Intro to Gallbladder & Pancreas Pathology
|
|
|
- Patricia Cox
- 6 years ago
- Views:
Transcription
1 Cholecystitis acute chronic Gallbladder tumors Adenomyoma (benign) Adenocarcinoma Pancreatitis i acute chronic Pancreatic tumors Intro to Gallbladder & Pancreas Pathology Helen Remotti M.D. Dept. of Pathology her2007@columbia.edu
2 Gallstones (Cholelithiasis) 10-20% Adults 35% Autopsy: Over 65 Over 20 Million 600,000 Cholecystectomies #2 reason for abdominal operations
3 Cholesterol/mixed stones
4 Choledocholithiasis (Stones in the common bile duct) Pain: Epigastric, RUQ-stones may be passed Obstructive Jaundice-may be intermittent Ascending Cholangitis- 20%: No pain; 25% no jaundice Infection: to liver
5 Acute cholecystitis i = ischemic i injury
6 Chronic Cholecystitis Associated with calculi in 95% of cases. Multiples episodes of inflammation cause GB thickening with chronic inflammation/ fibrosis and muscular hypertrophy. Rokitansky - Aschoff Sinuses (mucosa herniates through the muscularis mucosae) With longstanding inflammation GB becomes fibrotic and calcified porcelain GB
7
8 Chronic cholecystitis
9 Rokitansky-Aschoff sinuses
10 Chronic Cholecystitis Fibrosis Chronic Inflammation Rokitansky - Aschoff Sinuses Hypertrophy: Muscularis




11 Cholesterolosis F l l ti f h l t l ld h i Focal accumulation of cholesterol-laden macrophages in lamina propria of gallbladder (incidental finding).
12 Adenomyoma of Gall Bladder
13
14
15
16 Carcinoma: Gall Bladder Uncommon: 5,000 cases / year Fewer than 1% resected G.B. Sx: same as with stones 5 yr. survival: Less than 5% (survival relates to stage) 90%: Stones Long Hx: symptomatic stones Stones: predispose to CA., but uncommon complication
17
18
19 Gallbladder carcinoma
20 Case 1 56 year old woman presents to ER in shock, following rapid onset of severe upper abdominal pain, developing over the previous day. Hx: heavy alcohol use. LABs: Elevated serum amylase and elevated peritoneal fluid lipase
21 Acute Pancreatitis Patient developed rapid onset of respiratory failure necessitating intubation and mechanical ventilation. Over 48 hours, she was increasingly unstable, with evolution to multi-organ failure, and she expired 82 hours after admission. An autopsy was performed.
22 Acute pancreatitis








23



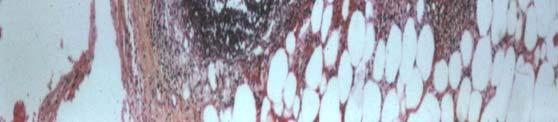
24 Elastase destruction of blood vessels with hemorrhage
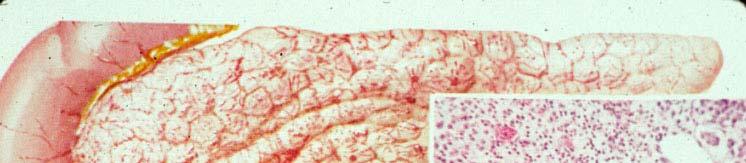
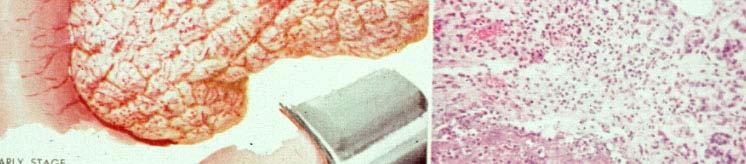




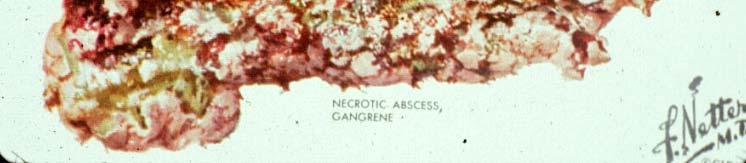
25 Acute Pancreatitis Edema, congestion Advanced hemorrhagic pancreatitis, fat necrosis Necrotic abscess, gangrene
26
27 Acute Pancreatitis US: 45% of cases have gallstones and choledocholithiasis; 35% associated with heavy alcohol ingestion Pathology: Enzyme release is triggered with digestion of pancreas, necrosis of fat and lobules, hemorrhage from damaged blood vessels. Variable severity: may lead to liquefactive necrosis, hemorrhage. Mild cases may have local complications: abscess, pseudocyst.
28 Chronic Pancreatitis Continuing inflammation with irreversible changes in architecture, structure and function. Fibrosis of parenchyma with distortion of duct architecture, loss of exocrine secretory function. Changes may be focal or widespread.
29 Chronic pancreatitis with Stones
30
31 Chronic pancreatitis
32 Chronic Pancreatitis
33 Complications of Chronic Pancreatitis Chronic abdominal pain, severe and unremitting, radiating to back Malabsorption due to reduced d enzyme secretion. (After 90% of pancreas is fibrotic, reduced lipase and trypsin secretion lead to steatorrhea). Pancreatic diabetes associated with decreased islets. Pancreatic pseudocysts with extension or rupture in adjacent organs.
34 Case 2 67 year old woman with recent onset painless jaundice. History of 15lb weight loss over last 3 months. She smoked 1 pack per day x 35 years. Physical exam: palpable GB ERCP was performed with Endoscopic Ultrasound (EUS) evidence of a large mass in the head of the pancreas. An endoscopic FNA was performed.
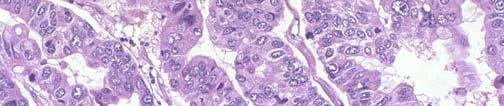
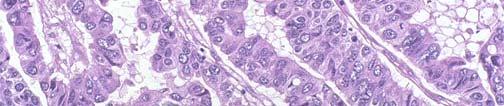
35 Normal pancreas ductal epithelium Patient s FNA Dx: Adenocarcinoma
36 Curvoissier s Law enlarged palpable GB
37 Pancreatic Ductal Adenocarcinoma: Clinical Represents the most common pancreatic neoplasm 2nd most common GIT cancer 4th leading cause of cancer death M > F; > 50 years at initial iti presentation ti usually Symptoms: Abdominal pain, weight loss, jaundice, pancreatic insufficiency, malabsorption; lb Migratory thrombophlebitis hlbii (hypercoagulable lbl state) Trousseau s sign Site: head (60-70%) 0%) > body (10-15%) 1%) > tail il( (5-10%) Contributing factors: smoking, carcinogens, genetics
38
39
40 Pancreatic Ductal Adenocarcinoma: Pathology Macroscopic: Usually a solitary mass poor demarcation firm to gritty consistency depends upon location, but bile stasis specifically for the head of pancreas neoplasms
41 Chronic Pancreatitis: FNA
42 Pancreatic Ductal Adenocarcinoma: FNA
43 Normal AdenoCA




44 Benign lobular Malignant- haphazard
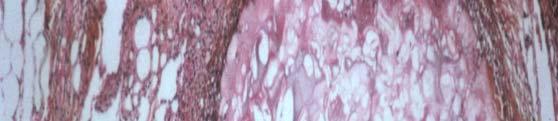
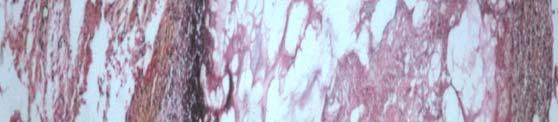
45 Invasive growth with associated desmoplasia
46 Invasion into peripancreatic soft tissue
47 Pancreatic adenocarcinoma Lymph node metastases
48 Pancreatic adenocarcinoma perineural invasion
49 Pancreatic Ductal Adenocarcinoma: Pathology Microscopic: loss of lobular architecture architectural and cytomorphologic features indicative of malignancy: loss of cell differentiation, hyperchromatic nuclei, increased N:C, prominent nucleoli, mitotic activity intraductal carcinoma invasive growth associated with desmoplasia neurotropism, extratumoral vascular invasion extension into peripancreatic soft tissue secondary ypancreatitis due to obstruction
50 Critical area to evaluate- uncinate margin Margin most likely To be positive is the Uncinate margin - Retroperitoneal/mesenteric Margin along the right Lateral border of the SMA And should be inked.
 Pancreatic distal")

51 Margin evaluation: (Black posterior) Bile duct (Yellow anterior) Pancreatic distal Posterior/Retroperitoneal Uncinate Tumor size: Measure Gross Submit 2 complete cross sections.
52 Definition of Tumor (T) TX Primary tumor cannot be assessed T0 No evidence of primary tumor Tis In situ carcinoma T1 Tumor limited it dto the pancreas, 2 cm or less in greatest t dimension T2 Tumor limited to the pancreas, more than 2 cm in greatest t dimension i T3 Tumor extends directly into any of the following: duodenum, bile duct, peripancreatic tissues T4 Tumor is not resectable and extends directly into any of the following: stomach, spleen, colon, adjacent large vessels
53 Pancreatic Cancer 2 yr survival 28% 5 yr survival 3-12% Prognosis Mean survival in untreated patients 3 mo. Mean survival after radical resection mo (Less than 20% of patients are surgical candidates).
54 Pancreas Cancer Genetics 5-10% of cases are familial, some with defined genetic syndromes Hereditary Pancreatitis: germline mutations in trypsinogen gene on 7q35 with 40% lifetime i risk of developing pancreatic cancer. Pancreatic cancers described in BRCA2 mutations in familial breast cancer kindreds. Associated with germline p16 mutations, and HNPCC. Role of oncogenes: KRAS-90%, p16-95%, p53-75%
55 In sit progression to Cancer In-situ progression to Cancer Takaori and Hruban Pancreas :

56 Pan IN (Pancreatic Intraepithelial Neoplasia) PanIN-1A-flat epithelium; basal nuclei, abundant supranuclear cytoplasm PanIN-1B papillary, micropapillary architecture; cytology same as 1A.
 PanIN-2-")


57 Pan IN-2 (Pancreatic Intraepithelial Neoplasia Moderate Dysplasia ) PanIN-2- flat or papillary, micropapillary; some nuclear abnormalities (some loss of polarity, nuclear crowding, enlarged nuclei, pseudostratification, and hyperchromasia but less than PanIN-3)
 PanIN3 cribriform,")
 (marked loss of polarity,")

58 Pan IN (Pancreatic Intraepithelial Neoplasia) PanIN3 cribriform, papillary, micropapillary (rarely flat) (marked loss of polarity, nuclear crowding, enlarged nuclei, pseudostratification, and hyperchromasia, abnormal mitoses)
59 Pancreatic Cystic Lesions Mucinous cystic neoplasm (benign, borderline or malignant) Intraductal papillary mucinous neoplasm (benign, borderline or malignant) Serous cystadenoma (benign) Pseudocyst (benign NOT a NEOPLASM)
60 PANCREATIC CYSTIC LESIONS MCN
61 Mucinous cystic Neoplasm Mucinous cystic Neoplasm NOT connected with pancreatic ducts!


62 Mucinous cystadenoma Mucinous cystadenocarcinoma
63 Mucinous cystic neoplasm Mucinous epithelium; ovarian type stroma Clinical spectrum: benign to malignant
64 Mucinous Cystic Neoplasms MCNs Mainly Females (mean age 45) Abdominal Pain or Mass Sample extensively to rule out invasive component Classification: Mucinous cystadenoma (minimal atypia) Borderline MCN (moderate atypia, papillary architecture) MCN with CIS (high grade cytology, cribriform architecture) Invasive CA (destructive stromal invasion, usual ductal CA) Gross: large (mean 10cm); Body/Tail; Multilocular, unilocular rare NO communication with pancreatic duct. Micro: Columnar mucin cells; intestinal or gastric foveolar type. Ovarian stroma (ER+, PR+, inhibin+) DD: IPMN (Head/communicate with ducts/ no ovarian stroma) Pancreatic Pseudocyst (MCN lining can be denuded)
65
66 PANCREATIC CYSTIC LESIONS IPMN MCN
67 Intraductal Papillary Mucinous Neoplasm (IPMN)




68 IPMNs (Intraductal Papillary Mucinous Neoplasms) Communicates with hduct Mucin oozes out of ampullae
69 Intraductal papillary mucinous neoplasm (IPMN) Associated with the pancreatic duct Clinical spectrum: benign to malignant
70 Intraductal Papillary Mucinous Neoplasm (IPMN) IPMT (first named in 1995) Radiologic or grossly visible lesion (>1cm) Contiguous or multicentric with cytologic atypia Head of pancreas; More common in male >60 y. Invasive tumors associated with 30% of IPMNs (often colloid type more indolent clinical i lbehavior than usual linvasive i ductal-nos.) Resection often with frozen sections, since most lesions are contiguous. Grade (Benign, Borderline, Intraductal CA); DD: Mucinous cystic neoplasms, PanIN (resembles small IPMN)
71
72 PANCREATIC CYSTIC LESIONS Serous Cystadenoma IPMN MCN
73 Pancreatic serous cystadenoma BENIGN
74 Serous Cystadenoma Aka microcystic adenoma, glycogen rich adenoma F/M =7/1; mean age 66y Association with von Hippel Lindau syndrome Symptoms: none, local pain, obstruction if in head Clinical behavior: benign Gross: mean 11 cm; multiloculated mass, cysts filled with clear fluid; spongy; often central scar. Micro: small cystic spaces lined with cuboidal cells with clear cytoplasm (glycogen rich); round nuclei; some cases papillary.
75 PANCREATIC CYSTIC LESIONS Serous Cystadenoma IPMN Pseudocyst MCN
76 Pancreatic Pseudocyst NOT NEOPLASTIC - RESULT OF ACUTE PANCREATITIS
77 Pseudocyst Localized collections of pancreatic secretions that follow pancreatitis, trauma, ductal calculi. Symptoms: Painful, Hemorrhage, Infection, Perforation Treatment: excise small pseudocysts in body/tail; drain cysts in head. Gross: 85% solitary, usually unilocular l in/near pancreas; thick irregular wall, ragged inner surface. Micro: No epithelial lining, fluid has high amylase Cyst arises from drainage of pancreatic secretions from damaged ducts into interstitial tissue; wall consists of fibrous tissue/granulation tissue.
78 Pancreatic Endocrine Neoplasms 5% of pancreatic neoplasms Islet cell Tumors inaccurate; arise from pluripotential ductal cells that differentiate along neuroendocrine lines. All have malignant potential except microadenomas (<5mm); No definite criteria to distinguish i between benign and malignant (except for mets)
79



80 Pancreatic Endocrine Tumors
81
82 Pancreatic c Endocrine Neoplasms s Microscopic Nests of uniform polygonal cells Delicate vasculature Salt and Pepper (stippled) chromatin. Often (no necrosis, low mitotic activity) Immunostains do not correlate with secretion. (Other than chromogranin and synaptophysin; specific stains: glucagon, insulin, PP, VIP, ACTH, somatostatin not really useful.)
83 Pancreatic Endocrine Neoplasms Functional - recognizable syndrome; detect hormone in serum. Insulinoma (most common); hypoglycemia; 10% malignant 10% assoc with MEN1 Gastrinoma; duodenal ulcers; 75% malignant 25% assoc with MEN1 Nonfunctional - no syndrome; normal serum hormone levels (except Pancreatic Polypeptide). Incidental; Obstructive Sx- head of pancreas; 50 90% malignant.
84 Pancreatic Endocrine Neoplasms Usually occur in body/tail Hypervascular, circumscribed Highlighted with Octreotide Scan (somatostatin receptors) Usually slow growing, mets to LNs, liver, bone (recommend resection of mets)
85 Pancreatic Endocrine Neoplasms Classification: Neuroendocrine neoplasm, well differentiated Low grade: 0-1 mit/50hpf; no necrosis Intermediate grade: > or = 2mit/50 HPF; +/- necrosis Reference: Hochwald et al. J Clin Oncol 2002; 20: Neuroendocrine carcinoma, high grade - Small cell carcinoma / large cell neuroendocrine High grade: >10mit/10 HPF; widespread necrosis
86
87 Questions or Comments Please me.. (all feedback welcome negative or positive.. your imput will help improve lectures for the next year of medical students )
Intro to Gallbladder & Pancreas Pathology
 Cholecystitis acute chronic Gallbladder tumors Adenomyoma (benign) Adenocarcinoma Pancreatitis acute chronic Pancreatic tumors Intro to Gallbladder & Pancreas Pathology Helen Remotti M.D. Gallstones (Cholelithiasis)
Cholecystitis acute chronic Gallbladder tumors Adenomyoma (benign) Adenocarcinoma Pancreatitis acute chronic Pancreatic tumors Intro to Gallbladder & Pancreas Pathology Helen Remotti M.D. Gallstones (Cholelithiasis)
Case 1. Intro to Gallbladder & Pancreas Pathology. Case 1 DIAGNOSIS??? Acute Cholecystitis. Acute Cholecystitis. Helen Remotti M.D.
 Cholecystitis acute chronic Gallbladder tumors Adenomyoma (benign) Adenocarcinoma Pancreatitis acute chronic Pancreatic tumors Intro to Gallbladder & Pancreas Pathology Helen Remotti M.D. Case 1 70 year
Cholecystitis acute chronic Gallbladder tumors Adenomyoma (benign) Adenocarcinoma Pancreatitis acute chronic Pancreatic tumors Intro to Gallbladder & Pancreas Pathology Helen Remotti M.D. Case 1 70 year
Neoplasias Quisticas del Páncreas
 SEAP -Aproximación Práctica a la Patología Gastrointestinal- Madrid, 26 de mayo, 2006 Neoplasias Quisticas del Páncreas Gregory Y. Lauwers, M.D. Director, Service Massachusetts General Hospital Harvard
SEAP -Aproximación Práctica a la Patología Gastrointestinal- Madrid, 26 de mayo, 2006 Neoplasias Quisticas del Páncreas Gregory Y. Lauwers, M.D. Director, Service Massachusetts General Hospital Harvard
Anatomy of the biliary tract
 Harvard-MIT Division of Health Sciences and Technology HST.121: Gastroenterology, Fall 2005 Instructors: Dr. Jonathan Glickman Anatomy of the biliary tract Figure removed due to copyright reasons. Biliary
Harvard-MIT Division of Health Sciences and Technology HST.121: Gastroenterology, Fall 2005 Instructors: Dr. Jonathan Glickman Anatomy of the biliary tract Figure removed due to copyright reasons. Biliary
Select problems in cystic pancreatic lesions
 Disclosure Select problems in cystic pancreatic lesions Five Prime Therapeutics shareholder Adicet Bio shareholder Bristol-Meyer Squibb advisory board grace.kim@ucsf.edu Pancreatic cystic lesions Intraductal
Disclosure Select problems in cystic pancreatic lesions Five Prime Therapeutics shareholder Adicet Bio shareholder Bristol-Meyer Squibb advisory board grace.kim@ucsf.edu Pancreatic cystic lesions Intraductal
40th European Congress of Cytology Liverpool, UK, 2-5 th October 2016
 40th European Congress of Cytology Liverpool, UK, 2-5 th October 2016 EUS FNA of abdominal organs: An approach to reporting and triage for ancillary testing Date and time: Sunday 2 nd October 2016 15.00-16.30
40th European Congress of Cytology Liverpool, UK, 2-5 th October 2016 EUS FNA of abdominal organs: An approach to reporting and triage for ancillary testing Date and time: Sunday 2 nd October 2016 15.00-16.30
Pancreatic Cystic Lesions 원자력병원
 Pancreatic Cystic Lesions 원자력병원 박선 후 Lines of cellular differentiation Ductal Acinar Undetermined Ductal adenocarcinoma Serous/ mucinous tumor Intraductal papillary mucinous neoplasm Acinar cell carcinoma
Pancreatic Cystic Lesions 원자력병원 박선 후 Lines of cellular differentiation Ductal Acinar Undetermined Ductal adenocarcinoma Serous/ mucinous tumor Intraductal papillary mucinous neoplasm Acinar cell carcinoma
Biliary tract tumors
 Short Course 2010 Annual Fall Meeting of the Korean Society for Pathologists Biliary tract tumors Joon Hyuk Choi, M.D., Ph.D. Professor, Department of Pathology, Yeungnam Univ. College of Medicine, Daegu,
Short Course 2010 Annual Fall Meeting of the Korean Society for Pathologists Biliary tract tumors Joon Hyuk Choi, M.D., Ph.D. Professor, Department of Pathology, Yeungnam Univ. College of Medicine, Daegu,
Unusual Pancreatic Neoplasms RTC 2/11/2011
 Unusual Pancreatic Neoplasms RTC 2/11/2011 Objectives Intraductal Papillary Mucinous Neoplasm (IPMN) Mucinous Cystic Neoplasm (MCN) Islet Cell Tumors Insulinoma Glucagonoma VIPoma Somatostatinoma Gastrinoma
Unusual Pancreatic Neoplasms RTC 2/11/2011 Objectives Intraductal Papillary Mucinous Neoplasm (IPMN) Mucinous Cystic Neoplasm (MCN) Islet Cell Tumors Insulinoma Glucagonoma VIPoma Somatostatinoma Gastrinoma
Outline 11/2/2017. Pancreatic EUS-FNA general aspects. Cytomorphologic features of solid neoplasms/lesions of the pancreas
 ENDOSCOPIC ULTRASOUND GUIDED-FINE NEEDLE ASPIRATION CYTOLOGY OF PANCREAS Khalid Amin M.D. Assistant Professor Department of Laboratory Medicine and Pathology University of Minnesota Outline Pancreatic
ENDOSCOPIC ULTRASOUND GUIDED-FINE NEEDLE ASPIRATION CYTOLOGY OF PANCREAS Khalid Amin M.D. Assistant Professor Department of Laboratory Medicine and Pathology University of Minnesota Outline Pancreatic
Matthew McCollough, M.D. April 9, 2009 University of Louisville
 Matthew McCollough, M.D. April 9, 2009 University of Louisville List the differential diagnosis for pancreatic cysts Review the epidemiology Illustrate the types of cysts through case discussions Discuss
Matthew McCollough, M.D. April 9, 2009 University of Louisville List the differential diagnosis for pancreatic cysts Review the epidemiology Illustrate the types of cysts through case discussions Discuss
CT 101 :Pancreas and Spleen
 CT 101 :Pancreas and Spleen Shikha Khullar,, MD, MPH Division of Radiology University of South Alabama The Pancreas Normal Pancreas 3 Phase Pancreatic CT Non contrast Arterial phase : 30-35 35 second
CT 101 :Pancreas and Spleen Shikha Khullar,, MD, MPH Division of Radiology University of South Alabama The Pancreas Normal Pancreas 3 Phase Pancreatic CT Non contrast Arterial phase : 30-35 35 second
Standardized Terminology in Pancreatobiliary Cytology: The Papanicolaou Society Guidelines
 Standardized Terminology in Pancreatobiliary Cytology: The Papanicolaou Society Guidelines Barbara Ann Centeno. M.D. Vice-Chair, Clinical Services, Anatomic Pathology Assistant Chief, Pathology Service
Standardized Terminology in Pancreatobiliary Cytology: The Papanicolaou Society Guidelines Barbara Ann Centeno. M.D. Vice-Chair, Clinical Services, Anatomic Pathology Assistant Chief, Pathology Service
Radiology Pathology Conference
 Radiology Pathology Conference Nadia F. Yusaf, M.D. PGY-3 1/29/2010 Presentation material is for education purposes only. All rights reserved. 2010 URMC Radiology Page 1 of 90 Case 1 60 year- old man presents
Radiology Pathology Conference Nadia F. Yusaf, M.D. PGY-3 1/29/2010 Presentation material is for education purposes only. All rights reserved. 2010 URMC Radiology Page 1 of 90 Case 1 60 year- old man presents
Pancreas composed of 2 parts: 1- exocrine gland 2- endocrine gland
 pancreas Pancreas composed of 2 parts: 1- exocrine gland 2- endocrine gland Acute pancreatitis Inflammation of the pancreas associated with acinar cell injury Clinical features: 1-abdominal pain cardinal
pancreas Pancreas composed of 2 parts: 1- exocrine gland 2- endocrine gland Acute pancreatitis Inflammation of the pancreas associated with acinar cell injury Clinical features: 1-abdominal pain cardinal
CHRONIC PANCREATITIS OR DUCTAL ADENOCARCINOMA? N. Volkan Adsay, \ MD
 CHRONIC PANCREATITIS OR DUCTAL ADENOCARCINOMA? N. Volkan Adsay, \ MD Case for discussion 67 y/o male Back pain and weight loss CT: 4.5 cm ill-defined, solid lesion in the head FNA/Core bx: Inconclusive
CHRONIC PANCREATITIS OR DUCTAL ADENOCARCINOMA? N. Volkan Adsay, \ MD Case for discussion 67 y/o male Back pain and weight loss CT: 4.5 cm ill-defined, solid lesion in the head FNA/Core bx: Inconclusive
Pancreas Quizzes c. Both A and B a. Directly into the blood stream (not using ducts)
") Pancreas Quizzes Quiz 1 1. The pancreas produces hormones. Which type of hormone producing organ is the pancreas? a. Endocrine b. Exocrine c. Both A and B d. Neither A or B 2. Endocrine indicates hormones
Pancreas Quizzes Quiz 1 1. The pancreas produces hormones. Which type of hormone producing organ is the pancreas? a. Endocrine b. Exocrine c. Both A and B d. Neither A or B 2. Endocrine indicates hormones
Pancreatitis: A Potential Pitfall in Endoscopic Ultrasound Guided Pancreatic FNA
 Pancreatitis: A Potential Pitfall in Endoscopic Ultrasound Guided Pancreatic FNA Jack Yang, MD Department of Pathology, Medical University of South Carolina Objectives Understand the indication of EUS
Pancreatitis: A Potential Pitfall in Endoscopic Ultrasound Guided Pancreatic FNA Jack Yang, MD Department of Pathology, Medical University of South Carolina Objectives Understand the indication of EUS
The Pancreas. Basic Anatomy. Endocrine pancreas. Exocrine pancreas. Pancreas vasculature. Islets of Langerhans. Acinar cells Ductal System
 SGNA: Back to Basics Rogelio G. Silva, MD Assistant Clinical Professor of Medicine University of Illinois at Chicago Department of Medicine Division of Gastroenterology Advocate Christ Medical Center GI
SGNA: Back to Basics Rogelio G. Silva, MD Assistant Clinical Professor of Medicine University of Illinois at Chicago Department of Medicine Division of Gastroenterology Advocate Christ Medical Center GI
Papillary Lesions of the breast
 Papillary Lesions of the breast Emad Rakha Professor of Breast Pathology The University of Nottingham Papillary lesions of the breast are a heterogeneous group of disease, which are characterised by neoplastic
Papillary Lesions of the breast Emad Rakha Professor of Breast Pathology The University of Nottingham Papillary lesions of the breast are a heterogeneous group of disease, which are characterised by neoplastic
X-ray Corner. Imaging of The Pancreas. Pantongrag-Brown L
 X-ray Corner 125 Imaging of The Pancreas Modern imaging modalities commonly used in pancreas include ultrasound (US), CT, and MRI. Pancreas is a retroperitoneal organ which makes it difficult to visualize
X-ray Corner 125 Imaging of The Pancreas Modern imaging modalities commonly used in pancreas include ultrasound (US), CT, and MRI. Pancreas is a retroperitoneal organ which makes it difficult to visualize
Evaluation and Management of Cystic Lesions of the Pancreas: When to Resect, When to Follow and When to Forget
 Evaluation and Management of Cystic Lesions of the Pancreas: When to Resect, When to Follow and When to Forget Randall Brand, MD Professor of Medicine Division of Gastroenterology, Hepatology and Nutrition
Evaluation and Management of Cystic Lesions of the Pancreas: When to Resect, When to Follow and When to Forget Randall Brand, MD Professor of Medicine Division of Gastroenterology, Hepatology and Nutrition
Pancreatobiliary Frozen Section Nightmares
 Pancreatobiliary Frozen Section Nightmares Aatur D. Singhi, MD PhD Assistant Professor University of Pittsburgh Medical Center Department of Pathology singhiad@upmc.edu Objectives Briefly give an overview
Pancreatobiliary Frozen Section Nightmares Aatur D. Singhi, MD PhD Assistant Professor University of Pittsburgh Medical Center Department of Pathology singhiad@upmc.edu Objectives Briefly give an overview
The role of endoscopy in the diagnosis and treatment of cystic pancreatic neoplasms
 The role of endoscopy in the diagnosis and treatment of cystic pancreatic neoplasms CYSTIC LESIONS AND FLUID COLLECTIONS OF THE PANCREAS Their pathology ranges from pseudocysts and pancreatic necrosis
The role of endoscopy in the diagnosis and treatment of cystic pancreatic neoplasms CYSTIC LESIONS AND FLUID COLLECTIONS OF THE PANCREAS Their pathology ranges from pseudocysts and pancreatic necrosis
Management A Guideline Based Approach to the Incidental Pancreatic Cysts. Common Cystic Pancreatic Neoplasms.
 Management 2016 A Guideline Based Approach to the Incidental Pancreatic Cysts ISMRM 2016 Masoom Haider, MD, FRCP(C) Professor of Radiology, University of Toronto Clinician Scientist, Ontario Institute
Management 2016 A Guideline Based Approach to the Incidental Pancreatic Cysts ISMRM 2016 Masoom Haider, MD, FRCP(C) Professor of Radiology, University of Toronto Clinician Scientist, Ontario Institute
Dr. Attila Zalatnai PATHOLOGY OF THE BILIARY TRACT AND PANCREAS
 Dr. Attila Zalatnai PATHOLOGY OF THE BILIARY TRACT AND PANCREAS MAIN COMPONENST OF THE BILE bile acid salts bilirubin (conjugated, direct!) cholesterol phospholipids fatty acids mucoproteins calcium water
Dr. Attila Zalatnai PATHOLOGY OF THE BILIARY TRACT AND PANCREAS MAIN COMPONENST OF THE BILE bile acid salts bilirubin (conjugated, direct!) cholesterol phospholipids fatty acids mucoproteins calcium water
Pancreatic Lesions. Valerie Jefford Pediatric Surgery Rounds June 6, 2003
 Pancreatic Lesions Valerie Jefford Pediatric Surgery Rounds June 6, 2003 Embryology 4 th week 2 buds of endodermal origin from caudal foregut Dorsal and ventral bud Ventral migrates dorsally with CBD (below/behind
Pancreatic Lesions Valerie Jefford Pediatric Surgery Rounds June 6, 2003 Embryology 4 th week 2 buds of endodermal origin from caudal foregut Dorsal and ventral bud Ventral migrates dorsally with CBD (below/behind
Case Scenario 1. Discharge Summary
 Case Scenario 1 Discharge Summary A 69-year-old woman was on vacation and noted that she was becoming jaundiced. Two months prior to leaving on that trip, she had had a workup that included an abdominal
Case Scenario 1 Discharge Summary A 69-year-old woman was on vacation and noted that she was becoming jaundiced. Two months prior to leaving on that trip, she had had a workup that included an abdominal
Video Microscopy Tutorial 19
 Video Microscopy Tutorial 19 EUS FNA of Pancreatic Cysts Martha Pitman, MD There are no disclosures necessary. EUS-FNA of Pancreatic Cysts Martha Bishop Pitman, M.D. Massachusetts General Hospital Harvard
Video Microscopy Tutorial 19 EUS FNA of Pancreatic Cysts Martha Pitman, MD There are no disclosures necessary. EUS-FNA of Pancreatic Cysts Martha Bishop Pitman, M.D. Massachusetts General Hospital Harvard
BREAST PATHOLOGY. Fibrocystic Changes
 BREAST PATHOLOGY Lesions of the breast are very common, and they present as palpable, sometimes painful, nodules or masses. Most of these lesions are benign. Breast cancer is the 2 nd most common cause
BREAST PATHOLOGY Lesions of the breast are very common, and they present as palpable, sometimes painful, nodules or masses. Most of these lesions are benign. Breast cancer is the 2 nd most common cause
Salivary Glands 3/7/2017
 Salivary Glands 3/7/2017 Goals and objectives Focus on the entities unique to H&N Common board type facts Information for your future practice Salivary Glands Salivary Glands Major gland. Paratid. Submandibular.
Salivary Glands 3/7/2017 Goals and objectives Focus on the entities unique to H&N Common board type facts Information for your future practice Salivary Glands Salivary Glands Major gland. Paratid. Submandibular.
The pathology of pancreas
 5. Practice The pathology of pancreas 2017/2018. 2nd semester MACROSCOPY- MICROSCOPY THE STRUCTURE OF PANCREAS Exocrine: 80-85% Enzymes in the zymogenic granules of acinar cells: trypsin, chymotrypsin,
5. Practice The pathology of pancreas 2017/2018. 2nd semester MACROSCOPY- MICROSCOPY THE STRUCTURE OF PANCREAS Exocrine: 80-85% Enzymes in the zymogenic granules of acinar cells: trypsin, chymotrypsin,
Management of Pancreatic Islet Cell Tumors
 Management of Pancreatic Islet Cell Tumors Ravi Dhanisetty, MD November 5, 2009 Morbidity and Mortality Conference Case Presentation 42 yr female with chronic abdominal pain. PMHx: Uterine fibroids Medications:
Management of Pancreatic Islet Cell Tumors Ravi Dhanisetty, MD November 5, 2009 Morbidity and Mortality Conference Case Presentation 42 yr female with chronic abdominal pain. PMHx: Uterine fibroids Medications:
Pancreatic Cysts. Darius C. Desai, MD FACS St. Luke s University Health Network
 Pancreatic Cysts Darius C. Desai, MD FACS St. Luke s University Health Network None Disclosures Incidence Widespread use of cross sectional imaging Seen in over 2% of patients having abdominal imaging
Pancreatic Cysts Darius C. Desai, MD FACS St. Luke s University Health Network None Disclosures Incidence Widespread use of cross sectional imaging Seen in over 2% of patients having abdominal imaging
Mody. AIS vs. Invasive Adenocarcinoma of the Cervix
 Common Problems in Gynecologic Pathology Michael T. Deavers, M.D. Houston Methodist Hospital, Houston, Texas Common Problems in Gynecologic Pathology Adenocarcinoma in-situ (AIS) of the Cervix vs. Invasive
Common Problems in Gynecologic Pathology Michael T. Deavers, M.D. Houston Methodist Hospital, Houston, Texas Common Problems in Gynecologic Pathology Adenocarcinoma in-situ (AIS) of the Cervix vs. Invasive
Case 1. Case 1: EUS Report 5/1/2017. Interesting Cases of Pancreatic Masses
 Interesting Cases of Pancreatic Masses Martha Bishop Pitman, MD Professor of Pathology Harvard Medical School Director of Cytopathology Massachusetts General Hospital Boston, MA MASSACHUSETTS GENERAL PHYSICIANS
Interesting Cases of Pancreatic Masses Martha Bishop Pitman, MD Professor of Pathology Harvard Medical School Director of Cytopathology Massachusetts General Hospital Boston, MA MASSACHUSETTS GENERAL PHYSICIANS
Disorders of Cell Growth & Neoplasia. Histopathology Lab
 Disorders of Cell Growth & Neoplasia Histopathology Lab Paul Hanna April 2010 Case #84 Clinical History: 5 yr-old, West Highland White terrier. skin mass from axillary region. has been present for the
Disorders of Cell Growth & Neoplasia Histopathology Lab Paul Hanna April 2010 Case #84 Clinical History: 5 yr-old, West Highland White terrier. skin mass from axillary region. has been present for the
Pancreatic Cancer: The ABCs of the AJCC and WHO
 Pancreatic Cancer: The ABCs of the AJCC and WHO Aatur D. Singhi, MD PhD Assistant Professor University of Pittsburgh Medical Center Department of Pathology singhiad@upmc.edu Case presentation Objectives
Pancreatic Cancer: The ABCs of the AJCC and WHO Aatur D. Singhi, MD PhD Assistant Professor University of Pittsburgh Medical Center Department of Pathology singhiad@upmc.edu Case presentation Objectives
Pancreatic Cytopathology: A pragmatic approach. By Dr Miguel Perez-Machado MD. PhD. MRCPath Royal Free Hospital
 Pancreatic Cytopathology: A pragmatic approach. By Dr Miguel Perez-Machado MD. PhD. MRCPath Royal Free Hospital Indications of Cytology Sampling To document malignancy in patients with malignant appearing
Pancreatic Cytopathology: A pragmatic approach. By Dr Miguel Perez-Machado MD. PhD. MRCPath Royal Free Hospital Indications of Cytology Sampling To document malignancy in patients with malignant appearing
Case Scenario 1: Thyroid
 Case Scenario 1: Thyroid History and Physical Patient is an otherwise healthy 80 year old female with the complaint of a neck mass first noticed two weeks ago. The mass has increased in size and is palpable.
Case Scenario 1: Thyroid History and Physical Patient is an otherwise healthy 80 year old female with the complaint of a neck mass first noticed two weeks ago. The mass has increased in size and is palpable.
Objectives. Intraoperative Consultation of the Whipple Resection Specimen. Pancreas Anatomy. Pancreatic ductal carcinoma 11/10/2014
 Intraoperative Consultation of the Whipple Resection Specimen Pathology Update Faculty of Medicine, University of Toronto November 15, 2014 John W. Wong, MD, FRCPC Department of Anatomical Pathology Sunnybrook
Intraoperative Consultation of the Whipple Resection Specimen Pathology Update Faculty of Medicine, University of Toronto November 15, 2014 John W. Wong, MD, FRCPC Department of Anatomical Pathology Sunnybrook
Chief Complaint. Retroperitoneal cystic mass incidentally found at health examination center.
 Personal Information Age: 34 y/o Sex: female Past history: major systemic medical history(-) surgical history(-), family history(-) Denied food or drug allergy Chief Complaint Retroperitoneal cystic mass
Personal Information Age: 34 y/o Sex: female Past history: major systemic medical history(-) surgical history(-), family history(-) Denied food or drug allergy Chief Complaint Retroperitoneal cystic mass
Case in discussion. Common diagnostic problems in gallbladder pathology 62, F
 Common diagnostic problems in gallbladder pathology N. Volkan Adsay, M.D. 62, F Case in discussion Underwent cholecystectomy with the diagnosis of chronic cholecystititis and cholelithiasis Professor and
Common diagnostic problems in gallbladder pathology N. Volkan Adsay, M.D. 62, F Case in discussion Underwent cholecystectomy with the diagnosis of chronic cholecystititis and cholelithiasis Professor and
Role of Imaging Methods in Diagnosis of Acute Pancreatitis. Válek V. Radiologická klinika, FN Brno a LF MU v Brně
 Role of Imaging Methods in Diagnosis of Acute Pancreatitis Válek V. Radiologická klinika, FN Brno a LF MU v Brně New Classification: Acute Pancreatitis 2007 revision of Atlanta classification and definitions
Role of Imaging Methods in Diagnosis of Acute Pancreatitis Válek V. Radiologická klinika, FN Brno a LF MU v Brně New Classification: Acute Pancreatitis 2007 revision of Atlanta classification and definitions
Cystic Pancreatic Lesions: Approach to Diagnosis
 Cystic Pancreatic Lesions: Approach to Diagnosis Poster No.: R-0130 Congress: RANZCR-AOCR 2012 Type: Educational Exhibit Authors: A. AGARWAL, R. M. Mendelson; Perth/AU Keywords: Cysts, Biopsy, Endoscopy,
Cystic Pancreatic Lesions: Approach to Diagnosis Poster No.: R-0130 Congress: RANZCR-AOCR 2012 Type: Educational Exhibit Authors: A. AGARWAL, R. M. Mendelson; Perth/AU Keywords: Cysts, Biopsy, Endoscopy,
Diseases of the breast (1 of 2)
") Diseases of the breast (1 of 2) Introduction A histology introduction Normal ducts and lobules of the breast are lined by two layers of cells a layer of luminal cells overlying a second layer of myoepithelial
Diseases of the breast (1 of 2) Introduction A histology introduction Normal ducts and lobules of the breast are lined by two layers of cells a layer of luminal cells overlying a second layer of myoepithelial
CYTOLOGY OF EUS- GUIDED FNA OF THE PANCREAS AND THE UPPER GI TRACT
 CYTOLOGY OF EUS- GUIDED FNA OF THE PANCREAS AND THE UPPER GI TRACT Barbara A. Centeno, M.D. Vice-Chair, Clinical Services Assistant Chief of Pathology Director of Cytopathology Department of Anatomic Pathology/Moffitt
CYTOLOGY OF EUS- GUIDED FNA OF THE PANCREAS AND THE UPPER GI TRACT Barbara A. Centeno, M.D. Vice-Chair, Clinical Services Assistant Chief of Pathology Director of Cytopathology Department of Anatomic Pathology/Moffitt
Papillary Lesions of the Breast A Practical Approach to Diagnosis. (Arch Pathol Lab Med. 2016;140: ; doi: /arpa.
 Papillary Lesions of the Breast A Practical Approach to Diagnosis (Arch Pathol Lab Med. 2016;140:1052 1059; doi: 10.5858/arpa.2016-0219-RA) Papillary lesions of the breast Span the spectrum of benign,
Papillary Lesions of the Breast A Practical Approach to Diagnosis (Arch Pathol Lab Med. 2016;140:1052 1059; doi: 10.5858/arpa.2016-0219-RA) Papillary lesions of the breast Span the spectrum of benign,
PATHOLOGY MCQs. The Pancreas
 PATHOLOGY MCQs The Pancreas A patient with cystic fibrosis is characteristically: A. more than 45 years of age B. subject to recurring pulmonary infections C. obese D. subject to spontaneous fractures
PATHOLOGY MCQs The Pancreas A patient with cystic fibrosis is characteristically: A. more than 45 years of age B. subject to recurring pulmonary infections C. obese D. subject to spontaneous fractures
Intraductal Papillary Mucinous Neoplasms: We Still Have a Way to Go! Francesco M. Serafini, MD, FACS
 Intraductal Papillary Mucinous Neoplasms: We Still Have a Way to Go! Francesco M. Serafini, MD, FACS Brooklyn VAMC September 21 st GI Grand Rounds - What is it? - Clinical entity that has emerged from
Intraductal Papillary Mucinous Neoplasms: We Still Have a Way to Go! Francesco M. Serafini, MD, FACS Brooklyn VAMC September 21 st GI Grand Rounds - What is it? - Clinical entity that has emerged from
Genetics of Pancreatic Cancer. October 6, If you experience technical difficulty during the presentation:
 Genetics of Pancreatic Cancer October 6, 2016 If you experience technical difficulty during the presentation: Contact WebEx Technical Support directly at: US Toll Free: 1-866-229-3239 Toll Only: 1-408-435-7088
Genetics of Pancreatic Cancer October 6, 2016 If you experience technical difficulty during the presentation: Contact WebEx Technical Support directly at: US Toll Free: 1-866-229-3239 Toll Only: 1-408-435-7088
Case Report Solid Serous Adenoma of the Pancreas: A Case Report and Review of the Literature
 Case Reports in Surgery Volume 2016, Article ID 3730249, 5 pages http://dx.doi.org/10.1155/2016/3730249 Case Report Solid Serous Adenoma of the Pancreas: A Case Report and Review of the Literature Anastasios
Case Reports in Surgery Volume 2016, Article ID 3730249, 5 pages http://dx.doi.org/10.1155/2016/3730249 Case Report Solid Serous Adenoma of the Pancreas: A Case Report and Review of the Literature Anastasios
Appendix 4: WHO Classification of Tumours of the pancreas 17
 S3.01 The WHO histological tumour type must be recorded. CS3.01a The histological type of the tumour should be recorded based on the current WHO classification 17 (refer to Appendices 4-7). Appendix 4:
S3.01 The WHO histological tumour type must be recorded. CS3.01a The histological type of the tumour should be recorded based on the current WHO classification 17 (refer to Appendices 4-7). Appendix 4:
04/10/2018. Intraductal Papillary Neoplasms Of Breast INTRADUCTAL PAPILLOMA
 Intraductal Papillary Neoplasms Of Breast Savitri Krishnamurthy MD Professor of Pathology Deputy Division Head The University of Texas MD Anderson Cancer Center 25 th Annual Seminar in Pathology Pittsburgh,
Intraductal Papillary Neoplasms Of Breast Savitri Krishnamurthy MD Professor of Pathology Deputy Division Head The University of Texas MD Anderson Cancer Center 25 th Annual Seminar in Pathology Pittsburgh,
Breast pathology. 2nd Department of Pathology Semmelweis University
 Breast pathology 2nd Department of Pathology Semmelweis University Breast pathology - Summary - Benign lesions - Acute mastitis - Plasma cell mastitis / duct ectasia - Fat necrosis - Fibrocystic change/
Breast pathology 2nd Department of Pathology Semmelweis University Breast pathology - Summary - Benign lesions - Acute mastitis - Plasma cell mastitis / duct ectasia - Fat necrosis - Fibrocystic change/
CLINICAL SIGNIFICANCE OF BENIGN EPITHELIAL CHANGES
 Papillomas. Papillomas are composed of multiple branching fibrovascular cores, each having a connective tissue axis lined by luminal and myoepithelial cells ( Fig. 23-11 ). Growth occurs within a dilated
Papillomas. Papillomas are composed of multiple branching fibrovascular cores, each having a connective tissue axis lined by luminal and myoepithelial cells ( Fig. 23-11 ). Growth occurs within a dilated
GASTROINTESTINAL IMAGING STUDY GUIDE
 GASTROINTESTINAL IMAGING STUDY GUIDE Pharynx Diverticula Foreign bodies Trauma o Motility Disorders Esophagus Diverticula Trauma Esophagitis Barrett esophagus Rings, webs, and strictures Varices Benign
GASTROINTESTINAL IMAGING STUDY GUIDE Pharynx Diverticula Foreign bodies Trauma o Motility Disorders Esophagus Diverticula Trauma Esophagitis Barrett esophagus Rings, webs, and strictures Varices Benign
DIAGNOSTIC CHALLENGES Pancreas FNAB. Dr. M. Weir Oct 2017
 DIAGNOSTIC CHALLENGES Pancreas FNAB Dr. M. Weir Oct 2017 CONFLICT OF INTEREST DISCLOSURE I have not had in the past 3 years, a financial interest, arrangement or affiliation with one or more organizations
DIAGNOSTIC CHALLENGES Pancreas FNAB Dr. M. Weir Oct 2017 CONFLICT OF INTEREST DISCLOSURE I have not had in the past 3 years, a financial interest, arrangement or affiliation with one or more organizations
Gallbladder & Pancreas Ultrasonography
 복부초음파 : 담낭과췌장 Gallbladder & Pancreas Ultrasonography 김정훈 Department of Radiology 1 Interaction of sound with matter (1) 반사 (Reflection) (2) 굴절 (Refraction) (3) 흡수 (Absorption) (4) 산란 (Scattering) 음향저항
복부초음파 : 담낭과췌장 Gallbladder & Pancreas Ultrasonography 김정훈 Department of Radiology 1 Interaction of sound with matter (1) 반사 (Reflection) (2) 굴절 (Refraction) (3) 흡수 (Absorption) (4) 산란 (Scattering) 음향저항
Biliary Tract Neoplasia: A Cyto-histologic Review. Michelle Reid, MD, MSc Professor of Pathology Director of Cytopathology Emory University Hospital
 Biliary Tract Neoplasia: A Cyto-histologic Review Michelle Reid, MD, MSc Professor of Pathology Director of Cytopathology Emory University Hospital Bile Duct Brushings (BDB) BDBs are the initial diagnostic
Biliary Tract Neoplasia: A Cyto-histologic Review Michelle Reid, MD, MSc Professor of Pathology Director of Cytopathology Emory University Hospital Bile Duct Brushings (BDB) BDBs are the initial diagnostic
Patient History. A 58 year old man presents with a 16 mm cyst in the pancreatic tail. The cyst is unilocular with a thick wall and no mural nodule.
 Case 1 Martha Bishop Pitman, MD Director of Cytopathology Massachusetts General Hospital Associate Professor of Pathology Harvard Medical School Boston, MA Patient History A 58 year old man presents with
Case 1 Martha Bishop Pitman, MD Director of Cytopathology Massachusetts General Hospital Associate Professor of Pathology Harvard Medical School Boston, MA Patient History A 58 year old man presents with
GOBLET CELL CARCINOID. Hanlin L. Wang, MD, PhD University of California Los Angeles
 GOBLET CELL CARCINOID Hanlin L. Wang, MD, PhD University of California Los Angeles Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee) in a position to
GOBLET CELL CARCINOID Hanlin L. Wang, MD, PhD University of California Los Angeles Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee) in a position to
GOBLET CELL CARCINOID
 GOBLET CELL CARCINOID Hanlin L. Wang, MD, PhD University of California Los Angeles Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee) in a position to
GOBLET CELL CARCINOID Hanlin L. Wang, MD, PhD University of California Los Angeles Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee) in a position to
Greater Manchester and Cheshire HPB Unit Guidelines for the Assessment & Management of Hepatobiliary and Pancreatic Disease Chapter 14
 Greater Manchester and Cheshire HPB Unit Guidelines for the Assessment & Management of Hepatobiliary and Pancreatic Disease Chapter 14 Contents 14. Neuroendocrine Tumours 161 14.1. Diagnostic algorithm
Greater Manchester and Cheshire HPB Unit Guidelines for the Assessment & Management of Hepatobiliary and Pancreatic Disease Chapter 14 Contents 14. Neuroendocrine Tumours 161 14.1. Diagnostic algorithm
ACG Clinical Guideline: Diagnosis and Management of Pancreatic Cysts
 ACG Clinical Guideline: Diagnosis and Management of Pancreatic Cysts Grace H. Elta, MD, FACG 1, Brintha K. Enestvedt, MD, MBA 2, Bryan G. Sauer, MD, MSc, FACG (GRADE Methodologist) 3 and Anne Marie Lennon,
ACG Clinical Guideline: Diagnosis and Management of Pancreatic Cysts Grace H. Elta, MD, FACG 1, Brintha K. Enestvedt, MD, MBA 2, Bryan G. Sauer, MD, MSc, FACG (GRADE Methodologist) 3 and Anne Marie Lennon,
Pancreatico-biliary cytology: a practical approach to diagnosis. Corina Cotoi
 Pancreatico-biliary cytology: a practical approach to diagnosis Corina Cotoi Pancreatico-biliary lesions Solid: Ductal adenocarcinoma Cholangiocarcinoma Acinar cell carcinoma Neuroendocrine tumour / carcinoma
Pancreatico-biliary cytology: a practical approach to diagnosis Corina Cotoi Pancreatico-biliary lesions Solid: Ductal adenocarcinoma Cholangiocarcinoma Acinar cell carcinoma Neuroendocrine tumour / carcinoma
Neoplasia 2018 Lecture 2. Dr Heyam Awad MD, FRCPath
 Neoplasia 2018 Lecture 2 Dr Heyam Awad MD, FRCPath ILOS 1. List the differences between benign and malignant tumors. 2. Recognize the histological features of malignancy. 3. Define dysplasia and understand
Neoplasia 2018 Lecture 2 Dr Heyam Awad MD, FRCPath ILOS 1. List the differences between benign and malignant tumors. 2. Recognize the histological features of malignancy. 3. Define dysplasia and understand
Tumors of kidney and urinary bladder
 Tumors of kidney and urinary bladder Overview of kidney tumors Benign and malignant Of the benign: papillary adenoma -cortical -small (0.5cm) -in 40% of population -clinically insignificant The most common
Tumors of kidney and urinary bladder Overview of kidney tumors Benign and malignant Of the benign: papillary adenoma -cortical -small (0.5cm) -in 40% of population -clinically insignificant The most common
Recommendations for the Reporting of Pancreatic Specimens Containing Malignant Tumors
 AJCP / REPORTING RECOMMENDATIONS FOR PANCREATIC SPECIMENS CONTAINING MALIGNANT TUMORS Recommendations for the Reporting of Pancreatic Specimens Containing Malignant Tumors Jorge AlboresSaavedra, David
AJCP / REPORTING RECOMMENDATIONS FOR PANCREATIC SPECIMENS CONTAINING MALIGNANT TUMORS Recommendations for the Reporting of Pancreatic Specimens Containing Malignant Tumors Jorge AlboresSaavedra, David
Team approach is essential incorporating: radiology, gastroenterology, surgery and pathology Successful performance is operator dependent
 Committee V Post Brushing and FNA Testing Managment Options Daniel Kurtycz, M.D. Chair Committee V Committee V - Post brushing and FNA management options Team approach is essential incorporating: radiology,
Committee V Post Brushing and FNA Testing Managment Options Daniel Kurtycz, M.D. Chair Committee V Committee V - Post brushing and FNA management options Team approach is essential incorporating: radiology,
Hepatobiliary and Pancreatic Malignancies
 Hepatobiliary and Pancreatic Malignancies Gareth Eeson MD MSc FRCSC Surgical Oncologist and General Surgeon Kelowna General Hospital Interior Health Consultant, Surgical Oncology BC Cancer Agency Centre
Hepatobiliary and Pancreatic Malignancies Gareth Eeson MD MSc FRCSC Surgical Oncologist and General Surgeon Kelowna General Hospital Interior Health Consultant, Surgical Oncology BC Cancer Agency Centre
Dr Claire Smith, Consultant Radiologist St James University Hospital Leeds
 Dr Claire Smith, Consultant Radiologist St James University Hospital Leeds Imaging in jaundice and 2ww pathway Image protocol Staging Limitations Pancreatic cancer 1.2.4 Refer people using a suspected
Dr Claire Smith, Consultant Radiologist St James University Hospital Leeds Imaging in jaundice and 2ww pathway Image protocol Staging Limitations Pancreatic cancer 1.2.4 Refer people using a suspected
Kidney Case 1 SURGICAL PATHOLOGY REPORT
 Kidney Case 1 Surgical Pathology Report February 9, 2007 Clinical History: This 45 year old woman was found to have a left renal mass. CT urography with reconstruction revealed a 2 cm medial mass which
Kidney Case 1 Surgical Pathology Report February 9, 2007 Clinical History: This 45 year old woman was found to have a left renal mass. CT urography with reconstruction revealed a 2 cm medial mass which
Kenneth D. Chi, MD Medical Director GI Lab Advocate Lutheran General Hospital
 Kenneth D. Chi, MD Medical Director GI Lab Advocate Lutheran General Hospital Advances in Digestive Health for the Primary Care Physician Symposium May 2, 2015 None Case Presentation Types of Pancreatic
Kenneth D. Chi, MD Medical Director GI Lab Advocate Lutheran General Hospital Advances in Digestive Health for the Primary Care Physician Symposium May 2, 2015 None Case Presentation Types of Pancreatic
5/21/2018. Prostate Adenocarcinoma vs. Urothelial Carcinoma. Common Differential Diagnoses in Urological Pathology. Jonathan I.
 Common Differential Diagnoses in Urological Pathology Jonathan I. Epstein Prostate Adenocarcinoma vs. Urothelial Carcinoma 1 2 NKX3.1 NKX3.1 3 4 5 6 Proposed ISUP Recommendations Option to use PSA as a
Common Differential Diagnoses in Urological Pathology Jonathan I. Epstein Prostate Adenocarcinoma vs. Urothelial Carcinoma 1 2 NKX3.1 NKX3.1 3 4 5 6 Proposed ISUP Recommendations Option to use PSA as a
B. Environmental Factors. a. The major risk factor to papillary thyroid cancer is exposure to ionizing radiation, during the first 2 decades of life.
 B. Environmental Factors. a. The major risk factor to papillary thyroid cancer is exposure to ionizing radiation, during the first 2 decades of life. b. Deficiency of dietary iodine: - Is linked with a
B. Environmental Factors. a. The major risk factor to papillary thyroid cancer is exposure to ionizing radiation, during the first 2 decades of life. b. Deficiency of dietary iodine: - Is linked with a
Chronic pancreatitis mimicking intraductal papillary mucinous neoplasm of the pancreas; Report of tow cases
 Jichi Medical University Journal Chronic pancreatitis mimicking intraductal papillary mucinous neoplasm of the pancreas; Report of tow cases Noritoshi Mizuta, Hiroshi Noda, Nao Kakizawa, Nobuyuki Toyama,
Jichi Medical University Journal Chronic pancreatitis mimicking intraductal papillary mucinous neoplasm of the pancreas; Report of tow cases Noritoshi Mizuta, Hiroshi Noda, Nao Kakizawa, Nobuyuki Toyama,
16 April 2010 Resident Teaching Conference. Pancreatitis. W. H. Nealon, M.D., F.A.C.S. J.J. Smith, M.D., D.W.D.
 16 April 2010 Resident Teaching Conference Pancreatitis W. H. Nealon, M.D., F.A.C.S. J.J. Smith, M.D., D.W.D. Santorini Wirsung anatomy.med.umich.edu/.../ duodenum_ans.html Bud and ductology Ventral pancreatic
16 April 2010 Resident Teaching Conference Pancreatitis W. H. Nealon, M.D., F.A.C.S. J.J. Smith, M.D., D.W.D. Santorini Wirsung anatomy.med.umich.edu/.../ duodenum_ans.html Bud and ductology Ventral pancreatic
LYMPHATIC DRAINAGE AXILLARY (MOSTLY) INTERNAL MAMMARY SUPRACLAVICULAR
 INTERNAL MAMMARY SUPRACLAVICULAR") BREAST LYMPHATIC DRAINAGE AXILLARY (MOSTLY) INTERNAL MAMMARY SUPRACLAVICULAR HISTOLOGY LOBE: (10 in whole breast) LOBULE: (many per lobe) ACINUS/I, aka ALVEOLUS/I: (many per lobule) DUCT(S): INTRA- or
BREAST LYMPHATIC DRAINAGE AXILLARY (MOSTLY) INTERNAL MAMMARY SUPRACLAVICULAR HISTOLOGY LOBE: (10 in whole breast) LOBULE: (many per lobe) ACINUS/I, aka ALVEOLUS/I: (many per lobule) DUCT(S): INTRA- or
Digestive system L 4. Lecturer Dr. Firdous M. Jaafar Department of Anatomy/Histology section
 Digestive system L 4 Lecturer Dr. Firdous M. Jaafar Department of Anatomy/Histology section objectives 1-Describe the structure of liver. 2-Define liver lobule, and identify its zones. 3-Define portal
Digestive system L 4 Lecturer Dr. Firdous M. Jaafar Department of Anatomy/Histology section objectives 1-Describe the structure of liver. 2-Define liver lobule, and identify its zones. 3-Define portal
CELL AND TISSUE INJURY COURSE-II PATHOLOGY LABORATORY. PATHOLOGY of MASS LESIONS and TISSUE DEFECTS -MACROSCOPY Assoc. Professor Rengin Ahıskalı
 CELL AND TISSUE INJURY COURSE-II PATHOLOGY LABORATORY PATHOLOGY of MASS LESIONS and TISSUE DEFECTS -MACROSCOPY Assoc. Professor Rengin Ahıskalı M1 - RENAL TUBERCULOSIS cavitary areas caseous necrosis fibrous
CELL AND TISSUE INJURY COURSE-II PATHOLOGY LABORATORY PATHOLOGY of MASS LESIONS and TISSUE DEFECTS -MACROSCOPY Assoc. Professor Rengin Ahıskalı M1 - RENAL TUBERCULOSIS cavitary areas caseous necrosis fibrous
An Approach to Pancreatic Cysts. Introduction
 An Approach to Pancreatic Cysts Nalini M. Guda, MD Aurora St. Luke s Medical Center, Milwaukee Clinical Adjunct Professor of Medicine, University of Wisconsin School of Medicine and Public Health Introduction
An Approach to Pancreatic Cysts Nalini M. Guda, MD Aurora St. Luke s Medical Center, Milwaukee Clinical Adjunct Professor of Medicine, University of Wisconsin School of Medicine and Public Health Introduction
Female Genital Tract Lab. Dr. Nisreen Abu Shahin Assistant Professor of Pathology University of Jordan
 Female Genital Tract Lab Dr. Nisreen Abu Shahin Assistant Professor of Pathology University of Jordan Ovarian Pathology A 20-year-old female presented with vague left pelvic pain. Pelvic exam revealed
Female Genital Tract Lab Dr. Nisreen Abu Shahin Assistant Professor of Pathology University of Jordan Ovarian Pathology A 20-year-old female presented with vague left pelvic pain. Pelvic exam revealed
Pancreatic Cytopathology: The Solid Neoplasms
 Pancreatic Cytopathology: The Solid Neoplasms Syed Z. Ali, M.D. Professor of Pathology and Radiology Director of Cytopathology The Johns Hopkins Hospital Baltimore, Maryland Pancreatic Cytopathology: Past,
Pancreatic Cytopathology: The Solid Neoplasms Syed Z. Ali, M.D. Professor of Pathology and Radiology Director of Cytopathology The Johns Hopkins Hospital Baltimore, Maryland Pancreatic Cytopathology: Past,
Basement membrane in lobule.
 Bahram Memar, MD Basement membrane in lobule. Normal lobule-luteal phase Normal lobule-follicular phase Lactating breast Greater than 95% are adenocarcinomas in situ carcinomas and invasive carcinomas.
Bahram Memar, MD Basement membrane in lobule. Normal lobule-luteal phase Normal lobule-follicular phase Lactating breast Greater than 95% are adenocarcinomas in situ carcinomas and invasive carcinomas.
Combatting Pancreatic Cancer: Keys to Early Recognition and Diagnosis
 Transcript Details This is a transcript of an educational program accessible on the ReachMD network. Details about the program and additional media formats for the program are accessible by visiting: https://reachmd.com/programs/clinicians-roundtable/combatting-pancreatic-cancer-keys-earlyrecognition-and-diagnosis/7286/
Transcript Details This is a transcript of an educational program accessible on the ReachMD network. Details about the program and additional media formats for the program are accessible by visiting: https://reachmd.com/programs/clinicians-roundtable/combatting-pancreatic-cancer-keys-earlyrecognition-and-diagnosis/7286/
5/2/2018. Low Grade Dysplasia of GI Tract. High Grade Dysplasia of GI Tract. Dysplasia in Gastrointestinal Tract: Practical Pearls and Issues
 Dysplasia in Gastrointestinal Tract: Practical Pearls and Issues Arief Suriawinata, M.D. Professor of Pathology and Laboratory Medicine Geisel School of Medicine at Dartmouth Department of Pathology and
Dysplasia in Gastrointestinal Tract: Practical Pearls and Issues Arief Suriawinata, M.D. Professor of Pathology and Laboratory Medicine Geisel School of Medicine at Dartmouth Department of Pathology and
DIABETES MELLITUS: COMPLICATION. Benyamin Makes Dept. of Anatomic Pathology FMUI - Jakarta
 DIABETES MELLITUS: COMPLICATION Benyamin Makes Dept. of Anatomic Pathology FMUI - Jakarta COMPLICATION OF DIABETES Susceptibility to infections including tuberculosis, pneumonia, pyelonephritis, and mucocutaneous
DIABETES MELLITUS: COMPLICATION Benyamin Makes Dept. of Anatomic Pathology FMUI - Jakarta COMPLICATION OF DIABETES Susceptibility to infections including tuberculosis, pneumonia, pyelonephritis, and mucocutaneous
BREAST PATHOLOGY MCQS
 BREAST PATHOLOGY MCQS 1) :The most important factor in breast enlargement during pregnancy is A. stromal edema B. secretion of chorionic gonadotropin C. glandular hyperplasia D. proliferation of stroma
BREAST PATHOLOGY MCQS 1) :The most important factor in breast enlargement during pregnancy is A. stromal edema B. secretion of chorionic gonadotropin C. glandular hyperplasia D. proliferation of stroma
CPC 4 Breast Cancer. Rochelle Harwood, a 35 year old sales assistant, presents to her GP because she has noticed a painless lump in her left breast.
 CPC 4 Breast Cancer Rochelle Harwood, a 35 year old sales assistant, presents to her GP because she has noticed a painless lump in her left breast. 1. What are the most likely diagnoses of this lump? Fibroadenoma
CPC 4 Breast Cancer Rochelle Harwood, a 35 year old sales assistant, presents to her GP because she has noticed a painless lump in her left breast. 1. What are the most likely diagnoses of this lump? Fibroadenoma
Epithelial tumors. Dr. F.F. Khuzin, PhD Dr. M.O. Mavlikeev
 Epithelial tumors Dr. F.F. Khuzin, PhD Dr. M.O. Mavlikeev Epithelial tumors Tumors from the epithelium are the most frequent among tumors. There are 2 group features of these tumors: The presence in most
Epithelial tumors Dr. F.F. Khuzin, PhD Dr. M.O. Mavlikeev Epithelial tumors Tumors from the epithelium are the most frequent among tumors. There are 2 group features of these tumors: The presence in most
PANCREAS DUCTAL ADENOCARCINOMA PDAC
 CONTENTS PANCREAS DUCTAL ADENOCARCINOMA PDAC I. What is the pancreas? II. III. IV. What is pancreas cancer? What is the epidemiology of Pancreatic Ductal Adenocarcinoma (PDAC)? What are the risk factors
CONTENTS PANCREAS DUCTAL ADENOCARCINOMA PDAC I. What is the pancreas? II. III. IV. What is pancreas cancer? What is the epidemiology of Pancreatic Ductal Adenocarcinoma (PDAC)? What are the risk factors
Objectives. Atypical Glandular Cells. Atypical Endocervical Cells. Reactive Endocervical Cells
 2013 California Society of Pathologists 66 th Annual Meeting San Francisco, CA Atypical Glandular Cells to Early Invasive Adenocarcinoma: Cervical Cytology and Histology Christina S. Kong, MD Associate
2013 California Society of Pathologists 66 th Annual Meeting San Francisco, CA Atypical Glandular Cells to Early Invasive Adenocarcinoma: Cervical Cytology and Histology Christina S. Kong, MD Associate
2 to 3% of All New Visceral Cancers Peak Incidence is 6th Decade M:F = 2:1 Grossly is a Bright Yellow, Necrotic Mass with a Pseudocapsule
 GENITOURINARY PATHOLOGY Kathleen M. O Toole, M.D. Renal Cell Carcinoma 2 to 3% of All New Visceral Cancers Peak Incidence is 6th Decade M:F = 2:1 Grossly is a Bright Yellow Necrotic Mass Grossly is a Bright
GENITOURINARY PATHOLOGY Kathleen M. O Toole, M.D. Renal Cell Carcinoma 2 to 3% of All New Visceral Cancers Peak Incidence is 6th Decade M:F = 2:1 Grossly is a Bright Yellow Necrotic Mass Grossly is a Bright
Cytyc Corporation - Case Presentation Archive - March 2002
 FirstCyte Ductal Lavage History: 68 Year Old Female Gail Index: Unknown Clinical History: Negative Mammogram in 1995 6 yrs. later presents with bloody nipple discharge Subsequent suspicious mammogram Suspicious
FirstCyte Ductal Lavage History: 68 Year Old Female Gail Index: Unknown Clinical History: Negative Mammogram in 1995 6 yrs. later presents with bloody nipple discharge Subsequent suspicious mammogram Suspicious
Case Study: #3: Gallbladder Carcinoma?
 Case Study: #3: Gallbladder Carcinoma? By: Megan Wyatt K. SON Wyatt 225 2B1 RDMS, RVT Patient: Male 85 YOA Caucasian Indication: Elevated Alkaline Phosphatase History Annual physical showed elevated alkaline
Case Study: #3: Gallbladder Carcinoma? By: Megan Wyatt K. SON Wyatt 225 2B1 RDMS, RVT Patient: Male 85 YOA Caucasian Indication: Elevated Alkaline Phosphatase History Annual physical showed elevated alkaline
Lesions Mimicking Adenoid Cystic Carcinoma. Diagnostic Problems in Salivary Gland Pathology An Update 5/29/2009
 Diagnostic Problems in Salivary Gland Pathology An Update Lesions Mimicking Adenoid Cystic Carcinoma Stacey E. Mills, M.D. W.S. Royster Professor of Pathology Director of Surgical and Cytopathology University
Diagnostic Problems in Salivary Gland Pathology An Update Lesions Mimicking Adenoid Cystic Carcinoma Stacey E. Mills, M.D. W.S. Royster Professor of Pathology Director of Surgical and Cytopathology University
Pancreas Case Scenario #1
 Pancreas Case Scenario #1 An 85 year old white female presented to her primary care physician with increasing abdominal pain. On 8/19 she had a CT scan of the abdomen and pelvis. This showed a 4.6 cm mass
Pancreas Case Scenario #1 An 85 year old white female presented to her primary care physician with increasing abdominal pain. On 8/19 she had a CT scan of the abdomen and pelvis. This showed a 4.6 cm mass
Surgical Therapy of GEP-NET: An Overview
 Surgical Therapy of GEP-NET: An Overview Pierce K.H Chow MBBS, MMed, FRCSE, FAMS, PhD Professor, Duke-NUS Graduate School of Medicine Senior Consultant Surgeon, Singapore General Hospital Visiting Senior
Surgical Therapy of GEP-NET: An Overview Pierce K.H Chow MBBS, MMed, FRCSE, FAMS, PhD Professor, Duke-NUS Graduate School of Medicine Senior Consultant Surgeon, Singapore General Hospital Visiting Senior
Sonography of Gall Bladder
 Sonography of Gall Bladder Vikram Dogra,MD Professor of Radiology, Urology and BME Director of Ultrasound Associate Chair of Education and Research University of Rochester, NY Objectives Describe the Congenital
Sonography of Gall Bladder Vikram Dogra,MD Professor of Radiology, Urology and BME Director of Ultrasound Associate Chair of Education and Research University of Rochester, NY Objectives Describe the Congenital