have a bladder tumour (cancer). Bladder growths vary in severity and can range from a minor
Bladder Tumours Urology Patient Information Leaflet Page 1 Bladder Tumours You have just been informed that you have a bladder tumour (cancer). Bladder growths vary in severity and can range from a minor
A schematic of the rectal probe in contact with the prostate is show in this diagram.
 Hello. My name is William Osai. I am a nurse practitioner in the GU Medical Oncology Department at The University of Texas MD Anderson Cancer Center in Houston. Today s presentation is Part 2 of the Overview
Hello. My name is William Osai. I am a nurse practitioner in the GU Medical Oncology Department at The University of Texas MD Anderson Cancer Center in Houston. Today s presentation is Part 2 of the Overview
Urinary Bladder, Ureter, and Renal Pelvis
 Urinary Bladder, Ureter, and Renal Pelvis Protocol applies to all carcinomas of the urinary bladder, ureter, and renal pelvis. Protocol revision date: January 2005 Based on AJCC/UICC TNM, 6th edition Procedures
Urinary Bladder, Ureter, and Renal Pelvis Protocol applies to all carcinomas of the urinary bladder, ureter, and renal pelvis. Protocol revision date: January 2005 Based on AJCC/UICC TNM, 6th edition Procedures
Etiology and diagnosis of bladder cancer
 Etiology and diagnosis of bladder cancer Introduction Incidence: the most common urothelial tumor, representing the 2 nd most common urological tumor in men (4 th in overall frequency) and the 1 st in
Etiology and diagnosis of bladder cancer Introduction Incidence: the most common urothelial tumor, representing the 2 nd most common urological tumor in men (4 th in overall frequency) and the 1 st in
Urethral Stricture Management. AUA Guidelines. Michael Coburn, MD Scott Department of Urology Baylor College of Medicine Houston, Texas
 Urethral Stricture Management AUA Guidelines Michael Coburn, MD Scott Department of Urology Baylor College of Medicine Houston, Texas Urethral Stricture Guidelines Systematic peer-reviewed literature review
Urethral Stricture Management AUA Guidelines Michael Coburn, MD Scott Department of Urology Baylor College of Medicine Houston, Texas Urethral Stricture Guidelines Systematic peer-reviewed literature review
Blue Ridge Urogynecology
 Surgery for Stress Urinary Incontinence Surgery has proved to be a very effective treatment for stress incontinence. The best surgical procedures improve or cure the incontinence in 85 to 90 percent of
Surgery for Stress Urinary Incontinence Surgery has proved to be a very effective treatment for stress incontinence. The best surgical procedures improve or cure the incontinence in 85 to 90 percent of
Bladder Case # 1. Principal Diagnosis: Bladder Tumor, Suspect Transitional Cell Carcinoma. Secondary Diagnoses: 1. Hypertension. 2. Hyperlipidemia.
 DISCHARGE SUMMARY Bladder Case # 1 Date: 04/22/2010 Principal Diagnosis: Bladder Tumor, Suspect Transitional Cell Carcinoma. Secondary Diagnoses: 1. Hypertension. 2. Hyperlipidemia. Hospital Course: Mr.
DISCHARGE SUMMARY Bladder Case # 1 Date: 04/22/2010 Principal Diagnosis: Bladder Tumor, Suspect Transitional Cell Carcinoma. Secondary Diagnoses: 1. Hypertension. 2. Hyperlipidemia. Hospital Course: Mr.
5/21/2018. Prostate Adenocarcinoma vs. Urothelial Carcinoma. Common Differential Diagnoses in Urological Pathology. Jonathan I.
 Common Differential Diagnoses in Urological Pathology Jonathan I. Epstein Prostate Adenocarcinoma vs. Urothelial Carcinoma 1 2 NKX3.1 NKX3.1 3 4 5 6 Proposed ISUP Recommendations Option to use PSA as a
Common Differential Diagnoses in Urological Pathology Jonathan I. Epstein Prostate Adenocarcinoma vs. Urothelial Carcinoma 1 2 NKX3.1 NKX3.1 3 4 5 6 Proposed ISUP Recommendations Option to use PSA as a
CYSVIEW. CONFIDENCE AT FIRST SIGHT
 CYSVIEW. CONFIDENCE AT FIRST SIGHT Blue Light Cystoscopy with CYSVIEW Cysview Indication Cysview is an optical imaging agent indicated for use in the cystoscopic detection of non-muscle invasive papillary
CYSVIEW. CONFIDENCE AT FIRST SIGHT Blue Light Cystoscopy with CYSVIEW Cysview Indication Cysview is an optical imaging agent indicated for use in the cystoscopic detection of non-muscle invasive papillary
Information for Patients. Bladder Cancer. English
 Information for Patients Bladder Cancer English Table of contents What is the function of the bladder?... 3 What is bladder cancer?... 3 What causes bladder cancer?... 3 Stages of the disease... 3 Risk
Information for Patients Bladder Cancer English Table of contents What is the function of the bladder?... 3 What is bladder cancer?... 3 What causes bladder cancer?... 3 Stages of the disease... 3 Risk
Management of High-Risk Non-Muscle Invasive Bladder Cancer. Seth P. Lerner, MD, FACS
 Management of High-Risk Non-Muscle Invasive Bladder Cancer Seth P. Lerner, MD, FACS Professor of Urology, Beth and Dave Swalm Chair in Urologic Oncology, Scott Department of Urology, Baylor College of
Management of High-Risk Non-Muscle Invasive Bladder Cancer Seth P. Lerner, MD, FACS Professor of Urology, Beth and Dave Swalm Chair in Urologic Oncology, Scott Department of Urology, Baylor College of