Colorectal procedure guide
|
|
|
- Nora Small
- 5 years ago
- Views:
Transcription




1 Colorectal procedure guide Illustrations by Lisa Clark Biodesign ADVANCED TISSUE REPAIR cookmedical.com
2 2
3 INDEX Anal fistula repair Using the Biodesign plug with no button Anal fistula repair Using the Biodesign plug with the button... 8 Ventral hernia repair Ventral rectopexy...16 The techniques presented in this guide are recommendations that should help you achieve optimum results, but this guide is not meant to be a substitute for the instructions for use. 3

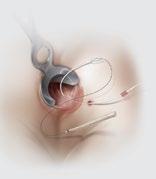
4 Anal fistula repair Using the Biodesign plug with no button The Biodesign Anal Fistula Plug Set is used for the repair of anorectal fistulas. The surgeon should decide whether to perform bowel preparation and/or a small-volume enema. A single preoperative dose of systemic antibiotic is recommended. A continuous dosage of the antibiotic is unnecessary. 4

5 ANAL FISTULA REPAIR 1. Place a draining seton if any signs of sepsis or infection are present, and allow the tract to mature and stabilize for six to eight weeks before you place the plug. After you inspect the seton and fistula, irrigate the tract with hydrogen peroxide or a similar fluid. Cut the seton and attach a suture to the cut end. 2. Tie the suture to the Cook Fistula Brush. Pull the brush catheter into the fistula tract. Using a back-and-forth motion, clean and remove nonvascular tissue. A small amount of blood at the tract and on the brush s bristles indicates adequate debridement. Do not mechanically debride the fistula tract in a way that would likely make the tract wider and harder to close. 5


6 ANAL FISTULA REPAIR 3. Hydrate the plug in sterile saline for no more than one minute. Tie the plug onto the suture. Use hydrogen peroxide or a similar fluid again to irrigate the tract and flush loose debris. 4A. Blind-pass technique: Pull the plug, narrow end first, into the fistula tract until you feel slight resistance. Affix the plug by using a 2-0 long-term absorbable suture on a UR6 or comparable needle. Adjacent to the internal opening, pass a stitch deep into the sphincter muscles and directly through the center of the plug, exiting on the opposite side. Gently pull the plug partially out of the internal opening to verify that the stitch went directly through the plug. Pull the plug back to its original position. Remove any slack from the sutures in the fistula tract. Some products or part numbers may not be available in all markets. Contact your local Cook representative or Customer Service for details. 6

, and make a stitch perpendicular to your first stitch.")
7 4B. Direct-visualization technique: Place the plug as described in step 4A, then pull the plug partially out of the internal opening. Adjacent to the internal opening, pass a stitch deep into the sphincter muscles without piercing the plug. Continue the stitch by passing the needle directly through the center of the plug. Continue the stitch by passing the needle down alongside the plug, deep into the sphincter muscles. 5. Repeat the previous step (4A or 4B depending on which technique you chose), and make a stitch perpendicular to your first stitch. Note: If you are using the direct-visualization technique, then at the end of this step, pull the plug back to its original position. 6. Tie off the sutures over the top of the plug, effectively pulling the mucosal layer over the top of the plug. No part of the plug should be visible at the internal opening. Trim any external portion of the plug flush with the skin. Slightly enlarge the external opening to facilitate drainage. Drainage is expected for a minimum of 2 weeks and can continue for up to 12 weeks. Provide the patient with the postoperative patient guide. The patient s compliance with the guide directly affects the success of the plug. 7

8 Anal fistula repair Using the Biodesign plug with the button The Biodesign Fistula Plug Set is used for the repair of rectovaginal and anorectal fistulas. The surgeon should decide whether to perform bowel preparation and/or a small-volume enema. A single preoperative dose of systemic antibiotic is recommended. A continuous dosage of the antibiotic is unnecessary. 8


9 ANAL FISTULA REPAIR 1. Place a draining seton if any signs of sepsis or infection are present, and allow the tract to mature and stabilize for six to eight weeks before you place the plug. After you inspect the seton and fistula, irrigate the tract with hydrogen peroxide or a similar fluid. Cut the seton and attach a suture to the cut end. 2. Tie the suture to the Cook Fistula Brush. Pull the brush catheter into the fistula tract. Using a back-and-forth motion, clean and remove nonvascular tissue. A small amount of blood at the tract and on the brush s bristles indicates adequate debridement. Do not mechanically debride the fistula tract in a way that would likely make the tract wider and harder to close. 9



10 ANAL FISTULA REPAIR 3. Hydrate the plug in sterile saline for no more than one minute. Tie the plug onto the suture. Use hydrogen peroxide or a similar fluid again to irrigate the tract and flush loose debris. 4A. Superficial placement: Pull the plug, narrow end first, into the fistula tract until the button is flush against the mucosa. Affix the plug by using a 2-0 long-term absorbable suture on a UR6 or comparable needle. Place four sutures through the center of the plug, deep into the sphincter muscles. Some products or part numbers may not be available in all markets. Contact your local Cook representative or Customer Service for details. 10


11 4B. Submucosal placement: Create small mucosal flaps or undermine the mucosa circumferentially to create a small pocket that can accommodate the button portion of the plug. Place the plug as described in step 4A; the button portion should be flush with the internal sphincter. Then reapproximate the mucosal edges, and completely cover the button. 5. Trim any external portion of the plug flush with the skin. Slightly enlarge the external opening to facilitate drainage. Drainage is expected for a minimum of 2 weeks and can continue up to 12 weeks. Provide the patient with the postoperative patient guide. The patient s compliance with the guide directly affects the success of the plug. 11


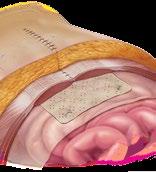
12 Ventral hernia repair The Biodesign Hernia Graft is used to reinforce soft tissue where weakness exists, including a hernia or body wall defect. 12



13 VENTRAL HERNIA REPAIR 1. Hydrate the graft for no longer than one minute in a roomtemperature, sterile, lactated Ringer s solution or sterile saline. 2. If you use an open procedure to place the graft, preperitoneal, retrorectus, or intraperitoneal placement is recommended. For a laparoscopic procedure, intraperitoneal placement is recommended. 13

14 VENTRAL HERNIA REPAIR 3. Trim the graft to fit the site, providing an allowance for overlap. Fundamental surgical principles suggest recurrence can be minimized if the mesh overlaps the surrounding tissue by 4-5 cm in all directions 1. When 5 cm of overlap is not attainable, overlap as much tissue as possible. 4. Bridging the hernia with only the graft is not recommended. To attain primary closure of the defects, use relaxing incisions, perform component separation, or perform retrorectus placement. If bridging is unavoidable, follow the best practices described in the IFU. 1. Klinge U, Conze J, Krones, C, et al. Incisional Hernia: Open Techniques. World J Surg. 2005;29(8): Some products or part numbers may not be available in all markets. Contact your local Cook representative or Customer Service for details. 14



15 5. Use permanent or long-term absorbable sutures and tacks. The horizontal mattress suture technique is recommended. Place sutures 3 cm apart and with a bite depth of 1 cm. 6. Place closed suction drains, and leave them in place for two to six weeks. Remove the drains when their output is < 20 ml per 24 hours for at least two consecutive days or until the drains are dry. 15


16 Ventral rectopexy The Biodesign Rectopexy Graft is intended to reinforce soft tissue where weakness exists in the gastroenterological anatomy including the transabdominal repair of colon and rectal prolapse. Ventral rectopexy is one option for repairing rectal prolapse. Surgeons should use their own judgement to decide which procedure fits each patient. 16




17 VENTRAL RECTOPEXY 1. Put your patient in the modified Lloyd Davies position. Secure the patient s arms. Establish access to the pneumoperitoneum and the laparoscopic port. 2. Perform a technique of your preference to retract the sigmoid colon and uterus. 17




18 VENTRAL RECTOPEXY 3. Incise the peritoneum superficially from the sacral promontory down to the pouch of Douglas. Excise the pouch of Douglas, and continue to dissect the rectovaginal plane to the anal canal. Dissect laterally as necessary. 4. Shape the Biodesign graft according to your preference, and hydrate in sterile lactated Ringer s solution or in sterile saline for less than one minute. 18



19 5. Position the Biodesign graft so that the distal portion touches the anterior rectum and the proximal portion touches the sacral promontory. Suture the distal portion to the anterior rectum with approximately six interrupted, long-term absorbable sutures. Trim excess graft material as required. Use either tacks or sutures to secure the graft to the sacral promontory in a way that keeps the graft under minimal tension. An additional suture in the posterior vaginal wall can secure the rectovaginal plane closure. Additional sutures can secure the surrounding tissues to the graft. 6. To help the body remodel Biodesign, ensure maximum contact between the graft and the tissue, and ensure that the graft is under minimal tension. Close the exposed peritoneal edges with a continuous suture over the Biodesign graft. Confirm hemostasis. Release the sigmoid colon and pelvic structures, and close the port sites. 19
20 MEDICAL COOK 09/2017 SUR-D37168-EN-F
Robot Assisted Rectopexy
 1. Abdominal cavity approach 1A Trocars Introduce Introduce five trocars to gain access to the abdominal cavity (in da Vinci Si type; In Xi type the trocar placement may differ slightly). First the camera
1. Abdominal cavity approach 1A Trocars Introduce Introduce five trocars to gain access to the abdominal cavity (in da Vinci Si type; In Xi type the trocar placement may differ slightly). First the camera
Case Report. XCM Biologic Tissue Matrix. Components separation using sandwich technique for reconstruction of abdominal wall defect.
 Case Report XCM Biologic Tissue Matrix. Components separation using sandwich technique for reconstruction of abdominal wall defect. XCM Biologic Tissue Matrix. Components separation using sandwich technique
Case Report XCM Biologic Tissue Matrix. Components separation using sandwich technique for reconstruction of abdominal wall defect. XCM Biologic Tissue Matrix. Components separation using sandwich technique
Ventral Hernia Repair
 Ventral Hernia Repair Ventrio ST Hernia Patch Ventrio Hernia Patch Technique Guide Open and Laparoscopic Ventral Hernia Repair SOFT TISSUE REPAIR Right Procedure. Right Product. Right Outcome. This Technique
Ventral Hernia Repair Ventrio ST Hernia Patch Ventrio Hernia Patch Technique Guide Open and Laparoscopic Ventral Hernia Repair SOFT TISSUE REPAIR Right Procedure. Right Product. Right Outcome. This Technique
RECTAL INJURY IN UROLOGIC SURGERY. Inadvertent rectal injury from a urologic procedure is often subtle but has serious postoperative consequences.
 RECTAL INJURY IN 27 UROLOGIC SURGERY Inadvertent rectal injury from a urologic procedure is often subtle but has serious postoperative consequences. With good mechanical bowel preparation plus antibiotic
RECTAL INJURY IN 27 UROLOGIC SURGERY Inadvertent rectal injury from a urologic procedure is often subtle but has serious postoperative consequences. With good mechanical bowel preparation plus antibiotic
Technique Guide. Bard MK Hernia Repair. Featuring Modified Onflex Mesh SOFT TISSUE REPAIR. Anterior Approach to a Preperitoneal Inguinal Hernia Repair
 Bard MK Hernia Repair Featuring Modified Onflex Mesh Technique Guide Anterior Approach to a Preperitoneal Inguinal Hernia Repair SOFT TISSUE REPAIR Right Procedure. Right Product. Right Outcome. The opinions
Bard MK Hernia Repair Featuring Modified Onflex Mesh Technique Guide Anterior Approach to a Preperitoneal Inguinal Hernia Repair SOFT TISSUE REPAIR Right Procedure. Right Product. Right Outcome. The opinions
Transfemoral Amputation
 Transfemoral Amputation Pre-Op: 42 year old male who sustained severe injuries in a motorcycle accident. Note: he is a previous renal transplant recipient and is on immunosuppressive treatments. His injuries
Transfemoral Amputation Pre-Op: 42 year old male who sustained severe injuries in a motorcycle accident. Note: he is a previous renal transplant recipient and is on immunosuppressive treatments. His injuries
Rectal Prolapse: A 10-Year Experience
 24 The Ochsner Journal Volume 7, Number 1, Spring 2007 25 Rectal Prolapse: A 10-Year Experience Figure 2. Physical examination. A. Concentric folds of prolapsed rectum. B. Radial folds of hemorrhoids (mucosal
24 The Ochsner Journal Volume 7, Number 1, Spring 2007 25 Rectal Prolapse: A 10-Year Experience Figure 2. Physical examination. A. Concentric folds of prolapsed rectum. B. Radial folds of hemorrhoids (mucosal
Summary and conclusion. Summary And Conclusion
 Summary And Conclusion Summary and conclusion Rectal prolapse remain a disorder for which no single ideal treatment was approved for all cases. Complete rectal prolapse (procidentia) is the circumferential
Summary And Conclusion Summary and conclusion Rectal prolapse remain a disorder for which no single ideal treatment was approved for all cases. Complete rectal prolapse (procidentia) is the circumferential
EPISIOTOMY & PERINEAL TEARS Anatomy &Functionality May Dr. Annie Leong MBBS, FRANZCOG, CU
 EPISIOTOMY & PERINEAL TEARS Anatomy &Functionality May 2011 Dr. Annie Leong MBBS, FRANZCOG, CU Restore normal perineal anatomy Achieve good haemostasis Avoid infection and wound breakdown Avoid coital
EPISIOTOMY & PERINEAL TEARS Anatomy &Functionality May 2011 Dr. Annie Leong MBBS, FRANZCOG, CU Restore normal perineal anatomy Achieve good haemostasis Avoid infection and wound breakdown Avoid coital
Index. Note: Page numbers of article title are in boldface type.
 Index Note: Page numbers of article title are in boldface type. A Abscess(es) in Crohn s disease, 168 169 IPAA and, 110 114 as unexpected finding in colorectal surgery, 46 Adhesion(s) trocars-related laparoscopy
Index Note: Page numbers of article title are in boldface type. A Abscess(es) in Crohn s disease, 168 169 IPAA and, 110 114 as unexpected finding in colorectal surgery, 46 Adhesion(s) trocars-related laparoscopy
Robotic Ventral Rectopexy
 Robotic Ventral Rectopexy What is a robotic ventral rectopexy? The term rectopexy refers to an operation in which the rectum (the part of the bowel nearest the anus) is put back into its normal position
Robotic Ventral Rectopexy What is a robotic ventral rectopexy? The term rectopexy refers to an operation in which the rectum (the part of the bowel nearest the anus) is put back into its normal position
8 A SIMPLE FISTULA REPAIR, STEP BY STEP
 8 A SIMPLE FISTULA REPAIR, STEP BY STEP The first step is to suture the labia to the thighs and cover the anus with a swab (Figure 31). Figure 31 The labia are sutured to the thighs and the anus is covered
8 A SIMPLE FISTULA REPAIR, STEP BY STEP The first step is to suture the labia to the thighs and cover the anus with a swab (Figure 31). Figure 31 The labia are sutured to the thighs and the anus is covered
INSTRUCTIONS FOR USE FOR:
 INSTRUCTIONS FOR USE FOR: en English INSTRUCTIONS FOR USE GORE ENFORM PREPERITONEAL BIOMATERIAL Carefully read all instructions prior to use. Observe all instructions, warnings, and precautions noted throughout.
INSTRUCTIONS FOR USE FOR: en English INSTRUCTIONS FOR USE GORE ENFORM PREPERITONEAL BIOMATERIAL Carefully read all instructions prior to use. Observe all instructions, warnings, and precautions noted throughout.
INGUINAL HERNIA REPAIR PROCEDURE GUIDE
 ROOM CONFIGURATION The following figure shows an overhead view of the recommended OR configuration for a da Vinci Inguinal Hernia Repair (Figure 1). NOTE: Configuration of the operating room suite is dependent
ROOM CONFIGURATION The following figure shows an overhead view of the recommended OR configuration for a da Vinci Inguinal Hernia Repair (Figure 1). NOTE: Configuration of the operating room suite is dependent
Transfemoral Amputation
 Transfemoral Amputation Preop This 26 year old male sustained a gunshot wound to the left thigh. He was treated emergently with revascularization and fasciotomies. He was transferred to our regional trauma
Transfemoral Amputation Preop This 26 year old male sustained a gunshot wound to the left thigh. He was treated emergently with revascularization and fasciotomies. He was transferred to our regional trauma
REINFORCED BIOSCAFFOLDS
 REINFORCED BIOSCAFFOLDS Midline Incisional Open OviTex 1S Resorbable Clinical Case Study: Open Abdomen Incisional Herniorrhaphy in Contaminated (CDC Class IV) Operative Field Performed by Dr. Michael Sawyer,
REINFORCED BIOSCAFFOLDS Midline Incisional Open OviTex 1S Resorbable Clinical Case Study: Open Abdomen Incisional Herniorrhaphy in Contaminated (CDC Class IV) Operative Field Performed by Dr. Michael Sawyer,
Anorectal malformations include a wide spectrum of
 JOURNAL OF LAPAROENDOSCOPIC & ADVANCED SURGICAL TECHNIQUES Volume 20, Number 1, 2010 ª Mary Ann Liebert, Inc. DOI: 10.1089=lap.2008.0343 Laparoscopic-Assisted Pull-Through for Congenital Rectal Stenosis
JOURNAL OF LAPAROENDOSCOPIC & ADVANCED SURGICAL TECHNIQUES Volume 20, Number 1, 2010 ª Mary Ann Liebert, Inc. DOI: 10.1089=lap.2008.0343 Laparoscopic-Assisted Pull-Through for Congenital Rectal Stenosis
Abdominal Wall Modification for the Difficult Ostomy
 Abdominal Wall Modification for the Difficult Ostomy David E. Beck, M.D. 1 ABSTRACT A select group of patients with major stomal problems may benefit from operative modification of the abdominal wall.
Abdominal Wall Modification for the Difficult Ostomy David E. Beck, M.D. 1 ABSTRACT A select group of patients with major stomal problems may benefit from operative modification of the abdominal wall.
Surgical Procedure in Guided Tissue Regeneration with the. Inion GTR Biodegradable Membrane System
 Surgical Procedure in Guided Tissue Regeneration with the Inion GTR Biodegradable Membrane System 1 Introduction This presentation familiarizes you with the basic steps how to use the Inion GTR membrane
Surgical Procedure in Guided Tissue Regeneration with the Inion GTR Biodegradable Membrane System 1 Introduction This presentation familiarizes you with the basic steps how to use the Inion GTR membrane
Desara TV and Desara Blue TV
 Desara TV and Desara Blue TV Sling for Female Stress Urinary Incontinence Instructions For Use D I Prescription Use only Do not reuse Sterilized using ethylene oxide Available Electronically M Manufactured
Desara TV and Desara Blue TV Sling for Female Stress Urinary Incontinence Instructions For Use D I Prescription Use only Do not reuse Sterilized using ethylene oxide Available Electronically M Manufactured
FIG The inferior and posterior peritoneal reflection is easily
 PSOAS HITCH, BOARI FLAP, AND COMBINATION OF PSOAS 7 HITCH AND BOARI FLAP The psoas hitch procedure, Boari flap, and transureteroureterostomy are useful operative procedures for reestablishing continuity
PSOAS HITCH, BOARI FLAP, AND COMBINATION OF PSOAS 7 HITCH AND BOARI FLAP The psoas hitch procedure, Boari flap, and transureteroureterostomy are useful operative procedures for reestablishing continuity
What the radiologist needs to know!
 What the radiologist needs to know! Clare Molyneux Sam Treadway Sathi Sukumar Wal Baraza Abhiram Sharma Karen Telford University Hospital of South Manchester Manchester UK Introduction Indications Investigations
What the radiologist needs to know! Clare Molyneux Sam Treadway Sathi Sukumar Wal Baraza Abhiram Sharma Karen Telford University Hospital of South Manchester Manchester UK Introduction Indications Investigations
Motility Disorders. Pelvic Floor. Colorectal Center for Functional Bowel Disorders (N = 701) January 2010 November 2011
 January 2010 November 2011") Motility Disorders Pelvic Floor Colorectal Center for Functional Bowel Disorders (N = 71) January 21 November 211 New Patients 35 3 25 2 15 1 5 Constipation Fecal Incontinence Rectal Prolapse Digestive-Genital
Motility Disorders Pelvic Floor Colorectal Center for Functional Bowel Disorders (N = 71) January 21 November 211 New Patients 35 3 25 2 15 1 5 Constipation Fecal Incontinence Rectal Prolapse Digestive-Genital
-primarily by apposition of the anterior rectus
 2 Component separation Cop HARVEY CHIM, KAREN KIM EVANS, AND SAMIR MARDINI Mater al Introduction 7 Preoperative markings 7 Intraoperative details 9 Technique modification: Component separation with preservation
2 Component separation Cop HARVEY CHIM, KAREN KIM EVANS, AND SAMIR MARDINI Mater al Introduction 7 Preoperative markings 7 Intraoperative details 9 Technique modification: Component separation with preservation
Colostomy & Ileostomy
 Colostomy & Ileostomy Indications, problems and preference By Waleed Omar Professor of Colorectal surgery, Mansoura University. Disclosure I have no disclosures. Presentation outline Stoma: Definition
Colostomy & Ileostomy Indications, problems and preference By Waleed Omar Professor of Colorectal surgery, Mansoura University. Disclosure I have no disclosures. Presentation outline Stoma: Definition
Early View Article: Online published version of an accepted article before publication in the final form.
 : Online published version of an accepted article before publication in the final form. Journal Name: Journal of Case Reports and Images in Surgery doi: To be assigned Early view version published: November
: Online published version of an accepted article before publication in the final form. Journal Name: Journal of Case Reports and Images in Surgery doi: To be assigned Early view version published: November
Approach to the Repair of Chronic Perineal Lacerations and Rectovaginal Fistula (RVF)
") Approach to the Repair of Chronic Perineal Lacerations and Rectovaginal Fistula (RVF) Blair B. Washington MD, MHA Urogynecology & Reconstructive Pelvic Surgery Virginia Mason Medical Center Disclosures
Approach to the Repair of Chronic Perineal Lacerations and Rectovaginal Fistula (RVF) Blair B. Washington MD, MHA Urogynecology & Reconstructive Pelvic Surgery Virginia Mason Medical Center Disclosures
Transabdominal pre peritoneal (TAPP) vs totally extraperitoneal (TEP) laparoscopic techniques for inguinal hernia repair
 vs totally extraperitoneal (TEP) laparoscopic techniques for inguinal hernia repair") Transabdominal pre peritoneal (TAPP) vs totally extraperitoneal (TEP) laparoscopic techniques for inguinal hernia repair An inguinal hernia (hernia of the groin) is a weakness in the wall of the abdominal
Transabdominal pre peritoneal (TAPP) vs totally extraperitoneal (TEP) laparoscopic techniques for inguinal hernia repair An inguinal hernia (hernia of the groin) is a weakness in the wall of the abdominal
Meniscus Reconstruction: Trough Surgical Technique
 Meniscus Reconstruction: Trough Surgical Technique Technique Consultant Jeffrey L. Halbrecht, M.D. San Francisco, CA ABOUT THE TROUGH TECHNIQUE The trough technique for meniscal allograft reconstruction
Meniscus Reconstruction: Trough Surgical Technique Technique Consultant Jeffrey L. Halbrecht, M.D. San Francisco, CA ABOUT THE TROUGH TECHNIQUE The trough technique for meniscal allograft reconstruction
The use of peritoneal flaps in the repair of large incisional hernia
 The use of peritoneal flaps in the repair of large incisional hernia Marc Huyghe MD GZA St Augustinus Hospital (Antwerp) Mesh 2017 - Paris Peritoneal flap in the repair of incisional hernia - definition
The use of peritoneal flaps in the repair of large incisional hernia Marc Huyghe MD GZA St Augustinus Hospital (Antwerp) Mesh 2017 - Paris Peritoneal flap in the repair of incisional hernia - definition
Desara and Desara Blue
 Desara and Desara Blue Sling for Female Stress Urinary Incontinence Instructions For Use D I Prescription Use only Do not reuse Sterilized using ethylene oxide M Manufactured by: Caldera Medical, Inc.
Desara and Desara Blue Sling for Female Stress Urinary Incontinence Instructions For Use D I Prescription Use only Do not reuse Sterilized using ethylene oxide M Manufactured by: Caldera Medical, Inc.
Stapled transanal rectal resection for obstructed defaecation syndrome
 Stapled transanal rectal resection for obstructed Issued: June 2010 www.nice.org.uk/ipg351 NHS Evidence has accredited the process used by the NICE Interventional Procedures Programme to produce interventional
Stapled transanal rectal resection for obstructed Issued: June 2010 www.nice.org.uk/ipg351 NHS Evidence has accredited the process used by the NICE Interventional Procedures Programme to produce interventional
This information is intended as an overview only
 This information is intended as an overview only Please refer to the INSTRUCTIONS FOR USE included with this device for indications, contraindications, warnings, precautions and other important information
This information is intended as an overview only Please refer to the INSTRUCTIONS FOR USE included with this device for indications, contraindications, warnings, precautions and other important information
Technique Guide. *smith&nephew N8TIVE ACL Anatomic ACL Reconstruction System
 Technique Guide *smith&nephew N8TIVE ACL Anatomic ACL Reconstruction System N8TIVE ACL System The N8TIVE ACL Anatomic Reconstruction System provides a novel and simple approach to ACL repair. The N8TIVE
Technique Guide *smith&nephew N8TIVE ACL Anatomic ACL Reconstruction System N8TIVE ACL System The N8TIVE ACL Anatomic Reconstruction System provides a novel and simple approach to ACL repair. The N8TIVE
Knee Disarticulation Amputation
 Knee Disarticulation Amputation Pre-Op 64 year old man, previous spinal cord injury, diabetes, renal failure, and a history of spasticity with dynamic knee flexion contracture. He had an open left ankle
Knee Disarticulation Amputation Pre-Op 64 year old man, previous spinal cord injury, diabetes, renal failure, and a history of spasticity with dynamic knee flexion contracture. He had an open left ankle
Laparoscopic Ventral. Mesh Rectopexy (LVMR)
") Laparoscopic Ventral Mesh Rectopexy (LVMR) Questions & Answers GLASGOW COLORECTAL CENTRE Ross Hall Hospital 221 Crookston Road Glasgow G52 3NQ e-mail: info@colorectalcentre.co.uk Ph: Main hospital switchboard
Laparoscopic Ventral Mesh Rectopexy (LVMR) Questions & Answers GLASGOW COLORECTAL CENTRE Ross Hall Hospital 221 Crookston Road Glasgow G52 3NQ e-mail: info@colorectalcentre.co.uk Ph: Main hospital switchboard
Surgical Technique. Achilles Tendon Repair Using Conexa Reconstructive Tissue Matrix. conexatm. Surgical Technique Described by Tom Chang, DPM
 Surgical Technique Achilles Tendon Repair Using Conexa Reconstructive Tissue Matrix Surgical Technique Described by Tom Chang, DPM conexatm r e c o n s t r u c t i v e t i s s u e m a t r i x Achilles
Surgical Technique Achilles Tendon Repair Using Conexa Reconstructive Tissue Matrix Surgical Technique Described by Tom Chang, DPM conexatm r e c o n s t r u c t i v e t i s s u e m a t r i x Achilles
Biodesign E NTEROCUTANEOUS FISTULA PLUG
 Offer a new alternative to patients who have enterocutaneous fistulas, even after standard treatments have been tried. Illustration by Lisa Clark Biodesign E NTEROCUTANEOUS FISTULA PLUG MEDICAL How is
Offer a new alternative to patients who have enterocutaneous fistulas, even after standard treatments have been tried. Illustration by Lisa Clark Biodesign E NTEROCUTANEOUS FISTULA PLUG MEDICAL How is
Breast Reconstruction Postmastectomy. Using DermaMatrix Acellular Dermis in breast reconstruction with tissue expander.
 Breast Reconstruction Postmastectomy. Using DermaMatrix Acellular Dermis in breast reconstruction with tissue expander. Strong and flexible Bacterially inactivated Provides implant support Breast Reconstruction
Breast Reconstruction Postmastectomy. Using DermaMatrix Acellular Dermis in breast reconstruction with tissue expander. Strong and flexible Bacterially inactivated Provides implant support Breast Reconstruction
Inguinal and Femoral Hernias. August 10, 2016 Basic Science Lecture Department of Surgery University of Tennessee Health Science Center
 Inguinal and Femoral Hernias August 10, 2016 Basic Science Lecture Department of Surgery University of Tennessee Health Science Center Background Approximately 20 million groin hernias are repaired each
Inguinal and Femoral Hernias August 10, 2016 Basic Science Lecture Department of Surgery University of Tennessee Health Science Center Background Approximately 20 million groin hernias are repaired each
STOMA SITING & PARASTOMAL HERNIA MANAGEMENT
 STOMA SITING & PARASTOMAL HERNIA MANAGEMENT Professor Hany S. Tawfik Head of the Department of Surgery & Chairman of Colorectal Surgery Unit Benha University Disclosure No financial affiliation to disclose
STOMA SITING & PARASTOMAL HERNIA MANAGEMENT Professor Hany S. Tawfik Head of the Department of Surgery & Chairman of Colorectal Surgery Unit Benha University Disclosure No financial affiliation to disclose
Ultrapro Hernia System Bi Layer Dr Cosmas Gora T SpB-KBD. dffdfdfxxgfxgfxgffxgxgxg
 Bi Layer Dr Cosmas Gora T SpB-KBD dffdfdfxxgfxgfxgffxgxgxg Why UHS? Lightweight Mesh Covering entire myopectineal orifices with underlay mesh in preperitoneal space (posterior repair) Covering the inguinal
Bi Layer Dr Cosmas Gora T SpB-KBD dffdfdfxxgfxgfxgffxgxgxg Why UHS? Lightweight Mesh Covering entire myopectineal orifices with underlay mesh in preperitoneal space (posterior repair) Covering the inguinal
Anorectal Anomalies CHAPTER 27. Alberto Peña, Marc A. Levitt INTRODUCTION
 CHAPTER 27 Anorectal Anomalies INTRODUCTION Anorectal malformations, represent a wide spectrum of defects. Surgical techniques useful to repair the most common types of anorectal malformations seen by
CHAPTER 27 Anorectal Anomalies INTRODUCTION Anorectal malformations, represent a wide spectrum of defects. Surgical techniques useful to repair the most common types of anorectal malformations seen by
The Emergency Hernia or The call you don t want at 2:00 a.m.*
 or The call you don t want at 2:00 a.m.* *Or even at 8:00 a.m. Michael G. Sarr, MD Professor of Surgery Mayo Clinic South Canada WEST CANADA EAST CANADA Clinical talk Hernias Inguinal Umbilical Incisional
or The call you don t want at 2:00 a.m.* *Or even at 8:00 a.m. Michael G. Sarr, MD Professor of Surgery Mayo Clinic South Canada WEST CANADA EAST CANADA Clinical talk Hernias Inguinal Umbilical Incisional
CASE REPORT An Innovative Solution to Complex Inguinal Defect: Deepithelialized SIEA Flap With Mini Abdominoplasty
 CASE REPORT An Innovative Solution to Complex Inguinal Defect: Deepithelialized SIEA Flap With Mini Abdominoplasty Augustine Reid Wilson, MS, Justin Daggett, MD, Michael Harrington, MD, MPH, and Deniz
CASE REPORT An Innovative Solution to Complex Inguinal Defect: Deepithelialized SIEA Flap With Mini Abdominoplasty Augustine Reid Wilson, MS, Justin Daggett, MD, Michael Harrington, MD, MPH, and Deniz
ABSITE Review: Hernias
 ABSITE Review: Inguinal and Femoral Hernias Sybile Val M.D. SUNY Downstate Medical Center Department of Surgery June 27, 2008 Objectives www.downstatesurgery.org Correctly identify anatomical landmarks
ABSITE Review: Inguinal and Femoral Hernias Sybile Val M.D. SUNY Downstate Medical Center Department of Surgery June 27, 2008 Objectives www.downstatesurgery.org Correctly identify anatomical landmarks
Laparoscopic Resection Of Colon & Rectal Cancers. R Sim Centre for Advanced Laparoscopic Surgery, TTSH
 Laparoscopic Resection Of Colon & Rectal Cancers R Sim Centre for Advanced Laparoscopic Surgery, TTSH Feasibility and safety Adequacy - same radical surgery as open op. Efficacy short term benefits and
Laparoscopic Resection Of Colon & Rectal Cancers R Sim Centre for Advanced Laparoscopic Surgery, TTSH Feasibility and safety Adequacy - same radical surgery as open op. Efficacy short term benefits and
Surgical Management of IBD in the Age of Biologics
 Surgical Management of IBD in the Age of Biologics Lisa S. Poritz, M.D Associate Professor of Surgery Division of Colon and Rectal Surgery Objectives Discuss surgical management of IBD When to operate
Surgical Management of IBD in the Age of Biologics Lisa S. Poritz, M.D Associate Professor of Surgery Division of Colon and Rectal Surgery Objectives Discuss surgical management of IBD When to operate
Strattice Reconstructive Tissue Matrix used in the repair of rippling
 Clinical case study Strattice Tissue Matrix Strattice Reconstructive Tissue Matrix used in the repair of rippling Steven Teitelbaum, MD* Santa Monica, CA Case summary A 48-year-old woman with a history
Clinical case study Strattice Tissue Matrix Strattice Reconstructive Tissue Matrix used in the repair of rippling Steven Teitelbaum, MD* Santa Monica, CA Case summary A 48-year-old woman with a history
Postoperative Care for Pelvic Fistulae. Peter Jeppson, MD October 3, 2017
 Postoperative Care for Pelvic Fistulae Peter Jeppson, MD October 3, 2017 No Disclosures Rational for Postoperative Care Intraoperative injury may be managed by: Identification Closure Continuous post-operative
Postoperative Care for Pelvic Fistulae Peter Jeppson, MD October 3, 2017 No Disclosures Rational for Postoperative Care Intraoperative injury may be managed by: Identification Closure Continuous post-operative
Postoperative Surgical Site Infection after Incisional Hernia Repair: Link to Previous Surgical Site Infection? Zulfiqar Ali, AG Rehan
 Original Article Postoperative Surgical Site Infection after Incisional Hernia Repair: Link to Previous Surgical Site Infection? Zulfiqar Ali, AG Rehan ABSTRACT Objective: Aim of the study was to determine
Original Article Postoperative Surgical Site Infection after Incisional Hernia Repair: Link to Previous Surgical Site Infection? Zulfiqar Ali, AG Rehan ABSTRACT Objective: Aim of the study was to determine
BICEPTOR Tenodesis System
 BICEPTOR Tenodesis System Sub-Pectoral Biceps Tenodesis A Shoulder Series Technique Guide As described by: Nikhil N. Verma, MD As described by: Nikhil N. Verma, MD Midwest Orthopedics at Rush Chicago,
BICEPTOR Tenodesis System Sub-Pectoral Biceps Tenodesis A Shoulder Series Technique Guide As described by: Nikhil N. Verma, MD As described by: Nikhil N. Verma, MD Midwest Orthopedics at Rush Chicago,
JuggerKnot Soft Anchor 1.0 mm Mini. Scapholunate Ligament Repair/Reconstruction. Brochure and Surgical Technique
 JuggerKnot Soft Anchor 1.0 mm Mini Scapholunate Ligament Repair/Reconstruction Brochure and Surgical Technique One Surgeon. One Patient. Over 1 million times per year, Biomet helps one surgeon provide
JuggerKnot Soft Anchor 1.0 mm Mini Scapholunate Ligament Repair/Reconstruction Brochure and Surgical Technique One Surgeon. One Patient. Over 1 million times per year, Biomet helps one surgeon provide
6 THE OPERATIONS BASIC PRINCIPLES
 6 THE OPERATIONS BASIC PRINCIPLES Basic principles are described here; strategies for specific situations are discussed in later sections. The basic principles in the repair of a fistula are: adequate
6 THE OPERATIONS BASIC PRINCIPLES Basic principles are described here; strategies for specific situations are discussed in later sections. The basic principles in the repair of a fistula are: adequate
Pelvic Floor Disorders. Amir Darakhshan MD FRCS (Gen Surg) Consultant Colorectal and General Surgeon
 Consultant Colorectal and General Surgeon") Pelvic Floor Disorders Amir Darakhshan MD FRCS (Gen Surg) Consultant Colorectal and General Surgeon What is Pelvic Floor Disorder Surgical perspective symptoms of RED, FI or prolapse on the background
Pelvic Floor Disorders Amir Darakhshan MD FRCS (Gen Surg) Consultant Colorectal and General Surgeon What is Pelvic Floor Disorder Surgical perspective symptoms of RED, FI or prolapse on the background
Staging of rectal cancer on MRI: What the surgeons want to know.
 Staging of rectal cancer on MRI: What the surgeons want to know. Poster No.: C-1108 Congress: ECR 2014 Type: Educational Exhibit Authors: G. Ayub, R. Chittal, A. Lowe, A. S. Punekar ; Leeds/, 1 2 1 2 2
Staging of rectal cancer on MRI: What the surgeons want to know. Poster No.: C-1108 Congress: ECR 2014 Type: Educational Exhibit Authors: G. Ayub, R. Chittal, A. Lowe, A. S. Punekar ; Leeds/, 1 2 1 2 2
MOVE BEYOND. to new hope for enterocutaneous fistulas. Enterocutaneous Fistula Repair
 MOVE BEYOND to new hope for enterocutaneous fistulas. Enterocutaneous Fistula Repair to an alternative treatment option Enterocutaneous fistulas can significantly affect patient health and quality of life.
MOVE BEYOND to new hope for enterocutaneous fistulas. Enterocutaneous Fistula Repair to an alternative treatment option Enterocutaneous fistulas can significantly affect patient health and quality of life.
NEW DEFINITION FORMAT AND DIFFICULT VARIABLE DEFINITIONS
 NEW DEFINITION FORMAT AND DIFFICULT VARIABLE DEFINITIONS Bruce L. Hall, MD, PhD, MBA, FACS Clinical Support Physician Lead Paula Farrell, RN, BSN ACS NSQIP Clinical Support Specialist Case Studies &
NEW DEFINITION FORMAT AND DIFFICULT VARIABLE DEFINITIONS Bruce L. Hall, MD, PhD, MBA, FACS Clinical Support Physician Lead Paula Farrell, RN, BSN ACS NSQIP Clinical Support Specialist Case Studies &
University College Hospital. Laparoscopic colorectal surgery. Gastrointestinal Services Division
 University College Hospital Laparoscopic colorectal surgery Gastrointestinal Services Division 2 Colon 3 If you would like a large print, audio or translated version of this document contact us on 0845
University College Hospital Laparoscopic colorectal surgery Gastrointestinal Services Division 2 Colon 3 If you would like a large print, audio or translated version of this document contact us on 0845
Surgical Atlas Orthotopic ileal neobladder
 Surgery Illustrated ORTHOTOPIC ILEAL NEOBLADDER U.E. STUDER ET AL. Surgical Atlas Orthotopic ileal neobladder U.E. STUDER, C. VAROL and H. DANUSER University of Bern, Department of Urology, Bern, Switzerland
Surgery Illustrated ORTHOTOPIC ILEAL NEOBLADDER U.E. STUDER ET AL. Surgical Atlas Orthotopic ileal neobladder U.E. STUDER, C. VAROL and H. DANUSER University of Bern, Department of Urology, Bern, Switzerland
Pelvic Prolapse. A Patient Guide to Pelvic Floor Reconstruction
 Pelvic Prolapse A Patient Guide to Pelvic Floor Reconstruction Pelvic Prolapse When an organ becomes displaced, or slips down in the body, it is referred to as a prolapse. Your physician has diagnosed
Pelvic Prolapse A Patient Guide to Pelvic Floor Reconstruction Pelvic Prolapse When an organ becomes displaced, or slips down in the body, it is referred to as a prolapse. Your physician has diagnosed
Posterior Deep Endometriosis. What is the best approach? Posterior Deep Endometriosis. Should we perform a routine excision of the vagina??
 Posterior Deep Endometriosis What is the best approach? Dept Gyn Obst Polyclinique Hotel Dieu CHU Clermont Ferrand France Posterior Deep Endometriosis Organs involved - Peritoneum - Uterine cervix -Rectum
Posterior Deep Endometriosis What is the best approach? Dept Gyn Obst Polyclinique Hotel Dieu CHU Clermont Ferrand France Posterior Deep Endometriosis Organs involved - Peritoneum - Uterine cervix -Rectum
CHAU KHAC TU M.D., Ph.D.
 CHAU KHAC TU M.D., Ph.D. Hue Central Hospital Vietnam LAPAROSCOPIC PROMONTOFIXATION FOR THE GENITAL PROLAPSE TREATMENT Chau Khac Tu MD.PhD. Hue central hospital CONTENT 3 1 INTRODUCTION 2 OBJECTIVE AND
CHAU KHAC TU M.D., Ph.D. Hue Central Hospital Vietnam LAPAROSCOPIC PROMONTOFIXATION FOR THE GENITAL PROLAPSE TREATMENT Chau Khac Tu MD.PhD. Hue central hospital CONTENT 3 1 INTRODUCTION 2 OBJECTIVE AND
Decision-Making in the Acute Management of Blunt and Penetrating Wounds Mary Somerville, DVM, DACVS
 Decision-Making in the Acute Management of Blunt and Penetrating Wounds Mary Somerville, DVM, DACVS Providing the best quality care and service for the patient, the client, and the referring veterinarian.
Decision-Making in the Acute Management of Blunt and Penetrating Wounds Mary Somerville, DVM, DACVS Providing the best quality care and service for the patient, the client, and the referring veterinarian.
Modified Brostrom-Gould Technique
 Surgical Technique Modified Brostrom-Gould Technique Modified Brostrom-Gould Technique for Lateral Ankle Ligament Reconstruction Modified Brostrom-Gould Technique for Lateral Ankle Ligament Reconstruction
Surgical Technique Modified Brostrom-Gould Technique Modified Brostrom-Gould Technique for Lateral Ankle Ligament Reconstruction Modified Brostrom-Gould Technique for Lateral Ankle Ligament Reconstruction
Laparoscopic Sacrocolpopexy with & without the Robot: Tips and Tricks for success and avoidance / management of complications
 Laparoscopic Sacrocolpopexy with & without the Robot: Tips and Tricks for success and avoidance / management of complications Course Faculty: Patrick Culligan, MD Peter Rosenblatt, MD What is a Sacrocolpopexy?
Laparoscopic Sacrocolpopexy with & without the Robot: Tips and Tricks for success and avoidance / management of complications Course Faculty: Patrick Culligan, MD Peter Rosenblatt, MD What is a Sacrocolpopexy?
Stop Coping. Start Living. Talk to your doctor about pelvic organ prolapse and sacrocolpopexy
 Stop Coping. Start Living Talk to your doctor about pelvic organ prolapse and sacrocolpopexy Did you know? One in three women will suffer from a pelvic health condition in her lifetime. Four of the most
Stop Coping. Start Living Talk to your doctor about pelvic organ prolapse and sacrocolpopexy Did you know? One in three women will suffer from a pelvic health condition in her lifetime. Four of the most
THE BEST OF TISSUE REGENERATION FOCUSED ON PATIENTS NEEDS
 THE BEST OF TISSUE REGENERATION FOCUSED ON PATIENTS NEEDS Tissue regeneration is a natural process by which the body forms a functional neo-tissue to repair a wound. This process requires the patient s
THE BEST OF TISSUE REGENERATION FOCUSED ON PATIENTS NEEDS Tissue regeneration is a natural process by which the body forms a functional neo-tissue to repair a wound. This process requires the patient s
Anus,Rectum and Colon
 JOURNAL OF THE Anus,Rectum and Colon http://journal-arc.jp CLINICAL RESEARCH Laparoscopic ventral rectopexy with sacrocolpopexy for coexisting pelvic organ prolapse and external rectal prolapse Yoshiyuki
JOURNAL OF THE Anus,Rectum and Colon http://journal-arc.jp CLINICAL RESEARCH Laparoscopic ventral rectopexy with sacrocolpopexy for coexisting pelvic organ prolapse and external rectal prolapse Yoshiyuki
INCISIONAL HERNIAS. Contents What is an Incisional Hernia?... 3
 Contents What is an Incisional Hernia?................... 3 When can I return to normal activities?....... 6 YOUR GUIDE TO INCISIONAL HERNIAS An IPRS Guide to provide you with exercises and advice to ease
Contents What is an Incisional Hernia?................... 3 When can I return to normal activities?....... 6 YOUR GUIDE TO INCISIONAL HERNIAS An IPRS Guide to provide you with exercises and advice to ease
7/2/2015. Incidence. *Mudge M et al, Br. J. Surg, 1985, 72:70-71
 Ventral Hernia Repair: Revisonal Surgery Natan Zundel MD FACS Professor of Surgery Vice-Chairman Department of Surgery FIU Herbert Wertheim College of Medicine. Miami Florida DISCLOSURE Ethicon Endosurgery
Ventral Hernia Repair: Revisonal Surgery Natan Zundel MD FACS Professor of Surgery Vice-Chairman Department of Surgery FIU Herbert Wertheim College of Medicine. Miami Florida DISCLOSURE Ethicon Endosurgery
Discharge information for patients Fistula plug for anal fistula
 Discharge information for patients Fistula plug for anal fistula Clinical Sciences Building Colorectal Surgery 0161 206 1249 All Rights Reserved 2017. Document for issue as handout.. What is an anal fistula?
Discharge information for patients Fistula plug for anal fistula Clinical Sciences Building Colorectal Surgery 0161 206 1249 All Rights Reserved 2017. Document for issue as handout.. What is an anal fistula?
EndoFast Reliant System vs. Tension- free Mesh in a Sheep Model; three arm Comparative Study Assessing the Mechanical Pullout Force of Mesh Over Time
 EndoFast Reliant System vs. Tension- free Mesh in a Sheep Model; three arm Comparative Study Assessing the Mechanical Pullout Force of Mesh Over Time Menachem Alcalay,M.D, Urogynecology unit, Sheba Medical
EndoFast Reliant System vs. Tension- free Mesh in a Sheep Model; three arm Comparative Study Assessing the Mechanical Pullout Force of Mesh Over Time Menachem Alcalay,M.D, Urogynecology unit, Sheba Medical
Absorbable Woven Polyglycolic Acid Mesh Tube (Absorbable Nerve Conduit Tube) INSTRUCTIONS FOR USE 2 6
 INSTRUCTIONS FOR USE 2 6") Absorbable Woven Polyglycolic Acid Mesh Tube (Absorbable Nerve Conduit Tube) INSTRUCTIONS FOR USE 2 6 1 0086 SYMBOL DEFINITIONS ENGLISH Do not Reuse Consult Instructions For Use Ethylene Oxide Sterilized
Absorbable Woven Polyglycolic Acid Mesh Tube (Absorbable Nerve Conduit Tube) INSTRUCTIONS FOR USE 2 6 1 0086 SYMBOL DEFINITIONS ENGLISH Do not Reuse Consult Instructions For Use Ethylene Oxide Sterilized
Rectal Cancer. About the Colon and Rectum. Symptoms. Colorectal Cancer Screening
 Patient information regarding care and surgery associated with RECTAL CANCER by Robert K. Cleary, M.D., John C. Eggenberger, M.D., Amalia J. Stefanou., M.D. location: Michigan Heart and Vascular Institute,
Patient information regarding care and surgery associated with RECTAL CANCER by Robert K. Cleary, M.D., John C. Eggenberger, M.D., Amalia J. Stefanou., M.D. location: Michigan Heart and Vascular Institute,
TRANSANAL ACCESS PLATFORM
 TRANSANAL ACCESS PLATFORM PROCEDURAL GUIDE FOR TRANSANAL MINIMALLY INVASIVE SURGERY (TAMIS) Featuring Tips & Tricks from Dr. Matthew Albert, Florida Hospital TAMIS is designed to resect benign polyps and
TRANSANAL ACCESS PLATFORM PROCEDURAL GUIDE FOR TRANSANAL MINIMALLY INVASIVE SURGERY (TAMIS) Featuring Tips & Tricks from Dr. Matthew Albert, Florida Hospital TAMIS is designed to resect benign polyps and
Educational Training Document
 Educational Training Document Table of Contents Part 1: Resource Document Disclaimer Page: 2 Part 2: Line Item Grade Sheets Page: 3 Release: 11/2016 Page 1 of 6 Part 1: Resource Document Disclaimer The
Educational Training Document Table of Contents Part 1: Resource Document Disclaimer Page: 2 Part 2: Line Item Grade Sheets Page: 3 Release: 11/2016 Page 1 of 6 Part 1: Resource Document Disclaimer The
Posterior leaflet prolapse is the most common lesion seen
 Techniques for Repairing Posterior Leaflet Prolapse of the Mitral Valve Robin Varghese, MD, MS, and David H. Adams, MD Posterior leaflet prolapse is the most common lesion seen in degenerative mitral valve
Techniques for Repairing Posterior Leaflet Prolapse of the Mitral Valve Robin Varghese, MD, MS, and David H. Adams, MD Posterior leaflet prolapse is the most common lesion seen in degenerative mitral valve
Wound Repair. Epidemiology. History. Location of Injuries Face/Scalp Extremities. Legal Risk Missed FB and Fx Infection
 Wound Repair Edwin W. Schaefer, DNP, R.N. - FNP Emergency Nurse Practitioner Epidemiology Location of Injuries Face/Scalp Extremities Legal Risk Missed FB and Fx Infection History Mechanism of Injury Associated
Wound Repair Edwin W. Schaefer, DNP, R.N. - FNP Emergency Nurse Practitioner Epidemiology Location of Injuries Face/Scalp Extremities Legal Risk Missed FB and Fx Infection History Mechanism of Injury Associated
Breast debridement and closure cpt
 Breast debridement and closure cpt Close Breast debridement cpt code Medicare Billing Guidelines, Medicare payment and reimbursment, Medicare codes. Here is a list of CPT codes and Diagnoses that are.
Breast debridement and closure cpt Close Breast debridement cpt code Medicare Billing Guidelines, Medicare payment and reimbursment, Medicare codes. Here is a list of CPT codes and Diagnoses that are.
Meshes. Meshes. Non-absorbable meshes. Absorbable meshes
 Meshes Meshes Non-absorbable meshes Absorbable meshes Non-absorbable meshes hernia Premilene Mesh Premilene Mesh Plug Optilene Mesh Optilene Mesh LP Optilene Mesh Elastic Omyra Mesh Non-absorbable meshes
Meshes Meshes Non-absorbable meshes Absorbable meshes Non-absorbable meshes hernia Premilene Mesh Premilene Mesh Plug Optilene Mesh Optilene Mesh LP Optilene Mesh Elastic Omyra Mesh Non-absorbable meshes
Technique Guide. VersiTomic. ReelX STT Double-Row Achilles G-Lok. J. Martin Leland III, M.D. J. Martin Leland III, M.D. Proximal Biceps Tenodesis
 Technique Guide VersiTomic ReelX STT Double-Row Achilles G-Lok Tendon Sub-Pectoral Repair Proximal Biceps Tenodesis J. Martin Leland III, M.D. J. Martin Leland III, M.D. The opinions expressed are those
Technique Guide VersiTomic ReelX STT Double-Row Achilles G-Lok Tendon Sub-Pectoral Repair Proximal Biceps Tenodesis J. Martin Leland III, M.D. J. Martin Leland III, M.D. The opinions expressed are those
One hundred percent fascial approximation with sequential abdominal closure of the open abdomen
 The American Journal of Surgery 192 (2006) 238 242 HowIdoit One hundred percent fascial approximation with sequential abdominal closure of the open abdomen C. Clay Cothren, M.D. a,b, *, Ernest E. Moore,
The American Journal of Surgery 192 (2006) 238 242 HowIdoit One hundred percent fascial approximation with sequential abdominal closure of the open abdomen C. Clay Cothren, M.D. a,b, *, Ernest E. Moore,
CableFIX Xpress Carpometacarpal Fixation System. Operative technique
 CableFIX Xpress Carpometacarpal Fixation System Operative technique CableFIX Xpress Carpometacarpal Fixation System CableFIX Xpress Carpometacarpal Fixation System Contents 1. Indications and contraindications...
CableFIX Xpress Carpometacarpal Fixation System Operative technique CableFIX Xpress Carpometacarpal Fixation System CableFIX Xpress Carpometacarpal Fixation System Contents 1. Indications and contraindications...
Breast conservation surgery and sentinal node biopsy: Dr R Botha Moderator: Dr E Osman
 Breast conservation surgery and sentinal node biopsy: Dr R Botha Moderator: Dr E Osman Breast anatomy: Breast conserving surgery: The aim of wide local excision is to remove all invasive and in situ
Breast conservation surgery and sentinal node biopsy: Dr R Botha Moderator: Dr E Osman Breast anatomy: Breast conserving surgery: The aim of wide local excision is to remove all invasive and in situ
Name of Policy: Plugs for Fistula Repair
 Name of Policy: Plugs for Fistula Repair Policy #: 399 Latest Review Date: November 2013 Category: Surgical Policy Grade: A Background/Definitions: As a general rule, benefits are payable under Blue Cross
Name of Policy: Plugs for Fistula Repair Policy #: 399 Latest Review Date: November 2013 Category: Surgical Policy Grade: A Background/Definitions: As a general rule, benefits are payable under Blue Cross
(FIG.1) Landmarks of the external ear in dogs. (FIG.2) Anatomy of the ear.
 Landmarks of the external ear in dogs. (FIG.2) Anatomy of the ear.") SURGICAL ANATOMY of Ear (FIG.1) Landmarks of the external ear in dogs. (FIG.2) Anatomy of the ear. An aural (auricular) hematoma is a collection of blood within the cartilage plate of the ear. Suture placement
SURGICAL ANATOMY of Ear (FIG.1) Landmarks of the external ear in dogs. (FIG.2) Anatomy of the ear. An aural (auricular) hematoma is a collection of blood within the cartilage plate of the ear. Suture placement
To inject, to band or to excise? These were the alternatives for a colorectal surgeon
 CHAPTER 2 Hemorrhoids To inject, to band or to excise? These were the alternatives for a colorectal surgeon some 50 years ago, when sclerosant injection, rubber band ligation and hemorrhoidectomy were
CHAPTER 2 Hemorrhoids To inject, to band or to excise? These were the alternatives for a colorectal surgeon some 50 years ago, when sclerosant injection, rubber band ligation and hemorrhoidectomy were
7% - 15% Single Tunnel Repair of Plantar Plate. Savings of. are common with EcoSMART *Patent Pending
 * Provide Value Sterile kit packaging provides high quality, surgical grade instruments and implants making your O.R. more efficient. No hassles or expense from cleaning, storing, sterilizing, and maintaining
* Provide Value Sterile kit packaging provides high quality, surgical grade instruments and implants making your O.R. more efficient. No hassles or expense from cleaning, storing, sterilizing, and maintaining
QuadsTape System TM. For Quadriceps Tendon Reconstruction. Surgical Technique Manual
 QuadsTape System TM For Quadriceps Tendon Reconstruction Surgical Technique Manual 0086 Introduction QuadsTape System TM The QuadsTape System comprises a wide open weave Poly-Tape prosthesis with associated
QuadsTape System TM For Quadriceps Tendon Reconstruction Surgical Technique Manual 0086 Introduction QuadsTape System TM The QuadsTape System comprises a wide open weave Poly-Tape prosthesis with associated
Urogenital Surgery in the Horse Brett Woodie, DVM, MS, DACVS Rood & Riddle Equine Hospital, Lexington, KY, USA Rupture or tearing of the uterus
 Urogenital Surgery in the Horse Brett Woodie, DVM, MS, DACVS Rood & Riddle Equine Hospital, Lexington, KY, USA Rupture or tearing of the uterus occurs most commonly at foaling. It is thought that dystocias
Urogenital Surgery in the Horse Brett Woodie, DVM, MS, DACVS Rood & Riddle Equine Hospital, Lexington, KY, USA Rupture or tearing of the uterus occurs most commonly at foaling. It is thought that dystocias
MULTIFIX S Knotless Implants
 Technique Guide MULTIFIX S Knotless Implants The MULTIFIX S system offers 5.5mm and 6.5mm knotless, all-peek, poundin implants. The system provides multiple fixation options, a streamlined technique, and
Technique Guide MULTIFIX S Knotless Implants The MULTIFIX S system offers 5.5mm and 6.5mm knotless, all-peek, poundin implants. The system provides multiple fixation options, a streamlined technique, and
Peritoneal Dialysis Catheter Placement. Peritoneal Dialysis Catheter Placement. Peritoneal Dialysis Catheter Placement
 ASDIN Advanced Techniques Pre-course Feb. 24, 2012 New Orleans, La Randall L. Rasmussen, MD Special thank you to Drs. Rajeev Narayan, San Antonio, Tx and Hemant Dhingra, Fresno Ca for lending me slides
ASDIN Advanced Techniques Pre-course Feb. 24, 2012 New Orleans, La Randall L. Rasmussen, MD Special thank you to Drs. Rajeev Narayan, San Antonio, Tx and Hemant Dhingra, Fresno Ca for lending me slides
Desara Blue OV D I. Sling for Female Stress Urinary Incontinence. Instructions For Use
 Desara Blue OV Sling for Female Stress Urinary Incontinence Instructions For Use D I Prescription Use only Do not reuse Sterilized using ethylene oxide M Manufactured by: Caldera Medical, Inc. 5171 Clareton
Desara Blue OV Sling for Female Stress Urinary Incontinence Instructions For Use D I Prescription Use only Do not reuse Sterilized using ethylene oxide M Manufactured by: Caldera Medical, Inc. 5171 Clareton
TissueMend. Arthroscopic Surgical Technique. Arthroscopic Insertion of a Biologic Rotator Cuff Tissue Augment After Rotator Cuff Repair
 TissueMend Arthroscopic Surgical Technique Arthroscopic Insertion of a Biologic Rotator Cuff Tissue Augment After Rotator Cuff Repair Table of Contents Placement of suture anchors Placement of anteromedial
TissueMend Arthroscopic Surgical Technique Arthroscopic Insertion of a Biologic Rotator Cuff Tissue Augment After Rotator Cuff Repair Table of Contents Placement of suture anchors Placement of anteromedial
Surgical management of the undescended testis is performed
 Undescended Testes/Orchiopexy James C.Y. Dunn, MD, PhD, 1 Akemi L. Kawaguchi, MD, 2 and Eric W. Fonkalsrud, MD 1 Surgical management of the undescended testis is performed to prevent the potential complications
Undescended Testes/Orchiopexy James C.Y. Dunn, MD, PhD, 1 Akemi L. Kawaguchi, MD, 2 and Eric W. Fonkalsrud, MD 1 Surgical management of the undescended testis is performed to prevent the potential complications
Bard CapSure. Technique Guide. Permanent Fixation System SOFT TISSUE REPAIR. Laparoscopic Inguinal, Open and Laparoscopic Ventral Hernia Repair
 Bard CapSure Permanent Fixation System Technique Guide Laparoscopic Inguinal, Open and Laparoscopic Ventral Hernia Repair SOFT TISSUE REPAIR Right Procedure. Right Product. Right Outcome. The opinions
Bard CapSure Permanent Fixation System Technique Guide Laparoscopic Inguinal, Open and Laparoscopic Ventral Hernia Repair SOFT TISSUE REPAIR Right Procedure. Right Product. Right Outcome. The opinions
SOP: Urinary Catheter in Dogs and Cats
 SOP: Urinary Catheter in Dogs and Cats These SOPs were developed by the Office of the University Veterinarian and reviewed by Virginia Tech IACUC to provide a reference and guidance to investigators during
SOP: Urinary Catheter in Dogs and Cats These SOPs were developed by the Office of the University Veterinarian and reviewed by Virginia Tech IACUC to provide a reference and guidance to investigators during
REPAIR OF LARGE CYSTOCELE
 REPAIR OF LARGE CYSTOCELE WITH RAZ SUSPENSION 17 VAGINAL INCISION AND DISSECTION Premarin cream application to the anterior vagina daily for 1 month before cystocele repair enriches the vasculature and
REPAIR OF LARGE CYSTOCELE WITH RAZ SUSPENSION 17 VAGINAL INCISION AND DISSECTION Premarin cream application to the anterior vagina daily for 1 month before cystocele repair enriches the vasculature and