Shape the Future of Urological Surgery
|
|
|
- Alexander McDowell
- 6 years ago
- Views:
Transcription

1
2 Shape the Future of Urological Surgery THE ROLE OF LAPAROSCOPIC SURGERY IN NEW MILENNIUM Victor Chia-Hsiang Lin, MD Division of Urology, Department of Surgery Chi-Mei Medical Center
3 MY TALK TODAY IS Minimal Invasiveness in Urological Surgery Endoluminal & Percutaneous & Extraluminal (Laparoscopy) Real Impact of Laparoscopic Surgery on Urology Be the standard of care? The Realm of Laparoscopic S. In Urology Practice patterns in CCF Chi-Mei Experience The Future? Miniaturization Robotic surgery & Telesurgery Endoluminal reconstruction

4 Trend In Urological Surgery Big surgeons make a big wound?? Minimal Invasiveness Less analgesics Better cosmesis Shorter hospital stay Quicker convalescence


5 Minimal Invasiveness in Urology This trend is like Industrial Revolution, like Digital Revolution
6 TERRITORY of UROLOGICAL DISEASE Endoluminal Disease: Most urolithiasis,, benign obstructive stricture, BPH, superficial TCC, Extraluminal Disease: Adrenal tumor, renal cortex tumor, retroperitoneal tumor, whatever outer than urethra and transitional cell epithelial lining
7 Trend In Urological Surgery: MIS 3 main Strategies from 3 Revolutions: Endoluminal Endoscopic surgery (1960) Percutaneous Manipulation (1970) Extraluminal Endoscopic Surgery (1990) (Lap. S.)
8 CHANGES OF SURGICAL STRATEGIES IN UROLOGY Open Surgery Open Surgery Laparoscopic S. Endourol. S. Laparoscopic S. Endourol. S.
9 MY TALK TODAY IS Minimal Invasiveness in Urological Surgery Endoluminal & Percutaneous & Extraluminal (Laparoscopy) Real Impact of Laparoscopic Surgery on Urology Be the standard of care? The Realm of Laparoscopic S. in Urology Practice patterns in CCF Chi-Mei Experience The Future? Miniaturization Robotic surgery & Telesurgery Endoluminal reconstruction

10 Besides the minimal invasiveness, Can laparoscopic S. in urology be a new STANDARD OF CARE??? Think More
 Efficacious 2) Morbidity 3)")
 Widespread availability 6) Financial viability")

11 LAPAROSCOPIC RADICAL NEPHRECTOMY To provide you data as regards: 1) Efficacious 2) Morbidity 3) Oncological adequacy 4) All comers? 5) Widespread availability 6) Financial viability Secondary Ports Primary Port Thus to make a determination as to whether or not LRN can be e considered the standard-of of-care today?
12 FACTORS THAT DETERMINE STANDARD OF CARE STATUS 1) Efficacious(=Effective and Efficiency) 2) Morbidity 3) Oncological adequacy 4) All comers? 5) Widespread availability 6) Financial viability
13 RETROPERITONEOSCOPIC RADICAL NEPHRECTOMY THE CLEVELAND C CLINIC EXPERIENCE Laparoscopic (N=100) Open (N=60) P-value Age O.R. time (hrs) EBL (ml) Tumor size (cm) Spec. wt. (gm) Hosp. Stay (d) Gill et al: Cancer 92, 1843, 2001
14 RETROPERITONEOSCOPIC RADICAL NEPHRECTOMY THE CLEVELAND CLINIC EXPERIENCE Laparoscopic (N=100) Open (N=60) P-value Narcotics (mg) <0.001 Open conversion 2 - Complications 5 (13%) 8 (24%) 0.5 Follow up (mos) <0.001
15 HOW ABOUT LARGER TUMORS.????
16 LAPAROSCOPIC RADICAL NEPHRECTOMY FOR TUMORS > 5 cm. IN SIZE: CCF EXPERIENCE LAPAROSCOPY OPEN P-valueP < 5 cm > 5 cm > 5 cm (n=48) (n=28) (n=20) Age (yrs) BMI ASA Class Tumor size (cm) Spec. Wt. (gm)
17 LAPAROSCOPIC RADICAL NEPHRECTOMY FOR TUMORS > 5 cm IN SIZE: CCF EXPERIENCE LAPAROSCOPY OPEN P-valueP < 5 cm > 5 cm > 5 cm (n=48) (n=28) (n=20) O.R. time (hrs) Blood loss (cc) Narcotics (mg) < Hosp. Stay (d) < Complic. (%) Followup (mos) <0.0001
18 HOW ABOUT OLDER PATIENTS.????
19 LAPAROSCOPIC RADICAL NEPHRECTOMY OCTAGENARIANS & NONAGENARIANS Cleveland Clinic Experience LAPAROSCOPY (n=11) OPEN (n=6) Urology, 53:1121, 1999 P-value Age 87 (80-98) 81 (80-82) 82) ASA Class 5.1 (2-8) 5 (3-10) 0.42 Co-morbidities O.R. times (hrs) Hosp. stay (d) 2 (1-7) 6 (6-11) <0.001 Complications (%) 4 (36%) 2 (33%) 0.9 Convalescence (wks) < 0.001
20 FACTORS THAT DETERMINE STANDARD OF CARE STATUS 1) Efficacious 2) Morbidity 3) Oncological adequacy 4) All comers? 5) Widespread availability 6) Financial viability
21 MORCELLATION versus INTACT EXTRACTION
22 We prefer intact extraction for ALL CANCER adrenal, kidney, bladder, prostate, testis

23 SPECIMEN RETRACTION
24 Laparoscopic Radical Nephrectomy Cleveland Clinic Experience (N=100) FOLLOW-UP = 16.1 mos (1-36 mos) Port-site recurrences : 0 Local recurrences : 0 Distant metastases : 2 Mortality : 1 (11mon) Gill et al: Cancer,1843, 2001
25 LAPAROSCOPIC RADICAL NEPHRECTOMY LONG-TERM CANCER CONTROL Ono, J Urol, 165:762, 2001 SMALL VOLUME DISEASE (<5CM) Median Follow-up: 33 mos Laparoscopy (n=119) Open (n=44) 5-yr disease free 95% 88% 5-yr patient survival 95% 96%
26 LAPAROSCOPIC RADICAL NEPHRECTOMY LONG-TERM CANCER CONTROL Ono, J Urol, 165:762, 2001 SMALL VOLUME DISEASE ( 5CM)( Median Follow-up: 25 mos Laparoscopy (n=39) Open (n=30) 3-yr disease free 100% 82% 3-yr patient survival 91% 88%
27 FACTORS THAT DETERMINE STANDARD OF CARE STATUS 1) Efficacious 2) Morbidity 3) Oncological adequacy 4) All comers? 5) Widespread availability 6) Financial viability

28 Retroperitoneoscopic Radical Nephrectomy THE CLEVELAND CLINIC EXPERIENCE INDICATIONS: 2005 All comers with. T1-T3aNoMo renal tumors No evidence of IVC involvement No perirenal invasion
29 Retroperitoneoscopic Radical Nephrectomy The Cleveland Clinic Experience CONTRAINDICATIONS : 2005 IVC involvement Locally invasive tumors Bulky lymphadenopathy Tumor size?
 All comers?")
30 FACTORS THAT DETERMINE STANDARD OF CARE STATUS 1) Efficacious 2) Morbidity 3) Oncological adequacy 4) All comers? 5) Widespread availability 6) Financial viability
31 WIDESPREAD AVAILABILITY > 3000 cases performed Available in all continents Performed at multiple hospitals by multiple surgeons
 All comers?")
32 FACTORS THAT DETERMINE STANDARD OF CARE STATUS 1) Efficacious 2) Morbidity 3) Oncological adequacy 4) All comers? 5) Widespread availability 6) Financial viability Expensive or Cheap??
33 LAPAROSCOPIC RADICAL NEPHRECTOMY FINANCIAL ANALYSIS WE COMPARED THE HISTORICAL CHARGES OF Open radical nephrectomy (n=20) ( ) vs. Laparoscopic radical nephrectomy (n=18) ( ) vs. Laparoscopic radical nephrectomy (n=15) ( )
34 LAPAROSCOPIC RADICAL NEPHRECTOMY FINANCIAL ANALYSIS Open (n=20) Laparoscopic (n=18) Laparoscopic (n=15) Age (yrs) Tumor size (cm) O.R. time (hrs) Hosp. stay (d) 5.9 <1 <1
35 LAPAROSCOPIC RADICAL NEPHRECTOMY FINANCIAL ANALYSIS Open (n=20) Laparoscopic (n=18) Laparoscopic (n=15) Intra-op $2755 $5565 $3661 Post-op op $2289 $1155 $753 TOTAL $5044 $6721 $4414
36 LAPAROSCOPIC RADICAL NEPHRECTOMY FINANCIAL ANALYSIS Open (n=20) Laparoscopic (n=18) Laparoscopic (n=15) Intra-op 1 102% higher 33% higher Post-op op 1 49% lower 67% lower TOTAL 1 33% higher 12.5% lower
37 LAPAROSCOPIC RADICAL NEPHRECTOMY FINANCIAL ANALYSIS UNDER-ESTIMATED ESTIMATED SOCIO-ECONOMIC VALUE Patient Care: Cost of family care (time, fee ) Postop Recovery: Earlier to resume work Less Morbidity and Complication
38 Laparoscopic Radical Nephrectomy The Cleveland Clinic Experience Summary In 2005 Cosmetically superior O.R. time same as open surgery ( hrs) Shorter hospital stay (1.4 vs 5.8 days) Quicker recovery; considerably less morbidity Equivalent cancer control Financially 12.5% cheaper than open
39 If the difficulty is the only excuse of reluctance to laparoscopic radical nephrectomy, laparoscopic radical nephrectomy will be the treatment of choice in the near future!!
40 QUIZ? So, today If President Chen presents to you With a CT-scan diagnosed 8-10 cm organ-confined Kidney tumor
41 Should LRNx not be e considered as the standard-of of-care in this kind of VIP -class patient??
42 MY TALK TODAY IS Minimal Invasiveness in Urological Surgery Endoluminal & Percutaneous & Extraluminal (Laparoscopy) Real Impact of Laparoscopic Surgery on Urology Be the standard of care? The Realm of Laparoscopic S. Practice patterns in CCF Chi-Mei Experience The Future? Miniaturization Robotic surgery & Telesurgery Endoluminal reconstruction
43 Standard Laparoscopic Surgeries in CCF * indicates till November 30, * Adrenalectomy Open Lap Nephrectomy Open Lap NU Open Lap Live Donor Nx Open Lap
44 Advanced Laparoscopic Surgeries in CCF * NSS Open Lap Prostatectomy Open Lap Cystectomy Open Lap * indicates till November 30, 2002.
45 Open Adrenalectomy Open Nephrectomy Lap Adrenalectomy Lap Nephrectomy ` Open NU Lap NU Open LDN Lap LDN
46 Open RP Lap RP Open NSS Lap NSS Open RC Lap RC
47 CURRENT STATUS OF LAP. S. IN CCF Feasible Viable alternate Tx of choice Lap. Ad + Lap. RN, NU + Lap DNx + Lap PNx +? Lap RP +? Lap RC +?
48 Chi Mei Experience in Laparoscopic Urology 1997 ~ 2000: Developing Stage Lap. Adrenalectomy & Simple nephrectomy 2000 ~ 2002: Introduction of Hand Assisted Laparoscopic Surgery 2002 ~ present: The era of pure laparoscopy for all advanced procedures
49 Tiers of Laparoscopic Urology Where are we now?? st Tier Diagnostic laparoscopy UDT Renal cyst 2nd Tier Adrenalectomy Simple Nx Radical Nx,, NU+BCE, Live DNx Pyeloplasty 3rd Tier Ileal ureter Partial Nx Radical prostatectomy Radical cystectomy with ileal conduit, continent pouch, neobladder
50 I. Laparoscopic Adrenalectomy 20 th Consensus (Bangkok, 2000) in World Congress of Endourology and th World Congress of Endourology and Shockwave Lithotripsy Laparoscopic Adrenalectomy is the Treatment of Choice for Benign Adrenal Tumor.

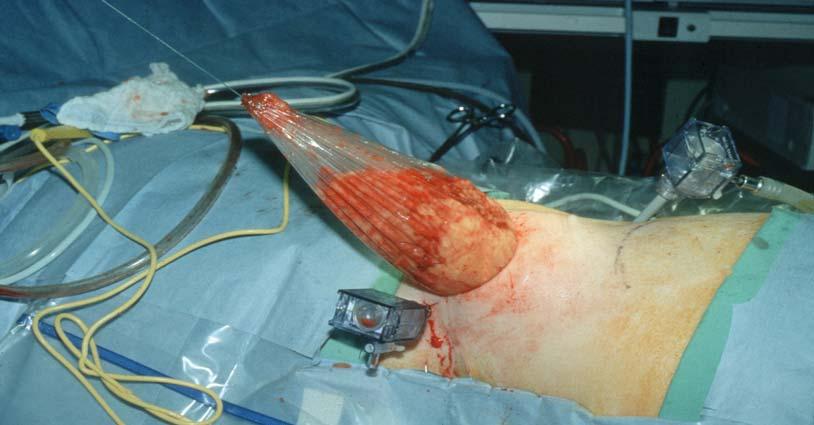
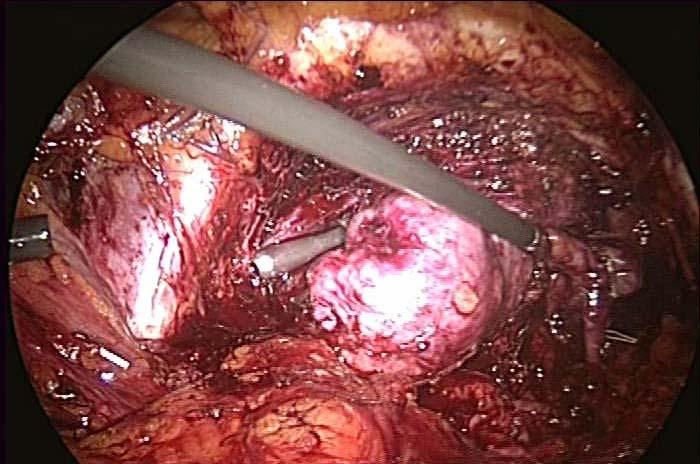
51 Adrenal Corticocarcinoma Laparoscopic Right Adrenalectomy Tumor Rt Kidney


52 Adrenal Corticocarcinoma Laparoscopic Adrenalectomy Surgical Time 5.5 hrs. Adrenal Size - 16 cm Specimen Wt 560 gm Blood Loss cc Postop Hospital Stay 3 days


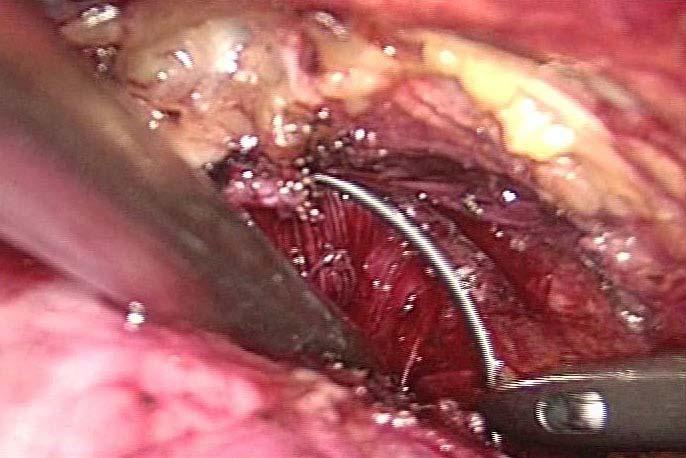
53 Port Configuration & Postop View
54 Laparoscopic Adrenalectomy Indications Yesterday Conn s adenoma Cushing s s adenoma Non-function Adenoma >4 cm Today Pheochromocytoma Adrenal Ca - if no infiltration Solitary metastasis
55 Laparoscopic Adrenalectomy Contraindications Yesterday Adrenal Size > cm Pheochromocytoma Adrenal Cancer Prior Surgery Coagulopathy Poor anesthetic risk Today Large infiltrating adrenal cancer Unacceptable anesthetic risk Coagulopathy Tumor size??
56 II. From Hand-Assistance to Pure Laparoscopic Nephrectomy Myth or Reality? - hand-assisted assisted laparoscopy decreases operative time?? J Urol, 167: , June 2002 TM Complications related to hand-port TM BJU Int., 90(4): 364-7, Sept 2002
57 Comparison of Purely versus Hand Assisted Laparoscopic Radical Nephrectomy for Renal Cell Carcinoma -Chi Mei Medical Center Experience Annual Meeting of Taiwan Surgical Association March 2004
58 Comparison of Pure Laparoscopic versus Hand-Assisted Laparoscopic Nephroureterectomy and Bladder Cuff Excision for Upper Tract Transitional Cell Carcinoma Chi Mei Medical Center Experience 14 th Annual Meeting, Taiwan Urological Association, August 2004


59 Ergonomic
60 Results (I) Group 1 (pure) Group 2 (hand) No. patients p value Mean operative time (mins.) 231 ± ± Mean blood loss (ml.) 166 ± ± 251 <0.05 Mean blood transfusion (units of PRBC) Mean specimen wt. (gm.) Duration of Foley indwelling (days) 0.25 ± ± 1.3 < ± ± 67 < ± ±
61 Mean analgesics (mg. morphine sulfate) Mean days of oral intake (days) Mean days of hospital stay (days) Cost Wound for specimen Results (II) Group 1 (pure) Group 2 (hand) p value 16.6 ± ± 42 < ± ± ± ± 2.7 <0.05 Hand- port TM (-) Flexible* Hand-port TM (+) Fixed Complication (%) 1/16 (6%) 1/16 (6%) *Gibson, Pfannenstiel incision, old scar, vaginal extraction
62 Discussions Purely Hand assisted Technique Ergonomic Wound complication Cost Cosmetic
 However, HAL is still essential for neophyte laparoscopists to go through the")
63 Conclusion Purely laparoscopic Nx and NxUx as efficacious as HAL in experienced hand offer the advantages flexible choice of wound for specimen extraction ergonomic less cost (without hand-port TM relatively earlier recovery TM ) However, HAL is still essential for neophyte laparoscopists to go through the learning curve
64 Laparoscopic Radical Nephroureterectomy with Concomitant Radical Cystectomy for Multi-focal Transitional Cell Carcinoma in Uremic Patients Annual Meeting, 19 th Taiwan Surgical Association, March 2005
65 Drawbacks of traditional open surgery in uremic patients Extremely long incision Increased morbidity Difficulty in postoperative care Prolong postoperative recovery
66 Case 1 64 y/o, male ESRD under hemodialysis Left ureteral TCC (T1) s/p laparoscopic NxUx + BCx for 3 years (retroperitoneal hand-assisted) assisted) Recurrent bladder TCC (high grade, T2a) s/p TUR-BT Suspicious right renal tumor


67 Laparoscopic left NxUx + radical cystoprostatectomy Operation time: 260 min Estimated blood loss: 200 ml Post-OP hospital stay: 3 days


68 Laparoscopic left NxUx + radical cystoprostatectomy
69 Case 2 64 y/o, male Hemodialysis for 5 years PSVT s/p RF ablation, ASA III Left ureter TCC (T3) s/p laparoscopic NxUx + BCx for 0.5 years (pure trnasperitoneal) Reccrrent bladder TCC s/p TUR-BT (grade II, T1)
70 Dx: Reccrrent TCC of right ureter and urinary bladder Laparoscopic right NxUx + radical cystoprostatectomy Operation time: 300 min Estimated blood loss: 300 ml Post-OP hospital stay: 6 days

")
71 Transitional cell carcinoma, right ureter (T3) Transitional cell carcinoma, urinary bladder (T2)

72 Vaginal Delivery of Specimen
73 Conclusion Laparoscopic nephroureterectomy and concomitant radical cystectomy is a minimally alternate for multifocal TCC in uremic patients.


74 Laparoscopic Radical Prostatectomy - Initial Experience Annual Meeting, 19th Taiwan Surgical Association, March 2005
75 Rationale of LRP Introduction Minimally Invasiveness under laparoscopic magnification Equivalent oncological control, urine continence and sexual function preservation Pioneering LRP 1997 Schuessler: : 9 pt; 9.4 hrs; 3 complications 1997 Raboy: : 1 case report of Retroperitoneal RP 1999 Guillonneau and Abbou: : the first 2 largest series with promising results
76 Material and Methods From March 2004 to January 2005 Total 12 patients who were diagnosed as clinically localized prostate cancer underwent transperitoneal LRP The preoperative demographic data and the postoperative outcomes and functional results (continence and sexual function) were analyzed.
77 Operative data Mean OP time: 418 mins ( ) Mean estimated blood loss: 204 cc ( cc) Blood transfusion: Nil Neurovascular bundle preservation: 8 pts Rt: : 3 Lt: 3 Bil: : 2 Bilateral pelvic node dissection: 2 due to high PSA (13.57 and 15.3 ng/ml) Conversion to open surgery: Nil
78 Results Oncological control: Organ confined : 11, Extracapsular extension with negative surgical margin: 1 Serum PSA all fell below 0.2 ng/ml Continence: no one need pad protection Sexual preservation: 5 (70%) regained erection 3 (43%) achieved satisfactory vaginal penetration
 with intravesical protrusion Provide LRP or not?")
79 Ultimate Challenge?? 69 y/o male. PSA: 18 ng/ml ct1c Huge prostate gland (165 gm) with intravesical protrusion Provide LRP or not?? Annual Meeting, 19th Taiwan Surgical Association, March 2005


80 Critical Procedures
81 Conclusion Our preliminary results suggest LRP can be performed safely and effectively. Is LRP easier than Open RP due to laparoscopic magnification after learning curve? We believe that LRP will hold promising in Taiwan in the near future.
82 What Can NOT Be Done Laparoscopically In 2005? 1st Tier Diagnostic laparoscopy UDT Renal cyst 2nd Tier Adrenalectomy Simple, Radical Nx,, NU+BCE, Live DNx Pyeloplasty 3rd Tier Ileal ureter Augmentation cystoplasty Partial Nx Radical prostatectomy Radical cystectomy with ileal conduit, continent pouch, or neobladder Medical contraindication Severe intraabdominal adhesion (No working space) Bulky tumor with local or node infiltration Tumor size??
83 MY TALK TODAY IS Minimal Invasiveness in Urological Surgery Endoluminal & Percutaneous & Extraluminal (Laparoscopy) Real Impact of Laparoscopic Surgery on Urology Be the standard of care? The Realm of Laparoscopic S. Practice patterns in CCF Chi-Mei Experience The Future? Miniaturization Robotic surgery & Telesurgery Endoluminal reconstruction


84 MINIATURIATION NEEDLESCOPIC

 Needlescopic Adrenalectomy ( 2 wks")
85 Mini Minimal Invasiveness Needlescopic vs. Conventional Laparoscopy Traditional Laparoscopic Adrenalectomy ( 6 mos post-op ) Needlescopic Adrenalectomy ( 2 wks post-op )




86 ROBOTICS (Beyond the Quality of Hand-Made)
87 ROBOTICS (Beyond the Quality of Hand- Made) DaVinci and Zeus Six degrees of freedom human wrist Filters hand tremor 1:5 motion scaling Full wrist action 12 X magnification True 3D viewing
88 ROBOTIC PYELOPLASTY: Mayo Clinic Experience: IS IT BETTER? Std. Lap. Robotic Patients 4 4 O.R. time (hrs) Suturing time (hrs) Hosp. Stay (d) 4 4 No long term follow-up data provided. Gettman M. et al: Eur. Urol 42:453,2002



89 From Lab to Clinical More Investigations Endoluminal plastic technique (e.g. endopyeloplasty) (e.g. endoluminal ureteroplasty)
90 Fire Continues between Lap. S and Open S. The easier open procedures have obviously been overtaken by MIS The remainings for open S. are the disease with extensive adhesion, complicated reconstruction, huge tumor Open Surgery Laparoscopic S. Endourol. S. Continue to raise the bar? Nerve-sparing radical cystectomy with orthotopic bladder substitute



91 Many Thanks to the invitation to share my idea my teachers all the patients who trust me


92 THANKS FOR YOUR ATTENTION!! Victor Chia-Hsiang Lin
da Vinci Prostatectomy My Greek personal experience
 da Vinci Prostatectomy My Greek personal experience Vassilis Poulakis MD, PhD, FEBU Ass. Prof. of Urology Director of Urologic Clinic Doctors Hospital Athens Laparoscopy - golden standard in Urology -
da Vinci Prostatectomy My Greek personal experience Vassilis Poulakis MD, PhD, FEBU Ass. Prof. of Urology Director of Urologic Clinic Doctors Hospital Athens Laparoscopy - golden standard in Urology -
Laparoscopic Surgery. The Da Vinci Robot. Limits of Laparoscopy. What Robotics Offers. Robotic Urologic Surgery: A New Era in Patient Care
 Laparoscopic Surgery Robotic Urologic Surgery: A New Era in Patient Care Laparoscopic technique was introduced in urologic surgery in the 1990s Benefits: Improved recovery time, decreased morbidity Matthew
Laparoscopic Surgery Robotic Urologic Surgery: A New Era in Patient Care Laparoscopic technique was introduced in urologic surgery in the 1990s Benefits: Improved recovery time, decreased morbidity Matthew
Minimally invasive surgery in urology oncology. Dr. Tongchai Nakamont 23 Jan 2014
 Minimally invasive surgery in urology oncology Dr. Tongchai Nakamont 23 Jan 2014 Urology oncology Renal cell carcinoma ( RCC) Transitional cell carcinoma (TCC) Kidney Ureter Bladder Prostate cancer Urological
Minimally invasive surgery in urology oncology Dr. Tongchai Nakamont 23 Jan 2014 Urology oncology Renal cell carcinoma ( RCC) Transitional cell carcinoma (TCC) Kidney Ureter Bladder Prostate cancer Urological
da Vinci Prostatectomy
 da Vinci Prostatectomy Justin T. Lee MD Director of Robotic Surgery Urology Associates of North Texas (UANT) USMD Prostate Cancer Center (www.usmdpcc.com) Prostate Cancer Facts Prostate cancer Leading
da Vinci Prostatectomy Justin T. Lee MD Director of Robotic Surgery Urology Associates of North Texas (UANT) USMD Prostate Cancer Center (www.usmdpcc.com) Prostate Cancer Facts Prostate cancer Leading
Who are Candidates for Laparoscopic or Open Radical Nephrectomy. Arieh Shalhav
 Who are Candidates for Laparoscopic or Open Radical Nephrectomy Arieh Shalhav Fritz Duda Chair of Urologic Surgery Professor of Surgery and the Comprehensive Cancer Research Center Who are Candidates for
Who are Candidates for Laparoscopic or Open Radical Nephrectomy Arieh Shalhav Fritz Duda Chair of Urologic Surgery Professor of Surgery and the Comprehensive Cancer Research Center Who are Candidates for
Arieh L. Shalhav Is There a Risk in Robotic Nephroureterectomy?
 Arieh L. Shalhav Is There a Risk in Robotic Nephroureterectomy? 80 patients LNU (n = 40) or ONU (n = 40) CSS (p = 0.2), BRFS (p = 0.86), MFS (p = 0.12) similar for the entire cohort Subgroups of pt3 UTUC
Arieh L. Shalhav Is There a Risk in Robotic Nephroureterectomy? 80 patients LNU (n = 40) or ONU (n = 40) CSS (p = 0.2), BRFS (p = 0.86), MFS (p = 0.12) similar for the entire cohort Subgroups of pt3 UTUC
Index. Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type. A Adenocarcinoma, pancreatic ductal, laparoscopic distal pancreatectomy for, 61 Adrenal cortical carcinoma, laparoscopic adrenalectomy for, 114
Note: Page numbers of article titles are in boldface type. A Adenocarcinoma, pancreatic ductal, laparoscopic distal pancreatectomy for, 61 Adrenal cortical carcinoma, laparoscopic adrenalectomy for, 114
Open Prostatectomy is Best
 Open Prostatectomy is Best William J. Catalona, M.D. The Trifecta Trifecta Cure Continence Potency Northwestern University Feinberg School of Medicine Eastham, J et al, JUrol 179:2207 Continence (Pad Free
Open Prostatectomy is Best William J. Catalona, M.D. The Trifecta Trifecta Cure Continence Potency Northwestern University Feinberg School of Medicine Eastham, J et al, JUrol 179:2207 Continence (Pad Free
The Correction of Common Coding Problems in Urology
 2012 AAPC National Conference Las Vegas, Nevada April 1-4, 2012 Michael A. Ferragamo MD, FACS Clinical Assistant Professor of Urology State University of New York Stony Brook, Long Island, New York Editor:
2012 AAPC National Conference Las Vegas, Nevada April 1-4, 2012 Michael A. Ferragamo MD, FACS Clinical Assistant Professor of Urology State University of New York Stony Brook, Long Island, New York Editor:
Robot-Assisted Gynecologic Surgery. Gynecologic Surgery
 Robot-Assisted Gynecologic Surgery Alison F. Jacoby, MD Department of Obstetrics, Gynecology and Reproductive Sciences University of California, San Francisco Robot-Assisted Gynecologic Surgery Clinical
Robot-Assisted Gynecologic Surgery Alison F. Jacoby, MD Department of Obstetrics, Gynecology and Reproductive Sciences University of California, San Francisco Robot-Assisted Gynecologic Surgery Clinical
From laparoscopic to robo.c surgical urology 2 years of experience
 From laparoscopic to robo.c surgical urology 2 years of experience Ass. Professor V. Poulakis MD, PhD, FEBU Director of Urological Clinic Athens Medical Center Doctors Hospital Athens Laparoscopy golden
From laparoscopic to robo.c surgical urology 2 years of experience Ass. Professor V. Poulakis MD, PhD, FEBU Director of Urological Clinic Athens Medical Center Doctors Hospital Athens Laparoscopy golden
MUSCLE - INVASIVE AND METASTATIC BLADDER CANCER
 10 MUSCLE - INVASIVE AND METASTATIC BLADDER CANCER Recommendations from the EAU Working Party on Muscle Invasive and Metastatic Bladder Cancer G. Jakse (chairman), F. Algaba, S. Fossa, A. Stenzl, C. Sternberg
10 MUSCLE - INVASIVE AND METASTATIC BLADDER CANCER Recommendations from the EAU Working Party on Muscle Invasive and Metastatic Bladder Cancer G. Jakse (chairman), F. Algaba, S. Fossa, A. Stenzl, C. Sternberg
When to Integrate Surgery for Metatstatic Urothelial Cancers
 When to Integrate Surgery for Metatstatic Urothelial Cancers Wade J. Sexton, M.D. Senior Member and Professor Department of Genitourinary Oncology Moffitt Cancer Center Case Presentation #1 67 yo male
When to Integrate Surgery for Metatstatic Urothelial Cancers Wade J. Sexton, M.D. Senior Member and Professor Department of Genitourinary Oncology Moffitt Cancer Center Case Presentation #1 67 yo male
Robotic Surgery for Prostate Cancer: A Realistic Approach to Getting Started The Evolution of a Robotic Surgeon
 Robotic Surgery for Prostate Cancer: A Realistic Approach to Getting Started The Evolution of a Robotic Surgeon Douglas S. Scherr, M.D. Clinical Director, Urologic Oncology Weill Medical College of Cornell
Robotic Surgery for Prostate Cancer: A Realistic Approach to Getting Started The Evolution of a Robotic Surgeon Douglas S. Scherr, M.D. Clinical Director, Urologic Oncology Weill Medical College of Cornell
Department of Urology, Cochin hospital Paris Descartes University
 Technical advances in the treatment of localized prostate cancer Pr Michaël Peyromaure Department of Urology, Cochin hospital Paris Descartes University Introduction Curative treatments of localized prostate
Technical advances in the treatment of localized prostate cancer Pr Michaël Peyromaure Department of Urology, Cochin hospital Paris Descartes University Introduction Curative treatments of localized prostate
Laparoscopic Nephrectomy: New Standard of Care?
 Original Article Laparoscopic Nephrectomy: New Standard of Care? Hong Gee Sim, Sidney K.H. Yip, Chee Yong Ng, Yee Sze Teo, Yeh Hong Tan, Woei Yun Siow and Wai Sam Cheng, Department of Urology, Singapore
Original Article Laparoscopic Nephrectomy: New Standard of Care? Hong Gee Sim, Sidney K.H. Yip, Chee Yong Ng, Yee Sze Teo, Yeh Hong Tan, Woei Yun Siow and Wai Sam Cheng, Department of Urology, Singapore
Robotic Surgery for Upper Tract Urothelial Carcinoma. Li-Ming Su, MD
 Robotic Surgery for Upper Tract Urothelial Carcinoma Li-Ming Su, MD David A. Cofrin Professor of Urology, Associate Chairman of Clinical Affairs, Chief, Division of Robotic and Minimally Invasive Urologic
Robotic Surgery for Upper Tract Urothelial Carcinoma Li-Ming Su, MD David A. Cofrin Professor of Urology, Associate Chairman of Clinical Affairs, Chief, Division of Robotic and Minimally Invasive Urologic
Laparoscopic Radical Nephrectomy- the current gold standard
 Laparoscopic Radical Nephrectomy- the current gold standard Anoop M. Meraney, M.D Director, Urologic Oncology, Helen and Harry Gray Cancer Center, Hartford Hospital and Connecticut Surgical Group. Is it
Laparoscopic Radical Nephrectomy- the current gold standard Anoop M. Meraney, M.D Director, Urologic Oncology, Helen and Harry Gray Cancer Center, Hartford Hospital and Connecticut Surgical Group. Is it
LAPAROSCOPIC RADICAL NEPHRECTOMY FOR LARGE (GREATER THAN 7 CM, T2) RENAL TUMORS
 RENAL TUMORS") 0022-5347/04/1726-2172/0 Vol. 172, 2172 2176, December 2004 THE JOURNAL OF UROLOGY Printed in U.S.A. Copyright 2004 by AMERICAN UROLOGICAL ASSOCIATION DOI: 10.1097/01.ju.0000140961.53335.04 LAPAROSCOPIC
0022-5347/04/1726-2172/0 Vol. 172, 2172 2176, December 2004 THE JOURNAL OF UROLOGY Printed in U.S.A. Copyright 2004 by AMERICAN UROLOGICAL ASSOCIATION DOI: 10.1097/01.ju.0000140961.53335.04 LAPAROSCOPIC
Attachment #2 Overview of Follow-up
 Attachment #2 Overview of Follow-up Provided below is a general overview of follow-up and this may vary based on specific patient or cancer characteristics. Of note, Labs and imaging can be performed closer
Attachment #2 Overview of Follow-up Provided below is a general overview of follow-up and this may vary based on specific patient or cancer characteristics. Of note, Labs and imaging can be performed closer
Ureteroscopy Is Indicated in every patient with suspected Upper Tract Urothelial Tumor
 Ureteroscopy Is Indicated in every patient with suspected Upper Tract Urothelial Tumor Scott G. Hubosky, MD The Demetrius H. Bagley Jr., MD Associate Professor of Urology Director of Endourology Vice Chair
Ureteroscopy Is Indicated in every patient with suspected Upper Tract Urothelial Tumor Scott G. Hubosky, MD The Demetrius H. Bagley Jr., MD Associate Professor of Urology Director of Endourology Vice Chair
Atlas of Urologic Surgery
 Atlas of Urologic Surgery Hinman, F ISBN-13: 9781416042105 Table of Contents Section I: Surgical Basics Chapter 1 Surgical Basics Section II: The Urologist at Work Chapter 2 Basic Surgical Techniques Chapter
Atlas of Urologic Surgery Hinman, F ISBN-13: 9781416042105 Table of Contents Section I: Surgical Basics Chapter 1 Surgical Basics Section II: The Urologist at Work Chapter 2 Basic Surgical Techniques Chapter
Pioneering Robotic-Assisted Laparoscopic Prostatectomy in The Pretoria Urology Hospital and the South African urological environment:
 Pioneering Robotic-Assisted Laparoscopic Prostatectomy in The Pretoria Urology Hospital and the South African urological environment: Dr. Lance Coetzee Pretoria Urology Hospital SOUTH AFRICA Minimum of
Pioneering Robotic-Assisted Laparoscopic Prostatectomy in The Pretoria Urology Hospital and the South African urological environment: Dr. Lance Coetzee Pretoria Urology Hospital SOUTH AFRICA Minimum of
Index. Surg Oncol Clin N Am 14 (2005) Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type.") Surg Oncol Clin N Am 14 (2005) 433 439 Index Note: Page numbers of article titles are in boldface type. A Abdominosacral resection, of recurrent rectal cancer, 202 215 Ablative techniques, image-guided,
Surg Oncol Clin N Am 14 (2005) 433 439 Index Note: Page numbers of article titles are in boldface type. A Abdominosacral resection, of recurrent rectal cancer, 202 215 Ablative techniques, image-guided,
Q&A. Fabulous Prizes. Collecting Cancer Data: Bladder, Renal Pelvis, and Ureter 5/2/13. NAACCR Webinar Series
 Collecting Cancer Data Bladder & Renal Pelvis NAACCR 2012 2013 Webinar Series Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching
Collecting Cancer Data Bladder & Renal Pelvis NAACCR 2012 2013 Webinar Series Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching
Mini-Invasive Treatment in Urological Diseases Dott. Alberto Saita Responsabile Endourologia Istituto Clinico Humanitas - Rozzano
 Dipartimento di Urologia Direttore Prof. Giorgio Guazzoni Mini-Invasive Treatment in Urological Diseases Dott. Alberto Saita Responsabile Endourologia Istituto Clinico Humanitas - Rozzano alberto.saita@humanitas.it
Dipartimento di Urologia Direttore Prof. Giorgio Guazzoni Mini-Invasive Treatment in Urological Diseases Dott. Alberto Saita Responsabile Endourologia Istituto Clinico Humanitas - Rozzano alberto.saita@humanitas.it
Morbidity Audit and Logbook Tool SNOMED Board Reporting Terms for SET and IMG Urology ENDOSCOPIC LOWER URINARY TRACT
 ENDOSCOPIC LOWER URINARY TRACT Cystolitholapaxy Cystoscopic removal of foreign body from bladder Cystoscopic removal of ureteric stent Cystoscopy and cystodiathermy Cystoscopy and transurethral biopsy
ENDOSCOPIC LOWER URINARY TRACT Cystolitholapaxy Cystoscopic removal of foreign body from bladder Cystoscopic removal of ureteric stent Cystoscopy and cystodiathermy Cystoscopy and transurethral biopsy
Role of surgery. Theo M. de Reijke MD PhD FEBU Department of Urology Academic Medical Center Amsterdam
 Role of surgery Theo M. de Reijke MD PhD FEBU Department of Urology Academic Medical Center Amsterdam Surgery and alternative treatments Radical prostatectomy Open Laparoscopic Robot-assisted Temperature
Role of surgery Theo M. de Reijke MD PhD FEBU Department of Urology Academic Medical Center Amsterdam Surgery and alternative treatments Radical prostatectomy Open Laparoscopic Robot-assisted Temperature
M E M O R A N D U M. RE: Resident Surgical Index Case List Redefined For 2009: Recommended Minimum Numbers and Core Domains Emphasized
 M E M O R A N D U M TO: FROM: Urology Program Directors Louise King Executive Director, Residency Review Committee for Urology 312.755.5498 lking@acgme.org Members, Review Committee for Urology DATE: February
M E M O R A N D U M TO: FROM: Urology Program Directors Louise King Executive Director, Residency Review Committee for Urology 312.755.5498 lking@acgme.org Members, Review Committee for Urology DATE: February
Bladder replacement in men and women: when and when not? Outline. Continent Diversion History
 1 Bladder replacement in men and women: when and when not? Eila C. Skinner, MD Professor of Clinical Urology Keck USC School of Medicine Outline 1) Selection criteria for orthotopic diversion: Tumor-related
1 Bladder replacement in men and women: when and when not? Eila C. Skinner, MD Professor of Clinical Urology Keck USC School of Medicine Outline 1) Selection criteria for orthotopic diversion: Tumor-related
MUSCLE-INVASIVE AND METASTATIC BLADDER CANCER
 MUSCLE-INVASIVE AND METASTATIC BLADDER CANCER (Text update March 2008) A. Stenzl (chairman), N.C. Cowan, M. De Santis, G. Jakse, M. Kuczyk, A.S. Merseburger, M.J. Ribal, A. Sherif, J.A. Witjes Introduction
MUSCLE-INVASIVE AND METASTATIC BLADDER CANCER (Text update March 2008) A. Stenzl (chairman), N.C. Cowan, M. De Santis, G. Jakse, M. Kuczyk, A.S. Merseburger, M.J. Ribal, A. Sherif, J.A. Witjes Introduction
ROBOTIC VS OPEN RADICAL CYSTECTOMY
 ROBOTIC VS OPEN RADICAL CYSTECTOMY A REVIEW Colin Lundeen December 14, 2016 Objectives Review the history of radical cystectomy Critically analyze recent RCTs comparing open radical cystectomy (ORC) to
ROBOTIC VS OPEN RADICAL CYSTECTOMY A REVIEW Colin Lundeen December 14, 2016 Objectives Review the history of radical cystectomy Critically analyze recent RCTs comparing open radical cystectomy (ORC) to
Complications in robotic surgery!! Review of the literature! RALP, RAPN and RARC!
 Complications in robotic surgery Review of the literature RALP, RAPN and RARC Anna Wallerstedt, MD Karolinska University Hospital Stockholm, Sweden Agenda The importance of reporting surgical complications
Complications in robotic surgery Review of the literature RALP, RAPN and RARC Anna Wallerstedt, MD Karolinska University Hospital Stockholm, Sweden Agenda The importance of reporting surgical complications
PREFACE... V. CONTRIBUTORS... xiii. 1. SURGICAL INCISIONS... 3 J. Stephen Jones
 Contents PREFACE... V CONTRIBUTORS... xiii PART I: THE KIDNEY AND ADRENAL 1. SURGICAL INCISIONS... 3 2. ADRENAL DISEASE: OPEN SURGERY... 17 3. LAPAROSCOPIC ADRENALECTOMY... 23 Mihir M. Desai and Inderbir
Contents PREFACE... V CONTRIBUTORS... xiii PART I: THE KIDNEY AND ADRENAL 1. SURGICAL INCISIONS... 3 2. ADRENAL DISEASE: OPEN SURGERY... 17 3. LAPAROSCOPIC ADRENALECTOMY... 23 Mihir M. Desai and Inderbir
Recovery of sexual function after radical cystectomy with orthotopic neobladder
 Recovery of sexual function after radical cystectomy with orthotopic neobladder C. Gingu, V. Olaru, A. Dick, C. Baston, M. Crăsneanu, C. Surcel, S. Voinea, Liliana Domnişor, I. Sinescu Center of Urological
Recovery of sexual function after radical cystectomy with orthotopic neobladder C. Gingu, V. Olaru, A. Dick, C. Baston, M. Crăsneanu, C. Surcel, S. Voinea, Liliana Domnişor, I. Sinescu Center of Urological
LOGBOOK EBU ORAL EXAM 2015
 LOGBOOK EBU ORAL EXAM 2015 Surname First Name Date of Birth (daymonthyear) MEDICAL DEGREE (MD) UROLOGIST TRAINING: - Training in urology - Training in surgery (as part of the urology training) - Other
LOGBOOK EBU ORAL EXAM 2015 Surname First Name Date of Birth (daymonthyear) MEDICAL DEGREE (MD) UROLOGIST TRAINING: - Training in urology - Training in surgery (as part of the urology training) - Other
LAPAROSCOPIC RADICAL PROSTATECTOMY IN THE ERA OF ROBOT-ASSISTED TECHNOLOGY
 LAPAROSCOPIC RADICAL PROSTATECTOMY IN THE ERA OF ROBOT-ASSISTED TECHNOLOGY *Iason Kyriazis, 1 Marinos Vasilas, 1 Panagiotis Kallidonis, 2 Vasilis Panagopoulos, 1 Evangelos Liatsikos 3 1. Resident in Urology,
LAPAROSCOPIC RADICAL PROSTATECTOMY IN THE ERA OF ROBOT-ASSISTED TECHNOLOGY *Iason Kyriazis, 1 Marinos Vasilas, 1 Panagiotis Kallidonis, 2 Vasilis Panagopoulos, 1 Evangelos Liatsikos 3 1. Resident in Urology,
RAPN. in T1b Renal Masses? A. Mottrie. G. Denaeyer, P. Schatteman, G. Novara
 RAPN in T1b Renal Masses? A. Mottrie G. Denaeyer, P. Schatteman, G. Novara Department of Urology O.L.V. Clinic Aalst OLV Vattikuti Robotic Surgery Institute Aalst Belgium Guidelines on Renal Cell Carcinoma
RAPN in T1b Renal Masses? A. Mottrie G. Denaeyer, P. Schatteman, G. Novara Department of Urology O.L.V. Clinic Aalst OLV Vattikuti Robotic Surgery Institute Aalst Belgium Guidelines on Renal Cell Carcinoma
THE LATEST STEP FORWARD IN SURGERY. LESS Laparo-Endoscopic Single-Site Surgery
 THE LATEST STEP FORWARD IN SURGERY LESS Laparo-Endoscopic Single-Site Surgery THE ROUTE FROM OPEN SURGERY TO MINIMALLY INVASIVE SURGERY An operation is generally a radical experience for any patient. In
THE LATEST STEP FORWARD IN SURGERY LESS Laparo-Endoscopic Single-Site Surgery THE ROUTE FROM OPEN SURGERY TO MINIMALLY INVASIVE SURGERY An operation is generally a radical experience for any patient. In
Open RRP versus LRP in Asian Men. International Braz J Urol Vol. 35 (2): , March - April, 2009
: , March - April, 2009") Clinical Urology Open RRP versus LRP in Asian Men International Braz J Urol Vol. 35 (2): 151-157, March - April, 2009 Perioperative Outcomes of Open Radical Prostatectomy versus Laparoscopic Radical Prostatectomy
Clinical Urology Open RRP versus LRP in Asian Men International Braz J Urol Vol. 35 (2): 151-157, March - April, 2009 Perioperative Outcomes of Open Radical Prostatectomy versus Laparoscopic Radical Prostatectomy
Attachment #2 Overview of Follow-up
 Attachment #2 Overview of Follow-up Provided below is a general overview of follow-up and this may vary based on specific patient or cancer characteristics. Of note, Labs and imaging can be performed closer
Attachment #2 Overview of Follow-up Provided below is a general overview of follow-up and this may vary based on specific patient or cancer characteristics. Of note, Labs and imaging can be performed closer
Robotic assisted laparoscopic radical cystectomy for bladder carcinoma: early experience and oncologic outcomes
 Formosan Journal of Surgery (2012) 45, 178e182 Available online at www.sciencedirect.com journal homepage: www.e-fjs.com ORIGINAL ARTICLE Robotic assisted laparoscopic radical cystectomy for bladder carcinoma:
Formosan Journal of Surgery (2012) 45, 178e182 Available online at www.sciencedirect.com journal homepage: www.e-fjs.com ORIGINAL ARTICLE Robotic assisted laparoscopic radical cystectomy for bladder carcinoma:
ENDOSCOPIC URETERECTOMY DURING NEPHROURETERECTOMY FOR UPPER URINARY TRACT TRANSITIONAL CELL CARCINOMA
 ENDOSCOPIC URETERECTOMY DURING NEPHROURETERECTOMY FOR UPPER URINARY TRACT TRANSITIONAL CELL CARCINOMA Il. Saltirov, Ts. Petkov, G. Georgiev, K.Petkova Department of Urology and Nephrology, Military Medical
ENDOSCOPIC URETERECTOMY DURING NEPHROURETERECTOMY FOR UPPER URINARY TRACT TRANSITIONAL CELL CARCINOMA Il. Saltirov, Ts. Petkov, G. Georgiev, K.Petkova Department of Urology and Nephrology, Military Medical
Urological Tumours 1 Kidney tumours 2 Bladder tumours
 Urological Tumours 1 Kidney tumours 2 Bladder tumours Tim Bracey SpR Histopathology Derriford Hospital Kidney tumours What are we going to talk about?! Anatomy of urinary tract! Types of kidney tumours!
Urological Tumours 1 Kidney tumours 2 Bladder tumours Tim Bracey SpR Histopathology Derriford Hospital Kidney tumours What are we going to talk about?! Anatomy of urinary tract! Types of kidney tumours!
Long-Term Oncologic Outcome after Laparoscopic Radical Nephroureterectomy for Upper Tract Transitional Cell Carcinoma
 european urology 51 (2007) 1639 1644 available at www.sciencedirect.com journal homepage: www.europeanurology.com Laparoscopy Long-Term Oncologic Outcome after Laparoscopic Radical Nephroureterectomy for
european urology 51 (2007) 1639 1644 available at www.sciencedirect.com journal homepage: www.europeanurology.com Laparoscopy Long-Term Oncologic Outcome after Laparoscopic Radical Nephroureterectomy for
RADICAL CYSTECTOMY. Solutions for minimally invasive urologic surgery
 RADICAL CYSTECTOMY Solutions for minimally invasive urologic surgery The da Vinci Surgical System High-definition 3D vision EndoWrist instrumentation 3D HD Vision 3D HD visualization facilitates accurate
RADICAL CYSTECTOMY Solutions for minimally invasive urologic surgery The da Vinci Surgical System High-definition 3D vision EndoWrist instrumentation 3D HD Vision 3D HD visualization facilitates accurate
Male genital tract tumors. SiCA. Division of Urology, Department of Surgery, Faculty of Medicine Siriraj Hospital.
 Male genital tract tumors Division of Urology, Department of Surgery, Faculty of Medicine Siriraj Hospital. adenocarcinoma Prostate Cancer most common male cancer in western countries more detected in
Male genital tract tumors Division of Urology, Department of Surgery, Faculty of Medicine Siriraj Hospital. adenocarcinoma Prostate Cancer most common male cancer in western countries more detected in
Robotic Technology at the Service of Surgery
 Robotic Technology at the Service of Surgery -The Challenge of Robotic Urology - Vassilis Poulakis MD, PhD, FEBU Ass. Professor of Urology, University of Frankfurt, Germany Director of Urologic Clinic
Robotic Technology at the Service of Surgery -The Challenge of Robotic Urology - Vassilis Poulakis MD, PhD, FEBU Ass. Professor of Urology, University of Frankfurt, Germany Director of Urologic Clinic
Cytoreductive Radical Prostatectomy for de Novo Metastatic Prostate Cancer
 Cytoreductive Radical Prostatectomy for de Novo Metastatic Prostate Cancer Timothy G. Wilson, MD Professor and Chair of Urology John Wayne Cancer Institute Santa Monica, California Disclosures I am on
Cytoreductive Radical Prostatectomy for de Novo Metastatic Prostate Cancer Timothy G. Wilson, MD Professor and Chair of Urology John Wayne Cancer Institute Santa Monica, California Disclosures I am on
RESEARCH ARTICLE. Abstract. Introduction
 DOI:10.31557/APJCP.2018.19.12.3495 Laparoscopic Cysto-Nephro-Ureterectomy RESEARCH ARTICLE Editorial Process: Submission:04/05/2018 Acceptance:11/27/2018 Outcomes and Complications of Simultaneous Laparoscopic
DOI:10.31557/APJCP.2018.19.12.3495 Laparoscopic Cysto-Nephro-Ureterectomy RESEARCH ARTICLE Editorial Process: Submission:04/05/2018 Acceptance:11/27/2018 Outcomes and Complications of Simultaneous Laparoscopic
Transperitoneal Robotic-Assisted Laparoscopic Prostatectomy After Prosthetic Mesh Herniorrhaphy
 SCIENTIFIC PAPER Transperitoneal Robotic-Assisted Laparoscopic Prostatectomy After Prosthetic Mesh Herniorrhaphy Costas D. Lallas, MD, Mark L. Pe, MD, Jitesh V. Patel, MD, Pranav Sharma, Leonard G. Gomella,
SCIENTIFIC PAPER Transperitoneal Robotic-Assisted Laparoscopic Prostatectomy After Prosthetic Mesh Herniorrhaphy Costas D. Lallas, MD, Mark L. Pe, MD, Jitesh V. Patel, MD, Pranav Sharma, Leonard G. Gomella,
Retroperitoneoscopic Transureteroureterostomy with Cutaneous Ureterostomy to Salvage Failed Ileal Conduit Urinary Diversion
 available at www.sciencedirect.com journal homepage: www.europeanurology.com Case Study of the Month Retroperitoneoscopic Transureteroureterostomy with Cutaneous Ureterostomy to Salvage Failed Ileal Conduit
available at www.sciencedirect.com journal homepage: www.europeanurology.com Case Study of the Month Retroperitoneoscopic Transureteroureterostomy with Cutaneous Ureterostomy to Salvage Failed Ileal Conduit
INCIDENTAL PROSTATE CANCER IN PATIENTS UNDERGOING RADICAL CYSTOPROSTATECTOMY FOR BLADDER CANCER
 & INCIDENTAL PROSTATE CANCER IN PATIENTS UNDERGOING RADICAL CYSTOPROSTATECTOMY FOR BLADDER CANCER Mustafa Hiroš *, Hajrudin Spahović, Mirsad Selimović, Sabina Sadović Urology Clinic, University of Sarajevo
& INCIDENTAL PROSTATE CANCER IN PATIENTS UNDERGOING RADICAL CYSTOPROSTATECTOMY FOR BLADDER CANCER Mustafa Hiroš *, Hajrudin Spahović, Mirsad Selimović, Sabina Sadović Urology Clinic, University of Sarajevo
UNM SRMC UROLOGY CLINICAL PRIVILEGES.
 o o o Initial privileges (initial appointment) Renewal of privileges (reappointment) Expansion of privileges (modification) INSTRUCTIONS All new applicants must meet the following requirements as approved
o o o Initial privileges (initial appointment) Renewal of privileges (reappointment) Expansion of privileges (modification) INSTRUCTIONS All new applicants must meet the following requirements as approved
Segmental ureterectomy does not compromise the oncologic outcome compared with nephroureterectomy for pure ureter cancer
 Int Urol Nephrol (2014) 46:921 926 DOI 10.1007/s11255-013-0514-z UROLOGY - ORIGINAL PAPER Segmental ureterectomy does not compromise the oncologic outcome compared with nephroureterectomy for pure ureter
Int Urol Nephrol (2014) 46:921 926 DOI 10.1007/s11255-013-0514-z UROLOGY - ORIGINAL PAPER Segmental ureterectomy does not compromise the oncologic outcome compared with nephroureterectomy for pure ureter
Kaiser Oakland Urology
 Kaiser Oakland Urology What is Laparoscopy? Minimally invasive surgical alternative to standard surgery How is Laparoscopy Performed? A laparoscope and video camera are used to visualize internal organs
Kaiser Oakland Urology What is Laparoscopy? Minimally invasive surgical alternative to standard surgery How is Laparoscopy Performed? A laparoscope and video camera are used to visualize internal organs
Indications For Partial
 Indications For Partial Nephrectomy Christopher G. Wood, M. D., FACS Professor and Deputy Chairman Douglas E. Johnson, M. D. Endowed Professorship in Urology Department of Urology The University of Texas
Indications For Partial Nephrectomy Christopher G. Wood, M. D., FACS Professor and Deputy Chairman Douglas E. Johnson, M. D. Endowed Professorship in Urology Department of Urology The University of Texas
Comparative Analysis Research of Robotic Assisted Laparoscopic Prostatectomy
 Comparative Analysis Research of Robotic Assisted Laparoscopic Prostatectomy By: Jonathan Barlaan; Huy Nguyen Mentor: Julio Powsang, MD Reader: Richard Wilder, MD May 2, 211 Abstract Introduction: The
Comparative Analysis Research of Robotic Assisted Laparoscopic Prostatectomy By: Jonathan Barlaan; Huy Nguyen Mentor: Julio Powsang, MD Reader: Richard Wilder, MD May 2, 211 Abstract Introduction: The
Case Discussions: Prostate Cancer
 Case Discussions: Prostate Cancer Andrew J. Stephenson, MD FRCSC FACS Chief, Urologic Oncology Glickman Urological and Kidney Institute Cleveland Clinic Elevated PSA 1 54 yo, healthy male, family Hx of
Case Discussions: Prostate Cancer Andrew J. Stephenson, MD FRCSC FACS Chief, Urologic Oncology Glickman Urological and Kidney Institute Cleveland Clinic Elevated PSA 1 54 yo, healthy male, family Hx of
Robotic radical prostatectomy Technique and results of nerve sparing approach EAU 2009 March 19 th 2009
 Robotic radical prostatectomy Technique and results of nerve sparing approach EAU 2009 March 19 th 2009 J.H. Witt Department of Urology and Pediatric Urology Prostate Center Northwest St. Antonius-Hospital
Robotic radical prostatectomy Technique and results of nerve sparing approach EAU 2009 March 19 th 2009 J.H. Witt Department of Urology and Pediatric Urology Prostate Center Northwest St. Antonius-Hospital
RESIDENCY TRAINING PROGRAMME IN UROLOGY CERTIFICATION APPLICATION FORM PARTICIPATING INSTITUTE(S)
") Date application Name primary institute RESIDENCY TRAINING PROGRAMME IN UROLOGY CERTIFICATION APPLICATION FORM Name affiliated institute(s) Name Programme Director PARTICIPATING INSTITUTE(S) This form
Date application Name primary institute RESIDENCY TRAINING PROGRAMME IN UROLOGY CERTIFICATION APPLICATION FORM Name affiliated institute(s) Name Programme Director PARTICIPATING INSTITUTE(S) This form
Outcomes. Glickman Urological & Kidney Institute
 Outcomes 28 Glickman Urological & Kidney Institute Prostate Cryotherapy Cryotherapy has recently been used for treatment of prostate cancer as primary treatment and after failure of radiation treatment.
Outcomes 28 Glickman Urological & Kidney Institute Prostate Cryotherapy Cryotherapy has recently been used for treatment of prostate cancer as primary treatment and after failure of radiation treatment.
State-of-the-art: vision on the future. Urology
 State-of-the-art: vision on the future Urology Francesco Montorsi MD FRCS Professor and Chairman Department of Urology San Raffaele Hospital Vita-Salute San Raffaele University Milan, Italy Disclosures
State-of-the-art: vision on the future Urology Francesco Montorsi MD FRCS Professor and Chairman Department of Urology San Raffaele Hospital Vita-Salute San Raffaele University Milan, Italy Disclosures
The 6-month course of the program is mainly dedicated to clinical experience (research time is also provided).
.") Oncology Fellowship The oncology fellowship training course at Yonsei University Health System (Severance Hospital), comprising a 6-month and 1-year format, provides good quality and wide experience in
Oncology Fellowship The oncology fellowship training course at Yonsei University Health System (Severance Hospital), comprising a 6-month and 1-year format, provides good quality and wide experience in
RADICAL CYSTECTOMY. Solutions for minimally invasive urologic surgery
 RADICAL CYSTECTOMY Solutions for minimally invasive urologic surgery The da Vinci Surgical System High-definition 3D vision EndoWrist instrumentation Intuitive motion RADICAL CYSTECTOMY Maintains the oncologic
RADICAL CYSTECTOMY Solutions for minimally invasive urologic surgery The da Vinci Surgical System High-definition 3D vision EndoWrist instrumentation Intuitive motion RADICAL CYSTECTOMY Maintains the oncologic
Urothelial Tumors of the Upper Tract: Diagnosis and Management. Daniel Rapoport April 11, 2007 Urology Grand Rounds
 Urothelial Tumors of the Upper Tract: Diagnosis and Management Daniel Rapoport April 11, 2007 Urology Grand Rounds 1 Overview Background Epidemiology and risk factors Natural history and prognostic factors
Urothelial Tumors of the Upper Tract: Diagnosis and Management Daniel Rapoport April 11, 2007 Urology Grand Rounds 1 Overview Background Epidemiology and risk factors Natural history and prognostic factors
Radical Cystectomy Often Too Late? Yes, But...
 european urology 50 (2006) 1129 1138 available at www.sciencedirect.com journal homepage: www.europeanurology.com Editorial 50th Anniversary Radical Cystectomy Often Too Late? Yes, But... Urs E. Studer
european urology 50 (2006) 1129 1138 available at www.sciencedirect.com journal homepage: www.europeanurology.com Editorial 50th Anniversary Radical Cystectomy Often Too Late? Yes, But... Urs E. Studer
Transition from open to robotic-assisted radical prostatectomy: 7 years experience at Hackensack University Medical Center
 J Robotic Surg (27) 1:155 159 DOI 1.7/s1171-7-23- ORIGINAL ARTICLE Transition from open to robotic-assisted radical prostatectomy: 7 years experience at Hackensack University Medical Center Ravi Munver
J Robotic Surg (27) 1:155 159 DOI 1.7/s1171-7-23- ORIGINAL ARTICLE Transition from open to robotic-assisted radical prostatectomy: 7 years experience at Hackensack University Medical Center Ravi Munver
Clinical Commissioning Policy Proposition: Robotic Assisted Surgery for Bladder Cancer
 Clinical Commissioning Policy Proposition: Robotic Assisted Surgery for Bladder Cancer Reference: NHS England B14X08 Information Reader Box (IRB) to be inserted on inside front cover for documents of 6
Clinical Commissioning Policy Proposition: Robotic Assisted Surgery for Bladder Cancer Reference: NHS England B14X08 Information Reader Box (IRB) to be inserted on inside front cover for documents of 6
Questions & Answers about Sexuality and Intimacy after Bladder Cancer. Part III: Causes and Treatments for Sexual Dysfunction
 Questions & Answers about Sexuality and Intimacy after Bladder Cancer A Valentine's chat with Dr. Trinity Bivalacqua Monday, February 13, 2017 Part III: Causes and Treatments for Sexual Dysfunction Presented
Questions & Answers about Sexuality and Intimacy after Bladder Cancer A Valentine's chat with Dr. Trinity Bivalacqua Monday, February 13, 2017 Part III: Causes and Treatments for Sexual Dysfunction Presented
Retroperitoneal Laparoscopic Radical Nephroureterectomy for High Urothelial Tumours
 Retroperitoneal Laparoscopic Radical Nephroureterectomy for High Urothelial Tumours A. Hașegan 1, V. Pîrvuț 1, I. Mihai 1, N. Grigore 1 1 Lucian Blaga University of Sibiu, Faculty of Medicine Clinical
Retroperitoneal Laparoscopic Radical Nephroureterectomy for High Urothelial Tumours A. Hașegan 1, V. Pîrvuț 1, I. Mihai 1, N. Grigore 1 1 Lucian Blaga University of Sibiu, Faculty of Medicine Clinical
Regions Hospital Delineation of Privileges Urology
 Regions Hospital Delineation of s Urology Applicant s Name: Last First M. Instructions: Place a check-mark where indicated for each core group you are requesting. Review education and basic formal training
Regions Hospital Delineation of s Urology Applicant s Name: Last First M. Instructions: Place a check-mark where indicated for each core group you are requesting. Review education and basic formal training
Partial Nephrectomy Techniques for Renal Preservation: Historical and Modern Approaches
 Partial Nephrectomy Techniques for Renal Preservation: Historical and Modern Approaches Cary N Robertson MD FACS Associate Professor Division of Urology Associate Director Urologic Oncology Duke Cancer
Partial Nephrectomy Techniques for Renal Preservation: Historical and Modern Approaches Cary N Robertson MD FACS Associate Professor Division of Urology Associate Director Urologic Oncology Duke Cancer
Prostate Cancer. David Wilkinson MD Gulfshore Urology
 Prostate Cancer David Wilkinson MD Gulfshore Urology What is the Prostate? Male Sexual Gland Adds nutrients and fluids for sperm This fluid is added to sperm during ejaculation Urethra (urine channel)
Prostate Cancer David Wilkinson MD Gulfshore Urology What is the Prostate? Male Sexual Gland Adds nutrients and fluids for sperm This fluid is added to sperm during ejaculation Urethra (urine channel)
Case Report Left Transperitoneal Adrenalectomy with a Laparoendoscopic Single-Site Surgery Combined Technique: Initial Case Reports
 Volume 2011, Article ID 651380, 4 pages doi:10.1155/2011/651380 Case Report Left Transperitoneal Adrenalectomy with a Laparoendoscopic Single-Site Surgery Combined Technique: Initial Case Reports Yasuhiro
Volume 2011, Article ID 651380, 4 pages doi:10.1155/2011/651380 Case Report Left Transperitoneal Adrenalectomy with a Laparoendoscopic Single-Site Surgery Combined Technique: Initial Case Reports Yasuhiro
Research Article Laparoscopic Pyeloplasty for Ureteropelvic Junctions Obstruction in Adults: 6 Years Experience in One Center
 Hindawi BioMed Research International Volume 2017, Article ID 6743512, 4 pages https://doi.org/10.1155/2017/6743512 Research Article Laparoscopic Pyeloplasty for Ureteropelvic Junctions Obstruction in
Hindawi BioMed Research International Volume 2017, Article ID 6743512, 4 pages https://doi.org/10.1155/2017/6743512 Research Article Laparoscopic Pyeloplasty for Ureteropelvic Junctions Obstruction in
Oncourology COMPLICATIONS OF PARTIAL NEPHRECTOMY AT OPERATIVE TREATMENT OF RENAL CELL CARCINOMA
 1 Oncourology COMPLICATIONS OF PARTIAL NEPHRECTOMY AT OPERATIVE TREATMENT OF RENAL CELL CARCINOMA Address: Eduard Oleksandrovych Stakhovsky, 03022, Kyiv, Lomonosova Str., 33/43, National Cancer Institute
1 Oncourology COMPLICATIONS OF PARTIAL NEPHRECTOMY AT OPERATIVE TREATMENT OF RENAL CELL CARCINOMA Address: Eduard Oleksandrovych Stakhovsky, 03022, Kyiv, Lomonosova Str., 33/43, National Cancer Institute
 A Personal History NIH CWRU U of TN U of Miami Animal Model for Bladder Cancer Carcinogen induced FANFT Three Models Primary tumors individual tumors, simulates clinical scenario of locally advanced cancer
A Personal History NIH CWRU U of TN U of Miami Animal Model for Bladder Cancer Carcinogen induced FANFT Three Models Primary tumors individual tumors, simulates clinical scenario of locally advanced cancer
Monday. Morning. Afternoon
 Monday l 8.30 am Welcome to participants ANESTHESIA Principles and specificities of anesthesia for laparoscopy EQUIPMENT Operating theatre - choice of equipment - the laparoscopic unit Conventional laparoscopic
Monday l 8.30 am Welcome to participants ANESTHESIA Principles and specificities of anesthesia for laparoscopy EQUIPMENT Operating theatre - choice of equipment - the laparoscopic unit Conventional laparoscopic
URINARY DIVERSIONS. Winter 2016 Dr P. O Malley
 URINARY DIVERSIONS Winter 2016 Dr P. O Malley OVERVIEW Who gets diversions? What s involved with cystectomy? What are the different types of diversions? What are the problems with various diversions? How
URINARY DIVERSIONS Winter 2016 Dr P. O Malley OVERVIEW Who gets diversions? What s involved with cystectomy? What are the different types of diversions? What are the problems with various diversions? How
Radical Cystectomy in the Treatment of Bladder Cancer: Oncological Outcome and Survival Predictors
 ORIGINAL ARTICLE Radical Cystectomy in the Treatment of Bladder Cancer: Oncological Outcome and Survival Predictors Chen-Hsun Ho, 1,2 Chao-Yuan Huang, 1 Wei-Chou Lin, 3 Shih-Chieh Chueh, 1 Yeong-Shiau
ORIGINAL ARTICLE Radical Cystectomy in the Treatment of Bladder Cancer: Oncological Outcome and Survival Predictors Chen-Hsun Ho, 1,2 Chao-Yuan Huang, 1 Wei-Chou Lin, 3 Shih-Chieh Chueh, 1 Yeong-Shiau
Causes of Raised PSA A very large prostate Gland Infection of urine or Prostate Gland Possibility of prostate Cancer
 Causes of Raised PSA A very large prostate Gland Infection of urine or Prostate Gland Possibility of prostate Cancer Gleason score Gleason score 2-4: well differentiated (seldom reported now): Low risk
Causes of Raised PSA A very large prostate Gland Infection of urine or Prostate Gland Possibility of prostate Cancer Gleason score Gleason score 2-4: well differentiated (seldom reported now): Low risk
In the past radical nephrectomy necessitated a large
 A Prospective Study of Laparoscopic Radical Nephrectomy for T1 Tumors Is Transperitoneal, Retroperitoneal or Hand Assisted the Best Approach? Robert B. Nadler,* Stacy Loeb, J. Quentin Clemens, Robert A.
A Prospective Study of Laparoscopic Radical Nephrectomy for T1 Tumors Is Transperitoneal, Retroperitoneal or Hand Assisted the Best Approach? Robert B. Nadler,* Stacy Loeb, J. Quentin Clemens, Robert A.
3.1 Investigations for Patients Presenting with Haematuria Table 1
 3.1 Investigations for Patients Presenting with Haematuria Table 1 Patients at risk of bacterial endocarditis should be given antibiotic prophylaxis as per local guidelines. Patients with heart valve replacements
3.1 Investigations for Patients Presenting with Haematuria Table 1 Patients at risk of bacterial endocarditis should be given antibiotic prophylaxis as per local guidelines. Patients with heart valve replacements
Prostate Case Scenario 1
 Prostate Case Scenario 1 H&P 5/12/16: A 57-year-old Hispanic male presents with frequency of micturition, urinary urgency, and hesitancy associated with a weak stream. Over the past several weeks, he has
Prostate Case Scenario 1 H&P 5/12/16: A 57-year-old Hispanic male presents with frequency of micturition, urinary urgency, and hesitancy associated with a weak stream. Over the past several weeks, he has
SURGERY, TRANSPLANTATION AND POLYCYSTIC DISEASE. Mr Nick Inston PhD FRCS Consultant Transplant Surgeon Queen Elizabeth Hospital Birmingham
 SURGERY, TRANSPLANTATION AND POLYCYSTIC DISEASE Mr Nick Inston PhD FRCS Consultant Transplant Surgeon Queen Elizabeth Hospital Birmingham What are polycystic kidneys and livers?! Cystic degenerative condition!
SURGERY, TRANSPLANTATION AND POLYCYSTIC DISEASE Mr Nick Inston PhD FRCS Consultant Transplant Surgeon Queen Elizabeth Hospital Birmingham What are polycystic kidneys and livers?! Cystic degenerative condition!
Laparoscopic Resection Of Colon & Rectal Cancers. R Sim Centre for Advanced Laparoscopic Surgery, TTSH
 Laparoscopic Resection Of Colon & Rectal Cancers R Sim Centre for Advanced Laparoscopic Surgery, TTSH Feasibility and safety Adequacy - same radical surgery as open op. Efficacy short term benefits and
Laparoscopic Resection Of Colon & Rectal Cancers R Sim Centre for Advanced Laparoscopic Surgery, TTSH Feasibility and safety Adequacy - same radical surgery as open op. Efficacy short term benefits and
Early radical cystectomy in NMIBC Marko Babjuk
 Early radical cystectomy in NMIBC Marko Babjuk Dept. of Urology, 2nd Faculty of Medicine, Hospital Motol, Praha, Czech Republic We Are The European Association of Urology We Are Urologists, residents,
Early radical cystectomy in NMIBC Marko Babjuk Dept. of Urology, 2nd Faculty of Medicine, Hospital Motol, Praha, Czech Republic We Are The European Association of Urology We Are Urologists, residents,
BJUI. Robotic nephrectomy for the treatment of benign and malignant disease
 . JOURNAL COMPILATION 2008 BJU INTERNATIONAL Laparoscopic and Robotic Urology ROGERS et al. BJUI BJU INTERNATIONAL Robotic nephrectomy for the treatment of benign and malignant disease Craig Rogers, Rajesh
. JOURNAL COMPILATION 2008 BJU INTERNATIONAL Laparoscopic and Robotic Urology ROGERS et al. BJUI BJU INTERNATIONAL Robotic nephrectomy for the treatment of benign and malignant disease Craig Rogers, Rajesh
Staging and Grading Last Updated Friday, 14 November 2008
 Staging and Grading Last Updated Friday, 14 November 2008 There is a staging graph below Blood in the urine is the most common indication that something is wrong. Often one will experience pain or difficulty
Staging and Grading Last Updated Friday, 14 November 2008 There is a staging graph below Blood in the urine is the most common indication that something is wrong. Often one will experience pain or difficulty
SINGLE INCISION ENDOSCOPIC SURGERY (SIES)
") EAES CONSENSUS CONFERENCE SINGLE INCISION ENDOSCOPIC SURGERY (SIES) STATEMENTS AND RECOMMENDATIONS EAES appreciates your input! Please give your opinion on the below statements and recommendations of the
EAES CONSENSUS CONFERENCE SINGLE INCISION ENDOSCOPIC SURGERY (SIES) STATEMENTS AND RECOMMENDATIONS EAES appreciates your input! Please give your opinion on the below statements and recommendations of the
Training Course for Advanced Oncologic Laparoscopy. Robotic Urology. Ch.-H. Rochat Geneva
 Training Course for Advanced Oncologic Laparoscopy Robotic Urology Ch.-H. Rochat Geneva St Petersbourg 16 February 2006 Urology and mini-invasive surgery radical prostatectomy nephrectomy (partial or total)
Training Course for Advanced Oncologic Laparoscopy Robotic Urology Ch.-H. Rochat Geneva St Petersbourg 16 February 2006 Urology and mini-invasive surgery radical prostatectomy nephrectomy (partial or total)
Minimal Invasive Approach ro radical cystectomy: Results of the European multicentric study
 Minimal Invasive Approach ro radical cystectomy: Results of the European multicentric study Dr Alexandre Peltier Institut Jules Bordet, Bruxelles (BE) The 9 th Congress of the Lebanese Urology Society
Minimal Invasive Approach ro radical cystectomy: Results of the European multicentric study Dr Alexandre Peltier Institut Jules Bordet, Bruxelles (BE) The 9 th Congress of the Lebanese Urology Society
Multidisciplinary management of retroperitoneal sarcomas
 Multidisciplinary management of retroperitoneal sarcomas Eric K. Nakakura, MD UCSF Department of Surgery UCSF Comprehensive Cancer Center San Francisco, CA 7 th Annual Clinical Cancer Update North Lake
Multidisciplinary management of retroperitoneal sarcomas Eric K. Nakakura, MD UCSF Department of Surgery UCSF Comprehensive Cancer Center San Francisco, CA 7 th Annual Clinical Cancer Update North Lake
Killing Tumors with Scans Not Scalpels: Kidney Cancer Ablation. Basics. What is Percutaneous Ablation? Where are your kidneys?
 Killing Tumors with Scans Not Scalpels: Kidney Cancer Ablation Ronald J. Zagoria, M.D. UCSF Professor and Vice Chair Abdominal Imaging Section Chief Basics Where are your kidneys? What is ablation? Facts
Killing Tumors with Scans Not Scalpels: Kidney Cancer Ablation Ronald J. Zagoria, M.D. UCSF Professor and Vice Chair Abdominal Imaging Section Chief Basics Where are your kidneys? What is ablation? Facts
Outcomes. Glickman Urological & Kidney Institute
 Outcomes 28 Glickman Urological & Kidney Institute Surgical Overview To promote quality improvement, Cleveland Clinic has created a series of Outcomes books similar to this one for many of its institutes.
Outcomes 28 Glickman Urological & Kidney Institute Surgical Overview To promote quality improvement, Cleveland Clinic has created a series of Outcomes books similar to this one for many of its institutes.
Challenges in RCC surgery. Treatment Goals. Surgical challenges. Management options in VHL associated RCCs
 Management options in VHL associated RCCs Challenges in RCC surgery JJ PATARD, MD, PhD Paris XI University Observation, Radical nephrectomy, Renal parenchymal sparing surgery, Open, laparoscopic, robotic
Management options in VHL associated RCCs Challenges in RCC surgery JJ PATARD, MD, PhD Paris XI University Observation, Radical nephrectomy, Renal parenchymal sparing surgery, Open, laparoscopic, robotic
6 TH INTERNATIONAL TECHNO-UROLOGY MEETING (TUM) NEW TECHNOLOGIES FOR A MORE PRECISE SURGERY
 NEW TECHNOLOGIES FOR A MORE PRECISE SURGERY") Azienda Sanitaria Ospedaliera S.Luigi Gonzaga Orbassano (To) Department of Urology, San Luigi Gonzaga Hospital School of Medicine - University of Torino, Orbassano, Torino, Italy Chairmen: Prof. Francesco
Azienda Sanitaria Ospedaliera S.Luigi Gonzaga Orbassano (To) Department of Urology, San Luigi Gonzaga Hospital School of Medicine - University of Torino, Orbassano, Torino, Italy Chairmen: Prof. Francesco
BLK Centre for Renal Sciences & Kidney Transplant
 24-Hour Helpline: 011-30403040 BLK Super Speciality Hospital Pusa Road, New Delhi - 110005 (India). www.blkhospital.com BLK Centre for Renal Sciences & Kidney Transplant Introduction The BLK Renal Sciences
24-Hour Helpline: 011-30403040 BLK Super Speciality Hospital Pusa Road, New Delhi - 110005 (India). www.blkhospital.com BLK Centre for Renal Sciences & Kidney Transplant Introduction The BLK Renal Sciences