Prolapse and Urogynae. By Sarah Rangan & Daniel Warrell
|
|
|
- Amy Taylor
- 5 years ago
- Views:
Transcription
1 Prolapse and Urogynae By Sarah Rangan & Daniel Warrell

2 Anatomy and physiology of the pelvic supports The pelvic floor supports the pelvic viscera and vaginal, urethral and rectal openings Endopelvic fascial attachments support the vagina at three levels Level 1: cardinal and uterosacral ligaments support the cervix and upper third of vagina Level 2: mid vagina is attached to the pelvic sidewalls via the endopelvic fascia Level 3: lower third of the vagina is supported by the levator ani and perineal body
 Enterocoele : upper posterior wall of vagina or pouch of Douglas (can contain loops of bowel) Rectocoele : lower posterior wall")
3 Types of Prolapse Prolapse is classified anatomically Urethrocoele : lower anterior vaginal wall involving urethra Cystocoele : upper anterior vaginal wall involving bladder and often urethra Apical Prolapse : uterus, cervix and upper vagina (or vault if uterus removed) Enterocoele : upper posterior wall of vagina or pouch of Douglas (can contain loops of bowel) Rectocoele : lower posterior wall of vagina involving rectum
 scoring system Conditions of measurement must be specified : position, rest/straining,")
4 Grading Of prolapse Most widely achieved by the ICS s (International Continent Society) Pelvic Organ Prolapse (POP) scoring system Conditions of measurement must be specified : position, rest/straining, traction
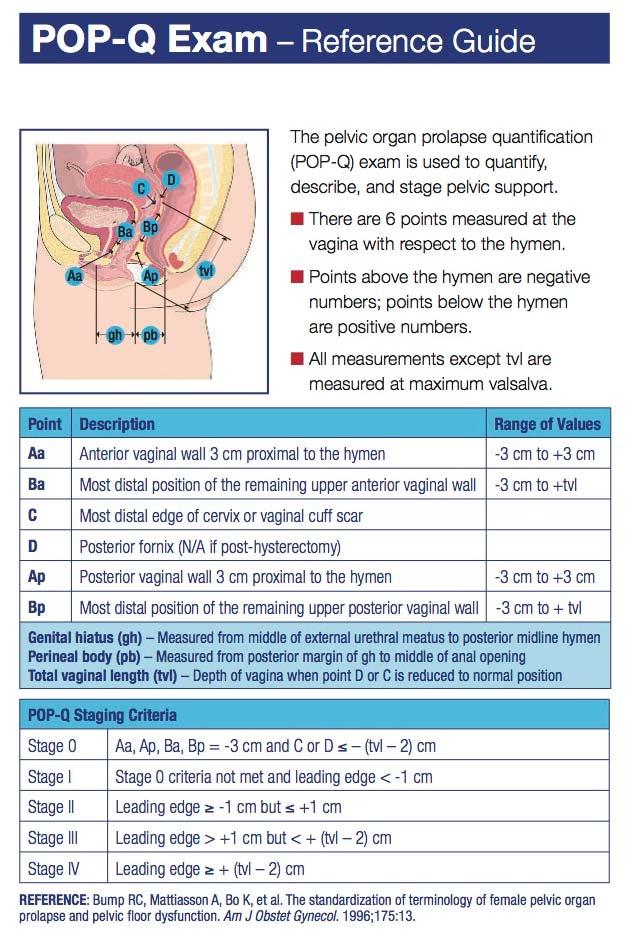
5
6 Aetiology of prolapse Up to half of parous women have some degree of prolapse Prolapse is the most common reason for hysterectomy in women aged over 50. Causes of Prolapse: Vaginal delivery and Pregnancy, risk increased with large infants, instrumental deliveries and prolonged second stage Congenital Factors such as connective tissue disorders (due to abnormal collagen metabolism) Menopause possibly due to deterioration of collagenous tissue following oestrogen withdrawal Chronic predisposing factors such as raised intre abdominal pressure in chronic cough, obesity constipation or pelvic mass. Iatrogenic factors such as pelvic surgery (hysterectomy) or continence procedures
7 Clinical Features of Prolapse HISTORY Dragging sensation or sensation of a lump Worsens on standing or at the end of the day Interference with intercourse Bleeding and discharge possible due to ulceration Urinary frequency and incomplete bladder emptying Associated stress continence Necessity to digitally manipulate prolapse to pass stool or urine EXAMINATION Abdomen and Bimanual to exclude pelvic masses Use Sim s Speculum and ask patient to bear down To separate enterocoele from rectocoele place a finger in the rectum it will cause a rectocoele to bulge! Test stress continence by asking patient to cough while reducing the prolapse.
8 Investigation and Prevention of Prolapse Investigations Consider pelvic US if a mass is suspected Consider Urodynamic testing Assess fitness for surgery often elderly patients Prevention Good intrapartum care to avoid prolonged labour Pelvic floor exercises

9 Management of Prolapse CONSERVATIVE Watchful waiting Weight loss Smoking cessation Physiotherapy and pelvic floor exercises MEDICAL Ring pessary Shelf pessary HRT or topical oestrogen to prevent ulceration
10 Management of Prolapse SURGICAL Very effective but a combination of procedures may be required Indications for surgery are: failure of pessary, a patient who wants definitive treatment, prolapse combined with urinary or faecal incontinence. The choice of procedure depends on whether the woman is sexually active, whether her family is complete, her general fitness, and surgeon's preference. Surgery may be by the abdominal route, or vaginal. Evidence supports the greater efficacy of the abdominal route. Surgery may use a mesh or not. There are many types of mesh used, including biological grafts. Types of surgery which necessitate the use of mesh include sacrocolpopexy, infracoccygeal sacropexy, uterine suspension sling, and colpoperineopexy. Types of surgery which do not use mesh include hysterectomy, cervical amputation, and uterine/vault suspension.
11 Disorders of the Urinary Tract
12 Anatomy and function Normal filling requires adequate bladder capacity and urethral sphincter function Normal voiding requires detrusor muscle contraction coordinated with urethral relaxation
13 Anatomy and function Smooth wall of bladder detrusor muscle Bladder can normally store 500ml 500 ml
14 Anatomy and function Smooth wall of bladder detrusor muscle Bladder can normally store 500ml Void urge starts at 200ml 200 ml
15 Anatomy and function Smooth wall of bladder detrusor muscle Bladder can normally store 500ml Void urge starts at 200ml Drain by 4cm long urethra
16 Anatomy and function Smooth wall of bladder detrusor muscle Bladder can normally store 500ml Void urge starts at 200ml Drain by 4cm long urethra External orifice is the vestibule just above vaginal introitus
17 Anatomy and function Neural control
18 Anatomy and function Neural control Parasympathetic Nerves aid voiding Sympathetic Nerves prevent voiding
19 Anatomy and function Neural control
20 Anatomy and function Neural control Reflex afferent fibres detect stretch
21 Anatomy and function Neural control Efferent parasympathetic Contraction of detrusor muscle Pelvic nerve ACH binds to M3 receptor Relaxation of external sphincter Pudendal nerve ACH binds to nicotinic receptor
22 Continence Continence Pressure of the urethra higher than the pressure in the bladder Bladder pressure influenced by detrusor muscles pressure intra abdominal pressure (external pressure) i.e. a cough, sneeze Urethra pressure influenced by muscle tone of urethra Intra abdominal pressure Pelvic floor muscles
23 Continence Continence Pressure of the urethra higher than the pressure in the bladder Detrusor muscle is expandable No increase in pressure as fills Increase in intra abdominal pressure distributed equally between urethra and bladder as both lie within abdominal cavity Normally a cough would not lead to incontinence
24 Micturition Bladder pressure exceeds urethral pressure achieved through voluntary coordination
25 Incontinence Generally two types Uncontrolled increase in detrusor pressure overactive bladder
26 Incontinence Generally two types Uncontrolled increase in detrusor pressure detrusor overactivity overactive bladder Increase in intra abdominal pressure transmitted to bladder rather than both bladder and urethra urinary stress incontinence
27 Incontinence Generally two types Uncontrolled increase in detrusor pressure detrusor overactivity overactive bladder Increase in intra abdominal pressure transmitted to bladder rather than both bladder and urethra urinary stress incontinence Rarer causes fistula, or over flow incontinence caused by obstruction or neurogenic causes
28 Incontinence Generally two types Uncontrolled increase in detrusor pressure detrusor overactivity overactive bladder Increase in intra abdominal pressure transmitted to bladder rather than both bladder and urethra urinary stress incontinence Rarer causes fistula, or over flow incontinence caused by obstruction or neurogenic causes
29 Urinary tract investigations Urine dipstick Nitrates suggest infection sent for microscopy and culture to confirm Glucose diabetes Haematuria calculi, carcinoma, infection
30 Urinary tract investigations Urine dipstick Nitrates suggest infection sent for microscopy and culture to confirm Glucose diabetes Haematuria calculi, carcinoma, infection Urinary diary record of fluid intake and micturition, drinking habits, frequency and bladder capacity
31 Urinary tract investigations Urine dipstick Nitrates suggest infection sent for microscopy and culture to confirm Glucose diabetes Haematuria calculi, carcinoma, infection Urinary diary record of fluid intake and micturition, drinking habits, frequency and bladder capacity Ultrasound excludes incomplete bladder emptiness, congenital abnormalities, calculi, tumours, cortical scaring of the kidneys Abdo x ray foreign bodies and calculi Abdo CT with contrast examine ureter integrity and route Cystoscopy inspection of bladder, tumour, stones, fistula etc.
32 Urinary tract investigations Cystometry Detects pressure in the bladder and intraabdominal pressure to work out the pressure generated by the detrusor muscle. This test can determine whether the incontinence is urinary stress incontinence (USI) or detrusor overactivity (DOA) Usually not indicated unless lifestyle and drug therapies have failed, or considering surgery for stress incontinence.
33 Urinary tract investigations Cystometry Bladder Pressure Intra abdo Pressure Detrusor Pressure Urine Flow Cough Filling A Cough Filling B Cough Filling C A normal bladder, No increase in detrusor muscle when filling No detrusor contraction when cough No urine flow when cough B Urinary stress incontinence No increase in detrusor muscle when filling No detrusor contraction when cough Urine flow when cough C Detrusor overactivity Detrusor contraction after cough Urine flow with detrusor contraction if pressure is so much to overcome urethral pressure
34 Urinary stress incontinence Involuntary leakage of urine on effort or exertion, or sneezing and coughing Can be confirmed by excluding DOA using cystometry. Epidemiology almost 50% of all causes of incontinence, in more than 10% of all women Pelvic floor Urethra Bladder pressure Bladder A Ureter Urethral pressure Aetiology pregnancy, prolonged vaginal delivery, forceps delivery, obesity, age, and previous hysterectomy Bladder pressure Normally during an increase in abdominal pressure both the bladder and urethra experience it equally. However if the bladder neck slips down due to a weak pelvic floor, the remainder of the urethra and the pelvic floor will be unable to compensate which will result in incontinence. Pelvic floor Urethra Bladder B Ureter Bladder pressure
35 Urinary stress incontinence Clinical features History Frequency, urgency, and urge incontinence, I leak when I cough Examination Speculum may reveal cystocoele or urethrocele, leakage of urine may be seen when coughing. Palpate abdomen to exclude distended bladder
36 Urinary stress incontinence Clinical features History Frequency, urgency, and urge incontinence, I leak when I cough Examination Speculum may reveal cystocoele or urethrocele, leakage of urine may be seen when coughing. Palpate abdomen to exclude distended bladder Investigations Urine dipstick to exclude infection, cystometry if necessary.
37 Urinary stress incontinence Management Generally conservative lose weight, eliminate causes of cough and sneezing allergies, smoking etc, advise on excessive fluid intake Pelvic floor training exercises Drugs duloxetine. For severe USI, serotonin and noradrenaline reuptake inhibitor to enhance urethral sphincter muscle activity side effects, dyspepsia, dry mouth, dizziness, insomnia Surgery when conservative measures have failed. Tans obturator tape usually first line. Cure rates up to 90%. Complications include perforations, post operative voiding difficulty, bleeding, infection.
38 Overactive bladder Urgency with or without urge incontinence, usually with frequency or nocturia, in the absence of infection. Usually caused by detrusor overactivity during the filling phase. This can occur spontaneously or provoked i.e. with coughing therefore can be confused for USI Result of 35% of female incontinence Most commonly idiopathy, but can occur in underlying neuropathy such as multiple sclerosis or spinal cord injury
39 Overactive bladder Clinical features History urgency, urge incontinence, frequency and nocturia. Stress incontinence is common, coughing, sneezing, orgasm. Childhood history of enuresis is common Examination normally normal, incidental cystocoele may be present. Investigations Urinary diary, cystometry
40 Overactive bladder Management Conservative advise of fluid intake, caffeine restriction, bladder training delaying going to toilet Drugs review current medication diuretics and antipsychotics Anticholinergics to supress detrusor activity Oestrogen in postmenopausal women can reduce symptoms of urgency Bo tox into detrusor muscle, very effective 60 93%, though can cause urinary retention. Surgery ileocystoplasty, increases bladder capacity
41 Other disorders of the Urinary Tract Acute urinary retention unable to pass urine for 12 hours Causes epidural, post vulval/perineal surgery, anticholinergics, retroverted gravid uterus, pelvic mass, neurological disease (MS) Treatment catheterisation whilst cause is treated. Chronic retention/urinary overflow overdistension causing overflow Causes masses or detrusor inactivity. Presentation may mimic USI, examination reveals non tender distended bladder. Diagnosis confirmed by ultrasound. Treatment self catheterisation
42 Other disorders of the Urinary Tract Fistulae very rear 0.3% 1. Urethrovaginal fistulae Uterus 3 Ureter 2. Vesicovaginal fistulae Bladder 3. Vesicouterine fistulae Urethra 4. Ureterovaginal fistulae 1 Vaginal canal 2 4
43 Thank you
John Laughlin 4 th year Cardiff University Medical Student
 John Laughlin 4 th year Cardiff University Medical Student Prolapse/incontinence You need to know: Pelvic floor anatomy in relation to uterovaginal support and continence The classification of uterovaginal
John Laughlin 4 th year Cardiff University Medical Student Prolapse/incontinence You need to know: Pelvic floor anatomy in relation to uterovaginal support and continence The classification of uterovaginal
Prolapse and Urogynae Incontinence. Lucy Tiffin and Hannah Wheldon-Holmes
 Prolapse and Urogynae Incontinence Lucy Tiffin and Hannah Wheldon-Holmes 66 year old woman with incontinence PC: 7 year Hx of urgency, frequency, nocturia (incl. incontinence at night), and stress incontinence
Prolapse and Urogynae Incontinence Lucy Tiffin and Hannah Wheldon-Holmes 66 year old woman with incontinence PC: 7 year Hx of urgency, frequency, nocturia (incl. incontinence at night), and stress incontinence
Ben Herbert Alex Wojtowicz
 Ben Herbert Alex Wojtowicz 54 year old female presenting with: Dragging sensation Urinary incontinence Some faecal incontinence HPC Since May 14 had noticed a mass protruding from the vagina when going
Ben Herbert Alex Wojtowicz 54 year old female presenting with: Dragging sensation Urinary incontinence Some faecal incontinence HPC Since May 14 had noticed a mass protruding from the vagina when going
By:Dr:ISHRAQ MOHAMMED
 By:Dr:ISHRAQ MOHAMMED Protrusion of an organ or structure beyond its normal confines. Prolapses are classified according to their location and the organs contained within them. 1-Anterior vaginal wall
By:Dr:ISHRAQ MOHAMMED Protrusion of an organ or structure beyond its normal confines. Prolapses are classified according to their location and the organs contained within them. 1-Anterior vaginal wall
Gynecology Dr. Sallama Lecture 3 Genital Prolapse
 Gynecology Dr. Sallama Lecture 3 Genital Prolapse Genital(utero-vaginal )prolapse is extremely common, with an estimated 11% of women undergoing at least one operation for this condition. Definition: A
Gynecology Dr. Sallama Lecture 3 Genital Prolapse Genital(utero-vaginal )prolapse is extremely common, with an estimated 11% of women undergoing at least one operation for this condition. Definition: A
Content. Terminology Anatomy Aetiology Presentation Classification Management
 Prolapse Content Terminology Anatomy Aetiology Presentation Classification Management Terminology Prolapse Descent of pelvic organs into the vagina Cystocele ant. vaginal wall involving bladder Uterine
Prolapse Content Terminology Anatomy Aetiology Presentation Classification Management Terminology Prolapse Descent of pelvic organs into the vagina Cystocele ant. vaginal wall involving bladder Uterine
Urogynaecology. Colm McAlinden
 Urogynaecology Colm McAlinden Definitions Urinary incontinence compliant of any involuntary leakage of urine with many different causes Two main types: Stress Urge Definitions Nocturia: More than a single
Urogynaecology Colm McAlinden Definitions Urinary incontinence compliant of any involuntary leakage of urine with many different causes Two main types: Stress Urge Definitions Nocturia: More than a single
Management of Female Stress Incontinence
 Management of Female Stress Incontinence Dr. Arvind Goyal Associate Professor (Urology& Renal Transplant) Dayanand Medical College & Hospital, Ludhiana, Punjab, India Stress Incontinence Involuntary loss
Management of Female Stress Incontinence Dr. Arvind Goyal Associate Professor (Urology& Renal Transplant) Dayanand Medical College & Hospital, Ludhiana, Punjab, India Stress Incontinence Involuntary loss
INCONTINENCE. Continence and Pelvic Floor Rehabilitation TYPES OF INCONTINENCE STRESS INCONTINENCE STRESS INCONTINENCE STRESS INCONTINENCE 11/08/2015
 INCONTINENCE Continence and Pelvic Floor Rehabilitation Dr Irmina Nahon PhD Pelvic Floor Physiotherapist www.nahonpfed.com.au Defined as the accidental and inappropriate passage of urine or faeces (ICI
INCONTINENCE Continence and Pelvic Floor Rehabilitation Dr Irmina Nahon PhD Pelvic Floor Physiotherapist www.nahonpfed.com.au Defined as the accidental and inappropriate passage of urine or faeces (ICI
Prolapse & Urogynaecology. Hester Mannion and Fabi Sica
 Prolapse & Urogynaecology Hester Mannion and Fabi Sica Take home messages Prolapse and associated incontinence is very common It has a devastating effect on the QoL of the patient and their partner Strategies
Prolapse & Urogynaecology Hester Mannion and Fabi Sica Take home messages Prolapse and associated incontinence is very common It has a devastating effect on the QoL of the patient and their partner Strategies
LAPAROSCOPIC REPAIR OF PELVIC FLOOR
 LAPAROSCOPIC REPAIR OF PELVIC FLOOR Dr. R. K. Mishra Elements comprising the Pelvis Bones Ilium, ischium and pubis fusion Ligaments Muscles Obturator internis muscle Arcus tendineus levator ani or white
LAPAROSCOPIC REPAIR OF PELVIC FLOOR Dr. R. K. Mishra Elements comprising the Pelvis Bones Ilium, ischium and pubis fusion Ligaments Muscles Obturator internis muscle Arcus tendineus levator ani or white
Prediction and prevention of stress urinary incontinence after prolapse surgery van der Ploeg, J.M.
 UvA-DARE (Digital Academic Repository) Prediction and prevention of stress urinary incontinence after prolapse surgery van der Ploeg, J.M. Link to publication Citation for published version (APA): van
UvA-DARE (Digital Academic Repository) Prediction and prevention of stress urinary incontinence after prolapse surgery van der Ploeg, J.M. Link to publication Citation for published version (APA): van
Karanvir Virk M.D. Minimally Invasive & Pelvic Reconstructive Surgery 01/28/2015
 Karanvir Virk M.D. Minimally Invasive & Pelvic Reconstructive Surgery 01/28/2015 Disclosures I have none Objectives Identify the basic Anatomy and causes of Pelvic Organ Prolapse Examine office diagnosis
Karanvir Virk M.D. Minimally Invasive & Pelvic Reconstructive Surgery 01/28/2015 Disclosures I have none Objectives Identify the basic Anatomy and causes of Pelvic Organ Prolapse Examine office diagnosis
Moneli Golara Consultant Obstetrician and Gynaecologist Royal Free NHS Trust Barnet Hospital
 Moneli Golara Consultant Obstetrician and Gynaecologist Royal Free NHS Trust Barnet Hospital Pelvic Organ Prolapse (POP)- herniation of pelvic organs into vaginal walls Common Huge impact on daily activities
Moneli Golara Consultant Obstetrician and Gynaecologist Royal Free NHS Trust Barnet Hospital Pelvic Organ Prolapse (POP)- herniation of pelvic organs into vaginal walls Common Huge impact on daily activities
URINARY INCONTINENCE. Urology Division, Surgery Department Medical Faculty, University of Sumatera Utara
 URINARY INCONTINENCE Urology Division, Surgery Department Medical Faculty, University of Sumatera Utara Definition The involuntary loss of urine May denote a symptom, a sign or a condition Symptom the
URINARY INCONTINENCE Urology Division, Surgery Department Medical Faculty, University of Sumatera Utara Definition The involuntary loss of urine May denote a symptom, a sign or a condition Symptom the
4. Know how to examine and name relevant test performed on patients
 Chapter 18 Female Urinary lncontinence Dr Zeelha Abdool Ed ucational Objectives : After completion of this chapter you should be able to: 1. Understand the pathophysiology of incontinence 2. Define and
Chapter 18 Female Urinary lncontinence Dr Zeelha Abdool Ed ucational Objectives : After completion of this chapter you should be able to: 1. Understand the pathophysiology of incontinence 2. Define and
Urogynaecology & Prolapse. Alexander Denning and Leifa Jennings
 + Urogynaecology & Prolapse Alexander Denning and Leifa Jennings + Contents What even is prolapse / urogynaecology? Pelvic floor anatomy Prolapse Urinary incontinence Prevention The end (woot) + Urogynaecology
+ Urogynaecology & Prolapse Alexander Denning and Leifa Jennings + Contents What even is prolapse / urogynaecology? Pelvic floor anatomy Prolapse Urinary incontinence Prevention The end (woot) + Urogynaecology
The Management of Female Urinary Incontinence. Part 1: Aetiology and Investigations
 The Management of Female Urinary Incontinence Part 1: Aetiology and Investigations Dr Oseka Onuma Gynaecologist and Pelvic Reconstructive Surgeon 4 Robe Terrace Medindie SA 5081 Urinary incontinence has
The Management of Female Urinary Incontinence Part 1: Aetiology and Investigations Dr Oseka Onuma Gynaecologist and Pelvic Reconstructive Surgeon 4 Robe Terrace Medindie SA 5081 Urinary incontinence has
Advanced Care for Female Overactive Bladder & Urinary Incontinence. Department of Urology Kaiser Permanente Santa Rosa
 Advanced Care for Female Overactive Bladder & Urinary Incontinence Department of Urology Kaiser Permanente Santa Rosa Goals Participants will: Review normal urinary tract anatomy and function Understand
Advanced Care for Female Overactive Bladder & Urinary Incontinence Department of Urology Kaiser Permanente Santa Rosa Goals Participants will: Review normal urinary tract anatomy and function Understand
Objectives. Prevalence of Urinary Incontinence URINARY INCONTINENCE: EVALUATION AND CURRENT TREATMENT OPTIONS
 URINARY INCONTINENCE: EVALUATION AND CURRENT TREATMENT OPTIONS Lisa S Pair, MSN, CRNP Division of Urogynecology and Pelvic Reconstructive Surgery Department of Obstetrics and Gynecology University of Alabama
URINARY INCONTINENCE: EVALUATION AND CURRENT TREATMENT OPTIONS Lisa S Pair, MSN, CRNP Division of Urogynecology and Pelvic Reconstructive Surgery Department of Obstetrics and Gynecology University of Alabama
Urinary Incontinence. Lora Keeling and Byron Neale
 Urinary Incontinence Lora Keeling and Byron Neale Not life threatening. Introduction But can have a huge impact on quality of life. Two main types of urinary incontinence (UI). Stress UI leakage on effort,
Urinary Incontinence Lora Keeling and Byron Neale Not life threatening. Introduction But can have a huge impact on quality of life. Two main types of urinary incontinence (UI). Stress UI leakage on effort,
Pelvic organ prolapse
 Page 1 of 11 Pelvic organ prolapse Introduction The aim of this leaflet is to give you information about a pelvic organ prolapse, its causes and available treatments but does not replace advice given by
Page 1 of 11 Pelvic organ prolapse Introduction The aim of this leaflet is to give you information about a pelvic organ prolapse, its causes and available treatments but does not replace advice given by
Ina S. Irabon, MD, FPOGS, FPSRM, FPSGE Obstetrics and Gynecology Reproductive Endocrinology and Infertility Laparoscopy and Hysteroscopy
 Ina S. Irabon, MD, FPOGS, FPSRM, FPSGE Obstetrics and Gynecology Reproductive Endocrinology and Infertility Laparoscopy and Hysteroscopy Comprehensive Gynecology 7 th edition, 2017 (Lobo RA, Gershenson
Ina S. Irabon, MD, FPOGS, FPSRM, FPSGE Obstetrics and Gynecology Reproductive Endocrinology and Infertility Laparoscopy and Hysteroscopy Comprehensive Gynecology 7 th edition, 2017 (Lobo RA, Gershenson
Continence Promotion in
 Everybody s Business- Continence Promotion in Aged Care Melissa O Grady Clinical Nurse Consultant Continence Warning Some graphic images are contained in this presentation Objectives What is Old Age? What
Everybody s Business- Continence Promotion in Aged Care Melissa O Grady Clinical Nurse Consultant Continence Warning Some graphic images are contained in this presentation Objectives What is Old Age? What
Northwest Rehabilitation Associates, Inc.
 Pelvic Health Patient Intake Form Name: Date: Please answer the following questions as honestly and thoroughly as you can. Your responses will help us better understand your condition and provide the best
Pelvic Health Patient Intake Form Name: Date: Please answer the following questions as honestly and thoroughly as you can. Your responses will help us better understand your condition and provide the best
Pelvic organ prolapse. Information for patients Continence Service
 Pelvic organ prolapse Information for patients Continence Service What is a pelvic organ prolapse? A pelvic organ prolapse occurs when the uterus (womb), vagina, bladder or bowel slips out of place, resulting
Pelvic organ prolapse Information for patients Continence Service What is a pelvic organ prolapse? A pelvic organ prolapse occurs when the uterus (womb), vagina, bladder or bowel slips out of place, resulting
Urogynecology ICD-9 to ICD-10 Crosswalks
 1100 Wayne Ave, Suite 825 Silver Spring, MD 20910 301.273.0570 Fax 301.273.0778 info@augs.org www.augs.org Urogynecology ICD-9 to ICD-10 Crosswalks ICD 9 ICD 9 Description ICD 10 Code ICD 10 Description
1100 Wayne Ave, Suite 825 Silver Spring, MD 20910 301.273.0570 Fax 301.273.0778 info@augs.org www.augs.org Urogynecology ICD-9 to ICD-10 Crosswalks ICD 9 ICD 9 Description ICD 10 Code ICD 10 Description
Module 3 Causes Of Urinary Incontinence
 Causes Of Urinary Incontinence V4: Last Reviewed September 2017 Learning Outcomes Appreciate the numerous requirements and skills necessary for the person to achieve and maintain urinary continence Discuss
Causes Of Urinary Incontinence V4: Last Reviewed September 2017 Learning Outcomes Appreciate the numerous requirements and skills necessary for the person to achieve and maintain urinary continence Discuss
Neurogenic bladder. Neurogenic bladder is a type of dysfunction of the bladder due to neurological disorder.
 Definition: Neurogenic bladder Neurogenic bladder is a type of dysfunction of the bladder due to neurological disorder. Types: Nervous system diseases: Congenital: like myelodysplasia like meningocele.
Definition: Neurogenic bladder Neurogenic bladder is a type of dysfunction of the bladder due to neurological disorder. Types: Nervous system diseases: Congenital: like myelodysplasia like meningocele.
Incontinence: Risks, Causes and Care
 Welcome To Incontinence: Risks, Causes and Care Presented by Kamal Masaki, MD Professor and Chair Department of Geriatric Medicine John A. Burns School of Medicine, UH Manoa September 5, 2018 10:00 11:00
Welcome To Incontinence: Risks, Causes and Care Presented by Kamal Masaki, MD Professor and Chair Department of Geriatric Medicine John A. Burns School of Medicine, UH Manoa September 5, 2018 10:00 11:00
Management of Urinary Incontinence in Older Women. Dr. Cecilia Cheon Department of Obs. & Gyn. Queen Elizabeth Hospital
 Management of Urinary Incontinence in Older Women Dr. Cecilia Cheon Department of Obs. & Gyn. Queen Elizabeth Hospital Epidemiology Causes Investigation Treatment Conclusion Elderly Women High prevalence
Management of Urinary Incontinence in Older Women Dr. Cecilia Cheon Department of Obs. & Gyn. Queen Elizabeth Hospital Epidemiology Causes Investigation Treatment Conclusion Elderly Women High prevalence
Pelvic Support Problems
 AP012, April 2010 ACOG publications are protected by copyright and all rights are reserved. ACOG publications may not be reproduced in any form or by any means without written permission from the copyright
AP012, April 2010 ACOG publications are protected by copyright and all rights are reserved. ACOG publications may not be reproduced in any form or by any means without written permission from the copyright
4) Urinary Incontinence - Dr. Abeer
 Urinary Incontinence - Dr. Abeer") 4) Urinary Incontinence - Dr. Abeer INTRODUCTION Involuntary loss of urine Social and hygienic problem It affects individuals physical, psychological and social which is associated with a significant reduction
4) Urinary Incontinence - Dr. Abeer INTRODUCTION Involuntary loss of urine Social and hygienic problem It affects individuals physical, psychological and social which is associated with a significant reduction
Functional anatomy of the female pelvic floor and lower urinary tract Stefano Floris, MD, PhD Department of Obstetrics and Gynaecology
 Functional anatomy of the female pelvic floor and lower urinary tract Stefano Floris, MD, PhD Department of Obstetrics and Gynaecology Ospedale San Giovanni di Dio, Gorizia, Italy ANATOMY URINARY CONTINENCE
Functional anatomy of the female pelvic floor and lower urinary tract Stefano Floris, MD, PhD Department of Obstetrics and Gynaecology Ospedale San Giovanni di Dio, Gorizia, Italy ANATOMY URINARY CONTINENCE
Incontinence. Anatomy The human body has two kidneys. The kidneys continuously filter the blood and make urine.
 Incontinence Introduction Urinary incontinence occurs when a person cannot control the emptying of his or her urinary bladder. It can happen to anyone, but is very common in older people. Urinary incontinence
Incontinence Introduction Urinary incontinence occurs when a person cannot control the emptying of his or her urinary bladder. It can happen to anyone, but is very common in older people. Urinary incontinence
Urinary incontinence. Urology Department. Patient Information Leaflet
 Urinary incontinence Urology Department Patient Information Leaflet Introduction This leaflet is for people who have been diagnosed with urinary incontinence. It contains information about the bladder,
Urinary incontinence Urology Department Patient Information Leaflet Introduction This leaflet is for people who have been diagnosed with urinary incontinence. It contains information about the bladder,
Various Types. Ralph Boling, DO, FACOG
 Various Types Ralph Boling, DO, FACOG The goal of this lecture is to increase assessment and treatment abilities for physicians managing urinary incontinence (UI) patients. 1. Effectively communicate with
Various Types Ralph Boling, DO, FACOG The goal of this lecture is to increase assessment and treatment abilities for physicians managing urinary incontinence (UI) patients. 1. Effectively communicate with
Pelvic Floor and More.. Urinary Continence. Urinary Incontinence. Normal Bladder Function
 Pelvic Floor and More.. Jo Pitts Women s and Men s Health Physiotherapist Milton Keynes University Hospital Women s and Men s Health Physiotherapy at MKUH Pregnancy-related back and pelvic girdle pain
Pelvic Floor and More.. Jo Pitts Women s and Men s Health Physiotherapist Milton Keynes University Hospital Women s and Men s Health Physiotherapy at MKUH Pregnancy-related back and pelvic girdle pain
Toning your pelvic floor WELCOME
 Toning your pelvic floor WELCOME Introductions Amelia Samuels, Physiotherapist, Active Rehabilitation Physiotherapy Supporting the Continence Foundation of Australia Continence Foundation of Australia
Toning your pelvic floor WELCOME Introductions Amelia Samuels, Physiotherapist, Active Rehabilitation Physiotherapy Supporting the Continence Foundation of Australia Continence Foundation of Australia
Female Urinary Incontinence: What It Is and What You Can Do About It
 Female Urinary Incontinence: What It Is and What You Can Do About It Urogynecology Patient Information Sheet What is Urinary Incontinence? Stress Incontinence is a leakage of urine that occurs, for example,
Female Urinary Incontinence: What It Is and What You Can Do About It Urogynecology Patient Information Sheet What is Urinary Incontinence? Stress Incontinence is a leakage of urine that occurs, for example,
Pelvic Prolapse. A Patient Guide to Pelvic Floor Reconstruction
 Pelvic Prolapse A Patient Guide to Pelvic Floor Reconstruction Pelvic Prolapse When an organ becomes displaced, or slips down in the body, it is referred to as a prolapse. Your physician has diagnosed
Pelvic Prolapse A Patient Guide to Pelvic Floor Reconstruction Pelvic Prolapse When an organ becomes displaced, or slips down in the body, it is referred to as a prolapse. Your physician has diagnosed
NEUROGENIC BLADDER. Dr Harriet Grubb Dr Alison Seymour Dr Alexander Joseph
 NEUROGENIC BLADDER Dr Harriet Grubb Dr Alison Seymour Dr Alexander Joseph OUTLINE Definition Anatomy and physiology of bladder function Types of neurogenic bladder Assessment and management Complications
NEUROGENIC BLADDER Dr Harriet Grubb Dr Alison Seymour Dr Alexander Joseph OUTLINE Definition Anatomy and physiology of bladder function Types of neurogenic bladder Assessment and management Complications
Lower Urinary Tract Symptoms K Kuruvilla Zachariah Associate Specialist
 Lower Urinary Tract Symptoms K Kuruvilla Zachariah Associate Specialist Lower Urinary Tract Symptoms Storage Symptoms Frequency, urgency, incontinence, Nocturia Voiding Symptoms Hesitancy, poor flow, intermittency,
Lower Urinary Tract Symptoms K Kuruvilla Zachariah Associate Specialist Lower Urinary Tract Symptoms Storage Symptoms Frequency, urgency, incontinence, Nocturia Voiding Symptoms Hesitancy, poor flow, intermittency,
Imaging of Pelvic Floor Weakness. Dr Susan Kouloyan-Ilic Radiologist Epworth Medical Imaging The Women s, Melbourne
 Imaging of Pelvic Floor Weakness Dr Susan Kouloyan-Ilic Radiologist Epworth Medical Imaging The Women s, Melbourne Outline Overview and Epidemiology Risk Factors, Causes and Results Review of Relevant
Imaging of Pelvic Floor Weakness Dr Susan Kouloyan-Ilic Radiologist Epworth Medical Imaging The Women s, Melbourne Outline Overview and Epidemiology Risk Factors, Causes and Results Review of Relevant
Female Symptom Monitor
 Occupation Female Symptom Monitor Presenting problems When did this start? Please fill out each section that is relevant to your problem Gynecological History What age did your period start? Is your cycle
Occupation Female Symptom Monitor Presenting problems When did this start? Please fill out each section that is relevant to your problem Gynecological History What age did your period start? Is your cycle
NATIONAL INSTITUTE FOR CLINICAL EXCELLENCE SCOPE. Urinary incontinence: the management of urinary incontinence in women
 NATIONAL INSTITUTE FOR CLINICAL EXCELLENCE 1 Guideline title SCOPE Urinary incontinence: the management of urinary incontinence in women 1.1 Short title Urinary incontinence 2 Background a) The National
NATIONAL INSTITUTE FOR CLINICAL EXCELLENCE 1 Guideline title SCOPE Urinary incontinence: the management of urinary incontinence in women 1.1 Short title Urinary incontinence 2 Background a) The National
Clinical Curriculum: Urogynecology
 Updated July 201 Clinical Curriculum: Urogynecology GOAL: The primary goal of the Urogynecology rotation at the University of Alabama at Birmingham (UAB) is to train physicians to have a broad knowledge
Updated July 201 Clinical Curriculum: Urogynecology GOAL: The primary goal of the Urogynecology rotation at the University of Alabama at Birmingham (UAB) is to train physicians to have a broad knowledge
Dr. Aso Urinary Symptoms
 Haematuria The presence of blood in the urine (haematuria) is always abnormal and may be the only indication of pathology in the urinary tract. False positive stick tests and the discolored urine caused
Haematuria The presence of blood in the urine (haematuria) is always abnormal and may be the only indication of pathology in the urinary tract. False positive stick tests and the discolored urine caused
Female Symptom Monitor
 Female Symptom Monitor Occupation: Recreational Activities: Presenting problems: 1. 2. When did this start? Gynecological History: Please fill out each section that is relevant to your problem What age
Female Symptom Monitor Occupation: Recreational Activities: Presenting problems: 1. 2. When did this start? Gynecological History: Please fill out each section that is relevant to your problem What age
Stop Coping. Start Living. Talk to your doctor about pelvic organ prolapse and sacrocolpopexy
 Stop Coping. Start Living Talk to your doctor about pelvic organ prolapse and sacrocolpopexy Did you know? One in three women will suffer from a pelvic health condition in her lifetime. Four of the most
Stop Coping. Start Living Talk to your doctor about pelvic organ prolapse and sacrocolpopexy Did you know? One in three women will suffer from a pelvic health condition in her lifetime. Four of the most
Loss of Bladder Control
 BLADDER HEALTH: Bladder Prolapse Loss of Bladder Control Bladder Prolapse Don t Let Bladder Prolapse Keep You from Enjoying Life. What is the Bladder? The bladder is a hollow, balloon-like organ made mostly
BLADDER HEALTH: Bladder Prolapse Loss of Bladder Control Bladder Prolapse Don t Let Bladder Prolapse Keep You from Enjoying Life. What is the Bladder? The bladder is a hollow, balloon-like organ made mostly
Normal micturition involves complex
 NEW TARGET FOR INTERVENTION: THE NEUROUROLOGY CONNECTION * Donald R. Ostergard, MD, FACOG ABSTRACT Urine storage and release are under the control of the parasympathetic, sympathetic, and somatic nervous
NEW TARGET FOR INTERVENTION: THE NEUROUROLOGY CONNECTION * Donald R. Ostergard, MD, FACOG ABSTRACT Urine storage and release are under the control of the parasympathetic, sympathetic, and somatic nervous
Dr Anil Sharma. Gynaecologist Auckland
 Dr Anil Sharma Gynaecologist Auckland 16:30-17:25 WS #165: Managing Prolapse and Stress Incontinence Without Mesh and Slings and Things 17:35-18:30 WS #177: Managing Prolapse and Stress Incontinence Without
Dr Anil Sharma Gynaecologist Auckland 16:30-17:25 WS #165: Managing Prolapse and Stress Incontinence Without Mesh and Slings and Things 17:35-18:30 WS #177: Managing Prolapse and Stress Incontinence Without
URINARY INCONTINENCE
 Center for Continence Care and Pelvic Medicine What is urinary incontinence? URINARY INCONTINENCE Urinary incontinence is the uncontrollable loss of urine. The amount of urine leaked can vary from only
Center for Continence Care and Pelvic Medicine What is urinary incontinence? URINARY INCONTINENCE Urinary incontinence is the uncontrollable loss of urine. The amount of urine leaked can vary from only
Dr John Short. Obstetrician and Gynaecologist Christchurch Women s Hospital, Oxford Women's Health, Christchurch
 Dr John Short Obstetrician and Gynaecologist Christchurch Women s Hospital, Oxford Women's Health, Christchurch 8:30-9:25 WS #142: Peeling Back the Layers - The Pelvic Floor Uncovered 9:35-10:30 WS #152:
Dr John Short Obstetrician and Gynaecologist Christchurch Women s Hospital, Oxford Women's Health, Christchurch 8:30-9:25 WS #142: Peeling Back the Layers - The Pelvic Floor Uncovered 9:35-10:30 WS #152:
Review Article Pelvic Floor Dysfunction, Body Excreta Incontinence and Continence
 Cronicon OPEN ACCESS GYNAECOLOGY Review Article Pelvic Floor Dysfunction, Body Excreta Incontinence and Continence Abdel Karim M El Hemaly 1 * and Laila ASE Mousa 1 1 Professor of Obstetrics and gynaecology,
Cronicon OPEN ACCESS GYNAECOLOGY Review Article Pelvic Floor Dysfunction, Body Excreta Incontinence and Continence Abdel Karim M El Hemaly 1 * and Laila ASE Mousa 1 1 Professor of Obstetrics and gynaecology,
Patient Information. Tension Free Vaginal/ Obturator Tape (TVT) Royal Devon and Exeter NHS Foundation Trust
 Royal Devon and Exeter NHS Foundation Trust") Tension Free Vaginal/Obturator Tape (TVT) Royal Devon and Exeter NHS Foundation Trust Patient Information Tension Free Vaginal/ Obturator Tape (TVT) Reference Number: CW 08 011 003 (version date: September
Tension Free Vaginal/Obturator Tape (TVT) Royal Devon and Exeter NHS Foundation Trust Patient Information Tension Free Vaginal/ Obturator Tape (TVT) Reference Number: CW 08 011 003 (version date: September
Overactive Bladder Syndrome
 Overactive Bladder Syndrome behavioural modifications to pharmacological and surgical treatments Dr Jos Jayarajan Urologist Austin Health, Eastern Health Warringal Private, Northpark Private, Epworth Overactive
Overactive Bladder Syndrome behavioural modifications to pharmacological and surgical treatments Dr Jos Jayarajan Urologist Austin Health, Eastern Health Warringal Private, Northpark Private, Epworth Overactive
Management of Urogenital Prolapse of Women in Primary Care. Lizzie McManus MBE RGN RMN Practice nurse Womens health practitioner
 Management of Urogenital Prolapse of Women in Primary Care Lizzie McManus MBE RGN RMN Practice nurse Womens health practitioner Primary Care Womens Health Forum www.pcwhf.org.uk Useful websites RCN genital
Management of Urogenital Prolapse of Women in Primary Care Lizzie McManus MBE RGN RMN Practice nurse Womens health practitioner Primary Care Womens Health Forum www.pcwhf.org.uk Useful websites RCN genital
5/29/2015. Objectives. Functions of the PFM. Various phases of PFM. Evaluation of the PFM
 The Physical Therapist s Approach to the Female Pelvic Floor Musculature Examination and Treatment. Presented By: Evelyne Burtis, DPT Objectives Core and pelvic floor muscles (PFM) Functions of the PFM
The Physical Therapist s Approach to the Female Pelvic Floor Musculature Examination and Treatment. Presented By: Evelyne Burtis, DPT Objectives Core and pelvic floor muscles (PFM) Functions of the PFM
Mr. GIT KAH ANN. Pakar Klinikal Urologi Hospital Kuala Lumpur.
 Mr. GIT KAH ANN Pakar Klinikal Urologi Hospital Kuala Lumpur drgitka@yahoo.com 25 Jan 2007 HIGHLIGHTS Introduction ICS Definition Making a Diagnosis Voiding Chart Investigation Urodynamics Ancillary Investigations
Mr. GIT KAH ANN Pakar Klinikal Urologi Hospital Kuala Lumpur drgitka@yahoo.com 25 Jan 2007 HIGHLIGHTS Introduction ICS Definition Making a Diagnosis Voiding Chart Investigation Urodynamics Ancillary Investigations
gynaecology in family medicine
 gynaecology in family medicine John Short Obstetrician and Gynaecologist Christchurch john.short@oxfordclinic.co.nz www.christchurch-gynaecologist.co.nz What s going on down there? http://www.youtube.com/watch?v=4-
gynaecology in family medicine John Short Obstetrician and Gynaecologist Christchurch john.short@oxfordclinic.co.nz www.christchurch-gynaecologist.co.nz What s going on down there? http://www.youtube.com/watch?v=4-
Urodynamics in women. Aims of Urodynamics in women. Why do Urodynamics?
 Urodynamics in women Chendrimada Madhu MD, MA, MRCOG Subspecialty Trainee in Urogynaecology Southmead Hospital 2013 Aims of Urodynamics in women n Confirmation of incontinence and its cause n Definition
Urodynamics in women Chendrimada Madhu MD, MA, MRCOG Subspecialty Trainee in Urogynaecology Southmead Hospital 2013 Aims of Urodynamics in women n Confirmation of incontinence and its cause n Definition
Physiology & Neurophysiology of lower U.T.
 Physiology & Neurophysiology of lower U.T. Classification of voiding dysfunction Evaluation of a child with voiding dysfunction Management Storage Ø Adequate volume of urine Ø At LOW pressure Ø With NO
Physiology & Neurophysiology of lower U.T. Classification of voiding dysfunction Evaluation of a child with voiding dysfunction Management Storage Ø Adequate volume of urine Ø At LOW pressure Ø With NO
Tools for Evaluation. Urodynamics Case Studies. Case 1. Evaluation. Case 1. Bladder Diary SUI 19/01/2018
 Urodynamics Case Studies Christopher K. Payne, MD Vista Urology & Pelvic Pain Partners Emeritus Professor of Urology, Stanford University Tools for Evaluation Ears, Eyes, and Brain Bladder diary Stress
Urodynamics Case Studies Christopher K. Payne, MD Vista Urology & Pelvic Pain Partners Emeritus Professor of Urology, Stanford University Tools for Evaluation Ears, Eyes, and Brain Bladder diary Stress
Pelvic Floor Therapy for the Neurologic Client Carina Siracusa, PT, DPT, WCS
 Pelvic Floor Therapy for the Neurologic Client Carina Siracusa, PT, DPT, WCS OhioHealth, Columbus Ohio Disclosures I have nothing to disclose Objectives Describe the role of a pelvic floor therapist in
Pelvic Floor Therapy for the Neurologic Client Carina Siracusa, PT, DPT, WCS OhioHealth, Columbus Ohio Disclosures I have nothing to disclose Objectives Describe the role of a pelvic floor therapist in
FEMALE URINARY INCONTINENCE: WHAT IT IS AND WHAT YOU CAN DO ABOUT IT
 URO-GYNECOLOGY PATIIENT IINFORMATIION SHEET FEMALE URINARY INCONTINENCE: WHAT IT IS AND WHAT YOU CAN DO ABOUT IT What is Urinary Incontinence? Stress Incontinence is a leakage of urine that occurs, for
URO-GYNECOLOGY PATIIENT IINFORMATIION SHEET FEMALE URINARY INCONTINENCE: WHAT IT IS AND WHAT YOU CAN DO ABOUT IT What is Urinary Incontinence? Stress Incontinence is a leakage of urine that occurs, for
Tension Free vaginal tape. Mrs Ami Shukla, Consultant Urogynaecologist Northampton General Hospital Northampton NN1 5BD
 Tension Free vaginal tape Mrs Ami Shukla, Consultant Urogynaecologist Northampton General Hospital Northampton NN1 5BD What is a TVT procedure? A TVT (Tension Free Vaginal Tape) procedure is an operation
Tension Free vaginal tape Mrs Ami Shukla, Consultant Urogynaecologist Northampton General Hospital Northampton NN1 5BD What is a TVT procedure? A TVT (Tension Free Vaginal Tape) procedure is an operation
TREATMENT METHODS FOR DISORDERS OF SMALL ANIMAL BLADDER FUNCTION
 Vet Times The website for the veterinary profession https://www.vettimes.co.uk TREATMENT METHODS FOR DISORDERS OF SMALL ANIMAL BLADDER FUNCTION Author : SIMONA T RADAELLI Categories : Vets Date : July
Vet Times The website for the veterinary profession https://www.vettimes.co.uk TREATMENT METHODS FOR DISORDERS OF SMALL ANIMAL BLADDER FUNCTION Author : SIMONA T RADAELLI Categories : Vets Date : July
Loss of Bladder Control
 BLADDER HEALTH Loss of Bladder Control Bladder Prolapse AUA FOUNDATION OFFICIAL FOUNDATION OF THE AMERICAN UROLOGICAL ASSOCIATION What Is the Bladder? The bladder is a hollow, balloon-like organ made mostly
BLADDER HEALTH Loss of Bladder Control Bladder Prolapse AUA FOUNDATION OFFICIAL FOUNDATION OF THE AMERICAN UROLOGICAL ASSOCIATION What Is the Bladder? The bladder is a hollow, balloon-like organ made mostly
Bill Landry BScPT, BScH, MCPA, CAFCI Family Physiotherapy Centre of London
 Bill Landry BScPT, BScH, MCPA, CAFCI blandry@fpclondon.com Family Physiotherapy Centre of London Objectives To describe the scope of post-prostatectomy incontinence To describe what s been done To provide
Bill Landry BScPT, BScH, MCPA, CAFCI blandry@fpclondon.com Family Physiotherapy Centre of London Objectives To describe the scope of post-prostatectomy incontinence To describe what s been done To provide
NEUROMODULATION FOR UROGYNAECOLOGISTS
 NEUROMODULATION FOR UROGYNAECOLOGISTS Introduction The pelvic floor is highly complex structure made up of skeletal and striated muscle, support and suspensory ligaments, fascial coverings and an intricate
NEUROMODULATION FOR UROGYNAECOLOGISTS Introduction The pelvic floor is highly complex structure made up of skeletal and striated muscle, support and suspensory ligaments, fascial coverings and an intricate
Tension-free Vaginal Tape (TVT)
") Page 1 of 7 Tension-free Vaginal Tape (TVT) Introduction This leaflet will provide you with basic information about the Tension--free Vaginal Tape (TVT) procedure. What is a TVT? TVT is an operation to
Page 1 of 7 Tension-free Vaginal Tape (TVT) Introduction This leaflet will provide you with basic information about the Tension--free Vaginal Tape (TVT) procedure. What is a TVT? TVT is an operation to
Using Physiotherapy to Manage Urinary Incontinence in Women
 Using Physiotherapy to Manage Urinary Incontinence in Women Bladder control problems are common, and affect people of all ages, genders and backgrounds. These problems are referred to as urinary incontinence
Using Physiotherapy to Manage Urinary Incontinence in Women Bladder control problems are common, and affect people of all ages, genders and backgrounds. These problems are referred to as urinary incontinence
A PATIENT GUIDE TO Understanding Stress Urinary Incontinence
 A PATIENT GUIDE TO Understanding Stress Urinary Incontinence Q: What is SUI? A: Stress urinary incontinence is defined as the involuntary leakage of urine. The problem afflicts approximately 18 million
A PATIENT GUIDE TO Understanding Stress Urinary Incontinence Q: What is SUI? A: Stress urinary incontinence is defined as the involuntary leakage of urine. The problem afflicts approximately 18 million
Latest Treatments for a Leaky Bladder None
 Latest Treatments for a Leaky Bladder None Financial Disclosures Jeremiah McNamara, MD, OBGYN Boulder Women s Care 303-500-1947 Boulder Women s Care Agenda: Prolapse & Urinary Incontinence The Pelvic Floor
Latest Treatments for a Leaky Bladder None Financial Disclosures Jeremiah McNamara, MD, OBGYN Boulder Women s Care 303-500-1947 Boulder Women s Care Agenda: Prolapse & Urinary Incontinence The Pelvic Floor
Neuropathic Bladder. Magda Kujawa Consultant Urologist Stockport NHS Foundation Trust 12/03/2014
 Neuropathic Bladder Magda Kujawa Consultant Urologist Stockport NHS Foundation Trust 12/03/2014 Plan Physiology- bladder and sphincter behaviour in neurological disease Clinical consequences of Symptoms
Neuropathic Bladder Magda Kujawa Consultant Urologist Stockport NHS Foundation Trust 12/03/2014 Plan Physiology- bladder and sphincter behaviour in neurological disease Clinical consequences of Symptoms
Incontinence; Lets talk about it. Karanvir Virk M.D. Minimally Invasive and Pelvic Reconstructive Surgery
 Incontinence; Lets talk about it Karanvir Virk M.D. Minimally Invasive and Pelvic Reconstructive Surgery Select the most appropriate subtitle for this talk A: Bladders gone wild! B: There s no such thing
Incontinence; Lets talk about it Karanvir Virk M.D. Minimally Invasive and Pelvic Reconstructive Surgery Select the most appropriate subtitle for this talk A: Bladders gone wild! B: There s no such thing
The Neurogenic Bladder
 The Neurogenic Bladder Outline Brandon Haynes, MD Resident Physician Department of Urology Jelena Svircev, MD Assistant Professor Department of Rehabilitation Medicine Anatomy and Bladder Physiology Bladder
The Neurogenic Bladder Outline Brandon Haynes, MD Resident Physician Department of Urology Jelena Svircev, MD Assistant Professor Department of Rehabilitation Medicine Anatomy and Bladder Physiology Bladder
Urinary Incontinence
 Urinary Incontinence Q: What is urinary incontinence and what causes it? A: When you are not able to hold your urine until you can get to a bathroom, you have what s called urinary incontinence (also called
Urinary Incontinence Q: What is urinary incontinence and what causes it? A: When you are not able to hold your urine until you can get to a bathroom, you have what s called urinary incontinence (also called
REVIEW OF CAUSES, EVALUATION, AND TREATMENTS URINARY INCONTINENCE 101
 REVIEW OF CAUSES, EVALUATION, AND TREATMENTS URINARY INCONTINENCE 101 March 5, 2014 Kevin E Miller, MD Department of Obstetrics and Gynecology University of Kansas School of Medicine- Wichita URINARY INCONTINENCE
REVIEW OF CAUSES, EVALUATION, AND TREATMENTS URINARY INCONTINENCE 101 March 5, 2014 Kevin E Miller, MD Department of Obstetrics and Gynecology University of Kansas School of Medicine- Wichita URINARY INCONTINENCE
Urogynecology in EDS. Joan L. Blomquist, MD Greater Baltimore Medical Center August 2018
 Urogynecology in EDS Joan L. Blomquist, MD Greater Baltimore Medical Center August 2018 One in three like me Voiding Issues Frequency/Urgency Urinary Incontinence neurogenic bladder Neurologic supply
Urogynecology in EDS Joan L. Blomquist, MD Greater Baltimore Medical Center August 2018 One in three like me Voiding Issues Frequency/Urgency Urinary Incontinence neurogenic bladder Neurologic supply
Management of OAB. Lynsey McHugh. Consultant Urological Surgeon. Lancashire Teaching Hospitals
 Management of OAB Lynsey McHugh Consultant Urological Surgeon Lancashire Teaching Hospitals Summary Physiology Epidemiology Definitions NICE guidelines Evaluation Conservative management Medical management
Management of OAB Lynsey McHugh Consultant Urological Surgeon Lancashire Teaching Hospitals Summary Physiology Epidemiology Definitions NICE guidelines Evaluation Conservative management Medical management
Voiding Diary. Begin recording upon rising in the morning and continue for a full 24 hours.
 Urodvnamics Your physician has scheduled you for a test called URODYNAMICS. This test is a series of different measurements of bladder function and can be used to determine the cause of a variety of bladder
Urodvnamics Your physician has scheduled you for a test called URODYNAMICS. This test is a series of different measurements of bladder function and can be used to determine the cause of a variety of bladder
Posterior intravaginal slingplasty for vault and uterovaginal prolapse: an initial experience
 Gynecol Surg (2006) 3: 88 92 DOI 10.1007/s10397-005-0168-7 ORIGINAL ARTICLE R. Oliver. C. Dasgupta. A. Coker Posterior intravaginal slingplasty for vault and uterovaginal prolapse: an initial experience
Gynecol Surg (2006) 3: 88 92 DOI 10.1007/s10397-005-0168-7 ORIGINAL ARTICLE R. Oliver. C. Dasgupta. A. Coker Posterior intravaginal slingplasty for vault and uterovaginal prolapse: an initial experience
Urogynecology Curriculum for the PGY III and IV Resident
 Urogynecology Curriculum for the PGY III and IV Resident Sinai Hospital of Baltimore Maryland Department of Obstetrics and Gynecology I. Educational Purpose: The dedicated Urogynecology rotation is intended
Urogynecology Curriculum for the PGY III and IV Resident Sinai Hospital of Baltimore Maryland Department of Obstetrics and Gynecology I. Educational Purpose: The dedicated Urogynecology rotation is intended
This information is intended as an overview only
 This information is intended as an overview only Please refer to the INSTRUCTIONS FOR USE included with this device for indications, contraindications, warnings, precautions and other important information
This information is intended as an overview only Please refer to the INSTRUCTIONS FOR USE included with this device for indications, contraindications, warnings, precautions and other important information
Questionnaire for Incontinent Patients
 Questionnaire for Incontinent Patients Name Date: Date of birth: weight: height: Vaginal deliveries: Caesarean Sections: profession: No Yes Sometimes Yes 50% or more Do you lose urine during sneezing or
Questionnaire for Incontinent Patients Name Date: Date of birth: weight: height: Vaginal deliveries: Caesarean Sections: profession: No Yes Sometimes Yes 50% or more Do you lose urine during sneezing or
Incontinence. When I was given this topic in urology to discuss with you today I
 Incontinence When I was given this topic in urology to discuss with you today I was slightly disappointed. I personally see mostly men for problems such as stones, benign prostatic hyperplasia, prostate
Incontinence When I was given this topic in urology to discuss with you today I was slightly disappointed. I personally see mostly men for problems such as stones, benign prostatic hyperplasia, prostate
Women s & Children s Directorate The TVT Operation - a guide for patients
 Women s & Children s Directorate The TVT Operation - a guide for patients This leaflet was written for women who are considering having a TVT operation. If you have any questions that aren't answered by
Women s & Children s Directorate The TVT Operation - a guide for patients This leaflet was written for women who are considering having a TVT operation. If you have any questions that aren't answered by
Urinary Incontinence
 Urinary Incontinence Millions of women experience involuntary loss of urine called urinary incontinence (UI). Some women may lose a few drops of urine while running or coughing. Others may feel a strong,
Urinary Incontinence Millions of women experience involuntary loss of urine called urinary incontinence (UI). Some women may lose a few drops of urine while running or coughing. Others may feel a strong,
Disease Management. Incontinence Care. Chan Sau Kuen Continence Nurse Consultant United Christian Hospital 14/11/09
 Disease Management in Incontinence Care Chan Sau Kuen Continence Nurse Consultant United Christian Hospital 14/11/09 What is incontinence? Definition of Incontinence - Is the compliant of any involuntary
Disease Management in Incontinence Care Chan Sau Kuen Continence Nurse Consultant United Christian Hospital 14/11/09 What is incontinence? Definition of Incontinence - Is the compliant of any involuntary
Lower Urinary Tract Symptoms (LUTS) and Nurse-Led Clinics. Sean Diver Urology Advanced Nurse Practitioner candidate Letterkenny University Hospital
 and Nurse-Led Clinics. Sean Diver Urology Advanced Nurse Practitioner candidate Letterkenny University Hospital") Lower Urinary Tract Symptoms (LUTS) and Nurse-Led Clinics Sean Diver Urology Advanced Nurse Practitioner candidate Letterkenny University Hospital 01/02/2018 Lower Urinary Tract Symptoms LUTS - one of
Lower Urinary Tract Symptoms (LUTS) and Nurse-Led Clinics Sean Diver Urology Advanced Nurse Practitioner candidate Letterkenny University Hospital 01/02/2018 Lower Urinary Tract Symptoms LUTS - one of
The Pelvic Floor Muscles - a Guide for Women
 The Pelvic Floor Muscles - a Guide for Women This booklet is supported by WWWWW Wellbeing of Women Registered Charity No. 239281 www.wellbeingofwomen.org.uk Introduction Up to a third of all women experience
The Pelvic Floor Muscles - a Guide for Women This booklet is supported by WWWWW Wellbeing of Women Registered Charity No. 239281 www.wellbeingofwomen.org.uk Introduction Up to a third of all women experience
Pelvic Floor Disorders. Amir Darakhshan MD FRCS (Gen Surg) Consultant Colorectal and General Surgeon
 Consultant Colorectal and General Surgeon") Pelvic Floor Disorders Amir Darakhshan MD FRCS (Gen Surg) Consultant Colorectal and General Surgeon What is Pelvic Floor Disorder Surgical perspective symptoms of RED, FI or prolapse on the background
Pelvic Floor Disorders Amir Darakhshan MD FRCS (Gen Surg) Consultant Colorectal and General Surgeon What is Pelvic Floor Disorder Surgical perspective symptoms of RED, FI or prolapse on the background
Clean Intermittent Self-Catheterisation (CISC)
") Saint Mary s Hospital & Trafford General Hospital Uro-gynaecology Service Information for Patients Clean Intermittent Self-Catheterisation (CISC) What is catheterisation? Catheterisation involves passing
Saint Mary s Hospital & Trafford General Hospital Uro-gynaecology Service Information for Patients Clean Intermittent Self-Catheterisation (CISC) What is catheterisation? Catheterisation involves passing
Glossary of terms Urinary Incontinence
 Patient Information English Glossary of terms Urinary Incontinence Anaesthesia (general, spinal, or local) Before a procedure you will get medication to make sure that you don t feel pain. Under general
Patient Information English Glossary of terms Urinary Incontinence Anaesthesia (general, spinal, or local) Before a procedure you will get medication to make sure that you don t feel pain. Under general
Stress Incontinence. Susannah Elvy Urogynaecology CNS
 Stress Incontinence Susannah Elvy Urogynaecology CNS Definitions Prevalence Assessment Investigation Treatment Surgery Men International Continence Society define as the complaint of any involuntary leakage
Stress Incontinence Susannah Elvy Urogynaecology CNS Definitions Prevalence Assessment Investigation Treatment Surgery Men International Continence Society define as the complaint of any involuntary leakage
Diane K. Newman DNP, ANP-BC, PCB-PMD, FAAN
 Diane K. Newman DNP, ANP-BC, PCB-PMD, FAAN Diane K. Newman, DNP is a Biofeedback Certified Continence Specialist. With over 35-years experience, she is an expert in the assessment and management of pelvic-floor
Diane K. Newman DNP, ANP-BC, PCB-PMD, FAAN Diane K. Newman, DNP is a Biofeedback Certified Continence Specialist. With over 35-years experience, she is an expert in the assessment and management of pelvic-floor
Pregnancy related pelvic floor dysfunction- suggested teaching presentation for Midwives
 Pregnancy related pelvic floor dysfunction- suggested teaching presentation for Midwives 1 Aims of this self assessment competency To equip Midwives with the knowledge and skills to teach pelvic floor
Pregnancy related pelvic floor dysfunction- suggested teaching presentation for Midwives 1 Aims of this self assessment competency To equip Midwives with the knowledge and skills to teach pelvic floor