Dysfunctional Uterine Bleeding (DUB) OB/GYN Hospital of Fudan University Weiwei Feng, MD,Ph D Tel:
|
|
|
- Dwight Welch
- 6 years ago
- Views:
Transcription


1 Dysfunctional Uterine Bleeding (DUB) OB/GYN Hospital of Fudan University Weiwei Feng, MD,Ph D wfeng7347@aliyun.com Tel:
2 Contents DUB: definition, mechanism of normal menses, causes and classification Anovulatory DUB: Etiology, pathophysiology, pathological change, diagnosis, differential diagnosis, diagnostic methods, treatment (principle) Ovulatory menstrual dysfunction: classification, diagnosis, differential diagnosis, diagnostic methods, treatment
3 Definition Abnormal uterine bleeding with no organic causes what s normal menstruation? what s meaning of the no organic causes? A diagnosis of exclusion

4 Normal Menses Cycle: a range of 21 to 35 days, Duration: 2~8 days Average blood loss: 20~60ml.

5 Endocrine and endometrial change in menstrual cycle


6 Normal menses The shedding of the decidua functionalis
7 Terminology of abnormal menses Term Interval Duration Amount Menorrhagia Regular Prolonged Excessive Metrorrhagia Irregular prolonged Normal Menometrorrhagia Irregular Prolonged Excessive Polymenorrhea Frequent, Normal Normal regular Hypomenorrhea Regular Normal Less Intermenstrual bleeding Oligomenorrhea Occurs between bleeding otherwise normal menstrual cycles Infrequent, Variable Scanty irregular
8 DUB Causes Malnutrition Emotional change Endocrine disease,etc. Dysfunction of Hypothalamic-pituitary-ovarian axis (HPO axis) DUB
9 Classification 70~80% Anovulatory DUB most in puberty and menopausal transition period 20~30% Ovulatory menstrual dysfuction most in reproductive age
10 Contents DUB: definition, mechanism of normal menses, causes and classification Anovulatory DUB: Etiology, pathophysiology, pathological change, diagnosis, differential diagnosis, diagnostic methods, treatment (principle) Ovulatory menstrual dysfunction: classification, diagnosis, differential diagnosis, diagnostic methods, treatment
11 Case A 17-year-old girl, Amenorrhea for 4 months, First 5 days drop bleeding, with subsequent heavy bleeding for 7 days, Short of breath, pale, Bp: 80/50mmHg, Hb: 50g/L Diagnosis? Any other examinations needed? Treatment?
12 Etiology of Anovulatory DUB 1. Puberty Immaturity of HPO axis Low FSH and LH Anovulation Persistent E2 No Progesterone
13 Etiology of Anovulatory DUB 2. Menopausal Transition Period Ovarian failure, follicle reduced Insensitive to FSH and LH, low estrogen Anovulation Persistent E2 No Progesterone
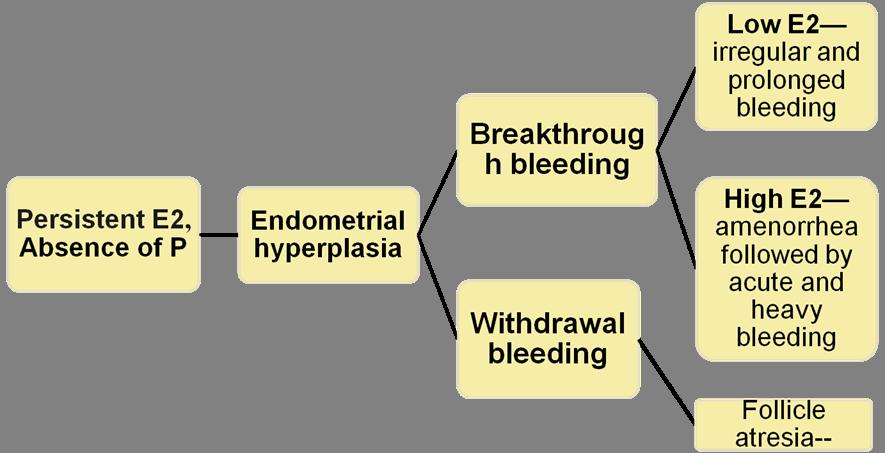
14 Pathophysiology
15 Dysfunction of self-limiting mechanism of menstruation Fragile endometrium (lack of stromal support) Irregular shedding Abnormal vascular structure and function Dysfunction of coagulation and fibrinolysis Disorder of vascular factors (PGE2 )
16 Pathological change 1. Proliferative phase endometrium 2. Endometrial hyperplasia ( simple, complex, atypical) 3. Atrophic endometrium Based on architectual and cytologic features

17 Simple hyperplasia Architectual : Dilated or cystic glands, Slightly irregular shapes, No glandular crowding Increased glandular-to-stromal ratio Progression to cancer: 1% Cytologic: No cytologic atypia 17

18 Complex hyperplasia Architectural: Complex (budding and infolding) Crowded glands with less intervening stroma Progression to cancer: 3% Cytologic: Without atypia 18

19 Atypical hyperplasia Architectural: Simple or complex Cytologic: Atypia Progression to cancer: 23% Large nuclei of variable size and shape that have lost polarity 2. Prominent nucleoli 3. Irregularly clumped chromatin 4. Increased nuclear-tocytoplasmic ratios Not DUB, organic disease



20 Theories of development of Type I endometrial cancer Chronic Oestrogen Overstimulation Genetic hit with clonal expansion Normal endometrum Simple hyperplasia Complex hyperplasia Proliferative Endometrium Estrogen Genetic hit Atypical hyplasia Endometrial cancer Kurman 1984 Endometrial Intraepithelial Neoplasia Endometrial Cancer Benign Reactive Hyperplasia Mutter 2000
21 Diagnosis Medical history Physical examination Laboratory tests Imaging tests A diagnosis of exclusion
22 Differential diagnosis All diseases resulting in irregular vaginal bleeding should be excluded Pregnancy related disease Reproductive tumor Infection Trauma Hormone therapy & IUD Systemic disease (ITP etc.)
23 Cause of bleeding by approximate frequency and age group Adolescent reproductive perimenopausal Anovulation Exogenous hormone use Exogenous hormone use Pregnancy Anovulation Fiboroids Pregnancy Anovulation Cervical or endometrial polyps or cancer Coagulopathy Leiomyoma Thyroid dysfunction Cervical or endometrial polyps or cancer Thyroid dysfunction
24 Diagnostic methods Medical history Symptoms Contraception methods Medicine history (hormone therapy) Systemic disease (liver disease, hematological disease, thyroid disease)
25 Diagnostic methods Physical examination Systemic examination A complete pelvic examination--- to rule out organic causes ( eg. Cervix cytology : to rule out cervical cancer)
26 Diagnostic methods Initial Lab tests and Imaging tests 1. HCG to rule out pregnancy 2. A complete blood count How severe her with platelets anemia is? 3. Blood coagulation tests (PT, APTT, Fbs) 4. Ultrasonography Coagulopathy?


27 Further inspections 4. Hormone test (FSH, LH, E2, PRL, T, PRL, TSH, FT3, FT4) 5. Cervical mucus Is this case an anovulatory DUB or ovulatory DUB?

28 6. BBT (basal body temperature) Is this case an anovulatory DUB or ovulatory DUB? Normal BBT
29 7. MRI if nessecessory 8. Endometrial sampling Dilation and curettage, D & C Endometrial biopsy 9. Hysteroscopy
30 Treatment Nonsurgical management Surgical treatment
31 Non surgical management Medicine for hemostat: Hormone therapy, NSAIDs, Antifibrinolytics Treatment of anemia Vitamin C iron supplements blood transfusion Prevent infection Antibiotics Nutrition

32 Medication : First line therapy Principle very important
33 Step 1: Hemostasis Mild bleeding : use lowest dose of hormone Acute heavy bleeding: use high dose hormone take effect in 6~8h, stop bleeding in 24~48h if >96h bleeding continues, reevaluated the patients, organic diseases?
34 1. high dose estrogen: to stop heavy bleeding in anovulatory DUB in adolescents and reproductive age patients Conjugated estrogen 2.5mg q6h Heavy bleeding 2.5mg q8hx3d 2.5mg q12hx3d 1.25mg q8hx3d 1.25mg q12hx3d Hb>90g/L, add Progestin X10d 1.25mg qd Withdrawal bleeding Day begin therapy Contraindications: thrombus, coagulation diseases
35 2. (1) Progesterone in second half of the cycle medication curettage For patients with moderate level of estrogen, Hb>80g/l, vital signs stable Convert proliferative endometrium to secretion phase Progesterone used in Second half of the cycle mild bleeding progesterone bleeding Withdrawal bleeding Day begin therapy Menstrual cycle
36 (2) Progesterone in whole cycle For heavy bleeding with moderate E2 norethindrone. 5mg q6h until bleeding stops Heavy bleeding 5mg q8hx3d 5mg q12hx3d 3.75mg q12hx3d 5mg qdx11d Withdrawal bleeding Day begin therapy Stop bleeding 1 20
37 3. Combined estrogen and progesterone (Oral Contraceptive ) Mild bleeding Diane-35, Marvelon, Minulet 1# qd for 21d, 3-6 months Heavy bleeding Diane-35, et al 1~2 # q6h/q8h reduce dose 1/3 every 3d 1# qd for 21d
38 4)Androgen : anti-estrogen effect 5)Levonorgestrel-releasing IUD : reduce 80-90% of total bleeding 39
39 Medication: First line therapy Principle very important
40 Step 2: Regulating menstrual cycle For adolescents and reproductive patients: To restore the H-P-O function For peri-menopause patients: To control the volume and prevent endometrial hyperplasia
41 1. Sequential E-P therapy (artificial cycle) For adolescents and reproductive patients with low level estrogen estrogen Progestrone bleeding Withdrawal bleeding Day begin therapy Artificial cycle
42 2. Oral contraceptives (E+P combined therapy) for patients in reproductive period with high level estrogen and perimenopausal patients contraceptives bleeding Withdrawal bleeding Day begin therapy 1 21 menstrual cycle 5 26
43 3. Progesterone used in second half of the cycle for adolescents and peri-menopaual patients progesterone bleeding Withdrawal bleeding Day begin therapy Menstrual cycle
44 Medication: First line therapy Principle very important
45 Step 3: Prompting ovulation for reproductive age patients desire for birth Mostly, spontaneous ovulating begins as soon as the sequential and combined E-P therapy stops Not recommended for adolescents For those failed the therapy: Clomiphene citrate,hmg,hcg et,al
46 Step 3 Prevent cancer For patients who had long history of anovulation 1. Surgical treatment 1) D & C Objective: hemostasis & diagnosis >35 years old, but not limited to these women Ineffective to medicine Risk for endometrial cancer 2) Endometrial ablation (hysteroscopy) 3) Hysterectomy
47 2. Hormone therapy : 1) Oral contraceptive 2) Progesterone used in second half of cycle simple hyperpalsia 3) Progestrone used in whole cycle complex hyperplasia
48 Summary : hormone therapy for A-DUB 1. Hemostasis 1)E 2)P 3) E+P, E+P+T 4)T 5)IUD-P 6) other 2. Regulating menstrual cycle 1) Sequential E-P therapy 2) E+P combined therapy 3)Progesterone used in Second half of the cycle 3. promote ovulation or prevent cancer 1)CC 2) HMG 3) HCG or 1) surgery 2) P
49 Contents DUB: definition, mechanism of normal menses, causes and classification Anovulatory DUB: Etiology, pathophysiology, pathological change, diagnosis, differential diagnosis, diagnostic methods, treatment (principle) Ovulatory menstrual dysfunction: classification, diagnosis, differential diagnosis, diagnostic methods, treatment
50 Contents DUB: definition, mechanism of normal menses, causes and classification Anovulatory DUB: Etiology, pathophysiology, pathological change, diagnosis, differential diagnosis, diagnostic methods, treatment (principle) Ovulatory menstrual dysfunction: classification, diagnosis, differential diagnosis, diagnostic methods, treatment
51 Ovulatory mentrual dysfunction Classification Menorrhagia: Intermenstrual bleeding Peri-ovulation bleeding Luteal dysfunction Luteal phase defect, LPD Irregular shedding of endometrium
52 Menorrhagia Regular period, normal duration, excessive bleeding >80ml Normal endometrium, normal hormone level Mechanism: increased fibrionolysis, prostglandins inbalance Treatment: anti-fibrionolytics, OC, levonorgestrel-releasing IUD, P-whole cycle
53 Luteal dysfunction Causes: 1. Luteal Phase Defect, LPD Low FSH--Dysplasia of the follicles Insufficiency of the LH peak Defects in the lower LH impulse after LH peak Hyperprolactinemia LH receptor defect of granulose cell
54 Pathology Mechanism Not adequate progesterone production, Secretory endometrium : Inadequate Glands secretion No obvious Stroma edema Gland and stroma not comparable Short secretory phase Quick regression of the corpus luteum Symptoms Polymenorrhea Short high temperature phase in BBT <11d Infertility or loss of early pregnancy

55 Diagnosis of LPD 1.Clinical symptoms 2.BBT, high temperature phase <11d 3.Endometrial biopsy: secretion later than 2 days
56 LPD Treatment Stimulating follicular development CC 50mg/day for 5 days from 1st day Enhancing the LH peak HCG 5,000 or 10,000IU when the follicles are mature Stimulating luteal function HCG for 5 days during luteal phase Replacement therapy Progesterone 10mg for days in luteal phase Hyperprolactinemia Bromocriptine mg/d
57 Luteal dysfunction 2. Irregular shedding of endometrium Normal Ovulation Normal Luteal development Uncompleted regression of the corpus luteum
58 Pathology Secretory endometrium on the 5 th day Mechanism Persistent progesterone s effect Incomplete shedding of endometrium Symptoms Prolonged menstruation 9-10 days Regular cycle Heavy bleeding
59 Diagnosis of irregular shedding of endometrium 1. Prolonged menstruation 2. High temperature presents slow returning to the lower temperature phase 3. Biopsy at 5 th day: secretory endometrium

60 Normal BBT
61 Treatment of irregular shedding of endometrium 1. Stimulating luteal function HCG for 5 days during luteal phase 2. Replacement therapy Progesterone 10mg for days in luteal phase 3. OC
62 Return to case discussion A 17-year-old girl, amenorrhea 4 months First 5 days drop bleeding, with subsequent heavy bleeding for 7 days, Short of breath, pale, Bp: 80/50mmHg, Hb: 50g/L Diagnosis? Additional lab tests or check-up? Differential diagnosis? Treatment?
63 Thank you!
Conflicts 10/5/2016. Abnormal Uterine Bleeding. Objectives Review diagnosis and updated nomenclature. Management options for acute and chronic AUB.
 Abnormal Uterine Bleeding Barbara L. Keller, MD JD Naval Hospital Oak Harbor OB/GYN Physician Conflicts I have no conflicts or financial interests to disclose. Objectives Review diagnosis and updated nomenclature.
Abnormal Uterine Bleeding Barbara L. Keller, MD JD Naval Hospital Oak Harbor OB/GYN Physician Conflicts I have no conflicts or financial interests to disclose. Objectives Review diagnosis and updated nomenclature.
Cynthia Morris DO, FACOOG, FACOS Medical Director, Women s Wellness Center Fayette County Memorial Hospital
 Cynthia Morris DO, FACOOG, FACOS Medical Director, Women s Wellness Center Fayette County Memorial Hospital Touchdown to CME Eighth District Academy of Osteopathic Medicine & Surgery October 8. 2017 Goals
Cynthia Morris DO, FACOOG, FACOS Medical Director, Women s Wellness Center Fayette County Memorial Hospital Touchdown to CME Eighth District Academy of Osteopathic Medicine & Surgery October 8. 2017 Goals
Frequency of menses. Duration of menses 3 days to 7 days. Flow/amount of menses Average blood loss with menstruation is 60-80cc.
 Frequency of menses 24 days (0.5%) to 35 days (0.9%) Age 25, 40% are between 25 and 28 days Age 25-35, 60% are between 25 and 28 days Teens and women over 40 s cycles may be longer apart Duration of menses
Frequency of menses 24 days (0.5%) to 35 days (0.9%) Age 25, 40% are between 25 and 28 days Age 25-35, 60% are between 25 and 28 days Teens and women over 40 s cycles may be longer apart Duration of menses
5/5/2010 FINANCIAL DISCLOSURE. Abnormal Uterine Bleeding. Is This A Problem? About me % of visits to gynecologist
 Abnormal Uterine FINANCIAL DISCLOSURE I HAVE NO FINANCIAL INTEREST IN ANY OF THE PRODUCTS MENTIONED IN MY PRESENTATION Bryan K. Rone, M.D. University of Kentucky Obstetrics and Gynecology May 5, 2010 About
Abnormal Uterine FINANCIAL DISCLOSURE I HAVE NO FINANCIAL INTEREST IN ANY OF THE PRODUCTS MENTIONED IN MY PRESENTATION Bryan K. Rone, M.D. University of Kentucky Obstetrics and Gynecology May 5, 2010 About
Reproductive Health and Pituitary Disease
 Reproductive Health and Pituitary Disease Janet F. McLaren, MD Assistant Professor Division of Reproductive Endocrinology and Infertility Department of Obstetrics and Gynecology jmclaren@uabmc.edu Objectives
Reproductive Health and Pituitary Disease Janet F. McLaren, MD Assistant Professor Division of Reproductive Endocrinology and Infertility Department of Obstetrics and Gynecology jmclaren@uabmc.edu Objectives
Management of Abnormal Uterine Bleeding. Julie Strickland MD, MPH University of Missouri Kansas City Department of Obstetrics and Gynecology
 Management of Abnormal Uterine Bleeding Julie Strickland MD, MPH University of Missouri Kansas City Department of Obstetrics and Gynecology AUB Abnormal uterine bleeding (AUB): fairly broad term referring
Management of Abnormal Uterine Bleeding Julie Strickland MD, MPH University of Missouri Kansas City Department of Obstetrics and Gynecology AUB Abnormal uterine bleeding (AUB): fairly broad term referring
Dysfunctional Uterine Bleeding
 Long term effects of PCOS Dysfunctional Uterine Bleeding Dr. Arulmozhi Ramarajan Church of South India Hospital, Bangalore Abnormal uterine bleeding Affects health-related QOL Causes social embarrasment
Long term effects of PCOS Dysfunctional Uterine Bleeding Dr. Arulmozhi Ramarajan Church of South India Hospital, Bangalore Abnormal uterine bleeding Affects health-related QOL Causes social embarrasment
Elaina Sexton, MD, MSc Obstetrics and Gynecology St. Vincent s Hospital. Objectives
 Elaina Sexton, MD, MSc Obstetrics and Gynecology St. Vincent s Hospital Objectives Definition of normal menstrual cycle and abnormal uterine bleeding (AUB) Evaluation of AUB Medical options for AUB Surgical
Elaina Sexton, MD, MSc Obstetrics and Gynecology St. Vincent s Hospital Objectives Definition of normal menstrual cycle and abnormal uterine bleeding (AUB) Evaluation of AUB Medical options for AUB Surgical
Endometrial line thickness in different conditions.
 Endometrial line thickness in different conditions 1 Endometrial thickens in response to Rising estrogen levels during the menstrual cycle and then shedding endometrial at the times of menses 2 The thickens
Endometrial line thickness in different conditions 1 Endometrial thickens in response to Rising estrogen levels during the menstrual cycle and then shedding endometrial at the times of menses 2 The thickens
5 Mousa Al-Abbadi. Ola Al-juneidi & Obada Zalat. Ahmad Al-Tarefe
 5 Mousa Al-Abbadi Ola Al-juneidi & Obada Zalat Ahmad Al-Tarefe Abnormal Uterine Bleeding (AUB) AUB is a very common scenario or symptom where women complain of menorrhagia (heavy and/or for long periods),
5 Mousa Al-Abbadi Ola Al-juneidi & Obada Zalat Ahmad Al-Tarefe Abnormal Uterine Bleeding (AUB) AUB is a very common scenario or symptom where women complain of menorrhagia (heavy and/or for long periods),
Abnormal Uterine Bleeding. Richard Dover Specialist gynaecologist
 Abnormal Uterine Bleeding Richard Dover Specialist gynaecologist A pragmatic guide. Wide topic range What s not coming up Precocious puberty Menorrhagia well maybe just a little Topics Adolescents IMB
Abnormal Uterine Bleeding Richard Dover Specialist gynaecologist A pragmatic guide. Wide topic range What s not coming up Precocious puberty Menorrhagia well maybe just a little Topics Adolescents IMB
The reproductive lifespan
 The reproductive lifespan Reproductive potential Ovarian cycles Pregnancy Lactation Male Female Puberty Menopause Age Menstruation is an external indicator of ovarian events controlled by the hypothalamicpituitary
The reproductive lifespan Reproductive potential Ovarian cycles Pregnancy Lactation Male Female Puberty Menopause Age Menstruation is an external indicator of ovarian events controlled by the hypothalamicpituitary
CASE 41. What is the pathophysiologic cause of her amenorrhea? Which cells in the ovary secrete estrogen?
 CASE 41 A 19-year-old woman presents to her gynecologist with complaints of not having had a period for 6 months. She reports having normal periods since menarche at age 12. She denies sexual activity,
CASE 41 A 19-year-old woman presents to her gynecologist with complaints of not having had a period for 6 months. She reports having normal periods since menarche at age 12. She denies sexual activity,
International Journal of Health Sciences and Research ISSN:
 International Journal of Health Sciences and Research www.ijhsr.org ISSN: 2249-9571 Original Research Article Evaluation of Thyroid Profile in Patients with Abnormal Uterine Bleeding Rema. V. Nair 1*,
International Journal of Health Sciences and Research www.ijhsr.org ISSN: 2249-9571 Original Research Article Evaluation of Thyroid Profile in Patients with Abnormal Uterine Bleeding Rema. V. Nair 1*,
1. During the follicular phase of the ovarian cycle, the hypothalamus releases GnRH.
 1. During the follicular phase of the ovarian cycle, the hypothalamus releases GnRH. 2. This causes the anterior pituitary to secrete small quantities of FSH and LH. 3. At this time, the follicles in the
1. During the follicular phase of the ovarian cycle, the hypothalamus releases GnRH. 2. This causes the anterior pituitary to secrete small quantities of FSH and LH. 3. At this time, the follicles in the
Dr. Nancy Van Eyk Associate Professor, Dalhousie University Chief of Gynaecology, IWK Health Centre
 Dr. Nancy Van Eyk Associate Professor, Dalhousie University Chief of Gynaecology, IWK Health Centre AUB Outline Terminology Classification/Etiology Assessment Treatment Referral to Gynaecology U c pt 4
Dr. Nancy Van Eyk Associate Professor, Dalhousie University Chief of Gynaecology, IWK Health Centre AUB Outline Terminology Classification/Etiology Assessment Treatment Referral to Gynaecology U c pt 4
Healthcare Education Research
 Healthcare Education Research Heavy menstrual bleeding: investigation, diagnosis & management An update for health professionals Assessment of heavy menstrual bleeding in primary care Dr Amanda Newman
Healthcare Education Research Heavy menstrual bleeding: investigation, diagnosis & management An update for health professionals Assessment of heavy menstrual bleeding in primary care Dr Amanda Newman
Abnormal Uterine Bleeding: Evaluation of Premenopausal Women. Vanessa Jacoby, MD, MAS Assistant Professor Ob, Gyn, & Reproductive Sciences UCSF
 Abnormal Uterine Bleeding: Evaluation of Premenopausal Women Vanessa Jacoby, MD, MAS Assistant Professor Ob, Gyn, & Reproductive Sciences UCSF Objectives Define normal and abnormal uterine bleeding Review
Abnormal Uterine Bleeding: Evaluation of Premenopausal Women Vanessa Jacoby, MD, MAS Assistant Professor Ob, Gyn, & Reproductive Sciences UCSF Objectives Define normal and abnormal uterine bleeding Review
Page # 1. Endometrium. Cellular Components. Anatomical Regions. Management of SIL Thomas C. Wright, Jr. Most common diseases:
 Endometrium Pathology of the Endometrium Thomas C. Wright Columbia University, New York, NY Most common diseases: Abnormal uterine bleeding Inflammatory conditions Benign neoplasms Endometrial cancer Anatomical
Endometrium Pathology of the Endometrium Thomas C. Wright Columbia University, New York, NY Most common diseases: Abnormal uterine bleeding Inflammatory conditions Benign neoplasms Endometrial cancer Anatomical
Polycystic Ovarian Syndrome (PCOS) LOGO
 LOGO") Polycystic Ovarian Syndrome (PCOS) Ma qianhong Ob/Gyn Department LOGO Contents Epidemiology and Definition Pathophysiology, Endocrinological Features Diagnostic Criteria Treatment Prognosis Introduction
Polycystic Ovarian Syndrome (PCOS) Ma qianhong Ob/Gyn Department LOGO Contents Epidemiology and Definition Pathophysiology, Endocrinological Features Diagnostic Criteria Treatment Prognosis Introduction
Investigation: The Human Menstrual Cycle Research Question: How do hormones control the menstrual cycle?
 Investigation: The Human Menstrual Cycle Research Question: How do hormones control the menstrual cycle? Introduction: The menstrual cycle (changes within the uterus) is an approximately 28-day cycle that
Investigation: The Human Menstrual Cycle Research Question: How do hormones control the menstrual cycle? Introduction: The menstrual cycle (changes within the uterus) is an approximately 28-day cycle that
Abnormal Uterine Bleeding Case Studies
 Case Study 1 Abnormal Uterine Bleeding Case Studies Abigail, a 24 year old female, presents to your office complaining that her menstrual cycles have become a problem. They are now lasting 6 7 days instead
Case Study 1 Abnormal Uterine Bleeding Case Studies Abigail, a 24 year old female, presents to your office complaining that her menstrual cycles have become a problem. They are now lasting 6 7 days instead
Female genital tract II.
 Female genital tract II. Pathology of the uterine corpus Lilla Madaras 2 nd Department Of Pathology Semmelweis University Budapest 9 th April 2018 Anatomy 2 The normal endometrium Histology Regulation
Female genital tract II. Pathology of the uterine corpus Lilla Madaras 2 nd Department Of Pathology Semmelweis University Budapest 9 th April 2018 Anatomy 2 The normal endometrium Histology Regulation
Gynecologic Decision Making Based on Sonographic Findings
 Gynecologic Decision Making Based on Sonographic Findings Mindy Goldman, MD Department of Obstetrics & Gynecology & Vickie A. Feldstein, MD Department of Radiology University of California, San Francisco
Gynecologic Decision Making Based on Sonographic Findings Mindy Goldman, MD Department of Obstetrics & Gynecology & Vickie A. Feldstein, MD Department of Radiology University of California, San Francisco
The Human Menstrual Cycle
 The Human Menstrual Cycle Name: The female human s menstrual cycle is broken into two phases: the Follicular Phase and the Luteal Phase. These two phases are separated by an event called ovulation. (1)
The Human Menstrual Cycle Name: The female human s menstrual cycle is broken into two phases: the Follicular Phase and the Luteal Phase. These two phases are separated by an event called ovulation. (1)
POTION OR POISON? MEDICAL TREATMENT ALTERNATIVES TO THE PILL. Lester Ruppersberger, D.O., FACOOG,CNFPI NFP only Gynecologist
 POTION OR POISON? MEDICAL TREATMENT ALTERNATIVES TO THE PILL Lester Ruppersberger, D.O., FACOOG,CNFPI NFP only Gynecologist THE PILL Released to US market in 1960 10-15 x dose of hormones in HRT Over 10-14
POTION OR POISON? MEDICAL TREATMENT ALTERNATIVES TO THE PILL Lester Ruppersberger, D.O., FACOOG,CNFPI NFP only Gynecologist THE PILL Released to US market in 1960 10-15 x dose of hormones in HRT Over 10-14
TRHC.UEMEE Ph P y h si s o i logy l of fmen M str st u r at a i t on i
 . TRHCUEMEE Physiology of Menstruation Learning objectives: By the end of this lecture the students should be able to: Define menstruation. List the Characters of normal menstruation Enumerate Components
. TRHCUEMEE Physiology of Menstruation Learning objectives: By the end of this lecture the students should be able to: Define menstruation. List the Characters of normal menstruation Enumerate Components
Overview of Reproductive Endocrinology
 Overview of Reproductive Endocrinology I have no conflicts of interest to report. Maria Yialamas, MD Female Hypothalamic--Gonadal Axis 15 4 Hormone Secretion in the Normal Menstrual Cycle LH FSH E2, Progesterone,
Overview of Reproductive Endocrinology I have no conflicts of interest to report. Maria Yialamas, MD Female Hypothalamic--Gonadal Axis 15 4 Hormone Secretion in the Normal Menstrual Cycle LH FSH E2, Progesterone,
Polycystic ovarian disease and Endometriosis
 Polycystic ovarian disease and Endometriosis Objectives: At the end of this lecture, the student should be able to: Know the clinicopathologic features of endometriosis with special emphasis on: definition,
Polycystic ovarian disease and Endometriosis Objectives: At the end of this lecture, the student should be able to: Know the clinicopathologic features of endometriosis with special emphasis on: definition,
Chapter 100 Gynecologic Disorders
 Chapter 100 Gynecologic Disorders Episode Overview: 1. Describe the presentation and RF for Adnexal torsion 2. List the imaging findings of adnexal torsion (US vs CT) 3. What is the management of adnexal
Chapter 100 Gynecologic Disorders Episode Overview: 1. Describe the presentation and RF for Adnexal torsion 2. List the imaging findings of adnexal torsion (US vs CT) 3. What is the management of adnexal
Female Reproductive System. Lesson 10
 Female Reproductive System Lesson 10 Learning Goals 1. What are the five hormones involved in the female reproductive system? 2. Understand the four phases of the menstrual cycle. Human Reproductive System
Female Reproductive System Lesson 10 Learning Goals 1. What are the five hormones involved in the female reproductive system? 2. Understand the four phases of the menstrual cycle. Human Reproductive System
AMERICAN SOCIETY FOR REPRODUCTIVE MEDICINE
 AMERICAN SOCIETY FOR REPRODUCTIVE MEDICINE Formerly The American Fertility Society OVULATION DETECTION A Guide for Patients PATIENT INFORMATION SERIES Published by the American Society for Reproductive
AMERICAN SOCIETY FOR REPRODUCTIVE MEDICINE Formerly The American Fertility Society OVULATION DETECTION A Guide for Patients PATIENT INFORMATION SERIES Published by the American Society for Reproductive
Study of Endometrial Histopathological Findings in Women with Abnormal Uterine Bleedingand Correlation with Clinical Features
 Original article: Study of Endometrial Histopathological Findings in Women with Abnormal Uterine Bleedingand Correlation with Clinical Features Rajnish Kumar 1, Seema Acharya 2, Aparna Bhardwaj 3 1Associate
Original article: Study of Endometrial Histopathological Findings in Women with Abnormal Uterine Bleedingand Correlation with Clinical Features Rajnish Kumar 1, Seema Acharya 2, Aparna Bhardwaj 3 1Associate
Managing Menstrual Disorders
 Managing Menstrual Disorders David G. Weismiller, MD, ScM, FAAFP Professor Department of Family Medicine The Brody School of Medicine at East Carolina University Greenville, North Carolina Learning Objectives
Managing Menstrual Disorders David G. Weismiller, MD, ScM, FAAFP Professor Department of Family Medicine The Brody School of Medicine at East Carolina University Greenville, North Carolina Learning Objectives
Reproductive Hormones
 Reproductive Hormones Male gonads: testes produce male sex cells! sperm Female gonads: ovaries produce female sex cells! ovum The union of male and female sex cells during fertilization produces a zygote
Reproductive Hormones Male gonads: testes produce male sex cells! sperm Female gonads: ovaries produce female sex cells! ovum The union of male and female sex cells during fertilization produces a zygote
Hormonal Control of Human Reproduction
 Hormonal Control of Human Reproduction Bởi: OpenStaxCollege The human male and female reproductive cycles are controlled by the interaction of hormones from the hypothalamus and anterior pituitary with
Hormonal Control of Human Reproduction Bởi: OpenStaxCollege The human male and female reproductive cycles are controlled by the interaction of hormones from the hypothalamus and anterior pituitary with
Reproductive System. Testes. Accessory reproductive organs. gametogenesis hormones. Reproductive tract & Glands
 Reproductive System Testes gametogenesis hormones Accessory reproductive organs Reproductive tract & Glands transport gametes provide nourishment for gametes Hormonal regulation in men Hypothalamus - puberty
Reproductive System Testes gametogenesis hormones Accessory reproductive organs Reproductive tract & Glands transport gametes provide nourishment for gametes Hormonal regulation in men Hypothalamus - puberty
Reproduction and Development. Female Reproductive System
 Reproduction and Development Female Reproductive System Outcomes 5. Identify the structures in the human female reproductive system and describe their functions. Ovaries, Fallopian tubes, Uterus, Endometrium,
Reproduction and Development Female Reproductive System Outcomes 5. Identify the structures in the human female reproductive system and describe their functions. Ovaries, Fallopian tubes, Uterus, Endometrium,
MANAGEMENT OF REFRACTORY ENDOMETRIOSIS
 (339) MANAGEMENT OF REFRACTORY ENDOMETRIOSIS Serdar Bulun, MD JJ Sciarra Professor and Chair Department of Ob/Gyn Northwestern University ENDOMETRIOSIS OCs Teenager: severe dysmenorrhea often starting
(339) MANAGEMENT OF REFRACTORY ENDOMETRIOSIS Serdar Bulun, MD JJ Sciarra Professor and Chair Department of Ob/Gyn Northwestern University ENDOMETRIOSIS OCs Teenager: severe dysmenorrhea often starting
Polycystic Ovary Syndrome HEATHER BURKS, MD OU PHYSICIANS REPRODUCTIVE MEDICINE SEPTEMBER 21, 2018
 Polycystic Ovary Syndrome HEATHER BURKS, MD OU PHYSICIANS REPRODUCTIVE MEDICINE SEPTEMBER 21, 2018 Learning Objectives At the conclusion of this lecture, learners should: 1) Know the various diagnostic
Polycystic Ovary Syndrome HEATHER BURKS, MD OU PHYSICIANS REPRODUCTIVE MEDICINE SEPTEMBER 21, 2018 Learning Objectives At the conclusion of this lecture, learners should: 1) Know the various diagnostic
of AUB DISCLOSURES 10/29/2018
 of AUB DR. DEBRA GIERUT MD DEPARTMENT OF OBSTETRICS AND GYNECOLOGY KAISER PERMANENTE, ORANGE COUNTY DISCLOSURES I have no financial disclosures Lisa Samerdyke, the Director of National Accounts for Hologic
of AUB DR. DEBRA GIERUT MD DEPARTMENT OF OBSTETRICS AND GYNECOLOGY KAISER PERMANENTE, ORANGE COUNTY DISCLOSURES I have no financial disclosures Lisa Samerdyke, the Director of National Accounts for Hologic
Topics. Periods Menopause & HRT Contraception Vulva problems
 Girls stuff Topics Periods Menopause & HRT Contraception Vulva problems Menorrhagia Excessive menstrual loss occurring with regular or irregular cycles Ovulatory Anovulatory Usual blood loss 30-40ml per
Girls stuff Topics Periods Menopause & HRT Contraception Vulva problems Menorrhagia Excessive menstrual loss occurring with regular or irregular cycles Ovulatory Anovulatory Usual blood loss 30-40ml per
12/13/2017. Important references for PCOS. Polycystic Ovarian Syndrome (PCOS) for the Family Physician. 35 year old obese woman
 for the Family Physician. 35 year old obese woman") Polycystic Ovarian Syndrome (PCOS) for the Family Physician Barbara S. Apgar MD, MS Professor or Family Medicine University of Michigan Ann Arbor, Michigan Important references for PCOS Endocrine Society
Polycystic Ovarian Syndrome (PCOS) for the Family Physician Barbara S. Apgar MD, MS Professor or Family Medicine University of Michigan Ann Arbor, Michigan Important references for PCOS Endocrine Society
IMPORTANCE OF CLINICAL HISTORY AND ENDOMETRIAL HISTOMORPHOLOGY IN TREATMENT DYSFUNCTIONAL UTERINE BLEEDING
 IJCRR Section: Healthcare Sci. Journal Impact Factor 4.016 Research Article IMPORTANCE OF CLINICAL HISTORY AND ENDOMETRIAL HISTOMORPHOLOGY IN TREATMENT DYSFUNCTIONAL UTERINE BLEEDING Panchal Nirav S. 1,
IJCRR Section: Healthcare Sci. Journal Impact Factor 4.016 Research Article IMPORTANCE OF CLINICAL HISTORY AND ENDOMETRIAL HISTOMORPHOLOGY IN TREATMENT DYSFUNCTIONAL UTERINE BLEEDING Panchal Nirav S. 1,
Index. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A Abdominal myomectomy in leiomyoma management, 77 Abnormal uterine bleeding (AUB) described, 103 105 normal menstrual bleeding vs., 104
Index Note: Page numbers of article titles are in boldface type. A Abdominal myomectomy in leiomyoma management, 77 Abnormal uterine bleeding (AUB) described, 103 105 normal menstrual bleeding vs., 104
INFERTILITY CAUSES. Basic evaluation of the female
 INFERTILITY Infertility is the inability to conceive after 12 months of unprotected intercourse. There are multiple causes of infertility and a systematic way to evaluate the condition. Let s look at some
INFERTILITY Infertility is the inability to conceive after 12 months of unprotected intercourse. There are multiple causes of infertility and a systematic way to evaluate the condition. Let s look at some
Chapter 14 Reproduction Review Assignment
 Date: Mark: _/45 Chapter 14 Reproduction Review Assignment Multiple Choice Identify the choice that best completes the statement or answers the question. 1. Use the diagram above to answer the next question.
Date: Mark: _/45 Chapter 14 Reproduction Review Assignment Multiple Choice Identify the choice that best completes the statement or answers the question. 1. Use the diagram above to answer the next question.
Menstrual Disorders & Ambulatory Gynaecology
 Menstrual Disorders & Ambulatory Gynaecology Mr. Nagui Lewis Aziz M B, CH B, FRCOG Consultant Gynaecologist The Royal Oldham Hospital 01/09/2018 Heavy menstrual bleeding (HMB ) is a common problem responsible
Menstrual Disorders & Ambulatory Gynaecology Mr. Nagui Lewis Aziz M B, CH B, FRCOG Consultant Gynaecologist The Royal Oldham Hospital 01/09/2018 Heavy menstrual bleeding (HMB ) is a common problem responsible
PERIMENOPAUSE. Objectives. Disclosure. The Perimenopause Perimenopause Menopause. Definitions of Menopausal Transition: STRAW.
 PERIMENOPAUSE Patricia J. Sulak, MD Founder, Living WELL Aware LLC Author, Should I Fire My Doctor? Author, Living WELL Aware: Eleven Essential Elements to Health and Happiness Endowed Professor Texas
PERIMENOPAUSE Patricia J. Sulak, MD Founder, Living WELL Aware LLC Author, Should I Fire My Doctor? Author, Living WELL Aware: Eleven Essential Elements to Health and Happiness Endowed Professor Texas
Perimenopausal DUB. Mary Anne Jamieson, MD Associate Professor, OB/GYN Queen s University Kingston, Ontario
 Perimenopausal DUB Mary Anne Jamieson, MD Associate Professor, OB/GYN Queen s University Kingston, Ontario Objectives Clinicians will: Make a confident diagnosis for Perimenopausal DUB (know how/when to
Perimenopausal DUB Mary Anne Jamieson, MD Associate Professor, OB/GYN Queen s University Kingston, Ontario Objectives Clinicians will: Make a confident diagnosis for Perimenopausal DUB (know how/when to
Dr Mary Birdsall. Fertility Associates Auckland
 Dr Mary Birdsall Fertility Associates Auckland Period Problems Mary Birdsall Medical Director Fertility Associates Auckland Period Problems Basic Physiology No Periods Irregular Periods Heavy Periods
Dr Mary Birdsall Fertility Associates Auckland Period Problems Mary Birdsall Medical Director Fertility Associates Auckland Period Problems Basic Physiology No Periods Irregular Periods Heavy Periods
N. Shirazian, MD. Endocrinologist
 N. Shirazian, MD Internist, Endocrinologist Inside the ovary Day 15-28: empty pyfollicle turns into corpus luteum (yellow body) Immature eggs Day 1-13: 13: egg developing inside the growing follicle Day
N. Shirazian, MD Internist, Endocrinologist Inside the ovary Day 15-28: empty pyfollicle turns into corpus luteum (yellow body) Immature eggs Day 1-13: 13: egg developing inside the growing follicle Day
Reproductive Testing: Less is More G. Wright Bates, Jr., M.D. Professor and Director Reproductive Endocrinology and Infertility Objectives
 Reproductive Testing: Less is More G. Wright Bates, Jr., M.D. Professor and Director Reproductive Endocrinology and Infertility Objectives 1. Review definition of infertility and impact of age 2. Stress
Reproductive Testing: Less is More G. Wright Bates, Jr., M.D. Professor and Director Reproductive Endocrinology and Infertility Objectives 1. Review definition of infertility and impact of age 2. Stress
Perimenopausal Age Group (45-55yrs): For Early Detection And Treatment.
: For Early Detection And Treatment.") IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) e-issn: 2279-0853, p-issn: 2279-0861.Volume 17, Issue 9 Ver. 4 (September. 2018), PP 73-77 www.iosrjournals.org Perimenopausal Age Group (45-55yrs):
IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) e-issn: 2279-0853, p-issn: 2279-0861.Volume 17, Issue 9 Ver. 4 (September. 2018), PP 73-77 www.iosrjournals.org Perimenopausal Age Group (45-55yrs):
The 6 th Scientific Meeting of the Asia Pacific Menopause Federation
 Abnormal uterine bleeding in the perimenopause Perimenopausal menstrual problems are among the most common causes for family practitioner and specialist referral. Often it is due to the hormone changes
Abnormal uterine bleeding in the perimenopause Perimenopausal menstrual problems are among the most common causes for family practitioner and specialist referral. Often it is due to the hormone changes
Index. Cytoplasm, nonepithelial malignant tumor features 70
 Accurette device 23 Adenosarcoma, differential diagnosis 80, 81 Arias-Stella reaction 65 Atypical endocervical cells 8 Atypical endometrial cells 8 Atypical glandular cells (AGC) 8, 9 Atypical glandular
Accurette device 23 Adenosarcoma, differential diagnosis 80, 81 Arias-Stella reaction 65 Atypical endocervical cells 8 Atypical endometrial cells 8 Atypical glandular cells (AGC) 8, 9 Atypical glandular
Sexual dysfunction of chronic kidney disease. Razieh salehian.md psychiatrist
 Sexual dysfunction of chronic kidney disease Razieh salehian.md psychiatrist Disturbances in sexual function are a common feature of chronic renal failure. Sexual dysfunction is inversely associated with
Sexual dysfunction of chronic kidney disease Razieh salehian.md psychiatrist Disturbances in sexual function are a common feature of chronic renal failure. Sexual dysfunction is inversely associated with
Atypical Hyperplasia/EIN
 EIN Atypical Hyperplasia/EIN Based on scientific and diagnostic advances, in 2014 the WHO moved that the precursor lesion for endometrioid carcinoma be atypical hyperplasia/ein, rather than what was previously
EIN Atypical Hyperplasia/EIN Based on scientific and diagnostic advances, in 2014 the WHO moved that the precursor lesion for endometrioid carcinoma be atypical hyperplasia/ein, rather than what was previously
Endometrial Hyperplasia: A Clinicopathological Study in a Tertiary Care Hospital
 DOI 10.1007/s13224-013-0414-2 ORIGINAL ARTICLE Endometrial Hyperplasia: A Clinicopathological Study in a Tertiary Care Hospital Raychaudhuri Gargi Bandyopadhyay Anjali Sarkar Dipnarayan Mandal Sarbeswar
DOI 10.1007/s13224-013-0414-2 ORIGINAL ARTICLE Endometrial Hyperplasia: A Clinicopathological Study in a Tertiary Care Hospital Raychaudhuri Gargi Bandyopadhyay Anjali Sarkar Dipnarayan Mandal Sarbeswar
Study of Hypothyroidism in Women with Abnormal Uterine Bleeding
 IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) e-issn: 2279-0853, p-issn: 2279-0861.Volume 15, Issue 4 Ver. VI (Apr. 2016), PP 12-18 www.iosrjournals.org Study of Hypothyroidism in Women with
IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) e-issn: 2279-0853, p-issn: 2279-0861.Volume 15, Issue 4 Ver. VI (Apr. 2016), PP 12-18 www.iosrjournals.org Study of Hypothyroidism in Women with
Infertility DR. RAHUL BEVARA
 Infertility DR. RAHUL BEVARA Definitions Infertility is defined as the inability to conceive after one year of unprotected coitus. Affects 10-15% of couples Primary Infertility, that is inability to conceive
Infertility DR. RAHUL BEVARA Definitions Infertility is defined as the inability to conceive after one year of unprotected coitus. Affects 10-15% of couples Primary Infertility, that is inability to conceive
Hd Hydroxylase. Cholesterol. 17-OH Pregnenolne DHEA Andrstendiol. Pregnenolone. 17-OH Progestrone. Androstendione. Progestrone.
 PATHOPHISIOLOGY OF SEX HORMONES R. Mohammadi Biochemist (Ph.D.) Faculty member of Medical Faculty CHOLESTEROL IS THE PRECURSOR OF STERIOD HORMONES Cholesterol Pregnenolone 17-OH 17βHSD Pregnenolne DHEA
PATHOPHISIOLOGY OF SEX HORMONES R. Mohammadi Biochemist (Ph.D.) Faculty member of Medical Faculty CHOLESTEROL IS THE PRECURSOR OF STERIOD HORMONES Cholesterol Pregnenolone 17-OH 17βHSD Pregnenolne DHEA
FERTILITY & TCM. On line course provided by. Taught by Clara Cohen
 FERTILITY & TCM On line course provided by Taught by Clara Cohen FERTILITY & TCM FERTILITY AND TCM THE PRACTITIONER S ROLE CAUSES OF INFERTILITY RISK FACTORS OBJECTIVES UNDERSTANDING TESTS Conception in
FERTILITY & TCM On line course provided by Taught by Clara Cohen FERTILITY & TCM FERTILITY AND TCM THE PRACTITIONER S ROLE CAUSES OF INFERTILITY RISK FACTORS OBJECTIVES UNDERSTANDING TESTS Conception in
A study on correlation between bleeding pattern and histopathological findings of endometrium among perimenopausal women
 International Journal of Reproduction, Contraception, Obstetrics and Gynecology Nair R et al. Int J Reprod Contracept Obstet Gynecol. 25 Dec;4(6):1758-1762 www.ijrcog.org pissn 2320-1770 eissn 2320-1789
International Journal of Reproduction, Contraception, Obstetrics and Gynecology Nair R et al. Int J Reprod Contracept Obstet Gynecol. 25 Dec;4(6):1758-1762 www.ijrcog.org pissn 2320-1770 eissn 2320-1789
I. Endocrine System & Hormones Figure 1: Human Endocrine System
 I. Endocrine System & Hormones Figure 1: Human Endocrine System Endocrine System: a) Endocrine glands are ductless since they lack specific vessels for the transport of hormones throughout the body. Instead,
I. Endocrine System & Hormones Figure 1: Human Endocrine System Endocrine System: a) Endocrine glands are ductless since they lack specific vessels for the transport of hormones throughout the body. Instead,
GLOBAL ENDOMETRIAL ABLATION TECHNOLOGY
 GLOBAL ENDOMETRIAL ABLATION TECHNOLOGY Training: Part 1 Anatomy and Physiology Female Anatomy Normal Uterus Female Anatomy Normal Uterus Female Anatomy Uterine Positions Abnormal Uterus Retroflexed Normal
GLOBAL ENDOMETRIAL ABLATION TECHNOLOGY Training: Part 1 Anatomy and Physiology Female Anatomy Normal Uterus Female Anatomy Normal Uterus Female Anatomy Uterine Positions Abnormal Uterus Retroflexed Normal
CLEAR COVERAGE HYSTERECTOMY CHECKLISTS
 CLEAR COVERAGE HYSTERECTOMY CHECKLISTS Click on the link below to access the checklist sheet. Abnormal Uterine Bleeding Adenomyosis Chronic Abdominal or Pelvic Pain Endometriosis Fibroids General Guidelines
CLEAR COVERAGE HYSTERECTOMY CHECKLISTS Click on the link below to access the checklist sheet. Abnormal Uterine Bleeding Adenomyosis Chronic Abdominal or Pelvic Pain Endometriosis Fibroids General Guidelines
Abnormal Uterine Bleeding
 Abnormal Uterine Bleeding Randy A. Fink, MD, FACOG Obstetrics & Gynecology A simplified approach for primary care Disclosures I have no relevant disclosures pertaining to this program. Learning Objectives
Abnormal Uterine Bleeding Randy A. Fink, MD, FACOG Obstetrics & Gynecology A simplified approach for primary care Disclosures I have no relevant disclosures pertaining to this program. Learning Objectives
Received, June 29, 1904; accepted for publication
 THE AMEBICAN JOURNAL OF CLINICAL PATHOLOGY Copyright 1964 by The Williams & Wilkins Co. Vol. 42, No. 0 Printed in U.S.A. CARCINOMA IN SITU OF THE ENDOMETRIUM ISABELLE A. BUEHL, M.D., PRANK VELLIOS, M.D.,
THE AMEBICAN JOURNAL OF CLINICAL PATHOLOGY Copyright 1964 by The Williams & Wilkins Co. Vol. 42, No. 0 Printed in U.S.A. CARCINOMA IN SITU OF THE ENDOMETRIUM ISABELLE A. BUEHL, M.D., PRANK VELLIOS, M.D.,
9.4 Regulating the Reproductive System
 9.4 Regulating the Reproductive System The Reproductive System to unite a single reproductive cell from a female with a single reproductive cell from a male Both male and female reproductive systems include
9.4 Regulating the Reproductive System The Reproductive System to unite a single reproductive cell from a female with a single reproductive cell from a male Both male and female reproductive systems include
PCOS and Obesity DUB is better treated by OCPs
 PCOS and Obesity DUB is better treated by OCPs Dr. Ritu Joshi Senior consultant Fortis escorts Hospital, Jaipur Chairperson Family welfare com. FOGSI (20092012) Vice President FOGSI 2014 Introduction One
PCOS and Obesity DUB is better treated by OCPs Dr. Ritu Joshi Senior consultant Fortis escorts Hospital, Jaipur Chairperson Family welfare com. FOGSI (20092012) Vice President FOGSI 2014 Introduction One
Physiology of Male Reproductive System
 Physiology of Male Reproductive System the anterior pituitary gland serves as the primary control of reproductive function at puberty Ant Pituitary secretes FSH & large amounts of LH (ICSH) FSH & LH cause
Physiology of Male Reproductive System the anterior pituitary gland serves as the primary control of reproductive function at puberty Ant Pituitary secretes FSH & large amounts of LH (ICSH) FSH & LH cause
Chapter 27 The Reproductive System. MDufilho
 Chapter 27 The Reproductive System 1 Figure 27.19 Events of oogenesis. Before birth Meiotic events 2n Oogonium (stem cell) Mitosis Follicle development in ovary Follicle cells Oocyte 2n Primary oocyte
Chapter 27 The Reproductive System 1 Figure 27.19 Events of oogenesis. Before birth Meiotic events 2n Oogonium (stem cell) Mitosis Follicle development in ovary Follicle cells Oocyte 2n Primary oocyte
Phases of the Ovarian Cycle
 OVARIAN CYCLE An ovary contains many follicles, and each one contains an immature egg called an oocyte. A female is born with as many as 2 million follicles, but the number is reduced to 300,000 to 400,000
OVARIAN CYCLE An ovary contains many follicles, and each one contains an immature egg called an oocyte. A female is born with as many as 2 million follicles, but the number is reduced to 300,000 to 400,000
LUTEINIZED UNRUPTURED FOLLICLE SYNDROME: A SUBTLE CAUSE OF INFERTILITY*
 FERTILITY AND STERILITY Copyright c 1978 The American Fertility Society Vol. 29, No.3, March 1978 Printed in U.S.A. LUTEINIZED UNRUPTURED FOLLICLE SYNDROME: A SUBTLE CAUSE OF INFERTILITY* JAROSLA V MARIK,
FERTILITY AND STERILITY Copyright c 1978 The American Fertility Society Vol. 29, No.3, March 1978 Printed in U.S.A. LUTEINIZED UNRUPTURED FOLLICLE SYNDROME: A SUBTLE CAUSE OF INFERTILITY* JAROSLA V MARIK,
PALM-COEIN: Your AUB Counseling Guide
 PALM-COEIN: Your AUB Counseling Guide 10 million+ Treat the cause, not the symptom In the U.S, more than 10 million women between the ages of 35 and 49 are affected by AUB 1 Diagnosis Cause Structural
PALM-COEIN: Your AUB Counseling Guide 10 million+ Treat the cause, not the symptom In the U.S, more than 10 million women between the ages of 35 and 49 are affected by AUB 1 Diagnosis Cause Structural
Understanding Infertility, Evaluations, and Treatment Options
 Understanding Infertility, Evaluations, and Treatment Options Arlene J. Morales, M.D., F.A.C.O.G. Fertility Specialists Medical Group, Inc. What We Will Cover Introduction What is infertility? Briefly
Understanding Infertility, Evaluations, and Treatment Options Arlene J. Morales, M.D., F.A.C.O.G. Fertility Specialists Medical Group, Inc. What We Will Cover Introduction What is infertility? Briefly
Reproductive physiology
 Reproductive physiology Sex hormones: Androgens Estrogens Gestagens Learning objectives 86 (also 90) Sex Genetic sex Gonadal sex Phenotypic sex XY - XX chromosomes testes - ovaries external features Tha
Reproductive physiology Sex hormones: Androgens Estrogens Gestagens Learning objectives 86 (also 90) Sex Genetic sex Gonadal sex Phenotypic sex XY - XX chromosomes testes - ovaries external features Tha
Molly A. Brewer DVM, MD, MS Chair and Professor Department of Obstetrics and Gynecology University of Connecticut School of Medicine
 Molly A. Brewer DVM, MD, MS Chair and Professor Department of Obstetrics and Gynecology University of Connecticut School of Medicine Review causes of abnormal uterine bleeding: Adolescent Reproductive
Molly A. Brewer DVM, MD, MS Chair and Professor Department of Obstetrics and Gynecology University of Connecticut School of Medicine Review causes of abnormal uterine bleeding: Adolescent Reproductive
Gynecologic Considerations in Women with FA
 Gynecologic Considerations in Women with FA RAHEL GHEBRE, M.D., MPH University of Minnesota Medical School Objectives Recommendation for Gynecologic Care FA girls starting at age 16 should establish a
Gynecologic Considerations in Women with FA RAHEL GHEBRE, M.D., MPH University of Minnesota Medical School Objectives Recommendation for Gynecologic Care FA girls starting at age 16 should establish a
MULTIPLE CHOICE: match the term(s) or description with the appropriate letter of the structure.
 or description with the appropriate letter of the structure.") Chapter 27 Exam Due NLT Thursday, July 31, 2015 Name MULTIPLE CHOICE: match the term(s) or description with the appropriate letter of the structure. Figure 27.1 Using Figure 27.1, match the following:
Chapter 27 Exam Due NLT Thursday, July 31, 2015 Name MULTIPLE CHOICE: match the term(s) or description with the appropriate letter of the structure. Figure 27.1 Using Figure 27.1, match the following:
Web Activity: Simulation Structures of the Female Reproductive System
 differentiate. The epididymis is a coiled tube found along the outer edge of the testis where the sperm mature. 3. Testosterone is a male sex hormone produced in the interstitial cells of the testes. It
differentiate. The epididymis is a coiled tube found along the outer edge of the testis where the sperm mature. 3. Testosterone is a male sex hormone produced in the interstitial cells of the testes. It
Infertility: failure to conceive within one year of unprotected regular sexual intercourse. Primary secondary
 Subfertility Infertility: failure to conceive within one year of unprotected regular sexual intercourse. Primary secondary Infertility affects about 15 % of couples. age of the female. Other factors that
Subfertility Infertility: failure to conceive within one year of unprotected regular sexual intercourse. Primary secondary Infertility affects about 15 % of couples. age of the female. Other factors that
10.7 The Reproductive Hormones
 10.7 The Reproductive Hormones December 10, 2013. Website survey?? QUESTION: Who is more complicated: men or women? The Female Reproductive System ovaries: produce gametes (eggs) produce estrogen (steroid
10.7 The Reproductive Hormones December 10, 2013. Website survey?? QUESTION: Who is more complicated: men or women? The Female Reproductive System ovaries: produce gametes (eggs) produce estrogen (steroid
Gayatrri Anipindi *, Vani I. Original Research Article. Abstract
 Original Research Article Role of levonorgestrel releasing intrauterine device in management of heavy menstrual bleeding: A safe and effective option for all PALM COEIN variants Gayatrri Anipindi *, Vani
Original Research Article Role of levonorgestrel releasing intrauterine device in management of heavy menstrual bleeding: A safe and effective option for all PALM COEIN variants Gayatrri Anipindi *, Vani
Intrauterine delivery of progestogen in the peri- and postmenopausal women. Outline of the presentation. Levonorgestrel releasing IUS - Mirena
 QuickTime ja Valokuva - JPEG pakkauksen purkuohjelma tarvitaan elokuvan katselemiseen. Intrauterine delivery of progestogen in the peri- and postmenopausal women ESHRE Campus meeting 6.-7.10.2008 Oskari
QuickTime ja Valokuva - JPEG pakkauksen purkuohjelma tarvitaan elokuvan katselemiseen. Intrauterine delivery of progestogen in the peri- and postmenopausal women ESHRE Campus meeting 6.-7.10.2008 Oskari
The Science of your Cycle
 The Science of your Cycle Day 3: Get to know your cycle (Part I) with Jennifer Aldoretta Cofounder & CEO of Groove Today s goals Learn how your hormones work together to create the changes that happen
The Science of your Cycle Day 3: Get to know your cycle (Part I) with Jennifer Aldoretta Cofounder & CEO of Groove Today s goals Learn how your hormones work together to create the changes that happen
DIP.G.O. EXAMINATION 2007
 DIP.G.O. EXAMINATION 2007 GYNAECOLOGY Batch A/07 Time : 2 hrs. Question 1. a. Define Dysfunctional Uterine Bleeding 10 b. What are the various terms used to describe menstrual disorder? 10 Question 2.
DIP.G.O. EXAMINATION 2007 GYNAECOLOGY Batch A/07 Time : 2 hrs. Question 1. a. Define Dysfunctional Uterine Bleeding 10 b. What are the various terms used to describe menstrual disorder? 10 Question 2.
Female reproductive system II Enas Omar. Notes are in green
 Female reproductive system II Enas Omar Notes are in green C.Luteal phase a. Interval between ovulation and menstrual flow (15 th - 28 th day.( b. Duration is κ: 2± 14d (t½ = corpus luteum.( c. Day of
Female reproductive system II Enas Omar Notes are in green C.Luteal phase a. Interval between ovulation and menstrual flow (15 th - 28 th day.( b. Duration is κ: 2± 14d (t½ = corpus luteum.( c. Day of
THE MENSTRUAL CYCLE INA S. IRABON, MD, FPOGS, FPSRM, FPSGE OBSTETRICS AND GYNECOLOGY REPRODUCTIVE ENDOCRINOLOGY AND INFERTILITY
 THE MENSTRUAL CYCLE INA S. IRABON, MD, FPOGS, FPSRM, FPSGE OBSTETRICS AND GYNECOLOGY REPRODUCTIVE ENDOCRINOLOGY AND INFERTILITY REFERENCE Comprehensive Gynecology 7 th edition, 2017 (Lobo RA, Gershenson
THE MENSTRUAL CYCLE INA S. IRABON, MD, FPOGS, FPSRM, FPSGE OBSTETRICS AND GYNECOLOGY REPRODUCTIVE ENDOCRINOLOGY AND INFERTILITY REFERENCE Comprehensive Gynecology 7 th edition, 2017 (Lobo RA, Gershenson
Hitting the High Points Gynecologic Oncology Review
 Hitting the High Points is designed to cover exam-based material, from preinvasive neoplasms of the female genital tract to the presentation, diagnosis and treatment, including surgery, chemotherapy, and
Hitting the High Points is designed to cover exam-based material, from preinvasive neoplasms of the female genital tract to the presentation, diagnosis and treatment, including surgery, chemotherapy, and
Infertility. Review and Update Clifford C. Hayslip MD Intrauterine Inseminations
 Infertility Review and Update Clifford C. Hayslip MD Intrauterine Inseminations Beneficial effects of IUI not consistently documented in studies No deleterious effects on fertility 3-4 cycles of IUI should
Infertility Review and Update Clifford C. Hayslip MD Intrauterine Inseminations Beneficial effects of IUI not consistently documented in studies No deleterious effects on fertility 3-4 cycles of IUI should
Causes of Infertility and Treatment Options
 Causes of Infertility and Treatment Options Dr Mrs.Kiran D. Sekhar Former vice President-FOGSI Former Chairperson- Genetics and Foetal medicine-fogsi Founder and Medical Director-Kiran Infertility centre
Causes of Infertility and Treatment Options Dr Mrs.Kiran D. Sekhar Former vice President-FOGSI Former Chairperson- Genetics and Foetal medicine-fogsi Founder and Medical Director-Kiran Infertility centre
ROLE OF HORMONAL ASSAY IN DIAGNOSING PCOD DR GAANA SREENIVAS (JSS,MYSURU)
") ROLE OF HORMONAL ASSAY IN DIAGNOSING PCOD DR GAANA SREENIVAS (JSS,MYSURU) In 1935, Stein and Leventhal described 7 women with bilateral enlarged PCO, amenorrhea or irregular menses, infertility and masculinizing
ROLE OF HORMONAL ASSAY IN DIAGNOSING PCOD DR GAANA SREENIVAS (JSS,MYSURU) In 1935, Stein and Leventhal described 7 women with bilateral enlarged PCO, amenorrhea or irregular menses, infertility and masculinizing
lactotrophs 120 min- FSH 60 min- LH Hypothalamus GnRH pituitary Estradiol +/- Progesterone _ FSH L H Ovary Uterus Ovulation Antral follicle >2mm
 lactotrophs Hypothalamus GnRH 120 min- 60 min- LH Progesterone _ pituitary L H + Ovary + Estradiol +/- Uterus Antral follicle >2mm Ovulation Preovulatory follicles atresia Follicular phase Luteal phase
lactotrophs Hypothalamus GnRH 120 min- 60 min- LH Progesterone _ pituitary L H + Ovary + Estradiol +/- Uterus Antral follicle >2mm Ovulation Preovulatory follicles atresia Follicular phase Luteal phase
Embryology Lecture # 4
 1 Quick Review: Oogenesis : - Oogonia start appear in the ovary when the age of the fetus 1 is th (5 week). - Then the Oogonia transformed into 1ry Oocyte. - 1ry Oocyte is surrounded by a follicle (cover).
1 Quick Review: Oogenesis : - Oogonia start appear in the ovary when the age of the fetus 1 is th (5 week). - Then the Oogonia transformed into 1ry Oocyte. - 1ry Oocyte is surrounded by a follicle (cover).
Stage 4 - Ovarian Cancer Symptoms
 WELCOME Stage 4 - Ovarian Cancer Symptoms University of Baghdad College of Nursing Department of Basic Medical Sciences Overview of Anatomy and Physioloy II Second Year Students Asaad Ismail Ahmad,
WELCOME Stage 4 - Ovarian Cancer Symptoms University of Baghdad College of Nursing Department of Basic Medical Sciences Overview of Anatomy and Physioloy II Second Year Students Asaad Ismail Ahmad,
Outline. Male Reproductive System Testes and Sperm Hormonal Regulation
 Outline Male Reproductive System Testes and Sperm Hormonal Regulation Female Reproductive System Genital Tract Hormonal Levels Uterine Cycle Fertilization and Pregnancy Control of Reproduction Infertility
Outline Male Reproductive System Testes and Sperm Hormonal Regulation Female Reproductive System Genital Tract Hormonal Levels Uterine Cycle Fertilization and Pregnancy Control of Reproduction Infertility
Ph.D. THESIS ENDOMETRIAL HYPERPLASIAS IN PERIMENOPAUSE SUMMARY
 UNIVERSITY OF MEDICINE AND PHARMACY OF CRAIOVA FACULTY OF MEDICINE Ph.D. THESIS ENDOMETRIAL HYPERPLASIAS IN PERIMENOPAUSE SUMMARY SCIENTIFIC COORDINATOR: PROF. DR. MIHAI B. BRĂILA, Ph.D. Ph.D. Graduand:
UNIVERSITY OF MEDICINE AND PHARMACY OF CRAIOVA FACULTY OF MEDICINE Ph.D. THESIS ENDOMETRIAL HYPERPLASIAS IN PERIMENOPAUSE SUMMARY SCIENTIFIC COORDINATOR: PROF. DR. MIHAI B. BRĂILA, Ph.D. Ph.D. Graduand:
Chapter 28: REPRODUCTIVE SYSTEM: MALE
 Chapter 28: REPRODUCTIVE SYSTEM: MALE I. FUNCTIONAL ANATOMY (Fig. 28.1) A. Testes: glands which produce male gametes, as well as glands producing testosterone 2. Seminiferous tubules (Fig.28.3; 28.5) a.
Chapter 28: REPRODUCTIVE SYSTEM: MALE I. FUNCTIONAL ANATOMY (Fig. 28.1) A. Testes: glands which produce male gametes, as well as glands producing testosterone 2. Seminiferous tubules (Fig.28.3; 28.5) a.