How to make the best use of the natural cycle for frozen-thawed embryo transfer?
|
|
|
- Vivien O’Connor’
- 6 years ago
- Views:
Transcription



1 How to make the best use of the natural cycle for frozen-thawed embryo transfer? Ariel Weissman, MD IVF Unit, Dep. Ob/Gyn Wolfson Medical Center, Holon Sackler Faculty of Medicine, Tel Aviv University Disclosure information: Nothing to declare
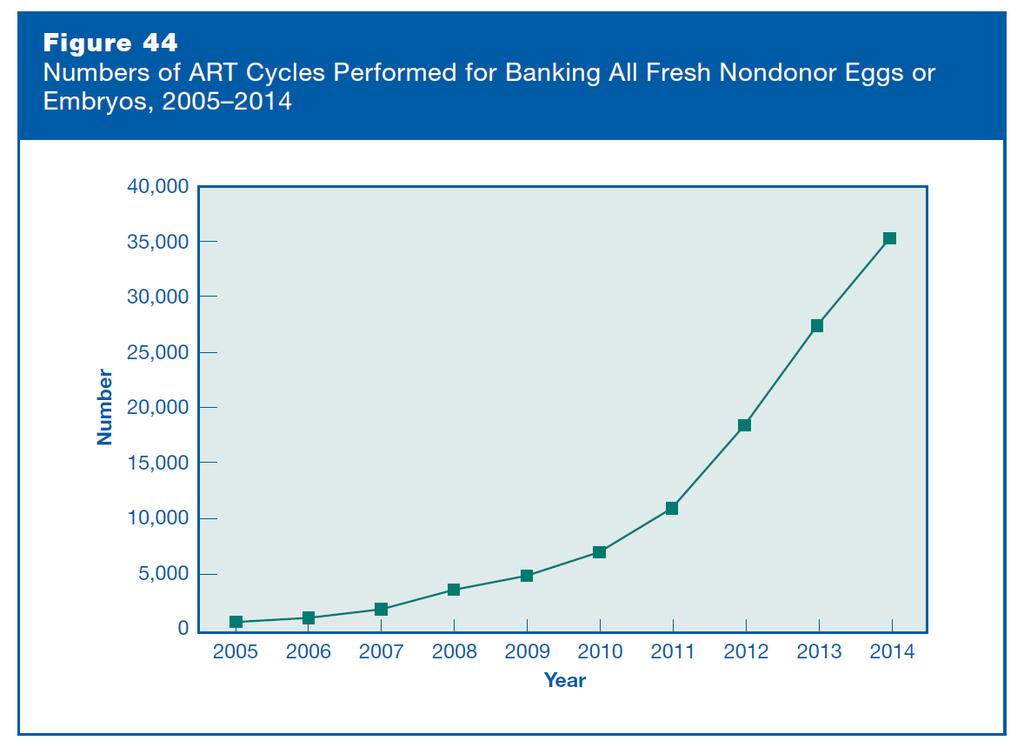
2 Embryo cryopreservation is on the rise Trends in the ratio of the numbers of reported frozen thawed embryo transfers to reported fresh cycle starts in each SART age group. From 2006 to 2012, the number of autologous FET reported to SART increased 82.5%, whereas fresh cycle starts increased by 3.1% Shapiro et al., Fertil Steril 102; 3-9: 2014
3
4
5 Why is the utilization of embryo cryopreservation on the rise? Improved cryopreservation techniques with reduced embryo cryo-damage Increased success rates Reassuring safety data Increased use of single embryo transfer Limitations on the number of embryos to be transferred Frequent use of a GnRH agonist trigger to prevent OHSS in high responders Increased use of GnRH antagonist protocols Increased use of PGS Transfer of confirmed euploid embryos may contribute to increasing FET success rates Increased use of elective cycle segmentation freeze all Suggested improved live birth rates and perinatal outcome Increased awareness to conditions with adverse outcome Premature P elevation, poor endometrial development, fluid in cavity, etc.
6 An exponential growth of FET utilization in clinical practice The most effective method to prepare the endometrium prior to FET is still a matter of debate Preparation of the endometrium in FET cycles I. Natural cycle With or without hcg administration With or without luteal phase support II. Artificial preparation of the endometrium [E+P] With or without GnRH-agonist down-regulation III. Stimulated cycles by gonadotropins/cc/ais
7 Terminology The International Society for Mild Approaches in Assisted Reproduction (ISMAAR) Natural cycle IVF: Modified natural cycle IVF: Unstimulated, spontaneous IVF cycle Semi-natural, controlled natural cycle IVF Nargund et al., Hum Reprod 2007

8
9 Why should we do natural/modified natural cycle FET? Pros: Natural/physiologic preparation of the endometrium for implantation No/minimal amount of medication required No prolonged and heavy luteal phase support required Time taken to complete the cycle is short Cons: Not an option for patients with irregular cycles Not an option for patients with limited access to monitoring Requires more intense monitoring Limited flexibility in timing embryo warming and transfer
10 What is the optimal means of preparing the endometrium in frozen-thawed embryo transfer cycles? A systematic review and meta-analysis Groenewoud et al. Hum Reprod Update. 2013;19: Groenewoud et al. Hum Reprod Update. 2017;23:
11 A randomized controlled, non-inferiority trial of modified natural versus artificial cycle for cryo-thawed embryo transfer: the ANTARCTICA trial Live birth Clinical Pregnancy Ongoing pregnancy Cancellation Cost Non-inferiority RCT From February 2009 to April patients included; 959 available for analysis. The primary outcome: live birth mnc-fet (57/495) 11.5% (94/495) 19% (57/495) 11.5% (101/495) 20.4% AC-FET (41/464) 8.8% (74/464) 16% 45/ % 124/ % Odds Ratio absolute dif % CI Conclusion: AC-FET is non-inferior to mnc-fet with regard to LBRs, clinical and ongoing pregnancy rates but AC-FET does result in higher cancellation rates P Groenewoud et al. Hum Reprod 2016
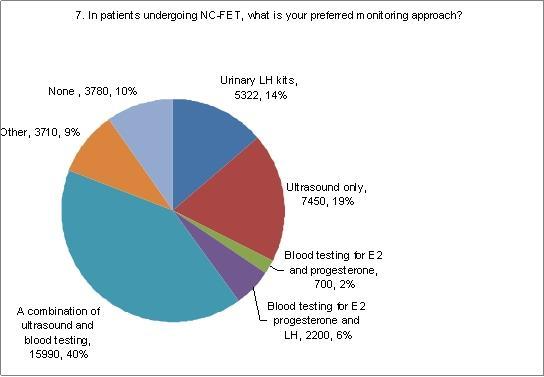
12 How to make the best use of the natural cycle for frozen-thawed embryo transfer? When should we carry out natural/modified natural cycle FET? Should we trigger or just detect ovulation? Should we add luteal phase support? How should we monitor the cycle?

13 When should we carry out natural/modified natural cycle FET?


14 When should we carry out natural/modified natural cycle FET?
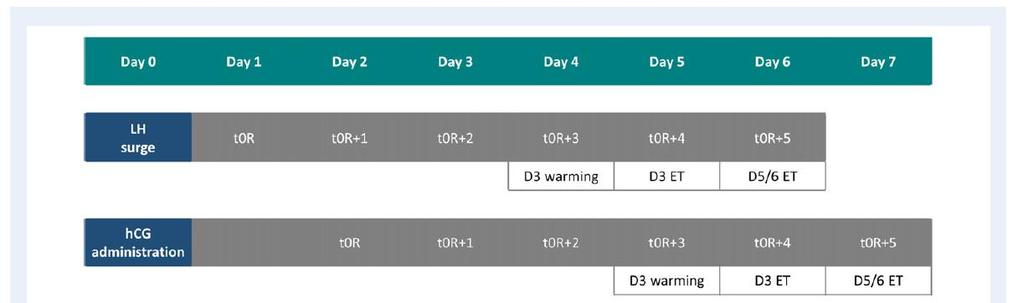
15 Does time from egg retrieval to embryo transfer affects live birth rates in a frozen embryo transfer cycles? Ref. Location Type Protocol CPR Immediate CPR delayed P value Mass et al. ASRM 2008 Stanford CA Retrospective HRT After failed fresh ET n= % n=166 21% 0.01 Santos-Ribeiro et al. Hum Reprod 2016 Brussels + Ho Chi Minh City Retrospective HRT After freeze all n= % n= % NS after multivariable regression analysis Santos-Ribeiro et al. Fertil Steril 2016 Brussels Retrospective HRT+NC After failed fresh ET n= % n= % Adjusted P Lattes et al. Hum Reprod 2017 Barcelona Retrospective HRT After freeze all n=263 LBR 37.6% n=249 LBR 27.3% 0.01 NS after multivariable regression analysis
16 When should we carry out natural/modified natural cycle FET? Level III data No evidence to support a washout period Best estimate: A washout period is not necessary Treatment can start right away
17 How to make the best use of the natural cycle for frozen-thawed embryo transfer? When should we carry out natural/modified natural cycle FET? Should we trigger or just detect ovulation? Should we add luteal phase support? How should we monitor the cycle?
18 Why should we use hcg in modified natural cycle FET? Pros: Allows timing of ovulation and embryo warming and transfer Allows some flexibility in timing embryo warming and transfer Shortens and simplifies the monitoring phase Provides luteal support in the form of hcg in case of possible luteal dysfunction Cons: Increased cost Inconvenience Adverse effect on endometrium? Yanushpolsky and Casper Fertil Steril 2016 Fatemi et al., Fertil Steril 2010 Montagut et al. Hum Reprod 2016
 drop of serum E2 concentration compared with the previous test (ii) rise of serum progesterone")
19 MNC Criteria for HCG administration included: (i) visualization of a leading follicle >17 mm in diameter by TVS (ii) serum E2 concentration >150 pg/ml (iii) serum progesterone concentration <1 ng/ml. NC Cycles monitored until documentation of ovulation Criteria for ovulation detection included: (i) drop of serum E2 concentration compared with the previous test (ii) rise of serum progesterone concentration >1.5 ng/ml (iii) disappearance or typical change in the shape of the leading follicle. In both groups, endometrial thickness 7 mm was considered mandatory for proceeding with embryo thawing Weissman et al. RBM Online 2009 Weissman et al. RBM Online 2011
20 ASRM 2009
21 RCT
22 Should we carry out natural/modified natural cycle FET? Conclusion: With hcg ovulation triggering: Significantly reduced number of monitoring visits No adverse effect on cycle outcome 2009
23 n=61 n=63 LH topu Day 3 Surge LH topu Day 3 Surge warming and transfer warming and transfer Ongoing PR 31.1% Ongoing PR 14.3% // Study was stopped hcg 5000 IU
24 A significant difference in the number of visits between the two groups 4.1±1.4 vs. 2.6 ± 1.1, P=0.001 Hypothesis: an adverse endometrial effect of hcg

25
 Following NC-FET + LPS (aor 1.67, 95% CI 1.31 2.")
26 Frozen thawed embryo transfers in natural cycles with spontaneous or induced ovulation CPR 29.7% 39.9% 46.9% NC-FET vs mnc-fet+lps P < NC-FET+LPS vs mnc-fet+lps P = After adjusting for potential confounders CPRs remained consistently higher: Following NC-FET (aor 2.18, 95% CI ) Following NC-FET + LPS (aor 1.67, 95% CI ) Conclusion: hcg may have a negative effect on endometrium receptivity Montagut et al. Hum Reprod 2016
27 mnc vs. artificial endometrial preparation for frozen-thawed single euploid blastocyst transfer RCT 236 patients undergoing euploid blastocyst FET mnc: hcg triggering + daily P-in-oil Artificial: GnRH-a down regulation+ oral E + P-in-oil No. of visits Cost comparison ( ) Implantation rate(%) Clinical pregnancy (%) Live birth rate (%) Conclusion: mnc n= ± ± (54.1) 59 (54.1) 50 (45.8) Artificial cycle n= ± ± (50.04) 57 (50.4) 47 (41.5) P value Both protocols are equally effective in terms of clinical outcomes, cost-benefit and patient compliance Greco et al. J Assist Reprod Genet 2016
28 Comparison of pregnancy outcomes between true NC-FET and modified NC-FET Clinical pregnancy Odds ratio (OR) adjusted: OR 0.90, 95% CI Ongoing pregnancy Odds ratio (OR) adjusted: OR % CI Groenewoud et al. Hum Reprod Update. 2013;19: Groenewoud et al. Hum Reprod Update. 2017;23:
29 Should we trigger or just detect ovulation? Level II data No clear evidence to support or refute ovulation triggering Best estimate: Ovulation triggering may simplify the monitoring and aid in programming the transfer
30 How to make the best use of the natural cycle for frozen-thawed embryo transfer? When should we carry out natural/modified natural cycle FET? Should we trigger or just detect ovulation? Should we add luteal phase support? How should we monitor the cycle?

31
32 Should luteal phase support be used in NC-FET? RCT- hcg for luteal support 450 women with regular cycles undergoing NC- FET Serial serum hormonal concentrations (E2+LH) were used to time natural ovulation US was performed to measure the endometrial thickness the day after the LH surge LH topu topu+1 topu+2 topu+3 topu+4 topu+5 topu+6 topu+7 Surge LH topu Day 2 warming and transfer Surge hcg 1500 IU/ NS hcg 1500 IU/ NS Lee et al. Hum Reprod 2017
33 Should luteal phase support be used in NC-FET? hcg (n=225) Control (n=225) OR 95% CI P Implantation Rate (%) 88/382 (23) 98/375 (26.1) Clinical Pregnancy (%) 74 (32.9) 82 (36.4) Live birth (%) 57 (25.3) 65 (28.9) Conclusion: the use of hcg in natural cycle FET dose not improve the ongoing pregnancy rate Lee et al. Hum Reprod 2017
34 Luteal phase support in NC- FET RCT 435 patients Ovulation detected by urinary LH kits Embryo warming and transfer 3 days after the LH surge Embryo freezing details NA LBR Natural cycle with vaginal P (400mg*2) (n=219) 29.7%* Natural cycle without P supplementation (n=216) 20.4% *P<0.05 Conclusion: Progesterone supplementation improves LBR after embryo transfer in natural cycles Bjuresten et al. Fertil Steril 2011
35 Luteal phase support in mnc-fet RCT 102 patients hcg given when follicle >18 mm and endometrium > 8 mm D3 vitrification CPR Natural cycle with hcg ovulation triggering + IM P (n=51) 33.3% Natural cycle with hcg ovulation triggering (n=51) 27.5% Conclusion: Luteal phase support does not affect clinical pregnancy rates in MNC-FET cycles Eftekhar et al. Int J Fertil Steril 2013
36 Luteal phase support in mnc-fet Ovulation triggered by hcg Group A- no luteal support Group B luteal support From day of presumed ovulation- Endometrin Vag. 100 mg, b.i.d. No luteal support With luteal support p n Clinical pregnancy (%) 5/22 (22.7) 11/29 (37.9) Miscarriage rate (%) 2/5 (40) 4/11 (36.3) 1.00 Ongoing/delivery (%) 3/22 (13.6) 7/29 (24.1) Implantation rate (%) 5/41 (12) 12/62 )19) Weissman et al. Clinicaltrials.gov NCT
37 Should we add luteal phase support? Level II data No distinction between the use or non use of hcg trigger No evidence to support or refute luteal phase support Best estimate: Luteal phase support in NC/mNC-FET may be unnecessary
38 How to make the best use of the natural cycle for frozen-thawed embryo transfer? When should we carry out natural/modified natural cycle FET? Should we trigger or just detect ovulation? Should we add luteal phase support? How should we monitor the cycle?
39
40 How tight should monitoring mnc/nc be? How important is LH monitoring? Prospective non-randomized trial Single center, 2-year period 233 cycles analyzed US monitoring: hcg given with follicle 17 mm Blood drawn for LH+P Patients and physicians blinded for LH results The primary outcome: ongoing pregnancy Results: LH surge (>10 IU/L) was observed in 52.4% of cycles LH surge No LH surge RR 95% CI P Clinical pregnancy 38.7% 38.5% NS Ongoing pregnancy 33.4% 34.8% NS Conclusion: LH surges demonstrate no significant effect on pregnancy rates Single LH determination prior to ovulation induction in mnc-fet does not seem to have added clinical value. Groenewoud et al. RBM Online 2012
41 The incidence and effect of elevated P levels before ovulation triggering in mnc-fet mnc arm of the ANTARCTICA trial 271 patients received hcg when follicle mm Blood drawn for E2, P and LH, results unavailable 24.4% Elevated P ( 4.6 nmol/l) Low P (<4.6 nmol/l) OR 95% CI Live birth rate 12.9% 10.6% % Elevated P and LH (>10) Low P and LH OR 95% CI Live birth rate 11.9% 17.5% Groenewoud et al. RBM Online 2017
42 Figure 1 Effect of preovulatory P elevation in NC-FET (28.4%) 23.6% 3.6% 1.15% Clinical and ongoing pregnancy rates of subjects with (>5 nmol/l) no P rise, or 2 day, 2 days, and 3 days of P rise Lee et al. Fertil Steril 2014
43 How to make the best use of the natural cycle for frozen-thawed embryo transfer? Summary and recommendations: Washout period: unnecessary Use hcg trigger: save time and money, increase convenience Luteal phase support: most likely unnecessary Best monitoring regimen: unresolved
44
45
46 New RCT: Clinicaltrials.gov NCT Prospective randomized clinical trial- Wolfson MC Ethics committee approval Written informed consent Inclusion criteria NC FET Age < 39 Regular menstrual cycle(25-35 days) Randomization: computer-generated random numbers on the day of inclusion Both the patients and the clinicians were aware of the allocated arm ofclinicaltrials.gov NCT
47 All patients were serially followed by transvaginal ultrasound and blood levels of estradiol and progesterone Ovulation was triggered by hcg (Ovitrelle, Merck Serono) 250 mg Endometrial thickness 7 mm A follicle of 17 mm Progesterone < 3.7 nmol/l,e2 700 pmol/l Group A- no luteal support Group B luteal support From day of presumed ovulation Endometrin Vag. 100 mg, b.i.d.
48 Results: 64 patients recruited (still ongoing) 41 are included in the interim analysis 23 patients were excluded from the analysis 5 patients have not completed their cycles yet 12 patients ovulated spontaneously (without hcg ) 2 patients had no viable embryos after thawing 4 patients failed to ovulate within 4 weeks of follow up > switched to a hormone replacement Patients in both groups were comparable in terms of demographic, clinical and embryology data
49 No luteal support With luteal support p n Age at freezing (years) 31.75± ± Age at FET (years) 33.5± ± Slow freeze vs. Vitrification 3/12 5/ No. frozen 5.8± ± No. thawed 2.42± ± No. transferred 2.0± ± No. of visits 3.0± ± Day of hcg 14.1± ± Endometrial thickness (mm) 8.7± ± E2 on hcg administration (pmol/l) ± ± P on hcg administration (nmol/l) 2.09± ± Dominant follicle size (mm) 18.9± ±

50 Clinical variables to be considered before choosing the optimal endometrial preparation for frozen-thawed embryo transfer Final decision must be based on individualization of the treatment based on patient characteristics prior to FET Ortegaa and Garcıa Velasco Curr Opin Obstet Gynecol 2015
 were used to time natural ovulation US was performed to measure the endometrial thickness the day after")
51 Should luteal phase support be used in NC-FET? 450 women with regular cycles undergoing NC- FET Serial serum hormonal concentrations (E2+LH) were used to time natural ovulation US was performed to measure the endometrial thickness the day after the LH surge Day 2 cleavage embryos were replaced FET on the third day after the LH surge Patients were randomized into either: Treatment group: 1500 IU hcg on the day of FET and 6 days after FET Control group: normal saline on these 2 days Lee et al. Hum Reprod 2017

52 Should luteal phase support be used in NC-FET? Conclusion: the use of hcg in natural cycle FET dose not improve the ongoing pregnancy rate Lee et al. Hum Reprod 2017
53 Levels of Evidence for Clinical Studies
54 Luteal phase support in NC/MNC FET Retrospective study 452 cycles hcg triggering when follicle 17 mm and endometrial thickness 7 mm Embryo warming and transfer 3 days after the LH surge Embryo freezing details NA Ongoing PR Natural cycle with hcg ovulation triggering + vag P (n=219) 22% Natural cycle with hcg ovulation triggering (n=216) 21% Conclusion: There is no convincing evidence to support the use of LPS in hcg-induced natural FET cycles, since there is no luteal phase defect Kyrou et al. Eur J Obstet Gynecol Reprod Biol 2010
55 Cycle regimens of vitrification thawed blastocyst transfer Retrospective analysis 611 patients (648 cycles) of blastocyst FET CPR Natural cycle + LS (n=310) 41.9%* Natural cycle with hcg ovulation triggering + LS (n=134) 41.8% Hormonally manipulated artificial cycle (n=204) 30.4%* Multivariate logistic regression analysis: *Significant difference in clinical pregnancy rate between Groups 3 and 1 OR ; 95% CI , P=0.006 Conclusion: In vitrification- thawed blastocyst transfer natural cycles with or without hcg treatment is associated with better outcomes than was the use of hormonally manipulated cycles. Chang et al. J Assist Reprod Genet 2011
 Clinical pregnancy/et (%) Deliveries/ET (%) Total pregnancy loss Natural cycle with luteal P 1019 272 (27.6) 248 (24.3) 211 (20.7) 61 (22.")
56 Retrospective analysis FET cycles Natural cycle + LS (26%; n=1,168) Natural cycle with hcg ovulation triggering + no LS (10%; n=444) Hormonally manipulated artificial cycle (64%; n=2,858) # ET Pregnancy test/et (%) Clinical pregnancy/et (%) Deliveries/ET (%) Total pregnancy loss Natural cycle with luteal P (27.6) 248 (24.3) 211 (20.7) 61 (22.4) Natural cycle with hcg induction (35.5) 95 (29.1) 77 (23.5) 39 (33.6) Substituted cycles (34.3) 691 (27.7) 500 (20.1) 354 (41.5) P value < NS NS < A logistic regression analysis showed that the type of protocol was the only predictor of pregnancy loss
57 Embryo cryopreservation is on the rise Trends in the ratio of the numbers of reported frozen thawed embryo transfers to reported fresh cycle starts in each SART age group. Trends in RR for live birth per transfer in FET vs. fresh transfer by SART age group. An RR exceeding 1.0 indicates greater birth rate with FET. From 2006 to 2012, the number of autologous FET reported to SART increased 82.5%, whereas fresh cycle starts increased by 3.1% By 2012 the birth rate per transfer with FET exceeded that for fresh transfer in the four oldest age groups. Shapiro et al., Fertil Steril 102; 3-9: 2014
58 hcg administered for the final oocyte maturation could potentially cause a luteal phase defect by suppressing the LH production via a short-loop feedback mechanism Miyake, et al., Fertil Steril 1982;36:251 2 The administration of hcg did not down-regulate the LH secretion in the luteal phase of normal, unstimulated cycles in normo-ovulatory women Tavaniotou and Devroey, Fertil Steril 2003; 80:654 5
59 mnc vs. artificial endometrial preparation for frozen-thawed single euploid blastocyst transfer RCT 236 patients undergoing euploid blastocyst FET mnc: hcg triggering + daily P-in-oil Artificial: GnRH-a down regulation+ oral E + P-in-oil No. of visits Cost comparison ( ) Implantation rate(%) Clinical pregnancy (%) Live birth rate (%) Conclusion: mnc n= ± ± (54.1) 59 (54.1) 50 (45.8) Artificial cycle n= ± ± (50.04) 57 (50.4) 47 (41.5) P value Both protocols are equally effective in terms of clinical outcomes, cost-benefit and patient compliance Greco et al. J Assist Reprod Genet 2016
60 A significant difference in the number of visits between the two groups 4.1±1.4 vs. 2.6 ± 1.1, P=0.001 Hypothesis: an adverse endometrial effect of hcg In fact, the interval between the LH surge in NC-FET cycles and the ovulation trigger in the mnc-fet cycles in that study was identical, which may have resulted in a clinical mismatch between the endometrial and embryo developmental stage in the hcg-triggered study arm Montagut et al. Hum Reprod 2016
61 How to make the best use of the natural cycle for frozen-thawed embryo transfer? When should we carry out natural/modified natural cycle FET? How should we monitor the cycle? Should we trigger or just detect ovulation? Should we add luteal phase support? What else can we do to improve cycle outcome?
62 NC-FET: how can we improve the outcome? Day -1 Day 0 Day 1 Day 2 Day 3 Day 4 Day 5 Day 6 Day 7 LH topu topu+1 topu+2 topu+3 topu+4 topu+5 topu+6 topu+7 Surge US+LH+E2+P monitoring LH topu Day 3 Surge warming Vag P Vag P Vag P and transfer Vag P Vag P Vag P Vag P hcg 250 mcg Orvieto et al. JARG 2016 Triptorelin 0.1 mg
63 NC I NC II HRT I HRT II n No. ET 1.8± ± ± ±0.8 IR 24/139 (17%) 33/106 (31%)* 29/213 (14%) 15/98 (15%) CPR 19/74 (26%) 30/59 (51%)* 26/113 (23%) 12/54 (22%) Ongoing PR 15/74 (20%) 27/59 (46%)* 18/113 (16%) 9/54 (17%) CPR: gestational sac Ongoing PR: FHB * P <0.05 Conclusion: hcg + GnRH-a modified luteal support may be the preparation protocol of choice
64 Effect of mid-luteal phase GnRH agonist on FET outcome during natural cycles RCT 98 patients US monitoring for follicle size and endo thickness Ovulation detected by urinary LH kit Crossover design The primary outcome: positive PR, CPR, LBR LH topu topu+1 topu+2 topu+3 topu+4 topu+5 topu+6 topu+7 Surge LH topu Day 3 Surge warming and transfer Vag P Vag P Vag P Vag P Vag P Triptorelin 0.1 mg Seikkula et al. Gynecol Endocrinol 2016
65 Effect of mid-luteal phase GnRH agonist on FET outcome during natural cycles GnRH-agonist n=65 Control n=62 OR 95% CI P Clinical Pregnancy 25 (38.7 %) 17 (27.4%) Live birth 20 (30.8%) 15 (24.2%) Miscarriage 3 (12%) 2 (11.8%) Conclusion: No statistically significant benefit of the single-dose triptorelin combined with routine luteal support in natural FET cycles In theory, GnRHa supplementation could enhance embryo development, corpus luteum function and endometrial receptivity in natural FET cycles as well Larger randomized controlled studies on natural FET cycles are needed Seikkula et al. Gynecol Endocrinol 2016

66 How to make the best use of the natural cycle for frozen-thawed embryo transfer? Summary and recommendations: Washout period: unnecessary Use hcg trigger: save time and money, increase convenience Luteal phase support: most likely unnecessary Best monitoring regimen: unresolved Luteal GnRH-a: awaits confirmation by large RCTs
How to make the best use of the natural cycle for frozen-thawed embryo transfer?
 How to make the best use of the natural cycle for frozen-thawed embryo transfer? Ariel Weissman, MD IVF Unit, Dep. Ob/Gyn Wolfson Medical Center, Holon Sackler Faculty of Medicine, Tel Aviv University
How to make the best use of the natural cycle for frozen-thawed embryo transfer? Ariel Weissman, MD IVF Unit, Dep. Ob/Gyn Wolfson Medical Center, Holon Sackler Faculty of Medicine, Tel Aviv University
Endometrial Preparation for Frozen Embryo Transfer (FET) Zitao Liu, MD, PhD New Hope Fertility Center, NY
 Zitao Liu, MD, PhD New Hope Fertility Center, NY") Endometrial Preparation for Frozen Embryo Transfer (FET) Zitao Liu, MD, PhD New Hope Fertility Center, NY Natural Cycle FET Protocol for endometrial preparation N FET, including modified N FET HRT FET:
Endometrial Preparation for Frozen Embryo Transfer (FET) Zitao Liu, MD, PhD New Hope Fertility Center, NY Natural Cycle FET Protocol for endometrial preparation N FET, including modified N FET HRT FET:
A Tale of Three Hormones: hcg, Progesterone and AMH
 A Tale of Three Hormones: hcg, Progesterone and AMH Download the Ferring AR ipad/iphone app from the Apple Store: http://bit.ly/1okk74m Interpreting Follicular Phase Progesterone Ernesto Bosch IVI Valencia,
A Tale of Three Hormones: hcg, Progesterone and AMH Download the Ferring AR ipad/iphone app from the Apple Store: http://bit.ly/1okk74m Interpreting Follicular Phase Progesterone Ernesto Bosch IVI Valencia,
Spontaneous ovulation versus HCG triggering for timing natural-cycle frozen thawed embryo transfer: a randomized study
 Reproductive BioMedicine Online (2011) 23, 484 489 www.sciencedirect.com www.rbmonline.com ARTICLE Spontaneous ovulation versus HCG triggering for timing natural-cycle frozen thawed embryo transfer: a
Reproductive BioMedicine Online (2011) 23, 484 489 www.sciencedirect.com www.rbmonline.com ARTICLE Spontaneous ovulation versus HCG triggering for timing natural-cycle frozen thawed embryo transfer: a
Luteal phase rescue after GnRHa triggering Progesterone and Estradiol
 Luteal phase rescue after GnRHa triggering Progesterone and Estradiol L. Engmann University of Connecticut Disclaimer Fertility Speaker Bureau Merck Pharmaceuticals Introduction GnRH agonist is effective
Luteal phase rescue after GnRHa triggering Progesterone and Estradiol L. Engmann University of Connecticut Disclaimer Fertility Speaker Bureau Merck Pharmaceuticals Introduction GnRH agonist is effective
Disclosure. Lyubov Mykhaylshyn IVF department Alternativa clinic Lviv, Ukraine
 Disclosure Lyubov Mykhaylshyn IVF department Alternativa clinic Lviv, Ukraine I do not currently have, nor have I had in the 12 months preceding the activity, a vested interest or affiliation with any
Disclosure Lyubov Mykhaylshyn IVF department Alternativa clinic Lviv, Ukraine I do not currently have, nor have I had in the 12 months preceding the activity, a vested interest or affiliation with any
LUTEAL PHASE SUPPORT. Doç. Dr. Nafiye Yılmaz. Zekai Tahir Burak Kadın Sağlığı Eğitim Araştırma Hastanesi
 LUTEAL PHASE SUPPORT Doç. Dr. Nafiye Yılmaz Zekai Tahir Burak Kadın Sağlığı Eğitim Araştırma Hastanesi TAJEV, 2014 1 ART & success *Live birth rate 2 Optimal luteal phase Etiology of luteal phase deficiency
LUTEAL PHASE SUPPORT Doç. Dr. Nafiye Yılmaz Zekai Tahir Burak Kadın Sağlığı Eğitim Araştırma Hastanesi TAJEV, 2014 1 ART & success *Live birth rate 2 Optimal luteal phase Etiology of luteal phase deficiency
Progesterone and clinical outcomes
 Synchronization of Slowly Developing Embryos Restores Implantation Success Richard T. Scott, Jr, MD, HCLD Clinical and Scientific Director, Reproductive Medicine Associates of New Jersey Professor and
Synchronization of Slowly Developing Embryos Restores Implantation Success Richard T. Scott, Jr, MD, HCLD Clinical and Scientific Director, Reproductive Medicine Associates of New Jersey Professor and
Universal Embryo Cryopreservation: Frozen versus Fresh Transfer. Zaher Merhi, M.D.
 Universal Embryo Cryopreservation: Frozen versus Fresh Transfer Zaher Merhi, M.D. Disclosure: None Fewer complications with IVF 1.5% children in US are born through ART 1.1 million children since 2006
Universal Embryo Cryopreservation: Frozen versus Fresh Transfer Zaher Merhi, M.D. Disclosure: None Fewer complications with IVF 1.5% children in US are born through ART 1.1 million children since 2006
Interpreting follicular Progesterone: Late follicular Progesterone to Estradiol ratio is not influenced by protocols or gonadotropins used
 Interpreting follicular Progesterone: Late follicular Progesterone to Estradiol ratio is not influenced by protocols or gonadotropins used Ellenbogen A., M.D., Shalom-Paz E., M.D, Asalih N., M.D, Samara
Interpreting follicular Progesterone: Late follicular Progesterone to Estradiol ratio is not influenced by protocols or gonadotropins used Ellenbogen A., M.D., Shalom-Paz E., M.D, Asalih N., M.D, Samara
A survey on luteal phase support:
 A survey on luteal phase support: An IVF Worldwide Survey results I have no conflict of interest! The reason why luteal phase support is needed: The normal physiological support of the corpus luteum the
A survey on luteal phase support: An IVF Worldwide Survey results I have no conflict of interest! The reason why luteal phase support is needed: The normal physiological support of the corpus luteum the
Recent Developments in Infertility Treatment
 Recent Developments in Infertility Treatment John T. Queenan Jr., MD Professor, Dept. Of Ob/Gyn University of Rochester Medical Center Rochester, NY Disclosures I don t have financial interest or other
Recent Developments in Infertility Treatment John T. Queenan Jr., MD Professor, Dept. Of Ob/Gyn University of Rochester Medical Center Rochester, NY Disclosures I don t have financial interest or other
Poor & Hyper responders: what is the best approach?
 Poor & Hyper responders: what is the best approach? A. La Marca ObGyn Dept University of Modena and Reggio Emilia Italy Center for Reproductive Medicine University Hospital of Modena Italy Criteria used
Poor & Hyper responders: what is the best approach? A. La Marca ObGyn Dept University of Modena and Reggio Emilia Italy Center for Reproductive Medicine University Hospital of Modena Italy Criteria used
Thrombosis during assisted reproduction. Scott Nelson Muirhead Chair in Obstetrics & Gynaecology
 Thrombosis during assisted reproduction Scott Nelson Muirhead Chair in Obstetrics & Gynaecology ART can be as safe as natural pregnancy!! What used to be the risk of thrombosis in ART!! We can use AMH
Thrombosis during assisted reproduction Scott Nelson Muirhead Chair in Obstetrics & Gynaecology ART can be as safe as natural pregnancy!! What used to be the risk of thrombosis in ART!! We can use AMH
Natural Cycle & Mild stimulation IVF/ICSI in women with Poor Ovarian Response (POR)
") Natural Cycle & Mild stimulation IVF/ICSI in women with Poor Ovarian Response (POR) Geeta Nargund Head of Reproductive Medicine St George s Hospital London ISMAAR Terminology Human Reprod Nargund et al
Natural Cycle & Mild stimulation IVF/ICSI in women with Poor Ovarian Response (POR) Geeta Nargund Head of Reproductive Medicine St George s Hospital London ISMAAR Terminology Human Reprod Nargund et al
Principles of Ovarian Stimulation
 Principles of Ovarian Stimulation Dr Genia Rozen Gynaecologist and Fertility Specialist Royal Women s Hospital and Melbourne IVF Learning objectives Why ovarian stimulation Recap physiology Ovarian cycle
Principles of Ovarian Stimulation Dr Genia Rozen Gynaecologist and Fertility Specialist Royal Women s Hospital and Melbourne IVF Learning objectives Why ovarian stimulation Recap physiology Ovarian cycle
IVF Protocols: Hyper & Hypo-Responders, Implantation
 IVF Protocols: Hyper & Hypo-Responders, Implantation Midwest Reproductive Symposium June 4-5, 4 2010 Subset : Hyper-Responders Mark R. Bush, MD, FACOG, FACS OBJECTIVE: Important goals for the PCOS patient
IVF Protocols: Hyper & Hypo-Responders, Implantation Midwest Reproductive Symposium June 4-5, 4 2010 Subset : Hyper-Responders Mark R. Bush, MD, FACOG, FACS OBJECTIVE: Important goals for the PCOS patient
STIMULATION AND OVULATION TRIGGERING
 STIMULATION AND OVULATION TRIGGERING Professor IOANNIS E. MESSINIS MD, PhD (Aberdeen, UK), FRCOG (UK) Department of Obs/Gynae University of Thessaly Larissa, GREECE DISCLOSURE Nothing to disclose Learning
STIMULATION AND OVULATION TRIGGERING Professor IOANNIS E. MESSINIS MD, PhD (Aberdeen, UK), FRCOG (UK) Department of Obs/Gynae University of Thessaly Larissa, GREECE DISCLOSURE Nothing to disclose Learning
Is it the seed or the soil? Arthur Leader, MD, FRCSC
 The Physiological Limits of Ovarian Stimulation Is it the seed or the soil? Arthur Leader, MD, FRCSC Objectives 1. To consider how ovarian stimulation protocols work in IVF 2. To review the key events
The Physiological Limits of Ovarian Stimulation Is it the seed or the soil? Arthur Leader, MD, FRCSC Objectives 1. To consider how ovarian stimulation protocols work in IVF 2. To review the key events
IVF AND PREIMPLANTATION GENETIC TESTING FOR ANEUPLOIDY (PGT-A) WHAT THE COMMUNITY PHYSICIAN NEEDS TO KNOW
 WHAT THE COMMUNITY PHYSICIAN NEEDS TO KNOW") IVF AND PREIMPLANTATION GENETIC TESTING FOR ANEUPLOIDY (PGT-A) WHAT THE COMMUNITY PHYSICIAN NEEDS TO KNOW Jon Havelock, MD, FRCSC, FACOG Co-Director - PCRM Disclosure No conflict of interest in relation
IVF AND PREIMPLANTATION GENETIC TESTING FOR ANEUPLOIDY (PGT-A) WHAT THE COMMUNITY PHYSICIAN NEEDS TO KNOW Jon Havelock, MD, FRCSC, FACOG Co-Director - PCRM Disclosure No conflict of interest in relation
Results of the Virtual Academy of Genetics (VAoGEN) questionnaire on Mosaicism in PGS
 questionnaire on Mosaicism in PGS") Results of the Virtual Academy of Genetics (VAoGEN) questionnaire on Mosaicism in PGS Ariel Weissman, MD IVF Unit, Dep. Ob/Gyn Wolfson Medical Center, Holon Sackler Faculty of Medicine, Tel Aviv University
Results of the Virtual Academy of Genetics (VAoGEN) questionnaire on Mosaicism in PGS Ariel Weissman, MD IVF Unit, Dep. Ob/Gyn Wolfson Medical Center, Holon Sackler Faculty of Medicine, Tel Aviv University
Disclosure. Robert Fischer Fertility Centre Hamburg Hamburg, Germany. Declared no potential conflict of interest.
 Disclosure Robert Fischer Fertility Centre Hamburg Hamburg, Germany Declared no potential conflict of interest. Updates on Luteal Phase supplementation Kiev 21.09.2018 Robert Fischer MVZ Fertility Center
Disclosure Robert Fischer Fertility Centre Hamburg Hamburg, Germany Declared no potential conflict of interest. Updates on Luteal Phase supplementation Kiev 21.09.2018 Robert Fischer MVZ Fertility Center
L2. Optimising IVF outcomes through increased number of oocytes... 03
 SCIENTIFIC HIGHLIGHTS EXCEMED Blended Education Ovarian stimulation strategies: maximizing efficiency in ART Rio de Janeiro, Brazil 6-7 April 2018 Preface Success rates following IVF treatment have increased
SCIENTIFIC HIGHLIGHTS EXCEMED Blended Education Ovarian stimulation strategies: maximizing efficiency in ART Rio de Janeiro, Brazil 6-7 April 2018 Preface Success rates following IVF treatment have increased
Središnja medicinska knjižnica
 Središnja medicinska knjižnica Kasum M., Kurdija K., Orešković S., Čehić E., Pavičić-Baldani D., Škrgatić L. (2016) Combined ovulation triggering with GnRH agonist and hcg in IVF patients. Gynecological
Središnja medicinska knjižnica Kasum M., Kurdija K., Orešković S., Čehić E., Pavičić-Baldani D., Škrgatić L. (2016) Combined ovulation triggering with GnRH agonist and hcg in IVF patients. Gynecological
Milder is better? Advantages and disadvantages of "mild" ovarian stimulation for human in vitro fertilization
 Milder is better? Advantages and disadvantages of "mild" ovarian stimulation for human in vitro fertilization Revelli et al. Reproductive Biology and Endocrinology 2011, 9:25 Presenter: R2 孫怡虹 Background
Milder is better? Advantages and disadvantages of "mild" ovarian stimulation for human in vitro fertilization Revelli et al. Reproductive Biology and Endocrinology 2011, 9:25 Presenter: R2 孫怡虹 Background
Intérêt de l hcg et induction de l ovulation. Christophe Blockeel, MD, PhD Centre for Reproductive Medicine, Brussels, Belgium
 Intérêt de l hcg et induction de l ovulation Christophe Blockeel, MD, PhD Centre for Reproductive Medicine, Brussels, Belgium Conflict of interest The opinions expressed in this document are the opinions
Intérêt de l hcg et induction de l ovulation Christophe Blockeel, MD, PhD Centre for Reproductive Medicine, Brussels, Belgium Conflict of interest The opinions expressed in this document are the opinions
President : Indian Society for Assisted Reproduction (ISAR) Past President FOGSI. Past Chairman ICOG. Founder Trustee Women s Empowerment Foundation
 Past President FOGSI. Past Chairman ICOG. Founder Trustee Women s Empowerment Foundation") Founder President: The PCOS Society, India Honorary Fellow of the Royal College of Obst.& Gyn. Prof.Duru Shah President : Indian Society for Assisted Reproduction (ISAR) Past President FOGSI. Past Chairman
Founder President: The PCOS Society, India Honorary Fellow of the Royal College of Obst.& Gyn. Prof.Duru Shah President : Indian Society for Assisted Reproduction (ISAR) Past President FOGSI. Past Chairman
Best practices of ASRM and ESHRE
 Best practices of ASRM and ESHRE Late submission Cortina d Ampezzo, Italy 1-3 March 2012 A joint meeting between the American Society for Reproductive Medicine and the European Society of Human Reproduction
Best practices of ASRM and ESHRE Late submission Cortina d Ampezzo, Italy 1-3 March 2012 A joint meeting between the American Society for Reproductive Medicine and the European Society of Human Reproduction
Are all-freeze cycles & frozen-thawed embryo transfers improving IVF outcomes?
 Are all-freeze cycles & frozen-thawed embryo transfers improving IVF outcomes? Andrea Weghofer Foundation for Reproductive Medicine 2017 New York, November 16-19 Conflict of interest No relevant financial
Are all-freeze cycles & frozen-thawed embryo transfers improving IVF outcomes? Andrea Weghofer Foundation for Reproductive Medicine 2017 New York, November 16-19 Conflict of interest No relevant financial
IVM in PCOS patients. Introduction (1) Introduction (2) Michael Grynberg René Frydman
 Introduction (2) Michael Grynberg René Frydman") IVM in PCOS patients Michael Grynberg René Frydman Department of Obstetrics and Gynecology A. Beclere Hospital, Clamart, France Maribor, Slovenia, 27-28 February 2009 Introduction (1) IVM could be a major
IVM in PCOS patients Michael Grynberg René Frydman Department of Obstetrics and Gynecology A. Beclere Hospital, Clamart, France Maribor, Slovenia, 27-28 February 2009 Introduction (1) IVM could be a major
INDICATIONS OF IVF/ICSI
 PROCESS OF IVF/ICSI INDICATIONS OF IVF/ICSI IVF is most clearly indicated when infertility results from one or more causes having no other effective treatment; Tubal disease. In women with blocked fallopian
PROCESS OF IVF/ICSI INDICATIONS OF IVF/ICSI IVF is most clearly indicated when infertility results from one or more causes having no other effective treatment; Tubal disease. In women with blocked fallopian
Freeze-All Policy: Is It Right for Everyone?
 Transcript Details This is a transcript of an educational program accessible on the ReachMD network. Details about the program and additional media formats for the program are accessible by visiting: https://reachmd.com/online-education/non-certified-non-accredited/freeze-all-policy-it-righteveryone/9879/
Transcript Details This is a transcript of an educational program accessible on the ReachMD network. Details about the program and additional media formats for the program are accessible by visiting: https://reachmd.com/online-education/non-certified-non-accredited/freeze-all-policy-it-righteveryone/9879/
Trends in Egg Donation. Vitaly A. Kushnir MD Center for Human Reproduction
 Trends in Egg Donation Vitaly A. Kushnir MD Center for Human Reproduction Disclosures No relevant financial relationships to disclose CHR views the commercial trade in human oocytes with considerable ethical
Trends in Egg Donation Vitaly A. Kushnir MD Center for Human Reproduction Disclosures No relevant financial relationships to disclose CHR views the commercial trade in human oocytes with considerable ethical
The effect of luteal phase progesterone supplementation on natural frozen-thawed embryo transfer cycles
 Original Article Obstet Gynecol Sci 2014;57(4):291-296 http://dx.doi.org/10.5468/ogs.2014.57.4.291 pissn 2287-8572 eissn 2287-8580 The effect of luteal phase progesterone supplementation on natural frozen-thawed
Original Article Obstet Gynecol Sci 2014;57(4):291-296 http://dx.doi.org/10.5468/ogs.2014.57.4.291 pissn 2287-8572 eissn 2287-8580 The effect of luteal phase progesterone supplementation on natural frozen-thawed
Menstruation-free interval and ongoing pregnancy in IVF using GnRH antagonists
 Human Reproduction Vol.21, No.4 pp. 1012 1017, 2006 Advance Access publication December 8, 2005. doi:10.1093/humrep/dei415 Menstruation-free interval and ongoing pregnancy in IVF using GnRH antagonists
Human Reproduction Vol.21, No.4 pp. 1012 1017, 2006 Advance Access publication December 8, 2005. doi:10.1093/humrep/dei415 Menstruation-free interval and ongoing pregnancy in IVF using GnRH antagonists
In vitro fertilization outcome in frozen versus fresh embryo transfer in women with elevated progesterone level on the day of HCG injection: An RCT
 Int J Reprod BioMed Vol. 15. No. 12. pp: 757-762, December 2017 Original article In vitro fertilization outcome in frozen versus fresh embryo transfer in women with elevated progesterone level on the day
Int J Reprod BioMed Vol. 15. No. 12. pp: 757-762, December 2017 Original article In vitro fertilization outcome in frozen versus fresh embryo transfer in women with elevated progesterone level on the day
Honorary Fellow of the Royal College of Obs. & Gyn. First Indian to receive FIGO s Distinguished Merit Award for Services towards women s health.
 Prof.Duru Shah Founder President The PCOS Society (India) President Elect of the Indian Society for Assisted Reproduction (ISAR) Honorary Fellow of the Royal College of Obs. & Gyn. First Indian to receive
Prof.Duru Shah Founder President The PCOS Society (India) President Elect of the Indian Society for Assisted Reproduction (ISAR) Honorary Fellow of the Royal College of Obs. & Gyn. First Indian to receive
Raoul Orvieto. The Chaim Sheba Medical Center Tel Hashomer, Israel. Declared no potential conflict of interest
 Raoul Orvieto The Chaim Sheba Medical Center Tel Hashomer, Israel Declared no potential conflict of interest LH in antagonist cycles; is the story really written? Raoul Orvieto M.D. Israel Overview Role
Raoul Orvieto The Chaim Sheba Medical Center Tel Hashomer, Israel Declared no potential conflict of interest LH in antagonist cycles; is the story really written? Raoul Orvieto M.D. Israel Overview Role
2015 Mar.; 26(1):
:") Journal of Reproduction & Contraception doi: 10.7669/j.issn.1001-7844.2015.01.0022 2015 Mar.; 26(1):22-30 E-mail: randc_journal@163.com Clinical outcomes of using three gonadatropins and medroxyprogestrone
Journal of Reproduction & Contraception doi: 10.7669/j.issn.1001-7844.2015.01.0022 2015 Mar.; 26(1):22-30 E-mail: randc_journal@163.com Clinical outcomes of using three gonadatropins and medroxyprogestrone
Scientific Highlights: First world conference on luteinizing hormone in ART: Landing in Asia Pacific
 This EXCEMED conference followed on from the First world conference on luteinizing hormone (LH) in ART, which took place in Naples in May 2016. Bringing the topic of LH to Asia Pacific provided an opportunity
This EXCEMED conference followed on from the First world conference on luteinizing hormone (LH) in ART, which took place in Naples in May 2016. Bringing the topic of LH to Asia Pacific provided an opportunity
Minimising IVF related mortality and morbidity. Scott Nelson Muirhead Professor in Obstetrics & Gynaecology
 Minimising IVF related mortality and morbidity Scott Nelson Muirhead Professor in Obstetrics & Gynaecology We rarely say no - so what I will cover today VTE as an example of a modifiable IVF complication
Minimising IVF related mortality and morbidity Scott Nelson Muirhead Professor in Obstetrics & Gynaecology We rarely say no - so what I will cover today VTE as an example of a modifiable IVF complication
Pregnancy loss after frozen-embryo transfer a comparison of three protocols
 ORIGINAL ARTICLES: EARLY PREGNANCY Pregnancy loss after frozen-embryo transfer a comparison of three protocols Candido Tomas, M.D., Ph.D., a Birgit Alsbjerg, M.D., b Hannu Martikainen, M.D., Ph.D., c and
ORIGINAL ARTICLES: EARLY PREGNANCY Pregnancy loss after frozen-embryo transfer a comparison of three protocols Candido Tomas, M.D., Ph.D., a Birgit Alsbjerg, M.D., b Hannu Martikainen, M.D., Ph.D., c and
Vaginal micronized progesterone versus intramuscular progesterone for luteal support in women undergoing in vitro fertilization embryo transfer
 Vaginal micronized progesterone versus intramuscular progesterone for luteal support in women undergoing in vitro fertilization embryo transfer Mohamed F. Mitwally, M.D., H.C.L.D., a Michael P. Diamond,
Vaginal micronized progesterone versus intramuscular progesterone for luteal support in women undergoing in vitro fertilization embryo transfer Mohamed F. Mitwally, M.D., H.C.L.D., a Michael P. Diamond,
Agonist versus antagonist in ICSI cycles: a randomized trial and cost effectiveness analysis Badrawi A, Zaki S, Al-Inany H, Ramzy A M, Hussein M
 Agonist versus antagonist in ICSI cycles: a randomized trial and cost effectiveness analysis Badrawi A, Zaki S, Al-Inany H, Ramzy A M, Hussein M Record Status This is a critical abstract of an economic
Agonist versus antagonist in ICSI cycles: a randomized trial and cost effectiveness analysis Badrawi A, Zaki S, Al-Inany H, Ramzy A M, Hussein M Record Status This is a critical abstract of an economic
Treatment of Poor Responders
 Treatment of Poor Responders Pathophysiology of Poor Responders Deficiency in systemic IGF 1 levels (Bahceci, 2007) Lower intra ovarian T levels Reduced FSH receptor expression (Cai, 2007) Bahceci, 2007,
Treatment of Poor Responders Pathophysiology of Poor Responders Deficiency in systemic IGF 1 levels (Bahceci, 2007) Lower intra ovarian T levels Reduced FSH receptor expression (Cai, 2007) Bahceci, 2007,
Comparison of serum and follicular fluid hormone levels with recombinant and urinary human chorionic gonadotropin during in vitro fertilization
 Comparison of serum and follicular fluid hormone levels with recombinant and urinary human chorionic gonadotropin during in vitro fertilization Peter Kovacs, M.D., a Timea Kovats, M.D., a Artur Bernard,
Comparison of serum and follicular fluid hormone levels with recombinant and urinary human chorionic gonadotropin during in vitro fertilization Peter Kovacs, M.D., a Timea Kovats, M.D., a Artur Bernard,
LOW RESPONDERS. Poor Ovarian Response, Por
 LOW RESPONDERS Poor Ovarian Response, Por Patients with a low number of retrieved oocytes despite adequate ovarian stimulation during fertility treatment. Diagnosis Female About Low responders In patients
LOW RESPONDERS Poor Ovarian Response, Por Patients with a low number of retrieved oocytes despite adequate ovarian stimulation during fertility treatment. Diagnosis Female About Low responders In patients
2013 Sep.; 24(3):
:") Journal of Reproduction & Contraception doi: 10.7669/j.issn.1001-7844.2013.03.0151 2013 Sep.; 24(3):151-158 E-mail: randc_journal@163.com Reducing the Trigger Dose of Human Chorionic Gonadotrophin Does
Journal of Reproduction & Contraception doi: 10.7669/j.issn.1001-7844.2013.03.0151 2013 Sep.; 24(3):151-158 E-mail: randc_journal@163.com Reducing the Trigger Dose of Human Chorionic Gonadotrophin Does
Serum progesterone levels on the day of hcg trigger and ICSI outcome: a retrospective observational cohort study
 International Journal of Reproduction, Contraception, Obstetrics and Gynecology Amin KV et al. Int J Reprod Contracept Obstet Gynecol. 2018 Aug;7(8):3194-3198 www.ijrcog.org DOI: http://dx.doi.org/10.18203/2320-1770.ijrcog20183316
International Journal of Reproduction, Contraception, Obstetrics and Gynecology Amin KV et al. Int J Reprod Contracept Obstet Gynecol. 2018 Aug;7(8):3194-3198 www.ijrcog.org DOI: http://dx.doi.org/10.18203/2320-1770.ijrcog20183316
Female Reproductive System. Lesson 10
 Female Reproductive System Lesson 10 Learning Goals 1. What are the five hormones involved in the female reproductive system? 2. Understand the four phases of the menstrual cycle. Human Reproductive System
Female Reproductive System Lesson 10 Learning Goals 1. What are the five hormones involved in the female reproductive system? 2. Understand the four phases of the menstrual cycle. Human Reproductive System
Hongjuan Ye 1*, Hui Tian 1, Wen He 2, Qifeng Lyu 2, Yanping Kuang 2, Qiuju Chen 2* and Lihua Sun 1*
 Ye et al. Reproductive Biology and Endocrinology (2018) 16:53 https://doi.org/10.1186/s12958-018-0373-7 RESEARCH Open Access Progestin-primed milder stimulation with clomiphene citrate yields fewer oocytes
Ye et al. Reproductive Biology and Endocrinology (2018) 16:53 https://doi.org/10.1186/s12958-018-0373-7 RESEARCH Open Access Progestin-primed milder stimulation with clomiphene citrate yields fewer oocytes
Fertility assessment and assisted conception
 Fertility assessment and assisted conception Dr Geetha Venkat MD FRCOG Director Pulse Learning Women s health 14 September 2016 Disclosure statement Dr Venkat is a director of Harley Street Fertility Clinic.
Fertility assessment and assisted conception Dr Geetha Venkat MD FRCOG Director Pulse Learning Women s health 14 September 2016 Disclosure statement Dr Venkat is a director of Harley Street Fertility Clinic.
Ovarian hyperstimulation syndrome (OHSS)
") Ovarian hyperstimulation syndrome (OHSS) OHSS OHSS: exaggerated response to gonadotropins and hcg Characterized by: ovarian enlargement increased vascular permeability fluid accumulation in abdomen Associated
Ovarian hyperstimulation syndrome (OHSS) OHSS OHSS: exaggerated response to gonadotropins and hcg Characterized by: ovarian enlargement increased vascular permeability fluid accumulation in abdomen Associated
FRESH OR FROZEN EMBYOS WHAT IS THE LATEST EVIDENCE? DR. ASMA MOMANI CLEVELAND CLINIC, ANDROLOGY LAB TRAINEE 2018
 FRESH OR FROZEN EMBYOS WHAT IS THE LATEST EVIDENCE? DR. ASMA MOMANI CLEVELAND CLINIC, ANDROLOGY LAB TRAINEE 2018 OBJECTIVES Hisory Indication of freezing embryos Slow freezing versus vitrification Advantages
FRESH OR FROZEN EMBYOS WHAT IS THE LATEST EVIDENCE? DR. ASMA MOMANI CLEVELAND CLINIC, ANDROLOGY LAB TRAINEE 2018 OBJECTIVES Hisory Indication of freezing embryos Slow freezing versus vitrification Advantages
No influence of the indication of freeze-all strategy on subsequent outcome to frozen-thawed embryo transfer cycle
 Original paper No influence of the indication of freeze-all strategy on subsequent outcome to frozen-thawed embryo transfer cycle T. Masschaele 1,2, F. VandekerckhoVe 2, P. de sutter 2, J. Gerris 2 1 AZ
Original paper No influence of the indication of freeze-all strategy on subsequent outcome to frozen-thawed embryo transfer cycle T. Masschaele 1,2, F. VandekerckhoVe 2, P. de sutter 2, J. Gerris 2 1 AZ
Does PCOS Compromise the oocyte and embryo quality or the endometrium?
 Does PCOS Compromise the oocyte and embryo quality or the endometrium? Richard S. Legro, M.D., Penn State College of Medicine, Dept of Ob/Gyn, Hershey, PA, USA Disclosures Consultant: Bayer, Ogeda (Euroscreen),
Does PCOS Compromise the oocyte and embryo quality or the endometrium? Richard S. Legro, M.D., Penn State College of Medicine, Dept of Ob/Gyn, Hershey, PA, USA Disclosures Consultant: Bayer, Ogeda (Euroscreen),
N. Shirazian, MD. Endocrinologist
 N. Shirazian, MD Internist, Endocrinologist Inside the ovary Day 15-28: empty pyfollicle turns into corpus luteum (yellow body) Immature eggs Day 1-13: 13: egg developing inside the growing follicle Day
N. Shirazian, MD Internist, Endocrinologist Inside the ovary Day 15-28: empty pyfollicle turns into corpus luteum (yellow body) Immature eggs Day 1-13: 13: egg developing inside the growing follicle Day
ERA. Endometrial Receptivity Analysis. Patented since
 Endometrial Receptivity Analysis Patented since 2009 www.igenomix.com ERA ERA analyzes by NGS the expression of 236 genes in order to determine the personalized window of implantation for each patient.
Endometrial Receptivity Analysis Patented since 2009 www.igenomix.com ERA ERA analyzes by NGS the expression of 236 genes in order to determine the personalized window of implantation for each patient.
In Vitro Fertilization in Clomiphene-Resistant Women with Polycystic Ovary Syndrome
 Original Article Effect of Laparoscopic Ovarian Drilling on Outcomes of In Vitro Fertilization in Clomiphene-Resistant Women with Polycystic Ovary Syndrome Maryam Eftekhar, M.D. 1, Razieh Deghani Firoozabadi,
Original Article Effect of Laparoscopic Ovarian Drilling on Outcomes of In Vitro Fertilization in Clomiphene-Resistant Women with Polycystic Ovary Syndrome Maryam Eftekhar, M.D. 1, Razieh Deghani Firoozabadi,
ERA Endometrial Receptivity Analysis Operations Manual
 ERA Endometrial Receptivity Analysis Operations Manual L_I_001_ERA_GHQ_EN_v1.0 Date of issue: 21 August 2017 Author: Alejandro Rincón Bertolín Authorized by: María Ruiz Alonso // Igenomix Quality Department
ERA Endometrial Receptivity Analysis Operations Manual L_I_001_ERA_GHQ_EN_v1.0 Date of issue: 21 August 2017 Author: Alejandro Rincón Bertolín Authorized by: María Ruiz Alonso // Igenomix Quality Department
Oocyte Freezing and Ovarian Tissue Cryopreservation:
 Oocyte Freezing and Ovarian Tissue Cryopreservation: Comparing Results of These Two Methods in One Program Dr. César Díaz García cesar.diaz@ivi.uk IVI London 83, Wimpole St. London, UK London Conflict
Oocyte Freezing and Ovarian Tissue Cryopreservation: Comparing Results of These Two Methods in One Program Dr. César Díaz García cesar.diaz@ivi.uk IVI London 83, Wimpole St. London, UK London Conflict
The effect of adding oral oestradiol to progesterone as luteal phase support in ART cycles a randomized controlled study
 Clinical research The effect of adding oral oestradiol to progesterone as luteal phase support in ART cycles a randomized controlled study Ashraf Moini 1,2, Shahrzad Zadeh Modarress 3, Elham Amirchaghmaghi
Clinical research The effect of adding oral oestradiol to progesterone as luteal phase support in ART cycles a randomized controlled study Ashraf Moini 1,2, Shahrzad Zadeh Modarress 3, Elham Amirchaghmaghi
Nuoveprospettive per la faseluteale.
 Nuoveprospettive per la faseluteale. Dr. Ilario Candeloro Centro di Procreazione Medicalmente Assistita ASST Papa Giovanni XXIII Bergamo The role of LH and progesterone in the luteal phase Totally responsible
Nuoveprospettive per la faseluteale. Dr. Ilario Candeloro Centro di Procreazione Medicalmente Assistita ASST Papa Giovanni XXIII Bergamo The role of LH and progesterone in the luteal phase Totally responsible
NICE fertility guidelines. Hemlata Thackare MPhil MSc MRCOG Deputy Medical Director London Women s Clinic
 NICE fertility guidelines Hemlata Thackare MPhil MSc MRCOG Deputy Medical Director London Women s Clinic About the LWC 4 centres around the UK London Cardiff Swansea Darlington The largest sperm bank in
NICE fertility guidelines Hemlata Thackare MPhil MSc MRCOG Deputy Medical Director London Women s Clinic About the LWC 4 centres around the UK London Cardiff Swansea Darlington The largest sperm bank in
Ovarian hyperstimulation syndrome- an optimal solution for an unresolved enigma
 Orvieto Journal of Ovarian Research 2013, 6:77 REVIEW Open Access Ovarian hyperstimulation syndrome- an optimal solution for an unresolved enigma Raoul Orvieto 1,2 Abstract Ovarian hyperstimulation syndrome
Orvieto Journal of Ovarian Research 2013, 6:77 REVIEW Open Access Ovarian hyperstimulation syndrome- an optimal solution for an unresolved enigma Raoul Orvieto 1,2 Abstract Ovarian hyperstimulation syndrome
New York Science Journal 2014;7(4)
") The Minimal Stimulation Protocol for ICSI: An Alternative Protocol for Ovarian Stimulation Adel Elsayed Ibrahim, MD Assisted Reproductive Unit Azhar University Adel.sayed29@gmail.com Abstract: Background:
The Minimal Stimulation Protocol for ICSI: An Alternative Protocol for Ovarian Stimulation Adel Elsayed Ibrahim, MD Assisted Reproductive Unit Azhar University Adel.sayed29@gmail.com Abstract: Background:
estrogen supplementation for luteal phase support.
 Rationale and regimens of progesterone and estrogen supplementation for luteal phase support. Cicinelli E. IV Dept. Ob/Gyn, University of Bari, Italy cicinelli@gynecology1.uniba.it Luteal phase defect
Rationale and regimens of progesterone and estrogen supplementation for luteal phase support. Cicinelli E. IV Dept. Ob/Gyn, University of Bari, Italy cicinelli@gynecology1.uniba.it Luteal phase defect
A rationale for timing of luteal support post GnRH agonist trigger. Address: IVF Unit, Elisha Hospital, 12 Yair Katz Street, Haifa, Israel,
 Short Review: A rationale for timing of luteal support post GnRH agonist trigger Shahar Kol, IVF Unit, Elisha Hospital, Haifa, Israel. Address: IVF Unit, Elisha Hospital, 12 Yair Katz Street, Haifa, Israel,
Short Review: A rationale for timing of luteal support post GnRH agonist trigger Shahar Kol, IVF Unit, Elisha Hospital, Haifa, Israel. Address: IVF Unit, Elisha Hospital, 12 Yair Katz Street, Haifa, Israel,
the transfer of a good-quality euploid embryo does not ensure a successful implantation or pregnancy standard protocol to optimize results
 Disclosures Chief of Department, Gyn outpatient, Infertility, Andrology at Department of Ob & Gyn, Turku University Hospital Ass. Professor in Reproductive Medicine, Univ of Turku Chairman, Finnish Fertility
Disclosures Chief of Department, Gyn outpatient, Infertility, Andrology at Department of Ob & Gyn, Turku University Hospital Ass. Professor in Reproductive Medicine, Univ of Turku Chairman, Finnish Fertility
Infertility Clinical Guideline
 Infertility Clinical Guideline Ovarian Stimulation Guideline Purpose: To provide sufficient background regarding various ovarian stimulation protocols for In Vitro Fertilization cycles. Goal: To assist
Infertility Clinical Guideline Ovarian Stimulation Guideline Purpose: To provide sufficient background regarding various ovarian stimulation protocols for In Vitro Fertilization cycles. Goal: To assist
Effect of ovarian stimulation on oocyte quality and embryonic aneuploidy: a prospective, randomised controlled trial
 FULL PROJECT TITLE: Effect of ovarian stimulation on oocyte quality and embryonic aneuploidy: a prospective, randomised controlled trial (STimulation Resulting in Embryonic Aneuploidy using Menopur (STREAM)
FULL PROJECT TITLE: Effect of ovarian stimulation on oocyte quality and embryonic aneuploidy: a prospective, randomised controlled trial (STimulation Resulting in Embryonic Aneuploidy using Menopur (STREAM)
Dr. Madhuri Patil. M.D., DGO, FCPS, DFP, FICOG. (Mum) Dr. Patil s Fertility & Endoscopy Clinic Bangalore
 Dr. Patil s Fertility & Endoscopy Clinic Bangalore") OHSS Have we found a solution? Dr. Madhuri Patil M.D., DGO, FCPS, DFP, FICOG. (Mum) Dr. Patil s Fertility & Endoscopy Clinic Bangalore Ovarian hyperstimulation syndrome Serious and detrimental complication
OHSS Have we found a solution? Dr. Madhuri Patil M.D., DGO, FCPS, DFP, FICOG. (Mum) Dr. Patil s Fertility & Endoscopy Clinic Bangalore Ovarian hyperstimulation syndrome Serious and detrimental complication
Dr Guy Gudex. Director Repromed. 17:00-17:30 Recent Advances in Fertility Management
 Dr Guy Gudex Director Repromed 17:00-17:30 Recent Advances in Fertility Management Recent Advances in Fertility Management Practice Nurses Programme NZMA GP CME June 2018 Dr Guy Gudex ART in NZ -2014 ACART
Dr Guy Gudex Director Repromed 17:00-17:30 Recent Advances in Fertility Management Recent Advances in Fertility Management Practice Nurses Programme NZMA GP CME June 2018 Dr Guy Gudex ART in NZ -2014 ACART
Fixed Schedule for in vitro Fertilization and Embryo Transfer: Comparison of Outcome between the Short and the Long Protocol
 Yamanashi Med. J. 14(3), 77 ~ 82, 1999 Original Article Fixed Schedule for in vitro Fertilization and Embryo Transfer: Comparison of Outcome between the Short and the Long Protocol Tsuyoshi KASAI and Kazuhiko
Yamanashi Med. J. 14(3), 77 ~ 82, 1999 Original Article Fixed Schedule for in vitro Fertilization and Embryo Transfer: Comparison of Outcome between the Short and the Long Protocol Tsuyoshi KASAI and Kazuhiko
Embryo Selection after IVF
 Embryo Selection after IVF Embryo Selection after IVF Many of human embryos produced after in vitro fertilization carry abnormal chromosomes. Placing a chromosomally normal embryo (s) into a normal uterus
Embryo Selection after IVF Embryo Selection after IVF Many of human embryos produced after in vitro fertilization carry abnormal chromosomes. Placing a chromosomally normal embryo (s) into a normal uterus
High Peak Estradiol Predicts Higher Miscarriage and Lower Live Birth Rates in High Responders Triggered with a GnRH Agonist in IVF/ICSI Cycles
 The Journal of Reproductive Medicine High Peak Estradiol Predicts Higher Miscarriage and Lower Live Birth Rates in High Responders Triggered with a GnRH Agonist in IVF/ICSI Cycles Ryan G. Steward, M.D.,
The Journal of Reproductive Medicine High Peak Estradiol Predicts Higher Miscarriage and Lower Live Birth Rates in High Responders Triggered with a GnRH Agonist in IVF/ICSI Cycles Ryan G. Steward, M.D.,
ORIGINAL ARTICLE ENDOMETRIAL THICKNESS AND PREGNANCY OUTCOME IN IUI CYCLES
 ENDOMETRIAL THICKNESS AND PREGNANCY OUTCOME IN IUI CYCLES Asha Verma 1, Rekha Mulchandani 2, Nupur Lauria 3, Kusum Verma 4, Sunita Himani 5 HOW TO CITE THIS ARTICLE: Asha Verma, Rekha Mulchandani, Nupur
ENDOMETRIAL THICKNESS AND PREGNANCY OUTCOME IN IUI CYCLES Asha Verma 1, Rekha Mulchandani 2, Nupur Lauria 3, Kusum Verma 4, Sunita Himani 5 HOW TO CITE THIS ARTICLE: Asha Verma, Rekha Mulchandani, Nupur
(BMI)=18.0~24.9 kg/m 2 ;
=18.0~24.9 kg/m 2 ;") 33 10 Vol.33 No.10 2013 10 Oct. 2013 Reproduction & Contraception doi: 10.7669/j.issn.0253-357X.2013.10.0672 E-mail: randc_journal@163.com - ( 400013) : () GnRH-a - () : IVF- ET 233 A (I~II 102 ) B (III~IV
33 10 Vol.33 No.10 2013 10 Oct. 2013 Reproduction & Contraception doi: 10.7669/j.issn.0253-357X.2013.10.0672 E-mail: randc_journal@163.com - ( 400013) : () GnRH-a - () : IVF- ET 233 A (I~II 102 ) B (III~IV
Chen et al. Reproductive Biology and Endocrinology (2018) 16:36 https://doi.org/ /s z
 16:36 https://doi.org/ /s z") Chen et al. Reproductive Biology and Endocrinology (2018) 16:36 https://doi.org/10.1186/s12958-018-0352-z RESEARCH Open Access Pregnancy outcomes of PCOS overweight/ obese patients after controlled ovarian
Chen et al. Reproductive Biology and Endocrinology (2018) 16:36 https://doi.org/10.1186/s12958-018-0352-z RESEARCH Open Access Pregnancy outcomes of PCOS overweight/ obese patients after controlled ovarian
Article Minimal ovarian stimulation with clomiphene citrate: a large-scale retrospective study
 RBMOnline - Vol 15. No 2. 2007 134-148 Reproductive BioMedicine Online; www.rbmonline.com/article/2711 on web 13 June 2007 Article Minimal ovarian stimulation with clomiphene citrate: a large-scale retrospective
RBMOnline - Vol 15. No 2. 2007 134-148 Reproductive BioMedicine Online; www.rbmonline.com/article/2711 on web 13 June 2007 Article Minimal ovarian stimulation with clomiphene citrate: a large-scale retrospective
Influence ovarian stimulation on oocyte and embryo quality. Prof.Dr. Bart CJM Fauser
 Influence ovarian stimulation on oocyte and embryo quality Prof.Dr. Bart CJM Fauser How to balance too much vs too little? Lecture Outline Context ovarian stimulation Impact ovarian stimulation on oocyte
Influence ovarian stimulation on oocyte and embryo quality Prof.Dr. Bart CJM Fauser How to balance too much vs too little? Lecture Outline Context ovarian stimulation Impact ovarian stimulation on oocyte
2013 Sep.; 24(3):
:") Journal of Reproduction & Contraception doi: 10.7669/j.issn.1001-7844.2013.03.0159 2013 Sep.; 24(3):159-172 E-mail: randc_journal@163.com Comparison of the Effects and Safety of Mild Ovarian Stimulation
Journal of Reproduction & Contraception doi: 10.7669/j.issn.1001-7844.2013.03.0159 2013 Sep.; 24(3):159-172 E-mail: randc_journal@163.com Comparison of the Effects and Safety of Mild Ovarian Stimulation
IVF (,, ) : (HP-hMG) - (IVF- ET) : GnRH, HP-hMG (HP-hMG )57, (rfsh )140, (Gn)
 : (HP-hMG) - (IVF- ET) : GnRH, HP-hMG (HP-hMG )57, (rfsh )140, (Gn)") 34 11 Vol.34 No.11 2014 11 Nov. 2014 Reproduction & Contraception doi: 10.7669/j.issn.0253-3X.2014.11.0892 E-mail: randc_journal@163.com IVF ( 710003) : (H-hMG) - (IVF- ET) : GnRH H-hMG (H-hMG ) (rfsh
34 11 Vol.34 No.11 2014 11 Nov. 2014 Reproduction & Contraception doi: 10.7669/j.issn.0253-3X.2014.11.0892 E-mail: randc_journal@163.com IVF ( 710003) : (H-hMG) - (IVF- ET) : GnRH H-hMG (H-hMG ) (rfsh
Modified natural cycle IVF and mild IVF: a 10 year Swedish experience
 Reproductive BioMedicine Online (2010) 20, 156 162 www.sciencedirect.com www.rbmonline.com ARTICLE Modified natural cycle IVF and mild IVF: a 10 year Swedish experience Arthur Aanesen *, Karl-Gösta Nygren,
Reproductive BioMedicine Online (2010) 20, 156 162 www.sciencedirect.com www.rbmonline.com ARTICLE Modified natural cycle IVF and mild IVF: a 10 year Swedish experience Arthur Aanesen *, Karl-Gösta Nygren,
AOGS COMMENTARY SHAHAR KOL 1, ROY HOMBURG 2,3, BIRGIT ALSBJERG 4 & PETER HUMAIDAN 5. Abstract
 A C TA Obstetricia et Gynecologica AOGS COMMENTARY The gonadotropin-releasing hormone antagonist protocol the protocol of choice for the polycystic ovary syndrome patient undergoing controlled ovarian
A C TA Obstetricia et Gynecologica AOGS COMMENTARY The gonadotropin-releasing hormone antagonist protocol the protocol of choice for the polycystic ovary syndrome patient undergoing controlled ovarian
Minimal ovarian stimulation combined with elective single embryo transfer policy: age-specific results of a large, single-centre, Japanese cohort
 Kato et al. Reproductive Biology and Endocrinology 2012, 10:35 RESEARCH Open Access Minimal ovarian stimulation combined with elective single embryo transfer policy: age-specific results of a large, single-centre,
Kato et al. Reproductive Biology and Endocrinology 2012, 10:35 RESEARCH Open Access Minimal ovarian stimulation combined with elective single embryo transfer policy: age-specific results of a large, single-centre,
Infertility treatment
 In the name of God Infertility treatment Treatment options The optimal treatment is one that provide an acceptable success rate, has minimal risk and is costeffective. The treatment options are: 1- Ovulation
In the name of God Infertility treatment Treatment options The optimal treatment is one that provide an acceptable success rate, has minimal risk and is costeffective. The treatment options are: 1- Ovulation
Endometrial advancement after triggering with recombinant or urinary HCG: a randomized controlled pilot study
 Reproductive BioMedicine Online (2010) 21, 50 55 www.sciencedirect.com www.rbmonline.com ARTICLE Endometrial advancement after triggering with recombinant or urinary HCG: a randomized controlled pilot
Reproductive BioMedicine Online (2010) 21, 50 55 www.sciencedirect.com www.rbmonline.com ARTICLE Endometrial advancement after triggering with recombinant or urinary HCG: a randomized controlled pilot
Embryo transfer and Luteal phase support
 Embryo transfer and Luteal phase support PATCHARADA AMATYAKUL, M.D. DEPARTMENT OF OBSTETRICS AND GYNECOLOGY FACULTY OF MEDICINE NARESUAN UNIVERSITY Embryo Transfer http://www.regionalfertilityprogram.ca/program-embryotransfer.php
Embryo transfer and Luteal phase support PATCHARADA AMATYAKUL, M.D. DEPARTMENT OF OBSTETRICS AND GYNECOLOGY FACULTY OF MEDICINE NARESUAN UNIVERSITY Embryo Transfer http://www.regionalfertilityprogram.ca/program-embryotransfer.php
International Journal of Women s Health and Reproduction Sciences Vol. 6, No. 2, April 2018, ISSN
 http://www.ijwhr.net Open Access doi 10.15296/ijwhr.2018.31 Original Article International Journal of Women s Health and Reproduction Sciences Vol. 6, No. 2, April 2018, 187 191 ISSN 2330-4456 Comparison
http://www.ijwhr.net Open Access doi 10.15296/ijwhr.2018.31 Original Article International Journal of Women s Health and Reproduction Sciences Vol. 6, No. 2, April 2018, 187 191 ISSN 2330-4456 Comparison
Pituitary down-regulation in IVF/ICSI: consequences for treatment regimens Mochtar, M.H.
 UvA-DARE (Digital Academic Repository) Pituitary down-regulation in IVF/ICSI: consequences for treatment regimens Mochtar, M.H. Link to publication Citation for published version (APA): Mochtar, M. H.
UvA-DARE (Digital Academic Repository) Pituitary down-regulation in IVF/ICSI: consequences for treatment regimens Mochtar, M.H. Link to publication Citation for published version (APA): Mochtar, M. H.
A prospective randomised study comparing a GnRH-antagonist versus a GnRH-agonist short protocol for ovarian stimulation in patients referred for IVF
 FVV IN OBGYN, 2012, 4 (2): 82-87 Original paper A prospective randomised study comparing a GnRH-antagonist versus a GnRH-agonist short protocol for ovarian stimulation in patients referred for IVF S. GORDTS,
FVV IN OBGYN, 2012, 4 (2): 82-87 Original paper A prospective randomised study comparing a GnRH-antagonist versus a GnRH-agonist short protocol for ovarian stimulation in patients referred for IVF S. GORDTS,
Frozen-thawed embryo transfer is associated with a significantly reduced incidence of ectopic pregnancy
 ORIGINAL ARTICLES: EARLY PREGNANCY Frozen-thawed embryo transfer is associated with a significantly reduced incidence of ectopic pregnancy Bruce S. Shapiro, M.D., Ph.D., a,b Said T. Daneshmand, M.D., a,b
ORIGINAL ARTICLES: EARLY PREGNANCY Frozen-thawed embryo transfer is associated with a significantly reduced incidence of ectopic pregnancy Bruce S. Shapiro, M.D., Ph.D., a,b Said T. Daneshmand, M.D., a,b
I. ART PROCEDURES. A. In Vitro Fertilization (IVF)
") DFW Fertility Associates ASSISTED REPRODUCTIVE TECHNOLOGY (ART) Welcome to DFW Fertility Associates/ Presbyterian-Harris Methodist Hospital ARTS program. This document provides an overview of treatment
DFW Fertility Associates ASSISTED REPRODUCTIVE TECHNOLOGY (ART) Welcome to DFW Fertility Associates/ Presbyterian-Harris Methodist Hospital ARTS program. This document provides an overview of treatment
Medicine. Wei Yang, MMed, Tao Zhang, MMed, Zhou Li, PhD, Xinling Ren, PhD, Bo Huang, PhD, Guijin Zhu, MMed, Lei Jin, PhD. Observational Study
 Observational Study Medicine Combined analysis of endometrial thickness and pattern in predicting clinical outcomes of frozen embryo transfer cycles with morphological good-quality blastocyst A retrospective
Observational Study Medicine Combined analysis of endometrial thickness and pattern in predicting clinical outcomes of frozen embryo transfer cycles with morphological good-quality blastocyst A retrospective
Bumiputera Sarawak Bumiputera Sabah. Others Foreigner. Had previous natural pregnancy Previous IVF pregnancies. IVF live births.
 a. Date of notification: b. Name of reporting site: c.name of doctor in charge: AI : FEMALE PATIENT DETAILS & DEMOGRAPHICS (Instruction: if Mykad is not available, please complete Old IC or other ID document
a. Date of notification: b. Name of reporting site: c.name of doctor in charge: AI : FEMALE PATIENT DETAILS & DEMOGRAPHICS (Instruction: if Mykad is not available, please complete Old IC or other ID document
L6: DuoStim: the alternative of oocytes/embryos accumulation programs Carlo Alviggi
 L6: DuoStim: the alternative of oocytes/embryos accumulation programs Carlo Alviggi Italy What is the aim of IVF? What is the measure of success in IVF? Cumulative live birth rate per started cycle Live
L6: DuoStim: the alternative of oocytes/embryos accumulation programs Carlo Alviggi Italy What is the aim of IVF? What is the measure of success in IVF? Cumulative live birth rate per started cycle Live
How do we choose the best progesterone to support the luteal phase
 How do we choose the best progesterone to support the luteal phase Prof. Dr. Herman Tournaye MSD Fertility Regional Stand Alone Scientific Symposium Lisbon In the last 3 years the speaker or the speaker
How do we choose the best progesterone to support the luteal phase Prof. Dr. Herman Tournaye MSD Fertility Regional Stand Alone Scientific Symposium Lisbon In the last 3 years the speaker or the speaker
FRESH VERSUS FROZEN EMBRYO TRANSFER OVERVIEW
 FRESH VERSUS FROZEN EMBRYO TRANSFER OVERVIEW Lynn Westphal, MD Professor Department of Obstetrics & Gynecology, Stanford University School of Medicine, Stanford, CA DISCLOSURES Celmatix: sponsored research
FRESH VERSUS FROZEN EMBRYO TRANSFER OVERVIEW Lynn Westphal, MD Professor Department of Obstetrics & Gynecology, Stanford University School of Medicine, Stanford, CA DISCLOSURES Celmatix: sponsored research