Neuro-urology for the Urogynaecologist and urologist W20, 15 October :00-18:00
|
|
|
- Lynette Morrison
- 5 years ago
- Views:
Transcription
1 Neuro-urology for the Urogynaecologist and urologist W20, 15 October :00-18:00 Start End Topic Speakers 14:00 14:05 Introduction to the Workshop Sohier Elneil 14:05 14:25 Neurology of the Bladder and the Pelvic Floor Daniel Engeler 14:25 14:45 Bladder Symptoms and their Assessment in the Michele Spinelli Neurological Patient 14:45 15:05 Pelvic Floor Dysfunction and its Assessment in the Alex Digesu Neurological Patient 15:05 15:20 Chronic Pelvic Pain in the Neurological Patient Daniel Engeler 15:20 15:30 Discussion All 15:30 16:00 Break None 16:00 16:30 Indications and Limitations of Botulinum Toxin in the Rizwan Hamid Neurogenic Bladder and Pelvic Floor 16:30 17:00 Indications and Limitations Neuromodulations Alex Digesu (PTNS) in the Neurogenic Bladder and Pelvic Floor 17:00 17:10 Discussion All 17:10 17:40 Indications and Limitations of Neurmodulation Michele Spinelli (SNM) in Neurogenic Bladder 17:40 17:50 SNM in Pelvic Floor Disorders Sohier Elneil 17:50 18:00 Discussion All Aims of course/workshop Aims and Objectives: -Current concepts relating to the neurological control of the bladder and the pelvic floor. -Urinary and pelvic floor symptoms in patients with cerebral lesions, multiple sclerosis, Parkinson's disease, spinal cord injury and cauda equina -Urinary and pelvic floor symptoms in bladder pain syndrome/ic and chronic pelvic pain syndromes (neurological basis of disease). -Investigating neurogenic bladder and pelvic floor dysfunction -Innovative therapies in treating neurogenic bladder and pelvic floor disorders: Indications and limitations of botulinum toxin -Innovative therapies in treating neurogenic bladder and pelvic floor disorders: Indications and limitations of neuromodulation Educational Objectives This workshop will provide a fresh approach to the understanding of the neurological basis of bladder and pelvic floor conditions encountered in urogynaecology and urology. All the speakers have worked extensively in this field and have published widely on the subject matter. Some knowledge of the neurological causes of bladder and pelvic floor dysfunction is essential for the general urogynaecologist and urologist. Patients with neurological disease are referred to both sets of clinicians for advice regarding their bladder and pelvic floor management. It is important to have an understanding of the nature of their neurology, especially when planning medical or surgical management. In addition, clinicians need to know what may be the presenting uro-genital symptoms of a patient with a neurological condition, and the minimal neurological examination necessary for recognising an underlying neurological problem. The areas covered in this workshop will help clinicians understand the neurological patient with bladder and pelvic floor dysfunction better. The speakers will discuss patient assessment, investigations and provide algorithms for managing this group of complex patients.
2 NEURO-UROLOGY FOR THE UROGYNAECOLOGIST AND UROLOGIST Chairman: Sohier Elneil Introduction The pelvic floor is highly complex structure made up of skeletal and striated muscle, support and suspensory ligaments, fascial coverings and an intricate neural network. Its dual role is to provide support for the pelvic viscera (bladder, bowel and uterus) and maintain functional integrity of these organs. In order to maintain good pelvic floor function, this elaborate system must work in a highly integrated manner. When this is system if damaged, either directly or as a consequence of an underlying neurological condition, pelvic floor failure ensues along with organ dysfunction. The aetiology is inevitably multi-factorial, and seldom as a consequence of a single aetiological factor. It can affect one or all three compartments of the pelvic floor, often resulting in prolapse and functional disturbance of the bladder (urinary incontinence and voiding dysfunction), rectum (faecal incontinence), vagina and/or uterus (sexual dysfunction). This compartmentalisation of the pelvic floor has resulted in the partitioning of patients into urology, gynaecology, colo-rectal surgery or neurology, depending on the patients presenting symptoms. In complete pelvic floor failure, all three compartments are inevitably damaged resulting in apical prolapse, with associated organ dysfunction. It is clear that in this state, the patient needs the clinical input of at least two of the three pelvic floor clinical specialities. Whilst the primary clinical aim is to correct the anatomy, it must also be to preserve or restore pelvic floor function. As a consequence, these patients need careful clinical assessment, appropriate investigations, and counselling before embarking on a welldefined management pathway. The latter includes behavioural and lifestyle changes, conservative treatments, pharmacotherapy, minimally invasive surgery, and radical specialised surgery. It is not surprising that in this complex group of patients, a multidisciplinary approach is not
3 only necessary, but critical, if good clinical care and governance is to be ensured. But it is of significant import that one has a good understanding of the neurology of the pelvis and its organs. Neural control of uro-genital system Voluntary control over the uro-genital system is critical to our social existence. Since its peripheral innervation derives from the most distal segments of the spinal cord, integrity of the long tracts of the central nervous system for physiological function is immediately apparent. In a survey of the site of the underlying neurological disease affecting a sample of patients referred to the department with bladder symptoms, spinal cord involvement of various pathologies was found to be the commonest cause of bladder symptoms. Because of the commonality of innervation shared by the bladder and genital organs, it might be expected that abnormalities of these two systems inevitably occur together. This however is not the case because although the organs share the same root innervation and have common peripheral nerves within the pelvis, each is controlled by its own unique set of central nervous system reflexes. In this workshop, a brief account of the neurophysiological control of the bladder and pelvic is given initially, followed by a description of the effect that neurological disease at different levels of the nervous system may have and finally the management of those conditions. The bladder performs only two functions - storage and voiding of urine- and the modern view of the control of these two mutually exclusive activities is that whereas storage is organised within the spinal cord, micturition results from activation by suprapontine influences of a centre in the dorsal tegmentum of the pons, the pontine micturition centre (PMC). In neurological disease, this delicate interaction can be severely disrupted, and manifests as a disorder of voiding or storage depending on the condition such as multiple sclerosis,
4 Parkinson's disease, multiple system atrophy and others. But commonly, it is direct injury to pelvic nerves that can give rise to quite marked bladder and pelvic floor dysfunction. The peripheral innervation of the pelvic organs can be damaged by extirpative pelvic surgery such as resection of rectal carcinoma, radical prostatectomy, or radical hysterectomy. The dissection necessary for rectal cancer is likely to damage the parasympathetic innervation to the bladder and genitalia, as the pelvic nerves take a medio-lateral course through the pelvis either side of the rectum and the apex of the prostate. The nerves may either be removed together with the fascia which covers the lower rectum or may be damaged by a traction injury as the rectum is mobilized prior to excision. Urinary incontinence following a radical prostatectomy or a radical hysterectomy which includes the upper part of the vagina, is probably also due to damage to the parasympathetic innervation of the detrusor and in the case of a radical prostatectomy, there may be additional direct damage to the innervation of the striated urethral sphincter The focus in the literature tends to focus on the effects of neurological disease on the bladder tends, but other pelvic floor effects should not be ignored, such as pelvic organ prolapse, pain syndromes and sexual dysfunction. Therapies to manage these conditions depend on a multi-disciplinary approach. This workshop will help guide practitioners on how to maximise the therapeutic options for their patients. Aims and Objectives of the Workshop
5 Current concepts relating to the neurological control of the bladder and the pelvic floor. Urinary and pelvic floor symptoms in patients with cerebral lesions, multiple sclerosis, Parkinson's disease, spinal cord injury and cauda equine Urinary and pelvic floor symptoms in bladder pain syndrome/ic and chronic pelvic pain syndromes (neurological basis of disease). Investigating neurogenic bladder and pelvic floor dysfunction Innovative therapies in treating neurogenic bladder and pelvic floor disorders: Indications and limitations of botulinum toxin Innovative therapies in treating neurogenic bladder and pelvic floor disorders: Indications and limitations of neuromodulation Neurology of the bladder and the pelvic floor (Daniel Engeler) Voluntary control of micturition is based on a complex neural circuitry highly distributed on different levels of the nervous system. A variety of neurotransmitters are involved in signalling of neural control. Understanding the pathways involved at the level of the brain, the spinal cord and the peripheral nervous system as well as the peripheral organ is important for the physician diagnosing and treating patients with neurogenic bladder and pelvic floor dysfunction. Diseases or injuries to this complex system may lead to abnormal function of the end organs, i.e. leading to pathologic storage or release of urine. Disruption of the normal neural pathways has different specific functional consequences in the lower urinary tract as well as the pelvic floor. Cerebral lesions, multiple sclerosis, Parkinson s disease and trauma to the nervous system at different levels, such as the brain, spinal cord, or cauda equina are therefore followed by a variety of functional disturbances, which can be derived from the pathways involved. Both, current concepts relating to the normal neurological control of the bladder and the pelvic floor, as well as disease or trauma specific pathologies are discussed here.
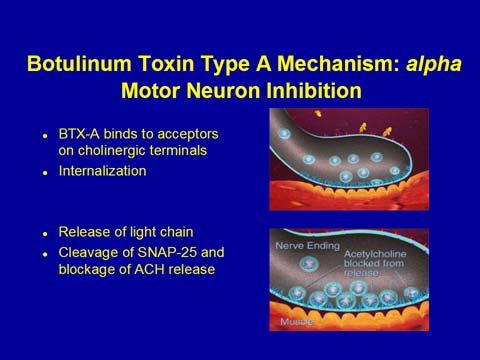
6 Bladder Symptoms and its Assessment in the Neurological Patient (Michele Spinelli) To be discussed in the workshop Pelvic Floor Dysfunction and its Assessment in the Neurological Patient (Alex Digesu) To be discussed in the workshop Neurological Aspects in Chronic Pelvic Pain (Daniel Engeler) A number of well-defined conditions may cause chronic pelvic pain in women, such as endometriosis, infection, or gynaecological malignancies. Indeed, many of the patients suffering from chronic pelvic pain (CPP) will not be found to have well-defined conditions as a treatable cause. The main focus for CPP in the past has been on pelvic end-organs, whereas research on chronic pain states has shown, many of the important mechanisms involved are based within the central nervous system. In this part of the workshop, urinary and pelvic floor symptoms in bladder pain syndrome/interstitial cystitis and chronic pelvic pain syndromes are discussed and relevant neurological aspects of the disease are highlighted. Indications and Limitations of Botulinum Toxin in Neurogenic Bladder and Pelvic Floor Disorders (Rizwan Hamid)


7


8

9
10
11
, anal incontinence and sexual dysfunctions are")
.")


12 Indications and Limitations Neuromodulation (PTNS) in the Neurogenic Bladder and Pelvic Floor (Alex Digesu) Pelvic floor disorders such as lower urinary tract symptoms (LUTS), anal incontinence and sexual dysfunctions are common disorders occurring in about 80% of neurogenic patients. Urgency represents the most bothersome LUTS and severely affects the quality of life (QOL). Neurogenic detrusor overactivity, detrusor sphincter dyssynergia and/or detrusor underactivity are the most common cause of LUTS in neurogenic patients. These bladder abnormalities tend to become more severe with the progression of the disease leading to voiding difficulties, urinary retention, recurrent urinary tract infections and need of clean intermittent self catheterization. Drugs, surgery and repeated intradetrusor injections of botulinum toxin have been suggested as therapeutic options. However, neurological patients
13 often fail to respond to drug therapy, report intolerable side effects and/or are reluctant to invasive surgical treatment. Neuromodulation is a mechanism by which the nervous system regulates electrical impulses flowing through neural tissues. Percutaneous tibial nerve stimulation (PTNS), a new minimally invasive neuromodulation technique, is able to modify the lower urinary tract behaviour by inhibiting involuntary detrusor contractions in patients with both neurogenic and idiopathic detrusor overactivity in an outpatient setting. PTNS has been demonstrated to be an effective, safe and well tolerated treatment in neurogenic patients affected by LUTS and unresponsive to anticholinergic drugs. Both subjective and objective improvement have been reported. A statistically significant improvement of patient perception of bladder condition, overactive bladder (OAB) symptoms, mean voided volume per micturition, post micturition residual and QOL parameters have been reported. Previous studies have also showed that PTNS is effective to suppress detrusor overactivity in MS patients. Usually pharmacological agents with a predominant anticholinergic action are widely used as first line treatment of LUTS in patients with neurogenic bladder. However, the effectiveness of these treatments has been evaluated in non-neurogenic patients and their applicability to patients with OAB syndrome and neurogenic patients is not known. In neurogenic patients OAB symptoms more difficult to manage and the symptoms themselves can exacerbate fatigue and increase disability. In addition, placebo controlled trials in more disabled populations where multiple factors can contribute to the production of urinary symptoms have not found the older anticholinergic agents to be effective due to side effects. Peters et al. compared in a randomized, multicenter, controlled study the effectiveness of PTNS to extended-release tolterodine. The study demonstrated that subject assessment of OAB symptoms compared to baseline was statistically significant in the PTNS arm with 79.5%
14 reporting cure or improvement compared to 54.8% of subjects on tolterodine (p < 0.01), without significant side effects. Based on these results, PTNS may be considered a clinically significant alternative therapy for OAB in those patients who do not respond to pharmacological therapy. The mechanism of action of PTNS is not completely understood yet. Long-latency somatosensory evoked potentials (LL-SEP) are well known to reflect information processing in the brain after stimulation of peripheral somatosensory system. Some authors found a modification of brain activity after PTNS and speculated that its efficacy is mediated by sacral and suprasacral centres of stimulus elaboration involving cortical associative areas. Considering its high safety, ease of use, lack of side effects and office-based convenience, PTNS could be consider as an ideal alternative treatment for neurogenic patients suffering from LUTS, expecially taking into account the lack of scientific evidence of anticholinergic efficacy in this group of patients. PTNS has been also demonstrated to be clinically effective in the treatment of Anal incontinence which is commonly associated to LUTS in neurogenic patients. The role of PTNS in the treatment of sexual dysfunctions has been suggested and speculated by some authors but it has not been demonstrated yet. The main limitation of PTNS is the longevity of action. In addition it is a time consuming treatment which requires dedicated personnel. Indications and Limitations in Neuromodulation (SNM) in Neurogenic Bladder (Michele Spinelli) The pelvic floor plays an important role in the urine storage, voiding, urine continence, anal continence to gas and feces, defecation and sexual activity. All these pelvic organ functions
15 are controlled by nervous pathways that involve neurons in the motor cortex of the brain, spinal cord and peripheral ganglia. In neurological diseases the alteration of these nervous pathways are responsible of the lack of coordination between the urinary bladder, urethra, rectum and pelvic floor muscle (PFM) leading to pelvic floor dysfunction (PFD). Symptoms commonly reported by patients with neurological diseases include urinary incontinence (37 70%), constipation (29 67%), and in men erectile dysfunction (40 60%). This indicates that the central nervous system is involved both in motor and autonomic pelvic functions. The pathogenesis of PFD in patients with neurological lesions is an active area of research. However, it is still unknown whether PFD are caused by lesions of the central nervous system or peripheral nerves. It has also been demonstrated that the prevalence of bladder and bowel dysfunction increased with the severity of the illness. Sakakibara et al., showed that the majority of patients with Parkinson s disease experienced pelvic organ dysfunction onset after the appearance of motor disorder. The most striking feature of bladder dysfunction in the Parkinson s disease patients is filling phase disorder and urinary incontinence. It has been suggested that in those patients, the decrease in central dopaminergic neurons (D1), which regulate the pontine micturition center, is responsible of detrusor hyperreflexia.
16 Voiding phase disorder is another feature seen in Parkinson s disease patients due to detrusor-sphincter dyssynergia. This disorder may be caused by peripheral a-adrenergic stimulation by anti-parkinsonian drugs such as levodopa or its metabolites. However, the effect of dopaminergic drugs on parkinsonian bladder shows conflicting results. In some reports, the use of apomorphine, levodopa, pergolide produced a lessening of detrusor hyperreflexia whereas in others, it provided amelioration of voiding difficulty. The most common bowel dysfunction in Parkinson s disease patients are constipation and prolonged colorectal transit time, difficulty in expulsion and paradoxical contraction of the puborectal muscle. These symptoms probably, reflect abnormalities in the colon and anorectum. Experimental study findings showed that a decreased intestinal motility occurs when there is a reduction in the number of central dopaminergic neurons, which modulate the pontine defecation centre. Other possible causes are peripheral nerve lesions or overextension injury secondary to faecal impaction. Sexual dysfunction is also very common in both men and women with Parkinson s disease. However, the mechanism of sexual dysfunction is less clear than that of bladder and bowel dysfunction. Whereas motor disorder, pain, and depression may affect sexual function, there is little evidence that autonomic dysfunction contributes to sexual dysfunction in those patients. Experimental studies have shown that the key area for sexual function is in the hypothalamus and particularly the medial preoptic area and paraventricular nucleus. People with multiple sclerosis experience high levels of sexual dysfunction which are mainly represented by hypoactive sexual behaviour, lack of sexual interest, decreased libido, often with problems in orgasmic capacity. Fatigue, spasticity, muscular weakness, bladder problems, pain, cognitive and behavioural changes also has an important impact on sexual dysfunction.
17 Different neurophysiological tests have been proposed in order to assess the direct and reflex responses to the pelvic floor. These include: the pudendoanal reflex, the bulbocavernosus reflex, the pudendal nerve terminal motor latency (PNTML). The cutaneoanal reflex and other somatosomatic and viscero-somatic reflexes have limited usefulness in pelvic floor investigations due to a large variability in the latency of these responses. The more commonly used electrophysiological investigations to investigate the integrity of the sacral reflex arc supplying pelvic floor muscle function are the PNTML and the sacral reflexes. These last tests can be elicited by mechanical, electrical or magnetic stimulation and involve the whole reflex arc, but do not differentiate the afferent and efferent branch of the reflex. The PNTML only explores the more distal portion of pudendal nerve, not looking at the portion of the nerve proximal to the site of the stimulation induced by the St. Mark s electrode. More recently, Fowler et al. described direct and reflex responses after S3 root stimulation, introducing wire electrode close to S3 sacral root. Direct motor and reflex responses from the external anal sphincter (EAS) by S3 electrical stimulation can provide valuable information on the functional integrity of the sacral reflex pathway, but differently from the pudendoanal and bulbocavernosus reflexes, can distinguish the efferent limb of the reflex pathway from the whole arc. EAS responses during S3 percutaneous electrical stimulation are easy to perform, not invasive neither too painful thus representing a useful electrophysiological technique for the selection of candidates to sacral nerve modulation (SNM). The EAS responses following the
18 stimulation of the same S3 fibres used for SNM, contribute to evaluate the functional integrity of the efferent branch of pudendal nerve and to exclude lesions at the sacral S2-S4 central cord levels. SNM in Pelvic Floor Disorders (Sohier Elneil) Electrical neuromodulation of the lower urinary tract began over a century ago, but it was the pioneering work of Tanagho and Schmidt at the University of California in the late 1980s that demonstrated electrical activation of efferent fibres to the striated urethral sphincter inhibited detrusor contractions [1]. Stimulation of the third sacral root (S3) has been shown to be effective in stimulating the urethral sphincter [2]. A large multicentre (Medtronic MDT USA, Canada and Europe) prospective randomised clinical trial was set up to look at efficacy and safety of chronic neuromodulation to the S3 nerve. Results of this study led to approval by the Food and Drugs Administration in October Over 25,000 neuromodulators (Interstim and Interstim II, Medtronic Inc, Minnesota, Minneapolis, USA) have so far been implanted for approved urinary indications, including functional non-neurogenic urinary retention or chronic urinary retention and voiding dysfunction secondary to urethral sphincter overactivity (Fowler s syndrome) [3, 4].. Indeed, SNM has been shown to be the only effective therapy in women with these conditions. Mechanism of Action in Urinary Retention Sacral neuromodulation restores voiding in women with chronic urinary retention [5], probably by resetting brainstem function [6]. SNM was first described as a treatment for urinary retention in the mid-1990s. At the time, SNM was introduced for the management of bladder dysfunction, paradoxically both intractable incontinence and retention. The first stage of SNM was an initial test procedure, known as a percutaneous nerve evaluation test (PNE) which if found to be positive and restore voiding ability, was followed by the implantation of a permanent sacral electrode. Success rates for women with retention for this
19 method were reported at 40 50% for the PNE, with approximately 60% voiding to completion with formal implantation [7], [8]. In the Department of Uro-neurology at the National Hospital for Neurology and Neurosurgery in London, the author s experience has been comparable, with two thirds of patients continuing to void without need for catheterization at a follow up of 5 years [9]. A retrospective study of 247 women referred to our Department, with urinary retention over a 4-year period showed that Fowler s syndrome is the commonest diagnosis although this only accounts for 58 %. In 32% no diagnosis could be made but in 2% there was a history of chronic opiate ingestion [10]. In 3% of the patients there appeared to be a relationship with chronic idiopathic pseudo-obstruction (CIPO), a rare disorder characterised by severe and chronic constipation without any demonstrable anatomical or mechanical lesion but thought to be due to a visceral neuropathy or myopathy (in infants or children) [11]. In men, there is an uncommon condition where painless urinary retention is present but it is not associated with constipation, and sexual function is preserved, but in whom extensive investigation fails to reveal any underlying abnormality. It has been speculated that this disorder is due to some abnormality of the intrinsic afferent innervation, possibly loss of the myofibroblast or interstitial cell, thought to be an integral part of the bladder stretch sensing mechanism [12] although no proof of that exists as yet. Presumably, this same condition makes up a proportion of the women with unexplained urinary retention. Though the mechanism of action of SNM remains indeterminate, there are various theories based on careful observations. Two components have been identified (i) activation of efferent fibres to the urethral sphincter with negative feedback to the bladder (pro-continence reflex) and (ii) activation of sacral spinal afferents resulting in inhibitory reflex efferent activity to the bladder. Reflex pathways at the spinal cord and supra spinal levels are thought to be modulated to achieve these effects [13, 14]. The prolonged beneficial effects of the stimulator, after it is switched off, support this observation. In urinary retention, SNM is
20 postulated to interfere with the inhibitory afferent activity arising from the urinary sphincter and thus restoring the sensation of bladder filling and the ability to void [4]. At a central level, decreases in regional cerebral blood flow measured by PET scanning was demonstrated in the cingulate gyrus, orbitofrontal cortex, midbrain and adjacent midline thalamus in chronically implanted patients with urge incontinence [13]. SNM appears to restore activity associated with brainstem auto regulation and attenuation of cingulate activity [14, 15], critical to bladder function. Historically, the management of urinary incontinence and retention, with SNM has classically been with successful pre-test stage using percutaneous nerve evaluation before permanent implantation. Success rates with this method have been reported at 40 50% [8, 16] for the PNE and approximately 60% voided to completion with formal implant and a further 14% reported significant improvement at 18 months our results show that a two third of patients continue to void without catheterization at a mean follow up of 5 years [17] and 78% at a mean follow-up of 10 years [18]. The relatively low success rate of the PNE and single stage implant has led to the development of the staged implant, whereby the permanent tined lead is inserted and a prolonged external stimulation period is assessed [19], if successful then the permanent IPG is implanted. Early reported results with this technique show 80% success rates [19, 20]. A pilot prospective randomised controlled trial comparing the 1-stage to the 2-staged shows a higher success rate for the staged operation. [21]. Results from our department are in line with these reports. Our Department has previously reported on the traditional implantation technique that was used first at our unit using a one-stage procedure [3], preceded by a PNE. This took place until August 2004, until the author took over the programme for the hospital. The PNE was a way of evaluating the success of the final implant without the cost and trauma of the final implant and surgery respectively. The testing wire would remain in place for up to 7 days and
21 if patients reported at least a 50% improvement in their symptoms and their bladder diary confirmed this, they would go on to have a permanent lead and stimulator. The disadvantage of the PNE was the rather variable success rate of 24-75% [8, 19, 21-26]. Although these patients were labelled as non-responders, the real reason for a proportion was dislodgement of the testing wire from the original optimum position close to the sacral branches of the pelvic plexus or pudendal nerve. Sacral radiographs often demonstrated that the wire had moved or was out of the foramen completely. In previous reports of this technique there were several drawbacks noted, as up to 40% of patients who responded to the temporary PNE, did not void on insertion of the permanent electrode. A possible reason for this is that the site of permanent electrode implantation may have differed from that of the successful PNE electrode [27]. Conversely the PNE temporary electrode may not be optimally placed leading to failure and patients not proceeding to permanent implantation [23]. In 1997, Janknegt et al., suggested the implantation of the permanent standard electrode in patients with a strong suggestive history, in whom the PNE failed [23]. In 2000 the two-stage percutaneous minimally invasive technique came into its own with the emergence of the self-securing tined electrode [8, 23]. This has a longer test phase to evaluate the procedure. Early data suggested that this has a higher success rate than the one-stage procedure of up to 80% [20, 21] and this has been our adopted method since Using a percutaneous technique, fluoroscopic guidance, and local or general anaesthesia a permanent electrode is implanted as the first stage, and connected to a temporary external battery. If the first stage fails, the electrode can be removed. It is the authors belief that the two-stage technique overcomes problems with PNE lead migration. It helps clinicians decide which patients should go on to have a permanent battery. The average battery life with
22 Interstim and Interstim II is around 8 and 5 years, respectively, but this varies with the settings used [28]. SNM is not without its complications and need for revision surgery. Therefore, it is important that patients are counselled regarding failure of the procedure (25%), the significant revision rate (30-50%), and the risk of box site pain, sciatica and nerve injury (very low). At 10 year follow-up at the National Hospital for Neurology and Neurosurgery, 78% of the patients who previously had significant impairment or inability to void, were able to void [10, 18]. Despite proven efficacy the procedure is not without a significant complication rate both at our and other centres using the same technique [3, 29]. This includes lead migration, pain at the Implantable Pulse Generator (IPG) site, leg pain, infection and failure of the device over time. This finding is confirmed by other studies which reported an incidence of 11% in lead migration [15] and 20% in lead breakages[27, 28]. Siegel et al. summarised their adverse events in the 219 patients who underwent implantation of the Interstim IPG and the most common complaint was pain at the IPG site in 15.3% of patients [26]. The surgical revision rate was 33%. Everaert et al. reported a 34% device related pain rate, with a 23% surgical revision rate [30]. Grunewald et al. reported a revision rate of 30% over 4 years. Lead migration was noted as 5.4% and IPG site pain as 8.1% [31]. Recently authors have reported much higher long term revision rates with 54% [3], 48.3% [28] and 43.9% [32] excluding normal battery changes. Similar results were obtained in a worldwide SNM clinical study in voiding dysfunction, carried out by Van Kerrebrock (2007) and colleagues [33]. The most important determinant of success, in women with chronic urinary retention or other pelvic floor symptoms (including pelvic pain syndromes, sexual dysfunction and bowel dysfunction) is the careful selection of the patient. This includes a urological and gynaecological history, pelvic examination to rule out surgical correctable causes and urine assessment to rule out infection and haematuria. We advocate the use of frequency-volume charts, urodynamic evaluation where indicated, post void residuals if they are able to void at
23 all and quality of life questionnaires to qualify the degree of improvement before and after the procedure. In the last decade there has been a plethora of innovative neuromodulation devices for treatment of lower urinary tract symptoms and pelvic floor dysfunction, though sacral neuromodulation remains the most widely used form of peripheral neuromodulation. In this workshop, a review of the role of pudendal neuromodulation, percutaneous tibial nerve stimulation and sacral dermal neuromodulation devices will also be considered. Their place in an algorithm of bladder and pelvic floor management will be devised. Take Home Message -Neurological basis of bladder and pelvic floor dysfunction is essential to all practitioners -In neurological patients, practitioners should investigate all aspects of bladder and pelvic floor dysfunction -Different therapeutic options should be made available and discussed with all patients References 1. Tanagho, E.A. and R.A. Schmidt, Electrical stimulation in the clinical management of the neurogenic bladder. J Urol, (6): p Tanagho, E.A., R.A. Schmidt, and B.R. Orvis, Neural stimulation for control of voiding dysfunction: a preliminary report in 22 patients with serious neuropathic voiding disorders. J Urol, (2 Pt 1): p Dasgupta, R., et al., Long-term results of sacral neuromodulation for women with urinary retention. BJU Int, (3): p Swinn, M.J., et al., Sacral neuromodulation for women with Fowler's syndrome. Eur Urol, (4): p
24 5. Swinn, M.J., et al., Sacral neuromodulation for women with Fowler's syndrome. European Urology, : p DasGupta, R., et al., Changes in brain activity following sacral neuromodulation for urinary retention. Journal of Urology, In Press 7. Jonas, U., et al., Efficacy of sacral nerve stimulation for urinary retention: results 18 months after implantation. Journal of Urology, : p Scheepens, W.A., et al., Long-term efficacy and safety results of the two-stage implantation technique in sacral neuromodulation. BJU Int, (9): p Dasgupta, R., et al., Long-term results of sacral neuromodulation for women with urinary retention. BJU Int, (3): p Kavia, R.B., et al., Urinary retention in women: its causes and management. BJU Int, (2): p Lapointe, S.P., et al., Urological manifestations associated with chronic intestinal pseudo-obstructions in children. J Urol, (4 Pt 2): p Wiseman, O.J., C.J. Fowler, and D.N. Landon, The role of the human bladder lamina propria myofibroblast. British Journal of Urology International, : p Blok, B.F., et al., Different brain effects during chronic and acute sacral neuromodulation in urge incontinent patients with implanted neurostimulators. BJU Int, (6): p Dasgupta, R., et al., Changes in brain activity following sacral neuromodulation for urinary retention. J Urol, (6): p Blok B, et al., Brain plasticity and urge incontinence:pet studies during the first hours of sacral neuromodulation. Neurourology and Urodynamics, (5). 16. Jonas, U., et al., Efficacy of sacral nerve stimulation for urinary retention: results 18 months after implantation. J Urol, (1): p Kavia, R.B.C., et al. Sacral Neuromodulation for women with urinary retention: Long term results for the first 30 patients. in BAUS Glasgow.
25 18. Datta, S.N., et al., Sacral neurostimulation for urinary retention: 10-year experience from one UK centre. BJU Int, (2): p Spinelli, M., et al., New sacral neuromodulation lead for percutaneous implantation using local anesthesia: description and first experience. J Urol, (5): p Kessler, T.M., H. Madersbacher, and G. Kiss, Prolonged sacral neuromodulation testing using permanent leads: a more reliable patient selection method? Eur Urol, (5): p Everaert, K., et al., A prospective randomized trial comparing the 1-stage with the 2- stage implantation of a pulse generator in patients with pelvic floor dysfunction selected for sacral nerve stimulation. Eur Urol, (5): p Borawski, K.M., et al., Predicting implantation with a neuromodulator using two different test stimulation techniques: A prospective randomized study in urge incontinent women. Neurourol Urodyn, (1): p Janknegt, R.A., E.H. Weil, and P.H. Eerdmans, Improving neuromodulation technique for refractory voiding dysfunctions: two-stage implant. Urology, (3): p Scheepens, W.A., et al., Predictive factors for sacral neuromodulation in chronic lower urinary tract dysfunction. Urology, (4): p Shaker, H. and M.M. Hassouna, Sacral root neuromodulation in the treatment of various voiding and storage problems. Int Urogynecol J Pelvic Floor Dysfunct, (5): p Siegel, S.W., et al., Long-term results of a multicenter study on sacral nerve stimulation for treatment of urinary urge incontinence, urgency-frequency, and retention. Urology, (6 Suppl 1): p Bosch, J.L. and J. Groen, Sacral nerve neuromodulation in the treatment of patients with refractory motor urge incontinence: long-term results of a prospective longitudinal study. J Urol, (4): p
26 28. van Voskuilen, A.C., et al., Long term results of neuromodulation by sacral nerve stimulation for lower urinary tract symptoms: a retrospective single center study. Eur Urol, (2): p Swinn, M.J., et al., Leg pain after sacral neuromodulation: anatomical considerations. BJU Int, (9): p Everaert, K., et al., Patient satisfaction and complications following sacral nerve stimulation for urinary retention, urge incontinence and perineal pain: a multicenter evaluation. Int Urogynecol J Pelvic Floor Dysfunct, (4): p ; discussion Grunewald, V., et al., Sacral electrical neuromodulation as an alternative treatment option for lower urinary tract dysfunction. Restor Neurol Neurosci, (2-3): p Elhilali, M.M., et al., Sacral neuromodulation: long-term experience of one center. Urology, (6): p van Kerrebroeck, P.E., et al., Results of sacral neuromodulation therapy for urinary voiding dysfunction: outcomes of a prospective, worldwide clinical study. J Urol, (5): p

27 Notes Record your notes from the workshop here
NEUROMODULATION FOR UROGYNAECOLOGISTS
 NEUROMODULATION FOR UROGYNAECOLOGISTS Introduction The pelvic floor is highly complex structure made up of skeletal and striated muscle, support and suspensory ligaments, fascial coverings and an intricate
NEUROMODULATION FOR UROGYNAECOLOGISTS Introduction The pelvic floor is highly complex structure made up of skeletal and striated muscle, support and suspensory ligaments, fascial coverings and an intricate
Neuromodulation and the pudendal nerve
 Neuromodulation and the pudendal nerve Stefan De Wachter, MD, PhD, FEBU Professor of Urology University of Antwerpen, Belgium Chairman dept of Urology, UZA Disclosures Consultant speaker: Astellas, Medtronic,
Neuromodulation and the pudendal nerve Stefan De Wachter, MD, PhD, FEBU Professor of Urology University of Antwerpen, Belgium Chairman dept of Urology, UZA Disclosures Consultant speaker: Astellas, Medtronic,
Sacral neuromodulation for lower urinary tract dysfunction
 World J Urol (2012) 30:445 450 DOI 10.1007/s00345-011-0780-2 TOPIC PAPER Sacral neuromodulation for lower urinary tract dysfunction Philip E. V. Van Kerrebroeck Tom A. T. Marcelissen Received: 22 August
World J Urol (2012) 30:445 450 DOI 10.1007/s00345-011-0780-2 TOPIC PAPER Sacral neuromodulation for lower urinary tract dysfunction Philip E. V. Van Kerrebroeck Tom A. T. Marcelissen Received: 22 August
Neural control of the lower urinary tract in health and disease
 Neural control of the lower urinary tract in health and disease Jalesh N. Panicker MD, DM, FRCP Consultant Neurologist and Clinical lead in Uro-Neurology The National Hospital for Neurology and Neurosurgery
Neural control of the lower urinary tract in health and disease Jalesh N. Panicker MD, DM, FRCP Consultant Neurologist and Clinical lead in Uro-Neurology The National Hospital for Neurology and Neurosurgery
Sacral neurostimulation for urinary retention: 10-year experience from one UK centre
 Original Articles SACRAL NEUROSTIMULATION FOR URINARY RETENTIONDATTA ET AL. Sacral neurostimulation for urinary retention: 1-year experience from one UK centre Soumendra N. Datta, Charlotte Chaliha, Anubha
Original Articles SACRAL NEUROSTIMULATION FOR URINARY RETENTIONDATTA ET AL. Sacral neurostimulation for urinary retention: 1-year experience from one UK centre Soumendra N. Datta, Charlotte Chaliha, Anubha
Sacral neuromodulation (SNM), using permanent foramen S3 electrode, Early versus late treatment of voiding dysfunction with pelvic neuromodulation
, using permanent foramen S3 electrode, Early versus late treatment of voiding dysfunction with pelvic neuromodulation") ORIGINAL RESEARCH Early versus late treatment of voiding dysfunction with pelvic neuromodulation Magdy M. Hassouna, MD, PhD; Mohamed S. Elkelini, MD See related article on page 111 Abstract Introduction:
ORIGINAL RESEARCH Early versus late treatment of voiding dysfunction with pelvic neuromodulation Magdy M. Hassouna, MD, PhD; Mohamed S. Elkelini, MD See related article on page 111 Abstract Introduction:
Neural control of the lower urinary tract
 Neural control of the lower urinary tract Jalesh N. Panicker Consultant Neurologist and Honorary Senior Lecturer The National Hospital for Neurology and Neurosurgery and UCL Institute of Neurology Queen
Neural control of the lower urinary tract Jalesh N. Panicker Consultant Neurologist and Honorary Senior Lecturer The National Hospital for Neurology and Neurosurgery and UCL Institute of Neurology Queen
Sacral Nerve Neuromodulation/Stimulation
 Protocol Sacral Nerve Neuromodulation/Stimulation (70169) Medical Benefit Effective Date: 01/01/14 Next Review Date: 09/14 Preauthorization No Review Dates: 01/08, 11/08, 09/09, 09/10, 09/11, 09/12, 09/13
Protocol Sacral Nerve Neuromodulation/Stimulation (70169) Medical Benefit Effective Date: 01/01/14 Next Review Date: 09/14 Preauthorization No Review Dates: 01/08, 11/08, 09/09, 09/10, 09/11, 09/12, 09/13
Sacral nerve stimulation in patients with detrusor overactivity
 Peer review Sacral nerve stimulation in patients with detrusor overactivity Abstract Detrusor overactivity, particularly with symptoms of urge incontinence, can be a debilitating and embarrassing condition.
Peer review Sacral nerve stimulation in patients with detrusor overactivity Abstract Detrusor overactivity, particularly with symptoms of urge incontinence, can be a debilitating and embarrassing condition.
Refractory Lower Urinary Tract Symptoms
 Sacral Neuromodulation for Treatment of Refractory Lower Urinary Tract Symptoms Alex Kavanagh, PGY3 Mar 30/2011 Goals 1. Define sacral neuromodulation (SNM) and review the clinical implementation 2. Provide
Sacral Neuromodulation for Treatment of Refractory Lower Urinary Tract Symptoms Alex Kavanagh, PGY3 Mar 30/2011 Goals 1. Define sacral neuromodulation (SNM) and review the clinical implementation 2. Provide
Sacral Neuromodulation Beyond Pelvic Pain!!!
 Sacral Neuromodulation Beyond Pelvic Pain!!! Dr. Hirachand S Mutagi. Senior Consultant Pain Physician. Head -Sakra World Hospital. Director ReLeaf Pain Services. Rapid advances in neurostimulation therapy
Sacral Neuromodulation Beyond Pelvic Pain!!! Dr. Hirachand S Mutagi. Senior Consultant Pain Physician. Head -Sakra World Hospital. Director ReLeaf Pain Services. Rapid advances in neurostimulation therapy
Technologies and architectures" Stimulator, electrodes, system flexibility, reliability, security, etc."
 March 2011 Introduction" Basic principle (Depolarization, hyper polarization, etc.." Stimulation types (Magnetic and electrical)" Main stimulation parameters (Current, voltage, etc )" Characteristics (Muscular
March 2011 Introduction" Basic principle (Depolarization, hyper polarization, etc.." Stimulation types (Magnetic and electrical)" Main stimulation parameters (Current, voltage, etc )" Characteristics (Muscular
Annual Scientific Update in Urogynaecology- Joint RCOG/BSUG Meeting Neurogenic bladder dysfunction
 Annual Scientific Update in Urogynaecology- Joint RCOG/BSUG Meeting Neurogenic bladder dysfunction Clare J.Fowler National Hospital for Neurology and Neurosurgery & Institute of Neurology, UCL Aims Background
Annual Scientific Update in Urogynaecology- Joint RCOG/BSUG Meeting Neurogenic bladder dysfunction Clare J.Fowler National Hospital for Neurology and Neurosurgery & Institute of Neurology, UCL Aims Background
Spinal Cord Injury. R Hamid Consultant Neuro-Urologist London Spinal Injuries Unit, Stanmore & National Hospital for Neurology & Neurosurgery, UCLH
 Spinal Cord Injury R Hamid Consultant Neuro-Urologist London Spinal Injuries Unit, Stanmore & National Hospital for Neurology & Neurosurgery, UCLH SCI 800 1000 new cases per year in UK Car accidents 35%
Spinal Cord Injury R Hamid Consultant Neuro-Urologist London Spinal Injuries Unit, Stanmore & National Hospital for Neurology & Neurosurgery, UCLH SCI 800 1000 new cases per year in UK Car accidents 35%
Summary. Neuro-urodynamics. The bladder cycle. and voiding. 14/12/2015. Neural control of the LUT Initial assessment Urodynamics
 Neuro-urodynamics Summary Neural control of the LUT Initial assessment Urodynamics Marcus Drake, Bristol Urological Institute SAFETY FIRST; renal failure, dysreflexia, latex allergy SYMPTOMS SECOND; storage,
Neuro-urodynamics Summary Neural control of the LUT Initial assessment Urodynamics Marcus Drake, Bristol Urological Institute SAFETY FIRST; renal failure, dysreflexia, latex allergy SYMPTOMS SECOND; storage,
Pelvic Floor Therapy for the Neurologic Client Carina Siracusa, PT, DPT, WCS
 Pelvic Floor Therapy for the Neurologic Client Carina Siracusa, PT, DPT, WCS OhioHealth, Columbus Ohio Disclosures I have nothing to disclose Objectives Describe the role of a pelvic floor therapist in
Pelvic Floor Therapy for the Neurologic Client Carina Siracusa, PT, DPT, WCS OhioHealth, Columbus Ohio Disclosures I have nothing to disclose Objectives Describe the role of a pelvic floor therapist in
The Presence of Fowler s Syndrome Predicts Successful Long-Term Outcome of Sacral Nerve Stimulation in Women with Urinary Retention
 european urology 51 (2007) 229 234 available at www.sciencedirect.com journal homepage: www.europeanurology.com Neuro-urology Voiding Dysfunction The Presence of Fowler s Syndrome Predicts Successful Long-Term
european urology 51 (2007) 229 234 available at www.sciencedirect.com journal homepage: www.europeanurology.com Neuro-urology Voiding Dysfunction The Presence of Fowler s Syndrome Predicts Successful Long-Term
Stimulation of the Sacral Anterior Root Combined with Posterior Sacral Rhizotomy in Patients with Spinal Cord Injury. Original Policy Date
 MP 7.01.58 Stimulation of the Sacral Anterior Root Combined with Posterior Sacral Rhizotomy in Patients with Spinal Cord Injury Medical Policy Section Issue 12:2013 Original Policy Date 12:2013 Last Review
MP 7.01.58 Stimulation of the Sacral Anterior Root Combined with Posterior Sacral Rhizotomy in Patients with Spinal Cord Injury Medical Policy Section Issue 12:2013 Original Policy Date 12:2013 Last Review
03/13/18. A. Symptoms lasting for greater than or equal to 12 months that have resulted to significant impairment in activities of daily living; and
 Reference #: MC/I008 Page: 1 of 5 PRODUCT APPLICATION: PreferredOne Administrative Services, Inc. (PAS) ERISA PreferredOne Administrative Services, Inc. (PAS) Non-ERISA PreferredOne Community Health Plan
Reference #: MC/I008 Page: 1 of 5 PRODUCT APPLICATION: PreferredOne Administrative Services, Inc. (PAS) ERISA PreferredOne Administrative Services, Inc. (PAS) Non-ERISA PreferredOne Community Health Plan
Overactive Bladder Syndrome
 Overactive Bladder Syndrome behavioural modifications to pharmacological and surgical treatments Dr Jos Jayarajan Urologist Austin Health, Eastern Health Warringal Private, Northpark Private, Epworth Overactive
Overactive Bladder Syndrome behavioural modifications to pharmacological and surgical treatments Dr Jos Jayarajan Urologist Austin Health, Eastern Health Warringal Private, Northpark Private, Epworth Overactive
Long Term Results of Neuromodulation by Sacral Nerve Stimulation for Lower Urinary Tract Symptoms: A Retrospective Single Center Study
 european urology 49 (2006) 366 372 available at www.sciencedirect.com journal homepage: www.europeanurology.com Female Urology Long Term Results of Neuromodulation by Sacral Nerve Stimulation for Lower
european urology 49 (2006) 366 372 available at www.sciencedirect.com journal homepage: www.europeanurology.com Female Urology Long Term Results of Neuromodulation by Sacral Nerve Stimulation for Lower
SACRAL NEUROMODULATION: EVOLUTION OVER TIME
 SACRAL NEUROMODULATION: EVOLUTION OVER TIME Anurag K. Das, MD, FACS Director Center for Neuro-urology and Continence Beth Israel Deaconess Medical Center Harvard Medical School Boston, MA First use of
SACRAL NEUROMODULATION: EVOLUTION OVER TIME Anurag K. Das, MD, FACS Director Center for Neuro-urology and Continence Beth Israel Deaconess Medical Center Harvard Medical School Boston, MA First use of
NEUROGENIC BLADDER. Dr Harriet Grubb Dr Alison Seymour Dr Alexander Joseph
 NEUROGENIC BLADDER Dr Harriet Grubb Dr Alison Seymour Dr Alexander Joseph OUTLINE Definition Anatomy and physiology of bladder function Types of neurogenic bladder Assessment and management Complications
NEUROGENIC BLADDER Dr Harriet Grubb Dr Alison Seymour Dr Alexander Joseph OUTLINE Definition Anatomy and physiology of bladder function Types of neurogenic bladder Assessment and management Complications
MEDICAL POLICY SUBJECT: SACRAL NERVE STIMULATION
 MEDICAL POLICY 01/16/14, 01/22/15, 03/15/16 PAGE: 1 OF: 8 If the member's subscriber contract excludes coverage for a specific service it is not covered under that contract. In such cases, medical policy
MEDICAL POLICY 01/16/14, 01/22/15, 03/15/16 PAGE: 1 OF: 8 If the member's subscriber contract excludes coverage for a specific service it is not covered under that contract. In such cases, medical policy
Contrasting the Percutaneous Nerve Evaluation Versus Staged Implantation in Sacral Neuromodulation
 Curr Urol Rep (2010) 11:310 314 DOI 10.1007/s11934-010-0128-2 Contrasting the Percutaneous Nerve Evaluation Versus Staged Implantation in Sacral Neuromodulation Chad Baxter & Ja-Hong Kim Published online:
Curr Urol Rep (2010) 11:310 314 DOI 10.1007/s11934-010-0128-2 Contrasting the Percutaneous Nerve Evaluation Versus Staged Implantation in Sacral Neuromodulation Chad Baxter & Ja-Hong Kim Published online:
The Neurogenic Bladder
 The Neurogenic Bladder Outline Brandon Haynes, MD Resident Physician Department of Urology Jelena Svircev, MD Assistant Professor Department of Rehabilitation Medicine Anatomy and Bladder Physiology Bladder
The Neurogenic Bladder Outline Brandon Haynes, MD Resident Physician Department of Urology Jelena Svircev, MD Assistant Professor Department of Rehabilitation Medicine Anatomy and Bladder Physiology Bladder
This Special Report supplement
 ...INTRODUCTION... Overactive Bladder: Defining the Disease Alan J. Wein, MD This Special Report supplement to The American Journal of Managed Care features proceedings from the workshop, Overactive Bladder:
...INTRODUCTION... Overactive Bladder: Defining the Disease Alan J. Wein, MD This Special Report supplement to The American Journal of Managed Care features proceedings from the workshop, Overactive Bladder:
Urinary Aspects of Multiple Sclerosis chronic condition with innovative treatment strategies. Dr. Boris Friedman May 2, 2012 OBJECTIVES
 Urinary Aspects of Multiple Sclerosis chronic condition with innovative treatment strategies Dr. Boris Friedman May 2, 2012 OBJECTIVES 1) Definition and classification of MS 2) Interventional radiology
Urinary Aspects of Multiple Sclerosis chronic condition with innovative treatment strategies Dr. Boris Friedman May 2, 2012 OBJECTIVES 1) Definition and classification of MS 2) Interventional radiology
Electrostimulation Part 3: Bladder dysfunctions
 GBM8320 Dispositifs Médicaux Intelligents Electrostimulation Part 3: Bladder dysfunctions Mohamad Sawan et al Laboratoire de neurotechnologies Polystim!!! http://www.cours.polymtl.ca/gbm8320/! mohamad.sawan@polymtl.ca!
GBM8320 Dispositifs Médicaux Intelligents Electrostimulation Part 3: Bladder dysfunctions Mohamad Sawan et al Laboratoire de neurotechnologies Polystim!!! http://www.cours.polymtl.ca/gbm8320/! mohamad.sawan@polymtl.ca!
GBM8320 Dispositifs Médicaux Intelligents. Electrostimulation. Part 3: Bladder dysfunctions
 GBM8320 Dispositifs Médicaux Intelligents Electrostimulation Part 3: Bladder dysfunctions Mohamad Sawan et al Laboratoire de neurotechnologies Polystim!!! http://www.cours.polymtl.ca/gbm8320/! mohamad.sawan@polymtl.ca!
GBM8320 Dispositifs Médicaux Intelligents Electrostimulation Part 3: Bladder dysfunctions Mohamad Sawan et al Laboratoire de neurotechnologies Polystim!!! http://www.cours.polymtl.ca/gbm8320/! mohamad.sawan@polymtl.ca!
What is the role for neurophysiology in the evaluation of patients with uro-genito-anal dysfunction?
 London, 2016 What is the role for neurophysiology in the evaluation of patients with uro-genito-anal dysfunction? David B. Vodušek Medical Faculty, University of Ljubljana, Slovenia vodusek.david.b@gmail.com
London, 2016 What is the role for neurophysiology in the evaluation of patients with uro-genito-anal dysfunction? David B. Vodušek Medical Faculty, University of Ljubljana, Slovenia vodusek.david.b@gmail.com
Regulation of the Urinary Bladder Chapter 26
 Regulation of the Urinary Bladder Chapter 26 Anatomy 1. The urinary bladder is smooth muscle lined internally by transitional epithelium and externally by the parietal peritoneum. Contraction of the smooth
Regulation of the Urinary Bladder Chapter 26 Anatomy 1. The urinary bladder is smooth muscle lined internally by transitional epithelium and externally by the parietal peritoneum. Contraction of the smooth
TREATMENT METHODS FOR DISORDERS OF SMALL ANIMAL BLADDER FUNCTION
 Vet Times The website for the veterinary profession https://www.vettimes.co.uk TREATMENT METHODS FOR DISORDERS OF SMALL ANIMAL BLADDER FUNCTION Author : SIMONA T RADAELLI Categories : Vets Date : July
Vet Times The website for the veterinary profession https://www.vettimes.co.uk TREATMENT METHODS FOR DISORDERS OF SMALL ANIMAL BLADDER FUNCTION Author : SIMONA T RADAELLI Categories : Vets Date : July
Sacral Neuromodulation for Refractory Lower Urinary Tract Dysfunction: Results of a Nationwide Registry in Switzerland
 european urology 51 (2007) 1357 1363 available at www.sciencedirect.com journal homepage: www.europeanurology.com Neuro-urology Sacral Neuromodulation for Refractory Lower Urinary Tract Dysfunction: Results
european urology 51 (2007) 1357 1363 available at www.sciencedirect.com journal homepage: www.europeanurology.com Neuro-urology Sacral Neuromodulation for Refractory Lower Urinary Tract Dysfunction: Results
Bladder dysfunction in ALD and AMN
 Bladder dysfunction in ALD and AMN Sara Simeoni, MD Department of Uro-Neurology National Hospital for Neurology and Neurosurgery Queen Square, London 10:15 Dr Sara Simeoni- Bladder issues for AMN patients
Bladder dysfunction in ALD and AMN Sara Simeoni, MD Department of Uro-Neurology National Hospital for Neurology and Neurosurgery Queen Square, London 10:15 Dr Sara Simeoni- Bladder issues for AMN patients
Urodynamic Results of Sacral Neuromodulation Correlate with Subjective Improvement in Patients with an Overactive Bladder
 European Urology European Urology 43 (2003) 282±287 Urodynamic Results of Sacral Neuromodulation Correlate with Subjective Improvement in Patients with an Overactive Bladder W.A. Scheepens a, G.A. van
European Urology European Urology 43 (2003) 282±287 Urodynamic Results of Sacral Neuromodulation Correlate with Subjective Improvement in Patients with an Overactive Bladder W.A. Scheepens a, G.A. van
Mr. GIT KAH ANN. Pakar Klinikal Urologi Hospital Kuala Lumpur.
 Mr. GIT KAH ANN Pakar Klinikal Urologi Hospital Kuala Lumpur drgitka@yahoo.com 25 Jan 2007 HIGHLIGHTS Introduction ICS Definition Making a Diagnosis Voiding Chart Investigation Urodynamics Ancillary Investigations
Mr. GIT KAH ANN Pakar Klinikal Urologi Hospital Kuala Lumpur drgitka@yahoo.com 25 Jan 2007 HIGHLIGHTS Introduction ICS Definition Making a Diagnosis Voiding Chart Investigation Urodynamics Ancillary Investigations
Sacral Nerve Neuromodulation/Stimulation. Description
 Subject: Sacral Nerve Neuromodulation/Stimulation Page: 1 of 16 Last Review Status/Date: June 2014 Sacral Nerve Neuromodulation/Stimulation Description Sacral nerve neuromodulation (SNM), also referred
Subject: Sacral Nerve Neuromodulation/Stimulation Page: 1 of 16 Last Review Status/Date: June 2014 Sacral Nerve Neuromodulation/Stimulation Description Sacral nerve neuromodulation (SNM), also referred
Sacral Nerve Neuromodulation / Stimulation
 Sacral Nerve Neuromodulation / Stimulation Policy Number: 7.01.69 Last Review: 2/2018 Origination: 2/2001 Next Review: 2/2019 Policy Blue Cross and Blue Shield of Kansas City (Blue KC) will provide coverage
Sacral Nerve Neuromodulation / Stimulation Policy Number: 7.01.69 Last Review: 2/2018 Origination: 2/2001 Next Review: 2/2019 Policy Blue Cross and Blue Shield of Kansas City (Blue KC) will provide coverage
AUAUpdateSeries. Lesson 19 Volume Treatment of Non-Neurogenic Overactive Bladder with Electrical Stimulation
 AUAUpdateSeries Lesson 19 Volume 27 2008 Treatment of Non-Neurogenic Overactive Bladder with Electrical Stimulation Learning Objective: At the conclusion of this continuing medical education activity,
AUAUpdateSeries Lesson 19 Volume 27 2008 Treatment of Non-Neurogenic Overactive Bladder with Electrical Stimulation Learning Objective: At the conclusion of this continuing medical education activity,
Updates in the nonpharmacological. treatment on overactive bladder
 Updates in the nonpharmacological treatment on overactive bladder Overactive Bladder Also known as urgency-frequency syndrome Symptoms Urgency Daytime frequency Nocturia Urge urinary incontinence Sudden
Updates in the nonpharmacological treatment on overactive bladder Overactive Bladder Also known as urgency-frequency syndrome Symptoms Urgency Daytime frequency Nocturia Urge urinary incontinence Sudden
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE SCOPE
 NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE 1 Guideline title SCOPE Urinary incontinence in women: the management of urinary incontinence in women 1.1 Short title Urinary incontinence in women
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE 1 Guideline title SCOPE Urinary incontinence in women: the management of urinary incontinence in women 1.1 Short title Urinary incontinence in women
Urodynamic and electrophysiological investigations in neuro-urology
 Urodynamic and electrophysiological investigations in neuro-urology Pr. Gerard Amarenco Neuro-Urology and Pelvic-Floor Investigations Department Tenon Hospital, Assistance Publique Hôpitaux de Paris, Er6,
Urodynamic and electrophysiological investigations in neuro-urology Pr. Gerard Amarenco Neuro-Urology and Pelvic-Floor Investigations Department Tenon Hospital, Assistance Publique Hôpitaux de Paris, Er6,
Management of OAB. Lynsey McHugh. Consultant Urological Surgeon. Lancashire Teaching Hospitals
 Management of OAB Lynsey McHugh Consultant Urological Surgeon Lancashire Teaching Hospitals Summary Physiology Epidemiology Definitions NICE guidelines Evaluation Conservative management Medical management
Management of OAB Lynsey McHugh Consultant Urological Surgeon Lancashire Teaching Hospitals Summary Physiology Epidemiology Definitions NICE guidelines Evaluation Conservative management Medical management
Neuromodulation for pelvic floor dysfunctions: exploring tibial, sacral and pudendal nerve stimulation. W18, 15 October :00-17:00
 Neuromodulation for pelvic floor dysfunctions: exploring tibial, sacral and pudendal nerve stimulation. W18, 15 October 2012 14:00-17:00 Start End Topic Speakers 14:00 14:10 Introduction Stefan de Wachter
Neuromodulation for pelvic floor dysfunctions: exploring tibial, sacral and pudendal nerve stimulation. W18, 15 October 2012 14:00-17:00 Start End Topic Speakers 14:00 14:10 Introduction Stefan de Wachter
Objectives. Prevalence of Urinary Incontinence URINARY INCONTINENCE: EVALUATION AND CURRENT TREATMENT OPTIONS
 URINARY INCONTINENCE: EVALUATION AND CURRENT TREATMENT OPTIONS Lisa S Pair, MSN, CRNP Division of Urogynecology and Pelvic Reconstructive Surgery Department of Obstetrics and Gynecology University of Alabama
URINARY INCONTINENCE: EVALUATION AND CURRENT TREATMENT OPTIONS Lisa S Pair, MSN, CRNP Division of Urogynecology and Pelvic Reconstructive Surgery Department of Obstetrics and Gynecology University of Alabama
INJINTERNATIONAL. Radiographic Position of the Electrode as a Predictor of the Outcome of InterStim Therapy. Original Article INTRODUCTION
 Official Journal of Korean Continence Society / Korean Society of Urological Research / The Korean Children s Continence and Enuresis Society / The Korean Association of Urogenital Tract Infection and
Official Journal of Korean Continence Society / Korean Society of Urological Research / The Korean Children s Continence and Enuresis Society / The Korean Association of Urogenital Tract Infection and
Sacral Nerve Neuromodulation/Stimulation for Pelvic Floor Dysfunction
 Medical Policy Manual Surgery, Policy No. 134 Sacral Nerve Neuromodulation/Stimulation for Pelvic Floor Dysfunction Next Review: December 2018 Last Review: June 2018 Effective: July 1, 2018 IMPORTANT REMINDER
Medical Policy Manual Surgery, Policy No. 134 Sacral Nerve Neuromodulation/Stimulation for Pelvic Floor Dysfunction Next Review: December 2018 Last Review: June 2018 Effective: July 1, 2018 IMPORTANT REMINDER
GUIDELINES ON NEUROGENIC LOWER URINARY TRACT DYSFUNCTION
 GUIDELINES ON NEUROGENIC LOWER URINARY TRACT DYSFUNCTION M. Stöhrer (chairman), D. Castro-Diaz, E. Chartier-Kastler, G. Kramer, A. Mattiasson, J-J. Wyndaele Introduction NLUTD (neurogenic lower urinary
GUIDELINES ON NEUROGENIC LOWER URINARY TRACT DYSFUNCTION M. Stöhrer (chairman), D. Castro-Diaz, E. Chartier-Kastler, G. Kramer, A. Mattiasson, J-J. Wyndaele Introduction NLUTD (neurogenic lower urinary
Neural Control of Lower Urinary Tract Function. William C. de Groat University of Pittsburgh Medical School
 Neural Control of Lower Urinary Tract Function William C. de Groat University of Pittsburgh Medical School Disclosures Current funding: NIH Grants, DK093424, DK-091253, DK-094905, DK-090006. Other financial
Neural Control of Lower Urinary Tract Function William C. de Groat University of Pittsburgh Medical School Disclosures Current funding: NIH Grants, DK093424, DK-091253, DK-094905, DK-090006. Other financial
Neuroanatomy, Neurophysiology and Clinical Presentation of Visceral Urological Pain
 Neuroanatomy, Neurophysiology and Clinical Presentation of Visceral Urological Pain Prof Dr K. Everaert Functional urology Department of Urology Ghent University Hospital Gent, Belgium Chronic pelvic pain
Neuroanatomy, Neurophysiology and Clinical Presentation of Visceral Urological Pain Prof Dr K. Everaert Functional urology Department of Urology Ghent University Hospital Gent, Belgium Chronic pelvic pain
Functional anatomy of the female pelvic floor and lower urinary tract Stefano Floris, MD, PhD Department of Obstetrics and Gynaecology
 Functional anatomy of the female pelvic floor and lower urinary tract Stefano Floris, MD, PhD Department of Obstetrics and Gynaecology Ospedale San Giovanni di Dio, Gorizia, Italy ANATOMY URINARY CONTINENCE
Functional anatomy of the female pelvic floor and lower urinary tract Stefano Floris, MD, PhD Department of Obstetrics and Gynaecology Ospedale San Giovanni di Dio, Gorizia, Italy ANATOMY URINARY CONTINENCE
OHTAC Recommendation
 OHTAC Recommendation Sacral Nerve Stimulation for the Management of Urge Incontinence, Urgency-Frequency, Urinary Retention and Fecal Incontinence March 2, 2005 1 The Ontario Health Technology Advisory
OHTAC Recommendation Sacral Nerve Stimulation for the Management of Urge Incontinence, Urgency-Frequency, Urinary Retention and Fecal Incontinence March 2, 2005 1 The Ontario Health Technology Advisory
Sacral Nerve Neuromodulation/Stimulation. Description
 Subject: Sacral Nerve Neuromodulation/Stimulation Page: 1 of 17 Last Review Status/Date: September 2015 Sacral Nerve Neuromodulation/Stimulation Description Sacral nerve neuromodulation (SNM), also referred
Subject: Sacral Nerve Neuromodulation/Stimulation Page: 1 of 17 Last Review Status/Date: September 2015 Sacral Nerve Neuromodulation/Stimulation Description Sacral nerve neuromodulation (SNM), also referred
Ben Herbert Alex Wojtowicz
 Ben Herbert Alex Wojtowicz 54 year old female presenting with: Dragging sensation Urinary incontinence Some faecal incontinence HPC Since May 14 had noticed a mass protruding from the vagina when going
Ben Herbert Alex Wojtowicz 54 year old female presenting with: Dragging sensation Urinary incontinence Some faecal incontinence HPC Since May 14 had noticed a mass protruding from the vagina when going
W28: Neuromodulation in Complex Pelvic Floor Disorders Workshop Chair: Sohier Elneil, United Kingdom 27 August :00-18:00
 W28: Neuromodulation in Complex Pelvic Floor Disorders Workshop Chair: Sohier Elneil, United Kingdom 27 August 2013 14:00-18:00 Start End Topic Speakers 14:00 14:20 An Overview of Complex Pelvic Floor
W28: Neuromodulation in Complex Pelvic Floor Disorders Workshop Chair: Sohier Elneil, United Kingdom 27 August 2013 14:00-18:00 Start End Topic Speakers 14:00 14:20 An Overview of Complex Pelvic Floor
Posterior Tibial Nerve Stimulation for Treating Neurologic Bladder in Women: a Randomized Clinical Trial
 ORIGINAL ARTICLE Posterior Tibial Nerve Stimulation for Treating Neurologic Bladder in Women: a Randomized Clinical Trial Tahereh Eftekhar 1, Nastaran Teimoory 1, Elahe Miri 1, Abolghasem Nikfallah 2,
ORIGINAL ARTICLE Posterior Tibial Nerve Stimulation for Treating Neurologic Bladder in Women: a Randomized Clinical Trial Tahereh Eftekhar 1, Nastaran Teimoory 1, Elahe Miri 1, Abolghasem Nikfallah 2,
Urodynamics in Neurological Lower Urinary Tract Dysfunction. Mr Chris Harding Consultant Urologist Freeman Hospital Newcastle-upon-Tyne
 Urodynamics in Neurological Lower Urinary Tract Dysfunction Mr Chris Harding Consultant Urologist Freeman Hospital Newcastle-upon-Tyne Learning Objectives Review functional neurology relevant to lower
Urodynamics in Neurological Lower Urinary Tract Dysfunction Mr Chris Harding Consultant Urologist Freeman Hospital Newcastle-upon-Tyne Learning Objectives Review functional neurology relevant to lower
Neuropathic Bladder. Magda Kujawa Consultant Urologist Stockport NHS Foundation Trust 12/03/2014
 Neuropathic Bladder Magda Kujawa Consultant Urologist Stockport NHS Foundation Trust 12/03/2014 Plan Physiology- bladder and sphincter behaviour in neurological disease Clinical consequences of Symptoms
Neuropathic Bladder Magda Kujawa Consultant Urologist Stockport NHS Foundation Trust 12/03/2014 Plan Physiology- bladder and sphincter behaviour in neurological disease Clinical consequences of Symptoms
Applications of Neuromodulation of the Lower Urinary Tract in Female Urology
 Review Article Neuromodulation of the Lower Urinary Tract in Females International Braz J Urol Vol. 32 (3): 262-272, May - June, 2006 Applications of Neuromodulation of the Lower Urinary Tract in Female
Review Article Neuromodulation of the Lower Urinary Tract in Females International Braz J Urol Vol. 32 (3): 262-272, May - June, 2006 Applications of Neuromodulation of the Lower Urinary Tract in Female
Sacral Nerve Neuromodulation/Stimulation
 Protocol Sacral Nerve Neuromodulation/Stimulation (70169) Medical Benefit Effective Date: 01/01/16 Next Review Date: 09/18 Preauthorization No Review Dates: 01/08, 11/08, 09/09, 09/10, 09/11, 09/12, 09/13,
Protocol Sacral Nerve Neuromodulation/Stimulation (70169) Medical Benefit Effective Date: 01/01/16 Next Review Date: 09/18 Preauthorization No Review Dates: 01/08, 11/08, 09/09, 09/10, 09/11, 09/12, 09/13,
Prolapse & Urogynaecology. Hester Mannion and Fabi Sica
 Prolapse & Urogynaecology Hester Mannion and Fabi Sica Take home messages Prolapse and associated incontinence is very common It has a devastating effect on the QoL of the patient and their partner Strategies
Prolapse & Urogynaecology Hester Mannion and Fabi Sica Take home messages Prolapse and associated incontinence is very common It has a devastating effect on the QoL of the patient and their partner Strategies
Kathleen C. Kobashi, MD, FACS Head, Section of Urology and Renal Transplantation Virginia Mason Medical Center, Seattle, WA
 Kathleen C. Kobashi, MD, FACS Head, Section of Urology and Renal Transplantation Virginia Mason Medical Center, Seattle, WA Disclosures Advisory Board and/or Speaker Allergan Medtronic Astellas AUA Guidelines
Kathleen C. Kobashi, MD, FACS Head, Section of Urology and Renal Transplantation Virginia Mason Medical Center, Seattle, WA Disclosures Advisory Board and/or Speaker Allergan Medtronic Astellas AUA Guidelines
Posterior Tibial Nerve Stimulation
 Posterior Tibial Nerve Stimulation Policy Number: Original Effective Date: MM.02.025 01/01/2015 Lines of Business: Current Effective Date: HMO; PPO; QUEST Integration 02/01/2015 Section: Medicine Place(s)
Posterior Tibial Nerve Stimulation Policy Number: Original Effective Date: MM.02.025 01/01/2015 Lines of Business: Current Effective Date: HMO; PPO; QUEST Integration 02/01/2015 Section: Medicine Place(s)
URINARY INCONTINENCE. Urology Division, Surgery Department Medical Faculty, University of Sumatera Utara
 URINARY INCONTINENCE Urology Division, Surgery Department Medical Faculty, University of Sumatera Utara Definition The involuntary loss of urine May denote a symptom, a sign or a condition Symptom the
URINARY INCONTINENCE Urology Division, Surgery Department Medical Faculty, University of Sumatera Utara Definition The involuntary loss of urine May denote a symptom, a sign or a condition Symptom the
Neuromodulation for pelvic floor dysfunctions: exploring tibial, sacral and pudendal nerve stimulation. W3, 29 August :00-12:00
 Neuromodulation for pelvic floor dysfunctions: exploring tibial, sacral and pudendal nerve stimulation. W3, 29 August 2011 09:00-12:00 Start End Topic Speakers 09:00 09:10 Introduction Stefan De Wachter
Neuromodulation for pelvic floor dysfunctions: exploring tibial, sacral and pudendal nerve stimulation. W3, 29 August 2011 09:00-12:00 Start End Topic Speakers 09:00 09:10 Introduction Stefan De Wachter
EAU GUIDELINES ON NEURO-UROLOGY
 EAU GUIDELINES ON NEURO-UROLOGY (Limited text update March 2017) B. Blok (Co-chair), J. Pannek (Co-chair) D. Castro-Diaz, G. del Popolo, J. Groen, R. Hamid, G. Karsenty, T.M. Kessler Guidelines Associates:
EAU GUIDELINES ON NEURO-UROLOGY (Limited text update March 2017) B. Blok (Co-chair), J. Pannek (Co-chair) D. Castro-Diaz, G. del Popolo, J. Groen, R. Hamid, G. Karsenty, T.M. Kessler Guidelines Associates:
Medical Policy An independent licensee of the Blue Cross Blue Shield Association
 Sacral Nerve Neuromodulation / Stimulation Page 1 of 23 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: Sacral Nerve Neuromodulation / Stimulation Professional Institutional
Sacral Nerve Neuromodulation / Stimulation Page 1 of 23 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: Sacral Nerve Neuromodulation / Stimulation Professional Institutional
Recommandations de prise en charge des vessies neurogènes EAU 2006
 Annexe 4-1 Recommandations de prise en charge des vessies neurogènes EAU 2006 (Version courte) 685 686 GUIDELINES ON NEUROGENIC LOWER URINARY TRACT DYSFUNCTION M. Stöhrer (chairman), D. Castro-Diaz, E.
Annexe 4-1 Recommandations de prise en charge des vessies neurogènes EAU 2006 (Version courte) 685 686 GUIDELINES ON NEUROGENIC LOWER URINARY TRACT DYSFUNCTION M. Stöhrer (chairman), D. Castro-Diaz, E.
Guidelines on Neurogenic Lower Urinary Tract Dysfunction
 Guidelines on Neurogenic Lower Urinary Tract Dysfunction (Text update March 2009) M. Stöhrer (chairman), B. Blok, D. Castro-Diaz, E. Chartier- Kastler, P. Denys, G. Kramer, J. Pannek, G. del Popolo, P.
Guidelines on Neurogenic Lower Urinary Tract Dysfunction (Text update March 2009) M. Stöhrer (chairman), B. Blok, D. Castro-Diaz, E. Chartier- Kastler, P. Denys, G. Kramer, J. Pannek, G. del Popolo, P.
A joint venture between the Department of Uro-Neurology, Queen Square, University College London and the Neuro-Urology Promotion Committee of the ICS
 Neurogenic bladder 2-day course A joint venture between the Uro-Neurology,, University College London and the Neuro-Urology Promotion Committee of the ICS November 27 and 28, 2014 Venue: Clinical Neuroscience
Neurogenic bladder 2-day course A joint venture between the Uro-Neurology,, University College London and the Neuro-Urology Promotion Committee of the ICS November 27 and 28, 2014 Venue: Clinical Neuroscience
Neurogenic bladder. Neurogenic bladder is a type of dysfunction of the bladder due to neurological disorder.
 Definition: Neurogenic bladder Neurogenic bladder is a type of dysfunction of the bladder due to neurological disorder. Types: Nervous system diseases: Congenital: like myelodysplasia like meningocele.
Definition: Neurogenic bladder Neurogenic bladder is a type of dysfunction of the bladder due to neurological disorder. Types: Nervous system diseases: Congenital: like myelodysplasia like meningocele.
Perineal Electrophysiologic Tests
 Perineal disorders and emg! Perineal Electrophysiologic Tests Voiding dysfunction Stress Urinary Incontinence urgency OAB Urge Incontinence nocturia Pr. Gerard Amarenco Mixed Incontinence frequency Service
Perineal disorders and emg! Perineal Electrophysiologic Tests Voiding dysfunction Stress Urinary Incontinence urgency OAB Urge Incontinence nocturia Pr. Gerard Amarenco Mixed Incontinence frequency Service
POLICIES AND PROCEDURE MANUAL
 POLICIES AND PROCEDURE MANUAL Policy: MP091 Section: Medical Benefit Policy Subject: Sacral Nerve Stimulation I. Policy: Sacral Nerve Stimulation II. Purpose/Objective: To provide a policy of coverage
POLICIES AND PROCEDURE MANUAL Policy: MP091 Section: Medical Benefit Policy Subject: Sacral Nerve Stimulation I. Policy: Sacral Nerve Stimulation II. Purpose/Objective: To provide a policy of coverage
MEDICAL POLICY SUBJECT: PERCUTANEOUS POSTERIOR TIBIAL NERVE STIMULATION (PPTNS) POLICY NUMBER: CATEGORY: Technology Assessment
 POLICY NUMBER: CATEGORY: Technology Assessment") MEDICAL POLICY SUBJECT: PERCUTANEOUS POSTERIOR Clinical criteria used to make utilization review decisions are based on credible scientific evidence published in peer reviewed medical literature generally
MEDICAL POLICY SUBJECT: PERCUTANEOUS POSTERIOR Clinical criteria used to make utilization review decisions are based on credible scientific evidence published in peer reviewed medical literature generally
University College Hospital at Westmoreland Street. Percutaneous Tibial Nerve Stimulation (PTNS)
") University College Hospital at Westmoreland Street Percutaneous Tibial Nerve Stimulation (PTNS) Urology Directorate If you need a large print, audio or translated copy of this document, please contact
University College Hospital at Westmoreland Street Percutaneous Tibial Nerve Stimulation (PTNS) Urology Directorate If you need a large print, audio or translated copy of this document, please contact
Tuesday 24 June Poster Session 1: Voiding Dysfunction Chairmen: C. Chapple and L. Stewart
 Tuesday 24 June 10.30 11.30 Poster Session 1: Voiding Dysfunction Chairmen: C. Chapple and L. Stewart P001 Can oral antibiotic prophylaxis reduce the rate of infection after conventional urodynamic studies?
Tuesday 24 June 10.30 11.30 Poster Session 1: Voiding Dysfunction Chairmen: C. Chapple and L. Stewart P001 Can oral antibiotic prophylaxis reduce the rate of infection after conventional urodynamic studies?
MEDICAL POLICY SUBJECT: PERCUTANEOUS POSTERIOR TIBIAL NERVE STIMULATION (PPTNS)
") MEDICAL POLICY 03/19/15, 05/17/16 PAGE: 1 OF: 6 If the member's subscriber contract excludes coverage for a specific service it is not covered under that contract. In such cases, medical policy criteria
MEDICAL POLICY 03/19/15, 05/17/16 PAGE: 1 OF: 6 If the member's subscriber contract excludes coverage for a specific service it is not covered under that contract. In such cases, medical policy criteria
GI Physiology - Investigating and treating patients with pelvic floor dysfunction. Lynne Smith Department of GI Physiology NGH Sheffield
 GI Physiology - Investigating and treating patients with pelvic floor dysfunction Lynne Smith Department of GI Physiology NGH Sheffield Aims o o o To give an overview of lower GI investigations To demonstrate
GI Physiology - Investigating and treating patients with pelvic floor dysfunction Lynne Smith Department of GI Physiology NGH Sheffield Aims o o o To give an overview of lower GI investigations To demonstrate
PARTICULARS, SCHEDULE 2- THE SERVICES, A- SERVICE SPECIFICATIONS. A08/S/d Colorectal: Faecal Incontinence (Adult)
") A08/S/d 2013/14 NHS STANDARD CONTRACT FOR COLORECTAL: FAECAL INCONTINENCE (ADULT) PARTICULARS, SCHEDULE 2- THE SERVICES, A- SERVICE SPECIFICATIONS Service Specification No. Service Commissioner Lead Provider
A08/S/d 2013/14 NHS STANDARD CONTRACT FOR COLORECTAL: FAECAL INCONTINENCE (ADULT) PARTICULARS, SCHEDULE 2- THE SERVICES, A- SERVICE SPECIFICATIONS Service Specification No. Service Commissioner Lead Provider
Conservative Management of Functional Bowel & Pelvic Floor Disorders
 Conservative Management of Functional Bowel & Pelvic Floor Disorders Kathy Davis PhD BSc(Hons)SRN Specialist Nurse Consultant Parkside Hospital & Minerva Medical Clinic Overview Burden of disease Aims
Conservative Management of Functional Bowel & Pelvic Floor Disorders Kathy Davis PhD BSc(Hons)SRN Specialist Nurse Consultant Parkside Hospital & Minerva Medical Clinic Overview Burden of disease Aims
MEDICAL POLICY SUBJECT: SACRAL NERVE STIMULATION. POLICY NUMBER: CATEGORY: Technology Assessment
 MEDICAL POLICY SUBJECT: SACRAL NERVE STIMULATION EFFECTIVE DATE: 11/19/99 PAGE: 1 OF: 9 If a product excludes coverage for a service, it is not covered, and medical policy criteria do not apply. If a commercial
MEDICAL POLICY SUBJECT: SACRAL NERVE STIMULATION EFFECTIVE DATE: 11/19/99 PAGE: 1 OF: 9 If a product excludes coverage for a service, it is not covered, and medical policy criteria do not apply. If a commercial
EAU GUIDELINES ON NEURO-UROLOGY
 EAU GUIDELINES ON NEURO-UROLOGY (Limited text update March 2016) B. Blok (Co-chair), J. Pannek (Co-chair) D. Castro-Diaz, G. del Popolo, J. Groen, R. Hamid, G. Karsenty, T.M. Kessler. Guidelines Associates:
EAU GUIDELINES ON NEURO-UROLOGY (Limited text update March 2016) B. Blok (Co-chair), J. Pannek (Co-chair) D. Castro-Diaz, G. del Popolo, J. Groen, R. Hamid, G. Karsenty, T.M. Kessler. Guidelines Associates:
Sacral Neuromodulation for Dysfunctional Voiders Workshop 1 Monday, August 23, 09:00 10:30
 Sacral Neuromodulation for Dysfunctional Voiders Workshop 1 Monday, August 23, 09:00 10:30 Time Time Topic Speaker 09:00 09:05 Introduction to the aims of the workshop and the Magdy Hassouna participants
Sacral Neuromodulation for Dysfunctional Voiders Workshop 1 Monday, August 23, 09:00 10:30 Time Time Topic Speaker 09:00 09:05 Introduction to the aims of the workshop and the Magdy Hassouna participants
The cost of the Axonics sacral neuromodulation system is 475 for the trial phase, 9,210 for a
 pat hways Axonics sacral al neuromodulation system for overactive bladder and faecal incontinence Medtech innovation briefing Published: 10 December 2018 nice.org.uk/guidance/mib164 Summary The technology
pat hways Axonics sacral al neuromodulation system for overactive bladder and faecal incontinence Medtech innovation briefing Published: 10 December 2018 nice.org.uk/guidance/mib164 Summary The technology
CONTINENCE MODULE 1 MIMIMUM STANDARDS FOR THE SPECIALIST ASSESSMENT & CONSERVATIVE MANAGEMENT OF FEMALE LOWER URINARY TRACT SYMPTOMS
 CONTINENCE MODULE 1 MIMIMUM STANDARDS FOR THE SPECIALIST ASSESSMENT & CONSERVATIVE MANAGEMENT OF FEMALE LOWER URINARY TRACT SYMPTOMS The minimum standards required to initiate specialised conservative
CONTINENCE MODULE 1 MIMIMUM STANDARDS FOR THE SPECIALIST ASSESSMENT & CONSERVATIVE MANAGEMENT OF FEMALE LOWER URINARY TRACT SYMPTOMS The minimum standards required to initiate specialised conservative
NeuromodulationöSacral, Peripheral and Central: Current Status, Indications, Results and New Developments
 EAU Update Series EAU Update Series 2 (2004) 187 194 NeuromodulationöSacral, Peripheral and Central: Current Status, Indications, Results and New Developments Peter Martin Braun*, Christoph Seif, Christof
EAU Update Series EAU Update Series 2 (2004) 187 194 NeuromodulationöSacral, Peripheral and Central: Current Status, Indications, Results and New Developments Peter Martin Braun*, Christoph Seif, Christof
GUIDELINES ON NEURO-UROLOGY
 GUIDELINES ON NEURO-UROLOGY (Limited text update March 2015) B. Blok (Co-chair), J. Pannek (Co-chair), D. Castro Diaz, G. del Popolo, J. Groen, T. Gross (Guidelines ssociate), R. Hamid, G. Karsenty, T.M.
GUIDELINES ON NEURO-UROLOGY (Limited text update March 2015) B. Blok (Co-chair), J. Pannek (Co-chair), D. Castro Diaz, G. del Popolo, J. Groen, T. Gross (Guidelines ssociate), R. Hamid, G. Karsenty, T.M.
La vescica iperattiva: dalla diagnosi ai nuovi approcci terapeutici
 La Prostata nel Mirino Napoli, 1 dicembre 2016 La vescica iperattiva: dalla diagnosi ai nuovi approcci terapeutici Giorgio Annoni Cattedra e Scuola di Specializzazione in Geriatria Università degli Studi
La Prostata nel Mirino Napoli, 1 dicembre 2016 La vescica iperattiva: dalla diagnosi ai nuovi approcci terapeutici Giorgio Annoni Cattedra e Scuola di Specializzazione in Geriatria Università degli Studi
Incontinence. When I was given this topic in urology to discuss with you today I
 Incontinence When I was given this topic in urology to discuss with you today I was slightly disappointed. I personally see mostly men for problems such as stones, benign prostatic hyperplasia, prostate
Incontinence When I was given this topic in urology to discuss with you today I was slightly disappointed. I personally see mostly men for problems such as stones, benign prostatic hyperplasia, prostate
Coding for Sacral Neuromodulation
 301.273.0570 Fax 301.273.0778 Coding for Sacral Neuromodulation Sacral Neuromodulation (SNS) is a widely used technique in Female Pelvic Medicine and Reconstructive Surgery (FPMRS), with several FDA-approved
301.273.0570 Fax 301.273.0778 Coding for Sacral Neuromodulation Sacral Neuromodulation (SNS) is a widely used technique in Female Pelvic Medicine and Reconstructive Surgery (FPMRS), with several FDA-approved
How to manage a patient with bladder dysfunction
 3 rd Congress of the European Academy of Neurology Amsterdam, The Netherlands, June 24 27, 2017 Teaching Course 13 How to manage a patient with autonomic dysfunction - Level 2 How to manage a patient with
3 rd Congress of the European Academy of Neurology Amsterdam, The Netherlands, June 24 27, 2017 Teaching Course 13 How to manage a patient with autonomic dysfunction - Level 2 How to manage a patient with
University of Alberta Reconstructive Urology Fellowship
 FACULTY OF MEDICINE AND DENTISTRY DEPARTMENT OF SURGERY DIVISION OF UROLOGY Keith Rourke, MD, FRCSC Reconstructive Urology Professor Chair of Academic Urology Reconstructive Urology Fellowship Director
FACULTY OF MEDICINE AND DENTISTRY DEPARTMENT OF SURGERY DIVISION OF UROLOGY Keith Rourke, MD, FRCSC Reconstructive Urology Professor Chair of Academic Urology Reconstructive Urology Fellowship Director
Physiologic Anatomy and Nervous Connections of the Bladder
 Micturition Objectives: 1. Review the anatomical organization of the urinary system from a physiological point of view. 2. Describe the micturition reflex. 3. Predict the lines of treatment of renal failure.
Micturition Objectives: 1. Review the anatomical organization of the urinary system from a physiological point of view. 2. Describe the micturition reflex. 3. Predict the lines of treatment of renal failure.
Subject: Sacral Nerve Neuromodulation/Stimulation
 02-61000-23 Original Effective Date: 01/01/01 Reviewed: 06/28/18 Revised: 01/01/19 Subject: Sacral Nerve Neuromodulation/Stimulation THIS MEDICAL COVERAGE GUIDELINE IS NOT AN AUTHORIZATION, CERTIFICATION,
02-61000-23 Original Effective Date: 01/01/01 Reviewed: 06/28/18 Revised: 01/01/19 Subject: Sacral Nerve Neuromodulation/Stimulation THIS MEDICAL COVERAGE GUIDELINE IS NOT AN AUTHORIZATION, CERTIFICATION,
Clinical Policy: Urinary Incontinence Devices and Treatments
 Clinical Policy: Reference Number: CP.MP.142 Last Review Date: 03/18 See Important Reminder at the end of this policy for important regulatory and legal information. Coding Implications Revision Log Description
Clinical Policy: Reference Number: CP.MP.142 Last Review Date: 03/18 See Important Reminder at the end of this policy for important regulatory and legal information. Coding Implications Revision Log Description
GUIDELINES ON NEURO-UROLOGY
 GUIDELINES ON NEURO-UROLOGY (Text update pril 2014) J. Pannek (co-chair), B. Blok (co-chair), D. Castro-Diaz, G. del Popolo, J. Groen, G. Karsenty, T.M. Kessler, G. Kramer, M. Stöhrer Eur Urol 2009 Jul;56(1):81-8
GUIDELINES ON NEURO-UROLOGY (Text update pril 2014) J. Pannek (co-chair), B. Blok (co-chair), D. Castro-Diaz, G. del Popolo, J. Groen, G. Karsenty, T.M. Kessler, G. Kramer, M. Stöhrer Eur Urol 2009 Jul;56(1):81-8
Neurourology, especially the video urodynamic
 NEUROUROLOGIC FINDINGS WITH APPLICABILITY TO INCONTINENCE AND URETHRAL FUNCTION * Edward J. McGuire, MD ABSTRACT Neurourology is applicable to urinary incontinence and obstructive uropathy in the general
NEUROUROLOGIC FINDINGS WITH APPLICABILITY TO INCONTINENCE AND URETHRAL FUNCTION * Edward J. McGuire, MD ABSTRACT Neurourology is applicable to urinary incontinence and obstructive uropathy in the general